
Submitted:
25 June 2024
Posted:
27 June 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Knowing the number of cases of an epidemic is the first function of epidemiological surveillance. An important underreporting of cases was observed in many places during the first wave of COVID-19 pandemic. To estimate this underreporting in the COVID-19 outbreak of Borriana (Valencia Community, Spain), during “Falles” mass gathering events in March 2020, a cross-sectional study was performed in June 2020 querying public health register. Logistic regression models were used. From a total of 468 symptomatic COVID-19 cases diagnosed in the outbreak by anti-SARS-CoV-2 serology, 36 cases were reported (7.7%), thus an underreporting of 92.3% (95% Confidence Interval [CI] 89.5%-94.6%), 13 unreported cases for every reported case. Only positive SARS-CoV-2 polymerase chain reaction cases were predominantly reported due to a limited testing capacity and following a national protocol. Significant factors associated with underreporting were no medical assistance for COVID-19 disease, adjusted odds ratio [aOR] 10.83 (95% CI 2.49-47.11), no chronic illness, aOR=2.81 (95% CI 1.28-6.17), middle and lower social classes, aOR=3.12 (95% CI 1.42-6.85), younger age, aOR=0.97 (95% CI 0.94-0.99), shorter duration of illness, aOR=0.98 (95% CI 0.97-0.99). To improve surveillance, studies of representative population samples are necessary to estimate the magnitude of future epidemics, and novel approaches are recommended.
Keywords:
COVID-19
; SARS-CoV-2
; underreporting
; cross-sectional
; epidemiological surveillance
; factors
1. Introduction
Knowing the number of cases of an epidemic is the first and crucial function of epidemiological surveillance meaning an accurate reporting of cases to public health authorities to take adequate measures to tackle an epidemic: “information is for action” [1,2].To measure the magnitude of the pandemic and their evolution, a typical surveillance of the COVID-19 pandemic was initially based on the reporting of cases, hospitalizations, mortality, and case-fatality. However, during the first wave of the COVID-19 pandemic, a substantial underreporting of cases and deaths was observed in many places with extensive variations [3,4,5,6,7].
This underreporting, considering underestimation for some authors [8], included under-ascertainment at community-level and underreporting at health care level, depended on multiple factors such as proportion of mild and asymptomatic cases, public health and healthcare system, demographic characteristics, socio-economic development and political systems [9,10,11].
Different methods to estimate underreporting of COVID-19 cases and deaths have been used, including case-fatality and mortality rates, hospitalization rates, syndromic surveillance, mathematical models from reported cases, SARS-CoV-2 screening surveys, seroprevalence surveys and online open surveys [12,13,14,15,16,17,18,19].COVID-19 seroprevalence surveys are based on the determination of anti-SARS-CoV-2 antibodies and can measure symptomatic and asymptomatic cases in large population samples [20,21,22,23]. In addition, it is of special interest in preparedness to future epidemics to adopt specific measures to know the causes and factors associated with the underreporting during the first wave of the COVID-19 pandemic.
In this context, the COVID-19 outbreak associated with the mass gathering events (MGEs) of Falles Festival in Borriana, Valencia Community (Spain), occurred between 6 and 10 March 2020 before lockdown took place. During May and June 2020, a population-based retrospective cohort study of a representative sample of exposed population, the Borriana COVID-19 cohort, was carried out to estimate the incidence of COVID-19 and its association with these MGEs, and a seroprevalence survey of anti-SARS-CoV-2 antibodies was performed [24].
Considering that few seroprevalence surveys on the community level have been made during the first wave of the COVID-19 pandemic and its usefulness for prepared of future epidemic, the objective of this study was to estimate the reported COVID-19 cases by the health authorities in the Borriana outbreak in March 2020, and those factors associated with the underreporting.
2. Materials and Methods
2.1. Study Cross-Sectional
A population-based cross-sectional study was designed, and was implemented by the Public Health Center of Castellon and the Hospital de la Plana in Vila-real, Valencia Community (Spain). The study population was the Borriana COVID-19 cohort, and detailed information of this cohort has been described by Domènech and co-authors [24]. The study took place from January to June 2020 and 536 laboratory-confirmed COVID-19 cases through seroprevalence survey with anti-SARS-CoV-2 IgM/IgG Nucleocapsid antibodies were diagnosed. Asymptomatic cases were excluded. The laboratory technique used was a qualitative detection of antibodies against SARS-CoV-2 by an electrochemiluminescence immunoassay (ECLIA) (Elecsys® Anti-SARS-CoV-2, Roche Diagnostics) in the Clinical Analysis and Microbiology Service of the Hospital de la Plana [25]. In addition, a telephone survey to obtain information about demographic characteristics, occupations, lifestyles, chronic illnesses, symptoms of the COVID-19 disease, illness duration and received medical assistance for COVID-19 disease was performed by the health staff of Public Health Center, Emergency Service of Hospital de la Plana, and the Health Centers of Borriana, Vila-real, Onda and La Vall d’Uixò all them located at the Health Department of la Plana in Vila-real, Castellon.
To obtain the reported COVID-19 cases, official register of notification COVID-19 cases at the Public Health Center of Castellon was queried, including the informatics application of epidemiological surveillance analysis (AVE), considering the period January-June Following a national protocol, patients with suspected SARS-CoV-2 infection were confirmed by a positive SARS-CoV-2 polymerase chain reaction (PCR) test or other adequate molecular test, and being those confirmed cases, most of our reported cases [26,27]. PCR tests COVID-19 cases were performed at Microbiology Service of the Hospital de la Plana by multiple techniques and manufacturers due to the shortage of tests and material at that time.
2.2. Statistical Analysis
To describe the characteristic of the study population, we calculated percentages, means and standard deviations. Comparisons of variables between reported and underreported COVID-19 cases were made by Chi2 and Fisher exact tests for qualitative variables and Kruskal-Wallis for quantitative variables.
We defined underreported COVID-19 cases as dependent variable and a predictive variable was has received medical assistance for COVID-19 disease. Independent variables were age, sex, chronic illnesses, COVID-19 illness duration in days, occupation as social class to upper class (group I higher managerial and professional occupations) versus middle and lower social classes (groups II –VI intermediate and skilled non-manual and manual occupations) [28], and lifestyles, including body mass index (kg/m2), smoking habit, alcohol intake, habitual physical exercise and following a nutritional diet. Logistic regression models were applied to study the associations between underreporting COVID-19 cases and predictive and independent variables by odds ratio (OR) with a 95% Confidence Interval (CI). To control potential confounder factors a study of medical literature was addressed, and Directed Acyclic Graphics (DAGs) were employed [29]. Figure 1 describes the relations between the exposure (COVID-19 medical assistance), ancestors of exposure, and the outcome (COVID-19 reported). Statistical program Stata® 14 version 2 was used for all the calculation.
The study had the approval of the director of the Public Health Center of Castellon and the management of the Health Department of La Plana, where the COVID-19 outbreak took place. On the other hand, this study was exempt from the Ethics Review Board approval´s protocol following the Spanish legislation as part of the public health surveillance of the COVID-19 pandemic.
3. Results
Of a total 536 laboratory-confirmed symptomatic COVID-19 cases in the outbreak, 67 asymptomatic cases were excluded, and one case showed missing information. As a result of this, 468 cases were included in the study (99.8%). Only 36 (7.7%) cases were reported as COVID-19 cases by Public Health Center, thus case underreporting was 92.3% (95% CI 89.5%-94.6%), 13 unreported cases for every reported case. 34 cases (94.4%) were confirmed by PCR tests, and 2 cases were confirmed through anti-SARS-CoV-2 antibody serology. All the unreported cases were laboratory confirmed only by anti-SARS-CoV-2 antibody serology.
Characteristics of reported and unreported COVID-19 cases are shown in Table 1 Unreported cases were younger than reported cases (p=0.001), a higher proportion without medical assistance for COVID-19 disease, 54.6% versus 5.6% (p=0.000), and shorter illness duration, 10.5±14.9 days versus 24.2±21.9 (p=0.000). Not having a chronic illness was higher in the unreported cases 68.3% versus 38.8% (p=0.001). Middle and lower social classes were predominant in the unreported cases, 87.4% versus 69.4% (p=0.009). Other factors concerting lifestyles such as obesity, smoking, alcohol intake, habitual physical exercise, and following a nutritional diet were not associated with the underreporting.
Crude and adjusted logistic regression analysis of factors associated with underreporting is shown in Table 2 Significant factors associated with underreporting were younger age (aOR=0.97 95% CI 0.94-0.99), no medical assistance for COVID-19 disease (aOR=10.83 95% CI 2.49-47.11), shorter durationn illness in days (aOR=0.98 95% CI 0.97-0.99), and not having a chronic illness (aOR=2.81 95% CI 1.28-6.17). In addition, middle and lower social classes were significantly more related to underreporting versus higher class (aOR=3.12 95% CI 1.42-6.85). Lifestyle factors were not significantly associated with underreporting COVID-19 cases.
4. Discussion
Our results suggest that the underreporting of symptomatic COVID-19 cases in the Borriana COVID-19 cohort was very high during the first wave of COVID-19 pandemic. Factors associated with this underreporting of cases were younger age, no medical assistance for COVID-19 disease, shorter illness duration, not suffering from a chronic illness, and belonging to middle and lower social classes.
This COVID-19 outbreak took place during mass gathering events with a massive exposition of SARS-CoV-2, and an attack rate of 39.2%. [24].This exposition occurred between 6 and 10 March, five days before the lockdown was enforced. A higher proportion of cases had a milder illness, the medical assistance was limited, and cases were not reported to epidemiological surveillance in line with a Spanish official publication of the first wave COVID-19 pandemic [27]. This type of COVID-19 outbreak may illustrate how the COVID-19 epidemic spread in some places, and mass gathering events of last February and early March could have played an important role in Spain and in other countries [30,31,32,33,34,35].
Estimations of underreporting of cases and deaths presented important geographic variations, but this underreporting was very elevated during the first wave of the COVID-19 pandemic in most countries [4,36,37,38,39]. In seroprevalence studies, different methodologies and analytic techniques have been employed to estimate the dimensions of the COVID-19 pandemic and the proportion of asymptomatic cases [23,40].Considering some population-based seroprevalence surveys with detection anti-SARS-CoV-2 antibodies, the number of unreported cases for every reported COVID-19 case presented considerable differences: 2.8 cases in Santiago de Chile [41] 4 cases in Munich [42], 5 cases in Ethiopia [43], 6.5 cases in the United States [20], 8.9 cases in Finland, [44], 11.6 cases in Geneva [21], and 25.5 cases in Eswatini, Southern Africa [45]. Our results are consistent with the study of Sierra and co-authors [46], where the sensitivity of Spanish surveillance system was 9.7% (95% CI 8.96-10.29) with 13 unreported cases for every reported case following the national seroprevalence survey of Pollan and coauthors [22].
We can address some caused in Spain, responsible for the low reporting considering an unprecedented situation with a new disease and the countrywide lockdown. The causes may include the high proportion of milder and asymptomatic infections, an insufficient following of infected cases and contacts, restrictions and barriers for medical care access, limited capacity of SARS-CoV-2 laboratory testing, prioritization of medical assistance and laboratory SARS-CoV-2 PCR testing for patients with severe illness, predominant reported COVID-19 cases with positivity SARS-CoV-2 PCR, restriction in population mobility, and social isolation in a context of subordinate public health [4,11,27,47]. This underreporting could be associated with a delay of the health authorities to carry out mitigation strategies [48]. An official government document [49] indicated that the Spanish system of health was not sufficiently prepared for the COVID-19 pandemic, not having stock of material necessary to tackle a pandemic respiratory virus, the weakness of information systems and the insufficient diagnostic recourses. In addition, the healthcare system was overwhelmed and critical services were saturated during this first wave [27].
Factors associated with underreporting such as, no medical assistance for COVID-19 disease, younger age without a chronic illness, and shorter illness duration suggest a milder illness and few severe cases; which aligns with other studies[42,45,50]. In addition, patients belonging to middle and lower social classes were more underreported than upper class cases suggesting better access to healthcare to the latter. Less reporting of COVID-19 cases in manual occupations as waiter or taxi-has been observed in Norway [51]. Lifestyle factors were not associated with underreporting, but in some studies, obesity was associated with higher possibility to be tested and to be COVID-19 positive [52].
Our study presents some strengths and limitations. As strengths, we include that the Borriana COVID-19 cohort was a representative sample of the population exposed to SARS-CoV-2 during the Falles Festival with a high participation. This study was carried out during May-June 2022 in the first wave of the epidemic, and control of potential confounding factors was done by logistic regression models, sensitivity and specificity of the technique for Anti-SARS-CoV-2 antibodies were elevated, and asymptomatic COVID-19 cases were excluded in the estimation. Our proportion of asymptomatic cases was low, 12%, compared with reviews and meta-analysis studies [53]. As limitations, we include that the underreporting was studied during a COVID-19 outbreak, this is an unusual situation, and considering the elapsed time between the exposition and the start of the study, some recall and misclassification biases could be occurring. On the other hand, anti-SARS-CoV-2 antibodies decline over time. However, the study was implemented three months after the mass gathering events, and a 99% of anti-SARS-CoV-2 antibody persistence was found in a new study of this cohort in October 2020 [54].
In the public health arena many voices have indicated the necessity of a change in order to improve the surveillance of infectious diseases [46,55,56,57,58], and a critical review of the surveillance methods was performed in England [59]. In addition, considering that the possibility of future epidemics is not remote, novel approaches to surveillance used during the COVID-19 pandemic are recommended. Five areas could be contemplated. First, community approach with continued studies of representative population samples and household survey, including studies of incidence of infectious diseases and serological surveys, attendance to emergency departments, hospitalizations, primary health care, syndromic surveillance and high risk groups determination [59,60,61].Secondly, digital surveillance which experimented a high developing during the COVID-19 pandemic [62], including online self-reported population survey or digital apps[63], population-based surveillance application [64], mobile apps with different uses such as risk assessment and contact tracing [65,66], and big data and infodemiology to obtain useful public health information [67]. Thirdly, mathematical models to estimate the true dimensions of epidemics, including the asymptomatic infections with appliance of artificial intelligence, could be useful to complete the traditional epidemiological [68,69]. Some practical approaches are being implemented as a new surveillance index [70], and calculated refined reproduction number [71]. Fourthly, wastewater surveillance with determining the presence of SARS-CoV-2 in sewage system has had a considerable development considering its use in epidemic detection [72,73]. And lastly, an area of particular interest is Genomic surveillance that permits to detect new viral variants to make valuable use against SARS-CoV-2 in household transmission, outbreaks detections and national variants surveillance [74,75,76,77,78]. In addition, cycle threshold of SARS-CoV-2 RNA PCR results could be useful to forecast COVID-19 epidemics [79].
5. Conclusions
During the first wave of COVID-19 pandemic, the underreporting of COVID-19 cases was very high, indicating insufficient preparedness for large epidemics. New approaches to epidemiological surveillance are necessary to tackle future epidemics.
Author Contributions
Conceptualization, S.D.-M, M.R.P.-S., A.A.-P., and M.S.-U.; methodology, A.A.-P., S.D.-M., M.R.P.-S., D.S.-T., J.C.-S.; M.G-F., C.N.-R., O.P.-O., and M.A.R.-G.; software, A.A.-P., M.R.P.-S., and C.D.-L.; validation, S.D.-M., D.S.-T., O.P.-O., P.S.-M., M.G.-F.; formal analysis, A.A.-P., and M.R.P.-S.; investigation, S.D.-M., M.A.R.-G., D.S.-T., A.D.-G., M.S.-U., P.S.-M., R.B.-G., J.C.-S., M.G.-F., L.L.-D., C.N.-R.; O.P.-O., I.A.-G., C.D.-L., and A.A.-P. ; resources, S.D.-M., M.G.-F., L.L.-D., and O.P.-O.; data curation, A.D.-G., M.R.P.-S., M.S.-U., J.C.-S., C.D.-L., and A.A.-P.; writing—original draft preparation, A.A.-P; writing—review and editing, A.A.-P., O.P.-O., M.S.-U., S.D.-M., and D.S.-T.; visualization, R.B.-G., P.S.-M., D.S.-T., I.A.-G., and J.C.-S.; supervision, L.L.-D., and S.D.-M.; project administration, S.D.-M., L.L.-D. I.A.-G., and A.A.-P; funding acquisition, S.D.-M., and A.A.-P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. The study was part of the epidemiological surveillance of the COVID-19 outbreak in the Falles Festival in Borriana, which was exempted from Ethics Review Board approval’s protocol according to the Spanish legislation and regulations, including [80] the General Law of Health, [81] the Law of Cohesion and Quality of the National System of Health, and [82] the Law General of Public Health. .
Informed Consent Statement
All participants or the parents of minors provided the informed written consent to be included in the study.
Data Availability Statement
Data of the study can be consulted if the authors are requested.
Acknowledgments
We thank the participants of the Borriana COVI-19 cohort and the Borriana’s Falles organization for the support and help that made it possible to perform this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Thacker, S.B.; Birkhead, G. Surveillance. In Gregg, M.B. Field Epidemiology. Second edition. Oxford University Press New York 2020, pp. 26–50.
- Waldman, R. Epidemiological surveillance: information is for action. Public Health Action 2020;10, 86.
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Lau, H.; Khosrawipour, T.; Kocbach, P.; Ichii, H.; Bania, J.; Khosrawipour, V. Evaluating the massive underreporting and undertesting of COVID-19 cases in multiple global epicenters. Pulmonology 2021, 27, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Russell, T.W.; Golding, N.; Hellewell, J.; Abbott, S.; Wright, L.; Pearson, C.A.B.; van Zandvoort, K.; Jarvis, C.I.; Gibbs, H.; Liu, Y.; et al. Reconstructing the early global dynamics of under-ascertained COVID-19 cases and infections. BMC Med 2020, 18, 332. [Google Scholar] [CrossRef] [PubMed]
- Byambasuren, O.; Dobler, C.C.; Bell, K.; Rojas, D.P.; Clark, J.; McLaws, M.L.; Glasziou, P. Comparison of seroprevalence of SARS-CoV-2 infections with cumulative and imputed COVID-19 cases: Systematic review. PLoS One 2021, 16, e0248946. [Google Scholar] [CrossRef] [PubMed]
- Jayara,j V. J.; Ng, C.W.; Bulgiba, A., Appannan, M.R.; Rampal, S. Estimating the infection burden of COVID-19 in Malaysia. PLoS Negl Trop Dis 2022, 16, e0010887. [Google Scholar]
- Gibbons, C.L.; Mangen, M.J.; Plass, D.; Havelaar, A.H.; Brooke, R.J.; Kramarz, P.; Peterson, K.L.; Stuurman, A.L.; Cassini, A.; Fèvre, E.M.; et al. Measuring underreporting and under-ascertainment in infectious disease datasets: a comparison of methods. BMC Public Health 2014, 14, 147. [Google Scholar] [CrossRef] [PubMed]
- Ricoca-Peixoto, V.; Nunes, C.; Abrantes, A. Epidemic Surveillance of Covid-19: Considering Uncertainty and Under-Ascertainment. Port J Public Health 2020, 38, 1–7. [Google Scholar] [CrossRef]
- Ibrahim, N.K. Epidemiologic surveillance for controlling Covid-19 pandemic: types, challenges and implications. J Infect Public Health 2020, 13, 1630–1638. [Google Scholar] [CrossRef]
- Meadows, AJ, Oppenheim, B. ; Guerrero, J.; Ash, B.; Badker, R.; Lam, C.K.; Pardee, C.; Ngoon, C.; Savage, P.T.; Sridharan, V.; et al. Infectious disease underreporting is predicted by country-level preparedness, politics, and pathogen severity. Health Secur 2022, 20, 331–338.
- Albani, V.; Loria, J.; Massad, E.; Zubelli, J. COVID-19 underreporting and its impact on vaccination strategies. BMC Infect Dis 2021, 21, 1111. [Google Scholar] [CrossRef]
- You, C.; Gai, X.; Zhang, Y.; Zhou, X. Determining the Covertness of COVID-19 - Wuhan, China, China CDC Wkly 2021, 3, 170–173. 3.
- Havers, F.P.; Reed, C.; Lim, T.; Montgomery, J.M.; Klena, J.D.; Hall, A.J.; Fry, A.M.; Cannon, D.L.; Chiang, C.F.; Gibbons, A.; et al. Seroprevalence of antibodies to SARS-CoV-2 in 10 sites in the United States, -May 12, JAMA Intern Med 2020, 180, 1576–1586. 180, 23 March.
- Alves, T.H.E.; de Souza, T.A.; Silva, S.A.; Ramos, N.A.; de Oliveira, S.V. Underreporting of death by COVID-19 in Brazil's second most populous state. Front Public Health 2020, 8, 578645. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Agundez, A.; Ojo, O.; Hernández-Roig, H.A.; Baquero, C.; Frey, D.; Georgiou, C.; Goessens, M.; Lillo, R.E.; Menezes, R.; Nicolaou, N.; et al. Estimating the COVID-19 prevalence in Spain with indirect reporting via open surveys. Front Public Health 2021, 9, 658544. [Google Scholar] [CrossRef]
- Desta, B.N.; Ota, S.; Gournis, E.; Pires, S.M.; Greer, A.L.; Dodd, W.; Majowicz, S.E. Estimating the under-ascertainment of COVID-19 cases in Toronto, Ontario, March to May J Public Health Res 2023, 12, 22799036231174133.
- Milanesi, S.; De Nicolao, G. Correction of Italian under-reporting in the first COVID-19 wave via age-specific deconvolution of hospital admissions. PLoS One 2023, 18, e0295079. [Google Scholar] [CrossRef]
- Pullano, G.; Di Domenico, L.; Sabbatini, C.E.; Valdano, E.; Turbelin, C.; Debin, M.; Guerrisi, C.; Kengne-Kuetche, C.; Souty, C.; Hanslik, T.; et al. Underdetection of cases of COVID-19 in France threatens epidemic control. Nature 2021, 590, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Angulo, F.J.; Finelli, L.; Swerdlow, D.L. Estimation of US SARS-CoV-2 infections, symptomatic infections, hospitalizations, and deaths using seroprevalence surveys. JAMA Netw Open 2021, 4, e2033706. [Google Scholar] [CrossRef] [PubMed]
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; De Ridder, D.; Petrovic, D; Schrempft, S. ; Marcus K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): a population-based study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Li, Z.; Guan, X.; Mao, N.; Luo, H.; Qin, Y.; He, N.; Zhu, Z.; Yu, J.; Li, Y.; Liu, J.; et al. Antibody seroprevalence in the epicenter Wuhan, Hubei, and six selected provinces after containment of the first epidemic wave of COVID-19 in China. Lancet Reg Health West Pac 2021, 8, 100094. [Google Scholar] [CrossRef] [PubMed]
- Domènech-Montoliu, S.; Pac-Sa, M.R.; Vidal-Utrillas, P.; Latorre-Poveda, M.; Del Rio-González, A.; Ferrando-Rubert, S.; Ferrer-Abad, G.; Sánchez-Urbano, M.; Aparisi-Esteve, L.; Badenes-Marques, G.; et al. "Mass gathering events and COVID-19 transmission in Borriana (Spain): A retrospective cohort study". PLoS One 2021, 16, e0256747. [Google Scholar] [CrossRef]
- Egger, M.; Bundschuh, C.; Wiesinger, K.; Gabriel, C.; Clodi, M.; Mueller, T.; Dieplinger, B. Comparison of the Elecsys® Anti-SARS-CoV-2 immunoassay with the EDI™ enzyme linked immunosorbent assays for the detection of SARS-CoV-2 antibodies in human plasma. Clin Chim Acta 2020, 509, 18–21. [Google Scholar] [CrossRef]
- Boletín Oficial del Estado (BOE) Orden SND/404/2020, de 11 de mayo, de medidas de vigilancia epidemiológica de la infección por SARS-CoV-2 durante la fase de transición hacia una nueva normalidad (State offical newsletter (BOE) Order SND/404/2020 of May 11, on epidemiological surveillance measures for SARS-CoV-2 infection during the transition pahe to a new normality) . https://www.boe.es/eli/es/o/2020/05/11/snd404 (accessed on 28 February 2023).
- Working group for the surveillance and control of COVID-19 in Spain. The first wave of the COVID-19 pandemic in Spain: characterisation of cases and risk factors for severe outcomes, as at 27 April Euro Surveill 2020, 25, 2001431.
- Barry, A.M; Yuill, C. Understanding the sociology of health: An introduction. Second edition. Sage Publications Ltd London 2008; pp. 91–118.
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liskiewicz, M.; Ellison, G.T. Robust causal inference using directed acyclic graphs: the R package 'dagitty'. Int J Epidemiol 2016, 45, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- González-Val, R.; Marcén, M. Mass gathering events and the spread of infectious diseases: Evidence from the early growth phase of COVID-Econ Hum Biol 2022, 46, 101140. 46.
- Brandl, M.; Selb, R.; Seidl-Pillmeier, S.; Marosevic, D.; Buchholz, U.; Rehmet, S. Mass gathering events and undetected transmission of SARS-CoV-2 in vulnerable populations leading to an outbreak with high case fatality ratio in the district of Tirschenreuth, Germany. Epidemiol Infect 2020, 148, e252. [Google Scholar] [CrossRef] [PubMed]
- Herng, L.C.; Singh, S.; Sundram, B.M.; Zamri, A.S.S.M.; Vei, T.C.; Aris, T.; Ibrahim, H.; Abdullah, N.H.; Dass, S.C.; Gill, B.S. The effects of super spreading events and movement control measures on the COVID-19 pandemic in Malaysia. Sci Rep 2022, 12, 2197. [Google Scholar] [CrossRef] [PubMed]
- Rocha, I.C.N.; Pelayo, M.G.A.; Rackimuthu, S. Kumbh Mela religious gathering as a massive superspreading event: Potential culprit for the exponential surge of COVID-19 cases in India. Am J Trop Med Hyg 2021, 105, :868–871. [Google Scholar] [CrossRef] [PubMed]
- Stange, M.; Mari, A.; Roloff, T.; Seth-Smith, H.M.; Schweitzer, M.; Brunner, M.; Leuzinger, K.; Søgaard, K.K.; Gensch, A.; Tschudin-Sutter, S, et al. SARS-CoV-2 outbreak in a tri-national urban area is dominated by a B.1 lineage variant linked to a mass gathering event. PLoS Pathog 2021, 17, e1009374. [Google Scholar] [CrossRef] [PubMed]
- Phalippou, L.; Zhang, D. The cost of mass gatherings during a pandemic. SSM Popul Health 2023, 23, 101460. [Google Scholar] [CrossRef] [PubMed]
- Millimet, D.L.; Parmeter, C.F. COVID-19 severity: A new approach to quantifying global cases and deaths. J R Stat Soc Ser A Stat Soc 2022, 185, 1178–1215. [Google Scholar] [CrossRef] [PubMed]
- Krantz, S.G.; Rao, A.S.R.S. Level of underreporting including underdiagnosis before the first peak of COVID-19 in various countries: Preliminary retrospective results based on wavelets and deterministic modeling. Infect Control Hosp Epidemiol 2020, 41, 857–859. [Google Scholar] [CrossRef] [PubMed]
- Shang, W.; Wang, Y.; Yuan, J.; Guo, Z.; Liu, J.; Liu, M. Global excess mortality during COVID-19 pandemic: A systematic review and meta-analysis. Vaccines (Basel) 2022, 10, 1702. [Google Scholar] [CrossRef]
- Vandoros, S. Excess mortality during the Covid-19 pandemic: Early evidence from England and Wales. Soc Sci Med. 2020, 258, 113101. [Google Scholar] [CrossRef] [PubMed]
- Royo-Cebrecos, C.; Vilanova, D.; López, J.; Arroyo, V.; Pons, M.; Francisco, G.; Carrasco, M.G.; Piqué, J.M.; Sanz, S.; Dobaño, C.; et al. Mass SARS-CoV-2 serological screening, a population-based study in the Principality of Andorra. Lancet Reg Health Eur 2021, 5, 100119. [Google Scholar] [CrossRef]
- Vial, P.A.; González, C.; Apablaza, M.; Vial, C.; Lavín, M.E.; Araos, R.; Rubilar, P.; Icaza, G.; Florea, A.; Pérez, C.; et al. First wave of SARS-CoV-2 in Santiago Chile: Seroprevalence, asymptomatic infection and infection fatality rate. Epidemics 2022, 40, 100606. [Google Scholar] [CrossRef] [PubMed]
- Pritsch, M.; Radon, K.; Bakuli, A.; Le Gleut, R.; Olbrich, L.; Guggenbüehl-Noller, J.M.; Saathoff, E.; Castelletti, N.; Garí, M.; et al. Prevalence and risk factors of infection in the representative COVID-19 cohort Munich. Int J Environ Res Public Health 2021, 18, 3572. [Google Scholar] [CrossRef] [PubMed]
- Abdella, S.; Riou, S.; Tessema, M.; Assefa, A.; Seifu, A.; Blachman, A.; Abera, A.; Moreno, N.; Irarrazaval, F.; Tollera, G.; et al. Prevalence of SARS-CoV-2 in urban and rural Ethiopia: Randomized household serosurveys reveal level of spread during the first wave of the pandemic. EClinicalMedicine. 2021, 35, 100880. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, T.A.; Auranen, K.; Kulathinal, S.; Härkänen, T.; Melin, M.; Palmu, A.A.; Jokinen, J. Underreporting of SARS-CoV-2 infections during the first wave of the 2020 COVID-19 epidemic in Finland-Bayesian inference based on a series of serological surveys. PLoS One 2023, 18, e0282094. [Google Scholar] [CrossRef] [PubMed]
- Mutevedzi, P.C.; Lokotfwako, V.; Kwatra, G. , Maphalala, G.; Baillie, V.; Dlamini, L., Dlamini, S.; Mhlanga, F.; Dlamini, T.; Nhlabatsi, N.; et al. Prevalence and levels of anti-SARS-CoV-2 antibodies in the Eswatini population and subsequent severity of the fourth COVID-19 epidemic wave. COVID 2024, 4, 317–333. [Google Scholar] [CrossRef]
- Sierra-Moros, M.J.; Martínez-Sánchez, E.V.; Monge-Corella, S.; García-San Miguel, L.; Suárez-Rodríguez, B.; Simón-Soria, F. Lecciones de la vigilancia de la COVID-Necesidad urgente de una nueva vigilancia en salud pública. Informe SESPAS 2022. Gac Sanit 2022, 36 (Suppl 1), S68–S75. [Google Scholar] [CrossRef] [PubMed]
- Guillen, M.; Bardes Robles, I.; Bordera-Cabrera, E.; Acebes-Roldán, X.; Bolancé, C.; Jorba, D.; Moriña, D. Acute respiratory infection rates in primary care anticipate ICU bed occupancy during COVID-19 waves. PLoS One 2022, 17, e0267428. [Google Scholar] [CrossRef]
- Álvarez, I.C.; Orea, L.; Wall, A. Estimating the propagation of both reported and undocumented COVID-19 cases in Spain: a panel data frontier approximation of epidemiological models. J Product Anal 2023, 59, 259–279. [Google Scholar] [CrossRef]
- Hervada-Vidal, X; Pérez-Romero, C.; Rodríguez-Artalejo, F.; Urbanos-Garrido, R. Evaluación del desempeño del Sistema Nacional de Salud Español frente a la pandemia del COVID Lecciones de y para una pandemia. Ministerio de Sanidad Madrid 2023. https://www.sanidad.gob.es/areas/alertasEmergenciasSanitarias/alertasActuales/nCov/documentos/EVALUACION_DEL_DESEMPENO_DEL_SNS_ESPANOL_FRENTE_A_LA_PANDEMIA_DE_COVID-19.pdf (accessed on 6 May 2024).
- Omori, R.; Mizumoto, K.; Nishiura, H. Ascertainment rate of novel coronavirus disease (COVID-19) in Japan. Int J Infect Dis 2020, 96, 673–675. [Google Scholar] [CrossRef] [PubMed]
- Samant, Y.; Støver, M.; Haarberg, I.S.; Lohmann-Lafrenz, S.; Strømholm, T. Underreporting of work-related COVID-19 cases in Norway. New Solut 2023, 33, 149–153. [Google Scholar] [CrossRef]
- Wang, G.; Foney, D.M.; DiBari. J.; Hong, X.; Showell, N.; Kim, K.S.; Ji, H.; Pearson, C.; Mirolli, G.; Rusk, S.; Sharfstein, J.; et al. A prospective cohort study on the intersectionality of obesity, chronic disease, social factors, and incident risk of COVID-19 in US low-income minority middle-age mothers. Int J Obes (Lond) 2021, 45, 2577–2584. [Google Scholar] [PubMed]
- Alene, M.; Yismaw, L.; Assemie, M.A.; Ketema, D.B.; Mengist, B.; Kassie, B.; Birhan, T.Y. Magnitude of asymptomatic COVID-19 cases throughout the course of infection: A systematic review and meta-analysis. PLoS One 2021, 16, e0249090. [Google Scholar] [CrossRef] [PubMed]
- Domènech-Montoliu, S.; Puig-Barberà, J.; Pac-Sa, M.R.; Vidal-Utrillas, P.; Latorre-Poveda, M.; Del Rio-González, A.; Ferrando-Rubert, S.; Ferrer-Abad, G.; Sánchez-Urbano, M.; Aparisi-Esteve, L.; et al. Persistence of anti-SARS-CoV-2 antibodies six months after infection in an outbreak with five hundred COVID-19 cases in Borriana (Spain): A prospective cohort study. COVID 2021, 1, 71–82. [Google Scholar] [CrossRef]
- Kamalrathne, T.; Amaratunga, D.; Haigh, R.; Kodituwakku, L. Need for effective detection and early warnings for epidemic and pandemic preparedness planning in the context of multi-hazards: Lessons from the COVID-19 pandemic. Int J Disaster Risk Reduct 2023, 92, 103724. [Google Scholar] [CrossRef] [PubMed]
- Nuzzo, J.B. The United States' SARS-CoV-2 testing challenges underscore the need to improve surveillance ahead of the next health security crisis. Clin Chem 2021, 68, 30–32. [Google Scholar] [CrossRef]
- Han, Q.; Bragazzi, N.; Asgary, A.; Orbinski, J.; Wu, J.; Kong, J.D. Estimation of epidemiological parameters and ascertainment rate from early transmission of COVID-19 across Africa. R Soc Open Sci 2023, 10, 230316. [Google Scholar] [CrossRef]
- Farsalinos, K.; Poulas, K.; Kouretas, D.; Vantarakis, A.; Leotsinidis, M.; Kouvelas, D.; Docea, A.O.; Kostoff, R.; Gerotziafas, G.T.; Antoniou, M.N.; et al. Improved strategies to counter the COVID-19 pandemic: Lockdowns vs. primary and community healthcare. Toxicol Rep 2021, 8, 1–9. [Google Scholar] [CrossRef]
- Brainard, J.; Lake, I.R.; Morbey, R.A.; Jones, N.R.; Elliot, A.J.; Hunter, P.R. Comparison of surveillance systems for monitoring COVID-19 in England: a retrospective observational study. Lancet Public Health 2023, 8, e850–e858. [Google Scholar] [CrossRef]
- Ageron, F.X.; Hugli, O.; Dami, F.; Caillet-Bois, D.; Pittet, V.; Eckert, P.; Beysard, N.; Carron, P.N. Lessons from COVID-19 syndromic surveillance through emergency department activity: a prospective time series study from western Switzerland. BMJ Open 2022, 12, e054504. [Google Scholar] [CrossRef] [PubMed]
- Arnedo-Pena, A.; Guillen-Grima, F. Incidence and risk factors of the COVID-19 pandemic: An epidemiological approach. Epidemiologia 2023, 4, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.C.; Neumann, S.; Hopkins, S.; Kostopoulos, A.; Hagerman, L.; Dobbins, M. Changes to public health surveillance methods due to the COVID-19 pandemic: scoping review. JMIR Public Health Surveill 2024, 10, e49185. [Google Scholar] [CrossRef] [PubMed]
- Oliver, N.; Barber, X.; Roomp, K.; Roomp, K. Assessing the impact of the COVID-19 pandemic in Spain: Large-scale, online, self-reported population survey. J Med Internet Res 2020, 22, e21319. [Google Scholar] [CrossRef] [PubMed]
- Splinter, B.; Saadah, N.H.; Chavannes, N.H.; Kiefte-de Jong, J.C.; Aardoom, J.J. Optimizing the acceptability, adherence, and inclusiveness of the COVID radar surveillance app: Qualitative study using focus groups, thematic content analysis, and usability testing. JMIR Form Res 2022, 6, e36003. [Google Scholar] [CrossRef] [PubMed]
- Kondylakis, H.; Katehakis, D.G.; Kouroubali, A.; Logothetidis, F.; Triantafyllidis, A.; Kalamaras, I.; Votis, K.; Tzovaras, D. COVID-19 mobile apps: A systematic review of the literature. J Med Internet Res 2020, 22, e23170. [Google Scholar] [CrossRef]
- Anglemyer, A. , Moore, T.H.; Parker, L.; Chambers, T.; Grady, A.; Chiu, K.; Parry, M.; Wilczynska, M.; Flemyng, E.; Bero, L. Digital contact tracing technologies in epidemics: a rapid review. Cochrane Database Syst Rev 2020, 8, CD013699. [Google Scholar] [PubMed]
- Mavragani, A. Infodemiology and Infoveillance: Scoping Review. J Med Internet Res 2020, 22, e16206. [Google Scholar] [CrossRef] [PubMed]
- Mehraeen, E.; Pashaei, Z.; Akhtaran, F.K.; Dashti, M.; Afzalian, A.; Ghasemzadeh, A.; Asili, P.; Kahrizi, M.S.; Mirahmad, M.; Rahimi, E.; et al. Estimating Methods of the Undetected Infections in the COVID-19 Outbreak: A Systematic Review. Infect Disord Drug Targets. 2023, 23, e240123213106. [Google Scholar] [CrossRef]
- Chang, Z.; Zhan, Z.; Zhao, Z.; You, Z.; Liu, Y.; Yan, Z.; Fu, Y. , Liang, W.; Zhao, L. Application of artificial intelligence in COVID-19 medical area: a systematic review. J Thorac Dis. 2021, 13, 7034–7053. [Google Scholar] [CrossRef]
- Cildoz, M.; Gaston, M.; Frias, L.; Garcia-Vicuña, D.; Azcarate, C.; Mallor, F. Early detection of new pandemic waves. Control chart and a new surveillance index. PLoS One 2024, 19, e0295242. [Google Scholar] [CrossRef]
- Brizzi, A.; O'Driscoll, M.; Dorigatti, I. Refining reproduction number estimates to account for unobserved generations of infection in emerging epidemics. Clin Infect Dis 2022, 75, e114–e121. [Google Scholar] [CrossRef]
- Amereh, F.; Negahban-Azar, M.; Isazadeh, S.; Dabiri, H.; Masihi, N.; Jahangiri-Rad, M.; Rafiee, M. Sewage systems surveillance for SARS-CoV-2: Identification of knowledge gaps, emerging threats, and future research needs. Pathogens 2021, 10, 946. [Google Scholar] [CrossRef]
- Gogoi, G.; Singh, S.D.; Kalyan, E.; Koch, D.; Gogoi, P.; Kshattry, S.; Mahanta, H.J.; Imran, M.; Pandey, R.; Bharali, P. An interpretative review of the wastewater-based surveillance of the SARS-CoV-2: where do we stand on its presence and concern? Front Microbiol 2024, 15, 1338100. [Google Scholar] [CrossRef]
- Robishaw, J.D.; Alter, S.M.; Solano, J.J.; Shih, R.D.; DeMets, D.L.; Maki, D.G.; Hennekens, C.H. Genomic surveillance to combat COVID-19: challenges and opportunities. Lancet Microbe 2021, 2, e481–e484. [Google Scholar] [CrossRef]
- Bendall, E.E.; Paz-Bailey, G.; Santiago, G.A.; Porucznik, C.A.; Stanford, J.B.; Stockwell, M.S.; Duque, J.; Jeddy, Z.; Veguilla, V.; Major, C.; et al. SARS-CoV-2 genomic diversity in households highlights the challenges of sequence-based transmission inference. mSphere 2022, 7, e0040022. [Google Scholar] [CrossRef]
- Choi, Y.; Ladoy, A.; De Ridder, D.; Jacot, D.; Vuilleumier, S.; Bertelli, C.; Guessous, I.; Pillonel, T.; Joost, S.; Greub, G. Detection of SARS-CoV-2 infection clusters: The useful combination of spatiotemporal clustering and genomic analyses. Front Public Health 2022, 10, 1016169. [Google Scholar] [CrossRef]
- Bilal, M.Y.; Klutts, J.S. Molecular epidemiological investigations of localized SARS-CoV-2 outbreaks-utility of public algorithms. Epidemiologia 2022, 3, 402–411. [Google Scholar] [CrossRef]
- López, M.G.; Chiner-Oms, Á.; García de Viedma, D.; Ruiz-Rodriguez, P.; Bracho, M.A.; Cancino-Muñoz, I.; D'Auria, G.; de Marco, G.; García-González, N.; Goig, G.A.; et al. The first wave of the COVID-19 epidemic in Spain was associated with early introductions and fast spread of a dominating genetic variant. Nat Genet 2021, 53, 1405–1414. [Google Scholar] [CrossRef]
- Sharmin, M.; Manivannan, M.; Woo, D.; Sorel, O.; Auclair, J.R.; Gandhi, M.; Mujawar, I. Cross-sectional Ct distributions from qPCR tests can provide an early warning signal for the spread of COVID-19 in communities. Front Public Health 2023, 11, 1185720. [Google Scholar] [CrossRef]
- Ley 14/1986, de 25 de Abril, General de Sanidad (Law General of Health). Available online: https://www.boe.es/eli/es/l/1986/04/25/14/con (accessed on 2 May 2024). (In Spanish)..
- Ley 16/2003, de 28 de Mayo, de Cohesión y Calidad del Sistema Nacional de Salud. (Law of Cohesion and Quality of the National System of Health). Available online: https://www.boe.es/eli/es/l/2003/05/28/16 (accessed on 2 May 2024). (In Spanish)..
- Ley 33/2011, de 4 de Octubre, General de Salud Pública (Law General of Public Health). Available online: https://www.boe.es/eli/es/l/2011/10/04/33/con (accessed on 2 May 2024). (In Spanish)..
Figure 1.
Directed Acyclic Graphs (DAGs) of COVID-19 medical assistance (exposure) effect on reported COVID-19 case (outcome).Ancestors of exposure (in red) and outcome (in blue). Based on DAGitty version 3.1.
Figure 1.
Directed Acyclic Graphs (DAGs) of COVID-19 medical assistance (exposure) effect on reported COVID-19 case (outcome).Ancestors of exposure (in red) and outcome (in blue). Based on DAGitty version 3.1.
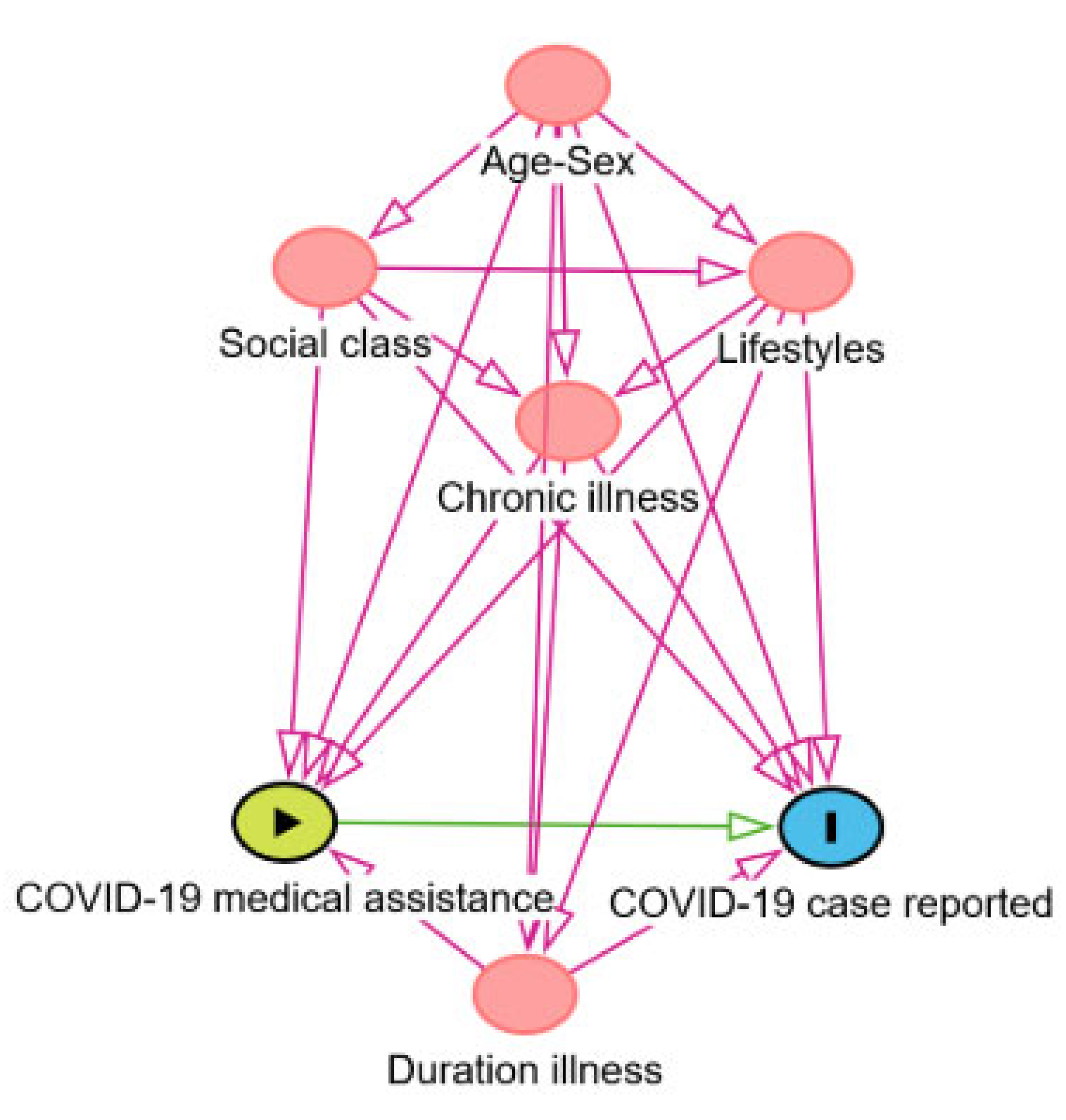

Table 1.
Characteristics of reported and unreported COVID-19 cases in the Borrriana COVID-19 cohort. January-June 2020.
Table 1.
Characteristics of reported and unreported COVID-19 cases in the Borrriana COVID-19 cohort. January-June 2020.
| Variables | Reported cases N=36 (%) |
Unreported cases N=432 (%) |
p-value |
|---|---|---|---|
| Age (years)±SD1 | 45.7±16.4 | 37.2±16.5 | 0.001 |
| Male | 14 (38.8) | 162 (37.5) | 0.860 |
| No received medical assistance for COVID-19 disease | 2 (5.6) | 236 (54.6) | 0.000 |
| Duration illness (days)±SD1,2 | 24.2±21.9 | 10.5±14.9 | 0.000 |
| No chronic illness4 | 14 (38.8) | 295 (68.3) | 0.001 |
| Middle and lower social classes5,6 | 25 (69.4) | 375 (87.4) | 0.009 |
| Body mass index (kg/m2)±SD1,7 | 26.4±5.8 | 25.0±5.0 | 0.183 |
| Obesity ≥30 kg/m2±SD1,8 | 10 (27.8) | 69 (16.1) | 0.102 |
| Current smoker9 | 3 (8.3) | 64 (15.3) | 0.333 |
| Alcohol intake yes10 | 11 (30.6) | 100 (23.8) | 0.417 |
| Habitual physical exercise yes | 17 (47.2) | 256 (59.3) | 0.164 |
| Nutritional diet yes11 | 10 (27.8) | 75 (17.4) | 0.121 |
1 Standard deviation.2 Missing answer from 48 participants.3 Missing answer from 5 participants.4 Missing answer from 4 participants.5 Higher managerial and professional occupations (group I).6 Missing answer from 3 participants.7 Missing answer from 4 participants.8 Missing answer from 4 participants.9 Missing answer from 13 participants.10 Missing answer from 11 participants.11 Missing answer from 1 participant.
Table 2.
Factors associated with unreported COVID-19 cases in the Borriana COVID-19 cohort by logistic regression. Crude and adjusted odds ratio (OR) and (aOR). 95% Confidence Interval (CI).
Table 2.
Factors associated with unreported COVID-19 cases in the Borriana COVID-19 cohort by logistic regression. Crude and adjusted odds ratio (OR) and (aOR). 95% Confidence Interval (CI).
| Variable | OR | 95% CI | aOR | 95% CI | p-value |
|---|---|---|---|---|---|
| Age (years)1 | 0.97 | 0.95-0.99 | 0.97 | 0.94-0.99 | 0.003 |
| Male2 | 0.94 | 0.47-1.89 | 1.16 | 0.94-2.35 | 0.690 |
| No medical assistance for COVID-19 disease3 | 17.6 | 4.86-86.30 | 10.83 | 2.49-47.11 | 0.001 |
| Duration illness (days)4 | 0.98 | 0.96-0.99 | 0.98 | 0.97-0.99 | 0.037 |
| No chronic illness5 | 3.34 | 1.66-6.72 | 2.81 | 1.28-6.17 | 0.010 |
| Middle and lower social classes,6 | 3.06 | 1.42-6.56 | 3.12 | 1.42-6.85 | 0.005 |
| Body mass index (kg/m2)7 | 0.94 | 0.88-1.01 | 0.98 | 0.91-1.06 | 0.651 |
| Obesity ≥30 kg/m2 7 | 0.50 | 0.33-1.08 | 0.64 | 0.28-1.47 | 0.294 |
| Current smoker8 | 1.98 | 0.59-6.67 | 2.14 | 0.62-7.41 | 0.228 |
| Alcohol intake yes9 | 0.70 | 0.34-1.49 | 0.59 | 0.26-1.33 | 0.203 |
| Habitual physical exercise10 yes | 1.63 | 0.2-3.21 | 1.91 | 0.91-4.00 | 0.085 |
| Nutritional diet yes11 | 0.55 | 0.25-1.18 | 0.65 | 0.29-1.48 | 0.307 |
1 Adjusted for sex.2 Adjusted for age.3 Adjusted for age, sex, social class, chronic illness, illness duration.4 Adjusted for age, sex, chronic illness, smoking, alcohol intake, physical exercise, nutritional diet, body mass index.5 Adjusted for age, sex, social class, smoking, alcohol intake, physical exercise, nutritional diet, body mass index.6 Adjusted for age, sex.7 Adjusted for age, sex, social class, smoking, alcohol intake, physical exercise, nutritional diet.8 Adjusted for age, sex, social class, alcohol intake, physical exercise, nutritional diet, body mass index.9 Adjusted for age, sex, social class, smoking, physical exercise, nutritional diet, body mass index.10 Adjusted for age, sex, social class, smoking, alcohol intake, nutritional diet, body mass index 11 Adjusted for age, sex, social class, smoking, alcohol intake, physical exercise, body mass index. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



