Submitted:
27 June 2024
Posted:
29 June 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: In Part I of this three-part series we report a retrospective, population-based cohort study assessing rates of adverse events (AEs) in pregnancy after COVID-19 vaccines compared to the same AEs after influenza vaccines and after all other vaccines. Methods: Data were collected from the U.S. Centers for Disease Control and prevention (CDC) and the U.S. Food and Drug Administration (FDA). The CDC/FDA Vaccine Adverse Event Reporting System (VAERS) database was queried from January 1, 1990, to April 26, 2024, for adverse events (AEs) involving pregnancy complications following COVID-19 vaccination. The time-period included 412 months for all vaccines except COVID-19 vaccines, having been used for only 40 of the 412 months (December 1, 2020, to April 26, 2024). Proportional reporting ratios (PRR) by time compared AEs after COVID-19 vaccination to those after influenza vaccination, and after all other vaccine products administered to pregnant women. In cases in which the PRR was not applicable, Chi-square analysis and Fisher’s exact tests were used according to CDC/FDA guidance. CDC/FDA stipulate a safety concern if a PRR is ≥ 2 or if a Chi-square is ≥ 4. Results: The CDC/FDA’s safety signals were breached for all 37 AEs following COVID-19 vaccination in pregnancy: miscarriage, fetal chromosomal abnormality, fetal malformation, cervical insufficiency, premature rupture of membranes, premature labor, premature delivery, placental calcification, placental infarction, placental thrombosis, placenta accreta, placental abruption, placental insufficiency, placental disorder, fetal maternal hemorrhage, fetal growth restriction, reduced amniotic fluid volume, preeclampsia, fetal heart rate abnormality, fetal cardiac disorder, fetal vascular mal-perfusion, fetal arrhythmia, fetal distress, fetal biophysical profile abnormal, hemorrhage in pregnancy, fetal cardiac arrest, fetal death (stillbirth), premature infant death, neonatal asphyxia, neonatal dyspnea, neonatal infection, neonatal hemorrhage, insufficient breast milk, neonatal pneumonia, neonatal respiratory distress, neonatal respiratory distress syndrome, and neonatal seizure. All p values were ≤ 0.001 with the majority being <0.000001. Summary statistics for the deviation from the CDC/FDA safety signals mean (n, range) are as follows: PRR 69.3 (46, 5.37 - 499); z statistic 9.64 (46, 3.29 - 27.0); and Chi-square was 74.7 (26, 28.9 - 148). Conclusions: We found unacceptably high breaches in safety signals for 37 AEs after COVID-19 vaccination in pregnant women. An immediate global moratorium on COVID-19 vaccination during pregnancy is warranted. The United States government, medical organizations, hospitals, and pharmaceutical companies have misled and/or deceived the public regarding the safety of COVID-19 vaccination in pregnancy. Promotion of these products must be immediately halted.
Keywords:
COVID-19 Vaccines
; Pregnancy Complications
; Cervical Insufficiency
; Miscarriage
; Stillbirth
; Preterm Delivery
; Preeclampsia
; Fetal Growth Restriction
; Fetal Malformations
; Premature Newborn Death
; Newborn Complications
Introduction
The “Golden Rule of pregnancy” has remained unchanged throughout millennia: Novel and/or potentially harmful substances are never used when new human life is being formed and nurtured within the womb. Even foods and beverages normally considered safe for most people are ill-advised during pregnancy such as unpasteurized milk, fermented foods (such as kombucha, yogurt, and certain cheeses), as well as some preparations and types of fish. Experts agree that small amounts of alcohol could potentially cause harm to the developing embryo and fetus and should therefore be avoided in pregnancy. The foregoing list is hardly exhaustive. Many other foods and beverages are avoided during pregnancy for the same reason – they have the potential to cause harm during pregnancy.
The Golden Rule of pregnancy was emblazoned on the collective consciousness of the global community after the thalidomide and diethylstilbestrol (DES) pregnancy disasters of the 20th century. Novel and untested medical interventions introduced during any stage of pregnancy are avoided, due to their high potential to cause short and long-term multigenerational harms that may not be discoverable for years or even decades. The thalidomide and DES disasters demonstrate how easily delicate and intricate processes in the developing embryo/fetus can be catastrophically damaged when a novel teratogenic agent is given during pregnancy. During the vulnerable embryonic stage, the intricate blueprint for a new human life is created, including formation of all major systems and structures. During the fetal development stage, critical growth and development of all the major organ systems takes place. Because of the graphic nature of severe birth defects caused by thalidomide, it is perhaps better remembered than DES. Yet thalidomide (which we discuss in part II) caused far less morbidity and mortality in pregnancy than did DES.
DES was widely prescribed to pregnant women for several decades with as many as 10 million exposed globally [1]. All physicians, especially obstetricians, know that DES was associated with cervical malformations in the daughters exposed in-utero. This tragically resulted in infertility, recurrent pregnancy loss, ectopic pregnancy, miscarriage, cervical insufficiency, preeclampsia, premature delivery, stillbirth, and neonatal death [2].
Ironically, the pharmaceutical industry marketed DES in pregnancy as a novel method to avoid pregnancy loss. Yet DES also caused clear cell adenocarcinoma of the cervix, vagina, and breast cancer [2]. DES complications were multigenerational and not limited to reproductive disasters in women. DES caused multiple complications in both sexes including autoimmune disease, neurodevelopmental alterations, psychosexual disorders, depression, immunologic complications, pancreatic disorders, early menopause, and cardiovascular problems [1,2]. Epigenetic alterations have been detected, and generational effects are observed in both DES daughters/sons, and DES granddaughters/grandsons [1,2]. As the data in this study demonstrates, the carnage caused by DES was unrivaled in history until administration of COVID-19 vaccines during pregnancy. The sheer volume of adverse event data following COVID-19 vaccination in pregnancy published even before this study moreover points toward the possibility (if not probability) of long-term, multigenerational harms.
The purpose of Part I presented here is to assess the effects of COVID-19 vaccines on pregnancy outcomes through the Vaccine Adverse Event Reporting System (VAERS) database. VAERS is a national early warning system for vaccine safety established in 1990 as an outgrowth of the National Childhood Vaccine Injury Act signed into law in 1986 [3]. VAERS is co-managed by the U.S. Centers for Disease Control and Prevention (CDC) and the U.S. Food and Drug Administration (FDA).
Methods
MedAlerts [4] is one of only two long-standing platforms used to query the CDC/FDA VAERS database. The study period was from January 1, 1990, through April 26, 2024, and this includes 412 months for all vaccines except for COVID-19 vaccines that were used only 40 months (December 1, 2020 to April 26, 2024).
The first column of Table 1 lists 37 pregnancy complications investigated. The second column of Table 1 shows the exact MedAlert’s “symptom(s)” used to investigate each of the 37 AEs in pregnancy. It is noteworthy that the CDC/FDA VAERS database lists AEs by British rather than American spelling.
MedAlerts “symptoms” involved complications of pregnancy and newborns including those specific symptoms listed under “abortion…”, “amniotic…”, “foetal…”, “neonatal…”, “placental…”, and “premature…”. Diagnoses having an AE with < 3 cases in the COVID-19 vaccine group were excluded. Proportional reporting ratios (PRR) calculated by time as previously validated [5] and were used in accordance with the CDC/FDA Vaccine Adverse Event Reporting System (VAERS) “Standard Operating Procedures” for COVID-19 and as previously validated. The CDC/FDA consider a PRR ≥ 2 or a Chi-square ≥ 4 to be a safety concern as outlined on page 15 of this document [6].
A recent publication analyzing the VAERS database used PRR based on three different variables: AE per time, AE per inoculation, and AE per individual vaccinated [5]. This publication [5] utilized Poisson distribution for a disproportionality analysis by time, by vaccination dose, and by person vaccinated and used a Poisson E-test to compute the p-value. Denominators for COVID-19 vaccinations and number of individuals vaccinated were obtained from Our World in Data [7]. Denominators for influenza vaccinations and numbers of individuals vaccinated were obtained using historical data combined with Monte Carlo simulation modeling. These extensive time/space consuming analyses were not necessary to repeat in this study since the AE/per time was validated by AE/dose and by AE/person vaccinated [5]. When there was a zero in the raw database (Table 1) the PRR is not applicable, and Fisher’s exact test and Chi-square analysis were performed instead. Standard statistical methods were used including PRRs and 95% confidence intervals, Fisher’s exact test, Chi-square, and summary statistics as appropriate using MedCalc® version 22.021 [8]. MedCalc® Statistical Software reports p-values as follows: for PRR the lowest p value reported is p < 0.0001 or an exact number if p > 0.0001, and for the Fisher exact test the lowest p value reported is p < 0.000001 (1 in a million) or an exact number if p > 0.000001.
Results
Table 1, Column 3 describes the raw data for each of the 37 AEs expressed as: case numbers in COVID-19 vaccines over 40 months / case numbers in influenza vaccines over 412 months / case numbers in all vaccines (including influenza) excluding only COVID-19 for 412 months. Table 2 describes the 37 AEs in Column 1, the PRR or Chi-square for COVID-19 vaccines / influenza vaccines in Column 2, and the PRR or Chi-square for COVID-19 vaccines / all other vaccines in Column 3. All 37 AEs in pregnancy far exceed the CDC/FDA safety signal: a PRR of ≥ 2 or a Chi-square of ≥ 4 (Table 2). Summary statistics for the 37 AEs mean (n, range) are as follows: PRR 69.2 (46, 5.37 - 499); z statistic 9.64 (46, 3.29 - 27.0); and Chi-square was 74.7 (26, 28.9 - 148). All p values were ≤ 0.001 with the majority being less than 0.000001 as MedCalc® only reports the lowest p-value for PRR as < 0.0001.
Discussion
Compared to influenza and all other vaccine products, COVID-19 vaccines in pregnancy have demonstrated unacceptable breaches in safety signals across all 37 AEs investigated, 27 antepartum and 10 postpartum/newborn. All 37 AEs breach CDC/FDA limits for safety and are consistent with the authors’ extensive clinical observations. Summary statistics for the deviation of safety signal breaches are described here: mean (n, range) of the PRR was 69.3 (46, 5.37 - 499), z statistic 9.64 (46, 3.29 - 27.0), and Chi-square was 74.7 (26, 28.9 - 148). The magnitude of these safety deviations is unparalleled given the CDC/FDA guidelines defining a PRR ≥ 2 or a Chi-square ≥ 4 as a cause for alarm. The z statistic is informative as it describes the standard deviation of AEs in the COVID-19 vaccines above other vaccines. Most p-values were in the range of one in a million or less.
The scope of the pregnancy complications in this study are of great concern and consistent with the vast obstetrical experience of the authors’ observations. The catastrophic effects of the COVID-19 vaccines in pregnancy are associated with nearly every obstetrical/neonatal complication imaginable. Placental abnormalities also exhibited a substantial breach in safety signals including placental insufficiency, placental calcification, placental infarction, placental thrombosis, placenta accreta, and other placental disorders. The placental abnormalities noted in this study are consistent with clinical observations from sonographers and physicians reviewing ultrasound images prior to birth and are depicted in Figure 1. Figure 1 depicts three separate women’s third trimester fetal ultrasound images documenting classic features observed after administration of COVID-19 vaccines earlier in pregnancy. Many of these findings are consistent with multiple pregnancy adverse events described in this report including placental calcifications, placental insufficiency, placental infarction, placental thrombosis, placenta accreta, placental disorders, reduced amniotic fluid volume, and fetal growth restriction. The placental images demonstrate calcifications (c), lacunae (L), and infarcts (i) as pictured in Figure 1. This present study investigating AEs in pregnancy following COVID-19 vaccination is consistent with two other Pfizer sources [9,10] and two prior FDA/CDC VAERS sources, as discussed below [5,11].
February 28, 2021: Pfizer’s 5.3.6 Post Market Surveillance Analysis Completed
The Pfizer 5.3.6 legally mandated post-market analysis [9] documents COVID-19 vaccines to be the most injurious and lethal medical product ever rolled out with 42,098 casualties (AEs) including 1,223 deaths in just 10 weeks (see page 7) thus documenting an “injure-to-kill” ratio of 33.4. Page 12 of Pfizer’s report [9] documents concerning pregnancy outcome as follows:
- -
- A miscarriage rate of 81% (26/32; 238/270 had no follow-up),
- -
- A five-fold increase in stillbirth rates from an expected rate 5.8/1000 to 31/1000 (1/32 rate),
- -
- An eight-fold increase in neonatal death rate from expected rate of 3.9/1000 to 31/1000 (1/32 rate), and
- -
- A 14% incidence of breast-feeding complications in those newborns whose mothers received the COVID-19 vaccines in pregnancy.
January 12, 2022: The American Board of Obstetrics and Gynecology (ABOG) Put on Notice Regarding the Unacceptable Breaches in VAERS Safety Signals
The American Board of Obstetrics and Gynecology (ABOG) published their “Statement Regarding Dissemination of COVID-19 Misinformation” on September 27, 2021 [14]. A senior constituent and former ABOG examiner personally complained to ABOG’s Executive Director about its unprecedented threats to 60,000 Ob/Gyn physicians, pushing physicians to recommend un-tested, experimental COVID-19 vaccinations in pregnancy. ABOG threatened to remove the licenses and board certifications of this senior board-certified ObGyn and maternal-fetal medicine physician.
In response, this physician compiled an open, public letter to ABOG published on January 12, 2022 [11]. This 98-page open letter to ABOG specifically reviewed the unacceptable breach in VAERS safety signals to the attention of ABOG’s senior officers and examiners. Under a section entitled “The VAERS Data Has Signaled Warnings that Can No Longer be Ignored” on page 12, the letter specifically detailed unprecedented deaths, fetal malformations, and pregnancy losses in the VAERS database. The letter also warned ABOG of multiple other major concerns among others not listed here:
- -
- Lipid nanoparticles (LNPs) were clearly designed to cross “all God-made barriers, including the blood brain barriers, the placental barrier, and the fetal blood brain barriers”,
- -
- LNPs were concentrated in ovaries,
- -
- A female fetus has only about 1 million gametes (ova) and each is exposed to the potentially toxic substances in the LNP’s including vaccine-mRNA,
- -
- Any inflammatory substance such as the COVID-19 vaccine, is dangerous in the developing embryo/fetus and may cause permanent damage, malformation, death, placental insufficiency, and potentially lifelong chronic diseases,
- -
- Disruption of the TOL7 and TOL8 receptors on cell may increase risk to infections and cancers,
- -
- An unprecedented number of stillbirths in the US, Canada, Scotland, Europe and many other locations, and
- -
- Scott Davison the CEO of OneAmerica insurance company has reported all-cause death rates up 40% in ages 18-64 years after the vaccine rollout and that a 10% uptick in all-cause mortality was catastrophic for the insurance industry.
The open letter to ABOG published January 12, 2022 also provided ABOG with references for 1,019 peer-reviewed medical journal publications in just 12 months after COVID-19 vaccines rolled out, documenting severe injuries and death [11]. As of June, 12 2024, 42 months after the COVID-19 vaccine rollout, there are now 3,580 such studies [15]. ABOG never responded to the letter but continued to recertify this physician in 2022 and in 2023.
Concerns were expressed by many regarding the potential of the mRNA-based vaccines to be reversed-transcribed into the human genome, including germ cells of men and women potentially creating a genetic alteration in offspring. As such, this would not just be an epigenetic multigenerational catastrophe as in the case of DES – it could have permanent consequences to the future of the human genome. Why was this not excluded prior to human experimentation? A strong case can be made that pushing novel COVID-19 vaccines in pregnancy is the greatest ethical breach in the history of medicine [16]. The litany of lies forced upon global citizens and concerned health care providers over the course of the pandemic years have been methodically proven false: [17]
- -
- COVID-19 vaccines would never be mandated,
- -
- hydroxychloroquine is unsafe and ineffective,
- -
- ivermectin is unsafe and ineffective,
- -
- there are no safety concerns with the COVID-19 vaccines during pregnancy,
- -
- mRNA from the COVID-vaccines remains localized in the deltoid muscle, and
- -
- mRNA in vaccines could never be reversed transcribed into the human genome.
But alarmingly, Aldén and colleagues demonstrated in February of 2022 that the vaccine mRNA is reverse-transcribed into human liver cells in-vitro [18], and two separate studies in 2022 [19], and 2023 [20], by lead author Hanna and colleagues demonstrated that intact vaccine mRNA is excreted into human breast milk, potentially vaccinating the newborn while breastfeeding.
This foregoing brings heightened urgency to the question of whether COVID-19 mRNA is being reverse-transcribed into the human genome. The American Journal of Obstetrics and Gynecology in early 2024 published an article by Lin and colleagues [21] documenting transplacental transmission of COVID-19 vaccine mRNA across the placenta into fetal blood, which also appears to be bioactive in production of spike protein expression in the placenta and decidua. This finding could potentially explain several of the pregnancy related AEs in this study including many of the placenta-related AEs as reflected in ultrasound images in Figure 1. The bioactivity of the vaccine mRNA in the decidua could also explain, at least in part, menstrual abnormalities and infertility. Lin and colleagues [21] validate the warnings over 2 years ago (January 2022) issued to the American Board of Obstetrics & Gynecology (ABOG) by the dissenting maternal-fetal medicine physician’s open, public letter [11]. Indeed, the lipid nanoparticles were designed to pass through the placenta and enter the fetal blood.
April 2023: VAERS Analysis of AEs in Pregnant and Menstruating Women
In a prior publication Thorp and colleagues [5] compared 18 AEs over 18 months after COVID-19 vaccination to AEs after influenza vaccines occurring over 282 months. This analysis used PRR based on three different variables: AE per time, AE per inoculation, and AE per individual vaccinated [5]. There were 17 obstetrical AEs and 1 AE assessing abnormalities in menstrual function. All 18 AEs documented significant breaches in the CDC/FDA’s safety signal of a PRR ≥ 2 including. The PRRs by time for menstrual abnormalities - 4257; miscarriage - 177; fetal malformation - 21; preeclampsia - 83; preterm delivery - 32.3; low amniotic fluid volume - 17; abnormal fetal surveillance - 83; and stillbirth - 135; all exceeded safety limits. All foregoing AEs had a p value of less than one in a million.
July 2023 Pfizer’s: Randomized, Double-Blind, Placebo Controlled Clinical Trial in Pregnant Women, COVID-19 vaccine versus Placebo
Also consistent with the findings in this present study is Pfizer’s “Randomized, Double-Blind, Placebo Controlled Clinical Trial in Pregnant Women, COVID-19 vaccine versus Placebo” released in July 2023. Pfizer’s phase 2/3 clinical trial, allegedly a randomized, double-blinded, placebo-controlled trial, was grossly underpowered [10]. There were only 324 pregnant women, 161 randomized to COVID-19 vaccines and 163 to placebo, resulting in at least 8 newborn outcomes of grave concern. These included the following:
- 1)
- low Apgar Scores (depressed newborns) increased by 100%;
- 2)
- meconium aspiration syndrome substantially increased;
- 3)
- neonatal jaundice increased by 80%;
- 4)
- congenital malformations increased by 70%;
- 5)
- atrial septal defect increased by 220%;
- 6)
- fetal growth restriction substantially increased;
- 7)
- congenital nevus increased by 200%; and perhaps most concerningly,
- 8)
- congenital anomalies with developmental delays at 6 months of life, increased by 310%.
How many women would have ever considered taking COVID-19 vaccines in pregnancy if their Ob/Gyn physicians informed them of these 8 newborn outcomes from Pfizer’s phase 2/3 clinical trial? It would seem unlikely that any women would have willingly taken the COVID-19 vaccines in pregnancy had they been given honest informed consent required by the Nuremberg Code of Ethics.
Are Any of Pfizer’s “Randomized, Placebo-Controlled, Double Blinded Clinicals Involving COVID-19 Vaccines Valid?
Turtles All The Way Down: Vaccine Science and Myth, a book of over 500 pages with more than 1200 references, states that there has never been a randomized, double-blind, placebo-controlled trial for any of the vaccines currently on the FDA schedule [22]. Published since 2019 no statement of fact in this book has ever been proven false by anyone in the world. All alleged clinical trials conducted by Pfizer and other vaccine manufacturers are not given true placebo groups and otherwise questionable given the corporate kleptocratic entanglement of the pharmaceutical and U.S. governmental complex. Legal claims challenging the integrity and veracity of Pfizer’s clinical trials are pending in state and federal courts. Whistleblower Brook Jackson working for Ventavia Research Group observed gross breach of standard clinical practices in Pfizer’s clinical trials stating that the company falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events reported in Pfizer’s pivotal phase III trial. Jackson’s testimony is detailed in the British Journal of Medicine [23]. Jackson stated that staff who conducted quality control checks were overwhelmed by the volume of problems they were finding. Jackson sued Pfizer in Federal court under the False Claims Act for fraud. Additionally, Pfizer is currently being sued by the Texas Attorney General [24] for violation of the Texas Deceptive Trade Practices Act and by the Kansas Attorney General [25] on multiple counts of misleading consumers. Pfizer and the U.S. government are misleading consumers and the government’s granting of US tax dollars to promote COVID-19 vaccines in many private entities [26] including medical organizations [27], hospitals [28], faith leaders [29], retail pharmacies including CVS and Walgreens [30], is even more concerning.
There are many strengths of this study. Including this report, there are now 5 studies obtained from biased sources all promoting COVID-19 vaccines in pregnancy (CDC/FDA and Pfizer) and yet, they all demonstrate unequivocal breach of safety signals [5,9,10,11]. Despite CDC/FDA’s and Pfizer’s extreme pro-vaccine bias, the government’s and Pfizer’s own data incriminate their positions that COVID-19 vaccination is safe in anyone, let alone the most vulnerable population of pregnant women, preborns and newborns. The continued promotion of COVID-19 vaccination even in the most vulnerable populations of pregnant women, preborns/newborns while making fraudulent claims of safety and efficacy is unjustified by science, by the law, or the ethical principles of the Nuremberg Code. The COVID-19 vaccination promotion needs to be halted immediately with appropriate warning to the global citizens.
In Part II of this series, we focus on how the U.S. Centers for Disease Control and Prevention (CDC) and Food and Drug Administration (FDA) have manipulated and throttled the Vaccine Adverse Event Reporting System (VAERS) and have allowed VAERS to be denigrated in order to move toward closed vaccine surveillance systems including V-safe, Vaccine Safety Datalink (VSD) system, and the and Biologics Effectiveness and Safety (BEST) system. We will also explore how the tentacles of government corruption pushed COVID-19 vaccination in pregnancy through the New England Journal of Medicine.
In Part III of this series, we will critically review all the published studies involving COVID-19 vaccinations in pregnancy.
Funding
No funding.
Conflicts of Interest
All the authors declare none.
Acknowledgements
The authors appreciate and are grateful for the assistance of others: Dr. Michael Deskevich PhD for his guidance and assistance with our mathematical modelling and statistical analysis, and his thoughtful review and editing. Dr. Stewart Tankersley for his thoughtful review and editing. Claire Rogers PA-C for her thoughtful review and editing. Kirstin Cosgrove for her review and editing.
References
- Zamora-Leon p. Are the Effects of DES Over? A Tragic Lesson from the past. Int J Environ Res public Health 2021 Oct, 18(19): 10309. published online 2021 Sept 30. https://www.ncbi.nlm.nih.gov/pmc/articles/pMC8507770/ (Accessed 6/25/2024).
- NIH National Cancer Institute. Diethylstilbestrol (DES) Exposure and Cancer. https://www.cancer.gov/about-cancer/causes-prevention/risk/hormones/des-fact-sheet (Accessed 6/25/2024).
- VAERS Vaccine Adverse Event Reporting System. https://vaers.hhs.gov/about.html (Accessed 6/25/2024).
- National Vaccine Information Center. Search the U.S. Government’s VAERS Data. MedAlerts.org. https://medalerts.org/index.php. (Accessed 6/25/2024).
- Thorp JA, Rogers C, Deskevich M, Tankersley S, Benavides A, Redshaw MD, McCullough PA. Covid-19 Vaccines: The Impact on pregnancy Outcomes and Menstrual Function. Journal of American physicians and Surgeons. https://www.jpands.org/vol28no1/thorp.pdf (Accessed 6/25/2024).
- CDC VAERS Team. Vaccine Adverse Event Reporting System (VAERS) Standard Operating procedures for Covid-19. February 2, 2022. See page 15 of the following document. https://www.cdc.gov/vaccinesafety/pdf/VAERS-COVID19-SOp-02-02-2022-508.pdf. (Accessed 6/25/2024).
- Our World in Data. Coronavirus (COVID-19) Vaccinations. https://ourworldindata.org/covid-vaccinations (Accessed 6/25/2024).
- MedCalc® Statistical Software version 22.021. MedCalc Software Ltd, Ostend, Belgium; 2024. https://www.medcalc.org (Accessed 6/25/2024).
- BNT162b2 5.3.6 Cumulative Analysis of post-authorization Adverse Event Reports. https://phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf (Accessed 6/25/2024).
- Pfizer phase 2/3 clinical trial. Study NCT04754594 to Evaluate the Safety, Tolerability, and Immunogenicity of BNT162b2 Against Covid-19 in Healthy pregnant Women 18 Years of Age and Older. Submitted Date: July, 14, 2023 (v21). Study Start date February 16, 2021 and Study Completion date: July 15, 2022. https://classic.clinicaltrials.gov/ct2/history/NCT04754594?V_21&embedded=true (Accessed 6/25/2024).
- Thorp JA. Open Letter to the American Board of Obstetrics and Gynecology (ABOG) on VAERS analytics and the Risks of the Covid-19 Vaccine in pregnancy. January 12, 2022. https://www.rodefshalom613.org/2022/01/dr-james-thorp-letter-to-american-board-obstetrics-gynecology-risk-covid19-vaccine-pregnancy/ (Accessed 6/25/2024).
- Celia Farber. Court-Ordered Pfizer Documents They Tried To Have Sealed For 55 years Show 1223 Deaths, 158,000 Adverse Events in 90 Days post EUA Release. The Most Shocking Document Release Of The Last 100 years. December 5, 2021. https://celiafarber.substack.com/p/court-ordered-pfizer-documents-they (Accessed 6/25/2024).
- Michelle Maluske. CTV News. ‘Data is power’: Experts weigh-in on court-ordered release of Pfizer vaccine documents. March 11, 2022. https://windsor.ctvnews.ca/data-is-power-experts-weigh-in-on-court-ordered-release-of-pfizer-vaccine-documents-1.5816089 (Accessed 6/25/2024).
- ABOG. American Board of Obstetrics and & Gynecology. Statement Regarding Dissemination of COVID-19 Misinformation. September 27, 2021. https://www.abog.org/about-abog/news-announcements/2021/09/27/statement-regarding-dissemination-of-covid-19-misinformation (Accessed 6/25/2024).
- React19. Science-based support for people suffering from long-term COVID-19 vaccine effects. June 14, 2024. https://react19.org/ (Accessed 6/25/2024).
- Thorp MM, Thorp JA. Pushing COVID-19 Shots in Pregnancy: The Greatest Ethical Breach in the History of Medicine. America Out Loud. February 12, 2023. https://www.americaoutloud.news/pushing-covid-19-shots-in-pregnancy-the-greatest-ethical-breach-in-the-history-of-medicine/ (Accessed 6/25/2024).
- Thorp MM, Thorp JA. A call for Immediate Moratorium on the use of COVID-19 Vaccines in pregnant women. America Out Loud. March 3, 2024. https://www.americaoutloud.news/a-call-for-immediate-moratorium-on-the-use-of-covid-19-vaccines-in-pregnant-women/ (Accessed 6/25/2024).
- Aldén M, Olofsson Falla F, Yang D, Barghouth M, Luan C, Rasmussen M, De Marinis Y. Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Curr Issues Mol Biol. 2022 Feb 25;44(3):1115-1126. https://pubmed.ncbi.nlm.nih.gov/35723296/ (Accessed 6/25/2024). [CrossRef] [PubMed]
- Hanna N, Heffes-Doon A, Lin X, Manzano De Mejia C, Botros B, Gurzenda E, et al. Detection of Messenger RNA COVID-19 Vaccines in Human Breast Milk. JAMA Pediatr. 2022 Dec 1;176(12):1268-1270. Erratum in: JAMA Pediatr. 2022 Nov 1;176(11):1154. https://pubmed.ncbi.nlm.nih.gov/36156636/ (Accessed 6/25/2024). [CrossRef] [PubMed]
- Hanna N, De Mejia CM, Heffes-Doon A, Lin X, Botros B, Gurzenda E, Clauss-Pascarelli C, Nayak A. Biodistribution of mRNA COVID-19 vaccines in human breast milk. EBioMedicine. 2023 Oct;96:104800. Epub 2023 Sep 19. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10514401/ (Accessed 6/25/2024). [CrossRef] [PubMed]
- Lin X, Botros B, Hanna M, Gurzenda E, Manzano De Mejia C, Chavez M, Hanna N, “Transplacental transmission of the COVID-19 vaccine messenger RNA: evidence from placental, maternal and cord blood analyses postvaccination”, American Journal of Obstetrics and Gynecology (2024), https://www.ajog.org/article/S0002-9378(24)00063-2/fulltext (Accessed 6/24/2025). [CrossRef]
- Authored by Two Anonymous Israeli Scientists published in 2019. Re-published Turtles All The Way Down: Vaccine Science and Myth. Forward Mary Holland, Edited by Zoey O’Toole and Mary Holland. https://drive.google.com/file/d/16qHPe0odDOweuCDlwIEjarF4Aiu7oyM9/view (Accessed 6/25/2024).
- Thacker PD. Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ 2021; 375. (published 02 November 2021). 2021,375:n2635. https://www.bmj.com/content/375/bmj.n2635 (Accessed 6/25/2024). [CrossRef]
- Ken Paxton Attorney General of Texas. Attorney General Ken paxton Sues Pfizer for Misrepresenting COVID-19 Vaccine Efficacy and Conspiring to Censor public Discourse. November 30, 2023. https://www.texasattorneygeneral.gov/news/releases/attorney-general-ken-paxton-sues-pfizer-misrepresenting-covid-19-vaccine-efficacy-and-conspiring (Accessed 6/25/2024).
- Fleetwood J. Substack. Kansas Attorney General Sues Pfizer for ‘Misleading Claims It Made Related to the COVID Vaccine’ (Video). “Pfizer made multiple misleading statements to deceive the public about its vaccine at a time when Americans needed the truth,” AG Kobach’s office said. 6/15/2024 Pfizer Complaint attached. June 17, 2024. https://jonfleetwood.substack.com/p/kansas-attorney-general-sues-pfizer (Accessed 6/25/2024).
- Thorp MM, Thorp JA. Tentacles of a Covert and Exploitative Propaganda Machine Compliments of the US Government. America Out Loud. October 28, 2022. https://www.americaoutloud.news/tentacles-of-a-covert-and-exploitative-propaganda-machine-compliments-of-the-us-government/ (Accessed 6/25/2024).
- Thorp MM, Thorp JA. FOIA Reveals Troubling Relationship between HHS/CDC & the American College of Obstetricians and Gynecologists. America Out Loud. May 7, 2023. https://www.americaoutloud.news/foia-reveals-troubling-relationship-between-hhs-cdc-the-american-college-of-obstetricians-and-gynecologists/ (Accessed 6/25/2024).
- Thorp MM, Thorp JA. COVID-19 Government Relief Funds Turned the Healthcare Industry on Its Head. America Out Loud. December 10, 2023. https://www.americaoutloud.news/covid-19-government-relief-funds-turned-the-healthcare-industry-on-its-head/ (Accessed 6/25/2024).
- Thorp MM, Thorp JA. US Government coerced leaders of faith to push COVID-19 vaccines on Americans. America Out Loud. January 14, 2024. https://www.americaoutloud.news/us-government-coerced-leaders-of-faith-to-push-covid-19-vaccines-on-americans/ (Accessed 6/25/2024).
- Thorp MM, Thorp JA. The Government Cartel paid billions to Walgreens and CVS not to fill Ivermectin – the question is why.. America Out Loud. May 20, 2024. https://www.americaoutloud.news/the-government-cartel-paid-billions-to-walgreens-and-cvs-not-to-fill-ivermectin-the-question-is-why/ (Accessed 6/25/2024).
Figure 1.
Depicted are three separate pregnant women’s ultrasound images in the third trimester documenting the classic features that have been noted after COVID-19 vaccines administered during pregnancy. Many of these findings are consistent with the multiple pregnancy adverse events related to COVID-19 vaccines in pregnancy in this report including placental calcifications, placental insufficiency, placental infarction, placental thrombosis, placental accreta, placental disorders, reduced amniotic fluid volume, and fetal growth restriction. The images represent calcifications (c), lacunae (L), and infarcts (i).
Figure 1.
Depicted are three separate pregnant women’s ultrasound images in the third trimester documenting the classic features that have been noted after COVID-19 vaccines administered during pregnancy. Many of these findings are consistent with the multiple pregnancy adverse events related to COVID-19 vaccines in pregnancy in this report including placental calcifications, placental insufficiency, placental infarction, placental thrombosis, placental accreta, placental disorders, reduced amniotic fluid volume, and fetal growth restriction. The images represent calcifications (c), lacunae (L), and infarcts (i).
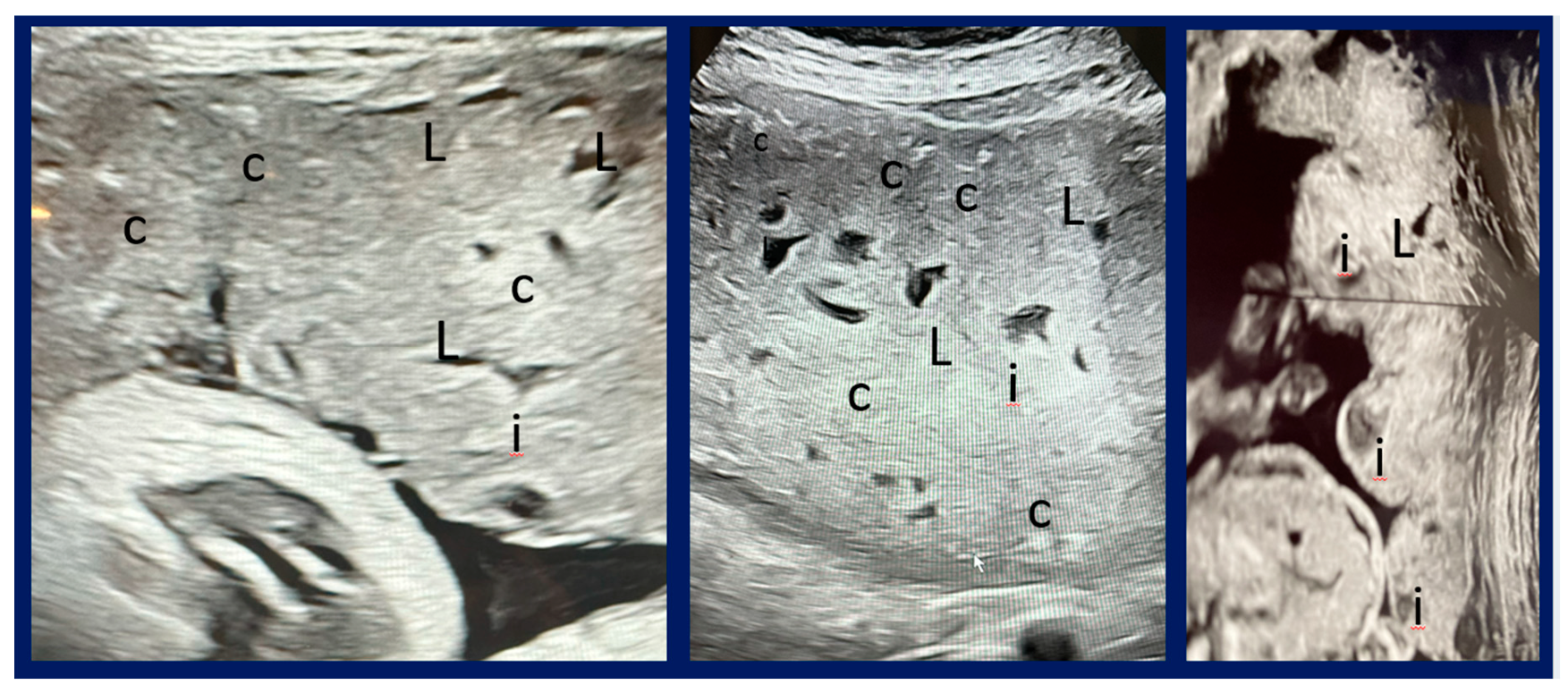

Table 1.
Thirty-seven pregnancy-related adverse events (AEs) were investigated in this study, 27 were antepartum AEs and 10 were postpartum/newborn AEs. The AEs are depicted in Column 1 and the actual MedAlert’s “symptoms” extracted are listed in Column 2. Noteworthy is that the U.S. CDC/FDA VAERS lists these complications in British spelling. Column 3 lists the raw data of AEs depicted as follows: COVID-19 vaccines / influenza vaccines / All other vaccines except COVID-19.
Table 1.
Thirty-seven pregnancy-related adverse events (AEs) were investigated in this study, 27 were antepartum AEs and 10 were postpartum/newborn AEs. The AEs are depicted in Column 1 and the actual MedAlert’s “symptoms” extracted are listed in Column 2. Noteworthy is that the U.S. CDC/FDA VAERS lists these complications in British spelling. Column 3 lists the raw data of AEs depicted as follows: COVID-19 vaccines / influenza vaccines / All other vaccines except COVID-19.
| Adverse Event | MedAlerts “Symptoms” Utilized | Adverse Events Raw Data Expressed as COVID-19 Vaccines / Influenza Vaccines / All Other Vaccines |
|---|---|---|
| Miscarriage (spontaneous abortion) | “abortion missed” or “abortion spontaneous” or “abortion spontaneous complete” or “abortion spontaneous complicated” or “abortion spontaneous incomplete” | 3494 / 315 / 936 |
| Fetal chromosome abnormality | “foetal chromosome abnormality” | 17 / 0 / 2 |
| Fetal malformation | “foetal cystic hygroma” or “foetal malformation” or “foetal megacystis” | 40 / 2 / 8 |
| Cervical insufficiency | “cervical incompetence” | 10 / 2 / 9 |
| Premature rupture of membranes | “premature rupture of membranes” | 114 / 14 / 53 |
| Premature labor | “premature labour” | 189 / 53 / 223 |
| Premature delivery | “premature baby” or “premature delivery” |
404 / 142 / 356 |
| Placental calcification | “placental calcification” | 5 / 0 /2 |
| Placental infarction | “placental infarction” | 8 / 0 / 2 |
| Placental thrombosis | “foetal placental thrombosis” | 6 / 0 / 0 |
| Placenta accreta | “placenta accreta” | 3 / 0 / 0 |
| Placental abruption | “premature separation of placenta” | 90 / 14 / 44 |
| Placental insufficiency | “placental insufficiency” | 24 / 0 / 2 |
| Placental disorder | “placental disorder” | 41 / 17 / 55 |
| Fetal-maternal hemorrhage | “foetal maternal hemorrhage” | 7 / 1 / 1 |
| Fetal growth restriction | “foetal growth abnormality” | 21 / 0 / 1 |
| Reduced amniotic fluid volume | “amniotic fluid index decreased” or “amniotic fluid volume decreased” | 17 / 1 / 11 |
| Preeclampsia | “pre-eclampsia” | 147 / 26 / 96 |
| Fetal heart rate abnormality | “foetal heart rate abnormal” or “foetal heart rate acceleration abnormal” or “foetal heart rate deceleration” or “foetal heart rate deceleration abnormal” or “foetal heart rate decreased” or “foetal heart rate disorder” or “foetal heart rate increased” or “foetal heart rate indeterminate” | 228 / 48 / 94 |
| Fetal cardiac disorder | “foetal cardiac disorder” | 22 / 4 / 8 |
| Fetal vascular malperfusion | “foetal vascular malperfusion | 19 / 0 / 0 |
| Fetal arrhythmia | “foetal arrhythmia” | 10 / 0 / 0 |
| Fetal distress | “foetal distress syndrome” | 18 / 6 / 27 |
| Fetal biophysical profile abnormal | “foetal biophysical profile abnormal” | 4 / 0 / 0 |
| Hemorrhage in pregnancy | “haemorrhage in pregnancy” | 164 / 7 / 25 |
| Fetal cardiac arrest | “foetal cardiac arrest” | 21 / 2 / 2 |
| Fetal death (Stillbirth)* | “foetal death” or “stillbirth” | 477 / 68 / 175 |
| Premature infant death | “premature baby death” | 12 / 0 / 1 |
| Neonatal asphyxia | “neonatal asphyxia” | 8 / 0 / 3 |
| Neonatal dyspnea | “neonatal dyspnea” | 13 / 0 / 1 |
| Neonatal infection | “neonatal infection” | 5 / 0 / 4 |
| Neonatal hemorrage | “haemorrhage neonatal” | 4 / 0 / 0 |
| Neonatal insufficient breast milk | “neonatal insufficient breast milk” | 10 / 0 / 0 |
| Neonatal pneumonia | “neonatal pneumonia” | 4 / 0 / 1 |
| Neonatal respiratory distress | “neonatal respiratory distress” | 12 / 0 / 7 |
| Neonatal respiratory distress syndrome | “neonatal respiratory distress syndrome” | 12 / 0 / 23 |
| Neonatal seizure | “neonatal seizure” | 7 / 0 / 6 |
Table 2.
Thirty-seven pregnancy-related adverse events (AEs), 27 antepartum AEs and 10 postpartum/newborn AEs, associated with COVID-19 vaccines over 40 months are compared to those after influenza vaccines, and those after all other vaccines (except COVID-19) over 412 months. A proportional reporting ratio (PRR) with 95% confidence intervals are depicted where appropriate. Fisher Exact and Chi-square analysis were used when PRR was not applicable in the cases where there were zero AEs in the comparison groups. FDA uses a breach of safety signal as a PRR of ≥ 2 and a Chi-square ≥ 4.
Table 2.
Thirty-seven pregnancy-related adverse events (AEs), 27 antepartum AEs and 10 postpartum/newborn AEs, associated with COVID-19 vaccines over 40 months are compared to those after influenza vaccines, and those after all other vaccines (except COVID-19) over 412 months. A proportional reporting ratio (PRR) with 95% confidence intervals are depicted where appropriate. Fisher Exact and Chi-square analysis were used when PRR was not applicable in the cases where there were zero AEs in the comparison groups. FDA uses a breach of safety signal as a PRR of ≥ 2 and a Chi-square ≥ 4.
| Adverse Event (AE) | COVID-19 Vaccines Over 40 Months vs Influenza Vaccines Over 412 Months | COVID-19 Vaccines Over 40 Months vs All Other Vaccines Over 412 Months |
|---|---|---|
| Miscarriage | PRR 114 95% CI 81.0 - 161 p < 0.0001, z statistic 27.0 |
PRR 38.4 95% CI 27.6 – 53.6 p < 0.0001, z statistic 21.5 |
| Fetal chromosome abnormality | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 127 |
PRR 87.6 95% CI: 19.5 – 393 p < 0.0001, z statistic 5.84 |
| Fetal malformation | PRR 206 95% CI: 48.0 – 884 p < 0.0001, z statistic 7.17 |
PRR 51.5 95% CI: 22.6 – 118 p < 0.0001, z statistic 9.36 |
| Cervical insufficiency | PRR 51.5 95% CI 10.9 - 243 p < 0.0001, z statistic 4.98 |
PRR 11.4 4.39 – 29.8 p < 0.0001, z statistic 4.99 |
| Premature rupture of membranes | PRR 83.9 95% CI: 44.1 – 160 p < 0.0001, z statistic 13.5 |
PRR 22.2 95% CI: 14.0 – 35.1 p < 0.0001, z statistic 13.2 |
| Premature labor | PRR 36.7 95% CI: 23.5 – 57.3 p < 0.0001, z statistic 15.9 |
PRR 8.73 95% CI: 5.98 – 11.2 p < 0.0001, z statistic 15.9 |
| Premature delivery | PRR 29.3 95% CI: 20.1 – 42.7 p < 0.0001, z statistic 17.6 |
PRR 11.7 95% CI 8.20 – 16.7 p < 0.0001, z statistic 13.6 |
| Placental calcification | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p = 0.000008 Chi-square 46.2 |
PRR 25.8 95% CI 4.84 – 137 p < 0.0001, z statistic 3.81 |
| Placental infarction | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 69.7 |
PRR 173 95% CI 9.81 – 3060 p = 0.0004, z statistic 3.52 |
| Placental thrombosis | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p = 0.000001 Chi-square 54.3 |
Significantly increased in COVID-19 vs All Other Vaccines Fishers Exact p = 0.000001 Chi-square 54.3 |
| Placenta accreta | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p = 0.00079 Chi-square 28.9 |
Significantly increased in COVID-19 vs All Other Vaccines Fishers Exact p = 0.00079 Chi-square 28.9 |
| Placental abruption | PRR 66.2 95% CI: 34.6 – 127 p < 0.0001, z statistic 12.6 |
PRR 21.1 95% CI: 13.0 – 34.2 p < 0.0001, z statistic 12.3 |
| Placental insufficiency | PRR 499 95% CI: 29.8 – 8360 p < 0.0001, z statistic 4.32 |
Significantly increased in COVID-19 vs All Other Vaccines Fishers Exact p < 0.000001 Chi-square 147 |
| Placental disorder | PRR 24.8 95% CI: 12.9 – 47.7 p < 0.0001, z statistic 9.7 |
PRR 18.1 95% CI: 9.61 – 34.0 p < 0.0001, z statistic 8.98 |
| Fetal-maternal hemorrhage | PRR 72.1 95% CI: 8.65 – 601 p < 0.0001, z statistic 3.96 |
PRR 72.1 95% CI: 8.65 – 601 p < 0.0001, z statistic 3.96 |
| Fetal growth restriction | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 148 |
Significantly increased in COVID-19 vs All Other Vaccines Fishers Exact p < 0.000001 Chi-square 140 |
| Reduced amniotic fluid volume | PRR 175 95% CI: 22.7 – 1350 p < 0.0001, z statistic 4.96 |
PRR 15.9 95% CI: 6.98 – 36.3 p < 0.0001, z statistic 6.58 |
| Preeclampsia | PRR 58.2 95% CI: 34.3 – 98.8 p < 0.0001, z statistic 15.1 |
PRR 15.8 95% CI: 10.4 – 23.9 p < 0.0001, z statistic 13.0 |
| Fetal heart rate abnormality | PRR 48.9 95% CI: 31.2 – 76.7 p < 0.0001, z statistic 17.0 |
PRR 25.0 95% CI: 16.7 – 37.4 p < 0.0001, z statistic 15.6 |
| Fetal cardiac disorder | PRR 56.7 95% CI: 18.6 – 173 p < 0.0001, z statistic 7.10 |
PRR 28.3 95% CI: 11.8 – 67.7 p < 0.0001, z statistic 7.52 |
| Fetal vascular malperfusion | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 148 |
Significantly increased in COVID-19 vs All Other Vaccines Fishers Exact p < 0.000001 Chi-square 140 |
| Fetal arrhythmia | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 84.0 |
Significantly increased in COVID-19 vs All Other Vaccines Fishers Exact p < 0.000001 Chi-square 84.0 |
| Fetal distress | PRR 30.9 95% CI: 11.6 – 82.3 p < 0.0001, z statistic 6.87 |
PRR 6.87 95% CI: 3.48 – 13.5 p < 0.0001, z statistic 5.56 |
| Fetal biophysical profile abnormal | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p 0.000076 Chi-square 37.7 |
Significantly increased in COVID-19 vs All Other Vaccines Fishers Exact p < 0.000076 Chi-square 37.7 |
| Fetal cardiac arrest | PRR 108 95% CI: 24.5 – 478 p < 0.0001, z statistic 6.18 |
PRR 108 95% CI: 24.5 – 478 p < 0.0001, z statistic 6.18 |
| Hemorrhage in pregnancy | PRR 241 106 – 550 p < 0.0001, z statistic 13.1 |
PRR 67.6 39.7 – 115 p < 0.0001, z statistic 15.5 |
| Fetal death (stillbirth) | PRR 72.3 95% CI: 47.8 – 109 p < 0.0001, z statistic 20.4 |
PRR 28.1 95% CI: 19.4 – 40.6 p < 0.0001, z statistic 13.0 |
| Prematue infant death | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 97.4 |
PRR 124 95% CI: 15.7 – 975 p < 0.0001, z statistic 4.57 |
| Neonatal asphyxia | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.0001 Chi-square 69.7 |
PRR 27.5 95% CI: 7.01 – 108 p < 0.0001, z statistic 4.75 |
| Neonatal dyspnea | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 104 |
PRR 134 95% CI: 17.1 – 1050 p < 0.0001, z statistic 4.66 |
| Neonatal infection | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p = 0.000008 Chi-square 46.2 |
PRR 12.9 95% CI: 3.32 – 49.9 p = 0.0002, z statistic 4.66 |
| Neonatal hemorrhage | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p = 0.000076 Chi-square 37.7 |
Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p = 0.000076 Chi-square 37.7 |
| Neonatal insufficient breast milk | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 84.0 |
Significantly increased in COVID-19 vs All Other Vaccines Fishers Exact p < 0.00001 Chi-square 84.0 |
| Neonatal pneumonia | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p = 0.000076 Chi-square 37.7 |
PRR 41.2 95% CI: 4.50 – 378 p = 0.0010, z statistic 3.29 |
| Neonatal respiratory distress | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p = 0.000080 Chi-square 97.4 |
PRR 17.7 95% CI: 6.58 – 47.4 p = 0.0010, z statistic 5.70 |
| Neonatal respiratory distress syndrome | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 97.4 |
PRR 5.37 95% CI: 2.49 – 11.6 p = 0.0010, z statistic 4.28 |
| Neonatal seizure | Significantly increased in COVID-19 vs influenza Vaccines Fishers Exact p < 0.000001 Chi-square 62.2 |
PRR 12.0 95% CI: 3.85 – 37.5 p = 0.0010, z statistic 4.28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



