
Submitted:
27 June 2024
Posted:
29 June 2024
You are already at the latest version
Abstract
Dermatological consultations are a significant aspect of daily operations at small animal clinics, with atopic dermatitis (CAD) affecting almost 15% of the canine population. The ECS role in the skin reveals its direct action on homeostasis and deregulation, contributing to dermatopathies. It also details its presence in specialized skin cells, revealing a delicate and complex therapeutic potential. Due to the difficulties and the growing scientific evidence of the therapeutic benefits of cannabis, this work aimed to evaluate the anti-inflammatory effect of cannabis oil in treating CAD. Thus, canines diagnosed with CAD were divided into two groups: the group treated using full spectrum high cannabidiol (CBD) [cannabis oil orally] and the control group (olive oil). The evaluation methods for the effectiveness of the therapy were based on the measurement RNAm of interleukins 6, 10, and 31 and oxidative stress in the blood. Despite the theoretical basis, no significant results were obtained between the groups in this work. Thus, it is concluded that oral administration of full spectrum high CBD cannabis oil 2,5 mg/kg twice a day is not efficient in reducing IL and oxidative stress compared to placebo; nevertheless, it still presents a promising approach in the multi-target treatment of CAD.
Keywords:
CAD
; CBD
; interleukin
; oxidative stress
; veterinary dermatology
1. Introduction
Canine atopic dermatitis (CAD) is a genetically determined syndrome characterized by chronic itching and inflammation [20,22]. Its pathogenesis is multifactorial, and although not fully understood, it is known to involve genetic predisposition, immune system alterations with skin inflammation, and defects in the skin barrier. It begins with sensitivity to environmental allergens, mainly house dust mites, which penetrate the skin and stimulate the recruitment of inflammatory cells and mast cell degranulation mediated by IgE antibodies [19,55]. Therefore, multimodal therapy is necessary to manage this disease, aiming to improve the skin barrier, modulate the immune system, and prevent allergy [52].
The endocannabinoid system (ECS) has immunomodulatory actions, and its dysregulation is associated with various chronic inflammations [2]. CB2 receptors are highly expressed in immune cells and play a key role in inflammation regulation [59]. The cannabinoid system is heavily involved in skin homeostasis, barrier formation, and regeneration, while its dysregulation favors the occurrence of diseases and disorders, including atopic dermatitis (AD) [64]. Current literature provides evidence that cannabinoids and cannabinoid-related receptors in specialized skin cells manipulate inflammation and suggest a new approach for treatment by regulating different mechanisms of atopic dermatitis [11].
Activation of Th2 cells leads to the production of interleukin (IL-31), which modulates keratinocyte differentiation, suppresses filaggrin expression, and enhances the expression of pro-inflammatory cytokines. This results in pruritus, mediated by receptors on sensory nerve fibers and diverse immune cells, including macrophages [13,45,48,61]. Inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α) and IL-6, further stimulate macrophages [3,48,53]. In canine atopic dermatitis lesions, IL-31 mRNA levels are elevated [40].
The persistence of inflammation via Th2 and the dysfunction of the skin barrier contribute to chronic inflammation and the overproduction of reactive oxygen species (ROS). Oxidative stress will amplify the inflammatory response by regulating genes, encoding more pro-inflammatory cytokines [5]. Advanced glycation end products (AGEs) also contribute to increased endothelial permeability and activation of mast cells and endothelial cells, further perpetuating and accelerating inflammation and oxidative stress [65]. In atopic dermatitis (AD), oxidative stress predominantly occurs in plasma lipids with HDL peroxidation and the production of lipid hydroperoxides [6]. In contrast, proteolytic enzymes are activated in order to neutralize reactive species (RS). To maintain the levels of RS under control, the enzyme superoxide dismutase (SOD) converts O2• into H2O2, which is then converted into water, a reaction catalyzed by catalase (CAT) and/or glutathione (GSH) [5]. Lipid oxidation and thiols groups can also be altered during CAD activating intracellular mechanisms. Some evidences suggest cannabidiol can act in oxidative signaling due to free radical scavenging capacity [56].
CB2 receptors are predominantly expressed in the immune system. The immune response, including the inflammatory cascade, is tightly controlled by a complex interaction of various cell types and their metabolites [35]. In this context, the endocannabinoid system (ECS) is involved in regulating several transcription factors within these cells, influencing the expression of various immune-related proteins, including surface receptors, and acting as a general modulator of the immune response [43,62]. The endocannabinoid anandamide (AEA) increases IL-10 production via CB2 receptors through different pathways, such as MAPK, and also inhibits the ability of NF-κB to reach transcription sites in the DNA [14]. While the phytocannabinoid CBD reduces oxidative conditions, preventing the formation of superoxide radicals [57] and also has been shown to increase mRNA levels antioxidant enzymes [56], mainly through interactions with receptors.
A nutraceutical blend containing polyphenols and cannabinoids has demonstrated the ability to reverse the overexpression of key inflammatory genes in atopic dermatitis via an epigenetic mechanism, paving the way for its application in sustained drug therapy and relapse prevention strategies [44].
Given the strong relationship between the endocannabinoid system and skin homeostasis, this study aimed to evaluate the efficacy of high-CBD full-spectrum cannabis oil in dogs with atopic dermatitis by measuring concentrations of pro- and anti-inflammatory cytokines and oxidative stress markers.
2. Material and Methods
2.1. Ethics Committee
This Research was approved by the Ethics Committee for Animal Experimentation of the Universidade Federal de Santa Maria (CEUA/UFSM) (no 8656301121 - ID 003662). It was conducted following the ethical principles of the National Council for Animal Experimentation Control (CONCEA).
2.2. Animal Selection
We selected dogs diagnosed with atopic dermatitis who had flea control, had previously undergone at least four to six weeks of hypoallergenic diet without the disappearance of clinical signs, according to Favrot’s criteria and conventional treatment for at least 30 days. All dogs were ectoparasites free and on preventive medications.
Canine subjects with a diagnosis of AD, with prior exclusion of food allergy and flea bite dermatitis, were selected according to the criteria of Favrot [22].
The inclusion criteria were: AD diagnosis; absence of concurrent diseases; no systemic treatment within the past 30 days. The exclusion criteria were: lack of regular flea control; presence of dental calculus; moderate-to-severe gingivitis; any other concurrent disease. No maximum or minimum CADESI values were stipulated for selection or exclusion. Additionally, there was no standardization in the use of shampoo for topical treatment or type of diet used, in order to mimic clinical routine.
The fourteen animals (Table 1) were randomly assigned to Group 1 (G1), the treatment group with cannabis oil, or Group 2 (G2), the control group treated with the exact same olive oil used to dilute the cannabis product, both orally. The treatment oil used was a high cannabidiol (CBD) full-spectrum cannabis oil (50 mg/mL) in a ratio of 21:1 (CBD:THC) from Association of Medicinal Cannabis Patients (AMA+ME) association. The treatment consisted of administering 2.5 mg/kg twice daily for 60 days. Evaluations were conducted before (T0) and after (T60) treatment. The frequency of baths, shampoos, and diets already used, whether therapeutic or not, were kept unchanged.
To check the dermatological condition of each patient, refer to Mariga [39] presents CADESI-04 and itching degree (PVAS) before and after treatment.
2.3. Oxidative Stress
The oxidative stress consists in imbalance between oxidant and antioxidant species. Here some markers of oxidative stress such as GST, CAT, SOD, TBARS and TSH were analyzed in whole blood or serum (Figure 1) in order to evaluated whether cannabidiol modulate oxidative stress in atopic dermatitis.
Glutathione S-transferase (GST) constitutes a superfamily of enzymes that plays a role in the detoxification of endogenous and exogenous compounds that use GSH as a co-substrate [26]. For the glutathione S-transferase (GST), in a 96-well plate, 20 uL of serum sample are added in sextuplicate, followed by 20uL of Milli-Q water, 10uL of GST (100mM) and finally the system - formed by the exact mixture of 20 mL of 0.1 M TFK (100 mM) pH 7.5, 0.0226 g EDTA (2.5 mM) 10.5 mL of Milli-Q H2O. After leaving the plate for 5 minutes at 37 degrees Celsius, 10uL of CDNB (20mM) is pipetted onto all test samples and read in kinetic mode, λ = 340 nm, 30 minutes, 30 second intervals between readings [21].
The thiobarbituric acid reactive substances (TBARS) assay is widely used to measure lipid oxidation. The most common method is through reaction of MDA with thiobarbituric acid (TBA) to produce a pink-coloured dimeric compound. In this method, MDA, an end product of fatty acid peroxidation, reacts with TBA to form a colored complex. The TBARS was analyzed in serum according Jentzsch [27]. The serum (200μl) was incubated at 95ºC for 60 min in acid medium containing 8.1% sodium dodecyl sulfate, 0.5 ml of acetic acid buffer (500 mM, pH 3.4) and 0.6% TBA (Table 2). TBARS levels were measured at 532 nm, and the absorbance was compared with the standard curve using malondialdehyde [27]. The results were expressed in nanomoles of μmol malondialdehyde/mg of protein.
The thiols groups (TSH) were measured spectrophotometrically with ELLMAN’s reagent [17]. An aliquot of 40 μL of serum were added in 60uL of distilled water, 100uL of TFK (1M - pH 7.4). Afterwards, 10uL of 10mM 5-5-dithio-bis (2-nitrobenzoic acid) (DTNB) was added. The reaction product was measured at 412 nm (17). A standard curve using cysteine was added to calculate the content of thiol groups in samples, and was expressed as μmol TSH/mL.
The superoxide (SOD) enzyme convert superoxide radical into hydrogen peroxide and molecular oxygen (O2), while the catalase (CAT) and peroxidases convert hydrogen peroxide into water and in the case of catalase to oxygen and water [67]. For superoxide dismutase (SOD), the samples with blood are diluted in a 1:20 ratio and the protein is read using the Comassie reagent. In a 96-well plate, pipette 4 different volumes of the sample (5uL, 10uL, 15uL and 20uL) in quadruplicate, adding glycine buffer (50 mM - pH 10.5) to close 200uL of volume in the well. The reading is carried out, first in end point mode at λ = 480 nm. After incubating the plate at 37 degrees Celsius for 5 minutes and in a dark environment, 10 µL of 60 mM adrenaline is added as quickly as possible to all test wells. The reading is carried out immediately in kinetic mode at λ = 480 nm for 5 minutes, with intervals of 10 seconds between each reading [46].
To catalase (CAT) analysis, the sample must be diluted 1:10 in saline, we measure the protein concentration to be used in the calculation. Nn the quartz cuvette we pipetted 668 µL of TFK buffer (50 mM - pH 7.0) at room temperature; 7 µL of sample, the device is reset and after zeroing, we add 25uL of hydrogen peroxide diluted in the proportion 5mL of distilled water to 180uL of hydrogen peroxide P.A. Read immediately in kinetic mode at λ = 240 nm, with cycles: 10 and number of readings 11 [50].
2.4. Analysis of Interleukins
2.4.1. Isolation of Peripheral Blood Mononuclear Cells (PBMCs)
Isolation of PBMCs was performed as follows. Briefly, after blood collection, 2 mL of whole blood was diluted in equal volume of 0.9% NaCl, followed by addition of 3mL of Ficoll-Paque PREMIUM1. Centrifugation was performed at 400xg for 15 minutes at room temperature. After centrifugation, the following layers were obtained: PBMC, Ficoll-Paque, PMN, and erythrocytes. The PBMCs were collected, and the samples were stored in a cryotube at -80˚C for subsequent total RNA extraction.
2.4.2. RNA Extraction, Reverse Transcription, and Real-Time PCR
Total RNA was extracted from the PMN cells using Tri Reagent (BD), according to the manufacturer’s recommendations. After the RNA extraction, the quantification and estimation of RNA purity was performed using Nanodrop spectrophotometer (Thermo Scientific, Waltham, MA, USA). The average RNA concentration of the samples was 157,36 ng/μl, minimum 22.9 ng/μl and maximum 386.5 ng/μl; Absorbance 260/280 nm ratio mean 1.91, minimum 1.8 and maximum 2.01).
After quantification, the RNA was treated with DNAse Amplification Grade (Thermo Fisher, Waltham, MA, USA) for 15 minutes at 27˚C to degrade any DNA molecules. DNAse was inactivated with 1 μl EDTA for 10 minutes at 65˚C. Reverse transcription was performed using iScript cDNA synthesis Kit (BioRad, Hercules, CA, USA) for 5 minutes at 25˚C followed by 30 minutes at 42˚C and 5 minutes at 85˚C. The cDNA synthesis was performed using 200ng of RNA each sample.
Quantitative polymerase chain reaction (qPCR) was conducted in a thermocycler (BioRad, Hercules, CA, USA) using cDNA, forward and reverse canine specific primers and SYBR fluorophore GoTaq1 Green Master Mix (Promega Corporation, Madison, USA). Samples were run in duplicate and the results of expression of all analyzed genes were expressed by ΔΔCq method, having internal control gene (ACTB) as reference gene. The genes assessed in this study were: IL-6 (F: CTGGCAGGAGATTCCAAGGAT, R: TCTGCCAGTGCCTCTTTGC; GenBank sequence NM_001003301), IL-10 (F: ACATCAAGAACCACGTGAACTCC, R: ACTCACTCATGGCTTTGTAGACACC; GenBank sequence NM_001003077), IL-31 (F: ATGGATGCTCCTTCTACTCTGTAAACT, R: CAGGAAATGTTCTCAGGCTTAGC; Genbank sequence NM_001165914.1), VEGF F: TGCGCCTATGGCAGGAGGAGAG, R: CGATCTCGTCAGGGTACTCCTGGAAG; GenBank sequence NM_001003175.2), ACTB (F: TGCGTGACATCAAGGAGAAG, R: GGAATTCACTCATGCAGCAA; GenBank sequence NM_001195845.3).
2.5. Statistical Analysis
Descriptive statistics were performed for qualitative variables, including the calculation of frequencies (simple and relative), while measures of central tendency and variability were calculated for quantitative variables. The Shapiro-Wilk test was used to assess the normality of the data. When comparing two groups, the independent samples t-test or paired t-test was used for normally distributed data, and the Mann-Whitney U test or Wilcoxon signed-rank test was used for non-normally distributed data.
For the variables TBARS, GST, IL-6, IL-10, and IL-31, the Shapiro-Wilk test was rejected (p<0.05) and the Wilcoxon signed-rank test was used for Group 1 (control), while for the remaining variables TSH, SOD, and CAT, the paired t-test was used as normality was detected (p>0.05). For Group 2 (Cannabis), the Wilcoxon signed-rank test was used for the variables TBARS, TSH, CAT, IL-6, IL-10, and IL-31, and the paired t-test was used for the other variables (GST, SOD).
Regarding pre- and -post treatment tests, the independent samples t-test was performed for the variables TBARS, TSH, GST, SOD, and CAT, as normality was found in the data, and the Mann-Whitney U test was used for the variables IL-6, IL-10, and IL-31, as normality was not achieved.
For the analyses, the Statistical Package for the Social Sciences (SPSS) version 17.0 was used, with a significance level of 5% (p<0.05). All tests were conducted as two-tailed tests.
3. Results
3.1. Oxidative Stress
There was no statistical difference among the control and pre and post treatments to GST (p=0.2246), TBARS (p=0.7212), TSH (p=0.7627), SOD (p=0.7882) and CAT (0.9271) levels (Figure 1 and Table 3). Insufficient serum volume in one sample limited the analysis of CAT post-treatment concentrations in the treatment group.
3.2. Interleukins
In the present study, no significant changes were observed in the levels of inflammatory (IL-6; p=0.5852), pruritic (IL-31; p=0.3603), and anti-inflammatory (IL-10; p=0.4695) interleukins (Figure 2).
The pre- and post-treatment of each dog can be seen in the Table 4.
4. Discussion
4.1. Oxidative Stress
A body of research evidence indicates that CBD modifies redox balance by altering the level and activity of antioxidant molecules [56]. Martinelli [41] showed that higher concentrations of CBD have been shown to reduce lipid peroxidation markers and preserve antioxidant proteins. Rajesh [58] also revels CBD reduces oxidative conditions, preventing the formation of superoxide radicals. It has also been shown to increase mRNA levels for SOD (superoxide dismutase) and certain variables responsible for the metabolism of superoxide radicals [57]. The antioxidant and scavenger properties occur indirectly through several receptors [4].
However, in the present study the topic use of cannabidiol did not altered the oxidative parameters evaluated (Figure 1). The authors believed that the absence of results can be associated to to the dosage used, and it should be noted that evaluating this directly on the skin would provide more reliable results. Additionally, the potential antioxidant action of olive oil, mainly through hydroxytyrosol, may have reduced the differences between the compared groups [68].
While there is no consensus in the literature regarding oxidative stress and canine atopic dermatitis (CAD), Kapun [29] demonstrated not only levels of malondialdehyde (MDA) and superoxide dismutase (SOD) in dogs affected by this syndrome but also values in healthy dogs. The MDA levels (µmol/L) found were 0.572±2.585 in atopic dogs compared to 0.477±1.298 in healthy dogs. In the present study, there was a variation in MDA levels (nmol/L) from 0.668±1.079 pre-treatment to 0.392±0.967 post-treatment with cannabis oil. Although our results did not show significance in terms of TBARS (nmol MDA/mL) levels, Kapun [29] revealed that dogs with severe atopic dermatitis [Canine Atopic Dermatitis Extent and Severity Index (CADESI) score] exhibited increased levels of MDA in plasma, which may be correlated with elevated lipid peroxidation in CAD pathogenesis.
This study presents laboratory results as a complement to the work of Mariga [39], which focuses on the dermatological and histopathological evaluation of the skin of atopic dogs. It is known that CBD can reduce the accumulation of reactive oxygen species (ROS) and damage to lipid membranes, preventing harm to cellular structure and DNA [10]. In another study, Kapun [28] compared the effect of vitamin E in animals with atopic dermatitis but did not find significance between the treated group and the placebo group in MDA values. Similar to the current study, it is believed that the lack of significance was due to the control group also including atopic and unhealthy animals [29].
Kapun [29] also reported erythrocyte superoxide dismutase (SOD) values (U/gHGB) of 1341.1±2002.5 in atopic dogs, compared to 1349.0±2209.3 in healthy dogs. In the present study, there was a variation in SOD levels (U/mg protein) from 294.8±335.6 pre-treatment to 263.8±343.283 post-treatment with cannabis oil. Even in different samples, similar to our study, Kapun [28,29], did not find significant values between SOD and canine atopic dermatitis (CAD). Given that SOD is an erythrocytic enzyme, we can infer that its elevation in our control group is due to the absence of healthy dogs, as in the case of the first referenced literature.
In rat studies, 10mg/kg of CBD intraperitoneal injection demonstrated antioxidant properties in cerebral ischemia by dose-dependently increasing levels of superoxide dismutase (SOD) and catalase (CAT) through endogenous antioxidant enzymes and lipid peroxidation [30]. Phyto-cannabinoids and polyphenols present in Cannabis sativa L. have been shown to impact redox balance by altering levels of oxidants and antioxidants [54]. Specific phytocannabinoids such as cannabigerol (CBG) can also mitigate oxidative stress, while terpenes like β-caryophyllene reduce reactive oxygen species (ROS) production through the NF-κB pathway, enhancing the synergistic effects of all substances in the plant [20]. Although the specific phytocannabinoid profile of this oil is unknown, full-spectrum oils generally exhibit synergistic interactions among their constituents [32]. The route of administration is important because oral administration undergoes first-pass metabolism, which can decrease bioavailability [42]. More studies are necessary, mainly focusing in analysis of oxidative stress in skin to verify whether the cannabidiol can modulate oxidative stress and inflammatory condition in canine atopic dermatitis.
4.2. Interleukins
In atopic dermatitis, allergens, microorganisms, and secondary self-trauma due to itching, stimulate the release of cytokines important for inflammation from keratinocytes, which leads to alterations in corneodesmosomal function and protein junctions, further intensifying penetration and local inflammation [18,31]. Loewinger [34] also found no difference in serum levels of IL-6 and IL-31 during four weeks of 2mg/kg CBD treatment in atopic dogs, but they found relief of pruritis. Consult the dermatological assessment work to check our results regarding itching [39]. However, a group of researchers who synthesized molecules from CBD observed a significant inhibition of IL-6 levels compared to the control group [36]. A review article [23] revealed that CBD, CBG, or CBD:THC consistently reduced levels of the pro-inflammatory cytokine IL-6, particularly in a dose-dependent manner. The expression of CB2, GPR55, and TRPA1 in T cells indicates a therapeutic target for cannabis, particularly in the involvement of these cells in the immune response of CAD, which results in a reduction in filaggrin production by keratinocytes, altering the function of the skin barrier [12]. In a study similar to ours [47], eight dogs treated with THC-free CBD oil at a dosage of 0.07-0.25mg/kg twice daily for eight weeks showed discrepancies between plasma C-reactive protein concentration and clinical evaluation; however, this study did not have a control group to compare the obtained data. The antagonistic action of CBD on GRP55 appears to prevent inflammation and neuropathic pain through the overexpression of endocannabinoids and IL-10 [60].
Herrmann [24] found no significance in the serum levels of IL-10 in untreated atopic dogs or healthy animals. Expanding on the findings of these authors, even when compared to healthy and conventionally medicated groups with oclacitinib, cyclosporine, and antigen immunotherapy, no significance was observed in IL-10 levels. A study involving 20 atopic dogs showed lower IL-10 levels compared to healthy dogs [37], while other studies [25,51] revealed an upregulation of IL-10 mRNA in peripheral blood mononuclear cells (PBMCs) or skin samples. Phytocannabinoids such as CBD [1], CBG [7], and CBD+THC [66] have an upregulating effect on the anti-inflammatory cytokine IL-10, although one CBD study reported no change in this cytokine [9].
IL-31 has been associated with diseases characterized by severe pruritus, including canine atopic dermatitis (CAD), and is also implicated in suppressing filaggrin differentiation [38,61]. Phytocannabinoids demonstrate a significant anti-inflammatory effect by reducing the release of pro-inflammatory interleukins, such as IL-31. However, the decrease in its expression by the anti-inflammatory action of THCV and CBGA was reversed by the blockade of the TRPV1 receptor by the binding of these phytocannabinoids and also by the inhibition of the cannabinoid degradation enzyme, MAGL [63].
There is a report [8] of a significant increase in IL-31 gene expression in PBMCs in atopic dogs compared to healthy ones. In this study, no significance was found between the treated group and the control group. Tamamoto-Mochizuki e Olivry [61] state in their work the difficulty and complexity of cytokines involved in CAD given the inconsistent results obtained involving IL-10 and IL-31. The values obtained in this study align with inconsistent outcomes in the complex assessment of CAD through interleukins.
In a brief individual analysis, we found that two patients from the cannabis group (patients’ number 4 and 7) showed six positive responses out of the eight analyses performed, and other patients (number 2) met 5 of the 8 criteria. In contrast, in the control group, only one patient (number 3) showed improvement in 5 of the 8 criteria. Thus, we found that the patients in the cannabis group (3 out of 7) exhibited positive responses, meaning there was a decrease in pro-inflammatory interleukins and oxidative molecules or an increase in anti-inflammatory interleukins and antioxidant molecules. We recall that there was no significant difference between the groups and within the group itself, but the patients in the cannabis group showed more positive responses compared to the control group. The referenced data is identified (*) in Table 3 and Table 4.
Although Cannabis can cause suppression in inflammation in healthy individuals, this effect may not be strong enough to alter the levels of inflammatory mediators in situations of highly dysfunctional inflammatory activation [33]. It is essential to note the difficulty in managing atopic dermatitis due to its multifactorial nature, requiring multimodal treatment for control. Therefore, even with the negative results obtained in the single therapy based on cannabis, there is a suspicion of its possible positive effects when used in conjunction with conventional and integrative therapy.
The absence of findings in the different assessments conducted in this study can be mainly justified by the fact that the animals had a dermatopathy, and these changes are primarily related to the dosage used. The small number of animals used it´s also important. Each animal’s body condition was not considered in the present study. According to the literature, phytocannabinoids are deposited in adipose tissue due to their lipophilic nature, and studies that considered this factor revealed a 20% increase in dosage for obese animals to overcome this characteristic [15]. Oral administration may reduce the bioavailability of phytocannabinoids, and the 2.5 mg/kg dosage might not have been sufficient for an anti-inflammatory effect [42], this is because the analyses were conducted only at the mRNA level, rather than measuring the actual amount of interleukins present in the blood. We remind you that regarding interleukins, only mRNA measurement was performed, which may result in variations in the actual amount of interleukins present in the blood, even though Loewinger [34] also did not observe changes in the actual cytokines. Dixon and colleagues [16] show in vitro that cannabinoids have an immunosuppressive effect through surpression of IFN-γ in canine PBMCs. However, there is no suppression of IFN-γ at the mRNA level, nor for TNF-α.
Limitations of this study include the small number of animals and the short-term nature of the therapy. However, despite the absence of significant findings in this study, cannabis oil can still be a promising option due to its various forms of intervening in the pathophysiology of this disease.
5. Conclusions
Despite the lack of significance in evaluating atopic dermatitis by measuring interleukins and oxidative stress, it is worth highlighting the individuality of each animal in response to the dosage used since a highly positive result was obtained in the cannabis group. It is also believed that the difference observed in the current standardized dosage of cannabis oil used in this study diminishes when compared to the effects of olive oil due to its antioxidant properties. This study reveals that cannabis oil with a higher prevalence of CBD at a dosage of 2.5mg/kg does not demonstrate a therapeutic advantage compared to olive oil concerning the analyzed parameters.
Therefore, we recommend conducting further clinical research to confirm or rule out potential therapeutic approaches to assess the control of dermatopathy in terms of interleukins and oxidative stress.
Author Contributions
CM conducted the experiment and wrote this manuscript; MWM and AQA performed the interleukin tests; JNN and NBB performed the oxidative stress tests; AISD carried out the statistical analysis; EA assisted in conducting this experiment; STLPF supervised the experiment
Acknowledgments
We express our gratitude for the partnership with the Brazilian Association of Medicinal Cannabis Patients (AMA+ME) for the realization of this work and the support from the Brazilian Association for Therapeutic Cannabis Access (ABRAFLOR). We also thank the Coordination for the Improvement of Higher Education Personnel (CAPES) and the National Council for Scientific and Technological Development (CNPq) for funding this research.
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Al-Ghezi, Z.Z.; Busbee, P.B.; Alghetaa, H.; Nagarkatti, P.S.; Nagarkatti, M. 2019. Combination of cannabinoids, delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD), mitigates experimental autoimmune encephalomyelitis (EAE) by altering the gut microbiome. Brain, Behaviour, and Immunity. 2019. 82:25–35. [CrossRef]
- Anil, S.M.; Peeri, H.; Koltai, H. Medical cannabis activity against 423 inflammation: active compounds and modes of action. Frontiers in Pharmacology, 2022. v. 13. [CrossRef]
- Asahina, R.; Maeda, S.A. Review of the roles of keratinocyte-derived cytokines and chemokines in the pathogenesis of atopic dermatitis in humans and dogs. Veterinary Dermatology. 2017. 28:16–e5. [CrossRef]
- Atalay, S.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Antioxidative and Antiinflammatory properties of cannabidiol. Antioxidants. 2020, 9, 21. [Google Scholar] [CrossRef]
- Bertino, L.; Guarneri, F.; Cannavò, S.P.; Casciaro, M.; Pioggia, G.; Gangemi, S. Oxidative Stress and Atopic Dermatitis. Antioxidants. 2020, 9, 196. [Google Scholar] [CrossRef] [PubMed]
- Borgia, F.; Pomi, F.L.; Vaccaro, M.; Alessandrello, C.; Papa, V.; Gangemi, S. Oxidative Stress and Phototherapy in Atopic Dermatitis: Mechanisms, Role, and Future Perspectives. 2022. Biomolecules, 12, 1904. [CrossRef]
- Borrelli, F.; Fasolino, I.; Romano, B.; Capasso, R.; Fracesco, M.; Coppola, D.; Orlando, P.; Battista, G.; Pagano, E.; Di Marzo, V.; Izzo, A.A. Beneficial effect of the nonpsychotropic plant cannabinoid cannabigerol on experimental inflammatory bowel disease. Biochemical Pharmacology. 2013. 85:1306–1316. [CrossRef]
- Bowen, S.; Aleo, M.; Corum, S.; Zeng, X.; Rincon, G.; Gonzales, A. Exploring the role of cytokines and chemokines in canine aller-gic skin disease. Veterinary Dermatology 2020, 31, 58. [Google Scholar]
- Britch, S.C.; Goodman, A.G.; Wiley, J.L.; Pondelick, A.M.; Craft, R.M. Antinociceptive and immune effects of delta-9-tetrahydrocannabinol or cannabidiol in male versus female rats with persistent inflammatory pain. Journal of Pharmacology and Experimental Therapeutics. 2020. 373:416–428. [CrossRef]
- Campos, A.C.; Fogaça, M.V.; Sonego, A.B.; Guimarães, F.S. Cannabidiol, neuroprotection and neuropsychiatric disorders. Pharmacology Research. 2016, 112, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Chiocchetti, R.; Salamanca, G.; De Silva, M.; Gobbo, F.; Aspidi, F.; Cunha, R.Z; Galiazzo, G.; Tagliavia, C.; Sarli, G.; Morini, M. Cannabinoid receptors in the inflammatory cells of canine atopic dermatitis. Frontiers in Veterinary Science. 2022. 15; 9:987132. [CrossRef]
- Combarros, D.; Cadiergues, M.; Simon, M. Update on canine filaggrin: a review. Veterinary Quarterly. 2020. 40:162–8. [CrossRef]
- Cornelissen, C.; Marquardt, Y.; Czaja, K.; Wenzel, J.; Frank, J.; LüscherFirzlaff, J.; Lüscher, B.; Baron, J.M. IL-31 regulates differentiation and filaggrin expression in human organotypic skin models. The Journal of Allergy and Clinical Immunology. 2012. 129:426– 33. [CrossRef]
- Correa, F.; Hernangómez, M.; Mestre, L.; LorÚa, F.; Spagnolo, A.; Docagne, F.; Di Marzo, V.; Guaza, C. Anandamide enhances IL-10 production in activated microglia by targeting CB2 receptors: Roles of ERK1/2, JNK, and NF-κB. Glia, 2010. 58, 135–147. [CrossRef]
- Corsetti, S.; Borruso, S.; Malandrucco, L.; Spallucci, V.; Maragliano, L.; Perino, R.; D’Agostino, P.; Natoli, E. Cannabis sativa L. may reduce aggressive behavior towards humans in shelter dogs. Scientific Reports. 2021. 11:2773. [CrossRef]
- Dixon, S.; Deb, A.; Archer, T.; Kaplan, B.L.F. Potential to use cannabinoids as adjunct therapy for dexamethasone: An in vitro study with canine peripheral blood mononuclear cell. Veterinary Immunology and Immunopathology. 2024, 269, 110727. [Google Scholar] [CrossRef] [PubMed]
- Ellman, G.L. Tissue sulfhydryl groups. Archives of Biochemistry and Biophysics, 1959. n. 82, p. 70–77. [CrossRef]
- Gedon, N.K.Y.; Mueller, R.S. Atopic dermatitis in cats and dogs: a difficult disease for animals and owners. Clinical and Translational allergy. 2018. 8:41. [CrossRef]
- Gugliandolo, E.; Palma, E.; Cordaro, M.; D´Amico, R.; Peritore, A.F.; Licata, P.; Crupi, R. Canine atopic dermatitis: Role of luteolin as new natural treatment. Veterinary Medicine and Science, 2020. 6:926-932, 2020. [CrossRef]
- Gugliandolo, A.; Pollastro, F.; Grassi, G.; Bramanti, P.; Mazzon, E. “In Vitro Model of Neuroinflammation: Eficacy of Cannabigerol, a Non-Psychoactive Cannabinoid,” International Journal of Molecular Sciences, 2018, vol. 19, no. 7, article E1992. [CrossRef]
- Hagib, W.H.; Pabst, M.J.; Jakoby, W.B. Glutathione S-transferases. The first enzymatic step in mercapturic acid formation. Journal of Biological Chemistry 1974, 249, 7130–7139. [Google Scholar]
- Hensel, P.; Santoro, D.; Favrot, C.; Hill, P.; Griffin, C. Canine atopic dermatitis: detailed guidelines for diagnosis and allergen identification. BMC Veterinary Research, 2015. 11:196. [CrossRef]
- Henshaw, F.R.; Dewsbury, L.S.; Lim, C.K.; Steiner, G.Z. The Effects of Cannabinoids on Pro- and Anti-Inflammatory Cytokines: A Systematic Review of In Vivo Studies. Cannabis and Cannabinoid Research. 2021. v. 6, n. 3. [CrossRef]
- Herrmann, I.; Mamo, L.B.; Holmes, J.; Mohammed, J.P.; Murphy, K.M.; Bizikova, P. Long-term effects of ciclosporin and oclacitinib on mediators of tolerance, regulatory T-cells, IL-10 and TGF-B, in dogs with atopic dermatitis. Veterinary Dermatology. 2023. 24:107-114. [CrossRef]
- Hoskova, Z.; Svoboda, M.; Satinska, D.; Matiasovic, J.; Leva, L.; Toman, M. Changes in leukocyte counts, lymphocyte subpopulations and the mRNA expression of selected cytokines in the peripheral blood of dogs with atopic dermatitis. Veterinární medicína - Czech, 2015, 518 60:644–53. [CrossRef]
- Huber, P.C.; Almeida, W.P.; Fátima, Â. Glutationa e enzimas relacionadas: papel biológico e importância em processos patológicos. Quím Nova. 2008. 31(5):1170–9. [CrossRef]
- Jentzsch, A.M.; Bachmann, H.; Fürst, P.; Biesalski, H.K. Improved analysis of malondialdehyde in human body fluids. Free Radical Biology and Medicine, 1996. 20:251-. [CrossRef]
- Kapun, A.P.; Salobir, J.; Levart, A.; Karcher, G.T.; Svete, A.N.; Kotnik, T. Vitamin E supplementation in canine atopic dermatitis: improvement of clinical signs and effects on oxidative stress markers. Veterinary Record, 2014, 29. [CrossRef]
- Kapun, A.P.; Salobir, J.; Levart, A.; Kotnik, T.; Svete, A.N. Oxidative stress markers in canine atopic dermatitis. Research in Veterinary Science. 2012. 92:469-470. [CrossRef]
- Khaksar, S.; Bigdeli, M.; Samiee, A.; Shirazi-Zand, Z. Antioxidant and antiapoptotic effects of cannabidiol in model of ischemic stroke in rats. Brain Research Bulletin. 2022, 180, 118–130. [Google Scholar] [CrossRef] [PubMed]
- Klonowska, J.; Glen, J.; Nowicki, R.J.; Trzeciak, M. New Cytokines in the Pathogenesis of Atopic Dermatitis – New Therapeutic Targets. International Journal of Molecular Sciences, 2018, 19, 3086. [CrossRef]
- Koltai, H.; Poulin, P.; Namdar, D. Promoting Cannabis Products to Pharmaceutical Drugs. European Journal of Pharmaceutical Sciences, 2019, 132, 118–120. [CrossRef]
- Lima, M.G.; Tardelli, V.S.; Brietzke, E.; Fidalgo, T.M. Cannabis and inflammatory mediators. European Addiction Research, 2021, 27:26-24. [CrossRef]
- Loewinger, M.; Wakshlag, J.J.; Bowden, D.; Peters-Kennedy, J.; Rosenberg, A. The effect of a mixed cannabidiol and cannabidiolic acidbased oil on client-owned dogs with atopic dermatitis. Veterinary Dermatology, 2022, 33:329-e77. [CrossRef]
- Lorimier, L.P.; Hazzah, T.; Amazonas, E.; Cital, S. Cannabinoids in oncology and immune response. In: Cital, S.; Kramer, K.; Hughston, L.; Gaynor, J.S. Cannabis Therapy in Veterinary Medicine: A complete guide. Springer, 2021, cap. 10, p. 240-249.
- Lubschinski, T.L.; Pollo, L.A.E.; Mohr, E.T.B.; Da Rosa, J.S.; Nardino, L.A.; Sndjo, L.P.; Biavatti, M.W.; Dalmarco, E.M. Effect of Aryl-Cyclohexanones and their derivatives on macrophage polarization in vitro. Inflammation, 2022, vol. 45, n. 4. [CrossRef]
- Majewska, A.; Gajewska, M.; Dembele, K.; Maciejewski, H.; Prostek, A.; Jank, M. Lymphocytic, cytokine and transcriptomic profiles in peripheral blood of dogs with atopic dermatitis. BMC Veterinary Research. 2016. 12:174. [CrossRef]
- Marsella, R. Advances in our understanding of canine atopic dermatitis. Veterinary Dermatology, 2021, 32:547-151. [CrossRef]
- Mariga, C.; Mateus, A.L.S.S.; Dullius, A.I.S.; da Silva, A.P.; Flores, M.M.; Soares, A.V.; Amazonas, E.; Pinto Filho, S.T.L. Dermatological evaluation in dogs with atopic dermatites treated with full-spectrum high cannabidiol oil: a pre study part 1. Frontiers in Veterinary Science, 2023, 10:1285384. [CrossRef]
- Martel, B.C.; Lovato, P.; Bäumer, W.; Olivry, T. Translational animal models of atopic dermatitis for preclinical studies. Yale Journal of Biology and Medicine 2017, 90, 389–402. [Google Scholar] [PubMed]
- Martinelli, G.; Magnavacca, A.; Fumagalli, M.; Dell’Agli, M.; Piazza, S.; Sangiovanni, E. Cannabis sativa and skin health: Dissecting the role of phytocannabinoids. Planta Medicinal. 2022, 88(7):492-506. [CrossRef]
- Martins, A.; Gomes, A.; Boas, I.; Marto, J.; Ribeiro, H. Cannabis-Based Products for the Treatment of Skin Inflammatory Diseases: A Timely Review. Pharmaceuticals. 2022, 15, 210. [Google Scholar] [CrossRef] [PubMed]
- Massi, P.; Vaccani, A.; Paloralo, D. Cannabinoids, immune system and cytokine network. Current Pharmaceutical Design, 2006, 12, 3135–3146. [CrossRef]
- Massimini, M.; Vedove, E.D.; Bachetti, B.; Di Pierro, F.; Ribecco, C.; D’ Addario, C.; Pucci, M. Polyphenols and Cannabidiol Modulate Transcriptional Regulation of Th1/Th2 Inflammatory Genes Related to Canine Atopic Dermatitis. Frontiers in Veterinary Science, 2021, 8:606197. [CrossRef]
- Mccandless, E.E.; Rugg, C.A.; Fici, G.J.; Messamore, J.E.; Aleo, M.M.; Gonzales, A.J. Allergen-induced production of IL-31 by canine Th2 cells and identification of immune, skin, and neuronal target cells. Veterinary Immunology Immunopathology. 2014. 157:42–8. [CrossRef]
- Mccord, J.M.; Fridovich, I. Superoxide dismutase: na enzymatic function for erythrocuprein (hemocuprein). Journal Biological Chemistry. 1969. v. 244, p. 6049-6055. [CrossRef]
- Mogi, C.; Yoshida, M.; Kawano, K.; Fukuyama, T.; Arai, T. Effects of cannabidiol without delta-9-tetragydrocannabinol on atopic dermatitis: a retrospective assessment of 8 cases. The Canadian Veterinary Journal 2022, 63, 423–426. [Google Scholar] [PubMed]
- Mmoore, P.F.A. review of histiocytic diseases of dogs and cats. Veterinary Pathology. 2014. 51:167–84. [CrossRef]
- Nakashima, C.; Otsuka, A.; Kabashima, K. Interleukin-31 and interleukin31 receptor: new therapeutic targets for atopic dermatitis. Experimental Dermatology. 2018. 27:327–31. [CrossRef]
- Nelson, D.P.; Kiesow, L.A. Enthalpy of decomposition of hydrogen peroxide by catalase at 25° C (with molar extinction coefficients of H2O2 solutions in the UV). Analytical Biochemistry, 1972, 49(2), 474–478. [CrossRef]
- Olivry, T.; Mayhew, D.; Paps, J.S.; Linder, K.E.; Peredo, C.; Rajpal, D.; Holfland, H.; Cote-Sierra, J. Early activation of Th2/Th22 inflammatory and pruritogenic pathways in acute canine atopic dermatitis skin lesions. Journal of Investigative Dermatology. 2016. 136:1961–9. [CrossRef]
- Olivry, T.; DeBoer, D.J.; Favrot, C.; Jackson, H.A.; Mueller, R.S.; Prélaud, T.P. Treatment of canine atopic dermatitis: clinical practice guidelines from the international task force on canine atopic dermatitis. Veterinary Dermatology, 2010, 21:233–48. [CrossRef]
- Parameswaran, N.; Patial, S. Tumor necrosis factor-alpha signaling in macrophages. Critical Reviews in Eukaryotic Gene Expression. 2010. 20:87–103. [CrossRef]
- Pellati, F.; Borgonetti, V.; Brighenti, V.; Biagi, M.; Benvenuti, S.; Corsi, L. Cannabis sativa L. And nonpsychoactive cannabinoids: Their chemistry and role against oxidative stress, inflammation, and cancer. BioMed Research International. 2018, 1691428. [CrossRef]
- Pereira, D.T.; Cunha, V.E.S.; Schmidt, C.; Magnus, T.; Krause, A. Sensitization study of dogs with atopic dermatitis in the central region of Rio Grande do Sul. Arquivo Brasileiro de Medicina Veterinária e Zootecnia, 2015, v.67, n., 6, p. 1533-1538, 2015. [CrossRef]
- Pereira, S.R.; Hackett, B.; O’Driscoll, D.N.; Sun, M.C.; Downer, E.J. Cannabidiol modulation of oxidative stress and signalling. Neuronal Signal; 2021, 5 (3). [CrossRef]
- Rajesh, M.; Mukhopadhyay, P.; Bátkai, S.; Patel, V.; Saito, K.; Matsumoto, S. ; Kashiwaya,Y.; Horváth, B.; Mukhopadhyay, B.; Becker, L.; Haskó, G.; Liaudet, L.; Wink, D.A.; Veses, A.; Mechoulam, R.; Pacher, P. Cannabidiol attenuates cardiac dysfunction, oxidative stress, fibrosis, and inflammatory and cell death signaling pathways in diabetic cardiomyopathy. Journal of the American College of Cardiology, 2010, 56, 2115–2125. [CrossRef]
- Rajesh, M.; Mukhopadhyay, P.; Bátkai, S.; Haskó, G.; Liaudet, L.; Drel, V.R.; Obrosova, I.G.; Pacher, P. Cannabidiol attenuates high glucose-induced endothelial cell inflammatory response and barrier disruption. American Journal of Physiology-Heart and Circulatory Physiology, 2007, 293, 610–619. [CrossRef]
- Rayman, N.; Lam, K.H.; Laman, J.D.; Simons, P.J.; Löwenberg, B.; Sonneveld, P.; Delwel, R. Distinct expression profiles of the peripheral cannabinoid receptor in lymphoid tissues depending on receptor activation status. Journal of Immunology, 2004, 172:2111–2117. [CrossRef]
- Sunda, F.; Arowolo, A. A molecular basis for the antiinflammatory and antifibrosis properties of cannabidiol. The FASEB Journal, 2020, 34:14083–92, 2020. [CrossRef]
- Tamamoto-Mochizuki, C.; Olivry, T. IL-31 and IL-31 receptor expression in acute experimental canine atopic dermatitis skin lesions. Veterinary Dermatology. 2021. 32:631–e169. [CrossRef]
- Tanasescu, R.; Constantinescu, C.S. Cannabinoids and the immune system: An overview. Immunobiology, 2010, 215(8), 588–597. [CrossRef]
- Tortolani, D.; Di Meo, C.; Standoli, S.; Ciaramellano, F.; Kadhim, S.; Hsu, E.; Rapino, C.; Maccarrone, M. Rare Phytocannabinoids Exert Anti-Inflammatory Effects on Human Keratinocytes via the Endocannabinoid System and MAPK Signaling Pathway. International Journal of Molecular Science. 2023, 24, 2721. [Google Scholar] [CrossRef] [PubMed]
- Tóth, K.F.; Ádám, D.; Bíró, T.; Oláh, A. Cannabinoid Signaling in the Skin: Therapeutic potential of the “c(ut)annabinoid” system. Molecules, 2019, 24, 918. [CrossRef]
- Tsukahara, H.; Shibata, R.; Ohta, N.; Sato, S.; Hiraoka, M.; Ito, S.; Noiri, E.; Mayumi, M. High levels of urinary pentosidine, an advanced glycation end product, in children with acute exacerbation of atopic dermatitis: Relationship with oxidative stress. Metabolism, 2003, 52, 1601–1605. [CrossRef]
- Verrico, C.D.; Wesson, S.; Konduri, V.; Hofferek, C.J.; Vazquez-Perez, J.; Blair, E.; Dunner Jr, K.; Salimpour, P.; Decker, W.K.; Halpert, M.M. A randomized, doubleblind, placebo-controlled study of daily cannabidiol for the treatment of canine osteoarthritis pain. Pain. 2020. 161:2191–2202. [CrossRef]
- Weydert, C.J.; Cullen, J.J. Measurement of superoxide dismutase, catalase and glutathione peroxidase in cultured cells and tissue. Nat Protoc. 2010. 5(1):51-66. [CrossRef]
- Zoric, N.; Horvat, I.; Kopjar, N.; Vucemilovic, A.; Kremer, D.; Tomic, S.; Kosalec, I. Hydroxytyrosol expresses antifungal activity in vitro. Curr Drug Targets, 2013, 14:992-998. [CrossRef]
Figure 1.
Distribution of oxidative stress markers GST, TBARS, TSH, SOD, and CAT in the control and cannabis groups before and after treatment, with a 60-day interval. The relative expression values are shown (mean ± SEM) in dogs from the cannabis oil group (green bars) and dogs from the control group (white bars). There was no difference in any oxidative stress market between the treatments (P>0.05) performed. (GST = Glutathione S-Transferase; TBARS: thiobarbituric acid-reactive substances; TSH: Protein Thiols, SOD: Superoxide dismutases; CAT: Catalase). GST, TBARS and TSH was used serum, while CAT and SOD was used blood. CDNB: 1-chloro 2, 4 dinitrobenzene, MDA: malondialdehyde, SH: thiol group, SOD: superoxide dismutase, CAT: catalase.
Figure 1.
Distribution of oxidative stress markers GST, TBARS, TSH, SOD, and CAT in the control and cannabis groups before and after treatment, with a 60-day interval. The relative expression values are shown (mean ± SEM) in dogs from the cannabis oil group (green bars) and dogs from the control group (white bars). There was no difference in any oxidative stress market between the treatments (P>0.05) performed. (GST = Glutathione S-Transferase; TBARS: thiobarbituric acid-reactive substances; TSH: Protein Thiols, SOD: Superoxide dismutases; CAT: Catalase). GST, TBARS and TSH was used serum, while CAT and SOD was used blood. CDNB: 1-chloro 2, 4 dinitrobenzene, MDA: malondialdehyde, SH: thiol group, SOD: superoxide dismutase, CAT: catalase.
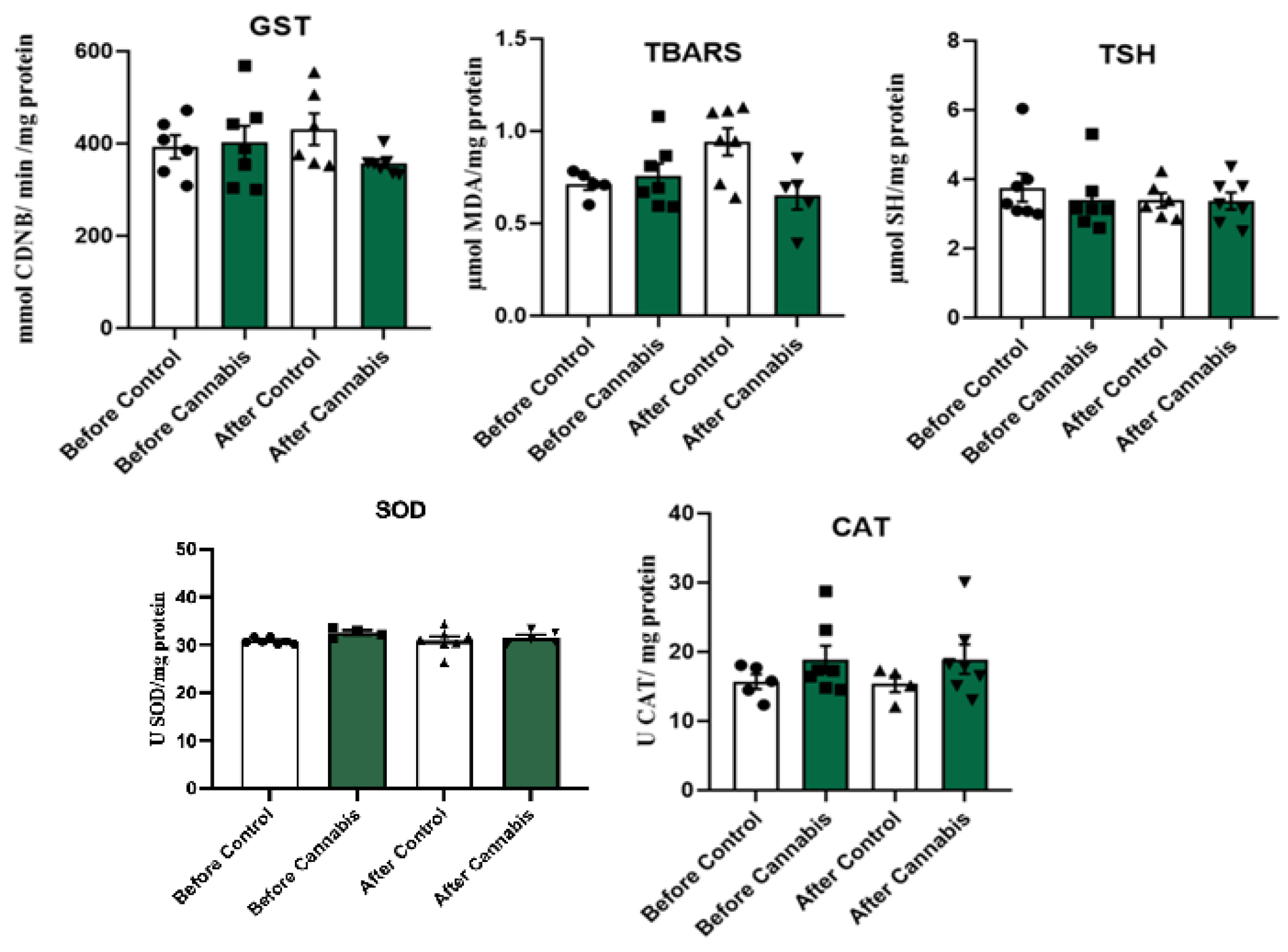
Figure 2.
Distribution of mRNA gene expression of interleukins IL-6, IL-10, and IL-31 in dogs with atopic dermatitis in the control group and treated with cannabis oil. Real-time quantitative PCR of interleukin genes (IL-6, IL-10, and IL-31) in peripheral blood polymorphonuclear cells (PMN) of dogs with atopic dermatitis treated with cannabis oil at a dosage of 2.5mg/kg twice daily and the control group - relative expression. Values are shown (mean ± SEM) in dogs from the cannabis oil group (gray bars) and dogs from the control group (black bars). There was no difference in gene expression between the treatments (P>0.05) performed.
Figure 2.
Distribution of mRNA gene expression of interleukins IL-6, IL-10, and IL-31 in dogs with atopic dermatitis in the control group and treated with cannabis oil. Real-time quantitative PCR of interleukin genes (IL-6, IL-10, and IL-31) in peripheral blood polymorphonuclear cells (PMN) of dogs with atopic dermatitis treated with cannabis oil at a dosage of 2.5mg/kg twice daily and the control group - relative expression. Values are shown (mean ± SEM) in dogs from the cannabis oil group (gray bars) and dogs from the control group (black bars). There was no difference in gene expression between the treatments (P>0.05) performed.
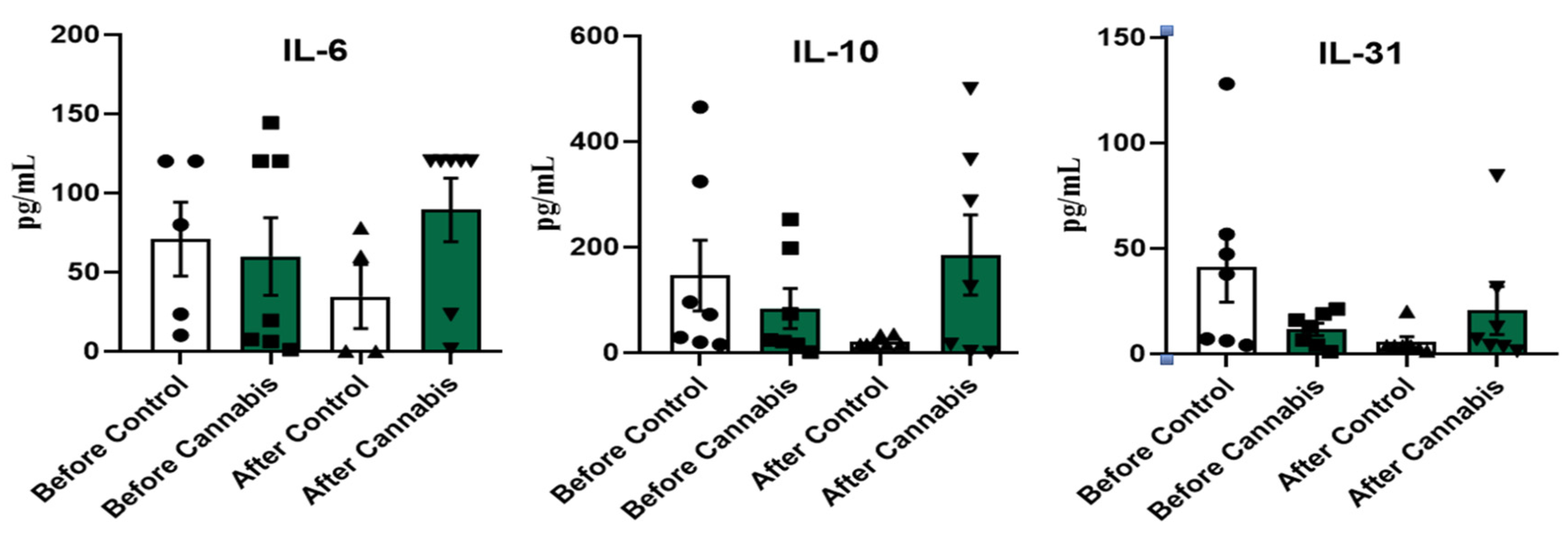

Table 1.
Animal Demographics.
| Group | Sex | Age | Breed | Age of disease |
|---|---|---|---|---|
| Control | ||||
| Animal 1 | Male | 12 years | Shih-tzu | 6 months |
| Animal 2 | Female | 1 year | Lhasa apso | 9 months |
| Animal 3 | Female | 5 years | Shih-tzu | 1 year |
| Animal 4 | Female | 1 year | Dachshund | 10 months |
| Animal 5 | Female | 11 years | Shih-tzu | 1 year |
| Animal 6 | Male | 7 years | Shih-tzu | 3 years |
| Animal 7 | Male | 6 years | Dachshund | 3 years |
| CBD | ||||
| Animal 1 | Female | 8 years | Shih-tzu | 6 months |
| Animal 2 | Female | 10 years | Shih-tzu | 3 years |
| Animal 3 | Male | 6 years | Golden Retriever | 1 year |
| Animal 4 | Female | 7 years | Shih-tzu | 3 years |
| Animal 5 | Female | 8 years | Lhasa apso | 2 years |
| Animal 6 | Male | 9 years | Shih-tzu | 1 year |
| Animal 7 | Male | 11 years | Shih-tzu | 3 years |
Table 2.
Thiobarbituric acid reactive substances (TBARS) with serum, pipette the following quantities into test tubes, in order:.
Table 2.
Thiobarbituric acid reactive substances (TBARS) with serum, pipette the following quantities into test tubes, in order:.
| d. H2O | Orthophosphoric acid (0,2M) | SERUM | TBA | |
| Test(quadruplicate) | 550 µL | 1 mL | 200 µL | 250 µL |
| ORDER | 1º | 2º | 3º | 4º |
Table 3.
Individual oxidative stress markers of pre- and post-Treatment in the control and Cannabis groups (mean), with 60-day interval in the fourteen dogs with atopic dermatitis. There was no difference in any oxidative stress market between the treatments (P>0.05) performed. (GST = Glutathione S-Transferase; TBARS: thiobarbituric acid-reactive substances; TSH: Protein Thiols, SOD: Superoxide dismutases; CAT: Catalase).
Table 3.
Individual oxidative stress markers of pre- and post-Treatment in the control and Cannabis groups (mean), with 60-day interval in the fourteen dogs with atopic dermatitis. There was no difference in any oxidative stress market between the treatments (P>0.05) performed. (GST = Glutathione S-Transferase; TBARS: thiobarbituric acid-reactive substances; TSH: Protein Thiols, SOD: Superoxide dismutases; CAT: Catalase).
| Group | n | TBARS (µmol) | TSH (µmol) | GST (mmol) | SOD (U) | CAT (U) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | ||
| Control | 1 | 0.78421 | 0.9511 | 2.59823 | 2.74486 | 333.401 | 554.747 | 30.056 | 28.2286 | 12.3625 | ** |
| 2 | 1.74781 | 0.71587 | 5.30367 | 2.49516 | 356.421 | 358.009 | 31.644 | 30.4248 | 24.9904 | 27.6665 | |
| 3 | 0.70938 | 1.1289 | 2.77795 | 3.28238* | 404.399 | 506.385* | 30.6962 | 28.0486 | 29.2066 | 17.3095 | |
| 4 | 0.7131 | 0.94617 | 3.64983 | 4.36559 | 360.975 | 376.152 | 30.5356 | 32.5754 | 15.7693 | 16.8921 | |
| 5 | 0.60136 | 0.64099 | 3.15261 | 3.13768 | 357.977 | 755.367 | 30.0909 | 31.1894 | 18.0806 | 12.0895 | |
| 6 | 1.04376 | 1.11017 | 3.13409 | 3.78031 | 346.502 | 352.918 | 30.5945 | 30.1121 | 17.7333 | 15.1305 | |
| 7 | 0.76196 | 1.10178 | 3.13615 | 3.79654 | 335.749 | 438.148 | 31.506 | 33.3308 | 14.4891 | 22.7313 | |
| Mean | 0.757 | 0.942 | 3.393 | 3.371 | 356.489 | 477.389 | 30.7525 | 30.5585 | 18.947 | 18.636 | |
| P value = | 0.2969 | 0.9656 | 0.01563 | 0.788 | 0.6454 | ||||||
| CBD | 1 | 0.66884 | 0.69438 | 3.08442 | 3.72348 | 300.175 | 472.419 | 29.4791 | 30.2396 | 17.2726 | 16.5049 |
| 2 | 0.59395 | 0.61255 | 2.99384 | 2.92304* | 353.695 | 408.548* | 32.1046 | 34.3283* | 28.7575 | 18.2596 | |
| 3 | 0.86726 | 0.9678 | 3.09898 | 4.2361 | 303.553 | 339.894 | 33.0177 | 32.215 | 16.426 | 13.0261 | |
| 4 | 1.0795 | 0.85289* | 6.04083 | 2.85237* | 455.872 | 441.996 | 29.9805 | 31.0952* | 23.159 | 30.0823* | |
| 5 | 0.59001 | 0.70661 | 3.29493 | 3.21848 | 389.773 | 308.881 | 29.7243 | 30.3239 | 14.5043 | 17.8689 | |
| 6 | 0.69374 | 1.86589 | 4.00329 | 2.55150 | 442.471 | 439.683 | 33.5601 | 26.3763 | 17.3806 | 15.0946 | |
| 7 | 0.81189 | 0.39209* | 3.79419 | 3.38714* | 568.803 | 385.939 | 31.3136 | 31.6196* | 14.7987 | 21.6696* | |
| Mean | 0.757 | 0.870 | 3.758 | 3.270 | 402.048 | 399.622 | 31.3114 | 30.8854 | 18.899 | 18.9294 | |
| P value = | 0.6875 | 0.4688 | 0.9558 | 0.7299 | 1.00 | ||||||
*The data referred to as a positive response in the overall analysis framework. **No amount to dilute.
Table 4.
Individual mRNA gene expression of inflammatory (IL-6), anti-inflammatory (IL-10) and pruritic interleukins (IL-31) pre- and post-Treatment in the control and Cannabis groups (mean), with 60-day interval in the fourteen dogs with atopic dermatitis.
Table 4.
Individual mRNA gene expression of inflammatory (IL-6), anti-inflammatory (IL-10) and pruritic interleukins (IL-31) pre- and post-Treatment in the control and Cannabis groups (mean), with 60-day interval in the fourteen dogs with atopic dermatitis.
| Group | n | IL-6 (pg/mL) |
IL-10 (pg/mL) |
IL-31 (pg/mL) |
||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |||
| Control | 1 | 3.56 | 120.26 | 20.37 | 15.67 | 6.32 | 3.94 | |
| 2 | 10.21 | 120.26 | 29.14 | 15.67 | 4.13 | 20.19 | ||
| 3 | 120.26 | 1.22* | 15.67 | 35.25* | 7.21 | 2.75* | ||
| 4 | 80.02 | 120.26 | 465.73 | 15.67 | 47.46 | 3.94 | ||
| 5 | 5.55 | 120.26 | 72.89 | 15.67 | 37.92 | 3.94 | ||
| 6 | 23.5 | 23.19 | 96.34 | 33.53 | 56.76 | 1.39 | ||
| 7 | 120.26 | 120.26 | 324.6 | 15.67 | 128.19 | 3.94 | ||
| Mean | 51.91 | 89.39 | 146.39 | 21.02 | 41.14 | 5.72 | ||
| P value = | 0.5294 | 0.07813 | 0.07813 | |||||
| CBD | 1 | 1 | 0,15 | 1 | 0,8 | 1 | 1,27 | |
| 2 | 144.47 | 78.05* | 24.06 | 287.38* | 16.02 | 31.41 | ||
| 3 | 120.26 | 60.15 | 252.76 | 500.13 | 4.24 | 84.38 | ||
| 4 | 120.26 | 0.2* | 15.67 | 2.33 | 21.32 | 3.41* | ||
| 5 | 19.59 | 120.26 | 73.54 | 125.21 | 12.96 | 6.88 | ||
| 6 | 6.33 | 120.26 | 21.36 | 15.67 | 6.72 | 3.94 | ||
| 7 | 7.55 | 485.63 | 198.23 | 366.01* | 18.95 | 12.7* | ||
| Mean | 59.92 | 123.53 | 83.80 | 185,36 | 11,60 | 20.57 | ||
| P value = | 0.8125 | 0.2188 | 0.9375 | |||||
*The data referred to as a positive response in the overall analysis framework. **IL = Interleukin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



