
Submitted:
24 June 2024
Posted:
26 June 2024
You are already at the latest version
Abstract
: Fluoride toxicity has become a global public health concern, and its significant source of exposure is drinking water. This study aimed to determine groundwater fluoride level and assess its related human health risks. Its level was measured from groundwater samples using an ion-selective electrode. The total hazard index was assessed based on the chronic daily oral intake and dermal absorbed dose of groundwater fluoride. Analyses were conducted using ArcGIS and SPSS. This study reported groundwater fluoride ranged from 0.3 mg/L to 38 mg/L, with a mean annual level of 15 mg/L. Groundwater fluoride level above 5 mg/L was reported in 60 % of the water samples. Total hazard index values among sampled locations varied from 0.18 to 22.56. Half (51.5 %) of infants, 85.5 % of children, 82.5 % of adolescents, and 67.5 % of adults had a risk of developing a non-carcinogenic health effect. This study demonstrated that the fluoride level of the groundwater sources was high, and the water was not suitable for drinking, a result that is of special importance for children and adults since they are a hypersensitive subgroup of the population.
Keywords:
Adama
; Wenji
; health quotient
; total hazard index
1. Introduction
Groundwater is widely used as a drinking water supply, for irrigation, and for industrial purposes [1]. It is microbiologically safe, and better protected from pollution and evaporation than surface water [1]. Due to geological or anthropogenic sources of pollution, groundwater may, however, contain compounds undesirable to human health, such as Fluoride (F-) [2]. Globally, more than 200 million people are exposed to groundwater F- concentrations that exceed the World Health Organization (WHO) guideline of 1.5 mg/L [3]. Such exposure leads to 70 million people worldwide suffering from skeletal fluorosis [4]. Africa Rift Valley regions, such as Kenya [5], Ethiopia, Tanzania,[6] and Malawi water sources, have substantially greater F- health hazards than other continents [7]. Moreover, in Ethiopia’s Rift Valley (ERV), 8 million people rely on water sources with high F- levels [7].
An average of 75 % to 90 % of ingested water F- is absorbed, mainly via the gastrointestinal tract, [4] and from there transported through the circulatory system in the human body [8]. Consumption of 0.8 to 1.5 mg/l F- in drinking water improves bone density, prevents caries, acts as an antibacterial agent in the mouth, and prevents osteoporosis [4]. In contrast, excessive F- (above 1.5 mg/L) intake is associated with diseases such as dental fluorosis, skeletal fluorosis, and systematic defects in small intestinal microvilli [9]. Furthermore, fluorosis can be non-skeletal, causing neurological symptoms [10], high blood pressure [11], effects on fetal development [12], and child attention-deficit hyperactivity disorder [13]. The plausible mechanisms may involve cellular damage, cell cycle arrest, DNA damage [14], endoplasmic reticulum stress, and inflammatory cell response [15].
There are a few local and national initiative in Ethiopia to rely only on water sources below the WHO guideline F- level of 1.5 mg/L [16], but these attempts have not been successful [17]. Due to the lack of safe water sources, which meet the WHO guidelines, it is challenging to achieve sustainable development goal no 6 [18]. Ethiopia, however, has a national drinking water F- guideline of 3 mg/L, thus admitting a certain degree of inevitable health risks [16]. Different approaches have been applied to estimate carcinogenic and non-carcinogenic health effects of F- from drinking water F- [19,20]. One such approach is health risk assessment (HRA), which associates the health risks with the daily intake of chemicals, e. g. F-, via water. It is determined by a total hazard index (THI) value. A THI value greater than or equal to one is an indicator for a high probability of developing non-carcinogenic health effects. While its value of less than one is considered to pose no health risk among the exposed population [21]. There is a lack of evidence concerning spatiotemporal variability of F- level, and the potential health effects on infants, children, adolescents, and adults have not been well studied. The aim of this study is, hence, to measure the groundwater F- level at Adama City and Wenji town, and to estimate its potential non-carcinogenic health effects.
2. Materials and Methods
2.1. Study setting description
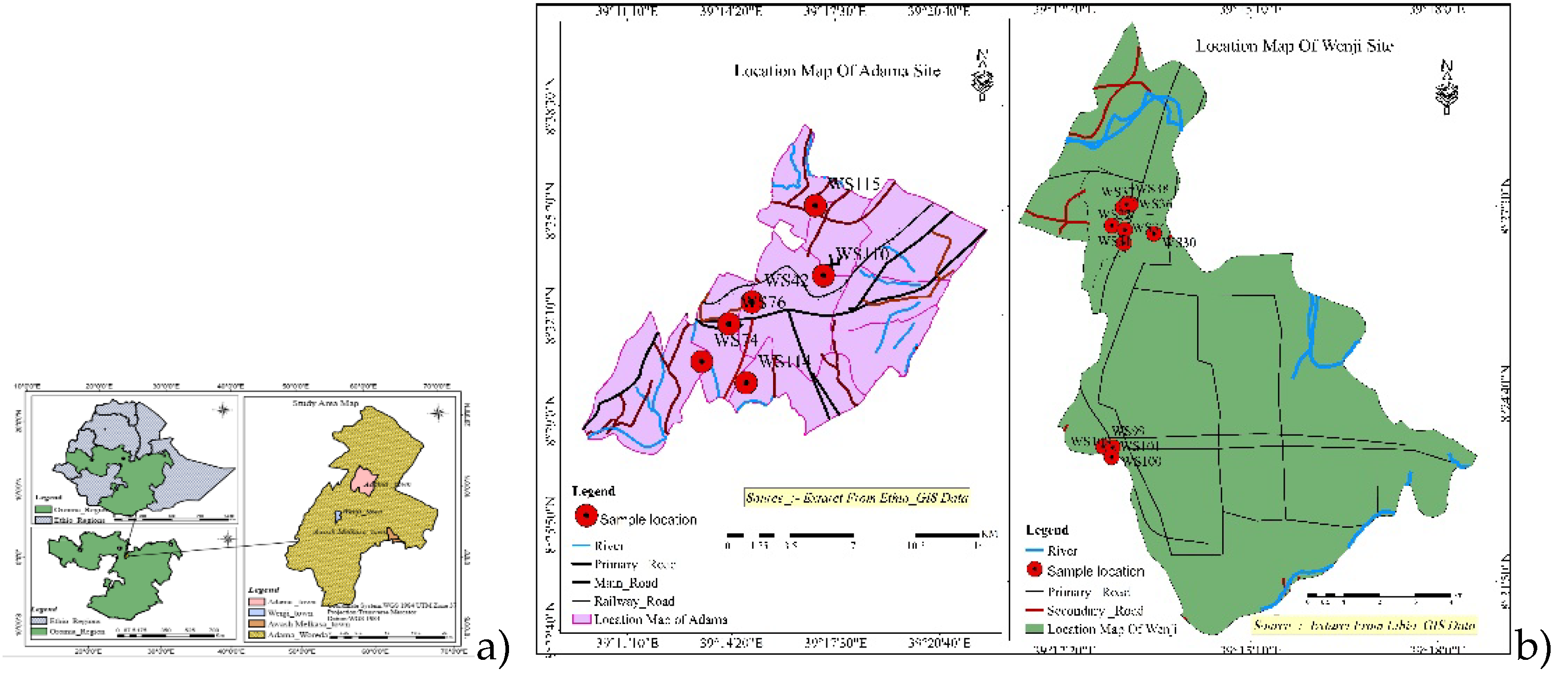
This study was performed in the Awash Basin Adama district in Ethiopia (Figure 1). The basin experiences a rainy season from June to September and a dry climate for the rest of the year with an annual mean temperature of 21.60c [22]. To provide Adama City with drinking water, there are several groundwater wells, which are used in addition to the treated main water supply [23]. The Wenji town residents access drinking water supply mainly from groundwater and rarely from treated public tap water. The projected total population of Wenji town and Adama city are 29, 886 and 214, 000 respectively [24].
2.2. Groundwater sample collection and geo-locating
We sampled 6 out of 6 wells in Adama, and 10 out of 17 wells in Wenji, the samples were collected during the wet season (August to September) and during the dry season (January to February) (Figure 1). The two-season sampling was done to accommodate the temporal variability of the groundwater F- level. The sample locations were selected from study sites and geo-recorded by using the smart Global Position System coordinate locator [25]. The samples were collected using a 50 ml polyethylene bottle which was rinsed with distilled water as well as with the actual groundwater before collecting the sample. The collected samples were stored at less than 4oC during the field campaign and during transportation and storage at the Addis Ababa University Water Resources Excellency Center laboratory according to the drinking water sample collection protocol described by USA EPA, (2016) [26].
2.3. Determination of fluoride concentration and quality control
The Ion Selective Electrode (ISE) method was used to determine groundwater F- concentration by using Crison-GLP 22 instrument in samples mixed at a 1:1 volume ratio with a total ionic strength adjustment buffer (TISAB) solution. A range of pH 5-5.5 was maintained during mixing the samples with buffer solution, to optimize the analyses [27]. A triplicate analysis was performed for each sample and an average value was recorded. Calibration of Crison-GLP 22 was performed before analysis, by using the 5 standard solutions of F- stock standard solution (1,000mg/L F) (CRISON INSTRUMENTS, S.A).
2.4. Exposure and health risk assessment of fluoride
The F- exposure is assessed as the chronic daily intake (CDI) through drinking water and dermally absorbed dose (DAD). A probabilistic non-carcinogenic health risks assessment was calculated according to the US EPA assumption of standard, which is the most practical method used to compare health risk analysis for chemicals in drinking water [28]. The study population was classified into four age categories: infants, children, adolescents and adults with quantitative values explained by Table 1 [28,29]. The exact location of study participants is not geocoded, but all study participants were permanent inhabitants of the towns, and we thus allocated their exposure based on mean levels of the towns they inhabited.
Non-carcinogenic health risk assessment was estimated by using hazard quotients for oral (HQoral) and dermal exposure (HQdermal).
Firstly, the CDI (mg/kg/day) was calculated using Equation 1.
where CW signifies the concentration of F- in groundwater (mg/L), IR is the ingestion rate (L/day), ED is the exposure duration (years), EF is the exposure frequency (days/ years), BW is the average body weight (Kg) and AT is the average time (days) (Average time over which exposure is averaged).
Secondly, the dermally absorbed daily dose (DAD, mg/kg/day) was calculated by using the Equation 2
Where TC is the contact duration (h/d) 0.4, Ki indicates the dermal adsorption parameters (cm/h: 0.001 cm/h), EV indicates the bathing frequency (times/day) 1 considered as time in a day), SSA is the skin surface area (cm2) 12,000 and 16,600 cm2 for children and females and 16,600 cm2 for males, CF indicates the conversion factors (0.001) and AT indicates the average time (days).
The results from Equation 1 and Equation 2 were used to estimate the non-carcinogenic health risk.
US EPA refers to the reference dose (RfD) of F- as 0.06 mg/kg/day which is no health risk [30]. The summation of HQoral and HQdermal is known as THI, in the case of this study for the non-carcinogenic health risk of F- through oral ingestion and dermal exposure combined.
2.5. Methodological considerations
The strength of this study is that it generated updated evidence on F- in groundwater accessible to communities. Wenji town has one public tap where water is scarce during the dry season and thus inaccessible. Additionally, a few households are accessing tap water every month or every two months from a private tap. Groundwater from a deep well found in Adama city center is blended into the main drinking water supply reservoir. Furthermore, it is distributed through car and horse-driven carts to different parts of the city. The limitation of this study is the lack of a geocoded location for each study participant, but the communities are permanent inhabitants of the towns. Additionally, exposure preference to beverages (tea, coffee, and alcohol) [31] and food [32] are not addressed by this study.
2.6. Statistical analysis
The data were entered into Microsoft Excel and exported to IBM (2011) IBM SPSS Statistics for Windows, Version 20. IBM Corp., Armonk, which was used for the descriptive statistics such as average, standard deviation, minimum, and maximum. Kruskal-Wallis Test was done, considering a significance level, P of less than 0.05. The map of sampling locations was developed by using Arc GIS 10.7.1 software (ESRI, Redlands, CA, USA). All GPS data which was collected to with degree, minutes, second coordinate system were converted to Universal Transverse Mercator (UTM) coordinates system.
2.7. Ethical consideration
The study has received ethical approval from Ethiopia Institute of Water Resources Addis Ababa University (Protocol No. EiWR043/11/18) and Armauer Hansen Research Institute (Protocol No. PO37/17). Additionally, a support letter was obtained from the local water supply and wastewater management authority. The data was handled with appropriate confidentiality.
3. Results
3.1. Level of fluoride in Groundwater
Groundwater pH and temperature ranged from 5.3 to 7.7 and from 21.5 to 280C respectively in the wet season. The F- concentration varied from 0.3 mg/L to 38 mg/L and 1.1 mg/L to 24 mg/L during the wet and dry seasons respectively. The mean annual F- concentration for Adama city and Wenji town were 1.9 mg/L and 23 mg/L respectively (Table 2).
The health effects of fluoride exposure in our study follow the WHO public health guideline of fluoride for drinking water i.e., 1.5 mg/l. Of our groundwater samples, 70 % (during the wet season) and 45 % of samples (during the dry season) had a F- level surpassing 5 mg/L (Supplementary materials). There is no significant difference of the F- level across the measurement sites in Wenji groundwater sources.
3.2. Health risk Assessment
A health risk assessment, expressed as THI of groundwater F- exposure via oral and dermal routes were performed to estimate non-carcinogenic health effects of infants, children, adolescents, and adults.
The CDI, DAD and their respective HQ were calculated according to equations 1-4 for the study groups during different seasons. The results are shown in Table 3. THI varied from 0.18 to 22.56, and 0.69 to 14.16 for study groups in wet and dry seasons, respectively.
On average, a large portion of the study population was at high probability of developing non-carcinogenic health effects due to groundwater fluoride exposure. For example, 70% of infants, 80% of children, 70% of adolescents, and 60% of adults had THI>1 in the wet season. In the dry season, 33% of infants, 91% of children, 83% of adolescents, and 75% of adults had THI >1 (Segmentary material). Table 3 describes the residents in Wenji town having a higher probability of developing non-carcinogenic health effects than the population in Adama city. Variation was observed in the probability of developing non-carcinogenic health effects according to THI value in the wet season for study population in Adama city and Wenji town. The wet season means THI values ranged from 0.01-35.89. Likewise, the dry season ranged from 0.16-22.53.
4. Discussion
In this study, groundwater F- level during the wet and dry seasons were assessed, and non-carcinogenic health risks were estimated using THI. There is a variation in the concentration of F- in Adama City and Wenji Town. These variations are due to the difference in aquifer types, for example, Wenji town and Adama city are alluvium and fractured crystalline aquifers respectively. Groundwater F- level in Adama city and Wenji town is higher during the dry and wet seasons respectively. Dry season high fluoride levels in Adama city agree with the previous study [33]. Evidence indicates that F- concentration depends on the depth of the well; shallow wells are highly vulnerable to anthropogenic activities such as agricultural activities [33]. However, another study reported that the F- level decreases with increment of well depth [34]. In our study, the Adama dry season maximum F- level was 3.55mg/L while the wet season was 1.49 mg/L. But the vice versa is true for Wenji town. Wet season high F- level in Wenji town is subject to anthropogenic sources of pollution due to runoff. High level of F- in Wenji town due to the interior part of the well not being lined, compared to Adamas which is lined at the top as well as protected by the concrete box. Being not lined facilitates the soil-groundwater interaction and contributes to high F- level. In Wenji town, large sugarcane plantation farms are applied herbicides and fertilizers which is an anthropogenic source of F- in groundwater [35].
Our finding revealed that the mean groundwater F- level is greater than countries located in the Global Rift Valley such as India [36], Iran [37], and Uganda [38]. Our study showed a mean F- level of 14.42 mg/L, which is higher than the mean F- level of 6.03 mg/l reported in the systematic review by Demelash et al., in Ethiopia Rift Valley [39]. The F- level of 0.3-38 mg/L suggest that the Adama-Wenji region is a hotspot for fluoride groundwater levels due to geological situations compared to other non-rift valley areas [40]. In this region, 16% of the groundwater samples were within the WHO guidelines. Indeed, the population in the study area is at risk for different types of fluorosis.
A finding from Tanzania, consumption of 4.7 mg/L of drinking water F- is associated with a 96.3% prevalence of dental fluorosis [41]. 50% of groundwater samples in Adama-Wenji are greater than 5 mg/L of F-. Indeed, the residents are exposed to F- levels that have the potential to cause fluorosis. In the Adama-Wenji region, the THI values were highest in the children group 1.23-19.26, followed by adolescents 0.87-13.83, adults 0.82-13.06, and infants 0.18-27.68 in that order. Recently, Haji et al reported THI values for groundwater F- exposure in the Southern Main Ethiopian Rift ranging from 0.75 to 8.44, 0.34–3.84 and 0.27–3.01 for children, women, and men, respectively [20]. A resident living in Adama and Wenji Rift Valley has a higher probability of developing F-related health effects compared to another non-rift valley area due to groundwater. Previous studies from part of Global Rift Valley countries such as India [21] and Iran [37] have reported mean values of HQoral for children, adolescents, and adults. Our finding reported that children and adults are higher than infants and adolescents for the probability of developing a non-carcinogenic health effect due to F- exposure. Similar findings have been reported from different parts of the Global Rift Valley such as Iran [29], Pakistan [42], Ghana [43] and India [44].
Adama-Wenji seasonal variation revealed that in the wet season, 70% of infants, 80% of children, 70% of adolescents, and 60% of adults had a higher risk value of THI. While, in the dry season, this was true for 33% infants, 91% children, 83% adolescents and 75% adults. Similarly, N. Adimalla et al 2019 reported a high probability of developing health effects from consumption of F- enriched groundwater in India men and women were 67.65% and 79.41% respectively with a value of THI greater than one, but for children the risk was even higher i.e., 82.35% [44]. Also, Yousefi et al reported that children and adolescents were at higher probability than the rest of the population developing non-carcinogenic health effects [45]. Furthermore, Rango et al reported that the effect of dental fluorosis leads to children being reluctant to smile and speak as well as being challenged with food choices and with less chewing efficacy [7]. THI values and its related health hazards from our finding could be expected due to the consumption of water with high F- level. We have no socio-demographic data for the actual study groups. But national age composition can support the age categories that are used to perform the risk assessment. Still, there is 4% of Ethiopians are age 65 or older and age categories less or equal to 65 account for 96% [46].
5. Conclusion
This study demonstrated that the high groundwater F- level in Ethiopia’s Awash basin make the water sources unsuitable for domestic purposes and undesirable for human health. Wenji town's mean groundwater F- level is fifteen times higher than the WHO drinking water guideline. But Adama city is less than Ethiopia's drinking water guidelines but greater than WHO. Sensitive groups of communities such as children and adolescents are at higher risk of developing non-carcinogenic health risks. The finding indicates an alarming stage of developing health risks from using F- contaminated groundwater sources among the communities. Furthermore, THI risk evaluation through oral and dermal exposure due to groundwater alone underestimates the actual risk of F- exposure. Therefore, applying a more inclusive risk evaluation of fluoride exposure via food and beverages will improve.
6. Implication
The annual mean groundwater F- level in the Adama City and Wenji Twon were 1.9 mg/L and 23 mg/L respectively. Wenji Town is higher than the Ethiopia National (3 mg/L) and the WHO (1.5 mg/L) guidelines. There is no applicable monitoring of fluoridation or fluoridation of drinking water supply in suburban and rural parts of Ethiopia but only few in cities. However, there are attempts to apply locally adopted defluorination techniques in the Ethiopia Rift Valley. But still, residents at North Ethiopia Rift Valley are subjected to higher levels of groundwater F- exposure due to a lack of safe water sources. Dental and skeletal fluorosis are well known public health problems due to drinking water F-, but other systematic effects are overlooked. Our findings highlight the probability of developing non-carcinogenic health effects due to groundwater F-. Accordingly, children and adolescents are at higher risk of developing different F- related health problems. F- exposure assessments, and quantifications of health risks, play a profound role in motivating policies and guidelines to protect public health.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Proportion of groundwater fluoride level in study area during dry and wet season; Table S2: Estimated daily intake, Health quotient and THI of groundwater fluoride for study population-based season.
Author Contributions
Conceptualization, A.A. (Asmamaw Abera), E.M., C.I., G.S. and A.A. (Abraham Aseffa); methodology, A.A. (Asmamaw Abera), B.M., A.A. (Abraham Aseffa), E.M., G.S. and C.I.; software, A.A. (Asmamaw Abera); validation, A.A. (Asmamaw Abera), G.S, B.M, E.M, and C.I.; formal analysis, A.A. (Asmamaw Abera), G.S., B.M, E.M, C.I and A.A. (Abraham Aseffa); investigation, A.A. (Asmamaw Abera), E.M., C.I., G.S. and A.A. (Abraham Aseffa); resources, G.S. and A.A. (Abraham Aseffa); data curation, A.A. (Asmamaw Abera), E.M., C.I. and G.S.; writing—original draft preparation, A.A. (Asmamaw Abera); writing—review and editing, A.A. (Asmamaw Abera), C.I., B.M., E.A., G.S., A.A. (Abraham Aseffaa); visualization, A.A. (Asmamaw Abera), C.I., G.S.; supervision, C.I., A.A. (Abraham Aseffa), and G.S.; project administration, E.M., C.I., and G.S.; funding acquisition, G.S., A.A. (Abraham Aseffaa). All authors have read and agreed to the published version of the manuscript.
Funding
This research was financially supported by the Armauer Hansen Research Institute Department of Non-Communicable Diseases under Biomedical Science Student PhD Project (BSSP), Swedish International Development Cooperation Agency SIDA.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors acknowledge the support given by Surafel Girma, Eyuel Asemahegn Bogale, Ali Gebeyewu, Fregenet Tesfaye, Eden Eritrea Desalegn and Mohammedsalih Hussen Ibrahim.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- E. Koncagül, M. Tran, and R. Connor, “The United Nations World Water Development Report 2021 Facts and figures VALUING WATER World Water Assessment Programme United Nations Educational, Scientific and Cultural Organization,” UNESCO, Paris, Mar. 2021. [Online]. Available: www.unesco.org/.
- F. Ligate et al., “Groundwater resources in the East African Rift Valley: Understanding the geogenic contamination and water quality challenges in Tanzania,” Sci. African, vol. 13, p. e00831, Sep. 2021. [CrossRef]
- E. Shaji, K. V. Sarath, M. Santosh, P. K. Krishnaprasad, B. K. Arya, and M. S. Babu, “Fluoride contamination in groundwater: A global review of the status, processes, challenges, and remedial measures,” Geosci. Front., vol. 15, no. 2, p. 101734, Mar. 2024. [CrossRef]
- J. Fawell, K. Bailey, J. Chilton, E. Dahi, and Y. Magara, Fluoride in drinking-water, 4th ed. London, UK: IWA publishing, 2006.
- J. Podgorski and M. Berg, “Global analysis and prediction of fluoride in groundwater,” Nat. Commun., vol. 13, no. 1, p. 4232, Aug. 2022. [CrossRef]
- J. Malago, E. Makoba, and A. N. . Muzuka, “Fluoride Levels in Surface and Groundwater in Africa: A Review,” Am. J. Water Sci. Eng., vol. 3, no. 1, p. 1, 2017. [CrossRef]
- T. Rango et al., “Groundwater Quality And Its Health Impact: An Assessment Of Dental Fluorosis In Rural Inhabitants Of The Main Ethiopian Rift,” Environ. Introd. , vol. 43, no. 1, pp. 37–47, Aug. 2012. [CrossRef]
- S. K. Jha, V. K. Mishra, D. M. Sharma, and T. Damodaran, “Fluoride in the Environment and Its Metabolism in Humans ,” Rev. Environ. Contam. Toxicol., vol. 211, pp. 121–142, 2011. [CrossRef]
- D. Mulualem, D. Hailu, M. Tessema, and S. J. Whiting, “Association Of Dietary Calcium Intake With Dental, Skeletal And Non-Skeletal Fluorosis Among Women In The Ethiopian Rift Valley,” Int. J. Environ. Res. Public Heal. , vol. 19, no. 4, p. 2119, Feb. 2022. [CrossRef]
- B. A. Ayele, T. R. Godebo, R. Tekle-Haimanot, and Y. M. Yifru, “Neuro-medical manifestations of fluorosis in populations living in the Main Ethiopian Rift Valley,” Environ. Geochem. Health, vol. 44, no. 3, pp. 1129–1136, Mar. 2022. [CrossRef]
- M. Davoudi et al., “Relationship of fluoride in drinking water with blood pressure and essential hypertension prevalence: a systematic review and meta-analysis,” Int. Arch. Occup. Environ. Health, vol. 9, no. 4, pp. 1137–1146, 2021.
- NRC, Fluoride in Drinking Water: A scientific review of EPA’s standards. Washington, D.C.: National Academies Press, 2007. [CrossRef]
- A. J. Malin and C. Till, “Exposure to fluoridated water and attention deficit hyperactivity disorder prevalence among children and adolescents in the United States: an ecological association,” Environ. Heal., vol. 14, no. 1, p. 17, Dec. 2015. [CrossRef]
- H. Zuo et al., “Toxic effects of fluoride on organisms,” Life Sci., vol. 198, pp. 18–24, Apr. 2018. [CrossRef]
- S. Zhang et al., “Fluoride-elicited developmental testicular toxicity in rats: Roles of endoplasmic reticulum stress and inflammatory response,” Toxicol. Appl. Pharmacol., vol. 271, no. 2, pp. 206–215, Sep. 2013. [CrossRef]
- Federal Democratic Republic Of Ethiopia Ministry Of Water Resources, “Ethiopian Water Technology Centre Ministry Of Water Resources (Mows) Butajira-Ziway Areas water quality Development Study,” Addis Ababa, Nov. 2008. Accessed: Nov. 25, 2021. [Online]. Available: https://www.scribd.com/document/477752551/fdocuments-us-pdf3232kb.
- H. A. Mengistu, M. B. Demlie, and T. A. Abiye, “Review: Groundwater resource potential and status of groundwater resource development in Ethiopia,” Hydrogeol. J., vol. 27, no. 3, pp. 1051–1065, May 2019. [CrossRef]
- L. Kaur, M. S. Rishi, and A. U. Siddiqui, “Deterministic and probabilistic health risk assessment techniques to evaluate non-carcinogenic human health risk (NHHR) due to fluoride and nitrate in groundwater of Panipat, Haryana, India,” Environ. Pollut., vol. 259, p. 113711, Apr. 2020. [CrossRef]
- M. Bodrud-Doza, S. M. D.-U. Islam, T. Rume, S. B. Quraishi, M. S. Rahman, and M. A. H. Bhuiyan, “Groundwater quality and human health risk assessment for safe and sustainable water supply of Dhaka City dwellers in Bangladesh,” Groundw. Sustain. Dev., vol. 10, p. 100374, Apr. 2020. [CrossRef]
- M. Haji, S. Karuppannan, D. Qin, H. Shube, and N. S. Kawo, “Potential Human Health Risks Due to Groundwater Fluoride Contamination: A Case Study Using Multi-techniques Approaches (GWQI, FPI, GIS, HHRA) in Bilate River Basin of Southern Main Ethiopian Rift, Ethiopia,” Arch. Environ. Contam. Toxicol., vol. 80, no. 1, pp. 277–293, Jan. 2021. [CrossRef]
- V. Laxmi Mohanta, S. Singh, and B. Kumar Mishra, “Human health risk assessment of fluoride-rich groundwater using fuzzy-analytical process over the conventional technique,” Groundw. Sustain. Dev., vol. 10, p. 100291, Apr. 2020. [CrossRef]
- M. Mulugeta, D. Tolossa, and G. Abebe, “Description of long-term climate data in Eastern and Southeastern Ethiopia,” Data Br., vol. 12, pp. 26–36, Jun. 2017. [CrossRef]
- S. Karuppannan and N. Serre Kawo, “Groundwater Quality Assessment Using Geospatial Techniques and WQI in North East of Adama Town, Oromia Region, Ethiopia,” Hydrospatial Anal., vol. 3, no. 1, pp. 22–36, Jan. 2020. [CrossRef]
- Worldometers.info, “Ethiopia Demographics,” Dec. . Accessed: Dec. 21, 2023. [Online]. Available: https://www.worldometers.info/demographics/ethiopia-demographics/.
- Go Get International LLC, “Smart GPD Coordinate Locator .” Accessed: Dec. 09, 2021. [Online]. Available: https://play.google.com/store/apps/details?id=com.dga.smart.gpslocation.share.photostamp.
- USAEPA, “Quick Guide To Drinking Water Sample Collection.” W 45th Dr. Golden, CO 80403, USA, 2016. [Online]. Available: https://www.epa.gov/sites/default/files/2015-11/documents/drinking_water_sample_collection.pdf.
- APHA, Standard Methods For The Examination Of Water And Wastewater, 18th ed. Washington, DC: American Public Health Association, American Water Works Association and Water Environment Federation, 1992.
- USEPA, Exposure Factors Handbook. National Center for Environmental Assessment, Washington, DC, 2011th ed. Springfield, VA: National Technical Information Service, Springfield, VA, 2011.
- M. Ghanbarian, M. Ghanbarian, T. Tabatabaie, M. Ghanbarian, and S. K. Ghadiri, “Distributing and assessing fluoride health risk in urban drinking water resources in Fars Province, Iran, using the geographical information system,” Environ. Geochem. Health, vol. 44, no. 3, pp. 771–781, Mar. 2022. [CrossRef]
- USEPA, Guidelines For Human Exposure Assessment. Washington, D.C: Risk Assessment Forum, U.S. EPA, 2019. [Online]. Available: http://www.epa.gov/risk.
- R. Satou, S. Oka, and N. Sugihara, “Risk assessment of fluoride daily intake from preference beverage,” J. Dent. Sci., vol. 16, no. 1, pp. 220–228, Jan. 2021. [CrossRef]
- A. De et al., “Fluoride Exposure and Probabilistic Health Risk Assessment Through Different Agricultural Food Crops From Fluoride Endemic Bankura and Purulia Districts of West Bengal, India,” Front. Environ. Sci., vol. 9, Aug. 2021. [CrossRef]
- H. U. U. Dibal, W. N. N. Dajilak, I. C. C. Lekmang, L. W. W. Nimze, and E. Y. Y. Yenne, “Seasonal Variation in Fluoride Content in Groundwaters of Langtang Area, Northcentral Nigeria,” Contemp. Trends Geosci., vol. 6, no. 1, pp. 11–27, Jun. 2017. [CrossRef]
- A. Yasar, T. Javed, F. Kausar, J. Shamshad, M. U. Hayat Khan, and R. Iqbal, “Ground water toxicity due to fluoride contamination in Southwestern Lahore, Punjab, Pakistan,” Water Supply, vol. 21, no. 6, pp. 3126–3140, Sep. 2021. [CrossRef]
- R. Fuge, “Fluorine in the environment, a review of its sources and geochemistry,” Appl. Geochemistry, vol. 100, pp. 393–406, Jan. 2019. [CrossRef]
- N. Adimalla and H. Qian, “Spatial distribution and health risk assessment of fluoride contamination in groundwater of Telangana: A state-of-the-art,” Geochemistry, vol. 80, no. 4, p. 125548, Dec. 2020. [CrossRef]
- M. Yousefi, M. Ghoochani, and A. Hossein Mahvi, “Health risk assessment to fluoride in drinking water of rural residents living in the Poldasht city, Northwest of Iran,” Ecotoxicol. Environ. Saf., vol. 148, pp. 426–430, Feb. 2018. [CrossRef]
- M. Egor and G. Birungi, “Fluoride contamination and its optimum upper limit in groundwater from Sukulu Hills, Tororo District, Uganda,” Sci. African, vol. 7, pp. e00241–e00241, Mar. 2020. [CrossRef]
- H. Demelash, A. Beyene, Z. Abebe, and A. Melese, “Fluoride concentration in ground water and prevalence of dental fluorosis in Ethiopian Rift Valley: systematic review and meta-analysis,” BMC Public Health, vol. 19, no. 1, p. 1298, Dec. 2019. [CrossRef]
- R. Tekle-Haimanot et al., “The geographic distribution of fluoride in surface and groundwater in Ethiopia with an emphasis on the Rift Valley,” Sci. Total Environ., vol. 367, no. 1, pp. 182–190, Aug. 2006. [CrossRef]
- E. A. M. A. M. Vuhahula, J. R. P. R. P. Masalu, L. Mabelya, and W. B. C. B. C. Wandwi, “Dental fluorosis in Tanzania Great Rift Valley in relation to fluoride levels in water and in ‘Magadi’ (Trona),” Desalination, vol. 248, no. 1–3, pp. 610–615, Nov. 2009. [CrossRef]
- S. Noor, A. Rashid, A. Javed, J. A. Khattak, and A. Farooqi, “Hydrogeological properties, sources provenance, and health risk exposure of fluoride in the groundwater of Batkhela, Pakistan,” Environ. Technol. Innov., vol. 25, p. 102239, Feb. 2022. [CrossRef]
- S. Y. Ganyaglo et al., “Groundwater fluoride contamination and probabilistic health risk assessment in fluoride endemic areas of the Upper East Region, Ghana,” Chemosphere, vol. 233, pp. 862–872, Oct. 2019. [CrossRef]
- N. Adimalla, P. Li, and H. Qian, “Evaluation of groundwater contamination for fluoride and nitrate in semi-arid region of Nirmal Province, South India: A special emphasis on human health risk assessment (HHRA),” Hum. Ecol. Risk Assess. An Int. J., vol. 25, no. 5, pp. 1107–1124, Jul. 2019. [CrossRef]
- M. Yousefi et al., “Spatial Distribution Variation and Probabilistic Risk Assessment of Exposure to Fluoride in Ground Water Supplies: A Case Study in an Endemic Fluorosis Region of Northwest Iran,” Int. J. Environ. Res. Public Health, vol. 16, no. 4, p. 564, Feb. 2019. [CrossRef]
- Ephi and ICF, “Ethiopian public health Institute (EPHI)[Ethiopia] and ICF,” Ethiop. mini Demogr. Heal. Surv., 2019.
Figure 1.
Description of study area (a) Oromia Regiona State Ethiopia (b) samplinglocation of Adama City and Wenji town.
Figure 1.
Description of study area (a) Oromia Regiona State Ethiopia (b) samplinglocation of Adama City and Wenji town.

| Model parameter | Unit | Exposure groups | |||
|---|---|---|---|---|---|
| Infants (less than 2 years) |
Children (2 to <6 years) |
Adolescents (6 to <16 years) |
Adults (≥16 years) |
||
| Ingestion rate | Liter/day | 0.08 | 0.85 | 2 | 2.5 |
| Average body weight | Kg | 10 | 15 | 50 | 75 |
| Average time-days | Days | 730 | 2,190 | 5,840 | 25,550 |
| Exposure duration | Years | 2 | 6 | 16 | 70 |
| Exposure frequency | Days/years | 365 | 365 | 365 | 365 |
| Reference dose (RfD) F- | Mg/kg/day | 0.06 | 0.06 | 0.06 | 0.06 |
Table 2.
Descriptive statistics of groundwater F- (mg/L) during wet and dry seasons. .
| Statistical values | Adama city | Wenji town | ||
|---|---|---|---|---|
| wet season | dry season | wet season | dry season | |
| Median | 1.77 | 0.56 | 16.99 | 29.60 |
| Min | 0.92 | 0.30 | 1.16 | 5.8 |
| Max | 3.55 | 1.49 | 23.83 | 38 |
| Stand. dev | 1.02 | 0.63 | 9.22 | 10.54 |
| average | 1.85 | 0.78 | 14.42 | 27.08 |
| Annual mean | 1.9 | 23 | ||
Table 3.
Description of CDI, THI and HQ exposure groups of study groups at Adama city and Wenji town.
Table 3.
Description of CDI, THI and HQ exposure groups of study groups at Adama city and Wenji town.
| Study site | Risk index parameter | Exposure groups | |||
|---|---|---|---|---|---|
| Infants | Children | Adolescents | Adults | ||
| Adama City | CDIoral | 0.01 | 0.07 | 0.05 | 0.05 |
| HQoral | 0.17 | 1.23 | 0.87 | 0.82 | |
| THI | 0.18 | 1.23 | 0.87 | 0.82 | |
| Wenji Town | CDIoral | 1.66 | 1.18 | 0.83 | 0.78 |
| HQoral | 27.27 | 19.60 | 13.83 | 13.06 | |
| THI | 27.68 | 19.61 | 13.83 | 13.06 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



