
Submitted:
25 June 2024
Posted:
26 June 2024
You are already at the latest version
Abstract
Combined hepatocellular cholangiocarcinoma (cHCC-ICC) is a rare malignancy that involves a combination of features of hepatocellular carcinoma and intrahepatic cholangiocarcinoma (ICC). cHCC-ICC is generally considered to exhibit a more aggressive clinical course compared to ICC; however, its risk factors and outcomes remain largely undefined. A single-center retrospective study of 82 patients diagnosed with ICC or cHCC-ICC from June 2011 and January 2023, all of whom underwent surgical resection. Our analysis included 70 patients with resected ICC and 12 with resected cHCC-ICC. The overall survival (OS) for the entire cohort was 21.6 months, with a recurrence-free survival (RFS) of 11.8 months. The cHCC-ICC group had significantly higher levels of AST and ALT (AST median 206 vs. 46; ALT median 165.5 vs. 48; p=0.012 and p=0.013, respectively), whereas the ICC group had higher alkaline phosphatase (median 66 vs. 104; p=0.03). CA 19-9 values (p=0.02) were higher in the ICC group, while AFP values were higher in the cHCC-ICC group (p=0.0004). The cHCC-ICC group had a significantly higher rate of recurrence (83% vs. 47%, p=0.028) with a significantly decreased RFS (4.7 months vs. 12.4 months; log-rank p=0.007). cHCC-ICC is a rare entity that needs to be further studied to improve patient outcomes. Our study showed that RFS is lower in the cHCC-ICC group as compared to ICC patients alone. Further studies are warranted and possibly suggest the need for more aggressive initial treatment strategies in patients diagnosed with cHCC-ICC.
Keywords:
Combined Hepatocellular Cholangiocarcinoma (cHCC-ICC)
; Intrahepatic Cholangiocarcinoma (ICC)
; Surgical Resection
; Recurrence-Free Survival
; Overall Survival
1. Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer, accounting for around 70% of all cases, followed by intrahepatic cholangiocarcinoma (ICC), which accounts for 15% [1,2]. Combined hepatocellular cholangiocarcinoma (cHCC-ICC) is an extremely rare subtype of a primary liver malignancy, which involves a combination of features of HCC and ICC and accounts for 2-3% of liver malignancies [3].
Compared to other malignancies, cHCC-ICC is generally considered to exhibit a more aggressive tumor behavior and usually has a poor prognosis.[4,5] The risk factors and characteristics of a typical patient diagnosed with cHCC-ICC are still largely unknown. One study suggested that the risk factors are highly influenced by geography [6]. This is plausible, considering the well documented variation in HCC incidence across the different regions of the world, particularly between the East and the West, likely due to the differences in the prevalence of viral hepatitis [7]. Several studies from East Asia have identified potential risk factors for cHCC-ICC, including heavy alcohol use, hepatitis B infection, male sex, cirrhosis, and diabetes mellitus [8,9].
Clinical diagnosis of cHCC-ICC without a biopsy can be extremely challenging. Several studies have looked retrospectively at tumor markers, including alpha-fetoprotein (AFP), carcinoembryonic antigen (CEA), cancer antigen 19-9 (CA 19-9), as well as imaging and failed to find any unique characteristic features for cHCC-ICC patients [10,11,12]. One retrospective study that was done in the Thai population found in a multivariate analysis that elevated CA 19-9 and intrahepatic bile duct dilation were prognostic for poor survival in cHCC-ICC patients [13]. Additionally, the presentation of cHCC-ICC is similar to that of HCC and ICC. The majority of patients present with generalized symptoms, including fatigue, abdominal pain, jaundice, and weight loss [14]. Patients who present at a more advanced stage may present with more severe symptoms including ascites, hepatomegaly, or acute cholangitis.[5]
Treatment modalities for cHCC-ICC depend on the stage of the disease. Several staging criteria originally designed for HCC and ICC, such as the Barcelona Clinic Liver Cancer (BCLC) system and the TNM classification, can be utilized to assess the stage of cHCC-ICC.[15,16] The only curative treatment for patients diagnosed with cHCC-ICC is surgical resection [6]. The role of a liver transplant or other systemic therapies continues to be highly debated in this patient population [17,18]. In fact, one study showed that those who underwent a liver transplant for cHCC-ICC had significantly worse survival compared to transplant patients with HCC.[19] One study looking at surgical outcomes in cHCC-ICC demonstrated that a resection margin of 1 cm or above showed better survival [20]. Additionally, another study showed that more aggressive surgical approaches were associated with better survival outcomes [21]. Given the rarity of the disease, the molecular understanding of cHCC-ICC is lacking, which contributes to the scarcity of treatment options [22,23]. Currently, various systemic therapies, such as chemotherapy, targeted therapy, and immunotherapy, are being explored [24]. Despite the perception that cHCC-ICC is typically associated with worse survival given the aggressive nature of the disease, several studies have shown similar or even better survival of cHCC-ICC compared to that of ICC [12,25,26,27,28].
The aim of this study is to compare the clinical characteristics and survival outcomes of patients diagnosed with ICC and cHCC-ICC who have undergone surgical resection in our institution. Our study did not include HCC as it falls outside the scope of our study.
2. Materials and Methods
2.1. Study Population
This was a single-center retrospective study of patients who were either diagnosed with ICC or cHCC-ICC between June 2011 and January 2023 at our university. The ICD diagnosis codes used to retrieve data include C22.0, C22.1, C24.0, C23, C24.9. During this period, there were initially 361 patients diagnosed with cholangiocarcinoma. Patients who were diagnosed with extrahepatic cholangiocarcinoma or gallbladder cancer were excluded. Additionally, patients who did not undergo resection were excluded. Eighty-two patients were included in the final analysis as seen in Figure 1. The study was approved by the University of Florida Institutional Review Board (IRB202300417) and conducted in a manner consistent with the principles in the Declaration of Helsinki.
2.2. Study Variables
This study focused on the clinical outcomes and survival characteristics of patients with cHCC-ICC compared to their counterparts with intrahepatic cholangiocarcinoma (ICC). This study evaluated various demographic variables, including age, race (White, Black, or Asian), ethnicity (Hispanic, non-Hispanic), and gender (male, female). Additionally, information regarding the patient’s medical history (prior other cancer, history of cirrhosis), laboratory values at diagnosis (AST, ALT, alkaline phosphatase, total bilirubin, CA 19-9, CEA, AFP, neutrophil/lymphocyte ratio) were obtained. Surgical and pathology data were obtained for all patients, including TNM staging, largest tumor size diameter after resection, presence of lymphovascular and perineural invasion, and type of resection done. Recurrence rate and recurrence location were also obtained.
2.3. Statistical Analysis
Descriptive statistics were used to create a table to summarize the baseline demographics. Survival data was calculated based on the date of diagnosis until the most recent follow-up date or death from any cause. Mann-Whitney U, Log-rank, Kruskal–Wallis, and Fisher’s tests were used where appropriate. A p-value of <0.05 was considered statistically significant. Statistical analyses were performed using GraphPad Prism Software, version 10.1.1.
3. Results
3.1. Baseline Characteristics
We identified 82 patients with either resected ICC or cHCC-ICC who were included in our analysis. Baseline patient characteristics are listed in Table 1. The median age at diagnosis was 64, with 52% of patients being male and 48% being female. The majority of patients (94%) were White. Sixteen percent of the patients had a prior diagnosis of another type of malignancy, while 9% had a history of cirrhosis prior to diagnosis. There was a significantly higher number of resected cHCC-ICC who had a history of cirrhosis compared to the resected ICC group (33% vs. 4%; p=0.008).
3.2. Disease Characteristics and Tumor Markers
Baseline tumor characteristics are included in Table 1 as well. The median AST, ALT, and alkaline phosphatase were 62 U/L, 57 U/L, and 87 U/L, respectively. The median total bilirubin was 0.8 mg/dL. The cHCC-ICC groups had significantly higher transaminase levels at the time of diagnosis (AST: 206 vs. 46, p=0.012; ALT: 165.5 vs. 48, p=0.013). On the contrary, alkaline phosphatase was significantly higher in the resected ICC group (104 vs. 66, p=0.03). For the entire cohort, the median CA 19-9, CEA, and AFP were 64.5, 2.4, and 3.8, respectively. In terms of the tumor markers, the resected ICC group had significantly higher CA 19-9 (76 vs. 22, p=0.02), while the cHCC-ICC group had significantly higher AFP levels (7.3 vs. 3.2, p=0.0004).
3.3. Surgical Procedural and Histological Data
An overview of surgical interventions is detailed in Table 1 and Figure 1, while histological outcomes after surgical resection can be found in Table 2. Overall, 10% of patients underwent extended resections, 71% underwent major resections, and 17% underwent minor resections. In the ICC group, 2 patients had liver transplants. The proportions of extended, major, and minor resections were not significantly different between the ICC and cHCC-ICC groups (p=0.173). The median largest resected tumor dimension was 4.8 cm in the ICC group and 5.5 cm in the cHCC-ICC patients. In terms of resection status, most patients in both groups underwent R0 resections with negative margins (86% in ICC and 83% in cHCC-ICC). Six patients in the ICC group had R1 resection status, and four patients had R2 status. In the cHCC-ICC group, two of the twelve patients had R1 resection status. The two groups showed a similar proportion (nearly half) of tumors with lymphovascular invasion. There was a significantly higher percentage of patients in the ICC group with perineural invasion (56% vs. 8%, p=0.007). Details for TNM staging are seen in Table 2.
3.4. Neoadjuvant and Adjuvant Treatment
The majority of patients in the ICC group received surgery alone (60%), while 33% of patients received adjuvant chemotherapy. There were 5 patients (7%) who received neoadjuvant chemotherapy. Similarly, in the cHCC-ICC cohort, the majority of patients had surgery alone (58%), while 33% had adjuvant chemotherapy. None of the cHCC-ICC patients received neoadjuvant treatment.
3.5. Tumor Recurrence
Among all patients, slightly more than half had tumor recurrence (recurrence rate of 52%). The details of the rate of recurrence, as well as the location of the recurrence, can be seen in Table 3. There was a significantly higher rate of recurrence in the cHCC-ICC group (83% vs. 47%, p=0.028), however patterns of recurrence did not seem to differ. In the resected ICC group, 64% had intrahepatic recurrence, 21% had extrahepatic recurrence, and 15% had both intrahepatic and extrahepatic recurrence. Similarly, in the resected cHCC-ICC group, 60% had intrahepatic recurrence, 20% had extrahepatic recurrence, and 20% had both intrahepatic and extrahepatic recurrence.
In the 33 resected ICC patients who experienced recurrence, 12 (36%) of patients did not undergo further treatment. 21% of patients had chemotherapy alone, and 21% had radiation alone. The remaining 22% of patients either had a combination of chemotherapy, radiation, and immunotherapy or enrolled in a clinical trial. In the resected cHCC-ICC group, 3 (30%) patients did not undergo further treatment, while 30% of patients had chemotherapy alone and 30% had radiation alone. There was 1 patient (10%) who received both chemotherapy and radiation.
3.6. Recurrence-Free Survival
The recurrence-free survival (RFS) was significantly decreased among patients diagnosed with cHCC-ICC (log-rank p=0.007), consistent with the previously stated higher rate of recurrence in this cohort; the RFS curves can be seen in Figure 2. Patients with ICC had a median RFS of 12.4 months (range 0.2-148.4 months), while patients with cHCC-ICC had a median RFS of 4.7 months (range 0.4-126.3). Although the cHCC-ICC group had a higher percentage of cirrhotic patients compared to the ICC group (33% vs. 4%), this did not seem to affect the finding that RFS was still significantly lower in non-cirrhotic patients (p=0.008).
We then further stratified RFS by resection type. In patients with ICC, the median RFS in months was 19.8, 12.2, and 12.3 for extended, major, and minor resections, respectively (p=0.763). In patients with cHCC-ICC, the median RFS was 3.7, 2, and 31.3 months for extended, major, and minor resections, respectively (p=0.053).
3.7. Overall Survival and Mortality Rates
OS did not differ between resected ICC and cHCC-ICC as seen in Figure 3. The overall survival (OS) of the entire group was 21.6 months (IQR 8.5-42.7 months). Patients diagnosed with ICC had a median OS of 21 months (range 0.2-147.8) while patients with cHCC-ICC had a median OS of 22.3 months (range 0.4-134). The respective 1-,3-,5-year mortality rates for ICC patients were 23%, 51%, and 57%. For cHCC-ICC, the 1-,3-,5-year mortality rates were 28%, 61%, and 61%, respectively.
As we had done for RFS, we stratified OS in the two separate groups by resection type. In the ICC group, the median OS was 22.8, 20.7, 19 months for extended, major, and minor resections, respectively (p=0.828). For the cHCC-ICC, the median OS in months was 16.5, 7.8, 49.3 for extended, major, and minor resections, respectively (p=0.053).
4. Discussion
In this single-center retrospective study of 82 patients with either resected cHCC-ICC or ICC, we found significantly decreased RFS among patients with resected cHCC-ICC. This study contributes insight to the limited literature and studies currently published. Among the 82 resected patients, 70 patients were diagnosed with intrahepatic cholangiocarcinoma while 12 patients were diagnosed with combined hepatocellular cholangiocarcinoma.
To the best of our knowledge, this study is among the first to report worse recurrence-free survival in patients with resected cHCC-ICC. A Korean study evaluated the prognosis of cHCC-CC in comparison to ICC in patients who underwent curative resection. For the cHCC-ICC group, the median time to recurrence (TTR) and OS were 5.4 and 18.0 months, respectively [29]. After adjusting for confounding factors, the cHCC-CC group had a shorter TTR compared to the ICC group (RR, 2.00; P=0.013). Similar to our study, the results of their study indicated that cHCC-CC is associated with a significantly poorer prognosis than ICC after curative resection.
In a study by Penzkofer et al., they explored surgical outcomes in resected ICC and cHCC-ICC patients in Germany [25]. The study looked at a total of 202 ICC patients and 14 cHCC-ICC patients. Although the median RFS in patients with ICC appears to be shorter than in those with cHCC-ICC — 7.3 months versus 16 months, respectively — the difference was not statistically significant (p=0.479) [25]. In another Korean study, Lee et al. evaluated 79 resected ICC and 33 cHCC-ICC patients. In the study, unlike our results, they found worse clinical outcomes for patients with resected ICC compared to those with cHCC-ICC; the median disease-free survival after hepatic resection was 15.5 months for ICC patients versus 23.4 months for cHCC-ICC patients (P < 0.0001). In their study, portal vein invasion was found to be the only single significant predictor of poor outcome after hepatic resection of cHCC-ICC patients [30]. In our study, there was a trend toward a higher incidence of portal vein invasion in the cHCC-ICC group compared to the ICC group (42% vs. 16%, p=0.051), which could partially explain the poorer clinical outcomes observed in the cHCC-ICC group.
Our study yielded results that differ from those reported in studies from Germany and Korea. This variation could potentially be partially due to geographic and racial differences, which may play roles in the disease’s manifestation and the resulting patient outcomes. The percentages of cirrhosis in the cHCC-ICC patients in our study, Penzkofer et al., and Lee et al. were 33%, 29%, and 48.5%, respectively. Additionally, our study had a significantly higher cHCC-ICC group with history of hepatitis C, while the other studies primarily had history of Hepatitis B due to the higher prevalence in Asia where those studies were conducted which could be another source of explanation. Having different outcomes underscores the need for further research to elucidate the full spectrum of factors influencing these prognostic variations. However, given the rarity of the cHCC-ICC, it is a limiting factor to conduct larger studies.
In our cohort, patients with resected ICC had similar overall survival to that of resected cHCC-ICC. Leoni et al. recently published a comprehensive review of previous retrospective studies looking at OS for resected cHCC-ICC patients showing a wide range of OS from 16.5 to 52.5 months [24]. In the study by Penzkofer et. al., they found that there was also no significant OS difference between the cHCC-ICC and ICC groups. However, interestingly, it was found that the median OS was 17.6 months in the ICC group, while the median OS in the cHCC-ICC group was 26 months [25]. This was contrasted in our study, where we found that the median OS was numerically higher in the cHCC-ICC group at 22.3 months compared to 21 months in the ICC group, which was not statistically significant. Several previous studies also found that there was no significant difference in OS between resected cHCC-ICC and ICC [29,30]. Similarly, a study by Yoon et al., which compared 53 cHCC-ICC patients and 149 ICC patients did not find a significant difference in overall survival (8 vs. 6 months for cHCC-ICC and ICC, respectively) [31]. Contrary to those studies that found no difference in OS, a SEER based study by Yang et. al., found that the OS for the cHCC-ICC group was significantly better than the ICC group. One speculation that the study had to explain these findings is that the cHCC-ICC patients were diagnosed at an earlier stage [28]. The discrepancy in OS among these studies is likely explained by various factors, but one aspect is that many of the studies included patients who also underwent liver transplantation.
The utilization of tumor markers in cHCC-ICC has been debated and several studies in the past have shown mixed conclusions. For example, one study suggested that the simultaneous elevation of both CA 19-9 and AFP may predict poorer outcomes [32]. Other studies have discussed the possible utility of tumor markers to aid in the differentiation of HCC and cHCC-ICC if both CA 19-9 and AFP are in concordance with imaging findings [5,33]. Although our study did not include HCC patients, we interestingly found significantly higher CA 19-9 values in the ICC group compared to the cHCC-ICC group, while AFP was significantly higher in the cHCC-ICC group. Given the rare occurrence of this disease, there are no well-defined guidelines on the management of these patients. Surgery continues to be the mainstay treatment in patients with resectable disease. However, in patients who are unresectable, the treatment options remain challenging with poor outcomes. There have been several studies looking at HCC and ICC separately; however, there is limited data on therapeutic long-term outcomes in those with cHCC-ICC [24].
Recurrence rates remain a challenge in this patient population. In our study, we found a significantly higher rate of recurrence in patients diagnosed with cHCC-ICC (83% vs. 47%). However, there have been mixed findings in previous studies [34,35]. Similar to previous studies, intrahepatic recurrence is most frequently seen in both of our cohorts. In the resected ICC group, recurrence rates have been reported to range from 61-73% in prior studies, which is slightly higher than our findings of 47% [36,37,38,39]. The slight difference in this could be accounted for as some patients may have been lost to follow-up. For cHCC-ICC, previously reported rates of recurrence had a wider range from around 30-90% [24,29,40]. In our study, we found the rate of recurrence in our cHCC-ICC patients to be 83%.
Although our study contributes to the reporting of survival outcomes of the rare entity of cHCC-ICC, there are several limitations to our study. The main limitation is that, given the rare occurrence of cHCC-ICC patients, the small patient sample size can limit the generalization of the conclusions made from the study. Secondly, the possible inherent bias of a retrospective study could impact the conclusions drawn. Third, selection bias associated with patients either referred or considered for surgical resection in either cohort can impact the inclusion of patients. Lastly, our study did not include molecular profiling nor was it large enough in the contemporary era to assess the impact of immunotherapy or other targeted therapies which now have a much more impactful benefit on survival outcomes for patients at the time of relapse. Despite these limitations, we believe that this study provides some groundwork to show that further studies need to be done in this patient population.
5. Conclusions
In summary, combined hepatocellular cholangiocarcinoma is a rare entity that needs to be further studied to improve the outcomes of our patients. Resection remains the only curative option for this patient population. Our study showed that the recurrence-free survival in the resected cHCC-ICC group was significantly lower than that of the resected ICC group. This suggests that we need to perform more studies in this patient population and perhaps a more aggressive initial approach which may include systemic treatments such as chemoimmunotherapy to prevent recurrence is warranted.
Author Contributions
Conceptualization, Rick Lin and Ilyas Sahin; Data curation, Rick Lin; Formal analysis, Rick Lin and Ilyas Sahin; Methodology, Rick Lin and Ilyas Sahin; Supervision, Ilyas Sahin; Writing – original draft, Rick Lin, Doga Kahramangil and Ilyas Sahin; Writing – review & editing, Rick Lin, Doga Kahramangil, Muhammet Ozer, Thomas George, Ibrahim Nassour, Steven Hughes, Ali Zarrinpar and Ilyas Sahin.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by University of Florida Institutional Review Board (IRB202300417).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank the patients and their families.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Altekruse, S.F.; Devesa, S.S.; Dickie, L.A.; McGlynn, K.A.; Kleiner, D.E. Histological classification of liver and intrahepatic bile duct cancers in SEER registries. J Registry Manag 2011, 38, 201–205. [Google Scholar] [PubMed]
- Massarweh, N.N.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Cancer Control 2017, 24, 1073274817729245. [Google Scholar] [CrossRef] [PubMed]
- Jarnagin, W.R.; Weber, S.; Tickoo, S.K.; Koea, J.B.; Obiekwe, S.; Fong, Y.; DeMatteo, R.P.; Blumgart, L.H.; Klimstra, D. Combined hepatocellular and cholangiocarcinoma: Demographic, clinical, and prognostic factors. Cancer 2002, 94, 2040–2046. [Google Scholar] [CrossRef]
- Zuo, H.Q.; Yan, L.N.; Zeng, Y.; Yang, J.Y.; Luo, H.Z.; Liu, J.W.; Zhou, L.X. Clinicopathological characteristics of 15 patients with combined hepatocellular carcinoma and cholangiocarcinoma. Hepatobiliary Pancreat Dis Int 2007, 6, 161–165. [Google Scholar] [PubMed]
- Maximin, S.; Ganeshan, D.M.; Shanbhogue, A.K.; Dighe, M.K.; Yeh, M.M.; Kolokythas, O.; Bhargava, P.; Lalwani, N. Current update on combined hepatocellular-cholangiocarcinoma. Eur J Radiol Open 2014, 1, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, C.; Dell’Aversana, F.; Fusco, R.; Grazzini, G.; Chiti, G.; Simonetti, I.; Bruno, F.; Palumbo, P.; Pierpaoli, L.; Valeri, T.; et al. Combined Hepatocellular-Cholangiocarcinoma: What the Multidisciplinary Team Should Know. Diagnostics (Basel) 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; El-Serag, H.B.; Loomba, R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 2021, 18, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.M.; Zhang, X.F.; Wu, L.P.; Sui, C.J.; Yang, J.M. Risk factors for combined hepatocellular-cholangiocarcinoma: A hospital-based case-control study. World J Gastroenterol 2014, 20, 12615–12620. [Google Scholar] [CrossRef] [PubMed]
- Park, S.E.; Lee, S.H.; Yang, J.D.; Hwang, H.P.; Hwang, S.E.; Yu, H.C.; Moon, W.S.; Cho, B.H. Clinicopathological characteristics and prognostic factors in combined hepatocellular carcinoma and cholangiocarcinoma. Korean J Hepatobiliary Pancreat Surg 2013, 17, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Panjala, C.; Senecal, D.L.; Bridges, M.D.; Kim, G.P.; Nakhleh, R.E.; Nguyen, J.H.; Harnois, D.M. The diagnostic conundrum and liver transplantation outcome for combined hepatocellular-cholangiocarcinoma. Am J Transplant 2010, 10, 1263–1267. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.D.; Park, S.J.; Han, S.S.; Kim, S.H.; Kim, Y.K.; Lee, S.A.; Ko, Y.H.; Hong, E.K. Clinicopathological features and prognosis of combined hepatocellular carcinoma and cholangiocarcinoma after surgery. Hepatobiliary Pancreat Dis Int 2014, 13, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.W.; Li, Q.F.; Chen, Y.Y.; Wang, K.; Pu, D.; Chen, X.R.; Li, C.H.; Jiang, L.; Wang, Y.; Li, Q.; et al. Clinicopathologic features, treatment, survival, and prognostic factors of combined hepatocellular and cholangiocarcinoma: A nomogram development based on SEER database and validation in multicenter study. Eur J Surg Oncol 2022, 48, 1559–1566. [Google Scholar] [CrossRef] [PubMed]
- Chantajitr, S.; Wilasrusmee, C.; Lertsitichai, P.; Phromsopha, N. Combined hepatocellular and cholangiocarcinoma: Clinical features and prognostic study in a Thai population. J Hepatobiliary Pancreat Surg 2006, 13, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Ayas, M.F.; Affas, S.; Ayas, Z.; Chand, M.; Hadid, T. Primary Combined Hepatocellular-Cholangiocarcinoma: A Case of Underdiagnosed Primary Liver Cancer. Cureus 2021, 13, e18224. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Tang, V.Y.; Yao, T.J.; Fan, S.T.; Lo, C.M.; Poon, R.T. Development of Hong Kong Liver Cancer staging system with treatment stratification for patients with hepatocellular carcinoma. Gastroenterology 2014, 146, 1691–1700. [Google Scholar] [CrossRef] [PubMed]
- Farges, O.; Fuks, D.; Le Treut, Y.P.; Azoulay, D.; Laurent, A.; Bachellier, P.; Nuzzo, G.; Belghiti, J.; Pruvot, F.R.; Regimbeau, J.M. AJCC 7th edition of TNM staging accurately discriminates outcomes of patients with resectable intrahepatic cholangiocarcinoma: By the AFC-IHCC-2009 study group. Cancer 2011, 117, 2170–2177. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Z.; Liao, Y.; Li, J.; Dong, H.; Peng, H.; Xu, W.; Fan, Z.; Gao, F.; Liu, C.; et al. Prediction of Survival and Analysis of Prognostic Factors for Patients With Combined Hepatocellular Carcinoma and Cholangiocarcinoma: A Population-Based Study. Front Oncol 2021, 11, 686972. [Google Scholar] [CrossRef] [PubMed]
- Garancini, M.; Goffredo, P.; Pagni, F.; Romano, F.; Roman, S.; Sosa, J.A.; Giardini, V. Combined hepatocellular-cholangiocarcinoma: A population-level analysis of an uncommon primary liver tumor. Liver Transpl 2014, 20, 952–959. [Google Scholar] [CrossRef]
- Vilchez, V.; Shah, M.B.; Daily, M.F.; Pena, L.; Tzeng, C.W.; Davenport, D.; Hosein, P.J.; Gedaly, R.; Maynard, E. Long-term outcome of patients undergoing liver transplantation for mixed hepatocellular carcinoma and cholangiocarcinoma: An analysis of the UNOS database. HPB (Oxford) 2016, 18, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.W.; Chok, K.S.H. Importance of surgical margin in the outcomes of hepatocholangiocarcinoma. World J Hepatol 2017, 9, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Belghiti, J. Oncologic resection for malignant tumors of the liver. Ann Surg 2011, 253, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Beaufrere, A.; Calderaro, J.; Paradis, V. Combined hepatocellular-cholangiocarcinoma: An update. J Hepatol 2021, 74, 1212–1224. [Google Scholar] [CrossRef] [PubMed]
- Xue, R.; Chen, L.; Zhang, C.; Fujita, M.; Li, R.; Yan, S.M.; Ong, C.K.; Liao, X.; Gao, Q.; Sasagawa, S.; et al. Genomic and Transcriptomic Profiling of Combined Hepatocellular and Intrahepatic Cholangiocarcinoma Reveals Distinct Molecular Subtypes. Cancer Cell 2019, 35, 932–947. [Google Scholar] [CrossRef] [PubMed]
- Leoni, S.; Sansone, V.; Lorenzo, S.; Ielasi, L.; Tovoli, F.; Renzulli, M.; Golfieri, R.; Spinelli, D.; Piscaglia, F. Treatment of Combined Hepatocellular and Cholangiocarcinoma. Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Penzkofer, L.; Groger, L.K.; Hoppe-Lotichius, M.; Baumgart, J.; Heinrich, S.; Mittler, J.; Gerber, T.S.; Straub, B.K.; Weinmann, A.; Bartsch, F.; et al. Mixed Hepatocellular Cholangiocarcinoma: A Comparison of Survival between Mixed Tumors, Intrahepatic Cholangiocarcinoma and Hepatocellular Carcinoma from a Single Center. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.W.; Wu, T.C.; Lin, H.Y.; Hung, C.M.; Hsieh, P.M.; Yeh, J.H.; Hsiao, P.; Huang, Y.L.; Li, Y.C.; Wang, Y.C.; et al. Clinical features and outcomes of combined hepatocellular carcinoma and cholangiocarcinoma versus hepatocellular carcinoma versus cholangiocarcinoma after surgical resection: A propensity score matching analysis. BMC Gastroenterol 2021, 21, 20. [Google Scholar] [CrossRef] [PubMed]
- Gentile, D.; Donadon, M.; Lleo, A.; Aghemo, A.; Roncalli, M.; di Tommaso, L.; Torzilli, G. Surgical Treatment of Hepatocholangiocarcinoma: A Systematic Review. Liver Cancer 2020, 9, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Shi, G. Survival outcomes of combined hepatocellular-cholangiocarcinoma compared with intrahepatic cholangiocarcinoma: A SEER population-based cohort study. Cancer Med 2022, 11, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Chung, G.E.; Yu, S.J.; Hwang, S.Y.; Kim, J.S.; Kim, H.Y.; Yoon, J.H.; Lee, H.S.; Yi, N.J.; Suh, K.S.; et al. Long-term prognosis of combined hepatocellular and cholangiocarcinoma after curative resection comparison with hepatocellular carcinoma and cholangiocarcinoma. J Clin Gastroenterol 2011, 45, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Lee, K.W.; Heo, J.S.; Kim, S.J.; Choi, S.H.; Kim, Y.I.; Joh, J.W. Comparison of combined hepatocellular and cholangiocarcinoma with hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Surg Today 2006, 36, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.I.; Hwang, S.; Lee, Y.J.; Kim, K.H.; Ahn, C.S.; Moon, D.B.; Ha, T.Y.; Song, G.W.; Jung, D.H.; Lee, J.W.; et al. Postresection Outcomes of Combined Hepatocellular Carcinoma-Cholangiocarcinoma, Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. J Gastrointest Surg 2016, 20, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Yang, D.; Tang, C.L.; Cai, P.; Ma, K.S.; Ding, S.Y.; Zhang, X.H.; Guo, D.Y.; Yan, X.C. Combined hepatocellular carcinoma and cholangiocarcinoma (biphenotypic) tumors: Clinical characteristics, imaging features of contrast-enhanced ultrasound and computed tomography. BMC Cancer 2016, 16, 158. [Google Scholar] [CrossRef] [PubMed]
- Eschrich, J.; Kobus, Z.; Geisel, D.; Halskov, S.; Rossner, F.; Roderburg, C.; Mohr, R.; Tacke, F. The Diagnostic Approach towards Combined Hepatocellular-Cholangiocarcinoma-State of the Art and Future Perspectives. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.C.; Lee, H.; Choi, M.S.; Lee, J.H.; Paik, S.W.; Yoo, B.C.; Rhee, J.C.; Cho, J.W.; Park, C.K.; Kim, H.J. Clinicopathologic features and prognosis of combined hepatocellular cholangiocarcinoma. Am J Surg 2005, 189, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Connell, L.C.; Harding, J.J.; Shia, J.; Abou-Alfa, G.K. Combined intrahepatic cholangiocarcinoma and hepatocellular carcinoma. Chin Clin Oncol 2016, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.F.; Beal, E.W.; Bagante, F.; Chakedis, J.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; et al. Early versus late recurrence of intrahepatic cholangiocarcinoma after resection with curative intent. Br J Surg 2018, 105, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.S.; Zhang, X.F.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Recurrence Patterns and Timing Courses Following Curative-Intent Resection for Intrahepatic Cholangiocarcinoma. Ann Surg Oncol 2019, 26, 2549–2557. [Google Scholar] [CrossRef] [PubMed]
- Yoh, T.; Hatano, E.; Seo, S.; Okuda, Y.; Fuji, H.; Ikeno, Y.; Taura, K.; Yasuchika, K.; Okajima, H.; Kaido, T.; et al. Long-Term Survival of Recurrent Intrahepatic Cholangiocarcinoma: The Impact and Selection of Repeat Surgery. World J Surg 2018, 42, 1848–1856. [Google Scholar] [CrossRef] [PubMed]
- Weber, S.M.; Jarnagin, W.R.; Klimstra, D.; DeMatteo, R.P.; Fong, Y.; Blumgart, L.H. Intrahepatic cholangiocarcinoma: Resectability, recurrence pattern, and outcomes. J Am Coll Surg 2001, 193, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Jung, D.H.; Hwang, S.; Song, G.W.; Ahn, C.S.; Moon, D.B.; Kim, K.H.; Ha, T.Y.; Park, G.C.; Hong, S.M.; Kim, W.J.; et al. Longterm prognosis of combined hepatocellular carcinoma-cholangiocarcinoma following liver transplantation and resection. Liver Transpl 2017, 23, 330–341. [Google Scholar] [CrossRef]
Figure 1.
Flowchart for study subject selection.
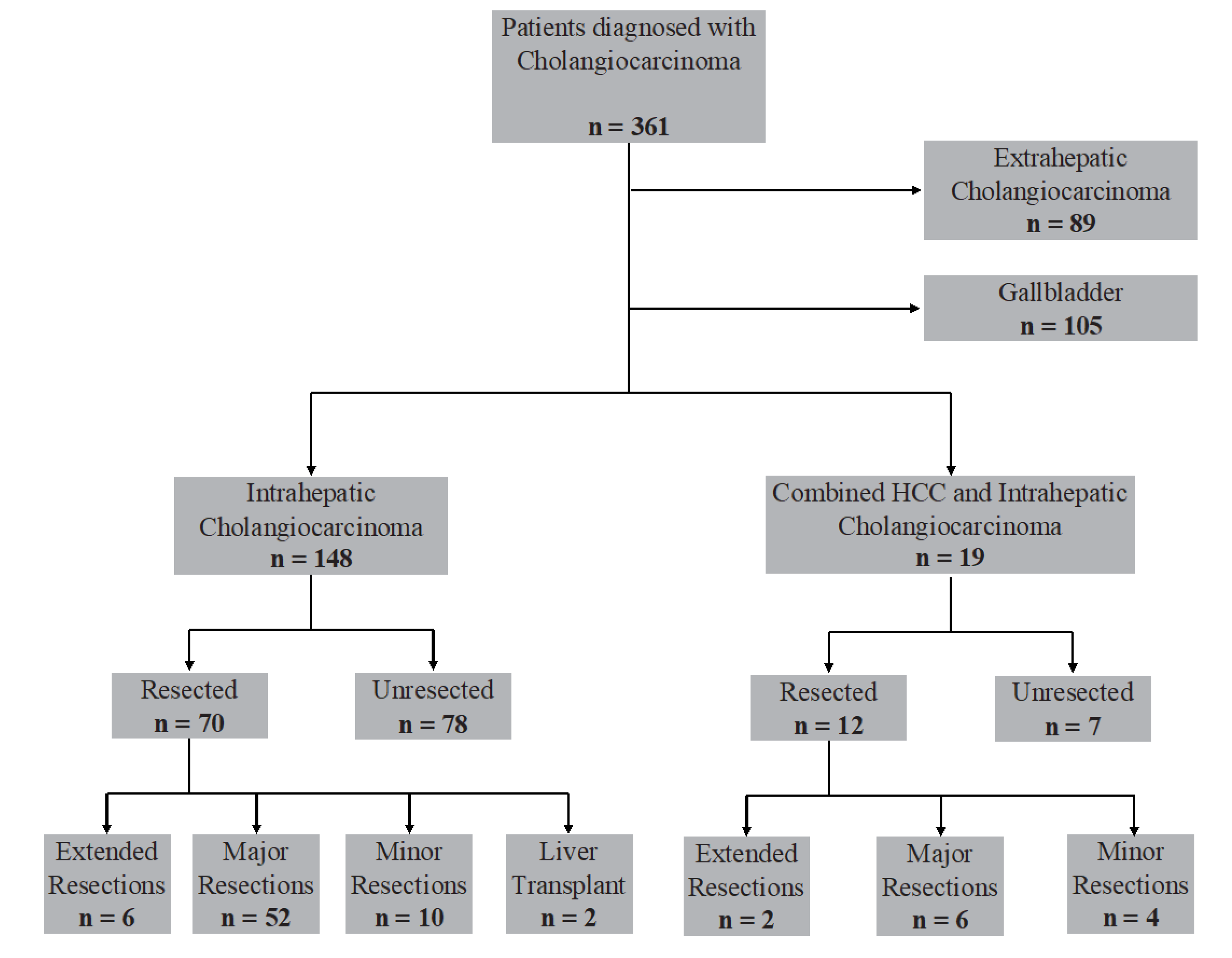
Figure 2.
Worse recurrence-free survival among patients with cHCC-ICC. The number of subjects was 82.
Figure 2.
Worse recurrence-free survival among patients with cHCC-ICC. The number of subjects was 82.
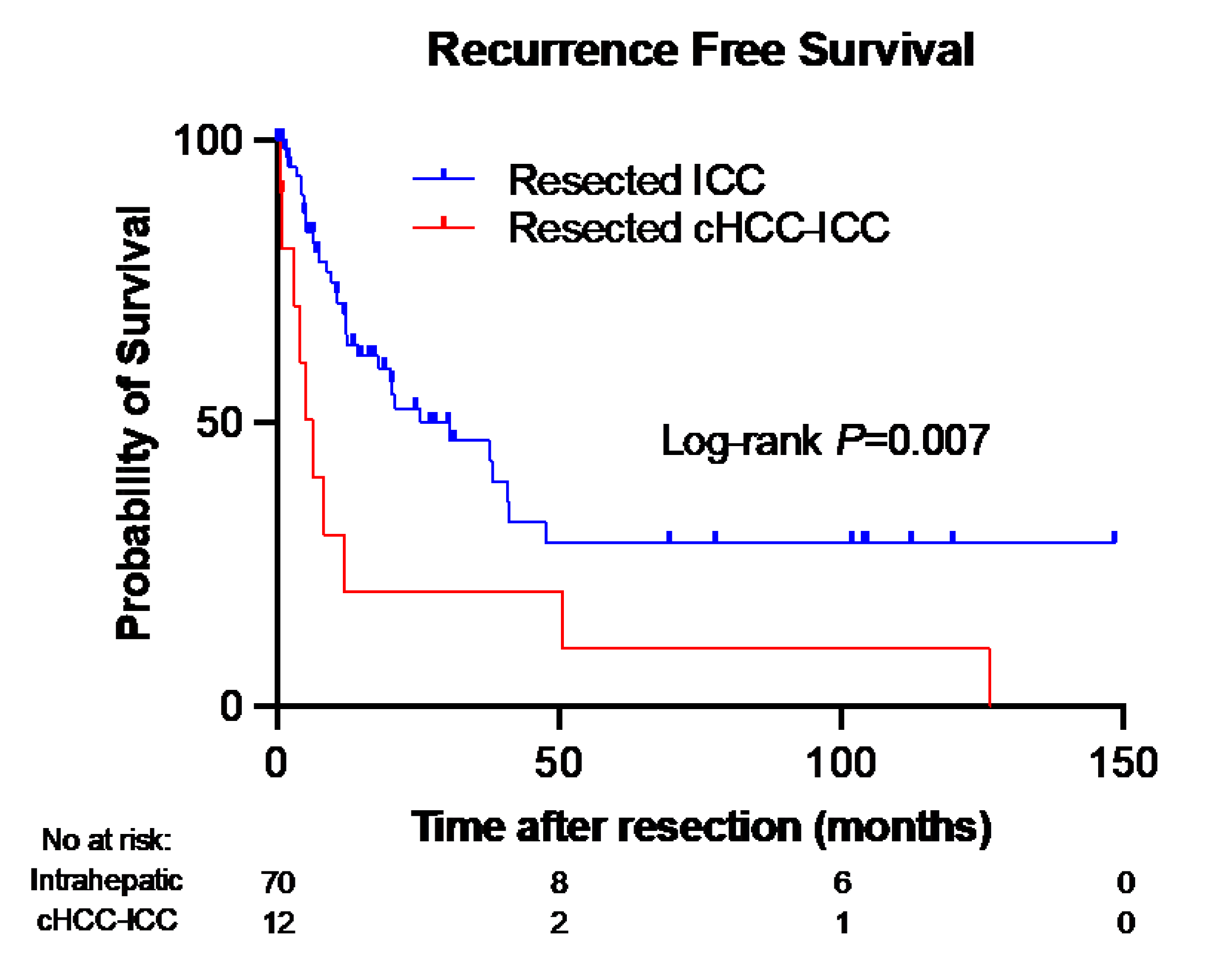
Figure 3.
Similar overall survival between cHCC-ICC and ICC patients. The number of subjects was 82.
Figure 3.
Similar overall survival between cHCC-ICC and ICC patients. The number of subjects was 82.
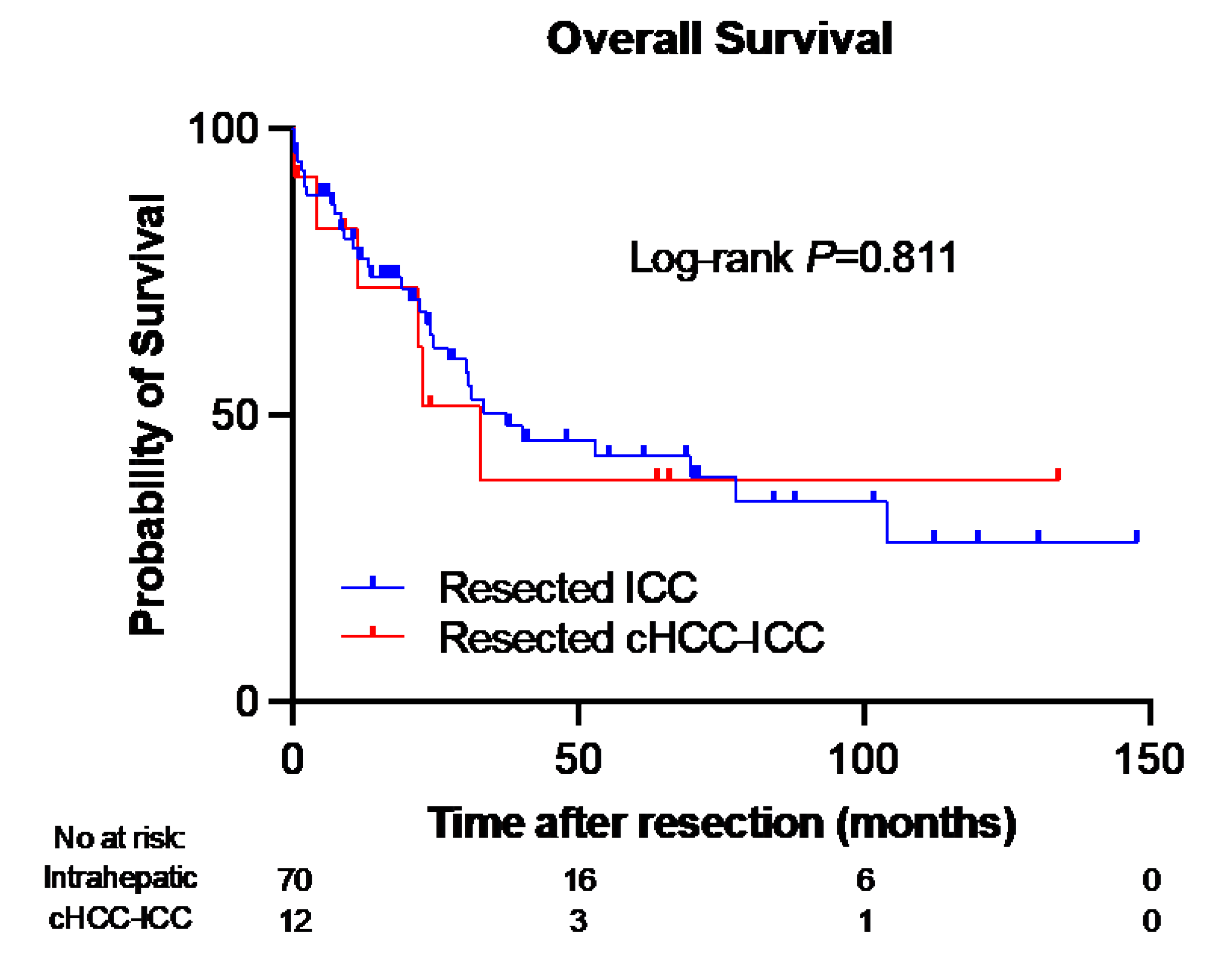

Table 1.
Resected Intrahepatic Cholangiocarcinoma vs. Combined Hepatocellular Carcinoma/Cholangiocarcinoma.
Table 1.
Resected Intrahepatic Cholangiocarcinoma vs. Combined Hepatocellular Carcinoma/Cholangiocarcinoma.
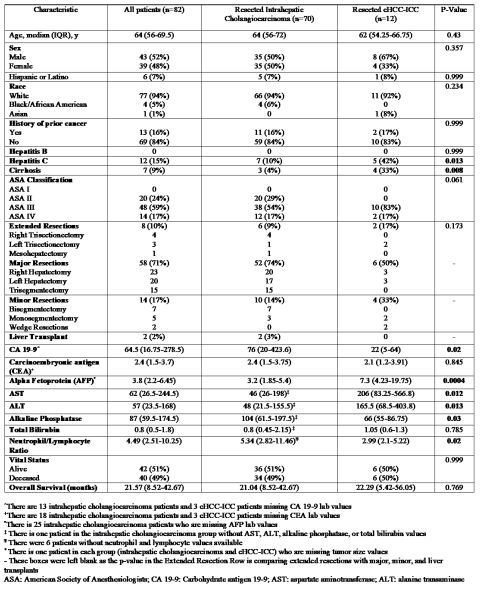 |
Table 2.
Histological Outcomes After Resection.
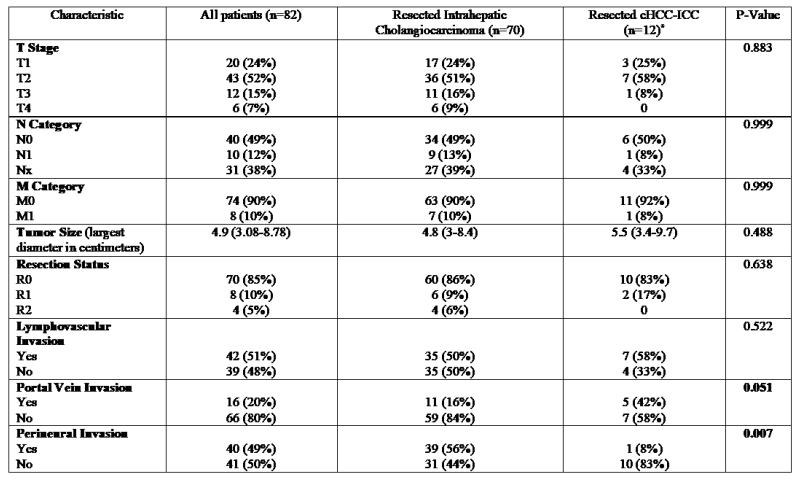 |
Table 3.
Location of Tumor Recurrence.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



