
Submitted:
15 June 2024
Posted:
17 June 2024
You are already at the latest version
Abstract
Background: The accelerated ageing of the world's population will lead to an increase in the number of older persons in the workforce. Computerized Cognitive Training (CCT) is effective in improving cognitive outcomes, but its benefits for older workers remain controversial. We investigate the real-world efficacy of CCT in the workplace, focusing on employees aged 50+ years from a public sector agency. Methods: Case managers (N = 82) were randomized to either Intervention group (24 40-minute CCT sessions two times per week) or waiting list passive Control group. Cognitive ability, wellbeing, job satisfaction, and productivity outcome measures were collected assessed before and after CCT or comparable Control wait time. Results: Participants undergoing CCT improved on a task of executive functioning (p = 0.04). There was a trend toward change in work productivity after CCT (p = 0.09) with the Control group showing a significant decrease (p = 0.02), while the Intervention group remained stable. Conclusions: CCT during office hours has a positive effect on cognition and well-being without affecting the productivity among white-collar office workers. CCT could be considered as an intervention to support the older workforce in managing the cognitive and behavioral challenges of changing workplace demands.
Keywords:
older employees
; 50+
; computerized cognitive training (CCT)
; productivity
; well-being
1. Introduction
The ongoing demographic shift, characterized by a declining proportion of young individuals and an increasing proportion of older people due to falling fertility rates and enhanced life expectancy [1,2], is fundamentally altering our global landscape. By 2030, the United Nations predicts that one in six individuals worldwide will be over 65 years old. Concurrently, this demographic transition will see a surge in the older workforce: The anticipated rise in the percentage of older workers (aged 55–64) relative to the total working population (aged 15–64) from 2014 to 2035 is projected to increase from an average of 12.1% in 2014 to an average of 24.8% in 2035 [3]. These shifts at the population level are already exerting significant pressure on workforce well-being and productivity.
1.1. Older Workforce
For quite some time, it has been established that cognitive abilities are the most significant predictor of work performance [4]. From a work standpoint, it is anticipated that older employees may encounter greater challenges due to issues with focus, resulting in difficulty inhibiting irrelevant information; reduced memory capacity, slowing learning new skills; and slower processing reducing productivity [4]. A meta-analysis conducted by Kubeck and colleagues showed that, compared to younger counterparts, older workers also struggle with learning new procedures, often requiring more time for mastery [5].
Not all work processes entail high demands. Tasks posing difficulties for the older workforce typically involve prolonged cognitive effort (e.g., scanning through pages of numbers or symbols) or those with time constraints (e.g., swiftly completing a project) [6,7,8,9,10,11]. Conversely, long-term repetitive and mentally undemanding work negatively impacts older workers' fluid cognitive functions [12]. Irrespective of job demands, whether high or low, it would be advantageous for the older workforce to receive support aimed at preserving and maintaining their cognitive capacity to sustain productivity until retirement.
1.2. Cognitive Aging
It is widely acknowledged that cognitive performance typically diminishes with advancing age [13], particularly in fluid abilities such as attention, processing speed, and reasoning [12]. These functions are crucial for swift and efficient action control and goal-directed behaviour, especially under the complex conditions often encountered in the workplace. They tend to decline first from middle adulthood, with variations in pace among individuals. Such functions encompass short-term memory, working memory, action planning and preparation, orientation and control of attention, searching for relevant information in the environment, inhibition of irrelevant information and reactions, multitasking, task-switching, and self-monitoring including error detection and correction. The changes in cognitive functions that accompany ageing become particularly pertinent in the ever-evolving modern work environment, marked by the introduction of new technologies such as increased electronic communication or new electronic devices to learn and master, which only add to the complexity in the workplace [14].
1.3. Cognitive Training (CT)
Over the past two decades, CT has emerged as a particularly popular intervention approach. CT and CCT, often referred to as brain training, aim to maintain or enhance cognitive abilities and processes through structured tasks designed to engage specific cognitive functions [15]. These approaches have been applied across various domains and populations [15]. Early on, researchers began exploring the use of CT and CCT in healthy ageing individuals as a means to mitigate age-related cognitive declines, with numerous studies reporting positive effects [16]. They have found that regular CT among healthy older adults can help maintain or even improve certain cognitive functions, leading to greater functional abilities and reduced pathological processes in ageing brains [17,18,19]. Furthermore, the benefits of CT/CCT may have longer-lasting effects [20] and/or potentially impact other domains such as mobility [21]. However, there is a notable gap in research regarding the use of CT/CCT with middle-aged adults. Gates et al. (2019) reported in their review of 317 publications on cognitive training with midlife adults that they found only one CCT article, which was of low quality. The authors were unable to determine whether computerized cognitive training is effective in maintaining global cognitive function among healthy adults in midlife and recommended future research on the effectiveness of CCT with midlife adults [22].
With an increased number of reports on the efficacy of CT/CCT, there has been a rise in systematic reviews, both with [23] and without meta-analyses [24]. However, recent systematic reviews present conflicting results [25,26]. Some reviews demonstrate clear benefits to trained abilities, such as executive function [27] and processing speed [28], particularly in older adults. Conversely, other reviews provide mixed evidence regarding the benefits of CT [29,30,31].
Despite the mixed evidence reported in reviews of CT efficacy among unimpaired older adults, researchers in this field still regard affordable and easily administered interventions like CT as promising avenues to mitigate age-related cognitive decline and maintain cognitive health well into late adulthood [32].
1.4. Cognitive Training with Older Workers
An extensive search has identified only four publications specifically related to CT in the workforce [33,34,35,36], each differing in various features of CT and the sampled workers. Among these, only Gajewski et al. [34] applied CT specifically with workers aged between 40 and 57 years; the others included workers of all ages and students (In terms of the CT methods employed, Gajewski et al. (utilized paper-pencil training tasks, whereas the others utilized CCT: Borness et al. [33] delivered online training sessions lasting 20 minutes, three times a week, targeting various cognitive domains such as memory, attention, language, executive function, and visuospatial abilities. Lampit et al. [35] utilized tasks focusing on attention, memory, and visuospatial skills, conducting one-hour sessions three to four times a week over a duration of 6 months. Miller et al. [36] delivered CCT online through the BrainHQ.com program, with participants categorized into long-training and short-training groups, with average durations of 30 hours and 7 hours, respectively.
The outcomes of CCT effectiveness also exhibit considerable variability[33] and did not find a positive impact of CCT on cognition or well-being among white-collar office workers. Similarly, Lampit et al. [35] reported that CCT participants did not show improvement in sustained attention tasks, although they did demonstrate significantly enhanced productivity in bookkeeping tasks. Conversely, Gajewski and colleagues [34] reported improvements in the accuracy of complex memory-based task switching immediately after and 3 months after the completion of the CT among manufacturing workers with long-term repetitive and unchallenging types of work. Additionally, Miller and colleagues (2019) found that after CCT, participants showed overall improvements in attention, executive function, and decision-making.
From this brief review, it is evident that there are mixed results regarding the effectiveness of CCT within the workforce. Such outcomes could be influenced by various key determinants of CCT, including the type of CCT (single domain, multi-domain), delivery method (paper-pencil, online), duration, dose (i.e., session duration), frequency (e.g., sessions per week or month), and the presence of a control group [37]. In summary, CT/CCT within the workforce context shows potential effectiveness, but further research is warranted, particularly concerning CCT with older workers.
1.5. Purpose of the Present Study
The present study aimed to assess the effectiveness of CCT in inducing changes in cognitive functions among administrative workers. To our knowledge, this is the second study to investigate trainer-guided CCT in an office setting. The study was structured as a randomized controlled intervention trial (RCT) with a wait-list control group, incorporating pre- and post-CCT assessments. In addition to examining general training effects on cognitive functions, our focus extended to evaluating the differential impact of CCT on work productivity and well-being, encompassing self-evaluations of life and job satisfaction, mood, and general health.
We hypothesize that CCT will: i) enhance cognitive functioning, preferably evidenced by far transfer effects, ii) improve self-evaluation outcomes related to perceived life and job satisfaction, mood, and general health, and iii) not impede work productivity even though the CCT sessions were conducted during regular work hours.
2. Methods
2.1. Participants
The participants for the study were recruited from employees of the Pension and Disability Insurance Institute of Slovenia (ZPIZ) and worked as insurance implementation clerks (e.g., case managers for retirement or disability requests). The workforce at PIDS consists primarily of women (81%). A pool of 82 potential participants was identified from the employee registry of the Institute (see Figure 1). Inclusion criteria included being above 50 years of age, currently working as a case manager, and having signed the consent form. From this pool, 76 participants agreed to participate and were then randomly assigned to either the Intervention or Control group (2.2. Studi design). At this stage, 10 subjects from the Intervention group and 2 subjects from the Control group were excluded due to incomplete responses on the neuropsychological tests. Thus, at the beginning of the CCT, there were 28 participants in the Intervention group and 36 subjects in the Control group. Basic demographic characteristics are presented in Table 1. All participants were right-handed, had normal or corrected-to-normal vision, and reported no history of cardiovascular disease, neurological, or psychiatric conditions. The study commenced on September 6th 2022 and concluded on December 22 th 2022. The pandemic COVID-19 was officially declared over, but the situation remained unstable due to the recurrence of new COVID-19 variants. This was the primary reason we decided to conduct group psychological testing and computerized cognitive training online. All procedures were conducted in accordance with the Declaration of Helsinki and were approved by Science and Research Centre Koper, Ethics Committee. Written informed consent was obtained from all participants prior to their involvement in the study.
2.2. Study Design
Each participant was randomly assigned to either the Intervention (INT) or passive Control (CNT) group (e.g., waitlist). The randomization process was conducted using a random-number generator in Microsoft Excel software. Prior to the CCT study, all participants underwent neuropsychological testing, followed by the administration of a demographic questionnaire, general health questionnaire, job satisfaction questionnaire, Cognitive Change Questionnaire, WHO-5 well-being questionnaire, and life satisfaction questionnaire.
Participants in the Intervention group underwent 24 sessions of CT with the maze navigation task, while participants in the Control group awaited potential replacement of drop-out participants from the Intervention group. After 12 weeks, when the CCT was completed, all participants from both the Intervention and Control groups were invited for a second round of neuropsychological testing using the same tests but in an alternative version and were asked to respond to the same questionnaires as in the initial testing.
Of the initial 28 participants assigned to the Intervention group, 2 dropped out after the initial CCT session, 6 dropped out after 2 to 4 CCT sessions, and 1 did not complete the post-CCT neuropsychological testing, resulting in 19 subjects who completed the CCT and both pre-and post-CCT testing. In the Control group, 13 participants did not attend the second testing session, resulting in a total of 23 participants in the Control group (see Figure 1).
2.3. Training Procedures
The computerized cognitive training (CCT) was offered as a health-promoting activity at the participants' workplace, either at the Pension and Disability Insurance Institute (ZPIZ) headquarters in Ljubljana, Slovenia, or at two regional offices. To familiarize the intervention group with CCT and the online virtual maze training, the first two sessions were held in the company’s conference rooms, with groups of 9 to 10 participants. During these initial sessions, an experimenter, research assistants (RAs), and an IT support specialist supervised and assisted participants with issues such as logging in and navigating the virtual maze. Subsequent CCT sessions were conducted online via a link to the company’s intranet, allowing the experimenter and IT support specialist to observe and assist participants with any logistical questions, such as logging into the server or navigating the Virtual Maze application. Participants conducted their training alone in an office or at home (remote work). The CCT was carried out in three small groups of 9 to 10 participants, scheduled on Tuesdays and Thursdays between 8 am and 12 pm during working hours, each session lasting approximately 45 minutes over a duration of 12 weeks.
2.4. Computerized Spatial Navigation Training (CCT) Protocol
Participants in the Intervention group were tasked with navigating mazes using the arrow keys on the keyboard, with each session lasting approximately 45 minutes across 22 CCT sessions. They traversed through several virtual maze environments, each designed to increase in complexity through the number of turns as the participant progressed through successively more complex levels, (task titration, see Figure 2). The tasks were displayed on a 17-inch flat panel LCD monitor positioned approximately 60 cm in front of the participants. All virtual environments were created using modified versions of Brain Powered Games: Maze Training, 2016.
The CCT task was presented from a first-person perspective and consisted of a series of interconnected hallways and alleys, with three available paths at each intersection or decision point. Some hallways led to the goal area, indicated by a trophy, while others led to dead ends. At each decision point (intersection), a pair of nonverbal cues (e.g., pictures of animals) was displayed at opposite corners. Participants were instructed to select the correct path as quickly and efficiently as possible, aiming to move toward the goal area (represented by a trophy picture) while staying in the centre of the path. Upon reaching the goal area, participants were "transported" back to the starting point to begin another learning trial of the same virtual environment. Participants began CCT with maze navigation featuring one intersection and progressed up to environments with nine intersections.
For each environment, participants were required to navigate to the goal area until successfully completing two consecutive trials without errors. Upon reaching this criterion, participants could advance to the next level of maze navigation. To mitigate practice effects across repeated testing, alternate forms with different spatial layouts were utilized for all levels of maze complexity.
2.5. Outcome Measures
All outcome measures, including questionnaires and tests, were obtained in a group setting prior to the start of CCT. Groups of employees consisting of 10 to 15 participants were comfortably seated in a conference room. After distributing brochures containing tests and questionnaires to each participant, the experimenter administered the tests by reading standard instructions aloud to all participants simultaneously. The only difference was that in some tests (e.g., AVLT, Digit span), participants were instructed to write their responses instead of verbally responding to the task at hand. Additionally, another trained experimenter supervised the test administration, overseeing participants' responses. Following the initial neuropsychological testing, 12 participants were excluded from further participation in the research project due to incomplete responses in their testing brochures (e.g., lack of responses, clearly incorrect responses, failure to follow test instructions).
2.5.1. Neuropsychological Tests
Tests assessing various cognitive domains were administered to evaluate the transfer of cognitive skills following CCT maze navigation from both proximal and distal domains. To streamline the administration of cognitive tests, a small group testing approach was adopted. Tests were conducted in small groups consisting of 5 to 10 participants, with appropriate modifications made to the test instructions. When selecting neuropsychological tests, priority was given to choosing tests that could be effectively administered in a group testing setting. For most of the selected tests, standard instructions were utilized. Further details regarding modifications to the test applications are provided for each test individually.
The Rey Auditory Verbal Learning Test [38,39,40,41] The Auditory Verbal Learning Test (AVLT) is a neuropsychological assessment tool designed to evaluate auditory verbal memory. Memory domains assessed include learning across trials representing immediate learning and delayed recall representing retention [40,42]. The AVLT comprises two lists (A and B), each containing 15 words. During the test, the administrator reads the 15 words from list A at a rate of one word per second. Following the presentation of the list, the participant is asked to recall and write down the words on paper, with no specific order required. This process is repeated five times, with the participant recalling the words on separate sheets of paper for each repetition. Subsequently, the participant is instructed to listen to list B, which serves as interference. Afterwards, another recall of words from list A is conducted. The participant is then asked to recall the words from list A after a delay of 20 to 30 minutes, reflecting longer term recall. To ensure accuracy in scoring, any confabulations (fabricated responses), intrusions, or substitutions are disregarded when counting correctly written words [40,42].
Verbal Fluency; This test measures the number of words recalled (written on paper) by a participant, typically within a specified category or in response to a particular letter, within a set time limit. This test assesses recall of longer term verbal storage and general verbal abilities and has also been related to basic executive functions [43,44,45]. We utilized two basic types of verbal fluency tests:
a) Letter Verbal Fluency (LVF) Test: In this test, participants were instructed to write down as many words as possible that begin with the letter "F" in the first testing session and "S" in the second testing session, within a time limit of 60 seconds.
b) Semantic Verbal Fluency (SVF) Test: Participants were asked to verbally generate and write down as many words as possible from the semantic categories of ‘animals’ during the pre-CCT testing and ‘fruits & vegetables’ during the post-CCT testing. They were allotted 60 seconds for each category.
The final raw score was determined by summing the words written in the test brochure within the specified time limit for each category in each task. Repetitions of the same word or intrusions (incorrect words) were not included in the final score.
Digit Span; The Digit Span test is a subtest of the Wechsler Adult Intelligence Scale-III (DSpan) [46]. This test assesses direct verbal digit recall and the components measure both basic attention and working memory/concentration. The test involves two different tasks. In the first task, the individual is required to recall numbers in the same order as they are originally presented (Digits Forward), while in the second task, the individual is asked to recall the given numbers in reverse order (Digits Backwards). The experimenter reads a continuous sequence of numbers, one per second that are then repeated. Each task consists of two attempts for each sequence of numbers, ranging from 2 to 9 in the Forward task and from 2 to 8 in the Backward task. During group testing, the experimenter reads all the sequences, from the lowest to the highest sequence. The result represents the number of correctly recalled numbers written in the testing brochure. Reliability coefficients over time range between 0.66 and 0.89, depending on the length of the interval and the age of the individuals [47].
Digit Symbol Substitution Test;The Digit Symbol Substitution Test, initially introduced to measure information processing speed [46], is a component of the Wechsler Battery of Intelligence Tests [40]. This test assesses psychomotor abilities by presenting the individual with a line containing nine numbers and corresponding symbols, serving as a key [47]. Each number is paired with a specific symbol. Initially, the test subject completes a trial section to familiarize themselves with the symbols associated with each number. Upon receiving a signal from the experimenter, the subject proceeds to fill in the blank fields with the appropriate symbols beneath each number. The objective is to fill in as many blank fields as possible within a limited time frame. In our study, we restricted the solving time to 60 seconds. The result is determined by the number of correctly written symbols within this time limit. The Digit Symbol Substitution Test demonstrates high reliability and stability over time [47,48], with reliability coefficients ranging from 0.82 to 0.88. Furthermore, the test exhibits sensitivity in identifying dementia and monitoring its progression.
Pattern Comparison The Pattern Comparison test [49,50], assesses cognitive abilities related to perceptual speed. In this test, participants are presented with 30 pairs of patterns, each consisting of 3-, 6-, or 9-line segments. Within a time, limit of 30 seconds per page, participants are instructed to indicate whether the patterns in each pair are the same (by writing "S") or different (by writing "D"). This test exhibits high reliability, with coefficients of 0.85 among students and 0.90 among older adults. Additionally, it is highly correlated with measures of perceptual speed [49].
For all above-listed neuropsychological tests, the primary outcome measures were number of correct responses.
2.5.2. Questionnaires
Job Satisfaction Questionnaire (MSQ); Job satisfaction is commonly understood as the array of feelings or affective responses linked to the job environment, or simply put, "how people feel about different aspects of their jobs" [51]. In 1967, Weiss et al. developed the short version of the Minnesota Satisfaction Questionnaire (MSQ), which employs a 5-point Likert-type scale comprising 20 items. This instrument has shown strong stability over time [52]. A systematic review by Van Saane [53] reported that the MSQ had an internal consistency of 0.92, a test-retest reliability of 0.89, and a convergent validity of 0.83.
General Health Questionnaire; This questionnaire developed by the research team is composed of 3 questions asking a participant to evaluate on 5-point scale (1 = very bad to 5 = very good) his/her overall health, and, separately, his/her physical and then mental health.
Cognitive Change Questionnaire (CCQ); The Cognitive Change Questionnaire (CCQ) [54] used during the COVID-19 pandemic, was modified for the self-assessment of cognitive change in this study. The questionnaire was comprised of 9 items self-reporting changes observed in everyday cognitive functions, specifically related to the speed of information processing, short-term storage, prospective memory, attention, and executive control. Participants were instructed to compare their cognitive functions before and after CCT training, using a 7-point scale. For items 1–5, the scale ranged from 1 = "much less often" to 7 = "much more often" compared to before the CCT. For items 6–9, the scale ranged from 1 = "much easier" to 7 = "much harder" than before the CCT. Scores on the CCQ range from 9 to 35, with higher scores indicating a greater self-perceived decline in cognitive functioning.
Satisfaction With Life Scale (SWLS); The Satisfaction With Life Scale (SWLS) [55], is a 5-item scale designed to measure overall life satisfaction based on an individual's own subjective criteria. This scale has been widely utilized and demonstrates internal consistency and temporal stability estimates ranging from 0.54 for a 4-year interval to as high as 0.89 for a 2-week interval [56]. Participants rate their agreement with each statement using a 7-point scale, ranging from 1 = "strongly disagree" to 7 = "strongly agree". Scores on the SWLS range from 5 to 35, with higher scores indicating greater life satisfaction.
The WHO-5 Well-Being Index [57], is a widely used questionnaire designed to measure well-being [57]. It consists of five items, such as "Over the last month I have felt cheerful and in good spirits," which are rated on a 6-point Likert scale. Responses range from 0 = "never" to 5 = "all the time." Higher scores on the WHO-5 indicate a greater state of well-being. The WHO-5 has been validated in numerous studies and has demonstrated good psychometric properties [58].
2.6. Productivity
Productivity is measured by a standard company measure, so-called ponder, a composite measure of productivity expressed in time needed for each clerical procedure as related to the complexity (demands) of documents to be produced. Higher number of ponders represents higher employee’s output.
2.7. CCT Satisfaction Measure
To obtain participants’ attitudes and opinion of the CCT experience, they were asked to respond to two questions related to their satisfaction with CCT training program and with administration of the CCT. This was done using a 4-point scale where 1 = completely satisfied and 4 = completely unsatisfied. Lower number represents higher satisfaction with CCT and the administration of CCT.
Productivity measures were recorded and provided by the work organization, while other measures were collected by the research team.
2.8. Statistical Procedures
The data were analyzed using IBM SPSS Statistics 22.0 software for Windows (SPSS, Inc., Chicago, IL, USA), and results are presented in tables displaying means ± standard deviations. Prior to analysis, the homogeneity of variances was assessed using Levene’s test, while the normality of parameter distributions was examined using the Shapiro–Wilk’s test. For variables with questionable assumptions regarding normality, the nonparametric Mann–Whitney U-test was employed. Additionally, the outcome measures underwent a two-way analysis of variance (ANOVA) with the time-point variable (pre-CCT, post-CCT) treated as a within-subject variable and the group (intervention, control) as a between-subject variable. To further elucidate the differences between the two groups, the η2 coefficient was calculated, with values of 0.01 representing a small effect size, 0.06 a medium effect size, and values above 0.14 indicative of a large effect size [59].
3. Results
3.1. Sample Univariate Description
The demographic results of the participants in the Intervention and Control groups are presented in Table 1. Independent sample t-test analyses showed that there were no statistically significant differences between the intervention and control groups for any of the variables. The intervention and control groups did not differ in age or years of education.
Participants from the Intervention group were above average satisfied with CCT and its administration (1.75 and 1.51 on 4-point scale with mean value of 2.50).
3.2. CCT Effectiveness
The performance scores for all neuropsychological tests for both groups from pre-and post-CCT are presented in Table 2.
Mixed ANOVAs did not show any significant main effects of group (p >. 14) across any of the outcome variables. However, the mixed ANOVA for the Verbal Fluency letter showed that there was a significant interaction effect between time and group f [F(1,40) = 4.387, p = 0.043, η2 = 0.099] (See Figure 3). A subsequent post hoc analysis indicated a significant improvement in both groups (p < 0.001), though there was a significant difference between the post-CCT score for the groups (p = 0.05), demonstrating that participants in the Intervention group significantly increased their performance on the Verbal Fluency Letter test more than participants in the Control group (from 9.16 to 17.32 vs. 9.39 to 15.13, respectively).
A mixed ANOVA also demonstrated a significant main effect for time on the AVLT Immediate and Delayed recall (p = 0.02), and Coding tests (p = 0.02). On each of these tests all participants on average improved their performance. For the Comparison test, there was a tendency (p = 0.08) for a decrease in performance after CCT. Specifically, there was a significant decrease in performance in the Control group (p = 0.04), while there was no significant change in the Intervention group (p = 0.87).
3.3. CCT Effects on Productivity and Well-Being
The responses for all the questionnaires for both groups from pre-and post-CCT are presented in Table 3. Mixed ANOVA showed that there were no significant main effects for group or time nor significant interaction effects. However, there was a non-significant trend for work productivity (p = 0.09). When this was evaluated further, it was revealed that there was no change in productivity between pre-and post-CCT for the Intervention group (p = 0.49), but a significant decrease in productivity in the Control group (p = 0.02) (see Figure 4).
In addition, although the Cognitive change Questionnaire did not show any significant differences between the Intervention and Control group, a further evaluation was carried out to evaluate the relationship between CCQ and health scores for each of the groups. Here, there was a significant negative correlation between CCQ and health score for the Control group (r = -0.46, p = 0.04) but not for Intervention group: (r = 0.01, p = 0.98): Control participants with higher self-evaluated cognitive issues also endorsed lower self-evaluated health status (see Figure 5). There was also a trend for a negative correlation between CCQ and wellbeing for the Control group (r = -0.41, p = 0.06) but not for the Intervention group (r = -0.07, p = 0.90).
On a 4-point scale, a one-sample t-test showed that participants from the intervention group were slightly more satisfied than average with the CCT (t = -1.68, p = 0.11) and highly satisfied with the administration of the CCT (t = -3.34, p = 0.004).
4. Discussion
The current study provides positive outcomes showing that a short course of CCT, conducted in an office setting during working hours, is effective for middle-aged workers in terms of enhancing aspects of their fluid cognitive functions while maintaining work productivity. Thus, the outcomes support our first hypothesis that CCT will enhance cognitive functioning, as evidenced by moderate but significant performance improvements on the VF-L measure related to executive functioning. We cannot accept the second hypothesis since we did not observe improved self-reported well-being or life satisfaction after the CCT in the Intervention group. We also accept the third hypothesis that CCT administered during regular work hours did not decrease the productivity of middle-aged workers involved in CT. These workers, performing moderately demanding jobs during the three-month engagement in CCT, did not show any decline in productivity. On the contrary, during the period of CCT administration, the older workers in the passive control group showed decreased productivity. Furthermore, those employees in the control group who self-evaluated increased difficulty in their cognitive functioning also reported a significant decline in their overall health status. In other words, CCT appears to have a sustaining or perhaps protective effect.
3.4. CCT and Cognitive Functioning
Findings from this study are comparable to those reported by Muller et al. [36], which showed that employees improved in executive functioning after CCT. They are also partially aligned with Gajewski [34], who reported improvements in task switching among manufacturing workers engaged in repetitive tasks. Additionally, our study's findings are consistent with Marusic [60], which reported improved executive functioning in healthy older adults after CCT during a 14-day bed rest period.
It is exciting to see improvement in VF-L in middle-aged employees after CCT. However, an intriguing question arises from this finding: can this improvement be considered a near or far transfer from two perspectives: i) the task utilized in CCT, and ii) the neurocognitive instrument used to evaluate executive functioning? Namely, CCT with virtual maze navigation is not based on any specific cognitive function but is rather task-based, encompassing a variety of cognitive functions, primarily working memory and executive functioning, for proper maze navigation. One can argue that maze navigation engages multiple cognitive functions, including attention, working memory, decision making, and executive functioning. This statement is supported by studies showing strong correlations between spatial navigation performance, both in-person and online in virtual reality, with spatial memory [61], episodic memory [62], and executive functioning [63,64]. Thus, adopting the notion that near transfer encompasses the same construct in the training task and the cognitive test [65] the improved performance on VF-L can be, or should be, considered near transfer.
The claim that improved performance on VF-L reflects near transfer must also consider the similarity of the task and test instrument in terms of their delivery and testing modality. Somewhat surprisingly, the greatest effect of the virtual maze navigation training, a purely visuospatial task, occurred on the VF-L test, which is a purely verbal test measuring working memory and executive functioning. Our previous study with virtual maze navigation CCT [66] also showed an increase in executive functioning, but it was measured with the TMT-B test, which is also primarily a visuospatial task. Therefore, our finding of significantly increased performance on VF-L could also be considered far transfer.
Another intriguing finding in our study is difference between the two verbal fluency tasks, VF-L and VF-S. After CCT we observed the transfer in VF-L but VF-S. Despite their traditional wide adoption in clinical and diagnostic practice, there is ongoing scientific discussion regarding the relationship between semantic and letter verbal fluency tasks and what brain functions underlie their performance. In the VF-S task, the constraint is that all produced words should belong to one semantic category (e.g., animals). In the VF-L task, the constraint is that all produced words should start with one letter (e.g., S). In general, verbal fluency tasks engage multiple neurocognitive functions, including executive functions, memory, and language components. The difference between the two tasks is often explained by the fact that in VF-S, one can follow associations for word production, whereas in VF-L, associations must also be monitored for their phonemic fit, which places additional executive function demands. In this study, the letter fluency significant finding may further emphasize the role of executive functioning.
In this study, it is also noticeable that there is a lack of transfer (i.e., improved performance) in memory testing with AVLT and in the speed of processing as measured by the Coding and Comparisons tests. In the AVLT delayed recall and Coding, we observed significant improvements in both the Intervention and Control groups. The most parsimonious explanation could be that delayed recall and processing speed are susceptible to practice effects and/or that the underlying neural networks underlying these two tasks are not specifically involved in training with virtual maze navigation and therefore did not improve primarily in the CCT group.
The initial publication of CCT within the workforce by Borness et al. [33] did not support the effectiveness of CCT in an office-based workforce but rather noted that documentary watching in the active control group appeared a more effective intervention. It is very likely that this initial report dampened further attempts to conduct CCT with an older workforce. Therefore, it is very important that our study adds to the CCT workplace literature with older, middle-aged workers in several regards: i) Demonstrating that CCT is feasible in the workplace and can improve some cognitive functions, albeit to a limited degree; ii) Indicating that devoting regular work hours to CCT does not cause a decline in productivity (e.g., highlighting the importance of a adding productivity measurement to the study); iii) CCT maintain the performance on the simple attentional test and their self-evaluation of their cognitive abilities after the CCT at the same level as pre-CCT in the Intervention group while there was indication of decline in Control group; and iv) Most importantly, confirming that CCT was not associated with any negative effects during or after the training.
3.5. CCT and Work Productivity
Results also showed that the CCT affected productivity not by increasing it, but by maintaining it. Productivity outcomes clearly demonstrated that employees in the intervention group maintained their productivity, while the productivity of participants in the control group significantly dropped. The decreased productivity among the control group participants is difficult to interpret. The most likely explanation for such outcome is the period at the end of 2022 was challenging for this agency due to an increased workload related not only to completing outstanding cases but also to pension and disability legislative changes that needed to be incorporated into the work process. Thus, it is very likely that toward the end of 2022, there was increased stress in the workplace due to the pressure related to finishing certain tasks and adapting to legislative changes. The key point is that participants in the intervention group maintained the same level of productivity despite dedicating two hours of their weekly working quota to CCT. It is also important to note that participants from the intervention group rated their satisfaction with the CCT process and its administration above average. This outcome is significant for future studies, conveying the message that the time devoted to CCT is unlikely to decrease the productivity of employees engaged in it.
3.6. CCT and Well-Being
An unexpected pattern observed between the association of self-reported changes in cognitive performance during the 3- months period of administration of CCT self-evaluated health status and well-being. Participants from the Control group who reported worsening of their cognitive functioning showed lower self-evaluated health status (Figure 5), while participants from the Intervention group did not report any decline in their health-status and well-being. These findings may suggest that the CCT effects are not only the improvement on cognitive performance but also preservation, maintenance of the health and well-being while maintaining productivity at the same level. To the best of our efforts, we could not find publications in this regard.
None of the studies on the effectiveness of CCT with employees have investigated the effects of CCT on participants' well-being, life satisfaction, or health status. According to Nedeljko et al. [67], digital technologies have the potential to improve the quality of working life for older workers [67]. Thus, our study is the first to report the effects of CCT on older employees' well-being. Employees in the intervention group reported their health status and well-being as unchanged after the CCT, while participants in the control group expressed a significant decline. The closest comparisons regarding the effectiveness of CCT on self-evaluated life satisfaction can be found in reports on the effectiveness of CCT with older adults. A few studies have reported improved self-evaluated well-being after CCT [68]. Similarly, Gordon et al. [69] reported that an online brain training program, MyBrainSolutions, positively affected well-being. The maintenance of well-being after CCT is consistent with findings reported in a review article by Sheng et al. [70], who noted significant improvements in well-being in older adults with subjective memory complaints. However, there are a few other meta-analyses investigating the effects of commercial video and action video games as tools for enhancing individuals' well-being, particularly in terms of cognitive and emotional enhancement [71,72,73].
Our findings are also in line with conclusions from a meta-analysis that reviewed publications related to the effectiveness of interventions for improving subjective well-being among workers [74]. They reported that mindfulness and cognitive-behavioural approaches may be useful for improving employees' well-being. We can now add that CCT can also help maintain older workers' well-being. Furthermore, a systematic literature review of cognitive intervention studies among individuals with mild cognitive impairment [75] suggested that some interventions were equally or more effective on subjective measures of mood and quality of life than on objective measures of cognitive domains. Therefore, an improvement or even no change in well-being and life satisfaction scales at the end of the CCT might be considered a desirable treatment outcome. In other words, the benefits of CCT may translate into the daily functioning and mood of the participants, which should be the ultimate goal of any cognitive program or intervention. This also supports the argument that CCT in the workplace may have more distal/far-transfer effects on workers and their life well-being.
3.7. Limitations of the Study
Despite its strengths, our study has several limitations. In addition to the small sample size, our sample was heavily biased by female participants. The use of a passive control group could also be considered a limitation, but due to the limited training staff, adding an active control group was not feasible. The testing of CCT efficiency for the older workforce was also limited because we focused exclusively on case managers, without including other job roles at ZPIZ in terms of complexity and educational level. It should be noted that ZPIZ indicated that the case manager was the most frequent job requiring a master’s degree level for education. Furthermore, our study lacks additional long-term post-CCT evaluations of cognitive and emotional outcome measures. For instance, Borness et al. [33] reported improved quality of life, psychological well-being, and decreased stress levels six months after the CCT, albeit in the active control group. Additionally, in our study, we evaluated cognitive functioning based on group testing, which not only limited the selection of neuropsychological tests for cognitive evaluation but also posed challenges for standardized administration and supervision of cognitive testing. The administration of online cognitive tests would have been a better approach, but at the time of the CCT, we did not have such tests available (e.g., the Slovenian version of computerized batteries like NIH Toolbox or CogState). Future research may explore how these listed shortcomings might affect specific cognitive domains and vice versa.
4. Conclusion
Our study, conducted in an office setting during regular office hours, contributes to the general view that CCT can be useful and effective for the older workforce and does not represent a burden for either employers or employees. Consistent with our expectations, CCT was effective in improving aspects of executive functioning while maintaining work productivity. Thus, CCT may be an important tool in business to improve adaptability and potentially attenuate cognitive decline in the ageing workforce. Future research can develop shorter, more focused CCT or multimodal short interventions that could be offered as brief units during breaks or even work hours, supported by both employers and employees [76]. In other words, CCT could enhance self-perceived health, improve emotional functioning, and increase cognitive functioning, and job satisfaction, leading to maintained or even improved productivity in the older workforce. This may, in turn, prolong employment and prevent premature retirement as the workforce ages.
Author Contributions
For the research articles the authors contribute as follows: conceptualization Z.M-K, V.K., B.G. and U.M.; methodology, Z.M-K, V.K., B.G. and U.M.; software, B.G.; validation, V.K., B.G. and U.M.; formal analysis, Z.M-K. and U.M.; investigation, Z.M-K.; data curation, Z.M-K.; writing—original draft preparation, Z.M-K. and V.K.; writing—review and editing, B.G. and U.M.; supervision, U.M.; project administration, Z.M-K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted by the Declaration of Helsinki and approved by the Ethics Committee by Science and Research Centre Koper, (protocol code 0624-74/22 from September 5th 2022), for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data will be available by a request to the first author after the conclusion of her PhD study.
Acknowledgments
The authors thank the research participants from the Pension and Disability Insurance Institute of Slovenia (ZPIZ) for their involvement in this study. Special thanks to the entire management team of ZPIZ, especially Director General Mr. Marijan Papež, who recognized the importance of our research for older employees, organized and coordinated all processes inside ZPIZ, and gave us all the support we needed so the process ran smoothly and without delay, Mrs. Ajša Hajzer, Head-Division Director I, Legal, Human Resources Development and Business Process Management Service, Mrs. Blanka Špoljarić, Head of Service I, Human Resources Development and Business Process Management Service, Mrs. Taja Žaberl, Head-Director of Regional Unit, Mr. Mitja Žiher, Head-Director of Regional Unit, and Mrs. Daša Selan, Senior Branch Adviser III, Human Resources Development and Business Process Management Service. Additional thanks, to Mrs. Sanja Medved, Head of Service II, Legal, Human Resources Development and Business Process Management Service, for providing invaluable assistance and operational support throughout the research conducted at the company. We also extend our gratitude to the Computer Communication and User Equipment Service, IT Division, for their efforts and support in recruitment and data collection, particularly Mr. Samo Kobal for his reliable technical support. Heartfelt thanks to all the study participants who persevered with us. We would like to thank the students Brina Vadnjal, Gabrijela Valenčič, Tisa Hodnik, and Mihael Nedeljko for their logistic assistance, to Lara Žepič for managing the work and data, as well as to Professor Mrs. Vida Bogataj for her general aid. Finaly, UM acknowledges the financial support from the Slovenian Research Agency (research core funding No. P5-0381) as well as financial support by the European Union's Horizon 2020 research and innovation program under grant agreement No. 952401 and Horizon Europe under grant agreement No. 101120150.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Schmidt, F.L. The Role of General Cognitive Ability and Job Performance: Why There Cannot Be a Debate. In <italic>Role of General Mental Ability in industrial, Work, and Organizational Psychology</italic>; Psychology Press, 2002 ISBN 978-1-4106-0880-2.
- Ree, M.J.; Earles, J.A.; Teachout, M.S. Predicting Job Performance: Not Much More than g. Journal of Applied Psychology 1994, 79, 518–524. [Google Scholar] [CrossRef]
- Aiyar, S.; SAiyar@imf.org; Ebeke, C.; CEbeke@imf.org The Impact of Workforce Aging on European Productivity. IMF Working Papers 2016, 16, 1. [CrossRef]
- Baltes, M.M.; Carstensen, L.L. The Process of Successful Aging: Selection, Optimization, and Compensation. In Understanding Human Development: Dialogues with Lifespan Psychology; Staudinger, U.M., Lindenberger, U., Eds.; Springer US: Boston, MA, 2003; ISBN 978-1-4615-0357-6. [Google Scholar]
- Kubeck, J.E.; Delp, N.D.; Haslett, T.K.; McDaniel, M.A. Does Job-Related Training Performance Decline with Age? Psychology and Aging 1996, 11, 92–107. [Google Scholar] [CrossRef] [PubMed]
- Schooler, C.; Mulatu, M.S.; Oates, G. The Continuing Effects of Substantively Complex Work on the Intellectual Functioning of Older Workers. Psychology and aging 1999, 14, 483. [Google Scholar] [CrossRef] [PubMed]
- Bosma, H.; van Boxtel, M.P.; Ponds, R.W.; Houx, P.J.; Burdorf, A.; Jolles, J. Mental Work Demands Protect against Cognitive Impairment: MAAS Prospective Cohort Study. Experimental aging research 2003, 29, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Marquié, J.-C.; Duarte, L.R.; Bessières, P.; Dalm, C.; Gentil, C.; Ruidavets, J.B. Higher Mental Stimulation at Work Is Associated with Improved Cognitive Functioning in Both Young and Older Workers. Ergonomics 2010, 53, 1287–1301. [Google Scholar] [CrossRef] [PubMed]
- Correa Ribeiro, P.C.; de Souza Lopes, C.; Alves Lourenço, R. Prevalence of Dementia in Elderly Clients of a Private Health Care Plan: A Study of the FIBRA-RJ, Brazil. Dementia and geriatric cognitive disorders 2013, 35, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Curreri, C.; Trevisan, C.; Grande, G.; Giantin, V.; Ceolin, C.; Maggi, S.; Noale, M.; Baggio, G.; Sergi, G. The Influence of Occupation Type and Complexity on Cognitive Performance in Older Adults. Psychiatry Research: Neuroimaging 2022, 326, 111542. [Google Scholar] [CrossRef] [PubMed]
- Kleineidam, L.; Wolfsgruber, S.; Weyrauch, A.-S.; Zulka, L.E.; Forstmeier, S.; Roeske, S.; van den Bussche, H.; Kaduszkiewicz, H.; Wiese, B.; Weyerer, S. Midlife Occupational Cognitive Requirements Protect Cognitive Function in Old Age by Increasing Cognitive Reserve. Frontiers in Psychology 2022, 13, 957308. [Google Scholar] [CrossRef]
- Craik, F.I.; Bialystok, E. Brain Changes in Development and Aging. Trends in Cognitive Sciences 2006, 3, 131–138. [Google Scholar] [CrossRef]
- Kavčič, V. <italic>Umovadba</italic>; Založba Miš, 2015.
- Bläsing, B. Dance Expertise, Embodied Cognition, and the Body in the Brain. In <italic>Dance data, cognition, and multimodal communication</italic>; Routledge, 2022; pp. 223–243.
- Bahar-Fuchs, A.; Martyr, A.; Goh, A.M.; Sabates, J.; Clare, L. Cognitive Training for People with Mild to Moderate Dementia. Cochrane Database of Systematic Reviews 2019. [Google Scholar] [CrossRef]
- Saczynski, J.S.; Rebok, G.W.; Whitfield, K.E.; Plude, D.L. Spontaneous Production and Use of Mnemonic Strategies in Older Adults. Experimental Aging Research 2007, 33, 273–294. [Google Scholar] [CrossRef] [PubMed]
- Buiza, C.; Etxeberria, I.; Galdona, N.; González, M.F.; Arriola, E.; De Munain, A.L.; Urdaneta, E.; Yanguas, J.J. A Randomized, Two-year Study of the Efficacy of Cognitive Intervention on Elderly People: The Donostia Longitudinal Study. Int J Geriat Psychiatry 2008, 23, 85–94. [Google Scholar] [CrossRef]
- Corbett, A.; Owen, A.; Hampshire, A.; Grahn, J.; Stenton, R.; Dajani, S.; Burns, A.; Howard, R.; Williams, N.; Williams, G.; et al. The Effect of an Online Cognitive Training Package in Healthy Older Adults: An Online Randomized Controlled Trial. Journal of the American Medical Directors Association 2015, 16, 990–997. [Google Scholar] [CrossRef]
- Klimova, B. Computer-Based Cognitive Training in Aging. Front. Aging Neurosci. 2016, 8. [Google Scholar] [CrossRef]
- Ball, K.; Berch, D.B.; Helmers, K.F.; Jobe, J.B.; Leveck, M.D.; Marsiske, M.; Morris, J.N.; Rebok, G.W.; Smith, D.M.; Tennstedt, S.L.; et al. Effects of Cognitive Training Interventions With Older AdultsA Randomized Controlled Trial. JAMA 2002, 288, 2271–2281. [Google Scholar] [CrossRef] [PubMed]
- Marusic, U.; Verghese, J.; Mahoney, J.R. Cognitive-Based Interventions to Improve Mobility: A Systematic Review and Meta-Analysis. Journal of the American Medical Directors Association 2018, 19, 484–491. [Google Scholar] [CrossRef]
- Gates, N.J.; Rutjes, A.W.; Di Nisio, M.; Karim, S.; Chong, L.-Y.; March, E.; Martínez, G.; Vernooij, R.W. Computerised Cognitive Training for Maintaining Cognitive Function in Cognitively Healthy People in Midlife. Cochrane Database of Systematic Reviews 2019. [Google Scholar] [CrossRef]
- Kelly, M.E.; Loughrey, D.; Lawlor, B.A.; Robertson, I.H.; Walsh, C.; Brennan, S. The Impact of Cognitive Training and Mental Stimulation on Cognitive and Everyday Functioning of Healthy Older Adults: A Systematic Review and Meta-Analysis. Ageing Research Reviews 2014, 15, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Žepič, Z.M. Improvement of Cognitive Abilities of Older Employees with Computerized Cognitive Training (CCT). IFAC-PapersOnLine 2021, 54, 651–656. [Google Scholar] [CrossRef]
- Makin, S. Brain Training: Memory Games. Nature 2016, 531, S10–S11. [Google Scholar] [CrossRef] [PubMed]
- Traut, H.J.; Guild, R.M.; Munakata, Y. Why Does Cognitive Training Yield Inconsistent Benefits? A Meta-Analysis of Individual Differences in Baseline Cognitive Abilities and Training Outcomes. Frontiers in Psychology 2021, 12, 662139. [Google Scholar] [CrossRef] [PubMed]
- Abd-Alrazaq, A.; Alajlani, M.; Alhuwail, D.; Toro, C.T.; Giannicchi, A.; Ahmed, A.; Makhlouf, A.; Househ, M. The Effectiveness and Safety of Serious Games for Improving Cognitive Abilities among Elderly People with Cognitive Impairment: Systematic Review and Meta-Analysis. JMIR serious games 2022, 10, e34592. [Google Scholar] [CrossRef] [PubMed]
- Von Bastian, C.C.; Reinhartz, A.; Udale, R.C.; Grégoire, S.; Essounni, M.; Belleville, S.; Strobach, T. Mechanisms of Processing Speed Training and Transfer Effects across the Adult Lifespan: Protocol of a Multi-Site Cognitive Training Study. BMC Psychol 2022, 10, 168. [Google Scholar] [CrossRef] [PubMed]
- Sala, G.; Aksayli, N.D.; Tatlidil, K.S.; Tatsumi, T.; Gondo, Y.; Gobet, F. Near and Far Transfer in Cognitive Training: A Second-Order Meta-Analysis. Collabra: Psychology 2019, 5, 18. [Google Scholar] [CrossRef]
- von Bastian, C.C.; Hyde, E.R.; Jiang, S. Tackling Cognitive Decline in Late Adulthood: Cognitive Interventions. Current Opinion in Psychology 2023, 101780. [Google Scholar] [CrossRef] [PubMed]
- Olegário, R.L.; Fernandes, S.R.; de Moraes Jr, R. Efficacy of Cognitive Training on Executive Functions in Healthy Older Adults: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Psychology & Health 2023, 1–28. [Google Scholar]
- Marusic, U.; Žepič, Z.; Kavčič, V. Učinkovitost Računalniškega Kognitivnega Treninga v Domovih Starejših Občanov / Effectiveness of Computerized Cognitive Training in Nursing Homes. Psihološka obzorja / Horizons of Psychology 2021, 47–54. [Google Scholar] [CrossRef]
- Borness, C.; Proudfoot, J.; Crawford, J.; Valenzuela, M. Putting Brain Training to the Test in the Workplace: A Randomized, Blinded, Multisite, Active-Controlled Trial. PLoS ONE 2013, 8, e59982. [Google Scholar] [CrossRef]
- Gajewski, P.D.; Freude, G.; Falkenstein, M. Cognitive Training Sustainably Improves Executive Functioning in Middle-Aged Industry Workers Assessed by Task Switching: A Randomized Controlled ERP Study. Front. Hum. Neurosci. 2017, 11. [Google Scholar] [CrossRef]
- Lampit, A.; Ebster, C.; Valenzuela, M. Multi-Domain Computerized Cognitive Training Program Improves Performance of Bookkeeping Tasks: A Matched-Sampling Active-Controlled Trial. Front. Psychol. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.; Chelian, S.; Mcburnett, W.; Tsou, W.; Kruse, A. An Investigation of Computer-Based Brain Training on the Cognitive and EEG Performance of Employees.; July 24 2019; Vol. 2019.
- Lampit, A.; Hallock, H.; Valenzuela, M. Computerized Cognitive Training in Cognitively Healthy Older Adults: A Systematic Review and Meta-Analysis of Effect Modifiers. PLoS Med 2014, 11, e1001756. [Google Scholar] [CrossRef] [PubMed]
- Rey, A. L’examen Psychologique Dans Les Cas d’encéphalopathie Traumatique.(Les Problems.). Archives de psychologie 1941. [Google Scholar]
- Schmidt, M. <italic>Rey Auditory Verbal Learning Test: RAVLT: A Handbook</italic>; Western Psychological Services, 1996.
- Lezak, M.D. <italic>Neuropsychological Assessment</italic>; Oxford University Press, 2004; ISBN 978-0-19-511121-7.
- Spreen, O.; Strauss, E. A Compendium of Neuropsychological Tests. 2nd Edn New York; NY: Oxford University Press, 1998. [Google Scholar]
- Fernaeus, S.-E.; Östberg, P.; Wahlund, L.-O.; Hellström, Å. Memory Factors in Rey AVLT: Implications for Early Staging of Cognitive Decline. Scandinavian Journal of Psychology 2014, 55, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Aita, S.L.; Beach, J.D.; Taylor, S.E.; Borgogna, N.C.; Harrell, M.N.; Hill, B.D. Executive, Language, or Both? An Examination of the Construct Validity of Verbal Fluency Measures. Applied Neuropsychology: Adult 2018. [Google Scholar] [CrossRef] [PubMed]
- Barry, D.; Bates, M.E.; Labouvie, E. FAS and CFL Forms of Verbal Fluency Differ in Difficulty: A Meta-Analytic Study. Applied neuropsychology 2008, 15, 97–106. [Google Scholar] [CrossRef]
- Boivin, M.J.; Giordani, B.; Berent, S.; Amato, D.A.; Lehtinen, S.; Koeppe, R.A.; Buchtel, H.A.; Foster, N.L.; Kuhl, D.E. Verbal Fluency and Positron Emission Tomographic Mapping of Regional Cerebral Glucose Metabolism. Cortex 1992, 28, 231–239. [Google Scholar] [CrossRef]
- Weschler, D. <italic>Weschler Adult Intelligence Scale</italic>; Tretja edicija.; Psychological Corporation New York, 1997. 1997.
- Matarazzo, J.D.; Herman, D.O. Base Rate Data for the WAIS-R: Test-Retest Stability and VIQ-PIQ Differences. Journal of Clinical and Experimental Neuropsychology 1984, 6, 351–366. [Google Scholar] [CrossRef]
- Rosano, C.; Perera, S.; Inzitari, M.; Newman, A.B.; Longstreth, W.T.; Studenski, S. Digit Symbol Substitution Test and Future Clinical and Subclinical Disorders of Cognition, Mobility and Mood in Older Adults. Age and ageing 2016, 45, 688–695. [Google Scholar] [CrossRef]
- Salthouse, T.A.; Babcock, R.L.; Shaw, R.J. Effects of Adult Age on Structural and Operational Capacities in Working Memory. Psychology and aging 1991, 6, 118. [Google Scholar] [CrossRef]
- Salthouse, T.A.; Babcock, R.L. Decomposing Adult Age Differences in Working Memory. Developmental psychology 1991, 27, 763. [Google Scholar] [CrossRef]
- Spector, P.E. <italic>Job Satisfaction: Application, Assessment, Causes, and Consequences</italic>; Sage, 1997; Vol. 3; ISBN 0-7619-8923-4.
- Fields, D.L. <italic>Taking the Measure of Work: A Guide to Validated Scales for Organizational Research and Diagnosis</italic>; Sage, 2002; ISBN 0-7619-2425-6.
- Van Saane, N.; Sluiter, J.K.; Verbeek, J.; Frings-Dresen, M.H. Reliability and Validity of Instruments Measuring Job Satisfaction—a Systematic Review. Occupational medicine 2003, 53, 191–200. [Google Scholar] [CrossRef]
- Podlesek, A.; Komidar, L.; Kavcic, V. The Relationship Between Perceived Stress and Subjective Cognitive Decline During the COVID-19 Epidemic. Front. Psychol. 2021, 12, 647971. [Google Scholar] [CrossRef]
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. Journal of personality assessment 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E. Review of the Satisfaction with Life Scale. Psychological assessment 1993, 5, 164. [Google Scholar] [CrossRef]
- Organization, W.H. Use of Well-Being Measures in Primary Health Care-the DepCare Project Health for All. Target 1998, 12, E60246. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychotherapy and psychosomatics 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. <italic>Statistical Power Analysis for the Behavioral Sciences.</italic>; Vol. 1988.
- Marusic, U.; Kavcic, V.; Giordani, B.; Gerževič, M.; Meeusen, R.; Pišot, R. Computerized Spatial Navigation Training during 14 Days of Bed Rest in Healthy Older Adult Men: Effect on Gait Performance. Psychology and Aging 2015, 30, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Lithfous, S.; Dufour, A.; Després, O. Spatial Navigation in Normal Aging and the Prodromal Stage of Alzheimer’s Disease: Insights from Imaging and Behavioral Studies. Ageing research reviews 2013, 12, 201–213. [Google Scholar] [CrossRef]
- Jebara, N.; Orriols, E.; Zaoui, M.; Berthoz, A.; Piolino, P. Effects of Enactment in Episodic Memory: A Pilot Virtual Reality Study with Young and Elderly Adults. Frontiers in aging neuroscience 2014, 6, 338. [Google Scholar] [CrossRef]
- Moffat, S.D.; Kennedy, K.M.; Rodrigue, K.M.; Raz, N. Extrahippocampal Contributions to Age Differences in Human Spatial Navigation. Cerebral Cortex 2007, 17, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Taillade, M.; Sauzéon, H.; Dejos, M.; Arvind Pala, P.; Larrue, F.; Wallet, G.; Gross, C.; N’Kaoua, B. Executive and Memory Correlates of Age-Related Differences in Wayfinding Performances Using a Virtual Reality Application. Aging, Neuropsychology, and Cognition 2013, 20, 298–319. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Murphy, K.; Andrews, G. Immediate and Long-Term Efficacy of Executive Functions Cognitive Training in Older Adults: A Systematic Review and Meta-Analysis. Psychological bulletin 2019, 145, 698. [Google Scholar] [CrossRef] [PubMed]
- Marusic, U.; Giordani, B.; Moffat, S.D.; Petrič, M.; Dolenc, P.; Pišot, R.; Kavcic, V. Computerized Cognitive Training during Physical Inactivity Improves Executive Functioning in Older Adults. Aging, Neuropsychology, and Cognition 2016, 25, 49–69. [Google Scholar] [CrossRef] [PubMed]
- Nedeljko, M.; Gu, Y.; Bostan, C.M. The Dual Impact of Technological Tools on Health and Technostress among Older Workers: An Integrative Literature Review. Cognition, Technology & Work 2024, 26, 47–61. [Google Scholar]
- Kang, S.Y.; Lee, C.M. Effects of a Cognitive Improvement Program on Cognition, Activities of Daily Living (ADL), Depression, Life Satisfaction, and Grasping Power in Small Groups. Journal of muscle and joint health 2016, 23, 169–178. [Google Scholar] [CrossRef]
- Gordon, E.; Palmer, D.M.; Liu, H.; Rekshan, W.; DeVarney, S. Online Cognitive Brain Training Associated with Measurable Improvements in Cognition and Emotional Well-Being. Technology & Innovation 2013, 15, 53–62. [Google Scholar]
- Sheng, C.; Yang, K.; Wang, X.; Li, H.; Li, T.; Lin, L.; Liu, Y.; Yang, Q.; Wang, X.; Wang, X. Advances in Non-Pharmacological Interventions for Subjective Cognitive Decline: A Systematic Review and Meta-Analysis. Journal of Alzheimer’s Disease 2020, 77, 903–920. [Google Scholar] [CrossRef] [PubMed]
- Boyle, E.A.; Hainey, T.; Connolly, T.M.; Gray, G.; Earp, J.; Ott, M.; Lim, T.; Ninaus, M.; Ribeiro, C.; Pereira, J. An Update to the Systematic Literature Review of Empirical Evidence of the Impacts and Outcomes of Computer Games and Serious Games. Computers & Education 2016, 94, 178–192. [Google Scholar]
- Lumsden, J.; Edwards, E.A.; Lawrence, N.S.; Coyle, D.; Munafò, M.R. Gamification of Cognitive Assessment and Cognitive Training: A Systematic Review of Applications and Efficacy. JMIR serious games 2016, 4, e5888. [Google Scholar] [CrossRef]
- Pallavicini, F.; Ferrari, A.; Mantovani, F. Video Games for Well-Being: A Systematic Review on the Application of Computer Games for Cognitive and Emotional Training in the Adult Population. Frontiers in psychology 2018, 9, 407892. [Google Scholar] [CrossRef]
- Sakuraya, A.; Imamura, K.; Watanabe, K.; Asai, Y.; Ando, E.; Eguchi, H.; Nishida, N.; Kobayashi, Y.; Arima, H.; Iwanaga, M. Corrigendum: What Kind of Intervention Is Effective for Improving Subjective Well-Being among Workers? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in Psychology 2023, 14, 1236746. [Google Scholar] [CrossRef]
- Jean, L.; Bergeron, M.-È.; Thivierge, S.; Simard, M. Cognitive Intervention Programs for Individuals With Mild Cognitive Impairment: Systematic Review of the Literature. The American Journal of Geriatric Psychiatry 2010, 18, 281–296. [Google Scholar] [CrossRef]
- Gajewski, P.D.; Stahn, C.; Zülch, J.; Wascher, E.; Getzmann, S.; Falkenstein, M. Effects of Cognitive and Stress Management Training in Middle-Aged and Older Industrial Workers in Different Socioeconomic Settings: A Randomized Controlled Study. Front. Psychol. 2023, 14, 1229503. [Google Scholar] [CrossRef]
Figure 1.
Study flow diagram.
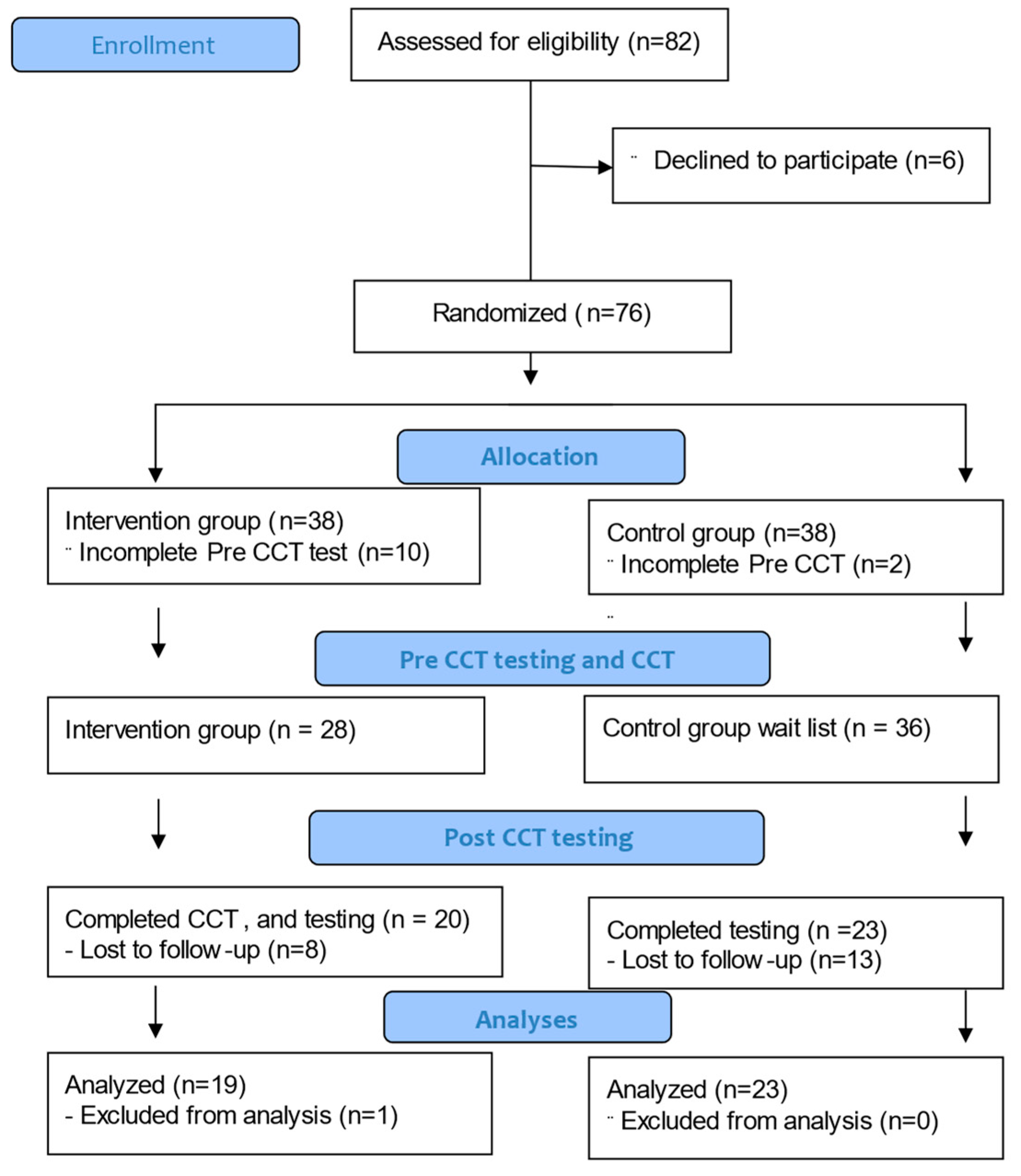
Figure 2.
illustrates an intersection within the computer-based spatial navigation application for CCT. At this juncture, participants must decide which direction to take – left, straight, or right – within a virtual maze offering three available paths.
Figure 2.
illustrates an intersection within the computer-based spatial navigation application for CCT. At this juncture, participants must decide which direction to take – left, straight, or right – within a virtual maze offering three available paths.
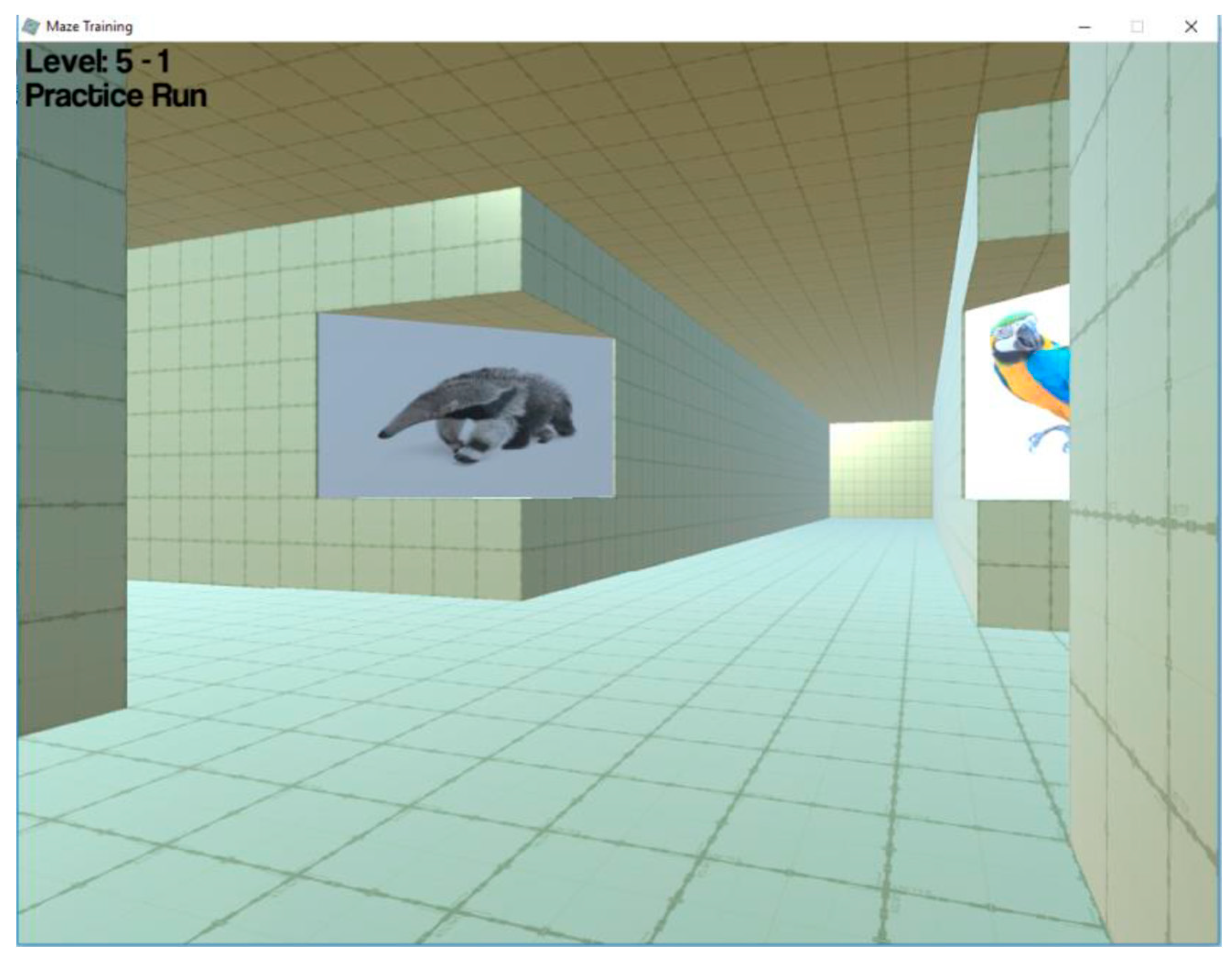
Figure 3.
The average scores on the Verbal Fluency Letter test for participants in the Intervention group (blue color) and Control group (red color) for pre and post CCT (error bars represent standard error of the mean).
Figure 3.
The average scores on the Verbal Fluency Letter test for participants in the Intervention group (blue color) and Control group (red color) for pre and post CCT (error bars represent standard error of the mean).
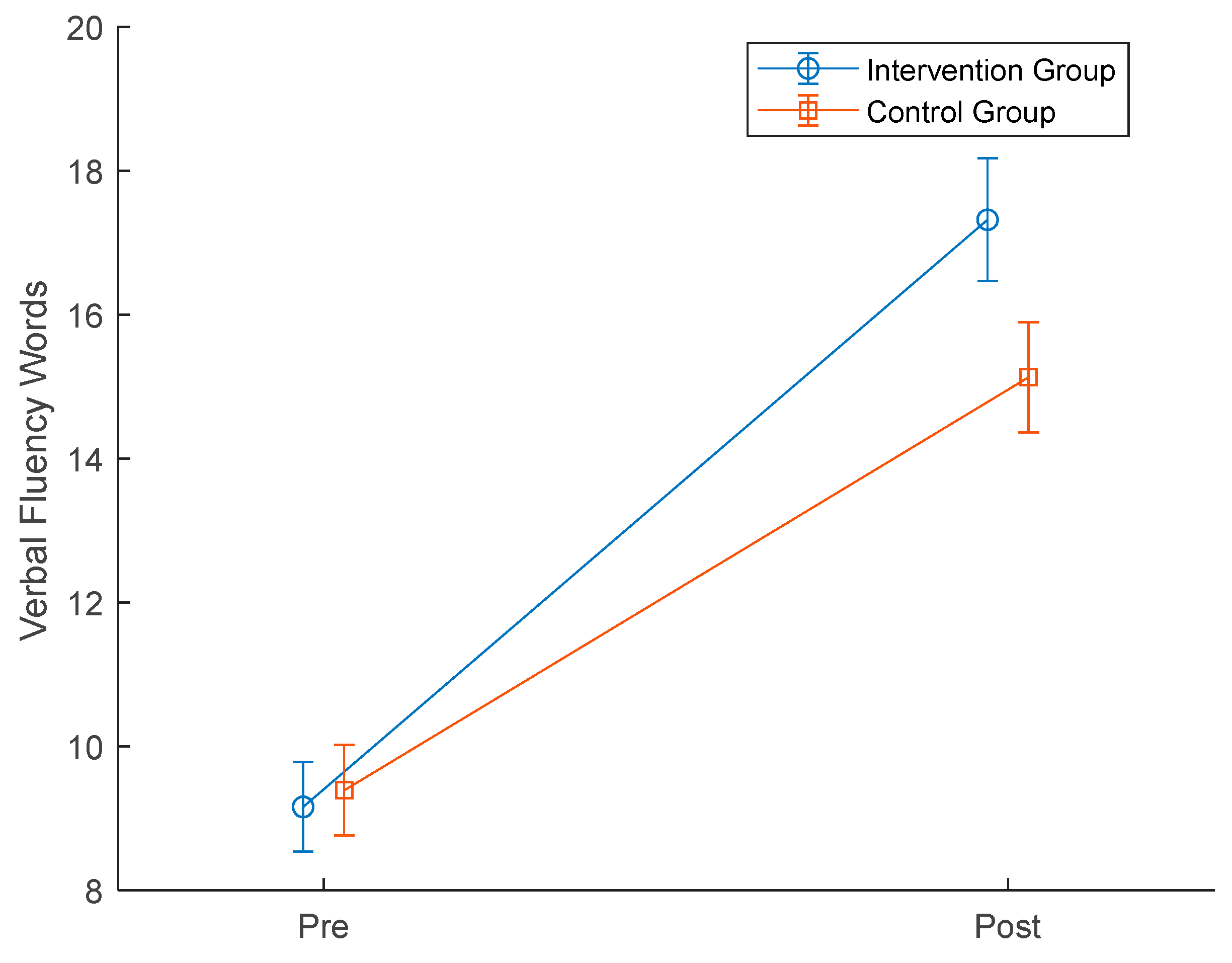
Figure 4.
Line graph of the average productivity for participants in the Intervention group (blue color) and Control group (red color) for pre and post CCT (error bars represent standard error of the mean).
Figure 4.
Line graph of the average productivity for participants in the Intervention group (blue color) and Control group (red color) for pre and post CCT (error bars represent standard error of the mean).
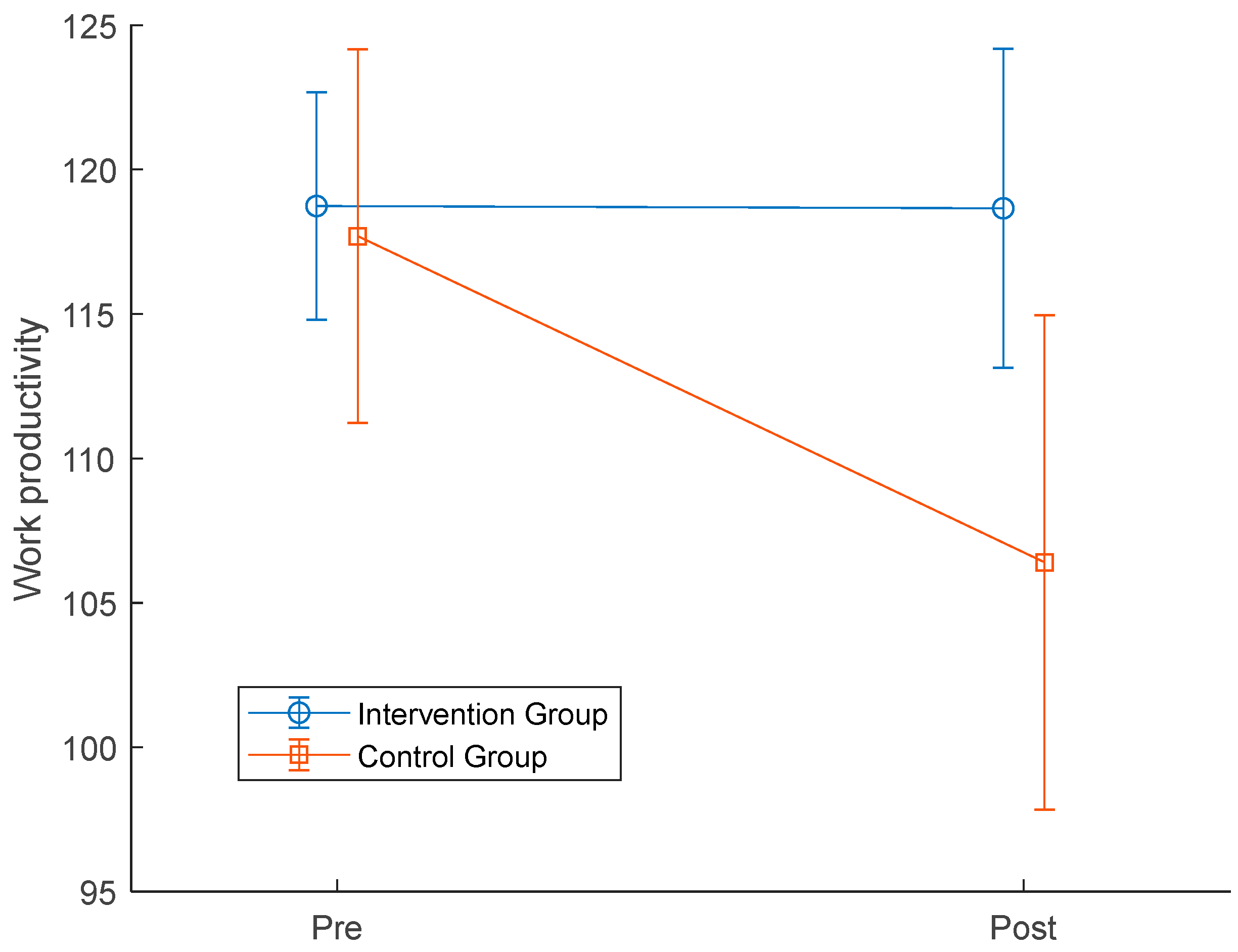
Figure 5.
Scatter plot for the self-evaluated cognitive change scores and health status for the Control group.
Figure 5.
Scatter plot for the self-evaluated cognitive change scores and health status for the Control group.
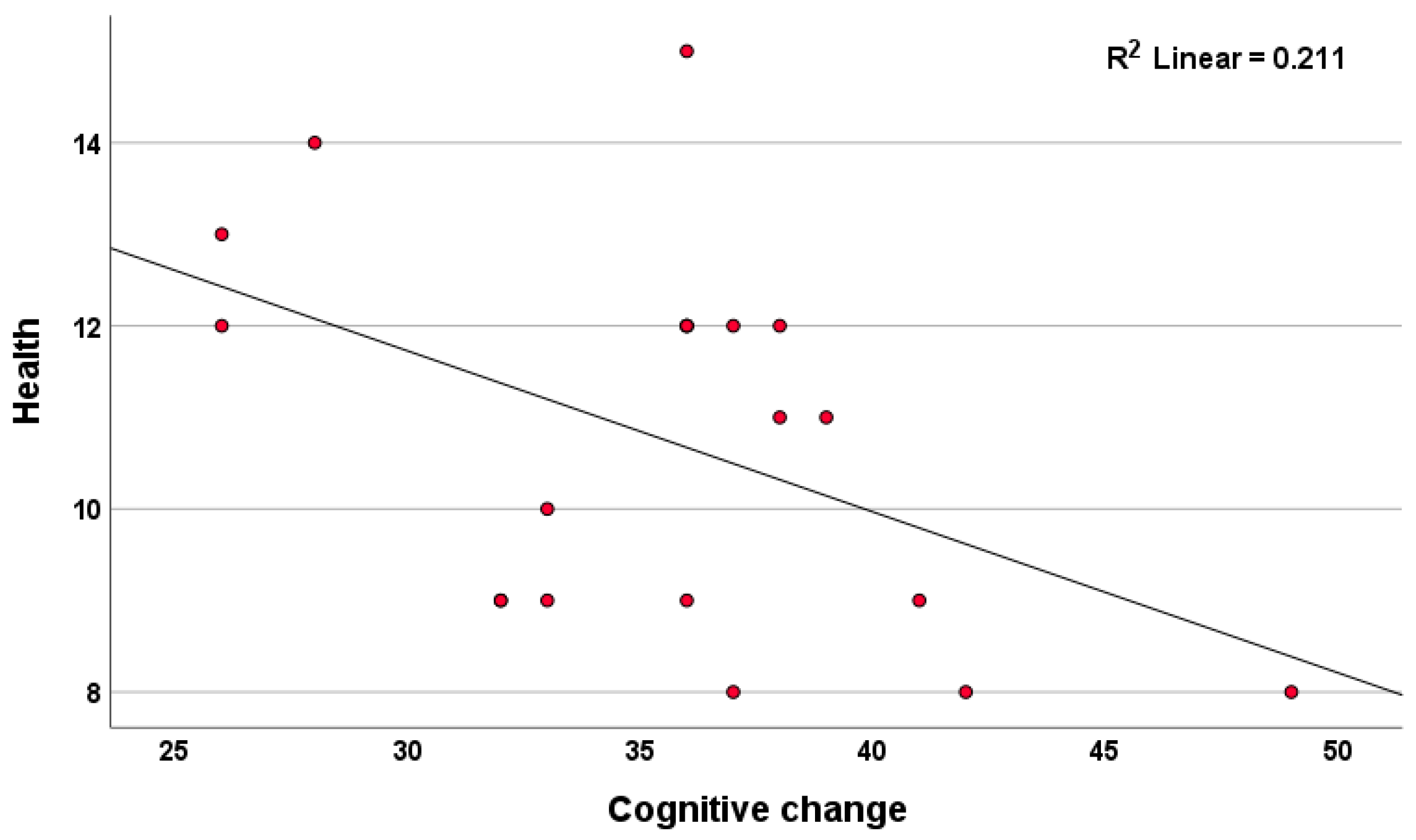

Table 1.
Demographic data for Intervention and Control group.
| Intervention group (n =19) | Control Group (n=23) | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p /value | |
| Age | 54.55 | 3.19 | 55.72 | 3.94 | 0.31 |
| Gender | F 20, M 0 | F 32, M 4 | |||
| Education (years) | 15.11 | 0.94 | 15.39 | 1.41 | 0.45 |
Table 2.
Means (M) and standard deviations (SD) of the neuropsychological test of the Intervention and Control group for pre and post CCT.
Table 2.
Means (M) and standard deviations (SD) of the neuropsychological test of the Intervention and Control group for pre and post CCT.
| Test | Pre-CCT | Post-CCT | RM ANOVA | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Time | Group | Interaction (time x group) | |||||||
| M | SD | M | SD | P value | P values | F value | P value | Partial η2 | |
| VF - L | <.001 | 0.24 | 4.387 | 0.04 | 0.099 | ||||
| Intervention | 9.16 | 2.79 | 17.32 | 3.82 | |||||
| Control | 9.39 | 2.81 | 15.13 | 3.43 | |||||
| VF - S | 0.06 | 0.14 | 2.31 | 0.14 | 0.061 | ||||
| Intervention | 20.00 | 6.71 | 19.72 | 6.61 | |||||
| Control | 22.45 | 4.27 | 20.03 | 5.35 | |||||
| Digit Span Forward | 0.44 | 0.91 | 0.98 | 0.33 | 0.024 | ||||
| Intervention | 6.32 | 1.06 | 6.37 | 1.01 | |||||
| Control | 6.52 | 1.28 | 6.21 | 1.68 | |||||
| Digit Span Backward | 0.06 | 0.61 | 0.223 | 0.63 | 0.006 | ||||
| Intervention | 5.84 | 1.17 | 6.16 | 1.54 | |||||
| Control | 5.52 | 1.56 | 6.04 | 1.65 | |||||
| AVLT Learning | 0.33 | 0.24 | 0.15 | 0.70 | 0.004 | ||||
| Intervention | 10.35 | 1.37 | 10.23 | 1.06 | |||||
| Control | 9.95 | 1.56 | 9.68 | 1.57 | |||||
| AVLT-IR | 0.27 | 0.23 | 1.49 | 0.23 | 0.037 | ||||
| Intervention | 9.11 | 3.09 | 9.05 | 1.93 | |||||
| Control | 7.68 | 3.76 | 8.82 | 3.02 | |||||
| AVLT-DR | 0.02 | 0.35 | 0.91 | 0.35 | 0.023 | ||||
| Intervention | 8.58 | 2.17 | 9.79 | 1.62 | |||||
| Control | 9.23 | 2.69 | 9.77 | 2.62 | |||||
| Coding | 0.02 | 0.60 | 0.05 | 0.83 | 0.001 | ||||
| Intervention | 51.11 | 8.31 | 54.05 | 9.07 | |||||
| Control | 52.43 | 11.89 | 55.96 | 12.67 | |||||
| Comparison | 0.08 | 0.12 | 0.28 | 0.12 | 0.007 | ||||
| Intervention | 20.37 | 3.37 | 20.26 | 3.56 | |||||
| Control | 20.09 | 4.24 | 18.32 | 2.55 | |||||
*Notes: Primary outcome measures were the number of correct responses for all tests. (VF – L: Verbal Fluency Letter, VF – S: Verbal Fluency Semantic, AVLT - IR: Auditory Verbal Learning Test-Immediate Recall, AVLT - DR: Auditory Verbal Learning Test-Delayed Recall).
Table 3.
Means (M) and standard deviations (SD) of the productivity and well-being questionnaires of the Intervention and Control group for pre and post CCT.
Table 3.
Means (M) and standard deviations (SD) of the productivity and well-being questionnaires of the Intervention and Control group for pre and post CCT.
| Questionnaire | Pre-CCT | Post-CCT | RM ANOVA | Partial η2 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Time | Group | Interaction | |||||||
| M | SD | M | SD | p value | p values | p value | p value | ||
| Work productivity | 0.086 | 0.433 | 3.015 | 0.09 | 0.070 | ||||
| Intervention | 118.74 | 17.62 | 118.66 | 24.75 | |||||
| Control | 117.70 | 28.91 | 106.40 | 38.31 | |||||
| Life Satisfaction | 00.28 | 0.89 | 0.43 | 0.52 | 0.011 | ||||
| Intervention | 21.17 | 4.23 | 22.44 | 4.93 | |||||
| Control | 21.86 | 5.77 | 22.18 | 5.56 | |||||
| Wellbeing | 0.73 | 0.48 | 1.34 | 0.26 | 0.034 | ||||
| Intervention | 14.33 | 4.72 | 15.00 | 4.50 | |||||
| Control | 14.23 | 5.51 | 13.00 | 6.06 | |||||
| Job satisfaction | 0.74 | 0.03 | 0.46 | 0.50 | 0.014 | ||||
| Intervention | 37.00 | 9.83 | 38.22 | 8.85 | |||||
| Control | 44.12 | 9.84 | 43.71 | 6.85 | |||||
| Health | 0.95 | 0.33 | 0.57 | 0.46 | 0.015 | ||||
| Intervention | 11.11 | 1.37 | 12.37 | 4.07 | |||||
| Control | 11.45 | 3.88 | 10.41 | 3.13 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



