
Submitted:
17 June 2024
Posted:
17 June 2024
You are already at the latest version
Abstract
Falls are considered a significant cause of disability, pain, and premature deaths in older adults, often due to sedentary lifestyles and various risk factors. Combining immersive virtual reality (IVR) with physical exercise, or exergames, enhances motivation and personalizes training, effectively preventing falls by improving strength and balance in older people. IVR technology may increase the ecological validity of the assessments. The main goal of our study was to assess the feasibility of using a KAVE-based VR platform combining simulations of Levadas and a Cable Car to perform a balanced assessment and profiling of the older adult population for high risk-of-falls and the related user experience. A VR-based platform using a Wii balance board and a CAVE was developed to assess balance and physical fitness. Validated by the Biodex Balance System (BBS), 25 older adults participated in this study. The usability and presence were measured through the System Usability Scale and ITC-SOPI questionnaires, respectively. The IVR system showed a high presence and a good usability score of 75. Significant effects were found in the maximum excursion of the Centre of Pressure (COP) on the anterior-posterior axis during the Cable Car Simulation (CCS), correlating with BBS metrics. Multiple discriminative analysis models and the support vector machine classified fall risk with moderate to high accuracy, precision, and recall. The system accurately identified all high-risk participants using the Leave-One-Out method. This study suggests that an IVR-based platform based on simulations with high ecological validity can be used to assess physical fitness and identify individuals at a higher risk of falls.
Keywords:
Virtual Reality
; Balance Assessment
; Posturography
; Ecological validity
; Physical Fitness
; Senior Fitness Tests
1. Introduction
Falls are most common in older adults and cause injuries that are the leading factor of disability, pain, dependency, and early death. According to the World Health Organization (WHO), 28-35 % of older adults aged 65 and above fall annually, increasing to 32-42% for those aged 70 and above [1]. Falls are becoming a global health problem because they create injuries and affect especially the lives of older people, their families, and society. Falls among the elderly population occur because of the interaction of several risk factors, such as a sedentary lifestyle, overuse of alcohol, and environmental barriers, e.g., narrow stairs, socioeconomic conditions, and multiple comorbidities. Neurological diseases such as Parkinson’s disease, multiple sclerosis, and traumatic brain injuries are also part of the risk factors for falls [1]. Some other risk factors include older age [2], poor muscle strength [3,4], gait disorders [5], cognitive deficits [6], and balance disorders [7]. Older adults with difficulties in daily life activities are particularly vulnerable to falls, leading to injuries, disabilities, poor quality of life, mortality, and financial dependency. Addressing these risk factors through interventions like physical exercise, home modifications, and medical management can help reduce the incidence and impact of falls among the elderly.[8].
In particular, physical exercise has been identified as one of the best solutions to reduce the risks of falls. Some exercises that can minimize the risks of falls are body stretch, strength and balance training, tai chi, and treadmill workouts[9]. Cognitive impairments, including low memory, self-control and response, is also linked with falls among older people [6,9]. Thus, cognitive-motor interference (CMI) challenges the ability of older adults to execute tasks effectively, such as walking and speaking simultaneously [10,11], putting them at higher risk of falls and experiencing difficulties executing those cognitive tasks [12,13].
Several organizations such as the Joint American and British Geriatric Society (ABGS), British Geriatric Society (ABGS) (Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society, 2011) and the National Institute of Clinical Excellence (NICE) UK have introduced a set of guidelines to assess and reduce the risk of falls [14]. It is well-known that poor strength and balance cause an increase in the risk of falls [15], and the efficacy of neuromuscular exercises has been tested to reduce falls [16]. It is also suggested that older adults should have moderate-to-high-intensity balance training in their multi-tier exercise program [17]. One study conducted home-based training sessions, which were successful for both men and women. It helped to reduce the risk of falls and associated injuries by about 35-45%. These sessions had multiple exercises, such as walking, muscle strength, and balance training, which health professionals and trained nurses at home advised. However, the need for health professionals to administer the training sessions is a known limitation [18].
Novel tech-based applications can effectively promote these training programs. Recent reviews and meta-analyses exposed new technologies such as virtual reality (VR), artificial intelligence (AI), and exergames that introduced new training programs specially designed to avoid incidents of falls [20,21,22]. VR may increase older adults’ motivation for their physical rehabilitation, which may be a valuable tool for achieving active aging goals [21].
To summarise, the literature highlights how common commercial exergames fall short in addressing the particular needs of older adults. The relevance of adequate, objective and automated user profiling is essential for effective personalization of an exergame intervention designed for older adults.
2. Related Work
The fall risk classification can be defined as a single or group of assessments performed to evaluate the risk of falls for individuals and to provide feedback if follow-up assessments or training are required. The standard methods are followed based on the individual's level of risk for falls to customize or implement assessments and interventions [21]. Some common fall risk classification methods include self-reported questionnaires, physical exercise tests, and posturography procedures. These methods have some limitations, advantages and drawbacks. For example, the Stay Independent Brochure is a valid and reliable instrument for risk assessment of falls [22]. However, it can be used for certain populations and takes longer to complete. Literature also highlighted other physical functional tests, such as the Timed-Up-and-Go (TUG) test, Berg balance scale or walking speed, as profiling tools [21]. However, these mobility tests require trained healthcare professionals to evaluate the risk of falls in healthy community-dwelling older adults [23]. Computer-based posturography is another way to assess the individual’s balance and quantify body sway. The posturographic parameters can be acquired for static and dynamic balance conditions, providing value information on postural controls [24]. The multivariate logistic regression may not be feasible to get the optimal fall risk classification as the posturographic parameters are highly correlated and may be no-linear. Therefore, utilizing Artificial Intelligence (AI)- based methods such as machine learning may solve the complexity of the data set [25]. The posturographic parameters and AI-based methods have been used in several studies for multiple types of elderly populations belonging to different groups or organizations [26,27,28,29,30] such as osteoporotic [31], parkinsonism [32], and multiple sclerosis [33]. The posturography systems comprise multiple hardware components such as force platforms [29,32,33], pressure platforms [28], inertial sensors [28,34], or depth cameras [30] to acquire posturographic data. The common machine learning algorithms are mostly used in studies of random forests, decision trees, neural networks, support vector machines (SVMs), and k-nearest neighbours [28,29,33]. The receiver’s operating characteristic (ROC) analysis [28] shows that these algorithms can get accuracy between 80 and 99.9% [29,31,33,35] or an area under the curve (AUC) between 85 and 88%.
Some studies evaluated the efficacy of wearable sensor-based functional assessments for predicting the risk of falls. The machine learning models were implemented to classify participants as fallers (F) and non-fallers (NF) based on the features of the sensor data. The following criteria were used to classify participants as F and NF: quantitative evaluation of the standard function procedure (e.g., BBS and Tinetti Gait and Balance Scale), self-reported fall incidents, and hospitalization history [55,56,57]. Wearable Sensor-based tools have been developed recently and are available commercially to assess the risk of falls in older adults. One recent instrument, FallSkip, assesses the risks of falls in the elderly. The tool modified the TUG test following the clinical protocol and used inertial sensors to record the metrics such as time and sway of COP [58]. Another tool is Mobility Lab™ (ML, APDM, Inc., Portland) [36], which comprises six wirelessly synchronized Inertial measurement units (IMUs) [37].
It has been considered that older people have low motivation for traditional physical exercise programs [38]. However, combining immersive VR (IVR) and physical exercise could be a suitable training program for older people’s physical needs and requirements [39]. The literature is scarce for the VR simulations to assess the risk of falls. However, most of the studies used VR-based exergames through interventions to reduce the risk of falls. Exergames are game-based physical training performed in a virtual environment and have been shown to improve physical fitness [40] and as a treatment option for multiple types of unhealthy subjects [41,42]. VR is an ideal platform for cognitive-motor interference because it offers physical exercise, joy, and cognitive functions in one platform, increasing the intervention’s ecological validity, safety, and acceptance.
The literature highlighted commercial VR-based exergames for multiple physical activities, such as balance and strength training for older adults. Thus, the efficacy and feasibility of VR technology have been acknowledged to minimize the risks of falls [43,44,45]. Habibnezhad et al. created a VR simulator to evaluate the risk of falls for construction workers. The VR system comprised three trackers, a VR headset, and a virtual environment. The inverse kinematic method was used for the body-joint simulations to create the virtual leg movements. The study showed that the VR simulator performed better than the traditional VR systems to asses upper-limb stability during gait movements [46]. Another study investigated the effect of multiple VR-based visual stimuli on postural control while standing in an upright posture. The participants’ postural stability was quantified by measuring the center of pressure (COP) in a VR environment. The authors created the virtual simulation of the rotary optokinetic drum and observed that visual stimuli invoked by the rotary optokinetic drum may enhance the instability greater than the stance with the eyes closed [47]. Yeh et al. examined the impact of delayed visual feedback and cognitive performance on postural control in healthy young and elderly populations. The participants were asked to position their COP(upright posture with eyes open) in a fixed target as precisely as possible with the visual and delayed-visual feedback of their COP position. They also performed arithmetic tasks (cognitive dual tasks). An increase in postural sway was observed in older adults with delayed visual feedback, which indicates that older adults rely more on vision to control their posture [48]. One study assessed the validity and reliability of the data from the Wii balance board (WBB) against a force platform (FP) in older adults with type 2 diabetes mellitus. The regression model showed that the WBB was able to describe most of the change in COP sway of the force platform between 42 and 72% for all test cases. The authors suggest that WBB is a valid and reliable tool for quantifying the COP excursion [49].
Another study created a VR-based tool to assess the risks of falls. The head-mounted display (HMD) was used along with motion sensors to record kinematic data during the tests. The results indicated that the participants who were at high risk of falls took longer execution time for interventions and a number of steps [50]. Garcia introduced a VR tool to assess the risk of falls in the elderly. The author implemented the Choice Stepping Reaction Time task (CSRT) and used an HTC Vive headset (VR headset), suggesting that the highly immersive VR tool can concentrate more on cognitive and motor tasks instead of the technology being used [51]. Similarly, an Oculus Rift headset was used in another study to assess dynamic balance through head mobility. The virtual park scene was created where participants had to ask to save their heads from approaching the balls. The objective of the task was to stimulate the vestibular function to quantify head movements and assess dynamic balance. The results indicated significant between-group differences in head paths, head accelerations, and peak frequencies. However, no significant differences were found in the postural sway parameters [52]. Another study used non-immersive VR and treadmill training to improve cognition and body movements and identified fewer incidents of falls when compared to treadmill training without VR [51]. Some studies showed the efficiency of novel tech-based intervention programs in improving balance [52,53] and locomotion for older adults [51,54].
Aspects such as the visual representation of the user’s body in a virtual environment affect the perception of spatial presence and may decrease the presence level if the user’s virtual body is not represented in the VR environment [53]. Augmented reality (AR) can offer a higher sense of presence and realism than VR. Applications for motor rehabilitation are an excellent example of the benefits of using AR [54]. It allows users to interact with real-world objects by implementing an adapted virtual environment, which is more ecologically valid, accessible and feasible for older adults [55].
Therefore, in this research, we created a custom immersive VR-based platform – based on validated protocols and with a high ecological validity – to assess physical fitness and static balance for older adults to enable adequate exergame personalization to avoid the occurrence of falls. We also examined the usability and the presence level of the VR application. The use of simulated functional activities in VR may enhance the validity of balance and fitness assessment. The following section of this paper describes methods (hardware and software) and the results of our study.
2. Methods
2.1. Participants
Following a repeated measures samples design, 25 participants (19 females, ages: M= 71.2 SD = 7.8) were recruited from a local senior gymnasium in Funchal, Portugal, by invitation of the sports science professionals who work at this gymnasium. The balance assessments were performed at the University of Madeira, Laboratory of Pedagogy and Optimisation of Sports Performance. The participants were healthy Portuguese older adults, were provided with informed written consent before the study, and received no compensation for their participation. Six participants were removed because they lost their heart rate data due to the connectivity issues of the chest band sensors to the system application. Following the Declaration of Helsinki, the procedures were implemented and supervised by an experienced, trained staff and approved by the Faculty of Human Kinetics Ethics Committee, CEIFMH Nº3/2023.
2.2. Apparatus
2.2.1. Hardware
We used the KAVE (Kinect-cave Automatic Virtual Environment) [56], designed and implemented at the NeuroRehabLab, to create an immersive virtual environment for our application. To project a virtual environment display, three white walls were built with width and height of 2.2 and 2.8 meters, respectively. Four HD projectors, external speakers, and a processing personal computer were the core parts of the Kave system Figure 1(a). The KAVE application integrates a Unity 3D plugin comprising scripts, prefabs, objects, and the Microsoft Kinect libraries (https://assetstore.unity.com/packages/tools/camera/kave-113090). Unity 3D is a cross-platform game engine with features such as advanced animations, particle systems, high-definition audio, and tools to create 2D and 3D games. The Kinect V2 tracking sensor (Microsoft, Redmond, USA) was used for full-body tracking to interact with the virtual environment and create a parallax effect.
The Wii Balance Board (WBB) platform (Nintendo Co. Ltd, Kyoto, Japan) was used to examine the static balance of the participants by computing the displacement of the center of pressure (COP). It works with Bluetooth technology, comprises four platform sensors, and has been used for commercial games such as WII. It has two variants with weight support limits of 135 kg and 156 kg. The maximum weight limit for the platform is 300 Kg (WiiBalanceBoardOperationsManual.Nintendo) [57] Figure 1(b).
The heart rate was measured using the chest band Polar H10 (Polar Electro Oy, Kempele, Finland) for cardiorespiratory endurance. The Polar H10 connects with ActiGraph’s WGT3X-BT accelerometer (Actigraph Corporation, Pensacola, FL, USA) to measure the intensity (magnitude vector) and the motion of the physical exercise. The accelerometer data (metrics) were processed by the ActiLife6 computer application (version 6.13.4, ActiGraph, Cary, NC, USA).
2.2.2. Software
A VR-based Cable Car Simulation (CCS) was created in Unity 3D (unity3d.com) to simulate a realistic and more ecologically valid environment to examine the static balance in older adults. The virtual environment has 3D assets such as mountains, trees, grass, cable car poles, wires, stations, etc. Some virtual environment assets of the simulation were created in the open-source 3D computer graphics software tool Blender (Blender Foundation, Amsterdam, Netherlands). Figure 2(a) Figure 2(b). The simulation application communicates with WBB through Bluetooth technology and records COP at 30 Hz during the study. The CCS circuit consists of 5 straight segments at five turning angles (0, 45, 90, -45 and -90 deg). The CCS circuit is performed 4 times at different speeds (3, 5, 7 and 9 m/s). After finishing a lap, the simulation restarts automatically with a different speed. The CCS measures the displacements of the COP for each combination of displacement speed and turning angle, which will then be used to assess static balance.
Additionally, a VR-based Virtual Levada simulation application previously created in our lab [58] assessed cardiorespiratory endurance and lower body strength. The virtual Levada tracks comprise computer-generated 3D objects such as trees, mountains, tunnels, and irrigation canals, designed and developed in Unity3D Engine and Blender software (Blender Foundation, Amsterdam, Netherlands). It simulates virtual hiking based on in-place stepping. Based on the assessments from the Senior Fitness Test (SFTs) [59], a two-minute step test (2MST) was implemented. The participants had to raise their knees at a certain height, which Kinect computed during the in-place stepping exercise, to navigate into virtual Levada tracks. Additionally, aversion of the 30-second chair sit-stand (30SCST) exercises was implemented to examine lower body strength.
As a means of comparison and validation of the system, we used Biodex Balance System (BBS) SD (biodexrehab.com) as a reference (Figure 2(c)). It offers both static and dynamic balance assessment and the risk of falls. The advantages of BBS are the development of muscle tone, balance and agility improvement and treatment for various pathologies. It is highly user-friendly, has a touch screen, and a step-by-step guide for executing static and dynamic balance training and protocols. The BBS is quick and efficient in profiling older adults for the risks of falls and has been extensively validated in this population [60]
2.3. Questionnaires and Balance
The 7-point Likert scale questionnaire was used to evaluate the participant’s cybersickness. Similarly, the System Usability Scale SUS [61] questionnaire was used to measure the system's usability.
The ITC-SOPI is a 5-item Likert scale (Strongly Disagree, Disagree, Neither Agree nor Disagree, Agree, and Strongly Agree) questionnaire used to assess a participant’s level of presence in an immersive virtual or a displayed environment, and it comprises four components: Spatial Presence, Engagement, Naturalness, and Negative Effects.
The balance assessment used the Biodex Balance System (Biodex, Shirley, NY, USA). Before each testing session, the equipment was adjusted according to the participant’s height. Participants underwent a single training session to ensure they understood the protocol and to mitigate learning effects during subsequent testing phases. A 60-second rest interval separated the testing sessions. Participants performed the protocol in a unilateral stance while barefoot for bilateral comparison. The assessment measured the overall stability index (OSI), the anteroposterior stability index (APSI), and the lateromedial stability index (LMSI). Each index was assessed under four levels of platform stability, ranging from level 4 (most stable) to level 1 (most unstable). Lower scores on these indexes indicate better balance, reflecting less deviation from the horizontal position [62].
2.4. Procedure
The participants were randomly assigned to one group, and informed consent was provided before the study. The study protocol and the two-minute demo session were given at the start of the study. The participants performed the static balance assessment tests on the BBS platform for 15-20 minutes. They were provided a ten-minute break after finishing BBS assessments.
Subsequently, participants performed the 2MST (Figure 3(a)) and 30SCST in the KAVE-based VR environment (Figure 3(b)). During the tests, they were asked to wear a Polar H10 chest band and an Actigraph device to monitor heart rate (minimum and maximum) and physical activity. A ten-minute rest was provided after finishing the fitness tests.
Participants were asked to stand on the WII balance board in an upright standing position for approximately five minutes during the CCS (Figure 3(c)). They were instructed not to move their body while standing on the balance board. However, they were allowed to move their head and eyes. The cybersickness, System Usability Scale [61] and ITC-SOPI [63] questionnaires were provided afterwards.
2.5. Statistical Analysis
The means (M) and standard deviation (SD) were computed for SUS, ITC-SOPI questionnaires, the number of steps, magnitude vector, and heart rate, respectively.
The independent variables from the CCS were track Angle and Speed, with five and four levels, respectively. The dependent variables were the maximum excursion of the COP in the anterior-posterior (AP) and medial-lateral (ML) directions and mean velocity, which were calculated for all combinations of speed and angle variations. The metrics from BBS include EOMeanScore; ECMeanScore; Composite Mean Score; Stability Overall; Stability Anterior-Posterior; Media-Lateral; Percent of Time in Zone A, B and C; Percent of Time in Quadrant 1, 2, 3 and 4; Stability Index Front-Back and Left-Right. The participants were classified as high-risk and low-risk falls based on the BBS’s feature Composite-Mean score.
The linear discriminant analysis and the LeaveOneOut cross-validation method in MatlabR2023b (Mathworks Inc., Natick, MA, USA) were used to estimate the classifiers' accuracy, precision, and recall. Therefore, a repeated-measures ANOVA was performed with Greenhouse–Geisser, Huynh–Feldt corrections applied to obtain a valid F-ratio when appropriate. The statistical analysis was performed using IBM SPSS Statistics version 26 (IBM, New York, USA).
3. Results
The participants reported high presence scores in the ITC-SOPI for all the components: Spatial Presence (Mean: 2.8; SD: 0.69), Engagement (Mean: 3.28; SD: 0.88), Naturalness (Mean: 3.67; SD: 0.84), and Negative Effects (Mean: 1.55; SD: 0.83). Examining the results, participants were highly engaged and perceived a highly ecologically valid VR environment. However, spatial presence was slightly lower. It was also observed that participants’ responses were low for the component of the negative effect of the environment (Figure 4). The mean score on the SUS was M = 73.8 (SD = 12.0) for the system’s usability. This indicates a good usability score (> 68) [64].
Table 1 shows the results from the repeated ANOVA, which was executed on all the 2MST, 30SCST and CCS parameters. We found significant differences (p < .05) in three of the CCS speeds and track angles in the anterior-posterior axis (speed= 5, angle =-90; speed= 7, angle =90; speed= 7, angle =-90). This indicates that the different CCS parameters can induce measurable behavioral differences.
The maximum excursion of COP in the AP direction for all combinations of Angles (0, 45, 90, -45, -90) and Speeds (3m/s, 5m/s, 7m/s, 9m/s) was correlated with nearly all metrics of BBS metrics such as EOMeanScore, ECMeanScore, and Composite Mean, etc. (Table 2). However, no significant correlations were observed between the BBS metrics and the maximum excursion of COP in medial-lateral directions. The mean angles are the parameters where angles were ignored, speed limits were selected, and vice versa. The COP mean velocity for almost all combinations of Angles (0, 45, 90, -45, -90) and speed limits (3m/s, 4m/s, 5m/s, 6m/s) of the CCS was observed to be significantly correlated with the parameters of BBS. Again, these findings indicate that the CCS is effective at inducing behavioral responses and that the COP metrics of the CCS are consistent with those of the BBS.

Table 2.
Correlation between the CCS’s COP in anterior-posterior direction for all angles and speed limits and BBS parameters (Pearson Correlation, Sig. (2-tailed) and N participants).
Table 2.
Correlation between the CCS’s COP in anterior-posterior direction for all angles and speed limits and BBS parameters (Pearson Correlation, Sig. (2-tailed) and N participants).
| Pearson Correlation Sig. (2-tailed) N |
Stability Overall | StabilityAntPost | Stability Media Lateral | PercentTimeinZoneA | PercentTimeinQuad1 | PercentTimeinQuad2 | PercentTimeinQuad4 | Stability IndexFB |
Stability IndexLR |
|---|---|---|---|---|---|---|---|---|---|
| mean_angle_0 | .559 .013 19 |
.519 .023 19 |
.631 .004 19 |
-.499 .030 19 |
-.494 .031 19 |
.64 <.01 19 |
-.469 .043 19 |
.520 .023 19 |
.630 .004 19 |
| mean_angle_45 | .57 .01 19 |
||||||||
| mean_angle_90 | .47 .04 19 |
||||||||
| mean_angle_minus_45 | .48 .03 19 |
-.46 .04 19 |
|||||||
|
mean_angle_minus_90 |
-.517 .023 19 |
.522 .022 19 |
|||||||
| mean_cc_speed3 |
.486 .035 19 |
-.50 .029 19 |
|||||||
| mean_cc_speed5 |
-.470 .042 19 |
.566 .011 19 |
|||||||
| mean_cc_speed7 | -.495 .031 19 |
||||||||
| mean_cc_speed9 | .459 .048 19 |
-.486 .035 19 |
.570 .011 19 |
.458 .049 19 |
|||||
| MaxHeartRate |
-.566 .011 19 |
A Discriminant Analysis (DA) was performed to assess the sensitivity of the KAVE simulations to profile and classify participants as high-risk-falls or low-risk-falls based on the assessment conducted by the BBS. The participants who were classified in the higher 50 percentile predicted Composite Mean score (11 points) were referred to as high-risk falls, and those below were in low-risk falls. Several DA models, such as linear, pseudolinear, diaglinear, pseudoquadratic, diagquadratic, and support vector machine (SVM), were built along with the Leave-One-Out cross-validation method to evaluate the performance of the models (accuracy, recall, precision, and F-score). The selected input features for the classifier included CCS speeds and turning angles, their average responses, 2MST, 30SCST and HR. DA with each feature was performed to establish the prediction power of each feature modality, and also posterior step-wise regression approach was used to perform the feature selection.
Discrimination accuracies differ substantially, with the best classification for HR at 55%, CCS at 72%, 2MST and 30SCST at 72%, and 100% for the combined features through step-wise regression (Table 2). The selected features were the maximum excursion of COP for high speeds at high turning angles for both AP and ML, the mean of the speeds at 45-degree turning angles for both AP and ML, the mean of the angles at high speeds in AP direction, and COP at high speeds for no rotation.
Table 2.
Maximum excursion of COP in anterior-posterior axis for Cable Car Speed.
| LOO Cross-Validation | CCS | Mean of Turns | Mean Speeds | 2MST & 30SCST | HR | Step-Wise Feature Selection |
|---|---|---|---|---|---|---|
| DA Model | Pseudolinear | Linear | Diagquadratic | SVM | Diagquadratic | Linear |
| Accuracy | 0.72 | 0.66 | 0.66 | 0.72 | 0.55 | 1 |
| Recall | 0.72 | 0.66 | 0.66 | 0.72 | 0.55 | 1 |
| Precision | 0.72 | 0.66 | 0.66 | 0.75 | 0.55 | 1 |
| F-score | 0.72 | 0.66 | 0.66 | 0.73 | 0.55 | 1 |
4. Discussion
The main goal of our study was to assess the feasibility of using a KAVE-based VR platform combining simulations of Levadas and a Cable Car to perform a balanced assessment and profiling of the older adult population for high risk-of-falls and the related user experience. Overall, the participants reported high presence scores in the ITC-SOPI questionnaire, suggesting the validity of the ecological functional simulation and good usability scores with the SUS.
To evaluate the feasibility and sensitivity of the system as a profiling method capable of detecting users with high risk of falls, we used the BBS as a gold-standard reference for balance assessment and predicting the risk of falls. In addition, two Senior Fitness Tests (2MST and 30SCST) were also implemented together with the CSS. The CCS COP data show that CCS trajectory angles and speeds impacted the participant’s balance in AP and ML directions. Significant differences in CoP metrics were observed for the higher speeds (5m/s and 7m/s) and turning angles (90 and -90). In addition, numerous features from the CCS were correlated with BBS features, which supports the validity of our CCS to induce behavioral responses and for balance assessment.
The performance of DA models was evaluated to classify participants as high-risk and low-risk falls. We achieved excellent results from the classification using a step-wise feature selection. A linear DA on the selected features rendered a classification accuracy of 100 percent, indicating that our VR simulation of ecological and functional activities is precise in identifying the risk of falls in older adults. This also suggests that immersive VR environments can be used to implement standard procedures for fitness and balance assessments, proposing alternatives to traditional and expensive laboratory setups and creating custom environments based on functional activities with higher ecological validity. Previous research reported 86% accuracy with a WBB-based exergame to assess the physical independence of the participants. A 30-second Sit-Stand test was used as a reference to compare the results [65]. Seo et al. developed a Balance Ability Diagnosis system for the elderly for balance assessment using a WII balance board. The stability index (SI) algorithm was implemented, and the center of pressure parameter was used to predict the stability index of the balance system (Biodex SD). High accuracy was observed for the SI algorithm, and the linear regression model confirmed that the R-values ranged between 0.943 and 0.983 [66]. Similarly, another study evaluated the effect of virtual reality exercises on balance and fall in older adults. The instruments used in this study included a demographic questionnaire, the Berg Balance Scale (BBS), the Timed Up and Go (TUG) test, the Falling Efficacy Scale (FES), and the Xbox Kinect 360 for VR exercises. The results showed that VR exercises may improve balance and reduce fear of falling among the elderly [67].
A systematic review was performed to assess the reliability and validity of the WBB. The authors confirmed the reliability of the WBB; however, they also reported the impact factors such as reference criteria, intervention duration, parameters, data acquisition platform, and sample size [68]. In one study, VR HMD and force platforms were compared to evaluate the balance of older adults. The participants at high risk of falls changed their body posture in the anterior-posterior direction significantly compared to the control group. The results showed that the VR HMD is portable with minimal VR simulation sickness, inexpensive, and provides visual perturbation compared to the traditional mechanical platforms for measuring the multiple sensory aspects of the balance [69].
To conclude, in this study, we showed that our KAVE-based VR platform can assess the risk of falls for older adults with very high accuracy and reliability, relying on COP data. Our system comprises multiple simulations, such as a Virtual Levada and a Cable Car Simulation. The Virtual Levada implemented VR-based senior fitness tests such as a 30-second sit-stand and two-minute step test.
5. Limitations
Both simulations use a KAVE-based VR environment, which requires an adequate laboratory setup. Hence, a mobile-based VR implementation could make this system more portable and facilitate its acceptance and widespread use. The Virtual Levada uses a Kinect sensor and sometimes does not detect gesture signals. It also requires players not to wear black clothes to facilitate the tracking. Also, Kinect has latency issues that, although they do not affect the measurements per se, can affect the user experience. Further, Microsoft does not provide software development kit (SDK) updates. Hence, an alternative system would be ideal for improved motion detection and interaction. Although the CCS resembles an actual cable car and its environment, it does not have a realistic motion. The CCS could be improved by changing the environment, tracks, and rotation speeds, implementing only those found to induce statistically significant behavioral responses. Finally, an even larger sample of older adults could be beneficial in future studies.
Author Contributions
Conceptualization, M.A.A., S.B.i.B. and E.R.G.; methodology, M.A.A.; software, M.A.A.; validation, S.B.i.B., E.R.G. and M.A.A.; formal analysis, M.A.A. and S.B.i.B.; investigation, M.A.A.; resources, S.B.i.B. and E.R.G.; writing—original draft preparation, M.A.A.; writing—review and editing, M.A.A., S.B.i.B. and E.R.G.; visualization, M.A.A. and S.B.i.B.; supervision, S.B.i.B. and E.R.G.; project administration, S.B.i.B. and E.R.G.; funding acquisition, S.B.i.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by MACBIOIDI2 and NOVA Laboratory for Computer Science and Informatics.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Faculty of Human Kinetics Ethics Committee, CEIFMH Nº3/2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the study’s design, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
References
- World Health Organization WHO Global Report on Falls Prevention in Older Age. Ageing and life course, family and community health : WHO global report on falls prevention in older age 2008.
- Peng, K.; Tian, M.; Andersen, M.; Zhang, J.; Liu, Y.; Wang, Q.; Lindley, R.; Ivers, R. Incidence, Risk Factors and Economic Burden of Fall-Related Injuries in Older Chinese People: A Systematic Review. Inj Prev 2019, 25, 4–12. [CrossRef]
- Ishigaki, E.Y.; Ramos, L.G.; Carvalho, E.S.; Lunardi, A.C. Effectiveness of Muscle Strengthening and Description of Protocols for Preventing Falls in the Elderly: A Systematic Review. Braz J Phys Ther 2014, 18, 111–118. [CrossRef]
- Orr, R. Contribution of Muscle Weakness to Postural Instability in the Elderly. A Systematic Review. Eur J Phys Rehabil Med 2010, 46, 183–220.
- Mignardot, J.-B.; Deschamps, T.; Barrey, E.; Auvinet, B.; Berrut, G.; Cornu, C.; Constans, T.; De Decker, L. Gait Disturbances as Specific Predictive Markers of the First Fall Onset in Elderly People: A Two-Year Prospective Observational Study. Front. Aging Neurosci. 2014, 6. [CrossRef]
- Muir, S.W.; Gopaul, K.; Montero Odasso, M.M. The Role of Cognitive Impairment in Fall Risk among Older Adults: A Systematic Review and Meta-Analysis. Age and Ageing 2012, 41, 299–308. [CrossRef]
- Imagama, S.; Ito, Z.; Wakao, N.; Seki, T.; Hirano, K.; Muramoto, A.; Sakai, Y.; Matsuyama, Y.; Hamajima, N.; Ishiguro, N.; et al. Influence of Spinal Sagittal Alignment, Body Balance, Muscle Strength, and Physical Ability on Falling of Middle-Aged and Elderly Males. Eur Spine J 2013, 22, 1346–1353. [CrossRef]
- Jiang, J.; Long, J.; Ling, W.; Huang, G.; Guo, X.; Su, L. Incidence of Fall-Related Injury among Old People in Mainland China. Arch Gerontol Geriatr 2015, 61, 131–139. [CrossRef]
- Guirguis-Blake, J.M.; Michael, Y.L.; Perdue, L.A.; Coppola, E.L.; Beil, T.L.; Thompson, J.H. Interventions to Prevent Falls in Community-Dwelling Older Adults: A Systematic Review for the U.S. Preventive Services Task Force; U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews; Agency for Healthcare Research and Quality (US): Rockville (MD), 2018;
- Shimada, H.; Suzukawa, M.; Tiedemann, A.; Kobayashi, K.; Yoshida, H.; Suzuki, T. Which Neuromuscular or Cognitive Test Is the Optimal Screening Tool to Predict Falls in Frail Community-Dwelling Older People? Gerontology 2009, 55, 532–538. [CrossRef]
- Woollacott, M.; Shumway-Cook, A. Attention and the Control of Posture and Gait: A Review of an Emerging Area of Research. Gait Posture 2002, 16, 1–14. [CrossRef]
- Verghese, J.; Buschke, H.; Viola, L.; Katz, M.; Hall, C.; Kuslansky, G.; Lipton, R. Validity of Divided Attention Tasks in Predicting Falls in Older Individuals: A Preliminary Study. J Am Geriatr Soc 2002, 50, 1572–1576. [CrossRef]
- Beauchet, O.; Dubost, V.; Herrmann, F.; Rabilloud, M.; Gonthier, R.; Kressig, R.W. Relationship between Dual-Task Related Gait Changes and Intrinsic Risk Factors for Falls among Transitional Frail Older Adults. Aging Clin Exp Res 2005, 17, 270–275. [CrossRef]
- Overview | Falls in Older People: Assessing Risk and Prevention | Guidance | NICE Available online: https://www.nice.org.uk/guidance/cg161 (accessed on 10 September 2023).
- Granacher, U.; Muehlbauer, T.; Gruber, M. A Qualitative Review of Balance and Strength Performance in Healthy Older Adults: Impact for Testing and Training. Journal of Aging Research 2012, 2012, 1–16. [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for Preventing Falls in Older People Living in the Community. Cochrane Database Syst Rev 2012, 2012, CD007146. [CrossRef]
- Granacher, U.; Muehlbauer, T.; Zahner, L.; Gollhofer, A.; Kressig, R.W. Comparison of Traditional and Recent Approaches in the Promotion of Balance and Strength in Older Adults. Sports Med 2011, 41, 377–400. [CrossRef]
- Robertson, M.C.; Campbell, A.J.; Gardner, M.M.; Devlin, N. Preventing Injuries in Older People by Preventing Falls: A Meta-Analysis of Individual-Level Data. J Am Geriatr Soc 2002, 50, 905–911. [CrossRef]
- Corregidor-Sánchez, A.I.; Segura-Fragoso, A.; Rodríguez-Hernández, M.; Criado-Alvarez, J.J.; González-Gonzalez, J.; Polonio-López, B. Can Exergames Contribute to Improving Walking Capacity in Older Adults? A Systematic Review and Meta-Analysis. Maturitas 2020, 132, 40–48. [CrossRef]
- Bergmann, J.; Krewer, C.; Bauer, P.; Koenig, A.; Riener, R.; Müller, F. Virtual Reality to Augment Robot-Assisted Gait Training in Non-Ambulatory Patients with a Subacute Stroke: A Pilot Randomized Controlled Trial. Eur J Phys Rehabil Med 2018, 54. [CrossRef]
- Montero-Odasso, M.; Van Der Velde, N.; Martin, F.C.; Petrovic, M.; Tan, M.P.; Ryg, J.; Aguilar-Navarro, S.; Alexander, N.B.; Becker, C.; Blain, H.; et al. World Guidelines for Falls Prevention and Management for Older Adults: A Global Initiative. Age and Ageing 2022, 51, afac205. [CrossRef]
- Loonlawong, S.; Limroongreungrat, W.; Jiamjarasrangsi, W. The Stay Independent Brochure as a Screening Evaluation for Fall Risk in an Elderly Thai Population. Clin Interv Aging 2019, 14, 2155–2162. [CrossRef]
- Beauchamp, M.K.; Kuspinar, A.; Sohel, N.; Mayhew, A.; D’Amore, C.; Griffith, L.E.; Raina, P. Mobility Screening for Fall Prediction in the Canadian Longitudinal Study on Aging (CLSA): Implications for Fall Prevention in the Decade of Healthy Ageing. Age Ageing 2022, 51, afac095. [CrossRef]
- Prieto, T.E.; Myklebust, J.B.; Hoffmann, R.G.; Lovett, E.G.; Myklebust, B.M. Measures of Postural Steadiness: Differences between Healthy Young and Elderly Adults. IEEE Trans Biomed Eng 1996, 43, 956–966. [CrossRef]
- Ren, P.; Huang, S.; Feng, Y.; Chen, J.; Wang, Q.; Guo, Y.; Yuan, Q.; Yao, D.; Ma, D. Assessment of Balance Control Subsystems by Artificial Intelligence. IEEE Trans Neural Syst Rehabil Eng 2020, 28, 658–668. [CrossRef]
- Forth, K.E.; Wirfel, K.L.; Adams, S.D.; Rianon, N.J.; Lieberman Aiden, E.; Madansingh, S.I. A Postural Assessment Utilizing Machine Learning Prospectively Identifies Older Adults at a High Risk of Falling. Front Med (Lausanne) 2020, 7, 591517. [CrossRef]
- Howcroft, J.; Kofman, J.; Lemaire, E.D. Prospective Fall-Risk Prediction Models for Older Adults Based on Wearable Sensors. IEEE Trans Neural Syst Rehabil Eng 2017, 25, 1812–1820. [CrossRef]
- Silva, J.; Madureira, J.; Tonelo, C.; Baltazar, D.; Silva, C.; Martins, A.; Alcobia, C.; Sousa, I. Comparing Machine Learning Approaches for Fall Risk Assessment: In Proceedings of the Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies; SCITEPRESS - Science and Technology Publications: Porto, Portugal, 2017; pp. 223–230.
- Savadkoohi, M.; Oladunni, T.; Thompson, L.A. Deep Neural Networks for Human’s Fall-Risk Prediction Using Force-Plate Time Series Signal. Expert Systems with Applications 2021, 182, 115220. [CrossRef]
- Dubois, A.; Mouthon, A.; Sivagnanaselvam, R.S.; Bresciani, J.-P. Fast and Automatic Assessment of Fall Risk by Coupling Machine Learning Algorithms with a Depth Camera to Monitor Simple Balance Tasks. J NeuroEngineering Rehabil 2019, 16, 71. [CrossRef]
- Cuaya-Simbro, G.; Perez-Sanpablo, A.-I.; Morales, E.-F.; Quiñones Uriostegui, I.; Nuñez-Carrera, L. Comparing Machine Learning Methods to Improve Fall Risk Detection in Elderly with Osteoporosis from Balance Data. J Healthc Eng 2021, 2021, 8697805. [CrossRef]
- Bargiotas, I.; Kalogeratos, A.; Limnios, M.; Vidal, P.-P.; Ricard, D.; Vayatis, N. Revealing Posturographic Profile of Patients with Parkinsonian Syndromes through a Novel Hypothesis Testing Framework Based on Machine Learning. PLoS One 2021, 16, e0246790. [CrossRef]
- Sun, R.; Hsieh, K.L.; Sosnoff, J.J. Fall Risk Prediction in Multiple Sclerosis Using Postural Sway Measures: A Machine Learning Approach. Sci Rep 2019, 9, 16154. [CrossRef]
- Martinez, M.; De Leon, P.L. Falls Risk Classification of Older Adults Using Deep Neural Networks and Transfer Learning. IEEE J Biomed Health Inform 2020, 24, 144–150. [CrossRef]
- Liao, F.-Y.; Wu, C.-C.; Wei, Y.-C.; Chou, L.-W.; Chang, K.-M. Analysis of Center of Pressure Signals by Using Decision Tree and Empirical Mode Decomposition to Predict Falls among Older Adults. J Healthc Eng 2021, 2021, 6252445. [CrossRef]
- Comprehensive Gait and Balance Analysis - APDM Wearable Technologies. APDM 2020.
- Mancini, M.; Horak, F.B. Potential of APDM Mobility Lab for the Monitoring of the Progression of Parkinson’s Disease. Expert Rev Med Devices 2016, 13, 455–462. [CrossRef]
- Mora, J.C.; Valencia, W.M. Exercise and Older Adults. Clin Geriatr Med 2018, 34, 145–162. [CrossRef]
- Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Feasibility and Effects of an Immersive Virtual Reality Exergame Program on Physical Functions in Institutionalized Older Adults: A Randomized Clinical Trial. Sensors 2022, 22, 6742. [CrossRef]
- Boulos, M.N.; Yang, S.P. Exergames for Health and Fitness: The Roles of GPS and Geosocial Apps. Int J Health Geogr 2013, 12, 18. [CrossRef]
- Ruivo, J.A. Exergames and Cardiac Rehabilitation: A Review. J Cardiopulm Rehabil Prev 2014, 34, 2–20. [CrossRef]
- Lange, B.; Koenig, S.; Chang, C.-Y.; McConnell, E.; Suma, E.; Bolas, M.; Rizzo, A. Designing Informed Game-Based Rehabilitation Tasks Leveraging Advances in Virtual Reality. Disabil Rehabil 2012, 34, 1863–1870. [CrossRef]
- Monteiro-Junior, R.S.; Vaghetti, C.A.O.; Nascimento, O.J.M.; Laks, J.; Deslandes, A.C. Exergames: Neuroplastic Hypothesis about Cognitive Improvement and Biological Effects on Physical Function of Institutionalized Older Persons. Neural Regen Res 2016, 11, 201–204. [CrossRef]
- Kayama, H.; Okamoto, K.; Nishiguchi, S.; Yamada, M.; Kuroda, T.; Aoyama, T. Effect of a Kinect-Based Exercise Game on Improving Executive Cognitive Performance in Community-Dwelling Elderly: Case Control Study. J Med Internet Res 2014, 16, e61. [CrossRef]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of Interactive Physical-Activity Video-Game Training on Physical and Cognitive Function in Older Adults. Psychol Aging 2012, 27, 589–600. [CrossRef]
- Habibnezhad, M.; Shayesteh, S.; Jebelli, H.; Puckett, J.; Stentz, T. Comparison of Ironworker’s Fall Risk Assessment Systems Using an Immersive Biofeedback Simulator. Automation in Construction 2021, 122, 103471. [CrossRef]
- Luo, H.; Wang, X.; Fan, M.; Deng, L.; Jian, C.; Wei, M.; Luo, J. The Effect of Visual Stimuli on Stability and Complexity of Postural Control. Front Neurol 2018, 9, 48. [CrossRef]
- Yeh, T.T.; Cluff, T.; Balasubramaniam, R. Visual Reliance for Balance Control in Older Adults Persists When Visual Information Is Disrupted by Artificial Feedback Delays. PLoS ONE 2014, 9, e91554. [CrossRef]
- Álvarez-Barbosa, F.; Del Pozo-Cruz, J.; Sañudo, B.; Alfonso-Rosa, R.M. Is the Wii Balance Board a Valid and Reliable Instrument to Assess Postural Stability in Older Adults with Type 2 Diabetes Mellitus? Diabetes Research and Clinical Practice 2020, 166, 108313. [CrossRef]
- Clanché, F.; Personeni, G.; Renaux, A.; Muhla, F.; Bastogne, T.; Gauchard, G. Virtual Reality as Assessment Tool of the Risk of Falls in the Elderly. IJSSN 2023. [CrossRef]
- Garcia, J.A. A Virtual Reality Game-Like Tool for Assessing the Risk of Falling in the Elderly. Stud Health Technol Inform 2019, 266, 63–69. [CrossRef]
- Lubetzky, A.V.; Hujsak, B.D.; Fu, G.; Perlin, K. An Oculus Rift Assessment of Dynamic Balance by Head Mobility in a Virtual Park Scene: A Pilot Study. Motor Control 2019, 23, 127–142. [CrossRef]
- Phan, H.L.; Kim, J.P.; Kim, K.; Hwang, C.H.; Koo, K. Wrist Rehabilitation System Using Augmented Reality for Hemiplegic Stroke Patient Rehabilitation: A Feasibility Study. Applied Sciences 2019, 9, 2892. [CrossRef]
- Li, X.; Xu, B.; Teng, Y.; Ren, Y.; Hu, Z. Comparative Research of AR and VR Technology Based on User Experience. In Proceedings of the 2014 International Conference on Management Science & Engineering 21th Annual Conference Proceedings; IEEE: Helsinki, August 2014; pp. 1820–1827.
- Chen, M.; Tang, Q.; Xu, S.; Leng, P.; Pan, Z. Design and Evaluation of an Augmented Reality-Based Exergame System to Reduce Fall Risk in the Elderly. IJERPH 2020, 17, 7208. [CrossRef]
- Gonçalves, A.; Bermúdez, S. KAVE: Building Kinect Based CAVE Automatic Virtual Environments, Methods for Surround-Screen Projection Management, Motion Parallax and Full-Body Interaction Support. Proc. ACM Hum.-Comput. Interact. 2018, 2, 1–15. [CrossRef]
- Wii Balance Board. Wikipedia 2023.
- Ahmad, M.; Sousa, H.; Quintal, É.; Bermúdez I Badia, S. Efficacy of Augmented Reality-Based Virtual Hiking in Cardiorespiratory Endurance: A Pilot Study: In Proceedings of the Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies; SCITEPRESS - Science and Technology Publications: Online Streaming, --- Select a Country ---, 2021; pp. 575–582.
- Llorens, R.; Latorre, J.; Noé, E.; Keshner, E.A. Posturography Using the Wii Balance BoardTM. Gait & Posture 2016, 43, 228–232. [CrossRef]
- Arnold, B.L.; Schmitz, R.J. Examination of Balance Measures Produced by the Biodex Stability System. J Athl Train 1998, 33, 323–327.
- Jhon, B. SUS: A “Quick and Dirty” Usability Scale; 1st ed.; 1996; ISBN 978-0-429-15701-1.
- Yamada, R.K.F.; Arliani, G.G.; Almeida, G.P.L.; Venturine, A.M.; Santos, C.V. dos; Astur, D.C.; Cohen, M. The Effects of One-Half of a Soccer Match on the Postural Stability and Functional Capacity of the Lower Limbs in Young Soccer Players. Clinics (Sao Paulo) 2012, 67, 1361–1364. [CrossRef]
- Lessiter, J.; Freeman, J.; Keogh, E.; Davidoff, J. A Cross-Media Presence Questionnaire: The ITC-Sense of Presence Inventory. Presence: Teleoperators & Virtual Environments 2001, 10, 282–297. [CrossRef]
- Sauro, J.; Lewis, J.R. Quantifying User Research. In Quantifying the User Experience; Elsevier, 2016; pp. 9–18 ISBN 978-0-12-802308-2.
- Becker, H.; Garcia-Agundez, A.; Müller, P.N.; Tregel, T.; Miede, A.; Göbel, S. Predicting Functional Performance via Classification of Lower Extremity Strength in Older Adults with Exergame-Collected Data. J NeuroEngineering Rehabil 2020, 17, 164. [CrossRef]
- Seo, J.-W.; Kim, T.; Kim, J.I.; Jeong, Y.; Jang, K.-M.; Kim, J.; Do, J.-H. Development and Application of a Stability Index Estimation Algorithm Based on Machine Learning for Elderly Balance Ability Diagnosis in Daily Life. Bioengineering 2023, 10, 943. [CrossRef]
- Zahedian-Nasab, N.; Jaberi, A.; Shirazi, F.; Kavousipor, S. Effect of Virtual Reality Exercises on Balance and Fall in Elderly People with Fall Risk: A Randomized Controlled Trial. BMC Geriatr 2021, 21, 509. [CrossRef]
- Clark, R.A.; Mentiplay, B.F.; Pua, Y.-H.; Bower, K.J. Reliability and Validity of the Wii Balance Board for Assessment of Standing Balance: A Systematic Review. Gait Posture 2018, 61, 40–54. [CrossRef]
- Saldana, S.; Marsh, A.P.; Rejeski, W.J.; Haberl, J.; Wu, P.; Rosenthal, S.; Ip, E. Assessing Balance through the Use of a Low-Cost Head-Mounted Display in Older Adults: A Pilot Study. CIA 2017, Volume 12, 1363–1370. [CrossRef]
Figure 1.
Hardware Setup (a) Schematic diagram of the KAVE Setup; (b) Nintendo Wii Balance Board.

Figure 2.
Software Setup (a) Cable Car track TopView; (b) Cable Car Inside View; (c) Biodex Balance System (BBS).
Figure 2.
Software Setup (a) Cable Car track TopView; (b) Cable Car Inside View; (c) Biodex Balance System (BBS).
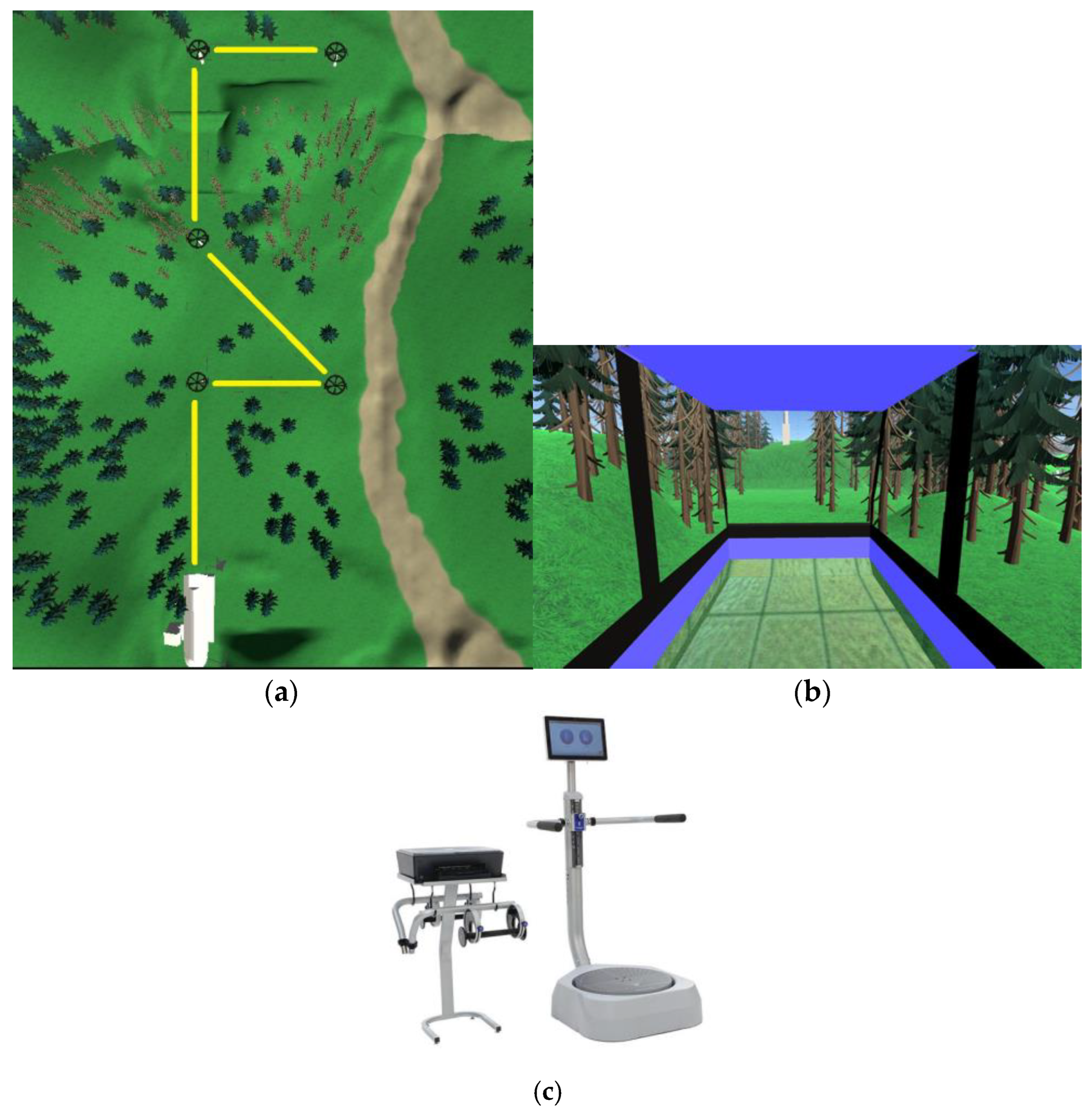
Figure 3.
The KAVE-based VR simulations include (a) Two-minute Step Test; (b) 30-Sec Sit-Stand; (c) Cable Car Simulation balance assessment .
Figure 3.
The KAVE-based VR simulations include (a) Two-minute Step Test; (b) 30-Sec Sit-Stand; (c) Cable Car Simulation balance assessment .

Figure 4.
Box Plot indicating the results of the ITC-SOPI Questionnaire.
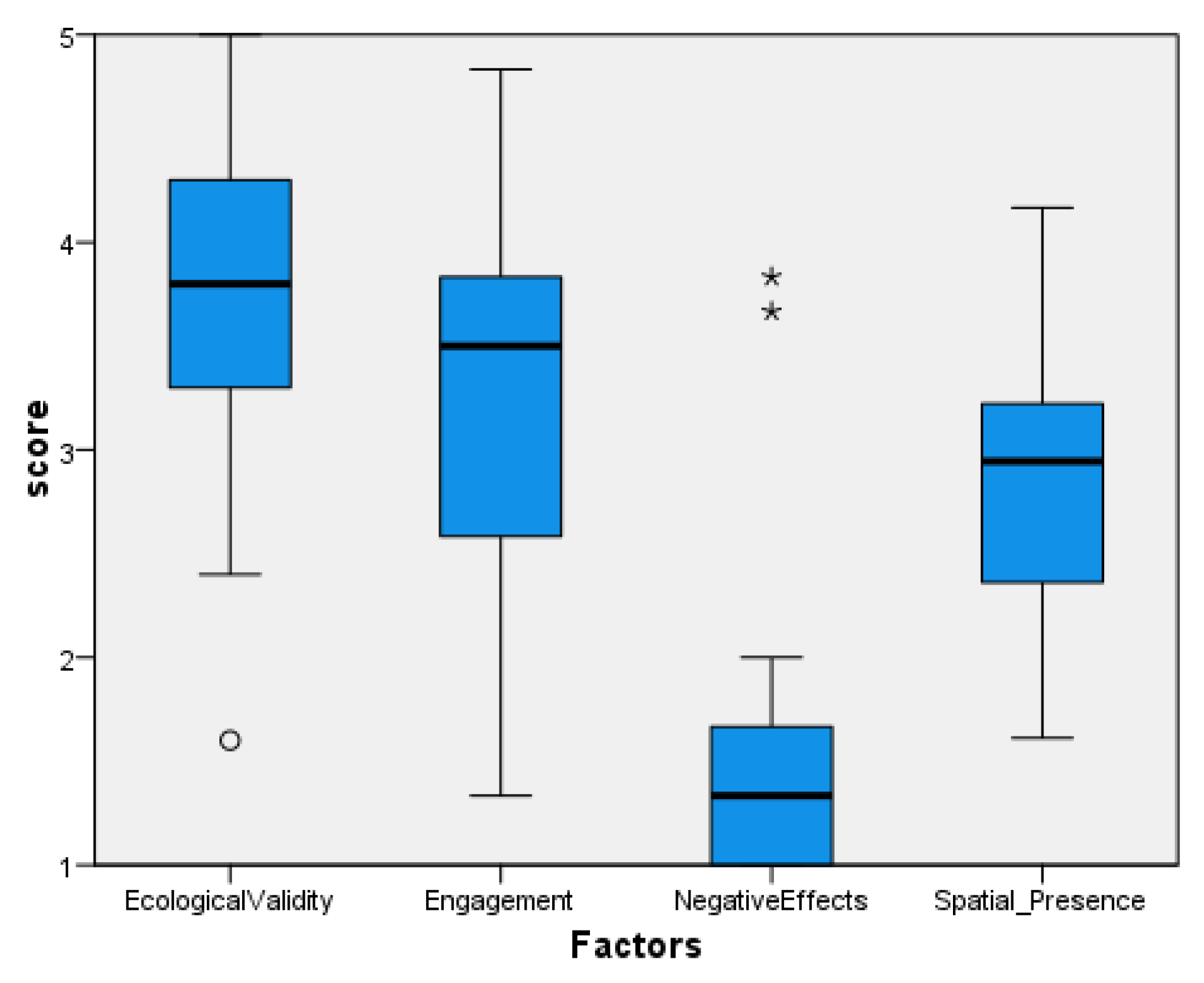
Table 1.
Maximum excursion of COP in anterior-posterior axis for Cable Car Speed and trajectory Angles.
Table 1.
Maximum excursion of COP in anterior-posterior axis for Cable Car Speed and trajectory Angles.
| Cable Car Speed and Trajectory Angles | F | Sig. |
|---|---|---|
| cable_car_speed5_angle_minus_90 | 4.461 |
.050 |
| cable_car_speed7_angle90 | 7.11 |
.016 |
| cable_car_speed7_angle_minus_90 | 5.10 | .037 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



