
Submitted:
26 June 2024
Posted:
27 June 2024
You are already at the latest version
Abstract
Background This study aimed to examine the acute effects of different pre-ST strategies on muscular performance and blood pressure (BP) responses in recreationally strength-trained women. Methods: Twelve overweight women with normal-to-elevated BP were recruited and performed six exper-imental protocols in a randomized order: 1) control protocol (CC) – BP assessed without exercises performed, 2) strength training (ST), 3) foam rolling warm-up followed by strength training (FR+ST), 4) specific warm-up followed by strength training (SW+ST), 5) aerobic exercise followed by strength training (AE+ST), and 6) stretching exercises followed by strength training (SE+ST). Strength training consisted of three sets at 80% of 10RM with a self-suggested rest interval between sets for bench press, back squat, bench press 45º, front squat, lat pull-down, leg press, shoulder press, and leg extension. Results: All experimental protocol had a lower total training volume, fa-tigue index, and repetitions performance in relation to ST (p
Keywords:
hemodynamic response
; manual therapies
; massage
; resistance exercise
; stretching
1. Introduction
Regular physical exercise represents a significant non-pharmacological approach to promoting health and enhancing physical performance [1]. Notably, when analyzing the American College of Sports Medicine Worldwide Survey of Fitness Trends for 2024 [2], it becomes evident that 8 out of the 10 major trends are closely linked to physical exercise. This trend aligns with the recommendations previously set forth by the World Health Organization, which was recently updated to encourage individuals to engage in 300 minutes of physical activity per week.
In a study with a similar design to our current investigation, Da Silva Telles et al. [3] explored various warm-up strategies [including strength training (ST) with ischemic preprotocoling, specific warm-up (SW), aerobic exercise (AE), and dynamic stretching] prior to two strength training exercises (bench press and leg press 45º). The authors observed improvements in muscular performance, specifically in terms of maximum repetition performance and total training volume, when utilizing the pre-ST strategy with ischemic preprotocoling. The findings from Da Silva Telles et al. [3] and the study's overall design have highlighted important research gaps, including the investigation of foam rolling (FR) or stretching as alternative pre-ST warm-up strategies. Notably, to the best of our knowledge, no prior studies have explored the effects of FR as a pre-ST strategy on BP and muscular responses (total training volume, maximum repetition performance, and fatigue index). Further research in this area could provide valuable insights into optimizing warm-up techniques in strength training settings.
Approximately 31.1% of adults worldwide in the last decade experiencing hypertension, the influence of regular physical exercise on BP is an important health consideration [4]. Hypertension is considered a major risk factor for cardiovascular diseases [5], generating worldwide concern [6]. Post-exercise hypotension (PEH) is an established physiological response to exercise. PEH is characterized as an immediate exercise-induced reduction in BP of 5-8 mmHg on average [7], a magnitude that has important clinical relevance to reducing cardiovascular risk throughout the day [7]. Several non-pharmacological strategies have been tested to promote PEH [7]. ST has recently been recommended as a non-pharmacological strategy in and of itself with several studies indicating its effectiveness in promoting PEH in adults with and without hypertension [6], whether by manipulating the exercise order, rest interval, and training methods.
Although not as extensively studied, similar PEH effects are observed when using FR [8,9] and stretching [10]. However, conflicting reports are indicating that the concurrent sequencing of stretching and strength training can impair, improve or have no effect on performance (e.g., total training volume, force output, hypertrophy). Furthermore, there is scant literature regarding BP responses to different intervention combinations (e.g., foam rolling, stretching (SE), AE, and ST). It is known that in relation to FR and stretching exercise (SE), the mechanical stimulus during exercise triggers the pressor reflex that increases sympathetic discharge through efferent stimuli coming from control centers located in the central nervous system, such as the nucleus of the solitary tract [11,12]. Thus, considering that the neural mechanisms that partly explain PEH are related to a flattening of the post-exercise sympathetic stimulus as a compensatory means of sympathetic activity during exercise, it is plausible to hypothesize that such strategies may interfere in the post-exercise BP response [13]. Vasodilator responses and reductions in cardiac output have been appointed as mechanisms for PEH caused by aerobic training [14]. Thus, considering that the strategies employed in the present study have an impact on BP responses, investigating possible congruences that attenuate the post-exercise BP response is a knowledge gap that should be investigated further.
Thus, the purpose of the present study was to examine the acute effects of different pre-ST strategies on total training volume, maximum repetition performance, fatigue index, and BP responses in recreationally strength-trained women. The present study had two initial hypotheses. First, ST performed in isolation may increase muscular performance when compared with another pre-ST strategy. Secondly, the combination of FR and stretching with ST has been shown to potentially reduce BP values.
2. Materials and Methods
2.1. Ethical Considerations
The procedures of the present study were carried out in accordance with Resolution No. 466/12 of the Brazilian National Health Council. The study was submitted and approved by the Augusto Motta University Centre ethics committee [4.611.983] and were conducted in accordance with the Declaration of Helsinki.
2.2. Participants
Twelve recreationally strength-trained (Resistance Training Experience: 29.8 ± 7.6 months) women with normal to elevated (Baseline Systolic BP: 118.33 ± 4.89 mmHg; Baseline Diastolic BP: 78.50 ± 4.10 mmHg) BP (Age: 27.2 ± 3.3 years; Height: 164.8 ± 5.5 cm; Body Weight: 69.8 ± 6.0 kg; Body Mass Index: 25.7 ± 2.3) were recruited for the present study based on a priori sample size calculation [15]. A priori sample size calculation (effect size = 0.65; 1-β = 0.95; α = 0.05; non-sphericity correction = 1.0) using G*Power [16] indicated that twelve subjects would be adequate to achieve the aforementioned statistical power. Inclusion criteria were as follows: 1) participation in a structured ST program for at least one year prior to the study. The ST program had to average at least 50-minute per session and consist of at least three sessions per week, using loads between 8-12RM and rest intervals between 1- to 3-min between sets and exercises; 2) being free from any functional limitations or medical protocols that could have compromised their health or confounded the study results.
During the seven weeks of data collection, the subjects were instructed not to engage in any non-study ST program or other strenuous physical activity. Subjects were recommended to maintain their eating and sleeping habits, avoiding caffeine and ergogenic, over the seven weeks of data collection. Prior to the study, all subjects were provided with verbal and written explanations of all study procedures, they then provided written informed consent and completed the Physical Activity Readiness Questionnaire
2.3. Procedure
A randomized and counter-balanced within-subject experimental design was used to examine the acute effects of different pre-ST strategies on total training volume, maximum repetition performance, fatigue index, and BP responses in recreationally strength-trained women. Subjects visited the laboratory for nine sessions during a seven-week period with at least forty-eight hours and one week between visits for ten repetition maximum tests (10RM) and each experimental protocol, respectively (see Figure 1).
The first session was used to familiarize subjects with all procedures. Sessions 2 and 3 were used for 10RM testing and re-testing, respectively, for bench press, back squat, bench press 45º, front squat, lat pull-down, leg press, shoulder press, and leg extension exercises to determine the exercise load to be used during all experimental protocols. Following 10RM testing, six experimental protocols followed in a randomized order: 1) control protocol (CC) – BP assessed without exercises performed, 2) ST isolated (ST), 3) FR warm-up followed by ST (FR+ST), 4) SW warm-up followed by ST (SW+ST), 5) AE warm-up followed by ST (AE+ST), and 6) SE followed by ST (SE+ST). The total training volume (repetition x load) was recorded following each exercise and protocol.
During each experimental session, BP was assessed after a 15-min passive rest period on arrival at the laboratory and at 10-, 20-, 30-, 50-, and 60-min following the interventions (Baseline, Post-10, Post-20, Post-30, Post-40, Post-50, and Post-60). All procedures were performed at the same time (in the morning) to avoid any confounding circadian rhythm effect. Subjects were instructed to maintain their regular respiratory pattern to avoid the Valsalva maneuver.
2.4. Load Test
Ten Repetition Maximum Test (10RM): The exercises performed in the 10RM test were bench press, back squat, bench press 45º, front squat, lat pull-down, leg press, shoulder press, and leg extension. Briefly, subjects initially performed a standardized warm-up consisting of 15 repetitions with a self-suggested load (representing approximately 50% of the normal training load). Following the warm-up, 10RM testing was performed for all exercises on the same day and in the same order with 10-min rest intervals between exercises. Execution of the exercises was standardized insofar as no pauses were allowed between concentric and eccentric portions of the lift. Repetitions were conducted at a constant velocity of 4 seconds per repetition (2-second concentric and 2-second eccentric) controlled by a metronome (Metronome Plus 2.0; M&M System, Lich, Germany). A maximum of three trials were allowed per testing session, separated by 3-min of passive rest. Testing was then repeated on another day at least 48 hours later (re-test). The greater load between the two testing days was deemed the 10RM load. Loads reproducibility between the two testing days was tested by the intraclass correlation coefficient. To minimize potential error variance, the following procedures were adopted for all subjects, for they: a) received standardized instructions about the exercise technique and data collection, b) received feedback regarding technique and were corrected when appropriate, and c) were always verbally encouraged. The same exercise apparatus was used for 10RM testing and during all strength training experimental sessions (ST, FR+ST, SW+ST, AE+ST, and SE+ST). Subjects’ load characteristics were provided in Table 1.
2.5. Instruments
Strength Training (ST): During the ST protocol, subjects performed all exercises until concentric failure throughout three sets of bench press, back squat, bench press 45º, front squat, lat pull-down, leg press, shoulder press, and leg extension exercises at 80% of their previously established 10RM, with a self-suggested rest interval between sets. The number of repetitions in each set was recorded for each protocol.
Foam Rolling (FR): FR protocol utilized a foam roller with a hard inner core enclosed in a layer of ethylene-vinyl acetate foam (Trigger Point Technologies, 5321 Industrial Oaks Blvd., Austin, Texas 78735, USA) which has been shown to produce more pressure on the soft tissue than a conventional foam roller without a hardcore. The FR was applied, unilaterally in a randomized order, in single sets of 90-sec to the lateral torso of the trunk, anterior (i.e., quadriceps) and posterior (i.e., hamstrings) thigh, and calf regions. The lateral torso of the trunk was rolled in a decubitus lateral position. Subjects were instructed to roll their lateral aspect of the trunk up and down on the foam roller, between the proximal third of the arm and the inferior part of the ribcage. Anterior and posterior thigh positions were performed in a plank and seated position, respectively, with the upper thigh of the dominant leg on the foam roller [17]. While keeping the knee of the dominant leg extended, subjects were instructed to use their arms and a contralateral leg to propel themselves backward and forward on the foam roller between the acetabulum and quadriceps tendon and between the ischial tuberosity and popliteal fossa for the anterior and posterior thigh, respectively, with fluid dynamic motions. The posterior leg was performed in a seated position with the legs extended and the feet relaxed. One leg was crossed over the other to allow more pressure to be directed over the plantar flexors being treated. Subjects were instructed to use their arms to propel their body back and forward, from the popliteal fossa to the Achilles tendon, in fluid motions. Subjects were encouraged to support as much of their entire body mass as possible with the foam roller, thus, maximizing pressure on the limb. For a better representation of typical or realistic training environments, subjects were free to choose the pace with which they performed the roller. FR was applied at different angles to target all areas with controlled pressure by a pain level scale in which a score of one represented no pain at all, and a score of 10 represented maximal tolerable pain. Subjects were instructed to maintain pressure resulting in a self-rated score self-rated score of 6 out of 10 on the pain level scale.
Stretching Exercise (SE): For each SE, the joint movement was taken into a position of slight discomfort [1], and then, the joint position was maintained. Subjects were instructed to maintain their usual respiratory pattern throughout all SEs. Static stretching was applied unilaterally, in a random order, with a single set for 90-sec to the lateral torso of the trunk, anterior (i.e., quadriceps) and posterior (i.e., hamstrings) thigh, and calf regions. The lateral torso of the trunk static stretching was performed in a seated position with the stretched lateral torso flexed and non-stretched relaxed in extension. The therapist performed the movement of lateral torso flexion with the knee flexed to maximize stretching of the lateral torso of the trunk. Anterior thigh static stretching was performed in decubitus lateralis with the stretched leg flexed and non-stretched relaxed in extension. The therapist performed the movement of knee flexion with hip extension to maximize stretching of the anterior thigh muscles. Posterior thigh static stretching was performed in a supine position with the stretched leg extended and the non-stretched leg relaxed and flexed at 45º of hip and knee flexion. The therapist performed the movement of hip extension with an extended knee. The participants engaged in active posterior leg static stretching while standing. They positioned one leg on the edge of a bench, extended the knee, and dorsiflexed the ankle, directing the heel toward the ground. During the stretch, subjects leaned on the wall for balance if needed. Static stretching was performed passively with the dominant leg in the stretching position. The rating perceived was controlled by a self-rated pain pressure level scale of 6 out of 10.
Aerobic Exercise (AE): The AE protocol consisted of walking on the treadmill at a light to moderate intensity between 30 and 60% of the heart rate reserve (HRR = (HR maximum -% intensity) + HR) for 12-minutes [3].
Specific Warm-Up (SW): The SW was composed of two sets of 15 repetitions with 40% of 10RM for bench press, back squat, bench press 45º, front squat, lat pull-down, leg press, shoulder press, and leg extension exercises. There was a 90-second rest interval between sets [18].
2.6. Measures
Blood Pressure (BP): Systolic and diastolic BP were measured using an automatic oscillometric device (Omron Hem 7113, São Paulo, Brazil) [19]. During each experimental session, blood pressure was assessed after a 15-min passive rest period on arrival at the laboratory and at 10-, 20-, 30-, 50-, and 60-min following the interventions (Baseline, Post-10, Post-20, Post-30, Post-40, Post-50, and Post-60). Measurements were performed on the left arm.
Muscular Response: The total training volume (repetition x load) was recorded following each exercise and protocol. The fatigue index was analyzed from the first (1st) and last (3rd) sets and calculated using the equation: Fatigue index = (third set ÷ first set)×100; where a higher percentage value (%) indicates a superior fatigue resistance: The value was noted at the end of each exercise set.
2.7. Statistical Analyses
Based on the sample size, the Shapiro-Wilk normality test was performed, followed by the symmetry and kurtosis analysis. Finally, the graphical distribution analysis with the histograms and QQ plots observation was tested. Variables that had their normality rejected were described using the median and the interquartile range as measures of central tendency and descriptive statistics dispersion, which indicates the variability of results, respectively. For the variables that did not have their normality rejected, descriptive variables were calculated as the mean as a measure of central tendency, as well as the standard deviation as a measure of the tendency of variability.
The total training volume had normality partially rejected, so the comparison between the protocols was made using the Friedman (all exercises except Bench Press 45o) and a two-way ANOVA (8 exercises*5 protocol) with repeated measures (normal distribution for Bench Press 45o) for non-parametric and parametric tests to determine between and within effects of total training volume for each exercise and protocol. Pairwise comparisons adjusted by Bonferroni corrections were employed to score within protocol differences and the Wilcoxon test between protocol. Maximum repetition performance and fatigue index did not achieve normality, so the comparison between protocol and sets was made using the Friedman non-parametric test followed by a pairwise comparison adjusted by Bonferroni corrections. Blood pressure responses were normally distributed, so the comparison between protocol was made using the ANOVA (8 exercises*6 protocols) with repeated measures followed by Bonferroni post hoc test if any statistical difference was evident.
The interquartile range was calculated based on dividing a data set into quartiles and subtracting the third quartile (upper limits) from the first quartile (lower limits). Additionally, Cohen’s d effect sizes were calculated using the formula d=Md/Sd, where Md is the mean difference and Sd is the standard deviation of differences. This calculation differs slightly from traditional Cohen’s d calculations, in that this formula better represents within-subject differences, whereas the traditional Cohen’s d formula is better for between-subject comparisons [20,21,22]. Cohen’s d effect-sizes were defined as small, medium, and large for 0.2, 0.5, and 0.8, respectively.
An alpha level of 0.05 was used. All analyses were performed using SPSS version 21 (SPSS Inc., Armonk, NY, USA).
3. Results
Descriptive characteristics and reproducibility of the 10RM test
All exercises presented intraclass correlation coefficient values above 0.5, indicating moderate reproducibility (Table 1).
3.1. Muscle Performance
3.1.1. Total Training Volume
With all exercises, ST consistently demonstrated the highest total training volume. A significantly (p=0.0001) greater bench press total training volume was achieved with the ST over FR+ST, SW+ST, and SE+ST. Similarly, the back squat total training volume was significantly (p=0.0001) higher with ST versus FR+ST and SW+ST protocols. With the front squat, ST demonstrated significantly more (p=0.0001) total training volume than FR+ST, AE+ST, SW+ST, and SE+ST protocols. For the lat pull-down, ST significantly (p=0.0001) exceeded FR+ST, SW+ST, SE+ST, and AE+ST. For the leg press, ST was significantly (p=0.0001) greater than FR+ST, SW+ST, SE+ST, and AE+ST. For the Shoulder press, ST was significantly (p=0.002) higher than FR+ST, SW+ST, and AE+ST. For the leg extension, ST was significantly (p=0.0001) higher than FR+ST and SW+ST. Finally, for the bench press 45º, ST demonstrated significantly (p=0.0001) higher total training volume than FR+ST, SW+ST, and AE+ST. The only significant difference that did not involve the ST protocol showed that the bench press 45º with SE+ST exhibited a higher total training volume than FR+ST (all interaction details illustrated in Table 2).
3.2. Maximum Repetition Performance
There was a significant reduction in the maximum repetitions between sets 3 and 1 with the FR+ST protocol: (Bench Press: p=0.003; Back Squat: p<0,001; Bench Press 45º: p<0.001; Front Squat: p<0.001; Lat Pull-Down: p<0.001; Leg Press: p=0.018; Shoulder Press: p=0.002; Leg Extension: p = 0.007). Similarly, significant reductions in the maximum repetitions were observed between sets 2 and 1 (Bench Press: p=0.024 and Shoulder Press: p=0.024), as well as between sets 3 and 1 (Bench Press: p<0.001; Back Squat: p=0.032; Bench Press 45º: p<0.032; Front Squat: p=0.007; Lat Pull-Down: p=0.009; Leg Press: p=0.001; Shoulder Press: p=0.002; Leg Extension: p=0.002) with the SW+FR protocol. Furthermore, AE+ST presented significant reductions in maximum repetitions between sets 3 and 1 for Bench Press (p=0.043), Front Squat (p=0.002), Leg Press (p=0.043), Shoulder Press (p=0.009), and Leg Press (p=0.013) exercises. Finally, significant reductions in the maximum repetitions were observed in the SE+ST protocol when comparing the third and second sets in the Front Squat exercise (p=0.032) and between the third and first sets in the Bench Press (p=0.024), Bench Press 45º (p=0.032), Front Squat (p=0.009), Lat Pull-Down (p=0.009), Leg Press (p=0.005), Shoulder Press (p=0.024), and Leg Press (p=0.007) exercises No other significant within-protocol differences were observed (all details presented in Table 3).
In the comparison between the experimental protocols, the Bench Press exercise presented a higher number of repetitions with set 2 in the ST protocol when compared to SW+ST (p=0.006), SE+ST (p=0.024), and FR+ST (p=0.030), as well as in set 3 when comparing SW+ST (p<0.001) and FR+ST (p<0.001) protocols. Likewise, a greater number of repetitions was performed in the Back Squat exercise with set 2 in the ST protocol when compared to SW+ST (p=0.037) and FR+ST (p=0.012), as well as in set 3 when compared to FR+ST (p<0.001). The Bench Press 45º exercise presented higher maximum repetitions in the ST protocol with set 2 when compared to FR+ST (p=0.012) and with set 3 in the FR+ST (p<0.001) and SW+ST (p=0.024) protocols. The Front Squat exercise presented greater maximum repetitions with ST with set 2 when compared to FR+ST (p=0.030) and AE+ST (p=0.045) and with set 3 in the FR+ST (p<0.001), AE+ST (p=0.004), SW+ST (p=0.037), and SE+ST (p=0.008). In addition, a greater number of repetitions was performed in the Lat Pull-Down exercise throughout set 2 in the ST protocol when compared to FR+ST (p=0.006) and AE+ST (p=0.037), as well as in set 3 when compared to FR+ST (p<0.001), SW+ST (p=0.019), and SE+ST (p=0.045). Furthermore, more repetitions were performed in the Leg Press with set 2 in the ST protocol when compared to FR+ST (p=0.045) and SE+ST (p=0.012), as well as in set 3 when compared to FR+ST (p=0.003), AE+ST (p=0.045), SW+ST (p=0.001), and SE+ST (p=0.005). The Shoulder Press exercise presented elevated maximum repetitions in the ST protocol with set 2 when compared to the FR+ST (p=0.019) and with set 3 in the FR+ST (p=0.006), SW+ST (p=0.019), and AE+ST (p=0.019). Finally, a higher number of repetitions was performed in the Leg Extension throughout set 2 in the ST protocol when compared to FR+ST (p=0.004) and SW+ST (p=0.012), as well as in set 3 when compared to FR+ST (p<0.001), AE+ST (p=0.019), SW+ST (p=0.001), and SE+ST (p=0.019) (all maximum repetitions details presented in Table 3).
3.3. Fatigue Index
The bench press presented a significantly higher fatigue index with ST when compared to the FR+ST (21.8%, p=0.010) and SW+ST (14.1%, p=0.016). Similar responses were observed with the Back Squat, which showed a significantly higher fatigue index with ST compared to FR+ST (29.2%, p=0.001), as well, AE+ST exceeded FR+ST (25.9%, p=0.006). With Bench Press 45º, the only significant difference showed a higher fatigue index with ST compared to FR+ST (24.9%, p=0.001). Front Squat demonstrated a higher fatigue index with ST versus FR+ST (46.3%, p<0.001), SE+ST (26.7%, p=0.019), and AE+ST (26.7%, p=0.030). With the Lat Pull-Down, ST was only significantly greater than FR+ST protocols (46.3%, p=0.005). With the Leg Press fatigue index, ST significantly exceeded SW+ST (20.4%, p=0.010) and SE+ST (20.9%, p=0.037). For the Shoulder Press, ST was only significantly higher than the FR+ST fatigue index (25.0%, p=0.045). Finally, Leg Extension promoted a significantly higher fatigue index with ST compared to FR+ST (20.7%, p=0.008), SW+ST (25.0%, p=0.012), and AE+ST (25.0%, p=0.037) (all fatigue index results presented in Table 3).
3.4. Blood Pressure
4. Discussion
A The purpose of the present study was to examine the acute effects of different pre-ST strategies on total training volume, maximum repetition performance, fatigue index, and BP responses in recreationally strength-trained women. The primary result indicates that higher maximum repetitions, total training volume, and resistance to fatigue were observed when ST was performed without any pre-ST strategies. These findings align with the study conducted by Da Silva Telles et al. [3], which also reported that isolated ST with ischemic preconditioning led to a higher number of repetitions compared to other pre-ST strategies. While Da Silva Telles et al. [3] is the only study with a similar experimental design, the present study is the first to compare various pre-ST strategies on muscular (total training volume and resistance to fatigue) and BP response.
The muscular results found partial support for the first hypothesis, which indicated that not using pre-ST strategies would allow for higher maximum repetitions and total training volume. Monteiro et al. [23] suggested that fewer repetitions would result due to the fatigue associated with reduced rest interval or when combining other exercises. Typically, the second exercise in a sequence would be expected to exhibit a greater degree of fatigue as non-local muscle fatigue can adversely affect the performance of previously non-exercised muscles [24,25,26].
Additionally, total training volume was reduced under all experimental protocols when compared to ST performed alone (Table 3). The resistance to fatigue reduction was expected, as hypothesized in this study, due to residual fatigue caused by the inclusion of another activity as a pre-strength training strategy. The finding of higher fatigue index was related to the lower maximum repetition performance and total training volume. The reduction in total training volume may adversely affect the hypertrophic training response, given that hypertrophy appears to be volume dependent. These results argue against the inclusion of other pre-ST strategies.
While non-local muscle fatigue has been attributed to physiological mechanisms, such as central nervous system inhibition, and psychological factors like the strength energy model (where prior fatiguing exercise affects subsequent motivation, focus, and attention), there is also evidence of central nervous system potentiation or excitation. For instance, studies by Halperin et al. [25], Aboodarda et al. [27], and Šambaher et al. [28] have demonstrated increased spinal and cortical excitability in contralateral muscles following unilateral fatiguing exercises. Aboodarda et al. [27] found enhanced spinal excitability in contralateral knee extensors after fatiguing unilateral elbow flexors, and Šambaher et al. [28] reported similar results with cervico-medullary evoked potentials. Furthermore, Aboodarda et al. [27,29] showed increased cortical excitability in contralateral elbow flexors after fatiguing unilateral elbow flexors and knee extensors, respectively. Overall, the impact of an exercise on subsequent performance is influenced by a delicate balance between fatiguing and potentiating mechanisms [30].
Similarly, active pre-ST protocols tend to generate higher fatigue, as reported by Monteiro et al. [23] who observed a reduction in resistance to fatigue when subjects performed 60 (FR60) and 120 (FR120) minutes of FR. However, Santana et al. [31] contradicted the previous literature by reporting an increase in the total training volume when FR was performed in combination with ST (agonist foam rolling, antagonist foam rolling, and paired (agonist/antagonist) foam rolling) when compared to the traditional ST. This presented scientific literature conflict highlights an important gap regards to total training volume when strength training was performed in combination to foam rolling.
Several strategies have been identified as intervening in the behavior of force production during exercise. For example, SE seems to have an impact on changing the musculotendinous unit’s length, as well as reducing muscle tone due to lower activation of muscle spindles, inhibiting their motor responses, and even modifying the overlapping arrangement of contractile filaments in a way that impairs their sliding and drag, directly interfering with force generation [32]. In the same way, FR and AE can compromise the performance of strength due to increased fatigue or the use of energy substrates that are intensity-dependent, respectively. Furthermore, crosstalk mechanisms between pgc1-α and mTOR pathways also compromise strength training adaptations as a function of aerobic activity [33,34]. On the other hand, SW can be considered a potentiating strategy of strength performance through the post-activation potential involving peripheral mechanisms such as facilitating myosin phosphorylation and central mechanisms such as greater motor neuron excitability and an increase in the number of recruited motor units [35]. Thus, it is observed that pre-ST strategies can have different impacts on muscular responses, thus, it is fitting to analyze different interventions in this sense to observe the outcome.
The BP results found partial support for the second hypothesis, which indicated that multi-joint with large muscle volumes exercises may induce previously clinically significant reductions in systolic BP values. Figueiredo et al. [36] have indicated that ST with higher total training volume seems to be more efficient to decrease systolic BP in young adults. The neural reflex via activation of chemical and mechanical receptors activates the afferent pathway to the nucleus of the solitary tract, which stimulates the sympathetic system while inhibiting the parasympathetic system [12]. Thus, large muscle groups can increase the absolute BP values [37], a phenomenon not observed in the present study. For example, Halliwill [14] hypothesizes the local metabolic effect as a PEH mechanism, which has a vasodilator and alpha-adrenergic receptor inhibitory action. These effects become more important than simple reductions in cardiac output, given the fact that reductions in cardiac output can be offset by a post-exercise reduction, exercise load, and increased myocardial contractility. It is, therefore, pertinent to hypothesize a possible effect of muscle mass size on the local metabolites production which supports the results of the present study that uses principally multi-joint exercises and indicates a large effect size post-exercise magnitude (FR+ST, SW+ST, SE+ST, and SE+ST).
Effect sizes indicated a clinical reduction with a large magnitude in systolic BP for the FR+ST (Post-50: ∆ = -5.00 mmHg) when compared to the baseline (Table 5). The findings observed in the FR+ST protocol are consistent with those presented by Monteiro et al. [38]. In their study, the authors also reported PEH in systolic BP for FR at Post-60 (p=0.020; effect size = -2.14) and in ST+FR at Post-50 (p=0.001; effect size = -2.03) and Post-60 (p<0.001; effect size = -2.38) time points. Similar results were described by Monteiro et al. [38] when observed PEH in systolic BP after massage alone (Post-50: p=0.011; effect size = -2.61; ∆ = -4.0 mmHg; Post-60: p = 0.011; ES = -2.74; ∆ = -4.0 mmHg) but not performed after ST. Although using different techniques, the literature consistently demonstrates similar effects between FR and massage techniques. In a systematic review with meta-analysis, Liao et al. [39] found that both FR and massage techniques significantly contributed to reductions in systolic (-7.39 mmHg; effect size = -0.728) and diastolic (-5.04 mmHg; effect size = -0.334) BP. Therefore, incorporating FR before and after ST appears to be a valuable clinical approach for PEH.
Different physiological mechanisms seem to justify the results found both in the present study and in the previous literature. First, Okamoto et al. [8] reported higher levels of Nitric Oxide following FR, suggesting a greater vasodilatory effect that may contribute to the reduction in BP. Similarly, Hotfiel et al. [9] observed increased local arterial perfusion in the lateral thigh region after FR, which they associated with vasodilation resulting from the elevation of Nitric Oxide levels following FR. Second, White and Raven [40] indicated that during exercise, there is a reversal in the action of the autonomic nervous system in the control of cardiac activity, in an attempt to maintain homeostasis, thus reducing vagal control. However, Farinatti et al. [41] systematic review indicates that relatively prolonged changes (≥ 30 min) in BP post-ST were shown to be inversely related to changes in sympathetic and directly related to changes in parasympathetic outflow; that is; PEH was systematically concomitant to increased sympathetic and decreased parasympathetic modulation, irrespective of the BP status of samples or study design.
Forjaz et al. [42], in a classic study, demonstrated that continuous low-intensity AE was efficient in providing PEH which would be related to reduced sympathetic activity as well as the vasodilator effect of local metabolites. Inami et al. [43] observed that systolic BP was transiently higher during SE and returned to baseline immediately post-intervention. The present results followed those found by Inami et al. [43] when observing that only the SW+ST (effects size = 0.94) and AE+ST (effect size = 1.96) protocols had a large magnitude in Post-10. A potential mechanism to explain the PEH after SE was reported by Kruse and Scheuermann [44], who indicate a reduction in blood flow by a reduction in the diameter of blood vessels through a mechanical obstruction generated by muscle contractions and also by the nutrient supply. Kruse and Scheuermann [44] observed mechanical vascular deformation at the beginning of stretching combined with an increase in the stimulation of group III afferent fibers, which initiates a cascade of events, resulting in peripheral vasodilation and an increase in heart rate, cardiac output, BP, and blood flow.
A point to consider when interpreting the findings in this study is the self-paced FR and ST either within or between individuals. This can be considered as both a limitation and a strength of this design. Specifically, the lack of control reduces the internal validity of the results, as the number/duration of each roll could influence the outcome. The freedom to choose the pace and duration of each repetition enhances the ecological validity and generalizability of the findings, as it better represents real-life training scenarios and suggests a more robust influence of strength training on muscular performance and blood pressure responses rather than having to meet tightly controlled parameters to elicit a response. The participants in the current study were all women. It has been well-documented that women generally exhibit lower relative muscle strength compared to men during dynamic contractions. The menstrual cycle's different phases can indeed influence responses, as reported by Queiroz et al. [45]. Their study indicated that the occurrence of menstrual bleeding may affect the magnitude of blood pressure decrease but not the overall occurrence of this phenomenon [46]. While it is essential to exercise caution when generalizing these findings, it is important to note that the primary focus of the present study was not to analyze mechanisms but rather to examine the blood pressure response. Consequently, the fact that the participants were women is not likely to pose significant issues when extrapolating the results to men, as the key difference between sexes lies in the underlying mechanisms rather than the blood pressure responses [45].
5. Conclusions
We found decreases in maximum repetitions, resistance to fatigue, and total training volume when were performed before ST as warm-up strategies. Thus, the pre-ST strategies of FR, SW, AE, and SE is not performed if the main objective of the ST protocol is improvements in muscular performance (for example, maintenance of the number of repetitions). However, these strategies indicated a clinical reduction in BP with a large and meaningful magnitude (effect size) in recreationally strength-trained women with normal to elevated BP. The results of this investigation may help to influence decision-making by practitioners who desire to elicit a PEH response in both subjects with normal BP and hypertension. In addition, while investigating chronic changes in PEH as a response to these interventions was beyond the scope of this current investigation, there is ample data to suggest that strength training can be a powerful tool to improve blood pressure. Practitioners who are looking to influence blood pressure parameters in their clients may wish to explore incorporating strength training in their plan of care.
Author Contributions
Conceptualization, E.R.M., V.G.C.N., and J.S.N.; methodology, E.R.M., V.G.C.N., and J.S.N.; formal analysis, E.R.M., L.S.P., L.L., M.J.C.M., P.H.M., V.G.C.N. and J.S.N.; investigation, E.R.M.; data curation, E.R.M., L.S.P., P.H.M., V.G.C.N., and J.S.N.; writing—original draft preparation, E.R.M., M.J.C.M., M.R.N., G.S.S., V.G.C.N., and J.S.N.; writing—review and editing, E.R.M., L.S.P., L.L., P.H.M., V.G.C.N., and J.S.N.; visualization, E.R.M., L.S.P., L.L., M.J.C.M., P.H.M., M.R.N., G.S.A., V.G.C.N. and J.S.N; supervision, V.G.C.N. and J.S.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Augusto Motta University Center (protocol code 4.611.983 approved on March 25, 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
No additional acknowledgment is applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American College of Sports Medicine Position Stand. Quantity and quality of exercise for developing and maintain cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med Sci Sport Exerc 2011, 43, 1334-1359.
- Thompson, W. R. Worldwide survey of fitness trends for 2023. ACM’s. Health & Fitness Journal 2023, 26, 11-20.
- Da Silva Telles, L. G. , Carelli, L. C., Bráz, I. D., Junqueira, C. J., Monteiro, E. R., Reis, V. M., et al. Effects of ischemic preprotocoling as a warm-up on leg press and bench press performance. J Hum Kinet 2020, 75, 267-277.
- Mills, K. T. , Stefanescu, He. J. The global epidemiology of hypertension. Nat Rev Nephrol 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Schiffrin, E. L. Immune mechanisms in hypertension and vascular injury. Clin Sci (Lond) 2014, 126, 267–274. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, H. V., Johnson, B. T, Huedo-Medina, T. B., Livingston, J., Forsyth, K. C., Kraemer, W. J, et al. Dynamic resistance training as stand-alone antihypertensive lifestyle therapy: a meta-analysis. J Am Heart Assoc 2016, 5, e003231.
- Pescatello, L. S., Buchner, D. M., Jakicic, J. M., Powell, K. E., Kraus, W. E., Bloodgood, B., et al. Physical activity to prevent and treat hypertension: a systematic review. Med Sci Sports Exerc 2019, 51, 1314-1323.
- Okamoto, T., Masuhara, M., Ikuta, K. Acute effects of self-myofascial release using a foam roller on arterial function. J Strength Cond Res 2014, 28, 69-73.
- Hotfiel, T. , Swoboda, B., Krinner, S., Grim, C., Engelhardt, M., Uder, M., et al. Acute effects of lateral thigh foam rolling on arterial tissue perfusion determined by spectral doppler and power doppler ultrasound. J Strength Cond Res 2017, 31, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Araújo, G. , Behm, D. G., Monteiro, E. R., Fiuza, A. G. F. deM., Gomes, T. M., Vianna, J. M., et al. Order effects of resistance and stretching exercises on heart rate variability and blood pressure in healthy adults. J Strength Cond Res 2018, 33, 2684–2693. [Google Scholar] [CrossRef] [PubMed]
- Spranger, M. D., Krishnan, A. C., Levi, P. D., O’leary, D. S., Smith, S. A. Blood flow restriction training and the exercise pressor reflex: a call for concern. Am J Physiol Heart Circ Physiol 2015, 309, H1440–H1452.
- Sidhu, S. K. , Weavil, J. C., Rossman, M. J., Jessop, J. E., Bledsoe, A. D., Buys, M. J., et al. Exercise Pressor Reflex Contributes to the Cardiovascular Abnormalities Characterizing Hypertensive Humans During Exercise. Hypertension 2019, 74, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Brasileiro-Santos, M. S., Santos, A. C. Neural mechanisms and post-exercise hypotension: The importance of experimental studies. Motriz 2017, 23, e101622.
- Halliwill, J. R. Mechanisms and Clinical Implications of Post-exercise Hypotension in Humans. Exerc Sport Sci Rev 2001, 29, 65–70. [Google Scholar] [PubMed]
- Beck, T. W. The importance of a priori sample size estimation in strength and conditioning research. J Strength Cond Res 2013, 27, 2323–2337. [Google Scholar] [CrossRef] [PubMed]
- Faul, F. , Erdfelder, E., Lang, A. G., Buchner, A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Zahiri, A. , Alizadeh, S., Daneshjoo, A., Pike, N., Konrad, A., Behm, D. G. Core muscle activation with foam rolling and static planks. Frontiers in Physiology 2022, 13, 852094. [Google Scholar] [CrossRef]
- Fermino, R. C. , Winiarski, Z. H., Da Rosa, R. J., Lorenci, L. G., Buso, S., Simão, R. Influence of the specific warm-up and stretching in the performance of the muscular force in 10 maximum repetitions. Rev Bras Cie e Mov, 2005, 13, 25-32.
- Parameswarppa, S. B. , Narayana, J. Impact of noise hearing and hypertension among works in steel industry. Int J Curr Microbiol App Sci 2015, 4, 124–133. [Google Scholar]
- Becker, B. Synthesizing standardized mean-change measures. British Journal of Mathematical and Statistical Psychology 1988, 41, 257–278. [Google Scholar] [CrossRef]
- Morris, S. B. Estimating effect sizes from pretest-posttest-control group designs. Organizational Research Methods 2007, 11, 364–386. [Google Scholar] [CrossRef]
- Smith Lindsey, J. Wolff and Beretvas, S. Natasha (2009) “Estimation of the standardized mean difference for repeated measures designs,” Journal of Modern Applied Statistical Methods: Vol.8: Iss. 2, Article 27.
- Monteiro, E. R. , Costa, P. B., Corrêa Neto, V. G., Hoogenboom, B. J., Steele, J., Silva Novaes, J. D. Posterior Thigh Foam Rolling Increases Knee Extension Fatigue and Passive Shoulder Range-of-Motion. J Strength Cond Res, 2019, 33, 987-994.
- Halperin, I. , Copithorne, D., Behm, D. G. Unilateral isometric muscle fatigue decreases force production and activation of contralateral knee extensors but not elbow flexors. Appl Physiol Nutr Metab 2014, 39, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Halperin, I. , Chapman, D. W., Behm, D. G. Non-local muscle fatigue: effects and possible mechanisms. Eur J Appl Physiol 2015, 115, 2031–2048. [Google Scholar] [CrossRef] [PubMed]
- Behm, D. G. , Alizadeh, S., Hadjizedah Anvar, S., Hanlon, C., Ramsay, E., Mahmoud, M. M. I., et al. Non-local muscle fatigue effects on muscle strength, power, and endurance in healthy individuals: A systematic review with meta-analysis. Sports Med, 2021, 51, 1893-1907. [CrossRef]
- Aboodarda, S. J. , Copithorne, D. B., Power, K. E., Drinkwater, E., Behm, G. Excitability of the knee extensors. Appl Physiol Nutr Metab, 2015, 40, 924-930.
- Šambaher, N. , Aboodarda, S. J., Behm, D. G. Bilateral knee extensor fatigue modulates force and responsiveness of the corticospinal path-way in the non-fatigued, dominant elbow flexors. Front Hum Neurosci, 2016, 10, 18-24.
- Aboodarda, S. J. , Šambaher, N., Millet, Gy., Behm, D. G. Knee extensors neuromuscular fatigue changes the corticospinal pathway excitability in biceps brachii muscle. Neuroscience 2017, 340, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Behm, D. G. , Button, D. C., Barbour, G., Butt, J. C., Young, W. B. Conflicting effects of fatigue and potentiation on voluntary force. J Strength Cond Res 2004, 18, 365–372. [Google Scholar] [PubMed]
- Santana, H. G. , Lara, B., da Silva, F. C. A., Eiras, P. M., Paz, G. A., Willardson, J. M., et al. Total training volume and muscle soreness parameters performing agonist or antagonist foam rolling between sets. Sports, 2021, 9, 57.
- Rubini, E. C. , Costa, A. L., Gomes, P. S. The Effects of Stretching on Strength Performance. Sports Med 2007, 37, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Atherton, P. J. , Babraj, J., Smith, K., Singh, J., Rennie, M. J., Wackerhage, H. Selective activation of AMPK-PGC-1alpha or PKB-TSC2-mTOR signaling can explain specific adaptive responses to endurance or resistance training-like electrical muscle stimulation. FASEB J, 2005, 19, 786-778.
- Ramadoss, R. , Stanzione, J. R., Volpe, S. L. A Comparison of Substrate Utilization Profiles During Maximal and Submaximal Exercise Tests in Athletes. Front Psychol 2022, 13, 854451. [Google Scholar] [CrossRef] [PubMed]
- Anthi, X. , Dimitrios, P., Christos, K. On the mechanisms of post-activation potentiation: the contribution of neural factors. Journal of Physical Education and Sport, 2014, 14, 134-137.
- Figueiredo, T. , Rhea, M. R., Peterson, M., Miranda, H., Bentes, C. M., Reis, V. M. R., et al. Influence of number of sets on blood pressure and heart rate variability after a strength training session. J Strength Cond Res 2015, 29, 1556–1563. [Google Scholar] [CrossRef]
- MacDougall, J. D. , Tuxen, D., Sale, D. G., Moroz, J. R., Sutton, J. R. Arterial blood pressure response to heavy resistance exercise. J Appl Physiol 1985, 58, 785–790. [Google Scholar] [CrossRef]
- Monteiro, E. R. , Vingren, J. L., Pescatello, L. S., Corrêa Neto, V. G., Brown, A. F., Kingsley, J. D, et al. Effects of foam rolling and strength training on post exercise hypotension in normotensive women: A cross-over study. J Bodyw Mov Ther, 2023, 34, 81-86.
- Liao, I. C. , Chen, S. L., Wang, M. Y., Tsai, P. S. Effects of massage on blood pressure in patients with hypertension and prehypertension: a meta-analysis of randomized controlled trials. J Cardiovasc Nurs, 2016, 31, 73-83.
- White, D. W. , Raven, P. B. Autonomic neural control of heart rate during dynamic exercise: Revisited. J Physiol, 2014, 592, 2491-2500.
- Farinatti, P. , Polito, M. D., Massaferri, R., Monteiro, W. D., Vasconcelos, D., Johson, B. T., et al. Postexercise hypotension due to resistance exercise is not mediated by autonomic control: a systematic review an meta-analysis. Autonomic Neuroscience, 2021, 234, 102825.
- Forjaz, C. L. deM., Santaella, D. F., Rezende, L. O., Barretto, A. C. P., Negrão, C. E. Exercise duration determines the magnitude and duration of post-exercise hypotension. Arquivos Brasileiros de Cardiologia, 1998, 70, 99-104.
- Inami, T. , Bara, R., Nakagari, A., Shimizu, T. Acute changes in peripheral vascular tonus and systemic circulation during static stretching. Res Sports Med 2015, 23, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Kruse, N. T. , Scheuermann, B. W. Cardiovascular responses to skeletal muscle stretching: “stretching” the truth or a new exercise paradigm for cardiovascular medicine? Sports Med 2017, 47, 2507–2520. [Google Scholar] [CrossRef] [PubMed]
- Esformes, J. L. , Norman, F., Sigley, J., Birch, K. M. The influence of menstrual cycle phase upon postexercise hypotension. Med Sci Sports Exerc 2006, 38, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, A. C. C. , Rezk, C. C., Teixeira, L., Tinucci, T., Mion, D., Forjaz, C. L. M. Gender influence on post-resistance exercise hypotension and hemodynamics. Int J Sports Med, 2013, 34, 939-944.
Figure 1.
Study design. CC = control condition; ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise warm-up followed by strength training; SE+ST = stretching exercise warm-up followed by strength training.
Figure 1.
Study design. CC = control condition; ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise warm-up followed by strength training; SE+ST = stretching exercise warm-up followed by strength training.
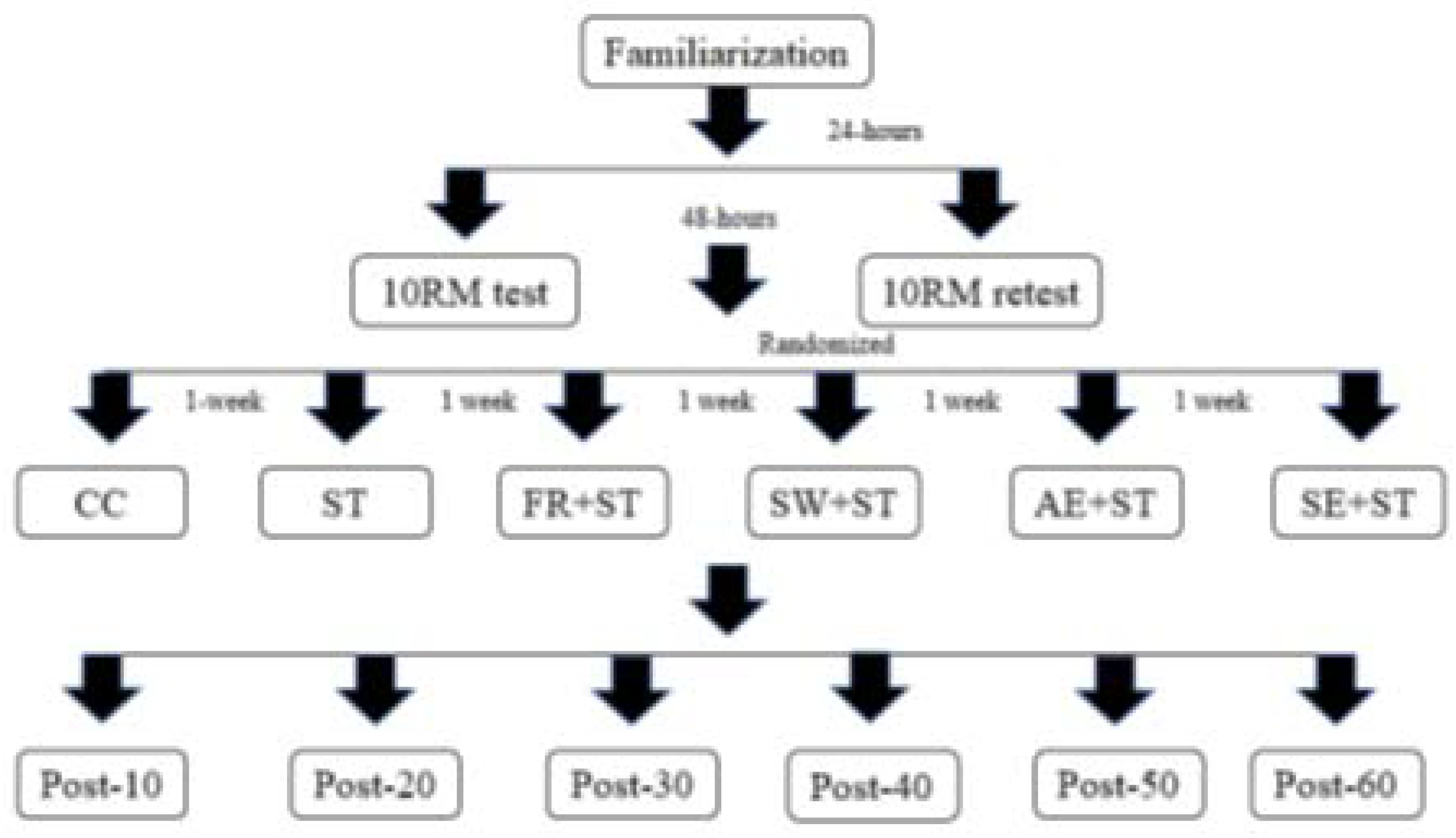
Figure 2.
CC = control condition; ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise warm-up followed by strength training; SE+ST = stretching exercise warm-up followed by strength training.
Figure 2.
CC = control condition; ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise warm-up followed by strength training; SE+ST = stretching exercise warm-up followed by strength training.
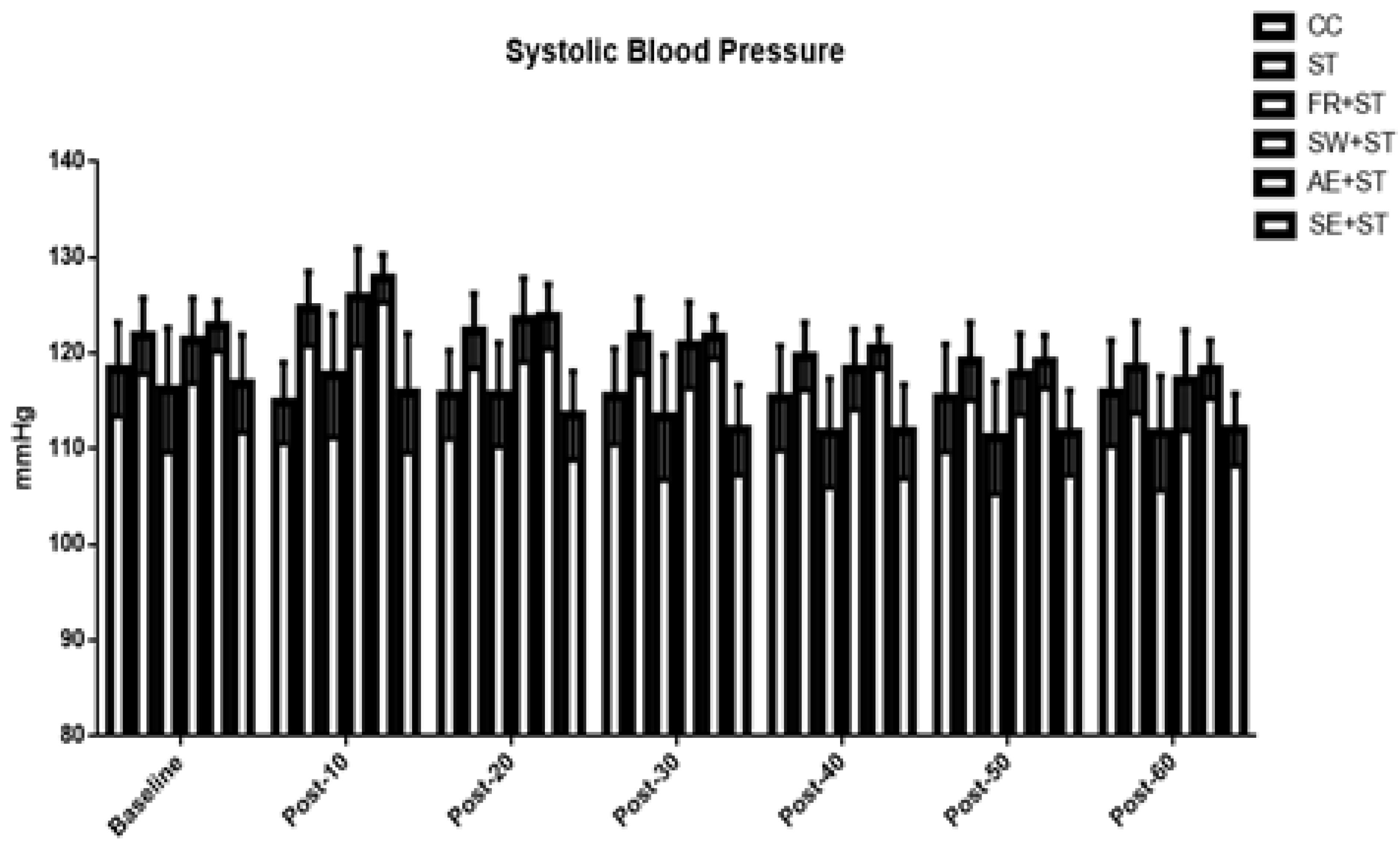
Figure 3.
CC = control condition; ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise warm-up followed by strength training; SE+ST = stretching exercise warm-up followed by strength training.
Figure 3.
CC = control condition; ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise warm-up followed by strength training; SE+ST = stretching exercise warm-up followed by strength training.
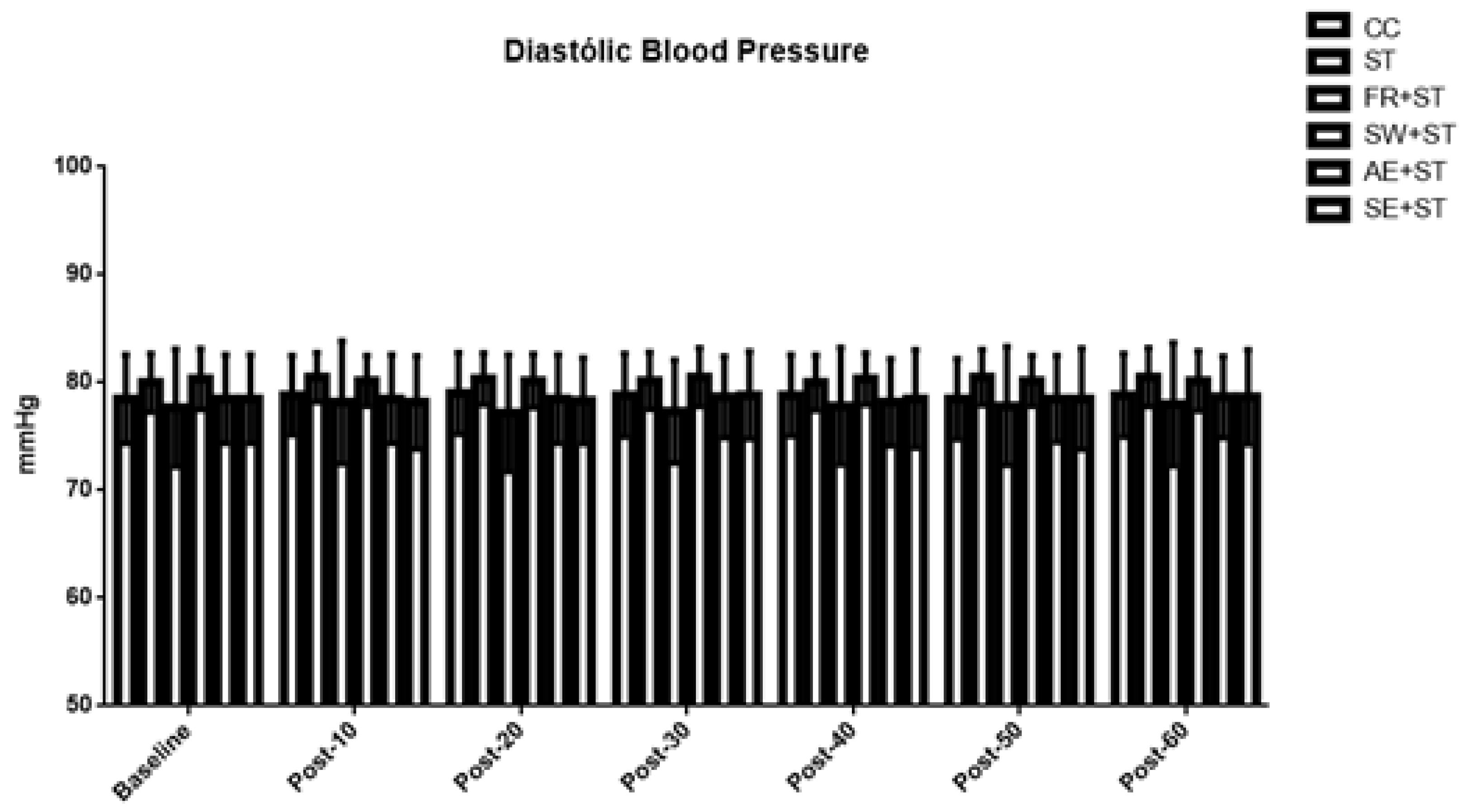

Table 1.
Subject’s load characteristics.
| Variable | Mean ± SD |
|---|---|
| Bench Press 10RM Test (kg) | 36.33 ± 3.98 |
| Bench Press 10RM Retest (kg) | 36.17 ± 3.46 |
| Bench Press 10RM ICC | 0.824 (CV% = 12.23) |
| Back Squat 10RM Test (kg) | 59.33 ± 10.49 |
| Back Squat 10RM Retest (kg) | 60.50 ± 13.35 |
| Back Squat 10RM ICC | 0.946 (CV% = 21.01) |
| Bench Press 45º 10RM Test (kg) | 34.00 ± 4.18 |
| Bench Press 45º 10RM Retest (kg) | 33.83 ± 3.01 |
| Bench Press 45º 10RM ICC | 0.555 (CV% = 13.68) |
| Front Squat 10RM Test (kg) | 44.83 ± 7.79 |
| Front Squat 10RM Retest (kg) | 43.33 ± 7.69 |
| Front Squat 10RM ICC | 0.861 (CV% = 19.98) |
| Lat Pull-Down 10RM Test (kg) | 42.92 ± 8.38 |
| Lat Pull-Down 10RM Retest (kg) | 41.6 ± 6.85 |
| Lat Pull-Down 10RM ICC | 0.908 (CV% = 8.37) |
| Leg Press 10RM Test (kg) | 233.33 ± 47.67 |
| Leg Press 10RM Retest (kg) | 231.67 ± 36.64 |
| Leg Press 10RM ICC | 0.9230 (CV% = 13.11) |
| Shoulder Press 10RM Test (kg) | 35.42 ± 4.75 |
| Shoulder Press 10RM Retest (kg) | 35.83 ± 5.47 |
| Shoulder Press 10RM ICC | 0.920 (CV% = 13.11) |
| Leg Extension 10RM Test (kg) | 80.83 ± 11.65 |
| Leg Extension 10RM Retest (kg) | 81.25 ± 10.69 |
| Leg Extension 10RM ICC | 0.972 (CV% = 13.17) |
Legend: 10RM = ten repetition maximum; ICC = Intraclass Coefficient for 10 RM test and Retest.
Table 2.
Total training volume throughout each exercise and conditions.
| Protocols | ||||||
|---|---|---|---|---|---|---|
| Exercises | ST | FR+ST | SW+ST | AE+ST | SE+ST | |
| Bench Press | 2550 (2360 - 2895) | 2172 (2017 - 2403)* | 2172 (2080 – 2397.5)* | 2217 (2097.5 – 2719.5) | 2311 (2166 – 2420.5)* | |
| Back Squat | 3080 (2657.5 – 3227.5) | 2465 (2262.5 - 2860)* | 2530 (2257.5 - 3117.5)* | 2860 (2447.5 - 3090) | 2725 (2447.5 - 3142.5) | |
| Bench Press 45º | 2377.5 ± 374.97 | 1955 ± 258.77* | 2056.5 ± 354.9* | 2109.5 ± 2776* | 2165.33 ± 311.47# | |
| Front Squat | 2094 (1981-2447) | 1812 (1528,5 - 1963,5)* | 1902 (1685.5 – 2189.5)* | 1818 (1632 - 2136)* | 1877 (1692 - 2315.5)* | |
| Lat Pull-Down | 2347.5 (2191.25 – 2683.75) | 2017.5 (1780-2197.5)* | 2062.5 (1927.5 - 2307.5)* | 2210 (1940 - 2250)* | 2185 (1807.5 – 2362.5)* | |
| Leg Press | 6810 (5600-7995) | 5740 (4800 - 6945)* | 5720 (5010 - 6500)* | 5880 (5220 - 7210)* | 5740 (4800 - 6665)* | |
| Shoulder Press | 997.5 (976.25 – 1156.87) | 842.5 (743.75 – 1023.75)* | 880 (770 - 1035)* | 918.75 (813.75 – 1059.37)* | 915 (817.5 - 1050) | |
| Leg Extension | 2280 (2115-2485) | 1865 (1697.5 - 2160)* | 2007.5 (1760 – 2197.5)* | 2058.75 (1852.5 - 2295) | 1988.75 (1825-2360) | |
Legend: ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise followed by strength training; SE+ST = stretching exercise followed by strength training. +Values represented by median and interquartile range. ++Values represented by mean and standard deviation. *Significant difference (p<0.05) in relation to the ST condition; #significant difference (p<0.05) in relation to the FR+ST protocol.
Table 3.
Maximum repetition performance and fatigue index values for each exercise and conditions (Median (Interquartile Range)).
Table 3.
Maximum repetition performance and fatigue index values for each exercise and conditions (Median (Interquartile Range)).
| Set 1 | Set 2 | Set 3 | FI (%) | |
|---|---|---|---|---|
| BENCH PRESS | ||||
| ST | 10 (9.25-10.75) | 10 (9-10.75) | 9 (9-10) | 90 (84.99-100) |
| FR+ST | 9 (8.25-10) | 8 (8-9)@ | 7 (6-8)*@ | 73.86 (63.54-86.66)@ |
| SW+ST | 9.5 (9-10) | 8 (7.25-8.5)#@ | 7.5 (7-8)*@ | 78.89 (70-86.66)@ |
| AE+ST | 9.5 (9-10) | 9 (8-9.75) | 8 (7-9)* | 85.35 (71.94-100) |
| SE+ST | 9 (9-10) | 8 (7.25-9)@ | 8 (7-9)* | 80 (77.78-100) |
| BACK SQUAT | ||||
| ST | 10 (9.25-10.75) | 9.5 (9-10) | 9 (9-10) | 90.45 (90-100) |
| FR+ST | 10 (9-10) | 8 (7-8.75)@ | 7 (5.25-7)*@ | 70 (60-77.78)@& |
| SW+ST | 9 (8-9.75) | 8 (7-9)@ | 7.5 (7-9)* | 87.5 (77.78-97.5) |
| AE+ST | 9 (9-10) | 9 (8-9) | 8 (7-9.75) | 88.19 (80-100) |
| SE+ST | 9.5 (9-10) | 9 (8.25-10) | 8 (7-8.75) | 80 (77.78-97.22) |
| BENCH PRESS 45º | ||||
| ST | 10 (9-10) | 10 (9-10) | 9.5 (9-10) | 95.45 (90-108.33) |
| FR+ST | 9 (8-10) | 8 (7.25-8.75)@ | 7 (6-7.75)*@ | 76.39 (71.25-80)@ |
| SW+ST | 9 (8-9.75) | 8 (8-9) | 7.5 (7-9)*@ | 88.19 (71.25-100) |
| AE+ST | 9 (9-10) | 8 (8-9) | 8 (7.25-9)* | 88.89 (80-100) |
| SE+ST | 9.5 (9-10) | 9 (8-10) | 8 (7-8.75) | 80 (77.78-97.22) |
| FRONT SQUAT | ||||
| ST | 10 (9.25-10.75) | 10 (9.25-10.75) | 9.5 (9-10) | 100 (83.86-107.5) |
| FR+ST | 9 (8.25-10) | 8 (7-9)@ | 7 (6-7)*@ | 72,5 (67.5-79.44)@ |
| SW+ST | 9 (9-10) | 8.5 (8-9) | 8 (7-8.75)*@ | 83.75 (77.78-90) |
| AE+ST | 9.5 (8.25-10) | 8 (7.25-9)@ | 7 (7-8)*@ | 78.89 (70-87.5)@ |
| SE+ST | 10 (9-10) | 95 (8-10.75) | 7.5 (7-8.75)*$@ | 78.89 (70-95)@ |
| LAT PULL-DOWN | ||||
| ST | 10 (9-10.75) | 10 (9-10) | 9 (9-10) | 100 (83.86-100) |
| FR+ST | 9.5 (9-10) | 8 (7.25-9)@ | 6.5 (6-7.75)*@ | 68.33 (56.67-79.44)@ |
| SW+ST | 9.5 (9-10) | 8.5 (8-9) | 7 (7-8)*@ | 78.89 (70-88.89) |
| AE+ST | 9.5 (9-10) | 8 (7.25-9)@ | 8 (7.25-9) | 88.19 (80-100) |
| SE+ST | 10 (9-10) | 8 (8-10) | 8 (7-8)*@ | 80 (77.78-95) |
| LEG PRESS | ||||
| ST | 10 (9-10) | 9.5 (9-10) | 9 (9-10) | 95 (90-111.11) |
| FR+ST | 9 (8.25-10) | 8 (8-8.75)@ | 7 (6.25-8)*@ | 77.78 (67.5-100) |
| SW+ST | 9 (9-10) | 8 (7.25-9) | 7 (7.25-8)*@ | 78.89 (71.25-85.62)@ |
| AE+ST | 9.5 (9-10) | 8 (7.25-9) | 8 (7-8)*@ | 80 (77.78-100) |
| SE+ST | 9 (9-10) | 8 (7-8.75)@ | 7.5 (7-8)*@ | 83.75 (71.94-88.89)@ |
| SHOULDER PRESS | ||||
| ST | 10 (9-10) | 9 (9-10) | 9 (9-10) | 100 (90-100) |
| FR+ST | 9 (8.25-10) | 8 (7-8)@ | 7.5 (6-8)*@ | 80 (66.67-88.54)@ |
| SW+ST | 9 (9-10) | 8 (7-8.75)# | 7 (7-8)*@ | 78.89 (70-89.72) |
| AE+ST | 9.5 (9-10) | 8 (7.25-9) | 7 (7-8.75)*@ | 77.78 (70-100) |
| SE+ST | 9.5 (9-10) | 9 (7.25-10) | 7.5 (7-9.5)* | 78.89 (75.69-100) |
| LEG EXTENSION | ||||
| ST | 10 (9-10) | 10 (9-10) | 9.5 (9-10) | 100 (92.5-100) |
| FR+ST | 9 (8-10) | 8 (7-8)@ | 7 (6-8)*@ | 82.85 (70-97.22)@ |
| SW+ST | 9 (8.25-10) | 8 (7-9)@ | 7 (7-8)*@ | 80 (70-88.54)@ |
| AE+ST | 9 (9-10) | 8.5 (7.25-9) | 8 (7-8)*@ | 80 (77.78-97.22) |
| SE+ST | 9.5 (9-10) | 8 (7.25-10) | 8 (7-8)*@ | 80 (75.69-88.89)@ |
Legend: CC = control condition; ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise followed by strength training; SE+ST = stretching exercise followed by strength training. FI = fatigue index. #significant difference between set 1 and set 2 (p < 0.05). *significant difference between set 1 and set 3 (p < 0.05). $significant difference between set 2 and set 3 (p < 0.05). @significant difference for ST (p < 0.05). &significant difference for AE+ST (p < 0.05).
Table 4.
Blood pressure effects sizes throughout all exercises and conditions.
| Protocol | Post-10 | Post-20 | Post-30 | Post-40 | Post-50 | Post-60 |
|---|---|---|---|---|---|---|
| Systolic Blood Pressure | ||||||
| CC | -0.76 (Medium) | -0.56 (Medium) | -0.57 (Medium) | -0.58 (Medium) | -0.57 (Medium) | -0.48 (Small) |
| ST | 0.72 (Medium) | 0.12 (No Effect) | 0.00 (No Effect) | -0.57 (Medium) | -0.66(Medium) | -0.76 (Medium) |
| FR+ST | 0.23 (Small) | -0.08 (No Effect) | -0.43 (Small) | -0.73 (Medium) | -0.80 (Large) | -0.72 (Medium) |
| SW+ST | 0.94 (Large) | 0.49 (Small) | -0.11 (No Effect) | -0.69 (Medium) | -0.80 (Large) | -0.85 (Large) |
| AE+ST | 1.96 (Large) | 0.33 (Small) | -0.47 (Small) | -0.98 (Large) | -1.30 (Large) | -1.42 (Large) |
| SE+ST | -0.17 (No Effect) | -0.68 (Medium) | -0.99 (Large) | -1.00 (Large) | -1.08 (Large) | -1.09 (Large) |
| Diastolic Blood Pressure | ||||||
| CC | 0.08 (No Effect) | 0.12 (No Effect) | 0.08 (No Effect) | 0.08 (No Effect) | 0.00 (No Effect) | 0.08 (No Effect) |
| ST | 0.20 (Small) | 0.12 (No Effect) | 0.06 (No Effect) | 0.00 (No Effect) | 0.18 (No Effect) | 0.18 (No Effect) |
| FR+ST | 0.08 (No Effect) | -0.09 (No Effect) | -0.06 (No Effect) | 0.02 (No Effect) | 0.02 (No Effect) | 0.05 (No Effect) |
| SW+ST | -0.06 (No Effect) | -0.06 (No Effect) | 0.06 (No Effect) | 0.00 (No Effect) | -0.06 (No Effect) | -0.05 (No Effect) |
| AE+ST | 0.00 (No Effect) | 0.00 (No Effect) | 0.04 (No Effect) | -0.08 (No Effect) | 0.00 (No Effect) | 0.04 (No Effect) |
| SE+ST | -0.07 (No Effect) | -0.04 (No Effect) | 0.08 (No Effect) | 0.00 (No Effect) | 0.00 (No Effect) | 0.04 (No Effect) |
Legend: CC = control condition; ST = strength training isolated; FR+ST = foam rolling warm-up followed by strength training; SW+ST = specific warm-up followed by strength training; AE+ST = aerobic exercise warm-up followed by strength training; SE+ST = stretching exercise warm-up followed by strength training.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



