
Submitted:
02 July 2024
Posted:
03 July 2024
You are already at the latest version
Abstract
Pulmonary artery stenosis represents a group of disorders involving main, branch or peripheral pulmonary arteries resulting either in pain, dyspnea, hemoptysis or even no symptoms. Early diagnosis and timely intervention are crucial for reducing mortality, while timely diagnosis is challenging due to the nonspecific symptoms. Computed tomography pulmonary angiography (CTPA) is useful in the diagnosis because it can provide more details about the abnormal changes in the lumen, vessel wall and adjacent mediastinal structures. Congenital and acquired pulmonary artery anomalies have some characteristics on CTPA, which can be useful for differential diagnosis. Awareness of these conditions and is important for the radiologists. This pictorial review provides an overview of CTPA imaging features of pulmonary artery stenosis.
Keywords:
Pulmonary artery stenosis
; congenital and acquired anomalies
; Computed tomography pulmonary angiography
; differential diagnosis
1. Introduction
Pulmonary artery stenosis (PAS) is caused by the formation of obstructive lesions in the pulmonary artery and its branches. Due to the decrease of cross-sectional area of pulmonary artery, the blood flow was impeded exiting the heart. This may raise the pressure of right ventricle (RV), which can cause the endothelial damage of PA and further lead to pulmonary artery hypertension (PAH). With all the causes, presenting as right heart failure can lead to bad prognosis and even death [1].
PAS can be categorized based on location. And there are four types of PAS, from proximal to sub-segmental. TypeⅠinvolves single central stenosis of the main pulmonary trunk or branches of the pulmonary artery. TypeⅡinvolves the bifurcation of the pulmonary artery. Type Ⅲ involves multiple peripheral stenosis. Type Ⅳ involves a combination of both main and peripheral stenosis [2].
The clinical presentation of PAS varies from shortness of breath, fatigue, tachycardia to the swelling of the feet, ankles, and abdomen which happen in the advanced stage, as a result of right heart failure. Thus, it is important to detect PAS as early as possible to improve the prognosis.
When the patient was present with those symptoms, chest radiography or computed tomography should be conducted. High resolution computed tomography (HRCT) and computed tomography pulmonary angiography (CTPA) are invaluable for examining the pulmonary vessels, which can provide details of the lumen, vessel wall, adjacent mediastinal structures and subsequent lung lesions, which are very important to identify the reasons of PAS.
The aim of this article is to review the imaging features of congenital and acquired anomalies which cause the stenosis of pulmonary artery, and to illustrate the typical CT characteristics of these anomalies. We will discuss the congenital diseases cause the decrease of right ventricular output volume, pulmonary artery and pulmonary vein atresia. To simplify the understanding, the acquired diseases will be categorized as anomalies affecting the vessel wall, intraluminal anomalies and extraluminal anomalies. Table 1 provides the content of these disease categorized by the reasons of PAS.
2. PAS Due to Congenital Etiology
2.1. Pulmonary Valvular Stenosis
Valvular pulmonary stenosis is the most common type of congenital pulmonic stenosis, followed by subvalvular and supravalvular types [3]. It accounts for about 8%-10% of all congenital heart disease and contribute to right ventricular outflow obstruction [4]. With the high-speed flow jet through the narrowed valve, poststenotic dilatation of the main and left pulmonary artery is most present [5]. In some cases, due to the decrease of blood flow, the diffused stenosis of distal lobular and segmental PA can be detected.
On chest radiograph and CT (Figure 1), the enlargement of the pulmonary trunk and left PA can be seen, but normal right PA, since the left PA is a direct continuation of the pulmonary trunk. Subject to the reduced blood flow of PA and elevated pressure overloaded of right ventricle related to the stenotic valve, stenosis of distal PA branches and right ventricular hypertrophy may be visible. Thickened pulmonic valve can also be apparent on ECG-gated computed tomography pulmonary angiography (CTPA) [6].
2.2. Pulmonary Artery Atresia
PA atresia accounts for 1 out of every 10,000 live births. There are two types of PA atresia, distinguished by the presence or absence of a ventricular septal defect (VSD) [7]. PA-VSD is often a variant of Tetralogy of Fallot (TOF) characterized by discontinuity between the RV and pulmonary arteries and associated with a VSD (Figure 2). This abnormality includes atresia of the right ventricular outflow tract (RVOT) or pulmonary valve with variable hypoplastic, discontinuous or absent MPA and central branch PAs. In that case, systemic collaterals must be present to supply the lung and mainly are either a patent ductus arteriosus (PDA), major aortopulmonary collaterals (MAPCAs) from the descending aorta, subclavian, celiac or coronary arteries. Infants usually present with cyanosis and hypoxia or heart failure [6].
CTPA illustrates the accurate length of pulmonary atresia, presence of branch PA confluence, size of the main, right and left PAs at the origin and hilum, and delineates the pulmonary blood supply, which is necessary for the surgical plan.
PA atresia with intact ventricular septum (PA-IVS) is less common than the former anomaly. The RV is usually hypoplastic and hypertrophied, as there is no blood flow through VSD to promote RV growth and there is RV outflow obstruction to cause myocardial remodeling. This is different from PA-VSD which RV cavity can grow [6]. In some cases with dysplastic tricuspid valve, enlargement of RV may be shown. Branch PAs and PDA are frequently normal. Blood flow to the PAs depends on a PDA [7]. There are also associated abnormalities in the coronary circulation such as ventriculocoronary connections, fistulae, coronary stenosis, or atresia.
2.3. Pulmonary Vein Atresia
Congenital pulmonary vein atresia (PVA) occurs due to complete or partial failure of incorporation of the developmental common pulmonary vein into the left atrium, which is divided into three categories based on the extent of venous involvement [8]. Among these categories, unilateral PVA results in lung hypoplasia and pulmonary artery stenosis [9]. Because PVA occurs after regression of embryological drainage to the systemic cardinal and umbilicovitelline system, an anomalous systemic venous connection is absent. Recurrent respiratory tract infections, hemoptysis or pulmonary hypertension may be the presenting complaint in unilateral PVA patients.
On CTPA, no pulmonary vein drainage to left atrium is shown in the affected lung, typically without evidence of outpouchings on the left atrium to indicate the rudimentary ostia. Because of the increased pulmonary venous pressure in the ipsilateral lung [9], the blood flow is reduced compared to the contralateral side, which is manifested as diminutive pulmonary arteries with diffused ground-glass pulmonary opacities, septal lines and bronchial wall thickening. The affected hilum is enlarged as engorged lymphatics and collateral venous channels (Figure 3).
3. PAS Due to Acquired Disease
3.1. Intraluminal Anomalies
3.1.1. Pulmonary Thromboembolism (PTE)
Pulmonary thromboembolism (PTE) which arises from venous thrombi occluding the pulmonary arteries is the most common disease blocking the pulmonary lumen [10]. Acute PTE is fatal, as it is associated with right ventricular dysfunction such as arrhythmia, hemodynamic collapse and shock [11]. Computed tomography pulmonary angiography (CTPA) is the current reference method for the diagnosis. A complete or partial filling defect in pulmonary arteries can be shown on CTPA (Figure 4). Complete filling defects show no enhancement of the entire lumen without distention, differing from tumor embolism and pulmonary artery sarcoma. Partial filling defects can be centrally and peripherally located in the vessel and be surrounded by contrast, showing the “railway track” sign on longitudinal images or forming acute angles with the artery wall [12]. Peripheral pulmonary infarction, producing peripheral wedge-shaped nonenhanced density in lung parenchyma is the significant indirect sign (Figure 4).
Chronic PTE is characterized by chronic thrombotic remains in the pulmonary arteries after acute PTE syndrome, which can lead to the potentially life-threatening disease chronic thromboembolic pulmonary hypertension (CTEPH) [13]. The remaining embolic material is incorporated into the vessel wall and covered over by a thin layer of endothelial cells. The filling defects of chronic PTE on CTPA includes as following: (a) retracted thrombi that present complete filling defect at the level of stenose PA with an abrupt cutoff or narrowing of the vessel; (b) organized thrombi that show peripheral lined filling defect adherent to the vessel wall, forming obtuse angles and occasionally containing calcifications; (c) recanalized thrombi that present contrast material traversing the arteries with thickened walls forming intraluminal webs or bands (Figure 5). As the affected arteries are stenotic or occlusive, the vessels distal to the embolus have smaller caliber, which can distinguish from acute PTE with normal or expanded vessels [14], but the MPA is widen. The secondary signs of chronic PTE include mosaic attenuation in lungs and abnormal enlargement of bronchial and systemic collateral vessels [15].
In CT(A), an enlarged PA diameter(PA diameter ≥30 mm, or a PA-to-aorta ratio>0.9, and enlarged right heart chambers (RV:LV ratio ≥1) or septal deviation ≥140°suggest the presence of PH (Figure 4), which has higher risk of poor prognosis in acute PE patients.
3.1.2. In Situ Pulmonary Artery Thrombosis (PAT)
In situ pulmonary artery thrombosis (PAT) refers to de novo thrombosis of the pulmonary arterial system, which associated with pulmonary infections, hypoxia, trauma, radiation therapy, pulmonary artery catheter, aberrant pulmonary structures (e.g. the pulmonary artery stump following pneumonectomy), severe pulmonary arterial hypertension, genetic mutations, immunological and hematological systemic diseases [16]. These factors lead to pulmonary vascular endothelial cell injury, which collectively trigger the coagulation cascade and induce thrombosis. And those can also result in intimal hyperplasia, vascular remodeling and even stenosis flowing hemodynamic factors, which may be less important for the initiation of PA thrombosis but they do affect permeability of the vascular wall and lead to the progression of thrombosis [17]. The feature of thrombus in proximal PA on CTPA is universally nonocclusive and eccentric with obtuse angles to the vessel wall and demonstrate lack of vascular distention [18] (Figure 6). However, de novo thrombosis in sub-segmental down to small PA of 2-5 mm in diameter are difficult to detect on CTPA.
3.1.3. Pulmonary Tumor Embolism and Pulmonary Tumor Thrombotic Microangiography (PTTM)
Tumor embolism in the pulmonary artery is a rare clinicopathological entity characterized by the occlusion of pulmonary vessels by tumor clots, which can via three ways: a). direct extension of thrombus from the systemic to the pulmonary vasculature; b). tumor in the proximal arteries (macro-embolism); c). tumor in the small vessels (micro-embolism) [19]. The direct extension of tumor thrombus presents enhanced filling defects in PA with or without lumen dilation on CTPA, distinguishing from acute PE (Figure 7). PTTM is an advanced form of PTE where the tumor cells nest in the small vessels and lymphatic channels, which triggers the proliferation of vessel endothelium and coagulation cascade [20]. Owing to pulmonary microvascular disease and lymphangitic carcinomatosis, centrilobular nodules, tree-in-bud sign, peribronchovascular ground-glass opacities, interlobular septal thickening can be seen On HRCT and CTPA [21] (Figure 8). For the suspicious cases, Maximum intensity projection (MIP) is recommended for showing the enlargement of pulmonary vasculature and small tumor embolus (Figure 8). With the occlusion of pulmonary vessels, PTTM can rapidly progress to PH and hypoxemia, even death.
3.1.4. Septic Pulmonary Embolism (SPE)
Septic pulmonary embolism is an uncommon and challenging disorder that can cause the decrease of cross-sectional area of pulmonary arteries. the thromboses of SPE containing microorganisms are implanted into PA, not only obstructing the vessels, but also leading to lung infarction and focal abscess. It’s associated with tricuspid valve endocarditis, septic thrombophlebitis, infected central venous catheters, heart pacemaker and immunocompromised patients. The main pathogens include gram-negative bacteria, gram-positive bacteria and fungi [22]. The typical characteristic of SPE is the filling defects detected inside pulmonary arteries, and those thromboses often situated at the site of turbulent flow or slow flow, which can be found in PDA (Figure 9). There are some abnormalities of lungs such as subpleural and wedge-shaped infiltrates with peripheral enhancement and occasional cavitation, sometimes with a visible feeding vessel [23,24] (Figure 9). The symptoms of SPE were not specific, most present as bacteremia, dyspnea, chest pain, cough and other respiratory symptoms [25].
3.1.5. Pulmonary Embolism caused by Foreign Bodies
Foreign bodies-induced pulmonary embolism is a stenosis or occlusion of the pulmonary vasculature by various organic and inorganic materials blockage, such as air, catheter, cement (polymethylmethacrylate), metallic mercury, talc, fat, silicone etc [26]. In contrast to the clinical symptoms of PTE, the pathophysiologic effects are not only mechanical but also a consequence of the nature of the offending material, which may trigger an inflammatory cascade that causes deterioration of vascular, pulmonary and cardiac function [27]. Cement injection within a vertebral body is a widely used technique in patients with vertebral fracture and kyphosis, which may cause PE via the external vertebral venous plexuses (Figure 10). CT may show tubular areas of branching linear opacities filling the distal pulmonary artery branches. Catheter embolism is one of the most common iatrogenic causes of embolism. The fragments of central venous catheters, venous port catheters, guidewires, and vascular sheaths may reach and occlude the pulmonary arteries, due to catheter tear, most often when catheters are removed [28]. And the CTPA often show the catheter in the pulmonary artery (Figure 11). Foreign bodies pulmonary embolism usually has contact history, which can assist in the diagnosis.
3.1.6. Pulmonary Artery Sarcoma
Pulmonary artery sarcoma (PAS) is a rare and lethal malignant tumor that arises from the intimal layer of the pulmonary artery, which is frequently misdiagnosed as pulmonary thromboembolism (PTE) with a poor prognosis. Early and correct diagnosis offer the only chance for survival. However, the clinical symptoms of PAS are always insidious, presenting with general cardiovascular or pulmonary symptoms, such as fever, anemia, weight loss, chest pain, cough, dyspnea, and syncope [29]. The distinguishing clinical features are unexplained pulmonary hypertension symptoms, lack of the risk factors for PTE or not responding well to anticoagulation [30]. Computed tomographic pulmonary angiography (CTPA) is considered a useful tool in clinically suspicious cases of PAS. The typical feature on CTPA imaging of PAS is that the lesions always involves the main PA, which can extend into the main pulmonary trunk and right ventricular outflow tract or pulmonary artery trunk or segmental PAs. And it tends to occupy the entire lumen with local aneurysmal dilatation, which means that PAS grows outside the artery. Other features include delay enhancement, wall eclipsing sign, proximal lobulated and bulging margins [31] (Figure 12). And the “wall eclipsing sign” and enhancement can be helpful in distinguishing PAS from thromboembolic disease [32].
3.2. Vessel Wall Lesions
3.2.1. Vasculitis
The vasculitis is a diverse group of diseases characterized by inflammation within and around blood vessel walls, which can affect large, medium-size and small vessels.
3.2.1.1. Takayasu Arteritis (TA)
Takayasu arteritis (TA) is an autoimmune large vessel vasculitis of unknown etiology that typically involves the aorta and its main branches, and pulmonary artery lesions are not uncommon. The disease is most prevalent among young Asian females, who under 40 years of age [33]. Pulmonary artery involvement is usually found in the late stage of TA, and the main clinical presentation are dyspnea, chest pain, hemoptysis, and cough [34]. The pathology is characterized by the involvement of all arterial layers with a variable inflammatory infiltration [35]. The most common imaging manifestations of pulmonary artery involvement were stenosis, followed by occlusion and arterial wall thickening [34] (Figure 13). CTPA displays thickened and enhancing vascular walls during the inflammatory phase and symmetric smoothly tapered areas of circumferential narrowing near the origin of the primary branches of the aorta often with copious collateral vessels in the occlusive phase [33]. Other than the PA stenosis, pulmonary infarction is also occasionally shown on HRCT. The clinical presentation of TA pulmonary artery involvement is different from classical TA, which may lead to misdiagnosed and inappropriate treatment, even PH. It’s crucial for radiologist to recognize these findings [35].
3.2.1.2. Behçet Disease (BD)
Behçet disease (BD) is a rare multisystemic and chronic inflammatory disorder with an unknown cause, and the clinical features of the disease are recurrent oral, genital ulcers and uveitis. The main pathologic process of BD is vasculitis and perivascular infiltration affecting vessels of various sizes; thus the characteristic manifestation of pulmonary artery involvement is pulmonary arterial aneurysm. Due to the vascular inflammation, in situ thrombus is commonly detected which cause stenosis of the distal vessels (Figure 14). CTPA is an important diagnostic imaging technique in the evaluation of patients with BD. The CTPA imaging features of BD are the dilatation of pulmonary arteries lumen with thrombosis, stenosis of the distal vessels, the enhancement of thickened arterial wall, the formation of collateral circulation [36]. Although TA and BD are both vasculitis, pulmonary artery stenosis is relatively common in TA rather than BD. according to the age, gender, and clinical features, it’s not difficult to distinguish these conditions.
3.2.1.3. Swyer James Macleod Syndrome (SJMS)
Swyer-James-MacLeod syndrome (SMJS) is a rare disease characterized by pulmonary artery hypoplasia, unilateral hyperlucency, and bronchiectasis, which is believed to be the result of childhood bronchiolitis obliterans. SJMS is often diagnosed in childhood with chronic pulmonary symptoms, although some patients are diagnosed only in adulthood [37]. Most commonly clinical symptoms of SJMS are cough, recurrent pulmonary infections, decrease in exercise capacity, and hemoptysis. The unilateral hyperlucency can be found on radiographs. Chest CT may demonstrate emphysema, bullae, bronchiectasis, atelectasis, and scarring. CTPA can demonstrate hypoplasia of the pulmonary vasculature in the affected lung or segment (Figure 15). The diagnosis of SJMS is based on clinical symptoms and imaging findings. Histopathology is not essential but further supports the diagnosis, which presents emphysema and cystic cavities in pathological section [37].
3.2.2. Arterial Dissection (AD)
Arterial Dissection (AD) is a lethal condition caused by an elevation in blood pressure leading to the separation of the layers of the media [38], followed by the formation of a false lumen within the arterial wall. Several primary conditions are known to be linked to elevated pulmonary arterial wall stress such as primary hypertension, patent ductus arteriosus (PDA) etc., which lead to the pulmonary AD and stenosis [39] (Figure 16). There are also some secondary conditions. For instance, when dissection happens, discontinuity of the media may involve the pulmonary artery due to the continuous adventitia of aorta and pulmonary artery, which can mimic pulmonary embolism and can be lethal. Without some proper treatments, the rupture of aortic dissection can develop into mediastinal hematoma which presses pulmonary arteries. In other cases, pulmonary AD may through the PDA, which causes adventitia-media separation followed by the intermural hematoma (IMH) [39].
3.3. Extraluminal Abnormalities
3.3.1. Fibrosis Mediastinitis (FM)
Fibrosis mediastinitis (FM) is a benign but lethal condition caused by proliferation of fibrous tissues in the mediastinum with encasement of mediastinal viscera and compression of mediastinal bronchovascular structures, therefore pulmonary hypertension is frequently observed. FM is divided into two subtypes: the granulomatous subtype and the nongranulomatous subtype. And the former one is usually associated with some infectious or inflammatory conditions, such as tuberculosis which is the common cause in China, whereas Histoplasma capsulatum in United states. The later one is less common, diffuse located and more related to autoimmune diseases [39]. The most common clinical symptoms include cough, dyspnea, hemoptysis and pleuritic chest pain. The FM triad of granulomatous subtype includes atelectasis, pleural effusion and prominent right heart border, which is the most typical feature on chest x-ray and CT [40]. Contrast-enhanced CT is the modality of choice for evaluating patients with suspected FM. The major body of the fibrous tissues (often with calcification) locally wrapped the same segment of bronchus and pulmonary vessels is with on or mild enhancement on CTPA and cause the stenosis of affected pulmonary vessels (Figure 17), which is the critical point to distinguish from other diseases (tumor or vasculitis). In contrast, the nongranulomatous subtype often shows the diffused noncalcified soft tissues around the stenosed pulmonary arteries (Figure 18).
3.3.2. Tumour Causing Pulmonary Artery Stenosis
Lung metastatic tumor, primary bronchogenic neoplasia and other tumour may locally invade and obliterate pulmonary arteries. Tumour can invade and grow along pulmonary vessels farther than its lung interface, which can completely obliterate the affected vessel. Tumour also can compress the pulmonary vessels because of mass effect. The pulmonary artery is described as one of the most invaded thoracic vessels in patients with advanced lung cancer, which could lead to life-threatening massive bleeding [41]. CTPA is better in finding tumor that may suggest the diagnosis. Primary lung cancer in CTPA, which often demonstrates compression and narrowing of the pulmonary artery (Figure 19). CT features characterized by wall thickening and lumen narrowing without occlusion is valuable for diagnosis and making surgical plan.
3.3.3. Aortic Aneurysm
Direct compression to pulmonary artery is a rare complication of the giant aortic aneurysm via a mass effect, which can cause pulmonary artery stenosis and even right heart failure [42]. A large aortic aneurysm compressing the adjacent pulmonary artery can be seen on CTA (Figure 20). With the elevated volume and pressure, enlargement of RV also be shown. aortic surgery is needed and CTA makes it easier to understand the anatomy and make proper surgical plan [43].
4. Complications of Radiofrequency Ablation Of Atrial Fibrillation
The complications of radiofrequency ablation of atrial fibrillation are pulmonary vein stenosis, pulmonary vein occlusion, lung infarction [44]. Further, it causes the pulmonary artery on the affected side becomes slender. The mechanism may be the ectopic foci of abnormal electrical activity in the ostia or muscular sleeves of the pulmonary veins, which are the target of ablation [45]. The clinical symptoms are similar to some respiratory diseases, such as dyspnea on exertion of escalating intensity, pleuritic chest pain, hemoptysis, persistent cough, and fever. The gold diagnostic standard is showing venous narrowing or occlusion at cardiac catheterization [46]. As a non-invasive and efficient tool, CTPA shows direct or indirect evidence of occlusion (Figure 21). These included findings of septal thickening in the left upper lobe, increased attenuation in the mediastinal fat adjacent to the left superior pulmonary vein and localized lymphadenopathy [44].
5. Conclusions
Pulmonary artery stenosis or occlusion can be caused by a variety of conditions with some associated with high mortality rates. However, clinical manifestation is often non-specific and insidious. CTPA can make a definitive diagnosis in the majority of the diseases and can also detect other associated conditions. It is important to recognize and classify these pulmonary vascular diseases through analysis of appropriate imaging features, as this is helpful for early diagnosis and interventions. This is especially important in the emergency department, since an accurate clinical evaluation is mandatory, together with diagnostic imaging, to reach a prompt diagnosis.
Author Contributions
Conceptualization, Y.L. and Z.S.; methodology, Q.L.; software, H.Z.; validation, M.Z., L.C. and C.B.; formal analysis, Q.S.; investigation, J.L.; resources, Y.L; data curation, C.B.; writing—original draft preparation, M.Z. and L.C; writing—review and editing, Z.S.; visualization, J.W.; supervision, Y.L.; project administration, Q.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable as this is a pictorial review article with only no patient’s information disclosed.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
Data are not available.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kim, C.W.; Aronow, W. S.; Dutta, T.; Spevack, D.M.; Frishman, W.H. Treatment of peripheral pulmonary artery stenosis. Cardiol. Rev. 2021, 29(3), 115-9. [CrossRef]
- Ngo, M. L. D.; Aggarwal, A.; Knudson, J. D. Peripheral pulmonary artery stenosis: an unusual case and discussion of genetic associations. Congent. Heart. Dis. 2014, 9(5), 448-52. [CrossRef]
- Newman, B.; Alkhori, N. Congenital central pulmonary artery anomalies: Part 2. Pediatr. Radiol. 2020, 50(8), 1030-40.. [CrossRef]
- Ruckdeschel, E.; Kim, Y.Y. Pulmonary valve stenosis in the adult patient: pathophysiology, diagnosis and management. Heart. 2019, 105, 414-422. [CrossRef]
- Castneda-Zuniga, W.R.; Formanek, A.; Amplatz, K. Radiologic diagnosis of different types of pulmonary stenoses. Cardiovasc. Radiol.1978, 1, 45-57. [CrossRef]
- Escalon, J.G.; Browne, L.P.; Bang, T.J.; Restrepo, C.S.; Ocazionez, D.; Vargas, D. Congenital anomalies of the pulmonary arteries: an imaging overview. Br. J. Radiol. 2019, 92(1093): 20180185. [CrossRef]
- Newman, B.; Alkhori, N. Congenital central pulmonary artery anomalies: Part 1. Pediatr. Radiol. 2020, 50(8), 1022-9. [CrossRef]
- Romberg, E.K.; Stanescu, A.L.; Bhutta, S.T.; Otto, R.K.; Ferguson, M.R. Computed tomography of pulmonary veins: review of congenital and acquired pathologies. Pediatr. Radiol. 2022, 52, 2510-2528. [CrossRef]
- Tang, C.; Duan, H.; Zhou, K,; Hua, Y.; Lu, X.; Li, X.; Wang, C. Isolated unilateral pulmonary vein atresia with hemoptysis in a child: A case report and literature review. Medicine (Baltimore). 2018, 97(34), e11882. [CrossRef]
- Khan, F.; Tritschner, T.; Kahn, S.R.; Rodger, M.A. Venous thromboembolism. Lancet. 2021, 398, 64-77. [CrossRef]
- Alp-Zaher, N.; Vitali, F.; Neurath, M.; Goertz, R.S. The positive rate of pulmonary angiography is high in an emergency department, even in low-risk or young patients. Med. Princ. Prac. 2021, 30:37-44.
- Palm, V.; Rengier, F.; Rajiah. P.; Heussel, C.P.; Partovi, S. Acute pulmonary embolism: Imaging techniques, findings, endovascular treatment and differential diagnosis. Rofo. 2020, 192:38-49. [CrossRef]
- Boon, G.J.A.; Ende-Verhaar, Y.M.; Beenen, L.F.; Coolen, J.; Delcroix, M.; Golebiowski, M.; et al. Prediction of chronic thromboembolic pulmonary hypertension with standardised evaluation of initial computed tomography pulmonary angiography performed for suspected acute pulmonary embolism. Eur. Radiol. 2022, 32, 2178-2187. [CrossRef]
- Castaner, E.; Gallardo, X.; Rimola, J.; Pallardo, Y.; Mata, J.M.; Perendreu, J.; Martin, C.; Gil, D. Congenital and acquired pulmonary artery anomalies in the adult: radiologic overview. Radiographics. 2006, 26(2), 349-71. [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Heart. J. 2020, 41(4), 543-603.
- Fletcher-Sanfeliu, D.; Redon, J.; Garcia-Granero, A.; Frasson, M.; Barreira, I.; Martinez-Leon, J.; Garcia-Fuster, M.J. Pulmonary thrombosis in situ’: risk factors, clinic characteristics and long-term evolution. Blood. Coagul. Fibrinolysis. 2020, 31(7), 469-75. [CrossRef]
- Cao, Y.; Geng, C.; Li, Y.; Zhang, Y. In situ pulmonary artery thrombosis: a previously overlooked disease. Front. Pharmacol. 2021, 12, 671589. [CrossRef]
- Baranga, L.; Khanuja, S.; Scott, J.A.; Provancha, I.; Gosselin, M.; Walsh, J.; Arancibia, R.; Bruno, M.A.; Waite, S. In Situ Pulmonary Arterial Thrombosis: Literature Review and Clinical Significance of a Distinct Entity. AJR. Am. J. Roentgenol. 2023, 221. 57-68. [CrossRef]
- Sahiti, S.; Rotman, S.; Benmachiche, M. Pulmonary tumor embolism. Rev. Med. Suisse. 2021, 17, 2034-2037.
- Lashari, B.H.; Kumaran, M.; Aneja, A.; Bull, T.; Rali, P. Beyond clots in the pulmonary circulation: pulmonary artery tumors mimicking pulmonary embolism. Chest. 2022, 161(6), 1642-50.. [CrossRef]
- Rajev, K.; Madan, U.; McMilan, S.; Wilson, K.; Fisher, K.; Hein, A. et al. Pulmonary tumor embolism and pulmonary tumor thrombotic microangiopathy causing rapidly progressive respiratory failure: a case series. J. Investig. Med. High. Impact. Case. Rep. 2022, 10, 23247096221086453. [CrossRef]
- Kwon, W.J.; Jeong, Y.J.; Kim, K.I.; Lee, I.S.; Jeon, U.B.; Lee, S.H, Kim, Y.D. Computed tomographic features of pulmonary septic emboli: comparison of causative microorganisms. J. Comput. Assist. Tomogr. 2007, 31(3) 390-4. [CrossRef]
- Kuhlman, J.E.; Fishman, E.K.; Teigen, C. Pulmonary septic emboli: diagnosis with CT. Radiology. 1990, 174(1): 211-3. [CrossRef]
- Matuscov, Y.; Tapson, V.F. Radiologic mimics of pulmonary embolism. Postgrad. Med. 2021, 133(sup1), 64-70. [CrossRef]
- Ye, R.; Zhao, L.; Wang, C.; Wu, X.; Yan, H. Clinical characteristics of septic pulmonary embolism in adults: a systematic review. Respir. Med. 2014, 108(1), 1-8. [CrossRef]
- Bach, A.G.; Restrepo, C.S.; Abbas, J.; Villanueva, A.; Lorenzo Dus, M.J, Schopf, R. et al. Imaging of nonthrombotic pulmonary embolism: biological materials, nonbiological materials, and foreign bodies. Eur. J. Radiol. 2013, 82(3), e120-e41. [CrossRef]
- McCabe, B.E.; Veseleis, C.A.; Goykhman, I.; Hochhold, J.; Eisenberg, D.; Son, H. Beyond pulmonary embolism; nonthrombotic pulmonary embolism as diagnostic challenges. Curr. Probl. Diagn. Radiol. 2019, 48(4), 387-92. [CrossRef]
- Unal, E.; Balci, S.; Atceken, Z.; Akpinar, E.; Ariyurek, O.M. Nonthrombotic pulmonary artery embolism: imaging findings and review of the literature. AJR. Am. J. Roentgenol. 2017, 208(3), 505-16. [CrossRef]
- Trongtorsak, A.; Tumkosit, M.; Chantranuwatana, P.; Ariyachaipanich, A.; Chattranukulchai, P.; Boonyaratavej, S.; Puwanant, S. Pulmonary artery sarcoma: an unusual cause of acquired supravalvular pulmonary stenosis. Cir. Cardiovass. Imaging. 2020, 13(1), e009932. [CrossRef]
- Yin, K.; Zhang, Z.; Luo, R.; Ji, Y.; Zheng, D.; Lin, Y.; Wang, C. Clinical features and surgical outcomes of pulmonary artery sarcoma. J. Thorac. Cardiovasc. Surg. 2018, 155(3), 1109-15. e1. [CrossRef]
- Liu, M.X.; Ma, Z.H.; Jiang, T.; Guo, X.J.; Yu, F.F.; Yang, Y.H.; Zhai, Z.G. Differential diagnosis of pulmonary artery sarcoma and central chronic pulmonary thromboembolism using CT and MR images. Heart Lung. Circ. 2018, 27(7), 819-27. [CrossRef]
- Kronzer, E.; Robinson, S.I.; Collins, D.A.; McBane 2nd, R.D. Primary pulmonary artery sarcoma versus pulmonary thromboembolism: a multimodal imaging comparison. J. Thromb. Thrombolysis. 2021, 52(4), 1129-32. [CrossRef]
- Adams, T.N.; Zhang, D.; Batra., K.; Fitzgerald, J.E. Pulmonary manifestations of large, medium, and variable vessel vasculitis. Respir. Med. 2018, 145, 182-91. [CrossRef]
- Xi, X.; Du, J.; Liu, J.; Zhu, G.; Qi, G.; Pan, L. Pulmonary artery involvement in Takayasu arteritis: a retrospective study in Chinese population. Clin. Rheumatol. 2021, 40, 635-44. [CrossRef]
- Saadoun, D.; Vautier, M.; Cacoub, P. edium-and large-vessel vasculitis. Circulation. 2021, 143(3), 267-82.
- Odev, K.; Tunc, R.; Varol, S.; Aydemir, H.; Yilmaz, P.D.; Korkmaz, C. Thoracic complications in Behçet’s disease: imaging findings. Can. Respir. J. 2020, 2020, 4649081. [CrossRef]
- Aksoy, E.; Aktas, O.; Tokgoz, F.; Kongar, N.; Goksenoglu, N.; Bodur, Y. et al. Cases diagnosed with Swyer James Macleod syndrome in adulthood. Turk. Thorac. J. 2015, 16(1), 36-42. [CrossRef]
- Yuan, X.; Mitsis, A.; Nienaber, C.A. Current understanding of aortic dissection. Life (Basel). 2022, 12(10), 1606. [CrossRef]
- Seferian, A.; Steriade, A.; Jais, X.; Planche, O.; Savale, L.; Parent F, et al. Pulmonary hypertension complicating fibrosing mediastinitis. Medicine. 2015, 94(44), e1800. [CrossRef]
- Zhou, M.; Li, B.; Chen, Y.; Wang, A.; Zhu, Y.; Li, Y, et al. Chest X-ray features facilitate screening for pulmonary hypertension caused by fibrosing mediastinitis. Ther. Adv. Chronic. Dis. 2022, 13, 20406223221143245. [CrossRef]
- Han, C.B.; Wang, W.L.; Quint, L.; Xue, J.X.; Matuszak, M.; Haken, R.T.; Kong, F.M. Pulmonary artery invasion, high-dose radiation, and overall survival in patients with non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89(2), 313-21. [CrossRef]
- Sugiyama, H.; Tohma, R.; Misato, T.; Okamoto, K.; Hayashi, T.; Tobe, S, et al. Right heart failure caused by direct pressure of distal arch aneurysm. Gen. Thoracic. Cardiovasc. Surg. 2019; 67, 263-265. [CrossRef]
- Abe, T.; Kamikubo, Y.; Taneichi, T,; Terada, T.; Sugiura, J.; Sakurai, T.; Tsuboi, N.; Sakurai, H. Right heart failure secondary to compression of the right pulmonary artery by a large proximal aortic aneurysm. Circulation; 2013: 128(14), 1588-9. [CrossRef]
- Alfudhili, K.M.; Hassan, H.H.; Abdullah, H.; Sherbiny, M. Pulmonary vein occlusion and lung infarction complicating non-treated moderate single pulmonary vein stenosis after radiofrequency ablation of atrial fibrillation. BJR|. Case. Rep. 2017, 18, 20160091. [CrossRef]
- Xu, L.; Cui, L.; Hou, J.; Wang, J.; Chen, B.; Xue, X.; Yang, Y.; Wu, J.; Chen, J. Clinical characteristics of patients with atrial fibrillation suffering from pulmonary vein stenosis after radiofrequency ablation. J. Int. Med. Res. 2020; 48(3), 0300060519881555. [CrossRef]
- Ravenel, J.G.; McAdams, H.P. Pulmonary venous infarction after radiofrequency ablation for atrial fibrillation. AJR. Am. J. Roentgenol. 2002, 178(3), 664-6. [CrossRef]
Figure 1.
Pulmonary valvular stenosis- bicuspid pulmonary valve. A: chest radiograph shows the prominence of left pulmonary artery and the right pulmonary artery (arrow) and hilum appear normal. B-C and D-E: belong to two different patients, but both show the stenotic bicuspid pulmonary valve (arrow) and poststenotic dilation of the main and left pulmonary artery, whereas the distal branches are relatively small. The jet of blood flow (arrow) forces through the stenotic valve to the left pulmonary artery on E. F: Volumeb rendering of pulmonary arteries indicate the poststenotic dilation of the main and left pulmonary artery.
Figure 1.
Pulmonary valvular stenosis- bicuspid pulmonary valve. A: chest radiograph shows the prominence of left pulmonary artery and the right pulmonary artery (arrow) and hilum appear normal. B-C and D-E: belong to two different patients, but both show the stenotic bicuspid pulmonary valve (arrow) and poststenotic dilation of the main and left pulmonary artery, whereas the distal branches are relatively small. The jet of blood flow (arrow) forces through the stenotic valve to the left pulmonary artery on E. F: Volumeb rendering of pulmonary arteries indicate the poststenotic dilation of the main and left pulmonary artery.
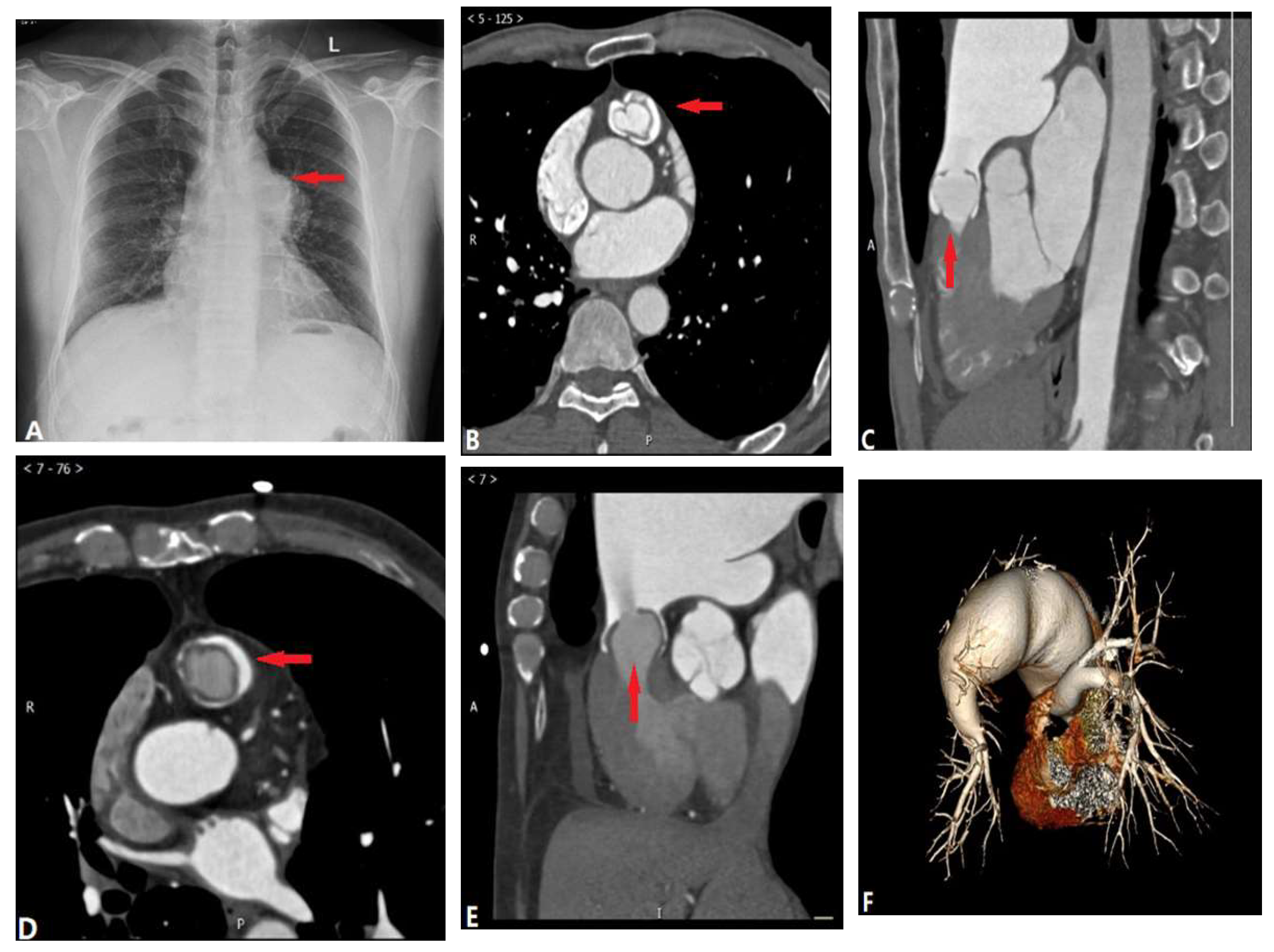
Figure 2.
Pulmonary artery atresia with ventricular septal defect. A: Coronal CT angiography shows that the main pulmonary artery was atretic and right pulmonary artery was slender (arrow). B: Oblique coronal CT shows outlet ventricular septal defect (arrow) and overriding aorta (AO). C: Oblique coronal CT demonstrates patent ductus arteriosus (arrow) originating from aorta to left pulmonary artery.
Figure 2.
Pulmonary artery atresia with ventricular septal defect. A: Coronal CT angiography shows that the main pulmonary artery was atretic and right pulmonary artery was slender (arrow). B: Oblique coronal CT shows outlet ventricular septal defect (arrow) and overriding aorta (AO). C: Oblique coronal CT demonstrates patent ductus arteriosus (arrow) originating from aorta to left pulmonary artery.
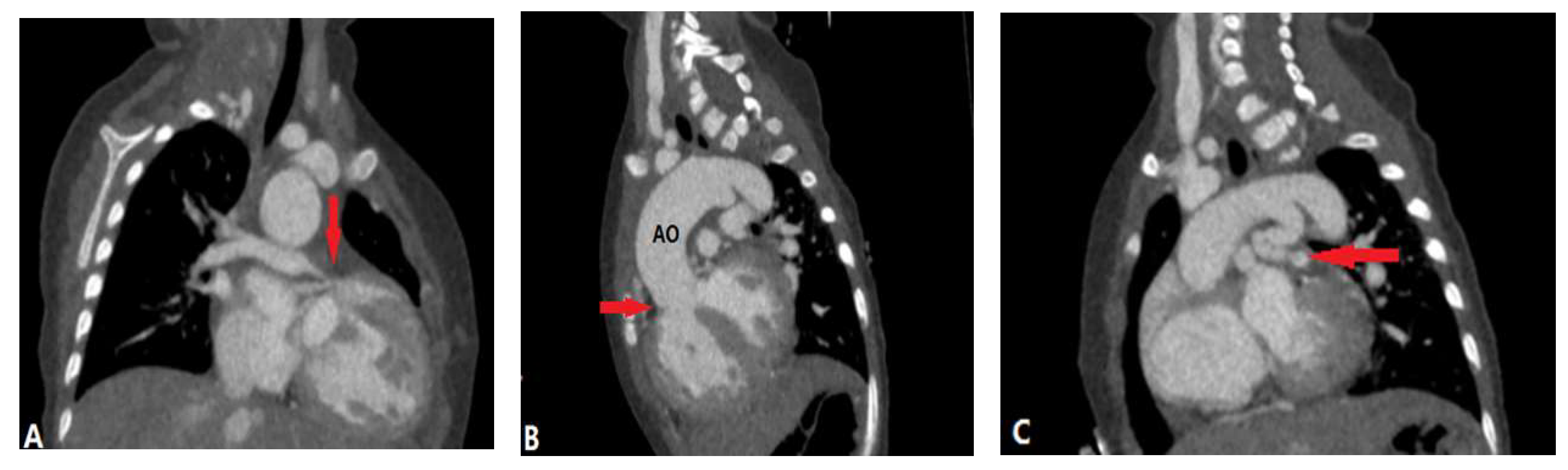
Figure 3.
Unilateral Pulmonary vein atresia. A: coronal CTA shows the absent of right pulmonary veins and without outpouchings on the left atrium (arrow). B-C: MIP and lung windowing coronal CT images show mass-like soft-tissue within the right hilum (arrow in B), the septal lines and bronchial wall thickening (arrow in C) which indicates the engorged lymphatics and collateral venous channels. D: VR of CTA shows the small caliber of right pulmonary arteries. CTA-computed tomography angiography, MIP-maximum-intensity projection, VR-volume rendering.
Figure 3.
Unilateral Pulmonary vein atresia. A: coronal CTA shows the absent of right pulmonary veins and without outpouchings on the left atrium (arrow). B-C: MIP and lung windowing coronal CT images show mass-like soft-tissue within the right hilum (arrow in B), the septal lines and bronchial wall thickening (arrow in C) which indicates the engorged lymphatics and collateral venous channels. D: VR of CTA shows the small caliber of right pulmonary arteries. CTA-computed tomography angiography, MIP-maximum-intensity projection, VR-volume rendering.
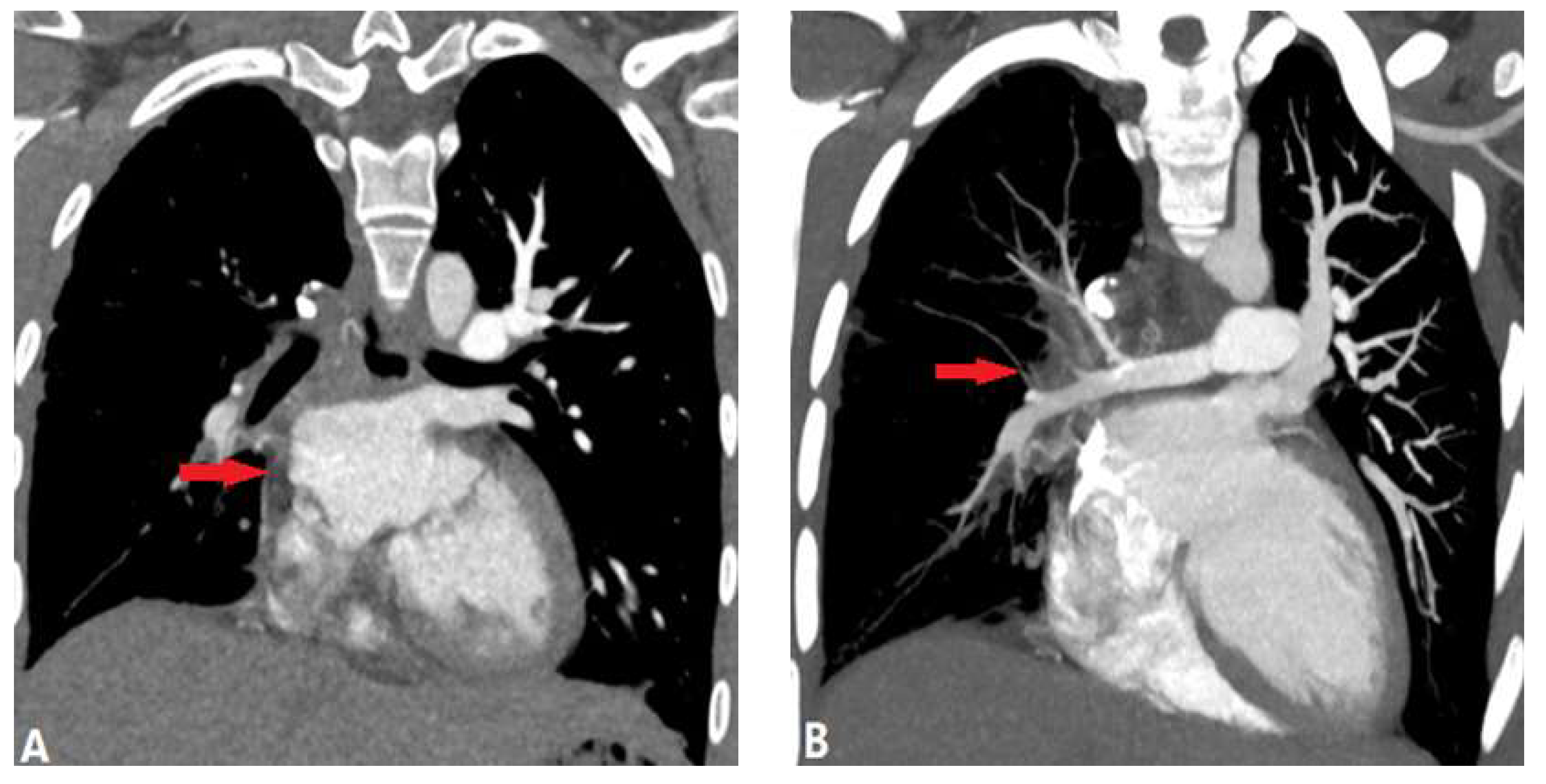
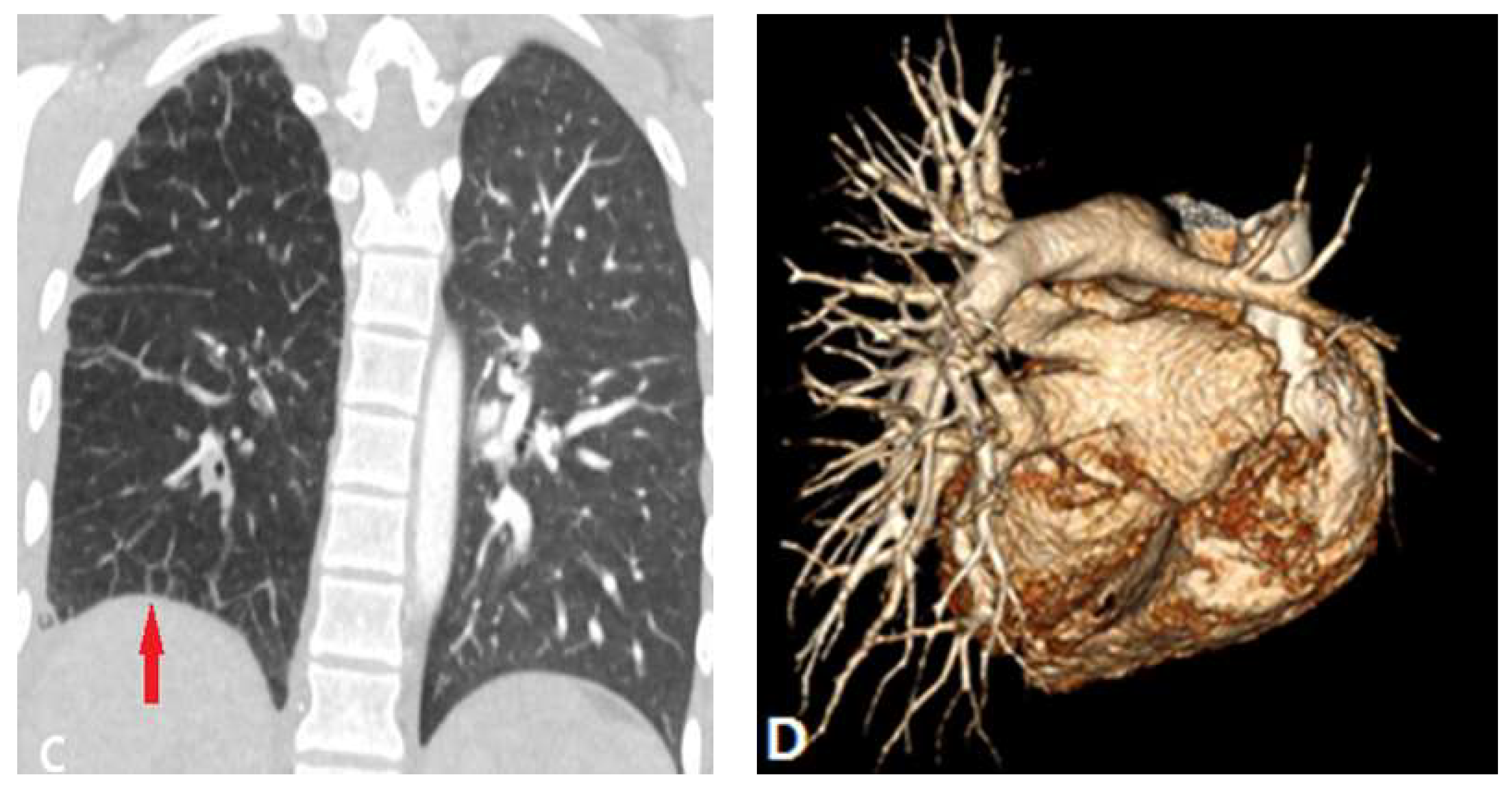
Figure 4.
Pulmonary thromboembolism. A: Axial CT images shows a partial filling defects in the left and right pulmonary arteries, which is non-enhanced and surrounded with contrast (arrow). B: Axial CT image shows the enlargement of right ventricle and atrium (RV:LV ratio >1) and 3D volume rendering image (C) shows the range of thrombus which is marked with red colors. D: Axial CT image shows the complete filling defects of another patient, which presents no enhancement of the entire lumen (arrow) and subpleural pulmonary infarction. E: Axial CT image of another patient who underwent the thrombolytic therapy shows the partial filling defects in pulmonary artery. F: After 4 months treatment, there are some band-like enhancements (arrow) in the thrombus which means thrombolysis. LV-left ventricle, RV-right ventricle.
Figure 4.
Pulmonary thromboembolism. A: Axial CT images shows a partial filling defects in the left and right pulmonary arteries, which is non-enhanced and surrounded with contrast (arrow). B: Axial CT image shows the enlargement of right ventricle and atrium (RV:LV ratio >1) and 3D volume rendering image (C) shows the range of thrombus which is marked with red colors. D: Axial CT image shows the complete filling defects of another patient, which presents no enhancement of the entire lumen (arrow) and subpleural pulmonary infarction. E: Axial CT image of another patient who underwent the thrombolytic therapy shows the partial filling defects in pulmonary artery. F: After 4 months treatment, there are some band-like enhancements (arrow) in the thrombus which means thrombolysis. LV-left ventricle, RV-right ventricle.
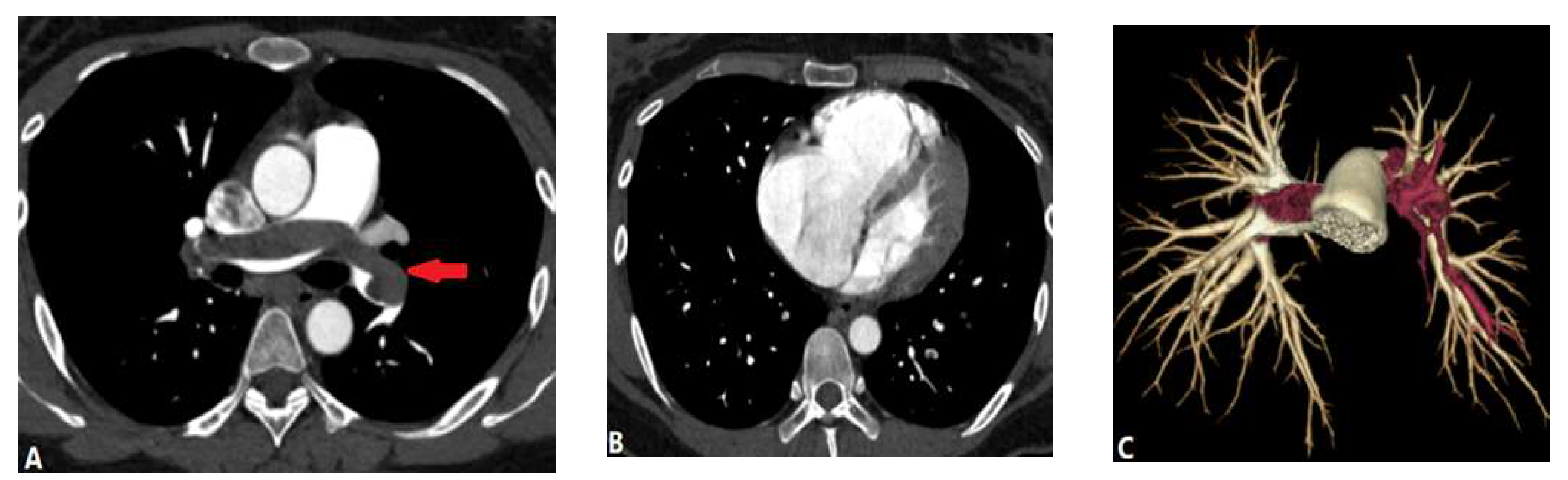
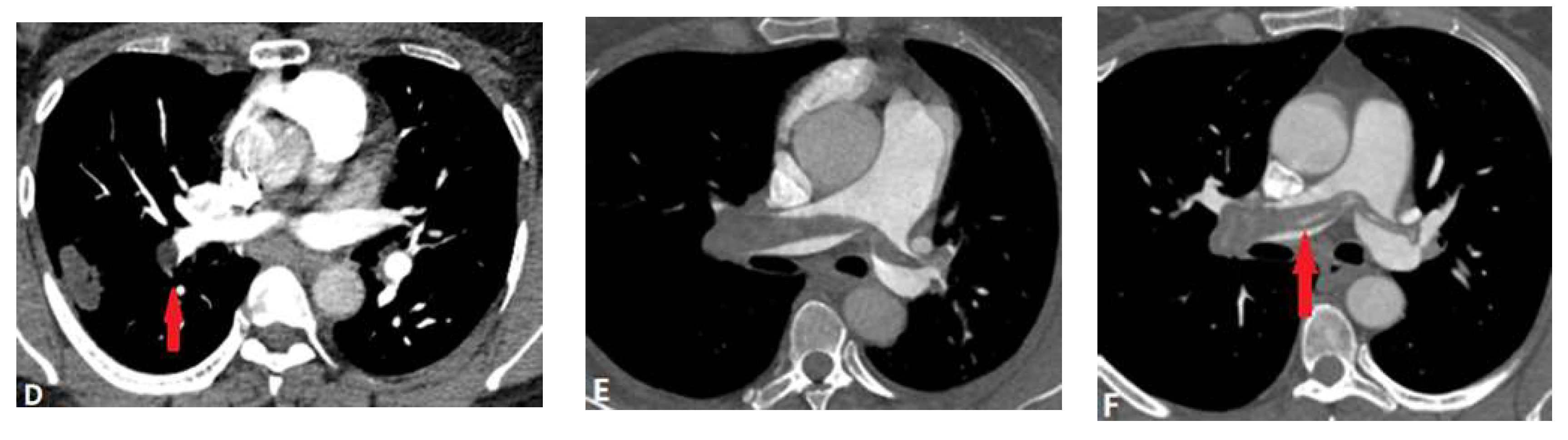
Figure 5.
Chronic pulmonary embolism. A: Axial CT image shows bilateral eccentric laminated filling defects and pulmonary arteries stenosis in the pulmonary arteries (arrows) in a patient with chronic pulmonary embolism. B: Coronal reconstruction CTA image in another patient with dyspnea shows a web (arrows) or band within a right lower lobar pulmonary artery, consistent with chronic PE. C: Coronal reconstruction CTA image in a patient with history of acute PE shows calcified obstructive thrombus (arrows) within bilateral pulmonary arteries. CTA-computed tomography angiography, PE-pulmonary embolism.
Figure 5.
Chronic pulmonary embolism. A: Axial CT image shows bilateral eccentric laminated filling defects and pulmonary arteries stenosis in the pulmonary arteries (arrows) in a patient with chronic pulmonary embolism. B: Coronal reconstruction CTA image in another patient with dyspnea shows a web (arrows) or band within a right lower lobar pulmonary artery, consistent with chronic PE. C: Coronal reconstruction CTA image in a patient with history of acute PE shows calcified obstructive thrombus (arrows) within bilateral pulmonary arteries. CTA-computed tomography angiography, PE-pulmonary embolism.
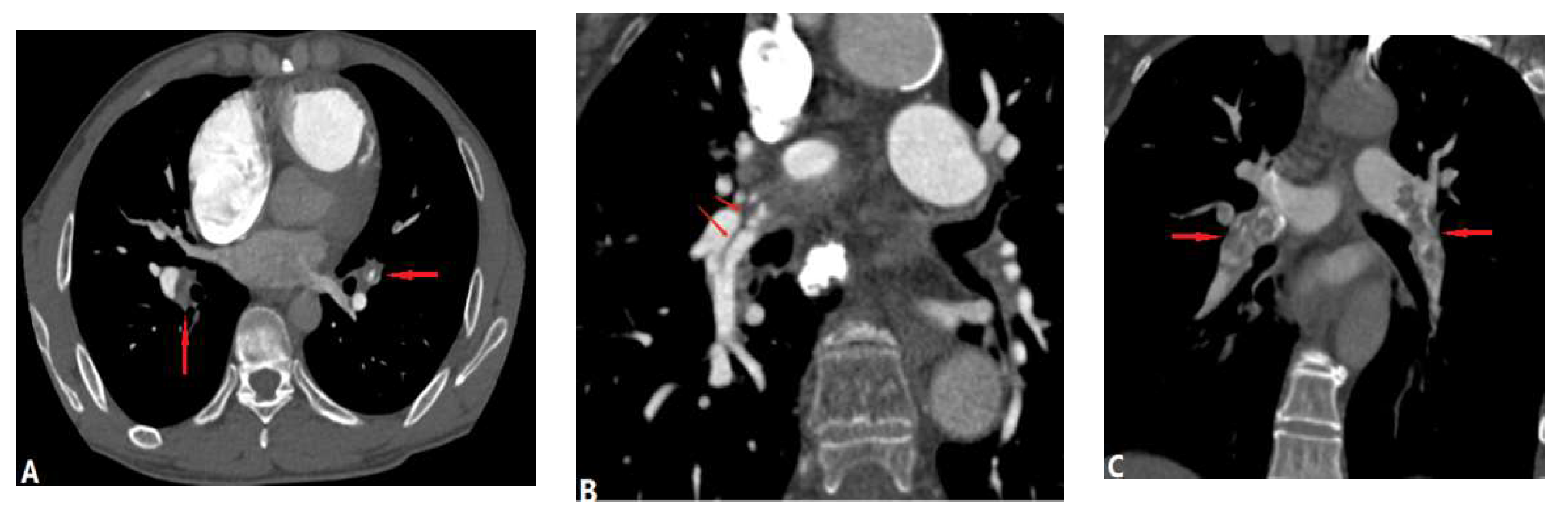
Figure 6.
In situ thrombosis in pulmonary hypertension in a 16-year-old girl with primary pulmonary hypertension. A and B: Axial and coronal CTA image show concentric, broad-based filling defects within massively dilated right pulmonary artery and the lumen (blood filing) is narrowed locally (arrow). The main and the left pulmonary arteries are also enlarged. C: Cross section of left pulmonary artery in MPR imaging show interface irregularities (arrow) of the thrombosis within the symmetric widening and smooth outline of the vessel, which rule out compression caused by mass effect. CTA-computed tomography angiogrpahy, MPR-multiplanar reformation.
Figure 6.
In situ thrombosis in pulmonary hypertension in a 16-year-old girl with primary pulmonary hypertension. A and B: Axial and coronal CTA image show concentric, broad-based filling defects within massively dilated right pulmonary artery and the lumen (blood filing) is narrowed locally (arrow). The main and the left pulmonary arteries are also enlarged. C: Cross section of left pulmonary artery in MPR imaging show interface irregularities (arrow) of the thrombosis within the symmetric widening and smooth outline of the vessel, which rule out compression caused by mass effect. CTA-computed tomography angiogrpahy, MPR-multiplanar reformation.
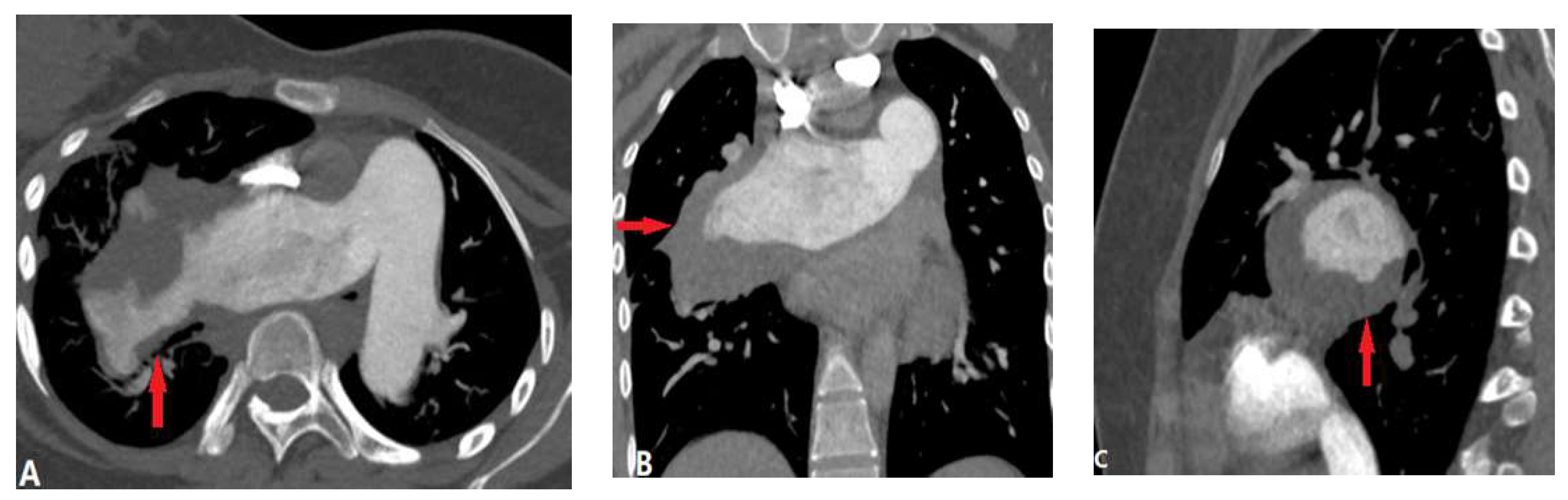
Figure 7.
Tumor embolism (benign). A: Sagittal MPR image in a patient with intravenous leiomyomatosis shows tumor embolism in the main pulmonary artery. B: Coronal MPR image shows the tumor originates from uterus, along the left ovarian vein-left renal vein-inferior vena cava-right atrium-right ventricle and then extend into pulmonary artery (arrows). C. Photograph of the resected tumor. MPR-multiplanar reformation.
Figure 7.
Tumor embolism (benign). A: Sagittal MPR image in a patient with intravenous leiomyomatosis shows tumor embolism in the main pulmonary artery. B: Coronal MPR image shows the tumor originates from uterus, along the left ovarian vein-left renal vein-inferior vena cava-right atrium-right ventricle and then extend into pulmonary artery (arrows). C. Photograph of the resected tumor. MPR-multiplanar reformation.
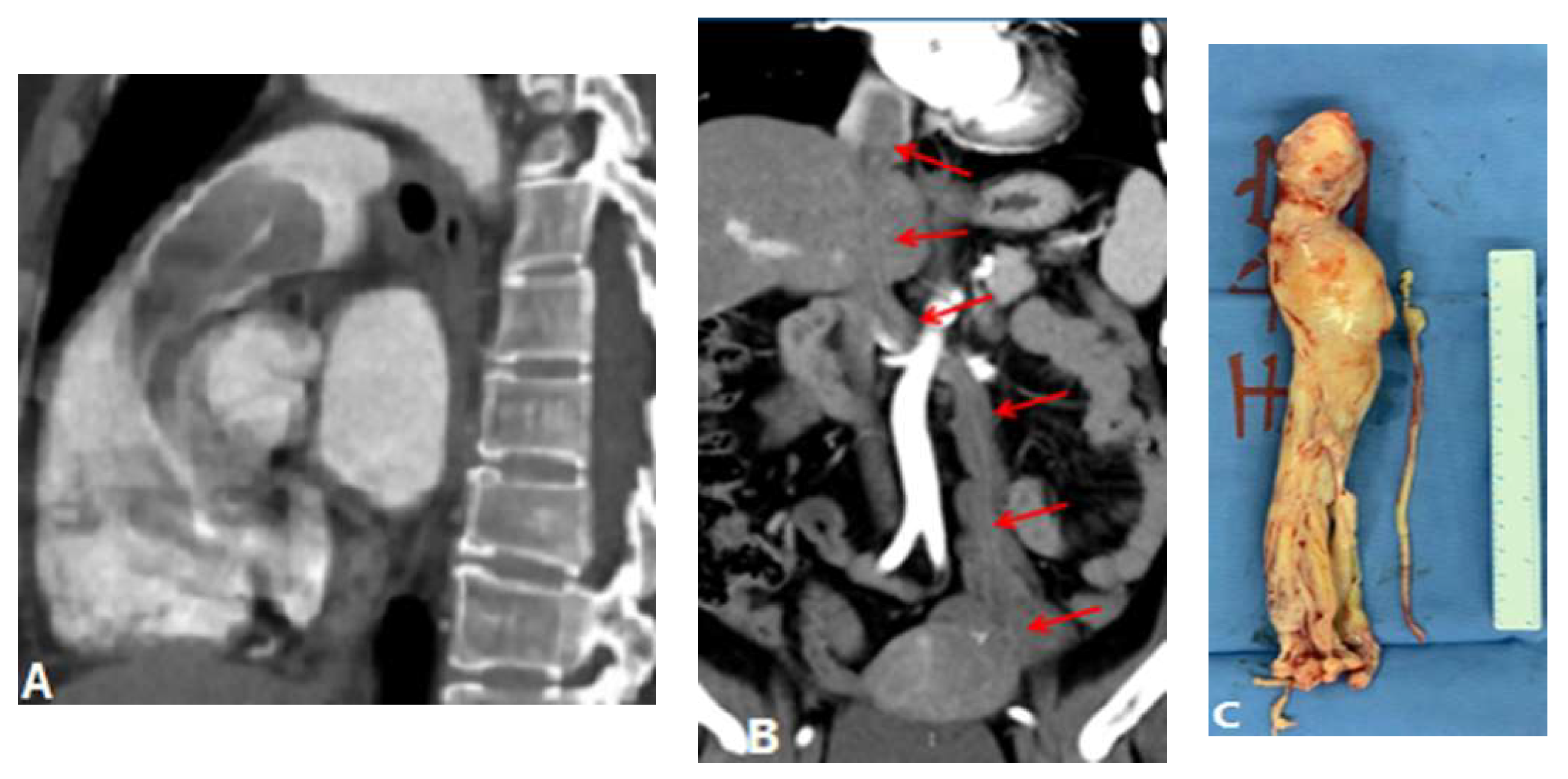
Figure 8.
Tumor embolism and PTTM. A: Coronal CT MPR image in a patient with right lung cancer shows tumor emboli in the subsegmental pulmonary arterial branches (arrows) and the lumen occlusion. B: Coronal CT scan image at the same level with soft tissue windowing shows the vascular dilatation and beading of subsegmental arteries of the right pulmonary artery (arrows). C: CT in another patient with right atrium tumor shows tumor emboli with a tree-in-bud appearance within secondary lobule arteries (short arrow) and beading of subsegmental arteries (long arrow), which indicate PTTM.
Figure 8.
Tumor embolism and PTTM. A: Coronal CT MPR image in a patient with right lung cancer shows tumor emboli in the subsegmental pulmonary arterial branches (arrows) and the lumen occlusion. B: Coronal CT scan image at the same level with soft tissue windowing shows the vascular dilatation and beading of subsegmental arteries of the right pulmonary artery (arrows). C: CT in another patient with right atrium tumor shows tumor emboli with a tree-in-bud appearance within secondary lobule arteries (short arrow) and beading of subsegmental arteries (long arrow), which indicate PTTM.
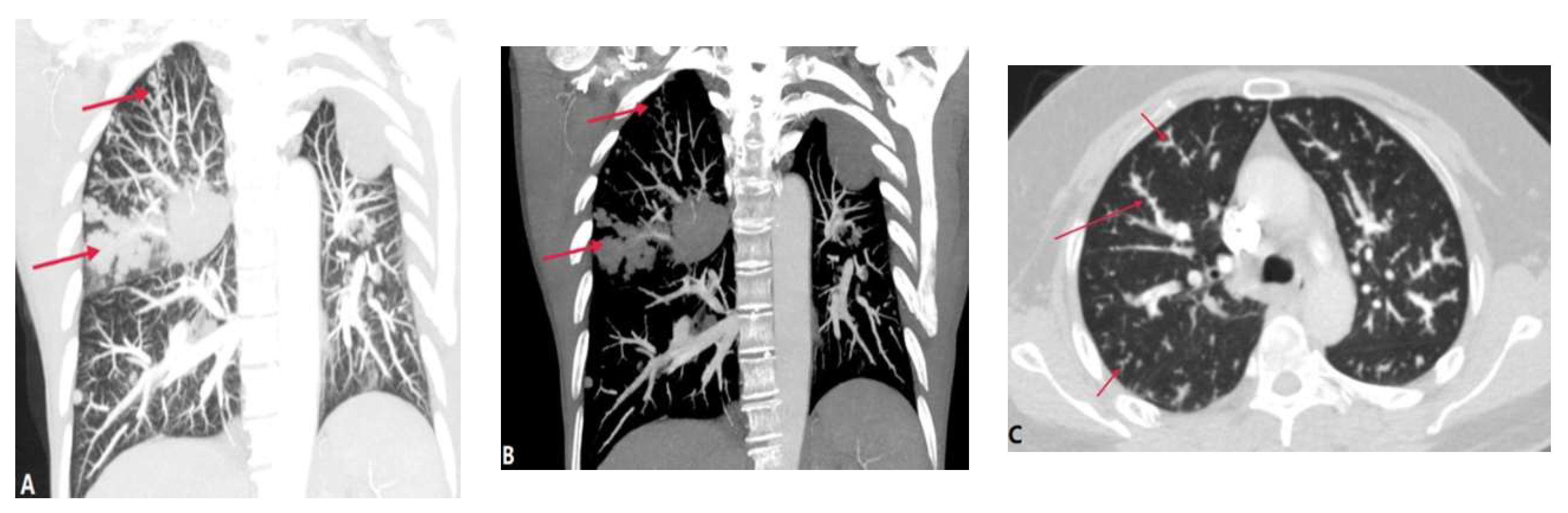
Figure 9.
Septic pulmonary embolism in a 29-year-old woman with PDA and infective endocarditis. A and B: Sagittal and axial CTPA images demonstrate a filling defect within the main pulmonary artery (long arrow)-at the end of PDA (short arrow). C: Axial CTPA on lung windowing shows subpleural opacity, consistent with peripheral infarction (arrow) which may be caused by the septic emboli. CTPA-computed tomography pulmonary angiography, PDA-patent ductus arteriosus.
Figure 9.
Septic pulmonary embolism in a 29-year-old woman with PDA and infective endocarditis. A and B: Sagittal and axial CTPA images demonstrate a filling defect within the main pulmonary artery (long arrow)-at the end of PDA (short arrow). C: Axial CTPA on lung windowing shows subpleural opacity, consistent with peripheral infarction (arrow) which may be caused by the septic emboli. CTPA-computed tomography pulmonary angiography, PDA-patent ductus arteriosus.
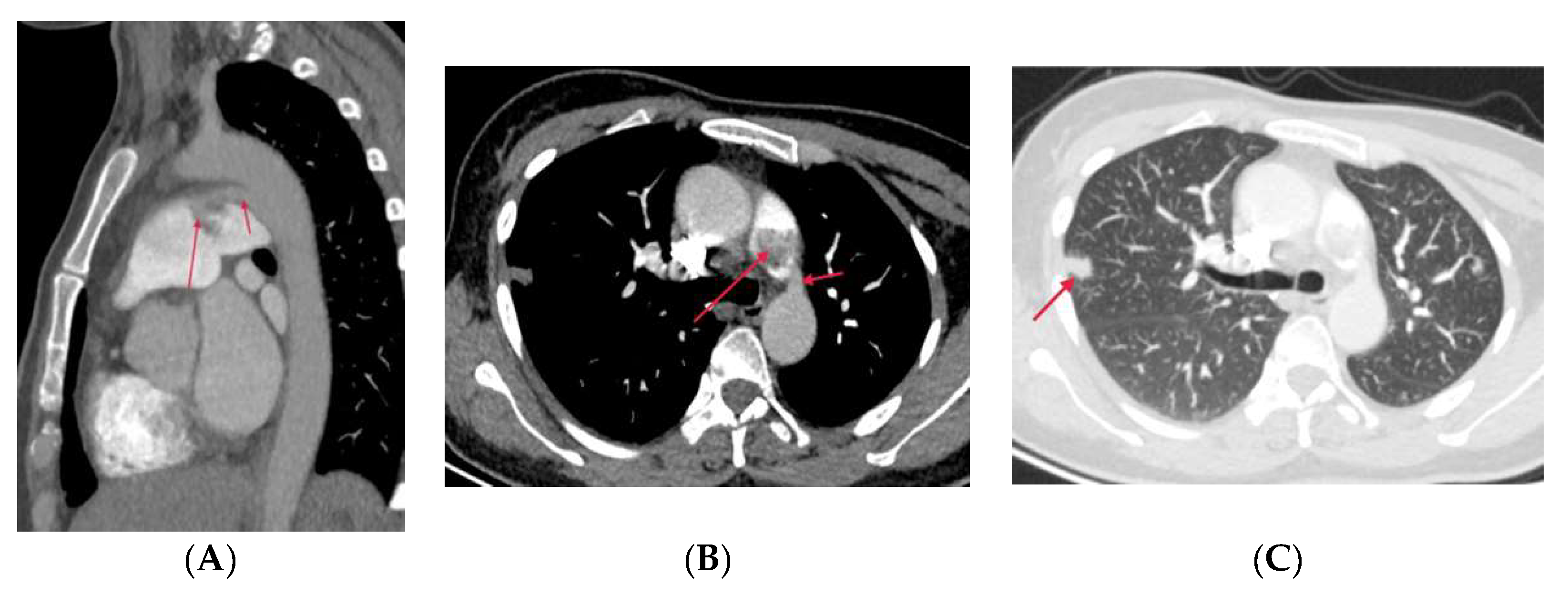
Figure 10.
Pulmonary cement embolism. A and B: axial CTPA and coronal MIP shows the cement embolus (high density) in the pulmonary arteries of right and left upper lobes. C: cement in the vertebral body and the external vertebral venous plexuses. CTPA- computed tomography pulmonary angiography, MIP-maximum-intensity projection.
Figure 10.
Pulmonary cement embolism. A and B: axial CTPA and coronal MIP shows the cement embolus (high density) in the pulmonary arteries of right and left upper lobes. C: cement in the vertebral body and the external vertebral venous plexuses. CTPA- computed tomography pulmonary angiography, MIP-maximum-intensity projection.
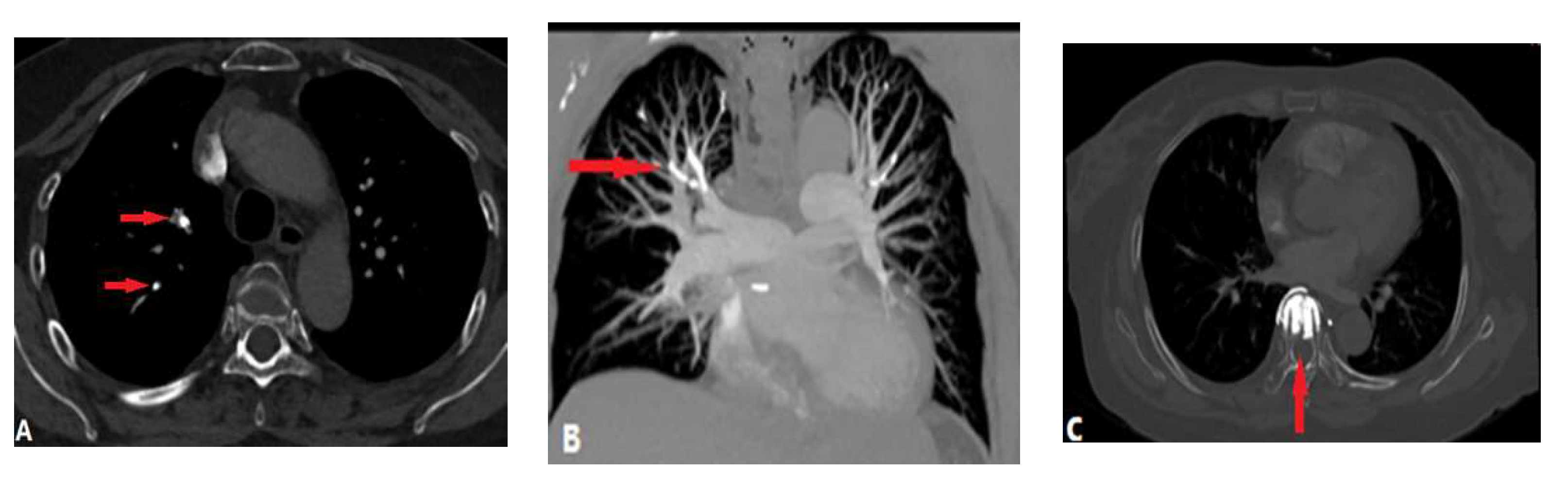
Figure 11.
Catheter-related thrombosis in a patient post-CABG. A. Axial CTA image shows filling defects extend from the main pulmonary to right pulmonary artery along with the catheter. B. Coronal CTA image shows the thrombus wrap around the catheter (arrow). C. Maximum-intensity projection image shows the path of the catheter and the peripheral consolidation, which is consistent with pulmonary infarction (arrows). CABG-coronary artery bypass grafting, CTA-computed tomography angiography.
Figure 11.
Catheter-related thrombosis in a patient post-CABG. A. Axial CTA image shows filling defects extend from the main pulmonary to right pulmonary artery along with the catheter. B. Coronal CTA image shows the thrombus wrap around the catheter (arrow). C. Maximum-intensity projection image shows the path of the catheter and the peripheral consolidation, which is consistent with pulmonary infarction (arrows). CABG-coronary artery bypass grafting, CTA-computed tomography angiography.
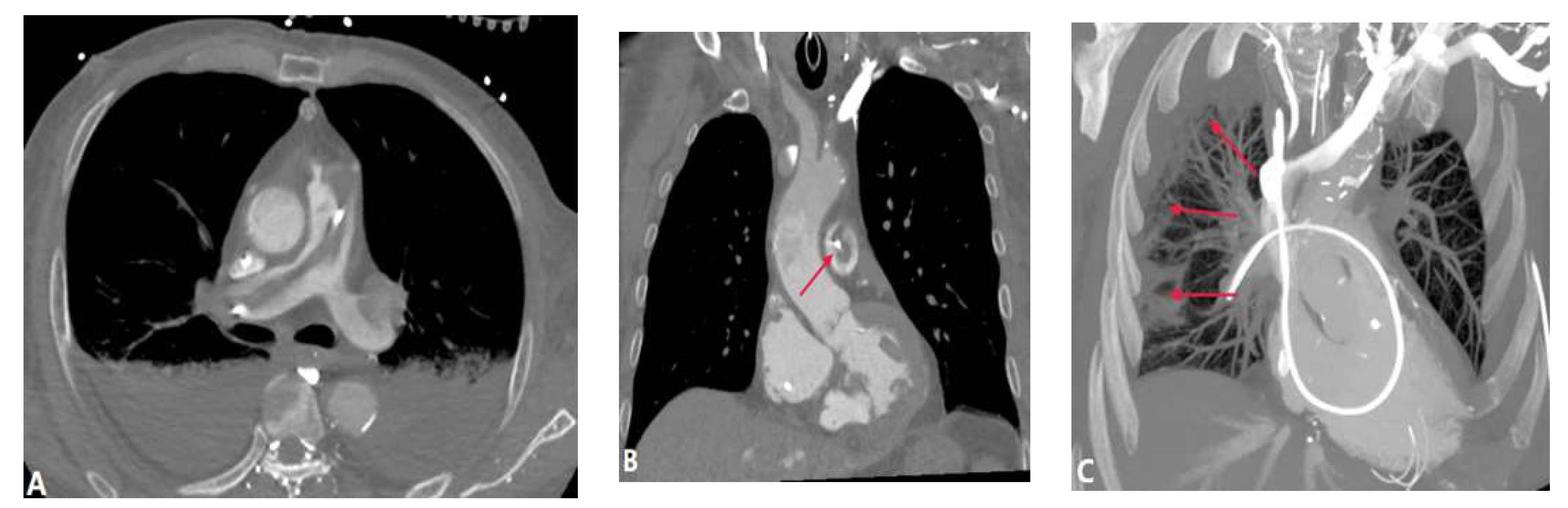
Figure 12.
Pulmonary artery sarcoma with extensive involvement of the main pulmonary artery and into the right trunk. A: Contrast-enhanced CT showing a soft tissue mass filling the main and left pulmonary arteries (arrow). B: The filling defects shows delayed enhancement.
Figure 12.
Pulmonary artery sarcoma with extensive involvement of the main pulmonary artery and into the right trunk. A: Contrast-enhanced CT showing a soft tissue mass filling the main and left pulmonary arteries (arrow). B: The filling defects shows delayed enhancement.
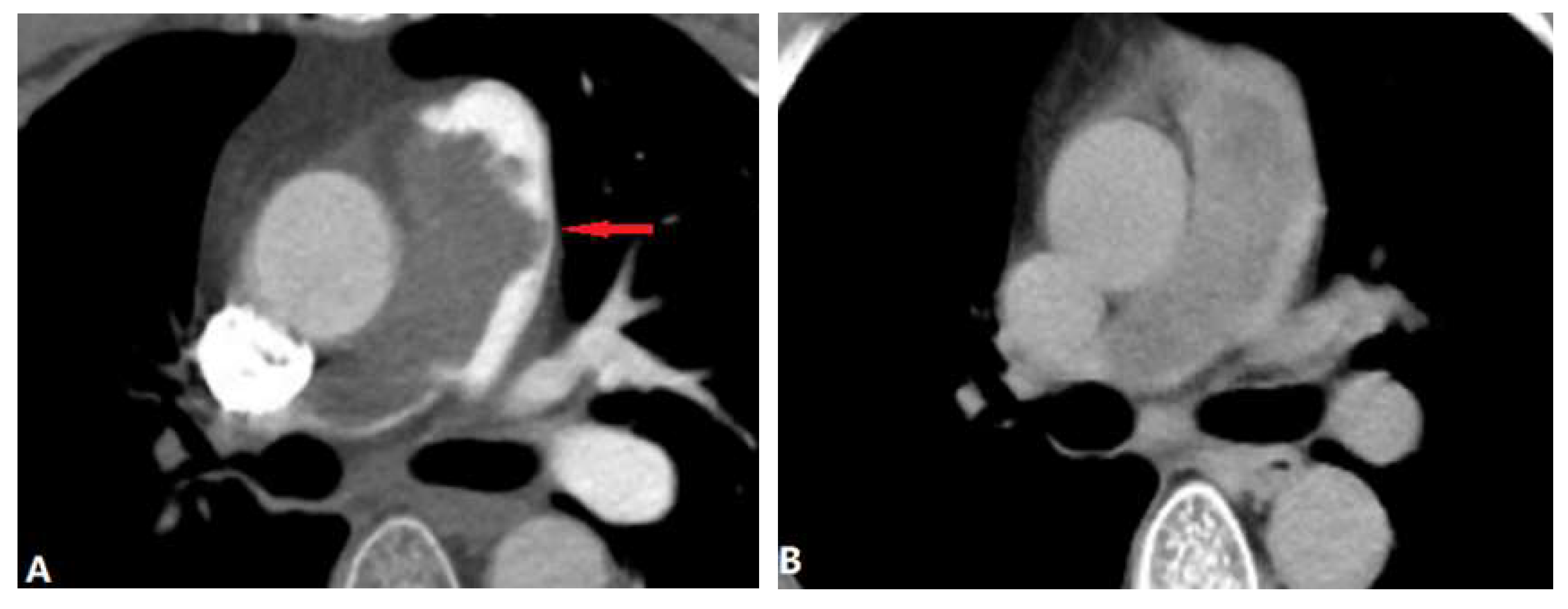
Figure 13.
Vasculitis-ralated pulmonary artery thrombosis. Takayasu arteritis in a 33-year-old woman with dizziness and chest compress. A: Contrast-enhanced axial CT demonstrates filling defect and occlusion of the right pulmonary artery wall (arrow) and the main pulmonary is dilated. B: Axial CT image shows the wall of right subclavian artery and right common carotid artery are thickening and the lumen is narrow (arrow). C: Coronal MIP contrast-enhanced MRA image shows the right brachicephalic artery, right subclavian artery and right common carotid artery are stenosis or occlusion, right pulmonary artery and distal segment are stenosis. D: Axial MR T1 image shows mild thickening of the right pulmonary artery (long arrow) and iso-intensity thrombosis (short arrow). MIP-maximum-intensity projection, MRA-magnetic resonance angiography.
Figure 13.
Vasculitis-ralated pulmonary artery thrombosis. Takayasu arteritis in a 33-year-old woman with dizziness and chest compress. A: Contrast-enhanced axial CT demonstrates filling defect and occlusion of the right pulmonary artery wall (arrow) and the main pulmonary is dilated. B: Axial CT image shows the wall of right subclavian artery and right common carotid artery are thickening and the lumen is narrow (arrow). C: Coronal MIP contrast-enhanced MRA image shows the right brachicephalic artery, right subclavian artery and right common carotid artery are stenosis or occlusion, right pulmonary artery and distal segment are stenosis. D: Axial MR T1 image shows mild thickening of the right pulmonary artery (long arrow) and iso-intensity thrombosis (short arrow). MIP-maximum-intensity projection, MRA-magnetic resonance angiography.
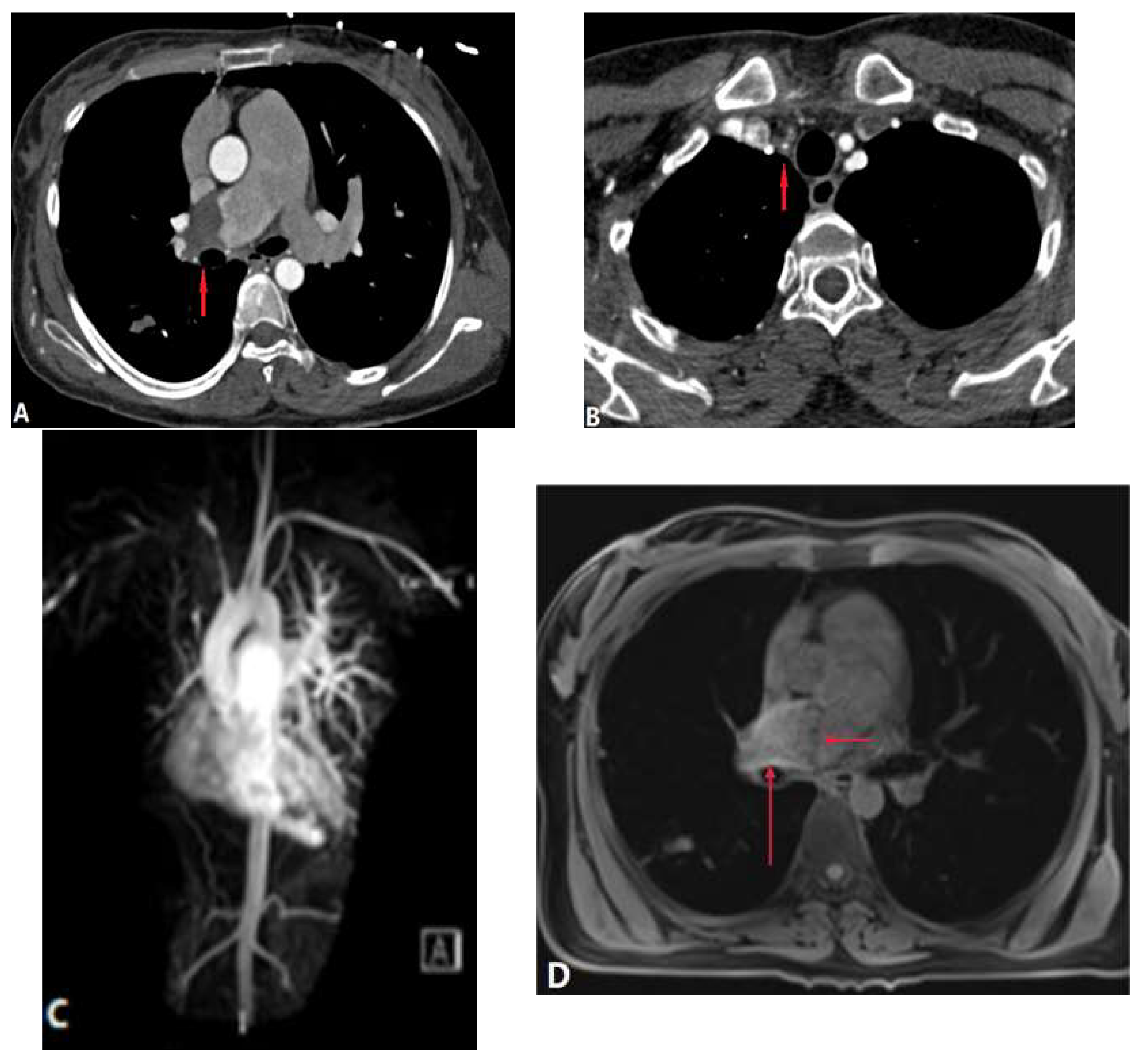
Figure 14.
Vasculitis-related pulmonary artery thrombosis. Behcet syndrome (10 years) in a 40-year-old man with hemoptysis. A,B: Axial and coronary CT MPR images show aneurysmal dilatation of bilateral lower lobe pulmonary artery with wall thickening and enhancement (long arrows), in situ thrombosis and stenosis or occlusion. In situ thrombosis also can be found in right ventricle (short arrow in A). MPR-multiplanar reformation.
Figure 14.
Vasculitis-related pulmonary artery thrombosis. Behcet syndrome (10 years) in a 40-year-old man with hemoptysis. A,B: Axial and coronary CT MPR images show aneurysmal dilatation of bilateral lower lobe pulmonary artery with wall thickening and enhancement (long arrows), in situ thrombosis and stenosis or occlusion. In situ thrombosis also can be found in right ventricle (short arrow in A). MPR-multiplanar reformation.
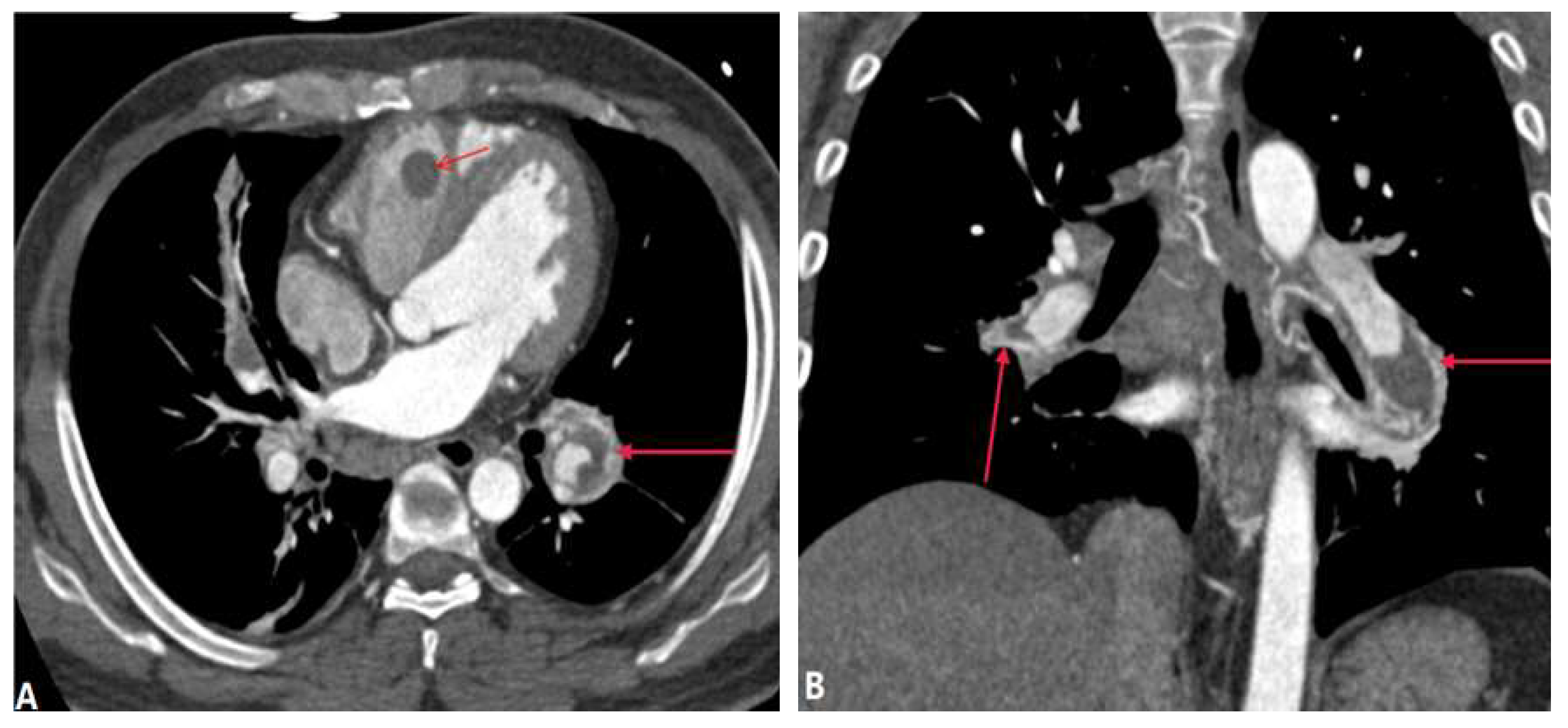
Figure 15.
SMJS. 71Y woman with Swyer-James-Macleod syndrome. A: lung window axial CT shows the bronchiectasis and infections in right and left lower lobes (arrow), and the hyperlucent right lung. B: coronal MIP of CTPA shows the hypoplasia of the pulmonary vasculature of left lung. CTPA-computed tomography pulmonary angiography, MIP-maximum-intensity projection.
Figure 15.
SMJS. 71Y woman with Swyer-James-Macleod syndrome. A: lung window axial CT shows the bronchiectasis and infections in right and left lower lobes (arrow), and the hyperlucent right lung. B: coronal MIP of CTPA shows the hypoplasia of the pulmonary vasculature of left lung. CTPA-computed tomography pulmonary angiography, MIP-maximum-intensity projection.
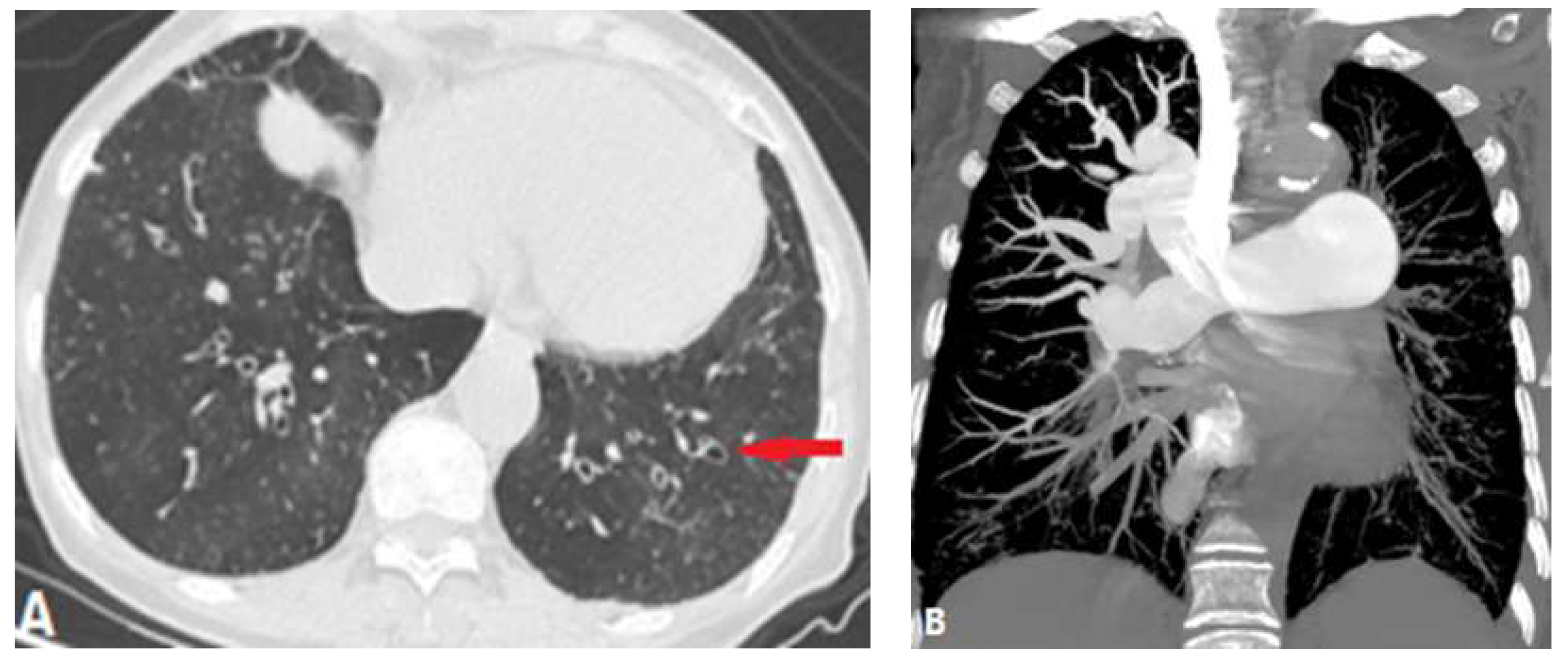
Figure 16.
Aortic dissection. A and B: Sagittal and coronal CTA shows the hematoma of aortic dissection extending to the pulmonary artery via PDA (white arrow), which causes the stenosis of PA (red arrow). C: another patient of aortic dissection presents with the stenosis of right pulmonary artery (red arrow), because the discontinuity of the media. CTA-computed tomography angiography PDA- patent ductus arteriosus.
Figure 16.
Aortic dissection. A and B: Sagittal and coronal CTA shows the hematoma of aortic dissection extending to the pulmonary artery via PDA (white arrow), which causes the stenosis of PA (red arrow). C: another patient of aortic dissection presents with the stenosis of right pulmonary artery (red arrow), because the discontinuity of the media. CTA-computed tomography angiography PDA- patent ductus arteriosus.
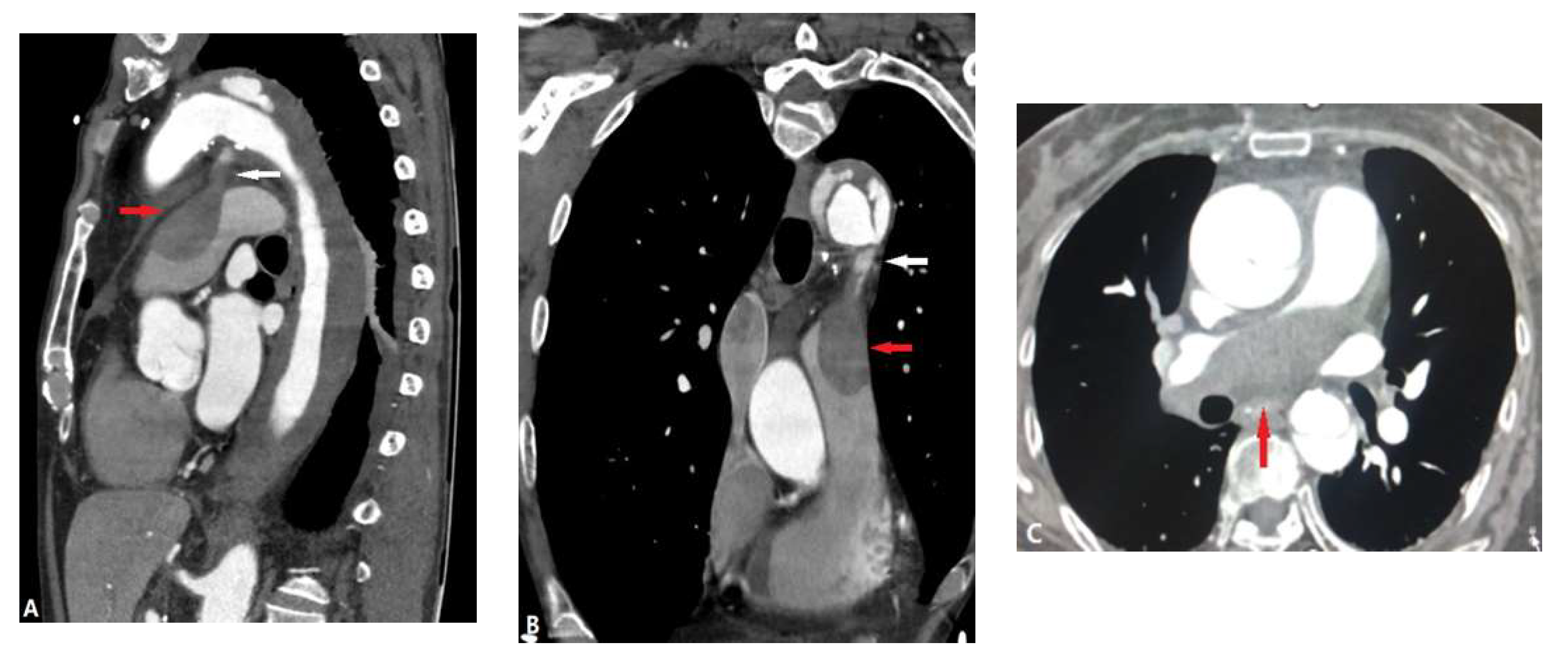
Figure 17.
TB-FM. A: Coronal MIP shows the dense and calcified tissues wrapped the pulmonary vasculatures cause stenosis and the atelectasis of right middle lobe (arrow). B and C: the coronal MIP and MinIP shows the same segment of bronchus and pulmonary vessels (arrows) were affected by the tissues. MIP-maximum-intensity projection, MinIP-minimum-intensity projection.
Figure 17.
TB-FM. A: Coronal MIP shows the dense and calcified tissues wrapped the pulmonary vasculatures cause stenosis and the atelectasis of right middle lobe (arrow). B and C: the coronal MIP and MinIP shows the same segment of bronchus and pulmonary vessels (arrows) were affected by the tissues. MIP-maximum-intensity projection, MinIP-minimum-intensity projection.
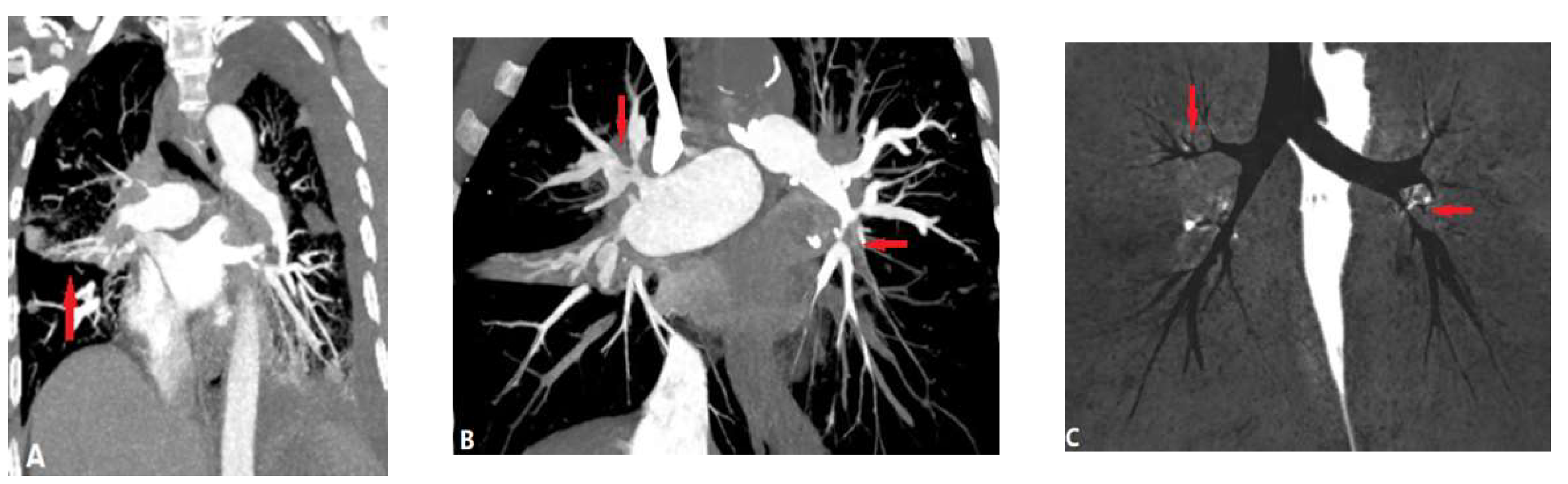
Figure 18.
IgG4-related FM. 3D volume rendering image (A) of pulmonary arteries and MIP (B) show the stenosed proximal segment of right and left pulmonary arteries which were caused by the infiltrative soft tissue, without calcification (arrow). MIP-maximum-intensity projection.
Figure 18.
IgG4-related FM. 3D volume rendering image (A) of pulmonary arteries and MIP (B) show the stenosed proximal segment of right and left pulmonary arteries which were caused by the infiltrative soft tissue, without calcification (arrow). MIP-maximum-intensity projection.
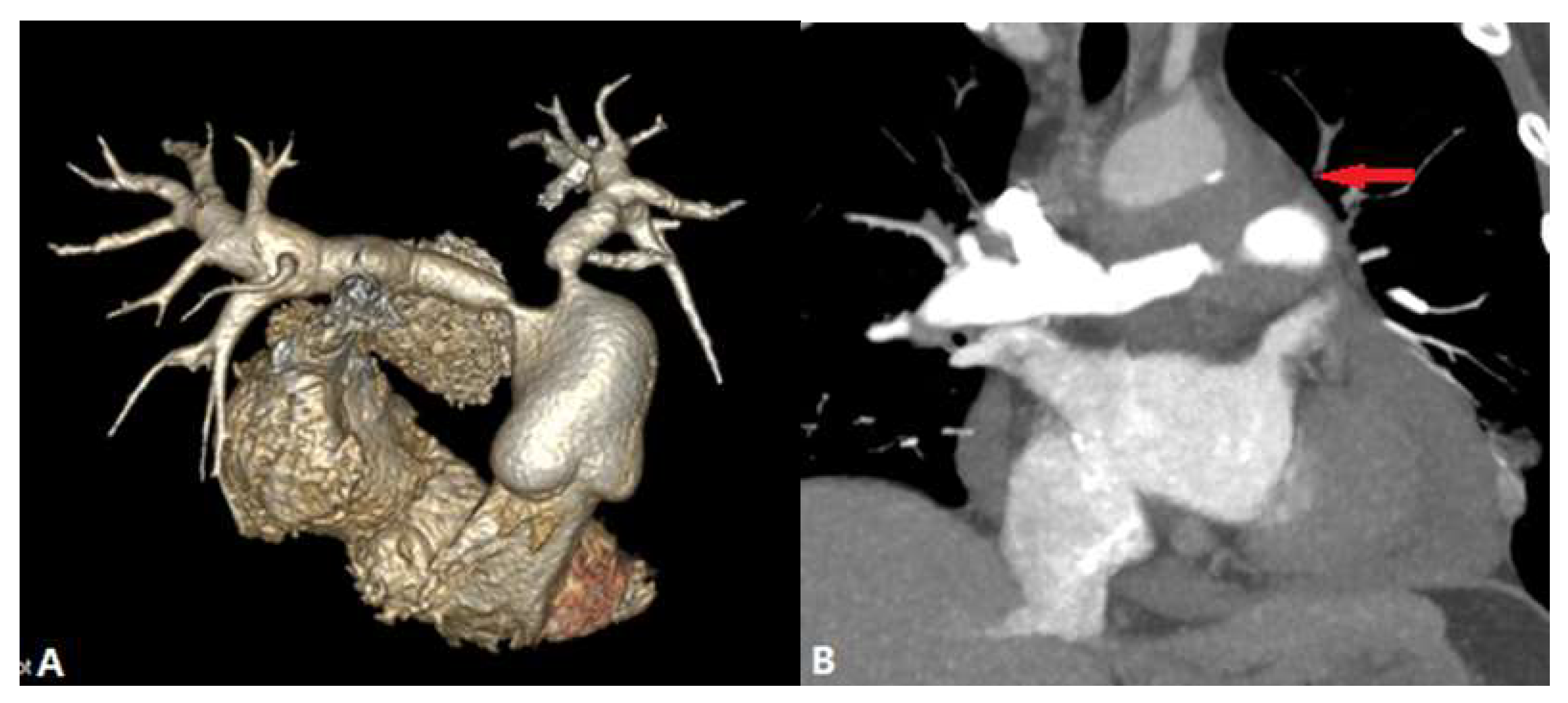
Figure 19.
Tumor in a 50 years old male with lung cancer. A and B: Axial MIP presents that the tumor infiltrates and compresses the pulmonary arteries of left lung, following the lumen narrowing (arrow). C: sagittal view shows the occluded bronchus (arrow). D: the enlarged lymph nodes (arrows) on coronal CT due to metastasis. MIP-maximum-intensity projection.
Figure 19.
Tumor in a 50 years old male with lung cancer. A and B: Axial MIP presents that the tumor infiltrates and compresses the pulmonary arteries of left lung, following the lumen narrowing (arrow). C: sagittal view shows the occluded bronchus (arrow). D: the enlarged lymph nodes (arrows) on coronal CT due to metastasis. MIP-maximum-intensity projection.
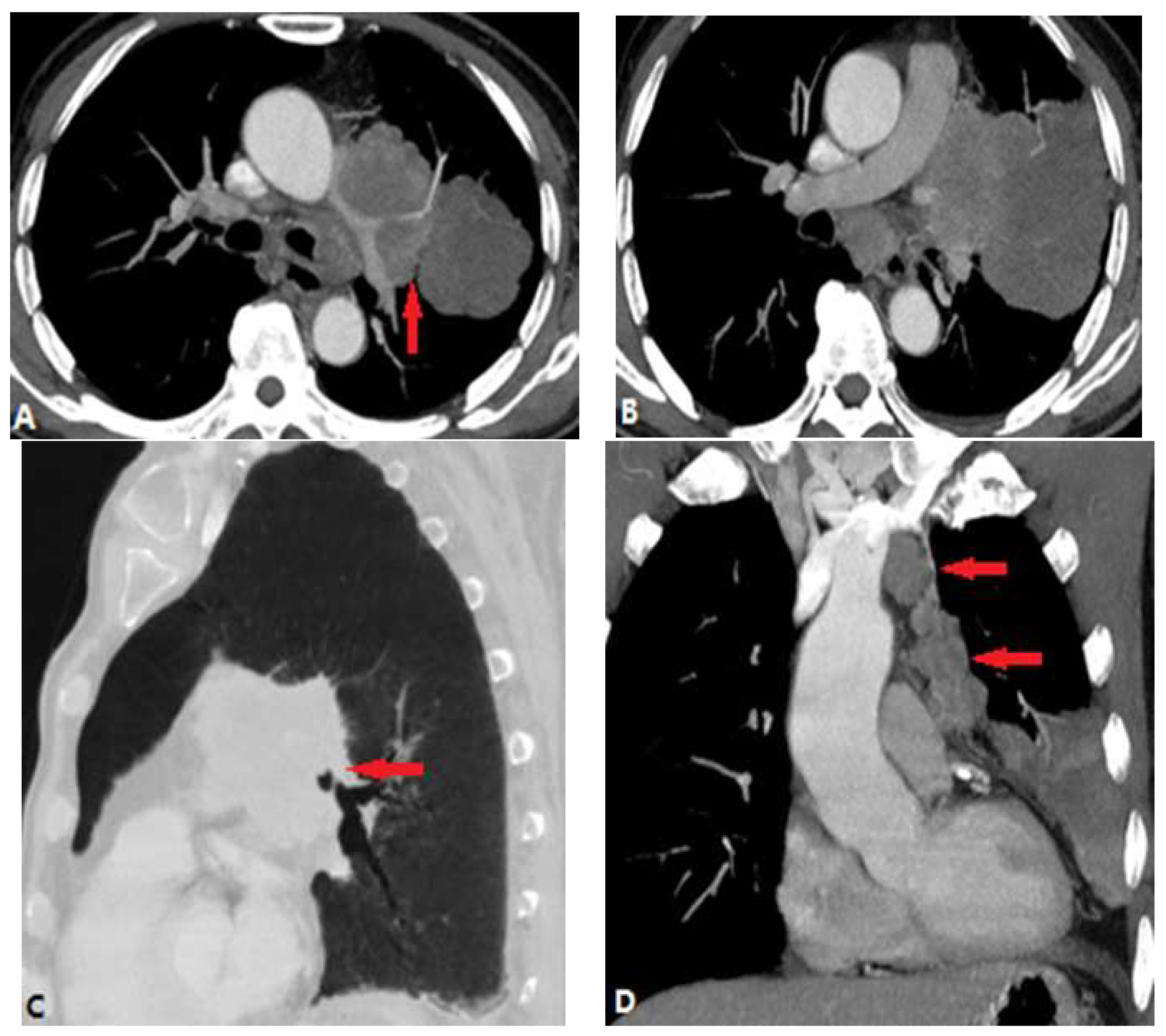
Figure 20.
Aortic aneurysm. A and B: Coronal and sagittal MIP show the direct compression of left pulmonary arteries by the giant aortic aneurysm (arrow). MIP-maximum-intensity projection.
Figure 20.
Aortic aneurysm. A and B: Coronal and sagittal MIP show the direct compression of left pulmonary arteries by the giant aortic aneurysm (arrow). MIP-maximum-intensity projection.
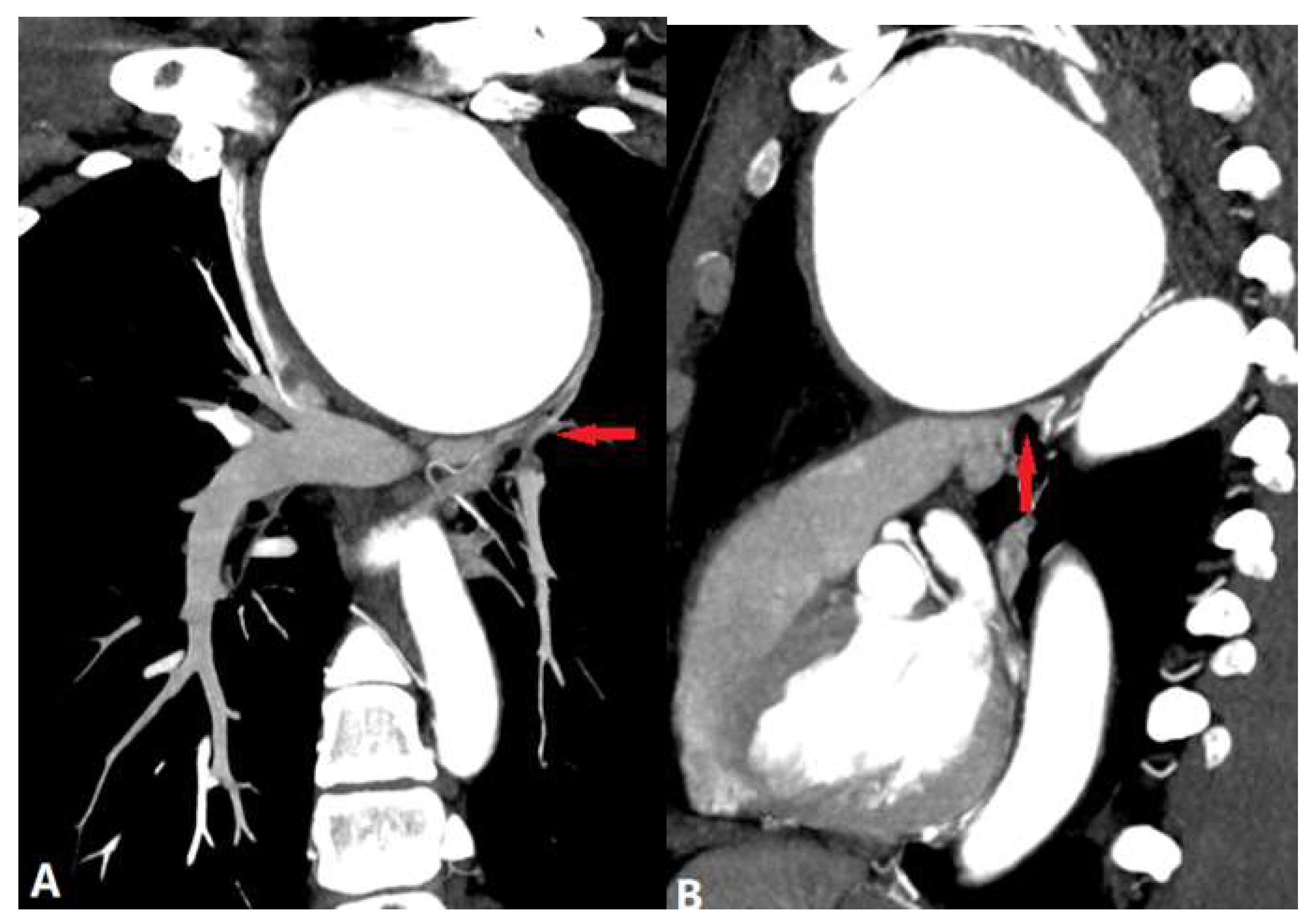
Figure 21.
Radiofrequency ablation of atrial fibrillation. A: Axial CTA shows beaklike narrowing of the left superior pulmonary vein (arrow). B: Axial CTA shows the occluded inferior pulmonary vein (arrow). C: Coronal MIP shows the slender of left pulmonary arteries due to the decreased blood flow (arrows). MIP-maximum-intensity projection.
Figure 21.
Radiofrequency ablation of atrial fibrillation. A: Axial CTA shows beaklike narrowing of the left superior pulmonary vein (arrow). B: Axial CTA shows the occluded inferior pulmonary vein (arrow). C: Coronal MIP shows the slender of left pulmonary arteries due to the decreased blood flow (arrows). MIP-maximum-intensity projection.
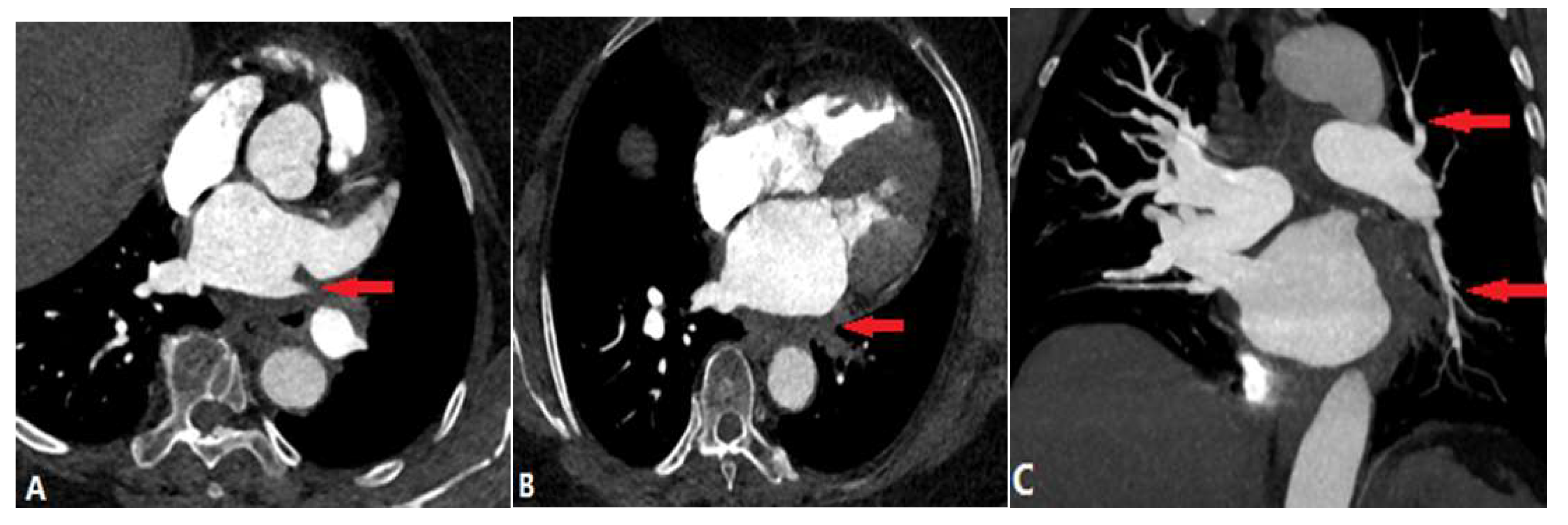

Table 1.
Causes of pulmonary artery stenosis.
| CONGENITAL DISEASE | |||
| Pulmonary valvular stenosis | |||
| Pulmonary artery atresia | |||
| Pulmonary vein atresia | |||
| ACQUIRED DISEASE | |||
| INTRALUMINAL ANOMALIES | |||
| Pulmonary thromboembolism | |||
| In situ pulmonary artery thrombosis | |||
| Pulmonary tumor embolism | |||
| Pulmonary tumor thrombotic microangiography | |||
| Septic pulmonary embolism | |||
| Foreign bodies pulmonary embolism | |||
| Pulmonary artery sarcoma | |||
| VESSEL WALL LESIONS | |||
| Takayasu arteritis | |||
| Behçet disease | |||
| Swyer James Macleod Syndrome | |||
| Arterial dissection | |||
| EXTRALUMINAL ANOMALIES | |||
| Fibrosis mediastinitis | |||
| Tumor | |||
| Aortic aneurysm | |||
| Complications of radiofrequency ablation of atrial fibrillation | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



