Submitted:
15 June 2024
Posted:
17 June 2024
You are already at the latest version
Abstract
This survey of research literature is an overview of the current state of science addressing DSM-5 diagnostic criteria as it relates to identifying Autism Spectrum Disorder (ASD) in young children. Selected sources are of high quality and have been published since 2020 in peer-reviewed journals relevant to children’s health. The narrative is organized from the earliest to the most recent publications and is divided into sections around categories and themes that highlight the main arguments, findings, and controversies identified by researchers. There are indications in the literature that while ASD can be identified and differentiated from other developmental disorders in young children, doing so requires that clinicians who have relied on the DSM-5 should also use multiple measures, including other formalized screening tools as assessments that gather observational input from parents and caregivers, as well as findings from physical examinations, laboratory investigations, and magnetic resonance imagining (MRI). This high level of corroboration points to an emerging diagnosis paradigm through which transdiagnostic approaches to early diagnosis and intervention may exist.
Keywords:
autism spectrum disorder
; young children
; DSM-5
; neurodiversity
; transdiagnosis
1. Introduction
There are few life circumstances that cause parents more concern and stress than the realization that an infant’s developmental processes are uncharacteristic of that of a typically developing infant. Major questions arise when a young child in the early months of life experiences difficulties in basic human functioning such as feeding and digestion, sleeping, senses, reflexes, language development, and acquisition of specific communication and social skills. Over time, when questions are unanswered by healthcare and medical providers and the child’s needs escalate, everyday life, despite best efforts, quickly becomes intolerable for the child and overwhelming and intense for parents and caregivers. As indicated in studies, a lack of specialized information results in tremendous uncertainty for families and caregivers and presents a public health crisis involving loss of quality of life and economic struggles associated with caring for a child at risk of various forms of neurodiversity [1-4]. This situation is particularly applicable to the many families and caregivers of a child with Autism Spectrum Disorder (ASD).
Defined by the Diagnostic and Statistical Manual of Mental Disorders [5], ASD is a complex neurodevelopmental disorder beginning in early childhood through the lifespan. It is characterized by impairments in language development and communication, problem-solving, and social skills. Restrictive repetitive behaviors and learning difficulties are common in ASD. According to the US Centers for Disease Control (CDC) and Prevention [6], in 2020, about 1 in 36 children aged 8 years (approximately 4% of boys and 1% of girls) were reported to have ASD according to estimates from the CDC’s Autism and Developmental Disabilities Monitoring (ADDM) Network. According to McCarty and Frye [7], “[t]he only proven therapy for core symptoms of ASD is behavioral therapy, particularly if it is started early in life” (p. 1), and long-term outcomes for the child are more likely the earlier the intervention. They further indicate that “the mean age of obtaining a diagnosis of ASD is 4 years 3 months and has not improved significantly over the 2 past decades to educate the public and health professionals” (p. 2).
An ASD (APA, DSM-5, 2013) diagnosis, which first appeared as the Pervasive Developmental Disorder class of conditions in the DSM-3 [8], has been useful for some individuals who begin life experiencing neurodevelopmental difficulties. In the US, the DSM-5 is the ultimate diagnostic reference with target symptoms for ASD. However, the DSM-5 does not provide a formal test for ASD. DSM-5 criteria provide a framework for a medical diagnosis of ASD. DSM results are used to legitimize education, medical, and social systems support and outcomes, with the lifetime social costs in the US estimated to be more than $7 trillion, which is predicted to increase to $11.5 trillion by 2029 if prevalence remains the same [9].
Without addressing ASD specifically and while identifying major challenges for transdiagnostic science, Dalgeish et al. [10] raised major concerns that traditional forms of diagnosis, such as diagnosis based on the DSM-5 that have in the past served to define and govern interventions and services, should be changed or given up in lieu of new approaches to conceptualizing, understanding onset, and responding to mental health conditions including conditions and concerns related to how the brain works. They argue against traditional psychiatric diagnosis in favor of a “transdiagnostic” (para. 1) approach to the diagnosis of ASD, new classification of mental health problems, and new approaches to addressing early difficulties in human functioning and acceptance of neurodiversity as an accepted way of life.
The current state of science about the DSM-5 diagnostic criteria for ASD and the future of proposed diagnostic innovations should be of high importance to parents, clinicians, and other stakeholders due to the widespread sociopolitical and pragmatic impact diagnostic tools have on children, their families and/or caregivers, and society as a whole. When considering that distinct psychiatric diagnoses may not clearly align with the complex configurations of human experience that manifest as ASD, it is prudent to also consider a biomedical model central to the current accepted diagnostic approach. Additionally, the confusion and anxiety experienced by parents and caregivers resulting in a frequent wait-and-see approach to diagnosis, putting diagnosis off indefinitely until the disorder is well established, may delay much-needed responses toward improving daily and lifespan quality of life.
2. Materials and Methods
The Dalgleish et al. [10] research and suggestions in favor of transdiagnosis are a starting point for this literature review. They suggest that new “transdiagnostic approaches may have the potential to represent better the clinical and scientific reality of mental health problems” (para. 1), improving how researchers and medical practitioners think in various ways about the extremes of the human condition. Focused across the intellectual domains of classification and nosology, basic biopsychosocial research, and clinical science, they address transdiagnostic as a complicated and complex departure from traditional diagnosis that will cut across traditional diagnostic boundaries, present new classifications for mental health problems and new approaches to management of various forms of diversity. A major shift to transdiagnosis raises a critical question addressed in this literature review: What is the state of science about DSM-5 criteria and early diagnosis of ASD? What are the implications of findings in current research for a proposed transdiagnostic approach to diagnosis and the steps to positively manage neurodiverse lives?
A search was conducted in MEDLINE, PsycINFO, and Psychology and Behavioral Sciences Collection (EBSCO) to identify studies examining the consequences of applying the most current impairment criterion of DSM-5 [5] to infants and young children. The keywords “ASD” and “DSM-5” were used in conjunction with control terms “toddlers,” “preschoolers,” “and “early childhood” to conduct comprehensive searches in the three databases. Following pre-DSM-5 publication predictions, the search focused on articles published between 2020 and 2023 to capture the most recent research and developments in the field, ensuring the findings reflect the latest evidence and practices. The initial search yielded a total of 41 articles. After removing duplicates and screening for relevance based on titles and abstracts, the final dataset comprised 15 articles (Table 1). Among these, five articles were published in 2020, five in 2021, one in 2022, and four in 2023.
To further categorize and analyze the selected articles, the Scimago Journal & Country Rank (ScimagoJR) website was used to identify the subject areas of the journals in which the articles were published. ScimagoJR provides comprehensive information on the scope and impact of scientific journals, allowing researchers to determine the primary disciplines associated with each publication accurately [11]. Classifying the journals into their respective subject areas can contextualize the findings within specific fields such as neurology, psychiatry, and psychology. The categorization facilitated a more nuanced understanding of the focus and implications of the studies, helping to highlight the interdisciplinary nature of research on ASD diagnosis in young children and the possibility of transdiagnosis. Selected sources by global populations demonstrate rigor in methodology, including sample size, data collection, and analysis. We organized studies into two groups, beginning with background studies predicting the use of the new DSM-5 ASD criteria and a carefully selected collection of post-publication DSM-5 studies from the four most current years (2020, 2021, 2022, and 2023) that are representatives of science at this time. A narrative review of selected studies includes the type of setting, population, design, measures, and broad findings and conclusions that highlight key points, main arguments, and controversies in publications.
3. Results
Among the selected 15 articles, one is a handbook chapter published by the American Psychology Association, and the remaining 14 are academic journal articles published across 11 different journals. Notably, "Autism" and "Frontiers in Psychiatry" each contributed two articles (Table 2). The journals primarily focus on developmental and educational psychology, psychiatry and mental health, and neurology. "Seminars in Pediatric Neurology," "Autism Research," and the "Journal of the American Academy of Child & Adolescent Psychiatry" cover more specialized areas, while "Pediatrics," "Children," and "Cureus" address broader fields like pediatrics and medicine.
In the DSM-5, ASD is considered a mental health problem and has therefore been addressed through the lens of the psychiatric diagnostic paradigm, likely influenced by general medicine and beliefs about states of health and causes of physical illnesses and diseases. The DSM-5 presents a diagnostic taxonomy useful for communication across stakeholder groups and facilitating clinical assessments and interventions. ASD symptoms are considered present or absent. Young children may appear to have symptoms that satisfy more than one developmental disorder, and children with the same diagnosis can have different symptoms. The DSM-5 criteria raises questions about symptoms that are common in typically developed young children, such as a strong desire for sameness in everyday life routines and fixed interests such as specific activities, objects, or subjects. ASD symptoms can change across developmental levels and the life span. These challenges are evidenced in the following studies that are presented as examples of research addressing diagnostic criteria.
3.1. Pre-Publication Investigations of DSM-5 Symptom Categories
3.1.1. Fewer Toddlers Diagnosed with DSM-5
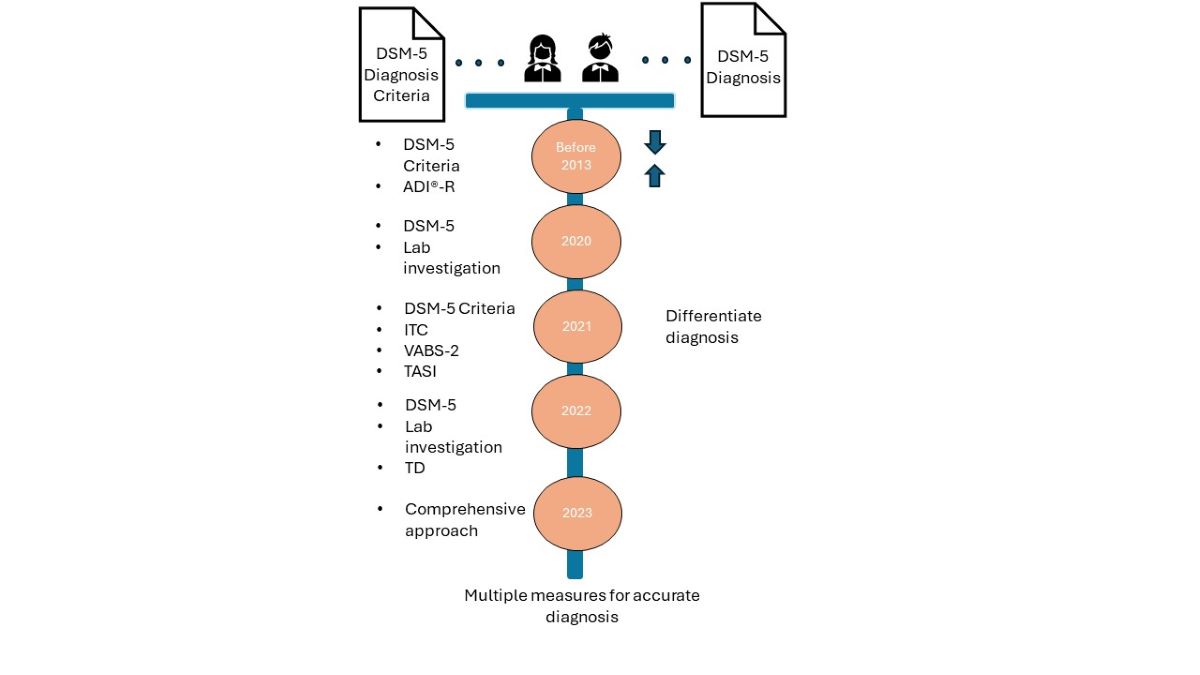
Even before the 2013 publication, there were controversies, concerns, and researchers’ questions about the appropriateness of the DSM-5 criteria relevant to toddlers at risk of developmental disorders [12]. For example, Matson et al. (2012) found in a large study of toddlers (n=2,721) that fewer toddlers where diagnosed with ASD when DSM-5 criteria were applied. They projected that the DSM-5 would result in far fewer persons being diagnosed and qualifying for needed autism services. Extending findings of previous studies, Barton et al. [13] investigated sensitivity and specificity of proposed DSM-5 criteria for ASD in toddlers who were believed to be vulnerable in the proposed DSM-5 when compared to the DSM-IV-TR in terms of stringent requirements of impairment in all three social-communication symptoms and two restricted/repetitive symptoms. Their sample from the coastal, eastern US was 422 toddlers ranging in age from 16.79 – 39.36 months who had screened positive on the Modified Checklist for Autism in Toddlers-Revised. The Autism Diagnostic Interview®-Revised (ADI®-R), the Autism Diagnostic Observation Schedule (ADOS), and DSM-5 evaluations were administered and data analyzed using SPSS 18.0. Receiver operating characteristic curves were generated using the sum of the ADI-R and ADOS threshold items contributing to each DSM-5 criterion. More participants with ASD were identified than in earlier studies in relatively high sensitivity and low specificity.
According to these researchers, “[s]ymptom presentation in young children is often less clear as symptoms may still be emerging when children are referred for early evaluations. Toddlers’ behavior may also be more affected by situational variables, and their parents may have less experience than the parents of older children with developmental processes and age-related expectations” (p. 1190). It was noted that “about half of the children who did not have ASD were also identified using these cutoffs, suggesting that a mild endorsement of one aspect of a DSM-5 criterion may not meet the threshold for clinically significant impairment characteristics of autism” (p. 1190). The researchers concluded that the proposed DSM-5 criteria should be modified because it may be too stringent for children younger than 3 years old.
3.2. Post-Publication of DSM-5 Diagnoses of ASD
3.2.1. 2020 Screening Procedures Including the DSM-5 Standard
In recognition of the importance of early therapeutic interventions, the American Academy of Pediatrics recommends universal screening by pediatricians for ASD in infants 18 to 24 months using a variety of screening tools. To address the limitations of universal screening and the high rate of 1 in 3 children initially identified by screening tools for toddlers, McCarty and Frye [7] developed training for pediatricians to improve their use of screening tools toward the goal of reducing the number of toddlers without an ASD diagnosis referred for further evaluation and to decrease the time between parental concerns and time of diagnosis and care of children with ASD. In 2019, they examined the use of screening procedures, including the DSM-5 criterion, which is always documented when making a diagnosis at The Early Access for Care, Arizona Project at Phoenix Children’s Hospital, which began in 2015. They found several areas to improve efficiency and effectiveness, including unnecessary procedures that could result in wasted resources. For example, they discovered that the length of the Screening for Autism in Toddler and Young Children instrument designed for use in the physician’s office may explain why screening was not universally implemented, and further that primary care physicians were not comfortable and did not document functional limitations found in children, which is necessary for confirmation of ASD and obtaining services offered by the Arizona State Department of Developmental Disabilities. With the priority for identifying children early to initiate treatment, these researchers emphasized that diagnosis includes efficient use of primary and secondary behavioral screening tools in combination with careful placement of five categories of biomarkers (prenatal, presymptomatic, diagnostic, subgrouping, and treatment) in the diagnostic process (not in isolation) to stratify risk, diagnose, and assist with ethological classification and treatment.
3.2.2. 2021 ASD Diagnosis Based of DSM-5 and Screening Tools
In consideration of significant ASD symptoms to necessitate the ASD diagnosis, Coulter et al. [14] addressed concerns about diagnosis using the DSM-5 given the occurrence of early atypical behaviors such as language delays, social communications deficits, and restricted and repetitive behaviors (RRB) in young children not only presenting in ASD but also in children with other developmental disorders. They point out that there is agreement in the literature that social and sensory differences typically appear during the second year of life and that differentiating ASD from other developmental disorders is more difficult in children younger than 24 months. Consequently, they designed a study of toddlers initially screened during a pediatric visit using the Infant-Toddler Checklist (ITC) by Wetherby and Prizant [15]. Toddlers who raised ASD concerns were evaluated using the DSM-5 and other measures of cognitive abilities (Mullen Scales of Early Learning) by Mullen [16]; adaptive behaviors in communication, socialization, daily living, and motor skills (Vineland Adaptive Behavior Scales-2 (VABS-2) by Sparrow, Cicchetti, and Balla (2005); play-based activities that show social affect and restricted and repetitive behaviors, and caregiver-report of ASD symptoms (Toddler Autism Symptom Inventory (TASI) by Coulter et al. [14]. Using all available data, the toddler participants (n=294) were assigned to one of three diagnostic groups with a mean age of 21 months higher in the ASD group: ASD (71), other Developmental Disorder (131), and Typical Development/No Diagnosis (91). Following a lengthy discussion of results indicating differences among diagnostic groups, it was pointed out that caregivers of children 12-36 months recognize and report more social communication symptoms and repetitive behaviors when compared to children in developmental disorders or typical development/no diagnosis groups. The DSM-5 symptoms most recognized in the ASD group and found to be the most effective at discriminating among diagnostic groups were stereotyped/repetitive motor movements, object use, and speech, deficits in relationships, deficits in social-emotional reciprocity, and restricted fixed interests. This contradicts earlier studies [13, 17] suggesting that RRBs may not be apparent until later in childhood. A key conclusion positively supporting the use of the DSM-5 is that the TASI is useful through organizing operationalized toddler behaviors into DSM-5 symptom categories so that clinicians can determine symptoms that are not presented based on caregiver reports and can differentiate among diagnoses.
3.2.3. 2022 ASD Diagnosis Advanced on the Basis of Biomarker
A promising biomarker for a new perspective in addition to the clinical behavioral diagnosis of ASD was discovered by Khan et al. [18] in urine samples of 85 subjects in a case-control study in the Department of Pathology and Laboratory Medicine in collaboration with the Department of Pediatrics and Child Health, Aga Khan University, Pakistan. ASD subjects (n=65) were diagnosed by a pediatric neurologist based on DSM-5 criteria and typically developing (TD) healthy controls from August 2019 to June 2021. Discriminant analysis showed that 3-hydroxyisovalericc, homovanillic acid, adipic acid, suberic acid, and indole acetic were significantly different between ASD and TD groups.
3.2.4. 2023 ASD Diagnosis Requires Behavior, Neurological, and Biological Measures
A comprehensive global review of early childhood ASD by Alrehaili et al. [19] indicates that ASD is a cluster of developmental disabilities that align with the diagnostic criteria in the DSM-5. They acknowledge studies that have demonstrated that ASD “can be identified at or below 18 months of age, with a more accurate evaluation possible by age 2” (p. 6). Without discussion of the merits of DSM-5 diagnostic criteria in diagnosing ASD, they assert that diagnosis of ASD in early childhood laying a roadmap for treatment requires a comprehensive, systematic, and structured approach through “behavioral observations, clinical presentations, or various imaging techniques such as functional MRI and diffusion imaging” [19] (p. 1), and they stated that the objective of ASD evaluation is to determine effective care for the child in the context of the family. These researchers further state that evaluation should go beyond behavioral assessments to identify signs of illness, self-harm, potential ill-treatment, and evaluation for ASD should include “neurological assessment, dysmorphism regulation, scrutiny for neurocutaneous stigma, and Woods light (ultraviolet light) examination” [19] (p. 1). They conclude that screening tools such as the Communication and Symbolic Behavior Scales; the Infant-Toddler Checklist; Ages and Stages Questionnaires; Modified Checklist for Autism in Toddlers; and the Parents’ Evaluation of Developmental Status have only “a pilot role in the early detection of ASD” [19] (p. 7), and ASD diagnosis should include lab investigations of potential biomarkers such as elevated whole-blood serotonin, melatonin deficits, identification of small-molecule peptides, proteins/peptides in cerebrospinal fluid, and expression of apolipoproteins in serum, and neuroimaging revealing insights about neuroanatomical structures and emotional processing.
4. Discussion
During the past two decades, studies, particularly in recent years, have progressively become more specific about the ineffectiveness of diagnostic criteria for ASD in the DSM-5 and more detailed as to what behavioral screening tools and laboratory tests should be included in the diagnostic process for young children. This is particularly momentous given that for approximately 40 years, the Diagnostic and Statistical Manual of Mental Disorders published by the American Psychological Association has been the goal standard in the US and other regions of the world for the diagnosis of what is known today as ASD.
Widely recognized databases for the dissemination of peer-reviewed publications searched in this review of scientific studies reveal documented, long-standing concerns about DSM-5 criteria for ASD. This documentation indicates deeply held concerns and repeated, significant efforts to justify DSM-5 diagnostic criteria in identifying young children with ASD. DSM-5 validation efforts involved the use of various screening tools wherein gathered observation and interview data are statistically evaluated for alignment with DSM-5 criteria. The greater the degree of alignment found in the study, the stronger a case for believability may be made for significance in determining an ASD diagnosis. In contrast, there are strong indications that the use of behavior assessments such as the DSM-5 and a variety of other screening tools are insufficient without lab investigations of potential biomarkers as measurable indicators, or tests, of biological states or conditions in ASD when compared to typically developing populations.
Recent studies addressing DSM-5 diagnostic criteria have in common that they focus on practices of using various screening tools in combination with the DSM-5, which alone is frequently insufficient in diagnosing young children. Albeit a quest to improve quality of life, researchers’ determination to develop and use screening tools designed to gather observation data by clinicians and from families and caregivers and biomedical data may be in part motivated by several factors identified in the present literature review. First, the suspected prevalence of ASD is increasing at a staggering rate each year. There is wide agreement that in young children, ASD can be differentiated from other developmental disabilities, and behavioral interventions are most effective early in the life of a child. There are life-long, high personal and societal financial costs directly associated with ASD. Despite the compelling recommendation by the American Academy of Pediatrics that children be screened for ASD during regular well-child doctor visits at 18 and 24 months, and despite organized educational efforts to improve universal screening by PDPs, there is evidence that many PCPs in the US are reluctant to do screening and/or to document limitation. With early identification of ASD as an integral function of the primary care medical home and the responsibility of pediatric healthcare providers, there appears to be a huge gap – a crisis situation – in identifying and diagnosing young children who present symptoms of ASD, potentially leaving many young children and families without frontline assistance and care.
Given the unintended yet complicated and complex state of science dominated by DSM-5 diagnostic criteria for ASD and the many young children experiencing distress in need of specialized care, a paradigm shift in the current state of science is needed that has the potential to reveal interpretations of neurologically diverse development and supports beginning in early childhood. Rather than dispense with the current diagnostic system altogether, it appears logical to adopt what Dalgleish et al. [10] describe as a “soft transdiagnostic” (p. 182) approach, keeping the “underlying diagnostic classification while seeking to elucidate processes or develop interventions that have relevance to one or more of the diagnoses as traditionally formulated” (p. 182). But first, there must be the desire to adopt a different set of meta-theoretical assumptions about science that address ASD not as a mental health condition but as research topics focused on ASD as a lifelong neurodevelopmental condition.
In keeping with Kuhn’s [20] notion of revolutionary science, for researchers and theorists to switch paradigms calls for a change, which is possible but not often achieved in practice. Burrell and Morgan [21] offer four paradigms for understanding the nature of science and society “in the hope that knowledge of the competing points of view will at least make us aware of the boundaries within which we approach our subject” (p. 25). Table 1 highlights two of Burrell and Morgan’s [21] four conceptualizations of social science paradigms with brief descriptions of each. This table describes the nature of each paradigm and shows clear boundaries between two paradigms that are relevant to the current state of science about ASD, wherein the functionalist paradigm is dominant and the interpretivist paradigm appears to be emerging. Each paradigm, or lens through which ASD is viewed, has its own accepted theory, assumptions, models, practices, and tools.
The functionalist paradigm has provided the dominant framework for the conduct of academic psychology and the study of the mind and behavior. The interpretivist paradigm is concerned with understanding the social construction of reality, the way people create and share meanings. Awareness of the boundaries of these two social science paradigms can provide some sign posts in a roadmap for conversations about a shift in the science of ASD to the transdiagnosis paradigm and guide an accelerated shift to more accepted theories, assumptions, models, practices, and tools useful in the diagnosis of ASD in the earliest stages of life and through the life span.

Table 3.
Characteristics of Paradigms of Social Science Thought to Identify and Guide Distinct Intellectual Traditions.
Table 3.
Characteristics of Paradigms of Social Science Thought to Identify and Guide Distinct Intellectual Traditions.
| Dominate Paradigm - Diagnostic Paradigm for ASD The Functionalist Paradigm [21] |
New Paradigm - Transdiagnosis Paradigm for ASD The Interpretivist Paradigm [21] |
|---|---|
|
|
The literature on early diagnosis of ASD has been published over the past four years in fields such as developmental and educational psychology, psychiatry, and neurology, demonstrating the diversity and interdisciplinary nature of research on ASD and the need for input from different scientific disciplines. However, the limited disciplines may also indicate the inadequacy of transdiagnostic approaches. While studies have demonstrated the potential of biomarkers for diagnosing ASD [18], more extensive efforts, such as promoting collaboration between researchers from various disciplines to create a more comprehensive understanding of ASD, are necessary to fully recognize and implement the benefits of biomarker-based diagnosis in clinical practice and to scale up transdiagnosis. Expanding research in this area may lead to more precise diagnoses, enabling personalized interventions and improving treatment outcomes for individuals with ASD [1, 3].
5. Future Study and Conclusions
Future research must acknowledge, uphold, and build on the many recent contributions of science to understanding ASD, as well as the existing high standards and expectations for the diagnosis of young children with ASD. Fortunately, licensed psychiatrists and physicians are accountable through their formal education and oath, pledging to act for the patient's good [22]. Because of the nature of their job and their moral and ethical responsibilities, making a diagnosis of ASD is high stakes for them, as well as for a young child and their parents and caregivers. Without a medical diagnosis communicating a young child’s strengths and challenges and informing interventions, necessary community support is frequently out of reach. Without minimizing professional responsibilities or progress in today’s society, a transdiagnosis approach to the diagnosis of ASD has the potential to widen the functionalist lens, enabling an interpretivist focus by researchers beyond the current occupation with DSM-5 criteria, allowing future research questions such as: What are individual, economic, educational, and social service benefits of access, dissemination, and use of research findings about ASD diagnostic criteria through open access journals? How can the involvement of parents and caregivers of young children who present symptoms of ASD positively improve the training of primary care physicians? What can adults with high literacy skills, minimal support, and who personally experience neurodiversity contribute to future discussions about DSM criteria for ASD?
In addition, future studies can explore the integration of advanced technologies, such as artificial intelligence and machine learning, in the diagnostic process to improve the accuracy, speed, and accessibility of ASD diagnosis while identifying the potential biomarkers and comparative studies between DSM-5 criteria and other diagnostic systems to further improve understandings of ASD characteristics. Fostering interdisciplinary research that combines insights from various disciplines, such as genetics, metabolomics, and proteomics, may provide possibilities to improve diagnostic practice and a comprehensive understanding of autism spectrum disorders.
Despite the researchers’ best efforts, the study has some limitations. The study used only three databases—MEDLINE, PsycINFO, and the Psychology and Behavioral Sciences Collection (EBSCO). The databases are comprehensive, however, it is possible that some relevant studies in other databases were not included in the current literature review, which may limit the review scope. In addition, the searches used specific keywords and control terms, such as “ASD,” “DSM-5,” and “toddler, preschoolers, and early childhood,” limiting the breadth of the search. While these terms are relevant, other relevant terms, or variations, could generate additional studies.
Today, ASD is widely understood as a complex neurodevelopmental disorder that appears in the early months of life. Diagnosis is dominated by criteria established for a mental health condition outlined in the DSM-5. A review of scientific literature reveals the current state of science about DSM-5 criteria and early diagnosis of ASD. Existing literature is replete with difficulties in diagnosis primarily associated with alignment to DSM-5 criteria for ASD that are recognized and significantly addressed by researchers, clinicians, and practitioners. There is growing recognition that developing and using biomarkers and MRIs in conjunction with screening methods such as the DSM-5 and a variety of others improves the diagnostic process and, subsequently, has the potential to enhance the quality of life and the prognosis for young children who begin life with symptoms uncharacteristic of a typically developing child. Studies indicate that frontline screening practices by primary care physicians are insufficient in addressing the urgent needs of young children and their families. Studies implicate urgency for a shift in the dominant diagnosis paradigm and a new lens for viewing ASD as an accepted, lifelong form of neurological development. The transdiagnosis lens and approaches, when accepted for designing research and communication, will open doors to new approaches to scientific discoveries about ASD as a neurodiverse, lived experience and provide interdisciplinary theories, models, practices, and tools with the potential for improving care, and legitimize a continuum of supports during early childhood and on the frontlines of a lifetime.
Author Contributions
Conceptualization, methodology, software, formal analysis, data curation, and writing, including original draft preparation, review, and editing are the joint efforts of both authors (Dow, M .J. & Wang, T). Both authors (Dow, M. J. & Wang T.) have read and agree to the publication of this manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Wang, T.; Lund, B.; Dow, M. Do hospitals satisfy our healthcare information needs for rare diseases? Comparison of healthcare information provided by hospitals with information needs of family caregivers. Health Commun 2023, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Lund, B.; Dow, M. Improving Health Information for Rare Disease Patients and Caregivers: A Survey of Preferences for Health Information Seeking Channels and Formats. J Hosp Librarian 2023, 2, 83–96. [Google Scholar] [CrossRef]
- Wang, T. Wang, T. Rare disease, rare information: Investigating healthcare information use in online global disability support groups. Doctoral Dissertation, Emporia State University, Emporia, KS, USA, May 13<sup>th</sup>, 2022.
- Wang, T.; Lund, B. Categories of information need expressed by parents of individuals with rare disorders in a Facebook community group: A case study with implications for information professionals. J Consum Health Internet 2020, 1, 20–34. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd edition (DSM-III); American Psychiatric Press: Washington, DC, USA, 2013. [Google Scholar]
- Centers for Disease and Prevention. Data & Statistics on Autism Spectrum Disorder. Available online: https://www.cdc.gov/autism/data-research/?CDC_AAref_Val=https://www.cdc.gov/ncbddd/autism/data.html(assessed on 6 June 2024).
- McCarty, P. , & Frye, R. E. Early detection and diagnosis of autism spectrum disorder: Why is it so difficult? Semin Pediatr Neurol 2020, 35, 100831. [Google Scholar] [CrossRef] [PubMed]
- 8. American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, W: American Psychiatric Press, 1980.
- Cakir J, Frye RE, Walker SJ. The lifetime social cost of autism: 1990–2029. Res Autism Spectr Disord. 2020, 72, 101502. [Google Scholar] [CrossRef]
- Dalgleish T, Black M, Johnston D, Bevan A. Transdiagnostic approaches to mental health problems: Current status and future directions. J Consult Clin Psychol 2020, 88, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Scimago Journal & Country Rank. About us. Available online: https://www.scimagojr.com/aboutus.php(assessed on 6 June 2024).
- Rosen NE, Lord C, Volkmar FR. The diagnosis of autism: From Kanner to DSM-III to DSM-5. J Autism Dev Disord 2021, 51, 4253–4270. [Google Scholar] [CrossRef] [PubMed]
- Barton ML, Robins DL, Jashar D, Brennan L, Fein D. Sensitivity and specificity of proposed DSM-5 criteria for autism spectrum disorder in toddlers. J Autism Dev Disord. 2013, 43, 5–1184. [Google Scholar] [CrossRef] [PubMed]
- 14. Coulter KL, Barton ML, Robins DL, Stone WL, Fein DA. DSM-5 symptom expression in toddlers. Autism, 1653; 202, 25, 6, 1653-1665. [CrossRef]
- Wetherby AM, Prizant BM. Communication and Symbolic Behavior Scales: Developmental Profile. Paul H. Brookes Publishing: Towson, MD, USA, 2002.
- Mullen, EM. Mullen Scales of Early Learning Manual. American Guidance Service, Inc: Circle Pines, MN, 1995.
- Wiggins LD, Robins DL, Adamson LB, Bakeman R, Henrich CC. Support for a dimensional view of autism spectrum disorders in toddlers. J Autism Dev Disord. 2012, 42, 2–191. [Google Scholar]
- Khan ZUN, Chand P, Majid H, et al. Urinary metabolomics using gas chromatography-mass spectrometry: potential biomarkers for autism spectrum disorder. BMC Neurol. 2022, 22, 1–101. [Google Scholar]
- Alrehaili RA, ElKady RM, Alrehaili JA, et al. Exploring early childhood autism spectrum disorders: A comprehensive review of diagnostic approaches in young children. Cureus. 2023, 15, 12. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, TS. The Structure of Scientific Revolutions, 4th ed. University of Chicago Press: Chicago, IL, USA, 1996.
- Burrell G, Morgan G. Sociological Paradigms and Organizational Analysis: Elements of the Sociology of Corporate Life. Routledge: New York, NY, 1979, 2016.
- Sidhu N, Srinivasraghavan J. Ethics and medical practice: Why psychiatry is unique. Indian J Psychiatry. 2016, 58 (Suppl 2), S199–S202. [Google Scholar] [CrossRef] [PubMed]
Table 1.
Studies by Article Title, Publication Journal Subject Area, and Findings from Investigations of DSM-5 Criteria to Infants and Young Children (2020 – 2023).
Table 1.
Studies by Article Title, Publication Journal Subject Area, and Findings from Investigations of DSM-5 Criteria to Infants and Young Children (2020 – 2023).
| Article Title | Journal Subject Area | Findings in Current Research |
|---|---|---|
| McCarty, P., & Frye, R. E. (2020, October). Early detection and diagnosis of autism spectrum disorder: Why is it so difficult?. Seminars in Pediatric Neurology, 35, 100831. | Pediatrics, Neurology | Improved training may increase the occurrence of practice by primary care physicians in ASD diagnosis. |
| Kaba, D., & Soykan Aysev, A. (2020). Evaluation of Autism Spectrum Disorder in Early Childhood According to the DSM-5 Diagnostic Criteria. Turk Psikiyatri Dergisi, 31(2). |
Psychiatry and Mental Health |
Children under 7 is the riskiest DSM-5 period for lost diagnosis, which leads to progressive loss of functionality. |
| Harris, H. K., Sideridis, G. D., Barbaresi, W. J., & Harstad, E. (2020). Pathogenic yield of genetic testing in autism spectrum disorder. Pediatrics, 146(4). | Pediatrics |
Toddlers with DSM-5 ASD diagnosis should be recommended for genetic testing. |
| Dow, D., Day, T. N., Kutta, T. J., Nottke, C., & Wetherby, A. M. (2020). Screening for autism spectrum disorder in a naturalistic home setting using the systematic observation of red flags (SORF) at 18–24 months. Autism Research, 13(1), 122-133. | Neurology, Genetics | ASD screening tools are not accurate enough in routine screening of toddlers. SORF provides beneficial video- recorded sample of child and family. |
| Hicks, S. D., Carpenter, R. L., Wagner, K. E., Pauley, R., Barros, M., Tierney-Aves, C., ... & Middleton, F. A. (2020). Saliva microRNA differentiates children with autism from peers with typical and atypical development. Journal of the American Academy of Child & Adolescent Psychiatry, 59(2), 296-308. | Psychiatry and Mental Health, Developmental and Educational Psychology |
Salivary microRNA is a noninvasive test that can improve accuracy in diagnosis of ASD in children. |
| Harris, H. K., Lee, C., Sideridis, G. D., Barbaresi, W. J., & Harstad, E. (2021). Identifying subgroups of toddlers with DSM-5 autism spectrum disorder based on core symptoms. Journal of Autism and Developmental Disorders, 1-15. | Developmental and Educational Psychology |
Social communication and restricted/repetitive behaviors may more precisely characterize subgroups within toddlers at time of ASD diagnosis |
| Kong, X. J., Sherman, H. T., Tian, R., Koh, M., Liu, S., Li, A. C., & Stone, W. S. (2021). Validation of rapid interactive screening test for autism in toddlers using autism diagnostic observation schedule™ second edition in children at high-risk for autism spectrum disorder. Frontiers in psychiatry, 12, 737890. | Psychiatry and Mental Health |
Rapid Interactive screening Test for Autism in Toddlers (RITA-T) was found to be valid for screening toddlers at high risk of ASD allowing initiation of services before formal diagnosis with DSM-5. |
| Coulter, K. L., Barton, M. L., Robins, D. L., Stone, W. L., & Fein, D. A. (2021). DSM-5 symptom expression in toddlers. Autism, 25(6), 1653-1665. | Developmental and Educational Psychology |
Contradicts earlier studies suggesting that restrictive and repetitive behavior may not be apparent until later in childhood. |
| Pellecchia, M., Dickson, K. S., Vejnoska, S. F., & Stahmer, A. C. (2021). The autism spectrum: Diagnosis and epidemiology. In L. M. Glidden, L. Abbeduto, L. L. McIntyre, & M. J. Tassé (Eds.), APA handbook of intellectual and developmental disabilities: Foundations (pp. 207–237). American Psychological Association | Developmental and Educational Psychology |
Presents ASD as one of seven conditions that result in intellectual and developmental disabilities. Addresses intellectual disabilities from multiple disciplines in biological, behavioral, and social science. |
| Haffner, D. N., Bartram, L. R., Coury, D. L., Rice, C. E., Steingass, K. J., Moore-Clingenpeel, M., ... & Group, N. E. D. (2021). The Autism Detection in Early Childhood Tool: Level 2 autism spectrum disorder screening in a NICU Follow-up program. Infant Behavior and Development, 65, 101650. | Developmental and Educational Psychology |
Autism Detection in Early Childhood is useful as a level 1 screening tool identifying children at risk for ASD in high-risk NICU. |
| Khan, Z. U. N., Chand, P., Majid, H., Ahmed, S., Khan, A. H., Jamil, A., … & Jafri, L. (2022). Urinary metabolomics using gas chromatography-mass spectrometry: potential biomarkers for autism spectrum disorder. BMC Neurology, 22(1), 101. | Neurology | Urine organic acids profiles are good discriminators between children with ASD and typically developing children. |
| Alrehaili, R. A., ElKady, R. M., Alrehaili, J. A., & Alreefi, R. M. (2023). Exploring Early Childhood Autism Spectrum Disorders: A Comprehensive Review of Diagnostic Approaches in Young Children. Cureus, 15(12). | Medicine | Various diagnostic modalities, including lab investigations and neuroimaging, contribute to early detection and comprehensive assessment of ASD. |
| Saban-Bezalel, R., Avni, E., Ben-Itzchak, E., & Zachor, D. A. (2023). Relationship between Parental Concerns about Social–Emotional Reciprocity Deficits and Their Children’s Final ASD Diagnosis. Children, 10(11), 1786. | Pediatrics | Parental concerns about their child’s development regarding deficits in social-emotional reciprocity are significant in predicting a final diagnosis of ASD. |
| Lavi, R., & Stokes, M. A. (2023). Reliability and validity of the Autism Screen for Kids and Youth. Autism, 27(7), 1968-1982. |
Developmental and Educational Psychology |
When children outgrow early childhood, the Autism Screen for Kids and Youth with items related to DSM-5 criteria is a promising screening tool. |
| Francés, L., Ruiz, A., Soler, C. V., Francés, J., Caules, J., Hervás, A., ... & Quintero, J. (2023). Prevalence, comorbidities, and profiles of neurodevelopmental disorders according to the DSM-5-TR in children aged 6 years old in a European region. Frontiers in Psychiatry, 14, 1260747. | Psychiatry and Mental Health |
Neurodevelopmental disorders (NDD) often coexist with other disorders and it is rare for them to occur alone. There is evidence of presence of comorbidities in language disorders and ADHD. Low economic resources, lower levels of education of parents, and lifestyle habits that can be improved can alert clinicians to the possibility of NDD. |
Table 2.
Studies by Journal Title, Journal Frequencies. and Journal Subject Area.
| Journal Title | Journal Frequencies |
Journal Subject Area |
|---|---|---|
| Autism | 2 | Developmental and Educational Psychology |
| Frontiers in Psychiatry | 2 | Psychiatry and Mental Health |
| Seminars in Pediatric Neurology | 1 | Pediatrics, Neurology |
| Turk Psikiyatri Dergisi | 1 | Psychiatry and Mental Health |
| Pediatrics | 1 | Pediatrics |
| Autism Research | 1 | Neurology, Genetics |
| Journal of the American Academy of Child & Adolescent Psychiatry | 1 | Psychiatry and Mental Health, Developmental and Educational Psychology |
| Journal of Autism and Developmental Disorders | 1 | Developmental and Educational Psychology |
| Infant Behavior and Development | 1 | Developmental and Educational Psychology |
| BMC Neurology | 1 | Neurology |
| Children | 1 | Pediatrics |
| Cureus | 1 | Medicine |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



