
Submitted:
10 June 2024
Posted:
11 June 2024
You are already at the latest version
Abstract
Mitral regurgitation (MR) is a broadly diffuse valvular heart disease (VHD) with a significant impact on healthcare system and patient’s prognosis. Transcatheter mitral valve interventions (TMVI) are now well-established techniques included in the therapeutic armamentarium for managing patients with mitral regurgitation, either primary or functional MR. Even if guidelines give indications regarding the correct management of this VHD, the wide heterogeneity of patient’s clinical background, valvular and heart’s anatomy make each patient a unique case, in which the appropriate device’s selection requires a multimodality imaging evaluation and a multidisciplinary discussion. Proper pre-procedural evaluation plays a pivotal role to judge the feasibility of TMVI, as well as a cooperative works between imagers and interventionalist is crucial for procedural success. This manuscript aims to provide an exhaustive overview of the main parameters that need to be evaluated for appropriate device selection, pre-procedural planning, intraprocedural guidance and post-operative assessment in the setting of TMVI. In addition, it tries to give some insights about next perspective of structural cardiovascular imaging.
Keywords:
TMVI
; MR
; Pre-procedural planning
; Intra-procedural guidance
; Multi-modality Imaging
1. Introduction
Mitral regurgitation (MR) represents the second most prevalent valve disease in Europe with a prevalence that increases with age and a reduced overall survival, if untreated [1,2,3]. Etiologically, MR is classified in primary or organic (PMR) and secondary or functional (FMR). In PMR the primum movens is an intrinsic leaflet pathology, whereas in FMR the disease arises from ventricular remodeling/dysfunction (V-FMR) or from left atrial dilatation (A-FMR), and the leaflets undergo further to secondary adaptation [4]. The Carpentier classification is the most used to emphasize the specific mechanism of MR (Figure 1):
This classification holds therapeutic implications and was originally used to guide surgical strategy. Type I MR may require annuloplasty in case of annular dilatation, or pericardial patch in case of leaflet perforation. In Type II different techniques (chordal implantation, chordal transfer, leaflet resection, sliding plasty, edge-to-edge), usually associated to annuloplasty, may be used. In Type IIIa surgical option may be commissurotomy, chordal fenestration or replacement. In Type IIIb surgical approach consists of annuloplasty in most cases. Transcatheter approach may be leaflet/chordal/annular approach or transcatheter valve replacement depending on anatomic assessment.
In recent years, particular attention has been paid to FMR, associated with worse outcomes than PMR, clarifying the existence of two different forms with distinct nature and prognosis [5,6]:
- A-FMR. The main mechanism is represented by annular dysfunction/dilatation and atriogenic leaflet tethering with reduced leaflet remodeling, leading to an annulus-leaflet area imbalance. It usually involves patients with preserved left ventricular (LV) systolic function, especially if they are affected by atrial fibrillation (AF) [7,8]. Optimal treatment remains debated and includes rhythm control, different transcatheter and surgical procedures, with the latter potentially able to treat all the mechanism of the disease: plication for left atrium (LA) enlargement, annuloplasty for annulus dilatation, patch augmentation for insufficient leaflet remodeling and Cox-Maze procedure for AF [9,10]. When feasible, MVr is probably associated to a better outcome than MVR [11].
- V-FMR. The main mechanism is LV dilatation and/or systolic dysfunction with global or regional remodeling of LV and/or asynchrony, leading to symmetric or asymmetric tethering of mitral leaflets. The best treatment usually involves a comprehensive use of the “classical” heart failure management strategies: optimal medical treatment, myocardial revascularization if indicated, cardiac resynchronization therapy, transcatheter edge-to-edge repair (TEER) [12].
The arrival of transcatheter approaches, in terms of both repair (TMVr) and replacement (TMVR), has offered an alternative to surgery in the spectrum of patients with MR, especially for patients unsuitable or at high risk for surgery [13]. The purpose of this review is to summarize the current literature on transcatheter mitral valve intervention (TMVI), highlighting the importance of echocardiography and multimodality imaging from the pre-procedural planning to the intraprocedural guidance and the post-procedural evaluation. Furthermore, relevant insights in the field of emerging imaging techniques will be addressed.
2. Materials and Methods
A comprehensive review of the literature was performed querying PubMed, Embase, Cochrane with the following keywords: “transcatheter mitral valve repair,” “transcatheter mitral valve replacement”, “TMVR”, “TMVr”, “transcatheter edge-to-edge repair”, ”MitraClip”, “PASCAL”, “Tendyne”, “primary mitral regurgitation”, “secondary mitral regurgitation”, “Carillon”, “Cardioband”, “multimodality imaging in structural heart disease”, “transesophageal guidance in structural heart intervention”. Studies that contained relevant information were selected and included in the subsequent discussion.
3. Transcatheter Mitral Valve Intervention
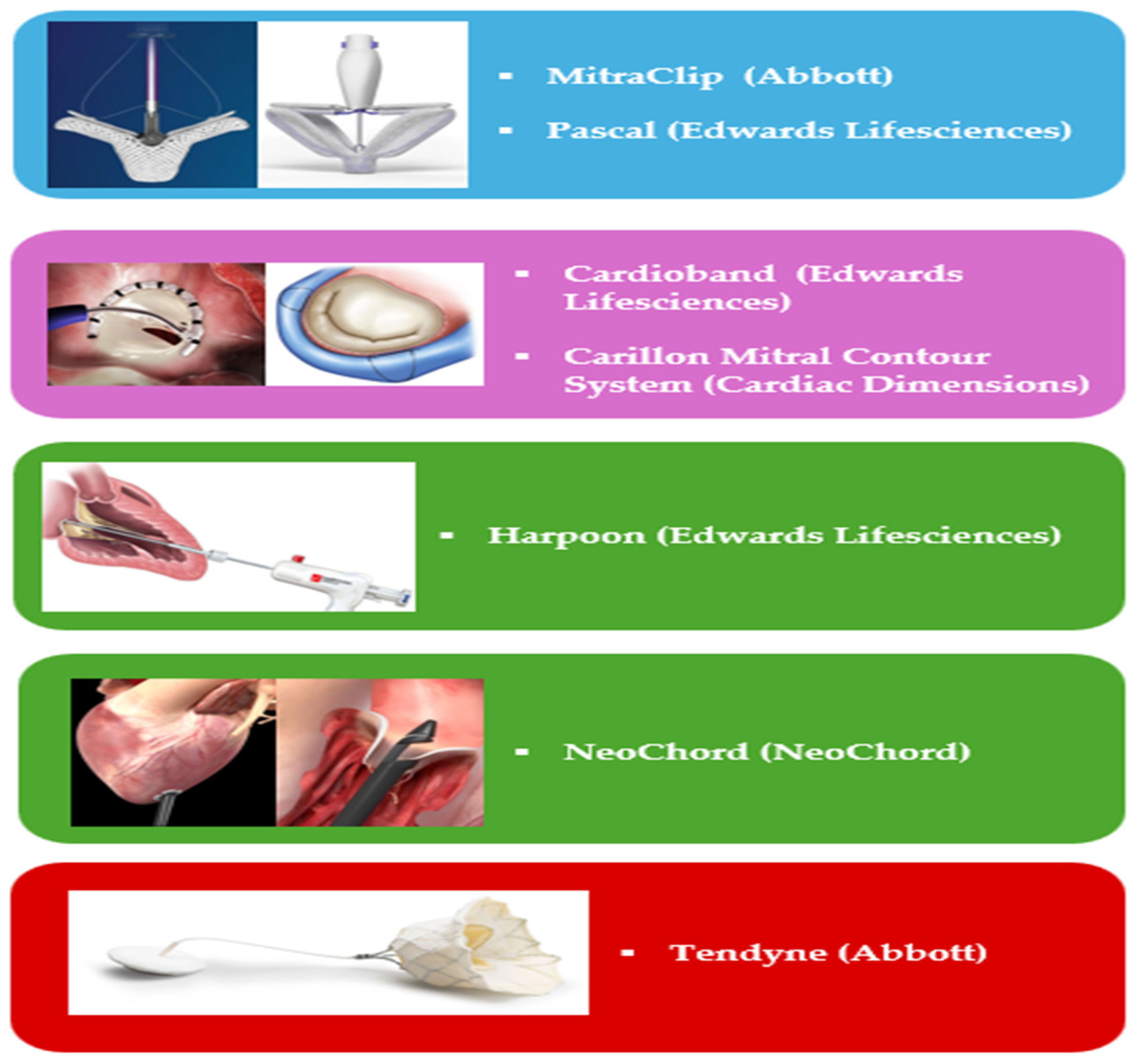
TMVr procedure encompasses the use of different devices and conceptually different techniques (Figure 2):
- -
- Leaflet’s approximation: MitraClip (Abbott Cardiovascular, Plymouth, MN, USA), PASCAL (Edwards Lifesciences, Irvine, CA, USA);
- -
- Direct Annuloplasty: Cardioband (Edwards Lifesciences, Irvine, CA, USA);
- -
- Indirect Annuloplasty: Carillon Mitral Contour System (Cardiac Dimensions, Washington DC, USA);
- -
- Chordal Repair: HARPOON (Edwards Lifesciences, Irvine, CA, USA). NeoChord (NeoChord Inc. Louise Park, MN, USA).
TMVR is now represented exclusively by Tendyne system (Abbott Cardiovascular, Plymouth, MN, USA), the only one with CE mark approval, whereas other devices are still under evaluation in clinical studies.
Figure 2.
Approved devices for TMVI. Abbreviations as in the text.
Leaflet’s approximation. TEER is the most widely used and studied TMVI and is inspired by surgical Alfieri’s edge-to-edge suture between the free edge of anterior (AL) and posterior mitral leaflet (PL). The two devices available are the MitraClip and the PASCAL system, both implantable by venous transfemoral access, trans-septal puncture (TSP) and general anesthesia with transesophageal (TEE) guidance.
The MitraClip system received CE mark approval in 2008 and was subsequently upgraded up to the last generation device (Figure 3).
It has a cobalt-chromium and nitinol core with a polyester cover, designed to promote tissue growth. Two arms and grippers allow the device to close on itself, capturing and approximating the leaflets. The system is formed by a steerable guide catheter (SGC) and a clip delivery system (CDS). The SGC consists of a catheter with an echogenic tapered dilator. The CDS is introduced into the body through the SGC and is composed by (a) the delivery catheter, (b) the steerable sleeve and (c) the MitraClip device. The device was firstly tested in the EVEREST I trial, showing a good efficacy and safety of the procedure both in PMR and FMR, and afterwards also in the EVEREST II trial, where it was associated with superior safety and similar improvement of clinical outcomes, but was less effective at reducing MR than conventional surgery [14,15]. Subsequently, attention shifted towards FMR, which had been underrepresented in earlier trials.
In this context, the MITRA-FR and COAPT trials have contributed to better delineate the subpopulation of FMR that may benefit the most from the procedure (the so called “COAPT-like” phenotype). This distinction holds true even when considering long-term outcomes [16,17]. The practical conclusion is that the MitraClip device yields the best result in patients with more severe MR and less advanced LV disease (characterized as “disproportionate MR”). Conversely, in patients with more advanced LV disease and less severe MR, known as “proportionate MR”, the procedure does not appear to affect prognosis.
Moreover, clinical benefit of TEER may be hampered by several factors, despite optimal procedural success in reducing MR. These factors include severe tricuspid regurgitation (TR), severe pulmonary hypertension, and right ventricular dysfunction, which should be carefully considered during patients’ selection [18,19,20].
The PASCAL system was designed to overcome some of the limitations associated with early-generation MitraClip devices, including limited maneuverability within the LA, limited implant dimensions, risk of leaflet damage in case of multiple grasping attempts and the potential for chordal injury in complex lesions, particularly in commissural zones. It consists of two components: an implant system (IS) and a guide sheath (GS). The IS consists of the steerable catheter (outermost layer), the implant catheter (innermost layer) and the implant device on its distal end; the implant is made of nitinol and is formed by a (1) central spacer, (2) two juxtapose paddles, and (3) two different clasps; the spacer covers the regurgitant orifice area (ROA) and provides a surface for leaflets’ coaptation, the paddles facilitate leaflet’s approximation, and the clasps adhere on the leaflets’ atrial side with only a row of grippers (4-6 rows in MitraClip system). The GS set includes a steerable guide sheath and an introducer. One of the main features of the system is its atraumatic behavior towards the leaflets. This is achieved through the shape and wide size of the paddles, which allow for more homogeneous stress and tension release on the leaflets. Additionally, the elongation properties of the device enable safe retraction from the sub-valvular area. Another significant advantage is the possibility of independent grasping, a feature that is only available in the 4th generation MitraClip system. In 2020, a second smaller device, the PASCAL Ace, was introduced to the market, further expanding the system’s compatibility with different valve anatomies. The procedure for PASCAL implantation is similar to that of the MitraClip and it is performed under general anesthesia, with TEE guidance and venous femoral access using transseptal puncture (TSP). The PASCAL system received CE approval for both primary mitral regurgitation (PMR) and functional mitral regurgitation (FMR) after demonstrating good safety, feasibility, and long-term durability in the CLASP study [21].
MitraClip vs PASCAL. The CLASP IID/IIF (ClincalTrials.Gov: NCT03706833) are prospective, multicenter, randomized, controlled trials ideated to compare the two TEER device in PMR and FMR, respectively. The 1-year outcome of the IID showed that PASCAL system was safe, effective, and non-inferior to MitraClip system in terms of clinical outcomes and echocardiographic features [22].
Indirect Annuloplasty. The only device with CE approval in this setting is the Carillon Mitral Contour System. It is positioned inside the coronary sinus (CS) or great cardiac vein (GCV) via jugular vein access, with general anesthesia usually required only when TEE guidance is used. The device consists of three components: (1) a proprietary implant intended for permanent placement inside CS/GCV, (2) a catheter-based delivery system, consisting of a curved delivery catheter, and (3) a sizing catheter. The implant is made of nitinol and titanium, manufactured with different length. It has also a distal and a proximal anchor, linked by the ribbon connector, and a proximal and distal crimp tube. The distal anchor is smaller and is placed inside the GCV, whereas the proximal one is larger and positioned near CS ostium which is located near the posteromedial commissure of MV. The arc-shaped ribbon is designed to be deployed, tensioned, and secured inside the CS/GCV. Two previous trial, AMADEUS and TITAN I, showed improved clinical and echocardiographic parameters in patients undergone to the procedure, with a good safety profile [23,24]. However, cases of distal anchor slippage were documented with the first-generation device, leading to reengineering to reduce device failure, as shown in the TITAN II trial [25]. The subsequent randomized sham-control REDUCE FMR trial showed a significant reverse LV remodeling and reduction of regurgitant volume [26]. This data was confirmed in a 5-year period, that also denoted a benefit in long-term survival [27]. Based on these promising results, a randomized trial is currently ongoing in Europe and USA (ClincalTrials.Gov: NCT03142152).
Direct Annuloplasty. The Cardioband Mitral System is a device used for direct annuloplasty TMVr through femoral vein access and TSP approach, under general anesthesia and TEE guidance. It consists of an implant and three main accessories: a) the Cardioband delivery system (CDS), b) the implantable metal anchors and anchors delivery shafts, and c) the size adjustment tool (SAT). The implant is a polyester sleeve, available in six sizes, with radiopaque markers; inside it, there is a metal wire connected to an adjusting spool, that permits shortening of the device at the end of procedure. The CDS is formed by an implant delivery system (IDS) and a transseptal steerable sheath (TSS); the IDS is formed by a steerable guide catheter (GC) and an implant catheter (IC) with the implant mounted on its distal tip. Between 12 and 17 stainless anchors are implanted using the delivery shaft. The SAT is used at the end of the procedure for cinching the device.
In a single-arm prospective multicenter experience of FMR treated with Cardioband system, the device showed reasonable performance and safety [28]. However, additional data are necessary to further validate these findings.
Chordal Repair. Chordal implantation is performed via transapical (TA) access in a mini-invasive procedure with two currently available devices: NeoChordDS1000 and HARPOON. These technologies allow for repair without annuloplasty and are considered viable alternative primarily in cases of in MR without annular dilatation and/or LV remodeling (early-stage disease). The main difference from the surgical technique is that the distal extremity of the chorda is not fixed to the papillary muscle, but rather to a large pledget located at the apical access site, prompting the need for investigation into the long-term consequences of this approach.
The NeoChord system has been the first TA chordal device available for use. The procedure is performed off-pump, under general anesthesia, through a left mini thoracotomy at the level of the intercostal space better suitable for TA access, and with TEE guidance [29]. Selecting the optimal entry site, usually postero-lateral, is crucial to avoid damage to the sub-valvular apparatus and ensure an equal distribution of tension among the neochordae. In some cases, alternative access sites and trajectories may be considered [30,31]. When right position at the leaflet is reached, the jaws of the device are opened, and the device is withdrawn from LA to LV to grasp the leaflet. If other chordae are necessary, the device can be reloaded. The TACT trial showed that artificial chordae implantation is technically safe and feasible [32]. The ReChord trial (ClinicalTrials.gov: NCT 02803957) is ongoing to evaluate the safety and efficacy of TA off-pump repair versus standard on-pump surgical techniques and the AcChord trial (ClinicalTrials.gov: NCT 04190602) is evaluating the 5-year outcomes of patients treated with NeoChord DS1000 in a post-marketing setting. Moreover, a TS device (NeoChord NeXuS system) from the same company is under pre-clinical evaluation.
The HARPOON MVRS is always a beating heart, off-pump, MVr system with TA approach performed under general anesthesia and TEE guidance. The system consists of an introducer and a delivery system. When the tip of the delivery system is positioned under the leaflet, the double-helix coil knot is released by penetration through the leaflet tissue. The TRACER trial has explored the feasibility and safety of the device with positive results [33]. Another trial (RESTORE) is ongoing (ClinicalTrial.gov: NCT04375332).
While early results are promising, the long-term durability and effectiveness of these procedures remain to be conclusively demonstrated. Ongoing research endeavors aim to address these critical aspects.
TMVR. Replacement is an alternative option for MR unsuitable for TMVr. The Tendyne system is the only CE marked device until now; however, others are under investigation: Sapien M3 (Edwards Lifesciences), Intrepid (Medtronic), EVOQUE (Edwards Lifesciences) and others. TMVR can be carried out by transfemoral or TA route, depending on the specific device, and is currently adopted in specific clinical settings, going from failed bioprosthesis [valve-in-valve (ViV)] to calcified valve [valve-in-mitral-annulus-calcification (Vi-MAC)] and failed prosthetic rings and bands [valve-in-ring (ViR)]. Each setting presents unique features, challenges, and outcomes [34]:
- Vi-V: this approach encompasses the implantation of a new bioprosthesis within a degenerated mitral bioprosthesis and is the most used out of the three. It is feasible via both TS and TA approaches. ViV procedures have demonstrated excellent results in terms of procedural (74%) and technical (94.4%) success rates, with a low incidence of post-procedural adverse events: 2.2% significant left ventricular outflow obstruction (LVOTO), less than 1% conversion to surgery, 3.3% significant paravalvular leak (PVL), and 6.2% 30-day mortality.
- Vi-R: it is based on the implantation of a bioprosthesis following a failed mitral valve annuloplasty. The procedural success rate (57.4%) is lower compared to ViV procedures, with an increased risk of adverse events: 5% LVOTO, 12.6% PVL, 12% requiring a second valve implantation, and 9.9% 30-day mortality. The higher incidence of peri-procedural complications, along with significant residual MR, partly accounts for this elevated mortality rate. It is noteworthy that in patients previously subjected to MVr with annuloplasty ring, TEER should be prioritized as the first option [35].
- Vi-MAC: This procedure poses significant technical challenges and is associated with a high-risk profile in the target population. Procedural success rates are comparatively lower (41.4%), with a higher incidence of complications: 8.6% conversion to surgery, 39.7% LVOTO, 6.9% valve embolization, 13% significant residual MR, 34.5% 30-day mortality, and over 60% 1-year mortality. Due to these complexities and risks, Vi-MAC procedures are considered the most challenging among the various TMVR approaches.
The Tendyne valve stands as the sole CE marked device for this indication, crafted for implantation in a beating heart, off-pump procedure using a TA approach.
Its design encompasses a self-expanded nitinol inner-frame, meticulously integrated with a porcine pericardial tissue tri-leaflet valve. A second self-expanding nitinol outer frame, fashioned with a d-shaped structure, is intricately linked to and envelops the inner frame. This outer frame is coated with porcine pericardium and a polyethylene terephthalate (PET) cuff, specifically engineered to enhance sealing with the native annulus and mitigate the risk of paravalvular leaks PVLs (Figure 4).
The Tendyne valve offers two distinct models, each available in various sizes (refer to Table 1 for specifics). Supplementary components include: (a) an apical pad, available in small (S) and large (L) sizes, facilitating device anchoring at the apex; (b) a tether, which serves to interconnect and stabilize the valve with the pad; (c) a loading system; (d) a 36 F delivery system; (e) a pad positioning system; and (f) a 36 F retrieval system.
The valve’s design is meticulously structured to position it at the LA floor, with the tether and paddle mechanisms strategically positioned to impede prosthesis migration into the LA. Notably, the Tendyne device boasts full repositionability and retrievability, underscoring its versatility and precision in clinical application.
Its safety and efficacy have been explored in two trials, showing a success rate of 97.2% with a 5.5% 30-day mortality and 1.8% of stroke rate. The 1-year mortality rate was 26%, mostly driven by cardiovascular mortality (85%). At 1-year all patients showed a residual MR ≤ mild [36,37]. The ongoing SUMMIT trial (ClinicalTrial.gov: NCT03433274) is going to evaluate TMVR with Tendyne system versus TEER with MitraClip.
4. Pre-Procedural Evaluation
Echocardiography is the mainstay of MR diagnosis and quantification. It should be performed according to the latest guidelines [38,39]. The multiparametric approach is considered the reference for optimal MR grading, considering qualitative, semi-quantitative and quantitative parameters. Qualitative parameters focus on structural aspects, such as MV morphology (prolapse, flail, perforation, ruptured papillary muscle, etc.), LV and LA size (normal or dilated), and Doppler signals – such as the color flow jet area (small/narrow/brief, large/eccentric/wall-impinging), the flow convergence (small/transient, large) and the continuous wave doppler jet trace (faint/partial/parabolic, dense/triangular/holosystolic). Semi-quantitative parameters rely on vena contracta width (VCW <0.3 cm, 0.3-0.6 cm, ≥ 0.7 cm), vena contracta area (VCA), pulmonary vein flow (systolic dominance, blunt and reverse flow) and mitral inflow (A-wave dominant, E-wave dominant > 1.2 m/s); the last ones, together with LA and LV size, are more useful for assessing hemodynamic impact than for MR quantification. Quantitative parameters can help subclassify the moderate MR group and are represented by effective ROA (EROA) – calculated by PISA method, volumetric method, or pulsed-wave doppler (PWD) method – regurgitant volume (RVol) and regurgitant fraction (RF).
It is important to be confident with the peculiarity and pitfalls of these different parameters. For example, VCW corresponds to the narrowest portion of the MR jet, located immediately downstream from the anatomic RO (Figure 5). It is scarcely influenced by flow status, but it cannot be used in presence of multiple jets and may overestimate MR when not holosystolic.
The VCA is measured with multiplanar reconstruction (MPR) from a 3D color dataset; this method offers the advantage of ensuring a precisely orthogonal cross-sectional area of the VC zone, free from dependence on flow-rate variations or any geometric assumption; its effectiveness is particularly pronounced in cases of non-circular shaped EROA [40]. Moreover, this method has been recently validated in a PMR population, suggesting an optimal cut-off of 0.45 cm2 for severe MR [41]. RVol, RF and EROA can be measured with different time-consuming methods, of which the most widely used is the PISA one. Nevertheless, PISA may not be accurate with multiple or eccentric jets or with marked elliptical-shape EROA. The PWD method is valid only if at least one semilunar valve (aortic or pulmonary) has a regurgitation of no more than mild and there are not intracardiac shunt; however, even in this case the risk of error is facilitated by the known nature of the equation used to calculate cross-sectional area of the outflow tract.
Concerning volumetric methods, the primary limitation is the potential underestimation of left ventricular (LV) volume. However, this limitation can be partially mitigated through the utilization of contrast echocardiography or advanced 3D imaging tools [42,43].
4.a Transcatether Edge-to-Edge Repair
Pre-procedural imaging screening of patients proposed for TEER serves the crucial purpose of evaluating the mechanism of MR and confirming the absence of absolute anatomical contraindications to the procedure. Procedural results are highly dependent on center experience. Therefore, it is currently more appropriate to classify anatomies into non-complex, complex, and very complex categories on one side, and hard or unfeasible anatomies on the other side (Figure 6). In cases of hard or impossible anatomies, consideration should be given to a replacement strategy or, ideally, referral to a high-volume center with specialized expertise in managing challenging cases [44].
Anatomical evaluation of mitral disease should adhere to specific guidelines and necessitate standardized views [45]. Interatrial septum (IAS) should be carefully evaluated, as certain anatomies may pose challenges during TSP, such as small fossa ovalis, floppy septum or atrial septal defect (ASD) closure device on site. In PMR, as previously observed, some criteria may predict successful grasping (flail gap < 10 mm, flail width < 15 mm) and the number of clips needed (flail width > or < 10 mm) [46]. The PASCAL system may be the choice in presence of challenging anatomies [47]. In FMR, the selection criteria should focus on the identification of the COAPT-like criteria that better stratify the outcomes: FMR ≥ 3+, LV ejection fraction ≥ 20%, LV end-systolic diameter ≤ 70 mm, TAPSE ≥ 15 mm, TR grade < 3+, systolic pulmonary artery pressure ≤ 70 mmHg [48].
4.b Indirect and Direct Annuloplasty
The role of TEE in patients candidate to Carillon device is only limited to the evaluation of MR mechanism, since the reference method to evaluate the CS anatomy and the correct size of the device is the invasive venography. With the Cardioband system, its necessary to give information on the MA morphology and size, the length of mitral leaflets, the course of CS and left circumflex artery (LCA), the anatomy of IAS and the risk of LVOTO. In this context, research is also exploring the feasibility of radiation-free pre-procedural planning, particularly in patient subgroups where contrast multi-detector computed tomography (cMDCT) is deemed unsafe [49].
CT plays a pivotal role in the preoperative planning for transcatheter annuloplasty. The configuration of the mitral apparatus varies throughout the cardiac cycle, therefore, for precise evaluation of the mitral valve’s shape and dimensions, it’s mandatory to utilize a retrospectively ECG-gated acquisition protocol [50,51]. This involves reconstructing CT datasets at intervals of 5% or 10% of the R-R interval, spanning from 0% to 100%. Tube voltage and tube current should be modulated to achieve the lowest possible radiation dose while maintaining good image quality, using 50-70 ml of contrast volume at flow rate of 4-6 ml/s. CT allows the evaluation of the CS and LCA. Specifically, the LCA typically courses along the left atrio-ventricular (AV) groove between the posterior mitral annulus (MA), the CS, and the great cardiac vein. In annuloplasty procedures, a very short distance between the MA and the LCA poses a risk of direct coronary damage or its compression during device fixation. CT, with volume rendering and multiplanar reconstructions enables the measure of the distance between the MA and the LCA, aiding the operator in assessing the patient’s suitability for annuloplasty. Additionally, a wide angle between the CS and the MA may lead to inadequate force transmission to the MA, potentially resulting in procedure failure [50,51,52,53].
4.c Chordal Repair
It is important to underline that not all anatomies are suitable for chordal repair. The ones expected to yield favorable outcomes are those with isolated prolapse/flail of P2, exhibiting a single jet lesion, lacking annular and left ventricular (LV) remodeling, and possessing an appropriate length of the posterior leaflet compared to the antero-posterior (AP) mitral annulus diameter. TEE plays a fundamental role in the pre-procedural evaluation of these patients. It is essential for accurately classifying mitral valve (MV) anatomy. In this regard, we can distinguish between several types:
- “Type A” (isolated central posterior prolapse/flail),
- “Type B” (posterior multi-scallop prolapse/flail),
- “Type C” (anterior or bileaflet prolapse/flail)
- “Type D” (paracommissural prolapse/flail or any significant annular or leaflet disease, e.g., calcification).
Outcomes are more favorable in type A and B pathologies, whereas type D is generally considered unsuitable. [54]. Mitral annulus (MA) dilatation is a critical determinant of procedural success. MA dilatation and loss of saddle-shape can increase traction on the leaflets, potentially leading to procedural failures. Evaluating calcifications is also crucial, ensuring their absence in the target zone of chordal insertion. One of the most important echocardiographic parameters to assess is the leaflet-to-annulus index (LAI). This index, expressed as the ratio between the sum of anterior (AL) and posterior (PL) leaflet lengths divided by the antero-posterior (AP) diameter of the mitral valve (AL+PL/AP), reflects the degree of leaflet-annulus mismatch. A cut-off value of ≥ 1.25 is associated with mild or less mitral regurgitation (MR) at 1-year follow-up [55]. Another key parameter is the gap ratio, defined as the ratio between the PL length and the distance between the free edge of the anterior leaflet (AL) and the hinge point of the posterior leaflet (PL). A gap ratio value ≥ 1.5 correlates with improved outcomes, ensuring adequate leaflet coaptation [33] (Figure 7). These parameters serve as valuable tools in pre-procedural planning and risk stratification for chordal repair
CT provides useful information about the pathology of mitral leaflets and MA size. It allows identification of prolapse with two- and three-chamber reconstructions that have high diagnostic accuracy compared to echocardiography [56]. In cases of mitral prolapse, small increments reconstruction of the cardiac cycle (e.g., 5%) may be useful to allow for a detailed evaluation of the leaflets during systole. Instead, MA dimension in patients with MR should be evaluated in systolic phases (20-40%), where the largest dimension was found [57,58]. Furthermore, CT is also fundamental to evaluate MAC displaying the best trajectory line, choosing the optimal location of TA access [30,59].
4.e TMVR
TMVR is a complex procedure with some characteristic complications (LVOTO, LCA compression, etc.), so the pre-procedural planning is undeniably crucial for accurate prediction of these risks and subsequent optimal planning.
TEE is necessary and can be potentially used also for pre-procedural screening of TMVR candidates [49]. However, cMDCT remains mandatory and is considered the reference method in this context. cMDCT provides detailed information regarding geometric remodeling of the mitral valve, including precise measurements of leaflet heights and angles. Moreover, it offers superior visualization of the dynamic nature of the mitral annulus, which undergoes changes in functional anomalies of the mitral valve. Understanding these anatomical nuances is crucial for correct device anchoring and can contribute to reducing fluoroscopic and procedural times [60,61]. By optimizing procedural planning and execution, cMDCT plays a pivotal role in enhancing the safety and efficacy of TMVR procedures. Furthermore, anomalies linked with LV dilation and wall motion abnormalities (WMAs) can lead to the outward displacement of the papillary muscle, annular dilatation, and basal remodeling of the myocardium. This process can result in the formation of a characteristic “myocardial shelf,” which is identifiable on CT imaging [62]. Since the morphology of the myocardial shelf changes throughout the cardiac cycle, ensuring proper anchoring of the device to the infero-lateral basal myocardium requires dynamic sizing of the posterior myocardial shelf in both systole and diastole. Additionally, CT imaging enables assessment of the extent and severity of mitral annulus (MA) and leaflet calcifications. In most severe cases, such calcifications can pose significant risks, potentially rendering the procedure extremely hazardous. Thus, thorough evaluation of these factors via CT imaging is crucial for pre-procedural planning and ensuring the safety and efficacy of interventions such as transcatheter mitral valve replacement (TMVR). CT also permits the differentiation of MAC from caseous calcification of the annulus, a rare variant, in which a large lesion occurs along the posterior annulus due to caseous transformation of the calcified ring material [63]. A fearful complication of TMVR is LVOTO. The mechanisms of obstructions can be either fixed, as in the case of prosthetic obstruction, or dynamic, due to the anterior systolic movement of the anterior mitral leaflet secondary to the prosthesis’s displacement. CT with postprocessing software can evaluate some elements that predict LVOTO such as the presence of a neo-LVOT area equal to or less than 1.7 cm2 [64]. CT allows optimization of the fluoroscopic angles used during the procedure to obtain correct visualization and implantation of the prosthetic device to minimize complications during deployment and positioning of the prosthesis [65,66].
5. Intra-Procedural Guidance
5.a Transcatether Edge-to-Edge Repair
Before starting the procedure, it may be beneficial to reassess the severity of mitral regurgitation (MR). This allows for a more accurate comparison of the post-procedural outcome with the baseline condition, taking into account the common anesthesia-induced intraprocedural downgrading of MR [67]. Moreover, the re-evaluation of MR is fundamental to confirm the correct site of device implantation. In addition to MR quantification, a standardized protocol evaluation may also include PWD evaluation of pulmonary vein flow, the trend of which has a significant impact on patient’s outcomes [68]. The procedural steps of TEER are:
- (1)
- TSP and SGC advancement,
- (2)
- Straddling and steering of the device,
- (3)
- Orientation,
- (4)
- Grasping
- (5)
- Final evaluation and release.
The trans-septal puncture (TSP) represents the most critical step, because a suboptimal crossing of IAS may negatively condition the complete procedure. The optimal site for the puncture is the postero-superior area of the fossa ovalis, identifiable through bicaval view (defining supero-inferior orientation) and short axis view at the aortic valve level (defining antero-posterior orientation). Tenting should be clearly visualized and the height from the MV plane must be measured in a modified mid-esophageal (ME) four chamber view. In patients with primary mitral regurgitation (PMR), the acceptable height may range from 4.5 to 5 cm, whereas in functional mitral regurgitation (FMR), a height of 3.5 to 4.0 cm may be acceptable due to the more ventricular displacement of the coaptation zone. Additionally, medial pathology necessitates a higher transseptal puncture (TSP) to ensure adequate space for the system to bend back towards itself without crossing the mitral valve (MV) plane. Conversely, lateral pathology may tolerate a lower TSP. Once the puncture has been performed, the guidewire is positioned inside the left upper pulmonary vein (LUPV). Subsequently, after removing the TSP system, the steerable guide catheter (SGC) with its dilator is advanced over the wire into the left atrium (LA). The echogenic knurled aspect of the dilator’s tip helps in its identification. Upon removal of the dilator, the double binary aspect of the SGC becomes visible. Although 3D imaging may seem attractive, 2D remains the preferred imaging modality to monitor this step due to its higher spatial and temporal resolution. At this point, the CDS is advanced inside the SGC to exit inside LA.
The straddling is substantially a fluoroscopic maneuver, involving the alignment of the two markers on the CDS shaft with the marker on the tip of the SGC (Figure 8). This orientation points the system towards the LUPV, providing more maneuvering space for subsequent steering.
After that the CDS is steered towards the MV plane, aiming for a perpendicular alignment. The TEE standard view to monitor this step are the simultaneous bi-plane with medio-esophageal (ME) commissural view (standard plane) and the long-axis (LAX) view (derivate plane). Once the clip has arrived at MV level, it is the time to align its arms perpendicularly to the coaptation line, using clockwise or counterclockwise rotation supported by a 3D en-face MV view (Figure 9).
Then the clip is advanced below the MV plane, with the arms partially closed. After that the arms are opened and the correct orientation is revaluated, as the system may rotate during the advancement (Figure 9). After that, the opened arms are withdrawn towards the leaflets and, when the leaflets lie on the arms, the grippers are lowered and the leaflets are grasped, with an ideal length of leaflet captured ≥ 5 mm. A good anatomical grasping is confirmed by the substantial reduction of leaflet mobility and the absence of regurgitant jet inside the clip, confirming the total insertion of the leaflet’s edge inside the clip (Figure 10).
Indirect indicators supporting mitral regurgitation (MR) reduction include reduction of LA pressure and the appearance or increase of spontaneous echo-contrast within the LA cavity. Additionally, it is crucial to assess the absence of stenosis, particularly when high flow velocity is observed on color Doppler. These assessments aid in confirming the effectiveness of the procedure and ensure that no complications, such as stenosis, have arisen as a result of the intervention. This evaluation relies on a multiparametric approach, considering not only the transmitral gradient, but also pressure half-time (PHT), and, most importantly, mitral valve area (MVA) measured with multiplane reconstruction (MPR). It’s crucial to note that each mitral orifice must be measured separately, as they lie in different planes. If the clip position is satisfactory, it is released and, if necessary, others can be implanted, always making a compromise between MR downgrading and MVA reduction. The subsequent clips are usually advanced with arms closed to minimize the risk of damage of the previous implanted one. When all the clips have been placed, the CDS is retracted inside the SGC and is important to carefully monitor this step, because the sharp tip of the shaft may damage the LA wall. With the CDS inside the SGC, all the system is then retracted and removed.
Using the PASCAL system follows similar procedural steps are as with the MitraClip system; with one notable exception: the “parallelism test”. This test is performed after TSP and used to ensure that the guide sheath tip flexes parallel to the MV plane. Monitoring this alignment can be achieved with a 3D view of the interatrial septum (IAS) from the left atrial (LA) perspective, with the MV positioned at 6 o’clock.
While fluoroscopy is traditionally considered a complementary modality, particularly for interventionalists who may initially rely more on fluoroscopic projections during the learning process, it also provides valuable support for interventional echocardiographers (IE) in maintaining procedural control. However, recent data suggest the potential feasibility of a radiation-free procedure. Additionally, in cases of complex mitral anatomy and challenging transesophageal echocardiography (TEE) imaging, the use of fluoroscopic-TEE fusion imaging may become necessary to enhance procedural guidance and accuracy [69,70].
5.b Indirect Annuloplasty
The first procedural step consists of the coronary artery angiography to evaluate possible coronary artery disease, the anatomy and flow of coronary artery and to identify the CS ostium with the venous phase after contrast injection. After that it proceeds to the cannulation of CS via right internal jugular vein access using the delivery catheter and a diagnostic catheter (i.e., multipurpose 6F or 7 F) in a telescopic manner, the last inside the first and over a guidewire, positioned up to the anterior interventricular vein (AIV). The diagnostic catheter is advanced up until to the GCV/AIV junction and, after that, the delivery catheter is advanced over the diagnostic one to reach the same position. Then both diagnostic catheter and guidewire are removed, and the sizing catheter is advanced inside the delivery catheter. A second coronary artery injection in right anterior oblique (RAO) caudal projection is performed to evaluate the relationship of LCA with CS/GCV, identified by the presence of the delivery catheter. At this point, a venogram of the coronary venous system is performed with a retrograde injection. Both angiographies are also repeated in left anterior oblique (LAO) caudal projection. For the sizing of the device an average of three measurements both in distal and proximal target zone is used (Figure 11).
The subsequent step involves the insertion of the device, followed by the release of the distal anchor and the retraction of the delivery catheter, which is then pushed forward to facilitate the expansion of the anchor. During this step, a coronary angiography injection is conducted to confirm the flow of the left coronary artery (LCA).
Following this, manual traction is applied to plicate the peri-annular tissue and cinch the annulus, after which the proximal anchor is released. Another coronary angiography is performed to ensure the absence of extrinsic compression of the device on the LCA.
At the conclusion of the procedure, if the patient is intubated, TEE can be utilized to assess the outcome. Alternatively, if the patient is only sedated, a transthoracic approach may suffice for evaluation.
5.c Direct Annuloplasty
TEE has a central role for Cardioband procedure, to allow the correct implantation of all anchors, necessary to gain procedural success.
The site of TSP is evaluated in pre-procedural planning with TEE/CT analysis and must be located above the postero-medial commissure at a > 3.5 cm height from MV plane. In this case 3DTEE may be extremely useful, allowing a direct visualization of the commissure and the IAS in a single view (3D LA perspective “en-face” IAS view); at this purpose, rotation of the 3D dataset in an overhead perspective, allows a better visualization of the tenting site.
After the TSP, the TSS and the IDS are advanced into LA. The first site of implantation is the antero-lateral commissure, near the left trigone, where the first anchor must be released. This zone is identified through fluoroscopy (LAO and RAO view pre-identified by CT) and TEE guidance, both 2D and 3D view.
This step is crucial as an incorrect implantation of the first anchor may jeopardize the success of the procedure. Subsequently, the second and third anchor are positioned near the first one, usually in the first 12 mm, to ensure a better stability of the device; the others are then implanted every 8 mm until the postero-medial commissure (right trigone) has been reached. Every anchor is positioned under fluoroscopy and TEE guidance, using both 3D en-face and MPR, because it is necessary to maintain an entry angle of 45° from the LA cavity towards the annulus and an angle of penetration of 90° along the implantation line. After release of the last anchor the IDS is withdrawn, and the SAT is inserted into TSS. The SAT allows the shrinkage of the device and annulus, gaining the reduction of MR grade.
5.d Chordal Repair
During these procedures, which are conducted under general anesthesia and TEE guidance, the latter is the sole imaging modality necessary and essential. After performing a left mini-thoracotomy, the apical access site is identified using bi-plane ME commissural (main plane) and ME-LAX views (derived plane) with the “finger poking” maneuver. Ensuring the correct site of entry is critical to preserve the integrity of the sub-valvular apparatus.
With the NeoChord system, the device is advanced to attain a position between the leaflets. Subsequently, its jaws are opened and then closed to grasp the leaflet, simultaneously releasing a loop suture and a girth hitch knot at the level of the mitral leaflet. After the first neochord release, the device can be reloaded, and additional sutures (typically up to 3-4) can be placed. The length of the neochordae can be adjusted to achieve the best anatomical result and optimal reduction of MR. The other end of each neochord is anchored to a pledget at the access site in the LV.
With the HARPOON device, TEE is used to confirm the correct position of the delivery system and the contact of the end effector with the leaflet; at this point the plunger is released to deploy a double-helical knot of e-polytetrafluoroethylene (ePTFE). If more than one ePTFE chords is required, the rule is to start lateral and go medial.
5.e TMVR
The only CE-marked device for TMVR is the Tendyne, so our focus will be on this device. The procedure is performed under general anesthesia, with hemodynamic monitoring in an operating room. The apex is reached with left mini-thoracotomy and a lateral puncture is performed to insert a J-tip guidewire from the LV to the LA. The correct site of puncture is chosen to be perpendicular to MV plane and to be safety towards subvalvular apparatus and the “finger poking” maneuver is used, as in chordal repair techniques. The procedure is monitored with bi-plane ME commissural and LAX view with. A 34 F sheath is advanced over the wire into the LA and the implant device is then inserted into the sheath and progressively extruded until it expands up to 85% of its final size. This step is monitored with an LA perspective en-face MV view using 3DTEE. The correct anatomical position is chosen in order to have the higher cuff leaning against the mitro-aortic curtain area. The device is then withdrawn towards the ventricle, gaining an intra-annular sealing. The valve is linked to the pad with the “tether” and the pad is fixed at the level of LV access. The tension of the tether is adjusted to ensure an optimal position of the device.
6. Post-Procedural Evaluation
Echocardiography plays a crucial role in the post-procedural evaluation of TMVI, being able to assess procedural success and check for potential complications. Procedural success evaluation relies on the accurate knowledge of the device-specific procedural steps and mechanism of function, also remembering that correct evaluation of residual regurgitation requires the integration of multiple parameters [71,72].
Regarding the complications, excluding those that can occur after numerous percutaneous procedures (e.g., bleedings, access site damage, contrast-induced nephropathy, pericardial effusion due to damage of cardiac wall, etc.), the focus will be moved onto the most common device-related complications.
6.a TEER
TEER is generally considered a safe procedure; however, it could be associated to some serious complications that need to be identified promptly. Some examples include cardiac tamponade, potentially correlated to suboptimal TSP, acute deterioration of LV dysfunction due to the afterload-mismatch, or unexpected worsening of MR: all these complications may lead to acute cardiogenic shock.
A feared complication is MR aggravation that can be potentially related to acute LV dysfunction, leaflet or chordal damage, loss of leaflet insertion (LLI) and partial leaflet detachment (PLD). While some of these factors may be predictable, others, such as iatrogenic leaflet or chordal damage, are considered avoidable complications that may result from technical errors during the procedure, such as multiple grasping attempts or navigating into non-chordal free areas [73].
Although the frequency of these complications may be relatively low, accurate patient selection is crucial to minimize their occurrence. Post-procedural evaluation should include a multiparametric approach to assess for complications such as mitral stenosis. This evaluation typically begins with the assessment of transmitral gradient and pressure half-time (PHT) and ends with the measurement of mitral valve area (MVA) using MPR techniques. MVA measurement with MPR is particularly valuable as it provides highly predictive information regarding adverse outcomes associated with mitral stenosis following TEER procedures [74]. Iatrogenic atrial septal defects (ASDs) resulting from TEER procedures are typically considered to have negligible clinical significance, particularly during long-term follow-up [75,76].
6.b Annuloplasty Devices
When utilizing annuloplasty devices, particular attention must be given to the risk of left circumflex artery (LCA) injury, which manifests as wall motion abnormalities (WMAs) within the LCA territory. In the context of Cardioband procedures, particularly in initial experiences, there is the additional concern of anchor disengagement. This complication may occur during the cinching step or following the pull test, potentially leading to partial device detachment, especially at the lateral commissure or within the P2 area. Additionally, the proximity of the medial commissure to the atrioventricular (AV) node necessitates consideration of the risk of AV conduction disorders, a concern applicable to all direct annuloplasty procedures.
6.c Chordal Repair
The specific complications associated with chordal repair techniques are comparable to those encountered in transcatheter edge-to-edge repair (TEER), as both involve a leaflet approach, albeit from different access points (e.g., apex). A primary concern in chordal repair is the potential detachment of the chord, leading to procedure failure. However, with careful patient selection, such occurrences are typically rare and can be considered anecdotal.
6.d TMVR
When discussing transcatheter mitral valve replacement (TMVR), it’s essential to distinguish between peri-procedural (short-term) and post-procedural (long-term) complications. Specifically focusing on device-related issues, critical aspects to assess include left ventricular outflow tract obstruction (LVOTO), valve embolization or migration, valve thrombosis or dysfunction, and the emergence of paravalvular leaks. [77].
LVOTO is a potentially life-threatening complications that necessitates prediction through pre-procedural evaluation, employing different modalities [49,78]. In this context, it is advisable to adopt strategies to prevent LVOTO, such as the transcatheter laceration and translocation of the anterior mitral leaflet (e.g., LAMPOON and BATMAN techniques), or septal ablation using radiofrequency or alcohol. The latter methods are also utilized to treat post-procedural LVOTO issues.
Valve migration or embolization can occur as an early complication due to suboptimal positioning of the device. Conversely, it may manifest as a delayed complication following an episode of prosthetic valve endocarditis or as a consequence of an undersized device experiencing delayed migration due to elevated left ventricular pressure, especially in the absence of extensive peri-device calcification [79].
Valve thrombosis or dysfunction and paravalvular leaks are complications that can occur with any prosthesis, and their pathophysiology closely resembles that of surgically implanted valves. Similarly, the methods for imaging detection and evaluation are akin to those used for surgical prostheses.
7. Emerging Techniques and Potential Future Directions
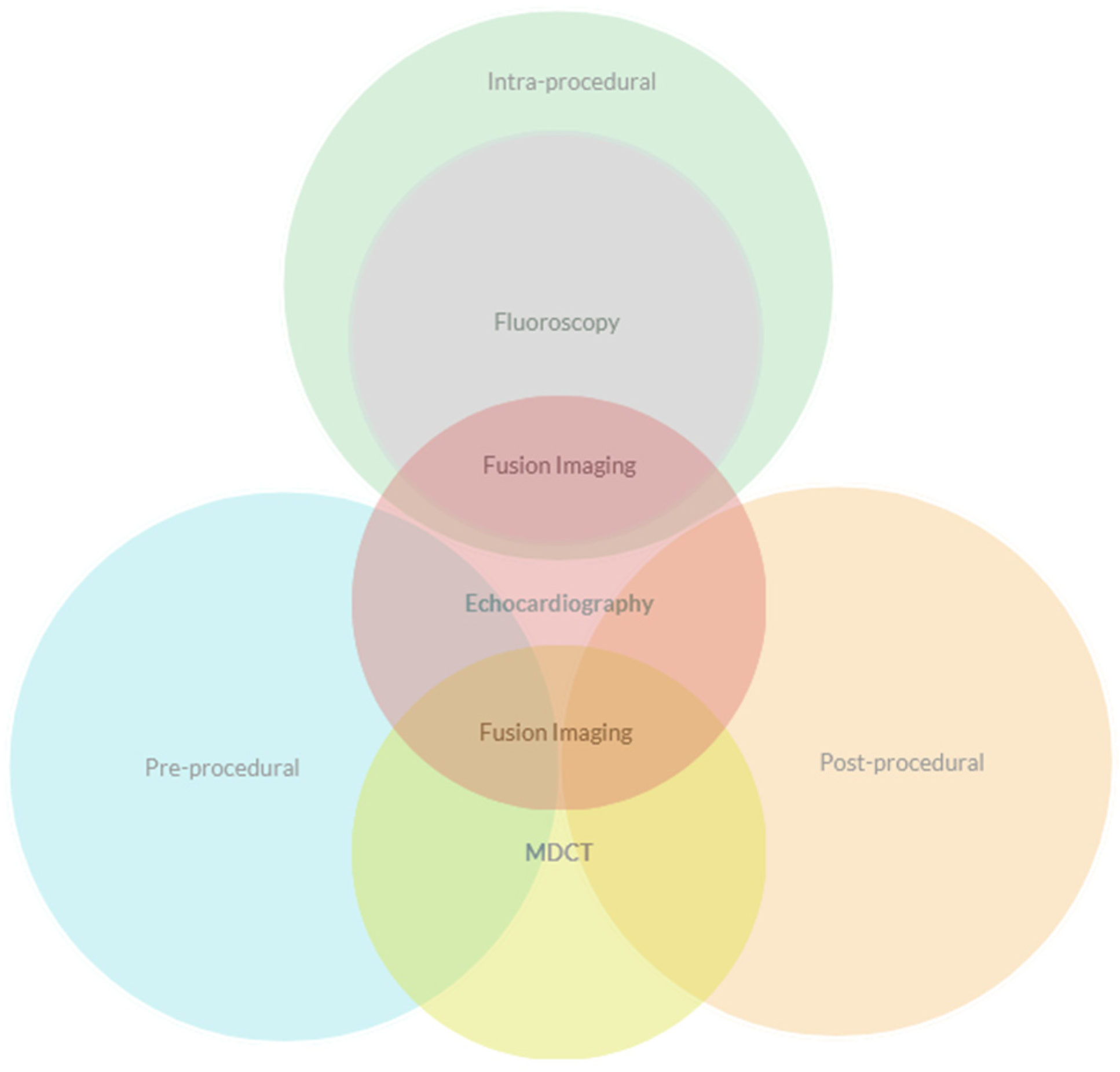
Echocardiography represents the cornerstone of imaging dedicated to TMVI. Despite its linchpin role in TEER, covering all the steps from pre- to intra- and post-procedural evaluation, it still needs the irreplaceable support of MDCT in many cases.
Figure 12.
Relationship of imaging methods in procedural steps of TMVI.
The sharp and unceasing progresses in the field of structural heart disease (SHD), as well as the evolution in imaging techniques, has pushed to turn our attention on the chance to take advantage of innovations to resolve different problems.
Radiation Exposure (RAE). One of the main issues in the field of SHD is the recent evidence of the considerable risk of RAE, underlining the imperative to mitigate this risk, especially for Interventional Echocardiographers (IE) [80]. In addressing this challenge, various approaches may be considered, ranging from the implementation of dedicated structural suite designs and shielding techniques to the development of tailored dose reduction programs, all with the ultimate goal of advancing towards minimally invasive and non-fluoroscopic procedures [69,81,82]. Efforts to reduce fluoroscopy time are paramount, with strategies such as implementing focused protocols or leveraging advancements in artificial intelligence (AI). AI holds promise in predicting the optimal fluoroscopic view from CT datasets through virtual fluoroscopy tools, as well as in facilitating fusion imaging for enhanced procedural guidance [83,84].
Education. Another aspect to consider is that IE is a pivotal player in the Heart Team and for all the step of the valvular heart disease management. Indeed, fulfilling this role requires comprehensive education encompassing clinical, anatomical, imaging, and surgical knowledge. However, the limited availability of dedicated structural imaging fellowships poses a challenge, especially if formal certification processes require supervision by certified faculty [85]. In light of the increasing prevalence of transcatheter techniques, it’s imperative to take steps to prevent the emergence of a class of IEs who are primarily self-educated. AI and virtual reality (VR) technologies can play a crucial role in addressing this issue by connecting individuals regardless of spatial and temporal constraints. These technologies facilitate real-time interactions in a 3D space with multimodality imaging capabilities, offering the potential for a comprehensive and immersive learning experience [86]. Indeed, this capability theoretically enables the sharing of numerous imaging cases, offering benefits for both operator learning and patient management.
Cooperation. Knowledge of the procedural steps of the different devices, of their different components and a correct integration of echocardiographic and fluoroscopic imaging is substantial for procedural success. The IE should possess the ability to swiftly transition between different views, often resorting to off-axis projections if necessary. This skill necessitates a profound understanding of the three-dimensional orientation of anatomical structures, as well as the capability to anticipate the movements of the interventionalist, alerting them in cases of dangerous positions or trajectories. Therefore, these two operators must exhibit the aptitude to work together in a collaborative and efficient manner. Fusion imaging serves as a point of connection, enabling both operators to overcome the limitations of a single imaging modality. It facilitates improved visualization of soft tissue in fluoroscopy and radiopaque materials, guidewires, and delivery systems in echocardiography. Additionally, fusion imaging aids in reducing fluoroscopy time, thereby enhancing safety, accuracy, and procedural effectiveness [65,83,87].
Prevision. The utilization of AI, as proposed by recent studies and with the aid of suitable tools, holds the potential to predict the outcomes of MVI in the near future. This prospect carries significant implications, including the ability to customize procedures more precisely, optimize device and patient selection, and impartially assess anatomical variables [88,89].
8. Conclusions
Transcatheter mitral valve interventions (TMVIs) have experienced significant growth in recent decades, emerging as a well-established alternative for treating mitral regurgitation (MR) in patients ineligible or at high-risk for surgery. Several devices have been developed, with some receiving regulatory approval such as CE mark and/or FDA approval, while others are undergoing evaluation. While the MitraClip system is the most widely utilized, several other devices are emerging as potential therapeutic options, particularly for patients with complex anatomies.
Cardiac imaging assumes a central role in assessing patients undergoing these procedures, requiring skills and knowledge distinct from those of basic echocardiography. This underscores the necessity for a specialized imaging sub-specialty with dedicated expertise [45,90]. Multimodality imaging is crucial throughout the TMVI process, aiding in preoperative evaluation of patient anatomy, predicting potential complications, guiding intraoperative interventions through hybrid imaging techniques, and promptly detecting postoperative complications.
The progress in interventional and imaging fields are inherently intertwined. Technological innovations can yield devices and procedures that are increasingly suitable and effective. Simultaneously, advancements in imaging empower us to make earlier diagnoses, preempting the onset of symptoms and thereby improving prognoses. Furthermore, ongoing research in multimodality imaging, machine learning, and virtual reality may enable us to harness the remarkable capabilities of artificial intelligence (AI) for processing, analysis, and data elaboration. This facilitates the utilization of these technologies not only to enhance the quality of disease treatment, but also for educational purposes.
Author Contributions
Conceptualization, L.B., M.R., F.V., C.L.; writing—original draft preparation, L.B. and M.R.; review and editing, L.B., M.R., C.L., M.F., I.C., F.P., P.T., K.M., M.N., A.M., G.F., G.S., P.E.P., N.S., A.D.R., M.D.E. and F.V.; supervision, F.V., M.R. and C.L. All authors have read and agreed to the published version of the manuscript.
Funding
No external funding received.
Institutional Review Board Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| AI | Artificial Intelligence |
| ASD | Atrial septal defect |
| AV | Atrio-ventricular |
| cMDCT | Contrast multidetector computed tomography |
| CS | Coronary sinus |
| FMR | Functional mitral regurgitation |
| GCV | Great cardiac vein |
| IAS | Interatrial septum |
| IE | Interventional Echocardiographer |
| LA | Left atrium, left atrial |
| LCA | Left circumflex artery |
| LV | Left ventricle, left ventricular |
| LVOT | Left ventricular outflow |
| LVOTO | Left ventricular outflow obstruction |
| MA | Mitral annulus |
| MR | Mitral regurgitation |
| PMR | Primary mitral regurgitation |
| PVL | Paravalvular leak |
| PWD | Pulsed-wave doppler |
| RAE | Radiation exposure |
| SHD | Structural heart disease |
| TEE | Transesophageal Echocardiography |
| TEER | Transcatheter edge-to-edge repair |
| TMVI | Transcatheter mitral valve intervention |
| TMVr | Transcatheter mitral valve repair |
| TMVR | Transcatheter mitral valve replacement |
| TR | Tricuspid regurgitation |
| Vi-MAC | Valve in MAC |
| Vi-R | Valve in ring |
| Vi-V | Valve in valve |
| VR | Virtual reality |
| WMAs | Wall motion abnormalities |
References
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006 Sep 16;368(9540):1005-11. [CrossRef] [PubMed]
- Agricola E, Ielasi A, Oppizzi M, Faggiano P, Ferri L, Calabrese A, Vizzardi E, Alfieri O, Margonato A. Long-term prognosis of medically treated patients with functional mitral regurgitation and left ventricular dysfunction. Eur J Heart Fail. 2009 Jun;11(6):581-7. Epub 2009 Apr 27. [CrossRef] [PubMed]
- Tribouilloy C, Rusinaru D, Grigioni F, Michelena HI, Vanoverschelde JL, Avierinos JF, Barbieri A, Pislaru SV, Russo A, Pasquet A, Théron A, Szymanski C, Lévy F, Enriquez-Sarano M; Mitral Regurgitation International Database (MIDA) Investigators. Long-term mortality associated with left ventricular dysfunction in mitral regurgitation due to flail leaflets: a multicenter analysis. Circ Cardiovasc Imaging. 2014 Mar;7(2):363-70. Epub 2013 Dec 20. [CrossRef] [PubMed]
- Chaput M, Handschumacher MD, Tournoux F, Hua L, Guerrero JL, Vlahakes GJ, Levine RA. Mitral leaflet adaptation to ventricular remodeling: occurrence and adequacy in patients with functional mitral regurgitation. Circulation. 2008 Aug 19;118(8):845-52. Epub 2008 Aug 4. [CrossRef] [PubMed]
- Sannino A, Smith RL 2nd, Schiattarella GG, Trimarco B, Esposito G, Grayburn PA. Survival and Cardiovascular Outcomes of Patients With Secondary Mitral Regurgitation: A Systematic Review and Meta-analysis. JAMA Cardiol. 2017 Oct 1;2(10):1130-1139. [CrossRef] [PubMed]
- Okamoto C, Okada A, Nishimura K, Moriuchi K, Amano M, Takahama H, Amaki M, Hasegawa T, Kanzaki H, Fujita T, Kobayashi J, Yasuda S, Izumi C. Prognostic comparison of atrial and ventricular functional mitral regurgitation. Open Heart. 2021 Feb;8(1):e001574. [CrossRef] [PubMed]
- Silbiger, J.J. Novel pathogenetic mechanisms and structural adaptations in ischemic mitral regurgitation. J Am Soc Echocardiogr. 2013 Oct;26(10):1107-1117. Epub 2013 Aug 14. [CrossRef] [PubMed]
- Deferm S, Bertrand PB, Verbrugge FH, Verhaert D, Rega F, Thomas JD, Vandervoort PM. Atrial Functional Mitral Regurgitation: JACC Review Topic of the Week. J Am Coll Cardiol. 2019 May 21;73(19):2465-2476. [CrossRef] [PubMed]
- Farhan S, Silbiger JJ, Halperin JL, Zhang L, Dukkipati SR, Vogel B, Kini A, Sharma S, Lerakis S. Pathophysiology, Echocardiographic Diagnosis, and Treatment of Atrial Functional Mitral Regurgitation: JACC State-of-the-Art Review. J Am Coll Cardiol. 2022 Dec 13;80(24):2314-2330. Erratum in: J Am Coll Cardiol. 2023 Feb 21;81(7):711. [CrossRef] [PubMed]
- Aranda-Domene R, Canovas SJ. Going further of mitral ring annuloplasty: the role of surgery in atrial functional mitral regurgitation. J Thorac Dis. 2023 May 30;15(5):2381-2384. Epub 2023 Apr 11. [CrossRef] [PubMed]
- Hirji SA, Cote CL, Javadikasgari H, Malarczyk A, McGurk S, Kaneko T. Atrial functional versus ventricular functional mitral regurgitation: Prognostic implications. J Thorac Cardiovasc Surg. 2022 Dec;164(6):1808-1815.e4. Epub 2020 Dec 31. [CrossRef] [PubMed]
- Alec Vahanian, Friedhelm Beyersdorf, Fabien Praz, Milan Milojevic, Stephan Baldus, Johann Bauersachs, Davide Capodanno, Lenard Conradi, Michele De Bonis, Ruggero De Paulis, Victoria Delgado, Nick Freemantle, Martine Gilard, Kristina H Haugaa, Anders Jeppsson, Peter Jüni, Luc Pierard, Bernard D Prendergast, J Rafael Sádaba, Christophe Tribouilloy, Wojtek Wojakowski, ESC/EACTS Scientific Document Group, ESC National Cardiac Societies, 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS), European Heart Journal, Volume 43, Issue 7, 14 February 2022, Pages 561–632. [CrossRef]
- Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Détaint D, Vanoverschelde JL, Butchart EG, Ravaud P, Vahanian A. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery? Eur Heart J. 2007 Jun;28(11):1358-65. Epub 2007 Mar 9. [CrossRef] [PubMed]
- Feldman T, Kar S, Rinaldi M, Fail P, Hermiller J, Smalling R, Whitlow PL, Gray W, Low R, Herrmann HC, Lim S, Foster E, Glower D; EVEREST Investigators. Percutaneous mitral repair with the MitraClip system: safety and midterm durability in the initial EVEREST (Endovascular Valve Edge-to-Edge REpair Study) cohort. J Am Coll Cardiol. 2009 Aug 18;54(8):686-94. [CrossRef] [PubMed]
- Feldman T, Kar S, Elmariah S, Smart SC, Trento A, Siegel RJ, Apruzzese P, Fail P, Rinaldi MJ, Smalling RW, Hermiller JB, Heimansohn D, Gray WA, Grayburn PA, Mack MJ, Lim DS, Ailawadi G, Herrmann HC, Acker MA, Silvestry FE, Foster E, Wang A, Glower DD, Mauri L; EVEREST II Investigators. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. J Am Coll Cardiol. 2015 Dec 29;66(25):2844-2854. [CrossRef] [PubMed]
- Obadia JF, Messika-Zeitoun D, Leurent G, Iung B, Bonnet G, Piriou N, Lefèvre T, Piot C, Rouleau F, Carrié D, Nejjari M, Ohlmann P, Leclercq F, Saint Etienne C, Teiger E, Leroux L, Karam N, Michel N, Gilard M, Donal E, Trochu JN, Cormier B, Armoiry X, Boutitie F, Maucort-Boulch D, Barnel C, Samson G, Guerin P, Vahanian A, Mewton N; MITRA-FR Investigators. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N Engl J Med. 2018 Dec 13;379(24):2297-2306. Epub 2018 Aug 27. [CrossRef] [PubMed]
- Stone GW, Abraham WT, Lindenfeld J, Kar S, Grayburn PA, Lim DS, Mishell JM, Whisenant B, Rinaldi M, Kapadia SR, Rajagopal V, Sarembock IJ, Brieke A, Marx SO, Cohen DJ, Asch FM, Mack MJ; COAPT Investigators. Five-Year Follow-up after Transcatheter Repair of Secondary Mitral Regurgitation. N Engl J Med. 2023 Jun 1;388(22):2037-2048. Epub 2023 Mar 5. [CrossRef] [PubMed]
- Doldi PM, Stolz L, Kalbacher D, Köll B, Geyer M, Ludwig S, Orban M, Braun D, Weckbach LT, Stocker TJ, Näbauer M, Higuchi S, Ruf T, Da Rocha E Silva J, Wild M, Tence N, Unterhuber M, Schofer N, Petrescu A, Thiele H, Lurz P, Lubos E, von Bardeleben S, Karam N, Samim D, Paradis JM, Iliadis C, Xhepa E, Hagl C, Massberg S, Hausleiter J; EuroSMR and PRIME-MR Investigators. Right ventricular dysfunction predicts outcome after transcatheter mitral valve repair for primary mitral valve regurgitation. Eur J Heart Fail. 2022 Nov;24(11):2162-2171. Epub 2022 Sep 15. [CrossRef] [PubMed]
- Karam N, Stolz L, Orban M, Deseive S, Praz F, Kalbacher D, Westermann D, Braun D, Näbauer M, Neuss M, Butter C, Kassar M, Petrescu A, Pfister R, Iliadis C, Unterhuber M, Park SD, Thiele H, Baldus S, von Bardeleben RS, Blankenberg S, Massberg S, Windecker S, Lurz P, Hausleiter J. Impact of Right Ventricular Dysfunction on Outcomes After Transcatheter Edge-to-Edge Repair for Secondary Mitral Regurgitation. JACC Cardiovasc Imaging. 2021 Apr;14(4):768-778. Epub 2021 Feb 10. [CrossRef] [PubMed]
- Shechter A, Vaturi M, Kaewkes D, Koren O, Koseki K, Solanki A, Natanzon SS, Patel V, Skaf S, Makar M, Chakravarty T, Makkar RR, Siegel RJ. Prognostic Value of Baseline Tricuspid Annular Plane Systolic Excursion to Pulmonary Artery Systolic Pressure Ratio in Mitral Transcatheter Edge-to-Edge Repair. J Am Soc Echocardiogr. 2023 Apr;36(4):391-401.e19. Epub 2023 Jan 16. [CrossRef] [PubMed]
- Szerlip M, Spargias KS, Makkar R, Kar S, Kipperman RM, O’Neill WW, Ng MKC, Smith RL, Fam NP, Rinaldi MJ, Raffel OC, Walters DL, Levisay J, Montorfano M, Latib A, Carroll JD, Nickenig G, Windecker S, Marcoff L, Cohen GN, Schäfer U, Webb JG, Lim DS. 2-Year Outcomes for Transcatheter Repair in Patients With Mitral Regurgitation From the CLASP Study. JACC Cardiovasc Interv. 2021 Jul 26;14(14):1538-1548. Epub 2021 May 18. Erratum in: JACC Cardiovasc Interv. 2022 Jul 11;15(13):1395. [CrossRef] [PubMed]
- Zahr F, Smith RL, Gillam LD, Chadderdon S, Makkar R, von Bardeleben RS, Ruf TF, Kipperman RM, Rassi AN, Szerlip M, Goldman S, Inglessis-Azuaje I, Yadav P, Lurz P, Davidson CJ, Mumtaz M, Gada H, Kar S, Kodali SK, Laham R, Hiesinger W, Fam NP, Keßler M, O’Neill WW, Whisenant B, Kliger C, Kapadia S, Rudolph V, Choo J, Hermiller J, Morse MA, Schofer N, Gafoor S, Latib A, Mahoney P, Kaneko T, Shah PB, Riddick JA, Muhammad KI, Boekstegers P, Price MJ, Praz F, Koulogiannis K, Marcoff L, Hausleiter J, Lim DS; CLASP IID Pivotal Trial Investigators. One-Year Outcomes From the CLASP IID Randomized Trial for Degenerative Mitral Regurgitation. JACC Cardiovasc Interv. 2023 Oct 26:S1936-8798(23)01358-4. Epub ahead of print. [CrossRef] [PubMed]
- Schofer J, Siminiak T, Haude M, Herrman JP, Vainer J, Wu JC, Levy WC, Mauri L, Feldman T, Kwong RY, Kaye DM, Duffy SJ, Tübler T, Degen H, Brandt MC, Van Bibber R, Goldberg S, Reuter DG, Hoppe UC. Percutaneous mitral annuloplasty for functional mitral regurgitation: results of the CARILLON Mitral Annuloplasty Device European Union Study. Circulation. 2009 Jul 28;120(4):326-33. Epub 2009 Jul 13. [CrossRef] [PubMed]
- Siminiak T, Wu JC, Haude M, Hoppe UC, Sadowski J, Lipiecki J, Fajadet J, Shah AM, Feldman T, Kaye DM, Goldberg SL, Levy WC, Solomon SD, Reuter DG. Treatment of functional mitral regurgitation by percutaneous annuloplasty: results of the TITAN Trial. Eur J Heart Fail. 2012 Aug;14(8):931-8. Epub 2012 May 21. [CrossRef] [PubMed]
- Lipiecki J, Siminiak T, Sievert H, Müller-Ehmsen J, Degen H, Wu JC, Schandrin C, Kalmucki P, Hofmann I, Reuter D, Goldberg SL, Haude M. Coronary sinus-based percutaneous annuloplasty as treatment for functional mitral regurgitation: the TITAN II trial. Open Heart. 2016 Jul 8;3(2):e000411. [CrossRef] [PubMed]
- Witte KK, Lipiecki J, Siminiak T, Meredith IT, Malkin CJ, Goldberg SL, Stark MA, von Bardeleben RS, Cremer PC, Jaber WA, Celermajer DS, Kaye DM, Sievert H. The REDUCE FMR Trial: A Randomized Sham-Controlled Study of Percutaneous Mitral Annuloplasty in Functional Mitral Regurgitation. JACC Heart Fail. 2019 Nov;7(11):945-955. Epub 2019 Sep 11. [CrossRef] [PubMed]
- Lipiecki J, Kaye DM, Witte KK, Haude M, Kapadia S, Sievert H, Goldberg SL, Levy WC, Siminiak T. Long-Term Survival Following Transcatheter Mitral Valve Repair: Pooled Analysis of Prospective Trials with the Carillon Device. Cardiovasc Revasc Med. 2020 Jun;21(6):712-716. Epub 2020 Feb 25. [CrossRef] [PubMed]
- Messika-Zeitoun D, Nickenig G, Latib A, Kuck KH, Baldus S, Schueler R, La Canna G, Agricola E, Kreidel F, Huntgeburth M, Zuber M, Verta P, Grayburn P, Vahanian A, Maisano F. Transcatheter mitral valve repair for functional mitral regurgitation using the Cardioband system: 1 year outcomes. Eur Heart J. 2019 Feb 1;40(5):466-472. [CrossRef] [PubMed]
- Hegeman RMJJ, Gheorghe LL, de Kroon TL, van Putte BP, Swaans MJ, Klein P. State-of-the-Art Review: Technical and Imaging Considerations in Novel Transapical and Port-Access Mitral Valve Chordal Repair for Degenerative Mitral Regurgitation. Front Cardiovasc Med. 2022 Apr 12;9:850700. [CrossRef] [PubMed]
- Colli A, Zucchetta F, Kliger C, Bellu R, Francone M, Sedati P, Jelnin V, Ruiz CE, Manzan E, Besola L, Bizzotto E, Gerosa G. CT for the Transapical Off-Pump Mitral Valve Repair With Neochord Implantation Procedure. JACC Cardiovasc Imaging. 2017 Nov;10(11):1397-1400. Epub 2017 May 17. [CrossRef] [PubMed]
- Colli A, Bizzotto E, Manzan E, Besola L, Pradegan N, Bellu R, Pittarello D, Gerosa G. Patient-Specific Ventricular Access Site Selection for the NeoChord Mitral Valve Repair Procedure. Ann Thorac Surg. 2017 Aug;104(2):e199-e202. [CrossRef] [PubMed]
- Seeburger J, Rinaldi M, Nielsen SL, Salizzoni S, Lange R, Schoenburg M, Alfieri O, Borger MA, Mohr FW, Aidietis A. Off-pump transapical implantation of artificial neo-chordae to correct mitral regurgitation: the TACT Trial (Transapical Artificial Chordae Tendinae) proof of concept. J Am Coll Cardiol. 2014 Mar 11;63(9):914-9. Epub 2013 Sep 24. [CrossRef] [PubMed]
- Gammie JS, Bartus K, Gackowski A, Szymanski P, Bilewska A, Kusmierczyk M, Kapelak B, Rzucidlo-Resil J, Duncan A, Yadav R, Livesey S, Diprose P, Gerosa G, D’Onofrio A, Pittarello D, Denti P, La Canna G, De Bonis M, Alfieri O, Hung J, Kolsut P, D’Ambra MN. Safety and performance of a novel transventricular beating heart mitral valve repair system: 1-year outcomes. Eur J Cardiothorac Surg. 2021 Jan 4;59(1):199-206. [CrossRef] [PubMed]
- Maisano F, Taramasso M. Mitral valve-in-valve, valve-in-ring, and valve-in-MAC: the Good, the Bad, and the Ugly. Eur Heart J. 2019 Feb 1;40(5):452-455. [CrossRef] [PubMed]
- Singh GD, Smith TW, Boyd WD, Rogers JH. Clipping the Ring: Transcatheter Edge-to-Ring Mitral Valve Repair in a Patient With Prior Mitral Annuloplasty Ring. JACC Cardiovasc Interv. 2018 Apr 9;11(7):e55-e58. Epub 2018 Jan 17. [CrossRef] [PubMed]
- Sorajja P, Gössl M, Babaliaros V, Rizik D, Conradi L, Bae R, Burke RF, Schäfer U, Lisko JC, Riley RD, Guyton R, Dumonteil N, Berthoumieu P, Tchetche D, Blanke P, Cavalcante JL, Sun B. Novel Transcatheter Mitral Valve Prosthesis for Patients With Severe Mitral Annular Calcification. J Am Coll Cardiol. 2019 Sep 17;74(11):1431-1440. [CrossRef] [PubMed]
- Sorajja P, Moat N, Badhwar V, Walters D, Paone G, Bethea B, Bae R, Dahle G, Mumtaz M, Grayburn P, Kapadia S, Babaliaros V, Guerrero M, Satler L, Thourani V, Bedogni F, Rizik D, Denti P, Dumonteil N, Modine T, Sinhal A, Chuang ML, Popma JJ, Blanke P, Leipsic J, Muller D. Initial Feasibility Study of a New Transcatheter Mitral Prosthesis: The First 100 Patients. J Am Coll Cardiol. 2019 Mar 26;73(11):1250-1260. [CrossRef] [PubMed]
- Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, Hahn RT, Han Y, Hung J, Lang RM, Little SH, Shah DJ, Shernan S, Thavendiranathan P, Thomas JD, Weissman NJ. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. 2017 Apr;30(4):303-371. Epub 2017 Mar 14. [CrossRef] [PubMed]
- Lancellotti P, Pibarot P, Chambers J, La Canna G, Pepi M, Dulgheru R, Dweck M, Delgado V, Garbi M, Vannan MA, Montaigne D, Badano L, Maurovich-Horvat P, Pontone G, Vahanian A, Donal E, Cosyns B; Scientific Document Committee of the European Association of Cardiovascular Imaging. Multi-modality imaging assessment of native valvular regurgitation: an EACVI and ESC council of valvular heart disease position paper. Eur Heart J Cardiovasc Imaging. 2022 Apr 18;23(5):e171-e232. [CrossRef] [PubMed]
- Kahlert P, Plicht B, Schenk IM, Janosi RA, Erbel R, Buck T. Direct assessment of size and shape of noncircular vena contracta area in functional versus organic mitral regurgitation using real-time three-dimensional echocardiography. J Am Soc Echocardiogr. 2008 Aug;21(8):912-21. Epub 2008 Apr 2. [CrossRef] [PubMed]
- Fiore G, Ingallina G, Ancona F, Gaspardone C, Biondi F, Margonato D, Morosato M, Belli M, Tavernese A, Stella S, Agricola E. Quantification of Mitral Regurgitation in Mitral Valve Prolapse by Three-Dimensional Vena Contracta Area: Derived Cutoff Values and Comparison With Two-Dimensional Multiparametric Approach. J Am Soc Echocardiogr. 2024 Mar 24:S0894-7317(24)00116-0. Epub ahead of print. [CrossRef] [PubMed]
- Hundley WG, Kizilbash AM, Afridi I, Franco F, Peshock RM, Grayburn PA. Administration of an intravenous perfluorocarbon contrast agent improves echocardiographic determination of left ventricular volumes and ejection fraction: comparison with cine magnetic resonance imaging. J Am Coll Cardiol. 1998 Nov;32(5):1426-32. [CrossRef] [PubMed]
- Barletta V, Hinojar R, Carbonell A, González-Gómez A, Fabiani I, Di Bello V, Jiménez-Nacher JJ, Zamorano J, Fernández-Golfín C. Three-dimensional full automated software in the evaluation of the left ventricle function: from theory to clinical practice. Int J Cardiovasc Imaging. 2018 Aug;34(8):1205-1213. Epub 2018 Mar 31. [CrossRef] [PubMed]
- Hausleiter J, Stocker TJ, Adamo M, Karam N, Swaans MJ, Praz F. Mitral valve transcatheter edge-to-edge repair. EuroIntervention. 2023 Jan 23;18(12):957-976. [CrossRef] [PubMed]
- Agricola E, Ancona F, Bartel T, Brochet E, Dweck M, Faletra F, Lancellotti P, Mahmoud-Elsayed H, Marsan NA, Maurovich-Hovart P, Monaghan M, Pontone G, Sade LE, Swaans M, Von Bardeleben RS, Wunderlich N, Zamorano JL, Popescu BA, Cosyns B, Donal E. Multimodality imaging for patient selection, procedural guidance, and follow-up of transcatheter interventions for structural heart disease: a consensus document of the EACVI Task Force on Interventional Cardiovascular Imaging: part 1: access routes, transcatheter aortic valve implantation, and transcatheter mitral valve interventions. Eur Heart J Cardiovasc Imaging. 2023 Aug 23;24(9):e209-e268. [CrossRef] [PubMed]
- Lesevic H, Karl M, Braun D, Barthel P, Orban M, Pache J, Hadamitzky M, Mehilli J, Stecher L, Massberg S, Ott I, Schunkert H, Kastrati A, Sonne C, Hausleiter J. Long-Term Outcomes After MitraClip Implantation According to the Presence or Absence of EVEREST Inclusion Criteria. Am J Cardiol. 2017 Apr 15;119(8):1255-1261. Epub 2017 Jan 25. [CrossRef] [PubMed]
- Praz F, Windecker S, Kapadia S. PASCAL: A New Addition to the Armamentarium of Transcatheter Repair Systems for Mitral Leaflet Approximation. JACC Cardiovasc Interv. 2019 Jul 22;12(14):1379-1381. Epub 2019 Jun 26. [CrossRef] [PubMed]
- Koell B, Orban M, Weimann J, Kassar M, Karam N, Neuss M, Petrescu A, Iliadis C, Unterhuber M, Adamo M, Giannini C, Melica B, Ludwig S, Massberg S, Praz F, Pfister R, Thiele H, Stephan von Bardeleben R, Baldus S, Butter C, Lurz P, Windecker S, Metra M, Petronio AS, Hausleiter J, Lubos E, Kalbacher D; EuroSMR Investigators. Outcomes Stratified by Adapted Inclusion Criteria After Mitral Edge-to-Edge Repair. J Am Coll Cardiol. 2021 Dec 14;78(24):2408-2421. [CrossRef] [PubMed]
- Piroli F, Boccellino A, Ingallina G, Rolando M, Melillo F, Ancona F, Stella S, Biondi F, Palmisano A, Esposito A, Denti P, Montorfano M, Maisano F, Castiglioni A, Agricola E. Feasibility and reliability of comprehensive three-dimensional transoesophageal echocardiography screening process for transcatheter mitral valve replacement. Eur Heart J Cardiovasc Imaging. 2023 Jul 24;24(8):1043-1051. [CrossRef] [PubMed]
- Kim JH, Kim EY, Jin GY, Choi JB. A Review of the Use of Cardiac Computed Tomography for Evaluating the Mitral Valve before and after Mitral Valve Repair. Korean J Radiol. 2017 Sep-Oct;18(5):773-785. Epub 2017 Jul 17. [CrossRef] [PubMed]
- Koo HJ, Yang DH, Oh SY, Kang JW, Kim DH, Song JK, Lee JW, Chung CH, Lim TH. Demonstration of mitral valve prolapse with CT for planning of mitral valve repair. Radiographics. 2014 Oct;34(6):1537-52. [CrossRef] [PubMed]
- Kishimoto N, Takahashi Y, Fujii H, Sakon Y, Izuta S, Kitada R, Morisaki A, Yoshida H, Ehara S, Shibata T. Computed tomography to identify risk factors for left circumflex artery injury during mitral surgery. Eur J Cardiothorac Surg. 2022 Feb 18;61(3):675-683. [CrossRef] [PubMed]
- Feirer N, Kornyeva A, Lang M, Sideris K, Voss B, Krane M, Lange R, Vitanova K. Non-robotic minimally invasive mitral valve repair: a 20-year single-centre experience. Eur J Cardiothorac Surg. 2022 Oct 4;62(5):ezac223. [CrossRef] [PubMed]
- Bergonzoni E, D’Onofrio A, Mastro F, Gerosa G. Microinvasive mitral valve repair with transapical mitral neochordae implantation. Front Cardiovasc Med. 2023 Jul 28;10:1166892. [CrossRef] [PubMed]
- Colli A, Besola L, Montagner M, Azzolina D, Soriani N, Manzan E, Bizzotto E, Zucchetta F, Bellu R, Pittarello D, Gerosa G. Prognostic impact of leaflet-to-annulus index in patients treated with transapical off-pump echo-guided mitral valve repair with NeoChord implantation. Int J Cardiol. 2018 Apr 15;257:235-237. Epub 2018 Jan 31. [CrossRef] [PubMed]
- Feuchtner GM, Alkadhi H, Karlo C, Sarwar A, Meier A, Dichtl W, Leschka S, Blankstein R, Gruenenfelder J, Stolzmann P, Cury RC. Cardiac CT angiography for the diagnosis of mitral valve prolapse: comparison with echocardiography1. Radiology. 2010 Feb;254(2):374-83. [CrossRef] [PubMed]
- Palmisano A, Nicoletti V, Colantoni C, Monti CB, Pannone L, Vignale D, Darvizeh F, Agricola E, Schaffino S, De Cobelli F, Esposito A. Dynamic changes of mitral valve annulus geometry at preprocedural CT: relationship with functional classes of regurgitation. Eur Radiol Exp. 2021 Aug 13;5(1):34. [CrossRef] [PubMed]
- Suh YJ, Lee S, Chang BC, Shim CY, Hong GR, Choi BW, Kim YJ. Utility of Cardiac CT for Preoperative Evaluation of Mitral Regurgitation: Morphological Evaluation of Mitral Valve and Prediction of Valve Replacement. Korean J Radiol. 2019 Mar;20(3):352-363. [CrossRef] [PubMed]
- Xu B, Kocyigit D, Wang TKM, Tan CD, Rodriguez ER, Pettersson GB, Unai S, Griffin BP. Mitral annular calcification and valvular dysfunction: multimodality imaging evaluation, grading, and management. Eur Heart J Cardiovasc Imaging. 2022 Feb 22;23(3):e111-e122. [CrossRef] [PubMed]
- Koo HJ, Kang JW, Oh SY, Kim DH, Song JM, Kang DH, Song JK, Kim JB, Jung SH, Choo SJ, Chung CH, Lee JW, Yang DH. Cardiac computed tomography for the localization of mitral valve prolapse: scallop-by-scallop comparisons with echocardiography and intraoperative findings. Eur Heart J Cardiovasc Imaging. 2019 May 1;20(5):550-557. [CrossRef] [PubMed]
- Maggiore P, Anastasius M, Huang AL, Blanke P, Leipsic J. Transcatheter Mitral Valve Repair and Replacement: Current Evidence for Intervention and the Role of CT in Preprocedural Planning-A Review for Radiologists and Cardiologists Alike. Radiol Cardiothorac Imaging. 2020 Feb 13;2(1):e190106. [CrossRef] [PubMed]
- Faggioni L, Gabelloni M, Accogli S, Angelillis M, Costa G, Spontoni P, Petronio AS, Caramella D. Preprocedural planning of transcatheter mitral valve interventions by multidetector CT: What the radiologist needs to know. Eur J Radiol Open. 2018 Aug 31;5:131-140. [CrossRef] [PubMed]
- Chiarito M, Sanz-Sanchez J, Pighi M, Cannata F, Rubbio AP, Munafò A, Cao D, Roccasalva F, Pini D, Pagnotta PA, Ettori F, Petronio AS, Tamburino C, Reimers B, Colombo A, Di Mario C, Grasso C, Mehran R, Godino C, Stefanini GG. Edge-to-edge percutaneous mitral repair for functional ischaemic and non-ischaemic mitral regurgitation: a systematic review and meta-analysis. ESC Heart Fail. 2022 Oct;9(5):3177-3187. Epub 2022 Jun 29. [CrossRef] [PubMed]
- Ranganath P, Moore A, Guerrero M, Collins J, Foley T, Williamson E, Rajiah P. CT for Pre- and Postprocedural Evaluation of Transcatheter Mitral Valve Replacement. Radiographics. 2020 Oct;40(6):1528-1553. [CrossRef] [PubMed]
- Blanke P, Dvir D, Naoum C, Cheung A, Ye J, Thériault-Lauzier P, Spaziano M, Boone RH, Wood DA, Piazza N, Webb JG, Leipsic J. Prediction of fluoroscopic angulation and coronary sinus location by CT in the context of transcatheter mitral valve implantation. J Cardiovasc Comput Tomogr. 2015 May-Jun;9(3):183-92. Epub 2015 Mar 3. [CrossRef] [PubMed]
- Thériault-Lauzier P, Andalib A, Martucci G, Mylotte D, Cecere R, Lange R, Tchétché D, Modine T, van Mieghem N, Windecker S, Buithieu J, Piazza N. Fluoroscopic anatomy of left-sided heart structures for transcatheter interventions: insight from multislice computed tomography. JACC Cardiovasc Interv. 2014 Sep;7(9):947-57. Epub 2014 Aug 13. [CrossRef] [PubMed]
- Ingallina G, Rampa L, Dicandia M, Boccellino A, Melillo F, Stella S, Ancona F, Biondi F, Fiore G, Slavich M, Denti P, Maisano F, Montorfano M, Agricola E. Anesthesia-Induced Intraprocedural Downgrading of Mitral Regurgitation During Transcatheter Edge-to-Edge Repair. Am J Cardiol. 2023 Mar 1;190:25-31. Epub 2022 Dec 20. [CrossRef] [PubMed]
- Ikenaga H, Yoshida J, Hayashi A, Nagaura T, Yamaguchi S, Rader F, Siegel RJ, Kar S, Shiota T. Usefulness of Intraprocedural Pulmonary Venous Flow for Predicting Recurrent Mitral Regurgitation and Clinical Outcomes After Percutaneous Mitral Valve Repair With the MitraClip. JACC Cardiovasc Interv. 2019 Jan 28;12(2):140-150. [CrossRef] [PubMed]
- Shuyi Feng, Pengxu Kong, Shouzheng Wang, Fujian Duan, Fengwen Zhang, Yongquan Xie, Zefu Li, Wenchao Li, Xiangbin Pan. Feasibility of a Percutaneous and Non-Fluoroscopic Procedure for Transcatheter Mitral Valve Edge-to-Edge Repair. Rev. Cardiovasc. Med. 2023, 24(12), 346. [CrossRef]
- Pascual I, Pozzoli A, Taramasso M, Maisano F, Ho EC. Fusion imaging for transcatheter mitral and tricuspid interventions. Ann Transl Med. 2020 Aug;8(15):965. [CrossRef] [PubMed]
- Zoghbi WA, Jone PN, Chamsi-Pasha MA, Chen T, Collins KA, Desai MY, Grayburn P, Groves DW, Hahn RT, Little SH, Kruse E, Sanborn D, Shah SB, Sugeng L, Swaminathan M, Thaden J, Thavendiranathan P, Tsang W, Weir-McCall JR, Gill E. Guidelines for the Evaluation of Prosthetic Valve Function With Cardiovascular Imaging: A Report From the American Society of Echocardiography Developed in Collaboration With the Society for Cardiovascular Magnetic Resonance and the Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2024 Jan;37(1):2-63. [CrossRef] [PubMed]
- Gheorghe L, Ielasi A, Rensing BJWM, Eefting FD, Timmers L, Latib A, Swaans MJ. Complications Following Percutaneous Mitral Valve Repair. Front Cardiovasc Med. 2019 Oct 18;6:146. [CrossRef] [PubMed]
- Perl L, Kheifets M, Guido A, Agricola E, Denti P, Wild MG, Praz F, Rubbio AP, Bedogni F, De Marco F, Beeri R, Shuvy M, Melillo F, Montorfano M, Freixa X, de la Fuente Mancera JC, Giordano A, Finizio F, Van Mieghem NM, Ooms JFW, Fam N, O’Connor C, Toggweiler S, Levi A, Shapira Y, Schwartzenberg S, Pidello S, D’Ascenzo F, Angelini F, Haberman D, Crimi G, Porto I, Cozzi O, Giannini F, Tarantini G, Maisano F, Kornowski R; MITRA-EF study *. Acute Reduction in Left Ventricular Function Following Transcatheter Mitral Edge-to-Edge Repair. J Am Heart Assoc. 2023 Jul 4;12(13):e029735. Epub 2023 Jun 22. [CrossRef] [PubMed]
- Utsunomiya H, Itabashi Y, Kobayashi S, Rader F, Hussaini A, Makar M, Trento A, Siegel RJ, Kar S, Shiota T. Effect of Percutaneous Edge-to-Edge Repair on Mitral Valve Area and Its Association With Pulmonary Hypertension and Outcomes. Am J Cardiol. 2017 Aug 15;120(4):662-669. Epub 2017 May 30. [CrossRef] [PubMed]
- Paukovitsch M, Schneider LM, Reichart C, Nita N, Rottbauer W, Keßler M, Markovic S. Prevalence of iatrogenic atrial septal defects (iASD) after mitral valve (MV) transcatheter edge-to-edge repair (TEER) in the long-term follow-up. Open Heart. 2021 Oct;8(2):e001732. [CrossRef] [PubMed]
- Beri N, Singh GD, Smith TW, Fan D, Boyd WD, Rogers JH. Iatrogenic atrial septal defect closure after transseptal mitral valve interventions: Indications and outcomes. Catheter Cardiovasc Interv. 2019 Nov 15;94(6):829-836. Epub 2019 Apr 19. [CrossRef] [PubMed]
- Kargoli F, Pagnesi M, Rahgozar K, Goldberg Y, Ho E, Chau M, Colombo A, Latib A. Current Devices and Complications Related to Transcatheter Mitral Valve Replacement: The Bumpy Road to the Top. Front Cardiovasc Med. 2021 Jun 11;8:639058. [CrossRef] [PubMed]
- Heiser L, Gohmann RF, Noack T, Renatus K, Lurz P, Thiele H, Seitz P, Gutberlet M. CT Planning prior to Transcatheter Mitral Valve Replacement (TMVR). Rofo. 2022 Apr;194(4):e1. English. Epub 2022 Apr 20. Erratum for: Rofo. 2022 Apr;194(4):373-383. [CrossRef] [PubMed]
- Bapat VV, Khaliel F, Ihleberg L. Delayed migration of Sapien valve following a transcatheter mitral valve-in-valve implantation. Catheter Cardiovasc Interv. 2014 Jan 1;83(1):E150-4. Epub 2013 Aug 12. [CrossRef] [PubMed]
- Crowhurst JA, Scalia GM, Whitby M, Murdoch D, Robinson BJ, Turner A, Johnston L, Margale S, Natani S, Clarke A, Burstow DJ, Raffel OC, Walters DL. Radiation Exposure of Operators Performing Transesophageal Echocardiography During Percutaneous Structural Cardiac Interventions. J Am Coll Cardiol. 2018 Mar 20;71(11):1246-1254. [CrossRef] [PubMed]
- Corrigan FE 3rd, Hall MJ, Iturbe JM, Condado JF, Kamioka N, Howell S, Thourani VH, Clements SD, Babaliaros VC, Lerakis S. Radioprotective strategies for interventional echocardiographers during structural heart interventions. Catheter Cardiovasc Interv. 2019 Feb 1;93(2):356-361. Epub 2018 Sep 9. [CrossRef] [PubMed]
- Paulus MG, Meindl C, Hamerle M, Schach C, Maier LS, Debl K, Birner C, Unsöld B. Reduction of radiation exposure during transcatheter edge-to-edge mitral valve repair. Catheter Cardiovasc Interv. 2022 Mar;99(4):1259-1267. Epub 2022 Jan 27. [CrossRef] [PubMed]
- Melillo F, Fisicaro A, Stella S, Ancona F, Capogrosso C, Ingallina G, Maccagni D, Romano V, Ruggeri S, Godino C, Latib A, Montorfano M, Colombo A, Agricola E. Systematic Fluoroscopic-Echocardiographic Fusion Imaging Protocol for Transcatheter Edge-to-Edge Mitral Valve Repair Intraprocedural Monitoring. J Am Soc Echocardiogr. 2021 Jun;34(6):604-613. Epub 2021 Jan 13. [CrossRef] [PubMed]
- Faza NN, Harb SC, Wang DD, van den Dorpel MMP, Van Mieghem N, Little SH. Physical and Computational Modeling for Transcatheter Structural Heart Interventions. JACC Cardiovasc Imaging. 2024 Apr;17(4):428-440. [CrossRef] [PubMed]
- Faza NN, Özden Tok Ö, Hahn RT. Imaging in Structural Heart Disease: The Evolution of a New Subspecialty. JACC Case Rep. 2019 Oct 2;1(3):440-445. [CrossRef] [PubMed]
- Złahoda-Huzior A, Januska J, Hecko J, Khokhar A, Dudek D. Virtual reality-assisted heart team consultation for complex structural heart intervention. Eur Heart J Case Rep. 2022 Dec 13;7(1):ytac477. [CrossRef] [PubMed]
- Veulemans V, Hellhammer K, Polzin A, Bönner F, Zeus T, Kelm M. Current and future aspects of multimodal and fusion imaging in structural and coronary heart disease. Clin Res Cardiol. 2018 Aug;107(Suppl 2):49-54. Epub 2018 Jun 12. [CrossRef] [PubMed]
- Dabiri Y, Yao J, Mahadevan VS, Gruber D, Arnaout R, Gentzsch W, Guccione JM, Kassab GS. Mitral Valve Atlas for Artificial Intelligence Predictions of MitraClip Intervention Outcomes. Front Cardiovasc Med. 2021 Dec 10;8:759675. [CrossRef] [PubMed]
- Dabiri Y, Mahadevan VS, Guccione JM, Kassab GS. Machine learning used for simulation of MitraClip intervention: A proof-of-concept study. Front Genet. 2023 Mar 9;14:1142446. [CrossRef] [PubMed]
- Little SH, Rigolin VH, Garcia-Sayan E, Hahn RT, Hung J, Mackensen GB, Mankad S, Quader N, Saric M. Recommendations for Special Competency in Echocardiographic Guidance of Structural Heart Disease Interventions: From the American Society of Echocardiography. J Am Soc Echocardiogr. 2023 Apr;36(4):350-365. Epub 2023 Feb 24. [CrossRef] [PubMed]
Figure 1.
Carpentier’s classification of MR. Ischemic: papillary muscles displacement/dysfunction, asynchrony. Non-ischemic: dilated cardiomyopathy, asynchrony. LVOT, left ventricular outflow tract; SAM, systolic anterior movement.
Figure 1.
Carpentier’s classification of MR. Ischemic: papillary muscles displacement/dysfunction, asynchrony. Non-ischemic: dilated cardiomyopathy, asynchrony. LVOT, left ventricular outflow tract; SAM, systolic anterior movement.
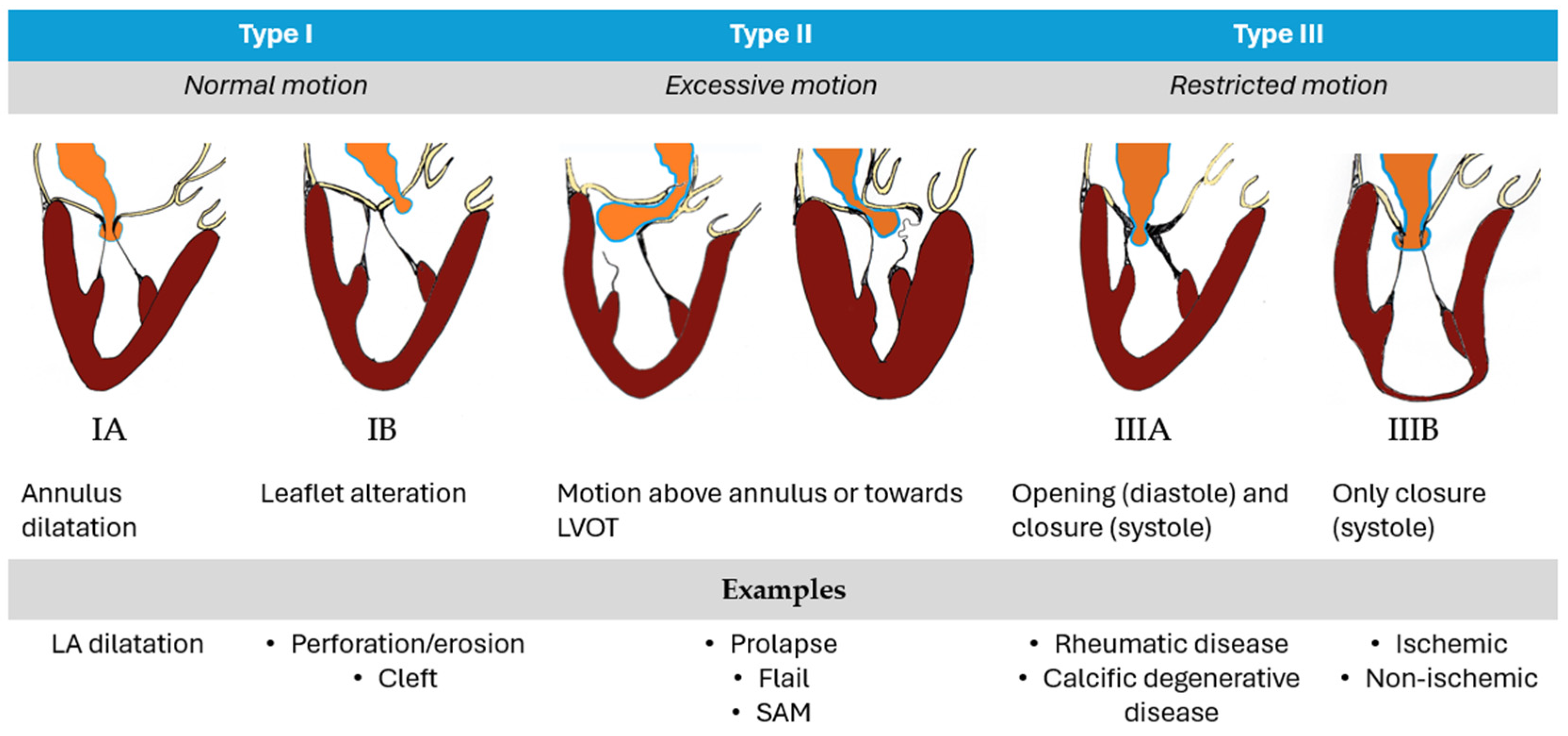
Figure 3.
Evolution of MitraClip System through different generation devices.
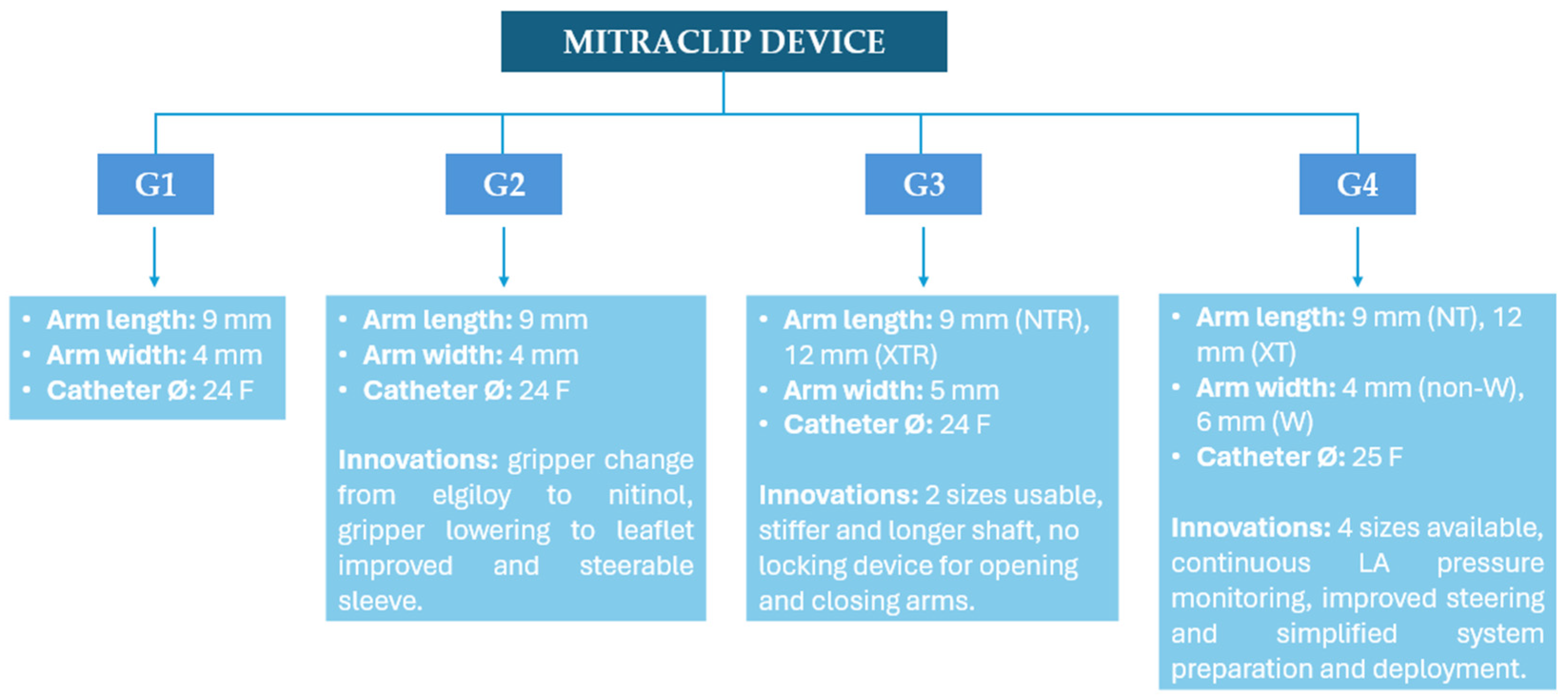
Figure 4.
Tendyne valve see from lateral (left) and overhead perspective (right). The black dark line corresponds to the valve. The red line to the sealing portion of the device. Courtesy of Abbott.
Figure 4.
Tendyne valve see from lateral (left) and overhead perspective (right). The black dark line corresponds to the valve. The red line to the sealing portion of the device. Courtesy of Abbott.
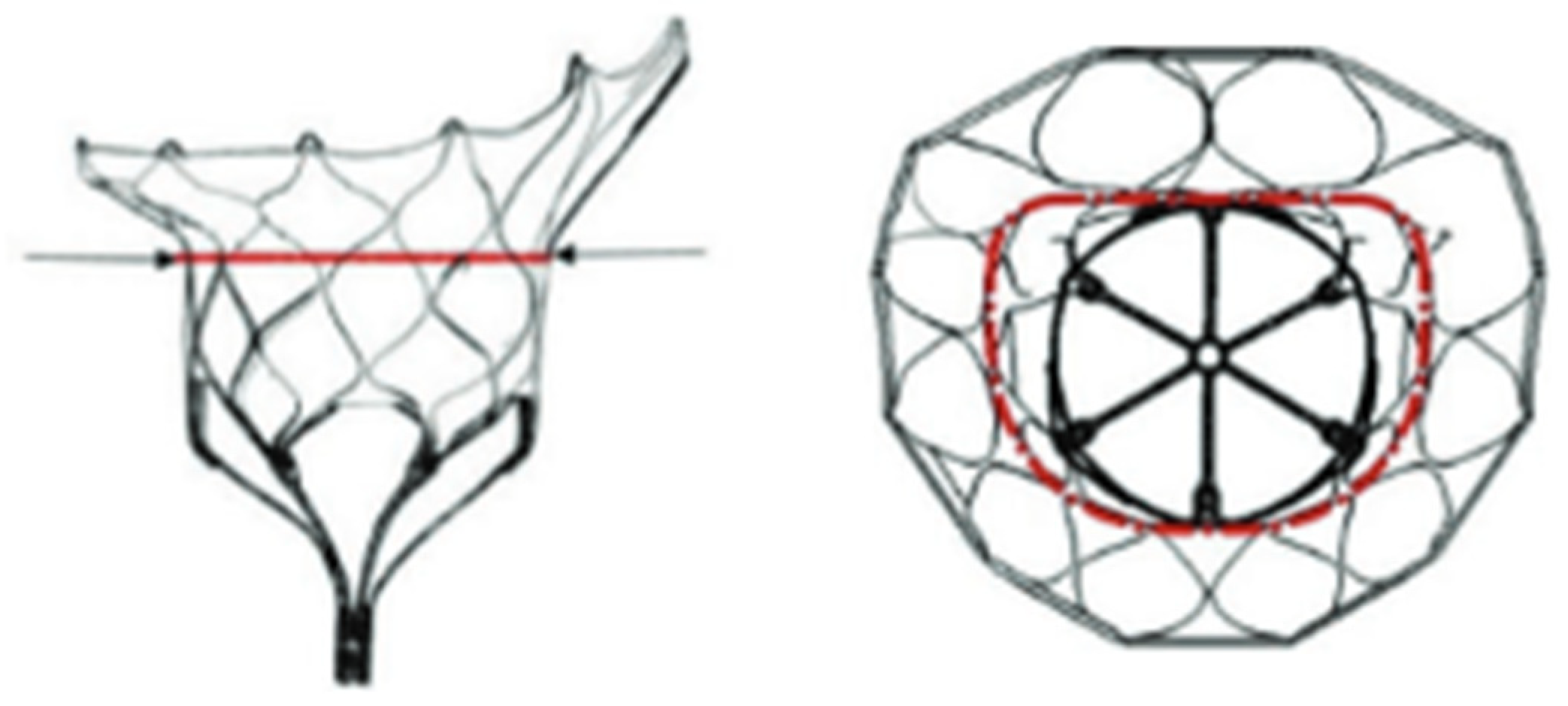
Figure 5.
3D Color transillumination rendering of LAX ME view of MR and vena contracta (red line). Abbreviations as in the text.
Figure 5.
3D Color transillumination rendering of LAX ME view of MR and vena contracta (red line). Abbreviations as in the text.
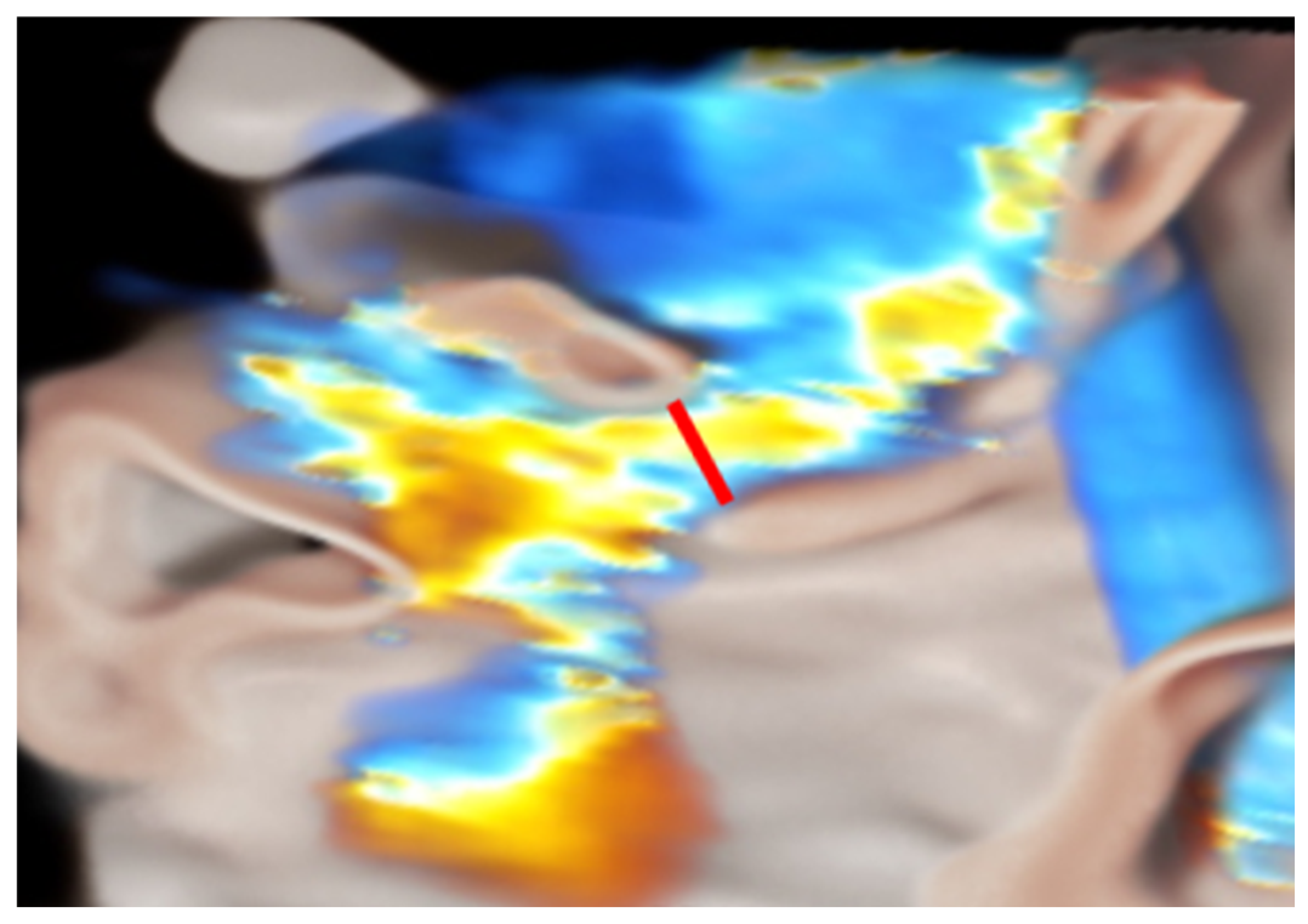
Figure 6.
Common criteria adopted to choose MVR. Abbreviations as in the text.
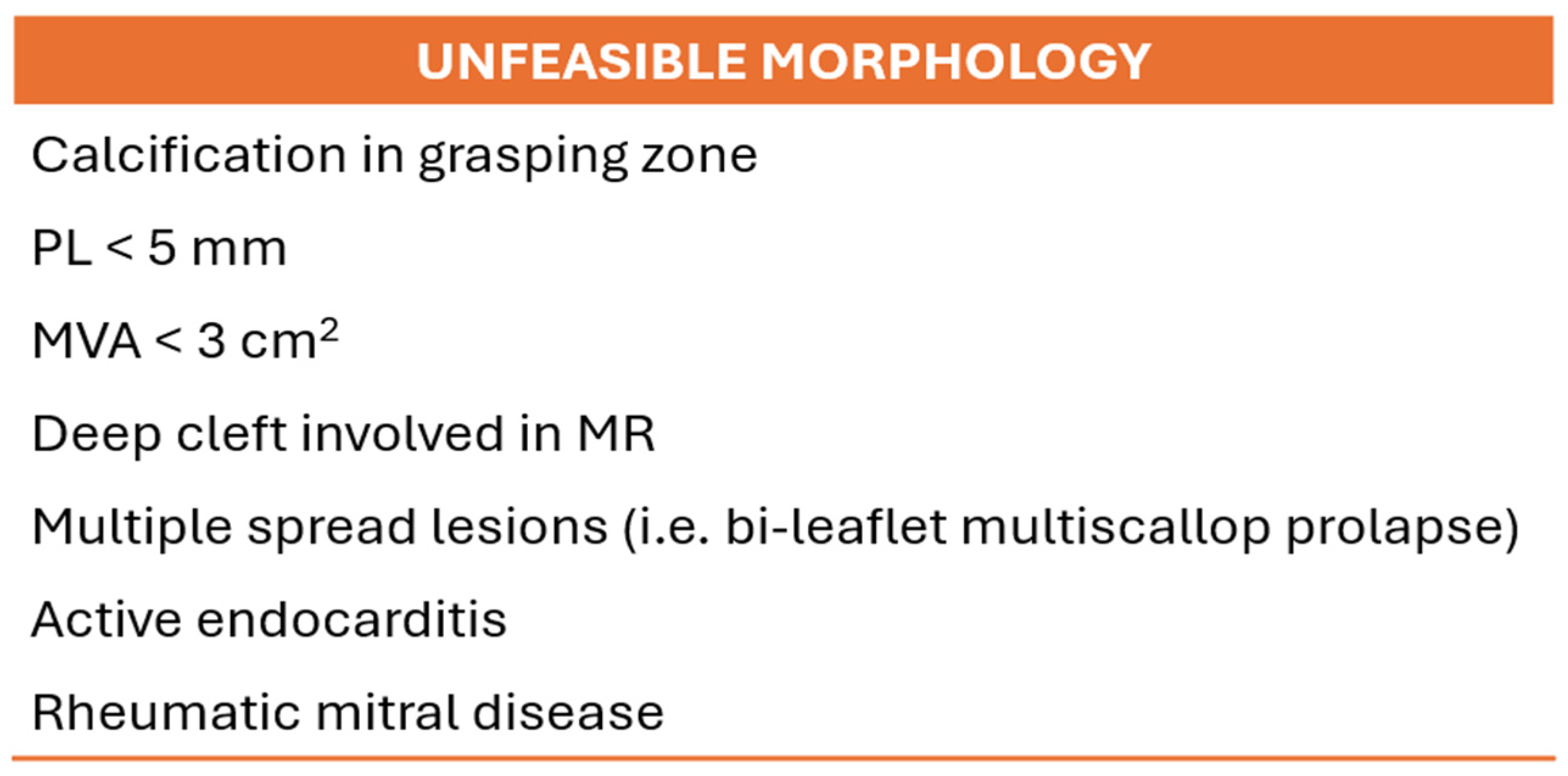
Figure 7.
(Left) LAI; yellow line is the PL length, green line the AL length and orange dotted line the AP diameter. (Right) Gap Ratio; red line is the PL length and blue line the gap size. Abbreviations as in the text.
Figure 7.
(Left) LAI; yellow line is the PL length, green line the AL length and orange dotted line the AP diameter. (Right) Gap Ratio; red line is the PL length and blue line the gap size. Abbreviations as in the text.
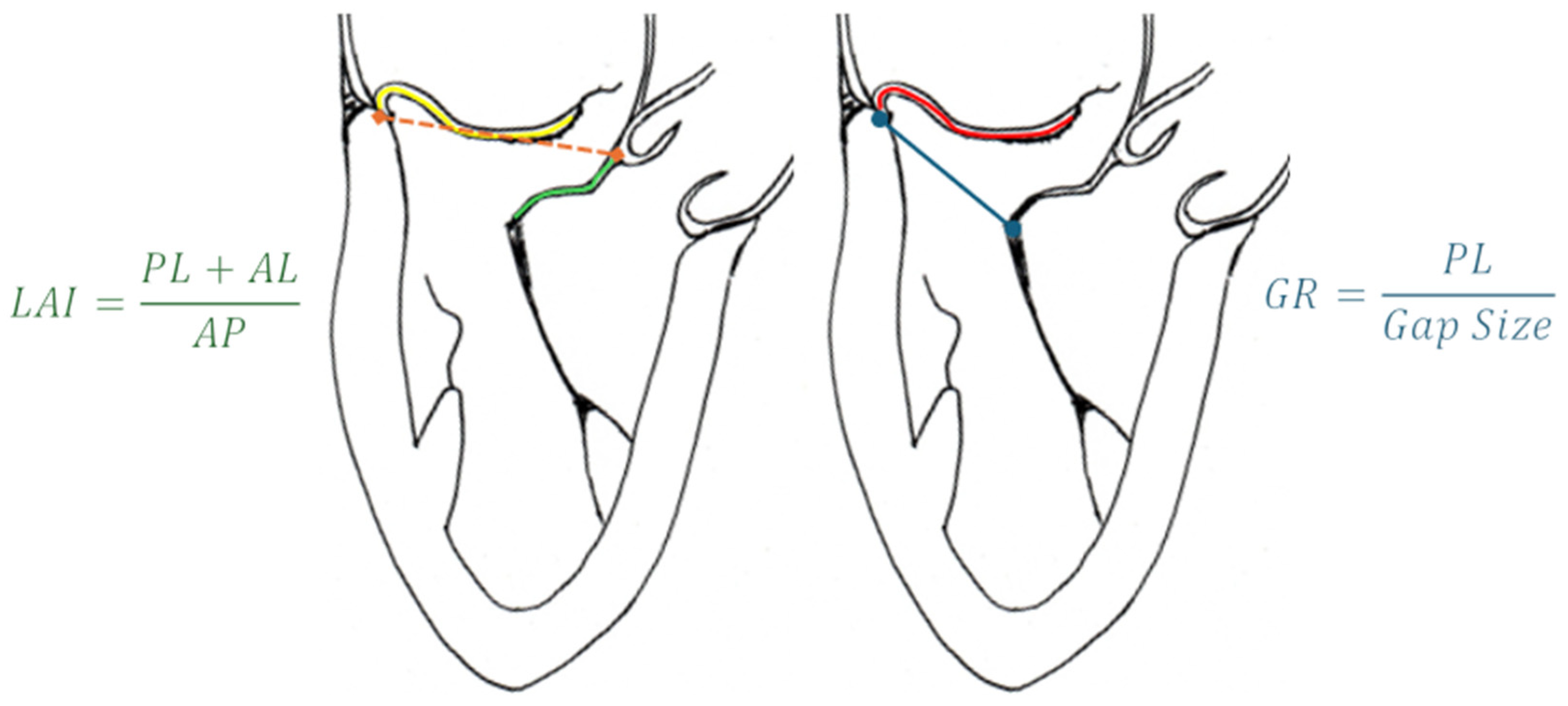
Figure 8.
Straddling step. Image on the left shows a focused representation of SGC and CDS, highlighting the radiopaque markers (adapted from Abbott). Image on the right enlightens the same markers on a fluoroscopic real-time view. (a, b, c and d) are radiopaque markers on the distal portion of CDS. (e) is the radiopaque marker on the SGC. Abbreviation as in the text.
Figure 8.
Straddling step. Image on the left shows a focused representation of SGC and CDS, highlighting the radiopaque markers (adapted from Abbott). Image on the right enlightens the same markers on a fluoroscopic real-time view. (a, b, c and d) are radiopaque markers on the distal portion of CDS. (e) is the radiopaque marker on the SGC. Abbreviation as in the text.

Figure 9.
Steering step (left and central panel) consists of the descend of the device towards the MV plane. The orientation (right panel) is important to ensure a perpendicular alignment with the coaptation line. Abbreviations as in the text.
Figure 9.
Steering step (left and central panel) consists of the descend of the device towards the MV plane. The orientation (right panel) is important to ensure a perpendicular alignment with the coaptation line. Abbreviations as in the text.
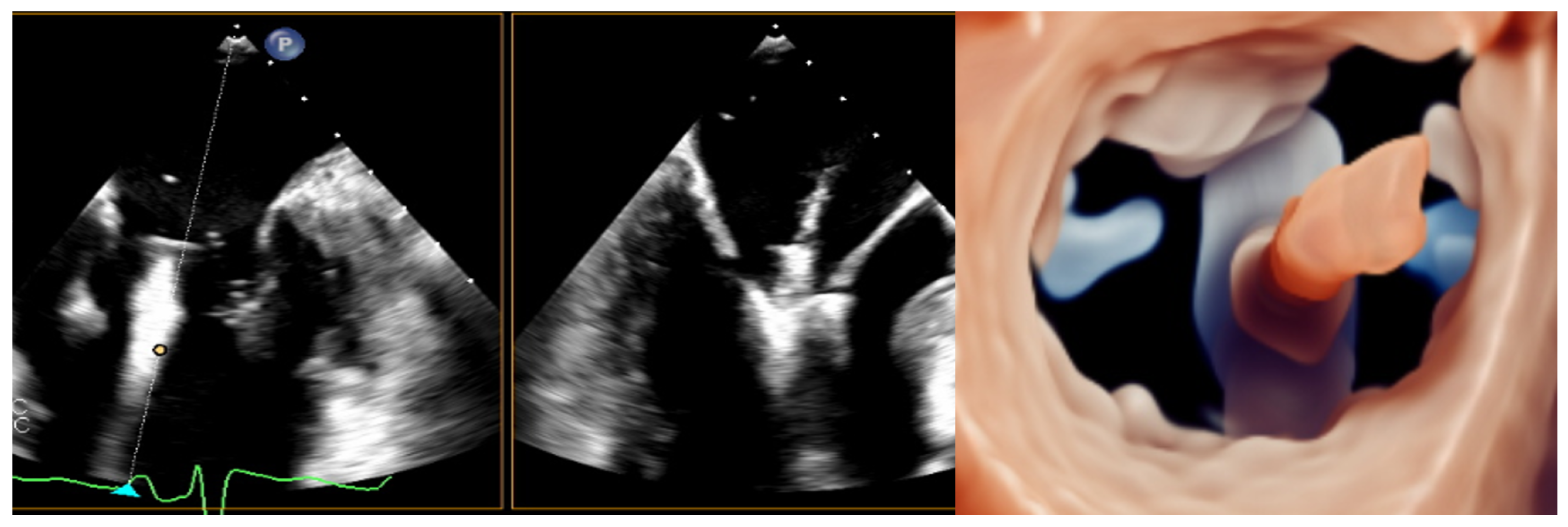
Figure 10.
3D zoom of MV post-clip implantation. The images are visualized from lateral (left), en-face LA side (central) and LV side (right) view, using transillumination tools, decreasing transparency to lower values. Abbreviations as in the text.
Figure 10.
3D zoom of MV post-clip implantation. The images are visualized from lateral (left), en-face LA side (central) and LV side (right) view, using transillumination tools, decreasing transparency to lower values. Abbreviations as in the text.
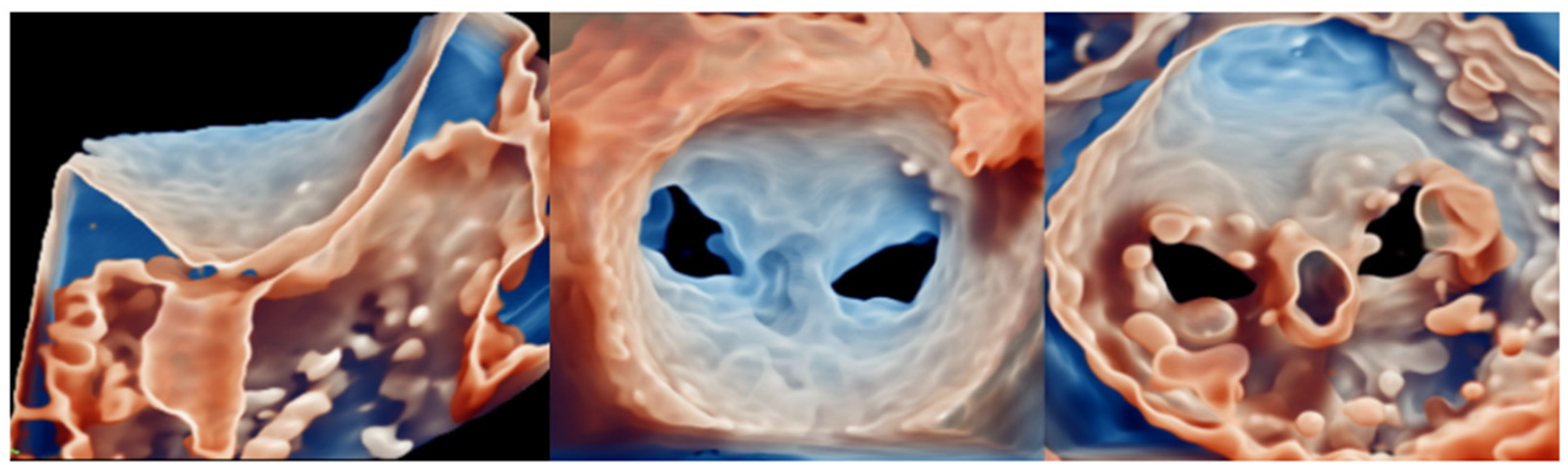
Figure 11.
CS venography with sizing measurements (left, courtesy of Cardiac Dimension) and Carillon XE2 sizing chart (right). Note that the distal anchor must be placed in a target zone with a minimum diameter of 3.5 mm, whereas the proximal anchor in a target zone with a maximum diameter of 13.5 mm. Abbreviations as in the text.
Figure 11.
CS venography with sizing measurements (left, courtesy of Cardiac Dimension) and Carillon XE2 sizing chart (right). Note that the distal anchor must be placed in a target zone with a minimum diameter of 3.5 mm, whereas the proximal anchor in a target zone with a maximum diameter of 13.5 mm. Abbreviations as in the text.
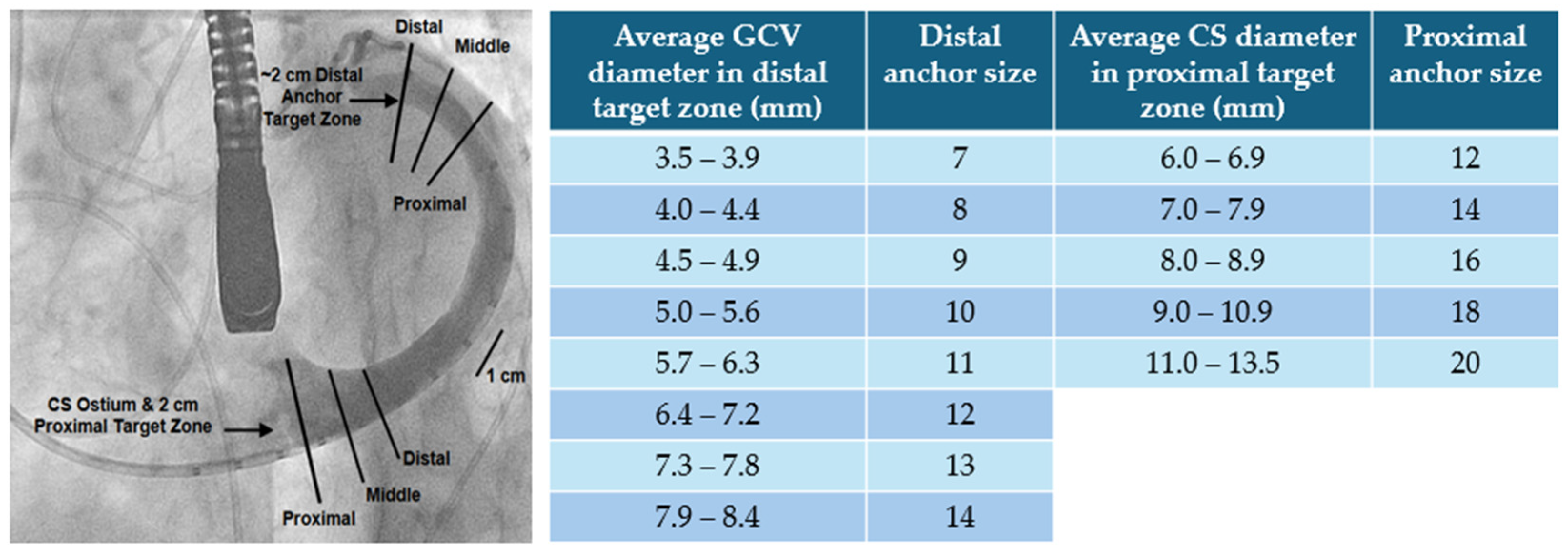

Table 1.
Sizing chart of Tendyne valve. AP, antero-posterior diameter. IC, intercommissural diameter. EOA, effective orifice area.
Table 1.
Sizing chart of Tendyne valve. AP, antero-posterior diameter. IC, intercommissural diameter. EOA, effective orifice area.
| Model | Number | AP (mm) | IC (mm) | Perimeter (mm) | EOA (cm2) |
|---|---|---|---|---|---|
| SP | 33S | 32.5 | 43.5 | 130 | 3.0 |
| 33M | 32.5 | 46.5 | 136 | ||
| 33L | 32.5 | 50.5 | 144 | ||
| 35M | 34.5 | 48.5 | 144 | ||
| 37S | 36.5 | 46.5 | 144 | ||
| 37L | 36.5 | 52.5 | 156 | ||
| 39M | 38.5 | 50.5 | 156 | ||
| 41S | 40.5 | 47.5 | 154 | ||
| LP | 29S | 29.0 | 42.5 | 119 | 2.2 |
| 29L | 29.0 | 47.5 | 129 | ||
| 33S | 32.5 | 43.5 | 130 | ||
| 35M | 34.5 | 48.5 | 144 | ||
| 37M | 36.5 | 49.5 | 150 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



