
Submitted:
06 June 2024
Posted:
10 June 2024
You are already at the latest version
Abstract
Native infective endocarditis is a global phenomenon, defined by infection of a native heart valve and involving the endocardial surface. The causes and epidemiology of the disease have evolved in recent decades, with a doubling of the average patient age. A higher incidence was observed in patients with implanted cardiac devices that can result in right-sided infection of the tricuspid valve. The microbiology of the disease has also changed. Previously, staphylococci, which are most often associated with health-care contact and invasive procedures, were the most common cause of the disease. Nevertheless, this has now been superseded by streptococci. While innovative diagnostic and therapeutic strategies have emerged, mortality rates have not improved over the past year and remain at 30%, which is higher than for many cancer diagnoses. The lack of randomized trials and logistical constraints impede clinical management, and long-standing controversies such as the use of antibiotic prophylaxis persist. This state of the art review addresses clinical practice, controversies, and strategies to combat this potentially devastating disease.
Keywords:
Infective Endocarditis
; Native Valve Endocarditis
; Vegetation
; gram-positive bacteria
1. Introduction: An Overview of the Epidemiological, Pathophysiological, and Clinical Features of Disease
Infective endocarditis (IE) of the native valve (NVE) is rare, with a frequency of approximately 2 to 10 cases per 100,000 person-years [1,2,3,4]. It is thought to be caused by injury to the endothelial or endocardial lining of the valve. In most cases, the presumed initial event is the lesion of the valvular endothelium or endocardium. This lesion results in the exposure of subendothelial collagen, as well as other matrix molecules, which then serve as a substrate for the formation of a complex conglomerate composed of platelets and fibrins. This process results in the formation of a microthrombotic lesion, which is medically referred to as a sterile vegetation. This can lead to a number of complications. Consequently, bacteria that are present in the circulatory system adhere to and colonize the aforementioned injured structure. A lack of an efficacious response by the host organism to the infection results in the replication of the bacterium within the lesion, which in turn stimulates further platelet and fibrin deposition. This process culminates in the formation of an infected vegetative structure, which is a defining feature of infective endocarditis [4,5].
A review of observational data on infective endocarditis (IE) indicates that the rate of mitral valve involvement is lower than that of the aortic valve. One study reporting the outcomes of 775 patients documented a prevalence of aortic valve involvement of 51%, with 59% of cases classified as prosthetic valve endocarditis (PVE) and 68% classified as invasive endocarditis.[4] In comparison, mitral valve involvement was observed in 30.7%, with PVE representing 29% and invasive endocarditis 35%. In a separate study, the prevalence of aortic valve involvement was 47% and that of mitral valve involvement was 31%. [4]According to the French registry of the Association Pour l’Etude et la Prevention de l’Endocardite Infectieuse, the incidence of IE ranges from 43.8% to 35.4%. Active IE can manifest as native valve endocarditis (NVE) or prosthetic valve endocarditis (PVE). NVE has been estimated to affect around 50% of cases, while PVE affects approximately 10%. The infection can affect a single valve or multiple valves in various combinations, with varying degrees of extension into the heart structures. In some cases, the infection can lead to extensive destructive damage to other valve components. In instances where the aortomitral curtain has been extended or there is a co-occurrence of two or more valves, which occurs in approximately 40% of cases, the mortality rates before and after the procedure increase significantly [4,5]. Figure 1
The vegetative microenvironment is weakly affordable to neutrophils and host defense molecules due to the protective effect it exerts. Vegetations are replete with bacteria at exceedingly high densities, with colony forming units (CFU) numbers in the range of 109 to 1010 per gram of vegetation. These bacteria have been found to facilitate high-grade bacteremia and the subsequent proliferation of the vegetation, which undergoes a transformation from a solid to a liquid state, becoming friable and readily fragmented into the circulation. Four mechanisms account for the majority of clinical manifestations of infective endocarditis. These include valvular destruction, paravalvular extension of infection and heart failure, microvascular and large vessel embolization, and metastatic infection of target organs. The affected organs include the brain, kidneys, spleen, and lungs. Additionally, immunologic phenomena such as hypocomplementemic glomerulonephritis and false positive serologic findings of rheumatoid factor, antineutrophil antibodies, or syphilis occur in response to the three conditions that drive the disease process: (1) high bacterial densities, (2) the growing vegetation, and (3) the friability and fragmentation of the vegetative growth [1,2,3,4,5].
Individuals with heart abnormalities are at an increased risk of developing infectious endocarditis. These abnormalities include congenital malformations such as ventricular septal defect and bicuspid aortic valve, as well as acquired valvular disease, such as degenerative valvular disease, aortic stenosis, and rheumatic heart disease. In contrast to low-income countries where rheumatic heart disease represents the most common predisposing feature for IE, it is unconventional in high-income countries where the most frequent predisposing cardiac conditions are degenerative valvular diseases, congenital valvular abnormalities, and intracardiac devices [3,4,5]. It is of paramount importance to consider non-cardiac risk factors when evaluating patients, which include intravenous drug user, hemodialysis treatment, bad dental hygiene, chronic liver disease, diabetes mellitus, compromised immunity, neoplastic disease, and the presence of indwelling intravascular devices.
Approximately 90% of patients with infective endocarditis present with a fever and a heart murmur, while 75% exhibit both of these symptoms. [1,2,6,7]. Acute infective endocarditis in situ is known to manifest with a rapidly progressive course, which may, on occasions, be complicated by congestive heart failure, stroke, systemic or pulmonary embolization, severe sepsis or septic shock. Alternatively, it may manifest subacutely with nonspecific symptoms such as low-grade fever, malaise, chills, sweats, dyspnea, back pain, arthralgias, and weight loss over a period of weeks or sometimes months. Furthermore, it should be acknowledged that microembolic or immunologic events such as splinter hemorrhages, conjunctival hemorrhages, Osler nodes, Janeway lesions, and Roth spots may be present in approximately 5 to 10% of cases [5].
2. Microbiological Characteristics
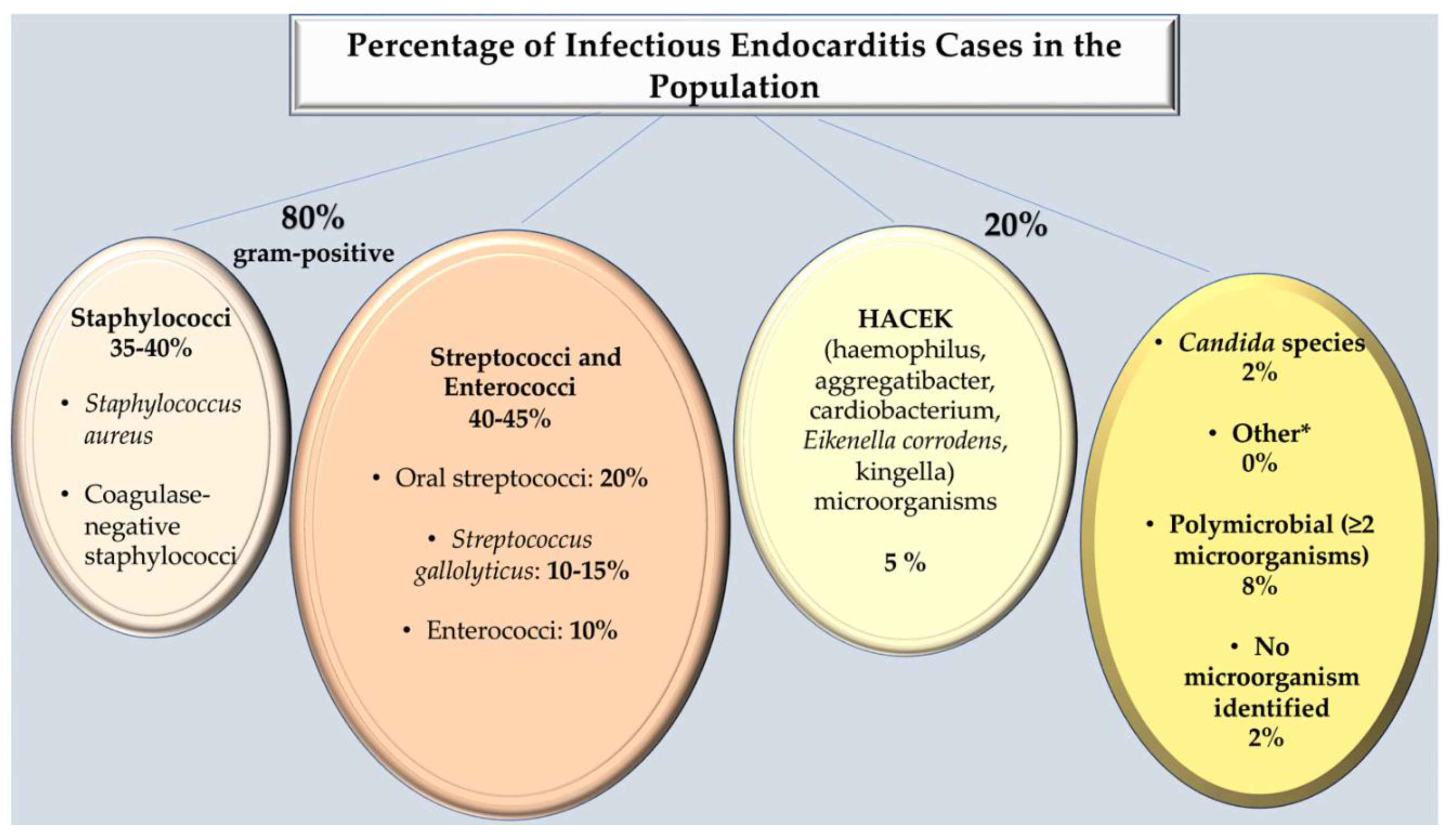
It is estimated that gram-positive bacteria account for approximately 80% of cases of NVE worldwide. In the majority of cases of native-valve infective endocarditis, bacteria are identified. These may include staphylococci (such as Staphylococcus aureus) in 35-40% of cases, streptococci (such as viridans streptococci, which are present in approximately 20% and Streptococcus gallolyticus, previously identified as S. bovis, which is found in approximately 15%) or enterococci (which are present in approximately 10%) [1,2,3,4]. It would be remiss of us not to mention that coagulase-negative staphylococci, a common cause of prosthetic-valve infective endocarditis, are uncommon in native-valve infective endocarditis, except for S. lugdunensis, which may be similar to S. aureus in terms of clinical presentation. It is important to note that in 5% of cases, HACEK species are isolated, including Haemophilus species, Aggregatibacter (formerly Actinobacillus] species, Cardiobacterium species, Eikenella corrodens, and Kingella species. In addition, fungi, polymicrobial infections, and in very rare instances, aerobic gram-negative bacilli are also identified. [1,2,3,8,9,10]
Figure 2.
Percentage of Infectious Endocarditis Cases in the Population. *Includes small numbers of Enterobacteriaceae, Propionibacterium acnes, Coxiella burnetii, Bartonella quintana, Tropheryma whipplei, Gordonia bronchialis, Bacillus spp, Erysipelothrix rhusiopathiae, Neisseria elongata, Moraxella catarrhalis, Veillonella spp, Listeria monocytogenes, Acinetobacter ursingii, Campylobacter fetus, Francisella tularensis, and Pseudoonas aeruginosa, Lactobacillus spp, Corynebacterium spp, Catabacter hongkongensi. Ref [1,2,3,4,5,6,7,8,9,10].
Figure 2.
Percentage of Infectious Endocarditis Cases in the Population. *Includes small numbers of Enterobacteriaceae, Propionibacterium acnes, Coxiella burnetii, Bartonella quintana, Tropheryma whipplei, Gordonia bronchialis, Bacillus spp, Erysipelothrix rhusiopathiae, Neisseria elongata, Moraxella catarrhalis, Veillonella spp, Listeria monocytogenes, Acinetobacter ursingii, Campylobacter fetus, Francisella tularensis, and Pseudoonas aeruginosa, Lactobacillus spp, Corynebacterium spp, Catabacter hongkongensi. Ref [1,2,3,4,5,6,7,8,9,10].
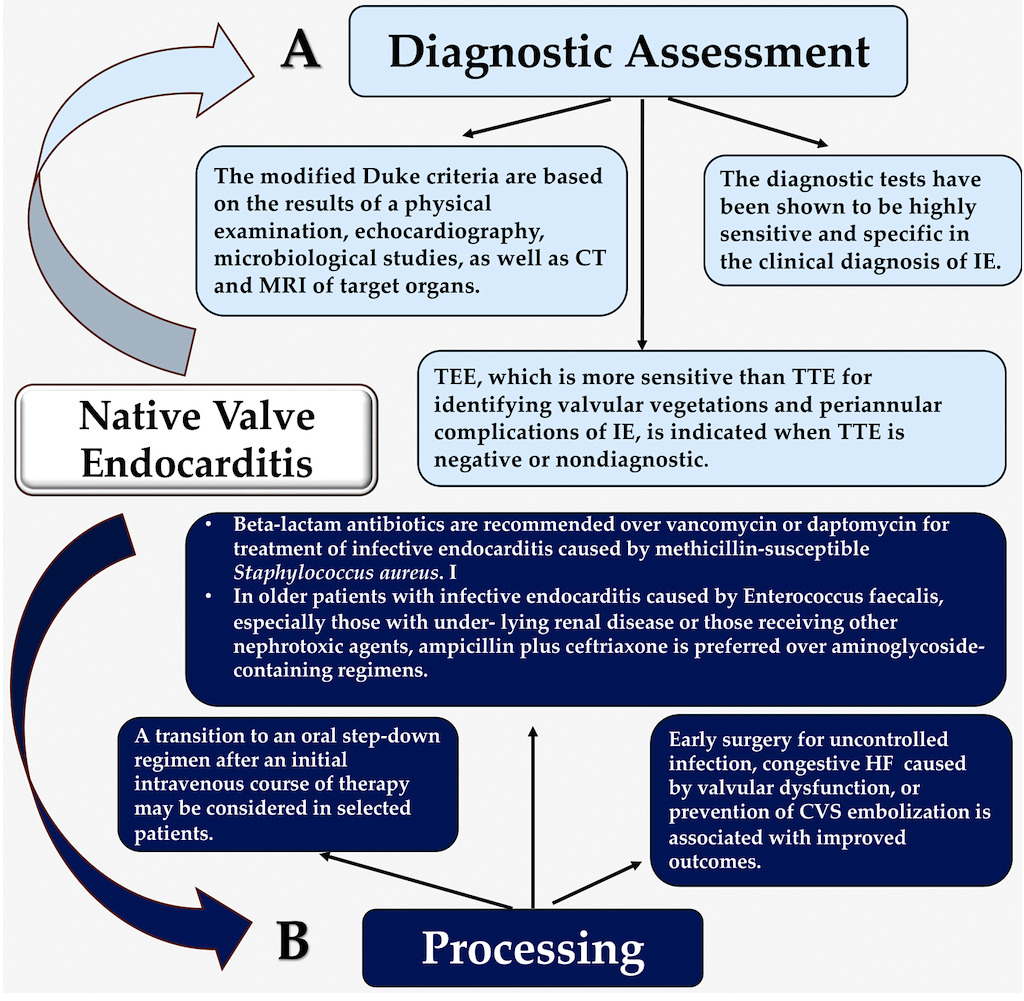
3. Strategy Assessment and Proof of Concept
The modified Duke criteria serve as the fundamental basis for the diagnosis of IE. If the infective pathogens are identified by histological analysis or culture of the vegetations, intracardiac abscesses, or peripheral emboluses, a final pathological diagnosis can be made. Alternatively, a confirmed pathological diagnosis can be made if the histologic evidence of vegetation or intracardiac abscess is validated by an analysis that demonstrates active endocarditis.[11,12,13] The diagnosis of infective endocarditis is made on the basis of a combination of both objective and subjective criteria, which are derived from microbiologic, echocardiographic, and clinical data With regard to sensitivity, it is possible to estimate that the modified Duke criteria for infective endocarditis are approximately 80% effective for cases that are definitively diagnosed and higher if possible cases are included. This is based on data from landmark studies by Habib and colleagues [14] and Li and colleagues [15]. In their observations, Habib et al. [14] determined that 24% of patients who had been definitively diagnosed with IE continued to be incorrectly classified as "possible IE," particularly when culture-negative and Q fever were suspected. They recommended that the diagnostic value of echographic criteria be increased in patients who had received prior antibiotic treatment, exhibited typical echocardiographic findings, and considered the serologic diagnosis of Q fever as an important criterion for IE diagnosis. This could further enhance the clinical diagnosis of IE. A study conducted by Li and colleagues [15] underscores the importance of validating diagnostic criteria, such as those proposed by Duke. Although the sensitivity and specificity of Duke's criteria for diagnosing IE have been validated by investigators in Europe and North America, several limitations remain. The Duke IE database, which contains >800 cases of both confirmed and probable IE from 1984 onward, provides valuable insights into the effectiveness of this approach. In addition, databases on echocardiograms and patients with Staphylococcus aureus bacteremia at Duke University Medical Center are also maintained. Our experience with the Duke criteria in clinical practice, analyses of these databases and of the work of others have led to the proposal that the following modifications be made to the Duke schema: the category "possible IE" should be redefined as having at least 1 major criterion and 1 minor criterion or 3 minor criteria. In light of the widespread use of transesophageal echocardiography (TEE) and the increasing prevalence of S. aureus bacteremia, it seems prudent to eliminate the minor criterion "echocardiogram consistent with IE but not meeting major criterion." Furthermore, given that bacteremia due to S. aureus is now recognized as a major criterion in the absence of either a nosocomially acquired infection or a removable source of infection, it would be advantageous to consider this as such. Similarly, positive Q-fever serology should be elevated to the status of a major criterion, given that it is a well-established risk factor for IE.
It should be noted that the aforementioned criteria exhibit diminished sensitivity when employed in the context of infections associated with prosthetic valves or cardiac devices. These infections are particularly challenging to diagnose and include those developing in the right side of the heart and those presenting with culture-negative infective endocarditis. [10,14,16,17,18] In the case of non-compliance with the criteria for either definite or probable infective endocarditis, the negative predictive value is approximately 90 percent.
Blood cultures represent a crucial diagnostic tool for the identification and treatment of infective endocarditis. Moreover, they fulfill a primary criterion established by the Duke criteria. The choice and dosing of antimicrobial agents largely depend on the blood culture isolate and its antimicrobial susceptibility profile. In approximately 90 to 95% of cases of NVE, a positive blood culture result is observed. In order to optimize recovery of a pathogen, a strategy involving the acquisition of three distinct sets of blood cultures at 30-minute intervals before the administration of antibiotics has proven to be effective. [1,19,20] The administration of antimicrobial therapies represents the most common cause of a negative blood culture result. Other potential etiological agents that can lead to a negative blood culture result include those pathogens that are unable to grow effectively or at all within the conventional parameters of standard blood culture media. These include Bartonella species, Coxiella burnetii, Tropheryma whipplei, and Legionella. [1,4,21]. Another factor that can result in a negative blood culture result is suboptimal specimen collection. [22]
Should a blood culture yield negative results, it is advisable to proceed with serologic and molecular testing for pathogens that are likely to be responsible. This testing is guided by epidemiological clues, such as the association between C. burnetii infection and exposure to farm animals, and between B. quintana infection and homelessness .
In adults, Bartonella spp. has emerged as the most common cause of blood culture-negative IE. The clinical manifestation, as well as the pathological findings observed upon renal biopsy in patients diagnosed with Bartonella infection-associated glomerulonephritis, exhibit subtle distinctions and distinctive characteristics, when compared to other bacterial pathogens associated with glomerulonephritis . The two most commonly implicated species causing IE in humans are Bartonella henselae and Bartonella quintana. [23,24] A subacute presentation, which primarily affects damaged native and/or prosthetic heart valves, is often accompanied by high titers of anti-neutrophil cytoplasmic antibodies, with the majority targeting proteinase-3 specificity. The bacteria are also fastidious and lack positive blood cultures. In addition, there is a higher frequency of focal glomerular crescents compared to other bacterial infection-related glomerulonephritis , a distinctive feature of Bartonella IE-associated glomerulonephritis. C3-dominant immunofluorescence staining is frequently observed, although C1q and IgM staining is also present. [23,24]
The study conducted by Kitamura and colleagues [25] revealed that a full-house immunofluorescence staining pattern has been observed in other cases, including those of infectious granulomatous nephritis caused by bacteria other than those associated with IE. The clinical presentation is characterized by non-specific generalized symptoms, cytopenia, heart failure, and organ damage due to embolic phenomena. These features require a multidisciplinary approach to management. It is crucial to be aware of the recently updated modified Duke criteria for IE, to have a high index of suspicion for underlying infection despite negative microbiologic cultures, to consider a history of exposure to animals, particularly cats, infected with Bartonella spp., and to utilize send-out serologic tests for Bartonella spp. early in the course of management in order to facilitate early diagnosis and initiate appropriate treatment. [21,23,24,25]
Molecular diagnostics are conducted via the amplification of nucleic acids through polymerase chain reaction (PCR) technology, which can be achieved through the utilisation of either specific primers for a particular species or genus, or broad-range primers that target 16S ribosomal RNA (rRNA) gene for the detection of bacterial pathogens or 18S rRNA gene for the identification of fungal pathogens. With regard to PCR-based diagnostic tests, sensitivities have been reported to range from approximately 33 to 90%, while specificities are estimated to lie between approximately 77 and 100%. These in vitro results have been documented by Fournier et al [21] and Liesman et al. [26] Next-generation sequencing technology, which is expected to be more accurate than polymerase chain reaction based approaches, is anticipated to gain prominence in the coming years. For molecular assays, the preferred specimen is an excised valve or vegetable. In cases where the pathogen is difficult to determine, plasma DNA amplification assays may facilitate microbial diagnosis.
Echocardiography is a fundamental diagnostic and management vehicle in the evaluation and treatment of infective endocarditis. [27,28,29,30,31,32,33] Transthoracic echocardiography (TTE) exhibits a sensitivity for detecting vegetations in native-valve infective endocarditis ranging between 50 and 60%. However, TEE has an enhanced sensitivity, with a reported range of 90% or higher. [13,14,15] Approximately 95% of the characteristics of the two are identical. Given that TTE has lower sensitivity in identifying intracardiac complications (e.g., paravalvular abscess), TEE is the preferred imaging modality to exclude infectious process in individuals suspected to have this condition and to assess for intracardiac complicating advents. [10,27,28]
Among the more recent developments in imaging technology, the 18F-fluorodeoxyglucose cardiac positron-emission tomography (PET) and computed tomography (CT) combination represents one of the most extensively researched techniques. [34,35] PET-CT is the most suitable method for the diagnosis and evaluation of prosthetic-valve infective endocarditis. It is noteworthy that the role of this imaging investigation in native-valve infective endocarditis has not yet been sufficiently evaluated, and its efficacy is yet to be established. [27,28,34,35,36]. The efficacy of specific diagnostic imaging techniques for the detection of IE is presented below. Figure 3
- Clinical Evidence: Imaging Criteria
Infective endocarditis is a complex disease with a high rate of morbidity and mortality during hospitalization. The management of IE is best approached through a multidisciplinary approach, including the formation of a dedicated Endocarditis Team, and by ensuring prompt access to advanced imaging techniques. Patients diagnosed with infective endocarditis should undergo a comprehensive evaluation of their presenting symptoms and a TTE. The objective of this evaluation is to ascertain the presence and development of vegetations affecting one or more leaflets, as well as the extent of the infection in heart and aorta components. This includes the leaflet, annulus, trigones, intervalvular fibrous, left atrium and aortic root, along with the size and function of the left ventricle.
Echocardiography remains the primary imaging technique for the identification of anatomical evidence of infective endocarditis, a condition for which the diagnostic criteria have been established (19,68–70). Furthermore, it is a pivotal criterion in the 2023 Duke-ISCVID IE Criteria [27,32,33,37]. Valvular vegetation is the most common echocardiographic sign of infective endocarditis , but other complications affecting the leaflets of the valves (such as perforation or pseudoaneurysm), the paravalvular structures (such as abscess or fistula), or prosthetic valves (such as valvular dehiscence) can also signal IE [27,28]. TTE has been found to be less sensitive than TEE for the diagnosis of IE. Consequently, TEE is typically required when IE is suspected, particularly in cases involving prosthetic valves, cardiac devices, or suspected complications such as perforation, paravalvular lesions, fistula, and prosthetic-valve dehiscence. These indications are in alignment with recommendations outlined in literature [27,28,29,30,32,33]. A recent study has indicated that the prevalence rate of IE in patients with haematogenous spondylodisciitis may be as high as 33% [37], thus justifying the recommendation of TEE in such cases. Despite the high sensitivity and specificity of TEE, complex clinical scenarios may arise in which echocardiography is incapable of either confirming or ruling out the diagnosis of infective endocarditis. In such circumstances, as well as for all cases of IE in patients with intracardiac implants or a suspected paravalvular extension, the utilization of additional diagnostic techniques may prove advantageous in the establishment of a definitive diagnosis [30].
TEE is a diagnostic tool that assesses the development and progression of abscesses, as well as the mechanism and severity of valve regurgitation. It is noteworthy that TTE demonstrates moderate sensitivity (75%) and specificity (>90%) in the detection of vegetations that confirm suspected native valvular endocarditis. This finding is consistent with the results of previous studies (e.g., [28,30,38]). In the case of subjects presenting negative or equivocal evidence of infection on TTE, yet possessing a high clinical probability of IE, it is recommended that they undergo TEE, given its sensitivity of more than 90%. A negative TEE indicating an absence of vegetations is a reliable indicator of the absence of disease, although, in the event of a high level of clinical suspicion, a repeat examination 7–10 days later is required to confirm the initial negative result. Should this test remain negative, it becomes possible to rule out the diagnosis of IE. Additional echocardiography would not yield any additional useful information. As the test's specificity is not 100% accurate, it is essential to exclude false positives for a more nuanced differential diagnosis [10,18,27,28,30,31,32,38,39,40,41].
In evaluating the development of cardiac lesions, TEE is more sensitive than TTE in detecting significant cardiac abnormalities, such as abscesses, leaflet perforations, and pseudoaneurysms. Consequently, in most instances, TEE should be conducted even in the absence of TTE findings that are sufficiently indicative to permit a definitive diagnosis. Research indicates that the sensitivity of TTE in the context of suspected endocarditis in patients with prosthetic valves is inadequate, with a range of between 36 and 69%. It is thus frequently required [10,18,27,30,32,40,41]. The selection of TEE is of paramount importance when dealing with a heart device infection. Moreover, if complications are suspected, or after completion of treatment for suspected endocarditis, it is necessary to perform a repeat TTE as a baseline for subsequent follow-up. Table 1
It is currently advised that the diagnostic procedure be completed with a CT scan, an 18F-FDG-PET/CT, and a cardiac MRI. In 2023, the ISCVID Working Group included cardiac computed tomography (CCT) as a supplementary imaging modality in the Duke-ISCVID IE Criteria. Although cardiac computed tomography (CCT) has inferior capability for the detection of vegetations compared to echocardiography, it demonstrates enhanced sensitivity in the detection of paravalvular lesions, due to its superior spatial resolution [27,39,40,43].
For example, CCT demonstrated greater efficacy in diagnosing pseudoaneurysm or abscess than TEE, with a sensitivity of 78% versus 69%. However, TEE was found to be more effective than CCT in detecting vegetations, valvular perforations, and paravalvular leakages. The combined use of computed tomography and echocardiography has been demonstrated to exhibit greater sensitivity than either modality alone in the diagnostic assessment of all valvular and paravalvular lesions [27,28,30]. Accordingly, the ISCVID Working Group considers these two imaging modalities to be mutually beneficial in suspected cases of infective endocarditis. Additionally, the use of CCT may serve as a valuable adjunctive technique in instances where TEE is contraindicated or when TEE images are suboptimal due to the effects of calcification or intracardiac implants.
The 2023 Duke-ISCVID IE Criteria now include positron emission CT with 18F-fluorodeoxyglucose ([18F] FDG PET/CT) as an imaging modality. [18F] FDG PET/CT has been demonstrated to outperform echocardiography in the evaluation of prosthetic material, leading to the reclassification of a significant proportion of suspected perivalvular leakage cases from the "possible" to the "definite" category of IE. Given the continued debate surrounding the efficacy of [18F] FDG PET/CT in ruling out infective endocarditis (IE), the International Society of Cardiovascular Disease Investigators (ISCVID) Working Group has prioritized research into the test's positive predictive value. The incorporation of [18F] FDG PET/CT as a primary criterion within the Duke Criteria has been demonstrated to markedly enhance the identification of definitive PVE (pooled sensitivity, 0.86 (0.81-0.89]; pooled specificity, 0.84 (0.79-0.88)) in comparison to echocardiography alone [27,28,44]. In the context of cardiac infections, [18F] FDG PET/CT holds particular significance for the diagnosis of such conditions in patients with intricate cardiac implants, including multiple prosthetic valves, combined aortic valves and grafts, and congenital heart disease [27,28,31,44,45,46].
4. Clinical Use: Antimicrobial Therapies
The recommended antibiotic regimens are based nearly exclusively on observational studies and not on randomized clinical trials. These recommendations are founded upon four underlying standards. The first is the ability of the regimen to kill the pathogen. The second is the administration of a prolonged course of therapy (i.e., weeks rather than days). The third is that the dosage should be intensive to ensure that the patient receives an adequate amount of the drug over the course of treatment. The fourth is source control. In general, a combination of vancomycin and ceftriaxone represents a reasonable empirical therapeutic option for patients with native-valve infective endocarditis, pending the results of cultures [46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. Figure 4 A–D
The application of beta-lactam antibiotics represents the primary mode of definitive therapy for strains that are sensitive to the treatment. In the absence of contraindications, these drugs are the preferred choice over others unless the patient is unable to tolerate them without adverse effects or has a substantiated prompt (type I) hypersensitivity reaction. In the event that a patient develops IE induced by a penicillin-resistant strain of viridans streptococcus, including S. gallolyticus, Abiotrophia species, or Granulicatella species, a combination of penicillin or ceftriaxone plus gentamicin can be employed as a therapeutic option. While vancomycin monotherapy represents an alternative treatment option, it should be acknowledged that its use in this context is less well-established than that of other drugs [46].
For infective endocarditis caused by methicillin-susceptible strains of S. aureus (MSSA), an antistaphylococcal penicillin (e.g., oxacillin) is the medication of preference. Randomized controlled trials have indicated that the combination of an antistaphylococcal penicillin with either gentamicin or rifampin does not result in superior clinical outcomes and is deemed to have an increased risk of adverse events. Consequently, this 2-pronged approach is not recommended [19,20,47,48]. In the event that patients with MSSA are unable to receive penicillin, cefazoline represents a reasonable alternative. This is based on the findings of studies which have demonstrated that cefazolin does not cause adverse reactions in these patients. These studies have also demonstrated the efficacy and tolerability of cefazolin in the treatment of MSSA infection [19,49,50,51]. A significant drawback associated with the antibiotic cefazolin is the potential occurrence of an "inoculum effect." This phenomenon, defined as a rise in the minimum inhibitory concentration (MIC) of the antibiotic in broth culture to 16 μg per milliliter or higher at an inoculum concentration of 5×107 CFU per milliliter (100 times the standard inoculum concentration of approximately 5×105 CFU per milliliter), necessitates careful consideration [52]. It has been demonstrated that the inoculum effect, which may be at least in part attributed to the hydrolysis of cefazolin by staphylococcal penicillinase, may be associated with clinical failure [53].
In the treatment of native-valve infectious endocarditis caused by methicillin-resistant Staphylococcus aureus (MRSA), daptomycin or vancomycin monotherapy is recommended, according to the literature [54,55]. Nevertheless, there is as yet no empirical evidence that the effectiveness of concurrent antibiotic therapy can be demonstrated. A randomized trial was conducted to evaluate the efficacy of vancomycin (or, in eight patients, daptomycin) alone or in combination with an anti-staphylococcal beta-lactam antibiotic (primarily flucloxacillin) for the treatment of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia. This study involved a total of 363 patients, including 42 individuals with infective endocarditis. The results indicated that the concurrent administration of these two medications did not confer any advantage in terms of the primary composite outcome of mortality at 90 days, persistent bacteremia at day 5, microbial relapse, or microbiological treatment failure [56]. In this RCT patients receiving concurrent antibiotic therapy, those who died within 90 days had a higher mortality rate despite the rapid clearance of their blood cultures. Furthermore, these patients experienced a significantly higher incidence of acute kidney injury [56]. Based on anecdotal evidence, combining a second agent (e.g., ceftaroline) with vancomycin or daptomycin may benefit patients who have persistent bacteremia or otherwise do not have a response. Nevertheless, the optimal utilization of concurrent antibiotic therapy remains uncertain [57,58,59].
It is recommended that therapies based on the association of antibiotics be applied in the treatment of enterococcal IE . The standard treatment for decades has been penicillin or ampicillin in combination with a low-dose, synergistic gentamicin. The efficacy of this regimen is constrained by gentamicin toxicity and an increasing prevalence of high-level resistance to gentamicin, which suggests a lack of synergy. Observation data indicates that a six-week treatment regimen of ampicillin and ceftriaxone represents a viable alternative to treat infectious endocarditis caused by ampicillin-susceptible strains of E. faecalis, particularly in the absence of contraindications [19,20,42,49,60]. In instances where the ampicillin–gentamicin combination therapeutic approach is utilized, the results of a two-week combined treatment followed by four to six weeks of ampicillin monotherapy have demonstrated comparable outcomes to those achieved by the standard concurrent antibiotic regimen over an equivalent four-to-six-week treatment duration. Additionally, the ampicillin–gentamicin approach exhibited reduced toxicity. [42,61,62,63].
It is strongly advised that molecular biology be integrated with microbiology in the context of shared decision-making, with the involvement of microbiological specialists. The use of combined intravenous therapy is generally preferred over monotherapy, in order to reduce the likelihood of resistance and to ensure antimicrobial synergism [64]. The laboratory information is encouraging, but the evidence from clinical studies is limited with regard to the use of combination beta-lactam therapy for this indication. Additional investigation is required to ascertain the potential advantages of beta-lactam combination therapy in comparison to monotherapy for the treatment of Gram-positive blood infections. Nevertheless, there is evidence to suggest that combining therapy may be beneficial in cases of bacteremia unresponsive to standard antibiotic treatment [64]. It should be noted that the only exceptions to this rule are S. aureus and E. faecalis, as they are susceptible to methicillin. There are a range of alternative treatment options for infections that have developed resistance to vancomycin, including linezolid, tigecycline and daptomycin [65,66].
Despite the low prevalence of beta-lactamase resistance among Enterococcus faecalis infections, a recent study employed reverse transcription polymerase chain reaction (RT-PCR) to identify the presence of antibiotic resistance genes (CTX-M, Van A, and Van B) within Enterococcus faecalis isolates obtained from children with bacteremia. In stark contrast, the pathogenic Escherichia coli ST131 actively secretes the CTX-M-15 β-lactamase [67]. In the study conducted by Sulainam et al. [67], 91.67% of Enterococcus faecalis isolates demonstrated susceptibility to levofloxacin, 83.33% to amoxicillin and clavulanic acid (Amoxiclav), 66.67% to erythromycin, 58.33% to gentamicin, 50% to ampicillin, and 33.33% to cefotaxime and ceftriaxone, respectively; in contrast, only 25% were sensible to the administration of vancomycin. The findings of the study indicate that 88.89% of the nine vancomycin-resistant isolates were associated with the Van A gene, as determined through real-time PCR analysis (p < 0.001). It is noteworthy that two crucial aspects merit further examination. Firstly, 77.78% of the isolates displayed production of the Van B gene, as identified by real-time PCR (p < 0.001). In a further analysis, it was found that all E. faecalis isolates resistant to cefotaxime and ceftriaxone produced the CTX gene, as detected via real-time PCR (p < 0.001) [67]. Recent research indicates that a considerable number of antibiotic resistance genes in bacteria can be attributed to genetics. It is widely accepted that the transfer of genetic material between bacteria, via transformation and transduction, is responsible for the majority of instances of antibiotic resistance observed in bacterial strains [68,69,70].
In light of the growing prevalence of antibiotic resistance, there has been a surge in interest in microbiological research that focuses on the use of bacterial factors as immunotherapeutic targets. The rationale for focusing on bacterial factors is that they play a significant role in an organism’s ability to colonize, infect, and ultimately cause disease (see [71]). MSCRAMMs have recently attracted significant attention due to their widespread prevalence and distinctive capacity to facilitate the initiation of infection, including endocarditis, in a wide range of pathogens, both traditional and opportunistic [71,72]. Of particular interest is their role in these processes. Unfortunately, complications have arisen in the isolation and definition of MSCRAMMs from E. faecalis, which has yielded limited success due to this microorganism’s inability to adhere to ECM proteins under laboratory growth conditions. This contrasts with the behavior exhibited by its relatives, such as staphylococci and streptococci, which demonstrate enhanced aggressiveness.
5. Clinical Use: Surgical Handling
For patients with native valve endocarditis, the timing of surgery is critical. Both the likelihood of complications and operative mortality and morbidity often increase when surgery is delayed. Unfortunately, most surgeons find that patients with IE are referred to them by cardiologists or other hospitals only after medical therapy has failed, when the patients are in refractory heart failure, or when the patients have experienced a major stroke or multi-system organ failure. In some cases, there is a lack of understanding of the surgical challenges, associated complications, and postoperative clinical outcomes of these cases. Coupled with the difficulty in identifying the causative pathogen, this leads to delays in surgical referral. Patients are offered surgery at a late stage, in a significantly compromised clinical status, and with elevated intraoperative risk. [45,46,73].
The strategy employed in the treatment of IE is of paramount importance for the survival of the affected individual. The decision regarding the optimal timing for the surgical intervention in question is the result of a shared, multidisciplinary deliberation process. A combination of clinical and echocardiographic assessments enables an accurate determination of the location, extent, and severity of the infectious field, which can include the mitral valve or the aortic valve. It is the responsibility of the multidisciplinary team to address three primary concerns: the presence of an uncontrolled infection, heart failure, and the prevention of embolism. [1,4,31,46,73,74,75].A persistently elevated temperature for a period of five to seven days in the absence of a negative blood culture suggests a state of uncontrolled infection, with the concomitant possibility of local abscess, extensive vegetation, a false aneurysm, fistula formation, and dehiscence of a prosthetic valve. In such instances, it is strongly recommended that emergency surgery be performed. By contrast, in instances where the infection is caused by fungi, multidrug-resistant organisms, or Pseudomonas aeruginosa, surgical intervention may be a viable option. [1,4,31,40,41,45,46,73,75].
A prospective cohort study of patients with native-valve infective endocarditis revealed that an indication for surgical intervention, irrespective of the success of the procedure, was an independent predictor of mortality [1,4,31,45,46,73,75,76]. The optimal timing of valve surgery remains poorly defined and is a highly individualized decision that is best made by an experienced multidisciplinary team [75,77]. An RCT examined the efficacy of early surgical intervention during the initial hospitalization period, within 48 hours of randomization in 37 patients, compared to conventional treatment in 39 patients. The trial evaluated patients diagnosed with endocarditis on the left side of the heart, severe valvular regurgitation (without heart failure) and large vegetations (> 10 mm in diameter) [78]. The early surgical intervention demonstrated a notable reduction in the risk of the combined endpoint of in-hospital mortality or embolic events within six weeks following randomization. However, this observed benefit was largely attributed to a decline in the risk of systemic embolism. It is important to note that the trial was limited by the inclusion of a relatively healthy patient population, with few underlying comorbidities. Additionally, the study population was biased towards patients with streptococcal infections and mitral-valve infective endocarditis. The results of two meta-analyses indicate that early surgery, in comparison to conventional therapy (i.e., medical treatment or late surgery after >20 days), is associated with a reduction of mortality from any cause of 40 to 60% [79,80]. However, the optimal method for identifying patients who are most likely to benefit from early valve surgery remains uncertain.
It should be noted that heart failure can result from infection of the mitral or aortic valve, or extensive aortomitral localization of endocarditis with valvular dysfunction. In addition, clinical manifestations and echocardiographic findings may suggest the presence of severe acute regurgitation or obstruction of the valve in the setting of cardiac failure. It is, therefore, important that appropriate medical treatment be administered in a timely manner. In contrast, the presence of pulmonary edema and cardiogenic shock—which are not responsive to medical treatment—may also be observed. Additionally, some patients may present with a fistula into a cardiac chamber or pericardium. In the event that cardiac failure can be managed with medical treatment, elective surgery may be planned. Conversely, urgent surgical intervention is indicated when the degree of cardiac failure is more severe. In the event that the patient exhibits signs of poor hemodynamic tolerance, accompanied by early MV closure or pulmonary hypertension, it is imperative that surgical intervention be promptly initiated. Enterococcus faecalis is responsible for the development of IE, which is caused by bacteria that have a specific mode of reproduction, or biogenesis, that allows them to colonize and cause disease. It is noteworthy that a considerable proportion of IE patients require surgical intervention. Consequently, in order to fully comprehend the severity of disease caused by these bacteria, it is imperative to standardize language and adhere to specific units and metrics. The most commonly encountered strain of enterococcus faecalis is responsible for both native NVE and prosthetic valve endocarditis in elderly patients or those with chronic disease who require a rapid surgical procedure [28,81]. Typical E. faecalis lesions are often progressive, forming large abscess cavities involving one or more valves. In the most aggressive forms of IE, extensive portions of the heart, such as the aortic root, intervalvular fibrosa, and cardiac trigones, are destroyed [9,10,40,42].
In cases where surgical intervention is deemed necessary, the only effective method of preventing embolism is emergency surgery. The following factors increase the risk of embolism: manifestations of cardiac failure, persistent infection or abscess, involvement of the MV or aortomitral junction with vegetations larger than 10 mm, or isolated very large vegetation larger than 15 mm. In the context of therapeutic intervention, the occurrence of any single or multiple embolic episodes within the initial two weeks of treatment is indicative of an inadequately controlled infection [4,18,31,45].
In the context of emergency surgery, the treatment of the infected valve is required within 24 hours following the completion of a diagnostic workup. Patients whose condition is considered urgent should receive surgery within a few days after it is indicated. Elective surgery should be performed after at least one to two weeks of antibiotic therapy. The type of surgery performed depends on the extent of the lesions. When only one leaflet or one scallop is involved, a conservative approach may be considered. However, when there is more extensive involvement of the valve, valve replacement is required [4,18,31,45].
It is therefore evident that the early involvement of an experienced cardiac surgeon is of the utmost importance in order to determine the optimal surgical option and timing, with the aim of providing the best possible outcome for patients with IE. For instance, the incidence of stroke is markedly elevated during the first two weeks of antibiotic therapy and in patients presenting with left-sided infective endocarditis , particularly those exhibiting valvular lesions within the mitral position. The decision to proceed with either a replacement or repair surgery is guided by the extent of the lesions that define the infectious focus. Furthermore, the potential for mitral valve repair in lieu of replacement can only be fully evaluated following a comprehensive discussion among experienced surgeons and echocardiologists [4,31,45].
It has been demonstrated that mitral valve repair can result in improved long-term survival and functional outcome in comparison to valve replacement; as a consequence, a heart team approach has become a crucial element in the success of mitral valve endocarditis treatment. The use of the Society of Thoracic Surgeons (STS) risk scoring system [82,83]can be considered a valid adjunct in discussions with other colleagues, offering a means of objectively defining the operative risk and allowing a more accurate estimation of the intraoperative risk. Infectious disease specialists are likewise essential team members, contributing to the delivery of critical expertise in matters such as the selection of appropriate antibiotics or antifungal agents, as well as their optimal timing and dosage. Furthermore, infectious disease experts can provide invaluable assistance in managing antibiotic-resistant organisms or complications associated with the prolonged use of antibiotics. In addition to the previously mentioned disciplines, the heart team should include experts in internal medicine, nephrology, obstetrics, and geriatrics. It is, therefore, essential that the decision-making derived from a multidisciplinary approach be centred upon the patient’s individual characteristics and that the relative specialist address special circumstances [75,82,83,84].A substantial proportion of individuals diagnosed with endocarditis are drug abusers; as such, a microbiologist should be consulted alongside a counsellor. A multidisciplinary approach to decision-making is evident in this case; however, it should be noted that the individual characteristics of the patient are of the utmost importance, with each relative specialist addressing the special circumstances that may arise in their respective fields. Notably, drug abusers constitute a significant proportion of the endocarditis population [85].Consequently, incorporating the advice of a microbiologist, in addition to specific counseling, into the diagnostic process for these cases is advised, in order to facilitate an appropriate diagnosis and subsequent treatment. It is imperative to consider the specific needs of young women of childbearing age, particularly in the context of valve replacement. In this context, the use of anticoagulants is contraindicated and a more detailed approach to counseling and discussion regarding the strategy for replacement of the valve is required [86,87,88,89,90,91,92]. In a comparable manner, patients who require long-term dialysis should be evaluated by a nephrologist prior to surgical intervention. Furthermore, an appropriate plan regarding the utilization of hemofiltration during the immediate postoperative phase should be established and discussed [4,45,74]. Figure 5
6. A Cursory Examination of Areas of Incertitude
The modified Duke criteria for the clinical diagnosis of IE are not inherently dependent on the results of molecular diagnostic testing. [14,15,28] It will be necessary to consider the role of these methods in diagnosis as their accuracy improves and becomes more widely available.
It remains uncertain whether the use of routine brain magnetic resonance imaging (MRI) in conjunction with other advanced imaging techniques such as PET in combination with CT, or PET-CT results in enhanced diagnostic, therapeutic, and outcome outcomes in patients presenting with NVE. It is established that MRI is a more sensitive technique for the detection of central nervous system injuries than computed CT. In vivo identification of asymptomatic embolic injuries patients with suspected infective endocarditis represents a minor supportive criterion for diagnosis in conjunction with clinical criteria and imaging studies [9,30,34,35,42,75,93]. It has been proposed that a routine MRI may serve as a method for detecting silent central nervous system injuries in patients who are eligible for valvular surgery [4,31,45,77,91]. Nevertheless, the impact of this approach on clinical outcomes remains to be determined.
The existing body of data from RCTs does not permit a clear understanding of the benefits and risks associated with the administration of oral antimicrobial agents in the context of infective endocarditis. A trial, known as the Partial Oral Treatment of Endocarditis (POET) investigation, [94] revealed that in individuals with infective endocarditis on the left aspect of the heart and whose condition had been stabilized, the administration of oral antibiotics after an inaugural course of intravenous antibiotics was noninferior to conventional intravenous antibiotic therapy at the conclusion of six months of follow-up. Subsequent longer-term follow-up did not reveal any adverse consequences of oral step-down therapy [95]. Nevertheless, a mere 20% of the individuals subjected to screening were ultimately enrolled. Additionally, only a small number had a S. aureus infection, with no instances of MRSA. Further information are required in order to elucidate the safety and efficacy of said metodology across a range of clinical setup [96].
The optimal managing timing of surgery for individuals with IE, the circumstances under which surgery should be postponed, and the factors predictive of surgical mortality and poor outcomes require further clarification. The majority of guidelines recommend postponing valve surgery for a minimum of four weeks in patients with substantial embolic central nervous system lesions or intracranial hemorrhage [4,16,19,20,31,45,49,73,74,75]. Nonetheless, it is feasible to proceed with early surgical intervention in carefully selected patients despite these conditions [4,31,45,97]. In patients presenting with small embolic cerebral injuries, those measuring up to a maximum of 2 cm in diameter without evidence of hemorrhage or significant neurological deficits, such an approach is deemed safe. A variety of scoring systems have been devised to anticipate the risk of mortality or postoperative complications in patients with infective endocarditis [82,83,84,98,99,100]; however, several limitations have been identified, including a lack of robust sample sizes, the reliance on retrospective data, the necessity to consider changes in surgical practice over time (which may extend over several decades), and a lack of large-scale external validation. Consequently, it has proven challenging to assess the accuracy of these systems.
7. How Should We Interpret the Guidelines?
Each of the American Heart Association, the European Society of Cardiology, the Japanese Society of Cardiology, and the American Association for Thoracic Surgery has published guidelines for the diagnosis and management of IE [19,20,27,28,49,75,77]. The aforementioned guidelines are, for the most part, concordant in their recommendations, though there are a few differences of note, particularly in regard to antimicrobial therapy, imaging modalities, and indications for and timing of surgical procedures. The recommendations set forth herein are generally consistent with the aforementioned guidance. Table 2
8. Conclusions
From the perspective of purely clinical indicators, the coexistence of bacteremia and a murmur in a febrile patient strongly points towards the potential presence of NVE. Upon initial assessment, patients must undergo investigation in order to ascertain the fulfilment of at least three of the established Duke criteria, which include fever, the isolation of two distinct bacterial cultures indicative of the causative pathogen, and, in the case of elderly individuals, the presence of a primary focus of pyelonephritis, which often occurs in conjunction with IE caused by Enterococcus faecalis. Nevertheless, it is possible that the patients did not meet the criteria for a major condition. Furthermore, the presence of aortic stenosis, a preexisting cardiac condition, further supports the possibility of endocarditis.
In order to meet the criteria for a diagnosis of infective endocarditis—persistent positive blood culture(s)—it would be prudent to obtain an additional blood culture(s). It is imperative that an echocardiogram be conducted as soon as possible to accurately diagnose the nature of the valvular lesion, determine the presence of vegetations, and ascertain the extent of any complications associated with infective endocarditis. Despite the greater sensitivity of TEE for identifying valvular vegetation and paravalvular complications, it is prudent to commence with TTE, as its noninvasive nature, ease of implementation, and superior myocardial function information (e.g., ejection fraction) render it a superior choice. In the event that a TTE is found to be either negative or inconclusive, a TEE should be conducted, given the strong suspicion that the patient may be suffering from infective endocarditis. In the event that TEE is non-diagnostic and the suspicion for infective endocarditis remains high, it would be advisable to repeat the examination several days later.
A multidisciplinary team would be constituted for the purpose of providing care, with specialists in cardiology, cardiovascular surgery, and infectious disease included among its members. The prompt administration of combination antimicrobial therapy is essential in the treatment of presumptive NVE. In the presence of E. faecalis bacteremia, although the susceptibility of the isolate to gentamicin should be confirmed, the patient’s age, diabetes, and chronic kidney disease place the patient at high risk for acute kidney injury from gentamicin. It is therefore recommended that the initial treatment should be based on the administration of ampicillin and ceftriaxone, in accordance with the relevant clinical protocols. Obtaining blood cultures is essential to confirm the clearance of bacteremia with therapy. Additionally, a meticulous evaluation of the patient is necessary to identify any indications for immediate valve surgery. It is recommended that antimicrobial therapy be continued for a period of six weeks following the conversion of blood cultures to a negative result. It is similarly vital to consider colonoscopy as a potential avenue in the diagnostic pathway. Some evidence suggests that, in a manner analogous to NVE in the elderly population, enterococcal infective endocarditis may be causally related to colonic neoplasms. Nevertheless, additional investigation is necessary to substantiate this correlation [9,42,101,102].
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Nappi, F.; Spadaccio, C.; Mihos, C. Infective endocarditis in the 21st century. Ann Transl Med. 2020, 8, 1620. [Google Scholar] [CrossRef]
- Cahill, T.J.; Prendergast, B.D. Infective endocarditis. Lancet 2016, 387, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Bin Abdulhak, A.A.; Baddour, L.M.; Erwin, P.J.; Hoen, B.; Chu, V.H.; Mensah, G.A.; Tleyjeh, I.M. Global and regional burden of infective endocarditis, 1990 2010: a systematic review of the literature. Glob Heart 2014, 9, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Spadaccio, C.; Dreyfus, J.; Attias, D.; Acar, C.; Bando, K. Mitral endocarditis: A new management framework. J. Thorac. Cardiovasc. Surg. 2018, 156, 1486–1495. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Avtaar Singh, S.S. Host-Bacterium Interaction Mechanisms in Staphylococcus aureus Endocarditis: A Systematic Review. Int J Mol Sci. 2023, 24, 11068. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miró, J.M.; Fowler, V.G., Jr.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; Chambers, S.T.; Chu, V.H.; Tattevin, P.; Olaison, L.; Freiberger, T.; Hurley, J.; Hannan, M.M.; Chu, V.; Hoen, B. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med 2009, 169, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Martuscelli, G.; Bellomo, F.; Avtaar Singh, S.S.; Moon, M.R. Infective Endocarditis in High-Income Countries. Metabolites. 2022, 12, 682. [Google Scholar] [CrossRef] [PubMed]
- Ambrosioni, J.; Hernandez-Meneses, M.; Téllez, A.; Tattevin, P.; Olaison, L.; Freiberger, T.; Hurley, J.; Hannan, M.M.; Chu, V.; Hoen, B.; et al. The changing epidemiology of infective endocarditis in the twenty-first century. Curr Infect Dis Rep 2017, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F. Current Knowledge of Enterococcal Endocarditis: A Disease Lurking in Plain Sight of Health Providers. Pathogens. 2024, 13, 235. [Google Scholar] [CrossRef]
- Nappi, F.; Iervolino, A.; Singh, S.S.A. The New Challenge for Heart Endocarditis: From Conventional Prosthesis to New Devices and Platforms for the Treatment of Structural Heart Disease. Biomed Res Int. 2021, 2021, 7302165. [Google Scholar] [CrossRef]
- Pettersson, G.B.; Hussain, S.T.; Shrestha, N.K.; Gordon, S.; Fraser, T.G.; Ibrahim, K.S.; Blackstone, E.H. Infective endocarditis:an atlas of disease progression for describing, staging, coding, and understanding the pathology. J Thorac Cardiovasc Surg 2014, 147, 1142–1149.e2. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.A.; Witten, J.C.; Lowry, A.M.; Shrestha, N.K.; Blackstone, E.H.; Unai, S.; Pettersson, G.B.; Wierup, P.; Endocarditis Study Group. Isolated mitral valve endocarditis: Patient, disease, and surgical factors that influence outcomes. J Thorac Cardiovasc Surg. 2024, 167, 127–140.e15. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Martínez, A.; Domínguez, F.; Muñoz, P.; Marín, M.; Pedraz, Á.; Fariñas, M.C.; Tascón, V.; de Alarcón, A.; Rodríguez-García, R.; Miró, J.M.; Goikoetxea, J.; Ojeda-Burgos, G.; Escrihuela-Vidal, F.; Calderón-Parra, J.; GAMES investigators. Clinical presentation, microbiology, and prognostic factors of prosthetic valve endocarditis. Lessons learned from a large prospective registry. PLoS One. 2023, 18, e0290998. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Derumeaux, G.; Avierinos, J.F.; Casalta, J.P.; Jamal, F.; Volot, F.; Garcia, M.; Lefevre, J.; Biou, F.; Maximovitch-Rodaminoff, A.; Fournier, P.E.; et al. Value and limitations of the Duke criteria for the diagnosis of infective endocarditis. J Am Coll Cardiol 1999, 33, 2023–2029. [Google Scholar] [CrossRef] [PubMed]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G., Jr.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 2000, 30, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, B.D. Diagnostic criteria and problems in infective endocarditis. Heart 2004, 90, 611–613. [Google Scholar] [CrossRef] [PubMed]
- Madershahian, N.; Strauch, J.T.; Breuer, M.; Bruhin, R.; Straube, E.; Wahlers, T. Polymerase chain reaction amplification as a diagnostic tool in culture-negative multiple-valve endocarditis. Ann Thorac Surg. 2005, 79, e21–e22. [Google Scholar] [CrossRef] [PubMed]
- Mihos, C.G.; Nappi, F. A narrative review of echocardiography in infective endocarditis of the right heart. Ann. Transl. Med. 2020, 8, 1622. [Google Scholar] [CrossRef] [PubMed]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; et al. Infective endocarditis in adults: diag- nosis, antimicrobial therapy, and manage- ment of complications: a scientific state- ment for healthcare professionals from the American HeartAssociation. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; et al. 2015 ESC Guidelines for the man- agement of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC) — endorsed by: Euro- pean Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015, 36, 3075–3128. [Google Scholar]
- Fournier, P.-E.; Gouriet, F.; Casalta, J.-P.; Lepidi, H.; Chaudet, H.; Thuny, F.; Collart, F.; Habib, G.; Raoult, D. Blood culture-negative endocarditis: improving the diagnostic yield using new diagnostic tools. Medicine (Baltimore) 2017, 96, e8392. [Google Scholar] [CrossRef] [PubMed]
- Subedi, S.; Jennings, Z.; Chen, S.C. Laboratory Approach to the Diagnosis of Culture-Negative Infective Endocarditis. Heart Lung Circ. 2017, 26, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Bannon, L.; Choshen, G.; Giladi, M.; Ablin, J. Bartonella endocarditis masquerading as systemic vasculitis with rapidly progressive glomerulonephritis (aka 'Löhlein nephritis'). BMJ Case Rep. 2019, 12, e231413. [Google Scholar] [CrossRef] [PubMed]
- Shahzad, M.A.; Aziz, K.T.; Korbet, S. Bartonella henselae Infective Endocarditis: A Rare Cause of Pauci-Immune Necrotizing Glomerulonephritis-A Case Report. Can J Kidney Health Dis. 2023, 10, 20543581221150554. [Google Scholar] [CrossRef]
- Kitamura, M.; Dasgupta, A.; Henricks, J.; Parikh, S.V.; Nadasdy, T.; Clark, E.; Bazan, J.A.; Satoskar, A.A. Clinicopathological differences between Bartonella and other bacterial endocarditis-related glomerulonephritis - our experience and a pooled analysis. Front Nephrol. 2024, 3, 1322741. [Google Scholar] [CrossRef] [PubMed]
- Liesman, R.M.; Pritt, B.S.; Maleszewski, J.J.; Patel, R. Laboratory diagnosis of infective endocarditis. J Clin Microbiol 2017, 55, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Ajmone Marsan, N.; de Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the management of endocarditis. Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [PubMed]
- Fowler, V.G.; Durack, D.T.; Selton-Suty, C.; Athan, E.; Bayer, A.S.; Chamis, A.L.; Dahl, A.; Di Bernardo, L.; Durante-Mangoni, E.; Duval, X.; et al. The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria. Clin. Infect. Dis. 2023, 77, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Afonso, L.; Kottam, A.; Reddy, V.; Penumetcha, A. Echocardiography in infective endocarditis: state of the art. Curr Cardiol Rep 2017, 19, 127. [Google Scholar] [CrossRef]
- Avtaar Singh, S.S.; Costantino, M.F.; D'Addeo, G.; Cardinale, D.; Fiorilli, R.; Nappi, F. A narrative review of diagnosis of infective endocarditis-imaging methods and comparison. Ann Transl Med. 2020, 8, 1621. [Google Scholar] [CrossRef]
- Nappi, F.; Spadaccio, C.; Moon, M.R. A management framework for left sided endocarditis: a narrative review. Ann Transl Med. 2020, 8, 1627. [Google Scholar] [CrossRef]
- Habib, G.; Badano, L.; Tribouilloy, C.; Vilacosta, I.; Zamorano, J.L.; Galderisi, M.; Voigt, J.U.; Sicari, R.; Cosyns, B.; Fox, K.; Aakhus, S.; European Association of Echocardiography. Recommendations for the practice of echocardiography in infective endocarditis. Eur J Echocardiogr 2010, 11, 202–219. [Google Scholar] [CrossRef] [PubMed]
- Bai, A.D.; Steinberg, M.; Showler, A.; Burry, L.; Bhatia, R.S.; Tomlinson, G.A.; Bell, C.M.; Morris, A.M. Diagnostic accuracy of transthoracic echocardiography for infective endocarditis findings using transesophageal echocardiography as the reference standard: a meta-analysis. J Am Soc Echocardiogr 2017, 30, 639–646.e8. [Google Scholar] [CrossRef]
- Gomes, A.; Glaudemans, A.W.J.M.; Touw, D.J.; et al. Diagnostic value of imaging in infective endocarditis: a systematic review. Lancet Infect Dis 2017, 17, e1–e14. [Google Scholar] [CrossRef]
- Wong, D.; Rubinshtein, R.; Keynan, Y. Alternative cardiac imaging modalities to echocardiography for the diagnosis of infective endocarditis. Am J Cardiol 2016, 118, 1410–1418. [Google Scholar] [CrossRef]
- Scialla, S.; Martuscelli, G.; Nappi, F.; Singh, S.S.A.; Iervolino, A.; Larobina, D.; Ambrosio, L.; Raucci, M.G. Trends in Managing Cardiac and Orthopaedic Device-Associated Infections by Using Therapeutic Biomaterials. Polymers (Basel). 2021, 13, 1556. [Google Scholar] [CrossRef] [PubMed]
- Behmanesh, B.; Gessler, F.; Schnoes, K.; Dubinski, D.; Won, S.Y.; Konczalla, J.; Seifert, V.; Weise, L.; Setzer, M. Infective endocarditis in patients with pyogenic spondylodiscitis: Implications for diagnosis and therapy. Neurosurg. Focus 2019, 46, E2. [Google Scholar] [CrossRef]
- De Castro, S.; Cartoni, D.; d’Amati, G.; Beni, S.; Yao, J.; Fiorell, M.; Gallo, P.; Fedele, F.; Pandian, N.G. Diagnostic accuracy of transthoracic and multiplane transesophageal echocardiography for valvular perforation in acute infective endocarditis: Correlation with anatomic findings. Clin. Infect. Dis. 2000, 30, 825–826. [Google Scholar] [CrossRef] [PubMed]
- Khalique, O.K.; Veillet-Chowdhury, M.; Choi, A.D.; Feuchtner, G.; Lopez-Mattei, J. Cardiac computed tomography in the contemporary evaluation of infective endocarditis. J. Cardiovasc. Comput. Tomogr. 2021, 15, 304–312. [Google Scholar] [CrossRef]
- Nappi, F.; Singh, S.S.A.; Nappi, P.; Spadaccio, C.; Nenna, A.; Gentile, F.; Chello, M. Heart Valve Endocarditis. Surg Technol Int. 2020, 37, 203–215. [Google Scholar]
- Nappi, F.; Spadaccio, C.; Mihos, C.; Shaikhrezai, K.; Acar, C.; Moon, M.R. The quest for the optimal surgical management of tricuspid valve endocarditis in the current era: a narrative review. Ann Transl Med. 2020, 8, 1628. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Avtaar Singh, S.S.; Jitendra, V.; Fiore, A. Bridging Molecular and Clinical Sciences to Achieve the Best Treatment of Enterococcus faecalis Endocarditis. Microorganisms. 2023, 11, 2604. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.; Guittet, L.; Hamon, M.; Hamon, M. Comparative value of cardiac CT and transesophageal echocardiography in infective endocarditis: A systematic review and meta-analysis. Radiol. Cardiothorac. Imaging 2020, 2, e190189. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.K.M.; Sánchez-Nadales, A.; Igbinomwanhia, E.; Cremer, P.; Griffin, B.; Xu, B. Diagnosis of infective endocarditis by subtype using (18)F-fluorodeoxyglucose positron emission tomography/computed tomography: A contemporary meta- analysis. Circ. Cardiovasc. Imaging 2020, 13, e010600. [Google Scholar] [CrossRef] [PubMed]
- Benedetto, U.; Spadaccio, C.; Gentile, F.; Moon, M.R.; Nappi, F. A narrative review of early surgery versus conventional treatment for infective endocarditis: Do we have an answer? Ann. Transl. Med. 2020, 8, 1626. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Singh, S.S.A.; Spadaccio, C.; Acar, C. Revisiting the guidelines and choice the ideal substitute for aortic valve endocarditis. Ann. Transl. Med. 2020, 8, 952. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, S.E.; Vigliani, G.A.; Fowler VGJr Abrutyn, E.; Corey, G.R.; Levine, D.P.; Rupp, M.E.; Chambers, H.F.; Karchmer, A.W.; Boucher, H.W. Initial low-dose gentamicin for Staphylococcus aureus bacteremia and endo- carditis is nephrotoxic. Clin Infect Dis 2009, 48, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Thwaites, G.E.; Scarborough, M.; Szubert, A.; Nsutebu, E.; Tilley, R.; Greig, J.; Wyllie, S.A.; Wilson, P.; Auckland, C.; Cairns, J.; Ward, D.; Lal, P.; Guleri, A.; Jenkins, N.; Sutton, J.; Wiselka, M.; et al. Adjunctive rifampicin for Staphylococcus aureus bacteraemia(ARREST): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2018, 391, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Nakatani, S.; Ohara, T.; Ashihara, K.; Izumi, C.; Iwanaga, S.; Eishi, K.; Okita, Y.; Daimon, M.; Kimura, T.; Toyoda, K.; Nakase, H.; Nakano, K.; Higashi, M.; Mitsutake, K.; et al. JCS 2017 guideline on prevention and treatment of infective endocarditis. Circ J 2019, 83, 1767–1809. [Google Scholar] [CrossRef]
- Rindone, J.P.; Mellen, C.K. Meta-analysis of trials comparing cefazolin to antistaphylococcal penicillins in the treatment of methicillin-sensitive Staphylococcus aureus bacteraemia. Br J Clin Pharmacol. 2018, 84, 1258–1266. [Google Scholar] [CrossRef]
- Weis, S.; Kesselmeier, M.; Davis, J.S.; Morris, A.M.; Lee, S.; Scherag, A.; Hagel, S.; Pletz, M.W. Cefazolin versus anti-staphylococcal penicillins for the treatment ofpatients with Staphylococcus aureus bacteraemia. Clin Microbiol Infect 2019, 25, 818–827. [Google Scholar] [CrossRef] [PubMed]
- Nannini, E.C.; Stryjewski, M.E.; Singh, K.V.; Bourgogne, A.; Rude, T.H.; Corey, G.R.; Fowler, V.G., Jr.; Murray, B.E. Inoculum effect with cefazolin among clinical isolates of methicillin-susceptible Staphylococcus aureus: frequency and possible cause of cefazolin treatment failure. Antimicrob Agents Chemother 2009, 53, 3437–3441. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Seas, C.; Carvajal, L.P.; Diaz, L.; Echeverri, A.M.; Ferro, C.; Rios, R.; Porras, P.; Luna, C.; Gotuzzo, E.; Munita, J.M.; Nannini, E.; Carcamo, C.; Reyes, J.; Arias, C.A. The cefazolin inoculum effect is associ- ated with increased mortality inmethicillin-susceptible Staphylococcus aureus bacteremia. Open Forum Infect Dis 2018, 5, ofy123. [Google Scholar] [CrossRef] [PubMed]
- Fowler, V.G., Jr.; Boucher, H.W.; Corey, G.R.; Abrutyn, E.; Karchmer, A.W.; Rupp, M.E.; Levine, D.P.; Chambers, H.F.; Tally, F.P.; Vigliani, G.A.; Cabell, C.H.; Link, A.S.; DeMeyer, I.; et al. Daptomycin versus standard therapy for bacteremia andendocarditis caused by Staphylococcus aureus. N Engl J Med 2006, 355, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Holland, T.L.; Arnold, C.; Fowler, V.G., Jr. Clinical management of Staphylococcus aureus bacteremia: a review. JAMA 2014, 312, 1330–1341. [Google Scholar] [CrossRef]
- Tong, S.Y.C.; Lye, D.C.; Yahav, D.; Sud, A.; Robinson, J.O.; Nelson, J.; Archuleta, S.; Roberts, M.A.; Cass, A.; Paterson, D.L.; Foo, H.; Paul, M.; Guy, S.D.; Tramontana, A.R.; Walls, G.B.; McBride, S.; Bak, N.; Ghosh, N.; Rogers, B.A.; Ralph, A.P.; Davies, J.; Ferguson, P.E.; et al. Effect of vancomycin or daptomycin with vs without an antistaphylococcal β-lactam on mortality, bacteremia, relapse, or treatment failure in patients with MRSA bacteremia: a randomized clinical trial. JAMA 2020, 323, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Geriak, M.; Haddad, F.; Rizvi, K.; Rose, W.; Kullar, R.; LaPlante, K.; Yu, M.; Vasina, L.; Ouellette, K.; Zervos, M.; Nizet, V.; Sakoulas, G. Clinical data on daptomycin plus ceftaro- line versus standard of care monotherapy in the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob Agents Chemother 2019, 63, e02483-18. [Google Scholar] [CrossRef] [PubMed]
- Gritsenko, D.; Fedorenko, M.; Ruhe, J.J.; Altshuler, J. Combination therapy with vancomycin and ceftaroline forrefractory methicillin-resistant Staphylococcus aureus bacteremia: a case series. Clin Ther 2017, 39, 212–218. [Google Scholar] [CrossRef]
- Holubar, M.; Meng, L.; Deresinski, S. Bacteremia due to methicillin-resistant Staphylococcus aureus: new therapeutic approaches. Infect Dis Clin North Am 2016, 30, 491–507. [Google Scholar] [CrossRef]
- Fernández-Hidalgo, N.; Almirante, B.; Gavaldà, J.; Gurgui, M.; Peña, C.; de Alarcón, A.; Ruiz, J.; Vilacosta, I.; Montejo, M.; Vallejo, N.; López-Medrano, F.; Plata, A.; López, J.; et al. Ampicillin plus ceftriaxone is as effective as ampicillin plus gentamicin for treating enterococcusfaecalis infective endocarditis. Clin Infect Dis 2013, 56, 1261–1268. [Google Scholar] [CrossRef]
- Dahl, A.; Rasmussen, R.V.; Bundgaard, H.; Hassager, C.; Bruun, L.E.; Lauridsen, T.K.; Moser, C.; Sogaard, P.; Arpi, M.; Bruun, N.E. Enterococcus faecalis infective endocarditis: a pilot study of the relationship between duration of gentamicin treatment and outcome. Circulation 2013, 127, 1810–1817. [Google Scholar] [CrossRef] [PubMed]
- Olaison, L.; Schadewitz, K. Enterococcal endocarditis in Sweden, 1995-1999: can shorter therapy with aminoglycosides be used? Clin Infect Dis 2002, 34, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F. Current Knowledge of Enterococcal Endocarditis: A Disease Lurking in Plain Sight of Health Providers. Pathogens. 2024, 13, 235. [Google Scholar] [CrossRef] [PubMed]
- Bartash, R.; Nori, P. Beta-lactam combination therapy for the treatment of Staphylococcus aureus and Enterococcus species bacteremia: A summary and appraisal of the evidence. Int. J. Infect. Dis. 2017, 63, 7–12. [Google Scholar] [PubMed]
- Li, G.; Walker, M.J.; De Oliveira, D.M.P. Vancomycin Resistance in Enterococcus and Staphylococcus aureus. Microorganisms 2022, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Rangama, S.; Lidbury, I.D.E.A.; Holden, J.M.; Borsetto, C.; Murphy, A.R.J.; Hawkey, P.M.; Wellington, E.M.H. Mechanisms Involved in the Active Secretion of CTX-M-15 β-Lactamase by Pathogenic Escherichia coli ST131. Antimicrob. Agents Chemother. 2021, 65, e0066321. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.M.; Hussein, S.A.; Husain, V.I. Detection of Antibiotic Resistance Genes (CTX-M, Van A and Van B) of Enterococcus faecalis Isolated from Children with Bacteremia by RT-PCR. Arch. Razi Inst. 2023, 78, 73–77. [Google Scholar] [CrossRef]
- Almahdawy, O.T.; Pricop, R.; Sadik, O.; Najee, H.; Pircalabioru, G.G.; Marutescu, L.; Czobor Barbu, I.; Banu, O.; Cristea, V.; Grigore, R.; et al. Description of vancomycin resistance genes in Enterococcus sp. clinical strains isolated from Bucharest, Romania. Rom. Biotechnol. Lett. 2019, 24, 395–399. [Google Scholar] [CrossRef]
- Guzman Prieto, A.M.; van Schaik, W.; Rogers, M.R.; Coque, T.M.; Baquero, F.; Corander, J.; Willems, R.J. Global emergence and dissemination of enterococci as nosocomial pathogens: Attack of the clones? Front. Microbiol. 2016, 7, 788. [Google Scholar] [CrossRef]
- Hammerum, A.M.; Justesen, U.S.; Pinholt, M.; Roer, L.; Kaya, H.; Worning, P.; Nygaard, S.; Kemp, M.; Clausen, M.E.; Nielsen, K.L.; et al. Surveillance of vancomycin-resistant enterococci reveals shift in dominating clones and national spread of a vancomycin-variable vanA Enterococcus faecium ST1421-CT1134 clone, Denmark, 2015 to March 2019. Eurosurveillance 2019, 24, 1900503. [Google Scholar] [CrossRef]
- Rivas, J.M.; Speziale, P.; Patti, J.M.; Hook, M. MSCRAMM-targeted vaccines and immunotherapy for staphylococcal infection. Curr. Opin. Drug Discov. Dev. 2004, 7, 223–227. [Google Scholar]
- Marston, H.D.; Dixon, D.M.; Knisely, J.M.; Palmore, T.N.; Fauci, A.S. Antimicrobial resistance. JAMA 2016, 316, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Avtaar Singh, S.S.; Timofeeva, I. Learning From Controversy: Contemporary Surgical Management of Aortic Valve Endocarditis. Clin Med Insights Cardiol. 2020, 14, 1179546820960729. [Google Scholar] [CrossRef] [PubMed]
- Pollari, F.; Spadaccio, C.; Cuomo, M.; Chello, M.; Nenna, A.; Fischlein, T.; Nappi, F. Sharing of decision-making for infective endocarditis surgery: a narrative review of clinical and ethical implications. Ann Transl Med. 2020, 8, 1624. [Google Scholar] [CrossRef] [PubMed]
- Satriano, U.M.; Nenna, A.; Spadaccio, C.; Pollari, F.; Fischlein, T.; Chello, M.; Nappi, F. Guidelines on prosthetic heart valve management in infective endocarditis: a narrative review comparing American Heart Association/American College of Cardiology and European Society of Cardiology guidelines. Ann Transl Med. 2020, 8, 1625. [Google Scholar] [CrossRef]
- Habib, G.; Erba, P.A.; Iung, B.; et al. Clini- cal presentation, aetiology and outcome of infective endocarditis: results of the ESC-EORP EURO-ENDO (European infec- tive endocarditis) registry: a prospective cohort study. Eur Heart J 2019, 40, 3222–3232. [Google Scholar] [CrossRef]
- AATS Surgical Treatment of Infective Endocarditis Consensus Guidelines Writing Committee. 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: surgical treatment of infective endocarditis: executive summary. J Thorac Cardiovasc Surg 2017, 153, 1241–1258. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-H.; Kim, Y.-J.; Kim, S.-H.; et al. Early surgery versus conventional treatment for infective endocarditis. N EnglJ Med 2012, 366, 2466–2473. [Google Scholar] [CrossRef] [PubMed]
- Anantha Narayanan, M.; Mahfood Haddad, T.; Kalil, A.C.; et al. Early versus late surgical intervention or medical manage- ment for infective endocarditis: a system- atic review and meta-analysis. Heart 2016, 102, 950–957. [Google Scholar] [CrossRef]
- Liang, F.; Song, B.; Liu, R.; Yang, L.; Tang, H.; Li, Y. Optimal timing for early surgery in infective endocarditis: a meta-analysis. Interact Cardiovasc Thorac Surg 2016, 22, 336–345. [Google Scholar] [CrossRef]
- Richards, M.J.; Edwards, J.R.; Culver, D.H.; Gaynes, R.P. Nosocomial infections in combined medical surgical intensive care units in the United States. Infect. Control Hosp. Epidemiol. 2000, 21, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Nashef, S.A.; Roques, F.; Michel, P.; et al. European system for cardiac operative risk evaluation (EuroSCORE). European journal of cardio-thoracic surgery. 1999, 16, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Gaca, J.G.; Sheng, S.; Daneshmand, M.A.; et al. Outcomes for endocarditis surgery in North America : a simplified risk scoring system. J Thorac Cardiovasc Surg 2011, 141, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cisneros, A.; Hernández-Meneses, M.; Llopis, J.; Sandoval, E.; Pereda, D.; Alcocer, J.; Barriuso, C.; Castellá, M.; Ambrosioni, J.; Pericàs, J.M.; Vidal, B.; Falces, C.; Ibáñez, C.; Perdomo, J.; Rovira, I.; García-de-la-María, C.; Moreno, A.; Almela, M.; Perisinotti, A.; Dahl, A.; Castro, P.; Miró, J.M.; Quintana, E.; Equip d’Endocarditis de l’Hospital Clínic de Barcelona. Risk scores' performance and their impact on operative decision-making in left-sided endocarditis: a cohort study. Eur J Clin Microbiol Infect Dis. 2023, 42, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Ejiofor, J.I.; Yammine, M.; Ando, M.; Camuso, J.M.; Youngster, I.; Nelson, S.B.; Kim, A.Y.; Melnitchouk, S.I.; Rawn, J.D.; MacGillivray, T.E.; Cohn, L.H.; Byrne, J.G.; Sundt, T.M. , 3rd. Surgical outcomes of infective endocarditis among intravenous drug users. J Thorac Cardiovasc Surg. 2016, 152, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Ejiofor, J.I.; Yammine, M.; Camuso, J.M.; Walsh, C.W.; Ando, M.; et al. Are homografts superior to conventional prosthetic valves in the setting of infective en- docarditis involving the aortic valve? J Thorac Cardiovasc Surg. 2016, 151, 1239–1246. [Google Scholar] [CrossRef]
- Nappi, F.; Spadaccio, C. Simplest solutions are not always the cleverest: Can we stitch in an infected annulus? Should we rethink the current guidelines? J. Thorac. Cardiovasc. Surg. 2017, 154, 1899–1900. [Google Scholar] [CrossRef]
- Nappi, F.; Spadaccio, C. keep fumbling around in the dark when it comes to infective endocarditis, or produce new, reliable data to redesign the guidelines? J. Thorac. Cardiovasc. Surg. 2018, 155, 75–76. [Google Scholar] [CrossRef]
- Nappi, F.; Acar, C. Monobloc or Separate Aortic and Mitral Homografts for Endocarditis of the Intervalvular Fibrosa? Ann. Thorac. Surg. 2021, 112, 1382–1383. [Google Scholar] [CrossRef]
- Nappi, F.; Nenna, A.; Petitti, T.; Spadaccio, C.; Gambardella, I.; Lusini, M.; Chello, M.; Acar, C. Long-term outcome of cryopreserved allograft for aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2018, 156, 1357–1365.e6. [Google Scholar] [CrossRef]
- Olivito, S.; Lalande, S.; Nappi, F.; Hammoudi, N.; D'Alessandro, C.; Fouret, P.; Acar, C. Structural deterioration of the cryopreserved mitral homograft valve. J. Thorac. Cardiovasc. Surg. 2012, 144, 313–320.e1. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Spadaccio, C.; Acar, C. Use of allogeneic tissue to treat infective valvular disease: Has everything been said? J. Thorac. Cardiovasc. Surg. 2017, 153, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Beganovic, M.; Luther, M.K.; Rice, L.B.; Arias, C.A.; Rybak, M.J.; LaPlante, K.L. A review of combination antimicrobial therapy for Enterococcus faecalis bloodstream infections and infective endocarditis. Clin Infect Dis 2018, 67, 30. [Google Scholar] [CrossRef] [PubMed]
- Iversen, K.; Ihlemann, N.; Gill, S.U.; et al. Partial oral versus intravenous antibiotic treatment of endocarditis. N EnglJ Med 2019, 380, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Bundgaard, H.; Ihlemann, N.; Gill, S.U.; et al. Long-term outcomes of partial oral treatment of endocarditis. N Engl JMed 2019, 380, 1373–1374. [Google Scholar] [CrossRef] [PubMed]
- Spellberg, B.; Chambers, H.F.; Musher, D.M.; Walsh, T.L.; Bayer, A.S. Evaluation of a paradigm shift from intravenous antibiotics to oral step-down therapy for the treatment of infective endocarditis: a narrative review. JAMA Intern Med 2020. [Google Scholar] [CrossRef] [PubMed]
- Venn, R.A.; Ning, M.; Vlahakes, G.J.; Wasfy, J.H. Surgical timing in infective endocarditis complicated by intracranial hemorrhage. Am Heart J 2019, 216, 102–112. [Google Scholar] [CrossRef]
- De Feo, M.; Cotrufo, M.; Carozza, A.; et al. The need for a specific risk prediction system in native valve infec- tive endocarditis surgery. Scientific World Journal. 2012, 2012, 307571. [Google Scholar] [CrossRef] [PubMed]
- Chu, V.H.; Park, L.P.; Athan, E.; et al. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis: a prospective study from the International Collaboration on Endocarditis. Circulation 2015, 131, 131–140. [Google Scholar] [CrossRef]
- Okita, Y.; Minakata, K.; Yasuno, S.; et al. Optimal timing of surgery for active infective endocarditis with cerebral complications: a Japanese multicentre study. Eur J Cardiothorac Surg 2016, 50, 374–382. [Google Scholar] [CrossRef]
- Escolà-Vergé, L.; Peghin, M.; Givone, F.; et al. Prevalence of colorectal disease in Enterococcus faecalis: results of an observa- tional multicenter study. Rev Esp Cardiol (Engl Ed) 2019. [Google Scholar]
- Pericàs, J.M.; Corredoira, J.; Moreno, A.; et al. Relationship between Enterococcus faecalis infective endocarditis and colorec- tal neoplasm: preliminary results from a cohort of 154 patients. Rev Esp Cardiol (Engl Ed) 2017, 70, 451–458. [Google Scholar] [PubMed]
Figure 1.
The echocardiographic findings in mitral valve endocarditis are presented. Figure A illustrates a normal mitral valve in two-dimensional transesophageal echocardiography (2D TEE) with the probe rotated to 120°. The thin valve leaflets are visualized in the open position, in mid-diastole, while the aortic valve is closed. The left atrium is not enlarged, and the left ventricle is normal in terms of size and wall thickness. B: Mitral xenograft endocarditis. C: Two-dimensional transesophageal echocardiography displays a vegetation on the atrial aspect of the anterior leaflet. D: Three-dimensional reconstruction of the mitral valve (surgeon’s view) depicts the vegetation in C. Prosthetic valve endocarditis is evident. E &F: The short-axis view (probe angle 59) and the long-axis view (probe angle 120) are presented with and without color-Doppler analysis of a mechanical aortic prosthesis with a posterior semilunar abscess involving the aortomitral junction.
Figure 1.
The echocardiographic findings in mitral valve endocarditis are presented. Figure A illustrates a normal mitral valve in two-dimensional transesophageal echocardiography (2D TEE) with the probe rotated to 120°. The thin valve leaflets are visualized in the open position, in mid-diastole, while the aortic valve is closed. The left atrium is not enlarged, and the left ventricle is normal in terms of size and wall thickness. B: Mitral xenograft endocarditis. C: Two-dimensional transesophageal echocardiography displays a vegetation on the atrial aspect of the anterior leaflet. D: Three-dimensional reconstruction of the mitral valve (surgeon’s view) depicts the vegetation in C. Prosthetic valve endocarditis is evident. E &F: The short-axis view (probe angle 59) and the long-axis view (probe angle 120) are presented with and without color-Doppler analysis of a mechanical aortic prosthesis with a posterior semilunar abscess involving the aortomitral junction.
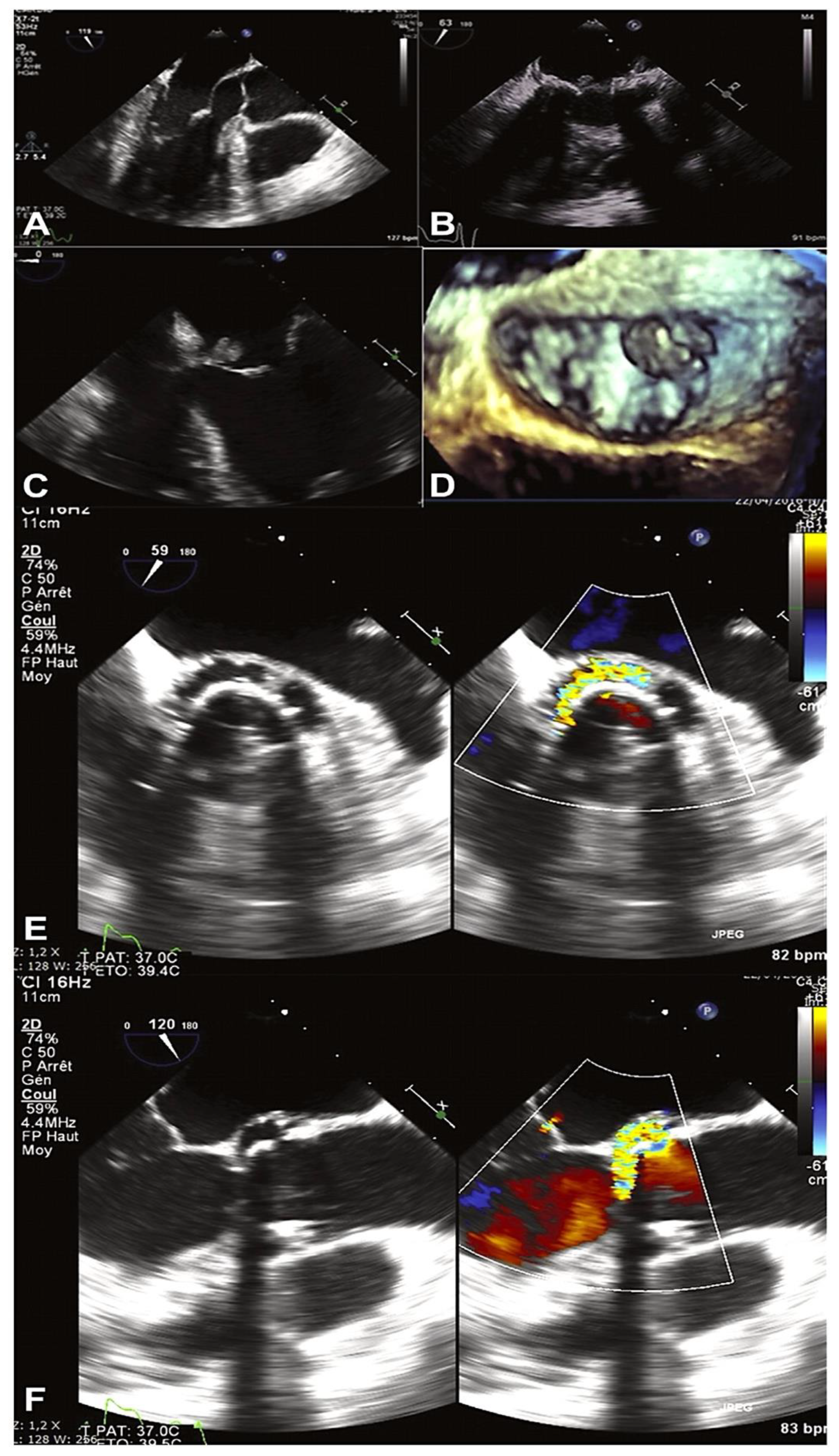
Figure 3.
Clinical evaluation and diagnosis flowchart. Ref 4-16,18-34.
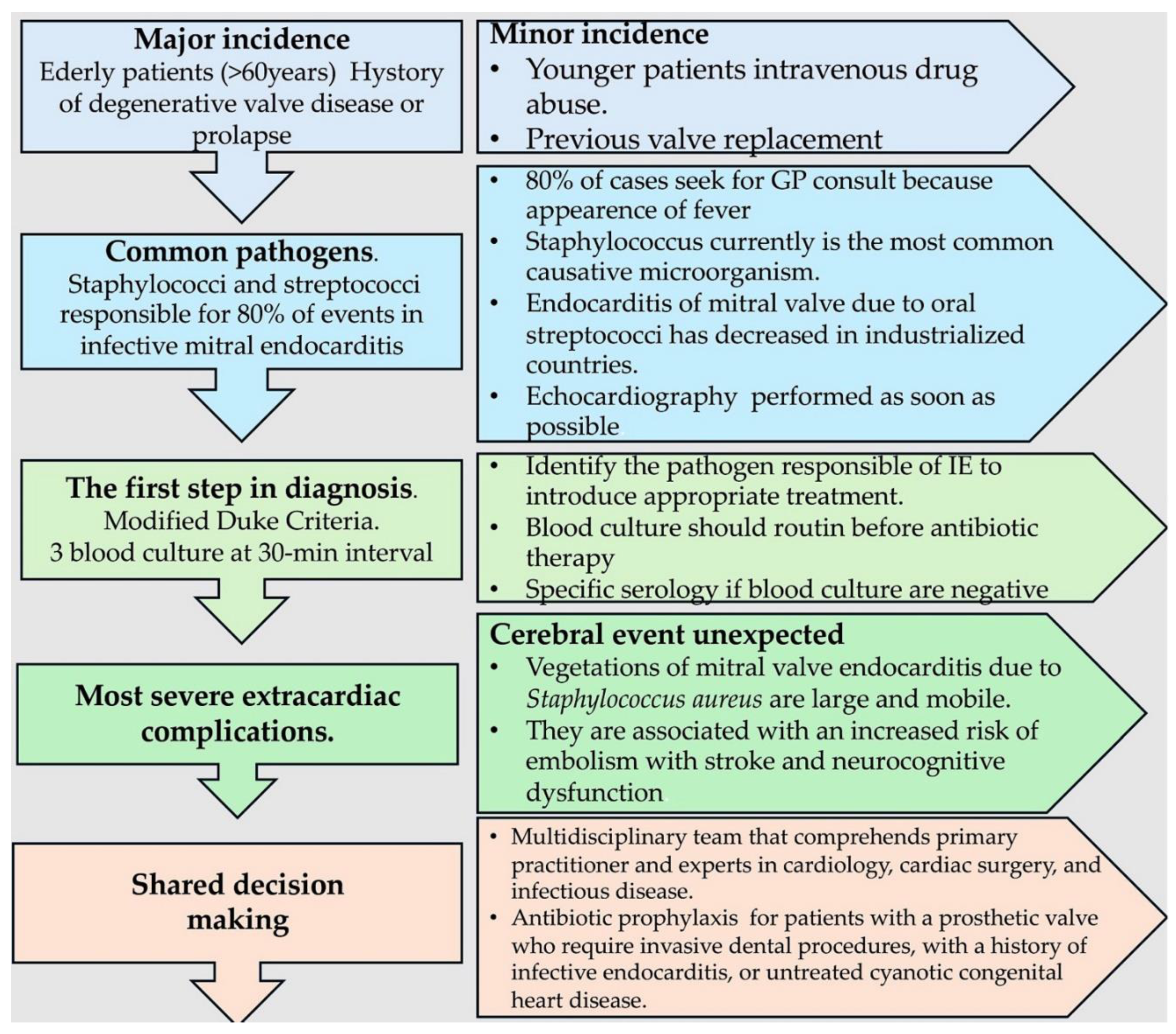
Figure 4.
(A) This illustration demonstrates the efficacy of antibiotic treatment in NVEs for viridans streptococci and Streptococcus gallolyticus at a penicillin MIC of ≤0.12 μg/ml. The duration of therapy once blood cultures have converted to negative is shown. Abbreviations; MIC, minimal inhibitory concentration ; wk,week. Ref [27,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. (B) This illustration demonstrates the efficacy of antibiotic treatment in NVEs for viridans streptococci and Streptococcus gallolyticus at a penicillin MIC of >0.12 to <0.5 μg/ml and for enterococci. The duration of therapy once blood cultures have converted to negative is shown. Abbreviations; MIC, minimal inhibitory concentration , wk,week. [27,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. (C) This illustration demonstrates the efficacy of antibiotic treatment in NVEs for Abiotrophia defectiva, granulicatella species, viridans streptococci, S. gallolyticus, at a penicillin MIC ≥0.5 μg/ml. The duration of therapy once blood cultures have converted to negative is shown. Abbreviations; MIC, minimal inhibitory concentration , wk,week. [27,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. (D) This illustration demonstrates the efficacy of antibiotic treatment in NVEs for methicillin-susceptible Staphylococcus aureus, methicillin-resistant S. aureus and HACEK. The duration of therapy once blood cultures have converted to negative is shown. Abbreviations; MIC, hr, hour; wk,week. *HACEK denotes haemophilus species, aggregatibacter (formerly actinobacillus) species, cardiobacterium species, Eikenella corrodens, and kingella species;[27,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72].
Figure 4.
(A) This illustration demonstrates the efficacy of antibiotic treatment in NVEs for viridans streptococci and Streptococcus gallolyticus at a penicillin MIC of ≤0.12 μg/ml. The duration of therapy once blood cultures have converted to negative is shown. Abbreviations; MIC, minimal inhibitory concentration ; wk,week. Ref [27,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. (B) This illustration demonstrates the efficacy of antibiotic treatment in NVEs for viridans streptococci and Streptococcus gallolyticus at a penicillin MIC of >0.12 to <0.5 μg/ml and for enterococci. The duration of therapy once blood cultures have converted to negative is shown. Abbreviations; MIC, minimal inhibitory concentration , wk,week. [27,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. (C) This illustration demonstrates the efficacy of antibiotic treatment in NVEs for Abiotrophia defectiva, granulicatella species, viridans streptococci, S. gallolyticus, at a penicillin MIC ≥0.5 μg/ml. The duration of therapy once blood cultures have converted to negative is shown. Abbreviations; MIC, minimal inhibitory concentration , wk,week. [27,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. (D) This illustration demonstrates the efficacy of antibiotic treatment in NVEs for methicillin-susceptible Staphylococcus aureus, methicillin-resistant S. aureus and HACEK. The duration of therapy once blood cultures have converted to negative is shown. Abbreviations; MIC, hr, hour; wk,week. *HACEK denotes haemophilus species, aggregatibacter (formerly actinobacillus) species, cardiobacterium species, Eikenella corrodens, and kingella species;[27,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72].
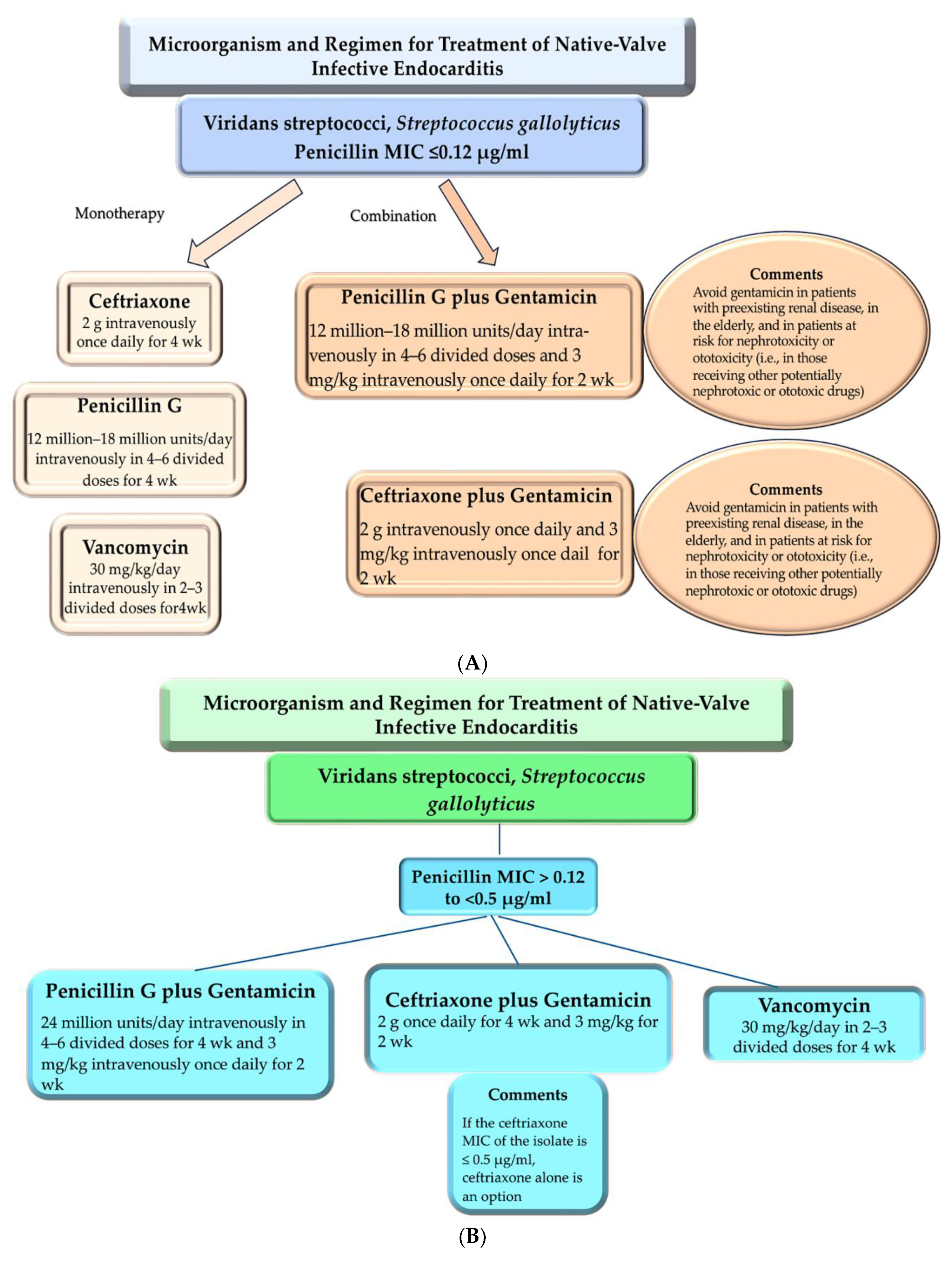
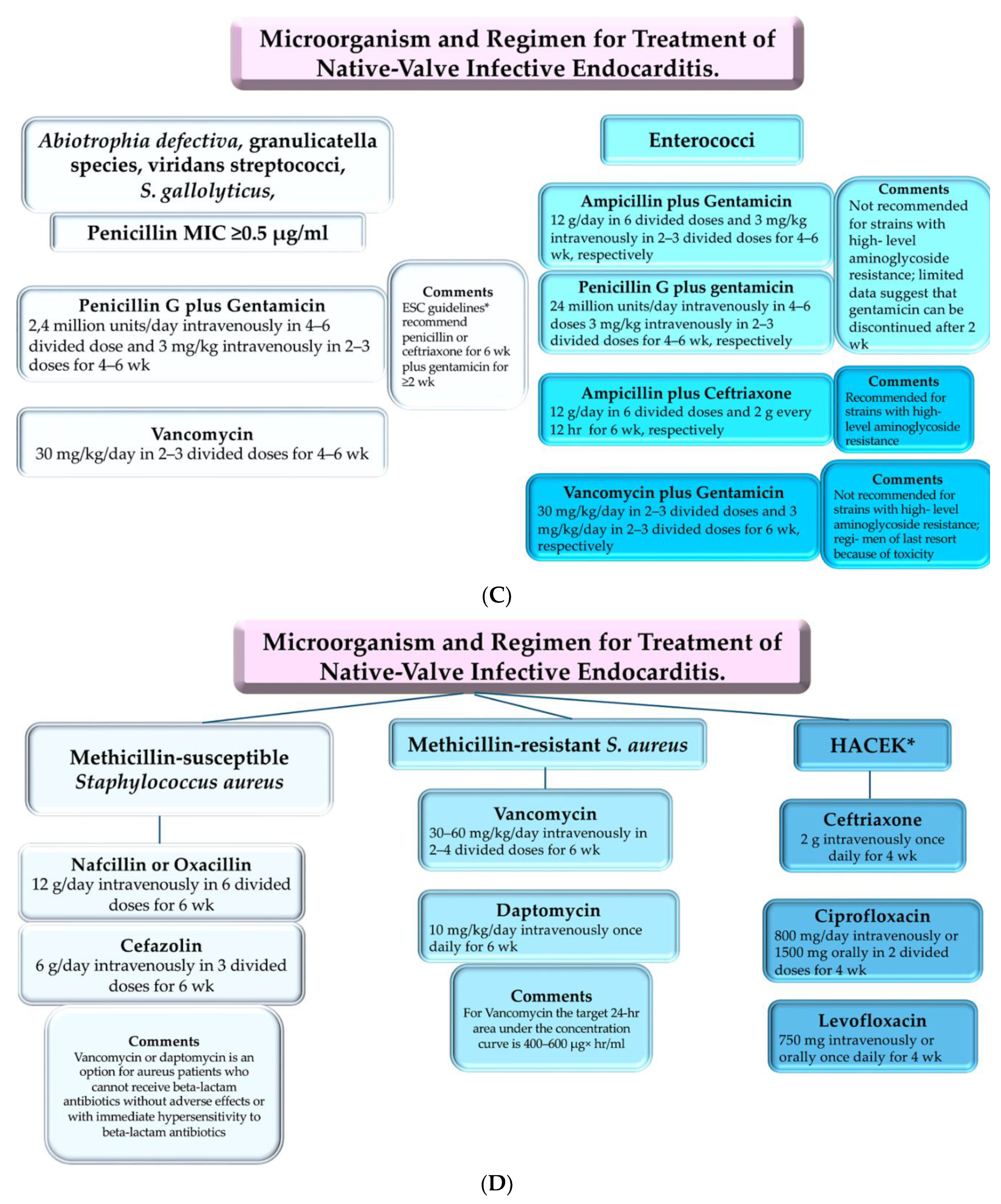
Figure 5.
Indications for surgery of isolated or complex mitral valve endocarditis. This illustration presents a summary of the 2023 ESC Guidelines for the management of endocarditis, 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria, JCS 2017 guideline on prevention and treatment of infective endocarditis and 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: surgical treatment of infective endocarditis: executive summary The guidelines are presented in the form of a flowchart, which depicts three different pathways (light blue, light green, and light grey box) according to the degree of urgency. The clinical presentation (red boxes) and imaging findings are described in each pathway. The decision-making algorithm for elective, urgent, or emergency surgery is presented in light blue, light green, or grey boxes in the flow chart, respectively. The choice of surgical strategy (i.e., repair or replacement) is based on the clinical and anatomic findings on preoperative imaging. If the IE is localized to a restricted portion of the valve leaflets, mitral valve repair should be considered. In cases of extensive anatomic involvement of the valve, surgical mitral valve replacement is recommended. The timing of surgery should be the result of a shared multidisciplinary decision. In emergency surgery, treatment of the infected valve is required within 24 hours after completion of the diagnostic workup. Patients whose condition is urgent should undergo surgery within a few days upon indication. Elective surgery should be performed after at least 1 to 2 weeks of antibiotic therapy. Ref 4,19,20,27,28,31,49,77.
Figure 5.
Indications for surgery of isolated or complex mitral valve endocarditis. This illustration presents a summary of the 2023 ESC Guidelines for the management of endocarditis, 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria, JCS 2017 guideline on prevention and treatment of infective endocarditis and 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: surgical treatment of infective endocarditis: executive summary The guidelines are presented in the form of a flowchart, which depicts three different pathways (light blue, light green, and light grey box) according to the degree of urgency. The clinical presentation (red boxes) and imaging findings are described in each pathway. The decision-making algorithm for elective, urgent, or emergency surgery is presented in light blue, light green, or grey boxes in the flow chart, respectively. The choice of surgical strategy (i.e., repair or replacement) is based on the clinical and anatomic findings on preoperative imaging. If the IE is localized to a restricted portion of the valve leaflets, mitral valve repair should be considered. In cases of extensive anatomic involvement of the valve, surgical mitral valve replacement is recommended. The timing of surgery should be the result of a shared multidisciplinary decision. In emergency surgery, treatment of the infected valve is required within 24 hours after completion of the diagnostic workup. Patients whose condition is urgent should undergo surgery within a few days upon indication. Elective surgery should be performed after at least 1 to 2 weeks of antibiotic therapy. Ref 4,19,20,27,28,31,49,77.
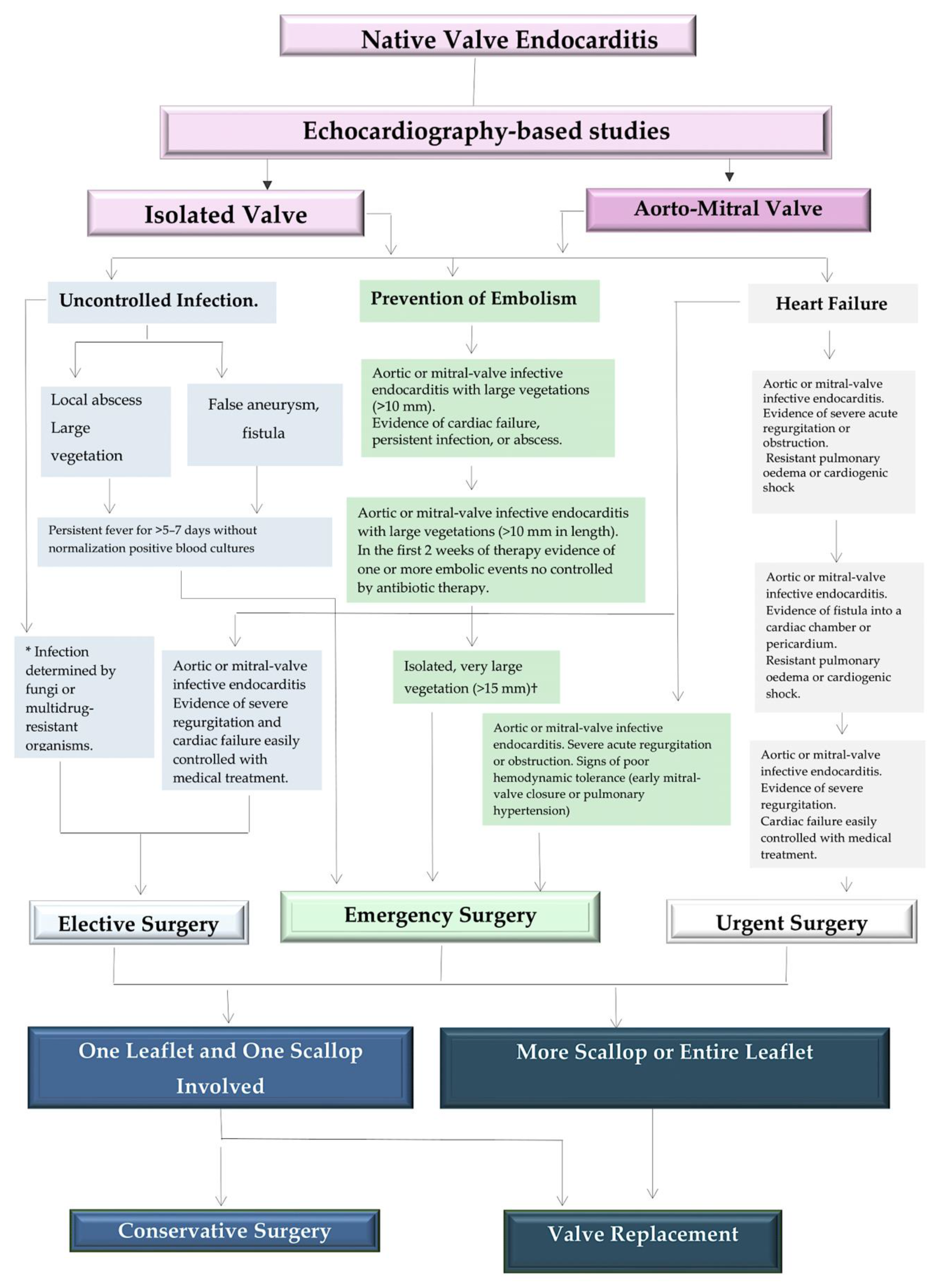

Table 1.
Sensitivity and specificities of echocardiography in the detection of abscesses. Adapted from Nappi et al. Ref [42].
Table 1.
Sensitivity and specificities of echocardiography in the detection of abscesses. Adapted from Nappi et al. Ref [42].
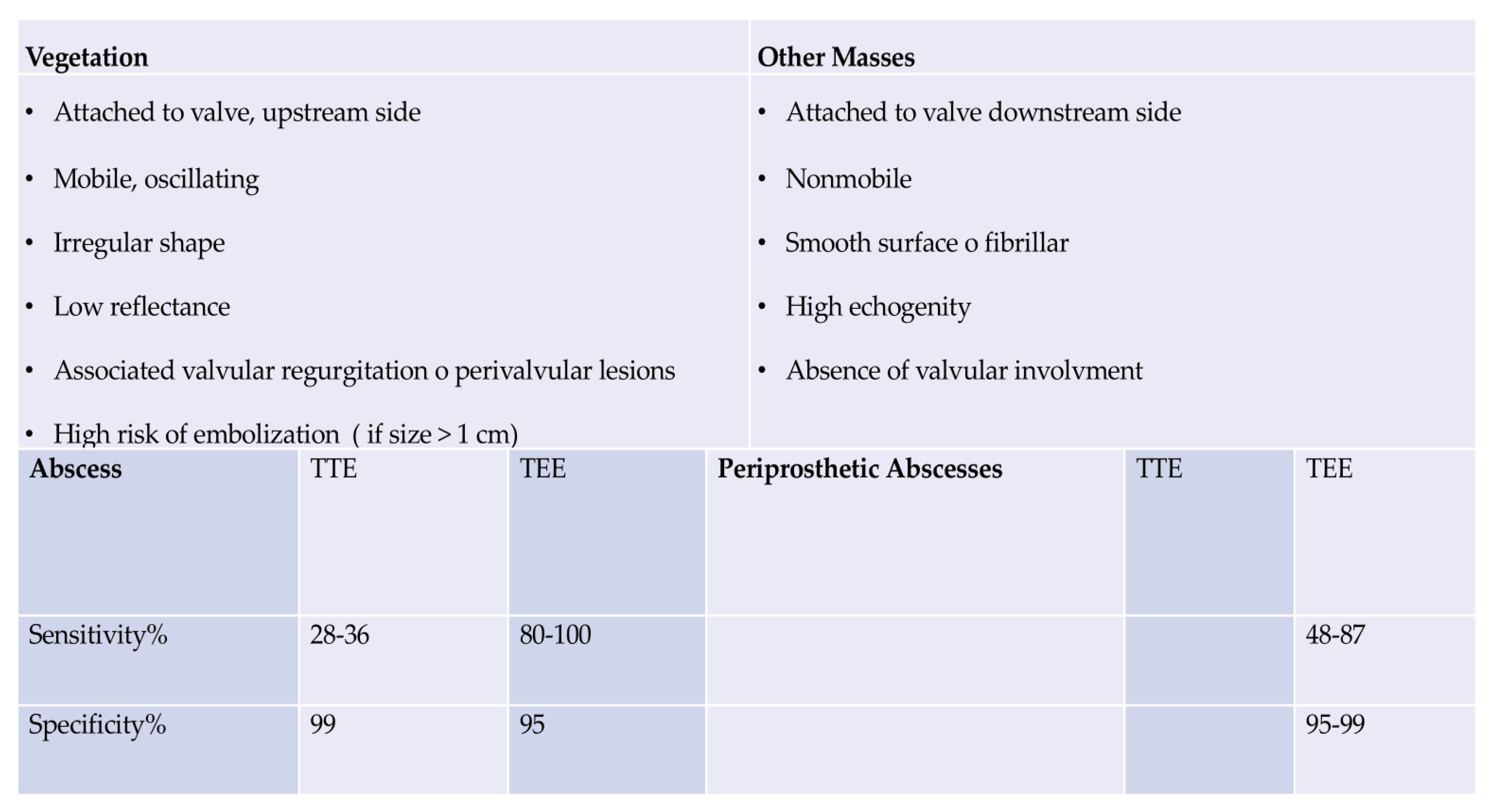
Table 2.
Guidelines for Infective Endocarditis. Ref 28,77.
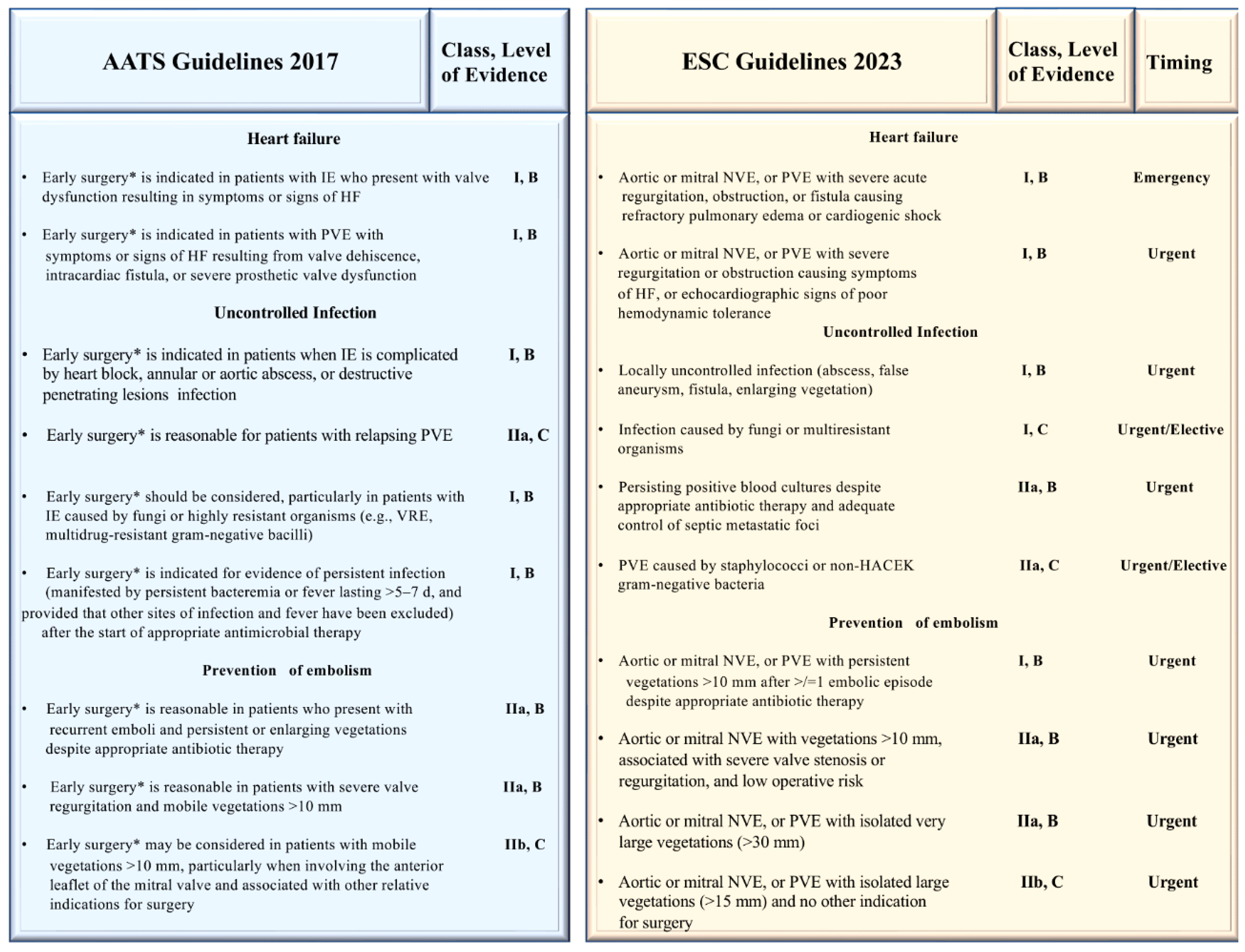
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



