Submitted:
20 June 2024
Posted:
21 June 2024
You are already at the latest version
Abstract
This study addresses a gap in literature by comprehensively analyzing the emotional well-being of healthcare workers. Methods: The study employed an analytical cross-sectional design utilizing both qualitative and quantitative methodologies among 84 healthcare workers. Quantitative data was analyzed using STATA version 17 while qualitative data was analyzed using thematic analysis. Ethical approval was sought from the University of Livingstonia Research Ethics Committee (UNILIA-REC). Results: 88% of the participants had experienced verbal abuse; stress and anger, 87% emotional tiredness, 22% depression, and 4% physical abuse. Emotional tiredness was associated with department (p=0.004) and work demand (p=0.0047), stress and anger were associated with experience (p=0.033), department (p=0.002) and work demand (p=0.002), depression was associated with age (p=0.035), experience (p=0.025), cadre (p=0.046), staffing (p=0.005) and work demand(p=0.044), verbal abuse was associated with department (p=0.035) and physical abuse was associated with knowledge of policies (p=0.002). Being aware of emotions and controlling them was the common coping strategy used by most (26%) of the respondents. The study established that most (78%) of healthcare workers did not receive formal training on coping skills for emotional disturbances. Conclusions: Healthcare workers experience some emotional disturbances within their professional roles. There is a need for healthcare workers to be trained on how to cope with emotional disturbances.
Keywords:
Emotional disturbance
; emotional labor
; healthcare workers
; well-being
; hospital
1. Introduction
Hochschild [1] described emotional labor as a process of regulating or managing emotional expression with others as part of one’s professional job role. This involves hiding one’s true feelings and expression to fulfill job requirements such as smiling at patients even if one is not willing to smile. Several studies have shown that individuals’ bodily and psychological well-being is impacted by emotional labor. The risk of emotional disturbance among healthcare employees is increasing because of an unfavorable work atmosphere, verbal and physical abuse from patients, families, and coworkers, and a lack of knowledge on how to cope with stress and emotional disturbances at work [2]. Globally, because of new trends in employment, the health industry is impacted by an emotionally charged workforce. Unhealthy workplace conditions, such as increased workloads, irrational nurse-patient ratios, and a lack of resources, pose a serious threat to professionals’ well-being [3]. These problems have led to a lack of interest in the healthcare profession among other people and a lack of job satisfaction among healthcare workers as well as affecting their emotional wellbeing.
According to the Bureau for Labor Statistics [4], the health industry in the United States comprising 11% of the labor population, was one of the largest in the country. Numerous physical and psychological stressors, such as shift work and long working hours, chemical and biological risks, an excessive workload, workplace aggression, and other emotional disturbances were documented in the healthcare industry. These result in musculoskeletal disorders, chronic illnesses, lack of sleep, emotional exhaustion, and depression in these health workers, among other conditions that are harmful to their physical and emotional health [5]. Suh and Punnett [6] reported on high emotional demands at work and poor mental health in client-facing workers in Korea such that half of respondents had high psychological demands and about 11% of all workers handled angry clients during more than half of their work time and were more likely to experience poor mental health for 75% of their working time.
In sub-Saharan Africa, reports reveal a high increase in emotional exhaustion among healthcare workers. A systematic review of the prevalence of burnout among nurses reports that Nurses in Sub-Saharan Africa experience high levels of burnout with prevalences ranging from 33% to 87% [7]. The prevalence of emotional exhaustion in Sub-Saharan Africa was 66%, 60% for depersonalization, and 49% for low personal achievement [7]. In Ghana, 91.1% of nurses from 5 health facilities reported experiencing moderate to high rates of emotional exhaustion. Seventy percent of physicians and nearly 50% of nurses have experienced either verbal or physical emotional disturbances [2]. In South Africa at a Psychiatric Hospital in Cape Town, the prevalence of personal, work-related, and client-related burnout was relatively high with no significant associations between burnout and gender, rank, or years of experience [8]. Nearly half of Ethiopia’s medical staff at the government-run clinics in Dire Dawa suffered from burnout. The prevalence of emotional exhaustion among 501 healthcare workers was 54.1% [9]. Reports from Bwaila and Zomba Central Hospitals in Malawi showed a high prevalence of emotional exhaustion (75%), depersonalization (28%), and reduced personal achievements (33%) among healthcare workers [10].
According to [11] nurses who had experienced verbal and physical abuse and concern about workplace violence had considerably higher risks of presenting high weariness, such as emotional exhaustion, depersonalization, and low professional accomplishment. The study offers proof that verbal and physical abuse are psychological determinants of emotional disturbance. Working in a hospital, age above 30 years, using at least one substance, having 6 –11 years of experience, having no job supervision, working in a Pediatric Unit, and profession type (Midwifery, Public health officer, Medical Laboratory professional) were some of the factors significantly associated with burnout in Ethiopia [9]. In Malawi, Kim et al. [5] reported sex, marital status, depression, type D personality, working at a health center versus working at a rural hospital, lack of a very supportive supervisor, dissatisfaction with work and/or team interaction, and career dissatisfaction as factors contributing to emotional exhaustion. The increase in emotional disturbance has led to low staff productivity, increased work-related infections, increased medical error, high incidence of patient falls, poor nurse-physician relations, job dissatisfaction, and poor quality of nursing care provided to patients and family members at a time when human health is a priority [7].
Healthcare workers use different coping strategies for emotional disturbances. According to [12], in Australia, community nurses who had more emotional intelligence i.e., the capacity to be aware, control, and express one’s emotions and handle interpersonal relationships judiciously and empathy, had less stress at work and were emotionally feeling better. However, nurses with low or no emotional intelligence reported poorer levels of well-being, and the more job stress the more emotional labor [dissonance] they encountered. In Sub-Saharan Africa, [13] conducted a study in Ghana that reported psychological capital, reutilization of emotions, religious resources, social support, and job security as the five main strategies nurses and midwives employ to deal with emotional labor. A similar study conducted among nursing students residing in any of the 20 Middle Eastern and North African countries reported that nursing students utilized problem-focused (dealing with the problem), emotion-focused (regulating the emotion), and dysfunctional (venting the emotions) stress coping mechanisms to alleviate their stress [14]. Hiding feelings always or most of the time was reported by 34% of the participants as a way of coping with depression or anxiety. However, poor mental health was also more frequent when hiding feelings [6].
Significance of the Study
Understanding the emotional well-being of healthcare workers can lead to the provision of knowledge on how to improve the mental health and well-being of healthcare workers. The study aimed at analyzing the well-being of the emotional labor force among healthcare providers. This will help identify potential stressors among healthcare providers and areas of improvement in terms of support structures, self-care strategies, and awareness of emotional labor involved in healthcare work to implement more effective approaches in managing and supporting the well-being of healthcare workers, thus improving their overall performance and quality of care to the patients.
Theoretical Framework
This study was guided by emotional regulation theory as proposed by Gross in 1999 [15]. In this input-output model, people are stimulated by the circumstance and respond with emotions. The scenario serves as a cue for the individual’s physiological, behavioral, and cognitive-emotional responses. These give information to the individual and others in the social context. Gross’s model proposes that emotion regulation can occur at two points in this process. First is antecedent-focused, in which an individual regulates the precursors of emotion such as the situation or the appraisal. Second is response-focused, the individual modifies the physiological or observable signs of emotions. These two processes of emotion control correspond to the emotional labor idea of deep and surface action. Applying general emotion theory to emotional labor can assist explain these emotion management mechanisms and predict their outcomes. According to emotional labor theories, expressing emotions by acting may have negative consequences for individuals.
In this study, healthcare providers do deep and surface acts when they encounter emotional situations to perform their duties. The events perceived as personally emotional demands can be appraised as either positive or stressful. These include possible harm, threat, or challenge. Then individuals evaluate their resources to deal with the demands of whether it is anger or frustration and others that constitute the secondary appraisal process. So, if the emotional demands exceed their resources, emotional labor occurs, they feel emotionally exhausted, and coping responses become activated so that they deal with the situation.
2. Materials and Methods
Study Site
The study was conducted at Rumphi District Hospital in Rumphi district, located in the northern part of Malawi. The district covers an area of 350,000 km2 and has a total population of 229,161 [16]. Rumphi District Hospital is one of the main referral hospitals for health facilities within the Rumpi district including rural hospitals, health centers, and private medical facilities. The Hospital comprises an estimated 107 healthcare workers.
Study Design and Population
The study was an analytical cross-sectional employing explanatory mixed method research. The study involved healthcare workers including clinicians (a person who is qualified in the clinical practice of medicine and psychology) and nurses (a person who is trained to give care to people who are sick or injured and is authorized by the appropriate regulatory authority to practice nursing in his or her country).
Inclusion and Exclusion Criteria
The study enrolled full-time nurses and clinicians working at Rumphi District Hospital because they had enough time to become familiar with the job role and its associated emotional labor.
Sampling Methods
A convenience sampling technique was used to enroll study participants working at the study site. Any participant meeting the inclusion criteria was included in a convenience sample. The instrument for quantitative data collection was a self-administered questionnaire consisting of closed-ended questions. Pre-testing was done in adjacent catchment areas not involved in the study. Purposive sampling was used to recruit subjects for focused group discussion (FGDs). Each focus group comprised of a maximum of 10 participants. Maximum variation sampling was employed, with spread based on age, sex level, and occupation. FGDs were conducted to obtain qualitative data. In this study, only three groups were involved, as the saturation point had been reached.
Ethical Approval
Before the commencement of the study, ethical approval was obtained from the University of Livingstonia Research Ethics Committee (UNILIA-REC/UGS/56/2023). Permission to conduct the study at the Hospital was obtained from the Rumphi District Health Research Committee and the Directorate of Health and Social Services (DHSS) of Rumphi district. A written informed consent was obtained from all the participants by clearly explaining the purpose and benefits of the study to them. The participants’ privacy and confidentiality were ensured concerning the information that was provided. Anonymity was used to maintain the privacy of the participants.
Sample size Determination
The Taro Yamane formula [17] was used to determine the sample size since the population size was known. The formula for Yamane is given;
where n = sample size N = Population size e = Level of precision or sampling error which is (±0.05). Taking N=107, the population of healthcare workers at the hospital, and e = ±0.05. The sample size was estimated as 84, comprising 62 nurses, 20 clinicians, and 2 medical doctors.
N = N/(1 + Ne^2) (1)
Data Analysis
Quantitative data was entered in Excel, cleaned, and imported into STATA version 17 for analysis. Frequencies for categorical variables were presented as percentages in tables and figures. Thematic content analysis was used to analyze qualitative data in which recorded audios were duly transcribed, and the observational notes taken during the FGDs were also incorporated. Specific points were identified and coded while contents/codes with comparable meanings were categorized into sub-themes and themes for appropriate discussion.
3. Results
A total of 84 participants (100%) fully participated in the quantitative part of the study and three FGDs were also facilitated. As presented in Table 1, the majority (61%) of the participants were females, were aged 30 years to 39 years (48%), had a diploma as the highest qualification (68%), and had less than five years of work experience (44%).
Prevalence of Emotional Disturbances
Table 2 shows that overall, 87% of the participants had at least experienced emotional tiredness. Additionally, only 26% of the participants experienced depression because of the nature of their work, 88% had experienced verbal abuse, only 4% had experienced physical abuse and 88% had at least experienced stress and anger. Furthermore, most participants experienced emotional disturbances five times or less in a month.
Concept of Emotional Labor Force among Nurses and Clinicians and Its Implications on Their Well-Being and Job Performance
Most focus group participants understood the term emotional labor and commonly described it as a situation where someone has to control his or her emotion[s] at work while satisfying the needs of patients. In addition, it was commonly described that despite emotional disturbances, nurses, clinicians, and all individuals working in hospitals were supposed to take care of the emotional needs of their patients while ignoring their own emotional needs. For example, one respondent stressed that “waliyose wakugwira kuchipatala wakwenera kuwa muntu wachitima” (anyone working in a hospital must be a sympathetic person) (Participant 3, FGD 1). This was in line with another participant who mentioned that:
“The comfort and happiness of my patient is my first priority, … one of my job’s standards is to suppress my negative emotions and express myself in a way that is acceptable to my patients, therefore even if the patient said anything that made me feel upset, I still try to console and ease their pain.”(Participant 2, FGD 2)
Implications of Emotional Disturbance
Participants identified emotional tiredness, tension, worry, and rage as some of the problems that have a detrimental impact on their well-being when they are emotionally disturbed.
“Whenever I am emotionally disturbed, I get irritated, overthink everything, and worry about my job, which makes me quite tired by the end of the day.”(Participant 2, FDH 3)
Participants stated that poor job performance harms both the quality of patient care provided and the on-the-job performance of healthcare employees. They defined an emotionally disturbed person as someone who is irrationally furious, sad, sorrowful, and susceptible to mood swings. These emotions may lead to medical mistakes and a lack of motivation in carrying out their jobs.
“There are instances when being disturbed makes me moody, which reduces my performance at work and the quality of care I provide to my patients.”(Participant 4, FDG 2)
Participants also emphasized the negative effects of emotional disturbances on healthcare workers’ personal and social lives, including emotional weariness, stress, anxiety, rage, and subpar job performance.
Factors Associated with Emotional Disturbance
As shown in Table 4 below, emotional tiredness was significantly associated with the age of the participant (p= 0.061), department (0.004), and work demand (0.047). Depression was significantly associated with sex (p = 0.084), age (p=0.035), education level (p=0.056), experience (p=0.025), cadre (p=0.046), department (p=0.067), adequacy of staffing (p=0.005) and work demand (p = 0.044). Verbal abuse was associated with the department in which one was working (p=0.035) while physical abuse was significantly associated with the department (p=0.071) and knowledge about how well policies are communicated (p=0.002). Stress and anger were also associated with experience (p=0.033), department (p=0.002), and work demand (p=0.003).
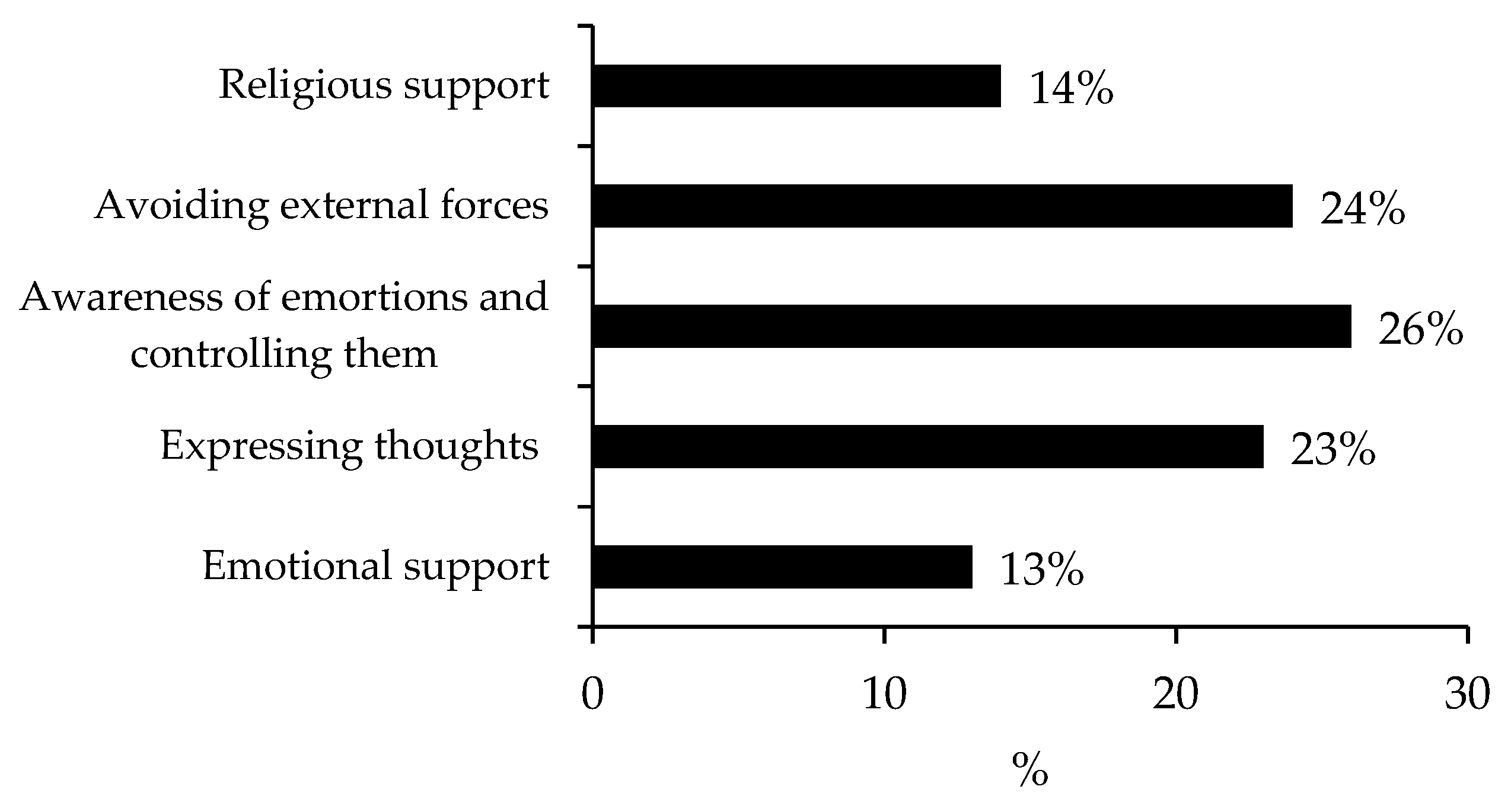
The majority (26%) of the participants were aware of their emotions and how to control them when disturbed. However, 24% were coping with emotional disturbance by avoiding external forces, 23% were expressing their thoughts, 14% were using religious support and 13% were using emotional support from the administration.
Figure 1.
Coping strategies for emotional disturbance.
When questioned about how they handle emotional issues at work, most FGD participants reported that they deal with emotional disturbances by among others; avoiding the issue at hand, speaking calmly and rationally with patients or other guardians, managing their emotions, and referring the person to another healthcare practitioner or higher authorities if the situation becomes out of hand.
“We always try to avoid a scenario as much as we can, we manage our emotions, and occasionally, we employ counseling to help the offender and the offended come to an understanding.”(Participant 5, FDG 2)
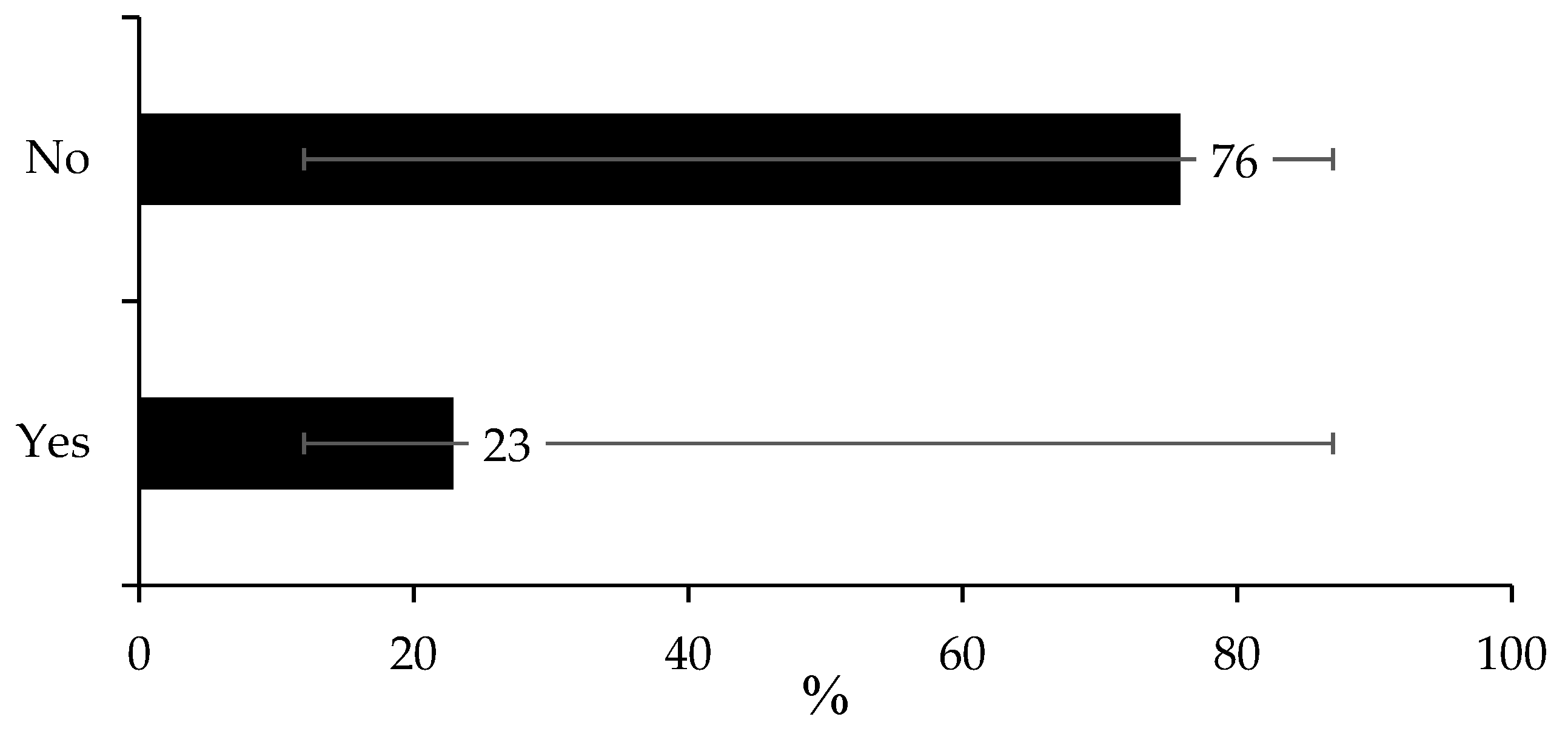
On whether the respondents received any inservice training majority (76%) of the respondents reported not receiving any formal or Inservice training on how to cope with emotional disturbances.
Figure 2.
Recipients of formal training on emotional disturbance.
In support, the results from FGDs conducted also showed that the majority of the participants did not receive in-depth training on how to deal with emotional disturbances. It was also mentioned that there were no procedures in place to monitor their well-being and that they did not have any regular methods for dealing with disturbances. Most participants suggested that having formal training would help them to deal with emotional disturbances experienced at work. Some of the participants mentioned that;
“In order to prevent emotional harm that results in bad emotional wellness and the nurse-patient connection, I wanted to emphasize that if training were implemented for the emotional labor force, it would assist us to be conscious of our emotions, how to deal with them, and where to go if such situations arise.”(Participant 1, FGD 3)
“I wanted to make the point that it would be beneficial if we could have well-trained health professionals who could offer emotional support and conduct mental health and wellbeing screenings, as doing so could improve the standard of treatment provided to patients.”(Participant, 7 FGD 1)
4. Discussion
On the prevalence of emotional disturbance, the study findings showed that most of the healthcare workers were experiencing emotional disturbance during their work. The emotional disturbances varied from emotional tiredness to verbal abuse, sadness, and anger while others reported experiencing depression and physical abuse. Similar studies consistently found that burnout percentages were much higher in developing countries than in developed countries [9], especially in Sub-Saharan Africa [7]. Another study conducted in South Korea reported that about 11% of all workers handling angry clients had experienced depression [6] A study in Ghana in Sub-Saharan Africa found that 91.1% of healthcare workers reported experiencing moderate to high rates of emotional exhaustion [18]. In Ethiopia, the prevalence of emotional exhaustion was more than half among Nurses [19]. The variance in the prevalence of emotional disturbances among developing and developed countries could be related to the differences in health system processes. Unlike most developing countries, developed countries have good healthcare infrastructures, good sanitation, roads, transportation, and electricity [20]. There are also differences in terms of shortages of human and material resources between developed and developing countries. In Malawi, a doctor serves 18000 people compared to approximately 3 to 7 American or British doctors serving one citizen [21]. As a result, healthcare workers may be frustrated with such conditions in developing countries due to the shortage and maldistribution of healthcare workers [22].
The study found that the age and gender of the participant, department, experience, adequacy of staffing, work demand, high workload, cadre, and poor communication from managers on policy were associated with emotional disturbances. In Ghana, the practice environment of the nurses explained 39.6% of the variance in emotional exhaustion [18]. Similarly, in Brazil, a study found that nurses who experienced verbal and physical abuse and were concerned about workplace violence for the past 12 months had considerably higher risks of presenting high weariness, such as emotional exhaustion, depersonalization, and low professional accomplishment [[11]. In other studies, the duration of time spent working [23] and high workload [24] were related to emotional disturbances. This shows high workload is a major source of emotional disturbance. The high workload can be attributed to the shortage of healthcare workers to accommodate the high demands of patients in hospital settings.
The findings also demonstrate that difficult working conditions and job characteristics contribute to emotional disturbances. [25] highlights the importance of understanding how organizational policies and practices are translated into the work environment. Most of the healthcare workers reported that there is poor communication from managers on policy and work-related issues. The role of management in supporting employees through effective communication is necessary in reducing work stress. A Cochrane review of preventing occupation stress by applying work-directed interventions concluded that interventions that included communication or nursing delivery change are effective in reducing burnout, stress, and general symptoms in healthcare workers when compared to no intervention [26].
Being aware of emotions and how to control them, avoiding external forces, expressing thoughts, using high-level support, and use of religious support were some of the strategies to cope with emotional disturbances and job-related stress. Literature has shown that in the United Kingdom, most nurses who were able to cope with their emotions through access to emotional resources, such as emotional support and releases for thoughts and feelings, were less likely to experience emotional exhaustion [27]. In addition, in Australia community nurses who had more emotional intelligence (the capacity to be aware, control, and express one’s emotions and handle interpersonal relationships judiciously and with empathy) had less stress at work and were emotionally feeling better [12]. However, nurses who had low or no emotional intelligence reported poorer levels of well-being and more job stress [12]. In Sub-Saharan Africa; and Ghana, five main strategies were employed by nurses and midwives to deal with emotional disturbances including psychological capital, reutilization of emotions, religious resources, social support, and job security [13].
The study found that the majority of healthcare workers were not trained on coping strategies for emotional disturbances at the workplace. Emotion-focused and problem-focused approaches were identified to be used to cope with emotional exhaustion. Similarly, in Middle East Africa nursing students were found to utilize problem-focused (dealing with the problem), emotion-focused (regulating the emotion), and dysfunctional (venting the emotions) stress coping mechanisms to alleviate their stress [14]. It is important to equip healthcare workers with knowledge and skills on coping with emotional disturbances to improve their well-being and performance at work
5. Conclusions
The study aimed at analyzing the well-being of healthcare workers including nurses, clinicians, and medical doctors at Rumphi District Hospital in Malawi. Emotional disturbance is a common problem among healthcare workers, affecting more than three-quarters of the healthcare workers. Emotional tiredness was associated with the department, work demand, experience, cadre, staffing, and knowledge of policies. Being aware of emotions and controlling them was the common coping strategy. However, most healthcare workers did not receive formal training or refresher courses on coping skills for emotional disturbances.
Funding
The authors declare that they did not request or use any source of funding.
Acknowledgments
We would like to express our deepest gratitude to the Rumphi Directorate of Health and Social Services for reviewing this study and providing us with a letter of permission to conduct the study at Rumphi District Hospital. They made this research possible.
Declaration for Human Participants
This study was approved by the University of Livingstonia Research and Ethics Committee Review Board (ethical clearance number: UNILIA-REC/UGC/56/2023) and Rumphi District Health Research Committee including the Directorate of Health and Social Services (DHSS) of Rumphi district in Malawi. The principles of the Helsinki Declaration were followed.
Conflicts of Interests
The authors declare that they have no competing interests.
Data availability
The data that support the findings of this study are available on request from the corresponding author.
Authors’ contributions
BMW and DN conceived the study, wrote the original draft, and conducted data analysis. DZ reviewed the original draft. MS edited the manuscript and provided critical comments.
References
- Hochschild AR. The Managed Heart: Commercialization of Human Feeling. Berkeley: University of California Press; 2012.
- Dubale BW, Friedman LE, Chemali Z, Denninger JW, Mehta DH, Alem A, Fricchione GL, Dossett ML, Gelaye B. Systematic review of burnout among healthcare providers in sub-Saharan Africa. BMC public health. 2019 Dec;19:1-20. [CrossRef]
- Liu L, Xu P, Zhou K, Xue J, Wu H. Mediating role of emotional labor in the association between emotional intelligence and fatigue among Chinese doctors: a cross-sectional study. BMC public health. 2018 Dec;18:1-8. [CrossRef]
- Bureau of Labor Statistics. Labor force statistics from the current population survey. https://www.bls.gov/cps/. 2018.
- Kim MH, Mazenga AC, Yu X, Simon K, Nyasulu P, Kazembe PN, Kalua T, Abrams E, Ahmed S. Factors associated with burnout amongst healthcare workers providing HIV care in Malawi. PLoS One. 2019 Sep 24;14(9):e0222638. [CrossRef]
- Suh C, Punnett L. High emotional demands at work and poor mental health in client-facing workers. International Journal of Environmental Research and Public Health. 2022 Jun 20;19(12):7530. [CrossRef]
- Owuor RA, Mutungi K, Anyango R, Mwita CC. Prevalence of burnout among nurses in sub-Saharan Africa: a systematic review. JBI Evidence Synthesis. 2020 Jun 1;18(6):1189-207. [CrossRef]
- Koen L, Niehaus DJ, Smit IM. Burnout and job satisfaction of nursing staff in a South African acute mental health setting. South African Journal of Psychiatry. 2020;26. [CrossRef]
- Ahmed F, Hawulte B, Yuya M, Birhanu S, Oljira L. Prevalence of burnout and associated factors among health professionals working in public health facilities of Dire Dawa city administration, Eastern Ethiopia. Frontiers in Public Health. 2022 Aug 11;10:836654. [CrossRef]
- Singano FK, Mazengera R, Mbendela I, Singano V. High burnout among maternity healthcare workers in Zomba and Lilongwe, Malawi [Internet]. Research Square. 2023. Available from: https://www.researchsquare.com/article/rs-3032062/v1.
- Tsukamoto SA, Galdino MJ, Barreto MF, Martins JT. Burnout syndrome and workplace violence among nursing staff: a cross-sectional study. Sao Paulo Medical Journal. 2021 Dec 17;140:101-7. [CrossRef]
- Karimi L, Leggat SG, Donohue L, Farrell G, Couper GE. Emotional rescue: The role of emotional intelligence and emotional labour on well-being and job-stress among community nurses. Journal of advanced nursing. 2014 Jan;70(1):176-86. [CrossRef]
- Lartey JK, Osafo J, Andoh-Arthur J, Asante KO. Emotional experiences and coping strategies of nursing and midwifery practitioners in Ghana: a qualitative study. BMC nursing. 2020 Dec;19:1-2. [CrossRef]
- Chaabane S, Chaabna K, Bhagat S, Abraham A, Doraiswamy S, Mamtani R, Cheema S. Perceived stress, stressors, and coping strategies among nursing students in the Middle East and North Africa: an overview of systematic reviews. Systematic reviews. 2021 May 5;10(1):136. [CrossRef]
- Gross JJ. Emotion regulation: Past, present, future. Cognition & emotion. 1999 Sep 1;13(5):551-73. [CrossRef]
- National Statistical Office. 2018 Malawi Population and Housing Census. [Internet]. 2019. Available from: http://www.nsomalawi.mw/images/stories/data_on_line/demography/census_2018/2018%20Malawi%20Population%20and%20Housing%20Census%20Main%20Report.pdf.
- Yamane, T. Statisics An Introductory Analysis. New York. 1967;2.
- Blankson-Stiles-Ocran S, Amissah EF, Mensah AO. Determinants of emotional labour among employees in the hospitality industry in Accra, Ghana. AJHTM. 2019 Jun 19;1(1):48–66. [CrossRef]
- Hailay A, Aberhe W, Mebrahtom G, Zereabruk K, Gebreayezgi G, Haile T. Burnout among Nurses Working in Ethiopia. Behav Neurol. 2020;2020:8814557. [CrossRef]
- Peters DH, Chakraborty S, Mahapatra P, Steinhardt L. Job satisfaction and motivation of health workers in public and private sectors: cross-sectional analysis from two Indian states. Hum Resour Health. 2010 Dec;8(1):27. [CrossRef]
- Kawale P, Pagliari C, Grant L. What does the Malawi Demographic and Health Survey say about the country’s first Health Sector Strategic Plan? Journal of Global Health. 2019 Jun;9(1):010314.
- Ahmat A, Okoroafor SC, Kazanga I, Asamani JA, Millogo JJS, Illou MMA, et al. The health workforce status in the WHO African Region: findings of a cross-sectional study. BMJ Glob Health. 2022 May;7(Suppl 1):e008317. [CrossRef]
- Dias JC, Silva SC, Rosario A. Emotional labor in healthcare: the role of work perceptions and personality traits. Academy of Strategic Management Journal. 2022;21(6).
- Portoghese I, Galletta M, Leiter MP, Cocco P, D’Aloja E, Campagna M. Fear of future violence at work and job burnout: A diary study on the role of psychological violence and job control. Burnout Research. 2017 Dec;7:36–46. [CrossRef]
- Poku CA, Donkor E, Naab F. Determinants of emotional exhaustion among nursing workforce in urban Ghana: a cross-sectional study. BMC Nurs. 2020 Dec;19(1):116. [CrossRef]
- Marine A, Ruotsalainen J, Serra C, Verbeek J. Preventing occupational stress in healthcare workers. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD002892.
- Kinman G, Leggetter S. Emotional Labour and Wellbeing: What Protects Nurses? Healthcare (Basel). 2016 Nov 30;4(4):89.

Table 1.
Demographic characteristics of participants.
| Variable | n | Proportion | 95% LCL | 95% UCL |
| Gender | ||||
| Male | 33 | 39% | 29% | 50% |
| Female | 51 | 61% | 50% | 71% |
| Age range in years | ||||
| 20 - 29 | 23 | 27% | 19% | 38% |
| 30 - 39 | 40 | 48% | 37% | 58% |
| 40 - 49 | 16 | 19% | 12% | 29% |
| 50 - 59 | 5 | 6% | 2% | 14% |
| Education level | ||||
| Certificate | 9 | 11% | 6% | 19% |
| Diploma | 57 | 68% | 57% | 77% |
| Degree | 18 | 21% | 14% | 32% |
| Marital status | ||||
| Single | 33 | 39% | 29% | 50% |
| Married | 51 | 61% | 50% | 71% |
| Work experience | ||||
| Less than five years | 37 | 44% | 34% | 55% |
| Five to ten years | 27 | 32% | 23% | 43% |
| Ten years above | 20 | 24% | 16% | 34% |
| Cadre | ||||
| Nurse | 62 | 74% | 63% | 82% |
| Clinician | 20 | 24% | 16% | 34% |
| Medical doctor | 2 | 2% | 1% | 9% |
| Department | ||||
| Male ward | 9 | 11% | 6% | 19% |
| Maternity | 31 | 37% | 27% | 48% |
| Pediatric | 10 | 12% | 6% | 21% |
| Female ward | 8 | 10% | 5% | 18% |
| OPD | 23 | 27% | 19% | 38% |
| Theater | 3 | 4% | 1% | 11% |
| LCL = Lower Confidence Level, UCL = Upper Confidence Level | ||||
Table 2.
Prevalence of emotional disturbances.
| Never | 1 - 5 times a month | > 5 times a month | ||
| Emotional disturbance | (n, %) | (n, %) | (n, %) | p value |
| Emotionally tired | 11(13%) | 50(60%) | 23(27%) | <0.001* |
| Depression | 62(74%) | 18(21%) | 4(5%) | <0.001* |
| Verbal abuse | 10(12%) | 49(58%) | 25(30%) | <0.001* |
| Physical abuse | 81(96%) | 3(4%) | <0.001* | |
| Stress and anger | 10(12%) | 48(57%) | 26(31%) | <0.001* |
Table 4.
Factors associated with emotional disturbance.
| Emotionally tired | Depression | Verbal abuse | Physical abuse | Stress and anger | |
| Variable | χ2(p value) | χ2 (p value) | χ2 (p value) | χ2 (p value) | χ2 (p value) |
| Sex | 2.321 (0.313) | 4.951 (0.084**) | 1.565 (0.457) | 0.046 (0.830) | 4.208 (0.122) |
| Age | 12.027 (0.061**) | 13.536 (0.035*) | 7.947 (0.242) | 4.874 (0.181) | 12.358 (0.054**) |
| Education | 6.226 (0.183) | 9.225 (0.056**) | 2.307 (0.679) | 0.54 (0.763) | 3.611 (0.461) |
| Experience | 5.44 (0.245) | 11.113 (0.025*) | 3.258 (0.516) | 1.104 (0.576) | 10.450 (0.033*) |
| Cardre | 3.302 (0.509) | 9.685 (0.046*) | 3.693 (0.449) | 1.104 (0.576) | 5.761 (0.218) |
| Department | 8.477 (0.004*) | 17.33 (0.067**) | 14.98 (0.035*) | 2.876 (0.071**) | 27.472 (0.002*) |
| Work environment | 5.433 (0.246) | 5.751 (0.218) | 5.183 (0.269) | 0.203 (0.903) | 5.888 (0.208) |
| Staffing | 2.358 (0.308) | 10.733 (0.005*) | 2.099 (0.350) | 0.283 (0.595) | 2.069 (0.355) |
| Policies | 6.381 (0.172) | 4.779 (0.311) | 1.786 (0.775) | 12.913 (0.002*) | 2.046 (0.727) |
| Work demand | 2.102 (0.047*) | 9.786 (0.044*) | 4.453 (0.348) | 0.789 (0.674) | 16.384 (0.003*) |
| **Association is significant at p<0.1 level (2-tailed). *Association is significant at p<0.05 level (2-tailed) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



