Submitted:
10 June 2024
Posted:
12 June 2024
You are already at the latest version
Abstract
Van Wyk Grumbach syndrome refers to the development of peripheral precocious puberty, long-standing hypothyroidism, and gonadal masses; when not diagnosed, an unnecessary gonadectomy may be done; Here we present a case of a 10-year-old girl with Down syndrome, short stature, and vitiligo presented with vaginal bleeding, and a pelvic mass, in whom bilateral gonadectomy was performed. Most cases of Van Wyk Grumbach syndrome present in women, and classic hypothyroidism symptoms always precede the diagnosis; 11% of patients have Down Syndrome, sometimes tumor markers get elevated, and some develop severe symptoms (myopathy, short stature, mental delay, ascites, pericardial effusion, Cullen sign, pituitary hyperplasia, and severe anemia), that respond to levothyroxine treatment; Conclusions: Children with peripheral precocious puberty and gonadal masses, must be studied for hypothyroidism before any radical decision is made. Keywords: Puberty, Precocious; Ovarian Cysts, gonadectomy, Van Wyk Grumbach Syndrome
Keywords:
Puberty
; Precocious
; Ovarian Cysts
; gonadectomy
; Van Wyk Grumbach Syndrome
1. Introduction
Unnecessary gonadectomies are frequent in girls with benign ovarian masses (21 to 77% of cases), resulting in infertility, osteopenia, and increased cardiovascular risk. Preoperative risk stratification algorithms can reduce unnecessary oophorectomies and prevent negative lifelong consequences [1,2].
Hypothyroidism has a significant burden of disease [3]; congenital hypothyroidism affects 1:2000 to 1/4000 newborns, but the screening only covers 30% of them worldwide [4,5]. Hypothyroidism symptoms are subtle and insidious, so populations with high risk, such as people with Down syndrome, must be screened annually to prevent severe symptoms (short stature, pericardial effusion, muscle injury, dyslipidemia, mental retardation) [6].
Thyroid-stimulating hormone (TSH) can activate the human FSH receptor because glycoproteins share a common α-subunit. As a result, hypothyroidism patients may present symptoms related to FSH stimulation, including precocious puberty and ovary cysts[7].
We present the case of a girl with Down syndrome who underwent bilateral gonadectomy for benign cysts caused by a non-treated chronic primary hypothyroidism. Moreover, we analyze the literature related to the Van Wyk-Grumbach Syndrome.
2. Materials and Methods
We present a case and review the literature. In brief, the terms van Wyk Grumbach Syndrome, precocious puberty, ovarian cyst, children, and hypothyroidism were searched in PubMed, Imbiomed, Google Academic, and Scopus. We included all articles that describe Van Wyk Syndrome compatible phenotype. From each article, we described the sex, age at presentation in the hospital, age at first hypothyroidism sign, continent of origin, comorbidities, hypothyroidism typical signs, bone age, height in cm, height in standard deviation by CDC charts, TSH concentration at diagnosis, pubertal sings, severe hypothyroidism signs, ultrasound findings, surgical treatment. SPSS V25 was used to analyze data.
3. Results
3.1. Case Presentation
A 10 year-old female with Down syndrome (karyotype 47XX(20)+21), vitiligo, and a two-month history of vaginal bleeding presented to Pediatric consultation with abdominal pain. An abdominopelvic ultrasound revealed an ovarian tumor of 21 x 8 cm.
The patient was referred to our hospital, where a second ultrasound found anechoic abdominal lesions with a round, dense material inside. A subsequent CT showed two pelvic lesions of 20 HU, one of 174 cc (right ovary) and the other of 333 cc (left ovary). The left one had a round interior image of 250 HU inside. The radiological diagnosis was adnexal vs. mesenteric cystic tumors (Figure 1a,b). Blood tumor markers were negative (Table 1).
A bilateral gonadectomy and salpingectomy were performed on the patient, and the histopathological study found normal salpinges, mucinous cystadenoma, and follicular cysts of the ovaries.
Biochemical tests performed after surgery because of Down syndrome showed severe primary hypothyroidism, LH suppression, elevated estrogens, and hyperlipidemia (Table 1). An endocrine-targeted approach of the patient revealed a history of asthenia, bone pain, progressive weight gain, and dry skin one year before surgery, obesity (BMI 59.7 Kg/m2), short stature (120 cm), and signs of peripheral puberty (Tanner stage 1 in breast and pubic hair, and vaginal bleeding).
Finally, a Van Wyk-Grumbach syndrome (severe primary hypothyroidism and isosexual peripheral precocious puberty) was diagnosed; she was treated with levothyroxine, and obesity, dry skin, asthenia, and short stature were resolved. Sexual hormone replacement started at the age of 13 years.
3.2. Literature Review
We found 54 patients reported with Van Wyk-Grumbach syndrome [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53], most from Asia. Their main characteristics are in Table 2, Table 3, Table 4, Table 5, Table 6, Table 7 and Table 8. The age at diagnosis was from 1.5 to 24 years. Every but one [12] case had typical hypothyroidism findings, and short stature was present in more than 60% of the patients. The most common symptoms that led to the diagnosis were abdominal pain and vaginal bleeding. Other manifestations were severe anemia [27,28,30,33], ascites [12,28,35], ovarian torsion [13,52], intracranial mass effect [21], and Cullen’s sign [45]. Ultrasound findings included cysts in 80% of cases and complex images in 6.7%. In some cases, tumor markers were measured (31.5%), resulting in positive in less than one-fifth of the cases (18.5%). Although thyroid substitution can reverse ovary cysts, seven patients underwent surgery (13%) (11,24,44,51), and in one case, an oophorectomy was avoided just in time [10].
4. Discussion
Van Wyk-Grumbach syndrome is caused by peripheral gonadal stimulation mediated by elevated TSH, which results in peripheral precocious puberty. Absent negative feedback by thyroid hormones causes pituitary hyperplasia. Gonadal enlargement and vaginal bleeding in girls can lead to gonadectomy and subsequent lifetime hormonal function loss [19].
The pathophysiology of Van Wyk-Grumbach syndrome remains unclear. It is associated with variable FSH receptor sensitivity and ovarian overstimulation by elevated TSH. This phenomenon is seen not only in children but also in adults with recombinant TSH treatment [54,55,56]. Some cases have demonstrated typical FSH receptors.
In almost every case of Grumbach syndrome, hypothyroidism classic symptoms precede precocious puberty, and some symptoms may be severe or life-threatening, such as severe hypercholesterolemia, anemia, intracranial mass effect, myopathy, galactorrhea, or mental retardation. In some reports, ovarian cysts due to hypothyroidism may elevate tumor markers.
In all cases, treatment with levothyroxine reversed the precocious puberty, the ovarian cysts, the tumor marker elevation, and dyslipidemia. Typical symptoms of hypothyroidism were also improved.
As in this case, delayed diagnosis of hypothyroidism results in unnecessary medical visits, tests, and treatments (gonadotrophin tests for precocious puberty, invasive tests for short stature, surgery).
About 11% of patients with Van Wyk-Grumbach syndrome have Down syndrome. Persons living with Down syndrome must be screened for thyroid disorders annually, before any surgery or when another autoimmune disease appears, 50% will develop any thyroid dysfunction in their lives (hypothyroidism 39%, congenital hypothyroidism 7%, hyperthyroidism 3%) [57] [58].
Irreversible treatment decisions in children, such as gonadectomy, must be based on reliable tools to avoid overtreatment and its long-term consequences [2].
Author Contributions
Conceptualization, Arellano-Llamas and Hernández Caballero; methodology, Arellano-Llamas and Hernández Caballero.; software, Arellano-Llamas and Hernández Caballero.; validation, Delgado-Mendoza and Catalán-Ruiz.; formal analysis, Arellano-Llamas.; investigation, Efren y alejandro.; resources, Arellano-Llamas.; data curation, Arellano-Llamas.; writing—original draft preparation, Arellano-Llamas.; writing—review and editing, Hernández Caballero.; visualization, Hernández Caballero.; supervision, Hernández Caballero.; project administration, Hernández Caballero.; funding acquisition, Hernández Caballero. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
“This research received no external funding”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Instituto Mexicano del Seguro Social (R-2024-3504-023).
Informed Consent Statement
“Written informed consent has been obtained from the patient(s) to publish this paper”.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
We acknowledge Instituto Mexicano del Seguro Social for its support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gonzalez, D.O.; Cooper, J.N.; Aldrink, J.H.; Hewitt, G.D.; Fallat, M.E.; Minneci, P.C.; Deans, K.J. Variability in Surgical Management of Benign Ovarian Neoplasms in Children. J. Pediatr. Surg. 2017, 52, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Minneci, P.C.; Bergus, K.C.; Lutz, C.; Aldrink, J.; Bence, C.; Breech, L.; Dillon, P.A.; Downard, C.; Ehrlich, P.F.; Fallat, M.; et al. Reducing Unnecessary Oophorectomies for Benign Ovarian Neoplasms in Pediatric Patients. JAMA 2023, 330, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Hepp, Z.; Lage, M.J.; Espaillat, R.; Gossain, V.V. The Direct and Indirect Economic Burden of Hypothyroidism in the United States: A Retrospective Claims Database Study. J. Med. Econ. 2021, 24, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Rendón-Macías, M.E.; Morales-García, I.; Huerta-Hernández, E.; Silva-Batalla, A.; Villasís-Keever, M.A. Birth Prevalence of Congenital Hypothyroidism in Mexico. Paediatr. Perinat. Epidemiol. 2008, 22, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Ford, G.; LaFranchi, S.H. Screening for Congenital Hypothyroidism: A Worldwide View of Strategies. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Feldt-Rasmussen, U.; Effraimidis, G.; Bliddal, S.; Klose, M. Risks of Suboptimal and Excessive Thyroid Hormone Replacement across Ages. J. Endocrinol. Invest. 2023. [Google Scholar] [CrossRef] [PubMed]
- Pierce, J.G.; Parsons, T.F. Glycoprotein Hormones: Structure and Function. Annu. Rev. Biochem. 1981, 50, 465–495. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, E.; Högler, W. An Unusual Presentation of Acquired Hypothyroidism: The Van Wyk-Grumbach Syndrome. Eur. J. Endocrinol. 2012, 166, 537–542. [Google Scholar] [CrossRef]
- Barbero, A.; Pagano, M.; Tuli, G.; Buganza, R.; de Sanctis, L.; Bondone, C. Menorrhagia as Main Presentation Sign of Severe Hypothyroidism in a Pediatric Patient: A Case Report. Ital. J. Pediatr. 2022, 48, 171. [Google Scholar] [CrossRef]
- Bhagwat, N.M.; Dalwadi, P.P.; Joshi, A.S.; Pawal, P.S.; Varthakavi, P.K. Asymmetrical Ovarian Enlargement: Caught Timely Before the Cut! J. Pediatr. Adolesc. Gynecol. 2015, 28, e83–85. [Google Scholar] [CrossRef]
- Biswas, M.; Sinha, M.K.; Das, M.K.; Sarkar, S. Van Wyk-Grumbach Syndrome with Hemangioma in an Infant. J. Pediatr. Endocrinol. Metab. JPEM 2018, 31, 1057–1060. [Google Scholar] [CrossRef] [PubMed]
- Browne, L.P.; Boswell, H.B.; Crotty, E.J.; O’Hara, S.M.; Birkemeier, K.L.; Guillerman, R.P. Van Wyk and Grumbach Syndrome Revisited: Imaging and Clinical Findings in Pre- and Postpubertal Girls. Pediatr. Radiol. 2008, 38, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Burns, L.P.; Pennesi, C.M.; Rosen, M.W.; Araya, A.; Baruch, A.; Arnold, M.A.; Quint, E.H. Interdisciplinary Care and a Focus on Fertility Preservation When Multi-Cystic Ovaries Cause Ovarian Torsion: A Case of a 9-Year-Old Girl with Severe, Undiagnosed Hypothyroidism. J. Pediatr. Adolesc. Gynecol. 2020, 33, 723–726. [Google Scholar] [CrossRef] [PubMed]
- Campaner, A.B.; Scapinelli, A.; Machado, R.O.; Dos Santos, R.E.; Beznos, G.W.; Aoki, T. Primary Hypothyroidism Presenting as Ovarian Tumor and Precocious Puberty in a Prepubertal Girl. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2006, 22, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, A.; Kumar, V.; Marulaiah, M. Polycystic Ovaries, Precocious Puberty and Acquired Hypothyroidism: The Van Wyk and Grumbach Syndrome. J. Pediatr. Surg. 2003, 38, 1390–1392. [Google Scholar] [CrossRef] [PubMed]
- Chemaitilly, W.; Trivin, C.; Adan, L.; Gall, V.; Sainte-Rose, C.; Brauner, R. Central Precocious Puberty: Clinical and Laboratory Features. Clin. Endocrinol. (Oxf.) 2001, 54, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Christens, A.; Sevenants, L.; Toelen, J.; Bullens, D.; Casteels, K. Van Wyk and Grumbach Syndrome: An Unusual Form of Precocious Puberty. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2014, 30, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Durbin, K.L.; Diaz-Montes, T.; Loveless, M.B. Van Wyk and Grumbach Syndrome: An Unusual Case and Review of the Literature. J. Pediatr. Adolesc. Gynecol. 2011, 24, e93–96. [Google Scholar] [CrossRef]
- Egodawaththe, N.S.; Seneviratne, S.N.; Gunasekara, S.; Amarasekara, S.M.; Weerasekara, K. Van Wyk-Grumbach Syndrome and Oligosyndactyly in a 6-Year-Old Girl: A Case Report. J. Med. Case Reports 2020, 14, 166. [Google Scholar] [CrossRef]
- Esen, I.; Demirel, F. Hypothyroidism-Associated Testicular Enlargement: Is It a Form of Precocious Puberty or Not? A Case Report. Turk. J. Pediatr. 2011, 53, 210–212. [Google Scholar]
- Guerrero, N.; Athanassaki, I.D.; Sebastian, M.R. Prolonged Untreated Disease and Limited English Proficiency: A Case of Van Wyk-Grumbach Syndrome. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2021, 69, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.M.; Austin, D.J.; Radovick, S.; Laufer, M.R. Primary Hypothyroidism Presenting as Severe Vaginal Bleeding in a Prepubertal Girl. J. Pediatr. Adolesc. Gynecol. 1997, 10, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-J.; Moon, J.-E.; Lee, G.-M.; Cho, M.-H.; Ko, C.W. An Alport Syndrome Boy with Van Wyk-Grumbach Syndrome Induced by Prolonged Untreated Congenital Hypothyroidism. Ann. Pediatr. Endocrinol. Metab. 2020, 25, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.; Lin-Su, K. Van Wyk-Grumbach Syndrome in a Female Pediatric Patient with Trisomy 21: A Case Report. Int. J. Pediatr. Endocrinol. 2020, 2020, 2. [Google Scholar] [CrossRef]
- Hansen, K.A.; Tho, S.P.; Hanly, M.; Moretuzzo, R.W.; McDonough, P.G. Massive Ovarian Enlargement in Primary Hypothyroidism. Fertil. Steril. 1997, 67, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Hunold, A.; Alzen, G.; Wudy, S.A.; Bluetters-Sawatzki, R.; Landmann, E.; Reiter, A.; Wagner, H.-J. Ovarian Tumor in a 12-Year Old Female with Severe Hypothyroidism: A Case of Van Wyk and Grumbach Syndrome. Pediatr. Blood Cancer 2009, 52, 677–679. [Google Scholar] [CrossRef] [PubMed]
- Indumathi, C.K.; Bantwal, G.; Patil, M. Primary Hypothyroidism with Precocious Puberty and Bilateral Cystic Ovaries. Indian J. Pediatr. 2007, 74, 781–783. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, S.; Seth, A.; Puri, A.; Anand, R.; Aneja, S. Ovarian Tumors with Elevated CA-125 Levels and Severe Juvenile Hypothyroidism: A Need for Increased Awareness. Indian J. Pediatr. 2010, 77, 693–694. [Google Scholar] [CrossRef]
- Kubota, K.; Itho, M.; Kishi, H.; Igarashi, S.; Minegishi, T. Primary Hypothyroidism Presenting as Multiple Ovarian Cysts in an Adult Woman: A Case Report. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2008, 24, 586–589. [Google Scholar] [CrossRef]
- Kumar, S.; Mahesh, D.M.; Vignesh, G.; Sagili, H.; Dhanapathi, H.; Hamide, A. Congenital Hypothyroidism Presenting as Menorrhagia in Adulthood. J. Assoc. Physicians India 2013, 61, 660–661. [Google Scholar]
- Leonardi, A.; Penta, L.; Cofini, M.; Lanciotti, L.; Principi, N.; Esposito, S. Rhabdomyolysis in a Young Girl with Van Wyk-Grumbach Syndrome Due to Severe Hashimoto Thyroiditis. Int. J. Environ. Res. Public. Health 2018, 15, 704. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.H.; Kil, H.R.; Kim, J.Y. Unusual Presentations of a Girl with Down Syndrome: Van Wyk-Grumbach Syndrome. J. Pediatr. Endocrinol. Metab. JPEM 2012, 25, 1209–1212. [Google Scholar] [CrossRef] [PubMed]
- Marr, A.; Hardy, K.; Curtis, J. A 14-Year-Old Girl with Short Stature, Incomplete Puberty and Severe Menstrual Bleeding. Paediatr. Child Health 2018, 23, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Guzmán, L.; Sandoval-Benítez, M.; Núñez-Hernández, J.; Sánchez-Castillo, J. Virilización Secundaria a Hiperandrogenismo Ovárico En Síndrome de Van Wyk-Grumbach: Reporte de Un Caso. Arch Inv Mat Inf 2015, 7, 104–106. [Google Scholar]
- Motamed, F.; Eftekhari, K.; Kiani, M.A.; Rabbani, A. Ovarian Cyst Enlargement in a 14 Year Old Female with Persistent Ascities, Severe Hypothyroidism and Elevated Serum CA-125 Level. Iran. Red Crescent Med. J. 2012, 14, 379–381. [Google Scholar] [PubMed]
- Oden Akman, A.; Tayfun, M.; Demirel, F.; Ucakturk, S.A.; Gungor, A. Association of Van Wyk Grumbach and Debre Semelaigne Syndromes with Severe Hypothyroidism. J. Pediatr. Adolesc. Gynecol. 2015, 28, e161–163. [Google Scholar] [CrossRef] [PubMed]
- Patni, N.; Cervantes, L.F.; Diaz, A. Elevated Alpha-Fetoprotein Levels in Van Wyk-Grumbach Syndrome: A Case Report and Review of Literature. J. Pediatr. Endocrinol. Metab. JPEM 2012, 25, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Bhadada, S.K.; Bhansali, A. An Unusual Presentation of a Usual Disorder: Van Wyk-Grumbach Syndrome. Indian J. Endocrinol. Metab. 2011, 15, S141–143. [Google Scholar] [CrossRef] [PubMed]
- Reddy, P.; Tiwari, K.; Kulkarni, A.; Parikh, K.; Khubchandani, R. Van Wyk Grumbach Syndrome: A Rare Consequence of Hypothyroidism. Indian J. Pediatr. 2018, 85, 1028–1030. [Google Scholar] [CrossRef]
- Rivera-Hernández, A.; Madrigal-González, M.M.; Espinosa-Peniche, R.; Zurita-Cruz, J.; Balcázar-Hernández, L. Van Wyk-Grumbach Syndrome and Trisomy 21. Proc. Bayl. Univ. Med. Cent. 2022, 35, 569–571. [Google Scholar] [CrossRef]
- Sherwani, P.; Nandolia, K.K.; Joshi, K.; Lourembam, R. Imaging in Van Wyk Grumbach Syndrome: An Uncommon Presentation of Hypothyroidism. SA J. Radiol. 2023, 27, 2572. [Google Scholar] [CrossRef] [PubMed]
- Shivaprasad, K.S.; Dutta, D.; Jain, R.; Kumar, M.; Maisnam, I.; Biswas, D.; Ghosh, S.; Mukhopadhyay, S.; Chowdhury, S. Huge Bilateral Ovarian Cysts in Adulthood as the Presenting Feature of Van Wyk Grumbach Syndrome Due to Chronic Uncontrolled Juvenile Hypothyroidism. Indian J. Endocrinol. Metab. 2013, 17, S164–166. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.M.; Ammini, A.C.; Kriplani, A. Ovarian Cyst in Juvenile Hypothyroidism. Arch. Gynecol. Obstet. 2005, 271, 262–263. [Google Scholar] [CrossRef] [PubMed]
- Sneha, L.M.; Thanasegarapandian, K.; Paramasivam, V.; Scott, J.X. Short Stature and an Interesting Association. Indian J. Hum. Genet. 2013, 19, 101–103. [Google Scholar] [CrossRef]
- Sultan, A.; Velaga, M.R.; Fleet, M.; Cheetham, T. Cullen’s Sign and Massive Ovarian Enlargement Secondary to Primary Hypothyroidism in a Patient with a Normal FSH Receptor. Arch. Dis. Child. 2006, 91, 509–510. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, K.; Deguchi, M.; Takeshima, Y.; Maruo, T. A Case of Multiple Ovarian Cysts in a Prepubertal Girl with Severe Hypothyroidism Due to Autoimmune Thyroiditis. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2004, 14, 543–545. [Google Scholar] [CrossRef] [PubMed]
- Ozgen, T.; Güven, A.; Aydin, M. Precocious Puberty in a Girl with Down Syndrome Due to Primary Hypothyroidism. Turk. J. Pediatr. 2009, 51, 381–383. [Google Scholar]
- Tran, S.; Kim, E.E.; Chin, A.C. Severe Menorrhagia, Unilateral Ovarian Mass, Elevated Inhibin Levels, and Severe Hypothyroidism: An Unusual Presentation of Van Wyk and Grumbach Syndrome. J. Pediatr. Surg. 2013, 48, e51–54. [Google Scholar] [CrossRef]
- Waddankeri, S.; Waddankeri, M.; Waddankeri, S.; Arora, K. The Clinical Septet of Van Wyk-Grumbach Syndrome: A Case Series from a Tertiary Care Centre in Kalyana Karnataka, India. TouchREVIEWS Endocrinol. 2023, 19, 98–102. [Google Scholar] [CrossRef]
- Iqbal, M.Z.; Saleem, M.; Shahzad, Z.A. A Case of van Wyk-Grumbach Syndrome. APSP J. Case Rep. 2013, 4, 24. [Google Scholar]
- Zhang, S.; Yang, J.; Zheng, R.; Jiang, L.; Wei, Y.; Liu, G. VanWyk-Grumbach Syndrome in a Male Pediatric Patient: A Rare Case Report and Literature Review. Exp. Ther. Med. 2017, 13, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Geng, N.; Wang, Y.; Tian, W.; Xue, F. Van Wyk and Grumbach Syndrome: Two Case Reports and Review of the Published Work. J. Obstet. Gynaecol. Res. 2014, 40, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Yang, Y.; Zhao, Y.; Tang, H.; Zhang, X.; Shi, R.; Zhao, Y.; Han, R. Primary Juvenile Hypothyroidism Concurrent with Huge Bilateral Cystic Ovaries: Case Report and Literature Review. Arch. Pediatr. Organe Off. Soc. Francaise Pediatr. 2021, 28, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Vasseur, C.; Rodien, P.; Beau, I.; Desroches, A.; Gérard, C.; de Poncheville, L.; Chaplot, S.; Savagner, F.; Croué, A.; Mathieu, E.; et al. A Chorionic Gonadotropin-Sensitive Mutation in the Follicle-Stimulating Hormone Receptor as a Cause of Familial Gestational Spontaneous Ovarian Hyperstimulation Syndrome. N. Engl. J. Med. 2003, 349, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Smits, G.; Olatunbosun, O.; Delbaere, A.; Pierson, R.; Vassart, G.; Costagliola, S. Ovarian Hyperstimulation Syndrome Due to a Mutation in the Follicle-Stimulating Hormone Receptor. N. Engl. J. Med. 2003, 349, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, T.; Rehm, P.K. Recombinant Human Thyrotropin Use Resulting in Ovarian Hyperstimulation: An Unusual Side Effect. Eur. Thyroid J. 2014, 3, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Bull, M.J.; Trotter, T.; Santoro, S.L.; Christensen, C.; Grout, R.W.; Burke, L.W.; Berry, S.A.; Geleske, T.A.; Holm, I.; et al.; COUNCIL ON GENETICS Health Supervision for Children and Adolescents With Down Syndrome. Pediatrics 2022, 149, e2022057010. [Google Scholar] [CrossRef]
- Rodriguez, L.; Dinauer, C.; Francis, G. Treatment of Hypothyroidism in Infants, Children and Adolescents. Trends Endocrinol. Metab. TEM 2022, 33, 522–532. [Google Scholar] [CrossRef]
Figure 1.
(a) Tomography image from two pelvic tumors; (b) Ultrasound image from a pelvic tumor.
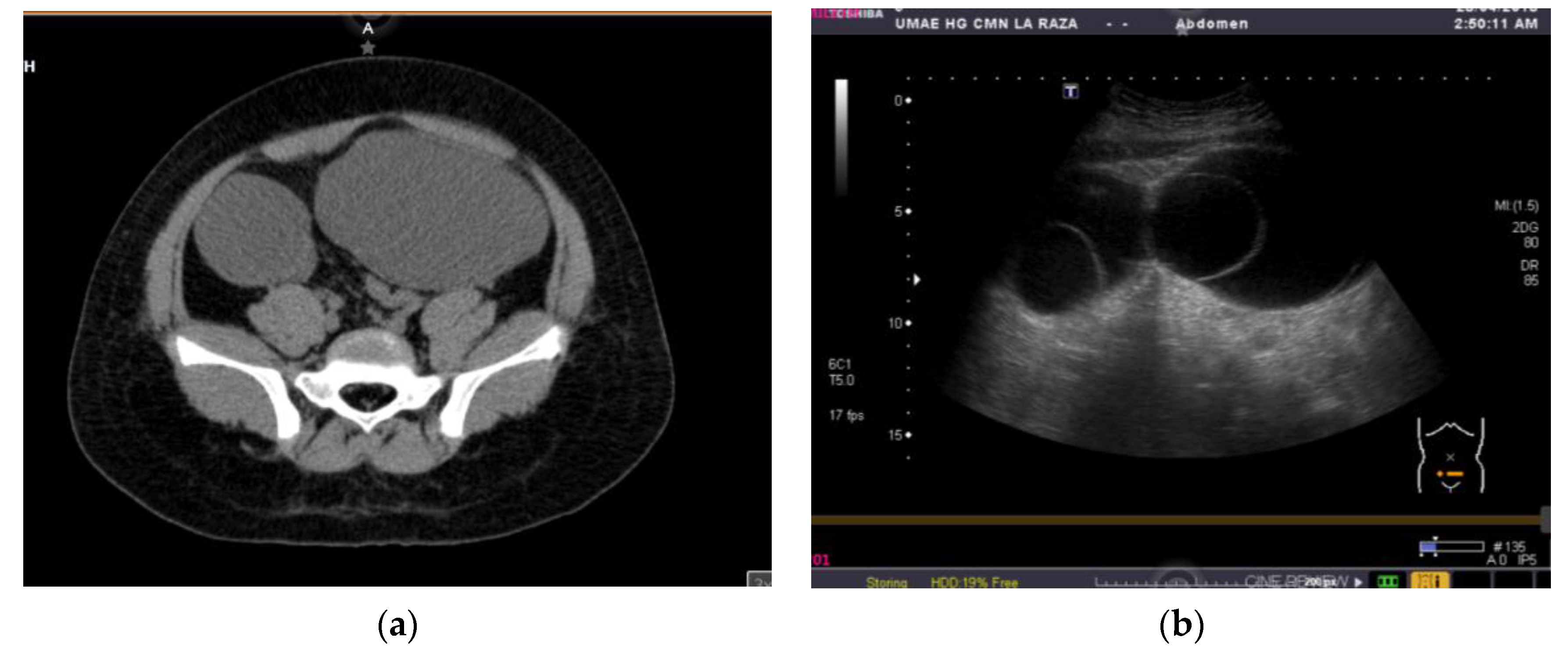

Table 1.
Initial laboratory findings in this case.
| Laboratory | Result | Normal range |
|---|---|---|
| Alpha-fetoprotein | 4.86 ng/mL | 0 to 7 ng/mL |
| Carcinoembryonic antigen | 3.84 ng/mL | 0 to 3.8 ng/mL |
| Chorionic gonadotropin | <0.10 | non detectable |
| CA-125 | 25.39 UI/mL | 0 to 35 UI/mL |
| TSH | 367.3 mUI/mL | 0.27 to 4.2 mUI/mL |
| Total T4 | 0.49 mg/dL | 5.1 a 14.1 mg/dL |
| Free T4 | 0.06 ng/dL | 0.93 to 1.7 ng/dL |
| Total T3 | <0.20ng/mL | 0.8 to 2 ng/mL |
| Free T3 | 1.59 pmol/L | 1.73 to 6.3 pmol/L |
| Anti thyroglobulin | 150.5 () | 5 to 100 |
| LH | <0.10 mUI/mL | <0.10 mUI/mL |
| Estradiol | 63.53 pg/mL | Non detectable |
| FSH | 5.19 mUI/mL | 0 to 5 mUI/mL |
| Total cholesterol | 305 mg/dL | 120 to 200 mg/dL |
| Triglycerides | 332 mg/dL | 35 to 135 mg/dL |
Table 2.
Main characteristics of reports of Van Wyk-Grumbach Syndrome.
| Variable | Result N (%) or *median (interquartile range). |
|---|---|
| Place of report | |
| Asia | 29 (53.7) |
| America | 18 (33.3) |
| Europe | 7 (13) |
| Female Sex | 51(94) |
| Age at diagnosis years. | 9.95 (7.37 to 14)* |
| Comorbidities | 9 (16.6) |
| Down syndrome | 6 (11.1) |
| Alport syndrome | 1(1.9) |
| Hemangioma | 1 (1.9) |
Table 3.
Hypothyroidism typical findings at presentation.
| Variable | n (%) from all studies or *median (interquartile range). | Percentage of studies that report the symptom |
| Mental retardation | 12 (22.2) | 13 (24.1) |
| Edema/myxedema | 18 (33.3) | 19 (35.2) |
| Dry skin | 22 (37) | 22 (37) |
| Puffy facies | 19 (33.3) | 19 (33.3) |
| Hypoactivity or asthenia | 23 (38.9) | 23 (38.9) |
| Constipation | 13 (24.1) | 14 (24.1) |
| Bradycardia | 8 (14.8) | 8 (14.8) |
| Anemia | 27 (46.3) | 25 (48.1) |
| Hb g/dL. | 9 (7.9 to 10)* | |
| Alopecia | 1 (1.9) | 1 (1.9) |
| Menstrual irregular rhythm | 6 (11.1) | 6 (11.1) |
| Myopathy or muscular weakness | 6 (11.1) | 6 (11.1) |
| Short stature | 34 (63) | 39 (72) |
| Height (CDC sz) | -3.47 (-2.45 to -4.76)* | |
| Obesity | 15 (27.8) | 17 (31.5) |
| Hypercholesterolemia | 7 (13) | 7 (13) |
| Total Cholesterol mg/dL. | 345 (299 to 444)* | |
| Delayed bone age | 31 (57.4) | 36 (64.7) |
| Bone age delay, years | -3 (-4 to -1.5)* | |
| Number of findings | ||
| 0 | 1 (1.9) | |
| 1 to 5 | 35 (64.6) | |
| 6 to 10 | 18 (33.5) | |
| Time from typical hypothyroidism findings to diagnosis, years | 2 (1 to 5) | |
| TSH mUI/mL | 490 (100 to 939)* | 35 (63.3) |
| TSH >100 | 42 (77.8) | |
| TSH <100 | 10 (18.5) |
Table 4.
Symptoms that led to medical consultation.
| Symptom | n(%) |
|---|---|
| Vaginal bleeding | 23 (42.3) |
| Abdominal pain | 15 (27.8) |
| Abdominal bloating | 3 (5.6) |
| Abnormal menstruation (irregularity or metrorrhagia) | 4 (7.4) |
| Other (ascites, headache, clitoromegaly, Cullen’s sign, ab-dominal mass, precocious puberty, short stature, muscular weakness) | 9 (16.6) |
Table 5.
Puberal or gonadal related findings of hypothyroidism at diagnosis.
| Symptom | n(%) |
| Puberal or sexual symptom | |
| Vaginal bleeding | 33 (61.1) |
| Macroorchidism | 3 (5.6) |
| Clitoromegaly | 2 (3.7) |
| Puberal delay | 1 (1.9) |
Table 6.
Severe findings of hypothyroidism at diagnosis.
| Symptom | n(%) |
| Anemia requiring transfusion | 2 (3.8) |
| Ascites | 4 (7.4) |
| Pericardial effusion | 5 (9.2) |
| Intracranial mass effect | 1 (1.9) |
| Cullen’s sign | 1 (1.9) |
| Ovarian torsion | 3 (5.5) |
| Pituitary hyperplasia | 18 (33.3) |
| Hyperprolactinemia | 29 (53.7) |
| Elevated AST | 1 (1.9) |
Table 7.
Gonadal ultrasound findings at diagnosis.
| Findings | n(%) |
| Multiple cysts | 23 (51.1) |
| Cysts | 13 (28.9) |
| Ovarian enlargement | 5 (11.1) |
| Ovarian tumor or complex images | 3 (6.7) |
| Other | 1 (2.2) |
Table 8.
Surgery indications.
| Type of surgery | n(%) |
| Cystectomy | 2 (28.5) |
| Ovary detorsion | 2 (28.5) |
| Ovary biopsy | 1 (14.2) |
| Bilateral oophorectomy | 1 (14.2) |
| Aborted oophorectomy | 1 (14.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



