Submitted:
02 July 2024
Posted:
02 July 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
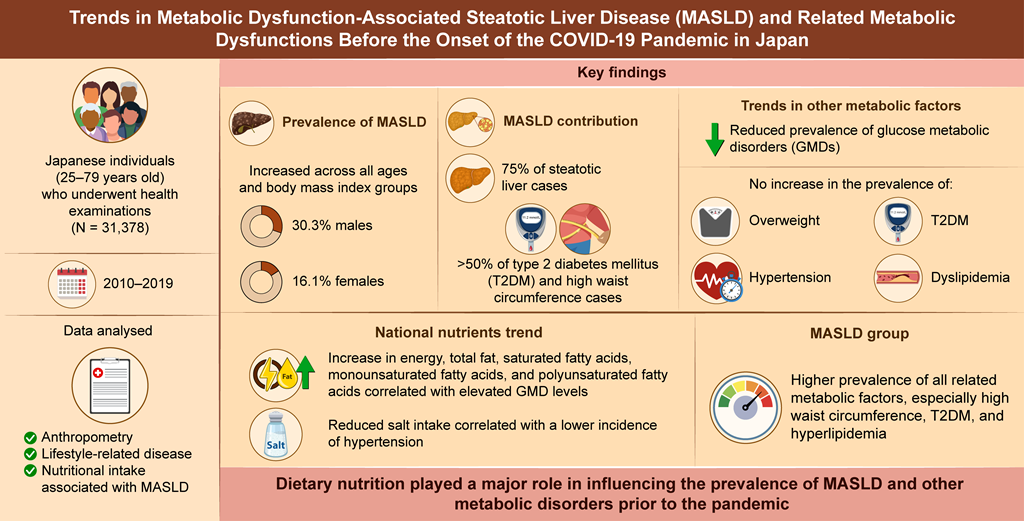
Background and Objectives: The trends in metabolic dysfunction-associated steatotic liver disease (MASLD) and related metabolic dysfunctions in Japan is unknown. Thus, we aimed to clarify the trends of these before the novel coronavirus disease 2019 pandemic in Japan. Materials and Methods: We included Japanese individuals aged 25-79 years who underwent health examinations at our center. We analyzed anthropometry, lifestyle-related disease, and nutritional intake in relation to MASLD trends from 2010-2019. Results: The prevalence of MASLD increased in all ages and body mass index (BMI) classes, reaching 30.3% in males and 16.1% in females, with MASLD accounting for 75% of steatotic liver cases and more than half of all type 2 diabetes mellitus (T2DM) and high waist circumference (HWC) cases. The increase in the prevalence of MASLD was due to an increase in that of steatotic liver itself, and there was no increase in the prevalence of other factors, such as overweight, T2DM, hypertension, and dyslipidemia. The prevalence of glucose metabolic disorders (GMDs) and hypertension decreased. National nutritional data showed an increase in energy intake, total fat, saturated fatty acids, monounsaturated fatty acids, and polyunsaturated fatty acids, which correlated with a decrease in GMDs. Salt intake also decreased, which correlated with hypertension. The MASLD group had a higher prevalence of all related metabolic factors than the non-MASLD group, especially HWC, T2DM, and hyperlipidemia. Conclusion: The prevalence of MASLD increased with that of steatotic liver, regardless of age or BMI. A relationship between increased dietary fat, increased steatotic liver, and decreased GMDs was suggested.
Keywords:
metabolic dysfunction-associated steatotic liver disease
; epidemiology
; dietary nutrient
; metabolic syndrome
; lifestyle-related disease
; prediabetes
; dietary fat
1. Introduction
The International Consensus Group proposed a change in terminology from “fatty liver disease” to “steatotic liver disease” (SLD) and the concept of metabolic dysfunction-associated SLD (MASLD) as an alternative to nonalcoholic fatty liver disease (NAFLD) [1,2]. While NAFLD is a diagnosis of exclusion to rule out secondary causes of liver disease (such as alcohol or viruses), this revision is significant in that it provides a better understanding of the etiology of the disease and eliminates the associated stigma. MASLD is a non-alcoholic SLD characterized by one or more metabolic dysfunctions, while NAFLD is associated with many metabolic dysfunctions [3]. Although there are numerous cross-sectional epidemiological studies on metabolic dysfunctions associated with NAFLD, there have been relatively few longitudinal epidemiological studies.
In this study, we sought to examine trends in MASLD and related metabolic dysfunctions before the onset of the novel coronavirus disease 2019 (COVID-19) pandemic in Japan. We found that the prevalence of MASLD increased with that of steatotic liver, regardless of age or body mass index (BMI). In addition, pre-diabetes decreased in related metabolic disorders, suggesting that dietary nutrition may play a role in this process.
2. Materials and Methods
2.1. Study Population and Design
Japanese individuals aged 25-79 years who underwent physical examinations, physiological examinations, abdominal ultrasonography (US), and blood screening examinations at the Sasaki Foundation Shonan Health Screening Center in the Kanto region during the fiscal years (FYs) 2010-2019 (April to March of the following year) were included in this study. Participants were included if they met the following criteria: (1) available BMI data, (2) available fasting blood glucose or glycated hemoglobin (HbA1c) data, and (3) known alcohol intake. Of the 48,225 examinees, 31,378 (16,238 males and 15,140 females) met the inclusion criteria. The characteristics of the subjects are shown in Table 1. The study protocol was approved by the Human Ethics Review Committee of the Sasaki Foundation (Tokyo, Japan) (certification no. 19728). Informed consent was obtained on an opt-out basis.
MASLD was diagnosed according to the NAFLD Nomenclature Consensus Group criteria [1]. High waist circumference (HWC) was defined as ≥ 85 cm for males and ≥ 90 cm for females, according to the Japanese metabolic syndrome diagnostic criteria [4]. Age was classified into three categories according to the criteria of the Ministry of Health, Labour and Welfare: 25-44 years as mature age, 45-64 years as middle age, and ≥ 65 years as old age. BMI was classified into the following categories according to the recommendation of the Western Pacific Region of the World Health Organization criteria that pertain to obesity: < 23.0 kg/m2 as normal, ≥ 23.0 kg/m2 as overweight, 23-24.9 kg/m2 as pre-obese (pre-Ob), 25-29.9 kg/m2 as obese-I (Ob-I), and ≥ 30 kg/m2 as obese-II (Ob-II).
All lifestyle-related diseases (LRDs; hypertension, glucose metabolism disorders [GMDs], and dyslipidemia) diagnoses were defined according to the International Consensus Group criteria for metabolic dysfunction [1] and were defined as those who were currently being treated with medications or met the following criteria: hypertension, defined as systolic blood pressure > 130 mmHg and/or diastolic blood pressure > 85 mmHg; GMDs, defined as fasting plasma glucose (FPG) > 100 mg/dL or HbA1c > 5.7%; type 2 diabetes mellitus (DM) (T2DM), defined as FPG > 126 mg/dL or HbA1c > 6.5%; prediabetes, defined as a FPG ≥ 100 mg/dL and < 126 mg/dL or HbA1c ≥ 5.7% and < 6.5% [5]; and dyslipidemia, defined as triglyceride levels of ≥ 150 mg/dL or a high-density lipoprotein cholesterol level of < 40 mg/dL for males and < 50 mg/dL for females.
2.2. Physical Examinations and Serum Biochemistry Analyses
Body weight and height were obtained for both sets of participants, and BMI was calculated. Skilled nurses measured waist circumference at the navel level while the participants were in a standing position. Venous blood samples were obtained from all participants from 8-10 AM following a 12-h overnight fast.
2.3. Protocol for Abdominal US and Definition of Fatty Liver
All participants underwent abdominal US to assess steatotic livers. The liver parenchyma of all patients was examined using a conventional convex array transducer. The presence of steatotic change was defined as increased echogenicity of the liver parenchyma compared with the renal parenchyma (bright liver and liver-kidney contrast), deep US attenuation in the right lobe of the liver (deep attenuation), and/or poor visualization of the hepatic vein (vascular blurring); the first two were considered definitive criteria, while the latter two were considered necessary. The US systems used were the Aloka SSDα5, Aloka Pro Soundα7, Aloka Pro Soundα7, and Aloka ARIETTA E50 (Hitachi Aloka Medical, Tokyo, Japan) with 3.5 MHz convex array transducers. Experienced sonographers trained by gastroenterologists performed all examinations. The technical parameters were adjusted for each subject using a standard US protocol. A board-certified gastroenterologist from the Japanese Society of Gastroenterology reviewed the images and diagnosed steatotic liver without referring to any other personal data of the participant.
2.4. Dietary Data Source
We used dietary data from the National Health and Nutritional Survey (NHNS) of Japan conducted by the National Institute of Health and Nutrition [6] The NHNS is a cross-sectional household interview and examination survey conducted annually since 1945 by local health centers under the supervision of the Ministry of Health, Labour and Welfare of Japan [7]. Details of the survey design have been described elsewhere [8]. This survey is conducted annually throughout Japan in November.
The number of households participating in the survey between 2010 and 2019 ranged from 2,836 (2019) to 12,750 (2012), with a response rate of approximately 50%. A total of 118,840 individuals participated in the survey between 2010 and 2019. This study used information from 98,403 individuals (4,927-26,726/year; average 9,840/year) aged ≥ 20 years in the NHNS survey to match the age distribution of the study population. Specifically, the number of people in each age group in the NHNS was converted to the number in the study population and the mean dietary nutrient level for each year was recalculated.
2.5. Statistical Analysis
Trend analyses of the prevalence of MASLD, LRDs, obesity, HWC, dietary nutrient intake, and MASLD were performed using Spearman’s rank correlation, and comparisons between MASLD and non-MASLD were performed by the Chi-square and student’s t-test with Stat Flex, version 7 (Artec, Osaka, Japan). A p value < 0.05 was considered statistically significant.
In addition, scatter plots were generated for the correlation of dietary nutrient intake and GMDs using Microsoft Excel, version 2403 (Microsoft Corporation, Redmond, WA, USA). The coefficients of determination (R2) were calculated, and the coefficients were interpreted according to Schober et al. [9].
3. Results
3.1. Trends in MASLD and Steatotic Liver
The prevalence of MASLD increased from 21.8% to 30.3% for males and from 10.4% to 16.1% for females over the 10-year period ending in FY 2018-2019 (Figure 1). This increase was linked to the prevalence of steatotic liver itself and of NAFLD (ρ = 1.0, p < 0.05 for both sexes), with the most recent MASLD overlap rates of 71.8% for steatotic liver and 95.3% for NAFLD in males and 86.8% and 94.1%, respectively, in females.
3.2. Trends in MASLD by Age and BMI
The prevalence of MASLD by age group increased in all age groups in males, especially in mature (from 21.9% to 29.1%) and middle age (from 22.9% to 32.5%) (p < 0.05) (Figure 2A and B). The prevalence also increased in females of all age groups (mature: 5.3% to 7.2%, middle: 13.1% to 19.3%, and old: 13.2% to 25.1%; p < 0.05).
The MASLD prevalence according to BMI increased in all BMI groups (p < 0.05), except for the Ob-II group in males, especially in the pre-Ob (18.8% to 29.5%) and Ob-I groups (40.9% to 54.3%) (Figure 2C and D). In females, there was a significant increase in the pre-Ob (from 14.1% to 27.1%), Ob-I (from 34.3% to 47.5%), and Ob-II (from 62.2% to 81.4%) groups (p < 0.05).
3.3. Trends in MASLD Factors
Regarding physical factors, the prevalence of steatotic liver increased in both males and females (from 29.4% to 43.4% in males and from 11.3% to 18.5% in females; p < 0.005) (Figure 3). However, there was no significant change in the prevalence of overweight (range: males, 57.2-58.9% and females, 31.0-31.5%) and HWC (range: males, 38.9-42.4% and females, 8.7-10.5%).
Regarding metabolism-related factors, both males (62.0% to 55.7%) (p = 0.0381) and females (45.0% to 31.4%) (p = 0.0042) had a decreased prevalence of GMDs, and the proportion of participants with prediabetes decreased (males: 52.1% to 46.0%, p = 0.0323 and females: 41.8 % to 31.4%, p = 0.0037). The prevalence of hypertension also showed a decreasing trend from 47.0% to 37.0% (p = 0.0601) in males, and a significant decrease from 26.5% to 19.8% (p = 0.0102) in females.
3.4. Nutritional Intake and Exercise Habits in the NHNS and Their Relationship to GMDs and Hypertension
Trends in nutrient intake according to the NHNS showed an increase in energy (EN) intake for both sexes (Table 2); a decreasing but not significant trend in carbohydrate (CHO) intake; and an increase in total fat, saturated fatty acid (SFA), monounsaturated fatty acid (MUFA), and polyunsaturated fatty acid (PUFA) intake for both sexes. Salt intake tended to decrease in both sexes, but was only significant in males. Exercise habits did not significantly change in either sex.
Nutrient intakes are listed only for the first and last fiscal year of the five periods from 2010-11 to 2018-19 that were analyzed by Spearman’s rank correlation test. Carbohydrate/En %: percentage of energy intake from carbohydrates, SFA: saturated fatty acid, MUFA: monounsaturated fatty acid, PUFA: polyunsaturated fatty acid (total of n-3 and n-6 PUFA)
EN intake showed an increasing trend but a strong inverse correlation with the prevalence of GMDs in males (R2 = 0.5146) and GMDs and prediabetes in females (R2 = 0.806 and R2 = 0.7925, respectively), and a moderate inverse correlation with the prevalence of prediabetes in males (R2 = 0.4633) (Figure 4a and b). CHO levels were strongly inversely correlated with the prevalence of GMDs and prediabetes in females (R2 = 0.7237 and R2 = 0.7238, respectively) (Figure 4d). Total fat showed a moderate inverse correlation with the prevalence of GMDs and prediabetes in males (R2 = 0.5848 and R2 = 0.5987, respectively) and a strong inverse correlation in females (R2 = 0.918 and R2 = 0.9109, respectively) (Figure 4e and f). SFA and MUFA showed moderate correlations in males (SFA: R2 = 0.4305 and R2 = 0.446 and MUFA: R2 = 0.4444 and R2 = 0.4583, respectively) (Figure 4g and i) and strong inverse correlations with the prevalence of GMDs and prediabetes in females (SFA: R2 = 0.7714 and R2 = 0.7615 and MUFA: R2 = 0.7346 and R2 = 0.7244, respectively) (Figure 4h and j). PUFA showed weak correlations in males (R2 = 0.3561 and R2 = 0.3765, respectively) and strong inverse correlations with the prevalence of GMDs and prediabetes in females (R2 = 0.7323 and R2 = 0.7194, respectively) (Figure 4k and l).
Salt intake was significantly reduced in males but weakly correlated with the prevalence of hypertension (R2 = 0.342). However, there was a moderate correlation with a reduced prevalence of hypertension in females (R2 = 0.483), where the reduction in salt intake was not significant (Figure 5a and b).
3.5. Clinical Features of MASLD
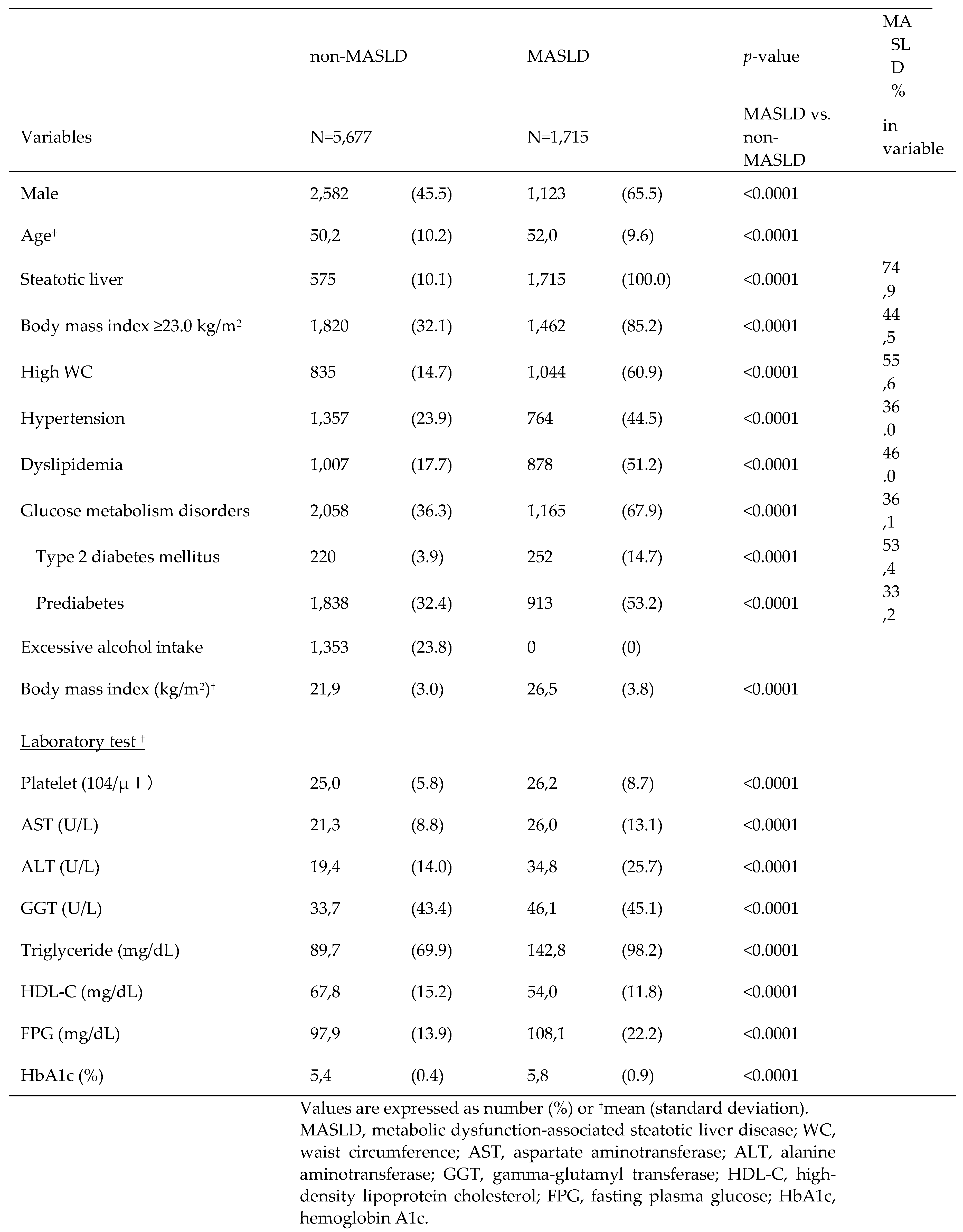
The MASLD group had a higher percentage of males (65.5%) (Table 3), mean age (52 years), and prevalence of overweight and HWC (85.2% and 60.9%, respectively) than did the non-MASLD group. Hypertension, dyslipidemia, T2DM, and prediabetes were present in 44.5%, 51.2%, 14.7%, and 53.2% of participants, respectively. In the MASLD group, 46.6% of patients had dyslipidemia and 53.4% had T2DM. BMI and various laboratory values other than platelet counts deviated more frequently from the reference values in patients with MASLD than in those without.
4. Discussion
This study revealed the following points. First, the prevalence of MASLD increased in almost all age and BMI groups of both sexes before the COVID-19 pandemic, which was associated with an increase in the prevalence of steatotic liver. Second, both males and females with MASLD-related LRDs exhibited a reduced prevalence of prediabetes. This was inversely correlated with the total fat and various fatty acid (FA) intakes in the national data. Third, MASLD was more prevalent in males than in individuals without MASLD, and individuals with MASLD were older and exhibited a higher prevalence of overweight HWC and LRDs than individuals without MASLD.
The prevalence of MASLD increased in almost all age and BMI groups as the prevalence of steatotic liver increased. In other words, MASLD is composed of multiple physical and metabolic factors, but no factors other than steatotic liver were found to be associated with the increased prevalence of MASLD. The MASLD prevalence trend was similar to that of NAFLD and steatotic liver, and as 96% of MASLD cases were NAFLD, the increase in the prevalence of MASLD was likely due to an increase in the prevalence of steatotic liver resulting from imbalanced fat intake, as previously reported [10]. In this study, we also referred to national data on exercise habits; however, there was no statistical change in the percentage of habitual exercisers from 2010 to 2019. Therefore, dietary nutrition seemed to play a major role in the increase in the prevalence of steatotic liver and MASLD in both males and females, with little impact of exercise habits.
It is noteworthy that the prevalence of GMDs decreased despite an increase in the prevalence of MASLD in both males and females. The decrease in the prevalence of GMDs was due to a decrease in the prevalence of prediabetes in both sexes, whereas the prevalence of T2DM remained unchanged. However, the prevalence of DM in Japan slightly increased in males and decreased in females, from 12.6% to 13.8% in males and from 7.8% to 7.7% in females, in the 2009 and 2019 national surveys, respectively, as noted by Goto et al. [11]. In addition, the World Bank Report [12] showed that the prevalence of DM in Japan decreased from 7.7% in 2011 to 6.6% in 2021. Although our data were limited to one region and the majority (55.9-58.4%) of the total population throughout the study period was middle-aged, which differs from the age structure of the Japanese general population, we do not consider this result unique in terms of a decrease in the prevalence of prediabetes or GMDs. Liver steatosis and glucose intolerance are closely linked and are mutually promoting factors. Therefore, the increase in the prevalence of steatotic liver and decrease in the prevalence of GMDs are anomalous, and we focused on dietary changes in the Japanese population as the cause.
National data showed a slight increase in EN intake over the past decade for both males and females, but a decreasing trend in CHO intake and the CHO/EN ratio. According to the guidelines of Hauner et al. [13], there is insufficient evidence of an association between T2DM risk and CHO intake and no association with intake ratio, and in a dose-response meta-analysis by Hosseini et al. [14], a CHO/EN ratio of 45-65% was not associated with T2DM risk. However, it is unknown whether prediabetes, and the possibility that this change contributed to the decrease in the prevalence of prediabetes in this study, can be ruled out.
On the other hand, dietary fat is increasing, and high-fat diets have been reported to induce insulin resistance and T2DM [15,16]. Furthermore, SFA induces insulin resistance [17]. Conversely, high fat does not contribute to the risk of T2DM [18,19] and an inverse association between total lipids and T2DM or prediabetes has recently been reported [20,21]. In addition, certain FAs have been reported to improve or suppress GMDs [19,22,23,24]. In a multiple-treatment meta-regression, Imamura et al. [25] demonstrated that the conversion of CHO to SFA lowered fasting insulin levels, the conversion to MUFA lowered HbA1c and homeostasis model assessment of insulin resistance, and the conversion to PUFA improved these outcomes, in addition to FPG and C-peptide.
In a dose-response meta-analysis, Neuenschwander et al. [18] reported a dose-dependent effect of vegetable fat, SFA, and n-6 FA on T2DM risk reduction. In the NHNS, SFA, MUFA, and PUFA intakes in Japan showed an increasing trend, and this change may have been responsible for the reduction in the prevalence of prediabetes in this study. Lipids are also closely related to the development of steatotic liver, and it has been reported that SFA directly induces hepatic steatosis [26,27], whereas MUFA and n-6 FA are both reported to act in an inhibitory manner [28,29]. Therefore, it may be possible to control both hepatic steatosis and abnormal glucose metabolism by maintaining an appropriate balance between the intake of these lipids and EN.
Hypertension decreased and salt intake was weakly correlated with hypertension in males and moderately correlated in females. Although several causes of hypertension exist, salt intake is extremely important. Salt intake decreased more slowly in females, but was correlated with a decrease in the prevalence of hypertension in females. This may be largely due to the lower absolute salt intake in females.
Individuals with MASLD had a significantly higher frequency of overweight, HWC, hypertension, and T2DM than individuals without MASLD. MASLD and NAFLD are almost identical [30] and their clinical backgrounds are similar. In a recent large Japanese study by Fujii et al. [31], the rates of hypertension and dyslipidemia in patients with NAFLD were slightly lower than those in our results. This may be due to the fact that the diagnostic criteria for LRDs in this study were based on the International Consensus Group criteria, as well as regional characteristics. Regarding laboratory values, MASLD deviated more from the reference values than non-MASLD, which is consistent with the previous report [31] and may be owing to a higher prevalence of LRDs. The large number of LRD holders in the MASLD demonstrates the importance of the fact that the MASLD was created for the purpose of proactively capturing at-risk individuals.
The limitations of this study included the following. First, the results were from a specific region of Japan, and the nutritional data were from national data and not from the participants themselves. This was a retrospective study and no nutritional surveys were conducted; therefore, data were not available. However, this is a typical medium-sized Japanese city, 60 km from the capital, with an average annual income that is approximately equal to the Japanese average, although slightly lower than the Japanese average for primary industry workers. Furthermore, the patient population was comprised of ordinary people. Thus, as the nutrition data were averages for Japan, the correlations were not expected to diverge significantly. However, future research should be conducted over a wider area, including participants’ nutritional and physical activity status.
The second limitation was the diagnosis of LRDs. In this study, we diagnosed abnormal blood pressure as hypertension; abnormal lipid metabolism as dyslipidemia, based on the International Consensus Group criteria [1]; and abnormal glucose metabolism as T2DM and prediabetes combined, based on the American Diabetes Association criteria [5]. However, these are slightly different from the Japanese diagnostic criteria. Therefore, it is necessary to discuss the criteria that should be adopted when studying MASLD in Japan.
5. Conclusions
The prevalence of MASLD increased in all age and sex groups from 2010 to 2019, as did the prevalence of SLD itself, while the prevalence of prediabetes decreased. A change in diet, primarily lipid-based, was considered a contributing factor in both cases.
Author Contributions
Conceptualization, A.S.; methodology, A.S.; formal analysis, R.N.; investigation, Y.O.; resources, R.N.; data curation, Y.O.; writing—original draft preparation, A.S.; writing—review and editing, T.M.; supervision, T.M.; project administration, T.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Human Ethics Review Committee of the Sasaki Foundation (No. ER2023-10; approval date: 15 March 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are not publicly available due to privacy and ethical restrictions.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023; 79:1542-1556.
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology, 1: 78, 1966. [Google Scholar]
- Hamaguchi, M.; Kojima, T.; Takeda, N.; et al. The metabolic syndrome as a predictor of nonalcoholic fatty liver disease. Ann Intern Med, 7: 143.
- Matsuzawa, Y. ; Metabolic syndrome - Definition and diagnostic criteria in Japan. J Atheroscler Thromb, 3: 12.
- American Diabetes Association. Understanding diabetes diagnosis. https://diabetes.org/about-diabetes/diagnosis; Accessed 3.05.2024.
- National Institute of Biomedical Innovation. Health Japan 21 National Health and Nutrition Survey. https://www.nibiohn.go.jp/eiken/kenkounippon21/eiyouchousa/keinen_henka_eiyou.html; Accessed 5.05.2024.
- Ministry of Health, Labour and Welfare. FY2019 National Health and Nutrition Survey Report. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/eiyou/r1-houkoku_00002.html; Accessed 5.05.2024.
- Ikeda, N.; Takimoto, H.; Imai, S.; Miyachi, M.; Nishi, N. Data resource profile: The Japan National Health and Nutrition Survey (NHNS). Int J Epidemiol, 1: 44, 1842. [Google Scholar]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate use and interpretation. Anesth Analg, 1: 126, 1763. [Google Scholar]
- Sato, A.; Oomori, Y.; Nakano, R.; Matsuura, T. Nonalcoholic fatty liver disease in Japan continue to increase even after the launch of specific health checkups. Intern Med. 2024; 63:763-771.
- Goto, A.; Noda, M.; Inoue, M.; Goto, M.; Charvat, H. Increasing number of people with diabetes in Japan: Is this trend real? Intern Med, 1: 55, 1827. [Google Scholar]
- The World Bank. Diabetes prevalence - Japan. https://data.worldbank.org/indicator/SH.STA.DIAB.ZS?end=2021&locations=JP&start=2011; Accessed 5.05.2024.
- Hauner, H.; Bechthold, A.; Boeing, H.; et al. Evidence-based guideline of the German Nutrition Society: Carbohydrate intake and prevention of nutrition-related diseases. Ann Nutr Metab, 1: 60 Suppl 1.
- Hosseini, F.; Jayedi, A.; Khan, T.A.; Shab-Bidar, S. Dietary carbohydrate and the risk of type 2 diabetes: An updated systematic review and dose-response meta-analysis of prospective cohort studies Sci Rep. 2022; 12:2491. 12.
- Qi, Y.; Wang, X. The Role of Gut Microbiota in High-Fat-Diet-Induced Diabetes: Lessons from Animal Models and Humans. Nutrients, 9: 15.
- Prasad, M.; Rajagopal, P.; Devarajan, N.; et al. A comprehensive review on high-fat diet-induced diabetes mellitus: An epigenetic view. J Nutr Biochem, 1: 107, 1090. [Google Scholar]
- Kennedy, A.; Martinez, K.; Chuang, CC.; LaPoint, K.; McIntosh, M. Saturated fatty acid-mediated inflammation and insulin resistance in adipose tissue: Mechanisms of action and implications. J Nutr, 1: 139.
- Neuenschwander, M.; Barbaresko, J.; Pischke, C.R.; et al. Intake of dietary fats and fatty acids and the incidence of type 2 diabetes: A systematic review and dose-response meta-analysis of prospective observational studies. PLoS Med, e: 17, 1003. [Google Scholar]
- Ley, SH.; Hamdy, O.; Mohan, V.; Hu, F.B. Prevention and management of type 2 diabetes: Dietary components and nutritional strategies. Lancet, 1: 383, 1999. [Google Scholar]
- Yaegashi, A.; Kimura, T.; Wakai, K.; Iso, H.; Tamakoshi, A. Association between total fat and fatty acid intake and the risk of type 2 diabetes mellitus among Japanese adults: Analysis based on the JACC study. J Epidemiol. [CrossRef]
- Slurink, I.A; Chen, L.; Magliano, D.J.; Kupper, N.; Smeets, T.; Soedamah-Muthu, S.S. Dairy product consumption and incident prediabetes in the Australian Diabetes, Obesity, and Lifestyle Study with 12 years of follow-up. J Nutr, 1: 153, 1742. [Google Scholar]
- Jiang, S.; Yang, W.; Li, Y.; et al. Monounsaturated and polyunsaturated fatty acids concerning prediabetes and type 2 diabetes mellitus risk among participants in the National Health and Nutrition Examination Surveys (NHANES) from 2005 to March 2020. Front Nutr, 20 March.
- Zhu, X.; Chen, L.; Lin, J.; et al. Association between fatty acids and the risk of impaired glucose tolerance and type 2 diabetes mellitus in American adults: NHANES 2005-2016. Nutr Diabetes. 2023. [Google Scholar] [CrossRef] [PubMed]
- Qian, F.; Ardisson Korat, A.V.; Imamura, F.; et al. n-3 Fatty acid biomarkers and incident type 2 diabetes: An individual participant-level pooling project of 20 prospective cohort studies. Diabetes Care, 1: 44, 1133. [Google Scholar]
- Imamura, F.; Micha, R.; Wu, J.H.; et al. Effects of saturated fat, polyunsaturated fat, monounsaturated fat, and carbohydrate on glucose-insulin homeostasis: A systematic review and meta-analysis of randomised controlled feeding trials. PLoS Med, e: 13, 1002. [Google Scholar]
- Hernández, E.Á.; Kahl, S.; Seelig, A.; et al. Acute dietary fat intake initiates alterations in energy metabolism and insulin resistance. J Clin Invest, 6: 127.
- Rosqvist, F.; Kullberg, J.; Ståhlman, M.; et al. Overeating saturated fat promotes fatty liver and ceramides compared with polyunsaturated fat: A randomized trial. J Clin Endocrinol Metab, 6: 104, 6207. [Google Scholar]
- Errazuriz, I.; Dube, S.; Slama, M.; et al. Randomized controlled trial of a MUFA or fiber-rich diet on hepatic fat in prediabetes. J Clin Endocrinol Metab, 1: 102, 1765. [Google Scholar]
- Cui, J.; Li, L.; Ren, L.; Sun, J.; Zhao, H.; Sun, Y. Dietary n-3 and n-6 fatty acid intakes and NAFLD: A cross-sectional study in the United States. Asia Pac J Clin Nutr, 8: 30.
- Hagström, H.; Vessby, J.; Ekstedt, M.; Shang, Y. 99% of patients with NAFLD meet MASLD criteria and natural history is therefore identical. J Hepatol, e: 80.
- Fujii, H.; Suzuki, Y.; Sawada, K.; et al. Prevalence and associated metabolic factors of nonalcoholic fatty liver disease in the general population from 2014 to 2018 in Japan: A large-scale multicenter retrospective study. Hepatol Res, 1: 53, 1059. [Google Scholar]
Figure 1.
Changes in prevalence of steatotic liver diseases. FY, fiscal year; MASLD, metabolic dysfunction-associated steatotic liver disease; NAFLD, non-alcoholic fatty liver disease; SL, steatotic liver; SLD, steatotic liver disease
Figure 1.
Changes in prevalence of steatotic liver diseases. FY, fiscal year; MASLD, metabolic dysfunction-associated steatotic liver disease; NAFLD, non-alcoholic fatty liver disease; SL, steatotic liver; SLD, steatotic liver disease
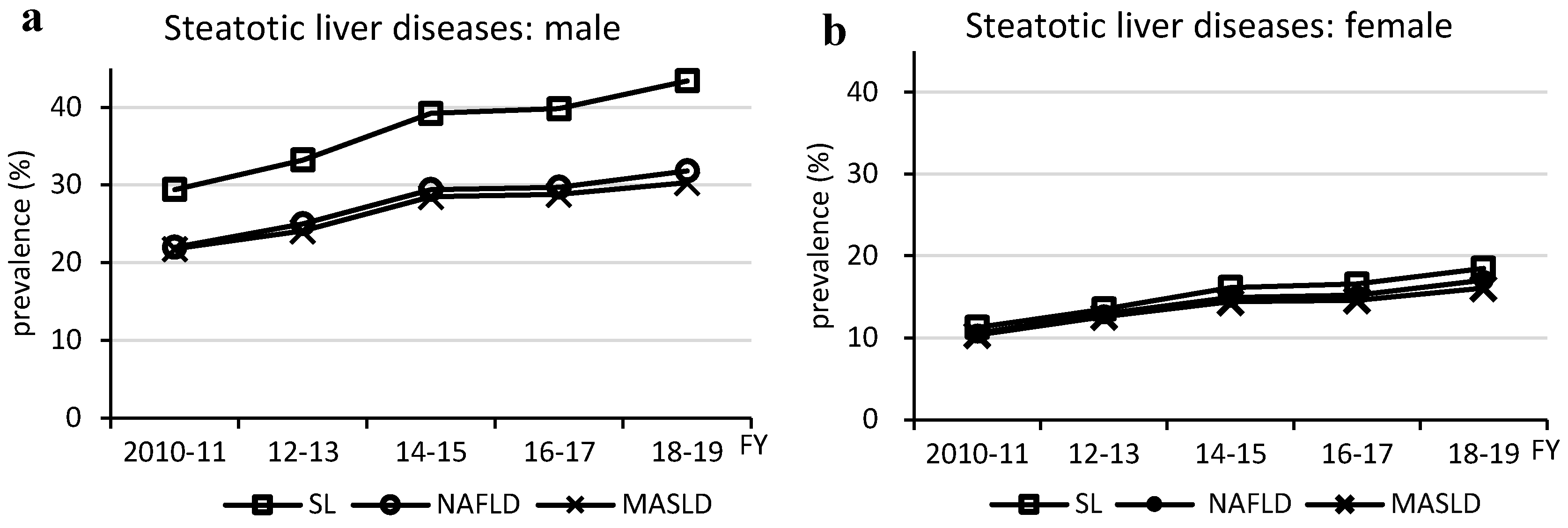
Figure 2.
Changes in prevalence of MASLD by age and BMI. MASLD, metabolic dysfunction-associated steatotic liver disease; BMI, body mass index; FY, fiscal year.
Figure 2.
Changes in prevalence of MASLD by age and BMI. MASLD, metabolic dysfunction-associated steatotic liver disease; BMI, body mass index; FY, fiscal year.
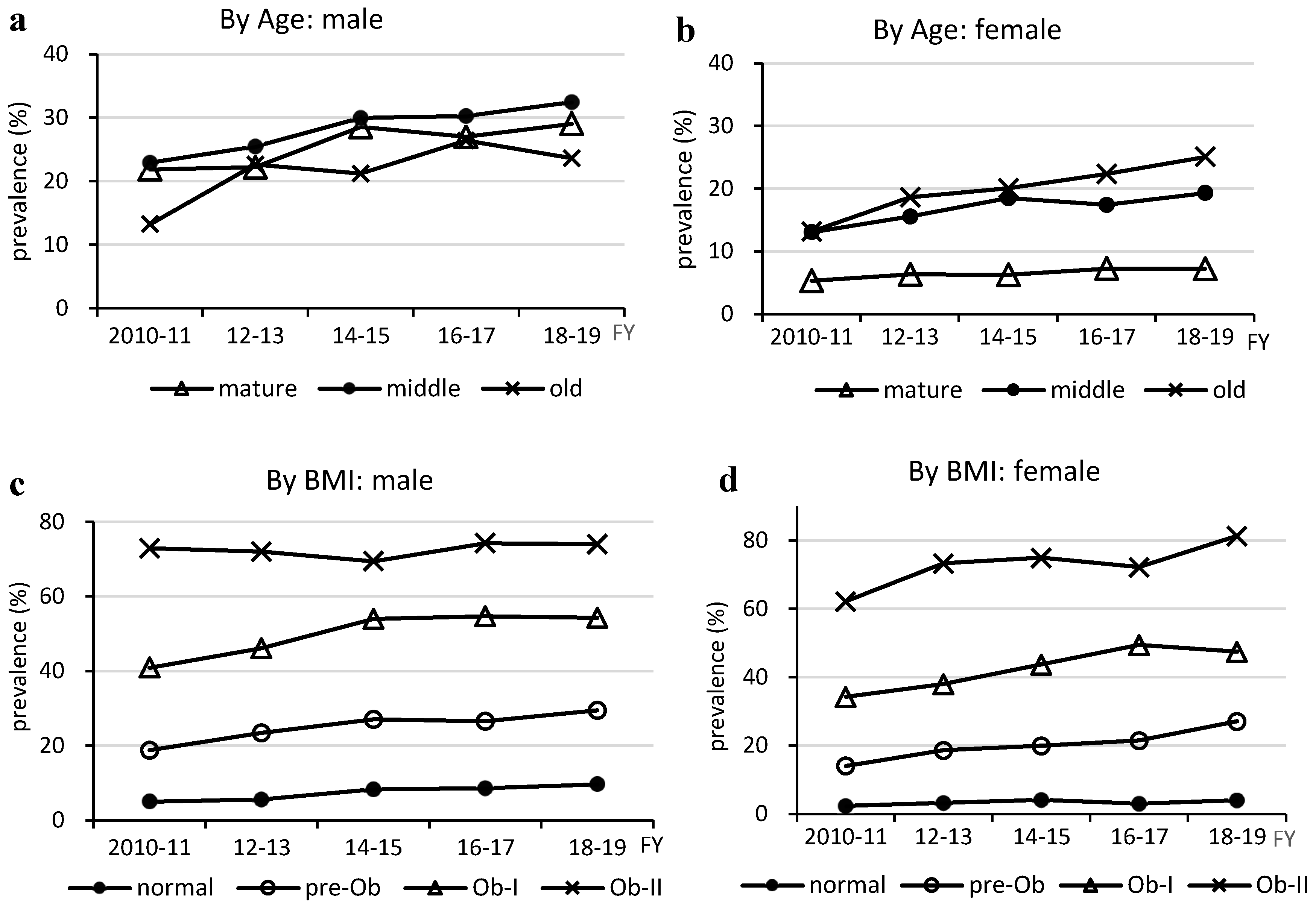
Figure 3.
Changes in prevalence of metabolic dysfunction-associated steatotic liver disease -related physical and metabolic disorders. Physical Disorders (a and b). Metabolic Disorders (c and d). DL, dyslipidemia; DM, type 2 diabetes; FY, fiscal year; GMD, glucose metabolism disorder; HT, hypertension; HWC, high waist circumference; preDM, prediabetes; SL, steatotic liver.
Figure 3.
Changes in prevalence of metabolic dysfunction-associated steatotic liver disease -related physical and metabolic disorders. Physical Disorders (a and b). Metabolic Disorders (c and d). DL, dyslipidemia; DM, type 2 diabetes; FY, fiscal year; GMD, glucose metabolism disorder; HT, hypertension; HWC, high waist circumference; preDM, prediabetes; SL, steatotic liver.
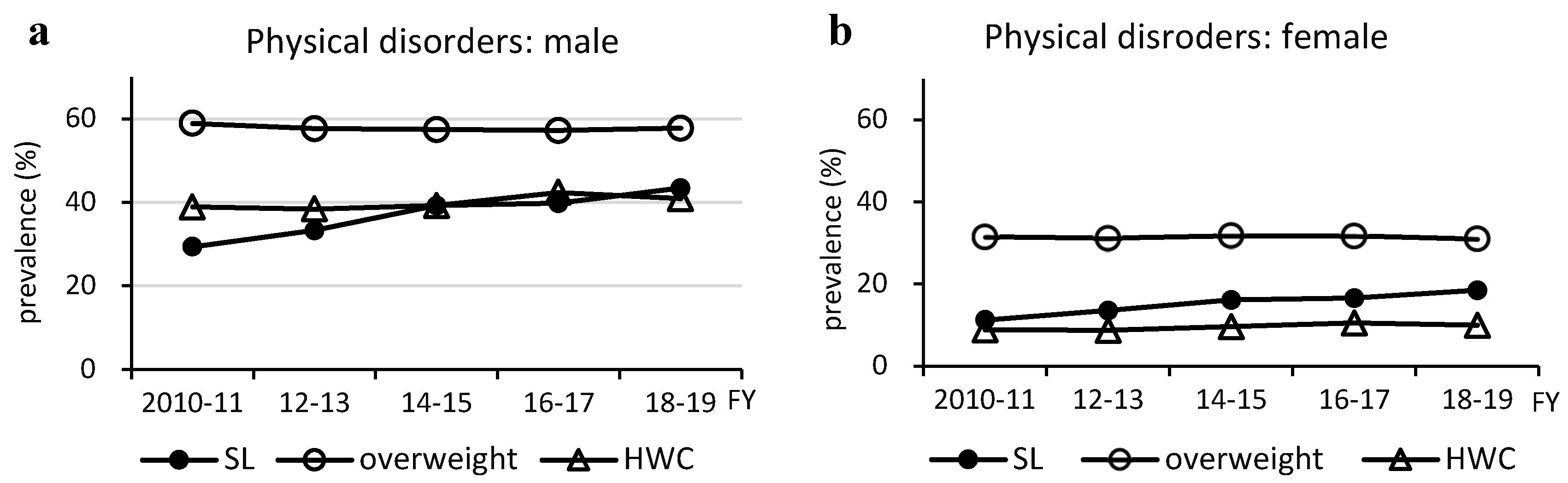
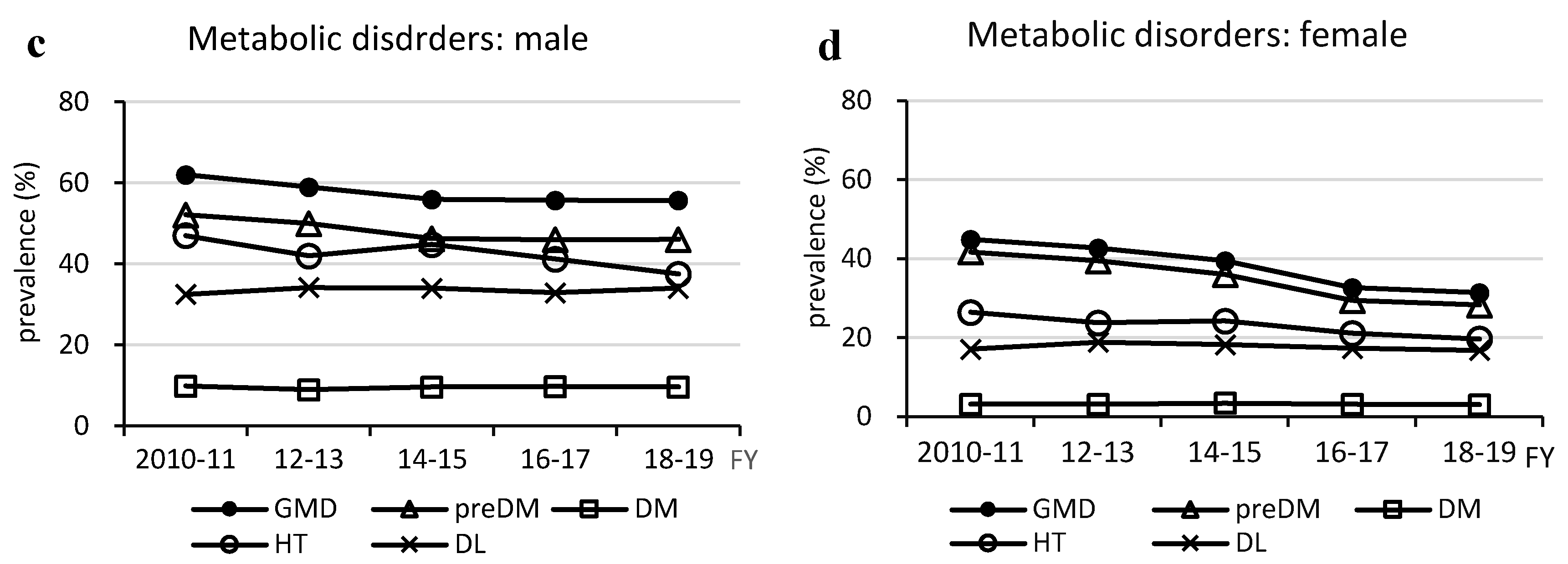
Figure 4.
Relationship between glucose metabolism disorders and nutrient intake. (a, b) Total energy intake, (c, d) total carbohydrate intake, (e, f) total fat intake, (g, h) saturated fatty acid intake, (i, j) monounsaturated fatty acid intake, and (k, l) polyunsaturated fatty acids (sum of n-3 and n-6 polyunsaturated fatty acid). DM, type 2 diabetes; GMD, glucose metabolism disorder; MUFA, monounsaturated fatty acids; preDM, prediabetes; PUFA, polyunsaturated fatty acids; SFA, saturated fatty acids.
Figure 4.
Relationship between glucose metabolism disorders and nutrient intake. (a, b) Total energy intake, (c, d) total carbohydrate intake, (e, f) total fat intake, (g, h) saturated fatty acid intake, (i, j) monounsaturated fatty acid intake, and (k, l) polyunsaturated fatty acids (sum of n-3 and n-6 polyunsaturated fatty acid). DM, type 2 diabetes; GMD, glucose metabolism disorder; MUFA, monounsaturated fatty acids; preDM, prediabetes; PUFA, polyunsaturated fatty acids; SFA, saturated fatty acids.
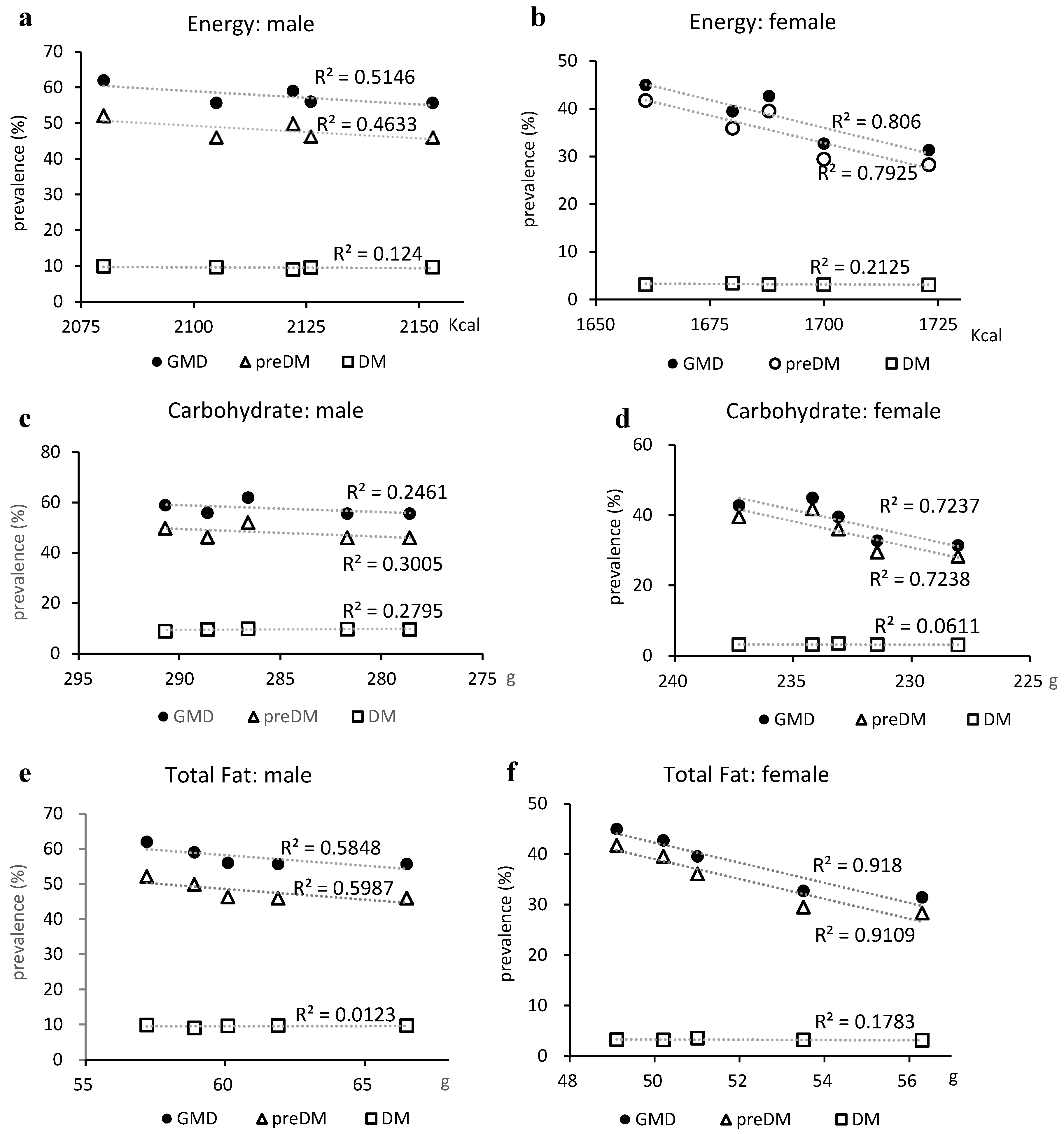
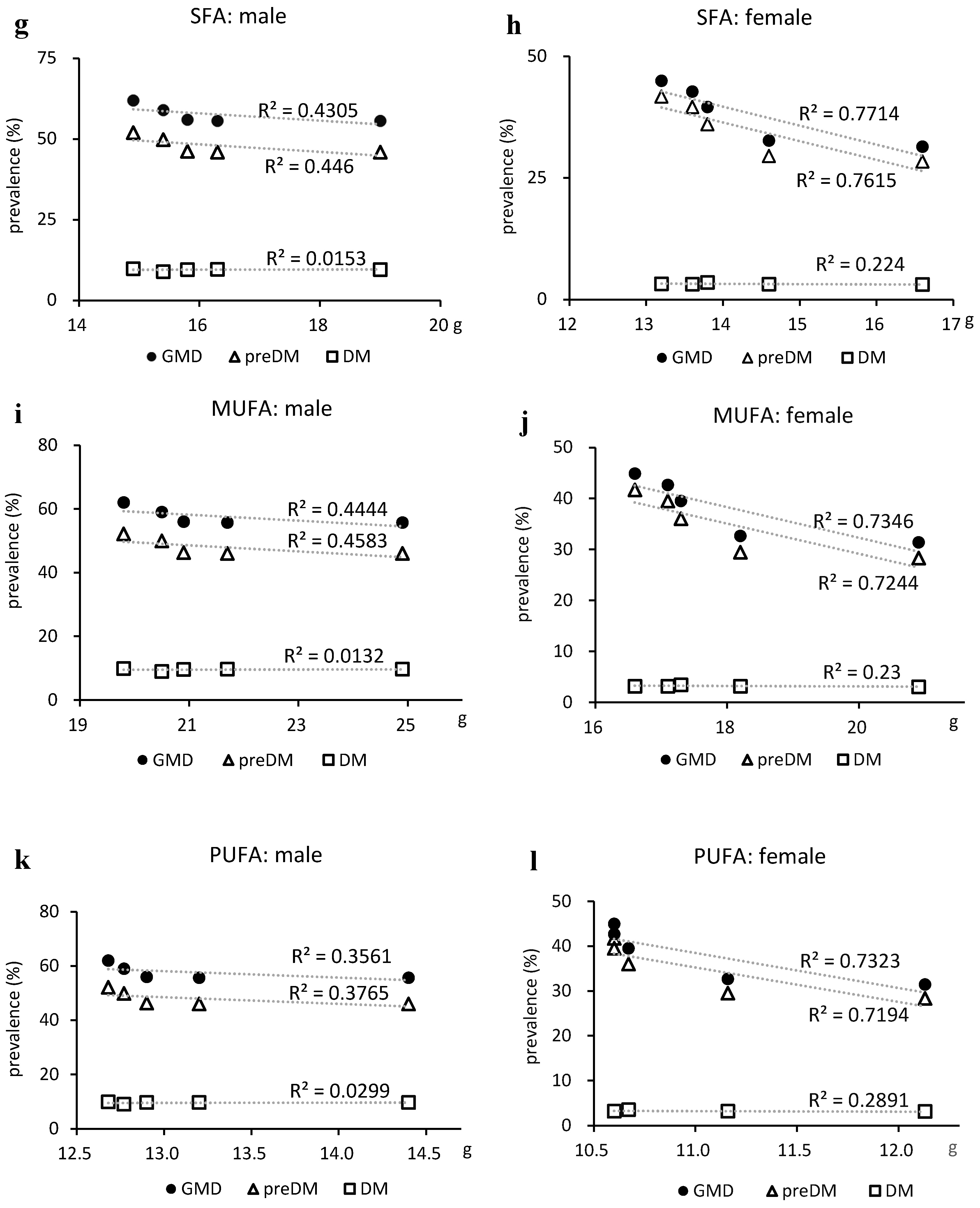
Figure 5.
Relationship between hypertension and salt intake. Salt intake was significantly reduced in males (from 11.4 g to 10.9 g, p=0.037) but weakly correlated with the prevalence of hypertension (R2 = 0.342). However, there was a moderate correlation with a reduced prevalence of hypertension in females (R2 = 0.483), where the reduction in salt intake was not significant (from 9.6 g to 9.2 g, p=0.089).
Figure 5.
Relationship between hypertension and salt intake. Salt intake was significantly reduced in males (from 11.4 g to 10.9 g, p=0.037) but weakly correlated with the prevalence of hypertension (R2 = 0.342). However, there was a moderate correlation with a reduced prevalence of hypertension in females (R2 = 0.483), where the reduction in salt intake was not significant (from 9.6 g to 9.2 g, p=0.089).
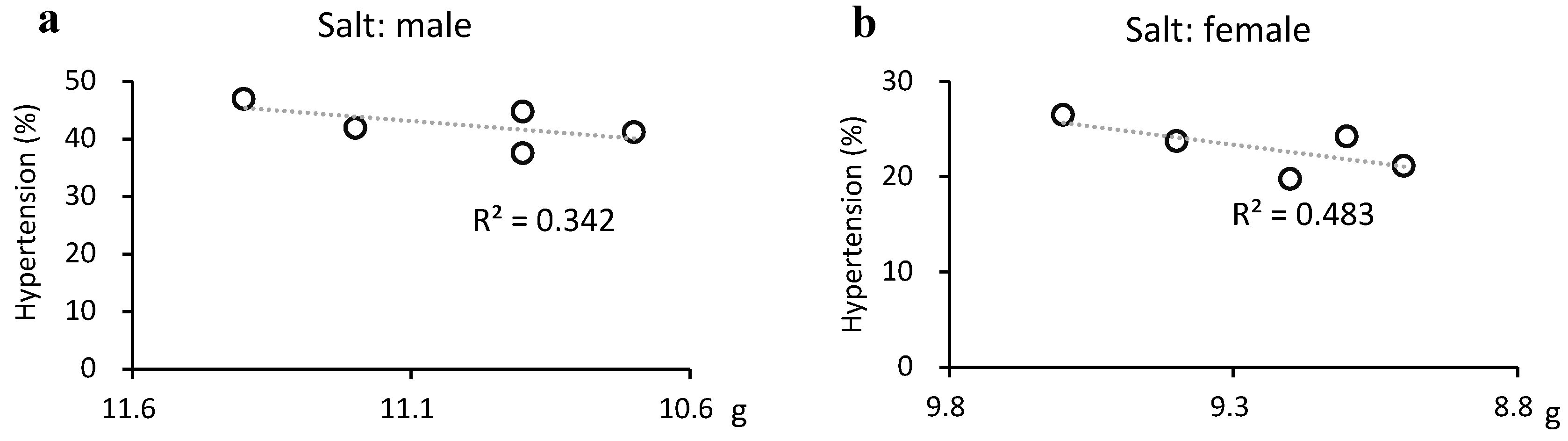

Table 1.
Characteristcs of the subjects.
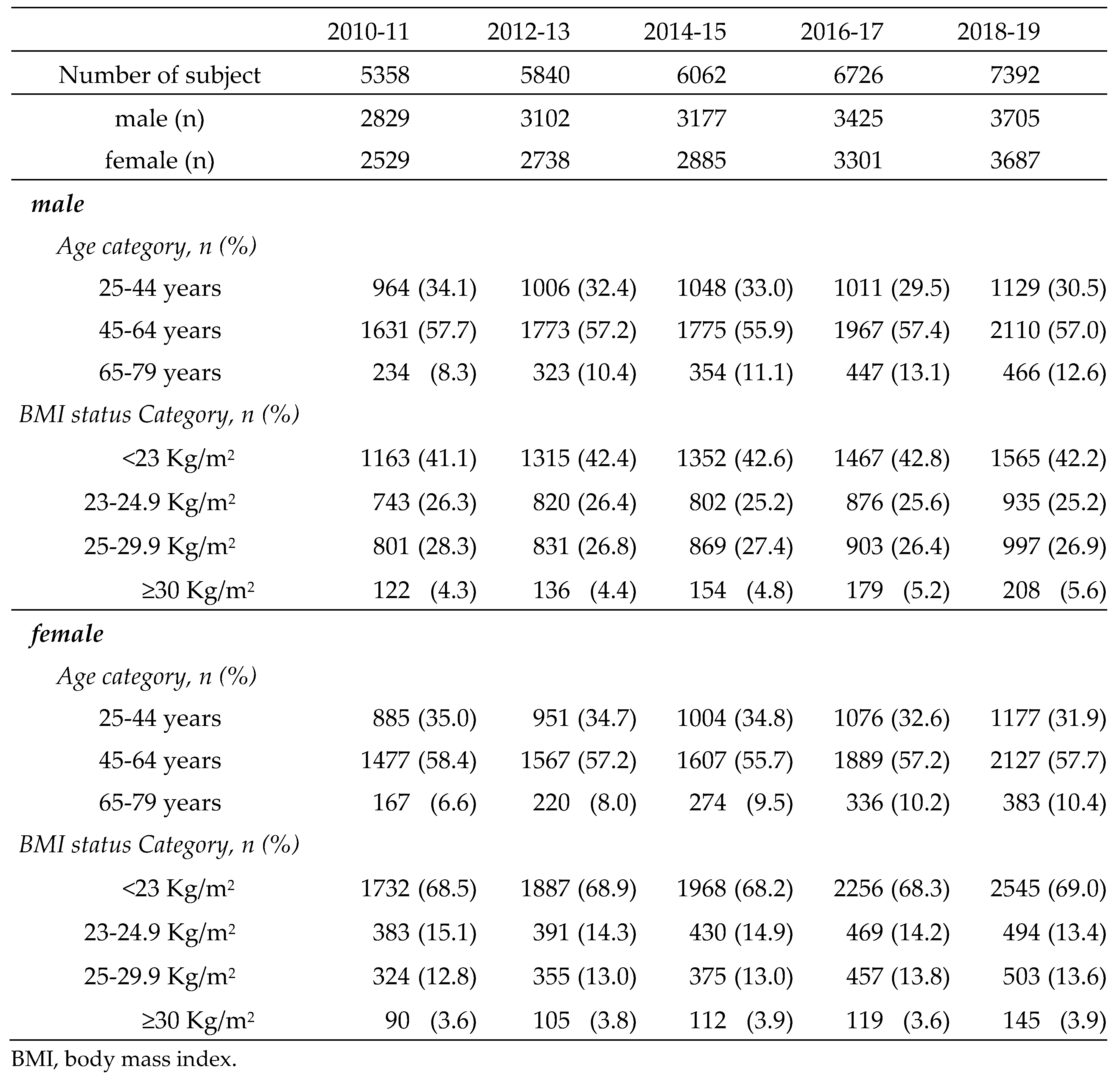
Table 2.
Trend of dietary nutrients and exercise habits (2010-2019).
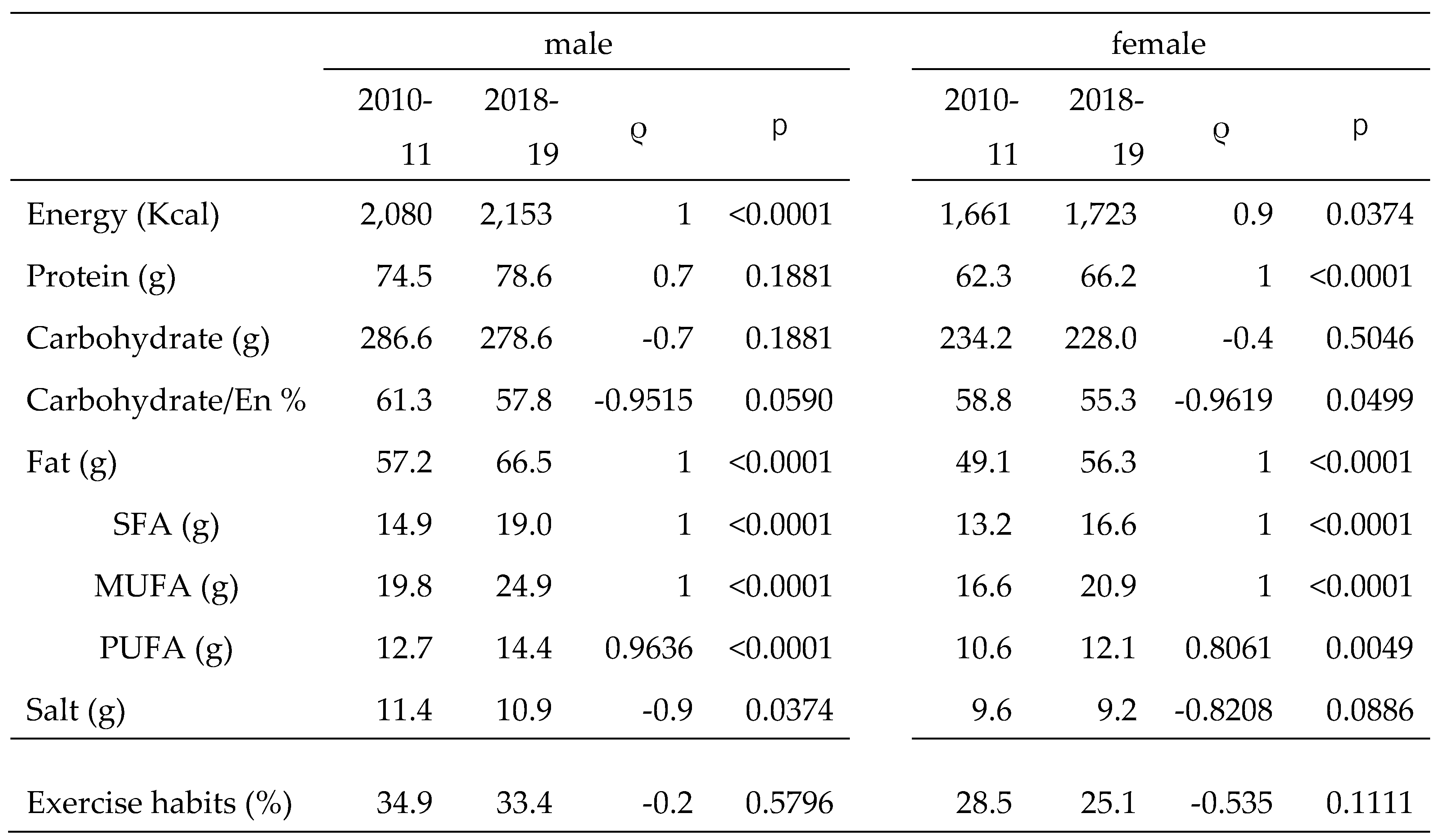
Table 3.
Comparison of MASLD and non-MASLD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



