
Submitted:
28 June 2024
Posted:
01 July 2024
You are already at the latest version
Abstract
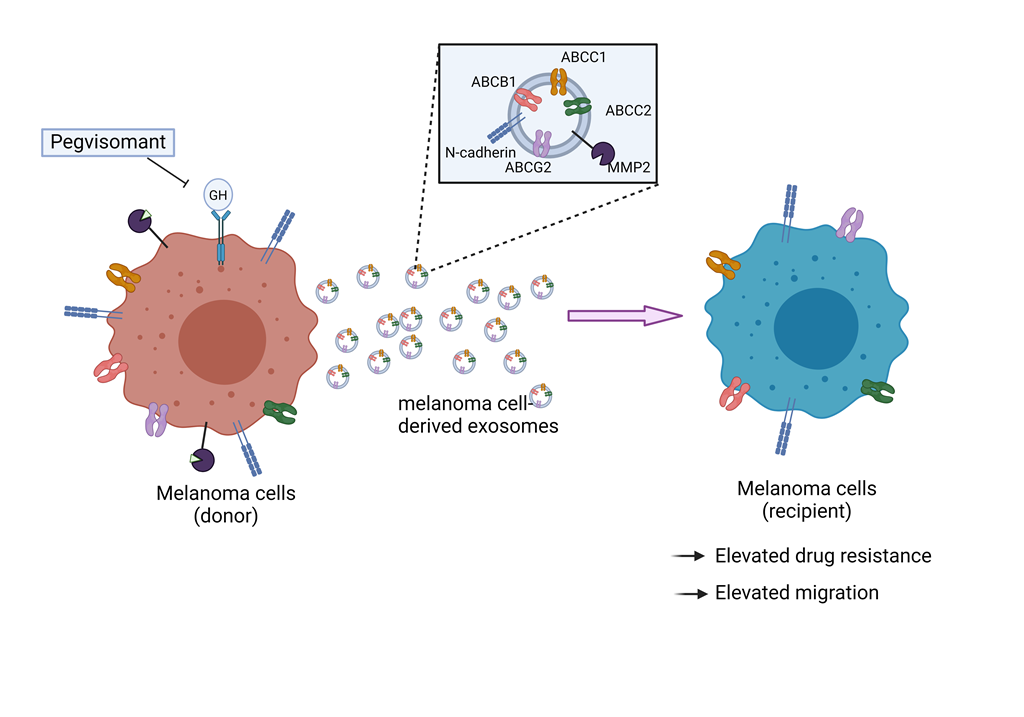
Drug resistance in melanoma is a major hindrance in cancer therapy. Growth hormone (GH) plays a pivotal role in contributing to resistance to chemotherapy. Knocking down or blocking the GH receptor has been shown to sensitize the tumor cells to chemotherapy. Extensive studies have demonstrated that exosomes, a subset of extracellular vesicles, play an important role in drug resistance by transferring key factors to sensitize cancer cells to chemotherapy. In this study, we explore how GH modulates exosomal cargoes from melanoma cells and their role in drug resistance. We treated the melanoma cells with GH, doxorubicin, and GHR antagonist, pegvisomant, and analyzed the exosomes released. Additionally, we administered these exosomes to recipient cells. The GH-treated melanoma cells released exosomes with elevated levels of ABC transporters (ABCC1 and ABCB1), N-cadherin and MMP2, enhancing drug resistance and migration in recipient cells. GHR antagonism reduced these exosomal levels, restoring drug sensitivity and attenuating migration. Overall, our findings highlight a novel role of GH in modulating exosomal cargoes that drive chemoresistance and metastasis in melanoma. This understanding provides insights to the mechanisms of GH in melanoma chemoresistance and suggests GHR antagonism as a potential therapy to overcome chemoresistance in melanoma treatment.
Keywords:
growth hormone
; exosomes
; melanoma
; chemotherapy resistance
; ABC transporters
; N-cadherin
; MMP2
; pegvisomant
1. Introduction
Melanoma, the most aggressive form of skin cancer, remains a significant public health concern, with the American Cancer Society projecting approximately 100,640 new cases in the US in 2024 [1]. Recent advancements in diagnostic options and therapeutic interventions have raised the five-year overall survival rate to an impressive 99%, but it significantly drops to 35% in advanced stages of the disease. This dismal drop in patient survival is mostly attributed to metastasis and resistance to existing therapies [2]. Understanding the complex mechanisms of tumor metastasis and drug resistance is crucial in developing groundbreaking treatment and improving patient outcomes.
Chemoresistance in melanoma involves multiple factors, including the tumor microenvironment (TME), enhanced drug efflux, and an elevated rate of epithelial to mesenchymal transition (EMT) [3,4,5]. Exosomes, tiny extracellular vesicles (EVs) released from the cells, are being recognized as key players in mediating these processes [6,7,8]. Exosomes are a subset of EVs that range from 50-150 nm in size, serving as vehicles for the transfer of proteins, RNA, and lipids -- collectively referred to as cargo -- from one cell to another [9].
EMT is a fundamental cellular process integral to embryonic development and wound healing, and it plays a crucial role in tumor growth [10]. During EMT, cancer cells lose their epithelial characteristics and acquire enhanced tumor cell motility, facilitating metastasis. Extensive studies have shown that EMT is intrinsically linked to cancer therapy resistance [11,12,13]. The mechanisms include the conversion of tumor cells into tumor stem cells [14], reduced expression of drug carriers essential for drug internalization [13], and the upregulation of EMT-transcription factors by non-coding RNAs [15,16]. Notably, tumor-derived exosomes have been implicated in transfer of drug efflux pumps and EMT markers to sensitive cancer cells, contributing to chemoresistance [17,18,19,20].
Growth hormone (GH), an anterior pituitary hormone, is crucial in regulating longitudinal growth, organ development, whole-body metabolism, as well as diseases like diabetes and cancer [21]. Remarkably, patients with excess GH secretion have increased risk of multiple cancers while patients with no GH action (Laron Syndrome) are protected from all types of cancer [22,23,24]. GH also exerts distinct autocrine and paracrine actions via multiple cells in TME [25,26,27]. Previously, we have identified the expression of GH receptor (GHR) gene in multiple NCI-60 cell lines, with overexpression observed in melanoma [28]. GHR activation of these cells leads to diverse cellular effects including induction of EMT, senescence, upregulation of multidrug efflux transporters, and down regulation of apoptosis [26]. Importantly, we have shown that GH upregulates expression of ATP-binding cassette-containing (ABC) transporters in melanoma and other cancers, which in turn, confers increased resistance to chemotherapy, both in vitro and in vivo [29,30,31,32]. Moreover, we and others have shown crucial roles of GH in induction of EMT in various cancers [33,34,35,36] including melanoma [37,38]. Several of these ABC transporters and EMT markers, mediated directly or indirectly by GH, are shown to be trafficked from drug resistant cancer cells via exosomes conferring drug resistance on the recipient cells [39,40].
Therefore, in the present work we aimed to elucidate the effects of GH on exosomal cargoes from donor cells and their subsequent effects on recipient cells, all contributing to drug resistance. For this, we investigated the influence of GH on drug efflux pumps, EMT markers, and matrix metalloproteinases (MMPs) implicated in tumoral chemoresistance [11,41,42]. Through this investigation we sought to uncover novel insights into molecular mechanism of GH action in driving chemoresistance via melanoma-derived exosomes.
2. Materials and Methods
- Cell culture and treatments: Human melanoma cell lines MALME-3M (HTB-64) and SK-MEL-28 (HTB-72) were obtained from American Type Culture Collection (ATCC, Manassas, VA), while SK-MEL-30 cell line was acquired from Creative Bioarray (Shirley, NY). Cells were grown and maintained in Iscove’s Modified Dulbecco’s Medium (IMDM), Eagle’s Minimum Essential Medium (EMEM), and Rosewell Park Memorial Institute (RPMI), media respectively supplemented with 10% fetal bovine serum (# 10-082-147, Thermo Fisher Scientific, Waltham, MA) and 100 U/ml penicillin-streptomycin (#15-140-22, Thermo Fisher Scientific, Waltham, MA). Cells were grown in a humidified incubator at 37 ˚C and 5% CO2. Recombinant human GH (#ABIN2017921, Antibodies-online, Pottstown, PA) at 50 ng/ml, doxorubicin at EC50 dosage, and Pegvisomant (Somavert, Pfizer) at 500 nM were added in the respective treatment media supplemented with 2% exosome-depleted fetal bovine serum (#EXO-FBS-250A-1, System Biosciences, Palo Alto, CA). The EC50 values were determined as 0.7 µM for Malme-3M, 1.5 µM for SK-MEL-28, and 2.8 µM for SK-MEL-30 (Supplementary Figure S1)
- Exosome isolation: The supernatant of the cell cultures from respective treatments were centrifuged at 3000g for 15 minutes at 4˚C to remove cell debris. Further, the supernatant was passed through the 0.22µm filter (Millipore Sigma, Burlington, MA) to remove relatively large vesicles. To effectively concentrate exosomes from large volumes, ultrafiltration was employed using Amicon Ultra 15 ml centrifugal filters (Millipore Sigma, Burlington, MA) [80]. Next, ExoQuick reagent was added to the supernatant in 1:5 ratio, according to the manufacturer’s instructions (Systems Biosciences, Palo Alto, CA) and incubated overnight at 4˚C with no rotation. Following incubation, the samples were centrifuged at 1,500 g for 30 minutes. The supernatant was aspirated, followed by a brief centrifugation step of 1,500g for 5 minutes to facilitate further removal of supernatant [81]. The final pellet was resuspended in phosphate buffered saline (PBS) for downstream analysis.
- Nanoparticle tracking analysis: Exosome labeling was conducted using EV tracker green NTA labeling kit (Systems Biosciences, Palo Alto, CA). Briefly, the pre-warmed reaction buffer was mixed with ExoGlowTM dye in a proportion of 5:1, and then 5 μl of the working solution was added to 200 μg of sample and then thoroughly mixed by pipetting. The samples were incubated at room temperature for 30 minutes while protected from light. Microscopic analysis was performed with Zetaview (Particle Matrix, Germany), equipped with a 520 nm laser, 550 nm long pass cutoff filter, and an sCOMS camera.
- Protein extraction and western blot: Protein extraction and western blot were performed as described previously [83]. Briefly, protein extraction was preformed using 1X RIPA buffer (#R-0278, Sigma Aldrich, St. Louis, MO) containing 1X HaltTM protease and phosphatase inhibitor cocktail (#78442, Thermo Fisher Scientific, Waltham, MA). Protein concentration was quantified using the Bradford assay (#B6916, Sigma Aldrich, St, Lou) and 30 μg of protein was loaded onto 4-16% gradient SDS-PAGE denaturing gels. Further, the proteins were transferred to the polyvinylidene fluoride membranes, blocked with 5% BSA solution in 1X TBST-T and probed using target specific antibodies. The exosomal markers in protein extracts from Malme-3M exosomes were determined using antibodies specific for CD63, CD9, CD81 (#EXOAB-CD63A-1, #EXOAB-CD9A-1, #EXOAB-CD81A-1 SBI, Palo Alto, CA). To determine the ABC transporters, EMT markers, and MMPs, protein extracts from Malme-3M exosomes were determined using antibodies specific for ABCC1, ABCC2, ABCB1, ABCG2, N-cadherin, E-cadherin, MMP2, MMP9 (#72202, #125595, #13342, #42078, #13116, #3195, #87809, #13667). β-actin (#4970, CST, Denver, MA) was used as a loading control. For detection, anti-rabbit IgG, HRP-linked secondary antibody (#7074, CST, Denver, MA) and SuperSignal West Femto Maximum Sensitivity Substrate (#34095, Thermo Fisher Scientific, Waltham, MA) were used.
- RNA extraction and RT-qPCR: RNA was extracted, and RT-qPCR was performed as previously described [83]. Briefly, total RNA was extracted using IBI Scientific total RNA extraction kit (Dubuque, IA), following manufacturer’s protocol. Up to 2000 ng of complementary DNA (cDNA) was synthesized from isolated exosomal RNA. Further, quantitative real time polymerase chain reaction (qRT-PCR) was performed using Applied Biosystems reagents (Thermo Fisher Scientific, Waltham, MA) following the manufacturer’s protocol. Primers used were GH (Forward: AGGAAACACAACAGAAATCC, Reverse: TTAGGAGGTCATAGACGTTG). The expression levels of differentially expressed RNAs were compared using 2-ΔΔCT method. β-actin (Forward: GACGACATGGAGAAAATCTG, Reverse: ATGATCTGGGTCATCTTCTC) was used as an internal control for the RNA. analysis
- Cell migration assay: Cells were seeded at 30,000 cells per well in 12-well plates. After 24 hours, a scratch wound was made using a 200 µl pipette tip along the midline of each well. Cultures were gently washed with PBS to remove loose cells. The cells were maintained in the respective media with Exocontrol (from PBS treated cells), ExoGH (from GH-treated cells), Exodoxo (from doxorubicin-treated cells), ExoGH+doxo (from cells treated with GH and doxorubicin), and ExoGH+doxo+Peg (from cells treated with GH, doxorubicin, and pegvisomant) for 24 hours. The scratch area was imaged at the start and end of the assay using a BioTek citation-3 microplate imager (Gen5v2.09.2 software) and quantified using ImageJ software. Three individual experiments were performed.
- Drug retention assay: Melanoma cells were treated for 12 hours with Exocontrol, ExoGH, Exodoxo, ExoGH+doxo, and ExoGH+doxo+Peg. On the day of assay, the cells were trypsinised, counted, suspended in cold DiOC2(3) dye on ice for 30 minutes (EMD Millipore, ECM 910). The cells were then centrifuged, supernatant was removed, and cell pellet were resuspended in cold efflux buffer. The resuspended cells were distributed in equal parts with one set serving as control with the other two parts kept at 37˚C water bath for 20 minutes and 60 minutes respectively. The cells were then washed, resuspended, and cells suspension were dispended into the wells of a black-walled 96-well plate, and fluorescence was measured using the fluorescent BioTek citation-3 microplate imager (Gen5v2.09.2 software) at an excitation wavelength of 485 nm and an emission wavelength of 530 nm. Two individual experiments were performed for each cell line.
- Statistical Analysis: For all experiments, analysis was performed by one-way or two-way ANOVA with Tukey’s multiple comparison test using GraphPad Prism 8.0 (GraphPad Software). P < 0.05 was considered statistically significant.
3. Results
3.1. GHR Antagonism Suppresses Melanoma Exosome Mediated Increase in Drug Efflux
The size and concentration quantification of melanoma-derived exosomes demonstrating peak size at 108.5 nm (Supplementary Figure S2A). The identification was further confirmed by exosomal markers CD63, CD9, and CD81 by immunoblotting (Supplementary Figure S2B).
GH has been shown to induce chemoresistance, both in vitro and in vivo, in melanoma [29], hepatocellular carcinoma [32], and pancreatic cancer [43], as shown by our laboratory. Blocking the GHR action attenuates this process, making the tumor cells drug sensitive. Recent studies reveal that drug resistant cancer cells release exosomes which assist drug sensitive cancer cells in acquiring chemoresistance [44,45,46]. To investigate if and how GH affects the transfer of chemoresistance via exosomes, we employed a drug retention assay in recipient melanoma cells.
For this study, we isolated exosomes from three melanoma cells lines: Malme-3M, SK-MEL-28, and SK-MEL30, each treated with the following conditions: either hGH or doxorubicin alone or hGH and doxorubicin, or a combination of hGH, doxorubicin, and pegvisomant (a GHR antagonist) [47,48,49]. The exosomes are referred as Exocontrol (from PBS treated cells), ExoGH (from GH-treated cells), Exodoxo (from doxorubicin-treated cells), ExoGH+doxo (from cells treated with GH and doxorubicin), and ExoGH+doxo+Peg (from cells treated with GH, doxorubicin, and pegvisomant). These exosomes were then administered to treatment-naïve melanoma cells (recipient cells). We then administered DiOC2(3), a surrogate dye for chemotherapy, to conduct the drug retention assay in the recipient cells (Figure 1A). We measured the amount of dye retained as an indicator of chemoresistance observed in the cells receiving the exosomes.
A significantly lower dye retention was observed in Malme-3M cells (by 20%) administrated with ExoGH as compared to control (Figure 1B). Similarly lower, but not significant, dye retention was observed in SK-MEL-28 or SK-MEL-30 as compared to respective controls (Figure 1C,D). Upon administering Exodoxo, a significant decrease in drug retention was observed in Malme-3M (by 10%) and SK-MEL-28 (by 20%) cells as compared to controls. A similar lower drug retention, albeit not significant, dye retention, was observed in all the three cell lines when administered with ExoGH+doxo.
The dye retention levels were rescued to control levels in the three cell lines when administered with ExoGH+dox+Peg (Figure 1B–D). A notable enhancement in drug retention was noted in cells treated with ExoGH+dox+Peg compared to those treated solely with ExoGH. Specifically, Malme-3M and SK-MEL28 cells exhibited a 30% increase in drug retention under this combined treatment regimen (Figure 1B,C). The dye retention was maintained in Malme-3M and exhibited even more pronounced retention (40%) in both SK-MEL-28 and SK-MEL-30 at a later time-point (60 mins), suggesting prolonged and enhanced drug retention.
Addition of GH alone or in combination with doxorubicin induces cells to release exosomes that relay a reduction in drug retention in recipient cells while pegvisomant treatment yields exosomes that elevate drug retention in recipient cells. These results suggest that the addition of GH and pegvisomant to melanoma cells modifies the drug efflux capacity in the recipient cells, mediated through exosomes.
3.2. GH Elevates the Expression of ABC Transporters in Melanoma-Derived Exosomes and in Corresponding Recipient Cells
3.2.1. Effects of GH on ABC Transporters in Melanoma-Derived Exosomes
As GH regulates ABC transporter (efflux pump) expression in tumor cells [31,32,38], we checked the ABC transporter levels within the released exosomes responsible for the modulation of drug retention in recipient cells. These pumps have been characterized and studied as efficient facilitators of drug efflux from cancer cells and correlated with increased chemoresistance. Studies have shown that exosomes transfer multiple ABC transporters, thereby conferring chemoresistance in tumors [39,44]. We specifically examined protein levels of ABCB1, ABCG2, ABCC1, and ABCC2 in exosomes, as they have been reported to contribute to drug resistance activity in association with GH [29,32]. Additionally, we have shown that the protein levels of ABCB1, ABCC1, ABCG2, and ABCC2 are elevated in presence of GH treatment on parent melanoma cells (Malme-3M, SK-MEL-28, and SK-MEL-30) (Supplementary Figure S3).
GH significantly increased the levels of exosomal ABCC1 in Malme-3M, SK-MEL-28, and SK-MEL-30 cells by 5-fold, 2.4-fold and 7.2-fold, respectively, compared to corresponding controls (Figure 2A,B, Table 1). Similarly significant increases were observed in exosomal ABCC1 following doxorubicin treatment in Malme-3M cells (by 5.4-fold) and SK-MEL-28 (by 3.3-fold). Furthermore, a significant increase in exosomal ABCC1 was observed in Malme-3M cells (by 4.9-fold), SK-MEL-28 (by 3.3-fold) following treatment with GH and doxorubicin combination. Importantly, addition of pegvisomant in combination with GH and doxorubicin rescued the exosomal ABCC1 levels back to those of control. More evidently, when compared with GH treatment alone, pegvisomant combination treatment exhibited a significant reduction in exosomal ABCC1 from Malme-3M cells and SK-MEL-30. Similar reductions were observed compared to doxorubicin treatment alone and in combination with GH.
Regarding exosomal ABCB1, GH significantly increased the levels of exosomal ABCB1 from Malme-3M (by 3.2-fold) as compared to control (Figure 2A,D, Table 1), an effect that was also observed following doxorubicin stimulation in Malme-3M cells (by 3.9-fold) as compared to control. Furthermore, combined GH and doxorubicin treatment also resulted in a significant increase in exosomal ABCB1 in Malme-3M cells (by 3.5-fold) as compared to control. Addition of pegvisomant strikingly reduced the exosomal ABCB1 levels as compared to GH and doxorubicin combination treatments. Related to exosomal ABCC2 and ABCG2, GH and doxorubicin increased, albeit not significant, the levels in all the three cell-lines as compared to controls (Figure 2A,C,E, Table 1). An increasing trend was observed for exosomal ABCC2 and ABCG2 levels following doxorubicin treatment in all three cell lines as compared to control. The fold-changes are shown in Table 1. These observations collectively suggest that GH and doxorubicin, alone or in combination, upregulate exosomal ABC transporters, while the addition of pegvisomant attenuates this increase.
3.2.2. Effects of GH-Induced Melanoma-Derived Exosomes on Recipient Cells
Based on these findings, the action of GH promoting exosomal ABC transporters strongly suggests the potential role of GH in disseminating these transporters to other sensitive cancer cells via exosomes. Also, the above findings of reduced drug retention post administration with ExoGH hint towards GH-mediated exosomal transfer of ABC transporters.
Our findings reveal a significant upregulation of ABCC1 levels in Malme-3M recipient cells, following ExoGH addition, exhibiting an approximate 2-fold increase compared to control (Figure 2F,G, Table 1). Similarly, significant increases were induced by Exodoxo administration in Malme-3M cells by 2-fold compared to control. Furthermore, ABCC1 transporter levels were significantly higher (1.6-fold) in Malme-3M recipient cells compared to control when Exodox was administered. A significant reduction in ABCC1 was observed in Malme-3M and SK-MEL-28 when ExoGH+dox+Peg was administered in Malme-3M cells as compared to ExoGH. Similar reductions were observed when compared to Exodoxo and ExoGH+doxo administration in Malme-3M cells. A similar, but not significant, increase in ABCB1 and ABCG2 was observed in melanoma recipient cells when administered with ExoGH, Exodoxo, and ExoGH+doxo as compared to controls (Figure 2F,H,I, Table 1). The fold-changes are shown in Table 1. These observations suggest that ABC transporters are elevated in recipient cells when administered with exosomes from GH and doxorubicin treated cells whereas the ABC transporter levels are reduced when exposed to exosomes from pegvisomant treated melanoma cells treated in combination with GH and doxorubicin.
3.3. Blocking Autocrine/Paracrine GH Action Attenuates Exosomal ABC Transporter Levels
Pegvisomant caused a notable attenuation of GH-mediated exosomal ABC transporter levels (discussed above). In some cases, the effect was even more pronounced, with exosomal ABC levels falling below those of controls, indicating suppression of autocrine/paracrine GH action. Extensive investigations by many groups have elucidated autocrine role of GH in driving potent cancer properties, including the reduction of tumor sensitivity to chemotherapy [50,51,52]. In our previous study, we have observed elevated levels of GH and GHR RNA in SK-MEL-28 melanoma cells following treatment with chemotherapies, including doxorubicin [53]. Interestingly, we detected basal levels of GH RNA, which were significantly downregulated when SK-MEL-28 and SK-MEL-30 were treated with pegvisomant (Supplementary Figure S4). This downregulation was more pronounced in SK-MEL-30 when treated with both pegvisomant and doxorubicin.
To delineate the effects of autocrine/paracrine GH action on exosomal cargoes, we isolated exosomes from three melanoma cells lines: Malme-3M, SK-MEL-38, and SK-MEL30, treated with pegvisomant and doxorubicin. The exosomes are referred to as Exocontrol (derived from PBS treated cells), Exodoxo (from doxorubicin-treated cells), ExoPeg (from pegvisomant-treated cells), and ExoPeg+dox (from cells treated with pegvisomant and doxorubicin). Interestingly, the addition of pegvisomant did not affect the levels of exosomal ABCC1 and ABCB1 as compared to controls (Figure 3A–C). As expected, a significant increase in exosomal ABCC1 and ABCB1 was observed when melanoma cells were treated with doxorubicin alone, consistent with the findings described above, serving as a positive control. Remarkably, addition of pegvisomant in combination with doxorubicin rescued the exosomal ABCC1 and ABCB1 levels back to those observed in the control groups. Hence, blocking autocrine/paracrine GH action inhibited doxorubicin-induced exosomal ABC transporters.
3.4. Pegvisomant Treatment of Donor Melanoma Cells Attenuates Exosomal EMT Inducing Effects
GH action plays a crucial role in regulating the migration of human tumors [54,55,56]. Multiple studies have shown that tumor-derived exosomes are involved in promoting migration [57,58]. To investigate the impact of GH-derived exosomes on the migration potential of melanoma cells, we utilized a wound healing scratch assay [59].
Upon administration of ExoGH to naïve melanoma recipient cells, SK-MEL-28 and SK-MEL-30, we observed a modest increase, though not significant, in migration by 10% and 5% respectively as compared to controls (Figure 4A–D). Interestingly, treatment with Exodoxo led to a significant acceleration in migration in SK-MEL-30 (by 5%) cells compared to controls (Figure 4D). Moreover, a notable enhancement in migration was observed in both the cell lines, with SK-MEL-30 showing a 5% increase and SK-MEL-28 exhibiting a more pronounced effect with 25% rise, when incubated with ExoGH+doxo (Figure 4B,D). Remarkably, the SK-MEL-28 cells incubated with ExoGH+doxo demonstrated significantly accelerated migration compared to cells administered solely with ExoGH (by 12%) and Exodoxo (by 15%) (Figure 4B). The migration potential in both the cell lines was restored to normal when treated with ExoGH+doxo+Peg as compared to administration with ExoGH+doxo.
The addition of GH and doxorubicin alone in donor cells accelerated the migration of recipient cells via exosomes. This acceleration was further amplified in the presence of GH and doxorubicin together, showing enhanced migration potential when combined, whereas pegvisomant dampened the effect on migration. These results indicate GH and pegvisomant, when added to melanoma cells, alter the migration potential of the recipient cells.
3.5. GH Elevates the Expression of N-cadherin and MMP2 in Melamona-Derived Exosomes and Only Transfers N-cadherin to Recipient Cells
3.5.1. Effects of GH on Cadherins and MMPs in Melanoma-Derived Exosomes
EMT is among the most well-known mechanisms underlying cancer cell migration/metastasis [60]. In addition, matrix metalloproteinases (MMPs), which are potent pro-EMT factors, modify the extracellular matrix of TME and increase the ability of cancer cells to migrate and infiltrate [61]. Studies have shown that GH serves as a potent driver of EMT in transformed cells [37,38] and has been shown to promote melanoma EMT in vitro and in vivo [32,38]. Studies have also shown the involvement of GH in elevating MMPs, particularly MMP2 and MMP9, thereby promoting cancer cell migration and invasion [62,63]. Additionally, we have shown that the protein levels of N-cadherin and MMP2 are elevated in presence of GH treatment on parent melanoma cells (Malme-3M, SK-MEL-28, and SK-MEL-30) (Supplementary 5). Extensive recent research has demonstrated that exosomes harbor these pro-EMT markers ultimately elevating the cancer cell migration and invasion [64,65,66,67]. To elucidate the potential of GH in modulating EMT and MMPs, we specifically examined protein levels of N-cadherin, E-cadherin, MMP2, and MMP9 as they have been demonstrated to be modulated by GH [29,32].
GH, albeit not significantly, elevated the levels of exosomal N-cadherin in Malme-3M and SK-MEL-30 cells as compared to controls (Figure 5A,B). No difference was observed in exosomal N-cadherin levels in doxorubicin-induced cells. Notably, a significant surge in N-cadherin was observed in Malme-3M cells (by 3.5-fold) when GH was combined with doxorubicin (Figure 5A,B, Table 2). Intriguingly, the addition of pegvisomant in the combination of GH and doxorubicin significantly reduced the exosomal N-cadherin levels, particularly in Malme-3M when compared to GH and doxorubicin combination treatment. No change was observed in exosomal E-cadherin in presence of GH or blocking the GH action (Supplementary Figure S6A,B).
Similarly, GH elevated exosomal MMP2 levels in all cell lines, with a significant increase in SK-MEL-30 cells (by 1.9-fold) as compared to control (Figure 5A,C, Table 2). No difference was observed in exosomal MMP2 levels in doxorubicin-induced cells. Furthermore, a significant increase in exosomal MMP2 was observed in SK-MEL-30 cells (by 2-fold) when GH was added in combination doxorubicin as compared to control (Figure 4A,C). Pegvisomant addition to the aforementioned combination significantly attenuated the exosomal MMP2 in SK-MEL-30 as compared to GH treatment alone and as compared to the combination of GH and doxorubicin combination treatment. No change was observed in exosomal MMP9 in presence of GH or blocking the GH action (Supplementary Figure S6A,C).
3.5.2. Effects of GH-induced Melanoma-Derived Exosomes on Cadherins and MMPs in Recipient Cells
The action of GH, particularly in presence of doxorubicin, in promoting exosomal N-cadherin and MMP2, along with accelerated cell migration, indicates a potential role of GH in disseminating these proteins to treatment-naïve melanoma cells via exosomes. We observed that ExoGH significantly augmented N-cadherin levels in Malme-3M recipient cells (by 2.5-fold) and SK-MEL-28 (by 2-fold) as compared to respective controls (Figure 5D,E, Table 2). Similarly, ExoGH+doxo administration led to a significant increase in exosomal N-cadherin levels in Malme-3M recipient cells (by 2-fold) as compared to control cells. Notably, a significant reduction in N-cadherin was observed in Malme-3M recipient cells when administered with ExoGH+doxo+Peg compared to ExoGH+doxo. However, GH and doxorubicin alone and in combination had no change in MMP2 levels in the recipient cells, whereas ExoGH+doxo+Peg had a slight decrease in MMP2 level in SK-MEL-30 as compared to ExoGH+doxo (Figure 5D,F, Table 2)
In summary, our results demonstrated that GH upregulates the expression of exosomal N-cadherin and MMP2, while pegvisomant attenuates this GH-induced increase in exosomal N-cadherin and MMP2. Furthermore, exosome treatment of recipient cells suggests that GH can mediate transfer of exosomal N-cadherin to recipient cells, potentially aiding the transition to a mesenchymal phenotype, with pegvisomant mitigating this transfer. Conversely, no significant difference was observed in MMP2 recipient cells, indicating that exosomal MMPs may act externally to modulate the TME.
4. Discussion
Drug resistance continues to be a serious factor in the treatment of multiple cancers. Elevated ABC transporters in cancer cells resulting in reduced intracellular drug accumulation has been considered to be the major cause of chemotherapy resistance [68,69]. Moreover, EMT and elevated MMP levels also contribute to invasion, migration, metastasis and chemoresistance. Extensive in vitro and in vivo studies have demonstrated that GH expression exacerbates chemotherapy resistance and cancer invasion in melanoma and other cancers via upregulating the levels of ABC transporters and EMT markers [29,32,70,71]. Conversely, these factors are significantly downregulated upon the inhibition of GHR, through GHR gene disruption (knock down) or pegvisomant. Several studies have highlighted the role of exosomes in disseminating these factors involved in drug resistance [44,72] [39]. Therefore, we hypothesized that GH facilitates packaging and transfer of these factors via exosomes, thereby modulating the drug efflux properties and migration of melanoma cells. In this study, we identify a novel role of GH in upregulating the packaging of multidrug efflux pumps and EMT makers in tumor-derived exosomes. Furthermore, we also demonstrate that GH-stimulated exosomal ABC transporters and EMT markers enhance drug efflux activity and promote migration in recipient cells. Notably, GHR antagonism attenuated the GH-stimulated exosomal ABC transporters and EMT markers. This consequently restored drug sensitivity and slowed cell migration. Additionally, we investigated the effects of blocking the autocrine/paracrine GH action, which highlighted the role of pegvisomant in attenuating the local GH-mediated exosomal ABC transporters.
Elevated ABC transporters in tumor cells resulting in decreased intracellular drug accumulation is a major reason for chemotherapy resistance in cancer. Exosomes are shown to transfer multiple ABC transporters from drug-resistant cells to drug-sensitive cells to upregulate drug resistance [73,74,75,76]. Chemotherapy drugs have been shown to stimulate release the exosomes to assist cancer cells in developing urgent chemoresistance. [44]. For example, glioblastoma stem cells deliver ABCB4 via exosomes conferring glioblastoma resistance to temozolomide [77]. Our group has shown that GH elevates the specific ABC transporters such as ABCC1, ABCC2, ABCB1 and ABCG2 in melanoma, hepatocellular carcinoma, and pancreatic cancer [32,43,70]. In the current study, we observed elevated levels of ABCC1 in exosomes from three melanoma cell lines stimulated with GH. Additionally, GH significantly increased the levels of exosomal ABCB1 from Malme-3M cells. The higher selectivity of GH packaging of ABCB1 in Malme-3M can be attributed to these cells having heightened sensitivity to GH action, a correlation supported by highest levels of GHR expression in Malme-3M cells compared to other melanoma cells within the NCI-60 panel, as previously reported by our lab [28]. The transfer of these ABC transporters via exosomes has been shown to promote chemoresistance in the recipient cells. Our finding reveals that GH stimulated exosomes transferred high amounts of ABCC1 to recipient cells in Malme3M, albeit less effectively in other cells lines. This data suggests that GH can not only provide the survival advantage to the cells within the chemotherapeutic milieu but promptly transfer the therapy resistance advantage to sensitive cancer cells.
Research from our lab and others have shown that inhibiting GHR action sensitize human melanoma cells to chemotherapy by reducing the expression of ABC drug efflux pumps [29,31,32]. Here we report that inhibiting GHR action via pegvisomant downregulates the levels of GH and doxorubicin-induced exosomal ABCC1 in all the three cell lines. In addition, pegvisomant downregulates ABCC2, ABCB1, ABCG2 in Malme-3M cells. Strikingly, the transfer of ABCC1 to Malme-3M recipient cells were even lower than controls indicating suppression of basal GH action. Mounting evidence has shown autocrine/paracrine GH expression within the microenvironment of multiple human cancers including breast, endometrial, colon, liver, liver, and prostate cancer. [78,79,80]. Studies from Lobie’s group and others have shown that ‘forced’ autocrine GH expression is sufficient to promote oncogenic transformation of mammary epithelial cells in vitro whereas exogenously added hGH does not result in oncogenic transformation [51,78]. Autocrine/paracrine GH has also been implicated in resistance to radiation [79] and several chemotherapies, including mitomycin-C and daunorubicin [52,81]. Notably, doxorubicin has been shown to induce DNA damage, which in turn, induces GH production via p53 upregulation [30]. Moreover, our previous research has shown elevated levels of GH and GHR RNA in SK-MEL-28 melanoma cells following treatment with chemotherapies, including doxorubicin [53]. Here we show, pegvisomant mitigates the doxorubicin-induced exosomal ABC transporters. Pegvisomant, thus effectively downregulates the exosomal packaging of ABC transporters by suppressing basal autocrine/paracrine and potential chemotherapy-induced GH.
EMT serves as a crucial initial process of metastasis. Exosomes from highly metastatic cells have shown to ‘educate’ cells with low metastatic potential to increase their migration and invasion [82]. Notably, these exosomes have been shown to elevate EMT by upregulating key markers such as N-cadherin and vimentin [82]. Exosomal N-cadherin has been identified as serum biomarker indicative of metastatic disease progression. Elevated levels of exosomal N-cadherin from serum has been detected in the serum of osteosarcoma patients with pulmonary metastasis compared to those without metastasis [83]. Another study has shown that exosomes from late-stage lung cancer serum can induce migration, invasion, and proliferation in non-cancerous recipient human bronchial epithelial cells [84]. Our group has previously shown that GH increases both protein and RNA levels of N-cadherin upon GH treatment while GHR knockdown downregulates the N-cadherin expression in melanoma [38]. Here we report that GH treatment significantly elevated N-cadherin levels in melanoma-derived exosomes when treated in combination with doxorubicin. While no significant elevation of N-cadherin levels was seen in GH-induced exosomes, a significant increase was observed when the GH-induced exosomes were administered in recipient cells, particularly in Malme-3M and SK-MEL-28. Interestingly, similar levels of N-cadherin were maintained in Malme-3M recipient cells when treated with exosomes from GH and doxorubicin combination, whereas no such increase was seen in recipient cells treated with exosomes form doxorubicin-only treated cells. These results suggest that GH-induced exosomes potentially transfer factors that promote expression of N-cadherin. Previous research have highlighted the role of various microRNAs, such as mir-19b-3p-derived from cancer stem cells, in exosome mediated transfer to renal cell carcinoma, resulting in the upregulation of N-cadherin via PTEN regulation [85]. Also, highly invasive gastric cancer has been shown to transfer lncRNA ZFAS1 to less invasive gastric cancer, thereby promoting migration and EMT through the upregulation of N-cadherin [86].
MMPs remodels ECM by breaking down collagen, thereby enhancing the aggressiveness of cancer cells. MMP2 is shown to be carried by exosomes released by endothelial cells in to extracellular space, where MMP14 activates MMP2, facilitating ECM breakdown [87]. Studies have implicated involvement of GH in MMP modulation thus creating an invasive environment for the cancer cells. Lobie and group has shown an upregulation of MMP9 in endometrial cancer cells [63] and upregulation of MMP2 and MMP9 in breast cancer cells when treated with GH [62]. In our study we show that GH increases MMP2 in melanoma-derived exosomes. However intriguingly, these elevated levels of exosomal MMP2 were not transferred to the recipient cells. This observation suggests that GH-induced upregulation of exosomal MMP2 may contribute to the breakdown of ECM, thereby aiding the melanoma cell migration.
5. Conclusions
Our results demonstrate that excess GH upregulates ABC transporters, particularly ABCC1, ABCG2, and ABCG2 in the melanoma derived exosomes, which in turn, can be transferred to treatment naïve melanoma cells making them drug resistant. Additionally, GH stimulation leads to upregulation of N-cadherin and MMP2 in melanoma-derived exosomes, with N-cadherin being transferred to treatment naïve melanoma cells, enhancing their migratory potential. Although MMP2 is elevated in GH-induced exosomes, its transfer is not observed, indicating its predominant role in ECM degradation. Pegvisomant effectively inhibits the GH-induced upregulation of these factors in exosomes, consequently lowering the drug resistance and slowing down cell migration. Together, our results indicate a novel role of GH in disseminating the drug efflux and migration-promoting factors, contributing to chemotherapy resistance. Moreover, these factors hold promise as potential biomarkers in GH-sensitive cancers, aiding in therapy-monitoring and assessment of aggressive potential. Targeting the GHR with pegvisomant or other GH receptor antagonists presents a therapeutics strategy to mitigate exosomes-mediated dissemination of these factors, thereby overcoming chemotherapy resistance.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1. EC50s (in µM) of the doxorubicin chemotherapy; Figure S2. Characterization of melanoma-derived exosomes; Figure S3. GH regulates ABC efflux pump levels in melanoma cells; Figure S4. Pegvisomant downregulates basal levels of GH in human melanoma cells; Figure S5. GH elevates ABC efflux pump levels in melanoma cells; Figure S6. Effects of GH and pegvisomant in E-cadherin and MMP9 in tumor-derived exosomes.
Author Contributions
Conceptualization, P.K., R.B. and J.K.; methodology, P.K., T.B., B.L. and N.M.; software, P.K. and N.M.; validation, P.K., R.B. and J.K.; formal analysis, P.K., T.B., B.L. and N.M.; investigation, P.K,; resources, P.K., and J.K.; data curation, P.K., R.B. and J.K.; writing—original draft preparation, P.K.; writing—review and editing, P.K., R.B. and J.K.; visualization, P.K.; supervision, R.B. and J.K.; project administration, R.B. and J.K.; funding acquisition, P.K., and J.K..
Funding
This work was supported, in part, by the State of Ohio’s Eminent Scholar Program that includes a gift from Milton and Lawrence Goll to JK; the John J. Kopchick Molecular Cell Biology/Translational Biomedical Sciences Award, Original Work Grant, Nanoscale & Quantum Phenomena Institute Award and Student Enhancement Award to PK; the AMVETS and the Edison Biotechnology Institute at Ohio University.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Acknowledgments
We acknowledge Mahima R. Sanyal (Ohio University) for her inputs in reviewing the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Melanoma Skin Cancer Statistics. Available online: https://www.cancer.org/cancer/types/melanoma-skin-cancer/about/key-statistics.html (accessed on 18 June 2024).
- Kozar, I.; Margue, C.; Rothengatter, S.; Haan, C.; Kreis, S. Many Ways to Resistance: How Melanoma Cells Evade Targeted Therapies. Biochim. Biophys. Acta BBA - Rev. Cancer 2019, 1871, 313–322. [Google Scholar] [CrossRef]
- Kalal, B.S.; Upadhya, D.; Pai, V.R. Chemotherapy Resistance Mechanisms in Advanced Skin Cancer. Oncol. Rev. 2017, 11, 326. [Google Scholar] [CrossRef]
- Huang, Y.; Hong, W.; Wei, X. The Molecular Mechanisms and Therapeutic Strategies of EMT in Tumor Progression and Metastasis. J. Hematol. Oncol.J Hematol Oncol 2022, 15, 129. [Google Scholar] [CrossRef]
- Falcone, I.; Conciatori, F.; Bazzichetto, C.; Ferretti, G.; Cognetti, F.; Ciuffreda, L.; Milella, M. Tumor Microenvironment: Implications in Melanoma Resistance to Targeted Therapy and Immunotherapy. Cancers 2020, 12, 2870. [Google Scholar] [CrossRef] [PubMed]
- Soekmadji, C.; Nelson, C.C. The Emerging Role of Extracellular Vesicle-Mediated Drug Resistance in Cancers: Implications in Advanced Prostate Cancer. BioMed Res. Int. 2015, 2015, 454837. [Google Scholar] [CrossRef]
- Mastronikolis, N.S.; Kyrodimos, E.; Spyropoulou, D.; Delides, A.; Giotakis, E.; Piperigkou, Z.; Karamanos, N.K. The Role of Exosomes in Epithelial–to-Mesenchymal Transition and Cell Functional Properties in Head and Neck Cancer. Cancers 2023, 15, 2156. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Xing, J.; Xu, K.; Liu, D.; Zhuo, Y. Exosomes in the Tumor Microenvironment: Promoting Cancer Progression. Front. Immunol. 2022, 13, 1025218. [Google Scholar] [CrossRef]
- Raposo, G.; Stoorvogel, W. Extracellular Vesicles: Exosomes, Microvesicles, and Friends. J Cell Biol 2013, 200, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Dongre, A.; Weinberg, R.A. New Insights into the Mechanisms of Epithelial–Mesenchymal Transition and Implications for Cancer. Nat. Rev. Mol. Cell Biol. 2019, 20, 69–84. [Google Scholar] [CrossRef]
- Xu, Z.; Zhang, Y.; Dai, H.; Han, B. Epithelial–Mesenchymal Transition-Mediated Tumor Therapeutic Resistance. Molecules 2022, 27, 4750. [Google Scholar] [CrossRef]
- Said, S.S.; Ibrahim, W.N. Cancer Resistance to Immunotherapy: Comprehensive Insights with Future Perspectives. Pharmaceutics 2023, 15, 1143. [Google Scholar] [CrossRef] [PubMed]
- Weadick, B.; Nayak, D.; Persaud, A.K.; Hung, S.W.; Raj, R.; Campbell, M.J.; Chen, W.; Li, J.; Williams, T.M.; Govindarajan, R. EMT-Induced Gemcitabine Resistance in Pancreatic Cancer Involves the Functional Loss of Equilibrative Nucleoside Transporter 1. Mol. Cancer Ther. 2021, 20, 410–422. [Google Scholar] [CrossRef]
- Huang, M.; Zhang, D.; Wu, J.Y.; Xing, K.; Yeo, E.; Li, C.; Zhang, L.; Holland, E.; Yao, L.; Qin, L.; et al. Wnt-Mediated Endothelial Transformation into Mesenchymal Stem Cell–like Cells Induces Chemoresistance in Glioblastoma. Sci. Transl. Med. 2020, 12, eaay7522. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Zhang, R.; An, X.; Li, Z.; Fang, C.; Pan, B.; Chen, W.; Xu, G.; Han, W. LncRNA HOXA-AS3 Confers Cisplatin Resistance by Interacting with HOXA3 in Non-Small-Cell Lung Carcinoma Cells. Oncogenesis 2019, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kirave, P.; Gondaliya, P.; Kulkarni, B.; Rawal, R.; Garg, R.; Jain, A.; Kalia, K. Exosome Mediated miR-155 Delivery Confers Cisplatin Chemoresistance in Oral Cancer Cells via Epithelial-Mesenchymal Transition. Oncotarget 2020, 11, 1157–1171. [Google Scholar] [CrossRef]
- Bebawy, M.; Combes, V.; Lee, E.; Jaiswal, R.; Gong, J.; Bonhoure, A.; Grau, G.E.R. Membrane Microparticles Mediate Transfer of P-Glycoprotein to Drug Sensitive Cancer Cells. Leukemia 2009, 23, 1643–1649. [Google Scholar] [CrossRef] [PubMed]
- Levchenko, A.; Mehta, B.M.; Niu, X.; Kang, G.; Villafania, L.; Way, D.; Polycarpe, D.; Sadelain, M.; Larson, S.M. Intercellular Transfer of P-Glycoprotein Mediates Acquired Multidrug Resistance in Tumor Cells. Proc. Natl. Acad. Sci. U. S. A. 2005, 102, 1933–1938. [Google Scholar] [CrossRef]
- Wang, B.; Tan, Z.; Guan, F. Tumor-Derived Exosomes Mediate the Instability of Cadherins and Promote Tumor Progression. Int. J. Mol. Sci. 2019, 20, 3652. [Google Scholar] [CrossRef] [PubMed]
- Hardin, H.; Helein, H.; Meyer, K.; Robertson, S.; Zhang, R.; Zhong, W.; Lloyd, R. Thyroid Cancer Stem-Like Cell Exosomes: Regulation of EMT via Transfer of LncRNAs. Lab. Investig. J. Tech. Methods Pathol. 2018, 98, 1133–1142. [Google Scholar] [CrossRef]
- Olarescu, N.C.; Gunawardane, K.; Hansen, T.K.; Møller, N.; Jørgensen, J.O.L. Normal Physiology of Growth Hormone in Adults. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., Dungan, K., Grossman, A., Hershman, J.M., Kaltsas, G., Koch, C., Kopp, P., Korbonits, M., McLachlan, R., Morley, J.E., New, M., Perreault, L., Purnell, J., Rebar, R., Singer, F., Trence, D.L., Vinik, A., Wilson, D.P., Eds.; MDText.com, Inc.: South Dartmouth (MA), 2000. [Google Scholar]
- Dal, J.; Leisner, M.Z.; Hermansen, K.; Farkas, D.K.; Bengtsen, M.; Kistorp, C.; Nielsen, E.H.; Andersen, M.; Feldt-Rasmussen, U.; Dekkers, O.M.; et al. Cancer Incidence in Patients With Acromegaly: A Cohort Study and Meta-Analysis of the Literature. J. Clin. Endocrinol. Metab. 2018, 103, 2182–2188. [Google Scholar] [CrossRef]
- Laron, Z.; Kauli, R.; Lapkina, L.; Werner, H. IGF-I Deficiency, Longevity and Cancer Protection of Patients with Laron Syndrome. Mutat. Res. Mutat. Res. 2017, 772, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Guevara-Aguirre, J.; Balasubramanian, P.; Guevara-Aguirre, M.; Wei, M.; Madia, F.; Cheng, C.-W.; Hwang, D.; Martin-Montalvo, A.; Saavedra, J.; Ingles, S.; et al. Growth Hormone Receptor Deficiency Is Associated With a Major Reduction in Pro-Aging Signaling, Cancer and Diabetes in Humans. Sci. Transl. Med. 2011, 3, 70ra13. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S. Extrapituitary Growth Hormone. Endocrine 2010, 38, 335–359. [Google Scholar] [CrossRef]
- Kopchick, J.J.; Basu, R.; Berryman, D.E.; Jorgensen, J.O.L.; Johannsson, G.; Puri, V. Covert Actions of Growth Hormone: Fibrosis, Cardiovascular Diseases and Cancer. Nat. Rev. Endocrinol. 2022, 18, 558–573. [Google Scholar] [CrossRef]
- Non-Pituitary GH Regulation of the Tissue Microenvironment in: Endocrine-Related Cancer Volume 30 Issue 7 (2023). Available online: https://erc.bioscientifica.com/view/journals/erc/30/7/ERC-23-0028.xml (accessed on 9 March 2024).
- Sustarsic, E.G.; Junnila, R.K.; Kopchick, J.J. Human Metastatic Melanoma Cell Lines Express High Levels of Growth Hormone Receptor and Respond to GH Treatment. Biochem. Biophys. Res. Commun. 2013, 441. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Baumgaertel, N.; Wu, S.; Kopchick, J.J. Growth Hormone Receptor Knockdown Sensitizes Human Melanoma Cells to Chemotherapy by Attenuating Expression of ABC Drug Efflux Pumps. Horm. Cancer 2017, 8, 143–156. [Google Scholar] [CrossRef]
- Basu, R.; Kopchick, J.J. The Effects of Growth Hormone on Therapy Resistance in Cancer. Cancer Drug Resist. 2019. [Google Scholar] [CrossRef]
- Arumugam, A.; Subramani, R.; Nandy, S.B.; Terreros, D.; Dwivedi, A.K.; Saltzstein, E.; Lakshmanaswamy, R. Silencing Growth Hormone Receptor Inhibits Estrogen Receptor Negative Breast Cancer through ATP-Binding Cassette Sub-Family G Member 2. Exp. Mol. Med. 2019, 51, 1–13. [Google Scholar] [CrossRef]
- Qian, Y.; Basu, R.; Mathes, S.C.; Arnett, N.A.; Duran-Ortiz, S.; Funk, K.R.; Brittain, A.L.; Kulkarni, P.; Terry, J.C.; Davis, E. Growth Hormone Upregulates Mediators of Melanoma Drug Efflux and Epithelial-to-Mesenchymal Transition in Vitro and in Vivo. Cancers 2020, 12, 3640. [Google Scholar] [CrossRef]
- Wu, Z.-S.; Yang, K.; Wan, Y.; Qian, P.-X.; Perry, J.K.; Chiesa, J.; Mertani, H.C.; Zhu, T.; Lobie, P.E. Tumor Expression of Human Growth Hormone and Human Prolactin Predict a Worse Survival Outcome in Patients with Mammary or Endometrial Carcinoma. J. Clin. Endocrinol. Metab. 2011, 96, E1619–1629. [Google Scholar] [CrossRef]
- Waters, M.J.; Conway-Campbell, B.L. The Oncogenic Potential of Autocrine Human Growth Hormone in Breast Cancer. Proc. Natl. Acad. Sci. 2004, 101, 14992–14993. [Google Scholar] [CrossRef] [PubMed]
- Subramani, R.; Lopez-Valdez, R.; Salcido, A.; Boopalan, T.; Arumugam, A.; Nandy, S.; Lakshmanaswamy, R. Growth Hormone Receptor Inhibition Decreases the Growth and Metastasis of Pancreatic Ductal Adenocarcinoma. Exp. Mol. Med. 2014, 46, e117. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; Wu, W.; Yuan, Y.; Pandey, V.; Wu, Z.; Lu, X.; Zhang, W.; Chen, Y.; Wu, M.; Zhang, M.; et al. Human Growth Hormone and Human Prolactin Function as Autocrine/Paracrine Promoters of Progression of Hepatocellular Carcinoma. Oncotarget 2016, 7, 29465–29479. [Google Scholar] [CrossRef]
- Brittain, A.L.; Basu, R.; Qian, Y.; Kopchick, J.J. Growth Hormone and the Epithelial-to-Mesenchymal Transition. J. Clin. Endocrinol. Metab. 2017, 102, 3662–3673. [Google Scholar] [CrossRef]
- Basu, R.; Wu, S.; Kopchick, J.J. Targeting Growth Hormone Receptor in Human Melanoma Cells Attenuates Tumor Progression and Epithelial Mesenchymal Transition via Suppression of Multiple Oncogenic Pathways. Oncotarget 2017, 8, 21579–21598. [Google Scholar] [CrossRef]
- Steinbichler, T.B.; Dudás, J.; Skvortsov, S.; Ganswindt, U.; Riechelmann, H.; Skvortsova, I.-I. Therapy Resistance Mediated by Exosomes. Mol. Cancer 2019, 18, 58. [Google Scholar] [CrossRef] [PubMed]
- Skarkova, V.; Vitovcova, B.; Matouskova, P.; Manethova, M.; Kazimirova, P.; Skarka, A.; Brynychova, V.; Soucek, P.; Vosmikova, H.; Rudolf, E. Role of N-Cadherin in Epithelial-to-Mesenchymal Transition and Chemosensitivity of Colon Carcinoma Cells. Cancers 2022, 14, 5146. [Google Scholar] [CrossRef]
- Tune, B.X.J.; Sim, M.S.; Poh, C.L.; Guad, R.M.; Woon, C.K.; Hazarika, I.; Das, A.; Gopinath, S.C.B.; Rajan, M.; Sekar, M.; et al. Matrix Metalloproteinases in Chemoresistance: Regulatory Roles, Molecular Interactions, and Potential Inhibitors. J. Oncol. 2022, 2022, 3249766. [Google Scholar] [CrossRef]
- Dart, A. EMT in Chemoresistance. Nat. Rev. Cancer 2023, 23, 349–349. [Google Scholar] [CrossRef]
- Basu, R.; Kulkarni, P.; Swegan, D.; Duran-Ortiz, S.; Ahmad, A.; Caggiano, L.J.; Davis, E.; Walsh, C.; Brenya, E.; Koshal, A.; et al. Growth Hormone Receptor Antagonist Markedly Improves Gemcitabine Response in a Mouse Xenograft Model of Human Pancreatic Cancer 2024.
- Wang, X.; Qiao, D.; Chen, L.; Xu, M.; Chen, S.; Huang, L.; Wang, F.; Chen, Z.; Cai, J.; Fu, L. Chemotherapeutic Drugs Stimulate the Release and Recycling of Extracellular Vesicles to Assist Cancer Cells in Developing an Urgent Chemoresistance. Mol. Cancer 2019, 18, 182. [Google Scholar] [CrossRef]
- Qin, X.; Yu, S.; Zhou, L.; Shi, M.; Hu, Y.; Xu, X.; Shen, B.; Liu, S.; Yan, D.; Feng, J. Cisplatin-Resistant Lung Cancer Cell–Derived Exosomes Increase Cisplatin Resistance of Recipient Cells in Exosomal miR-100–5p-Dependent Manner. Int. J. Nanomedicine 2017, 12, 3721–3733. [Google Scholar] [CrossRef]
- Wei, F.; Ma, C.; Zhou, T.; Dong, X.; Luo, Q.; Geng, L.; Ding, L.; Zhang, Y.; Zhang, L.; Li, N.; et al. Exosomes Derived from Gemcitabine-Resistant Cells Transfer Malignant Phenotypic Traits via Delivery of miRNA-222-3p. Mol. Cancer 2017, 16, 132. [Google Scholar] [CrossRef] [PubMed]
- Tritos, N.A.; Biller, B.M.K. Pegvisomant: A Growth Hormone Receptor Antagonist Used in the Treatment of Acromegaly. Pituitary 2017, 20, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Kopchick, J.J. Discovery and Mechanism of Action of Pegvisomant. Eur. J. Endocrinol. 2003, 148 Suppl 2, S21–25. [Google Scholar] [CrossRef]
- Kaseb, A.O.; Haque, A.; Vishwamitra, D.; Hassan, M.M.; Xiao, L.; George, B.; Sahu, V.; Mohamed, Y.I.; Carmagnani Pestana, R.; Lombardo, J.L.; et al. Blockade of Growth Hormone Receptor Signaling by Using Pegvisomant: A Functional Therapeutic Strategy in Hepatocellular Carcinoma. Front. Oncol. 2022, 12, 986305. [Google Scholar] [CrossRef] [PubMed]
- Kaulsay, K.K.; Mertani, H.C.; Törnell, J.; Morel, G.; Lee, K.-O.; Lobie, P.E. Autocrine Stimulation of Human Mammary Carcinoma Cell Proliferation by Human Growth Hormone. Exp. Cell Res. 1999, 250, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Mukhina, S.; Mertani, H.C.; Guo, K.; Lee, K.-O.; Gluckman, P.D.; Lobie, P.E. Phenotypic Conversion of Human Mammary Carcinoma Cells by Autocrine Human Growth Hormone. Proc. Natl. Acad. Sci. 2004, 101, 15166–15171. [Google Scholar] [CrossRef] [PubMed]
- Bougen, N.M.; Yang, T.; Chen, H.; Lobie, P.E.; Perry, J.K. Autocrine Human Growth Hormone Reduces Mammary and Endometrial Carcinoma Cell Sensitivity to Mitomycin C. Oncol. Rep. 2011, 26, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Kulkarni, P.; Qian, Y.; Walsh, C.; Arora, P.; Davis, E.; Duran-Ortiz, S.; Funk, K.; Ibarra, D.; Kruse, C.; et al. Growth Hormone Upregulates Melanocyte-Inducing Transcription Factor Expression and Activity via JAK2-STAT5 and SRC Signaling in GH Receptor-Positive Human Melanoma. Cancers 2019, 11, 1352. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-J.; You, M.-L.; Chong, Q.-Y.; Pandey, V.; Zhuang, Q.-S.; Liu, D.-X.; Ma, L.; Zhu, T.; Lobie, P.E. Autocrine Human Growth Hormone Promotes Invasive and Cancer Stem Cell-Like Behavior of Hepatocellular Carcinoma Cells by STAT3 Dependent Inhibition of CLAUDIN-1 Expression. Int. J. Mol. Sci. 2017, 18, 1274. [Google Scholar] [CrossRef]
- Vouyovitch, C.M.; Perry, J.K.; Liu, D.X.; Bezin, L.; Vilain, E.; Diaz, J.-J.; Lobie, P.E.; Mertani, H.C. WNT4 Mediates the Autocrine Effects of Growth Hormone in Mammary Carcinoma Cells. Endocr. Relat. Cancer 2016, 23, 571–585. [Google Scholar] [CrossRef]
- Wang, J.-J.; Chong, Q.-Y.; Sun, X.-B.; You, M.-L.; Pandey, V.; Chen, Y.-J.; Zhuang, Q.-S.; Liu, D.-X.; Ma, L.; Wu, Z.-S.; et al. Autocrine hGH Stimulates Oncogenicity, Epithelial-Mesenchymal Transition and Cancer Stem Cell-like Behavior in Human Colorectal Carcinoma. Oncotarget 2017, 8, 103900–103918. [Google Scholar] [CrossRef] [PubMed]
- Osaki, M.; Okada, F. Exosomes and Their Role in Cancer Progression. Yonago Acta Med. 2019, 62, 182–190. [Google Scholar] [CrossRef] [PubMed]
- McCready, J.; Sims, J.D.; Chan, D.; Jay, D.G. Secretion of Extracellular Hsp90α via Exosomes Increases Cancer Cell Motility: A Role for Plasminogen Activation. BMC Cancer 2010, 10, 294. [Google Scholar] [CrossRef] [PubMed]
- Freitas, J.T.; Jozic, I.; Bedogni, B. Wound Healing Assay for Melanoma Cell Migration. Methods Mol. Biol. Clifton NJ 2021, 2265, 65–71. [Google Scholar] [CrossRef]
- Hwang, S.T.; Yang, M.H.; Kumar, A.P.; Sethi, G.; Ahn, K.S. Corilagin Represses Epithelial to Mesenchymal Transition Process Through Modulating Wnt/β-Catenin Signaling Cascade. Biomolecules 2020, 10, 1406. [Google Scholar] [CrossRef] [PubMed]
- Niland, S.; Riscanevo, A.X.; Eble, J.A. Matrix Metalloproteinases Shape the Tumor Microenvironment in Cancer Progression. Int. J. Mol. Sci. 2021, 23, 146. [Google Scholar] [CrossRef] [PubMed]
- Mukhina, S.; Mertani, H.C.; Guo, K.; Lee, K.-O.; Gluckman, P.D.; Lobie, P.E. Phenotypic Conversion of Human Mammary Carcinoma Cells by Autocrine Human Growth Hormone. Proc. Natl. Acad. Sci. 2004, 101, 15166–15171. [Google Scholar] [CrossRef] [PubMed]
- Pandey, V.; Perry, J.K.; Mohankumar, K.M.; Kong, X.-J.; Liu, S.-M.; Wu, Z.-S.; Mitchell, M.D.; Zhu, T.; Lobie, P.E. Autocrine Human Growth Hormone Stimulates Oncogenicity of Endometrial Carcinoma Cells. Endocrinology 2008, 149, 3909–3919. [Google Scholar] [CrossRef]
- Dolo, V.; Ginestra, A.; Cassarà, D.; Violini, S.; Lucania, G.; Torrisi, M.R.; Nagase, H.; Canevari, S.; Pavan, A.; Vittorelli, M.L. Selective Localization of Matrix Metalloproteinase 9, Β1 Integrins, and Human Lymphocyte Antigen Class I Molecules on Membrane Vesicles Shed by 8701-BC Breast Carcinoma Cells. Cancer Res. 1998, 58, 4468–4474. [Google Scholar]
- Ginestra, A.; La Placa, M.D.; Saladino, F.; Cassarà, D.; Nagase, H.; Vittorelli, M.L. The Amount and Proteolytic Content of Vesicles Shed by Human Cancer Cell Lines Correlates with Their in Vitro Invasiveness. Anticancer Res. 1998, 18, 3433–3437. [Google Scholar] [PubMed]
- Roche, J. The Epithelial-to-Mesenchymal Transition in Cancer. Cancers 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Ginestra, A.; Monea, S.; Seghezzi, G.; Dolo, V.; Nagase, H.; Mignatti, P.; Vittorelli, M.L. Urokinase Plasminogen Activator and Gelatinases Are Associated with Membrane Vesicles Shed by Human HT1080 Fibrosarcoma Cells. J. Biol. Chem. 1997, 272, 17216–17222. [Google Scholar] [CrossRef]
- Alfarouk, K.O.; Stock, C.-M.; Taylor, S.; Walsh, M.; Muddathir, A.K.; Verduzco, D.; Bashir, A.H.H.; Mohammed, O.Y.; Elhassan, G.O.; Harguindey, S.; et al. Resistance to Cancer Chemotherapy: Failure in Drug Response from ADME to P-Gp. Cancer Cell Int. 2015, 15, 71. [Google Scholar] [CrossRef] [PubMed]
- Shen, D.-W.; Fojo, A.; Chin, J.E.; Roninson, I.B.; Richert, N.; Pastan, I.; Gottesman, M.M. Human Multidrug-Resistant Cell Lines: Increased Mdr1 Expression Can Precede Gene Amplification. Science 1986, 232, 643–645. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Qian, Y.; Mathes, S.; Terry, J.; Arnett, N.; Riddell, T.; Stevens, A.; Funk, K.; Bell, S.; Bokal, Z.; et al. Growth Hormone Receptor Antagonism Downregulates ATP-Binding Cassette Transporters Contributing to Improved Drug Efficacy against Melanoma and Hepatocarcinoma in Vivo. Front. Oncol. 2022, 12, 936145. [Google Scholar] [CrossRef]
- Basu, R.; Qian, Y.; Kopchick, J.J. MECHANISMS IN ENDOCRINOLOGY: Lessons from Growth Hormone Receptor Gene-Disrupted Mice: Are There Benefits of Endocrine Defects? Eur. J. Endocrinol. 2018, 178, R155–R181. [Google Scholar] [CrossRef]
- Raji, G.R.; Sruthi, T.V.; Edatt, L.; Haritha, K.; Sharath Shankar, S.; Sameer Kumar, V.B. Horizontal Transfer of miR-106a/b from Cisplatin Resistant Hepatocarcinoma Cells Can Alter the Sensitivity of Cervical Cancer Cells to Cisplatin. Cell. Signal. 2017, 38, 146–158. [Google Scholar] [CrossRef]
- Corcoran, C.; Rani, S.; O’Brien, K.; O’Neill, A.; Prencipe, M.; Sheikh, R.; Webb, G.; McDermott, R.; Watson, W.; Crown, J.; et al. Docetaxel-Resistance in Prostate Cancer: Evaluating Associated Phenotypic Changes and Potential for Resistance Transfer via Exosomes. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Lv, M.; Zhu, X.; Chen, W.; Zhong, S.; Hu, Q.; Ma, T.; Zhang, J.; Chen, L.; Tang, J.; Zhao, J. Exosomes Mediate Drug Resistance Transfer in MCF-7 Breast Cancer Cells and a Probable Mechanism Is Delivery of P-Glycoprotein. Tumor Biol. 2014, 35, 10773–10779. [Google Scholar] [CrossRef]
- Bebawy, M.; Combes, V.; Lee, E.; Jaiswal, R.; Gong, J.; Bonhoure, A.; Grau, G.E.R. Membrane Microparticles Mediate Transfer of P-Glycoprotein to Drug Sensitive Cancer Cells. Leukemia 2009, 23, 1643–1649. [Google Scholar] [CrossRef]
- Levchenko, A.; Mehta, B.M.; Niu, X.; Kang, G.; Villafania, L.; Way, D.; Polycarpe, D.; Sadelain, M.; Larson, S.M. Intercellular Transfer of P-Glycoprotein Mediates Acquired Multidrug Resistance in Tumor Cells. Proc. Natl. Acad. Sci. U. S. A. 2005, 102, 1933–1938. [Google Scholar] [CrossRef]
- Xu, X.; Zheng, Y.; Luo, L.; You, Z.; Chen, H.; Wang, J.; Zhang, F.; Liu, Y.; Ke, Y. Glioblastoma Stem Cells Deliver ABCB4 Transcribed by ATF3 via Exosomes Conferring Glioblastoma Resistance to Temozolomide. Cell Death Dis. 2024, 15, 318. [Google Scholar] [CrossRef]
- Zhu, T.; Starling-Emerald, B.; Zhang, X.; Lee, K.-O.; Gluckman, P.D.; Mertani, H.C.; Lobie, P.E. Oncogenic Transformation of Human Mammary Epithelial Cells by Autocrine Human Growth Hormone. Cancer Res. 2005, 65, 317–324. [Google Scholar] [CrossRef]
- Bougen, N.M.; Steiner, M.; Pertziger, M.; Banerjee, A.; Brunet-Dunand, S.E.; Zhu, T.; Lobie, P.E.; Perry, J.K. Autocrine Human GH Promotes Radioresistance in Mammary and Endometrial Carcinoma Cells. Endocr. Relat. Cancer 2012, 19, 625–644. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.K.; Wu, Z.-S.; Mertani, H.C.; Zhu, T.; Lobie, P.E. Tumour-Derived Human Growth Hormone As a Therapeutic Target in Oncology. Trends Endocrinol. Metab. 2017, 28, 587–596. [Google Scholar] [CrossRef]
- Zhu, Z.; Mukhina, S.; Zhu, T.; Mertani, H.C.; Lee, K.-O.; Lobie, P.E. P44/42 MAP Kinase-Dependent Regulation of Catalase by Autocrine Human Growth Hormone Protects Human Mammary Carcinoma Cells from Oxidative Stress-Induced Apoptosis. Oncogene 2005, 24, 3774–3785. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Guo, P.; He, Y.; Chen, Z.; Chen, L.; Luo, Y.; Qi, L.; Liu, Y.; Wu, Q.; Cui, Y.; et al. HCC-Derived Exosomes Elicit HCC Progression and Recurrence by Epithelial-Mesenchymal Transition through MAPK/ERK Signalling Pathway. Cell Death Dis. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, H.; Sun, X.; Wang, X.; Ren, T.; Huang, Y.; Zhang, R.; Zheng, B.; Guo, W. Exosomal PD-L1 and N-Cadherin Predict Pulmonary Metastasis Progression for Osteosarcoma Patients. J. Nanobiotechnology 2020, 18, 151. [Google Scholar] [CrossRef]
- Rahman, M.A.; Barger, J.F.; Lovat, F.; Gao, M.; Otterson, G.A.; Nana-Sinkam, P. Lung Cancer Exosomes as Drivers of Epithelial Mesenchymal Transition. Oncotarget 2016, 7, 54852–54866. [Google Scholar] [CrossRef]
- Wang, L.; Yang, G.; Zhao, D.; Wang, J.; Bai, Y.; Peng, Q.; Wang, H.; Fang, R.; Chen, G.; Wang, Z.; et al. CD103-Positive CSC Exosome Promotes EMT of Clear Cell Renal Cell Carcinoma: Role of Remote MiR-19b-3p. Mol. Cancer 2019, 18, 86. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Liang, W.; Fu, M.; Huang, Z.-H.; Li, X.; Zhang, W.; Zhang, P.; Qian, H.; Jiang, P.-C.; Xu, W.-R.; et al. Exosomes-Mediated Transfer of Long Noncoding RNA ZFAS1 Promotes Gastric Cancer Progression. J. Cancer Res. Clin. Oncol. 2017, 143, 991–1004. [Google Scholar] [CrossRef] [PubMed]
- Han, K.-Y.; Dugas-Ford, J.; Seiki, M.; Chang, J.-H.; Azar, D.T. Evidence for the Involvement of MMP14 in MMP2 Processing and Recruitment in Exosomes of Corneal Fibroblasts. Invest. Ophthalmol. Vis. Sci. 2015, 56, 5323–5329. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
GHR antagonism in melanoma donor cells increased the drug retention in recipient melanoma cells A. Changes in amounts of DiOC2(3) retained in the melanoma cells following administration with 20 μg/ml exosomes for 12-hours, isolated from melanoma cells treated with 50 ng/ml GH independently or in combination with EC50 dosage of doxorubicin and 500nM pegvisomant. The fluorescent readouts from intracellular DiOC2(3) are presented for Malme-3M (B), SK-MEL-28 (C) and SK-MEL-30 (D) melanoma cells. Two independent experiments were performed in triplicates and presented as the mean ± SD and p <0.05 (* / #) and p<0.005 (** / ##).
Figure 1.
GHR antagonism in melanoma donor cells increased the drug retention in recipient melanoma cells A. Changes in amounts of DiOC2(3) retained in the melanoma cells following administration with 20 μg/ml exosomes for 12-hours, isolated from melanoma cells treated with 50 ng/ml GH independently or in combination with EC50 dosage of doxorubicin and 500nM pegvisomant. The fluorescent readouts from intracellular DiOC2(3) are presented for Malme-3M (B), SK-MEL-28 (C) and SK-MEL-30 (D) melanoma cells. Two independent experiments were performed in triplicates and presented as the mean ± SD and p <0.05 (* / #) and p<0.005 (** / ##).
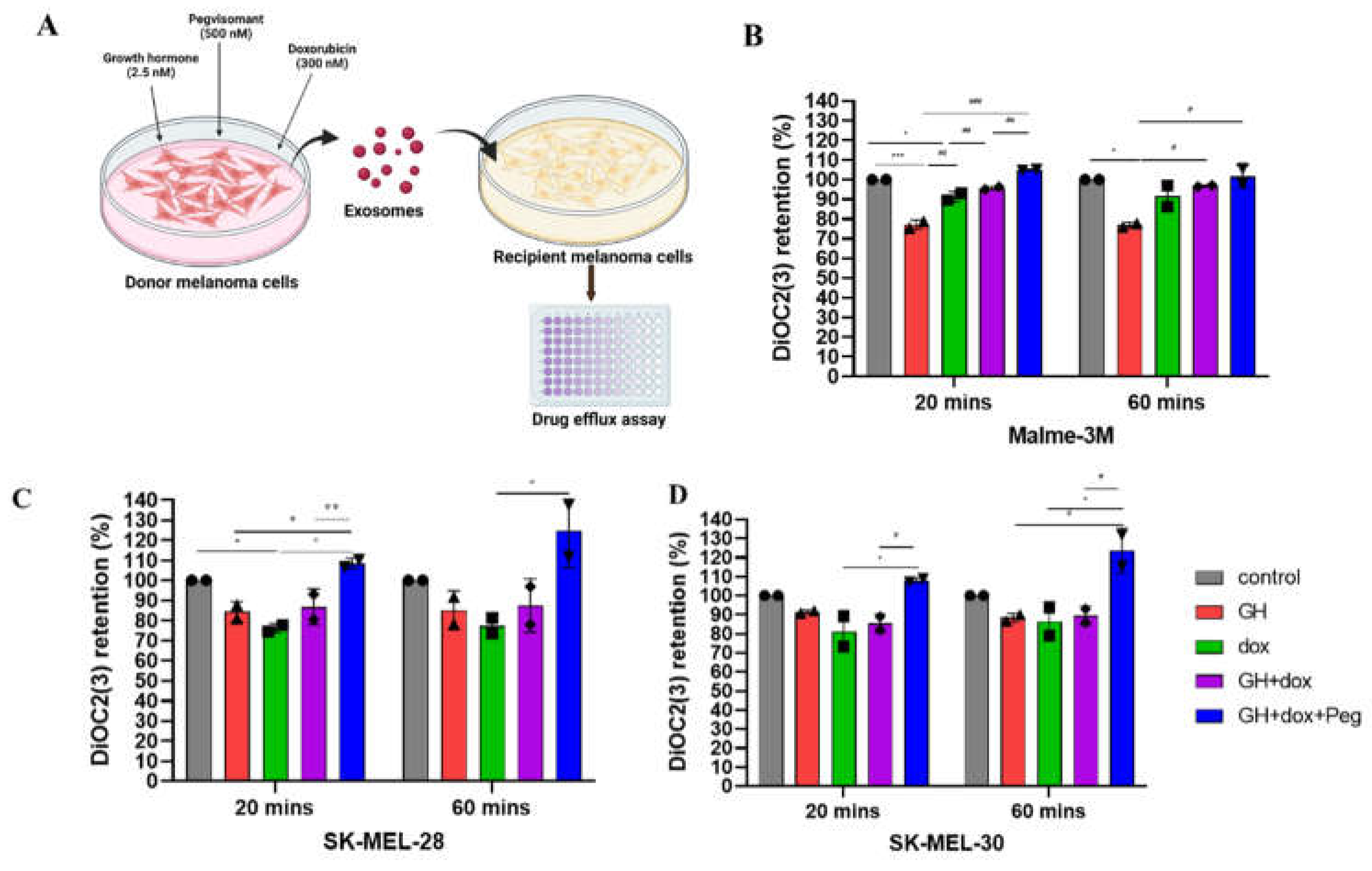
Figure 2.
GH elevates ABC efflux pump levels in melanoma tumor-derived exosomes and corresponding recipient cells. A. Protein levels of ABCC1, ABCC2, ACCB1, ABCG2 in exosomes isolated from human melanoma cells, Malme-3M, SK-Mel-28, and SK-MEL30, 96-hour post treatment with 50 ng/ml GH independently or in combination with EC50 dosage of doxorubicin, 500nM pegvisomant. B-E. Blots were quantified using ImageJ and protein levels were normalized using β-actin as a control and presented as relative protein expression. Blots from three independent experiments are presented as the mean ± SD and p <0.05 (* / #), p<0.005 (** / ##), p<0.0005 (*** / ###). F. Protein levels of ABCC1, ACCB1, ABCG2 in human melanoma cells: Malme-3M, SK-Mel-28, and SK-MEL30, treated with 20 μg/ml exosomes from above mentioned melanoma cells. G-I. Blots were quantified using ImageJ and expressions were normalized against β-actin and presented as relative protein expression. Blots from three independent experiments are presented as the mean ± SD and p <0.05 (* / #), p<0.005 (** / ##), p<0.0005 (*** / ###).
Figure 2.
GH elevates ABC efflux pump levels in melanoma tumor-derived exosomes and corresponding recipient cells. A. Protein levels of ABCC1, ABCC2, ACCB1, ABCG2 in exosomes isolated from human melanoma cells, Malme-3M, SK-Mel-28, and SK-MEL30, 96-hour post treatment with 50 ng/ml GH independently or in combination with EC50 dosage of doxorubicin, 500nM pegvisomant. B-E. Blots were quantified using ImageJ and protein levels were normalized using β-actin as a control and presented as relative protein expression. Blots from three independent experiments are presented as the mean ± SD and p <0.05 (* / #), p<0.005 (** / ##), p<0.0005 (*** / ###). F. Protein levels of ABCC1, ACCB1, ABCG2 in human melanoma cells: Malme-3M, SK-Mel-28, and SK-MEL30, treated with 20 μg/ml exosomes from above mentioned melanoma cells. G-I. Blots were quantified using ImageJ and expressions were normalized against β-actin and presented as relative protein expression. Blots from three independent experiments are presented as the mean ± SD and p <0.05 (* / #), p<0.005 (** / ##), p<0.0005 (*** / ###).
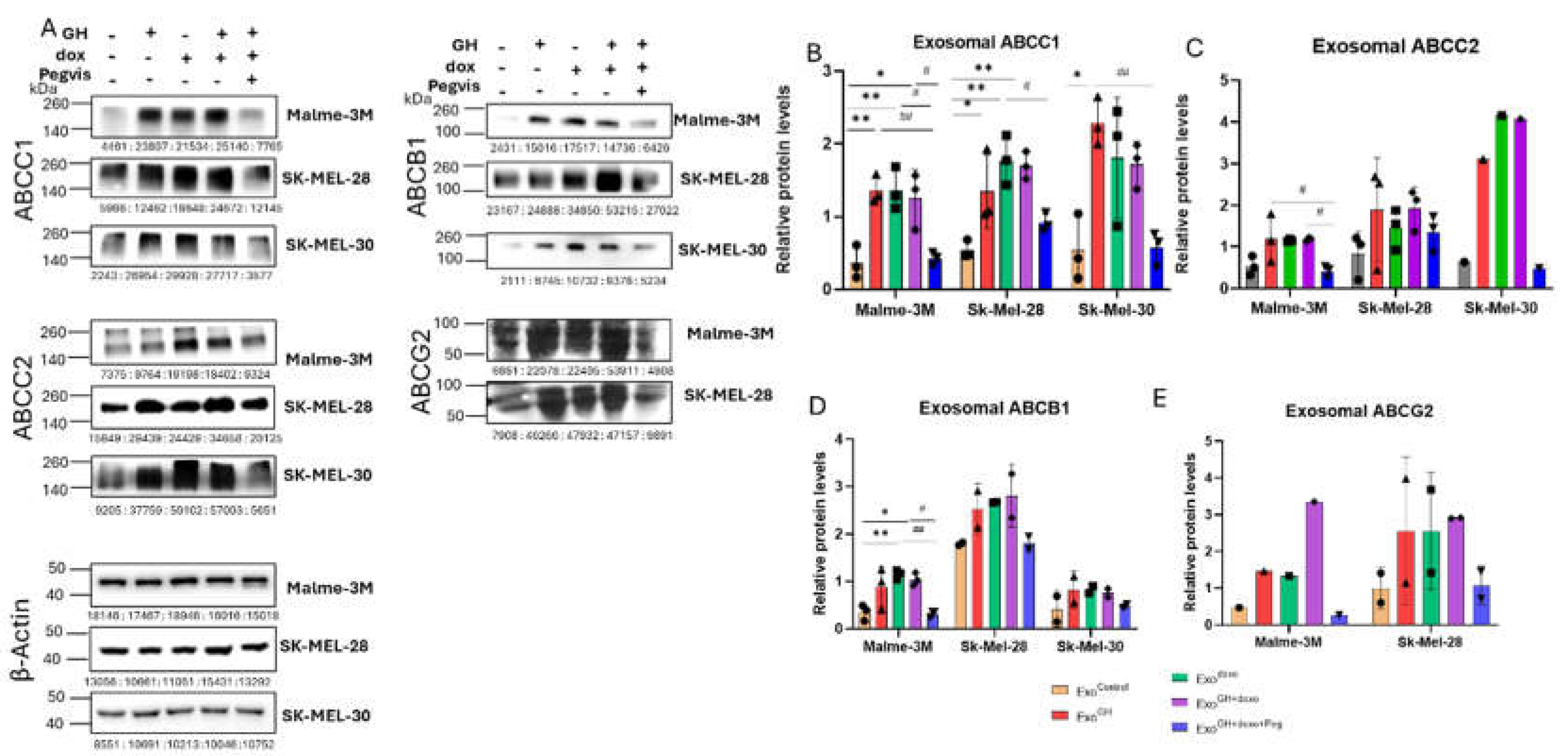
Figure 3.
Blocking autocrine/paracrine GH action in melanoma suppresses ABC efflux pumps in tumor-derived exosomes. A. Protein levels of ABCC1 and ABCB1 in exosomes isolated from human melanoma cells, Malme-3M, SK-Mel-28, and SK-MEL30, 96-hour post treatment with 500 nM pegvisomant and EC50 dosage of doxorubicin independently or in combination. B, C. Blots were quantified using ImageJ and expressions were normalized against β-actin and presented as relative protein expression. Blots from two independent experiments are presented as the mean ± SD and p <0.05 (*), p<0.005 (**).
Figure 3.
Blocking autocrine/paracrine GH action in melanoma suppresses ABC efflux pumps in tumor-derived exosomes. A. Protein levels of ABCC1 and ABCB1 in exosomes isolated from human melanoma cells, Malme-3M, SK-Mel-28, and SK-MEL30, 96-hour post treatment with 500 nM pegvisomant and EC50 dosage of doxorubicin independently or in combination. B, C. Blots were quantified using ImageJ and expressions were normalized against β-actin and presented as relative protein expression. Blots from two independent experiments are presented as the mean ± SD and p <0.05 (*), p<0.005 (**).
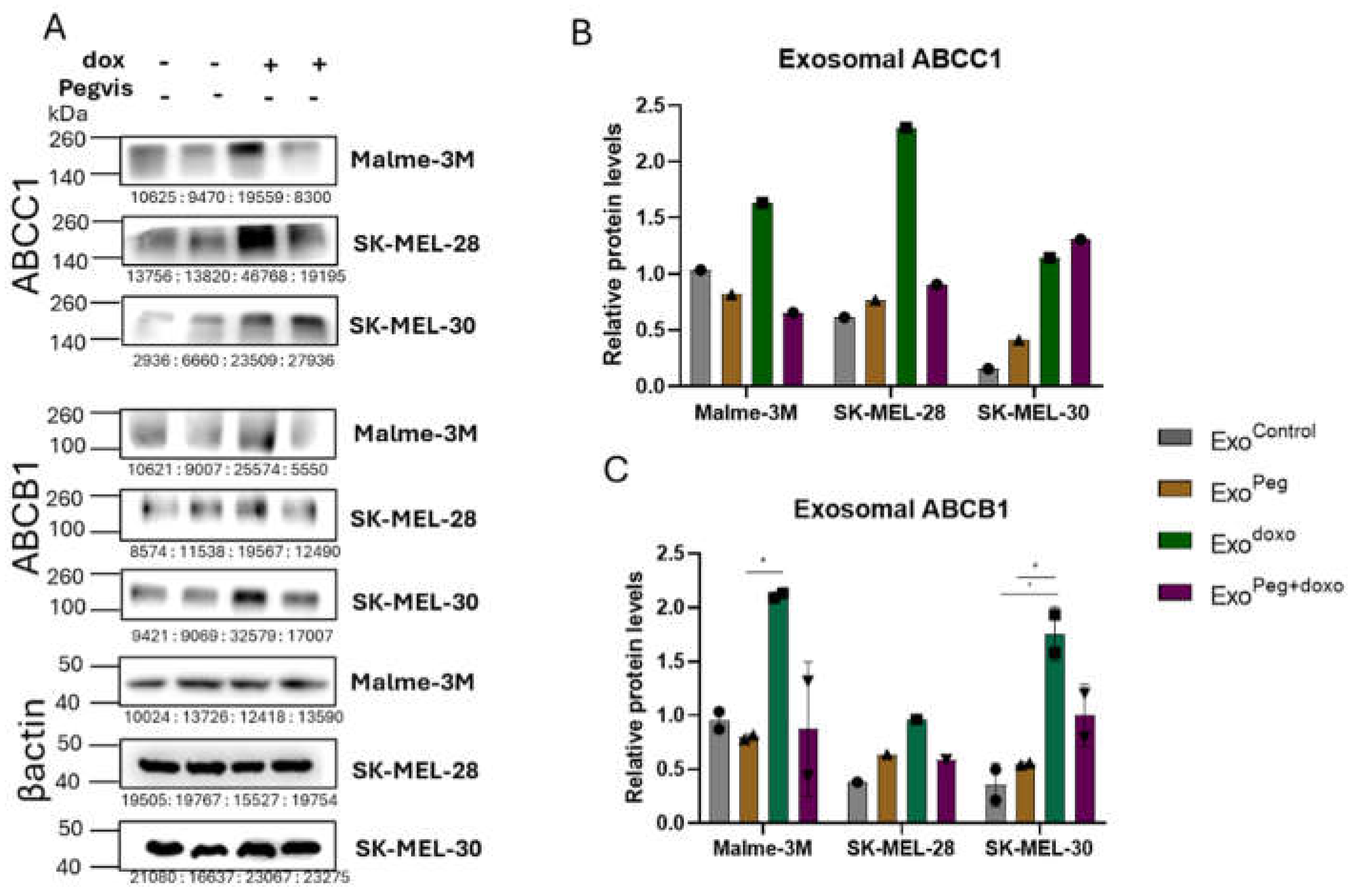
Figure 4.
Pegvisomant attenuates exosome induced cell migration in melanoma. Changes in wound closure following administration with 20 μg/ml exosomes, isolated from melanoma cells treated with 50 ng/ml GH independently or in combination with EC50 dosage of doxorubicin doxorubicin and 500nM pegvisomant. Representative images for cell migration at the indicated time points are shown for SK-MEL-28 (A), SK-MEL-30 (C), and their respective quantifications (B, D). Three independent experiments were performed and presented as the mean ± SD and p <0.05 (*) and p<0.005 (**).
Figure 4.
Pegvisomant attenuates exosome induced cell migration in melanoma. Changes in wound closure following administration with 20 μg/ml exosomes, isolated from melanoma cells treated with 50 ng/ml GH independently or in combination with EC50 dosage of doxorubicin doxorubicin and 500nM pegvisomant. Representative images for cell migration at the indicated time points are shown for SK-MEL-28 (A), SK-MEL-30 (C), and their respective quantifications (B, D). Three independent experiments were performed and presented as the mean ± SD and p <0.05 (*) and p<0.005 (**).
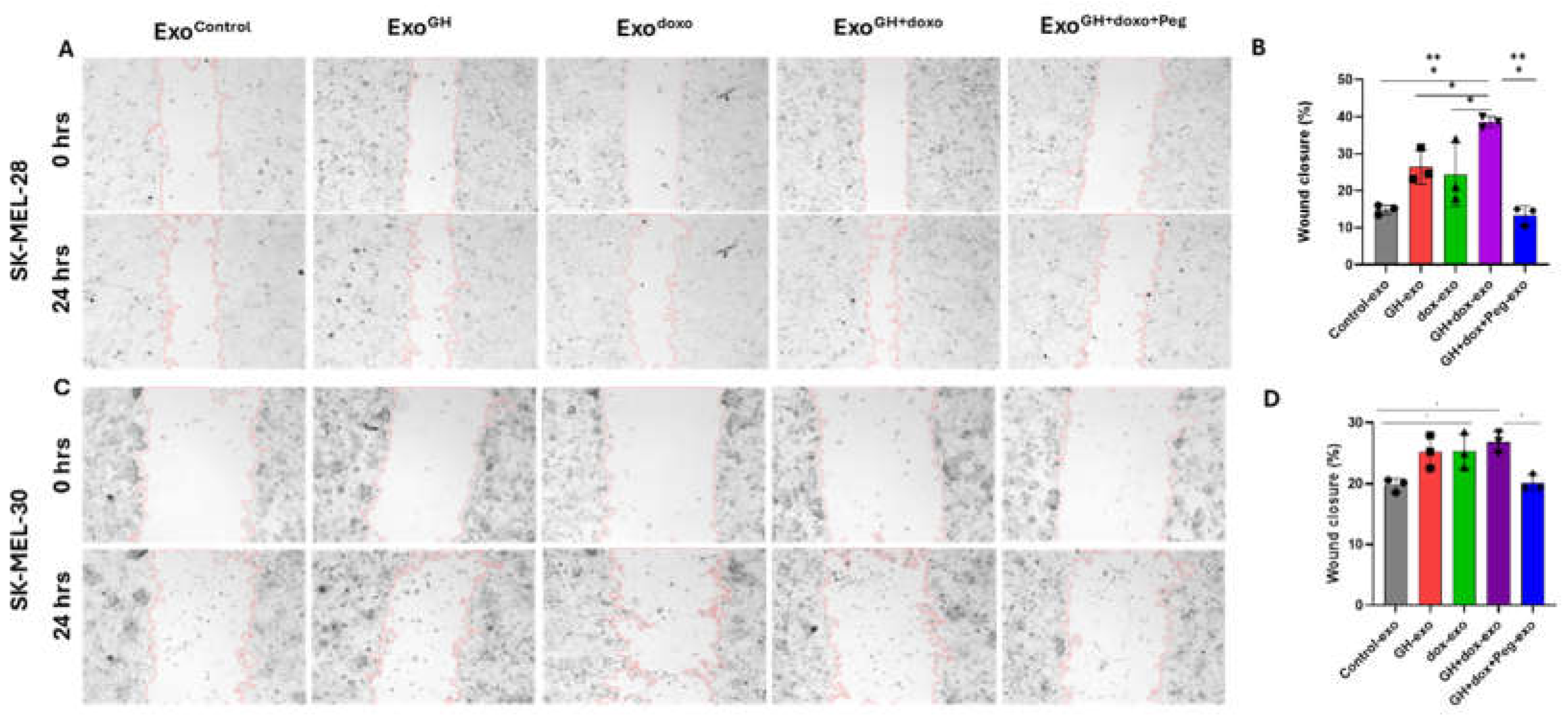
Figure 5.
GH elevates N-cadherin and MMP2 in melanoma-derived exosomes and elevates N-cadherin in corresponding recipient cells. A. Protein levels of N-cadherin and MMP2 in exosomes isolated from human melanoma cells, Malme-3M, SK-Mel-28, and SK-MEL30, 96-hour post treatment with 50 ng/ml GH independently or in combination with EC50 dosage of doxorubicin and 250 nM pegvisomant. B, C. Blots were quantified using ImageJ and expression was normalized using β-actin and presented as relative protein expression. Blots from two independent experiments are presented as the mean ± SD and p <0.05 (* / #), p<0.005 (** / ##), p<0.0005 (*** / ###). D. Protein levels of N-cadherin and MMP2 in human melanoma cells, Malme-3M, SK-Mel-28, and SK-MEL30, treated with 20 μg/ml exosomes from aforementioned treated melanoma cells, E, F. Blots were quantified using ImageJ and expression was normalized against β-actin and presented as relative protein expression. Blots from three independent experiments are presented as the mean ± SD and p <0.05 (* / #), p<0.005 (** / ##), p<0.0005 (*** / ###).
Figure 5.
GH elevates N-cadherin and MMP2 in melanoma-derived exosomes and elevates N-cadherin in corresponding recipient cells. A. Protein levels of N-cadherin and MMP2 in exosomes isolated from human melanoma cells, Malme-3M, SK-Mel-28, and SK-MEL30, 96-hour post treatment with 50 ng/ml GH independently or in combination with EC50 dosage of doxorubicin and 250 nM pegvisomant. B, C. Blots were quantified using ImageJ and expression was normalized using β-actin and presented as relative protein expression. Blots from two independent experiments are presented as the mean ± SD and p <0.05 (* / #), p<0.005 (** / ##), p<0.0005 (*** / ###). D. Protein levels of N-cadherin and MMP2 in human melanoma cells, Malme-3M, SK-Mel-28, and SK-MEL30, treated with 20 μg/ml exosomes from aforementioned treated melanoma cells, E, F. Blots were quantified using ImageJ and expression was normalized against β-actin and presented as relative protein expression. Blots from three independent experiments are presented as the mean ± SD and p <0.05 (* / #), p<0.005 (** / ##), p<0.0005 (*** / ###).
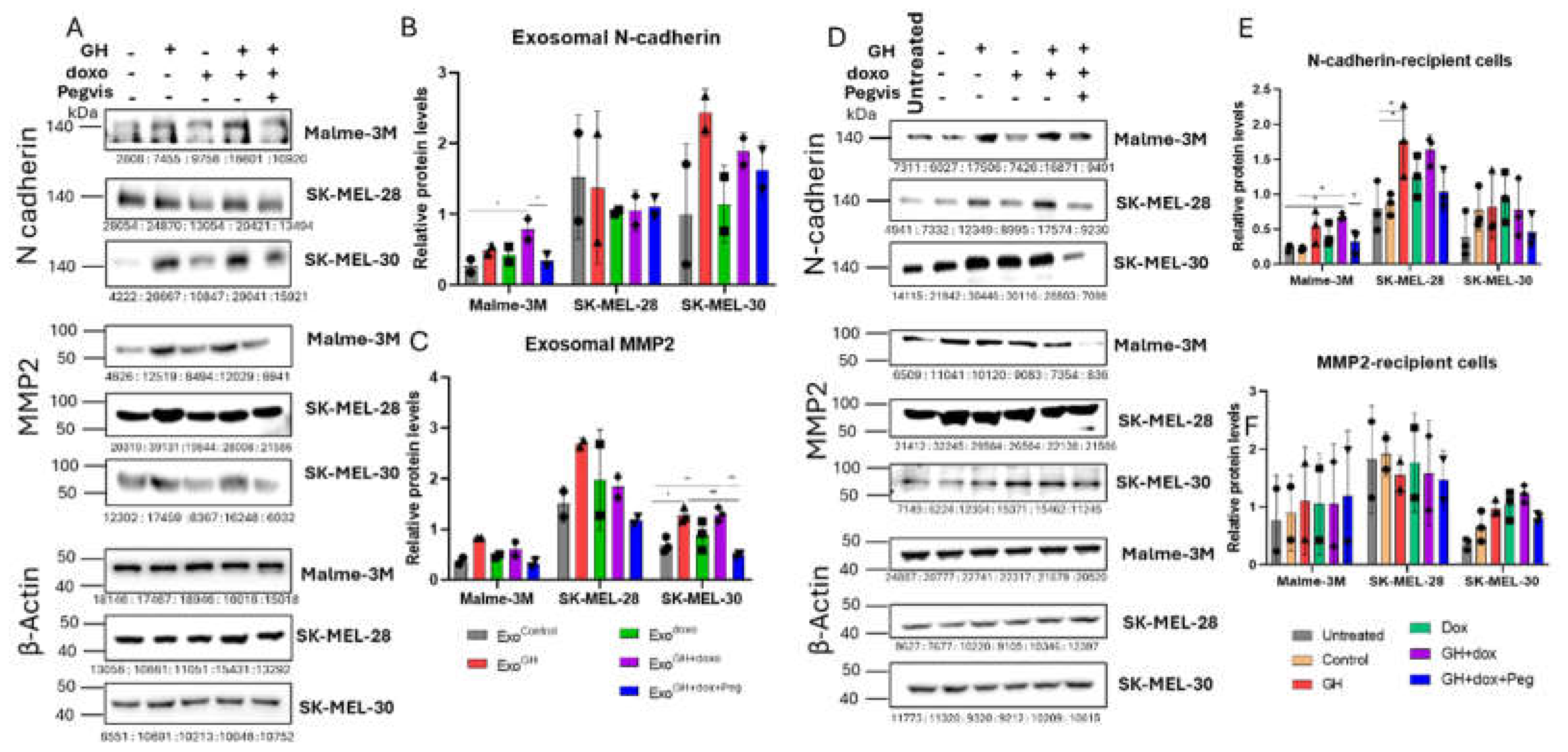

Table 1.
Average fold change in ABC transporter levels in exosomes and recipient cells.
| ABC transporter | Cell lines | Exosomes | ||||
|---|---|---|---|---|---|---|
| Control | GH | Doxo | Doxo+GH | Doxo+GH+Peg | ||
| ABCC1 | Malme-3M | 1.0 | 5.0 | 5.4 | 4.9 | 1.4 |
| SK-MEL-28 | 1.0 | 2.4 | 3.3 | 3.3 | 1.7 | |
| SK-MEL-30 | 1.0 | 7.2 | 6.0 | 6.1 | 1.4 | |
| ABCC2 | Malme-3M | 1.0 | 2.8 | 2.4 | 2.5 | 0.8 |
| SK-MEL-28 | 1.0 | 2.2 | 2.5 | 3.4 | 2.3 | |
| ABCB1 | SK-MEL-30 | 1.0 | 3.3 | 3.9 | 5.6 | 1.9 |
| Malme-3M | 1.0 | 3.2 | 3.9 | 3.5 | 1.2 | |
| ABCG2 | SK-MEL-28 | 1.0 | 1.4 | 1.5 | 1.6 | 1.0 |
| SK-MEL-30 | 1.0 | 2.7 | 3.2 | 2.9 | 1.9 | |
| Recipient cells | ||||||
| ExoControl | ExoGH | ExoDoxo | ExoDoxo+GH | ExoDoxo+GH+Peg | ||
| ABCC1 | Malme-3M | 1.0 | 2.0 | 2.0 | 1.6 | 0.5 |
| SK-MEL-28 | 1.0 | 1.0 | 1.6 | 1.4 | 0.8 | |
| ABCB1 | Malme-3M | 1.0 | 1.5 | 1.8 | 1.5 | 0.7 |
| SK-MEL-28 | 1.0 | 1.0 | 1.3 | 1.1 | 0.5 | |
| SK-MEL-30 | 1.0 | 1.5 | 2.1 | 1.5 | 0.9 | |
| ABCG2 | Malme-3M | 1.0 | 3.1 | 3.7 | 5.0 | 2.7 |
| SK-MEL-28 | 1.0 | 1.6 | 2.9 | 3.2 | 0.9 | |
| SK-MEL-30 | 1.0 | 1.7 | 1.3 | 1.5 | 1.8 | |
Average fold change is calculated based on corresponding controls.
Table 2.
Average fold change in MMP2 and N-cadherin levels in exosomes and recipient cells.
| ABC transporter | Cell lines | Exosomes | ||||
|---|---|---|---|---|---|---|
| Control | GH | Doxo | Doxo+GH | Doxo+GH+Peg | ||
| MMP2 | Malme-3M | 1.0 | 1.6 | 1.6 | 2.0 | 1.0 |
| SK-MEL-28 | 1.0 | 2.0 | 2.1 | 2.3 | 1.4 | |
| SK-MEL-30 | 1.0 | 1.9 | 1.4 | 2.0 | 0.7 | |
| N-cadherin | Malme-3M | 1.0 | 1.0 | 2.0 | 3.5 | 1.6 |
| SK-MEL-28 | 1.0 | 0.8 | 0.8 | 0.8 | 1.9 | |
| SK-MEL-30 | 1.0 | 4.5 | 1.7 | 4.0 | 2.9 | |
| Recipient cells | ||||||
| ExoControl | ExoGH | ExoDoxo | ExoDoxo+GH | ExoDoxo+GH+Peg | ||
| MMP2 | Malme-3M | 1.0 | 1.2 | 1.1 | 1.0 | 0.8 |
| SK-MEL-28 | 1.0 | 0.8 | 1.9 | 0.8 | 0.8 | |
| SK-MEL-30 | 1.0 | 1.6 | 1.8 | 2.0 | 1.4 | |
| N-cadherin | Malme-3M | 1.0 | 2.5 | 1.9 | 3.1 | 1.5 |
| SK-MEL-28 | 1.0 | 2.0 | 1.4 | 1.9 | 1.2 | |
| SK-MEL-30 | 1.0 | 1.0 | 1.2 | 1.0 | 0.7 | |
Average fold change is calculated based on corresponding controls.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



