
Submitted:
10 June 2024
Posted:
12 June 2024
You are already at the latest version
Abstract
The high prevalence of human papillomavirus (HPV) infection in oropharyngeal squamous cell carcinoma (OPSCC) is well-established, with p16 expression being a strong predictor. HPV-related tumors exhibit unique mechanisms targeting p16 and p53 proteins. However, re-search on HPV prevalence and the combined predictive value of p16 and p53 expression in head and neck cutaneous squamous cell carcinomas (HNCSCC), especially in Asian populations, is limited. This retrospective study surveyed 62 HNCSCC patients (2011–2020), excluding those with facial warts or other skin cancers. All patients underwent wide excision and biopsy. Immuno-histochemical staining for HPV, p16, and p53 yielded both positive and negative results. The relevance of each marker was investigated by categorizing the tumor locations into high-risk (Area H) and mid-risk (Area M) zones based on recurrence frequency. Of the 62 patients, 20 (32.26%) were male, with an average age of 82.27 years (26–103). Area H included 19 cases (30.65%), with the eyelid and lip being the most common sites (five cases, 8.06%). Area M in-cluded 43 cases (69.35%), with the cheek being the most common site (29 cases, 46.77%). p16 ex-pression was positive in 24 patients (38.71%), p53 expression in 42 patients (72.58%), and HPV in five patients (8.06%). No significant association was found between p16 expression and HPV presence (p > 0.99), with a positive predictive value of 8.33%. This indicates that p16, a surrogate marker of HPV in OPSCC, is not a reliable marker for HPV in HNCSCC. This study enhances our understanding of the relationship between HPV, p53, and p16 in HNCSCC in Asian populations and offers valuable insights for further research.
Keywords:
squamous cell carcinoma
; oropharyngeal
; non-oropharyngeal
; human papillomavirus
; p16
; p53
1. Introduction
Squamous cell carcinoma (SCC) is the second most common skin cancer, following basal cell carcinoma [1]. It typically arises with precancerous lesions, often in sun-exposed regions, notably the head and neck. Risk factors for the development of SCC include ultraviolet (UV) radiation, chemical carcinogens, genetic predisposition, immunosuppression, drugs, and viral infection [1]. Viral infections, particularly those caused by the human papillomavirus (HPV), are considered a potential carcinogen that indirectly impair DNA repair mechanisms or apoptotic responses to UV-induced damage [1]. The carcinogenic potential of HPV infection in SCC is relatively well-known, particularly in cases of epidermodysplasia verruciformis (EV). EV, an autosomal recessive hereditary dermatosis, presents a heightened risk for SCC development and exhibits high susceptibility to infection with beta-genus HPV-5 and HPV-8 [2]. In EV, SCC develops in chronically HPV-infected skin, particularly in sun-exposed areas [2]. Numerous studies have investigated the occurrence of HPV in oropharyngeal SCC (OPSCC) [3]. However, studies on the relationship between HPV and non-oropharyngeal cutaneous SCC (head and neck cutaneous squamous cell carcinomas [HNCSCC]) are limited. In addition, most studies have been conducted on Caucasians, and few studies have been conducted on Asians.
p53 is an important driver mutation in SCC with a tumor suppressor function against UV-induced damage [4]. However, to the best of our knowledge, no studies have been conducted on the p53 mutation rate in HNCSCC and its association with HPV, which is known to interfere with the repair of UV-induced damage. P16 is known as a surrogate marker for HPV with a high positive predictive value (PPV) in OPSCC and is associated with a favorable prognosis [5]. However, its association with HNCSCC has not yet been studied.
This study aimed to examine the relationship between HPV infection and HNCSCC in an Asian population. Additionally, we investigated the positivity rates of p53 and p16 in HNCSCC and their association with HPV.
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
A cohort of 62 patients diagnosed with HNCSCC who underwent excision and biopsy at a single institution between 2011 and 2020 was identified. All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Institutional Review Board of Soonchunhyang University Hospital (IRB exemption No. 2024-05-014). All patients were histopathologically diagnosed with SCC. Following registration, a computer-generated randomization process was conducted, resulting in the enrollment of 62 out of 269 patients. The process ensured balanced by incorporating clinical data including age, sex, and tumor location.
Patients diagnosed with verruca or other cutaneous malignancies of the head and neck region were excluded. Additionally, individuals of races other than Asian were excluded from the study to maintain homogeneity within the sample population. Patients with a history of treatment for head and neck cancer or those with incomplete medical records were also excluded to ensure data reliability.
2.2. Clinical Information
Clinical information, including sex, age, and patient medical history, was collected. Additionally, data on tumor size, depth, lymphovascular invasion, and perineural invasion were recorded. The tumor location was categorized as a high-risk zone (Area H) comprising the central facial regions (eyelids, eyebrows, periorbital, nose, lips, chin, mandible, preauricular, and postauricular areas) and a mid-risk zone (Area M) consisting of the cheeks, forehead, and scalp (Figure 1).
2.3. Construction of Tissue Microarray
Hematoxylin and eosin stained slides were prepared from formalin-fixed paraffin-embedded tissue blocks. The slides were reviewed under a light microscope to identify the most representative cancerous regions. The corresponding areas of each paraffin block were then cored twice using a 2 mm-diameter cylinder and transferred to a recipient paraffin block utilizing a tissue microarrayer (Unitma, Seoul, Korea).
2.4. Immunohistochemistry and Interpretation
Immunohistochemical (IHC) staining of individual 4-μm thick slide sections derived from tissue microarray (TMA) blocks was performed using the Ventana Benchmark XT automated staining system (Ventana Medical Systems, Tucson, AZ, USA), according to manufacturer’s protocol. The following primary antibodies were used: anti-p16 (dilution 1:2; clone E6H4; Roche, Tucson, AZ, USA), anti-HPV (dilution 1:100; clone K1H8; Dako, Glostrup, Denmark), and anti-p53 (dilution 1:900; clone DO-7; Dako, Glostrup, Denmark). HPV and p16 expression in tumor cells was classified as negative and positive (>1%) through cytoplasmic and nuclear staining (Figure 2A, B, Figure 4A, B). p53 expression in the tumor cells was evaluated as negative or positive by performing nuclear staining (Figure 3A, B).
2.5. Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows (version 26.0; IBM Corporation, Armonk, NY). Categorical variables are expressed as counts (percentages), while continuous variables are presented as mean ± standard deviation (SD). The chi-square test or Fisher's exact test for categorical variables and the independent sample t-test for continuous variables were used to compare the two groups. The Mann–Whitney U test was used to analyze continuous variables that were not normally distributed. Statistical significance was set at p>0.05.
3. Results
3.1. Patients Demographics and Tumor Characteristics
The patient demographics and tumor characteristics are shown in Table 1. Among the 62 HNCSCC patients, 20 (32.26%) were male. The average age of the patients was 82.27 years, and 93.55% were over 65 years of age. Nineteen (30.65%) and 43 (69.35%) patients had tumors in Area H and Area M, respectively. The average size and depth of tumors were 2.73 ± 4.60 cm2 and 4.06 ± 3.62 mm, respectively. The incidence of lymphovascular and perineural invasion was 4.84% (3/62). Diabetes mellitus and hypertension were present in 14.52% (9/62) and 43.55% (27/62) of patients, respectively (Table 1).
3.2. Location of Tumors
Tumor locations are presented in Table 2. Area H accounted for 30.65% (19/62) of the cases, of which the eyelids and lips were the most common (8.06%), followed by the ears (6.46%), nose (4.84%), and chin (3.23%). Area M comprised 69.35% (43/62), and the cheek (46.77%) was the most common, followed by the forehead (17.74%) and scalp (4.84%) (Table 2).
3.3. Immunohistochemical Study
The HPV, p16, and p53 statuses are presented in Table 3. p16 was positive in 24 (38.71%), p53 in 42 (72.58%), and HPV in five (8.06%) HNCSCC patients. HPV expression varied in intensity, mainly observed in well-developed tumor cells (Figure 2B). p53 staining often exhibits strong nuclear expression diffusely (Figure 3B). p16 positive staining showed strong nuclear and cytoplasmic expression in continuous tumor cells, which was defined as block positivity (Figure 4B). The positivity rates of HPV, p53, and p16 showed no significant differences according to sex or age (p=0.165, 0.125, 0.331, respectively).
There was no significant difference in the presence of HPV according to Area H/M; however, the Area M ratio in the HPV-positive group was 80%, which was higher than that in the HPV-negative group (68.42%) (p>0.99).
No statistically significant association was observed between p53 expression and HPV infection.(p>0.99). The Area H ratio in the p53-positive group was 35.56%, which was higher than that in the p53-negative group (17.65%), with no statistically significant difference (p=0.172).
There was no significant association between p16 expression and the presence of HPV, and the positive predictive rate of p16 for HPV was 8.33% (p>0.99). According to the tumor location, the Area H ratio in the p16-positive group was 25%, which was lower than that in the p16-negative group (34.21%; p=0.444; Table 3).
4. Discussion
SCC is the second most common type of non-melanoma skin cancer, accounting for approximately 40.2% of malignancies in the head and neck region [6]. Several risk factors for the development of HNSCC have been identified, including tobacco smoking, alcohol consumption, dietary factors, and HPV infection [7]. The role of HPV in oral and oropharyngeal carcinogenesis was first described by Syrjanen et al. in 1983 [8]. Since then, numerous studies have investigated the role of HPV in HNSCC, particularly in OPSCC. The HPV-positivity rate in OPSCC varies widely, typically ranging from 40% to 80%, depending on the sensitivity and specificity of the detection method used [3].
Notably, HPV-positive OPSCC exhibits distinct clinical and demographic characteristics compared to those of HPV-negative tumors [9]. For instance, HPV-positive OPSCC is more frequently observed in certain regions, such as the United States, than in Asia or Europe [10]. This geographical variation in HPV prevalence may be attributed to differences in sexual behavior, cultural practices, and HPV vaccination rates. Moreover, HPV-positive OPSCC tends to occur more frequently in younger patients and individuals with a history of multiple sexual partners and higher oral sex exposure [11]. These behavioral risk factors contribute to the transmission of HPV, particularly high-risk HPV genotypes such as HPV-16 and HPV-18, which are associated with oncogenic transformation and the development of OPSCC. Importantly, HPV-positive OPSCC is associated with a more favorable prognosis compared to that of HPV-negative tumors [12,13,14]. This improved prognosis is thought to be related to the distinct molecular and biological characteristics of HPV-positive tumors, including overexpression of the p16 protein and inactivation of the p53 tumor suppressor gene. These molecular alterations contribute to enhanced sensitivity to radiotherapy and chemotherapy, resulting in better treatment responses and overall survival rates in HPV-positive OPSCC patients [15,16,17].
Clinically, HPV-positive OPSCC typically presents as a single localized tumor in the oropharynx, most commonly in the tonsillar region or base of the tongue [18]. These tumors often have a smaller primary tumor size and a lower rate of lymph node involvement than that of HPV-negative tumors [19,20]. Unlike HPV-negative tumors, HPV-positive OPSCC are less frequently associated with tobacco and alcohol use, and patients may present with fewer comorbidities and a better performance status at the time of diagnosis [21].
Unlike OPSCC, HNCSCC has been relatively understudied. However, the HPV infection rate is higher in SCC, including those occurring in the head and neck regions, than in normal skin [22]. UV exposure, a known trigger for SCC, can induce immunosuppression, potentially increasing susceptibility to HPV infection. Conversely, evidence suggests that HPV infection may exacerbate UV-induced damage, potentially contributing to the development of SCC. Nevertheless, its role in the maintenance of SCC remains uncertain [23]. Previous studies have reported HPV positivity rates in HNCSCC ranging between 5% and 20%; however, it is unclear whether HPV is directly involved in the pathogenesis of HNCSCC [13,24]. Furthermore, most studies have been conducted in Caucasian populations, with few examining the role of HPV in HNCSCC among Asians [3].
In this study, the positive detection rate of HPV through IHC for HNCSCC was 8.06% (5/62). This was lower than that reported in a previous study using the polymerase chain reaction (PCR) method for North Americans, where the HPV positivity rate was 21.8% [25]. The difference in test methods is considered one of the reasons for this result. PCR testing is the most sensitive method for detecting HPV [26], and it may show a higher positivity rate than the IHC method used in this study. In addition, as mentioned above, HPV-positive OPSCC occurs more frequently in the United States than in Asia [10], and because of similar racial and cultural differences, HPV-positive HNCSCC is also thought to be lower than that reported in previous studies targeting North Americans.
p53 is the most commonly mutated gene in SCC, occurring in up to 90% of cases [27]. When a mutation occurs, tumor cells resist apoptosis and cell cycle arrest, leading to clonal expansion. Mutations in p53 caused by UV damage are involved in the development of SCC [4]. In the past, studies have been conducted on the effect of p53 overexpression on treatment response or prognosis in HNCSCC, but no consensus has been reached [28]. In addition, a study was conducted on the association between the presence of HPV and p53 in SCC. HPV E6 and E7 proteins suppress p53-mediated gene transcription. This may interfere with the UV-activated cell cycle checkpoint, exacerbating UV-induced DNA damage and ultimately the oncogenic potential of HPV [29,30,31].
In this study, p53 was overexpressed in 72.58% (45/62) HNCSCC patients. This is similar to the 79% reported in previous studies on SCC Korean patients [32]. The incidence of UV-induced SCC is inversely proportional to latitude, and the closer it is to the equator, the higher the incidence [33]. Moreover, the incidence is higher in the UV-sensitive fair skin type than in the dark skin type. This study was conducted in South Korea, and the frequency of p53 mutations caused by UV damage was anticipated to be lower than that reported in previous studies on Caucasians [32], but there was no significant difference. In addition, no significant association was observed between HPV and p53 expression in HNCSCC (p>0.99).
P16 has emerged as a cost-effective surrogate marker for HPV in OPSCC owing to its high sensitivity and specificity in detecting HPV-related tumors. IHC staining for p16 can reliably identify tumors with transcriptionally active HPV, making it a valuable tool for diagnostic and prognostic purposes. Additionally, p16 expression in OPSCC has been associated with a favorable prognosis, as HPV-positive tumors generally exhibit a better response to treatment and improved survival outcomes than that of HPV-negative tumors. However, the role of p16 in HNCSCC remains unclear. A study including HNCSCC patients reported that p16 expression was not related to high-risk HPV or prognosis [34]. The positivity rate of p16 in this study was 38.71% (24/62), which is similar to 31.9% in a previous study on HNCSCC. The PPV of p16 for HPV was 8.33%, which was very low compared with 92.9% for OPSCC in a previous study [34], and there was no significant relationship between HPV and p16. (p>0.99) This suggests that the relationship between p16 expression and HPV status may differ between OPSCC and HNCSCC, highlighting the need for further research to elucidate the role of p16 in HNCSCC pathogenesis and its potential utility as a prognostic biomarker.
One possible explanation for the low positivity rate of p16 in HNCSCC is the influence of UV radiation exposure, a known risk factor for cutaneous SCC. UV exposure induces DNA damage and promotes genomic instability, leading to the accumulation of mutations in key regulatory genes such as p53, which may disrupt normal cell cycle regulation and override the compensatory mechanism of p16 overexpression in HPV-related OPSCC [23]. Furthermore, other environmental and genetic factors specific to cutaneous SCC may modulate p16 expression independently of HPV status, further complicating its utility as a prognostic biomarker for HNCSCC. Overall, the contrasting positivity rates of p16 in OPSCC and HNCSCC highlight the complex interplay among HPV infection, UV radiation exposure, and other etiological factors in the pathogenesis of head and neck cancer. Further research is required to elucidate the mechanisms underlying p16 expression in HNCSCC and its potential prognostic significance in these tumors.
The location of HNCSCC was classified as Area H and the Area M to indirectly confirm the relationship between p16 expression and HNCSCC prognosis. According to the National Comprehensive Cancer Network guidelines, SCC located in Area H has a high probability of recurrence and metastasis and requires Mohs microsurgery [35]. In this study, the relationship between p16 and tumor location was not statistically significant (p=0.444), indication no correlation between p16 and a favorable prognosis in HNCSCC.
This study has several limitations that should be acknowledged. First, it was conducted at a single institution and focused on a specific racial demographic, which may limit the generalizability of the findings to other populations. Additionally, the sample size was relatively small, comprising only 62 cases with a limited number of HPV-positive samples. Furthermore, HPV, p16, and p53 statuses were determined using IHC staining methods rather than more sensitive techniques such as PCR. While IHC staining is commonly used for clinical diagnosis, its sensitivity and specificity for detecting HPV and other molecular markers may vary, potentially leading to the misclassification of cases [36]. Moreover, the lack of direct information on survival outcomes and prognosis limits the assessment of the long-term implications of HPV, p16, and p53 expression patterns on patient outcomes.
5. Conclusions
This study found that the positive rate of HPV in HNCSCC was lower than that reported in studies conducted in North America. Furthermore, the positive rate of p53 did not demonstrate a significant difference compared to findings in Caucasian populations. Notably, p16, which is often considered a surrogate marker for HPV in OPSCC, was not significantly associated with HPV in HNCSCC. The PPV of p16 for HPV was 8.33%, indicating that p16 may not be a suitable surrogate marker for HPV in HNCSCC. Additionally, p16 expression was not associated with a favorable prognosis in HNCSCC.
This study contributes to our understanding of the relationship between HPV, p53, and p16 in HNCSCC, an area that has received less attention than OPSCC in previous studies. Moreover, the study's focus on Asian populations provides valuable insights, as most previous studies have been conducted on Caucasians. Overall, this study may aid in further elucidating the complex interplay between HPV infection and the molecular markers of HNCSCC among Asian populations, thus providing future research directions and clinical management strategies.
Author Contributions
Ha Jong Nam and Ji-Hye Lee contributed to manuscript writing; Hyeong Rae Ryu contributed to conceptualization and methodology; Da Woon Lee and Je Yeon Byeon contributed to project administration; Soomin Lim contributed to data collection; Jun Hyuk Kim and Hwan Jun Choi contributed to manuscript review, editing, visualization, analysis and supervision. All authors have read and approved the final manuscript.
Funding
This research was funded by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (2020R1A2C1100891) and sponsored by the Soonchunhyang University Research Fund.
Institutional Review Board Statement
The study was approved for exemption by the Institutional Review Board of Soonchunhyang University Hospital (IRB exemption No. 2024-05-014).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available from the authors upon reasonable request.
Acknowledgments
This research was funded by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (2020R1A2C1100891) and sponsored by the Soonchunhyang University Research Fund.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Aldabagh, B.; Angeles, J.G.C.; Cardones, A.R.; Arron, S.T. Cutaneous squamous cell carcinoma and human papillomavirus: is there an association? Dermatol Surg 2013, 39, 1–23. [Google Scholar] [CrossRef]
- Harwood, C.A.; McGregor, J.M.; Proby, C.M.; Breuer, J. Human papillomavirus and the development of non-melanoma skin cancer. J Clin Pathol 1999, 52, 249–253. [Google Scholar] [CrossRef]
- Wookey, V.B.; Appiah, A.K.; Kallam, A.; Ernani, V.; Smith, L.M.; Ganti, A.K. HPV status and survival in non-oropharyngeal squamous cell carcinoma of the head and neck. Anticancer Res 2019, 39, 1907–1914. [Google Scholar] [CrossRef]
- Que, S.K.T.; Zwald, F.O.; Schmults, C.D. Cutaneous squamous cell carcinoma: incidence, risk factors, diagnosis, and staging. J Am Acad Dermatol 2018, 78, 237–247. [Google Scholar] [CrossRef]
- Jiromaru, R.; Yamamoto, H.; Yasumatsu, R.; Hongo, T.; Nozaki, Y.; Nakano, T.; Hashimoto, K.; Nakagawa, T.; Oda, Y. p16 overexpression and Rb loss correlate with high-risk HPV infection in oropharyngeal squamous cell carcinoma. Histopathology 2021, 79, 358–369. [Google Scholar] [CrossRef]
- Ciążyńska, M.; Kamińska-Winciorek, G.; Lange, D.; Lewandowski, B.; Reich, A.; Sławińska, M.; Pabianek, M.; Szczepaniak, K.; Hankiewicz, A.; Ułańska, M.; et al. The incidence and clinical analysis of non-melanoma skin cancer. Sci Rep 2021, 11, 4337. [Google Scholar] [CrossRef]
- Zur Hausen, H. Papillomaviruses in the causation of human cancers – a brief historical account. Virology 2009, 384, 260–265. [Google Scholar] [CrossRef]
- Syrjänen, K.; Syrjänen, S.; Lamberg, M.; Pyrhönen, S.; Nuutinen, J. Morphological and immunohistochemical evidence suggesting human papillomavirus (HPV) involvement in oral squamous cell carcinogenesis. Int J Oral Surg 1983, 12, 418–424. [Google Scholar] [CrossRef]
- Gordis, T.M.; Cagle, J.L.; Nguyen, S.A.; Newman, J.G. Human papillomavirus-associated oropharyngeal squamous cell carcinoma: A systematic review and meta-analysis of clinical trial demographics. Cancers (Basel) 2022, 14, 4061. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomarkers Prev 2005, 14, 467–475. [Google Scholar] [CrossRef]
- Lewis Jr., J. S.; Thorstad, W.L.; Chernock, R.D.; Haughey, B.H.; Yip, J.H.; Zhang, Q.; El-Mofty, S.K. p16 positive oropharyngeal squamous cell carcinoma:an entity with a favorable prognosis regardless of tumor HPV status. Am J Surg Pathol 2010, 34, 1088–1096. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W.; et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol 2011, 29, 4294–4301. [Google Scholar] [CrossRef]
- D’Souza, G.; Kreimer, A.R.; Viscidi, R.; Pawlita, M.; Fakhry, C.; Koch, W.M.; Westra, W.H.; Gillison, M.L. Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med 2007, 356, 1944–1956. [Google Scholar] [CrossRef]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst 2008, 100, 261–269. [Google Scholar] [CrossRef]
- Westra, W.H. The changing face of head and neck cancer in the 21st century: the impact of HPV on the epidemiology and pathology of oral cancer. Head Neck Pathol 2009, 3, 78–81. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med 2010, 363, 24–35. [Google Scholar] [CrossRef]
- Lassen, P.; Eriksen, J.G.; Hamilton-Dutoit, S.; Tramm, T.; Alsner, J.; Overgaard, J.; Danish Head and Neck Cancer Group (DAHANCA). HPV-associated p16-expression and response to hypoxic modification of radiotherapy in head and neck cancer. Radiother Oncol 2010, 94, 30–35. [Google Scholar] [CrossRef]
- D’Souza, G.; Dempsey, A. The role of HPV in head and neck cancer and review of the HPV vaccine. Prev Med 2011, 53, Suppl 1(Suppl 1):S5-S11, S5–S11. [CrossRef]
- O’Rorke, M.A.; Ellison, M.V.; Murray, L.J.; Moran, M.; James, J.; Anderson, L.A. Human papillomavirus related head and neck cancer survival: a systematic review and meta-analysis. Oral Oncol 2012, 48, 1191–1201. [Google Scholar] [CrossRef]
- Dayyani, F.; Etzel, C.J.; Liu, M.; Ho, C.H.; Lippman, S.M.; Tsao, A.S. Meta-analysis of the impact of human papillomavirus (HPV) on cancer risk and overall survival in head and neck squamous cell carcinomas (HNSCC). Head Neck Oncol 2010, 2, 15. [Google Scholar] [CrossRef]
- Gillison, M.L.; Broutian, T.; Pickard, R.K.L.; Tong, Z.Y.; Xiao, W.; Kahle, L.; Graubard, B.I.; Chaturvedi, A.K. Prevalence of oral HPV infection in the United States, 2009–2010. JAMA 2012, 307, 693–703. [Google Scholar] [CrossRef]
- Gillison, M.L.; Chaturvedi, A.K.; Anderson, W.F.; Fakhry, C. Epidemiology of human papillomavirus-positive head and neck squamous cell carcinoma. J Clin Oncol 2015, 33, 3235–3242. [Google Scholar] [CrossRef]
- Hasche, D.; Stephan, S.; Braspenning-Wesch, I.; Mikulec, J.; Niebler, M.; Gröne, H.J.; Flechtenmacher, C.; Akgül, B.; Rösl, F.; Vinzón, S.E. The interplay of UV and cutaneous papillomavirus infection in skin cancer development. PLOS Pathog 2017, 13, e1006723. [Google Scholar] [CrossRef]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst 2000, 92, 709–720. [Google Scholar] [CrossRef]
- Mehanna, H.; Beech, T.; Nicholson, T.; El-Hariry, I.; McConkey, C.; Paleri, V.; Roberts, S. Prevalence of human papillomavirus in oropharyngeal and nonoropharyngeal head and neck cancer—systematic review and meta-analysis of trends by time and region. Head Neck 2013, 35, 747–755. [Google Scholar] [CrossRef]
- Awan, M.S.; Irfan, B.; Zahid, I.; Mirza, Y.; Ali, S.A. Comparison of polymerase chain reaction and immunohistochemistry assays for analysing human papillomavirus infection in oral squamous cell carcinoma. J Clin Diagn Res 2017, 11, XC10–XC13. [Google Scholar] [CrossRef]
- Soussi, T.; Wiman, K.G. Shaping genetic alterations in human cancer: the p53 mutation paradigm. Cancer Cell 2007, 12, 303–312. [Google Scholar] [CrossRef]
- Tandon, S.; Tudur-Smith, C.; Riley, R.D.; Boyd, M.T.; Jones, T.M. A systematic review of p53 as a prognostic factor of survival in squamous cell carcinoma of the four main anatomical subsites of the head and neck. Cancer Epidemiol Biomarkers Prev 2010, 19, 574–587. [Google Scholar] [CrossRef]
- Dong, W.; Arpin, C.; Accardi, R.; Gissmann, L.; Sylla, B.S.; Marvel, J.; Tommasino, M. Loss of p53 or p73 in human papillomavirus type 38 E6 and E7 transgenic mice partially restores the UV-activated cell cycle checkpoints. Oncogene 2008, 27, 2923–2928. [Google Scholar] [CrossRef]
- Münger, K.; Baldwin, A.; Edwards, K.M.; Hayakawa, H.; Nguyen, C.L.; Owens, M.; Grace, M.; Huh, K. Mechanisms of human papillomavirus-induced oncogenesis. J Virol 2004, 78, 11451–11460. [Google Scholar] [CrossRef]
- Thomas, M.; Pim, D.; Banks, L. The role of the E6-p53 interaction in the molecular pathogenesis of HPV. Oncogene 1999, 18, 7690–7700. [Google Scholar] [CrossRef]
- Lee, S.Y.; Lee, M.; Yu, D.S.; Lee, Y.B. Identification of genetic mutations of cutaneous squamous cell carcinoma using whole exome sequencing in non-Caucasian population. J Dermatol Sci 2022, 106, 70–77. [Google Scholar] [CrossRef]
- Lomas, A.; Leonardi-Bee, J.; Bath-Hextall, F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol 2012, 166, 1069–1080. [Google Scholar] [CrossRef]
- Satgunaseelan, L.; Chia, N.; Suh, H.; Virk, S.; Ashford, B.; Lum, T.; Ranson, M.; Clark, J.; Gupta, R. p16 expression in cutaneous squamous cell carcinoma of the head and neck is not associated with integration of high risk HPV DNA or prognosis. Pathology 2017, 49, 494–498. [Google Scholar] [CrossRef]
- Schmults, C.D.; Blitzblau, R.; Aasi, S.Z.; Alam, M.; Andersen, J.S.; Baumann, B.C.; Bordeaux, J.; Chen, P.L.; Chin, R.; Contreras, C.M.; et al. [NCCN guidelines]® Insights: Squamous Cell Skin Cancer. J Natl Compr Canc Netw, version 1.2022, 2021; Vol. 19; pp. 1382–1394.
- Wentzensen, N.; Schwartz, L.; Zuna, R.E.; Smith, K.; Mathews, C.; Gold, M.A.; Allen, R.A.; Zhang, R.; Dunn, S.T.; Walker, J.L.; et al. Performance of p16/Ki-67 immunostaining to detect cervical cancer precursors in a colposcopy referral population. Clin Cancer Res 2012, 18, 4154–4162. [Google Scholar] [CrossRef]
Figure 1.
Classification of tumor location into high-risk zone (Area H) and mid-risk zone (Area M). Area H (Yellow area) encompasses central facial regions including eyelids, eyebrows, periorbital area, nose, lips, chin, mandible, preauricular, and postauricular areas. Area M (blue area) includes the cheeks, forehead, and scalp.
Figure 1.
Classification of tumor location into high-risk zone (Area H) and mid-risk zone (Area M). Area H (Yellow area) encompasses central facial regions including eyelids, eyebrows, periorbital area, nose, lips, chin, mandible, preauricular, and postauricular areas. Area M (blue area) includes the cheeks, forehead, and scalp.
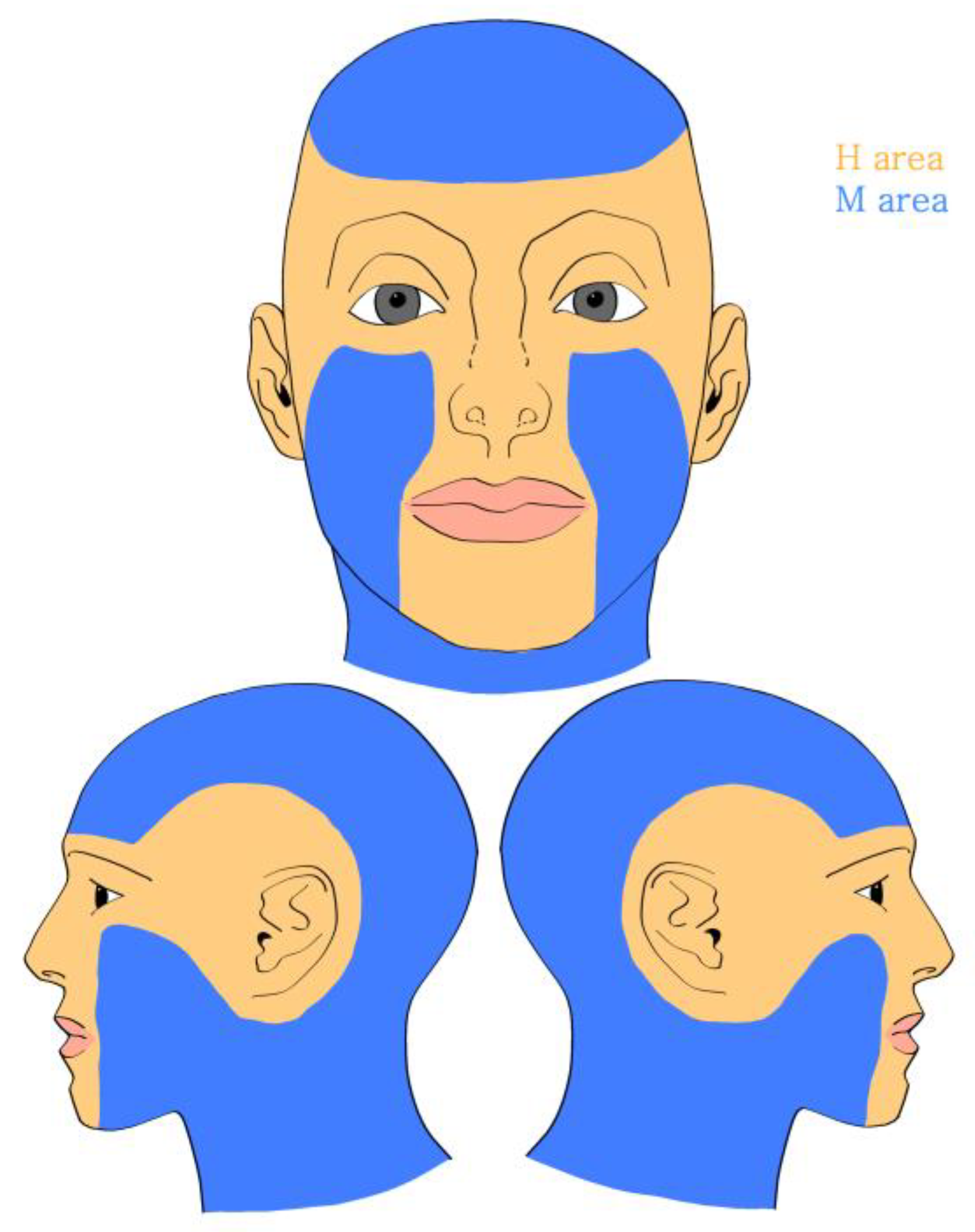
Figure 2.
Representative human papillomavirus (HPV) staining (A) negative (×200) (B) positive (×400).
Figure 2.
Representative human papillomavirus (HPV) staining (A) negative (×200) (B) positive (×400).
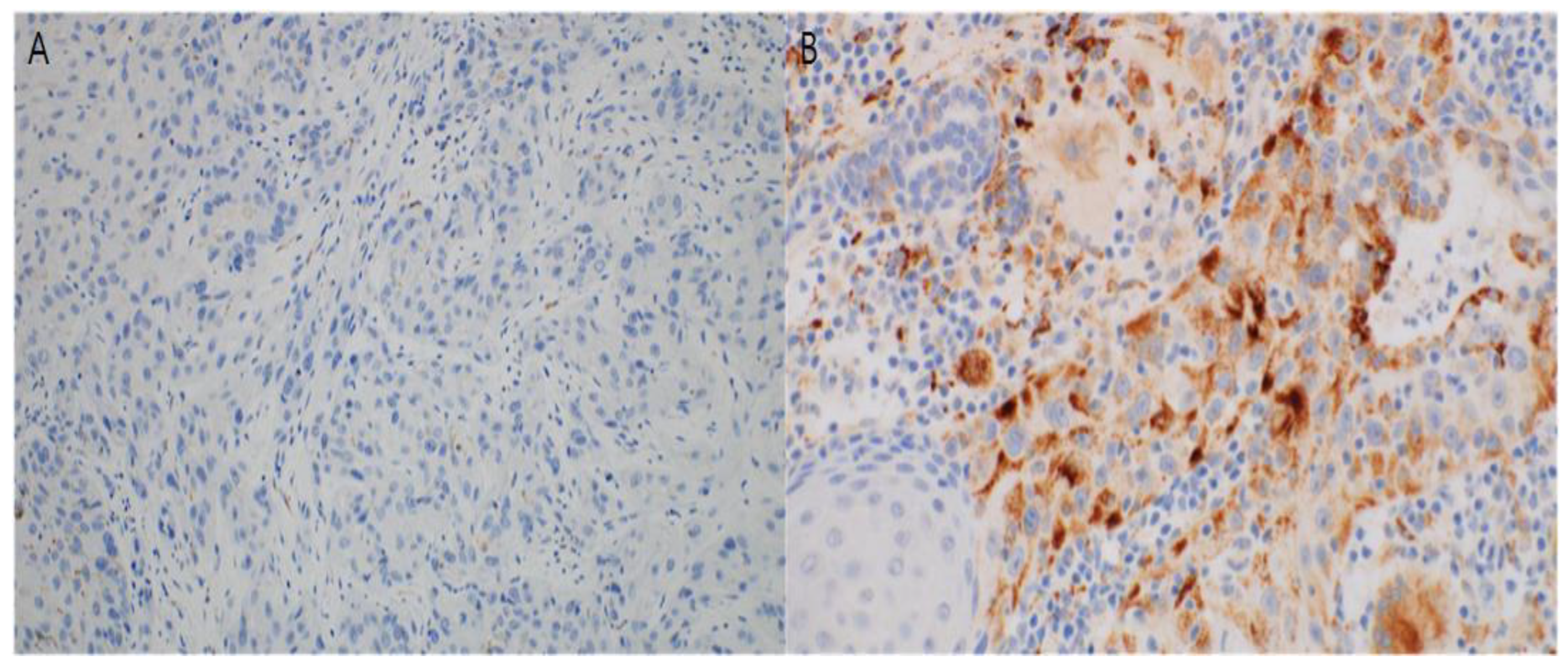
Figure 3.
Representative p53 staining (A) negative (×200) (B) positive (×200).
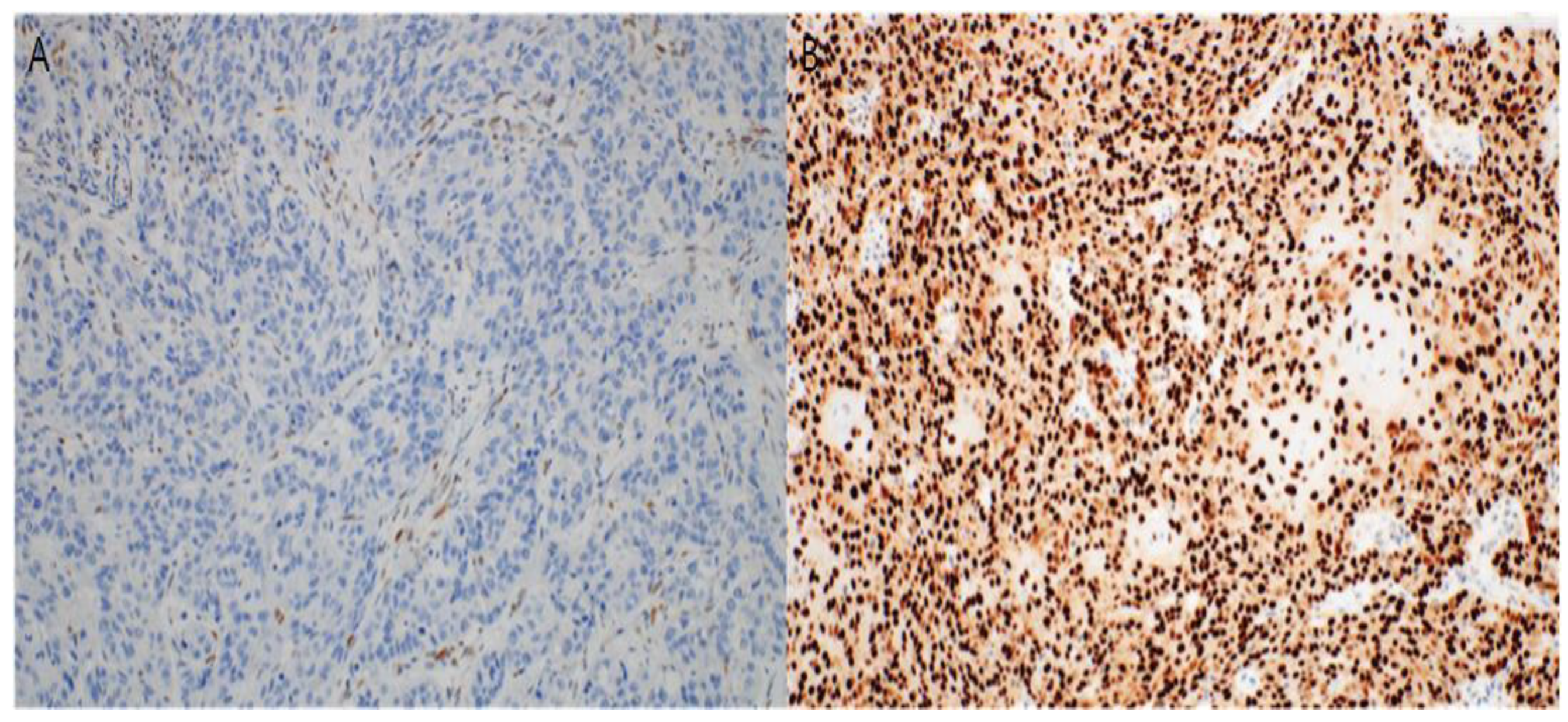
Figure 4.
Representative p16 staining (A) negative (×200) (B) positive (×200).
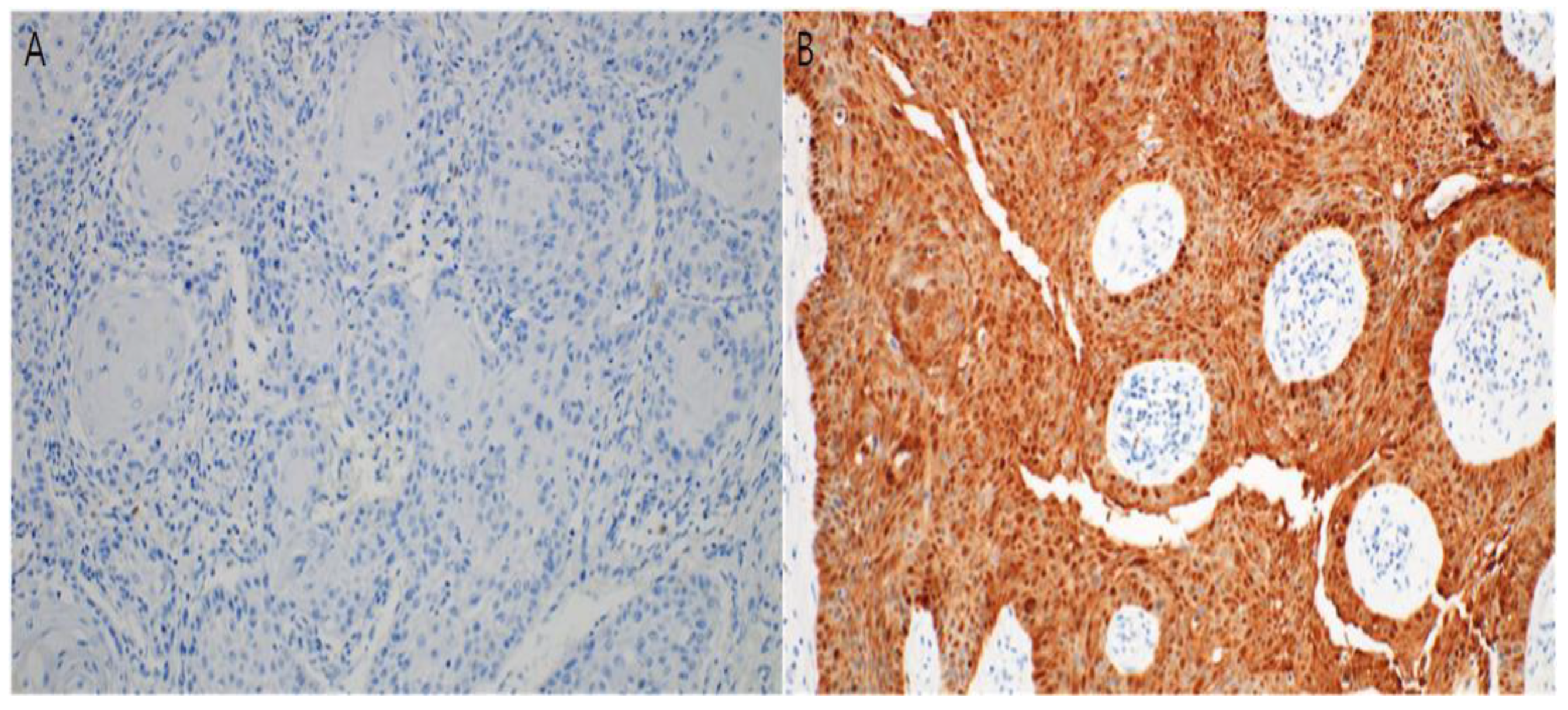

Table 1.
Patient demographics and tumor characteristics.
| N (%) | N=62 (%) |
|---|---|
| Sex | |
| Male | 20 (32.26) |
| Female | 42 (67.74) |
| Age group (years) | |
| ≤50 | 2 (3.22) |
| 51-65 | 2 (3.22) |
| >65 | 58 (93.55) |
| Location | |
| Area H | 19 (30.65) |
| Area M | 43 (69.35) |
| Size of tumor (cm2) |
2.73 ± 4.60 |
| Invasion depth (mm) |
4.06 ± 3.62 |
| Lymphovascular invasion |
|
| (+) | 3 |
| (-) | 59 |
| Perineural invasion |
|
| (+) | 3 |
| (-) | 59 |
| DM | |
| (+) | 9 |
| (-) | 53 |
| HTN | |
| (+) | 27 |
| (-) | 35 |
Table 2.
Location of tumors.
| N (%) | N=62 (%) |
|---|---|
| Area H | 19 (30.65) |
| Eyelid | 5 (8.06) |
| Nose | 3 (4.84) |
| Lip | 5 (8.06) |
| Chin | 2 (3.23) |
| Ear | 4 (6.46) |
| Area M | 43 (69.35) |
| Forehead | 11 (17.74) |
| Scalp | 3 (4.84) |
| Cheek | 29 (46.77) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



