
Submitted:
23 June 2024
Posted:
24 June 2024
You are already at the latest version
Abstract
Background. The role of exercise programs during Substance Use Disorder (SUD) treatment is considered particularly supportive in fostering positive psychological and behavioral changes. The aim of this feasibility study was to explore the acute effects of cycling exercise in an immersive virtual reality (IVR) environment on attentional control and self-efficacy expectations of indi-viduals undergoing SUD treatment.
Methods. A total of 20 individuals (mean age of 37.75 years) enrolled in a SUD treatment program participated in the study. They were instructed to complete a single session of cycling with a self-selected duration within the IVR system.
Results. Following the cycling session, pre-post measures indicated a statistically significant im-provement in self-efficacy expectations and attentional control measured with the Stroop test. The results revealed that participants expressed high levels of intention for future use, inter-est/enjoyment, and positive attitudes toward the IVR exercise system. Qualitative data indicated that participants found the IVR exercise system enjoyable, expressed a strong intention to use it, and did not encounter technical difficulties or negative emotions.
Conclusions: In conclusion, it seems that engaging in a brief period of self-selected exercise within a virtual environment can result in temporary activation of cognitive changes, heightened self-efficacy expectations, and a motivating approach to increasing physical activity participation among individuals with SUD, thus suggesting the feasibility of this approach.
Keywords:
exercise
; substance use disorders
; self-efficacy
; attention
; virtual reality
1. Introduction
Drug use poses a significant public health concern, with potential consequences including substance use disorders (SUD), mental health disorders, HIV infection, cancer, cirrhosis of the liver, hepatitis, overdose, premature death, and impaired cognitive function with chronic use [1]. In general, addiction is a disorder of altered cognition and the brain regions that are affected by SUD overlap with those involved in cognitive functions such as learning, memory, attention, reasoning, and impulse control. Chronic drug use can alter brain structure and function, leading to addiction [2], affecting memory and cognitive functions [3]. Drugs have negative effects on natural cognitive function, promote drug use, and hinder the development of behaviors supporting abstinence. During substance abstinence, individuals may experience cognition-related withdrawal symptoms caused by many drugs that are usually temporary, in contrast with long-term use symptoms that lead to lasting cognitive declines. Moreover, cognitive deficits related to drugs may have negative effects on the individual's well-being [4].
Individuals undergoing SUD treatment experience notable physical and cognitive benefits when incorporating exercise into their regimen. Research suggests that physical activity positively influences attention [5], contributing to enhanced cognitive functioning and potentially supporting addiction recovery. Exercise programs and physical activities seem to be helpful in reducing cravings for substance use and promoting abstinence, and acting as valuable components for prevention and intervention, complementing traditional therapy. Some of the benefits of exercise are prevention of relapse, repair of cardiovascular and muscular damage, reduced symptoms of anxiety and depression and improved mood, increased self-confidence, self-esteem, and body image, improved well-being and quality of life, personal satisfaction, optimism and adopting a healthy lifestyle [6-8]. Systematic reviews documented the importance of physical activity and exercise programs in SUD treatment [9,10].
Attention is a large and complex topic involving psychology and neuroscience. Generally, attention could be described as the flexible control of limited computational resources [11]. Many researchers have studied the influence of acute exercise on the Stroop effect (used widely to assess attention deficits) in healthy and clinical populations. The findings of a recent study, in which the Stroop test was applied pre, post, and 40 minutes post-resistance exercise, supported that acute exercise can lead to improved scores [12]. The use of a virtual reality platform can also offer cognitive flexibility and selective attention improvements in young males, as exercise does offer such benefits [13]. Therefore, a combination of VR and exercise may contribute to cognitive development. Furthermore, current investigations are delving into the potential advantages of high-intensity interval training for enhancing cognitive function in individuals with SUD [14]. Additionally, a recent randomized controlled trial revealed significant enhancements in cognitive functions and emotional well-being among patients with SUD participating in a group-based aerobic exercise program [15]. Notably, these findings underscore the promising role of exercise interventions in addressing cognitive deficits associated with SUD.
Self-efficacy is defined as the expectation that one can successfully perform a specific behavior required to produce a certain outcome [16]. Positive self-efficacy is related to individuals' perceptions of their ability to control their own functioning and the events that affect their lives while decreased self-efficacy may lead to doubt and easily giving up in the face of obstacles [17,18]. Research by Schwarzer et al. 2014 [19] indicates a strong connection between self-efficacy and both physical and mental health. There are, also, studies supporting that the consumption of illicit drugs is likely to impair individuals' self-control and self-efficacy [20]. Other researchers support that there is a significant positive correlation between self-efficacy and treatment motivation [21]. Increased levels of self-efficacy, and quality of life and social support were found to be negatively correlated with the relapse tendency in individuals with drug addiction [22,23]. The role of attitudes and intentions toward participation in sports and exercise programs has been documented. Positive attitudes and intentions toward substance abuse treatment are related to treatment completion. Attitude and control components are positively associated with intention and treatment participation or completion [17,18]. Furthermore, exercise can empower individuals under drug addiction therapy to achieve better fitness results and improve their psychological states, leading to positive changes in personality and psychological characteristics, including self-efficacy. Finally, exercise-induced improvements in self-efficacy can contribute to overall well-being and quality of life, promoting a positive mindset and sense of achievement throughout the recovery journey [24].
Self-efficacy expectations, as outlined by Bandura (1977) [16], pertain to an individual's belief in their capability to successfully execute behaviors required to produce specific outcomes in particular situations. This concept emphasizes the confidence an individual has in their ability to achieve desired results through their actions within specific contexts. The distinction between self-efficacy and self-efficacy expectations lies in their scope and focus. Self-efficacy encompasses a broader sense of overall competence and belief in one's abilities across various tasks and situations. In contrast, self-efficacy expectations are more specific, relating to an individual's confidence in their capacity to perform particular behaviors to achieve particular outcomes in defined circumstances [16].
Exercise in a virtual reality (VR) environment has been a rising method of exercise in recent years. Several studies were involved with VR exercise and support that it is suitable to offer positive effects on physiological, psychological, and rehabilitation factors compared to conventional exercise [25]. It has also been shown that exercise in a VR environment has positive effects on cognitive factors such as functional ability, attention, and memory and psychological factors such as depression and anxiety [26]. VR exercise combined with cognitive tasks, according to another study, appeared to be appropriate and had positive effects even in people with mild cognitive impairment [27]. Additionally, recent research by Krommidas et al. (2022) [28] has highlighted the potential of acute exercise and virtual reality tasks to positively impact children's memory function and exercise preference, providing valuable insights into the broader applications of VR-based exercise interventions. VR environments are also a reliable way for providing information about addictive disorders, such as the desire to use, and can influence emotional state, attention, and cognitive function [29]. At the same time, virtual environments can simulate reality without limitations in space and time, which makes them more attractive [30]. Individuals with attention deficits, or those who face difficulties participating in group activities, may benefit from the virtual environment [29].
To the best of our knowledge, there are few studies in the literature evaluating the effect of exercise in a virtual reality environment in populations in the treatment of SUD. According to what was mentioned above, it would be important to explore whether exercise in a VR environment could help to improve the self-efficacy expectations and attentional control of individuals in drug addiction treatment and be a useful and attractive tool to enhance their participation in an exercise program.
1.1. Research Questions and Hypotheses
In the present study, we sought to address several key research questions related to the utilization of IVR exercise as an intervention for individuals undergoing SUD treatment. Firstly, we investigated whether engaging in exercise with the IVR environment would lead to a significant improvement in self-efficacy expectations among participants in the SUD treatment program. We hypothesize that participation in IVR exercise would be associated with a noteworthy increase in self-efficacy expectations. Additionally, we explored potential differences in attentional control levels, as measured by the Stroop test, before and after a single session of cycling using the IVR system. We hypothesize that this intervention will decrease Stroop reaction time in people undergoing SUD treatment. Lastly, we delved into participants' attitudes, intentions for future use, and levels of interest/enjoyment regarding exercise within the IVR system. We hypothesize that individuals in the SUD treatment program would exhibit positive attitudes, express strong intentions for future use, and report high levels of interest/enjoyment concerning IVR-based exercise. Overall, these research questions and hypotheses were designed to comprehensively investigate the potential benefits of IVR exercise within the context of SUD treatment.
Therefore, the aim was to explore the acute effects of a pre- and post-exercise in an immersive virtual reality (IVR) environment on self-efficacy expectations and attentional control of individuals in SUD treatment. Additionally, their attitudes, intentions for future use, and interest/enjoyment about this type of exercise were investigated.
2. Materials and Methods
2.1. Participants & Setting
A convenience sample of 20 individuals in substance use disorder (SUD) treatment of KETHEA ITHAKI therapeutic community participated. KETHEA ITHAKI is a therapeutic community located in Sindos, Thessaloniki, Greece, that aims to help individuals struggling with addiction and substance abuse with a residential program without substitution (https://www.kethea.gr). The inclusion criteria encompassed individuals between the ages of 18 and 60, who were functionable and capable of participating in exercise, without colorblindness, and without significant psychiatric conditions including severe anxiety disorder, psychosis, aggressive and violent behavior, psychopathic, schizophrenic, or paranoid personality disorders, or hallucinations. According to an article from KETHEA (Therapy Center for Dependent Individuals) published in 2017, the ratio of women to men participating in substance use disorder treatment programs is approximately 1 to 5. This indicates that approximately 20% of all participants in the program are women. (https://www.kethea.gr/nea/oie-anagki-gia-ypostiriksi-ton-eksartimenon-gynaikon/). Their demographic characteristics are presented in Table 1.
2.2. Study Design
The study employed a quasi-experimental research design, chosen for its appropriateness in the context of being both exploratory and constrained by practical considerations. The rationale for adopting this design stems from the exploratory nature of the research, as only a limited number of studies have utilized virtual reality (VR) exercise for this particular population. Furthermore, the feasibility of alternative designs was restricted by the fact that the therapeutic community KETHEA ITHAKI had only 20 participants. Additionally, ethical and practical concerns were highlighted, as raised by the SUD therapists. They believed that it would be considered unethical or problematic to expose only a limited number of participants to the proposed VR exercise experience.
2.3. Ethics Approval and Consent to Participate
The studies involving humans were approved by the institution’s ethics committee (approval number: 1829, 13 October 2021). The confidentiality of personal data is assured with regulation (EU) 2016/679 (general data protection regulation). All participants and medical staff of KETHEA were informed orally of the procedure and participants provided written information and signed the consent form. Additionally, they were encouraged to ask questions and received complete and detailed answers.
2.4. IVR System
In our study, we employed a mixed methods approach, integrating both quantitative and qualitative methodologies. This comprehensive strategy allowed us to benefit from the strengths of each method, enhancing the depth and completeness of our findings. The methodology followed was based on our previous studies examining the effects of the IVR exercise system on patients with mild cognitive impairment and female office workers [27,31].
The IVR system consists of a cycle-ergometer (stationary seated bike type; Toorx, Chrono Line, BRX R 300) connected to a computer, the IVR head-mounted display and controllers, and the IVR application. The cycle-ergometer with Bluetooth capability (stationary seated bike type; Toorx, Chrono Line, BRX R 300) has been selected for the measurements as an ideal solution for the participants to control their training conditions and minimize the risk of falls. The IVR application includes motivational techniques to address the issue of low motivation to exercise. For the IVR projection, the Meta Quest 2 (Facebook technologies, LCC, Hacker Way, Menlo Park, CA, USA) device was used (Figure 1a,b). The IVR system was developed by ORAMA-VR and Biomechanical Solutions Engineering, based on interviews with older people with mild cognitive impairment.
The IVR application permits the user to choose their exercise goal (exercise duration) (Figure 2), have feedback for their training performance (cycling duration and total distance), task crafting (selection of music to enjoy while practicing), and self-monitoring (screen showing distance, time, and speed data). Additionally, the user could choose the landscape in which they would like to practice (forest, beach, snowy landscape) and which motivational word or phrase they would like to hear and repeat during their performance, such as “calmly”, “I can”, “I will do well”, “Very nice” or no words. As a selection mechanism, an IVR controller is used with a ray cast allowing the user to choose an answer by pointing the ray at the button and pressing the trigger button on the controller.
After that, each participant starts the cycling performance (Figure 34), and at the end, they receive feedback from the application about the time and distance they achieved and they can evaluate their experience through questions, e.g., “Are you tired today?”, “Did you like the way you exercised today?”, “How often did you repeat the word or phrase during the exercise?”
The IVR training system used is called VRADA (VR exercise App for Dementia and Alzheimer’s patients), Version 4.4. This IVR system (Version 3.7) was used with university students and patients with mild cognitive impairment as a dual-task training aimed to promote their physical and cognitive health and assess its acceptability, tolerability, and usability [27]. Additionally, Baldimtsi et al.,2023 [32] utilized the same IVR system with older adults diagnosed with MCI, conducting 32 physical and cognitive training sessions. Their findings suggest that the system effectively improves cognitive function. Given the promising results from both studies, further investigation into the applicability of VRADA across diverse populations could be warranted. The VRADA system, originally intended for dementia or Alzheimer's patients, underwent modification in our study. We utilized an updated version excluding cognitive tasks during exercise, opting for questionnaires more suitable for this population, focusing on aspects such as attention and self-efficacy expectations.
The VRADA system has advantages that can meet the needs of individuals in the treatment of SUD, such as mood improvement, anxiety and depression reduction. According to the results of a study, that examined the effects of acute VR exercise combined with cognitive tasks on children’s memory and exercise preference, children who experienced VR exercise noted higher scores in memory tests compared with children who experienced a traditional cycling session and control group. Additionally, children showed high levels of enjoyment, intention for future use, and attitudes toward cycling in a VR environment [28]. Acute VR exergaming can also lead to mood improvement according to Ochi et al. (2022) [33]. Furthermore, it is a very pleasant and attractive way to exercise, and it might also be applicable to addicted individuals, to maintain their physical health and avoid the negative effects of treatment factors such as withdrawal symptoms, relapse, treatment burnout etc.
2.5. Procedure
All participants were informed about the aim of this study and completed the consent form. The experimental procedure was completed in one visit and based on our previous study [31]. Then, they filled in a questionnaire with questions about their demographic characteristics, the TCU Drug screening questionnaire [34] and the IPAQ [35].
After that, each participant adjusted their seat on the stationary bike and familiarized themselves with the equipment of the IVR system. They simultaneously were informed in detail about the procedure, and how to use the equipment and were encouraged to ask questions. There were given 5 minutes to familiarize themselves with the virtual environment and understand how to use the equipment. Then, they completed the self-efficacy expectations scale [36,37] and underwent Stroop Test [38].
They were encouraged to choose the landscape (forest, beach, snowy landscape) and the duration of their cycling performance in the virtual reality environment. They could cycle from 5 to 30 minutes and were asked to cycle at a certain speed between 15-20 km/h. During their performance, they were informed on their screen about their speed, covered distance and time remaining, and could select the music they were listening to from a list of songs.
When they completed the cycling session, they underwent the Stroop test [38] and completed the self-efficacy expectations scale [36,37], a questionnaire assessing their attitudes and intention for future use [39] and their interest/enjoyment (intrinsic Motivation Inventory) [40] toward the IVR exercise system. In the end, they answered a semi-structured interview with questions about their experience. The duration of the process was approximately 1 hour (Table 2).
2.6. Measures
All participants first completed a questionnaire collecting data for their age, gender, educational level, years of substance use, days of treatment, participation in an exercise program, type of exercise, days per week, and minutes, TCU Drug Screen 5 according to Knight, Simpson & Hiller, 2002 [34], IPAQ questionnaire according to Craig et al.,2003 [35]. Pre- and post-IVR exercise they completed the Self-Efficacy Expectations Scale according to Bandura, 2006 [36] and Theodorakis,1996 [37] and the Stroop Test consisting of 3 tabs (naming, reading, and interference) according to Stroop, 1935 [41].
Self-efficacy expectations were evaluated by asking subjects to rate the strength and magnitude of their self-efficacy expectations for ten performance levels from 10 to 30 minutes. The format used is comparable to that of Bandura [36] recommendation (e.g. "I can perform this test by 10 minutes", Yes-No) and "How certain you are?" answered on a 10-point scale anchored by "certain" (10) and "uncertain" (1). The strength of perceived self-efficacy was the sum of the certainty scores for the ten levels of performance. Cronbach's alpha for the scale was .88.
After their performance, they completed questionnaires about attitudes [39] toward the IVR exercise and were assessed with 5 pairs of opposite words e.g. “I find VR exercise…” - “good-bad”, “healthy-unhealthy” etc. with scores on a differential scale of 7 points. The scoring scale ranged from 1 to 7 with higher scores indicating more positive attitudes. Intention for Future Use (IFU) of the IVR system was assessed with 3 questions e.g. “I intend to use the VR exercise system when available” with responses from “Yes sure” to “Not at all”. The scoring scale ranged from 1 to 5 with higher scores indicating greater intention for future use.
Interest/ enjoyment was assessed with the relative items of the Intrinsic Motivation Inventory (IMI) [40] with 6 items e.g. “I liked very much the VR exercise” with responses on a 1-5 Likert scale from “Not sure” to “Very sure”. The scoring scale ranged from 1 to 5 with higher scores indicating high interest/enjoyment. And at the end, they responded to a semi-structured interview consisting of 14 questions about the participants’ experience with the IVR system. They were asked to describe why they would like to use the IVR system to exercise, usability or utilization was assessed with 4 questions e.g. “What difficulties did you encounter while exercising with the IVR system?”, usability or learning was assessed with one question e.g. “Did it take long to figure out how the IVR system works?”, usability or pleasantness was assessed with 2 questions e.g. “What did you like the most and what did you like least about the IVR system?”, sense of presence or engagement was assessed with 2 questions e.g. “Were you easily distracted while exercising with the IVR system?”, sense of presence or realism was assessed with one question e.g. “How did you find the environment? Realistic or artificial?” and tolerability with 3 questions e.g. “Did you feel bad at any moment when exercising with the IVR system?” (Appendix A)
2.7. Statistical Analysis
All data are presented as means (M), Standard Deviation (SD), range, and percentages (%). Descriptive statistics, scatter plots, and frequencies were used for demographic characteristics, the IVR system questions, Stroop test scores, psychological factors, and IVR performance. The Kolmogorov-Smirnov Test was used to assess the normality of the distribution. Correlation among variables was assessed using the Pearson coefficient and Cronbach’s α reliability analysis was performed for all questionnaires. Paired samples t-test was used to identify self-efficacy expectations differences pre- and post-IVR exercise. Repeated measures ANOVA analysis was used to test the effect of days of treatment on the Stroop performance. Qualitative data from the semi-structured interview were analyzed with thematic analysis which can offer rich insights into attitudes and beliefs by identifying patterns of ideas and responses [42]. All statistical analyses were performed with IBM SPSS (Statistics Version 29) and the level of significance was set at p<.05. The analysis was not pre-registered and the results should be considered exploratory.
3. Results
3.1. Pre- and Post- IVR Exercise Measures
3.1.1. Stroop Test
Participants experienced a statistically significant reduction in completion time for the color, word, and word-color tasks of the Stroop test following the immersive virtual reality (IVR) exercise. Additionally, there was a decrease in the number of errors made, although this difference did not reach statistical significance. Table 3 presents the means, standard deviations (SD), and levels of significance for all 3 tabs of the Stroop test. Furthermore, a moderate negative correlation (r = -.45, p = .048) was observed between the time taken to complete the reading task before the VR exercise and the duration of the treatment days (M= 44.94, SD= 5.44). The Repeated Measures ANOVA analysis, including treatment days as a covariate, revealed non-significant effects across all tabs of the Stroop test. For Tab 1 (naming), F (1,18) =.10, p=.756; Tab 2 (reading), F (1,18) =1.982, p=.176; and Tab 3 (interference), F (1,18) =.09, p=.767.
To investigate the potential influence of a practice effect on the substantial improvement of reaction time observed in the Stroop test, our Stroop test effect sizes (Cohen's d) were compared with those of Zimmer et al.,2016 [43], who utilized the same test in a pre-post design with a control group, notable differences emerged. Our Cohen’s d values for the naming, reading, and interference tabs were 0.84, 0.29, and 0.88, respectively, while the respective values for Zimmer et al.'s [43] control group were 0.47, 0.43, and 0.16. Specifically, our study exhibited higher effect sizes in the naming (+.37) and interference (+.72) tabs compared to the control group. However, our Cohen’s d for the reading tab was lower (-.14) than that reported in the control group of Zimmer et al., 2016 [42] These findings suggest an additional effect beyond practice effects in our study, particularly in the naming and interference tabs.
3.1.2. Self-Efficacy Expectations
A paired-samples t-test was conducted to compare the self-efficacy expectations pre- and post-VR exercise. There was a statistically significant improvement in self-efficacy expectations after the VR experience M=56.8, SD= 4.87 compared with self-efficacy expectations before the VR experience M= 49.8, SD= 13.19, t (19) = -2.78, p=.01.
3.2. Post-IVR Exercise Measures
3.2.1. Attitudes, Intention for Future Use, Interest/Enjoyment
The participants expressed high levels of intention for future use (M= 4.5, SD= 0.6, Cronbach α .85), interest/enjoyment (M= 4.4 SD= 0 .6, Cronbach α .89), and positive attitudes towards the IVR exercise system (M= 6.6, SD= 0.4, Cronbach α .79).
3.2.2. IVR System Experience
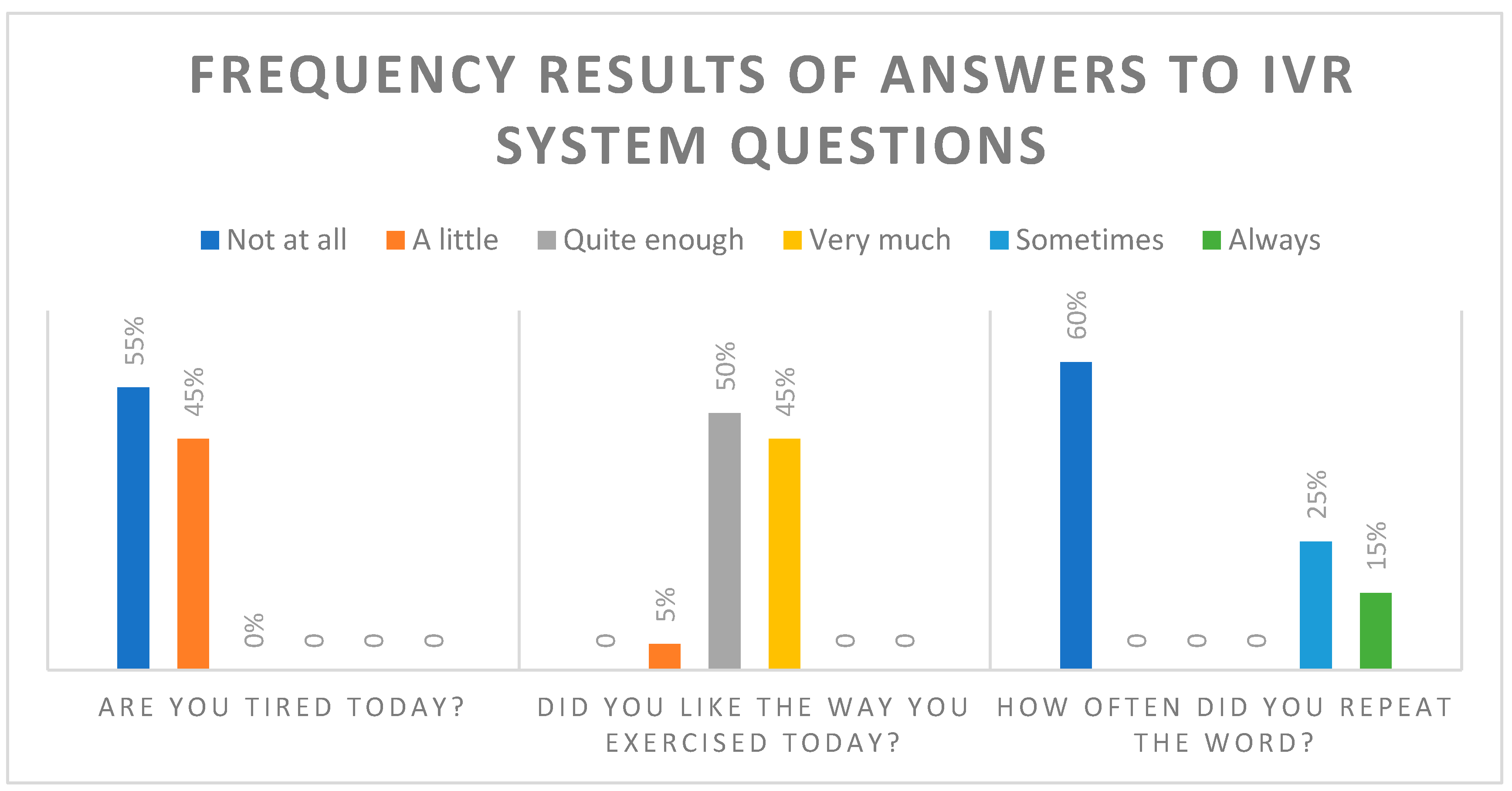
Following the completion of the cycling program within the IVR system, participants were asked to respond to three questions evaluating their IVR cycling experience. The responses indicated that the majority of participants did not feel tired from the cycling activity and expressed a positive liking towards it. Graph 1 presents the results of these questions.
Figure 1.
Frequency of answers to IVR system questions.
3.2.3. IVR Performance
In the self-selected duration of the IVR exercise, 25% of the participants chose to practice for 15 minutes, 45% for 20 minutes, and 30% for 30 minutes. All participants achieved their exercise goal and we didn’t have dropouts. The Mean and SD of their cycling time was 21.8±5.9 (Range 15.0-30.0). Their average speed was 19.05 with the guidance to cycle between 15 and 20 km/h (M= 19.1, SD= 0.7, Range 17.14-20.21) and an average of covered distance of 6.19 km (M= 6.2, SD= 1.7, Range 4.0-8.9).
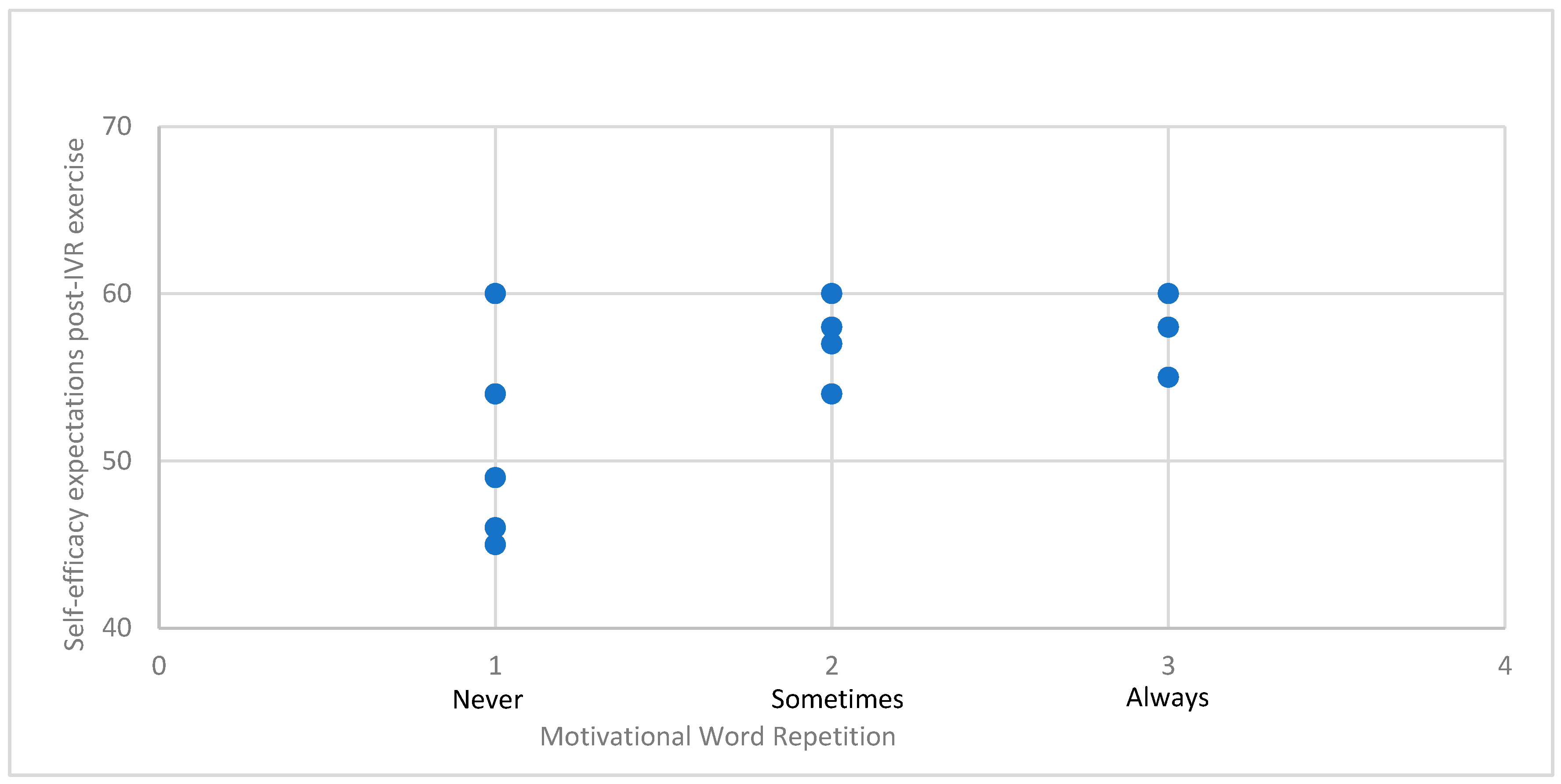
The scatter plot (Graph 2) observation indicates that those who used motivational words had higher scores in self-efficacy expectations. Nevertheless, despite this observation, both regression and correlation analyses failed to yield statistically significant findings. Specifically, the regression analysis indicated a multiple R of .021, which did not significantly deviate from zero (F (1,18) = .387, p = .542). Similarly, Spearman’s correlation analysis also did not reveal a statistically significant correlation between the variables (p = .715).
Figure 2.
Scatter plot: Relationship between self-efficacy and motivational word usage.
3.3. Technical Functionality, User Experience, and Emotional Responses toward the IVR Exercise System
A thematic analysis was conducted to analyze the qualitative data obtained from the semi-structured interviews, and the findings are presented in Table 4. According to the participants' reports, they did not encounter any technical issues and did not require additional time to understand the IVR exercise system. The majority of participants expressed satisfaction with the IVR system equipment, including the head-mounted display and joystick, although a few mentioned that the mask felt slightly heavy or tight. None of the participants experienced negative emotions, discomfort, or unusual thoughts during the cycling activity, except for one individual who initially felt some dizziness for a few seconds at the beginning of the IVR experience. All participants expressed a desire to continue using the IVR system for exercise, emphasizing that they found it enjoyable, relaxing, motivating, interesting, challenging, and capable of evoking feelings of happiness. They also mentioned that the system provided a means of escaping from reality and was easy to use.
4. Discussion
In our feasibility study, we aimed to explore the self-efficacy expectations and attentional control differences of individuals in SUD treatment pre- and post-exercise in an immersive virtual reality (IVR) system and to investigate their attitudes, intentions for future use, and interest/enjoyment about this type of exercise, immediately after the exercise session. The findings of this study provide insights regarding the effects of an IVR exercise system on exercise self-efficacy expectations and performance in the Stroop test. Additionally, the results indicated positive outcomes and acceptance of the IVR exercise system for people under SUD therapy, thus suggesting the feasibility of this approach.
4.1. The Effects of IVR Exercise on Self-Efficacy Expectations of Individuals in SUD Treatment
In our study, we evaluated self-efficacy expectations before and after the IVR exercise. Consistent with Bandura's definition [16], these expectations reflect an individual's confidence in their ability to accomplish tasks essential for desired outcomes in specific situations. Our findings revealed a significant improvement in self-efficacy expectations following the IVR experience. Panagiotounis et al.,2020 [44] assessed self-efficacy in individuals in the treatment of substance use disorders. According to this study, the intervention lasted 5 days and was an adventure-based therapy for the promotion of participants' therapeutic change involving physical activity. The results have shown that the participants' self-efficacy and self-esteem were positively affected [44]. Our findings did not unveil any significant relationship between self-efficacy and the repetition of motivational words; rather, this observation was discerned solely from the scatter plot. It is possible that the limited sample size may account for this outcome. According to our results, there were statistically significant differences in self-efficacy expectations, that can be positively influenced by one bout of exercise. This can be elucidated by emphasizing that, as previously noted, self-efficacy expectations are more precise, and engaging in exercise provides immediate successful experiences that strengthen individuals' confidence in their ability to participate in physical activity [16]. From our perspective, IVR exercise shows promise as a tool for indirectly enhancing self-efficacy after a few times of exercising as we found improvements in self-efficacy expectations scores in acute exercise.
4.2. The Effects of IVR Exercise on the Attentional Control of Individuals in SUD Treatment
According to our results, there was a statistically significant reduction in reaction time in the Stroop test after the IVR exercise. It was observed that individuals with important positions with many demands and responsibilities for the community, such as drivers and coordinators noted better scores in all tabs of the Stroop test compared with members who were less active in their community. Nevertheless, covariate analysis didn’t find a significant effect. Our results are consistent with those of Smith et al.,2021 [45] supporting that participants who engaged in a virtual reality exercise program as part of their treatment showed significant improvements in Stroop test performance after VR exercise [45]. Based on our findings, it is plausible to suggest that IVR exercise may contribute to enhancing cognitive restoration during therapy. Likewise, previous studies have shown that individuals with substance use disorder exhibited reduced reaction time in the Stroop test following a single session of Tai Chi or high-intensity interval training, with the latter demonstrating superior improvement [46]. The comparison of our Stroop test effect sizes with those of Zimmer et al., 2016 [43] provides valuable insights into the potential impact of exercise intervention on cognitive function. Despite the acknowledged vulnerability of the Stroop test to practice effects, our study revealed significant differences in effect sizes, particularly in the naming and interference tabs, indicating a potential contribution from acute exercise. The higher Cohen's d values observed in these tabs compared to the control group of Zimmer et al., 2016 [43] suggest temporary cognitive changes that extend beyond mere familiarity with the test. We also found significant relations between days in the treatment and the Stroop test pre-exercise score in the second tab of the Stroop test. There was a moderate negative relation between these variables and this can be a clue that maybe the days spent in abstinence from drugs may influence positively the cognitive function. Nevertheless, repeated measures ANOVA with covariate analysis on the relationship before and after IVR training Stroop test scores showed a non-significant effect of days in treatment. Research has consistently shown that longer durations of abstinence from drugs are associated with improved cognitive function, including attention, working memory, and executive control [47,48].
In our study, all participants were poly-users, but the vast majority of them reported that heroin was the substance that was the most difficult to abstain process. Heroin addiction has a negative effect on impulse control, attention, and flexibility. Moreover, the reaction time on heroin cues can be predicted by heroin craving levels [49]. Due to the small sample size and the fact that all participants were poly-users, comparative analyses were not performed to examine the potential impact of the specific substances they used on their Stroop test scores.
4.3. The Attitudes, Intention for Future Use, and Interest/Enjoyment of Individuals in SUD Treatment toward IVR Exercise
According to the results, most participants showed increased levels of interest/enjoyment, intention for future use, and positive attitudes toward the IVR exercise system indicating positive perceptions and high motivation. Interest/enjoyment is a dimension of intrinsic motivation and the high scores indicate positive motivation. These results suggest that the participants after using the IVR exercise system, had a favorable attitude toward the IVR exercise system, intended to use it in the future, and expressed strong interest and enjoyment during the VR cycling experience. These results align with participants' feedback regarding their virtual experience from the interview. Notably, there were no reports of adverse effects such as nausea or dizziness, and overall comments on the VR exercise application were highly positive. However, several participants mentioned that they found the landscape to be somewhat monotonous. While this feedback is valuable, it should be considered for future studies utilizing the VRADA application. Furthermore, the feedback gathered from questions presented on the screen following the cycling performance was overwhelmingly positive. The majority of participants expressed satisfaction with their exercise experience and reported no feelings of fatigue. However, there were fewer positive responses regarding the word repetition task, indicating that some participants found this aspect less enjoyable or engaging.
In our study, participants chose their preferred landscape (forest, beach, snowy landscape) and cycling duration (5 to 30 minutes) in the virtual reality environment, receiving real-time feedback on speed, distance, and remaining time, while also having the option to select music from a list of songs. Research consistently demonstrates that incorporating choices into individuals' exercise routines significantly enhances their experience and motivation. By allowing participants to select key elements such as exercise duration, preferred music, and the surrounding landscape, exercise programs become powerful tools for providing autonomy. This practice aligns with motivational techniques rooted in self-determination theory, fostering intrinsic motivation and a greater sense of ownership over one's fitness journey [50]. The ability to tailor exercise programs to individual preferences not only makes them more personalized but also increases engagement and enjoyment. Ultimately, these autonomy-supportive strategies contribute to a positive and individualized exercise experience, promoting sustained adherence and overall well-being.
Virtual reality exercise has emerged as a promising tool for individuals in substance use disorder treatment, as it offers a unique and immersive approach to physical activity. Studies assessing the effects of virtual reality exercise on individuals in substance use disorder treatment have found positive outcomes in terms of interest/enjoyment, attitudes towards exercise, self-efficacy, and cognitive function measured through the Stroop test. For instance, a study by Nesbitt et al.,2020 [51] investigated the use of virtual reality exercise among individuals in substance use disorder treatment and found that participants reported high levels of interest and enjoyment during virtual reality exercise sessions [50]. Another study demonstrated that virtual reality exercise interventions were associated with improved attitudes towards exercise and increased self-efficacy among individuals in substance use disorder treatment [52]. Furthermore, other researchers examined the effects of virtual reality exercise on cognitive function using the Stroop test in individuals with substance use disorder and found significant improvements in attention and inhibitory control following virtual reality exercise sessions [53].
4.4. Strengths & Limitations
This study contributes significantly to the emerging field of IVR exercise interventions for individuals undergoing substance use disorder (SUD) treatment. One of its primary strengths lies in its holistic approach, exploring not only the cognitive benefits but also participants' attitudes, intentions, and interest/enjoyment related to IVR exercise. The utilization of both quantitative measures, such as the Stroop test for attentional control, and qualitative data provides a comprehensive understanding of the intervention's impact.
Despite its strengths, this study has several limitations that warrant consideration. The relatively small sample size may limit the generalizability of the findings to a broader population. The study's focused exploration within a specific population undergoing substance use disorder treatment, coupled with resource constraints for intensive assessments, necessitated a smaller sample size of 20 participants. While limited in generalizability, this approach allowed for in-depth insights and laid the groundwork for future, more extensive investigations. The absence of a control group and random assignment is acknowledged, posing challenges in establishing causal relationships. The quasi-experimental design, while providing initial insights, necessitates caution in generalizing findings to long-term effects, highlighting the need for future studies with extended interventions and control conditions. According to Edwards et al., 1996 [54], it is possible that the practice effect from the Stroop test may have influenced the positive results regarding attention. Therefore, because our study design did not include a control group, we might have had the effect of practice when we compared the before–after Stroop test scores. Nevertheless, previous studies examining the effect of exercise on Stroop performance, indicated that an acute bout of exercise led to improved scores in the Stroop test, compared with a control group [55]. According to our findings the effect size of the Stroop task in our study was higher compared to the control group of Zimmer et al., 2016 [43]. These findings underscore the nuanced effects of exercise on cognitive performance and highlight the need for further research to elucidate the mechanisms underlying these effects. Additionally, in this study, we observed that individuals with important positions and numerous demands and responsibilities in the community, such as drivers and coordinators, achieved better scores in all tabs of the Stroop test compared to members who were less active in their community. This observation underscores the importance of considering such factors in future studies on this topic. In conclusion, there is a need for further research involving extended exercise interventions utilizing VR environments, larger sample sizes, randomized controlled trials, and prolonged follow-up periods. These endeavors will serve to validate and expand upon the current findings, shedding light on whether such exercise modalities could contribute to reduce drug use, and cravings or enhanced recovery self-efficacy.
5. Conclusions
In conclusion, IVR exercise can be a useful and promising tool to be used supplementally for SUD treatment. A short bout of self-selected exercise in a virtual environment can lead to increased scores in cognitive factors, enhance self-efficacy expectations levels, and can be a motivating way to improve physical activity participation levels of individuals with SUD. Further research in this field could explore the long-term effects and sustained benefits of IVR exercise interventions for individuals undergoing substance use disorder treatment. Additionally, investigations employing randomized controlled trials with larger and more diverse samples, extended intervention periods, and robust control conditions would contribute to establishing the efficacy and generalizability of such interventions, providing valuable insights for clinical applications.
Author Contributions
Conceptualization, E.T, M.H., F.P. and Y.T.; methodology E.T, M.H., F.P. and Y.T.; validation, M.H and Y.T.; formal analysis, E.T and V.S.; investigation, E.T.; data curation, E.T. and E.G; writing—original draft preparation, E.T..; writing—review and editing, M.H., V.S., F.P., E.G., M.G., Y.T..; resources, F.P., Y.T, visualization, M.H.; supervision, Y.T. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University of Thessaly (protocol code 1829, 13 October 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
We extend our gratitude to all staff members and residents of KETHEA Ithaki for their invaluable contributions to the successful implementation of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Drug Report. United Nations publication, Sales No. E.20.XI.6, 2020.
- Nestler, E. J. Cellular basis of memory for addiction. Dialogues Clin. Neurosci. 2013, 15, 431–443. [CrossRef]
- Goldstein, R.Z.; Volkow, N.D. Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications. Nat. Rev. Neurosci. 2011, 12(11), 652-669. https://www.nature.com/articles/nrn3119.
- Gould, T.J. Addiction Science & Clinical Practice, Addiction and Cognition. Addict. Sci. Clin. Pract. 2010, 5(2), 4-14. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3120118/pdf/ascp-05-2-4.pdf.
- Kutlu, M. G.; Gould, T. J. Effects of drugs of abuse on hippocampal plasticity and hippocampus-dependent learning and memory: contributions to development and maintenance of addiction. Learn. Mem. 2016, 23, 515–533. [CrossRef]
- Ellingsen, M.M.; Johannesen, S.L.; Martinsen, E.W.; Dahl, S.R.; Hallgren, M. Effects of Acute Exercise on Drug Craving, Self-Esteem, Mood, and Affect in Adults with Polysubstance Use Disorder: Protocol for a Multicenter Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9(10), e18553. [CrossRef]
- Rethorst, C. D.; Henley, S. S.; Carmody, T. J.; Dela Cruz, A.; Greer, T. L.; Walker, R.; Trivedi, M. Moderators of treatment response to exercise in participants with stimulant use disorder: Results from the Stimulant Reduction Using Dosed Exercise (STRIDE) CTN0037 study. Ment. Health Phys. Act. 2021, 21, 100421. [CrossRef]
- Panagiotounis, F.; Hassandra, M.; Koutsoukou, A.; Theodorakis, Y. What about sport and physical exercise in substance use disorder recovery? Perceptions of individuals undergoing SUD recovery. Life Skills Dev. 2022. [CrossRef]
- Ding, K.; Li, H. Digital Addiction Intervention for Children and Adolescents: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 4777. [CrossRef]
- Piché, F.; Daneau, C.; Plourde, C.; Girard, S.; Romain, A. J. Characteristics and impact of physical activity interventions during substance use disorder treatment excluding tobacco: A systematic review. PLOS ONE 2023, 18, e0283861. [CrossRef]
- Lindsay, W. G. Attention in Psychology, Neuroscience, and Machine Learning. Front. Comput. Neurosci. 2020, 14. [CrossRef]
- Chou, C.C.; Hsueh, M.C.; Chiu, Y.H.; Wang, W.Y.; Huang, M.Y.; Huang, C.J. Sustained Effects of Acute Resistance Exercise on Executive Function in Healthy Middle-Aged Adults. Front. Hum. Neurosci. 2021, 15. [CrossRef]
- Sanudo, B.; Abdi, E.; Bernardo-Filho, M.; Taiar, R. Aerobic Exercise with Superimposed Virtual Reality Improves Cognitive Flexibility and Selective Attention in Young Males. Appl. Sci. 2020, 10, 8029. [CrossRef]
- Haberstroh, C.; Weider, S.; Flemmen, G.; Loe, H.; Andersson, H.W.; Hallgren, M.; Mosti, M.P. The effect of high-intensity interval training on cognitive function in patients with substance use disorder: Study protocol for a two-armed randomized controlled trial. Front. Sports Act. Living 2022, 4, 954561. [CrossRef]
- Zhu, T.; Tao, W.; Peng, B.; Su, R.; Wang, D.; Hu, C.; Li, M.; Zhang, X.; Yang, Y.; Yu, S.; Yin, H.; Zhang, B.; Zhao, Y.; Ding, H.; Zhang, C.; Lu, X.; Huang, Y.; Chen, J.; Gao, F.; Zhang, L. Effects of a group-based aerobic exercise program on the cognitive functions and emotions of substance use disorder patients: a randomized controlled trial. Int. J. Ment. Health Addict. 2022, 20, 2349–2365. [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84(2), 191-215. [CrossRef]
- Bonny-Noach, H.; Shapira, B.; Baumol, P.; Tadmor, N.; Rosca, P.; Shoshan, S.; Harel-Fisch, Y.; Caduri, A. Substance use, harm reduction attitudes and behaviors among attendees of nature rave parties in Israel. Harm Reduct. J. 2023, 20. [CrossRef]
- Zemore, S. E.; Ajzen, I. Predicting substance abuse treatment completion using a new scale based on the theory of planned behavior. J. Subst. Abuse Treat. 2014, 46, 174–182. [CrossRef]
- Schwarzer, R. (Ed.). Self-efficacy: Thought control of action. Routledge: New York, NY, 2014. [CrossRef]
- Kadden, R.M.; Litt, M.D. The role of self-efficacy in the treatment of substance use disorders. Addict. Behav. 2011, 36(12), 1120-1126. [CrossRef]
- Mohamed, S. M.; Hassan, S. S.; Abdelmonem, R. M. Relationship between Self-Efficacy, Social Support and Treatment Motivation among Addict Patients. Minia Sci. Nurs. J. 2022, 12, 10.21608/MSNJ.2022.169551.1039.
- Nikmanesh, Z.; Baluchi, M.; Motlagh, A. The Role of Self-Efficacy Beliefs and Social Support on Prediction of Addiction Relapse. Int. J. High Risk Behav. Addict. 2017, 6, e21209.
- Jia, D.; Zhang, K.; Xu, Y. The Relationship Between Social Support and Relapse Tendency Among Those Who Struggle With Drug Addiction: Multiple Mediators of Exercise Self-Efficacy and Health-Related Quality of Life. J. Drug Issues 2023.
- Panagiotounis, F.; Hassandra, M.; Krommidas, C.; Theodorakis, Y. Effects of an exercise theory-based intervention program on craving during the early stage of adults’ SUD treatment. Ment. Health Phys. Act. 2022, 23. [CrossRef]
- Qian, J.; McDonough, D. J.; Gao, Z. The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4133. [CrossRef]
- Ge, S.; Zhu, Z.; Wu, B.; McConnell, E.S. Technology-based cognitive training and rehabilitation interventions for individuals with mild cognitive impairment: a systematic review. BMC Geriatr. 2018, 18, 213. [CrossRef]
- Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Mouzakidis, C.; Karathanasi, E.M.; Petridou, N.; Tsolaki, M.; Zikas, P.; Evangelou, G.; Papagiannakis, G.; Bellis, G.; Kokkotis, C.; Panagiotopoulos, S.R.; Giakas, G.; Theodorakis, Y. A Virtual Reality App for Physical and Cognitive Training of Older People With Mild Cognitive Impairment: Mixed Methods Feasibility Study. JMIR Serious Games 2021, 9(1). [CrossRef]
- Krommidas, C.; Galanis, E.; Tzormpatzakis, E.; Hassandra, M.; Hatzigeorgiadis, A.; Morres, I.D.; Comoutos, N.; Theodorakis, Y. The Effects of Acute Exercise and Virtual Reality Tasks on Children’s Memory Function and Exercise Preference. Int. J. Kinesiol. Sports Sci. 2022, 10(3), 7-17. [CrossRef]
- Mazza, M.; Kammler-Sucker, K.; Lemenager, T.; Kiefer, F.; Lenz, B. Virtual reality: a powerful technology to provide novel insight into treatment mechanisms of addiction. Transl. Psychiatry 2021, 11, 617. [CrossRef]
- Freina, L.; Ott, M. A Literature Review on Immersive Virtual Reality in Education: State of the Art and Perspectives. In The International Scientific Conference eLearning and Software for Education; "Carol I" National Defence University 2015, 1, 133-141. [CrossRef]
- Touloudi, E.; Hassandra, M.; Galanis, E.; Goudas, M.; Theodorakis, Y. Applicability of an Immersive Virtual Reality Exercise Training System for Office Workers during Working Hours. Sports 2022, 10, 104. [CrossRef]
- Baldimtsi, E.; Mouzakidis, C.; Karathanasi, E.M.; Verykouki, E.; Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Zikas, P.; Evangelou, G.; Papagiannakis, G.; Bellis, G.; Kokkotis, C.; Tsatalas, T.; Giakas, G.; Theodorakis, Y.; Tsolaki, M. Effects of Virtual Reality Physical and Cognitive Training Intervention On Cognitive Abilities of Elders with Mild Cognitive Impairment. J. Alzheimers Dis. Rep. 2023, 7, 1475-1490. IOS Press. [CrossRef]
- Ochi, G.; Kuwamizu, R.; Fujimoto, T.; Ikarashi, K.; Yamashiro, K.; Sato, D. The Effects of Acute Virtual Reality Exergaming on Mood and Executive Function: Exploratory Crossover Trial. JMIR Serious Games 2022, 10. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9557761/#!po=59.5238.
- Knight, K.; Simpson, D.D.; Hiller, M.L. Screening and referral for substance-abuse treatment in the criminal justice system. In Treatment of drug offenders: Policies and issues; Leukefeld, C.G., Tims, F., Farabee, D., Eds.; Springer: New York, 2002, pp. 259-272. https://www.ojp.gov/sites/g/files/xyckuh241/files/media/document/198805ncjrs.pdf.
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; Oja, P. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35(8), 1381-1395. PMID: 12900694. [CrossRef]
- Bandura, A. Guide for constructing self-efficacy scales. In Self-efficacy Beliefs of Adolescents; Pajares, F., Urdan, T., Eds.; Information Age Publishing 2006, pp. 307-337. [CrossRef]
- Theodorakis, Y. The influence of goals, commitment and self-efficacy on motor performance. J. Appl. Sport Psychol. 1996, 8, 171–182. [CrossRef]
- MacLeod, C. M. Half a century of research on the Stroop effect: An integrative review. Psychol. Bull. 1991, 109, 163–203. [CrossRef]
- Ajzen, I. Constructing a TPB questionnaire: conceptual and methodological considerations. Department of Psychology, University of Amherst 2002. Archived by WebCite® at http://www.webcitation.org/66zom97zq.
- Goudas, M.; Dermitzaki, I.; Bagiatis, K. Predictors of student’s intrinsic motivation in school physical education. Eur. J. Psychol. Educ. 2000, 15, 271-280. [CrossRef]
- Stroop, J. R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. https://www.frontiersin.org/articles/10.3389/fpsyg.2017.00557/full#B52.
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77-101. [CrossRef]
- Zimmer, P.; Stritt, C.; Bloch, W.; Schmidt, F.-P.; Hübner, S. T.; Binnebößel, S.; Schenk, A.; Oberste, M. The effects of different aerobic exercise intensities on serum serotonin concentrations and their association with Stroop task performance: a randomized controlled trial. Eur. J. Appl. Physiol. 2016. [CrossRef]
- Panagiotounis, F.; Theodorakis, Y.; Hassandra, M.; Morres, I. Psychological effects of an adventure therapy program in the treatment of substance use disorders: A Greek pilot study. J. Subst. Use 2020, 118–124. [CrossRef]
- Smith, A. L.; Jones, R.; Cooper, S. J.; Karageorghis, C. I.; Heather, N. Effects of a virtual reality exercise program on cognitive function and quality of life in individuals undergoing substance use disorder treatment. J. Subst. Abuse Treat. 2021, 128, 108410. [CrossRef]
- Yin, Y.; Yang, S.; Xiao, K.; Wang, T.; Wang, J.; Schöllhorn, W. I.; Zhu, D.; Pang, X. Comparison of the acute effects of Tai chi versus high-intensity interval training on inhibitory control in individuals with substance use disorder. Front. Psychol. 2022, 13. [CrossRef]
- Scott, J. C.; Woods, S. P.; Matt, G. E.; Meyer, R. A.; Heaton, R. K.; Atkinson, J. H.; Grant, I. Neurocognitive effects of methamphetamine: A critical review and meta-analysis. Neuropsychol. Rev. 2007, 17, 275–297. [CrossRef]
- Verdejo-García, A.; Pérez-García, M.; Bechara, A. Emotion, decision-making and substance dependence: A somatic-marker model of addiction. Curr. Neuropharmacol. 2006, 4, 17–31. [CrossRef]
- Lundqvist, T. Cognitive consequences of cannabis use: Comparison with abuse of stimulants and heroin, with regard to attention, memory, and executive functions. Pharmacol. Biochem. Behav. 2005, 81, 319–330. [CrossRef]
- Teixeira, P.; Marques, M. M.; Hagger, M. S.; Silva, M.; Brunet, J.; Duda, J.; Haerens, L.; La Guardia, J.; Lindwall, M.; Lonsdale, C.; Markland, D.; Michie, S.; Moller, A. C.; Ntoumanis, N.; Patrick, H.; Reeve, J.; Ryan, R. M.; Sebire, S.; Standage, M.; Vansteenkiste, M.; Weinstein, N.; Weman-Josefsson, K.; Williams, G. C.; Hagger, M. Classification of Techniques Used in Self-Determination Theory-Based Interventions in Health Contexts: An Expert Consensus Study. [CrossRef]
- Nesbitt, K. V.; Kolodziejczyk, K.; Hoelzle, J. B.; Bruening, D. A. Immersive exercise in substance use disorder treatment: The intersection of technology, health, and clinical care. Subst. Abuse 2020, 41, 174–179. [CrossRef]
- Fleming, T.M.; de Beurs, D.; Khazaal, Y.; Gaggioli, A.; Riva, G.; Botella, C.; Baños, R.M.; Aschieri, F.; Bavin, L.M.; Kleiboer, A.; Merry, S.; Lau, H.M.; Riper, H. Maximizing the Impact of e-Therapy and Serious Gaming: Time for a Paradigm Shift. Front. Psychiatry 2016, 7, 65. PMID: 27148094; PMCID: PMC4834305. [CrossRef]
- Keshavarz, M.; Bahrani, M.; Ardabili, H.E.; Habibi, D. The effect of virtual reality cognitive-motor exercises on executive functions in individuals with substance use disorder. J. Subst. Use 2020, 25(2), 174-179. [CrossRef]
- Edwards, S.; Brice, C.; Craig, C.; Penri-Jones, R. Effects of caffeine, practice, and mode of presentation on Stroop task performance. Pharmacol. Biochem. Behav. 1996, 54(2), 309-315. PMID: 8743589. [CrossRef]
- Sibley, B. A.; Etnier, J. L.; Le Masurier, G. C. Effects of an Acute Bout of Exercise on Cognitive Aspects of Stroop Performance. J. Sport Exerc. Psychol. 2006, 28, 285–299. https://psycnet.apa.org/record/2006-11698-008.
Figure 1.
The IVR system equipment – (a) cycle ergometer and (b) VR mask and joysticks.

Figure 2.
Selection of exercise duration in the IVR system [31].
Figure 2.
Selection of exercise duration in the IVR system [31].
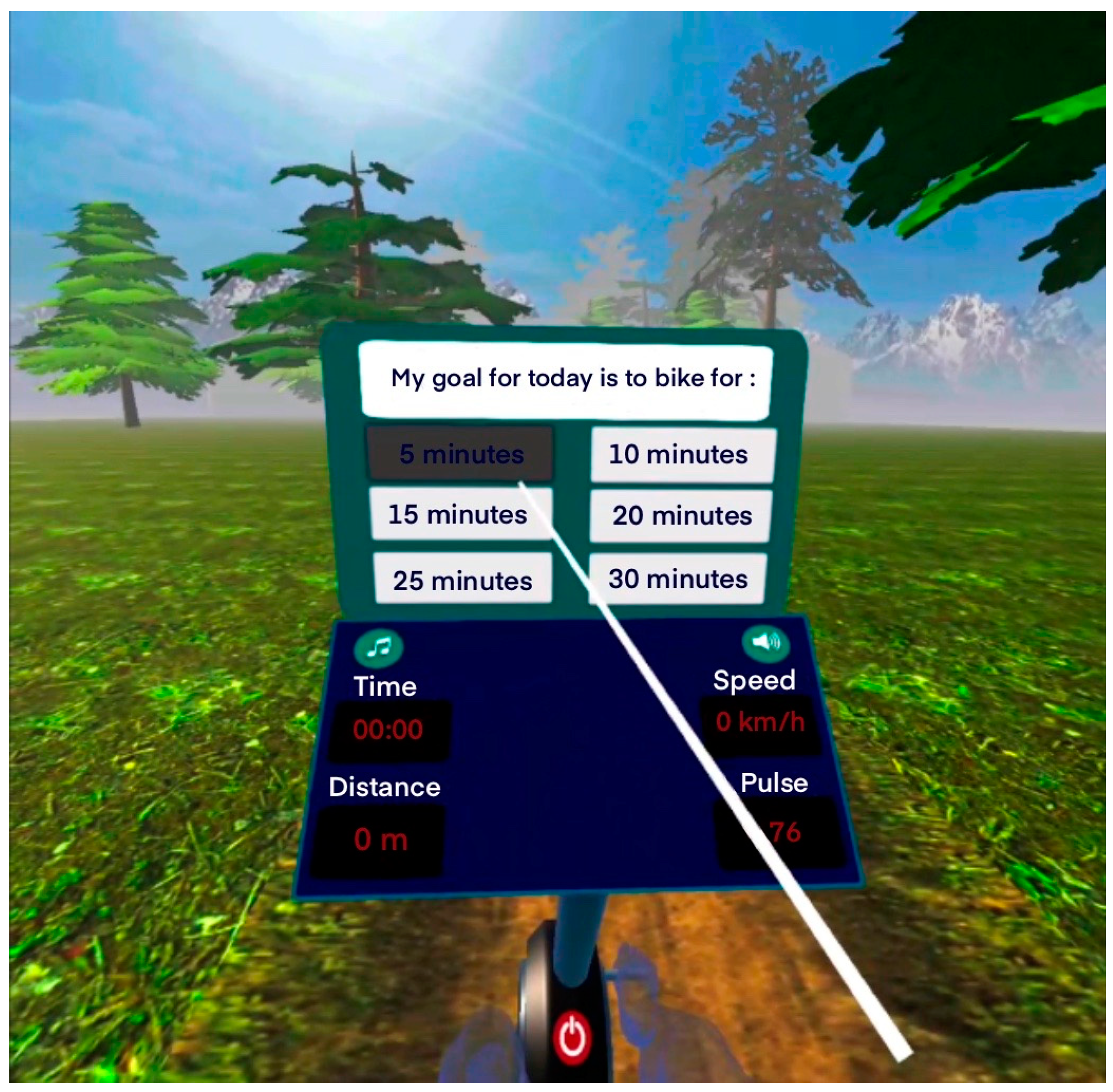
Figure 3.
Participant cycling in the IVR environment.
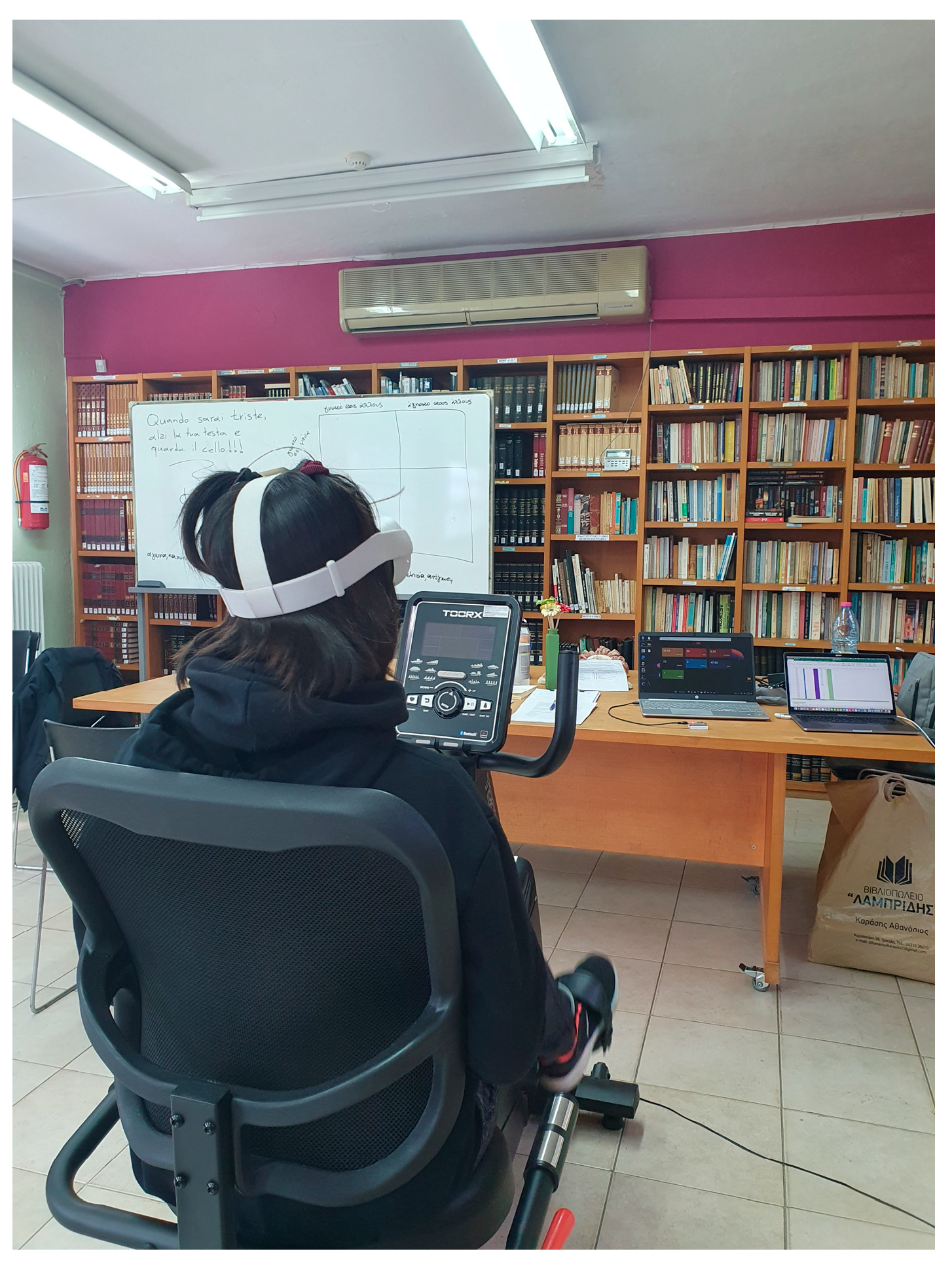

Table 1.
Demographic Characteristics.
| N=20 | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|
| Age | years | 37.75 | 8.33 | 24 | 54 |
| Sex | male, % | 90 | - | - | - |
| Educational level | Primary, % Secondary, % |
85% secondary 10% primary |
- | - | - |
| Exercise during treatment | yes, % | 50 | - | - | - |
| Treatment | days | 138.8 | 106.25 | 6 | 341 |
| Drug use | years | 19.4 | 9.88 | 1 | 37 |
Table 2.
Experimental procedure.
| Pre IVR exercise | Post IVR exercise | |
|---|---|---|
|
Self-selected duration IVR exercise |
|
Note: IVR= Immersive Virtual Reality, TCU= Texas Christian University Questionnaire, IPAQ= International Physical Activity Questionnaire, DASS-21= Depression Anxiety Stress Scales - 21 items.
Table 3.
Stroop test reaction time and mistakes. All data are presented as means and Standard Deviation (SD).
Table 3.
Stroop test reaction time and mistakes. All data are presented as means and Standard Deviation (SD).
| Stroop test | Pre IVR | Post IVR | P value, df | Pre IVR | Post IVR | P value, df |
|---|---|---|---|---|---|---|
| Naming | 60.9±13.1 | 51.9±7.6 | t(19)=4.178,p<.001 | 1.1±1.2 | 0.6±0.9 | t(19)=1.308, p=.21 |
| Reading | 41.9±5.4 | 40.2±6.2 | t(19)=3.202, p<.005 | 0.1±0.2 | 0.1±0.2 | t(19)= .152, p= 1.0 |
| Interference | 94.8±22.9 | 78.0±14.1 | t(19)= 6.242, p<.001 | 4.4±4.1 | 2.6±0.7 | t(19)=1.966, p=.06. |
Table 4.
Τhematic analysis of the semi-structured interview table.
| Main Theme | Subthemes | N | (%) |
|---|---|---|---|
| Reasons to use VRADA | Why would you use VRADA? | ||
| It is pleasant | 14 | 70% | |
| It is relaxing | 8 | 40% | |
| It is motivating | 3 | 15% | |
| Usability or utilization | General difficulties | ||
| None | 16 | 80% | |
| Difficulty adjusting to the speed limits | 3 | 15% | |
| Technical issues | |||
| None | 20 | 100% | |
| Joystick use difficulty | |||
| No | 20 | 100% | |
| VR mask use difficulties | |||
| None | 16 | 80% | |
| It was a little heavy | 2 | 10% | |
| It was a little tight | 2 | 10% | |
| Usability or learning | Need more time to understand the system | ||
| No | 20 | 100% | |
| Usability or pleasantness | Most enjoyable parts | ||
| The VR environment (landscape) | 15 | 75% | |
| Music | 3 | 15% | |
| Peacefulness and relaxation | 3 | 15% | |
| Least enjoyable parts | |||
| Repeated virtual parts, monotonous | 9 | 45% | |
| Graphics | 8 | 40% | |
| Music | 5 | 25% | |
| Feel uncomfortable | |||
| No | 20 | 100% | |
| Sense of presence or engagement | Distraction of attention | ||
| No | 19 | 95% | |
| Yes | 1 | 5% | |
| Duration of the experience | |||
| It could be more | 10 | 50% | |
| It was enough | 7 | 35% | |
| It could be more but I didn’t have time because of our demanding schedule | 3 | 15% | |
| Sense of presence or realism | VR environment was realistic or artificial | ||
| Artificial | 20 | 100% | |
| Tolerability | Feel bad during training | ||
| Νο | 20 | 100% | |
| Thinking of weird things | |||
| Νο | 20 | 100% | |
| Nausea, dizziness or other physical symptoms | |||
| Νο | 19 | 95% | |
| A little for the first seconds | 1 | 5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



