
Submitted:
26 June 2024
Posted:
26 June 2024
You are already at the latest version
Abstract
This study aimed to compare the flexural strength, surface roughness, and microhardness of a resin for three-dimensional (3D) printing and a conventional composite resin and to evaluate whether the printing orientation influences these properties. To evaluate the flexural resistance, test specimens were produced and divided into four groups: three groups of resins for 3D printing with inclinations of 0°, 45°, and 90°, and one group of conventional composite resin. Forty discs were produced and subjected to a sandpaper-polishing sequence, and the surface roughness was measured using a roughness meter. The Vickers microhardness test was performed at three different points, and the average was obtained. The results were subjected to ANOVA statistical analysis and Tukey's test. There were statistical differences in the flexural strength and microhardness between the conventional resin and the resin used for 3D printing. No statistical difference in surface roughness was observed. The resin for 3D printing exhibited lower flexural strength and microhardness than conventional composite resins. We concluded that the resin for 3D printing had lower flexural strength and hardness than the conventional composite resin but similar surface roughness. The printing orientation did not affect the flexural strength, whereas the hardness increased as the printing angle increased.
Keywords:
3D printing
; composite resin
; flexural strength
; microhardness
; surface roughness
1. Introduction
Computer-aided design and manufacturing (CAD/CAM) was introduced in dentistry in the 1980s, revolutionizing the production of prosthetic parts both in laboratories and offices, substantially reducing the number of steps carried out to create an indirect restoration and, consequently, the time to complete a restorative treatment [1]. The CAD/CAM technology is divided into two phases: CAD, which consists of the design of the restoration carried out using computer programs, and CAM, which represents the production stage of the restoration designed in the CAD phase. The CAM phase can be performed using two methods: subtractive manufacturing (MS) or milling and additive manufacturing (MA) or three-dimensional (3D) printing [2].
Subtractive manufacturing involves creating objects by milling or machining blocks and/or solid discs using milling cutters. It is widely used in materials such as zirconia (ZrO2), polymethylmethacrylate (PMMA), and glass ceramics, and its main advantages include a reduction in operational costs and human error compared to manual production [3]. However, its disadvantages include high consumption of cutters, wastage of raw materials, and difficulty in producing complex geometries [3,4].
Three-dimensional printing transforms a virtual object (CAD file) into a physical object by superimposing thin layers of raw material, which is a common characteristic of all 3D printing technologies [5]. Developed in the 1980s and patented in 1986 by Chuck Hull with the creation of a production technology called stereolithography (SLA), 3D printing began to be widely used both commercially and industrially after the patents expired, enabling the development of new technologies such as Digital Light Processing (DLP) and Mask Stereolithography (MSLA) [2,5,6].
Stereolithography technology uses a UV laser with a wavelength of 200–500 nm that covers the entire printing area and polymerizes the layers of photosensitive polymers. The DLP and MSLA technologies use the radiation produced by a UV light projector and light-emitting diodes, respectively, to solidify the polymer according to the contour of the object to be produced, making the printing process faster with lower investment and input costs. compared with SLA [6,7].
Three-dimensional printing is used in several specialties such as oral and maxillofacial surgery, implant dentistry, endodontics, and periodontics to produce surgical guides and models for surgical planning [8], orthodontics and dental prosthetics for the production of models, complete dentures, tray individuals [9], provisional indirect restorations [10], and more recently, for definitive or long-term indirect restorations [11]. To perform 3D printing of any device, it is necessary to use software to position and orient the object in relation to the ground, which can assume a parallel or perpendicular orientation or with variations in angulation. This orientation is directly related to the overlapping of material layers for the formation of the object during 3D printing, which can interfere with its mechanical properties [12].
With the increasing application of 3D printing, new polymeric materials are being developed to produce prostheses and restorations that can remain in the mouth for long periods [7]. Such materials have a composition similar to conventional resins and are categorized as nano-hybrid composite resins, presenting an organic matrix such as bisphenol A glycidyl methacrylate (Bis-GMA), Urethane dimethacrylate (UDMA), Bisphenol A/ethylene glycol/methyl dimethacrylate (Bis-EMA), and triethylene glycol dimethacrylate (TEGDMA) as well as inorganic ceramic fillers such as zirconia and silanized silica and barium glass, aiming to increase their mechanical and biocompatibility properties [7,13].
Three-dimensional printing plays a revolutionary role in dentistry, making it possible to obtain restorations that can be used temporarily or even long-lasting. Thus, evaluating the mechanical properties of the materials used to obtain these restorations and how impression orientation could influence these properties is essential for determining the biomechanical characteristics in comparison with restorations obtained using conventional techniques.
Considering this scenario, the objective of this study is to compare the flexural strength (σ), surface roughness (Ra), and microhardness of a nano-hybrid composite resin with silanized ceramic and zirconia fillers for 3D printing and a conventional nano-hybrid composite resin and evaluate whether printing orientation influences these properties. The null hypotheses tested were as follows: 1) there is no difference in the mechanical properties between the materials tested and 2) the printing orientation does not influence the mechanical properties of the resin for 3D printing.
2. Materials and Methods
2.1. Experimental Design
The materials used were the nano-hybrid composite resin with silanized ceramic and zirconia fillers priZma 3D Biocrown (Makertech Labs, Tatuí, São Paulo, Brazil) for 3D printing, and the conventional nano-hybrid composite resin FORMA A1B (Ultradent do Brasil, Indaiatuba, São Paulo, Brazil), as a control group (CT) (Table 1).
The specimens (CP) from the group with resin for 3D printing were divided into three subgroups: 1) 0°BC0, 2) 45°BC45, and 3) 90°BC90 according to the printing orientation (0°, 45°, and 90°) in relation to the ground, totaling four groups, three of which were made of resin for 3D printing and one of a conventional composite resin.
2.2. Preparation of Test Specimens
The specimens to evaluate the flexural resistance of the resin group for 3D printing (n=30) were designed using a CAD program Meshmixer (Autodesk, San Francisco, California, USA), in the shape of a bar with dimensions of L × W × E of 25 (±2) × 2 (± 0.1) × 2 (± 0.1) mm, following the recommendations of the International Organization for Standardization ISO 4049:2009 for testing polymer-based restorative materials [14].
Disc-shaped specimens with a diameter of 10 mm and thickness of 2 mm were designed (n=30) to evaluate the surface roughness and microhardness [15]. The bar and disk format designs were exported in STL (standard tessellation language) format and imported into the Chitubox Basic program (Chitubox, Shenzhen, Guangdong, China), a specific software for 3D printing.
The resin from the resin group for 3D printing was used to print the specimen in conjunction with a Photon D2 3D printer (Anycubic, Shenzhen, Guangdong, China) with DLP technology after mechanized shaking for 40 min to achieve homogenization, according to the manufacturer's instructions.
The specimens were printed with a layer thickness of 50 µm and the printing time parameters were defined based on a previously printed calibration object so that the specimen presented the specified dimensions (Figure 1).
After printing, the specimen was subjected to post-processing in two stages: washing in isopropyl alcohol for 10 min [6] to remove excess unpolymerized resin in a Form Wash washer (Formlabs Inc., Somerville, Massachusetts, USA) and post-curing in a Form Cure (Formlabs Inc., Somerville, Massachusetts, USA), a UV light cabinet with a wavelength of 405 nm for 60 min, according to the manufacturer's guidelines. The supports were removed, and the surface and the region with the support were regularized using a diamond disc and abrasive rubbers (Dhpro, Paranaguá, Paraná, Brazil) at low speed with the aid of a bench motor and straight handpiece (Beltec, Araraquara, São Paulo, Brazil) (Figure 2).
All specimens were measured using digital calipers (Mitutoyo Corp., Kanagawa, Japan) to validate their length, width, thickness, and diameter.
Specimens from the conventional composite resin group were fabricated in condensation silicone molds obtained from a matrix designed using the CAD program Meshmixer (Autodesk, San Francisco, California, USA) and printed. The molds followed the dimensions specified in the ISO 4049:2009 standard [14]. The composite resin was condensed with a metal spatula in a single increment until it filled the mold space, the excess was removed, and a 10 mm glass plate was placed on the mold to homogenize the surface. Photopolymerization of the specimens was performed using a single calibrated operator. The bar-shaped specimens (n=10) were photopolymerized in three areas (specimen divided into three thirds) for 60 s in each area on the glass plate, whereas in the disc-shaped specimens (n=10), photopolymerization was carried out at a central point on the glass plate using a Radii Plus photopolymerizer (SDI Limited, Bayswater, Victoria, Australia) [16]. (Figure 3).
2.3. Flexural Strength Test (σ)
The bar-shaped specimen was subjected to the 3-point flexural strength test on an Instron 3342 universal testing machine (Instron, Norwood, Massachusetts, USA) with a load cell of 500 N and a speed of 1 mm/min until rupture and values expressed in N were converted into flexural strength (σ) in Mpa using the following formula:
where,
σ = 3FL/2bd2,
- σ = flexural strength
- = Load (force) at the fracture point
- = length of support span
- = Width of the sample
- = Sample thickness
2.4. Surface Roughness Test (Ra)
The disc-shaped specimens were positioned in templates designed and printed with rigid resin, and the face with the supports was polished with water sandpaper with grits #600, #1200, #1500, and #2000 on an automated polishing machine (Ecomet 250, Buehler, Lake Bluff, Illinois, USA) for 30 s at 50 revolutions per minute (rpm) and a vertical pressure of 10 N on the specimens. After polishing, the discs were numbered on the template [17].
An SJ-301 rugosimeter (Mitutoyo Corp., Kanagawa, Japan) with ISO 1997 measurement parameters was used, and three measurements were performed in different directions for each specimen to obtain the average Ra value.
2.5. Microhardness Test
After the surface roughness test, the specimens were positioned in an HMG-V microhardness meter (Shimadzu do Brasil, Barueri, São Paulo, Brazil) to perform the Vickers Microhardness (VHN) test using a pyramidal-shaped diamond indenter with a load of 50 g for 30 s in three different areas and measured at 20× magnification to obtain an average value [18].
Statistical analysis
The Shapiro–Wilk test was conducted, and we found that in one of the groups, the flexural strength and surface roughness were not normally distributed. After data normalization using the Box-Cox transformation, analysis of variance (ANOVA) and Tukey's post hoc test were used to test the hypothesis that the 3D printing orientation did not influence the flexural strength, surface roughness, and microhardness of the resins.
The effects of 3D printing orientation on the flexural strength, surface roughness, and microhardness were calculated using Partial Eta squared (partial ƞ2).
All tests were performed using the SPSS 26.0 statistical program (IBM, Armonk, NY, USA). The significance level established was 5%.
3. Results
Figure 4 shows a multi-axis graph of the average values (standard deviations) of the flexural strength, surface roughness, and microhardness according to the 3D printing orientation.
There was a decrease in the flexural resistance values of the 3D printing groups with an increase in the printing angle; however, this was not statistically significant (p>0.05). The flexural resistance of the composite resin group was significantly greater than that of the 3D printing group (p<0.001).
There was no statistically significant difference in the surface roughness between the resin in the composite group and the groups with resin for 3D printing (p=0.387).
The average microhardness of the resin in the composite resin group was significantly higher than that of the resin in the 3D printing resin group (p<0.001). The BC90 group exhibited a higher average microhardness than the BC0 and BC45 groups.
Table 2 shows the mean values (standard deviations) and 95% confidence interval (95%CI) of the groups.
This section is divided into several subsections. A concise and precise description of the experimental results, their interpretation, and experimental conclusions that can be drawn.
4. Discussion
The results of this study showed that the first Ho proposal, which indicated no difference in the mechanical properties between 3D printed resin and conventional composite resin, was partially accepted. The flexural strength and microhardness properties showed significant differences between the two materials; however, no significant difference was observed in surface roughness. The second Ho proposal, which indicates that the printing orientation did not influence the mechanical properties of the materials, was also partially accepted. The flexural strength and microhardness variables were not influenced by the printing orientation, whereas the surface roughness variable was.
The resin for 3D printing showed lower flexural resistance on the three slopes than the conventional composite resin. The values obtained were also lower than the minimum resistance required for restorative materials based on Type 1, Class 2, and Group 2 polymers (100 Mpa for the occlusal face), according to ISO 4049:2009 [14]. Several studies that evaluated the flexural strength of impression resins indicated for temporary restorations found values between 49.87 and 159.9 Mpa, which would fit the resin tested in this category, diverging from the manufacturer's indication [16,17,20,21,22,23].
The literature shows that some factors can influence the mechanical properties of printed resins, such as the post-curing time associated with the increase in temperature during the process [21,24]. A duration of 30 min at 60 ºC significantly increased the flexural strength of the resin for permanent restorations, as measured by biaxial tests [24,25]. In this study, the post-printing stage followed the manufacturer's guidelines, which indicated a post-curing time of 30–60 min without increasing the temperature.
Hardness is a crucial characteristic of restorative materials, and microhardness tests indicate a high density of these materials, making them capable of resisting wear processes in the oral cavity [3]. The tested resin showed statistically significantly lower microhardness values than the conventional resin group. Studies have shown that printing resins containing inorganic fillers and tend to present higher microhardness values than materials based on PMMA [20,26].
Bora et al. characterized the composition of several resins for 3D printing and compared their mechanical properties with those of conventional resins and found that a greater amount of inorganic filler in the resins resulted in higher microhardness values [3]. These results corroborate the results of this study, as the resin in the conventional group had 67% inorganic filler by weight, whereas the resin in the 3D printing group had less than 35%.
The resin for 3D printing has UDMA as its main organic constituent, a high-molecular-weight and high-viscosity monomer, and diluent monomers that promote increased fluidity of the resin, enabling the 3D printing process to take place without failure [27]. Lin et al. studied the mechanical properties of different organic matrices used in the composition of printing resins and showed that UDMA in greater proportions increased the flexural strength and degree of conversion but reduced the microhardness [28]. These findings are consistent with those of the present study.
The inorganic phase of the tested resin was composed of silanized zirconia mixed oxide and other filler particles such as silanized silica and barium glass. The incorporation of spherical silica particles reduced the surface roughness while maintaining the resistance characteristics [29]. The presence of barium glass improves the optical properties of the resin, increases the radiopacity and translucency, and decreases the microhardness, which reduces the wear generated on the antagonists [29]. The addition of zirconia increases microhardness, which increases the resistance of the resin to wear [3].
The surface roughness of the tested resins did not show significant differences, which means that the resins obtained by 3D printing allowed finishing and polishing equivalent to those of conventional composite resins [17]. The surface roughness standard for composite resins after polishing is 0.2 µm, and values above this standard increase the risk of bacterial plaque accumulation [30]. Surface roughness patterns below this value were obtained for the resin tested at three printing inclinations, corroborating values reported in the literature [17].
Printing orientation is a critical aspect in obtaining satisfactory results in 3D printing and involves determining the direction in which the restoration is built in relation to the horizontal plane, which directly affects the number of layers and time required for the final print. [31]. The influence of this parameter on the mechanical properties of the resins was previously reported [32]. The reduction in flexural resistance values in the tested resin as the printing orientation angle increased has been reported in the literature, indicating that impressions parallel to the horizontal plane, with layer construction perpendicular to the direction of forces, tend to offer greater resistance [15,22,31]. However, resins for different applications such as surgical guides and occlusal plates used in printers with technologies that differ from those used in the present study may present divergent results [32,33].
Other studies evaluated the surface roughness and microhardness of specimens printed in different orientations, showing roughness levels above the minimum standard for resins, which is justified by the formation of small union lines between overlapping layers of the material [15,34]. However, these studies did not consider mechanical polishing of the surfaces after printing, which differs from the methodology and results of the present study. The literature also shows that changing the printing orientation does not change the microhardness values, because this property is more strongly related to the filler content present in the resins [18].
Another aspect to be considered is the printing accuracy between the technologies, owing to the dimensional reproduction capacity and precision of the object. The literature reports the superiority of DLP printers over MSLA [35,36]. Chen et al. found that the flexural strength of resins for restorations printed using a DLP printer was higher; however, this difference could be reduced by increasing the post-curing time [21]. The decrease in the costs of the DLP equipment and the positive results obtained in previous research support the choice of this technology in the present study [37].
Mechanical properties play a fundamental role in restorative materials as they must resist functional and parafunctional occlusal forces while maintaining their anatomical and surface polishing characteristics. Conventional composite resins are widely used in the manufacture of direct and indirect restorations because of their flexural resistance and surface roughness, which allow them to remain in the mouth for long periods [38,39,40]. However, new resin materials for 3D printing have been developed with improved inorganic filler contents, which provide mechanical properties closer to those of conventional resins while maintaining the benefits of low cost and increased production speed [13].
The present study has strengths, including the use of stable and precise printing technology, as well as the comparison between materials with similar characteristics and clinical applications, which differ in their composition and energy source for conversion; however, further studies are necessary to characterize new resins for 3D printing, to identify the types and percentages of inorganic fillers present in these materials, as these constituents can contribute to improving flexural resistance and hardness characteristics. Furthermore, studies that simulate the conditions of the oral cavity in vivo are essential to evaluate the longevity and maintenance of the characteristics of these new materials.
5. Conclusions
Based on the results obtained, it can be concluded that the tested 3D printing resin showed mechanical properties of flexural strength and hardness lower than those of conventional composite resins, but with similar surface roughness. The printing orientation did not affect the flexural strength, whereas the hardness increased as the printing angle increased.
Author Contributions
Data curation, L.V.A. and R.R.T.; investigation, L.V.A..; methodology, L.V.A., R.F.C. and F.S.G.; project administration, R.R.T.; resources, L.V.A. and R.R.T..; supervision, R.R.T.; writing—original draft, L.V.A.; R.R.T., E.M.M. and F.F.S.; writing—review and editing, D.B.D. and G.G.C. All authors have read and agreed to the published version of the manuscript.
Funding
No funding.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Duret F, Blouin JL, Duret B. CAD-CAM in dentistry. J Am Dent Assoc. 1988 Nov;117(6):715-20. [CrossRef] [PubMed]
- van Noort, R. The future of dental devices is digital. Dent Mater. 2012 Jan;28(1):3-12. Epub 2011 Nov 26. [CrossRef] [PubMed]
- Myagmar G, Lee JH, Ahn JS, Yeo IL, Yoon HI, Han JS. Wear of 3D printed and CAD/CAM milled interim resin materials after chewing simulation. J Adv Prosthodont. 2021 Jun;13(3):144-151. Epub 2021 Jun 25. [CrossRef] [PubMed]
- Valenti C, Isabella Federici M, Masciotti F, Marinucci L, Xhimitiku I, Cianetti S, Pagano S. Mechanical properties of 3D-printed prosthetic materials compared with milled and conventional processing: A systematic review and meta-analysis of in vitro studies. J Prosthet Dent. 2022 Aug 5:S0022-3913(22)00415-2 Epub ahead of print. [CrossRef] [PubMed]
- Kessler A, Hickel R, Reymus M. 3D Printing in Dentistry-State of the Art. Oper Dent. 2020 Jan/Feb;45(1):30-40. Epub 2019 Jun 7. [CrossRef] [PubMed]
- Nowacki B, Kowol P, Kozioł M, Olesik P, Wieczorek J, Wacławiak K. Effect of Post-Process Curing and Washing Time on Mechanical Properties of mSLA Printouts. Materials (Basel). 2021 Aug 26;14(17):4856. [CrossRef] [PubMed]
- Jockusch J, Özcan M. Additive manufacturing of dental polymers: An overview on processes, materials and applications. Dent Mater J. 2020 Jun 5;39(3):345-354. Epub 2020 Feb 7. [CrossRef] [PubMed]
- Tack P, Victor J, Gemmel P, Annemans L. 3D-printing techniques in a medical setting: a systematic literature review. Biomed Eng Online. 2016 Oct 21;15(1):115. [CrossRef] [PubMed]
- Revilla-León M, Özcan M. Additive Manufacturing Technologies Used for Processing Polymers: Current Status and Potential Application in Prosthetic Dentistry. J Prosthodont. 2019 Feb;28(2):146-158. Epub 2018 Apr 22. [CrossRef] [PubMed]
- Tahayeri A, Morgan M, Fugolin AP, Bompolaki D, Athirasala A, Pfeifer CS, Ferracane JL, Bertassoni LE. 3D printed versus conventionally cured provisional crown and bridge dental materials. Dent Mater. 2018 Feb;34(2):192-200. Epub 2017 Oct 27. [CrossRef] [PubMed]
- Zimmermann M, Ender A, Egli G, Özcan M, Mehl A. Fracture load of CAD/CAM-fabricated and 3D-printed composite crowns as a function of material thickness. Clin Oral Investig. 2019 Jun;23(6):2777-2784. Epub 2018 Oct 27. [CrossRef] [PubMed]
- Lu Y, Wang L, Dal Piva AMO, Tribst JPM, Čokić SM, Zhang F, Werner A, Kleverlaan CJ, Feilzer AJ. Effect of printing layer orientation and polishing on the fatigue strength of 3D-printed dental zirconia. Dent Mater. 2024 Feb;40(2):190-197. Epub 2023 Nov 17. [CrossRef] [PubMed]
- Bora PV, Sayed Ahmed A, Alford A, Pitttman K, Thomas V, Lawson NC. Characterization of materials used for 3D printing dental crowns and hybrid prostheses. J Esthet Restor Dent. 2024 Jan;36(1):220-230. Epub 2023 Nov 26. [CrossRef] [PubMed]
- International Organization for Standarization. ISO 4049:2009 Dentistry Polymer based restorative materials. 2009;2000.
- Shim JS, Kim JE, Jeong SH, Choi YJ, Ryu JJ. Printing accuracy, mechanical properties, surface characteristics, and microbial adhesion of 3D-printed resins with various printing orientations. J Prosthet Dent. 2020 Oct;124(4):468-475. Epub 2019 Dec 4. [CrossRef] [PubMed]
- Ribeiro AKC, de Freitas RFCP, de Carvalho IHG, de Miranda LM, da Silva NR, de Fátima Dantas de Almeida L, Zhang Y, da Fonte Porto Carreiro A, de Assunção E Souza RO. Flexural strength, surface roughness, micro-CT analysis, and microbiological adhesion of a 3D-printed temporary crown material. Clin Oral Investig. 2023 May;27(5):2207-2220. Epub 2023 Mar 18. [CrossRef] [PubMed]
- Scotti CK, Velo MMAC, Rizzante FAP, Nascimento TRL, Mondelli RFL, Bombonatti JFS. Physical and surface properties of a 3D-printed composite resin for a digital workflow. J Prosthet Dent. 2020 Nov;124(5):614.e1-614.e5. Epub 2020 Jul 4. [CrossRef] [PubMed]
- Al-Dulaijan YA, Alsulaimi L, Alotaibi R, Alboainain A, Alalawi H, Alshehri S, Khan SQ, Alsaloum M, AlRumaih HS, Alhumaidan AA, Gad MM. Comparative Evaluation of Surface Roughness and Hardness of 3D Printed Resins. Materials (Basel). 2022 Oct 1;15(19):6822. [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences Second Edition.
- Digholkar S, Madhav VN, Palaskar J. Evaluation of the flexural strength and microhardness of provisional crown and bridge materials fabricated by different methods. J Indian Prosthodont Soc. 2016 Oct-Dec;16(4):328-334. [CrossRef] [PubMed]
- Chen H, Cheng DH, Huang SC, Lin YM. Comparison of flexural properties and cytotoxicity of interim materials printed from mono-LCD and DLP 3D printers. J Prosthet Dent. 2021 Nov;126(5):703-708. [CrossRef]
- KEßLER A, Hickel R, Ilie N. In vitro investigation of the influence of printing direction on the flexural strength, flexural modulus and fractographic analysis of 3D-printed temporary materials. Dent Mater J. 2021 May 29;40(3):641-649. Epub 2021 Jan 15. [CrossRef] [PubMed]
- Soto-Montero J, de Castro EF, Romano BC, Nima G, Shimokawa CAK, Giannini M. Color alterations, flexural strength, and microhardness of 3D printed resins for fixed provisional restoration using different post-curing times. Dent Mater. 2022 Aug;38(8):1271-1282. Epub 2022 Jun 16. [CrossRef] [PubMed]
- Baytur S, Diken Turksayar AA. Effects of post-polymerization conditions on color properties, surface roughness, and flexural strength of 3D-printed permanent resin material after thermal aging. J Prosthodont. 2023 Dec 15. Epub ahead of print. [CrossRef] [PubMed]
- Miura D, Miyasaka T, Aoki H, Aoyagi Y, Ishida Y. Correlations among bending test methods for dental hard resins. Dent Mater J. 2017 Jul 26;36(4):491-496. Epub 2017 Apr 18. [CrossRef] [PubMed]
- Al-Qahtani AS, Tulbah HI, Binhasan M, Abbasi MS, Ahmed N, Shabib S, Farooq I, Aldahian N, Nisar SS, Tanveer SA, Vohra F, Abduljabbar T. Surface Properties of Polymer Resins Fabricated with Subtractive and Additive Manufacturing Techniques. Polymers (Basel). 2021 Nov 24;13(23):4077. [CrossRef] [PubMed]
- Pereira LDE, Couto Neto MP, Pereira RG, Schneider LFJ. Influence of resin matrix on the rheology, translucency, and curing potential of experimental flowable composites for bulk-fill applications. Dent Mater. 2021 Jun;37(6):1046-1053. Epub 2021 Apr 14. [CrossRef] [PubMed]
- Lin CH, Lin YM, Lai YL, Lee SY. Mechanical properties, accuracy, and cytotoxicity of UV-polymerized 3D printing resins composed of Bis-EMA, UDMA, and TEGDMA. J Prosthet Dent. 2020 Feb;123(2):349-354. Epub 2019 Jun 12. [CrossRef] [PubMed]
- Wang L, Ni X. The effect of the inorganic nanomaterials on the UV-absorption, rheological and mechanical properties of the rapid prototyping epoxy-based composites. Polymer Bulletin. 2017 Jun 1;74(6):2063–79.
- Devlukia S, Hammond L, Malik K. Is surface roughness of direct resin composite restorations material and polisher-dependent? A systematic review. J Esthet Restor Dent. 2023 Sep;35(6):947-967. Epub 2023 Jul 17. [CrossRef] [PubMed]
- Alharbi N, Osman R, Wismeijer D. Effects of build direction on the mechanical properties of 3D-printed complete coverage interim dental restorations. J Prosthet Dent. 2016 Jun;115(6):760-7. Epub 2016 Jan 21. [CrossRef] [PubMed]
- Unkovskiy A, Bui PH, Schille C, Geis-Gerstorfer J, Huettig F, Spintzyk S. Objects build orientation, positioning, and curing influence dimensional accuracy and flexural properties of stereolithographically printed resin. Dent Mater. 2018 Dec;34(12):e324-e333. Epub 2018 Oct 4. [CrossRef] [PubMed]
- Väyrynen VO, Tanner J, Vallittu PK. The anisotropicity of the flexural properties of an occlusal device material processed by stereolithography. J Prosthet Dent. 2016 Nov;116(5):811-817. Epub 2016 Jun 14. [CrossRef] [PubMed]
- Alharethi, NA. Evaluation of the Influence of Build Orientation on the Surface Roughness and Flexural Strength of 3D-Printed Denture Base Resin and Its Comparison with CAD-CAM Milled Denture Base Resin. Eur J Dent. 2024 Feb;18(1):321-328. Epub 2023 Jun 9. [CrossRef] [PubMed]
- Daher R, Ardu S, di Bella E, Krejci I, Duc O. Efficiency of 3D printed composite resin restorations compared with subtractive materials: Evaluation of fatigue behavior, cost, and time of production. J Prosthet Dent. 2024 May;131(5):943-950. Epub 2022 Nov 1. [CrossRef] [PubMed]
- Della Bona A, Cantelli V, Britto VT, Collares KF, Stansbury JW. 3D printing restorative materials using a stereolithographic technique: a systematic review. Dent Mater. 2021 Feb;37(2):336-350. Epub 2021 Jan 19. [CrossRef] [PubMed]
- Tsolakis IA, Gizani S, Panayi N, Antonopoulos G, Tsolakis AI. Three-Dimensional Printing Technology in Orthodontics for Dental Models: A Systematic Review. Children (Basel). 2022 Jul 23;9(8):1106. [CrossRef] [PubMed]
- van Dijken, JW. Direct resin composite inlays/onlays: an 11 year follow-up. J Dent. 2000 Jul;28(5):299-306. [CrossRef] [PubMed]
- Pallesen U, Qvist V. Composite resin fillings and inlays. An 11-year evaluation. Clin Oral Investig. 2003 Jun;7(2):71-9. Epub 2003 May 10. [CrossRef] [PubMed]
- Cetin AR, Unlu N, Cobanoglu N. A five-year clinical evaluation of direct nanofilled and indirect composite resin restorations in posterior teeth. Oper Dent. 2013 Mar-Apr;38(2):E1-11. Epub 2012 Dec 5. [CrossRef] [PubMed]
Figure 1.
Design of the specimens in CAD software and import into the software for 3D printing: (a) bar. (b) disc. (c) slash 90°. (d) bar 45°. (e) bar 0°. (f) disc at 0°, 45°, and 90°. (g) Anycubic Photon D2 printer.
Figure 1.
Design of the specimens in CAD software and import into the software for 3D printing: (a) bar. (b) disc. (c) slash 90°. (d) bar 45°. (e) bar 0°. (f) disc at 0°, 45°, and 90°. (g) Anycubic Photon D2 printer.
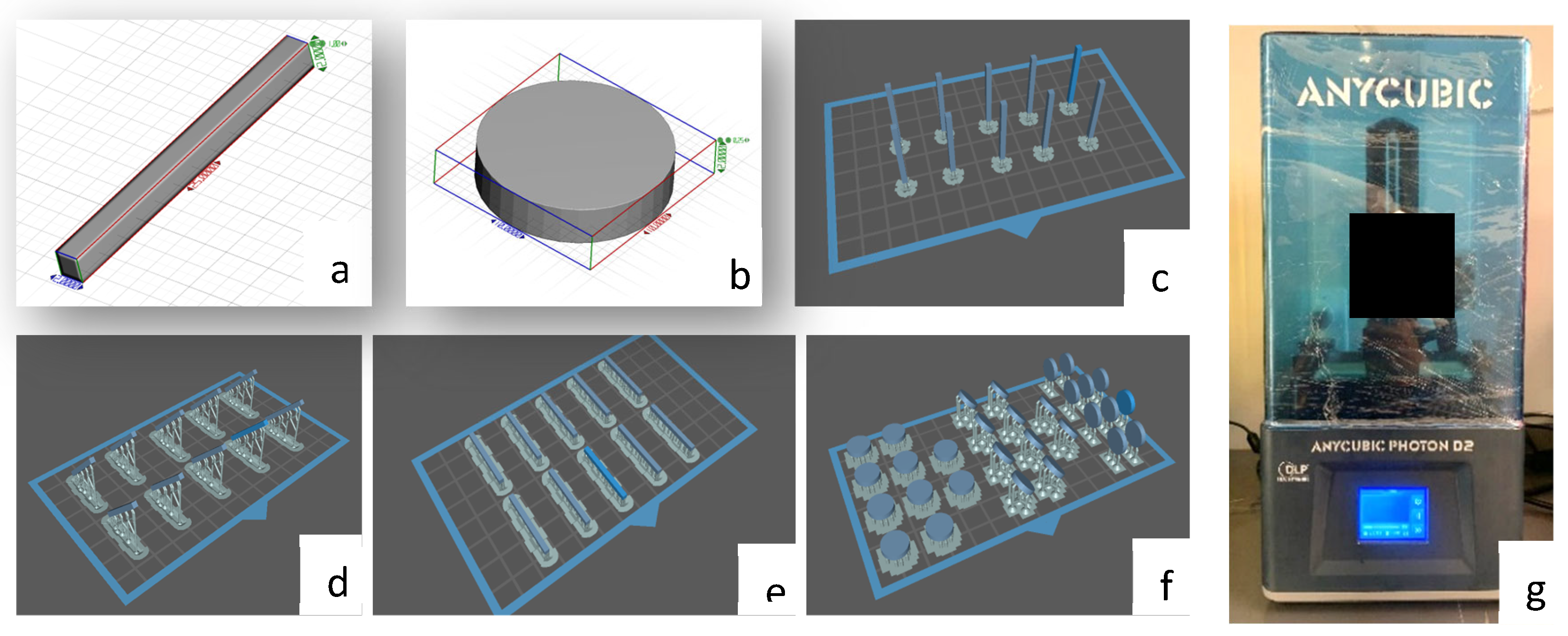
Figure 2.
Post-processing equipment: (a) Form Wash washer. (b) Isopropyl alcohol in the washer. (c) Form Cure light booth. (d) post-curing in UV light.
Figure 2.
Post-processing equipment: (a) Form Wash washer. (b) Isopropyl alcohol in the washer. (c) Form Cure light booth. (d) post-curing in UV light.
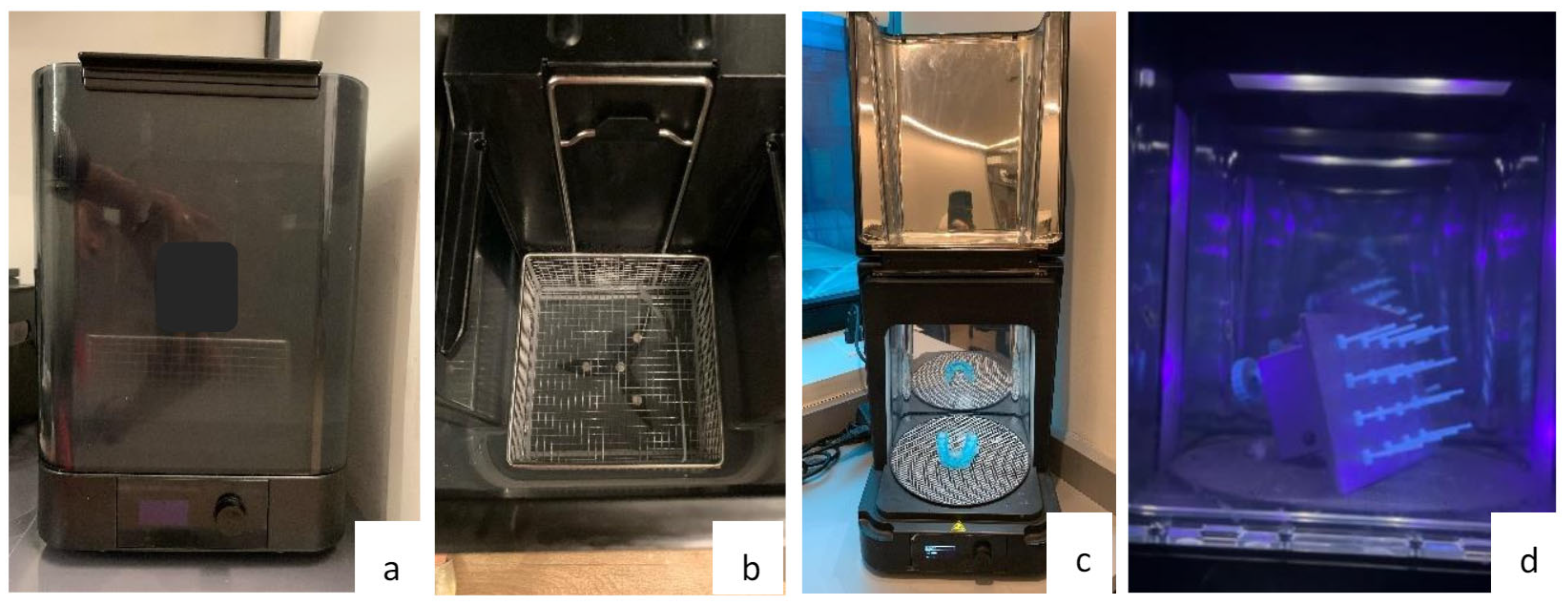
Figure 3.
silicone molds: (a) molds for bar and disc. (b) conventional composite resin condensed in the molds. (c) photoactivation of specimens in conventional composite resin.
Figure 3.
silicone molds: (a) molds for bar and disc. (b) conventional composite resin condensed in the molds. (c) photoactivation of specimens in conventional composite resin.
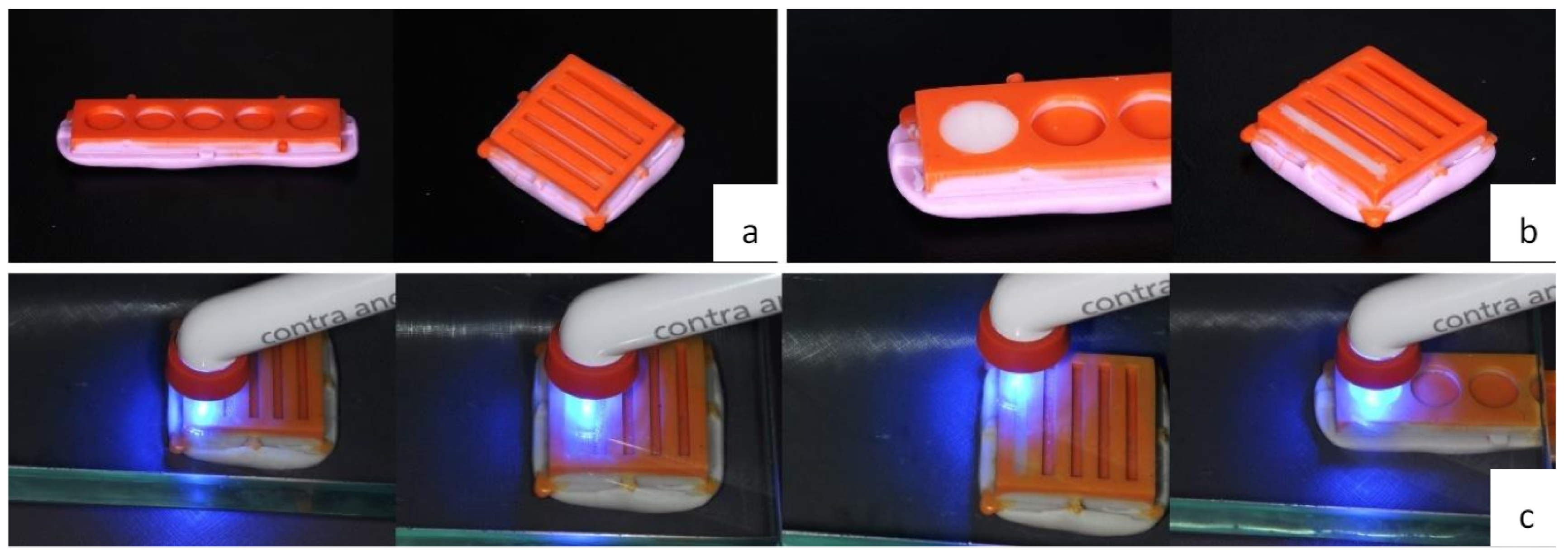
Figure 4.
Multi-axis graph showing average values of flexural strength, roughness, and microhardness according to 3D printing orientation.
Figure 4.
Multi-axis graph showing average values of flexural strength, roughness, and microhardness according to 3D printing orientation.
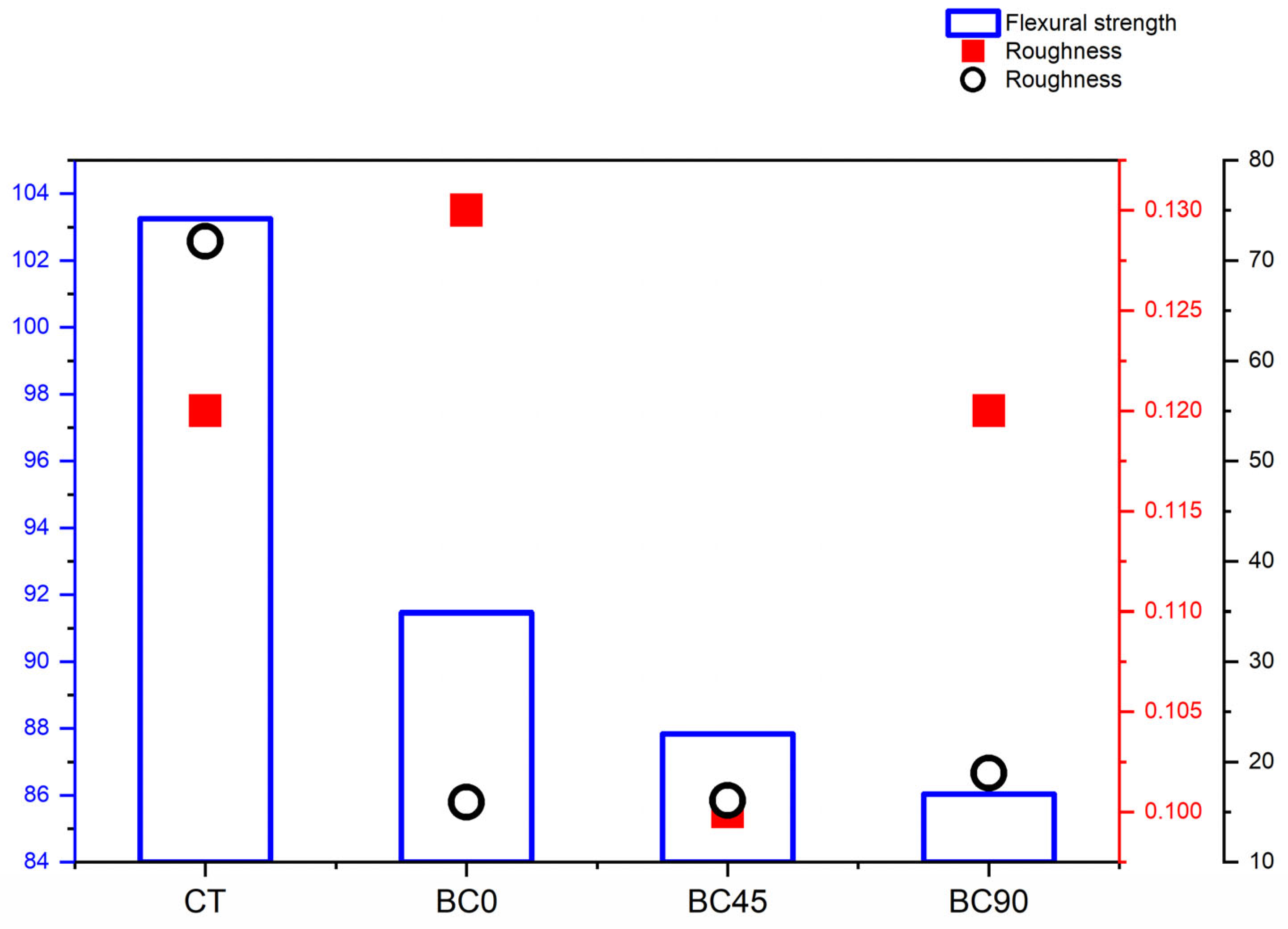

Table 1.
Materials used, composition, and batch.
| Material | Composition | Lote |
| Forma Resin (Ultradent from Brazil) | Bis-GMA; Bis-EMA; TEGDMA; B HT; PEGDMA; UDMA; Ytterbium trifluoride; fillers based on silane-treated ceramics, silanized silica, silanized silica-zirconium oxide and barium glass. | D0IEU |
| Prizma 3D Biocrown (Makertech Labs) |
UDMA > 40%; other methacrylated monomers > 20%; TPO <3%; Mixed Silanized Zirconia Oxide <10%; other filler particles (silanized silicas, nano, and micro barium glass) <25%; Pigments <2%; Blockers, stabilizers, and coactivators <2%. | 209623 |
* Bis-GMA: bisphenol A glycidyl methacrylate; BIS-EMA: Bisphenol A/ethylene glycol/methyl dimethacrylate; TEGDMA: Triethylene glycol dimethacrylate; BHT: butyl hydroxytoluene; PEGDMA: Polyethylene glycol dimethacrylate; UDMA: Urethane dimethacrylate; TPO: Trimethylbenzoyl-diphenyl phosphine oxide.
Table 2.
Mean values (standard deviation) and 95% confidence interval (95%CI) of the groups evaluated.
Table 2.
Mean values (standard deviation) and 95% confidence interval (95%CI) of the groups evaluated.
| Mean (Standard deviation) | IC95% | ||||
| Lower Bound | Upper Bound | ƞ2 parcial | |||
| Flexural Strength (Mpa) | CT | 103.26 (13.84)A | 93.35 | 113.16 | 0.386 |
| BC0 | 91.46 (7.83)B | 85.86 | 97.06 | ||
| BC45 | 87.83 (5,56)B | 83.85 | 91.81 | ||
| BC90 | 86.03 (5.89)B | 81.81 | 90.24 | ||
| Surface roughness (µm) | CT | 0.12 (0.02)A | 0.10 | 0.13 | |
| BC0 | 0.13 (0.04)A | 0.10 | 0.17 | ||
| BC45 | 0.10 (0.02)A | 0.09 | 0.12 | ||
| BC90 | 0.12 (0.05)A | 0.08 | 0.16 | ||
| Microhardness (VHN) | CT | 71.93 (2.51)A | 70.13 | 73.73 | |
| BC0 | 15.97 (1.68)B | 14.77 | 17.18 | 0.995 | |
| BC45 | 16.15 (1.55)B | 15.04 | 17.26 | ||
| BC90 | 18.89 (1.51)C | 17.80 | 19.98 | ||
* Statistically significant difference (P <0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



