
Submitted:
21 June 2024
Posted:
24 June 2024
You are already at the latest version
Abstract
Primary bone lymphoma of the spine (PBL) is a rare entity and the most shared type of non-Hodgkin lymphoma (LNH) appearing in bone lesions deprived of nodal or extra-nodal in-volvement and accounting for approximately 2% of all lymphomas. Most PBL are diffuse large B-cell lymphomas (DLBCL) and commonly involve the appendicular skeleton. Due to its atypical location and non-specific clinical imaging features mimicking certain neoplastic or infectious processes, this pathology may be misdiagnosed, thus complicating and delaying diagnosis. Our case reports a patient in her sixties who had been suffering from chronic low back pain for a year, and had gradually started to develop cruralgia and fever. She underwent a blood sample, magnetic resonance imaging (MRI), and positron emission tomography (18F-FDG-PET/CT) which revealed significant inflammatory syndrome, a pattern of spondylodiscitis at the L3-L4 level associated with morphological and metabolic invasion extending posteriorly, raising suspicion of epiduritis. No other lesions were found on the rest of the body. Neurosurgical management was performed and a biopsy was made. Histological results showed aggressive and diffuse large B-cell lymphoma, suggesting a diagnosis of PBL. This case highlights the first case of spondylodiscitis mimicking PBL in the lumbar spine, the intricacies of the diagnostic work-up, and the complexity of discriminating with an infectious process in the spine, as both have a similar, non-specific clinical presentation with different prognosis and therapeutic management.
Keywords:
Primary bone lymphoma
; Diffuse large B-cell lymphoma
; Spondylodiscitis
; 18F-FDG-PET/CT
; MRI.
Figure 1.
18F-FDG-PET/CT of the patient: (A) Maximum Intensity Projection (MIP) of the entire body, (B) Maximum Intensity Projection (MIP), (C) merged images, and (D) CT-images of the lumbosacral area. A 62-year-old patient without a significant pre-existing medical history presented with chronic mechanical low back pain since the summer of 2022. She had previously undergone a magnetic resonance imaging (MRI) of the spine in favor of a narrow lumbar canal (Figure 2A), for which she was treated with multiple analgesics and infiltrations until the summer of 2023, with an improvement of the symptomatology. However, since October 2023, her symptoms have worsened. The patient presented no nocturnal sweating, was pyretic (maximum of 38.5°C), and slightly decreased her appetite. On clinical examination, discrete paresis of the left quadriceps was observed. Bearing in mind the patient’s condition at the time of consultation, she was quickly admitted to the hospital where further exams were carried out. Laboratory tests showed a small elevated serum white-blood cells (12.2x10³/µL), predominantly neutrophilic (8.4x10³/µL), and a concentration of C-reactive protein (175mg/dL). The other biological tests came back unremarkable. She underwent an MRI, which revealed a very dubious image showing remodeling of the L3 vertebra (bone marrow replacement) and of the intervertebral disc between L3 and L4, suggesting suspected spondylitis vs spondylodiscitis (Figure 2B). Broad-spectrum antibiotics were subsequently started. In view of her symptoms and recent weight loss, she also underwent an 18F-FDG-PET/CT showing a higher uptake in this widespread invasion at the L3 level with an infectious appearance and more aggressive metabolic extension anteriorly and posteriorly, associated with epiduritis. No other lesions were found on the rest of the body (Figure 2). Neurosurgical management (decompression and L3-laminectomy) was performed and samples were taken. Histological results showed aggressive and diffuse large-cell B lymphoma (DLBCL), stage IV (Ann-Harbor classification). Immuno-histochemical were as follows: CD20+, PAX5+, CD3/CD5 -, BCL6+, MUM1-, Cycline D1-, BCL2+, cMyc-, Ki-67 80%, consistent with DLBCL, non-germinal center B-cell like (Figure 3). A diagnosis of primary bone lymphoma of the lumbar spine was made. Chemotherapy (R-CHOP and methotrexate) was administered to the patient with clinical, morphologic, and metabolic improvement after 4 cycles (Figure 4 and Figure 5). Firstly described by Oberling et al. in 1928, primary bone lymphoma in the spine (PBL) remains a scarce entity and the utmost shared type of non-Hodgkin lymphoma (LNH) appearing in bone lesions deprived of nodal or extra-nodal involvement, accounting for approximately 3-7% amongst primary bone tumors and 2% of all lymphomas [1]. The predominant diagnosis age of patients is over 30, with a median of 45, and more predominant in men than women, with a ratio of 1.5:1[1]. Most PBL are diffuse large B-cell lymphomas (DLBCL) and commonly involve the appendicular skeleton [2]. Because infection and malignant tumors have certain characteristics in common that complicate and delay diagnosis, PBL can be underdiagnosed, particularly with tumors invading the spine/spinal cord or nerves such as sarcoma, plasmacytoma, or infectious processes such as osteomyelitis or spondylodiscitis. Here, we present the first unique case of an atypical cruralgia in terms of tumor location and clinical presentation, the 18F-FDG-PET/CT and MRI findings, and therapeutic management. The non-specific clinical manifestations and inconclusive laboratory tests of PBL can be quite frustrating, and heterogeneous in its presentation, frequently resulting in a delayed diagnosis [2]. The most common symptom is localized bone pain, predominantly in the appendicular skeleton, which is difficult to relieve with rest and may progressively worsen over time [3]. Patients may sometimes experience ‘B’ symptoms including fever, night sweats, and unwanted weight loss. These symptoms occur in a minority of patients and are not as frequent in PBL as in systemic lymphoma [4]. In our case, the patient reported a “red flag” sign (unwanted weight loss) associated with cruralgia and inflammatory syndrome, suggesting an infectious process on the first hypothesis. PBL can arise in any part of the musculoskeletal system and can occasionally manifest as soft tissue masses that can be misidentified for infection or malignancy [5,6]. Moreover, symptoms of spinal cord compression are reported in approximately less than 20% [5,6]. According to the literature, this paper reported the first case of PBL mimicking an isolated infectious process in the spine. As far, few case reports of PBL infiltrated spinal nerve roots and ganglia have been described but nothing related to our case [7,8]. Since infections and malignant tumors share characteristics that complicate the differential diagnosis and delay appropriate treatment, multiple modalities including clinical examination, laboratory sampling, biopsy samples, and imaging techniques are required. In morphological imaging, magnetic resonance imaging (MRI) has been proven to be significant in the staging of PBL [9]. However, MRI cannot discriminate non-viable from viable malignancies as shown in our patient (Figure 2B), and therefore cannot be convenient where bone infections are present. In contrast, MRI is currently the method of choice for diagnosing spondylodiscitis, demonstrating a hyposignal in T1 and a hypersignal in T2 phase (Figure 2B) [10]. It provides information on bone marrow, vertebral disks, and neural structures. In metabolical imaging, management with 2-[18F]-fluoro-2-deoxy-D-glucose (18F-FDG) positron emission tomography combined with computed tomography (PET/CT) is mainly used to identify high-uptake lesions. This hybrid imaging method provides information on metabolic characteristics and anatomical location. It has been approved for the staging and therapeutic follow-up of patients with Hodgkin’s disease (HD) and NHL [11]. Study data with PBL also speculated that 18F-FDG-PET/CT may provide significant information for management decisions [11,12]. In spondylodiscitis, some studies have suggested that 18F-FDG-PET/CT is slightly more sensitive and accurate than MRI, particularly in the early stages, because the metabolism of the lesion appears much earlier than the morphological alterations on MRI [12,13]. Nevertheless, discrimination between malignant and infectious processes is sometimes challenging with 18F-FDG-PET/CT. While maximum higher standardized uptake values (SUVmax) are associated with a greater probability of malignancy, no threshold for uptake allows us to distinguish both processes [14]. For example, a prospective study conducted by Skawran et al. evaluated 77 cancerous and inflammatory/infectious lesions in 24 patients using different 18F-FDG-PET/CT parameters and showed no significant difference between infectious from malignant lesions using SUVmax [15]. In our case, the patient had no risk factors for spondylodiscitis (no recent spinal surgery, diabetes, pre-existing infection, iatrogenic or human immunosuppression, etc.), and the weight loss, fever, and cruralgia didn’t appear until very late (1 year). It is possible that the various lumbar infiltrations carried out to relieve the pain served as an entry point for a bacterium that could have proliferated, giving rise to the initial suspicion of spondylodiscitis. FDG-uptake in the L3-lesion was very intense (SUVmax: 35) and correlated with a metabolic image of anterior and posterior “inflammatory cast” invading the spinal cord, suggesting an infectious origin as a first hypothesis but which was misdiagnosed in favor of an aggressive LDBCL. Clearly, in most cases, biopsy or pathology results are required to confirm the final diagnosis. More recently, interest in the 18F-FDG-PET/MRI hybrid imaging has grown. This new modality combines the physiological information acquired by PET with the very high resolution of soft tissue and the contrast of MRI, reducing the number of examinations required for the patient and scanner-related irradiation (Figure 2C) [13]. In PBL, 18F-FDG-PET/MRI has shown encouraging results in early studies and exposed similar sensitivity with 18F-FDG-PET/CT [16]. In vertebral osteomyelitis, a prospective study conducted by Kouijzer et al. showed promising results as a complementary fusion-imaging technique with 18F-FDG-PET/MRI [17]. Mainly speaking, more studies are needed to fully demonstrate its benefit. In conclusion, our case illustrates the difficulty of discriminating between PBL and spondylodiscitis, as both have a similar, non-specific clinical and laboratory presentation, while morphological and metabolic findings may be similar to each other. For precise diagnosis, we recommend fully incorporating primary bone lymphoma as a differential diagnosis in patients presenting with an inflammatory syndrome associated with neurological defects and warning signs, and combining clinical diagnosis, laboratory tests, fusion imaging methods, and biopsies to avoid delaying appropriate treatment.
Figure 1.
18F-FDG-PET/CT of the patient: (A) Maximum Intensity Projection (MIP) of the entire body, (B) Maximum Intensity Projection (MIP), (C) merged images, and (D) CT-images of the lumbosacral area. A 62-year-old patient without a significant pre-existing medical history presented with chronic mechanical low back pain since the summer of 2022. She had previously undergone a magnetic resonance imaging (MRI) of the spine in favor of a narrow lumbar canal (Figure 2A), for which she was treated with multiple analgesics and infiltrations until the summer of 2023, with an improvement of the symptomatology. However, since October 2023, her symptoms have worsened. The patient presented no nocturnal sweating, was pyretic (maximum of 38.5°C), and slightly decreased her appetite. On clinical examination, discrete paresis of the left quadriceps was observed. Bearing in mind the patient’s condition at the time of consultation, she was quickly admitted to the hospital where further exams were carried out. Laboratory tests showed a small elevated serum white-blood cells (12.2x10³/µL), predominantly neutrophilic (8.4x10³/µL), and a concentration of C-reactive protein (175mg/dL). The other biological tests came back unremarkable. She underwent an MRI, which revealed a very dubious image showing remodeling of the L3 vertebra (bone marrow replacement) and of the intervertebral disc between L3 and L4, suggesting suspected spondylitis vs spondylodiscitis (Figure 2B). Broad-spectrum antibiotics were subsequently started. In view of her symptoms and recent weight loss, she also underwent an 18F-FDG-PET/CT showing a higher uptake in this widespread invasion at the L3 level with an infectious appearance and more aggressive metabolic extension anteriorly and posteriorly, associated with epiduritis. No other lesions were found on the rest of the body (Figure 2). Neurosurgical management (decompression and L3-laminectomy) was performed and samples were taken. Histological results showed aggressive and diffuse large-cell B lymphoma (DLBCL), stage IV (Ann-Harbor classification). Immuno-histochemical were as follows: CD20+, PAX5+, CD3/CD5 -, BCL6+, MUM1-, Cycline D1-, BCL2+, cMyc-, Ki-67 80%, consistent with DLBCL, non-germinal center B-cell like (Figure 3). A diagnosis of primary bone lymphoma of the lumbar spine was made. Chemotherapy (R-CHOP and methotrexate) was administered to the patient with clinical, morphologic, and metabolic improvement after 4 cycles (Figure 4 and Figure 5). Firstly described by Oberling et al. in 1928, primary bone lymphoma in the spine (PBL) remains a scarce entity and the utmost shared type of non-Hodgkin lymphoma (LNH) appearing in bone lesions deprived of nodal or extra-nodal involvement, accounting for approximately 3-7% amongst primary bone tumors and 2% of all lymphomas [1]. The predominant diagnosis age of patients is over 30, with a median of 45, and more predominant in men than women, with a ratio of 1.5:1[1]. Most PBL are diffuse large B-cell lymphomas (DLBCL) and commonly involve the appendicular skeleton [2]. Because infection and malignant tumors have certain characteristics in common that complicate and delay diagnosis, PBL can be underdiagnosed, particularly with tumors invading the spine/spinal cord or nerves such as sarcoma, plasmacytoma, or infectious processes such as osteomyelitis or spondylodiscitis. Here, we present the first unique case of an atypical cruralgia in terms of tumor location and clinical presentation, the 18F-FDG-PET/CT and MRI findings, and therapeutic management. The non-specific clinical manifestations and inconclusive laboratory tests of PBL can be quite frustrating, and heterogeneous in its presentation, frequently resulting in a delayed diagnosis [2]. The most common symptom is localized bone pain, predominantly in the appendicular skeleton, which is difficult to relieve with rest and may progressively worsen over time [3]. Patients may sometimes experience ‘B’ symptoms including fever, night sweats, and unwanted weight loss. These symptoms occur in a minority of patients and are not as frequent in PBL as in systemic lymphoma [4]. In our case, the patient reported a “red flag” sign (unwanted weight loss) associated with cruralgia and inflammatory syndrome, suggesting an infectious process on the first hypothesis. PBL can arise in any part of the musculoskeletal system and can occasionally manifest as soft tissue masses that can be misidentified for infection or malignancy [5,6]. Moreover, symptoms of spinal cord compression are reported in approximately less than 20% [5,6]. According to the literature, this paper reported the first case of PBL mimicking an isolated infectious process in the spine. As far, few case reports of PBL infiltrated spinal nerve roots and ganglia have been described but nothing related to our case [7,8]. Since infections and malignant tumors share characteristics that complicate the differential diagnosis and delay appropriate treatment, multiple modalities including clinical examination, laboratory sampling, biopsy samples, and imaging techniques are required. In morphological imaging, magnetic resonance imaging (MRI) has been proven to be significant in the staging of PBL [9]. However, MRI cannot discriminate non-viable from viable malignancies as shown in our patient (Figure 2B), and therefore cannot be convenient where bone infections are present. In contrast, MRI is currently the method of choice for diagnosing spondylodiscitis, demonstrating a hyposignal in T1 and a hypersignal in T2 phase (Figure 2B) [10]. It provides information on bone marrow, vertebral disks, and neural structures. In metabolical imaging, management with 2-[18F]-fluoro-2-deoxy-D-glucose (18F-FDG) positron emission tomography combined with computed tomography (PET/CT) is mainly used to identify high-uptake lesions. This hybrid imaging method provides information on metabolic characteristics and anatomical location. It has been approved for the staging and therapeutic follow-up of patients with Hodgkin’s disease (HD) and NHL [11]. Study data with PBL also speculated that 18F-FDG-PET/CT may provide significant information for management decisions [11,12]. In spondylodiscitis, some studies have suggested that 18F-FDG-PET/CT is slightly more sensitive and accurate than MRI, particularly in the early stages, because the metabolism of the lesion appears much earlier than the morphological alterations on MRI [12,13]. Nevertheless, discrimination between malignant and infectious processes is sometimes challenging with 18F-FDG-PET/CT. While maximum higher standardized uptake values (SUVmax) are associated with a greater probability of malignancy, no threshold for uptake allows us to distinguish both processes [14]. For example, a prospective study conducted by Skawran et al. evaluated 77 cancerous and inflammatory/infectious lesions in 24 patients using different 18F-FDG-PET/CT parameters and showed no significant difference between infectious from malignant lesions using SUVmax [15]. In our case, the patient had no risk factors for spondylodiscitis (no recent spinal surgery, diabetes, pre-existing infection, iatrogenic or human immunosuppression, etc.), and the weight loss, fever, and cruralgia didn’t appear until very late (1 year). It is possible that the various lumbar infiltrations carried out to relieve the pain served as an entry point for a bacterium that could have proliferated, giving rise to the initial suspicion of spondylodiscitis. FDG-uptake in the L3-lesion was very intense (SUVmax: 35) and correlated with a metabolic image of anterior and posterior “inflammatory cast” invading the spinal cord, suggesting an infectious origin as a first hypothesis but which was misdiagnosed in favor of an aggressive LDBCL. Clearly, in most cases, biopsy or pathology results are required to confirm the final diagnosis. More recently, interest in the 18F-FDG-PET/MRI hybrid imaging has grown. This new modality combines the physiological information acquired by PET with the very high resolution of soft tissue and the contrast of MRI, reducing the number of examinations required for the patient and scanner-related irradiation (Figure 2C) [13]. In PBL, 18F-FDG-PET/MRI has shown encouraging results in early studies and exposed similar sensitivity with 18F-FDG-PET/CT [16]. In vertebral osteomyelitis, a prospective study conducted by Kouijzer et al. showed promising results as a complementary fusion-imaging technique with 18F-FDG-PET/MRI [17]. Mainly speaking, more studies are needed to fully demonstrate its benefit. In conclusion, our case illustrates the difficulty of discriminating between PBL and spondylodiscitis, as both have a similar, non-specific clinical and laboratory presentation, while morphological and metabolic findings may be similar to each other. For precise diagnosis, we recommend fully incorporating primary bone lymphoma as a differential diagnosis in patients presenting with an inflammatory syndrome associated with neurological defects and warning signs, and combining clinical diagnosis, laboratory tests, fusion imaging methods, and biopsies to avoid delaying appropriate treatment.
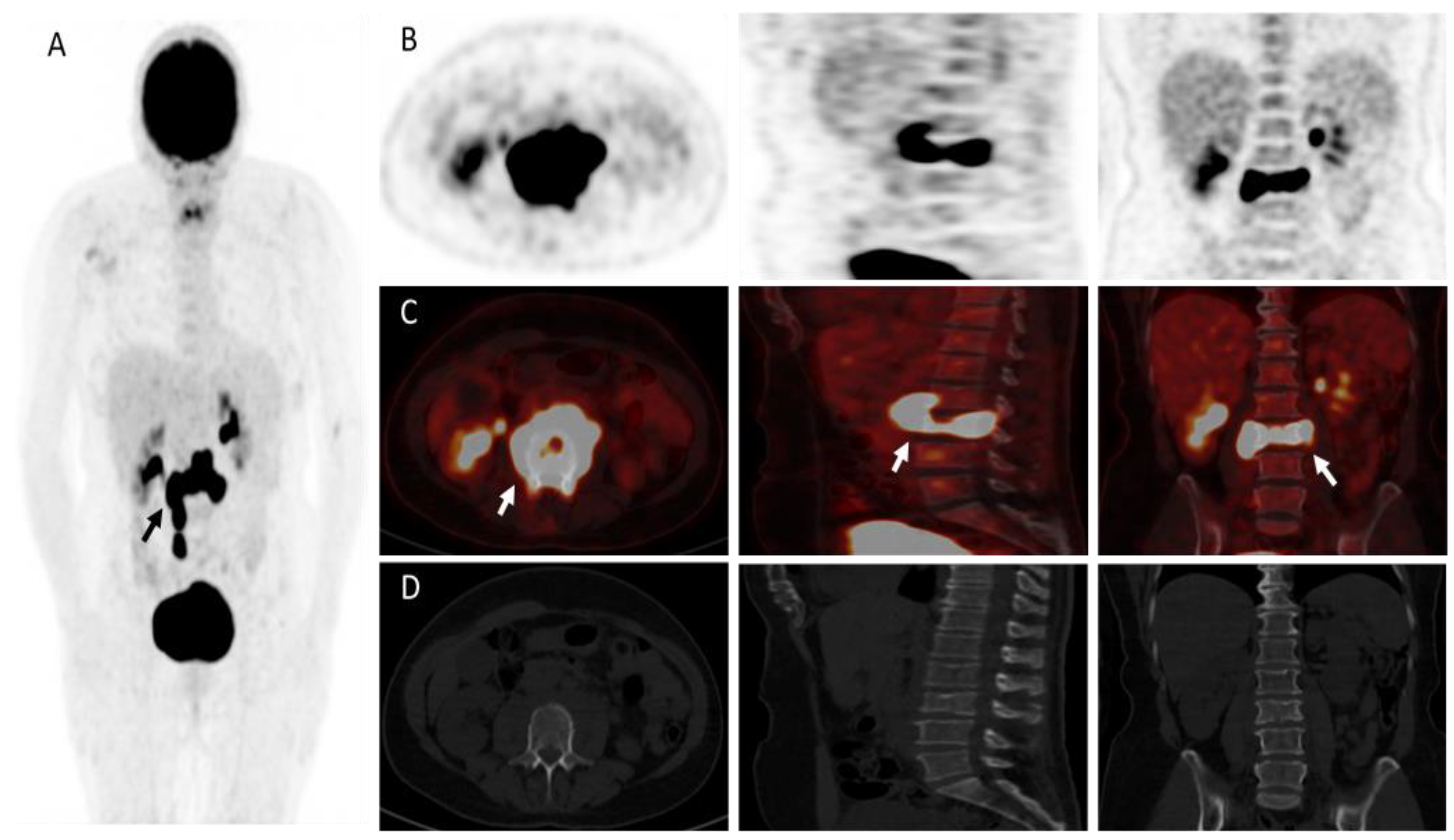
Figure 2.
MRI (T1-T2 phases) undergone in July 2022 showed disc disease in posterior L2-L3 and especially L3-L4 (white arrow), discreetly reducing the diameter of the canal, with a relative secondary narrowing of the canal (A). The MRI carried out in December 2023 showed bone marrow replacement of almost the entire L3-vertebral body in both phases and the intervertebral disc between L3 and L4 (long white arrow), suggesting suspected spondylitis vs spondylodiscitis (Figure 2B). However, a neoplastic pathology could not be ruled out. A merged image of 18F-FDG-PET and MRI showed aggressive widespread invasion at the L3 and doubtful at the L3-L4 level intervertebral disc, with an infectious appearance and metabolic extension anteriorly and posteriorly (head arrow), associated with epiduritis (C).
Figure 2.
MRI (T1-T2 phases) undergone in July 2022 showed disc disease in posterior L2-L3 and especially L3-L4 (white arrow), discreetly reducing the diameter of the canal, with a relative secondary narrowing of the canal (A). The MRI carried out in December 2023 showed bone marrow replacement of almost the entire L3-vertebral body in both phases and the intervertebral disc between L3 and L4 (long white arrow), suggesting suspected spondylitis vs spondylodiscitis (Figure 2B). However, a neoplastic pathology could not be ruled out. A merged image of 18F-FDG-PET and MRI showed aggressive widespread invasion at the L3 and doubtful at the L3-L4 level intervertebral disc, with an infectious appearance and metabolic extension anteriorly and posteriorly (head arrow), associated with epiduritis (C).
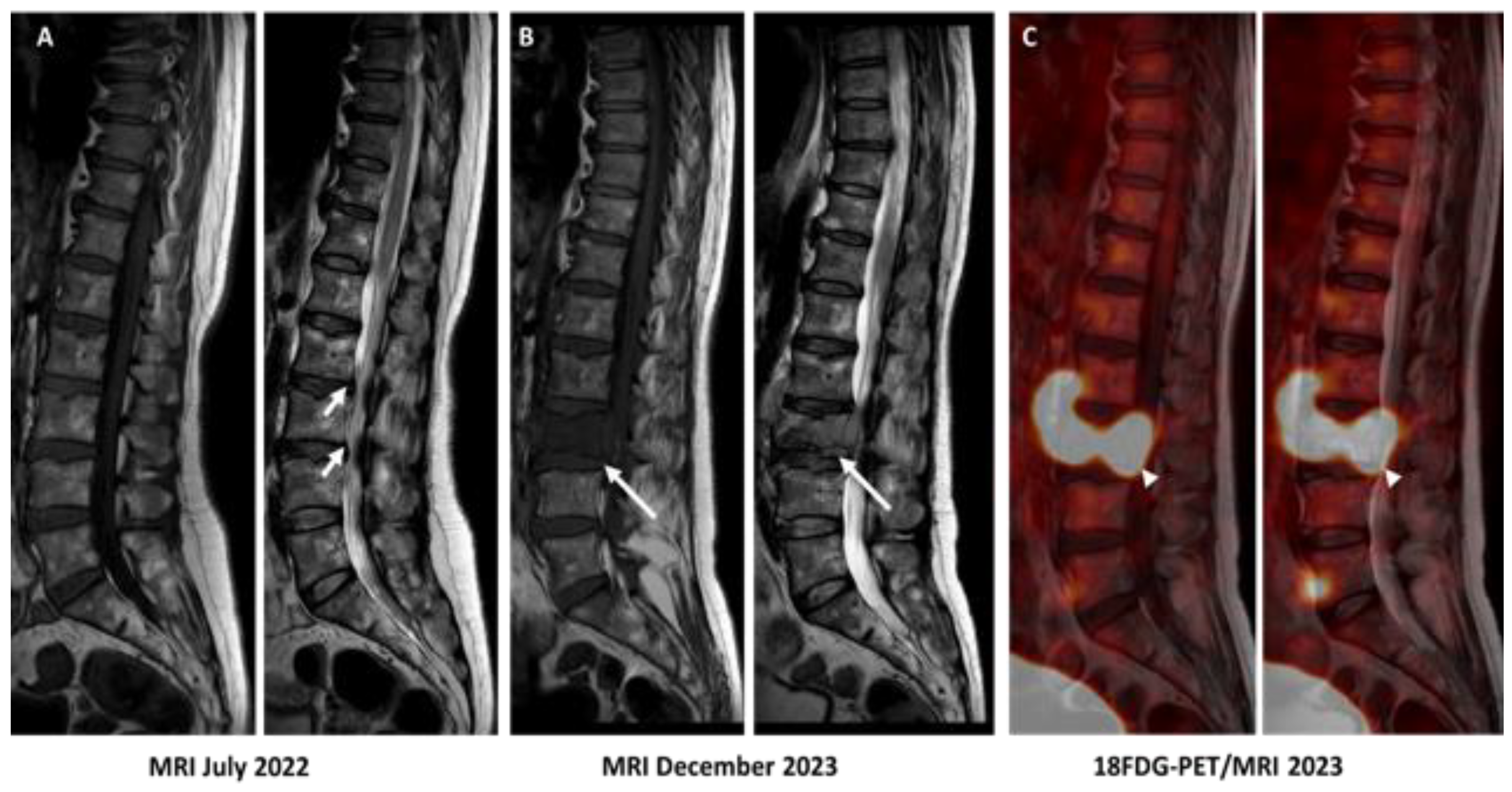
Figure 3.
Biopsy of infiltrating lesion of the L3 vertebra showing aggressive DLBCL. Immunostaining of the lesion is positive for hematoxylin-eosin HE (A), CD20+ (B), KI-67 (C), and BCL2 (D). Because PBLs are often DLBCLs, according to the literature, the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) associated with methotrexate for preventing central nervous system (CNS) is the most current protocol therapy for patients with aggressive DLBCL [18]. Our patient underwent 4 cycles of chemotherapy with an improvement in her symptomatology and morphological and metabolical imaging (Figure 4).
Figure 3.
Biopsy of infiltrating lesion of the L3 vertebra showing aggressive DLBCL. Immunostaining of the lesion is positive for hematoxylin-eosin HE (A), CD20+ (B), KI-67 (C), and BCL2 (D). Because PBLs are often DLBCLs, according to the literature, the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) associated with methotrexate for preventing central nervous system (CNS) is the most current protocol therapy for patients with aggressive DLBCL [18]. Our patient underwent 4 cycles of chemotherapy with an improvement in her symptomatology and morphological and metabolical imaging (Figure 4).
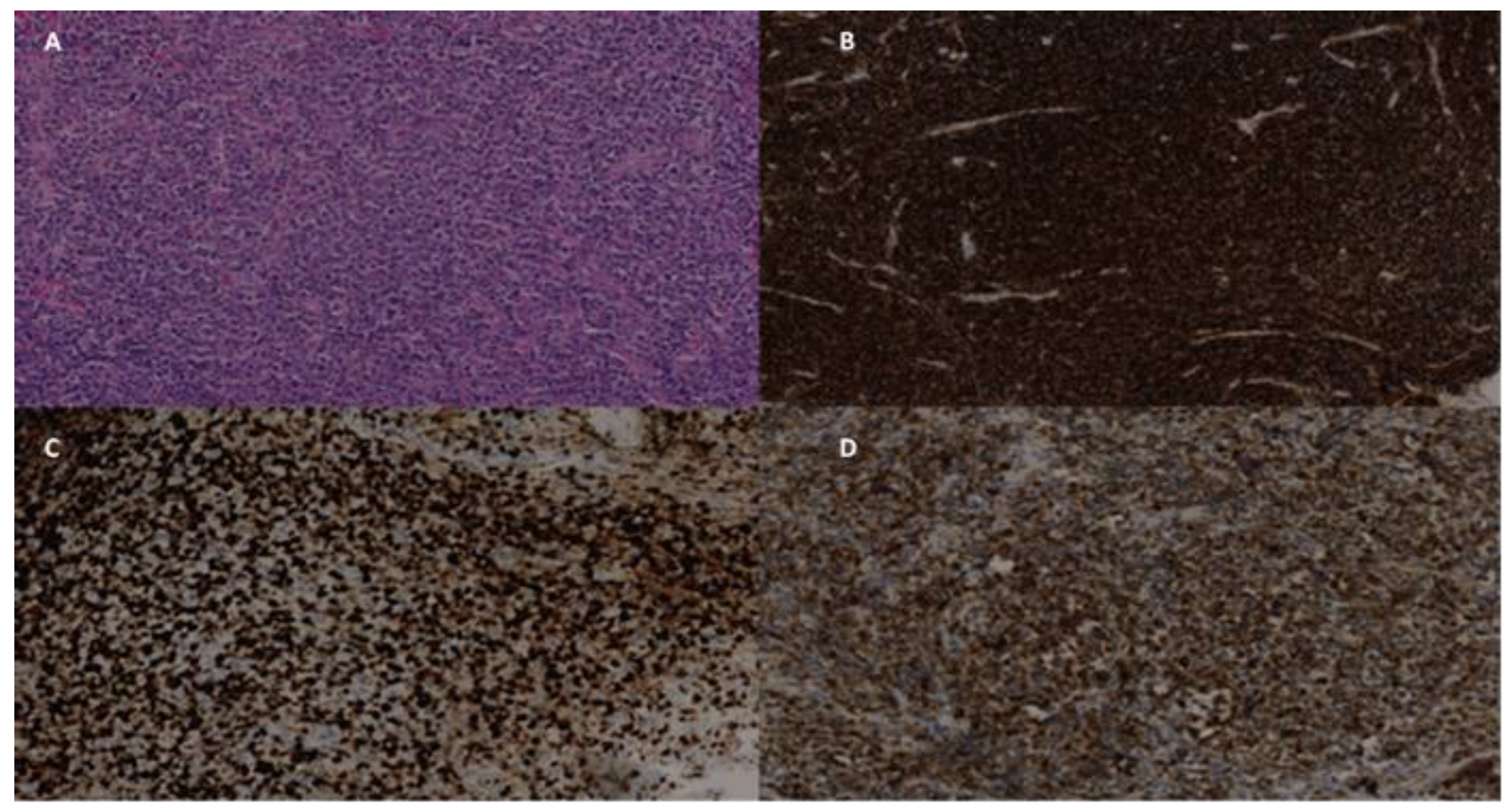
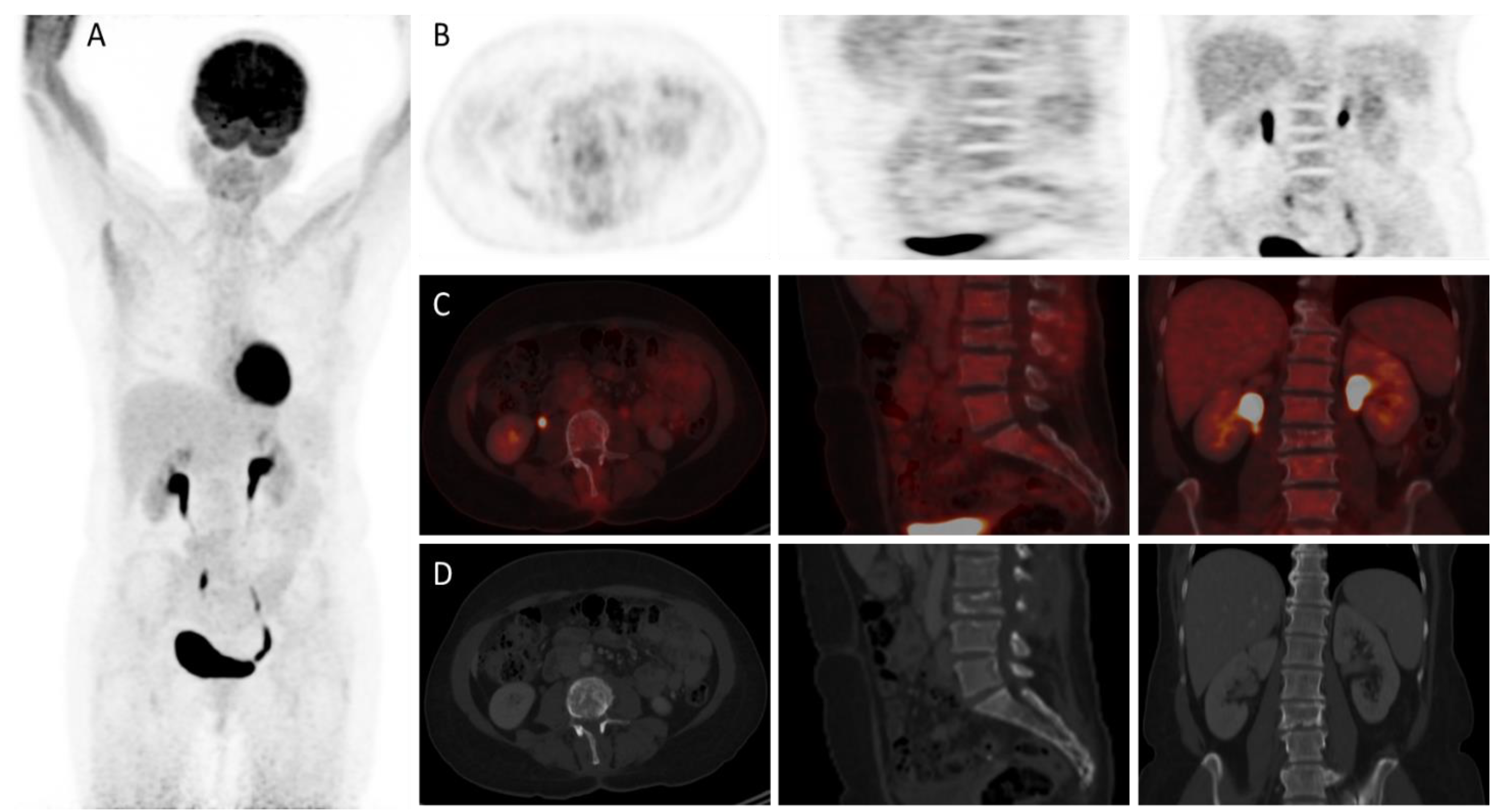
Figure 4.
18F-FDG-PET/CT showing complete metabolic response/normalization at the L3 vertebra level and the L3-L4 intervertebral disc after decompression and particularly 4 cycles of chemotherapy (white arrows).
Figure 4.
18F-FDG-PET/CT showing complete metabolic response/normalization at the L3 vertebra level and the L3-L4 intervertebral disc after decompression and particularly 4 cycles of chemotherapy (white arrows).
Authors contributions
“Conceptualization, A.J.; methodology, A.J, S.M.; software, A.J, A.C, C.M; formal analysis A.J, C.M, A.R.; investigation, A.J, S.M, R.A.; resources, O.R, A.T, C.M.; data curation, A.J, O.R, C.M, A.C, ; writing—original draft preparation, A.J; writing—review and editing, O.R, R.A, C.M; visualization, A.C, S.M; supervision, C.M. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not receive ethical review and approval due to the nature of the research (case report).
Informed Consent Statement
Written informed consent was obtained from the patient. The consent form was obtained on 01.03.2024.
Data Availability Statement
The data used and analyzed in this study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bhagavathi, S.; Fu, K. Primary lymphoma of bone: a review. Seminars in Diagnostic Pathology 2014, 31, 48–52. [Google Scholar] [CrossRef]
- Mikhaeel, N.G. Primary Bone Lymphoma. Clinical Oncology. 2012, 24, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Mika, J.; Schleicher, I.; Gerlach, U.; Adler, C.P.; Uhl, M.; Knoeller, S.M. Primary bone lymphomas thought to be osteomyelitis urgently demand a rapid diagnosis in bone pathology. Anticancer Res. 2012, 32, 4905–4912. [Google Scholar] [PubMed]
- Demircay, E.; Hornicek, F.J.; Mankin, H.J.; Degroot, H. Malignant Lymphoma of Bone: A Review of 119 Patients. Clinical Orthopaedics & Related Research. 2013, 471, 2684–2690. [Google Scholar]
- Kanavos, T.; Birbas, E.; Papoudou-Bai, A.; Hatzimichael, E.; Kitsouli, A.; Karpathiou, G.; et al. Primary Bone Lymphoma: A Review of the Literature with Emphasis on Histopathology and Histogenesis. Diseases [Internet] 2023, [cited 2023 Mar 9]. 11, 42. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Cao, D.L.; Xu, H.W.; Zhao, W.D.; Hu, T.; Wu, D.S. Development of Primary Diffuse Large B-Cell Lymphoma Around an Internal Fixation Implant After Lumbar Fusion Surgery: A Case Report and Review of the Literature. World Neurosurgery [Internet] 2020, [cited 2022 7]. 137, 140–145. [Google Scholar] [CrossRef]
- Kim, S.K.; Lee, S.H.; Kim, E.S.; Eoh, W. Diffuse Large B-Cell Lymphoma Mimicking Schwannoma of Lumbar Spine. Korean Journal of Spine. 2016, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.C. Non-Hodgkin’s B-cell lymphoma of a lumbar nerve root: A rare cause of lumbar radiculopathy. Journal of Clinical Neuroscience. 2013, 20, 1029–1031. [Google Scholar] [CrossRef]
- Zhou, H.; Gao, F.; Bu, B.; Fu, Z.; Sun, X.; Huang, C.; et al. Primary bone lymphoma: A case report and review of the literature. Oncology Letters [Internet]. 2014, 8, 1551–1556. [Google Scholar] [CrossRef]
- Herren, C.; Jung, N.; Pishnamaz, M.; Breuninger, M.; Siewe, J.; Sobottke, R. Spondylodiscitis: Diagnosis and Treatment Options. Deutsches Aerzteblatt Online [Internet] 2017. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, M.; Barrington, S.F. PET/CT for Therapy Response Assessment in Lymphoma. The Journal of Nuclear Medicine. 2009, 50 (Suppl 1), 21S30S. [Google Scholar] [CrossRef]
- Altini, C.; Lavelli, V.; Niccoli-Asabella, A.; Sardaro, A.; Branca, A.; Santo, G.; et al. Comparison of the Diagnostic Value of MRI and Whole Body 18F-FDG PET/CT in Diagnosis of Spondylodiscitis. Journal of Clinical Medicine. 2020, 9, 1581. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, A.H.; Raza, S.I.; Carrino, J.A.; Kosmas, C.; Gholamrezanezhad, A.; Basques, K.; et al. Applications of PET/CT and PET/MR Imaging in Primary Bone Malignancies. PET clinics [Internet] 2018, [cited 2021 Aug 18]. 13, 623–634. [Google Scholar] [CrossRef]
- Bleeker-Rovers, C.P.; Vos, F.J.; Graaf, W.T.A.; Oyen, W.J.G. Nuclear Medicine Imaging of Infection in Cancer Patients (With Emphasis on FDG-PET). The Oncologist. 2011, 16, 980–991. [Google Scholar] [CrossRef] [PubMed]
- Skawran, S.; Messerli, M.; Kotasidis, F.; Trinckauf, J.; Weyermann, C.; Kudura, K.; et al. Can Dynamic Whole-Body FDG PET Imaging Differentiate between Malignant and Inflammatory Lesions? Life [Internet]. 2022, 12, 1350. [Google Scholar]
- Rakheja, R.; Chandarana, H.; DeMello, L.; Jackson, K.; Geppert, C.; Faul, D.; et al. Correlation Between Standardized Uptake Value and Apparent Diffusion Coefficient of Neoplastic Lesions Evaluated With Whole-Body Simultaneous Hybrid PET/MRI. American Journal of Roentgenology. 2013, 201, 1115–1119. [Google Scholar] [CrossRef] [PubMed]
- Kouijzer, I.J.E.; Scheper, H.; de Rooy, J.W.J.; Bloem, J.L.; Janssen, M.J.R.; van den Hoven, L.; et al. The diagnostic value of 18F–FDG-PET/CT and MRI in suspected vertebral osteomyelitis – a prospective study. European Journal of Nuclear Medicine and Molecular Imaging. 2017, 45, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; Araujo IB de, O.; Berti, E.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022, 36, 1720–1748. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



