Submitted:
20 June 2024
Posted:
21 June 2024
You are already at the latest version
Abstract
Whole body electromyostimulation (WB-EMS) is frequently presented as a safe and attractive training technology, however evidence for this description is vague. Thus, the present study aimed to provide an overview of different aspects related to safety and attractiveness of WB-EMS in non-athletic cohorts. A systematic review of the literature according to PRISMA searched five electronic databases, two study registers and google scholar without language restrictions. Briefly, WB-EMS studies that reported adverse effects, loss to follow, withdrawal or attendance rates in non-athletic cohorts were included. Finally, 58 eligible studies were eligible. All studies applied low-frequency WB-EMS predominately 1-2x 20-25 min/week. Seventeen studies provided a superimposed protocol. While no study (n=56) reported serious adverse effects, four studies observed abnormal laboratory findings, albeit without clinical relevance. Loss to follow-up (10±11%) and withdrawal rate (5±6%) of WB-EMS trials were low, but did not differ from data for the non-training (10±12% and 4±6%) or exercise control groups (12±11% and 7±8%). In parallel, we observed high attendance rates (94±7%) in the WB-EMS groups that again did not relevantly vary from findings for the exercising control groups (n=20; 91±7%). WB-EMS can indeed be considered as a safe and attractive training technology for non-athletic cohorts, be it with or without health problems.
Keywords:
Electromyostimulation
; intervention
; safety
; attractiveness
; adherence
1. Introduction
Whole-body electromyostimulation (WB-EMS) is a novel training technology [1] that is gaining increasing attention in non-athletic cohorts [2]. While many studies have addressed outcomes related to physical fitness, function or the health-related domain [3], there has so far been no scoping review that summarized outcomes related to safety and attractiveness of WB-EMS application. Beside effectiveness, safety is considered the key aspect of exercise interventions in the physical fitness and health domain. Attractiveness of an intervention might be best indicated by low loss to follow-up or (even more applicable) withdrawal and high attendance rates, i.e. people vote on a program's attractiveness with their feet. The impact of such attractiveness of an exercise protocol might be underestimated. However, while low attendance rates weaken or even prevent the effectiveness of an exercise program on a given outcome, high withdraw rates question the entire applicability of the exercise protocol. Due its low orthopedic burden, joint friendliness, low voluntary effort, time effectiveness and consistent supervision [1], WB-EMS might be a particularly attractive and safe training technology for non-athletic cohorts. Thus, in the present review we aimed to determine safety and attractiveness of WB-EMS interventions in sedentary to non-athletic cohorts.
2. Materials and Methods
The present review is based on the systematic review of Beier et al. [2] which focuses on outcomes addressed by WB-EMS. Briefly, this systematic literature review searched five electronic databases (Medline, The Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing & Allied Health, SPORTDiscus, Physiotherapy Evidence Database) and two study registers (Clinical trial.gov and the ICTRP] published up to 6th March 2023 without language restrictions. Articles not published in English or German were translated by native speakers or using use online translators (e.g. https://www.deepl.com/home). To identify additional study reports, Google Scholar was searched manually. The full strategies can be found in supplemental table S1 (Appendix).
2.1. Selection Process
Titles, abstracts and full texts were independently screened by two reviewers according to the pre-specified eligibility criteria. Reasons for excluding ineligible studies were recorded. In the case of missing data or doubtful information, authors were contacted for a maximum of three times within a six-week period.
2.2. Eligibility Criteria
The eligibility criteria of the present slightly vary from the underlying work of Beier et al. [2]. This particularly refers to the PICOS criteria of intervention, outcome and study design.
2.2.1. Population
Only “non-athletic” cohorts were included. Studies that focus on athletes or sport students were excluded. However, recreational sports persons were accepted. We also excluded studies that focus on inpatient cohorts.
2.2.2. Intervention
Only studies that applied Whole-Body Electromyostimulation (WB-EMS) defined as “simultaneous application of electric stimuli via at least six current channels or participation of all major muscle groups, with a current impulse effective to trigger muscular adaptation” [1] were included.
2.2.3. Comparators
Type or even presence of a control group was not considered as an eligibility criterion.
2.2.4. Outcomes
In the present analysis on attractiveness and safety of WB-EMS, we included studies that reported participant loss to follow-up and/or attendance rates and/or adverse effects during or related to the WB-EMS interventions. Due to the fact that drop-out and loss to follow-up were frequently used synonymously, we subsumed the data under “loss to follow-up (FU)” fully aware that that the terms are not fully congruent. Where authors did not report loss to FU but gave the number of participants participating in pre- and post-tests, corresponding differences were considered as loss to FU. Potentially more important for the present topic of “attractiveness”, people who quit the study for personal reasons (e.g. loss of interest, lack of time, aversion to or discomfort with the intervention) were included under “withdrawals”. Hence, loss to follow up related to death, relocation, COVID-19 lock down, pregnancy, health problems or injuries not related to the WB-EMS application were not considered as withdrawal. However, participants reported as lost to FU for “other reasons” or “unknown reasons” were classed as withdrawals. If no loss to FU (i.e. n=0) was reported or evident, withdrawal was also considered as n=0, even if this aspect was not addressed. On the other hand, when no data on withdrawal were reported or evident, we transferred the loss to FU rate. Safety was predominately determined by adverse effects or laboratory findings reported by the trials. “Adverse effects” (AE) was defined as any untoward medical occurrence, disease or injury or any untoward clinical signs, including an abnormal laboratory finding (ALF) related to the WB-EMS application.
2.2.5. Study Design
We included all longitudinal study designs except single case studies. Review articles, editorials, conference abstracts, and letters were not considered, either. Only peer reviewed types of scientific work were accepted, i.e. bachelor, master, or doctor thesis were not considered.
2.3. Data management
Search results were downloaded and imported to Endnote. Duplicates were identified and excluded using the method proposed by Bramer et al. [4]. Title and abstract screening as well as full-text screening was conducted using Endnote. In cases of comprehensive projects (e.g. FitAging [5], TEST III [6], FORMOSA [7], FRANSO [8]) with multiple publications that all reported the outcomes addressed by the present, only the main publication was included.
2.4. Data Items
Two reviewers extracted relevant study, participant, and intervention characteristics of the included studies using a Microsoft Excel table. The table was structured into several domains. Publication characteristics refer to the study type, first author, year and country of the publication. Study characteristics included, for example, the number of study arms, sample size in WB-EMS and control group, type of comparator (predominately sedentary or active control) and methodologic quality of the studies as determined by the Physiotherapy Evidence Database (PEDro) Scale Risk of Bias Tool [9]. Intervention characteristics include (1) mode of application; (2) duration of the WB-EMS trial (in months); training frequency (sessions/week) and length of the session (in min); (3) impulse type (mono / bipolar), impulse frequency (in Hz), impulse breadth (in µs), impulse intensity, impulse application (continuous or intermitted impulse), length of the impulse phase (in s) and, if applied, intermittent impulse breaks (in s).
Special emphasis was placed on cohort characteristics that include in particular gender, age, BMI, baseline training status, conditions and diseases and particular loss to follow-up, withdrawals, attendance rates and adverse effects of the intervention(s).
2.5. Quality Assessment
The included studies were assessed for risk of bias by two independent reviewers applying the PEDro scale [9] specifically dedicated to physiotherapy and/or exercise studies. Studies with 5 points were considered low, 5-7 points moderate and >7 points were classified as high methodological quality studies [10].
2.6. Data Synthesis
Results are displayed for all studies in tables showing publication and study characteristics, exercise and stimulation characteristics and cohort/participant characteristics of the studies including loss to FU, withdrawals, adherence to the WB-EMS protocol and adverse effects of the intervention. In studies [11,12,13,14,15,16,17,18,19,20,21] that implemented two or more WB-EMS groups (e.g. WB-EMS with or without adjuvant exercise/diet), we summarized the results of the WB-EMS groups. If not already specified in the article, loss to follow up and withdrawal rate were calculated based on the initial sample size allocated to the study group at baseline. In parallel, mean average attendance/participation of the cohorts (i.e. WB-EMS, active control) was calculated and given as attendance rate (%). In order to show differences between the WB-EMS-groups and active or physically widely inactive control groups we applied non-parametrical statistical tests for group comparison in a few cases.
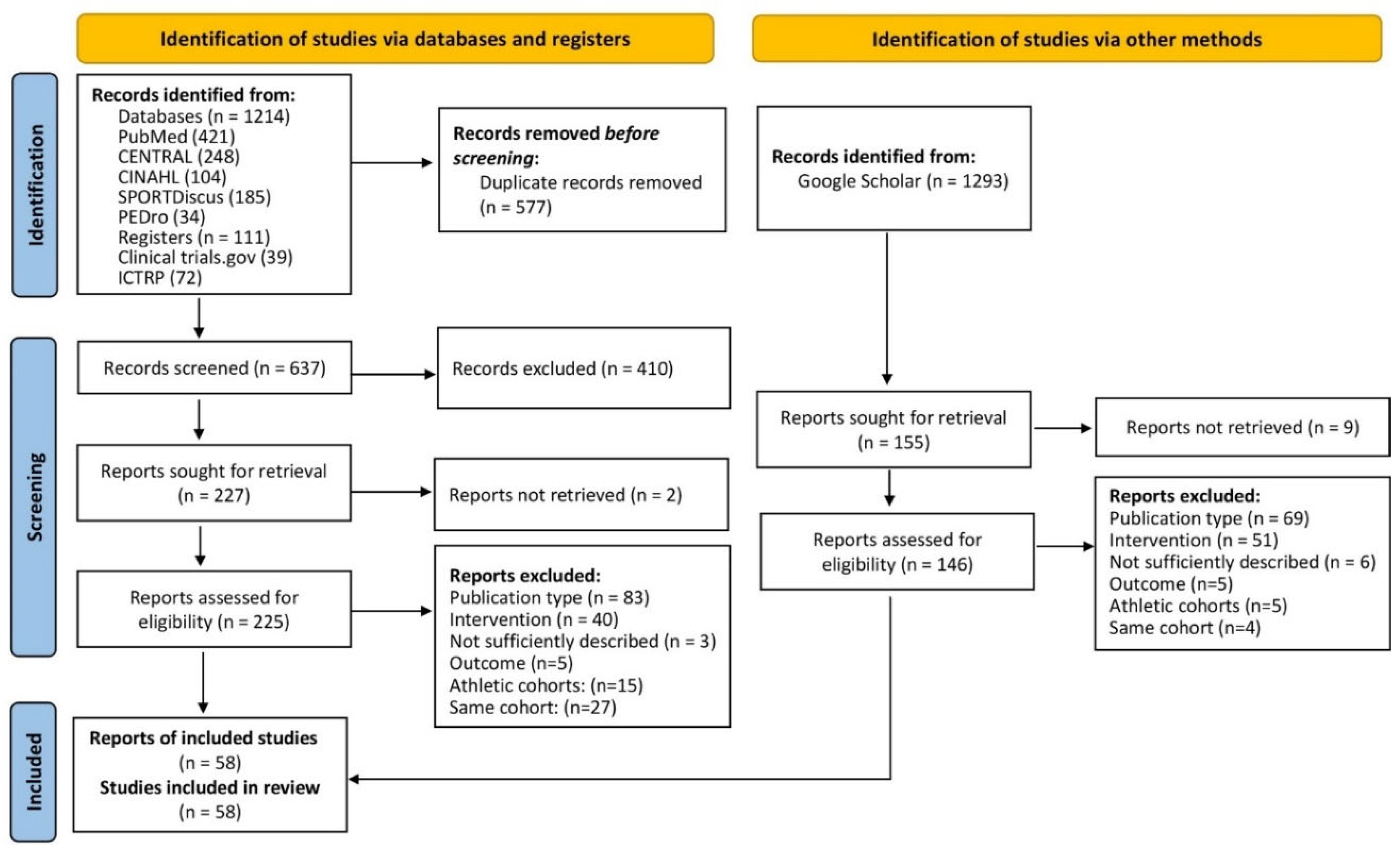
3. Results
In summary, 58 eligible studies were included [5,6,7,8,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64].
Figure 1.
Flow chart of the search process according to the PRISMA 2020 statement [80].
Figure 1.
Flow chart of the search process according to the PRISMA 2020 statement [80].
3.1. Study and Participant Characteristics
The majority of the studies (n=45) were designed as RCTs. Nine studies applied non-randomized controlled study designs, the remaining four trials applied a single group design without control group [27,31,57,60]. The number of study arms vary from one [27,31,57,60] to four [5,33,47,49]. The number of participants per study arm varies between five [22] and 96 [54]. Most studies were conducted in Europe (n=37) or Asia (n=18). The remaining three studies were completed in Brazil. About three quarters of the studies were published during the last 5 years. The methodological quality according to PEDro [9] varies between 3 and 9 points (Table 1).
Most projects included all genders, 38% focus on female and eleven projects addressed only male participants. The majority of the studies included cohorts largely independent of age. About half of the studies included participants 65 years and older. The oldest cohorts were close to 80 years old [7,65], the youngest cohorts were close to 20 years [17]. Twenty-five cohorts (43%) can be considered “healthy”; more than half of the cohorts were predominantly or exclusively overweight or obese (i.e. BMI mean ≥25 kg/m2). Most study cohorts (59%) included sedentary or at least untrained (i.e. no frequent exercise prior to the study) participants, 14 study cohorts can be considered as being moderately trained (1-2 sessions/week prior to the study) and six projects included [23,35,38,48,52,57] well trained (>2 sessions/week prior to the study) participants.
3.2. Intervention Characteristics
Intervention length averaged 11.3±7.4 weeks (range: 1-12 months). Training frequency per week vary between one [7,39,40,41,53,56] and five sessions [50] per week (2.0±0.8 sessions per weeks), however most studies (72%) applied a weekly WB-EMS frequency between 1.5 and 3 sessions. Length of the WB-EMS session usually (90%) ranged between 15-25 min, however four studies [37,43,46,47] provided 40-45 min of WB-EMS/session. All trials specified low frequency WB-EMS with an impulse frequency of between seven and 85 Hz. However, most studies (85%) applied the standard protocol [66] of 80-85 Hz with an impulse-width of 350-400 µs. The vast majority of studies applied intermitted WB-EMS with 2-6 s of impulse and 2-4 s of impulse break. Only a few studies used longer impulse bouts [42,53] or continuous impulse [30,53].
Of high relevance for the present topic, at least 17 studies applied “superimposed WB-EMS” i.e. either conventional exercise superimposed by WB-EMS or WB-EMS-protocols with adjuvant intensive dynamic or isometric exercises. (e.g. [5,15,17,22,23,29,30,32,37,38,43,44,45,46,47,53]. In parallel, mixed WB-EMS and conventional exercise programs (predominately DRT) were applied by few studies (e.g. [23,35]). The majority of studies that applied superimposed WB-EMS provided the corresponding exercise program for the control group. Although difficult to decide, most studies applied WB-EMS with slight voluntary movements. Of relevance, the majority of studies (n=30) implemented active control groups, three studies [5,40,49] compared the WB-EMS study arm with at least two active control groups. Most studies applied conventional exercise (predominately resistance exercise) in their active control group, two studies specified whole body vibration [34,40].
3.3. Study Outcomes
3.3.1. Loss to Follow-Up, Withdrawals
In summary, 56 studies either reported data at least for the WB-EMS or responded to our query or enabled loss to FU rates to be calculated from study data included. Mean value of loss to FU up in the WB-EMS groups averaged 9.7 ± 11.6%. While many studies (n=19) either reported no loss to follow up (or data indicated that no participants were lost), two studies with advanced cancer patients reported 40% [54] and 59% [55] loss to FU predominately due to disease progression, unplanned surgery or death. When comparing the WB-EMS subgroups with the 27 inactive control groups (9.6 ± 11.9%, range: 0% to 36%) no significant differences of loss to follow up rates were observed. In parallel, for the 36 active control groups an average loss to FU of 11.7 ± 10.9% (range 0% to 33%) was computed, not significantly different from the WB-EMS groups. A more detailed comparison that included studies with WB-EMS and inactive control (11.9 ± 14.1% vs. 9.6 ± 11.9%) or studies that compared WB-EMS with active control groups (8.5 ± 8.3% vs. 11.0 ± 11.0%) revealed no significant differences (p≥.131).
Unfortunately, only the minority of studies reported reasons for loss to FU in detail. Nevertheless summarizing the studies that allow assessment of withdrawal rates in the WB-EMS group the average was 4.8 ± 6.2% (range: 0 to 21%). Corresponding withdrawal rates in the inactive (n=24) or active control groups (n=33) were 3.9 ± 6.4% (0 to 23%) and 6.7 ± 8.3% (0 to 33%). Again a dedicated comparison of WB-EMS vs. inactive or active CG including only studies that implemented the groups did not indicate relevant differences between WB-EMS and inactive CG (4.0 ± 5.6% vs. 3.9 ± 6.4%, p=.959) or active CG (5.1 ± 6.2 vs. 6.0 ± 8.3%, p=.633).

Table 2.
Loss to follow-up and withdrawal rates of the trials.
| Author | Exercise Type active CG |
Loss to FU WB-EMS (%)3 |
Loss to FU CG (%) |
Loss to FU active CG (%) |
Withdrawal WB-EMS (%) | Withdrawal CG (%) |
Withdrawal active CG (%) |
|---|---|---|---|---|---|---|---|
| Akcay et al [11] | WB-EMS with or without diet | 0 | n.a. | n.a. | 0 | n.a. | n.a. |
| Almada et al [22] | Functional training | 0 | ----- | 0 | 0 | ----- | 0 |
| Amaro-Gahete et al. [23] | Running | 14 | ------ | 14 | 14 | ------ | 14 |
| FIT-Aging, Amaro-Gahete et al [5] | HIT AET + DRT | 17 | 36 | HIT: 30 | 8 | 9 | HIT: 22 |
| WHO PAR | PAR: 24 | PAR: 19 | |||||
| Andre et al [24] | Inactive CG | 15 | 5 | ------ | 10 | 5 | ------ |
| Bellia et al [25] | Inactive CG | 23 | 8 | ------ | n.g. | n.g.. | ------ |
| Berger et al [13] | Inactive CG | 12 | 13 | ------ | 5% | 0 | ------ |
| Blöckl et al [12] | All groups: WB-EMS | 12 | n.a. | n.a. | 8% | n.a. | n.a. |
| Bostan et al [26] | DRT | n.a. | ------ | n.a. | n.g. | ------ | n.a. |
| DiCagno et al [14] | Inactive CG | 0 | 0 | ------ | 0 | 0 | ------ |
| Dyaksa et al [27] | No CG | n.g. | ------ | ------ | n.g. | ------ | ------ |
| Ethem et al [28] | Inactive CG | 0 | 0 | ------ | 0 | 0 | ------ |
| Evangelista et al [30] | DRT | 16 | 0 | 16 | 16 | 0 | 15 |
| Evangelista et al [29] | Funktional Training | 33 | ------ | 33 | 20 | ------ | 33 |
| Fritzsche et al [31] | No CG | 0 | ------ | ------ | 0 | ------ | ----- |
| Ghannadi et al [32] | Aerobic exercise | 15 | ------ | 30 | 5 | ------ | 20 |
| Houdjijk et al [33] | No CG | 0 | ------ | ------ | 0 | ------ | ------ |
| Jee et al [15] | Inactive CG | 5 | 0 | ------ | 5 | 0 | ------ |
| Junger et al [16] | WB-EMS with or without diet | 0 | n.a. | n.a. | 0 | n.a. | n.a. |
| TEST I, Kemmler et al [35] | DRT | 0 | ------ | 0 | 0 | ------- | 0 |
| TEST II Kemmler et al [34] | WBV | 7 | ------ | 29 | 0 | ------ | 0 |
| HIT vs EMS, Kemmler et al [36] | DRT | 9 | ------ | 13 | 4 | ------ | 9 |
| FORMOSA; Kemmler et al [7] | Inactive CG | 10 | 12 | ----- | 4 | 4 | ----- |
| FRANSO, Kemmler et al [8] | Inactive CG/Protein CG | 9 | 7 | ------ | 5 | 4 | ------ |
| Kim et al [37] | Dance, RT, Stretching | 13 | ------ | 20 | 7 | ------ | 13 |
| Kim et al [17] | Isometric RT | 7 | ------ | 7 | 7 | ------ | 0 |
| Kiriscioglu et al [38] | Inactive CG | 0 | 0 | ------ | 0 | 0 | ------ |
| Konrad et al 1 [39] | Multimodal therapy | 6 | ---- | 5 | 0 | ----- | 0 |
| Ludwig et al [18] | Inaktive CG | 10 | 6 | ------ | 2 | 0 | ------ |
| Micke et al [40] | Whole Body Vibration | 9 | ------ | 13 | 3 | ------ | 5 |
| DRT | 13 | 8 | |||||
| Müllerova et al [41] | DRT | 18 | ------ | 20 | 18 | ------ | 20 |
| Öktem et al. [42] | DRT | 0 | ------ | 0 | 0 | ------ | 0 |
| Özdal et al [19] | WB-EMS with or without exercises | 0 | n.a. | n.a. | 0 | n.a. | n.a. |
| Pano-Rodriguez et al [81] | DRT | 6 | ------ | 6 | 6 | ------ | 6 |
| Park et al [46] | Aerobic dance | 6 | ------- | 6 | 6 | ------ | 6 |
| Park et al [45] | Isometric RT | 7 | 7 | 7 | 0 | 0 | 0 |
| Park et al [44] | Low intensity RT | 8 | --- | 0 | 8 | ------ | 0 |
| Park et al [47] | Step Aerobic | 7 | 7 | 0 | 7 | 0 | 0 |
| Qin et al [48] | DRT | 15 | ------ | 25 | 15 | ------ | 8 |
| Reljic et al [49] | HIT-DRT, 1 set protocol | 26 | 26 | 1 set: 18 | 13 | 23 | 1 set: 11 |
| HIT-DRT, 3 set protocol | 3 set: 21 | 3 set 13 | |||||
| Ricci et al [50] | Widely inactive CG | 0 | 0 | ------ | 0 | 0 | ------ |
| Sadeghipour et al [52] | DRT | 0 | 0 | 0 | 0 | 0 | 0 |
| Sadeghipour et al [51] | AE+DRT | 0 | 0 | 0 | 0 | 0 | 0 |
| Sanchez-Infante [53] | AE+DRT | 0 | ------ | 0 | 0 | ------ | 0 |
| Schink et al [54] | Inactive CG, diet | 40 | 31 | ------- | 14 | 17 | ------ |
| Schink et al [55] | Inactive CG, diet | 59 | 33 | ------ | 14 | 11 | ------ |
| Silvestri et al [20] | WB-EMS with or without stretching | 23 | n.a. | n.a | 21 | n.a. | n.a |
| Stephan et al [21] | WB-EMS with or without exercises | 7 | n.a. | n.a. | 7 | n.a. | n.a. |
| Teschler et al [57] | No CG | 0 | ------ | ------ | 0 | ------ | ------ |
| Teschler et al [56] | Local EMS (lower extremities) | 4 | 12 | 16 | 0 | 0 | 0 |
| Vacoulikova et al [58] | DRT | 18 | 0 | 20 | 18 | 0 | 20 |
| Vacoulikova et al [59] | DRT | 0 | 0 | 0 | 0 | 0 | 0 |
| van Buuren et al [61] | Local EMS (lower extremities) | 0 | 0 | 0 | 0 | 0 | 0 |
| van Buuren et al [60] | No CG | 0 | ------ | ------ | 0 | ------ | ------ |
| TEST III, von Stengel et al [6] | Low intensity gymnastics | 16 | ------ | 26 | 5 | ------- | 11 |
| Weissenfels et al [62] | Inactive CG | 7 | 7 | ------ | 0 | 7 | ------ |
| Willert et al [63] | Physical Activity | 3 | 17 | 10 | 0 | 13 | 7 |
| Zink et al [64] | Inactive CG | 33 | 33 | ------ | n.a | n.a. |
1 We compared the 4-week (multimodal therapy) versus 6-week (WB-EMS) assessment of Konrad et al. [39]; AET: Aerobic training; CG: Control group; DRT: Dynamic resistance exercise training; HIT: High intensity training; WHO-PAR: Physical activity recommendation World Health Organization.
3.3.2. Attendance Rate
Altogether 42 studies reported attendance rates at least for the WB-EMS study arm. Some authors responded to our queries but were unable to provide attendance rates retrospectively. This was the case particularly for the active control groups. A further few studies [30,41,58,59] excluded participants if the attendance rate failed to reach a certain level (<80%), thus the attendance rate was not applicable. In summary, mean attendance rate in the WB-EMS group averaged 94 ± 7% (range 77 to 100%). In detail, 15 studies reported a 100% attendance rate. Mean attendance rate of the 20 active CGs was comparably high (91 ± 7%, range: 72 to 100%). Five studies reported full attendance. A direct comparison of studies that reported attendance for the WB-EMS and active CG revealed no significant differences between the two study-arms (p=.142)
3.3.3. Adverse Effects
Five studies failed to report adverse effects related to the WB-EMS intervention [22,27,41,42,52] and did not respond to our queries. In summary, no study observed any acute events (e.g. stroke, cardiac arrest, renal failure), diseases (e.g. hypertension, cardiac arrhythmia), or musculoskeletal injuries (e.g. muscle rupture, muscle strain) related to WB-EMS or clinically relevant negative side effects. Nevertheless, a few studies did report abnormal laboratory findings. Particularly, the closely medically supervised trial of Teschler et al. [57] reported exceptionally high peak creatine kinase (MV: 23.940 IU/l) and myoglobin (MV: 2300 µg/l) levels, however without any other signs of severe rhabdomyolysis after very high (impulse) intensity WB-EMS in 25 young to middle aged healthy volunteers. But it should be noted that the aim of this study was to determine the amount of exertional rhabdomyolysis after inappropriate WB-EMS application in novice applicants and the repeated bout effects on creatine kinase and myoglobin after multiple WB-EMS applications. A sub-study [67] of the Franconian Sarcopenic Obesity (FRANSO) trial [8] that focused on safety determined slight but significant elevations of creatine kinase 140 IU/l after 16 weeks of combined WB-EMS and high-protein diet in Sarcopenic Obese elderly men. This was accompanied by a low-grade increase of creatine kinase–muscle brain (CK-MB) and high-sensitivity troponin (hsTnT) but without a higher risk of developing heart failure according to N-terminal prohormone of brain natriuretic peptide. Although a large number of biomarkers were sampled, no other negative side effects on renal or cardiac function were observed. In parallel, Schink et al. [54] reported significant post WB-EMS increases of CK from baseline to week 8 (with return to baseline level after 13 weeks), albeit below the 5-fold increase of resting CK levels considered as the threshold for (mild) rhabdomyolysis. More importantly, in his cohort of CHD patients, Fritsche et al. [31] reported a case of mild rhabdomyolysis (2770 IE/l) 24 h postexercise. In their study with NIDDM patients Houdijk et al. [33] listed two asymptomatic hypoglycaemia cases after WB-EMS application. In two further studies [8,36] one participant in each quit the study due to discomfort during WB-EMS. Unfortunately, data for adverse effects in active control groups are rare (Table 3). While about half of the studies implement an active control group, many studies did not adequately monitor adverse effects in their active control group. Further, most of the studies that applied superimposed WB-EMS scheduled the corresponding voluntary exercise for their active CGs, an approach that aggravates the interpretation of adverse effects. In summary however, the 26 studies with their 29 study groups either reported no adverse effects or retrospectively checked their patient data for their active CGs and recalled no serious adverse effects after our queries (n=11).
4. Discussion
Assessing parameters related to attractiveness and safety of WB-EMS by mean of a scoping review is a daunting task. Particular due to missing, inadequate or conflicting data, isolated WB-EMS without a control group and a divergent understanding of adverse effects it is difficult to determine the effect of WB-EMS application on parameters related to attractiveness and safety even in dedicated scientific settings. This particularly relates to the safety aspect of WB-EMS that was further complicated by the feature of superimposed WB-EMS and potential underreporting of adverse effects due to divergent definitions. Addressing the safety of WB-EMS by adverse effects none of the 58 trials reported “suspected unexpected serious adverse reaction” (SUSARs) during or after WB-EMS application. Nevertheless, four studies [31,54,57,67] reported abnormal laboratory findings after acute WB-EMS application or during the intervention. Two studies reported slight longitudinal increases of CK (1.6-fold after 16 weeks [67], 2.7-fold after eight weeks but normal after 12 weeks [54]) of WB-EMS with unclear clinical relevance. Further, Kemmler et al. [54] reported low but significant elevations of hsTnT and CK-MB, however not for NT-proBNP, which is considered as the more meaningful predictor of future events of heart failure [68]. Acute relevant side effects of WB-EMS were reported by two authors. While Fritsche et al. [31] observed one case of acute increase in CK indicating mild rhabdomyolysis, Teschler et al. [57] reported an average 96-fold CK increase after very intense WB-EMS in his cohort of novice WB-EMS applicants. Due to the intention of the latter study to focus on negative metabolic effects of excessive stimulus intensity in the early phase of WB-EMS training, the study finding of severe rhabdomyolysis (however without any clinical implication) can hardly be interpreted as an unexpected or unintended side effect. While the negative effect of too intensive WB-EMS on parameters related to rhabdomyolysis is well documented and addressed by an international guideline [69], the low orthopedic burden of WB-EMS per se might justify the expectation of decreased or absent musculoskeletal injuries. Unfortunately, this does not fully apply to superimposed WB-EMS [66] with its intensive adjuvant voluntary exercises. In contrast to WB-EMS, intervention-related adverse effects in studies that applied the correspondingly time-effective Whole-Body Vibration (WBV) technology were much more frequent. In their meta-analysis, de Oliveira et al. [70] reported adverse effects due to WBV in 6 of the 34 included WBV studies. Adverse effects involved injuries due to falls, complication of pre-existing orthopedic conditions, edema, knee and low back pain, dizziness, hypertension, forefoot inflammation and other less serious adverse effects (e.g. itching, erythema). Although the authors focus on an older (60 years+), potentially more vulnerable cohort, we conclude that the risk of adverse effects is considerably lower in WB-EMS compared with WBV, which addresses a similar target group. In summary and despite the aspect that the low number of abnormal laboratory findings and the entire absence of clinically relevant adverse effects in 58 WB-EMS groups (with about 500 patient years) might suggest underreporting, WB-EMS can be considered as a very safe training method based on the presently published data. Nevertheless, studies or registers that focus on adverse effects in commercial WB-EMS settings would be helpful to confirm our results.
While monitoring and reporting of “loss to follow-up” is a specified reporting criterion of RCTs [71], withdrawal rates were less frequently mentioned. This may be due to the uncertainty of what is to be regarded as withdrawal from an intervention. In exercise studies withdrawal is frequently considered as the voluntary discontinuation of physical activity with or without an associated medical cause [72]. However, withdrawal due to medical conditions is not really voluntary, thus we do not consider drop-out reasons related to medical conditions, pregnancy, COVID-19 lock-down(s) but also travel problems or relocation as withdrawal. In fact, our definition focuses on the “loss of interest”, “lack of time” and “discomfort with the intervention” aspect. We feel that a correspondingly applied withdrawal rate indicates the attractiveness of the training program more clearly, which is essential for the decision to transfer scientific studies to real world settings. In summary, we observed very low withdrawal rates in the WB-EMS group (5 ± 6%), even when considering the short intervention periods of about 11 weeks in average. However, withdrawal rates were similarly high compared to the inactive (4 ± 6%) and, more relevantly, to the active control groups (7 ± 8%). Withdrawal rates in usual fitness and health related settings are much higher [73,74,75]. Thus, we feel that the low withdrawal rate in the active control group might be largley motivated by study-related reasons (e.g. higher supervision, study nurse, limited study length). In contrast, the WB-EMS protocol applied in most studies was much closer to the real-world scenario of current WB-EMS concepts. This relates particularly to the consistently and closely supervised personal training approach of WB-EMS facilities, also recommended by the updated international guideline [69] (and respected by the vast majority of suppliers so far) and known to reduce drop-out [76,77].
Attendance rates can also be considered as a criterion of attractiveness of an intervention. In summary, we observed high attendance rates in the WB-EMS group (94 ± 7%) which, once again, did not differ significantly from data of the active CG (91 ± 7%). This result is supported by a study [36] which compared WB-EMS versus comparably time-effective HIT-RT that reported widely similar attendance rates (HIT-RT: 93 ± 7% versus WB-EMS: 90 ± 11%; p=.171) (Tab. 3). Attendance rates listed for supervised scientific studies on resistance exercise with comparable length and cohorts average around 80-90% [78], thus the high attendance rate in the predominately supervised active control groups is not a unique feature of this study. In parallel, a study that compared WB-EMS with a comparable time effective whole-body vibration [40] protocol reported similar attendance rates (WBV: 91 ± 7% versus WB-EMS: 92 ± 7%; p =.898). This finding is supported by the meta-analysis of de Oliveira et al. [70] that reported average attendance rates of 85% for WBV programs with people 60 years and older. Thus, although evidence for a superiority of WB-EMS versus other types of exercise or exercise technologies is limited, considering the 94% attendance rate determined by the present review, WB-EMS can be considered as a very attractive exercise technology.
Our review of the literature includes some limitations and features that might confound the easy interpretation of the results. Apart from the failure to consistently define adverse effects, loss to follow-up/withdrawal or attendance rate of several included studies, our classification of withdrawal rates might also be debatable. In short, we emphasize voluntary withdrawal due to reasons of low affinity to the WB-EMS application, which we see as a better indicator for the attractiveness of the intervention. Additionally our approach of refraining from a more quantitative approach (i.e. meta-analysis) might be open to question. However in the light of the inadequate and heterogeneous reference groups, we feel that a meta-analyses approach would not add further evidence for our findings. Another limitation is the new studies potentially not included due to their being published after March 2023. Nevertheless, the main issue refers to the generalization of our study results to the real world setting of commercial WB-EMS facilities. Considering that (for legal reasons) the vast majority of facilities (at least in Europe) fully respect the updated international guideline [69], commercial WB-EMS application closely reflects the protocol of scientific studies. This particularly includes the consistent and close supervision of the (maximum two) trainees by the certified trainer and the strict application of the rather restrictive contraindications [79]. Thus, we feel that the favorable data on safety (i.e. adverse effects) documented by the present study can be largely transferred to commercial facilities, or at least those compliant with current specifications. In parallel, the same can be said for the “attendance aspect” of the present study. As most WB-EMS suppliers contact clients in cases of missed sessions and permit alternative dates for cancelled or missed WB-EMS sessions free of charge, attendance rates in commercial WB-EMS can be considered as very high. This might also be substantiated by the non-negligible costs of commercial WB-EMS due to its personal training approach. On the other hand, in contrast to the free of charge scientific programs, withdrawal rates in commercial settings might be considerably higher. One may argue that the same is true for conventional exercise or WBV, but these types of exercise are usually much lower priced.
5. Conclusions
In summary, we provided evidence for safety, adherence and attractiveness of WB-EMS in non-athletic cohorts included in scientific studies. With respect to safety and attendance rates, evidence suggest to extend this finding on commercial settings that comply with present specifications on WB-EMS application. As a recommendation for future WB-EMS trials authors should place more emphasis on detailed reporting of adverse effects and reasons for loss to FU in all study arms.
Author Contributions
Conceptualization, WK, SvS, MU; methodology, WK, SvS; software, WK; validation, WK, SvS and MU; formal analysis, WK; investigation, WK, SvS; resources, MU; data curation, WK; writing—original draft preparation, WK; writing—review and editing, MU; visualization, WK; supervision, SvS.; project administration, WK. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
The authors acknowledge the support of all authors that provided missing data upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Table A1.
Search strategies and their results according to the underlying systematic search of Beier et al. [2].
Table A1.
Search strategies and their results according to the underlying systematic search of Beier et al. [2].
| Database | Search date | Search terms | Number of hits |
|---|---|---|---|
| Medline (PubMed) | 6th March 2023 | (WB-EMS[TIAB] OR “whole-body electromyostimulation”[TIAB] OR “whole body electromyostimulation”[TIAB] OR “whole-body electrostimulation”[TIAB] OR “whole body electrostimulation”[TIAB] OR electromyostimulation[TIAB] OR “EMS training”[TIAB] OR “EMS intervention”[TIAB] OR “EMS suit*”[TIAB] OR “EMS belt*”[TIAB] OR “B-SES”[TIAB] OR “belt electrode”[TIAB]) | 421 |
| CENTRAL | 6th March 2023 | (WB-EMS OR “whole-body electromyostimulation” OR “whole body electromyostimulation” OR “whole-body electrostimulation” OR “whole body electrostimulation” OR electromyostimulation OR “EMS training” OR “EMS intervention” OR “EMS suit*” OR “EMS belt*” OR “B-SES” OR “belt electrode”):ti,ab,kw | 248 |
| CINAHL | 6th March 2023 | 1. TI (WB-EMS OR “whole-body electromyostimulation” OR “whole body electromyostimulation” OR “whole-body electrostimulation” OR “whole body) electrostimulation” OR electromyostimulation OR “EMS training” OR “EMS intervention” OR “EMS suit*” OR “EMS belt*” OR “B-SES” OR “belt electrode” 2. AB (WB-EMS OR “whole-body electromyostimulation” OR “whole body electromyostimulation” OR “whole-body electrostimulation” OR “whole body) electrostimulation” OR electromyostimulation OR “EMS training” OR “EMS intervention” OR “EMS suit*” OR “EMS belt*” OR “B-SES” OR “belt electrode” 3. S1 OR S2 |
104 |
| SPORTDiscus | 6th March 2023 | 1. TI (WB-EMS OR “whole-body electromyostimulation” OR “whole body electromyostimulation” OR “whole-body electrostimulation” OR “whole body) electrostimulation” OR electromyostimulation OR “EMS training” OR “EMS intervention” OR “EMS suit*” OR “EMS belt*” OR “B-SES” OR “belt electrode” 2. AB (WB-EMS OR “whole-body electromyostimulation” OR “whole body electromyostimulation” OR “whole-body electrostimulation” OR “whole body) electrostimulation” OR electromyostimulation OR “EMS training” OR “EMS intervention” OR “EMS suit*” OR “EMS belt*” OR “B-SES” OR “belt electrode” 3. S1 OR S2 |
185 |
| PEDro | 6th March 2023 | Abstract & Title: “whole-body electromyostimulation” Method: clinical trial |
34 |
| Clinicaltrials.gov | 6th March 2023 | other terms: WB-EMS OR “whole-body electromyostimulation” OR “whole body electromyostimulation” OR “whole-body electrostimulation” OR “whole body electrostimulation” OR electromyostimulation OR “EMS suit*” OR “EMS belt*” OR “belt electrode*” | 39 |
| ICTRP | 6th March 2023 | Search: WB-EMS OR “whole-body electromyostimulation” OR “whole body electromyostimulation” OR “whole-body electrostimulation” OR “whole body electrostimulation” OR electromyostimulation OR “EMS suit*” OR “EMS belt*” OR “belt electrode*” | 72 |
| Google Scholar | 6th March 2023 | Advanced search: “whole body electromyostimulation” OR “WB EMS” OR “EMS suit” OR “belt electrode” with at least one of the words, anywhere in the article | 1293 |
References
- Kemmler, W.; Kleinoder, H.; Fröhlich, M. Editorial: Whole-Body Electromyostimulation: A Training Technology to Improve Health and Performance in Humans? Front Physiol. 2020, 11, 523. [Google Scholar] [CrossRef] [PubMed]
- Beier, M.; Schoene, D.; Kohl, M.; von Stengel, S.; Uder, M.; Kemmler, W. Non-athletic cohorts enrolled in longitudinal whole-body electromyostimulation trials - An evidence map. Sensors (Basel). 2024, 24, 972. [Google Scholar] [CrossRef] [PubMed]
- Le, Y.E.; Schoene, D.; Kohl, M.; von Stengel, S.; Uder, M.; Kemmler, W. Outcomes addressed by longitudinal whole-body electromyostimulation trials in middle aged-older adults - An evidence map. Japanese Journal of Medical Science. In print. 2023. [Google Scholar]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J Med Libr Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Amaro-Gahete, F.J.; De-la, O.A.; Jurado-Fasoli, L.; et al. Changes in Physical Fitness After 12 Weeks of Structured Concurrent Exercise Training, High Intensity Interval Training, or Whole-Body Electromyostimulation Training in Sedentary Middle-Aged Adults: A Randomized Controlled Trial. Front Physiol. 2019, 10, 451. [Google Scholar] [CrossRef] [PubMed]
- von Stengel, S.; Bebenek, M.; Engelke, K.; Kemmler, W. Whole-Body Electromyostimulation to Fight Osteopenia in Elderly Females: The Randomized Controlled Training and Electrostimulation Trial (TEST-III). J Osteoporos. 2015, 2015, 643520. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Teschler, M.; Weissenfels, A.; et al. Whole-body electromyostimulation to fight sarcopenic obesity in community-dwelling older women at risk. Resultsof the randomized controlled FORMOsA-sarcopenic obesity study. Osteoporos Int. 2016, 27, 3261–3270. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Weissenfels, A.; Teschler, M.; et al. Whole-body Electromyostimulation and protein supplementation favorably affect Sarcopenic Obesity in community-dwelling older men at risk. The Randomized Controlled FranSO Study. Clin Interv Aging. 2017, 12, 1503–1513. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Ribeiro de Avila, V.; Bento, T.; Gomes, W.; Leitao, J.; Fortuna de Sousa, N. Functional Outcomes and Quality of Life After Ankle Fracture Surgically Treated: A Systematic Review. J Sport Rehabil. 2018, 27, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Akçay, N.; Güney, H.; Kaplan, S.; Akgül, M. Electromyostimulation Exercise with Diet Program is More Effective on Body Composition than its Exercise without Diet. Mediterranean Journal of Sport Science. 2022, 4, 814–822. [Google Scholar]
- Bloeckl, J.; Raps, S.; Weineck, M.; et al. Feasibility and Safety of Whole-Body Electromyostimulation in Frail Older People-A Pilot Trial. Front Physiol. 2022, 13, 856681. [Google Scholar] [CrossRef]
- Berger, J.; Ludwig, O.; Becker, S.; Backfisch, M.; Kemmler, W.; Frohlich, M. Effects of an Impulse Frequency Dependent 10-Week Whole-body Electromyostimulation Training Program on Specific Sport Performance Parameters. J Sports Sci Med. 2020, 19, 271–281. [Google Scholar]
- di Cagno, A.; Buonsenso, A.; Centorbi, M.; et al. Whole body-electromyostimulation effects on serum biomarkers, physical performances and fatigue in Parkinson's patients: A randomized controlled trial. Front Aging Neurosci. 2023, 15, 1086487. [Google Scholar] [CrossRef]
- Jee, Y.-S. The effect of high-impulse-electromyostimulation on adipokine profiles, body composition and strength: A pilot study. J Isokinetics. 2019, 27, 163–176. [Google Scholar] [CrossRef]
- Junger, J.; Junger, A.; Ostrowski, P. Body composition of trainees undergoing EMS training with respect to their nutrition. Journal of Physical Education and Sport. 2020, 20, 97–101. [Google Scholar]
- Kim, K.; Eun, D.; Jee, Y.S. Higher Impulse Electromyostimulation Contributes to Psychological Satisfaction and Physical Development in Healthy Men. Medicina (Kaunas). 2021, 57, 197. [Google Scholar] [CrossRef]
- Ludwig, O.; Berger, J.; Becker, S.; Kemmler, W.; Frohlich, M. The Impact of Whole-Body Electromyostimulation on Body Posture and Trunk Muscle Strength in Untrained Persons. Front Physiol. 2019, 10, 1020. [Google Scholar] [CrossRef]
- Özdal, M.; Bostanci, Ö. Effects of whole-body electromyostimulation with and without voluntary muscular contractions on total and regional fat mass of women. Archives of Applied Science Research. 2016, 8, 75–79. [Google Scholar]
- Silvestri, A.; Ruscello, B.; Rosazza, C.; et al. Acute Effects of Whole-Body Electrostimulation Combined with Stretching on Lower Back Pain. Int J Sports Med. 2023, 44, 820–829. [Google Scholar] [CrossRef]
- Stephan, H.; Wehmeier, U.F.; Forster, T.; Tomschi, F.; Hilberg, T. Additional Active Movements Are Not Required for Strength Gains in the Untrained during Short-Term Whole-Body Electromyostimulation Training. Healthcare 2023, 11, 741. [Google Scholar] [CrossRef]
- Almada, R.; Molina Martín, J.J.; Tregón, P.S.; García, J.L. Comparación Entre los Efectos de un Programa de Entrenamiento de Fuerza Explosiva Mediante Bandas Elásticas y un Programa de Entrenamiento con Electro-Estimulación de Cuerpo Completo. Revista Kronos. 2016, 15. [Google Scholar]
- Amaro-Gahete, F.J.; De-la, O.A.; Sanchez-Delgado, G.; et al. Functional Exercise Training and Undulating Periodization Enhances the Effect of Whole-Body Electromyostimulation Training on Running Performance. Front Physiol. 2018, 9, 720. [Google Scholar] [CrossRef]
- Andre, L.D.; Basso-Vanelli, R.P.; Ricci, P.A.; et al. Whole-body electrical stimulation as a strategy to improve functional capacity and preserver lean mass after bariatric surgery: a randomized triple-blind controlled trial. Int J Obes (Lond). 2021, 45, 1476–1487. [Google Scholar] [CrossRef]
- Bellia, A.; Ruscello, B.; Bolognino, R.; et al. Whole-body Electromyostimulation plus Caloric Restriction in Metabolic Syndrome. Int J Sports Med. 2020, 41, 751–758. [Google Scholar] [CrossRef]
- Bostan, G.; Gümüş, M. Effects of fitness and electromyostimulation (EMS) training techniques on body composition [Antrenman Tekniklerinin Vücut Kompozisyonu Üzerine Etkileri]. Turkish Journal of Diabetes and Obesity. 2022, 6, 149–158. [Google Scholar] [CrossRef]
- Dyaksa, R.S.; Susilo, E.A.; Virdianto, A.W. The Effect of EMS Exercise on Body Circumstances in Sedentary Women [PENGARUH LATIHAN EMS TERHADAP LINGKAR TUBUH PADA WANITA SEDENTARY]. Journal of Physical Education, Sports and Health. 2022, 5, 264–270. [Google Scholar]
- Ethem, H.; Orhan, İ.; ÇAnakci, G. Investigation of the Effect of 6 Weeks Whole-Body Electromyostimulation and with Body Weight Strength Training on some Motoric Properties in Sedantery Women [Sedanter Kadınlarda Tüm Beden Elektromyostimülasyonla Kombine Dinamik Kuvvet Alıştırmalarının Bazı Motorik Özellikler Üzerine Etkisinin İncelenmesi]. Eurasian Research in Sport Science. 2019, 2, 83–96. [Google Scholar]
- Evangelista, A.L.; Alonso, A.C.; Ritti-Dias, R.M.; et al. Effects of Whole Body Electrostimulation Associated With Body Weight Training on Functional Capacity and Body Composition in Inactive Older People. Front Physiol. 2021, 12, 638936. [Google Scholar] [CrossRef]
- Evangelista, A.L.; Teixeira CV, S.; Barros, B.M.; et al. Does whole-body electrical muscle stimulation combined with strength training promote morphofunctional alterations? Clinics (Sao Paulo). 2019, 74, e1334. [Google Scholar] [CrossRef]
- Fritzsche, D.; Fruend, A.; Schenk, S.; et al. Elektromyostimulation (EMS) bei kardiologischen Patienten. Wird das EMS-Training bedeutsam für die Sekundärprävention? Herz. 2010, 35, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Ghannadi, S.; Halabchi, F.; Maleklou, F.; et al. The effect of 6 weeks electrical muscle stimulation training and aerobic exercise on body composition of overweight women: a randomized controlled study. Sport Sciences for Health. 2022, 18, 1387–1395. [Google Scholar] [CrossRef]
- Houdijk AP, J.; Bos, N.; Verduin, W.M.; Zwartkruis MA, L. Visceral fat loss by whole-body electromyostimulation is attenuated in male and absent in female older Non-Insulin-Dependent diabetes patients. Endocrinol Diabetes Metab. 2022, 5, e377. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Birlauf, A.; von Stengel, S. Einfluss von Ganzkörper-Elektromyostimulation auf das Metabolische Syndrom bei älteren Männern mit metabolischem Syndrom. Dtsch Z Sportmed. 2010, 61, 117–123. [Google Scholar]
- Kemmler, W.; Schliffka, R.; Mayhew, J.L.; von Stengel, S. Effects of Whole-Body-Electromyostimulation on Resting Metabolic Rate, Anthropometric and Neuromuscular Parameters in the Elderly. The Training and ElectroStimulation Trial (TEST). J Strength Cond Res. 2010, 24, 1880–1886. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Teschler, M.; Weissenfels, A.; et al. Effects of Whole-Body Electromyostimulation versus High-Intensity Resistance Exercise on Body Composition and Strength: A Randomized Controlled Study. Evid Based Complement Alternat Med. 2016, 2016, 9236809. [Google Scholar] [CrossRef]
- Kim, J.; Jee, Y. EMS-effect of Exercises with Music on Fatness and Biomarkers of Obese Elderly Women. Medicina 2020, 56, 156. [Google Scholar] [CrossRef]
- Kirişcioğlu, M.; Bicer, M.; Pancar, Z.; Doğan, İ. Effects of electromyostımulatıon traınıng on body composıtıon. Turkish Journal of Sport and Exercise. 2019, 21, 34–37. [Google Scholar]
- Konrad, K.L.; Baeyens, J.-P.; Birkenmaier, C.; et al. The effects of whole-body electromyostimulation (WB-EMS) in comparison to a multimodal treatment concept in patients with non-specific chronic back pain—A prospective clinical intervention study. PloS one 2020, 15, e0236780. [Google Scholar] [CrossRef]
- Micke, F.; Weissenfels, A.; Wirtz, N.; et al. Similar Pain Intensity Reductions and Trunk Strength Improvements following Whole-Body Electromyostimulation vs. Whole-Body Vibration vs. Conventional Back-Strengthening Training in Chronic Non-specific Low Back Pain Patients: A 3-armed randomized controlled trial. Front Physiol. 2021, 13, 664991. [Google Scholar]
- Müllerová, M.; Vaculíková, P.; Potúčková, A.; Struhár, I.; Balousová, D.N. Impact of Whole-Body Electromyostimulation and Resistance Training Programme on Strength Parameters and Body Composition in Group of Elderly Women at Risk of Sarcopenia. Studia sportiva. 2022, 16, 292–304. [Google Scholar] [CrossRef]
- Öktem, U.; Akin, M. Investigation of the Effects of Electrical Muscle Stimulation (EMS) and Traditional Training on Strength Gain and Anthropometric Properties in Sedentary Women [Sedanter Kadınlarda Elektriksel Kas Uyarımı (EMS) ve Geleneksel Antrenmanın Kuvvet Kazanımı ve Antropometrik Özellikler Üzerine Etkisinin İncelenmesi]. CBU Journal of Physical Education and Sport Science. 2022, 17, 70–79. [Google Scholar]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernandez-Gonzalez, V.; Reverter-Masia, J. Effects of Whole-Body Electromyostimulation on Physical Fitness in Postmenopausal Women: A Randomized Controlled Trial. Sensors (Basel). 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Na, S.M.; Choi, S.L.; Seon, J.K.; Do, W.H. Physiological Effect of Exercise Training with Whole Body Electric Muscle Stimulation Suit on Strength and Balance in Young Women: A Randomized Controlled Trial. Chonnam Med J. 2021, 57, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Min, S.; Park, S.H.; Yoo, J.; Jee, Y.S. Influence of Isometric Exercise Combined With Electromyostimulation on Inflammatory Cytokine Levels, Muscle Strength, and Knee Joint Function in Elderly Women With Early Knee Osteoarthritis. Front Physiol. 2021, 12, 688260. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Park, J.; Ham, J.A.; Jee, Y. Effects of aerobic dance with electrical stimulant on body composition and radiological circumference of obese elderly women. Gazzetta Medica Italiana Archivio per le Scienze Mediche. 2021, 180. [Google Scholar] [CrossRef]
- Park, W.; Lee, J.; Hong, K.; et al. Protein-Added Healthy Lunch-Boxes Combined with Exercise for Improving Physical Fitness and Vascular Function in Pre-Frail Older Women: A Community-Based Randomized Controlled Trial. Clin Interv Aging. 2023, 18, 13–27. [Google Scholar] [PubMed]
- Qin, Y.; Chen, H.; Liu, X.; Wu, J.; Zhang, Y. Effects of whole-body electromyostimulation training on upper limb muscles strength and body composition in moderately trained males: A randomized controlled study. Front Public Health. 2022, 10, 982062. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Iron Beats Electricity: Resistance Training but Not Whole-Body Electromyostimulation Improves Cardiometabolic Health in Obese Metabolic Syndrome Patients during Caloric Restriction-A Randomized-Controlled Study. Nutrients. 2021, 13, 1640. [Google Scholar] [CrossRef]
- Ricci, P.A.; Di Thommazo-Luporini, L.; Jurgensen, S.P.; et al. Effects of Whole-Body Electromyostimulation Associated with Dynamic Exercise on Functional Capacity and Heart Rate Variability After Bariatric Surgery: a Randomized, Double-Blind, and Sham-Controlled Trial. Obes Surg. 2020, 30, 3862–3871. [Google Scholar] [CrossRef]
- Sadeghipour, S.; Mirzaei, B. Effects of whole-body electromyostimulation with two different frequencies and combined training on lipid profile and body composition in overweight women. Physiotherapy Quarterly. 2022, 30, 79–85. [Google Scholar] [CrossRef]
- Sadeghipour, S.; Mirzaei, B.; Korobeynikov, G.; Tropin, Y. Effects of Whole-Body Electromyostimulation and Resistance Training on Body Composition and Maximal Strength in Trained Women. Health, Sport, Rehabilitation. 2021, 7, 18–28. [Google Scholar] [CrossRef]
- Sánchez-Infante, J.; Bravo-Sáncheza, A.; Abiánb, P.; Estebana, P.; Jimeneza, J.; Abián-Vicén, J. The influence of whole-body electromyostimulation training in middle-aged women. Isokinet Exerc Sci 2020, 1, 1–9. [Google Scholar] [CrossRef]
- Schink, K.; Herrmann, H.J.; Schwappacher, R.; et al. Effects of whole-body electromyostimulation combined with individualized nutritional support on body composition in patients with advanced cancer: a controlled pilot trial. BMC Cancer. 2018, 18, 886. [Google Scholar] [CrossRef]
- Schink, K.; Reljic, D.; Herrmann, H.J.; et al. Whole-Body Electromyostimulation Combined With Individualized Nutritional Support Improves Body Composition in Patients With Hematological Malignancies - A Pilot Study. Front Physiol. 2018, 9, 1808. [Google Scholar] [CrossRef]
- Teschler, M.; Heimer, M.; Schmitz, B.; Kemmler, W.; Mooren, F.C. Four weeks of electromyostimulation improves muscle function and strength in sarcopenic patients: a three-arm parallel randomized trial. J Cachexia Sarcopenia Muscle. 2021, 12, 843–854. [Google Scholar] [CrossRef]
- Teschler, M.; Weissenfels, A.; Bebenek, M.; et al. Very high creatine kinase CK levels after WB_EMS. Are there implications for health. Int J Clin Exp Med 2016, 9, 22841–22850. [Google Scholar]
- Vaculikova, P.; Paclíková, A.; Kotkova, M.; Struhar, I.; Balousova, D.N. Impact of Whole-Body Electromyostimulation and Resistance Training on Bone Mineral Density in women at risk for Osteopororosis. IJPESS. 2022, 69–79. [Google Scholar] [CrossRef]
- Vaculikova, P.; Paclíková, A.; Kotkova, M.; Struhar, I.; Balousova, D.; Rozsypal, R. Impact of Whole-Body Electromyostimulation and Resistance Training on the Level of Functional Fitness in Elderly Women. Studia Sportiva. 2023, 16, 115–126. [Google Scholar] [CrossRef]
- van Buuren, F.; Horstkotte, D.; Mellwig, K.; et al. Electrical Myostimulation (EMS) Improves Glucose Metabolism and Oxygen Uptake in Type 2 Diabetes Mellitus Patients—Results from the EMS Study. Diabetes Technol Ther. 2015, 17, 413–419. [Google Scholar] [CrossRef]
- van Buuren, F.; Mellwig K., P.; Prinz, C. , et al. Electrical myostimulation improves left ventricular function and peak oxygen consumption in patients with chronic heart failure: results from the exEMS study comparing different stimulation strategies. Clin Res Cardiol. 2013, 102, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Weissenfels, A.; Teschler, M.; Willert, S.; et al. Effects of whole-body electromyostimulation on chronic nonspecific low back pain in adults: a randomized controlled study. J Pain Res. 2018, 11, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Willert, S.; Weissenfels, A.; Kohl, M.; et al. Effects of Whole-Body Electromyostimulation (WB-EMS) on the energy-restriction-induced reduction of muscle mass during intended weight loss. Frontiers of Physiology. 2019, 1012. [Google Scholar] [CrossRef]
- Zink-Rückel, C.; Kohl, M.; von Stengel, S.; Kemmler, W. Once weekly whole-body electromyostimulation increase strength, stability and body composition in amateur golfers. A randomized controlled study. Int. J. Environ. Res. Public Health. 2021, 18, 5628. [Google Scholar] [CrossRef]
- Kemmler, W.; Bebenek, M.; Engelke, K.; von Stengel, S. Impact of whole-body electromyostimulation on body composition in elderly women at risk for sarcopenia: the Training and ElectroStimulation Trial (TEST-III). Age 2014, 36, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Fröhlich, M.; Eifler, C. Whole-Body Electromyostimulation. Effects, Limitations, Perspectives of an Innovative Training Method; Springer, 2024.
- Kemmler, W.; von Stengel, S.; Kohl, M.; et al. Safety of a Combined WB-EMS and High-Protein Diet Intervention in Sarcopenic Obese Elderly Men. Clin Interv Aging. 2020, 15, 953–967. [Google Scholar] [CrossRef] [PubMed]
- Linssen, G.C.; Bakker, S.J.; Voors, A.A.; et al. N-terminal pro-B-type natriuretic peptide is an independent predictor of cardiovascular morbidity and mortality in the general population. Eur Heart J. 2010, 31, 120–127. [Google Scholar] [CrossRef]
- Kemmler, W.; Fröhlich, M.; Ludwig, O.; et al. Position statement and updated international guideline for safe and effective whole-body electromyostimulation training-the need for common sense in WB-EMS application. Front Physiol. 2023, 14, 1174103. [Google Scholar] [CrossRef]
- de Oliveira TM, D.; Felicio, D.C.; Filho, J.E.; Fonseca, D.S.; Durigan JL, Q.; Malaguti, C. Effects of whole-body electromyostimulation on health indicators of older people: Systematic review and meta-analysis of randomized trials. J Bodyw Mov Ther. 2022, 31, 134–145. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010, 340, c869. [Google Scholar] [CrossRef]
- Phillips, E.M.; Katula, J.; Miller, M.E.; et al. Interruption of physical activity because of illness in the Lifestyle Interventions and Independence for Elders Pilot trial. J Aging Phys Act. 2010, 18, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Oldridge, N.B.; Donner, A.P.; Buck, C.W.; et al. Predictors of dropout from cardiac exercise rehabilitation. Ontario Exercise-Heart Collaborative Study. Am J Cardiol. 1983, 51, 70–74. [Google Scholar] [CrossRef]
- Pahmeier, I. Drop-out und Bindung im Breiten und Gesundheitssport. Sportwissenschaften. 1994, 24, 117–150. [Google Scholar]
- Pahmeier, I. Partizipation, bindung und dropout im freizeit-, breiten-und gesundheitssport. Anwendungen der Sportpsychologie. 2008, 2, 425–497. [Google Scholar]
- Vancampfort, D.; Sanchez CP, R.; Hallgren, M.; et al. Dropout from exercise randomized controlled trials among people with anxiety and stress-related disorders: A meta-analysis and meta-regression. J Affect Disord. 2021, 282, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Van Damme, T.; Brunner, E.; et al. Dropout From Exercise Interventions in Adults With Fibromyalgia: A Systematic Review and Meta-analysis. Arch Phys Med Rehabil. 2024, 105, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.; Steele, J.; Wolf, M.; Androulakis-Korakakis, P.; Smith, D.; Giessing, J.; Wescott, W.L. The role of supervision in resistance training; an exploratory systematic review and meta-analysis. Sportrxiv. 2021. [Google Scholar] [CrossRef]
- von Stengel, S.; Frohlich, M.; Ludwig, O.; et al. Revised contraindications for the use of non-medical WB-electromyostimulation. Evidence-based German consensus recommendations. Front Sports Act Living. 2024, 6, 1371723. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernandez-Gonzalez, V.; Nasarre-Nacenta, N.; Reverter-Masia, J. Impact of Whole Body Electromyostimulation on Velocity, Power and Body Composition in Postmenopausal Women: A Randomized Controlled Trial. Int J Environ Res Public Health. 2020, 17, 4982. [Google Scholar] [CrossRef]
Table 1.
Study and participant characteristics of the trials.
| Author | Publication year | Study design | Study groups [n] | Total sample size [n] | Gender | Age [years] |
Body Mass Index (BMI) (kg/m2)1 | Health status | Training status2 | methodological quality (PEDro) |
|
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Akcay et al [11] | 2022 | RCT | 2 | 104 | m+w | 33 ± 1 | 27.2 | healthy | untrained | 5 |
| 2 | Almada et al [22] | 2016 | RCT | 2 | 10 | m | 23 ± 3 | 23.7 | healthy | moderate | 4 |
| 3 | Amaro-Gahete et al [23] | 2018 | RCT | 2 | 12 | m | 27 ± 7 | 23.8 | healthy | well-trained | 6 |
| 4 | FitAging, Amaro-Gahete et al [5] | 2019 | RCT | 4 | 89 | m+w | 53 ± 5 | 26.8 | healthy | untrained | 6 |
| 5 | Andre et al [24] | 2021 | RCT | 2 | 39 | m+w | 39 ± 2 | 40.5 | Obese | untrained | 8 |
| 6 | Bellia et al [25] | 2020 | RCT | 2 | 25 | m+w | 49 ± 7 | 40.1 | Obese | moderate | 3 |
| 7 | Berger et al [13] | 2020 | RCT | 3 | 51 | m+w | 26 ± 3 | 23.8 | healthy | moderate | 6 |
| 8 | Blöckl et al [12] | 2022 | NRCT | 2 | 18 | m+w | 80 ± 4 | 26.2 | Frailty | untrained | 4 |
| 9 | Bostan et al [26] | 2022 | RCT | 2 | 128 | m+w | >18 | n.g. | healthy | untrained | 4 |
| 10 | DiCagno et al [14] | 2023 | RCT | 2 | 24 | m+w | 72 ± 6 | n.g. | Parkinson | untrained | 8 |
| 11 | Dyaksa et al [27] | 2022 | Intervention, single group | 1 | 10 | w | n.g. | n.g. | healthy | n.g. | 2 |
| 12 | Ethem et al [28] | 2019 | RCT | 2 | 18 | w | 38 ± 5 | 23.7 | healthy | untrained | 4 |
| 13 | Evangelista et al [30] | 2019 | RCT | 3 | 58 | m+w | 26 ± 4 | 25.2 | healthy | moderate | 4 |
| 14 | Evangelista et al [29] | 2021 | RCT | 2 | 30 | m | 75 ± 7 | n.g. | healthy | untrained | 5 |
| 15 | Fritzsche et al [31] | 2010 | Intervention, single group | 1 | 15 | m+w | 27 - 73 | 26.8 | CHD | untrained | 2 |
| 16 | Ghannadi et al [32] | 2022 | RCT | 2 | 40 | w | 33 ± 6 | 27.3 | healthy | untrained | 4 |
| 17 | Houdjijk et al [33] | 2022 | NRCT | 4 | 75 | m+w | 45-75 | 31.8 | NIDDP | untrained | 3 |
| 18 | Jee et al [15] | 2019 | RCT | 4 | 54 | m | 25 ± 2 | 22.0 | healthy | untrained | 5 |
| 19 | Junger et al [16] | 2020 | NRCT | 2 | 86 | m+w | 18-62 | 23.0 | healthy | moderate | 3 |
| 20 | TEST I, Kemmler et al [35] | 2010 | RCT | 2 | 30 | w | 65 ± 6 | 26.0 | Osteopenia | well-trained | 6 |
| 21 | TEST II, Kemmler et al [34] | 2010 | RCT | 2 | 28 | m | 69 ± 3 | 28.1 | MetS | untrained | 5 |
| 22 | HIT vs EMS, Kemmler et al [36] | 2016 | RCT | 2 | 46 | m | 30-50 | 28.5 | healthy | moderate | 7 |
| 23 | FORMOSA, Kemmler et al [7] | 2016 | RCT | 3 | 75 | w | 77 ± 4 | 25.1 | Sarcopenic Obesity | untrained | 8 |
| 24 | FRANSO, Kemmler et al [8] | 2017 | RCT | 3 | 100 | m | 77 ± 5 | 26.1 | Sarcopenic Obesity | untrained | 8 |
| 25 | Kim et al [37] | 2020 | RCT | 2 | 25 | w | 71 ± 3 | 30.9 | Obesity | untrained | 6 |
| 26 | Kim et al [17] | 2021 | RCT | 4 | 54 | m | 24 ± 2 | 25.1 | healthy | moderate | 7 |
| 27 | Kiriscioglu et al [38] | 2019 | NRCT | 2 | 41 | w | 34 ± 9 | 25.3 | healthy | well-trained | 3 |
| 28 | Konrad et al [39] | 2020 | NRCT | 2 | 128 | m+w | 56 ± 14 | n.g. | LBP | untrained | 2 |
| 29 | Ludwig et al [18] | 2019 | RCT | 3 | 58 | m+w | 25 ± 4 | 23.9 | healthy | moderate | 4 |
| 30 | Micke et al [40] | 2021 | RCT | 4 | 240 | m+w | 40-70 | 26.3 | LBP | moderate | 8 |
| 31 | Müllerova et al [41] | 2022 | RCT | 2 | 21 | w | 63 ± 2 | 26.6 | healthy | untrained | 4 |
| 32 | Özdal et al [19] | 2016 | RCT | 2 | 40 | w | 32 ± 8 | 24.5 | healthy | untrained | 3 |
| 33 | Öktem et al. [42] | 2022 | RCT | 2 | 20 | W | 22-27 | 23.6 | healthy | untrained | 4 |
| 34 | Pano-Rodriguez et al [43] | 2020 | RCT | 2 | 34 | w | 61 ± 4 | 26.5 | healthy | untrained | 7 |
| 35 | Park et al [46] | 2021 | RCT | 2 | 34 | w | 70 ± 4 | 27.5 | Obese | untrained | 7 |
| 36 | Park et al [45] | 2021 | RCT | 3 | 81 | w | 61-79 | 24.4 | Knee OA | untrained | 7 |
| 37 | Park et al [44] | 2021 | RCT | 2 | 24 | w | 20-40 | 25.0 | healthy | n.g. | 8 |
| 38 | Park et al [47] | 2023 | RCT | 4 | 60 | w | ≥65 | 25.4 | Pre-Frailty | untrained | 7 |
| 39 | Qin et al [48] | 2022 | RCT | 2 | 25 | m | 25 ± 4 | 24.0 | healthy | well-trained | 6 |
| 40 | Reljic et al [49] | 2022 | RCT | 4 | 103 | m+w | ≥18 | 37.2 | Obese, MetS |
untrained | 6 |
| 41 | Ricci et al [50] | 2020 | RCT | 2 | 20 | m+w | 32-45 | 38.2 | Obese | untrained | 9 |
| 42 | Sadeghipour et al [52] | 2021 | RCT | 3 | 30 | w | 26 ± 2 | 21.7 | healthy | well-trained | 5 |
| 43 | Sadeghipour et al [51] | 2022 | RCT | 3 | 45 | w | 32 ± 5 | 27.8 | healthy | moderate | 4 |
| 44 | Sanchez-Infante et al [53] | 2020 | RCT | 2 | 28 | w | 40-60 | 25.5 | healthy | moderate | 6 |
| 45 | Schink et al [54] | 2018 | NRCT | 2 | 131 | m+w | ≥18 | 25.2 | Advanced Cancer | untrained | 3 |
| 46 | Schink et al [55] | 2018 | NRCT | 2 | 31 | m+w | ≥18 | 25.4 | Advanced Cancer | untrained | 3 |
| 47 | Silvestri et al [20] | 2023 | NRCT | 2 | 52 | m+w | 43-81 | 24.3 | LBP | untrained | 3 |
| 48 | Stephan et al [21] | 2023 | RCT | 2 | 60 | m+w | 25-36 | 25.3 | healthy | untrained | 5 |
| 49 | Teschler et al [57] | 2016 | Intervention, single group | 2 | 11 | m | 20-50 | 24.9 | healthy | well-trained | 3 |
| 50 | Teschler et al [56] | 2021 | RCT | 3 | 134 | m+w | 56 ± 7 | 35.7 | Sarcopenia | untrained | 7 |
| 51 | Vacoulikova et al [58] | 2021 | RCT | 3 | 32 | w | 60-65 | 27.1 | healthy | untrained | 4 |
| 52 | Vacoulikova et al [59] | 2021 | RCT | 3 | 63 | w | 60-65 | 27.0 | Osteopenia | untrained | 4 |
| 53 | van Buuren et al [61] | 2014 | NRCT | 3 | 60 | m+w | 61 ± 13 | 29.7 | CHD | n.g. | 4 |
| 54 | van Buuren et al [60] | 2015 | Intervention, single group | 1 | 15 | m+w | 62 ± 3 | 34.6 | NIDDM | n.g. | 4 |
| 55 | TEST III, von Stengel et al [6] | 2015 | RCT | 2 | 76 | w | >70 | 22.2 | Osteopenia | untrained | 7 |
| 56 | Weissenfels et al [62] | 2018 | RCT | 2 | 30 | m+w | 57 ± 7 | 27.9 | LBP | moderate | 8 |
| 57 | Willert et al [63] | 2019 | RCT | 3 | 90 | w | 25-50 | 31.3 | Obese | moderate | 6 |
| 58 | Zink et al [64] | 2021 | RCT | 2 | 54 | m | 18-70 | 27.4 | healthy | moderate | 7 |
1 due to our approach of calculating BMI by body height and mass in case of missing BMI, we are unable to list the SD here; 2 untrained: no regular exercise; moderate: 1 session per week, well-trained: 2-3 sessions per week. CHD: Coronary Heart Disease; LBP: (chronic unspecific) Low Back Pain; MetS: Metabolic syndrome; NIDDM: Non-Insulin Dependent Diabetes Mellitus; NRCT: Non-randomized controlled trial; RCT: Randomized controlled trial.
Table 3.
Attendance rates and adverse effects of the trials. ALF: abnormal laboratory finding.
| Author | Sample size | Age (years) |
Active CG Type of exercise |
Attendance WB-EMS (%) |
Attendance active CG (%) | Adverse effects WB-EMS |
Adverse effects Active CG |
|
|---|---|---|---|---|---|---|---|---|
| 1 | Akcay et al [11] | 104 | 33 ± 1 | WB-EMS with or without diet | 90 | n.a. | No | n.a. |
| 2 | Almada et al [22] | 10 | 23 ± 3 | Funktional training | n.g. | n.g. | n.g. | n.g |
| 3 | Amaro-Gahete et al [23] | 12 | 27 ± 7 | Running | 96 | n.g. | no | n.g. |
| 4 | FitAging, Amaro-Gahete et al. [5] | 89 | 53 ± 5 | HIT Aerobic and DRT | 99 | 98 | no | no |
| WHO-Physical Activity | 99 | no | ||||||
| 5 | Andre et al [24] | 39 | 39 ± 2 | Inactive CG | 91 | ----- | no | ----- |
| 6 | Bellia et al [25] | 25 | 49 ± 7 | Inactive CG (diet) | 90 | ----- | no | ----- |
| 7 | Berger et al [13] | 51 | 26 ± 3 | Inactive CG | 100 | ----- | no | ----- |
| 8 | Blöckl et al [12] | 18 | 80 ± 4 | All groups: WB-EMS | 90 | n.a. | no | ----- |
| 9 | Bostan et al [26] | 128 | >18 | DRT | n.g. | n.g. | no | no |
| 10 | DiCagno et al [14] | 24 | 72 ± 6 | Inactive CG | 100 | ----- | no | ----- |
| 11 | Dyaksa et al [27] | 10 | n.g. | No CG | n.g. | ----- | n.g. | ----- |
| 12 | Ethem et al [28] | 18 | 38 ± 5 | Inactive CG | n.g. | ----- | no | ----- |
| 13 | Evangelista et al [30] | 58 | 26 ± 4 | DRT | n.a. | n.a. | no | no |
| 14 | Evangelista et al [29] | 30 | 75 ± 7 | Functional training | 100 | 100 | no | no |
| 15 | Fritzsche et al [31] | 15 | 27 - 73 | No CG | n.g. | ----- | ALF | ----- |
| 16 | Ghannadi et al [32] | 40 | 33 ± 6 | Aerobic exercise | 80 | 75 | no | no |
| 17 | Houdjijk et al [33] | 75 | 45-75 | No CG | 95 | ----- | no1 | ----- |
| 18 | Jee et al [15] | 54 | 25 ± 2 | Inactive CG | 100 | ----- | no | ----- |
| 19 | Junger et al [16] | 86 | 18-62 | WB-EMS with or without diet | 100 | n.a. | no | n.a. |
| 20 | TEST I, Kemmler et al [35] | 30 | 65 ± 6 | DRT | 98 | 80 | no | no |
| 21 | TEST II, Kemmler et al [34] | 28 | 69 ± 3 | Whole body Vibration | 78 | 74 | no | no |
| 22 | Kemmler et al [36] | 46 | 30-50 | DRT | 90 | 93 | no | no |
| 23 | FORMOSA; Kemmler et al [7] | 75 | 77 ± 4 | Inaktive CG | 89 | ----- | no | ----- |
| 24 | FRANSO, Kemmler et al [8] | 100 | 77 ± 5 | Inaktive CG | 91 | ----- | ALF | ----- |
| 25 | Kim et al [37] | 25 | 71 ± 3 | Dance, RT, Stretching | n.g. | n.g. | no | no |
| 26 | Kim et al [17] | 54 | 24 ± 2 | Isometric RT | n.g. | n.g | no | no |
| 27 | Kiriscioglu et al [38] | 41 | 34 ± 9 | Inactive CG | 95 | ------ | no | ----- |
| 28 | Konrad et al [39] | 128 | 56 ± 14 | Multimodal therapy | 85 | n.g. | no | n.g. |
| 29 | Ludwig et al [18] | 58 | 25 ± 4 | Inactive CG | 100 | ----- | no | ----- |
| 30 | Micke et al [40] | 240 | 40-70 | Whole Body Vibration | 92 | 91 | no | no |
| DRT | 88 | no | ||||||
| 31 | Müllerova et al [41] | 21 | 63 ± 2 | DRT | n.a. | n.a. | n.g. | n.g. |
| 33 | Öktem et al. [42] | 20 | 22-27 | DRT | n.g. | n.g. | n.g. | no |
| 32 | Özdal et al [19] | 40 | 32 ± 8 | WB-EMS with or without exercise | n.g. | n.a. | no | n.a. |
| 34 | Pano-Rodriguez et al [81]} | 34 | 61 ± 4 | DRT | 93 | 89 | no | no |
| 35 | Park et al [46] | 34 | 70 ± 4 | Aerobic dance | 100 | 100 | no | no |
| 36 | Park et al [45] | 81 | 61-79 | Isometric RT | 92 | n.g. | no | no |
| 37 | Park et al [44] | 24 | 20-40 | Low intensity RT | n.g. | n.g. | no | no |
| 38 | Park et al [47] | 60 | ≥65 | Step Aerobic | 91 | 97 | no | no |
| 39 | Qin et al [48] | 25 | 25 ± 4 | DRT | 100 | 100 | no | no |
| 40 | Reljic et al [49] | 103 | ≥18 | HIT-DRT single set | 93 | 94 | no | no |
| HIT-DRT multiple set (3 sets) | 95 | no | ||||||
| 41 | Ricci et al [50] | 20 | 32-45 | (Widely) inactive CG | 100 | ----- | no | ---- |
| 42 | Sadeghipour et al [52] | 30 | 26 ± 2 | DRT | n.g. | n.g. | n.g. | n.g. |
| 43 | Sadeghipour et al [51] | 45 | 32 ± 5 | Aerobic and DRT | 100 | 100 | no | no |
| 44 | Sanchez-Infante et al [53] | 28 | 40-60 | HIIT aerobic and DRT | 100 | n.g. | no | no |
| 45 | Schink et al [54] | 131 | ≥18 | Inactive CG (diet) | 87 | ----- | no | ----- |
| 46 | Schink et al [55] | 31 | ≥18 | Inactive CG (diet) | 77 | ---- | ALF | ----- |
| 47 | Silvestri et al [20] | 52 | 43-81 | WB-EMS with or without stretching | 91 | n.a. | no | n.a. |
| 48 | Stephan et al [21] | 30 | 20-36 | WB-EMS with or without exercise | n.g. | n.a. | no | n.a. |
| 49 | Teschler et al [57] | 11 | 20-50 | No CG | 100 | ------ | ALF2 | ----- |
| 50 | Teschler et al [56] | 134 | 56 ± 7 | Local EMS (lower extremities) | 98 | 98 | no | no |
| 51 | Vacoulikova et al [58] | 32 | 60-65 | DRT | n.a. | n.a. | no | no |
| 52 | Vacoulikova et al [59] | 63 | 60-65 | DRT | n.a. | n.a. | no | no |
| 53 | van Buuren et al [61] | 60 | 61±13 | Local EMS (lower extremities) | 100 | 100 | no | no |
| 54 | van Buuren et al [60] | 15 | 62 ± 3 | No CG | 100 | ------- | no | ----- |
| 55 | TEST III, von Stengel et al [6] | 76 | >70 | Low intensity gymnastics | 79 | 74 | no | no |
| 56 | Weissenfels et al [62] | 30 | 57 ± 7 | Inactive CG | 93 | ----- | no | ----- |
| 57 | Willert et al [63] | 90 | 25-50 | Physical activity (walking) | 100 | 72 | no | no |
| 58 | Zink et al [64] | 54 | 18-70 | Inactive CG | 95 | ----- | no | ----- |
1 except two asymptomatic hypoglycaemia cases after WB-EMS application….2 …however this study potentially provokes rhabdomyolysis by applying very high impulse intensity in novice WB-EMS applicants.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



