
Submitted:
26 June 2024
Posted:
26 June 2024
You are already at the latest version
Abstract
Balance is important in lifesaving competitions. We aimed to investigate the relationship between dynamic balance and physical function in elite lifesavers by measuring the foot muscle cross-sectional area, ankle joint muscle strength, toe grasp strength, plantar superficial sensation, and dynamic balance. In this observational study, we measured the foot muscle cross-sectional area, ankle dorsiflexion, plantar flexion, external flexion, isometric muscle strength, toe grasp strength, and superficial foot sensation of 15 adult lifesavers (12 males). The results showed that toe grasp strength and ankle plantar flexion isometric muscle strength are particularly important for the dynamic balance function of elite lifesavers working on sandy surfaces. Sand training improves intrinsic muscle training and dynamic balance function. However, high training intensity may cause a decrease in plantar surface sensation, which needs to be verified with sand training interventions in the future.
Keywords:
dynamic balance
; lifesaver
; sand training
; sandy beach
1. Introduction
Lifesaving is a sport in which participants compete in activities at sea, such as rescue and basic life support. These events are certified by the International Life Saving Federation and are separated into surf events performed at the seaside and beach events performed on the beach [1]. Lifesaving is recognized by the International Olympic Committee but not yet included in the Olympic program.
Lifesaving competitions are performed barefoot in environments with unstable footing such as beaches. These environments have attracted attention because they increase physical strength, leg strength, balance function, proprioceptive sensation, and spatial cognitive ability [2,3,4]. However, few studies have been conducted on lifesaving.
Compared with healthy adults, lifesavers have more developed intrinsic muscles in their foot [5], suggesting that the cross-sectional area thereof and strength of the toe grasp may be necessary for sand sports. Lifesavers run on unstable footing and may require a higher balance function using complex factors such as toe grasp strength, muscle strength around the ankle joint, ankle joint position sense, and plantar superficial sensation during foot contact on sandy ground compared with healthy people. However, it is not certain which foot function influences dynamic balance in athletic environments with unstable footing compared with athletes in other sports on hard ground [3,6,7,8]. We, therefore, aimed to clarify the physical characteristics of lifesavers operating in an unstable environment and effects of sand training by evaluating foot morphology and function.
2. Materials and Methods
2.1. Participants and Design
Fifteen elite lifesavers (12 male individuals, ≥18 years old) belonging to a lifesaving club were included. We excluded lifesavers with a history of lower limb surgery; lower limb trauma or disability within 6 months; and diabetes, joint disease, or neurological disease. The foot muscle cross-sectional area, ankle joint muscle strength, toe grasp strength, plantar superficial sensation, and muscle activity were measured. Fifteen participants were required for the present study design to achieve a power of 80%, an effect size (r) of 0.7, and an alpha level of 0.05.
The study was approved by the Ethics Committee of Waseda University (No. 2020-227). The participants were fully informed about the experiment before the experiment, and their written consent was obtained.
2.2. Ultrasound Imaging
The muscle cross-sectional area (short-axis image) was acquired in B-mode using an ultrasound imaging system (Aplio a Verifia, Canon Medical Systems Corporation, Japan) and linear probe (L55, 7.5 MHz). The participant sat and placed both feet on a template filled with water in a tank made of polymethylpentene resin, with the ankle joint in 0° dorsiflexion and the knee joint in 90° flexion, and the weight of the upper body placed behind the hands to minimize the application of weight on the foot [5,9,10]. The intrinsic (abductor hallucis brevis, abductor digiti minimi, flexor digitorum brevis, and flexor hallucis brevis) and extrinsic (peroneal longus and brevis, flexor hallucis longus, tibialis anterior, extensor digitorum longus, tibialis posterior, and flexor digitorum longus) muscles of the foot were measured. The extrinsic muscles of the foot and abductor digiti minimi were measured by applying the ultrasound probe to the skin, while the intrinsic muscles of the foot were measured from the plantar surface of the tank. The pressure from the probe was kept to a minimum to prevent force on the tissues, and ultrasound gel was applied to the skin and probe for all measurements. The probe was removed for each measurement of each muscle, and three measurements were obtained, with the average value used for analysis. The ultrasound scanning protocol was performed in accordance with previous studies’ protocols [5].
2.3. Ankle Isometric Muscle Strength Testing
Isometric muscle strength during dorsiflexion, plantar flexion, and external rotation of the right ankle joint was measured using a handheld dynamometer (HHD) (ANIMA, Tokyo, Japan). For dorsiflexion muscle strength, the participant was instructed to lie supine with hip joint internal/external rotation at 0° and grasp the sides of the bed. The belt attached to the HHD was fixed to the dorsal metatarsal head at 0° plantar dorsiflexion of the ankle joint, and the position was adjusted such that the belt and direction of muscle exertion were parallel. For plantar flexion muscle strength, the participant was instructed to kneel at 90° of the knee joint and place their hands on the ground. The belt attached to the HHD was fixed to the plantar side of the metatarsal head at 0° plantar dorsiflexion of the ankle joint, and the position was adjusted such that the belt and direction of muscle exertion were parallel. To measure abduction strength, a pillow was placed under the lower leg such that the right hip joint was in 0° of abduction in the left lateral recumbent position. The HHD was grasped and fixed to the base of the fifth metatarsal. Measurements were performed three times for a maximum muscle exertion of 5 s. The mean value normalized to body weight was used as the representative value [11].
2.4. Toe Grasp Force Measurement
A pressure sensor (BIGMAT, NITTA, Osaka, Japan), was used to measure toe pressure. The right foot was measured on the right side in all cases. The right foot was measured in all cases. The load on both legs was equalized at shoulder width during the measurement, and the participants were instructed to flex their toes toward the heel as much as possible while pressing hard on the ground (Figure 1). The maximum pressure of the big toe and toes 2–5 combined was calculated, and the average value of the five measurements was divided by the body weight as a representative value, normalized (% BW), and used for the analysis.
2.5. Superficial Sensory Measurements
Superficial sensory measurements of the feet were performed using a Semes–Weinstein monofilament (Sakai Medical Co., Ltd., Tokyo, Japan), taken at nine plantar points: the basolateral side of the fifth phalanx, basolateral side of the third phalanx, basolateral side of the first phalanx, basolateral side of the fifth metatarsophalangeal (MTP) joint, third MTP joint, first MTP joint, basolateral side of the fifth metatarsal base, basolateral side of the navicular bone, and central heel area (Figure 2). The participants closed their eyes and were placed in the supine position with the knee extended and the foot in a supinated position. The examiner lowered the filament vertically from 2.5 cm above the plantar foot for 1.5 s and applied pressure until the filament was deflected for 1.5 s, according to previous studies [12]. The participants were instructed to respond by raising their voice or hand when they felt filament contact; if they did not respond, the filament thickness was increased. The measurements were performed three times with the same filament at each location, and the value of the filament gaining a response to all three occasions was recorded.
2.6. Dynamic Balance Measurement
The maximum reaching distances to the anterior, posterior lateral, and posterior medial sides were measured when the right leg was supported using a Y-balance test kit (Perform Better Japan, Cranston, RI). Limb position was measured with both hands fixed to the waist, thrice in each direction. If the outstretched leg touched the ground, the hand left the waist, or the heel of the axis foot floated, the measurement was judged to have failed and was repeated.
The value obtained by dividing the sum of the maximum reach distances in the three directions was recorded, normalized by the leg length, and used as the representative value in the analysis. Leg length was measured as the distance from the superior anterior iliac spine to the medial cuticle using a tape measure [13]. A surface electromyogram was attached during measurement, and muscle activity at maximum reach was assessed. The participants held a maximum reaching position for 1 s, and muscle activity during 1 s was recorded.
2.7. Surface Muscle Activity Analysis
The activity of the peroneal muscles of the foot was recorded and analyzed during the dynamic balance test using Biosignal splux (PLUX wireless Biosignals, Portugal) and Gelled Self-Adhesive Disposable Ag/AgCl Electrodes (PLUX wireless Biosignals Portugal). The muscles measured were the abductor digiti adductus (AH), abductor digiti minor (AD), tibialis anterior (TA), peroneus longus (PL), peroneus brevis (PB), medial gastrocnemius (MG), and soleus (SL), with electrodes applied at the following locations: AH, one transverse finger below the navicular tubercle; AD, one transverse finger behind the base of the fifth metatarsal; TA, proximal third of the line connecting the lateral tibial condyle to the medial tubercle; PL, proximal quarter of the line connecting the fibular head to the external tubercle; PB, distal quarter of the line connecting the fibular head to the external tubercle; MG, site of maximum bulging at the medial gastrocnemius head when standing on tiptoes; and SL, site of maximum bulging at the medial head of the gastrocnemius muscle (distal third of the line connecting the medial epicondyle of the femur to the medial condyle of the femur) [14]. In the Y-balance test, the average muscle activity measured during 1 s of maximal reach was normalized using the maximum voluntary isometric contraction, and the average of three successful trials was recorded.
2.8. Statistical Analyses
IBM SPSS Statistics 26 (IBM Corp., Armonk, NY) was used for statistical analysis. The correlation between the basic information (age, height, weight, and body mass index [BMI]), muscle cross-sectional area, ankle isometric strength, toe grasp strength, plantar superficial sensation, muscle activity, and total reach distance in three directions of the dynamic balance test was investigated. The Shapiro–Wilk test was used to test for normality. Pearson’s correlation coefficient was used when a normal distribution was assumed for the correlations, and Spearman’s correlation coefficient was used when no normal distribution was assumed. The significance level was set at p<0.05.
3. Results
3.1. Participant Characteristics
Our participants were 24.5±5.4 years of age, 169.0±7.1 cm tall, 66.1±11.4 kg in weight, and had a BMI of 23±2.5 kg/m2 (Table 1); the recorded values of each measure are shown in Table 2 and Table 3. The dynamic balance test measurements of the maximum forward, backward-outward, and backward-inward reach distances normalized by leg length and their correlation with each physical characteristic are shown in Table 4.
3.2. Ankle Isometric Muscle Strength Measurements
There was a significant correlation between plantar flexor strength and the posterior medial reach distance (p<0.05), posterior lateral reach distance (r=0.588, p<0.05), and total reach distance in three directions (p<0.05).
3.3. Toe Grasp Strength
The anterior reach distance tended to be longer with increased toe grasp strength (p=0.057); the posterior medial reach distance increased with higher toe grasp strength (p<0.05); the posterior lateral reach distance increased with higher toe grasp strength (p<0.05); and the total reach distance in the three directions increased with higher toe grasp strength (p<0.05).
3.4. Plantar Superficial Sensation
The anterior reach distance increased with more dominant plantar superficial sensation of the third MTP joint (p<0.05). The posterior medial reach distance increased with plantar superficial sensation of the first and fifth MTP joints (both p<0.05). The posterolateral reach distance tended to increase with more dominant plantar surface sensation at the first and fifth MTP joints (p=0.051 and p=0.077, respectively). The total reach distance in the three directions was longer than the sensation in the first and fifth MTP joints (both p<0.05).
3.5. Muscle Activity
The reach distance in the posterolateral direction became shorter as the muscle activity of the abductor hallucis muscle increased (p<0.05). There was no significant correlation between the reach distance and muscle activity in the other directions.
4. Discussion
We examined the values of key physical indices, such as the foot muscle cross-sectional area, ankle isometric muscle strength, toe grasp strength, plantar superficial sensation, and muscle activity, and the dynamic balance test (Y-balance test) in lifesavers. The Y-balance test values of the lifesavers were related to toe grasp strength, ankle plantar flexion muscle strength, and plantar superficial sensation.
The Y-balance test values of the lifesavers differed from those of a previous study of 25 general participants of the same age group [15]. Dynamic postural control is stabilized by improving the gluteal, thigh, and trunk muscles [16], and the intrinsic foot muscles provide dynamic stability during the propulsive phase from plantar ground contact to toe-off [17]. Lifesavers have well-developed foot intrinsic muscles [5]. However, here, differences in the muscle cross-sectional area did not correlate with dynamic balance. In contrast, ankle plantar flexion and toe grasp strength significantly correlated with Y-balance test values in terms of muscle strength. In the backward-reaching distance movement, the ankle joint is dorsiflexed, the lower limb moves backward, and the center of gravity remains forward.
The center of gravity then shifts backward during the process, stabilized by supporting the weight shift with the plantar flexor muscle force and grasping the ground with the toe grasping force. Plantar flexor muscle strength is correlated with dynamic balance control [18], and similar results have been reported in lifesavers.
The involvement of toe grasp strength in balance function has also attracted attention, and this training has been used in rehabilitation. Menz et al. [19] and Yoshimoto et al. [20] examined the relationship between dynamic balance ability and toe flexor muscle strength in community-dwelling older people; a decline in dynamic balance ability was associated with a decline in toe flexor muscle strength. A study of university basketball players also reported that toe grasp strength improved with balance training [21], suggesting that toe grasp strength and plantar flexor muscle strength are important for dynamic balance function.
In terms of plantar superficial sensation, there was a significant correlation between the sensitivity of plantar superficial sensation at the first, third, and fifth MTP joints and Y-balance test value. While standing, only the plantar feet are in contact with the floor, and there are many sensory receptors for postural regulation in the plantar feet [22], with different distribution areas [23]. These plantar mechanoreceptors are the only mechanoreceptors that are in contact with the ground and receive sensory information related to ground reaction forces. This sensory information is important for spatial position perception and contributes significantly to balance function [24].
A good sense of touch under the first metatarsal head was found to correlate with somatosensory perception and dynamic balance function in different parts of the plantar surface [25], with cutaneous sensation and muscle strength being related to static and dynamic balance [18]. We also showed that poor sensation of the plantar surface causes a decrease in balance function and that the plantar surface sensation on the inside and outside of the plantar surface is involved in postural sway due to the appearance of internal and external postural sway in the Y-balance test.
The loss of sensory input from the plantar surface also affects foot muscular activity [26]. Overall, lifesavers tended to have a lower plantar superficial sensation. During sand training, barefoot athletes compete in hot, sandy conditions, and the plantar skin is continuously stimulated, causing it to thicken in response to the environment. As plantar mechanoreceptors are located in the dermis layer of the skin, when the skin thickens, the stratum corneum of the epidermis also thickens, which may reduce the superficial plantar sensation, resulting in reduced balance function due to reduced plantar superficial sensation; however, lifesavers may be able to maintain high balance function using toe grasp strength and periarticular muscular strength while maintaining balance.
On electromyography, the maximum reach distance in the posterolateral direction decreased as the activity of the abductor pollicis brevis muscle increased. Muscle activity during the Y-balance test in participants with tendinogenesis was the highest in the posterior and lateral directions of the TA muscle, followed by that of the PB tendon. Conversely, the activity was low in the anterior and medial directions [27]. In our lifesavers, a negative correlation was found between an increase in the muscle activity of the abductor pollicis brevis at maximum reach and a decrease in the maximum reach distance, suggesting that the abductor pollicis brevis muscle was active when there was postural sway at plantar ground contact during maximal reach, as per a previous study [28]. Lifesavers develop intrinsic foot muscles during sand training, use toe grasp and ankle plantar flexor muscle strength to stabilize the plantar ground surface, and show higher Y-balance test scores than those in the same age group, suggesting that prolonged sand training may cause a loss of plantar surface sensation associated with thickening of the plantar skin. This is useful to improve foot muscle strength and dynamic balance function.
The limitation of this study is that no comparison with healthy participants was made. The direct causal relationship between lifesaving activities and improvement in balance function is unclear because the study was only conducted at a single time point, and the evaluation of intrinsic sensation and toe grasp strength was not sufficiently divided into intrinsic and extrinsic muscles. Therefore, additional studies are warranted in the future.
5. Conclusions
We examined the relationship between physical characteristics of lifesavers and their dynamic balance function to investigate the effects of a competitive environment on foot function in sandy terrain. Toe grasp strength and ankle plantar flexor muscle strength are particularly important for dynamic balance in elite lifesavers operating in sand. Sand training improves intrinsic muscle training and dynamic balance function; however, the training intensity may cause a decrease in plantar superficial sensation, which needs to be verified with training interventions in the future.
Funding
This research was funded by JSPS KAKENHI grant number JP22K21251.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Waseda University (protocol code 2020-227 and date of approval).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to thank all the co-authors for their cooperation in writing this paper and all the elite lifesavers who participated in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Booth, D. Surf lifesaving: the development of an Australasian "sport". Int J Hist Sport 2000, 17, 167–187. [Google Scholar] [CrossRef]
- Binnie, M.J.; Dawson, B.; Arnot, M.A.; Pinnington, H.; Landers, G.; Peeling, P. Effect of sand versus grass training surfaces during an 8-week pre-season conditioning programme in team sport athletes. J Sports Sci 2014, 32, 1001–1012. [Google Scholar] [CrossRef] [PubMed]
- Binnie, M.J.; Dawson, B.; Pinnington, H.; Landers, G.; Peeling, P. Sand training: a review of current research and practical applications. J Sports Sci 2014, 32, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Pinnington, H.C.; Lloyd, D.G.; Besier, T.F.; Dawson, B. Kinematic and electromyography analysis of submaximal differences running on a firm surface compared with soft, dry sand. Eur J Appl Physiol 2005, 94, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, S.; Kumai, T.; Okunuki, T.; Maemichi, T.; Matsumoto, M.; Yabiku, H.; Liu, Z.; Yamaguchi, R.; Iwayama, A.; Ayukawa, G.; et al. Comparison of foot posture and foot muscle morphology between lifesaver athletes and healthy adults. Res Sports Med 2023, 31, 506–516. [Google Scholar] [CrossRef]
- Giatsis, G.; Panoutsakopoulos, V.; Kollias, I.A. Biomechanical differences of arm swing countermovement jumps on sand and rigid surface performed by elite beach volleyball players. J Sports Sci 2018, 36, 997–1008. [Google Scholar] [CrossRef] [PubMed]
- Hrysomallis, C. Balance ability and athletic performance. Sports Med 2011, 41, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Smith, R. Movement in the sand: training implications for beach volleyball. Strength and Conditioning Journal 2006, 28, 19–21. [Google Scholar] [CrossRef]
- Matsumoto, M.; Maemichi, T.; Wada, M.; Niwa, Y.; Inagaki, S.; Okunuki, T.; Ichikawa, S.; Kumai, T. Ultrasonic evaluation of the heel fat pad under weight-bearing conditions using a polymethylpentene resin plate: part 1. Ultrasound Med Biol 2022, 48, 358–372. [Google Scholar] [CrossRef]
- Matsumoto, M.; Maemichi, T.; Wada, M.; Niwa, Y.; Inagaki, S.; Taguchi, A.; Okunuki, T.; Tanaka, H.; Kumai, T. Ultrasonic evaluation of the heel fat pad under loading conditions using a polymethylpentene resin plate: part 2. reliability and agreement study. Ultrasound Med Biol 2023, 49, 460–472. [Google Scholar] [CrossRef]
- Chamorro, C.; Armijo-Olivo, S.; De la Fuente, C.; Fuentes, J.; Javier Chirosa, L. Absolute reliability and concurrent validity of hand held dynamometry and isokinetic dynamometry in the hip, knee and ankle joint: systematic review and meta-analysis. Open Med (Wars) 2017, 12, 359–375. [Google Scholar] [CrossRef]
- Bell-Krotoski, J.A.; Buford, W.L. The force/time relationship of clinically used sensory testing instruments. J Hand Ther 1997, 10, 297–309. [Google Scholar] [CrossRef]
- Powden, C.J.; Dodds, T.K.; Gabriel, E.H. The reliability of the star excursion balance test and lower quarter y-balance test in healthy adults: a systematic review. Int J Sports Phys Ther 2019, 14, 683–694. [Google Scholar] [CrossRef] [PubMed]
- SENIAM project. Recommendations for sensor locations on individual muscles. Available online: http://www.seniam.org/ (accessed on 10 June 2024).
- Herrington, L.; Hatcher, J.; Hatcher, A.; McNicholas, M. A comparison of Star Excursion Balance Test reach distances between ACL deficient patients and asymptomatic controls. Knee 2009, 16, 149–152. [Google Scholar] [CrossRef]
- Olmsted, L.C.; Carcia, C.R.; Hertel, J.; Shultz, S.J. Efficacy of the star excursion balance tests in detecting reach deficits in subjects with chronic ankle instability. J Athl Train 2002, 37, 501–506. [Google Scholar]
- Özkal, Ö.; Kara, M.; Topuz, S.; Kaymak, B.; Bakı, A.; Özçakar, L. Assessment of core and lower limb muscles for static/dynamic balance in the older people: An ultrasonographic study. Age Ageing 2019, 48, 881–887. [Google Scholar] [CrossRef]
- Song, Q.; Zhang, X.; Mao, M.; Sun, W.; Zhang, C.; Chen, Y.; Li, L. Relationship of proprioception, cutaneous sensitivity, and muscle strength with the balance control among older adults. J Sport Health Sci 2021, 10, 585–593. [Google Scholar] [CrossRef]
- Menz, H.B.; Morris, M.E.; Lord, S.R. Foot and ankle characteristics associated with impaired balance and functional ability in older people. J Gerontol A Biol Sci Med Sci 2005, 60, 1546–1552. [Google Scholar] [CrossRef]
- Yoshimoto, Y.; Oyama, Y.; Tanaka, M.; Sakamoto, A. Toe functions have little effect on dynamic balance ability in elderly people. J Phys Ther Sci 2017, 29, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Kamikura, S.; Sakuraba, K.; Miura, T. Effects of reach balance exercise on toe grip strength and balance in college basketball players. Prog Rehabil Med 2018, 3, 20180008. [Google Scholar] [CrossRef]
- Inglis, J.T.; Kennedy, P.M.; Wells, C.; Chua, R. The role of cutaneous receptors in the foot. Adv Exp Med Biol 2002, 508, 111–117. [Google Scholar] [PubMed]
- Fitzpatrick, R.; McCloskey, D.I. Proprioceptive, visual and vestibular thresholds for the perception of sway during standing in humans. J Physiol 1994, 478 Pt 1, 173–186. [Google Scholar] [CrossRef]
- Kavounoudias, A.; Roll, R.; Roll, J.P. The plantar sole is a 'dynamometric map' for human balance control. Neuroreport 1998, 9, 3247–3252. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Almeida, Y.; Black, M.L.; Christou, E.A.; Clark, D.J. Site-specific differences in the association between plantar tactile perception and mobility function in older adults. Front Aging Neurosci 2014, 6, 68. [Google Scholar] [CrossRef] [PubMed]
- Felicetti, G.; Thoumie, P.; Do, M.C.; Schieppati, M. Cutaneous and muscular afferents from the foot and sensory fusion processing: Physiology and pathology in neuropathies. J Peripher Nerv Syst 2021, 26, 17–34. [Google Scholar] [CrossRef] [PubMed]
- Karagiannakis, D.N.; Iatridou, K.I.; Mandalidis, D.G. Ankle muscles activation and postural stability with Star Excursion Balance Test in healthy individuals. Hum Mov Sci 2020, 69, 102563. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J.; Bramble, D.; Davis, I. The foot core system: a new paradigm for understanding intrinsic foot muscle function. Br J Sports Med 2015, 49, 290. [Google Scholar] [CrossRef]
Figure 1.
Toe grip strength measurement. (a) and (b) show photographs of the legs in which the activity of the leg muscles is dominant. To measure the muscles of the foot, the participants were instructed to bend their toes toward the heel as much as possible while pressing strongly against the ground.
Figure 1.
Toe grip strength measurement. (a) and (b) show photographs of the legs in which the activity of the leg muscles is dominant. To measure the muscles of the foot, the participants were instructed to bend their toes toward the heel as much as possible while pressing strongly against the ground.

Figure 2.
Measurement points for plantar surface perception.
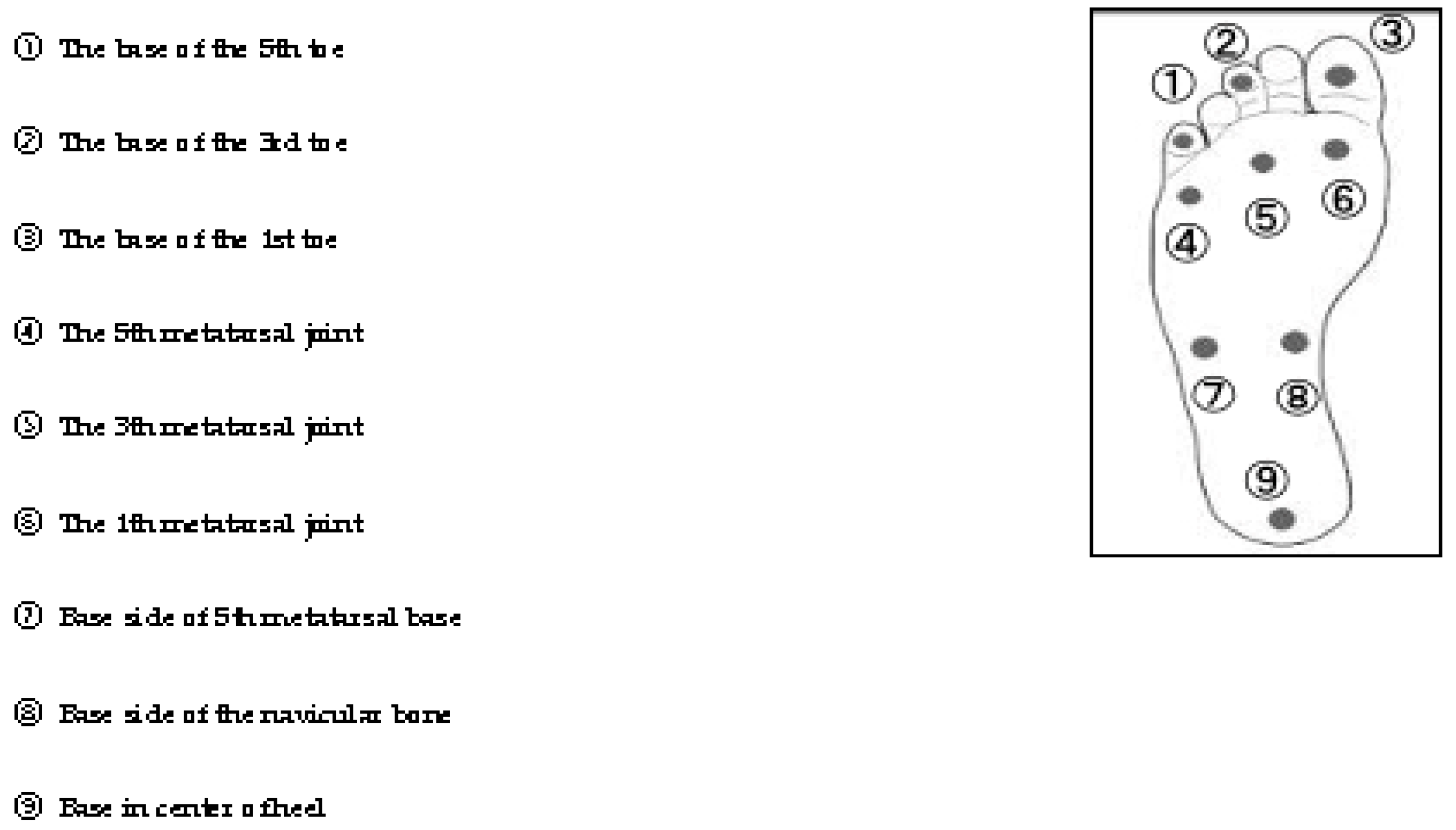

Table 1.
Participant characteristics.
| Lifesavers | |
| (N=15; 12 males 3 females) | |
| Variable | Mean (SD) |
| Age (years) | 24.5 (5.4) |
| Height (cm) | 169 (7.1) |
| Weight (kg) | 66.1 (11.4) |
| BMI (kg/m2) | 23 (2.5) |
BMI, body mass index; SD, standard deviation.
Table 2.
Descriptive data for the performance indicators.
| Peformance Indicators | Mean±Standard Deviation (N=15) | ||
|---|---|---|---|
| muscle strength (N/Kg) | Dorsiflexion | 3.88 | 1.15 |
| planter flexion | 2.45 | 0.56 | |
| Eversion | 2.31 | 0.61 | |
| toe grasp strength | %BW | 47.4 | 14.4 |
| cross section area(muscles) | Abductor hallucis(ABH) | 3.16 | 0.65 |
| Adductor digiti minimi (ADD) | 1.58 | 0.44 | |
| Flexor digitorum brevis( FDB) | 2.61 | 0.7 | |
| Flexor hallucis brevis( FHB) | 2.52 | 0.7 | |
| Tibialis anterior (TA) | 6.88 | 1.3 | |
| Peroneal longus and brevis(PL) | 4.94 | 1.14 | |
| Posterior tibialis (PT) | 5.32 | 1.03 | |
| Extensor digitorum longus (EDL) | 3.72 | 0.89 | |
| Flexor hallucis longus (FHL) | 2.75 | 0.9 | |
| Flexor digitorum longus (FDL) | 2.83 | 0.64 | |
| plantar superficial sensation | ①The base of the 5th toe | 3.42 | 0.66 |
| ②The base of the 3rd toe | 3.44 | 0.59 | |
| ③The base of the 1st toe | 3.64 | 0.56 | |
| ④The 5th metatarsal joint | 3.71 | 0.36 | |
| ⑤The 3th metatarsal joint | 3.65 | 0.44 | |
| ⑥The 1th metatarsal joint | 3.58 | 0.47 | |
| ⑦Base side of 5th metatarsal base | 3.70 | 0.52 | |
| ⑧Base side of the navicular bone | 3.42 | 0.50 | |
| ⑨Base in center of heel | 4.17 | 0.66 | |
| Y balance test | Reach distance(anterior) | 65.3 | 4.2 |
| Reach distance(posteromedial) | 112.4 | 6.5 | |
| Reach distance(posterolateral) | 110.4 | 6.3 | |
| Composite | 96.0 | 4.9 | |
Table 3.
Electromyography data during Y-balance test.
| Mean±Standard Deviation (N=15) | |||
|---|---|---|---|
| Y balance test | Reach distanc(anterior) | 65.3 | 4.2 |
| Electromyography | ABH | 50.2 | 20.3 |
| ADD | 33.8 | 39.6 | |
| TA | 40.7 | 16.9 | |
| PL | 38.4 | 18.4 | |
| PB | 32.0 | 12.0 | |
| GM | 11.6 | 8.3 | |
| SOL | 52.8 | 33.5 | |
| Reach distance (posteromedial) |
112.4 | 6.5 | |
| ABH | 45.4 | 20.9 | |
| ADD | 26.1 | 25.3 | |
| TA | 45.3 | 15.0 | |
| PL | 41.3 | 16.2 | |
| PB | 33.3 | 10.9 | |
| GM | 9.9 | 7.6 | |
| SOL | 47.8 | 36.0 | |
| Reach distance (posterolateral) |
110.4 | 6.3 | |
| ABH | 31.8 | 13.3 | |
| ADD | 29.8 | 21.1 | |
| TA | 46.9 | 11.0 | |
| PL | 36.6 | 15.3 | |
| PB | 28.4 | 10.0 | |
| GM | 9.8 | 8.2 | |
| SOL | 52.8 | 32.6 | |
ABH, abductor hallucis; ADD, adductor digiti minimi; FDB, flexor digitorum brevis; FHB, flexor hallucis brevis; TA, tibialis anterior; PL, peroneal longus and brevis; PT, posterior tibialis; EDL, extensor digitorum longus; FHL, flexor hallucis longus; FDL, flexor digitorum longus.
Table 4.
Correlations of lifesaver's physical functions with reach distance of the Y balance test (n = 15).
Table 4.
Correlations of lifesaver's physical functions with reach distance of the Y balance test (n = 15).
| Y balance test | Reach distance | anterior | posteromedial | posterolateral | Composite | ||||
|---|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | ||
| cross section area(muscles) | Abductor hallucis(ABH) | -0.085 | 0.762 | 0.246 | 0.377 | 0.206 | 0.461 | 0.174 | 0.535 |
| Adductor digiti minimi (ADD) | -0.006 | 0.983 | 0.311 | 0.259 | 0.148 | 0.599 | 0.201 | 0.474 | |
| Flexor digitorum brevis( FDB) | 0.140 | 0.618 | -0.006 | 0.984 | -0.006 | 0.983 | 0.035 | 0.902 | |
| Flexor hallucis brevis( FHB) | 0.184 | 0.512 | -0.033 | 0.907 | -0.163 | 0.563 | -0.032 | 0.909 | |
| Tibialis anterior (TA) | 0.064 | 0.821 | -0.243 | 0.384 | -0.302 | 0.274 | -0.22 | 0.432 | |
| Peroneal longus and brevis(PL) | 0.068 | 0.81 | -0.139 | 0.621 | -0.359 | 0.188 | -0.197 | 0.481 | |
| Posterior tibialis (PT) | -0.032 | 0.908 | -0.251 | 0.366 | -0.351 | 0.2 | -0.272 | 0.327 | |
| Extensor digitorum longus (EDL) | 0.089 | 0.752 | -0.322 | 0.242 | -0.455 | 0.089 | -0.313 | 0.255 | |
| Flexor hallucis longus (FHL) | 0.06 | 0.831 | 0.244 | 0.382 | 0.133 | 0.636 | 0.183 | 0.514 | |
| Flexor digitorum longus (FDL) | 0.069 | 0.806 | -0.021 | 0.94 | -0.007 | 0.979 | 0.007 | 0.98 | |
| muscle strength | Dorsiflexion | 0.438 | 0.103 | 0.428 | 0.112 | 0.443 | 0.098 | 0.505 | 0.055 |
| planter flexion | 0.276 | 0.319 | 0.572* | 0.026 | 0.695* | 0.004 | 0.632* | 0.012 | |
| Eversion | -0.051 | 0.857 | 0.097 | 0.731 | -0.038 | 0.892 | 0.012 | 0.965 | |
| toe grasp strength | %BW | 0.501 | 0.057 | 0.579* | 0.024 | 0.588* | 0.021 | 0.652* | 0.008 |
| plantar superficial sensation | ①The base of the 5th toe | 0.083 | 0.769 | -0.16 | 0.569 | -0.193 | 0.49 | -0.131 | 0.642 |
| ②The base of the 3rd toe | -0.036 | 0.9 | -0.108 | 0.702 | -0.162 | 0.564 | -0.128 | 0.65 | |
| ③The base of the 1st toe | -0.164 | 0.56 | -0.375 | 0.168 | -0.331 | 0.228 | -0.356 | 0.193 | |
| ④The 5th metatarsal joint | -0.474 | 0.075 | -0.607* | 0.016 | -0.47 | 0.077 | -0.607* | 0.016 | |
| ⑤The 3th metatarsal joint | -0.522* | 0.046 | -0.431 | 0.109 | -0.262 | 0.346 | -0.452 | 0.091 | |
| ⑥The 1th metatarsal joint | -0.409 | 0.131 | -0.552* | 0.033 | -0.511 | 0.051 | -0.581* | 0.023 | |
| ⑦Base side of 5th metatarsal base | -0.265 | 0.341 | -0.219 | 0.433 | -0.186 | 0.508 | -0.252 | 0.365 | |
| ⑧Base side of the navicular bone | -0.18 | 0.521 | -0.277 | 0.317 | -0.285 | 0.303 | -0.297 | 0.282 | |
| ⑨Base in center of heel | -0.297 | 0.282 | -0.495 | 0.061 | -0.449 | 0.093 | -0.498 | 0.059 | |
| Electromyography | Abductor hallucis(ABH) | 0.07 | 0.805 | -0.224 | 0.422 | -0.515* | 0.05 | ||
| Adductor digiti minimi (ADD) | 0.150 | 0.593 | -0.145 | 0.607 | -0.041 | 0.884 | |||
| Tibialis anterior (TA) | 0.143 | 0.611 | 0.257 | 0.355 | 0.253 | 0.363 | |||
| Peroneal longus(PL) | -0.233 | 0.404 | 0.075 | 0.791 | -0.065 | 0.817 | |||
| Peroneal brevis(PB) | -0.214 | 0.444 | 0.117 | 0.678 | 0.127 | 0.652 | |||
| Medial Gastrocnemius(MG) | 0.075 | 0.79 | 0.47 | 0.077 | 0.195 | 0.487 | |||
| Soleus (SOL) | 0.046 | 0.869 | -0.116 | 0.681 | -0.195 | 0.487 | |||
* The p-value was significant at the 0.05 level.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



