
Submitted:
21 June 2024
Posted:
24 June 2024
You are already at the latest version
Abstract
The aim of the study was to assess the effects of an 8-week cognitive-motor training program on postural control and knee proprioception under single and dual-task conditions. Design: Randomized clinical trial. Methods: 20 healthy and physically active older adults (73.255.98 years) volunteered to participate and were randomly assigned into an experimental and a control group (EG and CG). Postural control was measured with the Romberg test, with open (RBOE), closed eyes (RBCE) and under unipodal dominant side (RUDL) conditions. Proprioception was assessed by measuring participants’ ability to reposition their dominant knee at 45º. Finally, performance on the cognitive task was measured through a subscale of the Barcelona Test called “categorical evocation in associations.” The EG and the CG completed 8-week training programme with two sessions the 30 minutes per week of postural control and proprioception exercises. The EG additionally included music in each session. Results: The results showed significant differences in both group at the postural control tests (RBOE and RBCE) and proprioceptive test post intervention. Conclusion: The 8-week training program had a positive impact on the post-intervention results for motor control and proprioception, but not on the results of the cognitive task. There were no significant differences between the groups that carried out sessions with or without music.
Keywords:
motor control
; balance
; active aging
; music
; double task training
1. Introduction
The increased longevity of the current population has sparked researchers’ interest in studying the potential of different modalities of physical activity-based programs to delay the physical and cognitive decline associated with ageing, with the aim of improving the quality of life and overall wellbeing of the older adult population1. Experts predict a potential increase in the proportion of the population over 60 years of age in the near future2. Therefore, it is necessary to examine the influence of different kinds of exercise programs on the functioning of the nervous system (SN), as well as on the perceptual-motor qualities that depend on it. Indeed, it is believed that certain kinds of physical training can improve people’s level of motor control and cognitive functioning and, in turn, help them lead more effective everyday lives3.
As we go about our daily activities, the central nervous system (CNS) has to process both motor and cognitive information, sometimes separately and sometimes simultaneously4,5. The frequency with which this information is processed interferes with the functioning of the brain that has to process it. The cycle of receiving information, processing it and developing an appropriate response is called a task4. A simple task is defined as one in which a single task to be performed by the subject is prioritized, either motor or cognitive4. On the other hand, a double task or “dual task” is one that requires the simultaneous performance of two tasks that can be performed independently and measured separately and have different objectives5. The dual task is common in daily life, especially in activities that involve the simultaneous performance of a cognitive function and a motor task5.
By motor skill or task, we understand one that involves a response in the form of muscle contraction, for example, postural control or a response to proprioceptive afferents. These responses can be controlled directly or indirectly in cognitive processes that can be conscious or unconscious6. Initially, proprioception was defined as the functional state of the joints and muscles that allows us to be aware of the movement or position of a part of the body or to respond unconsciously to the involuntary modification of our joint position in order to maintain postural control, muscle tone or muscle coordination7. Meanwhile, postural control is defined as the ability to maintain the center of body mass within the base of support8. Postural control is achieved using information received from the vestibular apparatus and the inner ear, as well as other visual, pressure, tactile and proprioceptive information9. Elsewhere, the concept of cognitive ability or tasks has been defined as the skills and the processes within the brain that allow us to receive, process and elaborate information to carry out a task10. This includes attention, understanding, elaboration and memorization of said information11.
During the aging process, there is a decrease in the above-mentioned motor and cognitive abilities, either due to the appearance of diseases such as Alzheimer's or to factors associated with a person’s lifestyle and lifelong physical activity habits12. This is why doing more everyday social activities can lead to the improvement of motor and cognitive skills, given that performing single or double tasks has an effect on these skills4. Recent studies confirm that a higher educational and occupational level has a direct relationship with a high degree of Cognitive Reserve (CR)12, that is the capacity that the brain develops to more efficiently tolerate the effects of a greater number of neuropathologies (such as those associated with dementia) before the symptoms manifest clinically13.
Given the link between physical and cognitive tasks, performing physical exercise simultaneously with cognitive exercise improves motor and cognitive parameters, making it possible for the older adult population to delay the onset of diseases such as Alzheimer's or dementia or to slow the development of their symptoms14–16. Furthermore, Work on joint postural control and proprioception are one of the main objectives of researchers studying the older adult population because, since as people reach a certain age they are at a greater risk of suffering bone fractures that can limit their functionality in daily life17,18. Work on this abilities, has been demonstrated to reduce the risk of falls in older people19,20, thus reducing the risk of injury to the lower limbs (Riva et al., 2016), in addition to improving balance and gait21.
The literature on motor-cognitive training indicates that a dual training program should last between 8 and 12 weeks and feature two to three sessions a week, of 15 to 45 minutes in duration in order for it to have a positive effect22. Such training initiatives are based on imbalance and walking exercises, combined with cognitive exercises such as counting, word memorization or the Stroop test or music and rhythm, they have been shown to improve performance on motor and cognitive control tests15,23. Music is used by many authors to work with people with cognitive or motor pathologies such as Alzheimer's, Parkinson's, among others, due to its motivational nature that implies greater adherence of this population to dual training programs and an increase of self-esteem in critical stages of the disease24. Furthermore, in older people, music has a beneficial effect thanks to its multitasking nature, since listening to lyrics or musical notes activates different parts of the brain, working on aspects such as memory or concentration, and in turn, to follow the rhythm we pay attention to balance, space and coordination with colleagues, this influencing the prevention of falls, since maintaining a constant rhythm facilitates the rhythmic movements of walking23. This improvement positively correlates with correct motor and cognitive functioning, delaying the deterioration of these systems and improving the basic executive functions that are essential for daily life21,25,26.
Currently, many researchers are interested in the older adult population and in how training can improve their quality of life. A recent systematic review concludes that dual-task exercise is more effective than single-task exercise at reducing the risk of falls in healthy adults27. Prior studies have documented typical training programs to prevent falls in older adults, most of them focused on people with pathologies such as Parkinson's, Alzheimer's, dementia or knee joint problems that cause them to fall more easily22,27.
Despite this, there is still little information and few studies regarding the inclusion of double motor-cognitive tasks in training sessions focused on improving the quality of life of healthy and physically active older adults, which do not focus solely and exclusively on falls or cognitive impairments. Therefore, the aim of this study was to evaluate the effects of an 8-week cognitive-motor training program accompanied by a simultaneous cognitive task on the postural control and knee proprioception of healthy and physically active older adults.
We hypothesize that the inclusion of the dual motor-cognitive task in the training sessions will improve performance on the postural control and proprioception tests carried out with a simultaneous cognitive task after eight weeks compared to the control group which will not do dual training.
2. Materials and Methods
2.1. Design
A randomized clinical trial was used to determine the effects of the inclusion of a dual motor-cognitive task in postural control and proprioception training
2.2. Participants
The study included 20 healthy and physically active older adults [according to the results of the International Physical Activity Questionnaire (IPAQ) 3912.52 ± 1738.57; Metabolic Equivalents (METS)] of between (73.25 ± 5.98 years) and with (56,8 ± 16,78CR. They were recruited in a Barcelona sport center during October of 2019 and who volunteered to participate in the study. We were randomly allocated into an experimental or a control group (EG and CG). Exclusion criteria included: i) suffering from a neurological condition such as Alzheimer's or Parkinson's disease, ii) an inability to perform one or more of the parts of the test, iii) being on medication that altered the normal functioning of the nervous system and/or, iv) having recently had lower limb joint replacement surgery (in the 12 months prior to the tests).
The study was carried out in accordance with the ethical standards established in the latest version of the Declaration of Helsinki, and it was approved by the ethics committee of the Ramon Llull University, ID number 1718006D. All participants in the study were informed of the procedure and signed informed consent documents.
2.3. Proprioception
To evaluate proprioception, the Absolute Error of joint repositioning at 45º (AEr45º) of the knee of the dominant leg was calculated with a valid and reliable mobile application called Goniometer Pro, installed on a smartphone Galaxy J7 (Samsung, Seoul, South Korea). Using this application, previously validated28, the mobile device can be used as a digital goniometer (2.9, FiveFufFive co, Bloomfield, NJ, United States) providing instantaneous, accurate and repeatable readings of the range of movement (ROM), to measure the difference between the requested and developed knee angle29.
Firstly, orthopedic boots (Figure 1) were placed on each of the subjects' legs in order to cancel the adaptation made by the toes and ankle and focus on the exclusive use of the knee. Next, the researchers placed the smartphone aligned to the longitudinal of the femur, with the base of the device aligned to the interline of the femorotibial joint.
Although in previous works ski boots were used to limit the movement of the toes and ankle30, in this study the ski boot was replaced with the orthopedic one, due to the ease of putting on and remove the boot, in addition to being able to match all subjects equally in terms of sizes or support, since the boots had adjustable straps that adapted to any foot size, thus restricting plantar flexion and dorsiflexion.
Once the subjects were equipped with the instruments, they closed their eyes and the researchers placed them in a 45º knee flexion position and instructed them to maintain that position for six seconds. Subsequently, the subjects were asked to recover the initial standing position and, when they were ready, to flex their knees again until they reached the position in which they believed they had been previously positioned by the researcher with their eyes closed. The repositioning angles on the dominant knee were noted by repeating the measurement 3 times and recording the average of the results. The absolute value of the difference between the requested angle (45º) and the one realized was recorded, to determine the joint repositioning capacity of the participants, a variable through which conscious proprioception is quantified29.
2.4. Postural Control
Postural control was assessed with a Kistler force platform (Kistler Instruments AG, Winterthur, Switzerland) connected to a laptop computer running Kistler MARS 3.0 software. To evaluate bipodal and unipodal postural control, subjects were asked to stand on the platform and perform the Romberg test in 3 different conditions: Romberg bipodal open eyes (RBOE); Romberg bipodal closed eyes (RBCE); and Romberg unipodal dominant leg (RUDL). Prior to carrying out the test, participants received guidelines. They were told to stay upright with their gaze fixed on a point and their arms extended laterally close to the trunk. They were also asked to place their feet with at a width similar to that of their shoulders for the bipodal test. In the case of the unipodal postural control tests, the subjects were asked to perform a 45º knee flexion. As in the proprioceptive test, the subjects wore orthopedic boots on each of their legs to use the same conditions for the proprioceptive and postural control tests. The duration of each test was 30 seconds, and three repetitions were performed for each condition.
The postural control variables that were obtained from the Center of Pressure (CoP) signals acquired by the force platform were the total area and the average velocity in the antero-posterior (MVAP) and medio-lateral (MVML) directions. While the total area is an indicator of the performance of the postural control task, the MVAP and MVML reveal the neuromuscular activity used to maintain postural control31. In all the variables studied, lower values are associated with better performance on the task.
The measurements of variables related to proprioception and postural control were carried out in a room free of disturbances and distractions. The order of carrying out the tests was randomized for each subject, and each of the conditions was repeated three times for a period of 30 seconds.
2.5. Cognitive Control
To carry out the dual task performance, subjects performed a cognitive task while their postural control and proprioception were evaluated32. The cognitive task came from the subscale called “categorical evocation in associations”, which is part of the battery of subscales of the Revised Barcelona Test33. The task consisted of mentioning the maximum number of words possible for 30 seconds belonging to the same semantic field. The researchers determined the semantic fields so that they were known by all subjects regardless of age. The semantic fields chosen were the following: 1.Animals; 2.Fruits; 3.Cities; 4.Parts of the body; 5.Clothing; 6.Meals; 7.Countries; 8.Colors; 9.Women's names; 10.Men's names. The score obtained depended on the number of words remembered, scoring one point for each of them. No points were added for repeated words or synonyms33. To quantify the total number of words that the subjects said, they were recorded, and once the tests were finished, the total number of words mentioned in each repetition was counted.
Each motor test was performed three times, so for each of the repetitions the subjects were asked about different semantic fields so that prior learning or short-term memory did not influence the motor results.
2.6. Procedure
A few days before carrying out the measurement protocol, the researchers visited the institutions from which the participants had been recruited, to collect data by an anonymous formular sent by email to the participant. Prior to sending the email we check that older adults were familiar with the internet, and we gave them verbal instructions to fulfilling the formular. This included information on the participants’ physical characteristics, along with data to determine whether the individuals fulfilled the inclusion/exclusion criteria, not medical history was collected. In accordance with34 the participants’ lower limb dominance was established through a self-report on their performance on bilateral movement tasks involving the legs. To ensure that the order of the tests did not influence the results, the instruments were administered in a randomized order to each of the participants. In addition, the subjects answered a validated CR scale questionnaire which consisted of 24 questions related to their lifestyle to provide us with information about his life35. Finally, each participant completed the short version IPAQ36 to provide us with information about his or her self-reported degree of physical activity.
Once the tests were completed, the members of the sample were randomly assigned to the experimental EG and CG groups. After 8 weeks of intervention, the subjects were measured again on the postural control and proprioception tests with a cognitive task simultaneously.
2.7. Intervention Protocol
Once the pre-intervention measurements had been completed, an 8-week training protocol was carried out. The subjects, as previously mentioned, were randomly assigned into two groups, a control group and an experimental group.
Each participant of both the EG and CG conducted two sessions per week in different days to avoid contamination between the groups. Sessions lasted thirty minutes and consisted of a five-minute warm-up, a twenty-minute main section, and a five-minute cool-down period. During the main part of each session, the instructors worked to ensure that the exercises were technically executed in the correct manner in order to avoid injuries and to help promote the improvement of the participants' postural control and proprioception.
The main part began with a series of general mobility exercises. Next, a simple choreography was taught. The steps were divided into five measures of thirty-two beats, each of them divided into four parts of eight movements. The cool-down period consisted of breathing exercises and basic stretching.
The difference between the training protocols of the EG and the CG was in the inclusion in the EG sessions of the singing of unknown music. Meanwhile, the CG performed the same exercises without musical accompaniment. The EG was asked to make the mental effort required to memorize and learn the songs that were playing in the first sessions, and then to try to sing them while they were doing their motor exercises. Only two exercise choreographies were performed with the same music, one for the first four weeks and the other for the remaining weeks, in order to allow participants to become familiar with the lyrics. Meanwhile, the control group performed the motor exercises without music with the instructions of the person carrying out the session.
Four different sessions were designed (Annex 3). Each of these sessions was repeated for two full weeks during the 8 weeks, so the participants were able to learn to perform the various exercise techniques well to carry them out correctly. Sessions were designed to ensure that exercises got progressively more difficult, beginning with individual balance and proprioception exercises in the first session, then moving on to activities in pairs in the second, trios in the third, and groups of four in the fourth and until the end of the protocol. The proposed exercises included simple and complex walks, lateral movements, forward and backward movements, simple balances with both legs, and more complex ones performed along with classmates and with knee flexions of no more than 45º so that they would be related to the proprioception tests. For example, when performing a squat, imbalance activities were carried out with pairs or trios to compromise the stability of the participants, or participants were asked to do dances such as the twist or the conga. This was in addition to working on balance and promoting socialization and fun for the participants.
Once the intervention was completed, the subjects performed the measured postural control and proprioception tasks again, along with a simultaneous cognitive task (dual task), to help determine the effects of the intervention.
2.8. Statistical Analysis
Statistical analysis was performed using SPSS Version 21 software (SPSS Inc., Chicago, IL, USA). Prior to this analysis, the Kolmogorov-Smirnov test was applied to analyze the distribution of the variables. All variables showed a normal distribution, and, in order to verify the proposed hypotheses, a mixed model analysis of variance (ANOVA) was applied to evaluate the effects of an intra-subject factor (time: pre and post) and an inter-subject factor (group: control and experimental) under each of the execution conditions of postural control (open eyes (OE), closed eyes (CE) and unipodal leg (UDL)), proprioception and cognitive task.
The descriptive data on the variables are presented as mean ± SD. Follow-up of multivariate contrasts was performed using univariate contrasts. When statistically significant main or interaction effects were found, pairwise comparisons were performed using the Bonferroni correction. This correction was applied to all results. A value of p<0.05 was accepted as the level of significance for all statistical analyses.
3. Results
The multivariate contrasts in the RBOE condition showed a significant main effect of the time factor, indicating that both groups (control and experimental) recorded better results in the post-intervention measurements (F4,15 = 11.87, p < 0.001, η²p= 0.76). However, no significant group x time interaction effect was found, meaning that the results of the intervention program did not vary as a function of the group. The univariate analysis reported that the time effect was significant in all postural control variables in this condition but was not significant in the results of the cognitive task. The pairwise comparisons can be seen in Figure 2.
The multivariate analyzes under the RBCE condition showed a significant main effect of the time factor, with better results registered in the post-intervention measurements for both groups (control and experimental) (F4,15 = 11.62, p <0.001, η²p= 0.75). Nonetheless, as in the previous condition, no significant group x time interaction effect was found, so the intervention program had differing effects as a function of the group. The univariate analysis revealed that the effect of time was significant in all postural control variables in this condition but was not significant when it came to the results on the cognitive task. The differences between pairs can be seen in Figure 3.
The multivariate analyses carried out in the RUDL condition did not show a significant main effect of the time factor or a significant interaction of time x group. The differences between pairs can be seen in Figure 4.
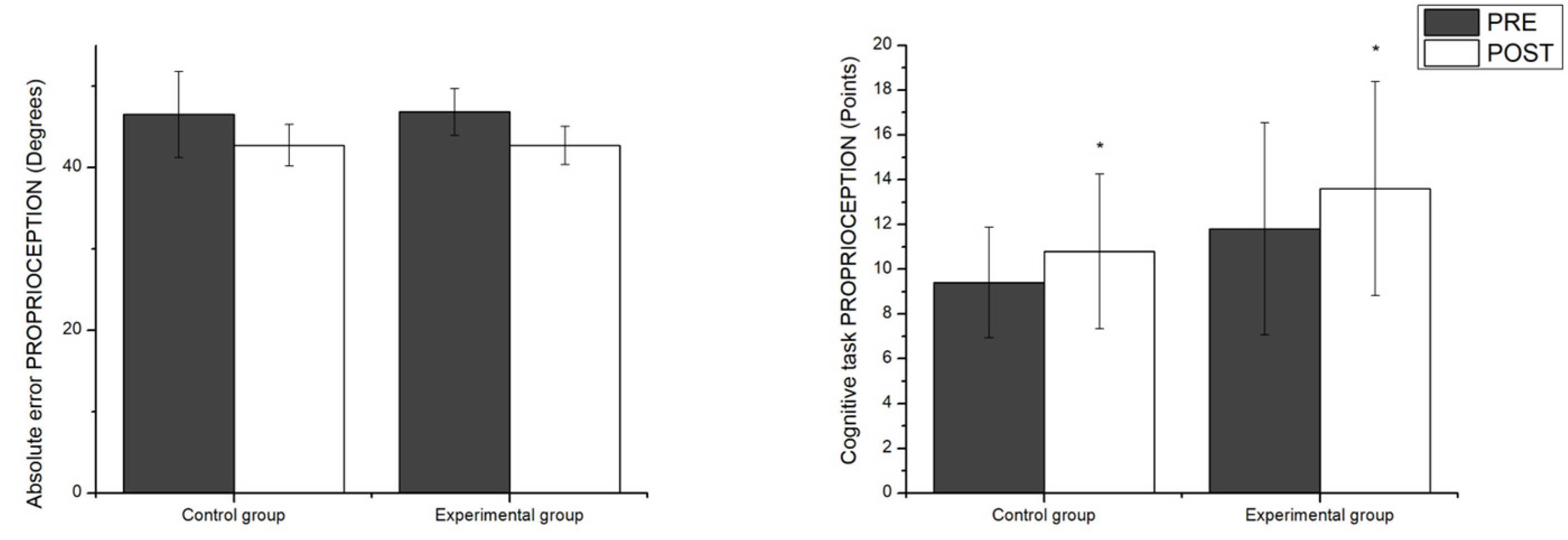
Meanwhile, a significant main effect of the time factor was found on the results for proprioception (F1,18 = 11.53, p <0.003, η²p= 0.39). It should be noted, though, that just as in the previous postural control conditions there was no significant interaction between group x time. The measuring the scores on the cognitive task performed during the proprioception tests did not show a significant main effect of the time factor or interaction. Differences between pairs of proprioception variables can be observed in Figure 5.
4. Discussion
The aim of this study was to evaluate the effects of an eight-week training program on the postural control and knee proprioception of healthy adults, with the inclusion of a cognitive task performed simultaneously.
The main finding shows that a physical training program aimed at improving motor skills, has a positive impact on the results of proprioception and postural control tests after eight weeks of training. That is, the scores on the proprioception and postural control tests with eyes open and closed, with a simultaneous cognitive task, improved both in the EG (who performed the motor task with sung music) and in the CG (who performed the same motor task without musical accompaniment). In light of the results, it seems that the intervention with the inclusion of a cognitive task such as singing unknown music did not post a greater cognitive processing challenge than the one posed to the control group, which only had verbal reinforcement from the researcher during the execution of the same exercises. A possible explanation for the absence of differences between the experimental and control groups may be that, in the absence of music, the researcher sought other ways to improve the motivational level of the control group participants. These efforts to motivate the members of the control group could have positively influenced their level of attention. It is well known that increasing the attentional capacity of subjects improves the conscious registration of perceptual-motor qualities, including proprioception and postural control37,38. The motivational intensity of the researcher may have been a contaminating factor in the study, since it could have served as a cognitive stimulus for the CG and might have thus contributed to the lack of differences between the scores on the cognitive task of the EG with respect to those of the CG. In other words, it is possible that both groups have trained indirectly under the same motor-cognitive dual task paradigm. In this sense, these results would be in line with studies that show that dual training plays an important role in the transfer of the skill worked on, so specific training of motor-cognitive skills can favor positive results in the analyzed tests. Such training methods have also been found to have durability over time18,39.
Another possible explanation for the main finding could be related to the kinds of athletic activities that the participants had carried out prior to the study. The members of both groups had participated in directed choreographed activities with musical accompaniment in their prior training programs with a frequency of 2 to 3 sessions per week. This could have interfered with the results, as the cognitive task of singing unfamiliar music when exercising may not have represented as great a difficulty for them. In other words, there may have been no additional challenge beyond they were used to, even if it was a different activity than usual40.
It is also possible that the characteristics of the proposed training, featuring the use of a fixed attentional focus for the motor task and a secondary focus on the cognitive task, could have contributed to improving the participants’ results on the motor-cognitive tests. However, no differences were found between the group with cognitive tasks and the one without. In line with what was mentioned above, the variable prioritization of the parameters to be trained, that is, the motor and cognitive tasks developed in the training, is considered essential for the effectiveness of dual training39, since it has been demonstrated that, in order for dual training to be effective at improving specific variables, it is necessary to give instructions that place a priority on these specific variables or skills. In other words, instructors must change the attentional focus of the motor and cognitive task sequentially41,42.
It should also be noted that few studies have specifically used music in training programs aimed at healthy and physically active subjects. This means that there is still little data in this regard, and a greater number of interventions are needed to paint a more complete picture of how music can affect performance on motor exercises. However, those authors who have introduced multitasking exercises based on music and rhythm in older adult populations have found that the available cognitive resources are increased, thus improving gait control43 and balance, as well as producing a reduction in the rate of falls in said population17. Furthermore, dance or choreographed workouts with music have been shown to be a therapeutic tool for people with cognitive and motor pathologies such as Parkinson's, cancer or neurological disorders44–46, as these activities include movements of all parts of the body and appear to improve adherence to sports activities, as well as leading to benefits in cognitive and balance parameters45,46. At the same time, activities with music have a strong social and motivational factor that favors the improvement of the well-being of subjects' lives and contributes to the fight against a sedentary lifestyle in people with previous pathologies47,48.
Considering the results, it seems that the simple physical training program of the perceptual motor qualities that was carried out here has led to improvements in the results on the postural control tests with open and closed eyes, as well as the results for knee proprioception. As confirmed by various authors, training programs that are aimed at single tasks (in this case motor tasks) and that work on parameters similar to those used in the measurement tests, tend to be an effective way to improve the results on said tests, due to automation and transfer of the tasks performed. Additionally, tasks that include explicit instructions that focus on postural control when training under dual tasks also improve motor results18,49,50. That is, training in specific concepts through frequent repetition of exercises replicating the specific tasks to be measured tends to improve performance51. Furthermore, it is known that focusing training on physical qualities such as proprioception and postural control delays the aging process, linked to the fragility of older adults, and prevents the risk of falls49,52.
Within the training program, both groups performed exercises where postural control and balance were compromised in positions in which the knee oscillated between 45º of flexion and full extension. It is accepted that the lower limbs, and especially the knee joint, play a very important role in postural control. The position of the knee, along with the position of the hip, ankle, and toes, provides greater stability to the body. This stability is achieved thanks to the continuous flow of proprioceptive information through the ligaments, joint capsules and muscles that surround these joints, which allows anteroposterior stabilization and rotation of the knee53. In turn, the 45º flexion position has a direct relationship with dynamic and static balance, since it is the position from which the ability to generate force in the quadriceps and hamstrings increases. These muscles are essential for motor skills and stability of the body54.
When it came to the effects of the training program on unipodal postural control, no significant differences were found between the pretest and the posttest. Indeed, there was even a slight worsening of motor performance on the second test, although it was not significant. It is possible that adding an auditory the auditory afferent of sung music in the experimental group may have worsened their conscious registration of the afferents related to balance, as well as of the proprioceptive afferents that could improve postural control and help maintain balance. This may have caused the results of the unipodal postural control tests to remain unchanged or to have worsened slightly after the intervention. This may be due to the inability of the nervous system (NS) to process a sensory input of a motor nature in the primary sensory cortex when the input is at a lower intensity and frequency than the auditory input, since the auditory and motor neuronal pathways and their brain processing area are closely linked55. The present results are in line with previous studies, as it has been shown that older adults make use of higher-level sensorimotor cortical areas during complex motor tasks (such as unipodal postural control), which may cause a greater dependence on cognitive information to process cortical sensory information that allows controlling movement56. It is also necessary to mention that both the difficulty of the motor task and the reduction of the support base when performing the exercises and motor tests can cause the results to vary, producing a greater displacement of the CoP57,58. When there is a reduction in the base of support, there is a higher requirement for proprioceptive information to align the joints as well as possible on the point of support, causing vision, touch, or vestibular information, are not the only ones who interfere59.
There were no significant differences between the pretest and posttest results on the cognitive task, which means that the subjects did not change the number of responses given to the semantic fields proposed in the “categorical evocation in associations test”, which was analyzed simultaneously with the motor tests. This may have several explanations, the first of which would be the possible adaptation by the subjects to the tests, given that the semantic fields proposed for the analysis of the cognitive task were not modified18. Furthermore, the fact that the cognitive training carried out had no direct relationship with the cognitive test may have influenced the degree of neuroplasticity created in the brain. When more specific exercises are worked on repetitively, this can lead to a greater change in test performance38,60. Additionally, the characteristics of the subjects in the sample may have influenced their performance on the cognitive test, since they had a high cultural level, as shown by the results on the CR scale. This seems to indicate that the cultural background of the subjects helped them to execute the double cognitive task, since the higher the cultural level of a subject, the greater the formation of neural networks that allow them to associate new learning with prior learning, thus improving cognitive functions and reducing their deterioration61,62.
There is controversy when it comes to determining the duration and type of dual-task training programs that improve the motor performance of healthy older adult subjects. Some researchers claim that in order to produce improvements one needs between 8 and 12 weeks of two to three sessions of 15 to 45 minutes per week22. Others, consider a minimum of 12 weeks of dual-task training to be necessary for the effect to be maintained over time, and they argue that variable-priority instructions must be given motor-cognitive tasks50. A recent systematic review highlights that the main limitation of dual-task training programs is the heterogeneity in the exercises carried out and the lack of specification of the difficulty of the secondary task18.
Although there is scientific evidence on the consequences of the cognitive-motor deterioration suffered by the older adult population18, there are few studies in populations of healthy and physically active older adults, so more studies are necessary to allow for the creation of training programs suitable for this population, especially given increases in longevity in a healthy society.
5. Conclusions
The development of an eight-week physical training program aimed at improving proprioception and postural control has improved the performance on postural control (with open eyes and closed eyes) and proprioceptive tests but has not improved control results for unipodal posture. The dual cognitive-motor task intervention with the inclusion of unknown sung music in the EG training sessions did not improve performance in the postural control and proprioception tests carried out with a simultaneous cognitive task with respect to the CG. More research is needed on dual training in healthy and physically active subjects to adapt training with dual motor-cognitive tasks to the needs of this population group.
Author Contributions
Conceptualization, J.M., M.S.-T. and A.N.-G.; Data curation, J.M., M.S.-T. and A.N.-G.; Formal analysis, J.M., M.S.-T., and A.N.-G.; Investigation, J.M., M.S.- T. and A.N-G.; Methodology, J.M., M.S.-T., C.C. and A.N.-G.; project administration J.M., M.S.-T. and A.N.-G.; Resources, J.M., M.S.-T., C.C. and A.N.-G.; software, J.M., M.S.-T., and A.N.-G.; Supervision, J.M., M.S.-T., C.C. and A.N.-G.; Validation, J.M., M.S.-T., C.C. and A.N.-G.; visu-alization, J.M., M.S.-T., C.C. and A.N.-G.; writing—original draft preparation, A.N.-G.; writing—review and editing J.M., M.S.-T., M.G.G. and A.N.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by INVESTIGO PROGRAM, for the recruitment of young people seeking employment to carry out research and innovation initiatives, within the framework of the Recovery, Transformation and Resilience Plan - financed by the European Union - Next Generation EU, for the year 2022, grant number 100045ID11.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and ap-proved by the Institutional Review Board (or Ethics Committee) of CER- FPCEE Blanquerna (protocol code 1718006D, date May 20th, 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data can be found at the following link: https://doi.org/10.6084/m9.figshare.25982335.v1.
Acknowledgments
The authors would like to thank all the participants who have taken part in this study.
Conflicts of Interest
The authors declare no conflict of interest
References
- Papathanasiou, I.V.; Rammogianni, A.; Papagiannis, D.; Tsaras, K.; Kaberi, F.; Kontopoulou, L.; Neroliatsiou, A.; Fradelos, E. Quality of Life among Elderly Population. Ment. Heal. Glob. Challenges J. 2019, 2. [Google Scholar]
- Williams, G.A.; Jacob, G.; Rakovac, I.; Scotter, C.; Wismar, M. Health Professional Mobility in the WHO European Region and the WHO Global Code of Practice: Data from the Joint OECD/EUROSTAT/WHO-Europe Questionnaire. Eur. J. Public Health 2020, 30 (Supplement_4), iv5–iv11. [Google Scholar] [CrossRef] [PubMed]
- Azadian, E.; Torbati, H.R.T.; Kakhki, A.R.S.; Farahpour, N. The Effect of Dual Task and Executive Training on Pattern of Gait in Older Adults with Balance Impairment: A Randomized Controlled Trial. Arch. Gerontol. Geriatr. 2016, 62, 83–89. [Google Scholar] [CrossRef]
- da Silva, E.M.; Sepúlveda-Loyola, W.; da Silva, J.M.; dos Santos, G.C.; Pereira, C. Comparación Entre Simple y Doble Tarea, Capacidad Cognitiva y Equilibrio Postural En Adultos Mayores Que Participan de 3 Modalidades de Ejercicio Físico. Fisioterapia 2020, 42, 33–38. [Google Scholar] [CrossRef]
- McIsaac, T.L.; Lamberg, E.M.; Muratori, L.M. Building a Framework for a Dual Task Taxonomy. Biomed Res. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Solana-Tramunt, M. Entrenament de La Propiocepció Conscient de La Columna Vertebral Lumbar: Una Aplicació a La Natació Subaquàtica. 2011, 316.
- Sherrington, C.S. Yale University Mrs. Hepsa Ely Silliman Memorial Lectures. The Integrative Action of the Nervous System. New Haven, CT, US: Yale. 1906. [CrossRef]
- Ivanenko, Y.; Gurfinkel, V.S. Human Postural Control. Front. Neurosci. 2018, 12, 171. [Google Scholar] [CrossRef]
- Gaerlan, M.G. The Role of Visual, Vestibular, and Somatosensory Systems in Postural Balance. Univ. Nevada Las Vegas 2010. [Google Scholar]
- Reed, S.K. Cognition: Theories and Applications; CENGAGE learning, 2012.
- Barca-Enriquez, E.; Brenlla, J.C.; Peralbo, M.; Almeida, L.S.; Porto, A.; Barca, A. Habilidades Cognitivas, Autoeficacia y Estrategias de Aprendizaje: Indicadores y Determinantes Del Rendimiento Académico En El Alumnado de Educación Secundaria. Rev. Estud. e Investig. en Psicol. y Educ. 2015, 83–89. [Google Scholar] [CrossRef]
- Liu, Y.; Lachman, M.E. Education and Cognition in Middle Age and Later Life: The Mediating Role of Physical and Cognitive Activity. Journals Gerontol. Ser. B 2020, 75, e93–e104. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive Reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef]
- Coelho, F.G.D.M.; Andrade, L.P.; Pedroso, R.V.; Santos-Galduroz, R.F.; Gobbi, S.; Costa, J.L.R.; Gobbi, L.T.B. Multimodal Exercise Intervention Improves Frontal Cognitive Functions and Gait in Alzheimer’s Disease: A Controlled Trial. Geriatr. Gerontol. Int. 2013, 13, 198–203. [Google Scholar] [CrossRef]
- Andrade, L.P.; Gobbi, L.T.B.; Coelho, F.G.M.; Christofoletti, G.; Riani Costa, J.L.; Stella, F. Benefits of Multimodal Exercise Intervention for Postural Control and Frontal Cognitive Functions in Individuals with Alzheimer’s Disease: A Controlled Trial. J. Am. Geriatr. Soc. 2013, 61, 1919–1926. [Google Scholar] [CrossRef] [PubMed]
- Real Pérez, M.; Robles Rodríguez, C.; Ponce González, J.G. Revisión Narrativa y Desarrollo de Un Programa de Intervención Para La Disminución de Los Efectos Del Alzheimer a Través de La Práctica Del Surf En Personas Mayores. RETOS. Nuevas Tendencias en Educ. Física, Deport. y Recreación 2017, No. 32.
- Trombetti, A.; Hars, M.; Herrmann, F.R.; Kressig, R.W.; Ferrari, S.; Rizzoli, R. Effect of Music-Based Multitask Training on Gait, Balance, and Fall Risk in Elderly People: A Randomized Controlled Trial. Arch. Intern. Med. 2011, 171, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Varela-Vásquez, L.A.; Minobes-Molina, E.; Jerez-Roig, J. Dual-Task Exercises in Older Adults: A Structured Review of Current Literature. J. Frailty, Sarcopenia Falls 2020, 5, 31. [Google Scholar] [CrossRef]
- Fernández, V.P.; SierraVinuesa, R.; Fernández, E.C. 14.-Importancia Del Desarrollo de Un Programa de Fisioterapia En La Reeducción Del Equilibrio En Nuestros Mayores. In VI Congreso internacional de deporte inclusivo: Salud, desarrollo y bienestar personal; Universidad Almería, 2018; Vol. 83, p 119.
- Velastegui Yunda, Z.F. Ejercicios de Equilibrio Como Método de Prevención Del Síndrome de Caída Para Los Usuarios Del Proyecto de Desarrollo Integral Del “Adulto Mayor” de La Parroquia Flores–Gad-R. Universidad Nacional de Chimborazo, 2018 2018.
- Falbo, S.; Condello, G.; Capranica, L.; Forte, R.; Pesce, C. Effects of Physical-Cognitive Dual Task Training on Executive Function and Gait Performance in Older Adults: A Randomized Controlled Trial. Biomed Res. Int. 2016, 2016. [Google Scholar] [CrossRef]
- Ghai, S.; Ghai, I.; Effenberg, A.O. Effects of Dual Tasks and Dual-Task Training on Postural Stability: A Systematic Review and Meta-Analysis. Clin. Interv. Aging 2017, 12, 557. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-L.; Pei, Y.-C. Musical Dual-Task Training in Patients with Mild-to-Moderate Dementia: A Randomized Controlled Trial. Neuropsychiatr. Dis. Treat. 2018, 1381–1393. [Google Scholar] [CrossRef] [PubMed]
- Haputhanthirige, N.K.H.; Sullivan, K.; Moyle, G.; Brauer, S.; Jeffrey, E.R.; Kerr, G. Effects of Dance on Gait and Dual-Task Gait in Parkinson’s Disease. PLoS One 2023, 18, e0280635. [Google Scholar] [CrossRef]
- Hiyamizu, M.; Morioka, S.; Shomoto, K.; Shimada, T. Effects of Dual Task Balance Training on Dual Task Performance in Elderly People: A Randomized Controlled Trial. Clin. Rehabil. 2012, 26, 58–67. [Google Scholar] [CrossRef]
- Shin, S.-S.; An, D.-H. The Effect of Motor Dual-Task Balance Training on Balance and Gait of Elderly Women. J. Phys. Ther. Sci. 2014, 26, 359–361. [Google Scholar] [CrossRef]
- Bayot, M.; Dujardin, K.; Dissaux, L.; Tard, C.; Defebvre, L.; Bonnet, C.T.; Allart, E.; Allali, G.; Delval, A. Can Dual-Task Paradigms Predict Falls Better than Single Task?–A Systematic Literature Review. Neurophysiol. Clin. 2020. [Google Scholar] [CrossRef] [PubMed]
- Melián-Ortiz, A.; Varillas-Delgado, D.; Laguarta-Val, S.; Rodríguez-Aparicio, I.; Senent-Sansegundo, N.; Fernández-García, M.; Roger-de Oña, I. Reliability and Concurrent Validity of the App Goniometer Pro vs Universal Goniometer in the Determination of Passive Knee Flexion. Acta Ortop. Mex. 2019, 33, 18–23. [Google Scholar] [PubMed]
- Mourcou, Q.; Fleury, A.; Diot, B.; Vuillerme, N. IProprio: A Smartphone-Based System to Measure and Improve Proprioceptive Function. In Engineering in Medicine and Biology Society (EMBC), 2016 IEEE 38th Annual International Conference of the; IEEE, 2016; pp 2622–2625.
- Noé, F.; García-Massó, X.; Delaygue, P.; Melon, A.; Paillard, T. The Influence of Wearing Ski-Boots with Different Rigidity Characteristics on Postural Control. Sport. Biomech. 2020, 19, 157–167. [Google Scholar] [CrossRef]
- Paillard, T.; Noé, F. Techniques and Methods for Testing the Postural Function in Healthy and Pathological Subjects. Biomed Res. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Ghai, S.; Driller, M.; Ghai, I. Effects of Joint Stabilizers on Proprioception and Stability: A Systematic Review and Meta-Analysis. Phys. Ther. Sport 2016. [Google Scholar] [CrossRef] [PubMed]
- Peña-Casanova, J. Test Barcelona Revisado [Revised Barcelona Test]. Barcelona: Masson 2005.
- van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to Determine Leg Dominance: The Agreement between Self-Reported and Observed Performance in Healthy Adults. PLoS One 2017, 12, e0189876. [Google Scholar] [CrossRef] [PubMed]
- Leon, I.; García-García, J.; Roldan-Tapia, L. Estimating Cognitive Reserve in Healthy Adults Using the Cognitive Reserve Scale. PLoS One 2014, 9, e102632. [Google Scholar] [CrossRef]
- Toloza, S.C.M.; Gómez-Conesa, A. El Cuestionario Internacional de Actividad Física. Un Instrumento Adecuado En El Seguimiento de La Actividad Física Poblacional. Rev. Iberoam. Fisioter. y Kinesiol. 2007, 10, 48–52. [Google Scholar] [CrossRef]
- Green, C.S.; Bavelier, D. Exercising Your Brain: A Review of Human Brain Plasticity and Training-Induced Learning. Psychol. Aging 2008, 23, 692. [Google Scholar] [CrossRef]
- Mang, C.S.; Campbell, K.L.; Ross, C.J.D.; Boyd, L.A. Promoting Neuroplasticity for Motor Rehabilitation after Stroke: Considering the Effects of Aerobic Exercise and Genetic Variation on Brain-Derived Neurotrophic Factor. Phys. Ther. 2013, 93, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- Lemke, N.C.; Werner, C.; Wiloth, S.; Oster, P.; Bauer, J.M.; Hauer, K. Transferability and Sustainability of Motor-Cognitive Dual-Task Training in Patients with Dementia: A Randomized Controlled Trial. Gerontology 2019, 65, 68–83. [Google Scholar] [CrossRef]
- Bayot, M.; Dujardin, K.; Tard, C.; Defebvre, L.; Bonnet, C.T.; Allart, E.; Delval, A. The Interaction between Cognition and Motor Control: A Theoretical Framework for Dual-Task Interference Effects on Posture, Gait Initiation, Gait and Turning. Neurophysiol. Clin. 2018, 48, 361–375. [Google Scholar] [CrossRef]
- Kramer, A.F.; Larish, J.F.; Strayer, D.L. Training for Attentional Control in Dual Task Settings: A Comparison of Young and Old Adults. J. Exp. Psychol. Appl. 1995, 1, 50. [Google Scholar] [CrossRef]
- Kumar, C. Effect of Training Balance under Dual Task with Fixed and Variable Priority Instructions with Balance Impairment in Institutionalized Elderly Population. Indian J. Physiother. Occup. Ther. 2014, 8, 152. [Google Scholar]
- Kim, S.J.; Yoo, G.E. Rhythm-Motor Dual Task Intervention for Fall Prevention in Healthy Older Adults. Front. Psychol. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Bruyneel, A.-V. Effects of Dance Activities on Patients with Chronic Pathologies: Scoping Review. Heliyon 2019, 5, e02104. [Google Scholar] [CrossRef]
- dos Santos Delabary, M.; Komeroski, I.G.; Monteiro, E.P.; Costa, R.R.; Haas, A.N. Effects of Dance Practice on Functional Mobility, Motor Symptoms and Quality of Life in People with Parkinson’s Disease: A Systematic Review with Meta-Analysis. Aging Clin. Exp. Res. 2018, 30, 727–735. [Google Scholar] [CrossRef]
- Patterson, K.K.; Wong, J.S.; Prout, E.C.; Brooks, D. Dance for the Rehabilitation of Balance and Gait in Adults with Neurological Conditions Other than Parkinson’s Disease: A Systematic Review. Heliyon 2018, 4, e00584. [Google Scholar] [CrossRef]
- Brewer, L.; Horgan, F.; Hickey, A.; Williams, D. Stroke Rehabilitation: Recent Advances and Future Therapies. QJM An Int. J. Med. 2013, 106, 11–25. [Google Scholar] [CrossRef]
- Quiroga Murcia, C.; Kreutz, G.; Clift, S.; Bongard, S. Shall We Dance? An Exploration of the Perceived Benefits of Dancing on Well-Being. Arts Health 2010, 2, 149–163. [Google Scholar] [CrossRef]
- Campbell, A.J.; Robertson, M.C. Otago Exercise Programme to Prevent Falls in Older Adults. Wellingt. ACC Thinksafe 2003, 3. [Google Scholar]
- Silsupadol, P.; Shumway-Cook, A.; Lugade, V.; van Donkelaar, P.; Chou, L.-S.; Mayr, U.; Woollacott, M.H. Effects of Single-Task versus Dual-Task Training on Balance Performance in Older Adults: A Double-Blind, Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2009, 90, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice; Lippincott Williams & Wilkins, 2007.
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Neumann, D.A. Neumann, D.A. Kinesiology of the Musculoskeletal System-E-Book: Foundations for Rehabilitation; Elsevier Health Sciences, 2013.
- Wang, H.; Ji, Z.; Jiang, G.; Liu, W.; Jiao, X. Correlation among Proprioception, Muscle Strength, and Balance. J. Phys. Ther. Sci. 2016, 28, 3468–3472. [Google Scholar] [CrossRef] [PubMed]
- Thaut, M.H. Neural Basis of Rhythmic Timing Networks in the Human Brain. Ann. N. Y. Acad. Sci. 2003, 999, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Heuninckx, S.; Wenderoth, N.; Swinnen, S.P. Systems Neuroplasticity in the Aging Brain: Recruiting Additional Neural Resources for Successful Motor Performance in Elderly Persons. J. Neurosci. 2008, 28, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Asseman, F.; Caron, O.; Cremieux, J. Effects of the Removal of Vision on Body Sway during Different Postures in Elite Gymnasts. Int. J. Sports Med. 2005, 26, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Caron, O.; Gélat, T.; Rougier, P.; Blanchi, J.-P. A Comparative Analysis of the Center of Gravity and Center of Pressure Trajectory Path Lengths in Standing Posture: An Estimation of Active Stiffness. J. Appl. Biomech. 2000, 16, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Lackner, J.R.; DiZio, P. Vestibular, Proprioceptive, and Haptic Contributions to Spatial Orientation. Annu. Rev. Psychol. 2005, 56, 115–147. [Google Scholar] [CrossRef]
- Voss, M.W.; Prakash, R.S.; Erickson, K.I.; Basak, C.; Chaddock, L.; Kim, J.S.; Alves, H.; Heo, S.; Szabo, A.; White, S.M. Plasticity of Brain Networks in a Randomized Intervention Trial of Exercise Training in Older Adults. Front. Aging Neurosci. 2010, 2, 32. [Google Scholar] [CrossRef]
- Park, D.C. Mecanismos Básicos Que Explican El Declive Del Funcionamiento Cognitivo Con El Envejecimiento. In Envejecimiento cognitivo; Editorial Médica Panamericana, 2002; pp 3–22.
- Samite, L.D.; Schipani, J. Flexibilidad Cognitiva y Reserva Cognitiva En Adultos y Adultos Mayores. 2016.
Figure 1.
Orthopedic boots used in the study.

Figure 2.
Pairwise comparisons of the group factor as a function of time in the open eyes postural control variables. RBOE = Romberg bipodal open eyes; MV AP = mean velocity anterior-posterior; MV ML = mean velocity medio-lateral.
Figure 2.
Pairwise comparisons of the group factor as a function of time in the open eyes postural control variables. RBOE = Romberg bipodal open eyes; MV AP = mean velocity anterior-posterior; MV ML = mean velocity medio-lateral.
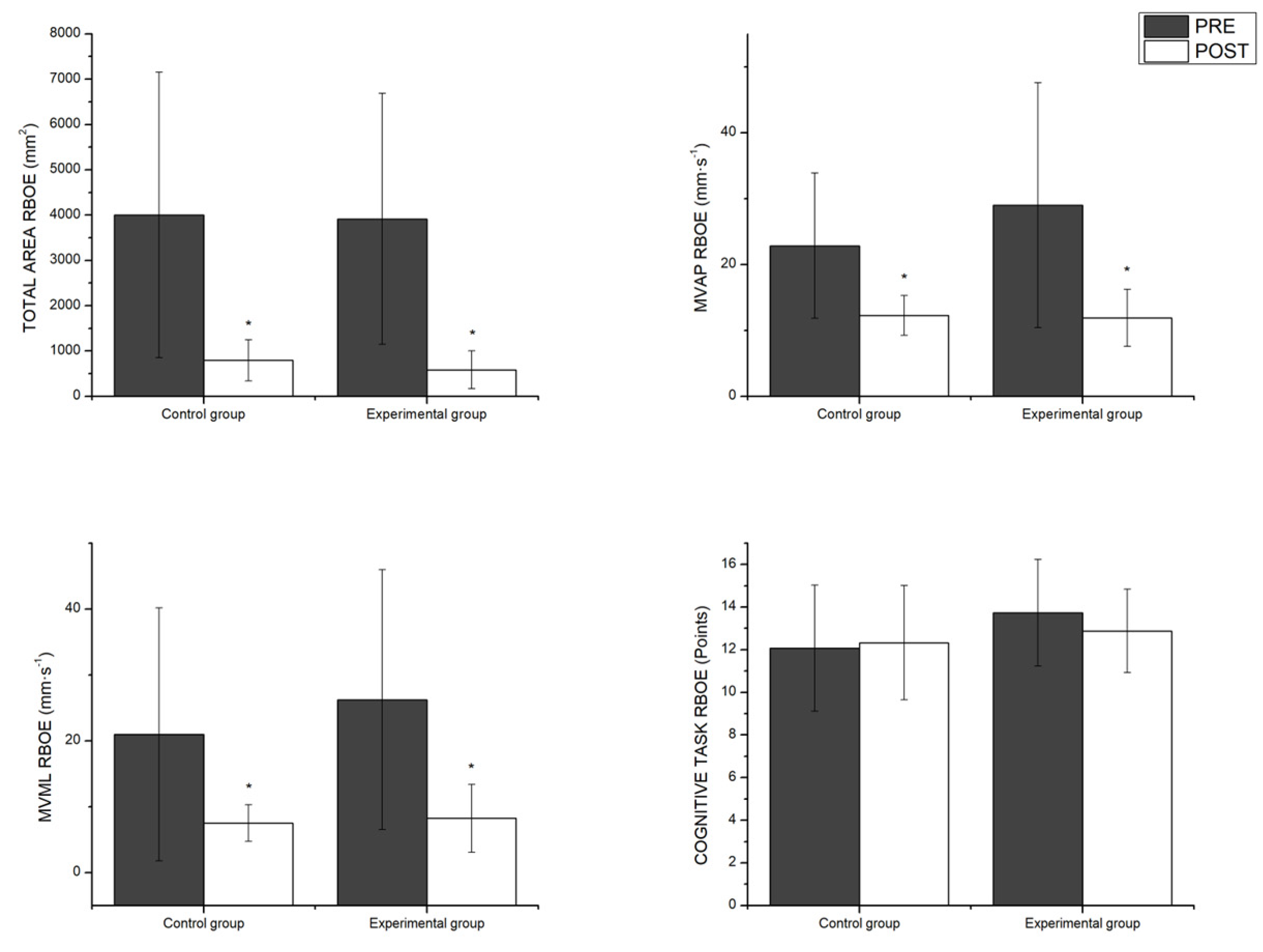
Figure 3.
Pairwise comparisons between groups as a function of time for the postural control and eyes closed variables. RBCE = Romberg bipodal closed eyes; MV AP = mean velocity anterior-posterior; MV ML = mean velocity medio-lateral.
Figure 3.
Pairwise comparisons between groups as a function of time for the postural control and eyes closed variables. RBCE = Romberg bipodal closed eyes; MV AP = mean velocity anterior-posterior; MV ML = mean velocity medio-lateral.
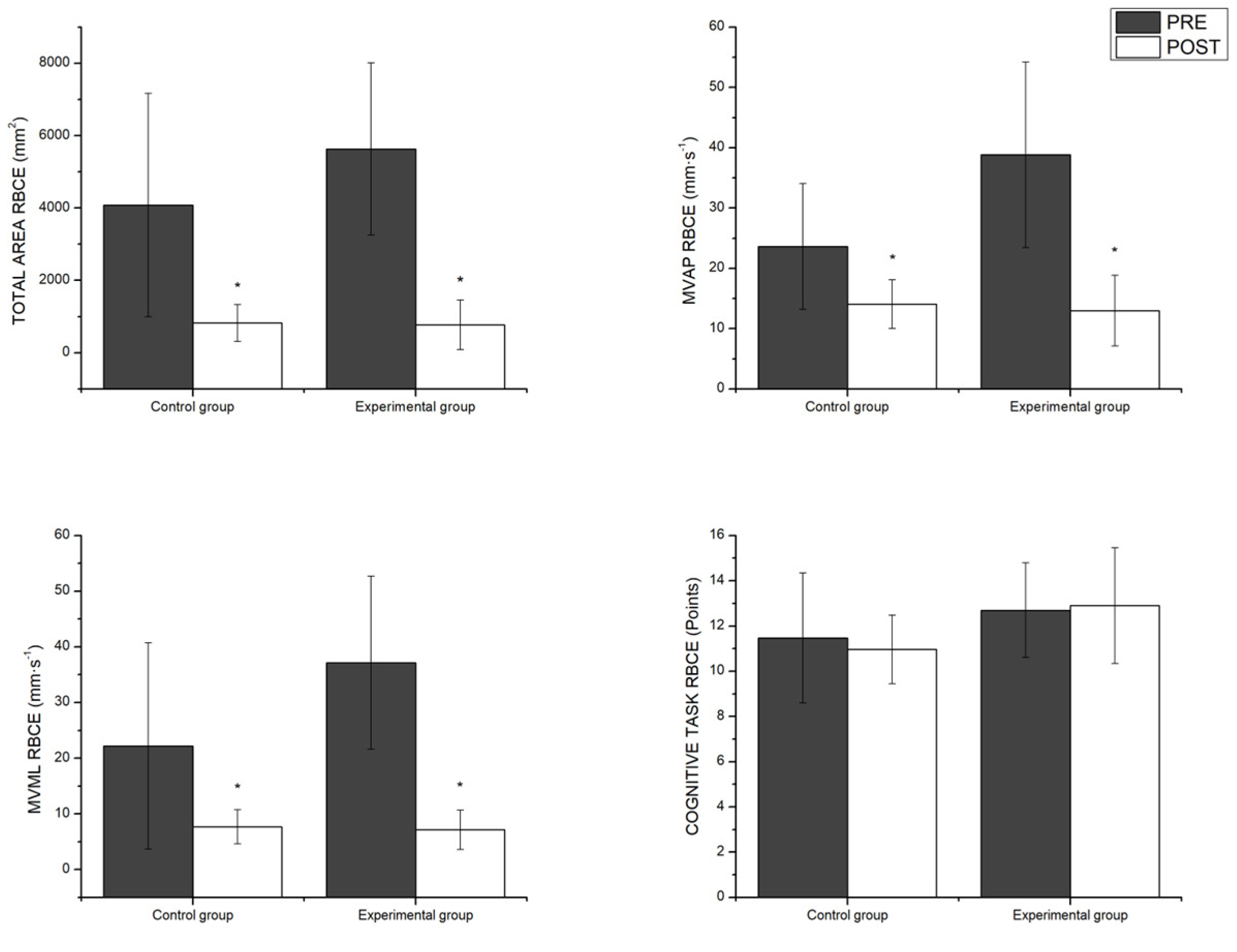
Figure 4.
Pairwise comparisons between groups as a function of time variables measuring unipodal postural control with the dominant leg. RUDL = Romberg unipodal dominant leg; MV AP = mean velocity anterior-posterior; MV ML = mean velocity medio-lateral.
Figure 4.
Pairwise comparisons between groups as a function of time variables measuring unipodal postural control with the dominant leg. RUDL = Romberg unipodal dominant leg; MV AP = mean velocity anterior-posterior; MV ML = mean velocity medio-lateral.
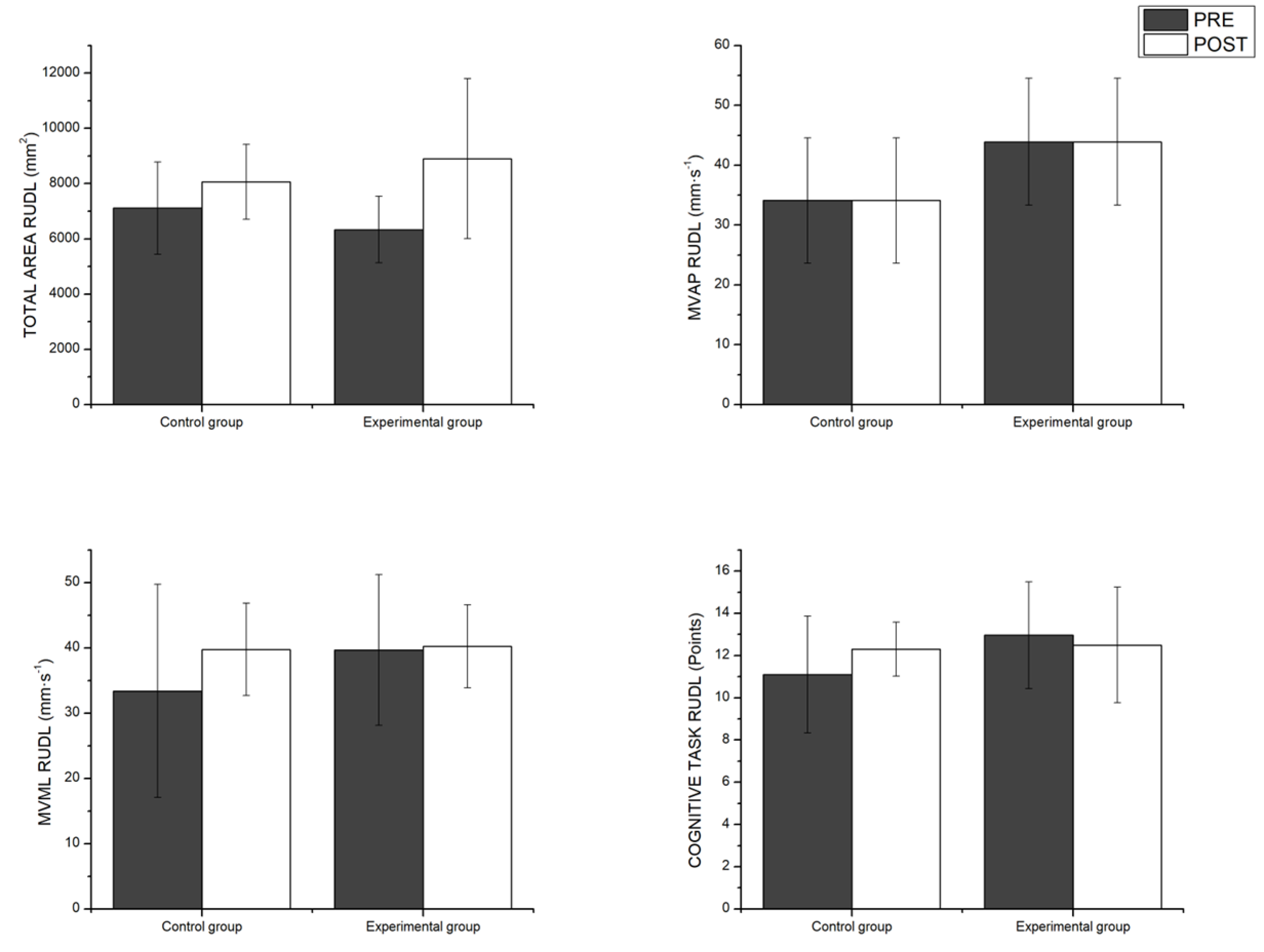
Figure 5.
Pairwise comparisons between groups as a function of time for the proprioception.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



