
Submitted:
27 June 2024
Posted:
29 June 2024
You are already at the latest version
Abstract
Myasthenia Gravis (MG) is a chronic autoimmune neuromuscular disorder characterized by muscle weakness and fatigue, which can significantly impact various facets of daily life, including physical capabilities, emotional well-being, and social interactions. The prognosis, when supported by optimal symptomatic, immunosuppressive, and supportive treatment, is generally favorable. However, compelling evidence underscores the presence of diminished quality of life among patients with MG. Notably, cognitive impairment, depressive symptoms, and sleep disorders emerge as clinically pertinent dimensions in affected individuals, warranting careful scrutiny and investigation. Individuals with this condition often encounter challenges stemming from a lack of knowledge about effective coping strategies. The core objective of our research is to delve into the coping strategies adopted by patients with MG. To this end, we conducted an extensive inquiry, administering a series of personalized questions and utilizing the short version of the Coping Orientation to Problems Experienced questionnaire, (COPE-NVI-25) survey. Generative Artificial Intelligence was also employed to gain a better understanding of patient responses. The outcomes of our study hold the potential to steer the development of targeted interventions, strategic approaches, and valuable resources designed to assist patients with MG in proficiently managing their condition and enhancing their overall well-being.
Keywords:
Myasthenia Gravis
; Coping impairment
; COPE-NVI-25 questionnaire
Introduction
Myasthenia Gravis (MG) is an autoimmune neuromuscular disorder that significantly hampers muscle strength and endurance, posing profound challenges to the daily lives of those affected [1,2]. It is estimated that over 700,000 people worldwide are affected by this condition [3]. This alteration is due to antibodies against the acetylcholine receptor (AChR), muscle-specific kinase (MuSK), or other AChR-related proteins in the postsynaptic muscle membrane. Localized or general muscle weakness is the predominant symptom and is induced by antibodies. Diagnosis is straightforward in most patients with typical symptoms and a positive antibody test, although a detailed clinical and neurophysiological examination is important in patients who test negative for antibodies. Comorbidity is common, especially in older patients [4].
The journey from diagnosis to management and care still involves many obstacles, starting with the lack of early diagnosis. The most important elements of diagnosis are the clinical history and the findings of fluctuating and fatigable weakness, particularly involving the extraocular and bulbar muscles. The period between the onset of symptoms and diagnosis can be very long, causing considerable anxiety and frustration in patients [5]. Even when the disease is diagnosed, the difficulty of accessing specialized care negatively impacts the experiences of the patients [6], especially during COVID-19 pandemic [7,8,9].
While the advancements in symptomatic, immunosuppressive, and supportive treatments have generally improved the prognosis, MG significantly impacts the quality of life with substantial psycho-physical consequences [10]. The disease manifests through various clinical dimensions, including cognitive deficits, depressive states, and sleep disturbances, all of which necessitate comprehensive clinical attention [11,12,13,14]. Moreover, the personal, social, and work spheres are affected, as well as physical and psychological well-being. A meta-analysis reveals that the employment rate is considerably low considering that the average age of patients with MG is about 48 years Often, in a family, caregivers are represented by family members who, lacking training and appropriate knowledge of the pathology, assist the patient in a rather approximate manner. All these conditions lead both caregivers and patients themselves to develop disorders such as depression [15] and loneliness, which compromise their relative quality of life [16], with a greater incidence in females [5].
A notable gap in existing research pertains to the coping strategies employed by these patients, which are crucial for managing the everyday implications of the disease effectively. Understanding these coping mechanisms is vital for devising targeted interventions that enhance patient resilience and overall well-being [17]. To address this knowledge gap, our study focuses on exploring the coping strategies utilized by patients with MG. By employing a methodological framework that integrates the Coping Orientation to Problems Experienced (COPE-NVI-25) questionnaire—a validated instrument tailored to assess coping orientations in response to health challenges—and the innovative use of Generative Artificial Intelligence, we aim to capture a nuanced understanding of how patients navigate the complexities imposed by MG. The findings from our study could contribute significantly to the development of specific therapeutic strategies and support systems, ultimately improving the quality of life for individuals with MG.
Methods
Design
From January to April 2023 a survey was administered among MG patients. The study involved an anonymous survey administered through a voluntary questionnaire. All questionnaire sections were digitalized using a pre-set format on the Google Drive platform, and the research was carried out via electronic distribution. We reached out to different Facebook groups and Instagram pages to share the digital questionnaires. The sampling technique employed was virtual snowball sampling until data saturation was achieved.
Survey Instrument
The survey comprised a set of questions designed to outline the socio-demographic characteristics of the sample and to investigate existential coping strategies of patients with MG by means the Coping Orientation to the Problems Experienced questionnaire (COPE-NVI-25).
Socio-demographic characteristics include gender, age, nationality, marital status, level of education, and employment status. Additionally, it gathers information related to patients knowledge about the disease and how the patient manages the illness, the treatments, and the management of difficulties. Two more questions were administered with the possibility of adding open-ended responses from the participants. These questions are: “If you find the treatments you are receiving unsatisfactory, can you indicate the reasons why?” and “Write freely what you would recommend or believe is essential to change in the management of the disease”.
The COPE-NVI-25 survey consisted of 25 items, each linked to a Likert scale ranging from 1 to 6, where 1 represented “I never do” and 6 represented “I always do.” These items were categorized into 5 sub-dimensions: Avoidance Strategies, Transcendent Orientation, Positive Attitude, Social Support, and Problem Orientation. Summing the items within each sub-dimension yielded a total score, with higher values indicating a stronger inclination towards a particular sub-dimension. The questionnaire validation was established through previous research, which demonstrated favorable psychometric properties [18].
Statistical Analysis
Data were collected in an Excel sheet and the answers of all respondents to the questionnaire items were reported using descriptive statistics. Continuous variables were summarized using the mean and standard deviation (SD), and categorical variables were summarized using frequencies and percentages. For the validated questionnaire, descriptive statistics for the item responses, such as the item median, standard deviation, skewness, floor and ceiling effects, and 95% confidence intervals, were assessed and reported for each scale score. Cronbach’s alpha was used to measure the scale internal consistency reliability. COPE-NVI-25 subscales’ scores were registered as means (µ) ± standard deviations (SD). To determine the factors that influence the coping strategies, a one-way ANOVA was performed. To further analyze the influencing factors of the coping strategies, Multiple linear regression analysis was performed. Each subscale score was used as the dependent variable and the influencing factors of the coping strategies in the Univariate analysis were used as the independent variables. For questions with open-ended responses, the generative artificial intelligence (ChatGPT version 4) was used to group similar answers together and to gather a summary of the results. The statistical analyses were conducted for all qualitative and quantitative variables using Matlab software, 2023b version. Statistical significance level was set at p<0.05.
Ethical Considerations
The study ethical concerns were explicitly explained in the questionnaire introduction. The questionnaire structure followed the guidelines established by the Italian Data Protection Authority (DPA). It was emphasized that taking part in the study was entirely optional, and participants had the freedom to discontinue their involvement at any point. Individuals who indicated their willingness to participate were provided with an informed consent form that reiterated the voluntary nature of their participation and guaranteed the confidentiality and anonymity of the gathered data. Additionally, to enhance the protection of participants privacy, all responses in the questionnaire were anonymized.
Results
Sample Demographics and Baseline Characteristics
A total of 215 patients were recruited in this study. Baseline characteristics were collected and reported in Table 1. Patients were 83% females and 17% males. The mean age of the responders was 46.17 years (SD 14.59), with a range of 19-82 years. Seventy-one percent of the sample was from Italy and the majority of the participants were married (64%). A predominant portion of the participants (34%) had achieved education at the higher secondary level, and 35% held a university degree. Among the participants, 66% were either students or employed, while 33% were without employment or retired.
Questionnaire Items
The questionnaire items were evaluated for all respondents and data were collected (Table 2, Table 3 and Table 4).
Table 2 delves into patients awareness and training regarding MG, as well as the sources of information they encountered about the condition. It also investigates whether participants received health education from nurses at the clinic and their perspectives on utilizing telecommunication for addressing challenges associated with MG. A noteworthy proportion of participants (83%) had not been familiar with MG prior to their diagnosis. Among those who responded positively, intriguingly, the impact of mass media, family, friends, school, and even the healthcare setting appeared to be relatively limited.
Participants reported that they do not receive health education from clinical professionals (72%) or from home nurses (92%). Additionally, 80% of patients indicated that nurses did not provide recommendations for daily strategies or alternative solutions to alleviate symptoms. Lastly, the majority of patients (81%) perceived MG as being less recognized compared to other conditions. Moreover, there was a consensus among patients that innovative forms of telecommunication could contribute to managing challenges associated with the disease. These findings underline the need for more comprehensive health education strategies, highlighting the potential of telecommunication to bridge informational gaps and enhance management approaches for MG.
Table 3 presents various aspects related to how patients manage their illness, treatment, and challenges, including living situation, autonomy, mobility aids, initial symptoms, medical care, and psychosocial support in relation to MG. While a substantial proportion of participants (87%) indicated that they do not live alone, the majority (66%) expressed being completely autonomous. Concerning mobility aids, the largest group (81%) stated that they did not require any aids, while smaller percentages used a walking stick (11%), wheelchair (5%), or walker (4%).
Participants detailed diverse initial symptoms: unstable gait (31%), blurred or double vision (64%), drooping eyelids (64%), limb weakness (66%), and breathing difficulties (38%). Moreover, 41% believed that their condition could impact their family. A notable number of participants (73%) attended a specialized center or clinic for the disease, with 15% doing so partially. Among those who attended, only half (53%) expressed satisfaction with the care they received.
Regarding psychological support, 56% of participants considered it essential for individuals with MG to cope with challenges, while 36% regarded it as partially necessary. These findings underscore the diverse experiences and perspectives of individuals living with MG, encompassing various aspects such as living arrangements, autonomy, medical care, and psychosocial needs.
Generative Artificial Intelligence was then utilized to categorize similar responses and generate a comprehensive summary of the outcomes for open-ended responses. The responses were derived from participants answers to the questionnaire, in which they provided suggestions and highlighted perceived essential changes required in the management of MG. This encompassed their recommendations and beliefs regarding pivotal alterations in disease management. This analysis facilitated the recognition and organization of various themes, which are delineated and presented in Table 4. Additionally, an inclusive summary of the results inferred by ChatGPT has been incorporated.
COPE Score Analysis
Table 5 presents the responses to the COPE-NVI-25 questionnaire along with their respective percentages. The distribution of scores for the subscales, expressed in percentages, is shown in Figure 1.
In Table 6, descriptive statistics provide insights into the score distribution for the COPE-NVI-25 questionnaire, shedding light on how participants employ coping strategies and orientations in the context of MG. Patients scores are moderately reported, ranging from 2.25 (Avoidance Strategies) to 4.50 (Positive Attitude). Notably, the lowest mean scores are observed in the Avoidance Strategies and Transcendent Orientation subscales, displaying positive skewness, indicating a leaning toward higher scores. These two subscales also exhibit a higher percentage at the floor (9.64% and 11.54%, respectively), suggesting certain patients tend toward lower scores. Conversely, other subscales demonstrate negative skewness, implying a slight leftward distribution. The internal consistency reliability, as measured by Cronbach’s alpha, is 0.87 for all items. The minimum Cronbach’s alpha exceeds 0.70. For 3 out of 5 scales, Cronbach’s alpha exceeds 0.80, while the Transcendent Orientation subscale surpasses 0.90, thus satisfying Nunnally’s criterion of 0.7 [19].
Univariate analysis was employed to discern factors influencing coping strategies and reported in Table 7. Notable differences in the Problem Orientation subscale were observed based on age (p<0.05). Additionally, the Transcendent Orientation subscale was influenced by the geographical area of origin (p<0.01). Several factors were significantly associated with various subscales. These factors include having received home health education and autonomy, which were both linked to Transcendent Orientation, Social Support, and Problem Orientation. Awareness of the disease existence and advice on daily strategies from healthcare professionals were associated with Avoidance Strategies (p<0.05). Hearing about the disease through mass media and friends influenced the Transcendent Orientation subscale (p<0.01) and Problem Orientation subscale (p<0.05), respectively. Intriguingly, learning about the disease at school demonstrated a strong association with nearly all subscales.
To further investigate the factors influencing the coping strategies score of patients, a multiple linear regression analysis was conducted (Table 8). The results indicated that two key variables, namely participants prior awareness of MG and the guidance received from clinic nurses regarding strategies to alleviate symptoms, significantly contribute to explaining the variance in Avoidance Strategies (p<0.01). However, it is important to note that the overall explanatory capacity of the model remains limited, suggesting that additional unexamined factors may also contribute to the variation in Avoidance Strategies. Similarly, the same conclusion can be drawn for the Transcendent Orientation subscale and Social Support, as both exhibit notable associations with variables such as having received information about the condition at school, the guidance provided by clinic nurses for symptom-alleviating strategies (for both subscales), and geographical area of origin, autonomy, and exposure to mass media (for Transcendent Orientation only) (p<0.01). Just as observed with Avoidance Strategies, it becomes apparent that while these identified variables demonstrate significance, the potential exists for additional unexplored factors to contribute to the observed variability in both the Transcendent Orientation and Social Support subscales.
Discussion
In this study, we explored the coping patterns among patients with Myasthenia Gravis (MG), leveraging a validated questionnaire, COPE-NVI-25 [20], and a series of ad hoc administered questions, including open-ended ones designed to gather in-depth information on patients knowledge about their disease and how they manage its difficulties.
Most patients (72.6%) attend a centre where MG is treated, but the majority are not satisfied with the care they receive for several reasons. These concerns relate to the lack of health education provided by the nurse at the clinic they visit. The nurses responsible for managing MG do not implement any health education, even at home, lacking the necessary training to do so, and consequently, they are unable to advise patients on significant strategies to alleviate the symptoms of such pathology or how to deal with it. Among the few studies present in the literature, there emerges a lack of knowledge among nurses, enough to compromise the care [21].
The application of the COPE-NVI-25 survey enabled us to quantify coping strategies across five distinct sub-dimensions: Avoidance Strategies, Transcendent Orientation, Positive Attitude, Social Support, and Problem Orientation. The survey results revealed moderate use of coping strategies, with the highest scores in Positive Attitude and the lowest in Avoidance Strategies and Transcendent Orientation. This suggests that patients are more inclined to adopt a positive outlook rather than avoid their problems, which can be seen as a proactive approach to managing their condition. This variation might indicate that while avoidance and spiritual coping are generally less favoured, they are significant for a subset of patients. These findings align with the broader literature that emphasizes the importance of a positive mindset in chronic disease management, where maintaining an optimistic outlook is associated with better quality of life and reduced depression and anxiety [22]. Conversely, the positive skewness in ‘Avoidance Strategies’ and ‘Transcendent Orientation’ indicates that there is a tail towards higher scores. There is a need to consider individual differences in coping preferences and effectiveness. Tailoring interventions to support each patient preferred coping style might help improve their overall management of the disease and enhance their quality of life.
Our findings also highlight significant associations between coping strategies and various factors like age, geographic origin, prior awareness of the disease, and access to health education. For instance, younger patients and those from different geographic regions exhibited different coping patterns, possibly reflecting cultural and systemic differences in health education and disease management approaches. Younger patients might be more proactive or reactive in facing the challenges posed by MG, indicating a potential need for age-specific support strategies that cater to their unique coping styles. Previous studies have similarly noted the influence of cultural and systemic factors on health behaviour and coping strategies in chronic diseases [23].
The association between awareness of the disease and professional advice with ‘Avoidance Strategies’ highlights the role of knowledge and external support in shaping how patients cope with MG. Patients who are more aware of their condition and receive advice on daily management strategies may be better prepared to face their condition head-on rather than resorting to avoidance. In addition, the significant impact of information sources like mass media and schools on coping strategies such as ‘Transcendent Orientation’ and ‘Problem Orientation’ emphasizes the power of information dissemination methods. This finding suggests that the way patients learn about their disease—whether through formal education or media—can profoundly affect how they cope with their illness.
The multiple linear regression analysis offers further insights into the factors influencing coping strategies among MG patients. The analysis identifies prior awareness of MG and the guidance received from clinic nurses about symptom alleviation as significant predictors for the use of ‘Avoidance Strategies’. This indicates that patients who are more informed about their condition and those who receive actionable advice from healthcare professionals are likely to avoid less effective coping mechanisms. For the ‘Transcendent Orientation’ and ‘Social Support’ subscales, the analysis again confirm the influence of education (information received at school) and healthcare interaction (guidance from clinic nurses) along with geographic and cultural factors (geographical area of origin and exposure to mass media). These findings suggest that both personal experiences and socio-cultural environments play significant roles in shaping coping behaviours, supporting the need for a multifaceted approach in patient education and support.
These insights are crucial for healthcare providers and policymakers as they highlight the need for targeted interventions that consider these various factors. By understanding the specific needs and influences of different demographic groups, interventions can be more precisely tailored to improve coping strategies among MG patients, ultimately enhancing their overall management and quality of life. This approach supports a more personalized medicine framework, where treatment and support are adapted to individual characteristics and needs.
In the present investigation, we also employed an innovative approach based on Generative Artificial Intelligence to analyze open-ended responses provided by questionnaire participants regarding the management of MG. The results highlight a range of key themes that reflect patients opinions and perspectives on enhancing care and treatment for this complex disease. A predominant theme emerging from the responses is the significance of personalized therapies. Participants underscored the need to consider variations in symptoms and severity among patients, calling for targeted therapeutic approaches and innovative options. This underscores the importance of tailored treatment that takes into account individual patient needs.
Another relevant theme pertains to communication and interaction between physicians and patients. Participants emphasized the necessity of improving the clinician-patient relationship through active listening and increased patient engagement in the decision-making process. The request for psychological support reflects the importance of addressing emotional aspects of the disease and ensuring empathetic and sensitive treatment.
Education and information emerged as crucial components. Participants expressed a desire for greater public awareness about MG and improved medical education regarding the disease. This highlights the importance of combating ignorance and promoting deeper understanding among both medical professionals and the general public.
The social and economic dimensions were equally significant. Patients called for increased financial support and legal recognition of the disease to ensure adequate safeguards. The importance of patient support networks and a multidisciplinary approach to care underscores the need for a holistic approach to addressing MG.
In conclusion, participants responses reflect the importance of a comprehensive, personalized, and interdisciplinary approach to managing MG. The requests for personalized therapies, effective communication, accurate information, and appropriate social and economic support underscore the need to comprehensively address this complex disease. This study provides further insights into patient perspectives and can inform the development of enhanced strategies for the management of MG.
Future research should explore additional factors that could influence coping strategies. This could include deeper psychological assessments, socio-economic factors, family dynamics, and broader community support systems, which might offer further insights into the complex nature of coping with chronic illnesses like MG.
Limits
While the study highlights the coping strategies and adaptation mechanisms employed by patients, it also acknowledges the limitations of the analysis. The use of virtual sampling and self-reported data may introduce bias, and the findings might not be generalizable to all MG populations. Furthermore, while our study provides insights into the associations between coping strategies and certain demographic and medical factors, it does not establish causality. Further research is warranted to explore additional factors that may influence coping strategies and to validate the observed patterns in larger and more diverse patient populations. Overall, our study highlights the importance of tailored interventions and resources aimed at empowering patients to manage their condition effectively.
Conclusions
Our study illuminates the coping strategies embraced by patients contending with the challenges posed by MG. The findings underscore the intricate nature of this chronic autoimmune neuromuscular disorder and its profound repercussions across various dimensions of daily life. Notably, our research unveils patients’ resolute determination to ameliorate the impact of the ailment across its diverse phases. However, a noteworthy proportion of participants encounter hurdles stemming from a dearth of knowledge regarding efficacious coping strategies. This underscores the imperative of tailored interventions and resources aimed at empowering patients in effectively managing their condition. In conclusion, this study contributes to a deeper understanding of how individuals with MG navigate the complexities of their condition. The insights gained have the potential to drive the development of more effective interventions, ultimately enhancing the quality of life for patients and improving their ability to cope with the challenges posed by this chronic disorder.
Consent for publication:
All authors have read and approved the final manuscript, and we consent to its publication
Availability of data and materials:
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval:
The questionnaire adhered to the Helsinki principles and was approved by the Ethical committee of the General hospital of Policlinic of Bari, Italy, with id number n. 7766 of 11/01/2023.
Conflicts of interest:
Authors declare no conflicts of interest.
Code availability:
The code used in this study is available from the corresponding author on reasonable request.
Funding
No funding was received for conducting this study
References
- Conti-Fine, B.M.; Milani, M.; Kaminski, H.J. Myasthenia Gravis: Past, Present, and Future. J. Clin. Invest. 2006, 116, 2843–2854. [Google Scholar] [CrossRef] [PubMed]
- Dresser, L.; Wlodarski, R.; Rezania, K.; Soliven, B. Myasthenia Gravis: Epidemiology, Pathophysiology and Clinical Manifestations. J. Clin. Med. 2021, 10, 2235. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswami, P.; Sanders, D.B.; Wolfe, G.; Benatar, M.; Cea, G.; Evoli, A.; Gilhus, N.E.; Illa, I.; Kuntz, N.L.; Massey, J.; et al. International Consensus Guidance for Management of Myasthenia Gravis: 2020 Update. Neurology 2021, 96, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Gilhus, N.E.; Tzartos, S.; Evoli, A.; Palace, J.; Burns, T.M.; Verschuuren, J.J.G.M. Myasthenia Gravis. Nat. Rev. Dis. Prim. 2019, 5, 30. [Google Scholar] [CrossRef]
- Bogdan, A.; Barnett, C.; Ali, A.; AlQwaifly, M.; Abraham, A.; Mannan, S.; Ng, E.; Bril, V. Chronic Stress, Depression and Personality Type in Patients with Myasthenia Gravis. Eur. J. Neurol. 2020, 27, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Law, N.; Davio, K.; Blunck, M.; Lobban, D.; Seddik, K. The Lived Experience of Myasthenia Gravis: A Patient-Led Analysis. Neurol. Ther. 2021, 10, 1103–1125. [Google Scholar] [CrossRef] [PubMed]
- Carriero, M.C.; Conte, L.; Calignano, M.; Lupo, R.; Calabrò, A.; Santoro, P.; Artioli, G.; Caldararo, C.; Ercolani, M.; Carvello, M.; et al. The Psychological Impact of the Coronavirus Emergency on Physicians and Nurses: An Italian Observational Study. Acta Biomed. 2021, 92, e2021030. [Google Scholar] [CrossRef]
- Vitale, E.; Conte, L.; Dell’Aglio, A.; Calabrò, A.; Ilari, F.; Bardone, L.; Benedetto, A.; Caldararo, C.; Zacchino, S.; Lezzi, A.; et al. Healthcare Workers Perceptions in the Difficult Moment of the End of Life and Coping Strategies Adopted during the COVID-19 Pandemic: An Italian Pilot Study. Acta Biomed. 2021, 92, e2021330. [Google Scholar] [CrossRef]
- Lupo, R.; Vitale, E.; Panzanaro, L.; Lezzi, A.; Lezzi, P.; Botti, S.; Rubbi, I.; Carvello, M.; Calabrò, A.; Puglia, A.; et al. Effects of Long COVID on Psycho-Physical Conditions in the Italian Population: A Statistical and Large Language Model Combined Description. Eur. J. Investig. Heal. Psychol. Educ. 2024, 14, 1153–1170. [Google Scholar] [CrossRef]
- Nadali, J.; Ghavampour, N.; Beiranvand, F.; Maleki Takhtegahi, M.; Heidari, M.E.; Salarvand, S.; Arabzadeh, T.; Narimani Charan, O. Prevalence of Depression and Anxiety among Myasthenia Gravis (MG) Patients: A Systematic Review and Meta-Analysis. Brain Behav. 2023, 13, e2840. [Google Scholar] [CrossRef] [PubMed]
- Stojanov, A.; Milošević, V.; Đorđević, G.; Stojanov, J. Quality of Life of Myasthenia Gravis Patients in Regard to Epidemiological and Clinical Characteristics of the Disease. Neurologist 2019, 24, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Gilhus, N.E.; Verschuuren, J.J.G.M.; Hovland, S.I.B.; Simmonds, H.; Groot, F.; Palace, J. Myasthenia Gravis: Do Not Forget the Patient Perspective. Neuromuscul. Disord. 2021, 31, 1287–1295. [Google Scholar] [CrossRef]
- Paul, R.H.; Mullins, L.L.; Gilchrist, J.M. The Impact of Myasthenia Gravis on Mood, Cognitive Function, and Quality of Life. In Myasthenia Gravis and Related Disorders; Humana Press: Totowa, NJ, 2009; pp. 279–292. [Google Scholar]
- Tascilar, N.F.; Saracli, O.; Kurcer, M.A.; Ankarali, H.; Emre, U. Is There Any Relationship between Quality of Life and Polysomnographically Detected Sleep Parameters/Disorders in Stable Myasthenia Gravis? Acta Neurol. Belg. 2018, 118, 29–37. [Google Scholar] [CrossRef]
- Mihalache, O.A.; Vilciu, C.; Petrescu, D.-M.; Petrescu, C.; Manea, M.C.; Ciobanu, A.M.; Ciobanu, C.A.; Popa-Velea, O.; Riga, S. Depression: A Contributing Factor to the Clinical Course in Myasthenia Gravis Patients. Medicina (Kaunas). 2023, 60. [Google Scholar] [CrossRef] [PubMed]
- Marbin, D.; Piper, S.K.; Lehnerer, S.; Harms, U.; Meisel, A. Mental Health in Myasthenia Gravis Patients and Its Impact on Caregiver Burden. Sci. Rep. 2022, 12, 19275. [Google Scholar] [CrossRef] [PubMed]
- Farrugia, M.E.; Goodfellow, J.A. A Practical Approach to Managing Patients With Myasthenia Gravis—Opinions and a Review of the Literature. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Ciceri, M.R.; Anolli, L.M. La Voce Delle Emozioni. Verso Una Semiosi Della Comunicazione Vocale Non-Verbale Delle Emozioni.; Angeli, F., Ed.; IV Edition.; Milano 2000. 2000. [Google Scholar]
- Nunnally, J. Psychometric Theory; Co, M.-H.B., Ed.; 2nd ed. Ne.; 1978. [Google Scholar]
- Caricati, L.; Foà, C.; Fruggeri, L.; Tonarelli, A. COPE-NVI-25: Validazione Italiana Della Versione Ridotta Della Coping Orientation to the Problems Experienced (COPE-NVI). Psicol. DELLA Salut. 2015, 123–140. [Google Scholar] [CrossRef]
- Suñer, R.; Mascort, Z. [Evaluation of Nursing Care in Patients with Myasthenia Gravis]. Rev. Neurol. 1997, 25, 255–256. [Google Scholar] [PubMed]
- Hohls, J.K.; König, H.-H.; Quirke, E.; Hajek, A. Anxiety, Depression and Quality of Life—A Systematic Review of Evidence from Longitudinal Observational Studies. Int. J. Environ. Res. Public Health 2021, 18, 12022. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Qian, X.; Chen, Z.; He, T. Health Literacy and Its Effect on Chronic Disease Prevention: Evidence from China’s Data. BMC Public Health 2020, 20, 690. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Frequency distributions (percent) for the five subscales of the COPE-NVI-25 questionnaire (panels A to E).
Figure 1.
Frequency distributions (percent) for the five subscales of the COPE-NVI-25 questionnaire (panels A to E).
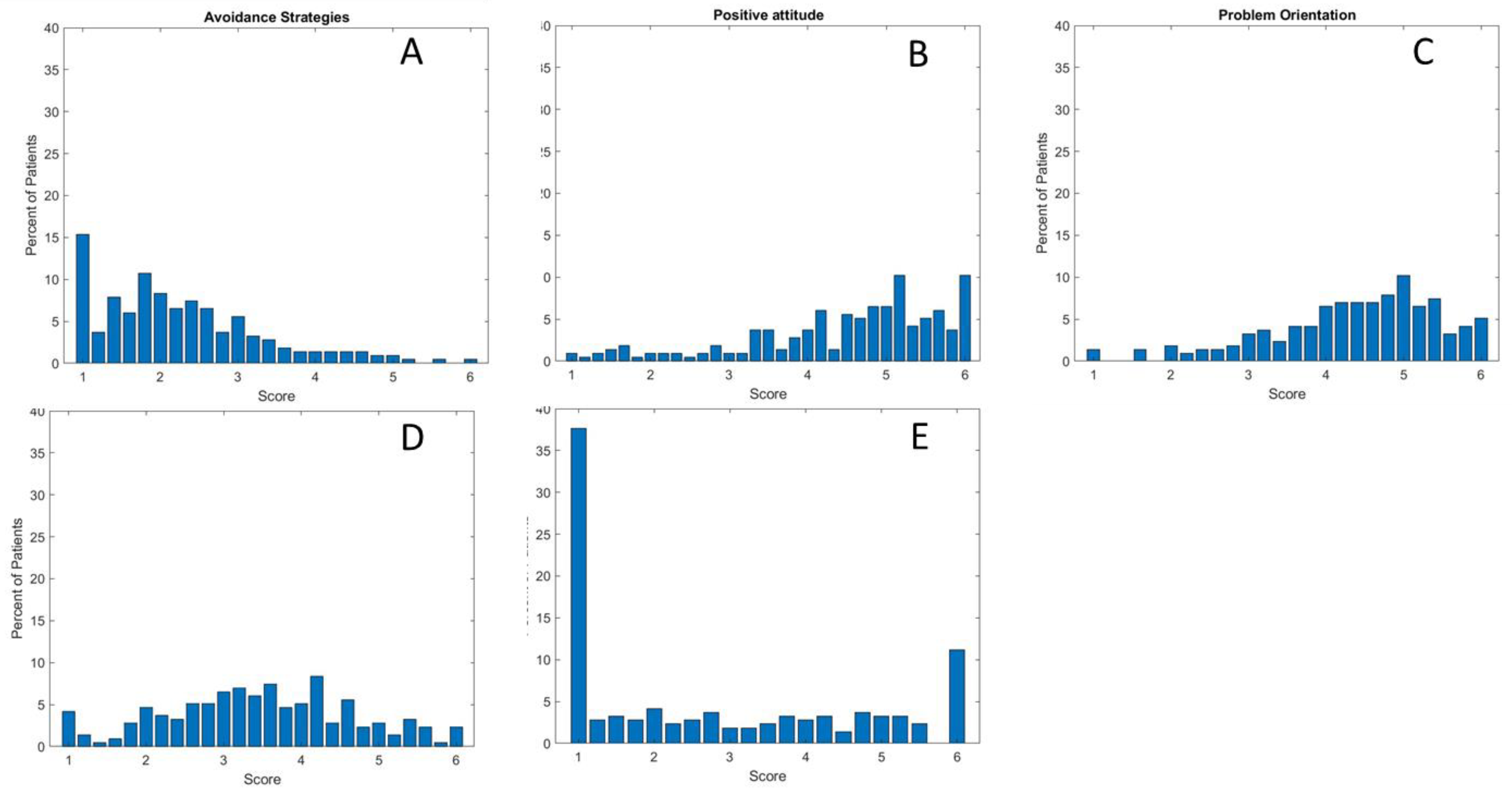

Table 1.
Sampling characteristics of all respondents (socio-demographics data and information about the patients) (n=215).
Table 1.
Sampling characteristics of all respondents (socio-demographics data and information about the patients) (n=215).
|
BASELINE CHARACTERISTICS |
N |
% |
|---|---|---|
| Socio-demographics | ||
|
Gender Female Male |
178 37 |
83 17 |
|
Age Range Mean SD |
19-82 46.17 14.59 |
|
| Nationality |
152 63 |
71 29 |
| Italians Non-Italians | ||
| Married status |
137 66 10 2 |
64 31 5 1 |
| Married Single/Celibate Separated/Divorced Widower | ||
|
Level of education No title |
4 |
2 |
| Lower secondary school certificate Higher Diploma Degree Postgraduate training |
14 73 76 48 |
7 34 35 22 |
| Employment status |
31 62 33 33 32 17 7 |
14 29 15 15 15 8 3 |
| Civil servant Private employee Freelancer Unemployed Retired Student Invalid | ||
Table 2.
Information about patients’ knowledge and training about the disease (n=215).
| N | % | |
|---|---|---|
| Before your diagnosis, had you ever heard of MG? |
179 36 |
83 17 |
| No Yes | ||
| If you answered YES to the previous question, in which field did you hear about it? |
0 0 15 19 181 2 0 9 7 197 1 2 9 12 191 0 0 7 11 197 |
0 0 7 9 84 1 0 4 3 92 0 1 4 6 89 0 0 3 5 92 |
|
MASS MEDIA Always Often Occasionally Rarely Never FAMILY Always Often Occasionally Rarely Never SCHOOL Always Often Occasionally Rarely Never FRIENDS Always Often Occasionally Rarely Never SANITARY | ||
| Always Often Occasionally Rarely Never |
4 0 20 28 163 |
2 0 9 13 76 |
|
For the management of the condition, have you ever received health education from the nurse practitioner at the outpatient clinic you go to? No Yes |
155 60 |
72 28 |
|
Have you ever received home health education from the nursing professional? No Yes |
198 17 |
92 8 |
|
In the outpatient clinic, does the nurse advise you on what strategies to implement on a daily basis and whether there are alternative solutions to alleviate your symptoms? No Yes |
173 42 |
80 20 |
|
In your opinion, is MG still an unknown or under-recognised pathology compared to other diseases? No Yes In part |
4 175 36 |
2 81 17 |
|
Do you believe that new forms of telecommunication can help to better manage MG- related problems? No Yes |
11 204 |
5 95 |
Table 3.
How the patient manages the illness, the treatments, and the management of difficulties (n=215).
Table 3.
How the patient manages the illness, the treatments, and the management of difficulties (n=215).
| N | % | |
|---|---|---|
|
Do you live alone? No Yes Yes, but I have children/neighbours who help me |
186 24 5 |
87 11 2 |
|
Are you autonomous? Yes but only at home, while I need help going out Yes, I am completely autonomous No, I totally need help No I need help in part |
19 142 24 30 |
9 66 11 14 |
|
To move around, do you need an aid? No, I don’t need anything Yes, I use the stick Yes, I use the wheelchair Yes, I use the walker |
174 23 10 8 |
81 11 5 4 |
|
What signs and symptoms did you experience in the early phase of the disease (more than one answer possible) Unsteady gait Blurred or double vision Eyelid ptosis Limb weakness Difficulty breathing Nothing |
67 145 138 142 81 6 |
31 67 64 66 38 3 |
|
Do you attend a centre and/or outpatient clinic that deals with the disease? No Yes In part |
27 156 32 |
13 73 15 |
| If you attend the centre and/or clinic, are you satisfied with the care you receive? |
29 114 71 1 |
13 53 33 0 |
| No Yes In part missing | ||
| Do you think that your life will now burden your family’s? |
40 89 |
19 41 |
| No Yes |
Table 4.
Generative Artificial Intelligence (ChatGPT) of open-ended responses and result summary.
| ChatGPT-found categories: | ChatGPT Summary of Results | |
|---|---|---|
| If you find the treatments you are receiving unsatisfactory, can you indicate the reasons why? |
Improvement of Therapies and Treatments:
|
Questionnaire participants expressed a range of suggestions and opinions regarding the management of MG. The majority emphasized the importance of personalized therapies, including alternative treatments and experimental interventions. Furthermore, they highlighted the need for open and collaborative communication with medical professionals, emphasizing active listening and psychological support. A common theme was the lack of information about the disease, with a call for greater awareness campaigns and education for both medical professionals and the general public. Participants stressed the significance of swift and accurate diagnosis, along with improved access to specialized tests and therapies. The social and economic dimensions emerged as relevant factors, with requests for increased financial support and legal recognition for patients. Participants also indicated the need for patient support networks and groups, in addition to underscoring the importance of a multidisciplinary approach to treatment. Overall, the responses underscore the importance of a holistic approach to managing MG, encompassing personalized therapies, effective communication, accurate information, and adequate social and economic support. |
| Write freely what you would recommend or believe is essential to change in the management of the disease |
Therapies and Treatments:
|
In the collected responses, a series of key points and suggestions for improving the management of MG emerge: Patients are calling for a more targeted and personalized approach to therapy, taking into account the variation in symptoms and their severity among patients. There is hope for a more effective therapy and the provision of innovative and personalized therapeutic options. Improving access to exams and treatments is a crucial aspect, reducing wait times for diagnoses and treatments. This could be facilitated through the implementation of specialized centers and the creation of medical support networks. A greater understanding of the disease among doctors from various specialties is requested, as well as better training for primary care physicians to promptly recognize symptoms and initiate the diagnostic process. The desire for better communication and interaction between doctors and patients is evident, with increased patient involvement in the decision-making process and greater attention to their needs. Psychological support, both in the form of therapy and counseling, is considered important for addressing the emotional aspects of the disease. Patients want to be treated with humanity and sensitivity by healthcare providers. Information and awareness are deemed crucial for both patients and society at large. MG is often poorly understood, so increased awareness could help combat ignorance and promote better understanding. Work-related concerns are evident, with requests for workplace support and potential adjustments to working conditions. Access to experimental treatments and alternative therapies is an interest, emphasizing the need for diverse therapeutic options. Lastly, patients desire to be treated with respect, understanding, and attention by medical staff, and they hope that the disease will be recognized as disabling to facilitate legal and social support. These suggestions and patient desires reflect the importance of a comprehensive and personalized approach to managing MG, aiming to improve patients’ quality of life and ensure adequate support in all aspects of their battle against the disease. |
Table 5.
The Coping Orientation to the Problems Experienced (COPE-NVI-25) questionnaire items. The survey consisted of 25 items, each linked to a Likert scale ranging from 1 to 6, where 1 represented “I never do” and 6 represented “I always do.”.
Table 5.
The Coping Orientation to the Problems Experienced (COPE-NVI-25) questionnaire items. The survey consisted of 25 items, each linked to a Likert scale ranging from 1 to 6, where 1 represented “I never do” and 6 represented “I always do.”.
|
COPE-NVI-25 QUESTIONNAIRE ITEMS |
N |
% |
|---|---|---|
|
1. I try to get advice from someone on what to do 1 2 3 4 5 6 |
32 25 49 39 34 36 |
15 12 23 18 16 17 |
|
2. I learn to live with the problem 1 2 3 4 5 6 |
10 10 24 25 51 95 |
5 5 11 12 24 44 |
|
3. I concentrate on dealing with this problem and, if necessary, put other things aside 1 2 3 4 5 6 |
14 17 45 49 45 45 |
7 8 21 23 21 21 |
|
4. I do not put much effort into solving the problem 1 2 3 4 5 6 |
101 37 33 21 13 10 |
47 17 15 10 6 5 |
|
5. I try to prevent other things from interfering with my coping efforts 1 2 3 4 5 6 |
17 22 42 50 42 42 |
8 10 20 23 20 20 |
|
6. I look for something positive in what happened 1 2 3 4 5 6 |
27 18 25 41 41 63 |
13 8 12 19 19 29 |
|
7. I refuse to believe that this happened 1 2 3 4 5 6 |
121 33 21 17 9 14 |
56 15 10 8 4 7 |
|
8. Seeking help in God 1 2 3 4 5 6 |
96 13 18 23 17 48 |
45 6 8 11 8 22 |
|
9. I do what needs to be done, one step at a time 1 2 3 4 5 6 |
8 7 16 33 54 97 |
4 3 7 15 25 45 |
|
10. I talk to someone to do something concrete to solve the problem 1 2 3 4 5 6 |
33 17 41 34 40 50 |
15 8 19 16 19 23 |
|
11. I pray more than usual 1 2 3 4 5 6 |
104 17 32 28 7 27 |
48 8 15 13 3 13 |
|
12. I try to learn something from experience 1 2 3 4 5 6 |
13 13 26 28 51 84 |
6 6 12 13 24 39 |
|
13. I make every effort to act on the situation 1 2 3 4 5 6 |
7 7 24 33 55 89 |
3 3 11 15 26 41 |
|
14. I try to find solace in my religion 1 2 3 4 5 6 |
102 20 20 23 13 37 |
47 9 9 11 6 7 |
|
15. I ask people how they have acted when faced with similar experiences 1 2 3 4 5 6 |
33 32 38 49 28 35 |
15 15 18 23 13 16 |
|
16. I try to use this experience to grow as a person 1 2 3 4 5 6 |
16 11 29 33 48 78 |
7 5 13 15 22 36 |
|
17. I act as if it never happened 1 2 3 4 5 6 |
101 35 31 23 12 13 |
47 16 14 11 6 6 |
|
18. Seeking moral support from friends and relatives 1 2 3 4 5 6 |
53 31 40 33 34 24 |
25 14 19 15 16 11 |
|
19. I put my hope in God 1 2 3 4 5 6 |
95 24 19 20 15 42 |
44 11 9 9 7 20 |
|
20. I think hard about what moves to make to deal with the problem 1 2 3 4 5 6 |
19 15 39 48 39 55 |
9 7 18 22 18 26 |
|
21. I recognise that I cannot do anything about it and abandon all attempts to act 1 2 3 4 5 6 |
115 41 27 13 4 15 |
53 19 13 6 2 7 |
|
22. I tend to fantasise to distract myself 1 2 3 4 5 6 |
80 35 35 30 23 12 |
37 16 16 14 11 6 |
|
23. I accept the reality of the facts 1 2 3 4 5 6 |
15 13 20 39 48 80 |
7 6 9 18 22 37 |
|
24. Trying to get used to the idea that this happened 1 2 3 4 5 6 |
12 13 21 47 51 71 |
6 6 10 22 24 33 |
|
25. Seeking someone’s understanding and solidarity 1 2 3 4 5 6 |
49 34 38 41 28 25 |
23 16 18 19 13 12 |
Table 6.
Descriptive statistics of score distributions for COPE-NVI-25 questionnaire. Cronbach’s alpha was used to measure the scales’ internal consistency reliability.
Table 6.
Descriptive statistics of score distributions for COPE-NVI-25 questionnaire. Cronbach’s alpha was used to measure the scales’ internal consistency reliability.
| Subscale COPE-NVI-25 |
No. of items | Score |
95% CI | Median | SD | % floor† | % ceiling‡ | Skewness | Cronbach’s α* Total items = 0.87 |
|---|---|---|---|---|---|---|---|---|---|
| Avoidance_Strategies | 5 | 2.25 | 2.25-2.26 | 1.6 | 0.0501 | 9.64 | 1.19 | 1.07 | 0.71 |
| Transcendent_Orientation | 4 | 2.75 | 2.75-2.77 | 2 | 0.12 | 11.54 | 4.48 | 0.59 | 0.96 |
| Positive Attitude | 6 | 4.50 | 4.50-4.51 | 0.093 | 1.57 | 1.20 | 6.09 | -0.84 | 0.88 |
| Social Support | 5 | 3.54 | 3.46-3.46 | 3.6 | 0.036 | 3.72 | 3.16 | -0.00403 | 0.76 |
| Problem Orientation | 5 | 4.36 | 4.36-4.37 | 4.4 | 0.104 | 1.21 | 6.10 | -0.68 | 0.81 |
†Percentage of patients with worst possible score. ‡Percentage of patients with best possible score. *Measure of internal consistency.
Table 7.
Univariate analysis of the COPE-NVI-25 subscales (n=215) according too socio-demographic characteristics, Information about patients’ knowledge and training about the disease and How the patient manages the illness, the treatments they receive, and the management of difficulties. A p-value <0.05 was considered statistically significant (*p<0.05; **p<0.01; ***p<0.001).
Table 7.
Univariate analysis of the COPE-NVI-25 subscales (n=215) according too socio-demographic characteristics, Information about patients’ knowledge and training about the disease and How the patient manages the illness, the treatments they receive, and the management of difficulties. A p-value <0.05 was considered statistically significant (*p<0.05; **p<0.01; ***p<0.001).
|
µ±s.d |
COPE-NVI-25 subscales p-value |
|||||
|---|---|---|---|---|---|---|
| COPE-NVI-25/ Socio-demographic characteristics |
Avoidance Strategies |
Transcendent Orientation |
Positive attitude | Social Support | Problem Orientation |
|
|
Gender Female Male |
112.1 ± 61.8 88 ± 60.8 |
0.315 |
0.468 |
0.755 |
0.476 |
0.722 |
|
Age <20 20-30 31-40 41-50 51-60 61-70 71-80 >81 |
93.3 ± 40.2 100.8 ± 71.5 90.09 ± 64.9 110.31 ± 3.26 115.37 ± 53.2 119.3 ± 62.04 109.2 ± 50.7 130.5 ± 14.8 |
0.209 |
0.545 |
0.334 |
0.260 |
<0.05* |
|
Geographic area Argentina Australia Bulgaria Canada Egitto Germania Giordania Grecia India Inghilterra Italia Libia Macedonia Malta Paesi Bassi Portorico Scozia Sud Africa USA |
186.5 ± 0.7 179.5 ± 17.6 193 ± 0 204 ± 0 164 ± 0 171 ± 0 179 ± 0 194.3 ± 18.9 190.6 ± 22.5 185 ± 14.1 77.3 ± 45.7 177 ± 0 185.6 ± 29.5 111 ± 0 185.5 ± 3.5 200 ± 0 182 ± 23.06 174.5 ± 28.9 181.06 ± 20.01 |
0.895 |
<0.01* |
0.841 |
0.566 |
0.786 |
|
Level of education No title Lower secondary school Higher Diploma Degree Postgraduate training |
88.2 ± 39.8 84.6 ± 48.7 78.9 ± 49.9 111.5 ± 4.3 155.06 ± 51.4 |
0.09 |
0.608 |
0.772 |
0.200 |
0.775 |
|
Employment status Employee Freelancer Student Retired Unemployed |
125.6 ± 63.09 96.6 ± 59.3 96.5 ± 62.2 126.5 ± 63.3 93.7 ± 62.8 |
0.362 |
0.08 |
0.837 |
0.560 |
0.428 |
|
Marital status Married Single/Celibate Separated/Divorced Widower |
110.4 ± 59.8 99.07 ± 66.2 131 ± 61.7 122 ± 100.4 |
0.125 |
0.3006 |
0.229 |
0.292 |
0.219 |
|
Before your diagnosis, had you ever heard of MG? No Yes |
103.3 ± 60.7 131 ± 65.01 |
<0.05* |
0.828 |
0.364 |
0.626 |
0.217 |
|
If you answered YES to the previous question, in which field did you hear about it? MASS MEDIA Always Often Occasionally Rarely Never FAMILY Always Often Occasionally Rarely Never SCHOOL Always Often Occasionally Rarely Never FRIENDS Always Often Occasionally Rarely Never HEALTHCARE SECTOR Always Often Occasionally Rarely Never |
0 0 84.7 ± 49.8 114.7 ± 70.6 106.01 ± 61.2 133.5 ± 37.4 0 89 ± 39.8 81.8 ± 74.3 107.3 ± 62.1 71 ± 0 190 ± 11.3 134 ± 0 136.6 ± 65.05 102.1 ± 60.5 0 0 128.7 ± 15.9 103.1 ± 72.7 106.7 ± 62.01 111.5 ± 30.1 0 80.3 ± 40.5 126.9 ± 63.6 102.3 ± 61.8 |
0.253 0.409 0.552 0.400 0.07 |
0.01** 0.109 <0.05* 0.258 0.403 |
0.905 0.348 <0.05* 0.222 0.267 |
0.483 0.349 <0.05* 0.423 0.305 |
0.523 0.199 <0.01* <0.05* 0.287 |
|
Have you ever received home health education from the nursing professional? No Yes |
111.4 ± 61.6 99.08 ± 63.3 |
0.07 |
0.203 |
0.435 |
0.09 |
0.345 |
|
Have you ever received home health education from the nursing professional? No Yes |
104.7 ± 61.8 146.5 ± 53.8 |
0.06 |
<0.05* |
0.332 |
<0.001*** |
0.05* |
|
In the outpatient clinic, does the nurse advise you on what strategies to implement on a daily basis and whether there are alternative solutions to alleviate your symptoms? No Yes |
108.1 ± 61.2 107.5 ± 66.8 |
<0.05* |
0.334 |
0.289 |
0.114 |
0.874 |
|
Are you autonomous? No, I totally need help No, I need help in part Yes |
93.6 ± 62.2 164.7 ± 36.05 103.3 ± 60.8 |
0.759 |
<0.05* |
0.429 |
0.01** |
<0.05* |
Table 8.
Multiple linear regression analysis performed with the COPE-NVI-25 subscales as the dependent variable (n=215). A p-value <0.05 was considered statistically significant (*p<0.05; **p<0.01; ***p<0.001).
Table 8.
Multiple linear regression analysis performed with the COPE-NVI-25 subscales as the dependent variable (n=215). A p-value <0.05 was considered statistically significant (*p<0.05; **p<0.01; ***p<0.001).
| Dependent variable |
Independent variable | R2 | R2 adj | F-statistic | p-value |
|---|---|---|---|---|---|
|
Avoiding strategies |
Prior to diagnosis, had you ever heard of MG In the outpatient clinic, does the nurse advise you on strategies to alleviate your symptoms? |
0.04 | 0.03 | 4.82 | <0.01** |
|
Transcendent Orientation |
Geographical area Heard about in the media Heard at School Have you ever received home health education? Autonomy |
0.07 | 0.05 | 3.38 | <0.01** |
| Positive attitude | Heard at School |
0.0004 | -0.004 | 0.09 | 0.761 |
| Social Support | Heard at School Have you ever received home health education? Autonomy |
0.05 | 0.04 | 3.9 | <0.01** |
|
Problem Orientation |
Age Heard at School Sentito parlare da Amici Have you ever received home health education? Autonomy |
0.03 | 0.01 | 1.58 | 0.168 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



