
Submitted:
27 June 2024
Posted:
28 June 2024
You are already at the latest version
Abstract
Background: Our previous study highlighted important healthcare access and utilization concerns among new immigrants. Hence, in this study, we aimed to explore the role of public and patient involvement (PPI) may have in enhancing the accessibility and their contribution to migration health studies. Method: An open and in-depth interactive consecutive virtual discussion was conducted among volunteer asylum seekers and refugees from Eritrea and Syria in Switzerland. The novel PPI establishment had three phases; inception, training phase, and contribution phase. Result: At the beginning, the concept of PPI was apprehensive to grasp, as it was a new approach. After training and consecutive discussions, volunteers were ardent to engage actively. Hence, among the prime findings were the PPI's role and effect in raising awareness, PPI's role in exploring and communicating the healthcare system accessibilities and utilization among their community, the impact of PPI in echoing the healthcare needs of their fellow migrants, and PPI's contribution in enhancing and strengthening migration health researches. Conclusion: The PPI volunteers in the study were keen to raise their community's awareness through their networks, and bridge the research gap between researchers and the public.
Keywords:
asylum seekers
; engagement
; Eritrea
; migration health research
; migrants
; public and patient involvement
; refugees
; Switzerland
; Syria
1. Introduction
1.1. Background and Context
Switzerland hosts a considerable number of refugees and asylum seekers every year, in addition to the regular workforce immigrants, which is comparable to other European countries. Among a population of 8.7 million in 2023 [1], the Swiss State Secretariat for Migration (SEM) reported nearly 2.3 million permanent and non-permanent foreign residents living in Switzerland in 2022 [2].
The mounting figure of migrants, asylum seekers and refugees raised concerns among the public, policy makers, social servants and healthcare service providers. Especially, health disparities among the arriving populations including, infectious diseases, undiagnosed and untreated non-communicable diseases, mental health issues, and mother-and-child health. In view of the constant challenge on healthcare provision of host countries, and in an attempt to elevate awareness of public health experts and to inform policy makers, specific research projects have been conducted. Such projects advanced understanding of health problems and needs of newly arriving refugees and asylum seekers. However, evidence regarding the contribution of migrants in health and care-related research activities, in terms of engagement and involvement as co-producers, stakeholders, consortium members, steering committee and other key positions in the life cycle of a research project is scarce.
In an interactive exchange and in-depth engagement with asylum seekers and refugees, we uncovered key perceptions and context-specific know-how of health research among migrants. We jointly explored views on how these perceptions and know-how can contribute to enhance quality and integrity of migration health research.
1.2. Experiences from Previous Research Project
In 2015-2016, a research project was implemented to assess the major healthcare disparities of newly arrived asylum seekers and refugees in Switzerland though screening and surveillance over a 12-month period [3]. Our study highlighted important public health concerns among newly arrived immigrants, limited understanding about host country’s healthcare system, inefficient utilization of services, uninformed about help-seeking behavior, especially for mental health [4]. Additionally, language barriers, fundamental to successful integration and acculturation process, and gainful employment were identified [5].
Perceived needs of asylum seekers are also connected with the so called economic capital, such as daily earnings [6]. This engagement in gainful employment contribute a significant role in the well-being of migrants [7]. However, asylum seekers seems to be not satisfied with the job opportunity offers [8].
Understanding how the new, host healthcare systems functions play key role in accessing and utilizing it. Most refugees from resource limited countries, are confronted with numerous challenges, such as cultural, language and religious barriers, unfamiliarity of the system and inability to cover cost-of-service. The more barriers are apparent, the less likely migrants access the health system and services, which further widens the gap between the service providers and the patients.
1.3. Public and Patient Involvement (PPI)
1.3.1. General Considerations
To address the aforementioned issues, the concept of a migration public and patient involvement (PPI) strategy, and subsequently a PPI group to inform on migration health research to promote research in this area was created at the Swiss Tropical and Public Health Institute (Swiss TPH). The concept of PPI implies working directly with the public in finding or co-creating adapted solutions. PPI is defined as “research being carried out ‘with’ or ‘by’ members of the public rather than ‘to’, ‘about’ or ‘for’ them” [9].
Through PPI group meetings, refugees and asylum seekers can learn how to efficiently access and make use of the available services, become contributors to improving the system for their purposes and actively participate as key informants for their fellow migrants. Additionally, they can learn how to support in developing research projects, by addressing critical questions, and generating evidence for the most relevant issues that interests their community. Hence, their participation and engagement can enhance the credibility of the research conducted in those community, as they say ‘nothing about us, without us’ [10].
1.3.2. The Concept of PPI
PPI in clinical research is a fundamental pillar to foster improved patient-oriented healthcare services and healthcare systems assessments. PPI plays a pivotal role in the interaction of key stakeholders in healthcare research activities, as it provides a link between the population and patients, the healthcare system to researchers [11]. Particularly, for older adult population with great diversity and prime consumers of healthcare system, as they are with rich and lived experiences, such as services provided, they play a key role in the important of health research [12,13]. PPI in clinical research aims to promote better understanding of all involved, and to provide evidence for problems or solutions that can inform policymakers and stakeholders to induce change (Figure 1).
The concept of PPI is not new (Appendix A). Indeed, despite of less frequently reported, only 20% of the recently peer reviewed papers included their PPI report [14], in many Western countries, PPI has been practiced over several decades. The report varies from 3.4% in China to 44.5% in the UK. Some countries have created international collaboration and exchange platforms to tackle challenges and share experiences related to PPI [15]. In Switzerland, along the rising importance of the implementation of the shared decision making process (SDM) within the highly decentralized health care system, the importance of PPI is also progressively being signified, particularly in area of research, clinical trials and as competence for medical school graduates [16]. Likewise, Swiss TPH researchers and their partners have practiced the concept of engaging the public in research for over 20 years [17,18,19].
As an institute with an 80-year history of research, education and services in public and global health with pointed emphasis on LMICs, understanding the cultural and traditional norms of the population before planning any research is unavoidable [20]. Hence, researchers start bilateral discussions with stakeholders in the research setting at the conception stage, setting the agenda together during the planning and preparatory phases of the research [21].
Multiple examples highlight important topics, not only concerning health care directly, but also indirectly such as land and water use, animal studies for one-health projects, mother-and-child health, to name a few [22,23,24]. This requires a transdisciplinary approach involving cross-cutting expertise bridging many disciplines, i.e., anthropology, data sciences, epidemiology, public health, sociology and veterinary medicine [25,26].
A systematic review on PPI practice in LMICs revealed a paucity of publications in engaging patients and the public in clinical research [27]. Though PPI is useful and supports research at every stage of the research life cycle [28], it is most appreciated and effective if implemented in the early stages of research projects, as it enhances the quality of research conducted and its appropriateness to the study population [29]. The production of quality and standardized publication from a co-designed and co-produced project involving the public and the patients have significant effect in reducing unnecessary health- and care-related research wastages [30]. Moreover, PPI not only is supportive to senior researchers, but is also pertinent to early career researchers and professionals to optimize the value, integrity and quality of their research [31].
2. Method
2.1. Exploring Migration PPI, through an Interactive In-Depth Exchange: PPI Group in Health Research during COVID-19 Pandemic
Despite the Coronavirus disease 2019 (COVID-19) pandemic and important public health measures implemented in 2021, we felt an urgency to start a PPI group. Hence, we contacted refugees and migrants with a view to engage them and enable us to have a better understanding of the research process among these populations. Our aim was to enhance trust for migrants to contribute, engage, and actively participate in public health research. Moreover, by creating a platform, we hoped to enable them to share their healthcare needs and priorities. As specific COVID-19 restrictions were imposed, including prolonged lockdowns over parts of 2021, the need for a PPI group, and avoiding isolation became even more apparent than initially anticipated. The PPI group consisted of seven adult males and seven adult females from Eritrea and Syria. Meetings were adapted and re-organized taking into consideration COVID-19 restrictions. The group thus met virtually.
2.2. Selection of Volunteers
Participants of this PPI project were either enrolled from a previous study [3], or invited to participate through existing networks. The three main reasons for contacting people to take part in the new PPI project were as follows. First, they were familiar with the home country healthcare services and its benefits and challenges. Second, as they arrived in Switzerland a while ago, they were somewhat acquainted and already integrated into the host country. Third, they had already settled in Switzerland and were part of the migrant network.
2.3. Stages of Establishing a PPI for Migration Health Research
As represented in the flow chart depicted in Figure 2, the establishment of a novel PPI for migration health research consisted of three distinctive phases; the inception phase, the training phase and the contribution phase. Asylum seekers and refugees, with no background in PPI were invited voluntary to take part in the current PPI project. No incentives were given.
During the inception or conception phase, necessary information, such as the meaning of a PPI, the roles and responsibilities of volunteers were explained. In the following training phase, through continuous meetings and discussions held virtually mainly due to COVID-19 restrictions, volunteers had the opportunity to practice and express their views, opinions, suggestions and other valuable information for PPI as part of their trainings. In the contribution phase, some of the volunteers were further involved into some existing health research projects or activities, such as serving as interpreters and translators.
From the early stage, every member of the PPI was motivated to share his or her opinion without guidance or lead to any specific point of discussion. This subsequently fostered a discussion, and “broke the ice” to allow for opinions, expressions and experiences to be shared without any limit or boundaries of ideas, thoughts and feelings. Through these continuous meetings and discussions, group members would advance in their understanding about the PPI, and raise important health concerns, which eventually could develop into a research question.
In the following stage, health research and its importance were the focus of discussion. Topics such as “What is health research”? “How it is conducted”? “Who is responsible”? “What procedure does it follow” were jointly explored. The moderator assisted in guiding the discussion and motivated the participants to raise critical issues to engage within the group.
In the advanced stage, the PPI group provided active input on either ongoing research projects or projects under construction. Involving the PPI group at the early stage of a research project, from setting the research question and proposal writing stage, is proven effective in producing quality research project [28,32,33,34].
2.4. Realization of the PPI Establishment
Due to the participants’ situation, such as work and family conditions, and accessibility and connectivity of the internet, conducting the regular monthly meetings were often challenging. Finding a convenient time for all participants was crucial. Hence, a meeting was arranged every 4-6 weeks. Table 1 summarizes the characteristics of the first meetings held among Eritrean and Syrian PPI volunteers that were conducted separately.
2.5. Criteria for Evaluation, Including Quantitative and Qualitative Indicators
In order to evaluate this PPI migration health research group, the first of its kind in Switzerland, some key indicators were identified for its success.
Participation rate and adherence: At every virtual meeting, participation of more than 70% of the volunteers was regarded as good intention and will of the group for the success of the initiation.
Active participation and contribution: bringing new ideas, questions, comments and suggestion about their community was regarded as measure of gradual increase in the concept of the PPI and their motivation.
Inviting new volunteer compatriots: this can be considered as a gage for the increasing awareness of the importance and effect of PPI in health research.
Proposing new discussion topics: this is an indication that volunteers and the way the reach out to their communities to explore about healthcare-related disparities or problems in their communities, is enhanced
3. Results
3.1. Reaching out Participants
Following multiple meetings with potential candidates and team members, volunteers were initially recruited through these existing migrant centers and networks due to the COVID-19 pandemic. In this first of its type initiative, 14 volunteers showed an interest to participate (Table 1).
The findings or views from this novel approach to explore the know-how of asylum seekers and refugees regarding PP,I and its role in health research activities are presented in the following four thematic subtopics. Thematic presentation of the broadly discussed PPI would funnel and transform the ideas, views, comments, suggestions, and remarks, and likes made by the participants into tangible evidence based proofs.
3.2. Orientation and Clarification of PPI among Migrants
The concept of PPI was initially hard to grasp for our participants, as it was new and they were not used to openly discuss about their health needs. Several questions and inquires underscore this issue. ’What is the difference between PPI and being participating in research?’, ‘What benefit does make PPI for migrants?’, ‘How does PPI works?’ and ‘What if someone does not have a medical background, or training as health professional?’
The clarifications provided by the coordinators proved effective, as participants became more involved in the discussions. Basic background of how a PPI works and the benefits it provides to the public, particularly in the research area, were explained to participants, including specific examples.
3.3. Willingness to Attend PPI Migration Health Research Program
All participants expressed interest in the initiative. They considered the project as an opportunity to openly share their know-how, exposure to, and personal experiences with, research, and discuss challenges with peers and instructors. We hoped that this open platform for discussions and exchange could uncover obstacles that hinder their access to healthcare system and its effective utilization. Moreover, this was an opportunity to bridge science and the public for a deeper understanding of health and well-being of vulnerable population. Migrants, particularly those deprived or isolated from the healthcare system facilities and privileges, undocumented migrants and asylum seekers who are still not yet granted a permit to stay in the host country, and cannot generate any form of income, are predominantly exposed to risk of isolation from the healthcare system. Hence, through PPI group representation of their community, their healthcare access barriers, health service needs and priorities could be shared with investigators, and subsequently to policy makers and funding organization.
3.4. Engagements and Contribution of Participants
Despite the diverse background of the participants, including non-health professionals, they actively contributed to lively and informative discussions. They abundantly shared personal experiences in healthcare services, be it in their home countries or while being a refugee in host country. Others shared experiences from their beloved ones. Others also shared what they acquired from the mass media and social media. Discussion were interactive and highly engaged, sharing a vast body of experiences, which provided valuable ideas for potential research topics in further studies.
3.5. Inputs and Propositions of PPI Members
Most inputs pertained to communities’ healthcare service challenges. Recurrent questions were asked such as: ‘How to overcome barriers in accessing healthcare services in Switzerland?’, ‘Why is the insurance system so difficult to understand?’, ‘Where can newly arrived refugees get information about how the healthcare service in the country works easily?’ and ‘How can culturally competent healthcare service be developed and implemented for migrants?’
Additionally, specific inquiries were raised that need consideration in migration health research, such as maternal and child health care, regular checkups, dental healthcare insurance, family physician and the regulations, among others. Others wondered about drug prescription such as antibiotics, as they noted considerable differences in their home county and the host country Switzerland.
4. Discussion
4.1. Role and Effect of PPI on Raising Awareness of Research Importance
In general, participants of this first PPI training session agreed that the initiative provides a bridge that connects the community with academia.
‘The migrant community need to be actively engaged in health research, as it is for their benefits and benefit of other community. In addition, also research is conducted for the benefit of future generation. Hence, the community needs to consider and care for future generations, by engaging themselves in research activities’ (37-year-old male migrant from Eritrea).
Additionally, it was emphasized as,
‘Health research is a means of educating the community, and provides an opportunity of gathering information for educating the public and raising awareness, and can positively impact the health of the people’ (37-year-old male migrant from Eritrea).
The following example highlights the personal experience of a PPI member from earlier migration health study [3].
‘I benefited from partaking in a migration health screening research project. Asymptomatic parasitic infectious diseases were diagnosed. Hence, self-involvements in health-related research projects benefits the participants both through access to medical care service and increasing awareness of the health system, and related information’ (40-year-old male migrant from Eritrea).
Despite the anxiety migrants have, they are aware of their needs to be screened and diagnosed for specific health issues. They are also aware of the importance of adequate treatment as quickly as possible according to what the healthcare system can offer. Nevertheless, due to misconceptions, mistrust, suspicions and fear of stigmatization, most of them hesitate to visit any facilities to seek help, and join research activities.
‘It is obvious that there are symptomatic and asymptomatic health problems. We have difficulties, and problems. We consider ourselves as healthy; however, we know that we are not. It was only after we were diagnosed, and participated in research projects such as the migration health study, conducted by Swiss TPH, that we became aware of some health issues. If our participation in research is low, you (the researchers) need to raise our awareness’ (40-year-old male migrant from Eritrea).
Researchers not only need to raise awareness of migrants to partake in research studies, but they also need to understand the problem of the community, in order to raise appropriate research questions.
‘Only the people themselves know best about their problems’ (38-year-old male migrant form Eritrea).
In order to identify the best solutions for migrants’ health problems, migrants themselves are able to provide valuable information, and can contribute to the facilitation of the problem solving. Hence, clinicians and researchers involved in migrant health need to critically assess whether they really involve, engage and empower the public and patients, through consulting, partnering and authorizing [35].
From migrants’ perspective, one PPI member emphasized on mental health related studies’ needs and commented as follows:
‘Most studies [medical research studies including mental health] focus on diseases instead of the causes for the diseases. Among the causes to be mentioned, for example, are worries and stress leading to different diseases. It is better to concentrate of the root cause for those worries, stressors and others’ (40-year-old male migrant from Eritrea).
This consideration suggests migrants’ intrinsic needs to fully understand the cumulative root causes of mental health burden, from pre-migration trauma to transit time shocks to post-migratory stressors and its influence and potential exacerbation of other health issues.
Another participant underlined the need for country specific and individualized approaches to mental health, including the need to avoid over generalization, which could exacerbate and prevent further health seeking behavior. The logic behind these considerations could be that, despite of their similar post-migration conditions, the stressors, including pre- and during-migration routes are different. Hence, they might have diverse effects in the migrants’ mental status and stability. As a result, different models of intervention and treatment of the mental health condition might need to be considered and applied separately to different communities.
‘It is not good to generalize among refugees, for example among Eritreans and Syrians. As Eritreans, we are different from the Syrians, many they arrive with their families together, but we [Eritreans] arrive through challenges of long migration journeys, and mostly we live alone by ourselves. To solve all those problems, specific treatment procedures need to be adapted to each group, rather than generalizing all together’ (33-year-old male migrant from Eritrea).
4.2. PPI on Communicating Healthcare System Accessibilities and Utilization
Among the first migrants’ PPI discussions, central themes emerged, such as healthcare system accessibility and its effective utilization, and understanding the insurance system. Regarding access to health systems, most of the PPI group members agreed that the health system is not easily understood by refugees, particularly for new arrivals. Despite the availability and legal rights to use it, many of the participants faced difficulties for reaching out and accessing it:
‘Even though there are ample healthcare access facilities here in Switzerland, how can we improve our awareness, so that we can utilize the health system provided for us effectively and efficiently?’ (28-year-old female migrant from Eritrea).
For example, a 29-year-old Eritrean female participant highlighted initiatives that are taken by individuals to raise awareness and enhance familiarization with the health system:
‘Due to limited awareness, we are not utilizing the system. Initiatives such as those by Dr. Fana Asefaw, are helping women to increase awareness of women health’.
Even after accessing the system and receiving the service, there is still a sense of dissatisfaction on the diagnosis process and treatment prescription offered. For refugees, the provided diagnosis and treatments seem to be slow and taking unnecessary time of their healing and recovering time. In addition, dosage prescription, antibiotics for example, could be different from the system in their home countries, as expressed by a 29-year-old Syrian female participant:
‘Medically it’s the best approach, to gradually increase the medications doses and start with the least ones, but the environment and the culture that we came from make it hard for us to understand that. In Syria, we directly take Augmentin 1000 mg for example for a slight flu with fever, and this high consumption of antibiotics did harm us. Now the lower doses does not work on our bodies at all’.
Finally, most refugees and asylum seekers in Switzerland that we encountered originated mainly from LMICs with weak healthcare system and out-of-pocket payments. Hence, they face challenges learning and negotiating the host county’s systems, often based on insurance coverage. This potentially affects how migrants and refugees access healthcare, preventing them from readily integrating, getting early diagnosis and treatment on time, which in-turn averts sequel from complication of treatable diseases. The following were among the issues discussed in the PPI meetings:
‘We did not get an explanation as refugees about the type of health insurance we have and the coverage’ (33-year-old male Syrian participant).
‘The insurance contracts is too hard to cancel, they need reasons and special dates to be cancelled, otherwise will be renewed automatically, the language barrier is a very important element here’ (26-year-old female Syrian participant). Another participant emphasized:
‘Some insurance wages differs from one year to another, we do not understand according to what, how to choose the best one when we have the choice’ (27-year-old female Syrian participant).
4.3. Limitation of the Migration PPI Group Interactive Exchange
In our experience to date and early PPI stage, most of the participants were at their initial stage of integration and settling into the host country. This perhaps also explain why their healthcare needs and challenges might seem more difficulty and are different in comparison to their compatriots who were at an advanced stage of integration within Switzerland. We might have had a deeper insight in case interaction were in person rather that online due to the COVID-19 pandemic. Communicating effectively and sharing of thoughts might have been more fruitful, had the meetings been in-person.
5. Conclusion
This small-scale, first of its kind migrants’ PPI initiative, highlighted the importance of PPI among migrant communities in Switzerland. It emphasizes migrants’ issues, involvement or lack of involvement in health-related research, gaps and concerns in accessing healthcare effectively. The following conclusions are offered for consideration. First, PPI is a means to increase awareness of migrants to partake in health research-related projects by bridging the scientific and the migrant communities. Second, PPI can support health researchers to reach out to migrants and identify appropriate research questions, which are meaningful and ethically accepted by the migrants. Third, PPI can mitigate migrants’ fear and suspicions of disseminating the importance of early screening, diagnosing and treatment. Fourth, PPI can enhance the appropriate use of the healthcare system of the host country. Fifth, PPI can facilitate health and appropriate help seeking behavior of migrants through their PPI members and improve their know-how about health systems and related health insurance schemes.
Author Contributions
AC, LA, and ER designed, trained PPI members, and conducted the study. DP has assessed the methodological quality, and reviewed the protocol. AC has conceptualized and drafted the manuscript. ER provided critical expert opinion and reviewed the manuscript. JU and DP supported the study. All authors have contributed to the crucial review of the manuscript, and approved the final version of the protocol.
Funding
No funding.
Ethics approval and consent to participate
Ethical approval is not required for people to get involved in establishing PPI and identifying the role of PPI in the respective groups, such as the current PPI for migration health research at Swiss TPH. Volunteers are solely acting as contributors, and not as research participants. Hence, they serve as external advisors, counselors and source of knowledge and information for the intended research project.
Acknowledgments
Authors are deeply grateful for the dedication and interest the PPI participants reflected despite of the COVID-19 crises. Moreover, we are very much thankful for their valuable experiences and views they shared for the improvement of migration health research.
Conflicts of Interests
The authors declare that they have no competing interests.
Appendix A. Public and Patient Involvement (PPI): Definition and Background
According to the Health Research Authority (HRA), at the National Health Services (NHS) in the United Kingdom (UK), the public and patient involvement (PPI) in health research is defined as research done ‘with’ or ‘by’ the public, and not ‘to’ or ‘for’ the public [36]. This is in-line with the principle of Sherry R. Arnstein’s ladder of citizen participation which was initiated in the 1960s to empower the public [37]. It implies equipping and empowering people to have a sense of ownership, and responsibilities and accountabilities of the research project, than having a mere ‘participatory’ role only. In this ladder. Citizen participation allotted into eight stages categorized into three main categories as non-participation, tokenism and citizen control on top. Likewise, in regards to health and care research, the role of the public and patients range from involvement in the bottom to engagement and to empowering on the top [35].
Public and patients who have received any sort of benefit or services and have an exposure to the health system would be in a position to provide valuable information. A study conducted in the famous rendezvous places, where people frequently gather, hangout together, and get socialized in Singapore, has proven to supplement with information that attracts attention to researchers, which they did not have thought about it or did not consider it [38].
Figure A1.
Sherry R. Arnstein’s ladder of participation [35].
Figure A1.
Sherry R. Arnstein’s ladder of participation [35].
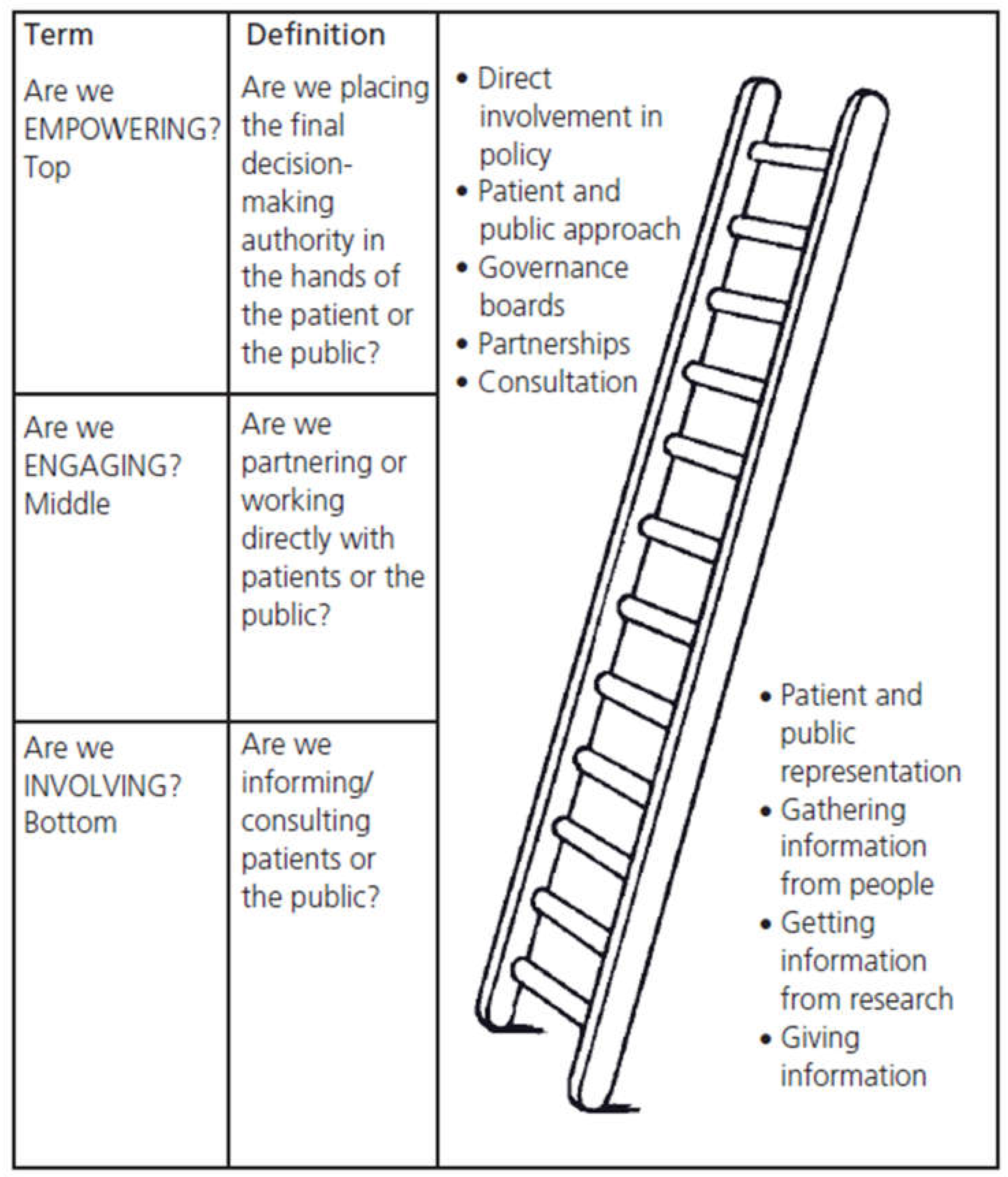
The National Institute for Health and Care Research (NIHR) attributes PPI with three key roles or ways by which the public and patient contribute to the research as involvement, engagement and participation [9]. Therefore, the role of PPI in the health and care research is mainly to encapsulate the vision of “nothing about me without me”, through a paradigm shift away from paternalism towards partnership through mutual collaboration of the public and researchers [39].
References
- FSO, Federal Statistics Office (FSO). Switzerland in 23 infographics: Society, economy, territory and environment - Edition March 2023. 2023.
- SEM, Secretariat for Migration (SEM). Foreign Population and Asylum Statistics 2022. 2023.
- Chernet, A.; Neumayr, A.; Hatz, C.; Kling, K.; Sydow, V.; Rentsch, K.; Utzinger, J.; Probst-Hensch, N.; Marti, H.; Nickel, B.; Labhardt, N. D., Spectrum of infectious diseases among newly arrived Eritrean refugees in Switzerland: a cross-sectional study. Int J Public Health 2018, 63 (2), 233-239. [CrossRef]
- Chernet, A.; Probst-Hensch, N.; Sydow, V.; Paris, D. H.; Labhardt, N. D., Mental health and resilience among Eritrean refugees at arrival and one-year post-registration in Switzerland: a cohort study. BMC Research Notes 2021, 14 (1).
- Melamed, S.; Chernet, A.; Labhardt, N. D.; Probst-Hensch, N.; Pfeiffer, C., Social Resilience and Mental Health Among Eritrean Asylum-Seekers in Switzerland. Qual Health Res 2019, 29 (2), 222-236. [CrossRef]
- Hugelius, K.; Semrau, M.; Holmefur, M., Perceived Needs Among Asylum Seekers in Sweden: A Mixed Methods Study. International Journal of Environmental Research and Public Health 2020, 17 (14), 4983.
- Ingvarsson, L.; Egilson, S. T.; Skaptadottir, U. D., “I want a normal life like everyone else”: Daily life of asylum seekers in Iceland. Scand J Occup Ther 2016, 23 (6), 416-24.
- Morville, A. L.; Erlandsson, L. K.; Danneskiold-Samsøe, B.; Amris, K.; Eklund, M., Satisfaction with daily occupations amongst asylum seekers in Denmark. Scand J Occup Ther 2015, 22 (3), 207-15. [CrossRef]
- NIHR, Briefing notes for researchers - public involvement in NHS, health and social care research. 2021.
- Rahman, A.; Nawaz, S.; Khan, E.; Islam, S., Nothing about us, without us: is for us. Research Involvement and Engagement 2022, 8 (1).
- Lauzon-Schnittka, J.; Audette-Chapdelaine, S.; Boutin, D.; Wilhelmy, C.; Auger, A.-M.; Brodeur, M., The experience of patient partners in research: a qualitative systematic review and thematic synthesis. Research Involvement and Engagement 2022, 8 (1). [CrossRef]
- The Lancet Healthy, L., Increasing patient and public involvement in clinical research. The Lancet Healthy Longevity 2024, 5 (2), e83.
- Riva-Rovedda, F.; Viottini, E.; Calzamiglia, M.; Manghera, F.; Manchovas, G.; Dal Molin, A.; Campagna, S.; Busca, E.; Di Giulio, P., Patient and public involvement in research. Assist Inferm Ric 2023, 42 (3), 152-157.
- Lang, I.; King, A.; Jenkins, G.; Boddy, K.; Khan, Z.; Liabo, K., How common is patient and public involvement (PPI)? Cross-sectional analysis of frequency of PPI reporting in health research papers and associations with methods, funding sources and other factors. BMJ Open 2022, 12 (5), e063356. [CrossRef]
- Staley, K.; Sandvei, M.; Horder, M., A problem shared…‘The challenges of public involvement for researchers in Denmark and the UK. 2019.
- Selby, K.; Durand, M.-A.; Von Plessen, C.; Auer, R.; Biller-Andorno, N.; Krones, T.; Agoritsas, T.; Cornuz, J., Shared decision-making and patient and public involvement: Can they become standard in Switzerland? Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen 2022, 171, 135-138.
- Wyss, K.; Bechir, M.; Schelling, E.; Daugla, D. M.; Zinsstag, J., [Health care services for nomadic people. Lessons learned from research and implementation activities in Chad]. Med Trop (Mars) 2004, 64 (5), 493-6.
- Zinsstag, J.; Hediger, K.; Osman, Y. M.; Abukhattab, S.; Crump, L.; Kaiser-Grolimund, A.; Mauti, S.; Ahmed, A.; Hattendorf, J.; Bonfoh, B.; Heitz-Tokpa, K.; Berger González, M.; Bucher, A.; Lechenne, M.; Tschopp, R.; Obrist, B.; Pelikan, K., The Promotion and Development of One Health at Swiss TPH and Its Greater Potential. Diseases 2022, 10 (3). [CrossRef]
- Acka, C. A.; Raso, G.; N’Goran E, K.; Tschannen, A. B.; Bogoch, II; Séraphin, E.; Tanner, M.; Obrist, B.; Utzinger, J., Parasitic worms: knowledge, attitudes, and practices in Western Côte d’Ivoire with implications for integrated control. PLoS Negl Trop Dis 2010, 4 (12), e910.
- Meier, L.; Casagrande, G.; Dietler, D., The Swiss Tropical and Public Health Institute: Past, present and future. Acta Tropica 2021, 223, 106077. [CrossRef]
- Söckli, B.; Wiesmann, U.; Lys, J., A Guide for Transboundary Research Partnerships: 11 Principles, 3rd edition (1st edition 2012), Bern, Switzerland. Swiss Commission for Research Partnerships with Developing Countries (KFPE). 2018.
- Schmidlin, T.; Hürlimann, E.; Silué, K. D.; Yapi, R. B.; Houngbedji, C.; Kouadio, B. A.; Acka-Douabélé, C. A.; Kouassi, D.; Ouattara, M.; Zouzou, F.; Bonfoh, B.; N’Goran, E. K.; Utzinger, J.; Raso, G., Effects of hygiene and defecation behavior on helminths and intestinal protozoa infections in Taabo, Côte d’Ivoire. PLoS ONE 2013, 8 (6), e65722. [CrossRef]
- Wallenborn, J. T.; Valera, C. B.; Kounnavong, S.; Sayasone, S.; Odermatt, P.; Fink, G., Urban-Rural Gaps in Breastfeeding Practices: Evidence From Lao People’s Democratic Republic. Int J Public Health 2021, 66, 1604062. [CrossRef]
- Zinsstag, J.; Kaiser-Grolimund, A.; Heitz-Tokpa, K.; Sreedharan, R.; Lubroth, J.; Caya, F.; Stone, M.; Brown, H.; Bonfoh, B.; Dobell, E.; Morgan, D.; Homaira, N.; Kock, R.; Hattendorf, J.; Crump, L.; Mauti, S.; Del Rio Vilas, V.; Saikat, S.; Zumla, A.; Heymann, D.; Dar, O.; de la Rocque, S., Advancing One human-animal-environment Health for global health security: what does the evidence say? Lancet 2023, 401 (10376), 591-604.
- Berger-González, M.; Stauffacher, M.; Zinsstag, J.; Edwards, P.; Krütli, P., Transdisciplinary Research on Cancer-Healing Systems Between Biomedicine and the Maya of Guatemala: A Tool for Reciprocal Reflexivity in a Multi-Epistemological Setting. Qual Health Res 2016, 26 (1), 77-91.
- Erismann, S.; Pesantes, M. A.; Beran, D.; Leuenberger, A.; Farnham, A.; Berger Gonzalez De White, M.; Labhardt, N. D.; Tediosi, F.; Akweongo, P.; Kuwawenaruwa, A.; Zinsstag, J.; Brugger, F.; Somerville, C.; Wyss, K.; Prytherch, H., How to bring research evidence into policy? Synthesizing strategies of five research projects in low-and middle-income countries. Health Research Policy and Systems 2021, 19 (1).
- Cook, N.; Siddiqi, N.; Twiddy, M.; Kenyon, R., Patient and public involvement in health research in low and middle-income countries: a systematic review. BMJ Open 2019, 9 (5), e026514. [CrossRef]
- NIHR-NHS, Patient and public involvement in health and social care research: A handbook for researchers. 2015.
- Brett, J.; Staniszewska, S.; Mockford, C.; Herron-Marx, S.; Hughes, J.; Tysall, C.; Suleman, R., Mapping the impact of patient and public involvement on health and social care research: a systematic review. Health Expectations 2014, 17 (5), 637-650. [CrossRef]
- Minogue, V.; Cooke, M.; Donskoy, A.-L.; Vicary, P.; Wells, B., Patient and public involvement in reducing health and care research waste. Research Involvement and Engagement 2018, 4 (1). [CrossRef]
- Biggane, A. M.; Olsen, M.; Williamson, P. R., PPI in research: a reflection from early stage researchers. Research Involvement and Engagement 2019, 5 (1). [CrossRef]
- Kaisler, R. E.; Kulnik, S. T.; Klager, E.; Kletecka-Pulker, M.; Schaden, E.; Stainer-Hochgatterer, A., Introducing patient and public involvement practices to healthcare research in Austria: strategies to promote change at multiple levels. BMJ Open 2021, 11 (8), e045618. [CrossRef]
- HRA_NHS, Public involvement in a pandemic: lessons from the UK COVID-19 public involvement matching service. 2021.
- Pandya-Wood, R.; Barron, D. S.; Elliott, J., A framework for public involvement at the design stage of NHS health and social care research: time to develop ethically conscious standards. Research Involvement and Engagement 2017, 3 (1). [CrossRef]
- Cartwright, J.; Crowe, S., Patient and Public Involvement Toolkit. 1st edition ed.; Blackwell Publishing Ltd.: 2011; p 29.
- HRA-NHS, Health Research Authority-National Health system (HRA-NHS); What is public involvement in research?
- Arnstein, S. R., A Ladder Of Citizen Participation. Journal of the American Institute of Planners 1969, 35 (4), 216-224. [CrossRef]
- Luna Puerta, L.; Smith, H. E., The “PPI Hawker”: an innovative method for patient and public involvement (PPI) in health research. Res Involv Engagem 2020, 6, 31. [CrossRef]
- Stephens, R.; Staniszewska, S., One small step…. Research Involvement and Engagement 2015, 1 (1).
Figure 1.
Pivotal role of a public and patient involvement (PPI) strategy in the relationship of key stakeholders of health and care research and services.
Figure 1.
Pivotal role of a public and patient involvement (PPI) strategy in the relationship of key stakeholders of health and care research and services.
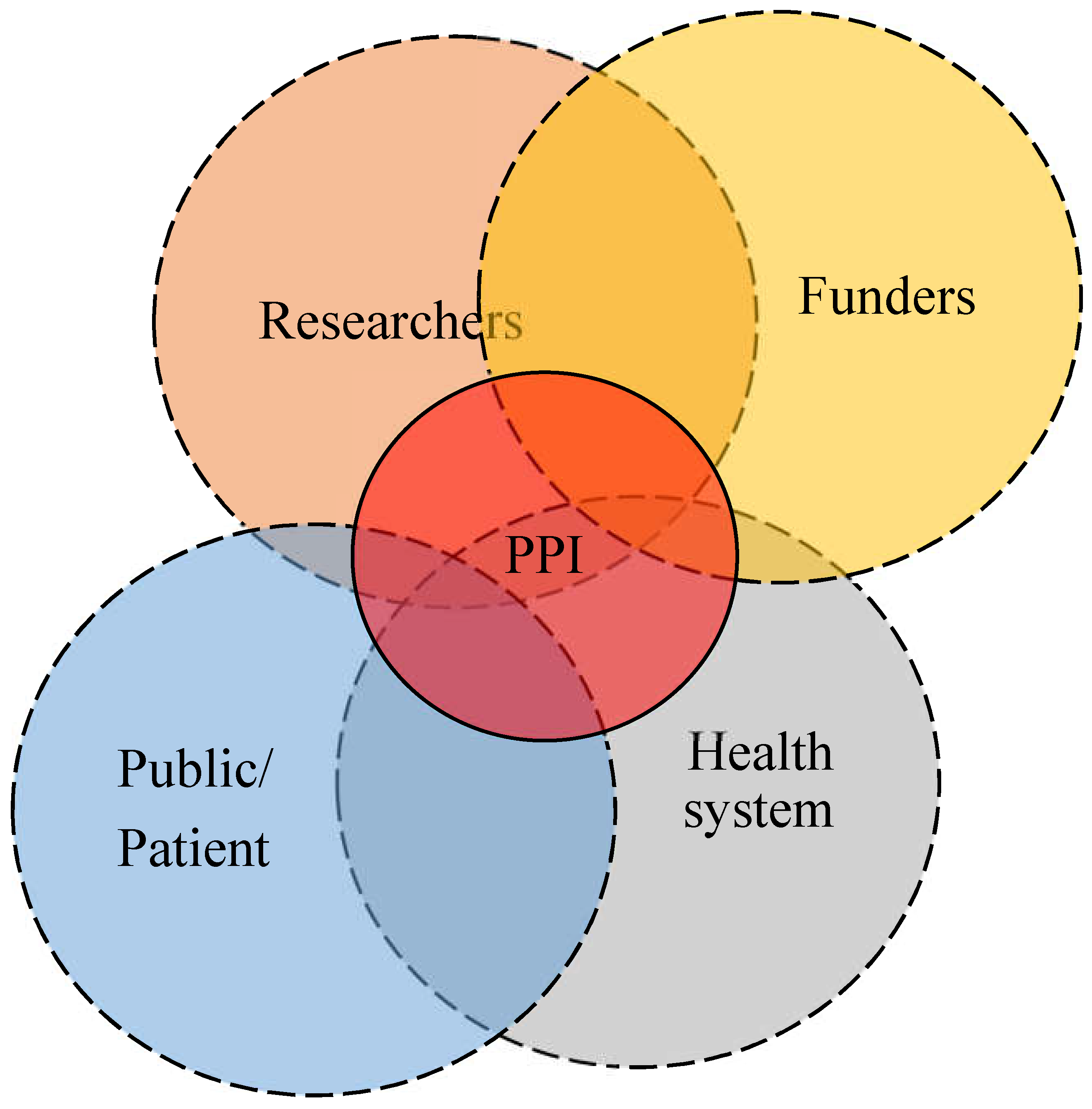
Figure 2.
Diagrammatical presentation of establishment and main phases of a PPI for migration health research.
Figure 2.
Diagrammatical presentation of establishment and main phases of a PPI for migration health research.
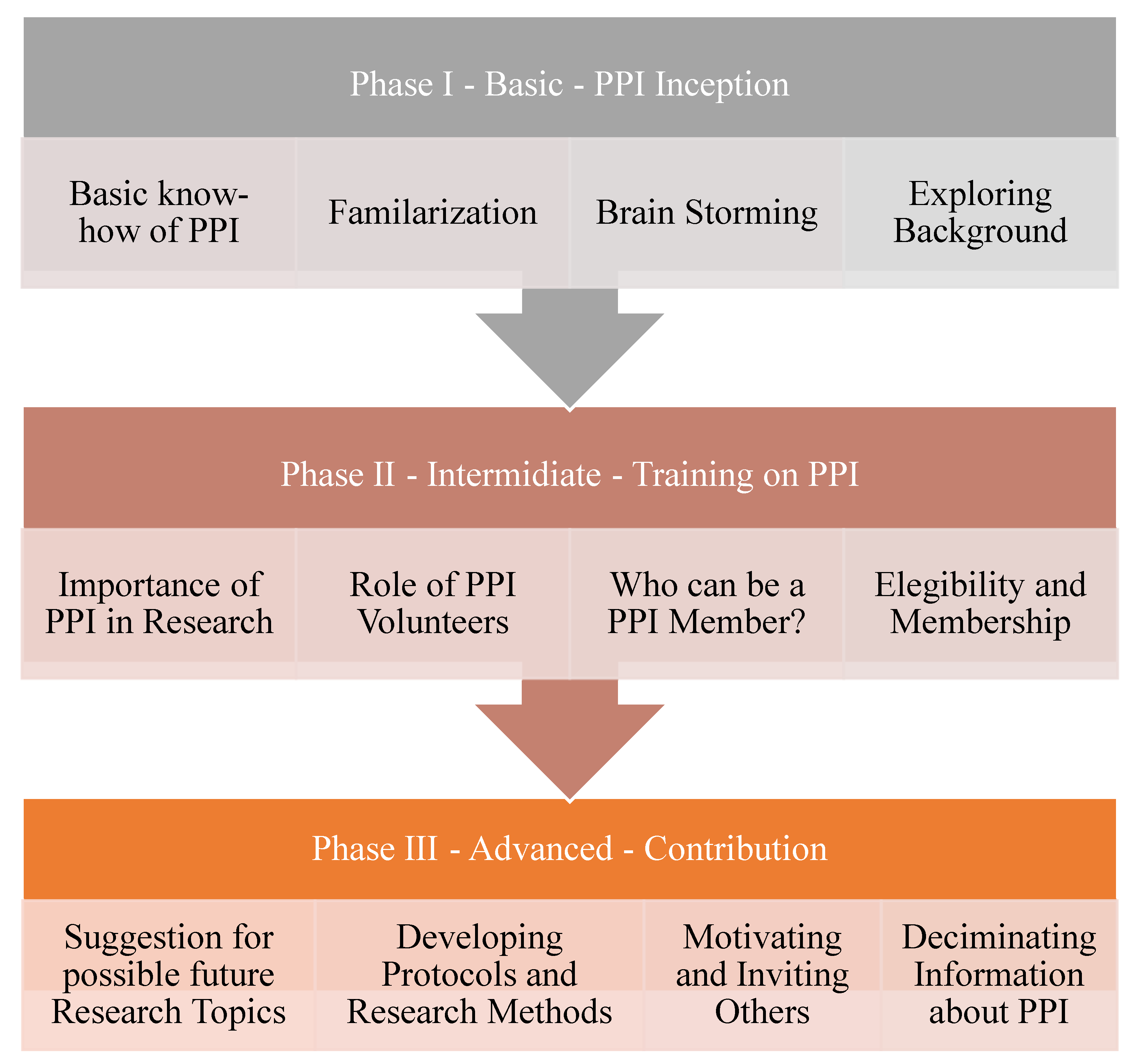

Table 1.
Characteristics of participants of first PPI pertaining to migration health research in Switzerland (N=14).
Table 1.
Characteristics of participants of first PPI pertaining to migration health research in Switzerland (N=14).
| Characteristics | Eritrea (N ) |
Syria (N) |
Total N (%) |
|
|---|---|---|---|---|
| Gender | Male | 5 | 2 | 7 (50.0) |
| Female | 4 | 3 | 7 (50.0) | |
| Median age (years) | 32 | 27 | 30.5 | |
| Educational attainment | Postgraduate | 2 | 0 | 2 (14.3) |
| College/graduate | 3 | 4 | 7 (50.0) | |
| High school | 4 | 1 | 5 (35.7) | |
| Marital status | Married | 9 | 1 | 10 (71.4) |
| Single | 0 | 2 | 2 (14.3) | |
| Divorced | 0 | 2 | 2 (14.3) | |
| Employment status | Employed | 4 | 2 | 6 (42.9) |
| Unemployed | 5 | 3 | 8 (57.1) | |
| Average duration in Switzerland (years) | 7 | 5 | 6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



