
Submitted:
02 July 2024
Posted:
03 July 2024
You are already at the latest version
Abstract
Intermittent religious fasting increases a risk of hypo- and hyperglycemia in individuals with diabetes, but its impact in those without diabetes is poorly investigated. The study aim was to examine the effects of religious Bahá'í fasting (BF) on glycemic control and variability and compare these effects with time-restricted eating (TRE). In a three-arm randomized controlled trial, 16 subjects without diabetes were assigned to a BF, 16:8 TRE or control group. Continuous glucose monitoring and food intake documentation was conducted before and during the 19 days of intervention, and 24-hour mean glucose, glycemic variability indices, and glucotypes were assessed. BF and TRE groups, but not the control group, markedly reduced the daily eating window while maintaining macronutrient composition. Only the BF group decreased caloric intake (-677.8 ± 357.6 kcal, p=0.013), body weight (-1.92 ± 0.95 kg, p=0.011) and BMI (-0.65 ± 0.28 kg, p=0.006). Higher maximum glucose values were observed during BF in the within-group (+1.41 ± 1.04, p=0.039) and between-group comparison (BF vs. Control: p= 0.010 and TRE vs. BF: p= 0.022). However, there were no alterations of 24-hour mean glucose, intra- and inter-day glycemic variability indices, or glucotypes in any group. Proportions of time above and below range (70-180mg/dl) and HbA1c values remained unchanged. BF and TRE do not exhibit negative effects on glycemic control and variability in subjects without diabetes.
Keywords:
continuous glucose monitoring
; glucose metabolism
; glycemic variability
; religious fasting
; intermittent fasting
; time-restricted eating
1. Introduction
Intermittent fasting (IF), characterized by alternating periods of voluntary fasting and eating, has gained popularity in recent years [1]. Preclinical and clinical studies on IF have demonstrated various health benefits, including effectiveness for weight loss [1], although findings are heterogenous and dependent on the IF form and animal model or study cohort. Notably, IF can also induce negative health effects. In particular, religious Ramadan fasting (RF) showed the amelioration of glycemic control [2,3].
Bahá'í fasting (BF) is a form of religious intermittent dry fasting, similar to RF, characterized by restrictions on food and fluid intake from sunrise to sunset [4]. Followers of the Bahá’í religion observe fasting as a significant spiritual duty, fasting for 19 consecutive days every year in March [5], whereas RF lasts for 29 or 30 days. In contrast to RF, where the fasting duration varies based on the lunar calendar and region [6], BF is performed when days and nights are approximately equal (equinox) [5]. This makes BF a more stable model for exploring the effects of intermittent dry fasting compared to RF.
Religious intermittent dry fasting involves significant changes in the diurnal eating and sleeping pattern, water balance, and hormonal patterns [7]. In subjects with diabetes, particularly in those receiving insulin therapy, these alterations may increase the risk of deterioration of glycemic control. Because only a few studies have investigated the BF impact on metabolism [5,8], effects of religious intermittent dry fasting on the glycemic control described below are based on RF studies. Published studies have reported that individuals with type 1 and type 2 diabetes have an increased risk of hypo- and hyperglycemic events during the religious intermittent dry fasting in the form of RF [2,3,9,10]. Severe hypoglycemia was more frequent in subjects who were treated with insulin and/or sulfonylureas, changed their dose of oral antidiabetic drugs or insulin, or modified their level of physical activity [2,3,10]. Despite these risks, some studies have reported improvements in HbA1c, fasting and postprandial glucose, body weight, and body fat after RF [11,12].
The development and increasing availability of continuous glucose monitoring (CGM) for 24-hour glucose patterns offer new opportunities for such investigations. In particular, CGM allows assessment of the glycemic variability (GV), which includes the amplitude, frequency, and duration of glycemic fluctuations around mean blood glucose. GV is recognized as an emerging target for blood glucose control [13] and an independent risk factor for micro- and macrovascular complications in subjects with and without diabetes [14]. Recent studies using CGM (or flash glucose monitoring, FGM) during RF have confirmed increased time in hyperglycemia and glucose variability, especially in subjects with type 1 diabetes receiving insulin therapy [15,16,17]. In contrast, subjects with type 2 diabetes with or without insulin treatment showed only a transient increase in glucose variability and no changes in glycemic control measures during RF [18,19]. Nevertheless, there is still a lack of sufficiently controlled CGM-based data on the impact of RF on glycemic control.
Time-restricted eating (TRE) is another form of IF that has gained popularity in recent years. It involves prolonged daily fasting and a reduction of the daily eating window to usually under 10 h/day, with variations in the timing and duration of it (e.g., early, midday, or late TRE) [20]. In contrast to RF, most TRE trials reported beneficial effects on metabolic outcomes, even though data are strongly heterogeneous [21]. A number of TRE studies showed improvements in glucose metabolism such as reductions in fasting, postprandial, and nocturnal glucose levels, lowered mean 24-hour glucose levels, and reduced glycemic excursions, improvements of HbA1c, reduced fasting insulin levels, insulin resistance, and improved insulin sensitivity [21]. However, whether TRE is a comparable to the intermittent religious dry fasting regimes regarding their effects on glucose patterns remains unclear.
Religious intermittent dry fasting is obligatory for healthy adult Muslims (in the form of RF) or followers of the Bahá’í religion (in form of BF) and the desire to participate is intense, even in risk groups, e.g. those with diabetes [10]. Managing diabetes during religious fasting is challenging, as taking countermeasures in case of hypoglycemia would lead to breaking the fast. Therefore, the question of whether or to what extent glucose metabolism could be out of control, especially with regard to glucose variability, in individuals without diabetes [22] has high clinical relevance and needs to be carefully investigated. Therefore, the main aim of this preliminary study was to examine how religious BF affects glycemic control and variability in adult individuals without diabetes and whether the effects are comparable to TRE.
2. Materials and Methods
2.1. Study Design
This three-arm randomized, controlled trial investigated the effects of two different fasting regimes, the religious dry BF and TRE compared to a control group. After a 5-7 day baseline phase, the intervention groups followed a corresponding fasting regimen for 19 days, whereas the control group did not receive any nutritional recommendations and was advised not to change its habitual food and eating timing (Figure 1). Before and at the end of the intervention phase, anthropometric parameters and blood pressure were assessed and a blood sample was collected for HbA1c measurement (visit 1 and visit 3). CGM and food intake documentation (dietary records) were conducted simultaneously during the baseline phase and during the entire intervention (Figure 1).
The trial was designed as a dental study with bleeding on probing index as the primary periodontal outcome parameter (Supplemental Figure S1). Here, we focus on the secondary outcomes related to glycemic control in a subcohort of 16 participants who underwent CGM assessment over the whole study duration. The study was approved by the ethics committee of the Charité-Universitätsmedizin Berlin on 06.05.2021 and registered at the German Clinical Trials register (DRKS, assessed on drks.de) under the identifier number DRKS00026701 on 15.10.2021 and conducted between November 2021 and May 2022. Recruitment of participants was performed in the Department for Periodontology, Oral Medicine, and Oral Surgery at Charité-Universitätsmedizin Berlin, Germany. Written informed consent was obtained from all study participants prior to the study.
2.2. Study Subjects and Eligibility Criteria
Study participants were males and females without periodontal disease aged between 18 and 69. For the BF group, participants had to be a member of the Bahá’í community who intended to fast. Subjects were randomly assigned to either the TRE or control group, stratified by gender, with random block sizes of 2 or 4 (blockrand backage in Rstudio version, 2022.12.01), whereas BF group participants were not randomized. Exclusion criteria were diabetes, pregnancy and breastfeeding, severe internal diseases, eating disorders and severe psychiatric illness, smoking (defined as >5 cigarettes daily), caries, periodontitis, ongoing orthodontic therapy, other pathological oral conditions, medication with antibiotics (in the last three months prior to study start) or anti-inflammatory drugs (while fasting period). Moreover, participants were excluded when participating in another intervention study or planned to interrupt (religious) fasting.
2.3. Fasting Interventions, Dietary Records and Assessment of the Timely Compliance
During the intervention phase, participants of the BF group consumed food and drinks only before sunrise and after sunset, without any fluid intake during the day (dry fasting). In the TRE group, participants were advised to consume habitual food and caloric drinks in a restricted eating window of 8 hours a day, followed by the 16-hour fasting window when only non-caloric drinks (e.g., water, herbal tea) were allowed. Participants were free to select their own mealtimes as long as they adhered to the 8-hour eating and 16-hour fasting window.
Participants were asked to document all consumed foods and drinks and the eating times during the baseline and intervention phases starting from visit 0 (Figure 1). They were instructed to weigh their food whenever possible, write down brand names, and use standard household measures (e.g., cups, glasses, tablespoon, teaspoon, etc.) when they go out for dinner. Dietary records during the baseline and intervention phases were analyzed for daily energy and macronutrient intake as well as for eating timing using the FDDB database (Fddb Internetportale GmbH, https://fddb.info/) as described [23].
For the assessment of dietary compliance, in the TRE group, the beginning of the first and the end of the last caloric intake were determined based on the dietary records, and the average daily eating and fasting window duration were calculated for each participant for the baseline and intervention phases. In the BF group, subjects usually ate two times per day - before sunrise (=after waking up) and after sunset (=before bedtime). To calculate the daily eating and fasting windows, time between the first and last caloric intake in the morning and the first and last caloric intake in the evening were summed. In the BF group, the adherence to sunrise and sunset times was additionally assessed using the sunrise-sunset calendar specific for every fasting day. Adherence to 8-hour eating windows during the TRE intervention and to specific sunrise and sunset times in BF intervention were considered as compliant with a 30-min tolerance window. Compliant days were calculated as a percentage of the number of all intervention days.
2.4. Anthropometric Measurements
Anthropometric measurements, e.g., body weight and body composition were performed using a scale and the body analyzer BF 508 (Omron, Mannheim, Germany). Waist and hip circumferences were assessed with a measurement tape.
2.5. Continuous Glucose Monitoring (CGM) and HbA1c Assessment
A 24-hour continuous glucose monitoring was performed with the CGM system by FreeStyle Libre Pro IQ (Abbott, Wiesbaden, Germany). The glucose sensor was placed on the upper arm and measured interstitial blood glucose in 15-min sampling intervals. The sensor was blinded, and therefore, participants were not able to check their blood glucose values. The first CGM recording period started 5-7 days before the intervention start (visit 0) and continued for 14 consecutive days. On the 7-10th day of the intervention (visit 2), the new sensor was fixed, and the second CGM recording period continued till the final visit at the end of the intervention (visit 3) (Figure 1).
Sensor data were read out by a study assistant and analyzed by the Excel tool EasyGV [24] quantifying an average 24-hour mean sensor glucose level (MSG) and relevant indices describing glycemic variability during the baseline and intervention phase as described [25]. To analyze the intra-day glycemic variability, the standard deviation (SD) was calculated for each mean glucose value as described [24]. The mean amplitude of glucose excursions (MAGE) was determined by SD values higher than 1 [24]. The inter-day glycemic variability was described using the continuous overlapping net glycemic action (CONGA) as an index for the glucose difference at various set intervals, which length was set at 60 min prior to analysis. The mean of absolute glucose change (MAG) was calculated as a sum of consecutive glucose level differences divided by the total time (hours) [26]. The mean of daily differences (MODD), which is an index describing the inter-day glycemic variability, was calculated with the averaged glucose values occurring at the same time on different days. Moreover, a classification of glucose values and their conversion to the risk scores, e.g., a low blood glucose index (LBGI <0) and a high blood glucose index (HBGI >0) has been made. The coefficient of variation in percentage (CV%) was calculated using the formula SD/MSG x 100 as described previously [27]. Time below range (TBR, percentage of glucose values <3.9 mmol/l), and time above range (TAR, percentage of glucose values >10 mmol/l) as well as the minimum and maximum glucose levels were assessed. To achieve an overview of the diurnal glucose profiles, glucose average was calculated at each time point for all days of the study period (intervention or baseline), and the area under the glucose curve (AUCGlu) was assessed with the trapezoidal rule.
HbA1c was assessed in Labor Berlin (Berlin, Germany) according to standardized procedures.
2.6. Glucotypes
“Glucotype” is a novel method of glucose variability assessment developed by Hall et al. [28] to examine glucose dynamics based on average and single-point measurements of total glycemia. Based on the CGM-based glucotype method, persons identified as normoglycemic using standard diagnostic methods, may be detected as prediabetic or diabetic [28]. An algorithm describes the individual percentage of time spent in a ‘low’, ‘moderate’, or ‘severe’ glucotype pattern [28]. Further, individual glucotypes were classified based on their most frequent variability pattern (‘low’, ‘moderate’ or ‘severe’) in the baseline and intervention phases for each group. For this analysis, CGM data were evaluated using the R package iglu with the statistics software R Studio [29].
2.7. Statistical Analysis
Study data were collected and managed using REDCap (Research Electronic Data Capture, Version 12.1.1) hosted at Charité-Universitätsmedizin Berlin. SPSS 25 (IBM, Chicago, IL, United States) was used for statistical analysis. Data were expressed as mean ± SD when normally distributed and median (IQR) when not normally distributed. For the analysis of the data distribution the Shapiro-Wilk test was used. Not normally distributed data were logarithmically transformed before analysis and proved again for the distribution. Normally distributed data served for parametric unpaired or paired Student’s t-test, whereas non-parametric Mann-Whitney or Wilcoxon tests were used for the analysis of not normally distributed values. For multiple group comparisons of intervention-induced changes, one-way ANOVA with Sidak post-hoc test for normally distributed data and Kruskal-Wallis test with Dunn post-hoc analysis for not normally distributed data were used. CGM glucose profiles were compared with repeated-measurement ANOVA (RM-ANOVA). The significance level was set at p < 0.05. The visualization of the data was performed using GraphPad Prism software version 5.0 (GraphPad Prism Inc, La Jolla, CA, USA).
3. Results
3.1. Baseline Characteristics of Study Population
A total of 16 participants consisting of 8 men and 8 women with an average age of 29 (26 – 34) years, BMI 26.4 ± 4.3 kg/m2 and HbA1c 5.10 ± 0.29% completed the study. No participants with known diabetes were enrolled in the trial. 6 participants (3 males, 3 females) were allocated to the BF group, 6 were allocated to the TRE group (3 males, 3 females), and 4 participants (2 males, 2 females) were allocated to the control group (Table 1). No differences between the BF, TRE and control group in anthropometric measurements and glycemic parameters including MSG and glycemic variability indices at the baseline were observed (Table 1).
3.2. Timely Compliance
High timely compliance to the prescribed eating timing and duration was achieved as assessed by adherence to the eating before sunrise and after sunset for the BF intervention and by adherence to the 8 h self-selected daily eating window for the TRE intervention. During the BF intervention, subjects markedly changed their eating regime from the eating in the daytime from 9:49 ± 0:32 h till 21:50 ± 2:00 h to the eating two times per day from 5:27 ± 01:00 h till 6:07 ± 00:47 h and from 18:32 ± 00:45 h till 21:48 ± 00:48 h in accordance with the specific sunrise-sunset times (Figure 2A). The total eating window duration was restricted from 11:59 ± 2:09 h to 4:09 ± 1:41 h in the BF group (p=0.008) (Figure 3A). During the TRE intervention, subjects proceeded to eat in the daytime only reducing the eating window duration compared to the baseline (Figure 2B). The total eating window duration was restricted from 11:17 ± 1:21 h to 7:03 ± 0:35 h in the TRE group (p=2.94x10-4) (Figure 3A). Further, the percentage of the individual eating time reduction was calculated relative to the baseline. The TRE group shortened the eating window to 62.8 ± 2.9% and the BF group to 36.9 ± 19.0% compared to baseline (100%) (Figure 3B). BF and TRE groups were compliant 100.0 (83.3 – 100.0) % and 100.0 (91.7 – 100.0) % of all intervention days, respectively. The control group did not change their habitual eating and fasting timing and duration during the intervention compared to the baseline.
3.3. Energy and Macronutrient Intake
The BF group showed a reduction in energy intake for 677.8 kcal ± 357.6 kcal compared to the baseline (p=0.013), whereas no changes in energy intake occurred in the TRE and control groups (Figure 3C). Macronutrient and fiber intake calculated as a percentage of the total energy intake were not altered in any group (Figure 3D–F).
3.4. Anthropometric Measurements and Blood Pressure
BF induced a decrease in body weight (-1.92 kg ± 0.95 kg, p=0.011) and BMI (-0.65 ± 0.28 kg, p=0.006) (Figure 4A,B), but no effect on waist circumference (Figure 4C). Anthropometric parameters in the TRE and control groups remained unchanged (Figure 4A–C), but no differences were found in the between-group comparison. Systolic and diastolic blood pressure did not change in any group (data not shown).
3.5. 24-Hour Glucose Profiles and Glycemic Parameters
The BF group showed alterations of the 24-hour glucose profiles during the intervention compared to the baseline phase (Pintervention*time=0.001), in contrast to the TRE and control groups, which demonstrated no changes (Pintervention*time=0.310 and Pintervention*time=0.388, respectively) (Figure 2A–C). In agreement with this, in the BF group, two highest glucose peaks appeared after sunrise and after sunset, whereas the lowest glucose values appeared immediately before sunset (Figure 2A). Correspondingly, maximum glucose values were markedly increased in the BF group (Supplemental Table 1), whereas they were slightly decreased in the control group during the intervention compared to the baseline phase (1.41 ± 1.04 mmol/L, p=0.039 and - 0.55 ± 0.19 mmol/L, p=0.011, respectively). The BF-induced change differed from both other groups in the between-group comparison (BF vs. TRE: p = 0.022; BF vs. control: p = 0.010) (Table 2).
The assessment of 24-hour CGM data shows no changes of the mean sensor glucose (MSG) and area under the glucose curve (AUCgluc) in any group (Table 2, Supplemental Table S1). CGM-derived indices of intra-day (SD, CV, MAGE, CONGA) and inter-day (MODD) glycemic variability, as well as LBGI and HBGI remained unchanged in any group compared to the baseline phase and in the between-group comparison. MAG index decreased in the control group during the intervention (-0.11 ± 0.06 mmol/L/h, p=0.036), but not in other groups. Further, no changes in the percentage of TAR and TIR (3.9-10.0 mmol/L) were observed in CGM data in any group (Table 2, Supplemental Table S1). In agreement with these observations, the HbA1c values remained unchanged after the intervention in all groups and in the between-group comparison (Table 2, Supplemental Table S1).
3.6. Glucotypes
Additionally, we analyzed subject’s glucotypes using a new metric for glucose variability (28). Individual glucotypes were classified as “moderate” during the baseline phase in all groups. During the intervention, 3 participants in the TRE group, 1 participant in the BF group, and 1 participant in the control group changed to a “low” glucotype (data not shown). However, the percentage of time spent in low, moderate, and severe variability patterns were not altered during any intervention compared to the baseline (Figure 5).
4. Discussion
This CGM-based study is the first to investigate the impact of religious intermittent dry fasting in the form of BF in comparison to another form of intermittent fasting, TRE, on glycemic control and variability in subjects without diabetes. Surprisingly, despite the reduction of body weight and BMI in the BF group, no alterations of 24-hour mean glucose, intra- and inter-day glycemic variability indices, as well as glucotypes and HbA1c, were found. Similarly, no changes in glycemic control and variability were observed in the TRE group, where body weight and BMI remained stable after the intervention.
To our knowledge, no long-term CGM-based studies have examined the effect of religious intermittent dry fasting, even in the form of RF, on glycemic control and variability in subjects without diabetes, whereas the metabolic effects of BF are generally very scarce investigated yet [5,8]. Till now, only one study conducted short-term CGM for two consequent days before and during RF in 7 subjects without diabetes [17]. To close this gap, we conducted a very detailed long-term analysis of glycemic variability using a range of widely used indices of inter- and intra-day variability as well as the novel methods of glucotype assessment in subjects without diabetes. Our results showed no alterations of 24-hour mean glucose, AUCgluc, intra- and inter-day glycemic variability indices (except for higher maximum glucose values), TAR and TIR, as well as glucotypes and HbA1c during BF despite the body weight and BMI reduction. These results align with Lesson et al., who also did not find changes in glycemic control in subjects without diabetes using short-term CGM [17]. Taken together, our findings suggest that BF in subjects without diabetes has no clinically relevant negative impact on glycemic control and glycemic variability. This indicates that healthy individuals without diabetes might be metabolically flexible enough to provide good glycemic control even upon BF and corresponding changes in daily routines, eating and sleeping patterns.
Studies on RF conducted in individuals with well controlled type 2 diabetes with or without insulin treatment showed similar results. They demonstrated only transient increase in glucose variability and no changes in glycemic control measures during RF [18,19] although subjects with insulin-treated diabetes showed greater glucose excursions than the other medication groups [17]. Based on these data, Elmalti et al. hypothesized that the initial and temporary increase in glucose variation is related to sudden changes in daily routines, eating and sleeping times, rather than changes in glycemic control or the effectiveness of diabetes treatment [18]. In contrast, studies included only subjects with type 1 diabetes receiving insulin therapy or individuals with both type 1 and type 2 diabetes showed increased time in hyperglycemia and glucose variability during RF [15,16,17]. Taken together, these data confirm the idea that the risk of severe hypoglycemia upon religious intermittent dry fasting is increased in subjects treated with insulin or has poorly controlled diabetes [2,3,10] but is less or not relevant for subjects without diabetes or with well-controlled type 2 diabetes.
Interestingly, no changes in glycemic control and variability were also observed in the TRE group where calorie intake was unaltered during the intervention and body weight remained stable after the intervention. The data on the TRE impact on glycemic control are controversial. A number of TRE studies showed improvements in glucose metabolism such as lowered fasting glucose levels [30,31,32,33,34], postprandial glucose levels in response to a standard meal or oral glucose tolerance test [35,36] and night-time glucose [37]. HbA1c, as an important indicator of long-term glycemic control, decreased in two trials after TRE intervention in overweight and obese participants [38,39], while no changes were detected in three other studies [40,41,42]. Few TRE trials applied CGM showed a decreased mean 24-h glucose, glycemic excursions [32], and mean fasting glucose [35]. The controversial TRE data might be explained by the heterogeneity of the study design (TRE duration, timing of the eating window), subject cohorts (healthy subjects, subjects with prediabetes or diabetes) [21] as well as different body weight reduction during the intervention. Most TRE trials showed the improvement of glycemic traits were accompanied by weight loss or did not carefully monitor body weight, which makes it difficult to disentangle the effects of the eating window shortening and weight loss. Our findings indicate that weight loss may be essential for the favorable effects of TRE on glycemic control. The lack of positive changes in glycemic control in the TRE group could be attributed to stable calorie intake and body weight during the intervention. However, further investigation in larger cohorts and different subjects’ categories in carefully controlled trials is needed to distinguish effects of eating timing and weight loss on glycemic control.
Similarly, to TRE, the beneficial effect of the BF on the glycemic control might be expected. The study of Koppold-Liebscher et al. [8] showed improvements of fasting glucose and HbA1c at the last week of BF accompanied by weight loss (-2.55 kg), and reduction of the BMI and body fat. In agreement with this, several RF studies demonstrated an improvement of HbA1c, fasting or postprandial glucose [11,12,43] in subjects with type 2 diabetes and/or obesity, which at least in part might be explained by a reduction of body weight and body fat. The transient improvement of body weight, BMI, and body fat following the RF month has been demonstrated in various original studies and meta-analyses [44,45] with obese subjects exhibiting more weight loss [44], although these findings are also controversial [46]. Nevertheless, in our study, which was accompanied by a minor decrease inbody weight (-1.92 kg), no improvements of CGM-based parameters of glycemic control were found. One possible explanation might be that study participants without diabetes had good glycemic control before the study started as shown by the low HbA1c levels in the baseline phase. This leads to the assumption, that religious intermittent fasting might have a greater potential for positive changes in subjects with glucose metabolism dysregulation, i.e. prediabetes and diabetes, than in individuals with normal glucose tolerance. Another explanation might be the shift of the second meal during the BF to the late evening which has a negative effect on metabolic state [47] and might counteract to the potential positive effect of weight loss.
The careful documentation of food intake in the present study, which was conducted simultaneously with CGM, allowed an assessment of timely compliance as well as energy and macronutrient intake during the intervention. The quantification of dietary records confirmed very high adherence to the prescribed eating timing and eating window duration in both BF and TRE groups, whereas the control group did not change its habitual eating timing (Figure 2). Notably, the eating window on BF was almost as twice as short (4:09 h) compared to the TRE intervention (7:03 h). The very limited time when food consumption was allowed obviously explains the reduction of calorie intake in the BF group, whereas it remained unchanged in the TRE and control groups. This, in turn, explains the weight loss in BF but not in TRE and control groups.
The simultaneous analysis of glucose pattern and dietary intake also allowed for a better interpretation of observed glucose excursions as visualized in Figure 2. Specifically, we observed two high glucose peaks after meals consumed both after sunrise and after sunset during the BF intervention. Correspondingly, maximum glucose values were markedly increased during the BF intervention compared to the baseline and the BF-induced change differed from those in the TRE and control groups in the between-group comparison. This change in the 24-hour glucose pattern during BF was apparently induced by the dramatic shift in eating timing, from daytime food intake to eating two times during the nighttime, before sunrise and after sunset. Furthermore, caloric intake during these two meals was apparently increased compared to the habitual meals during the non-fasting period. This might, at least in part, explain the markedly higher postprandial glucose rise in the BF intervention compared to the daytime meals consumed at baseline. Notably, while meals consumed during RF are usually characterized by the consumption of fatty and sugary foods, the BF group in the present study did not show alterations in macronutrient composition compared to the baseline, which means that BF subjects consumed their habitual food during the intervention. Other factors affecting the 24-hour glucose pattern during the BF intervention might include changes in daily routine, sleeping pattern as well as water balance and hormonal patterns described in detail for RF in a recently published review [7]. In particular, diurnal pattern changes of melatonin, cortisol, insulin, leptin, ghrelin, GLP-1, and FGF21 might affect the glucose pattern and glycemic variability in BF. During the TRE intervention, subject proceeded to consume food only during the daytime, reducing the daily eating window duration compared to the baseline, but the 24-hour glucose pattern was not significantly changed compared to baseline.
In the context of intermittent fasting, the possible role of the circadian clock needs to be discussed. The circadian clock is a molecular machinery generating 24-hour endogenous rhythms of physiology and metabolism, adapting them to the day-night changes [47]. Light, food intake, and exercise are important time cues (zeitgebers) that can entrain (shift) the circadian clock [47]. Therefore, dramatic changes in eating, sleeping, and physical activity patterns during BF would apparently affect clock rhythms, which, in turn, might contribute to rhythm changes in physiological functions. Indeed, Koppold-Liebscher et al. showed that BF markedly advanced the circadian phase of fasting individuals by more than 1 hour, which is reversed to normal levels 3 weeks after fasting patterns [8]. Similarly, TRE was also shown to affect endogenous clocks in animal and human studies, stabilizing the circadian clock and increasing the amplitude of circadian rhythms due to the modulation of eating pattern [48,49]. Despite this initial evidence, the interaction of fasting regimens and the circadian clock remains insufficiently investigated and needs to be studied in the future to provide a basis for the development of chrononutritional approaches [7].
The present study demonstrates several notable strengths compared to prior research. The main strength is the detailed CGM-based analysis of the effects of the religious intermittent dry fasting on glycemic control in subjects without diabetes, which was not investigated previously. The study, for the first time, evaluates a range of inter- and intra-day variability measures and introduces a novel method, glucotypes, for glycemic variability estimation in this category of individuals. Additionally, this study is the first to investigate the impact of BF on glycemic control. Another important strength of the present study is the careful control of timely compliance, energy and macronutrient intake, as well as 24-hour glucose patterns throughout the baseline and intervention phases, providing a comprehensive assessment over approximately 25 days for each subject. We revealed high timely compliance and unchanged macronutrient composition in all groups, as well as exactly quantified the energy intake during the intervention. These data were insufficiently controlled in most previously published trials. Finally, a clear strength of the study is that it uniquely compares two distinct forms of intermittent fasting (BF and TRE) while also including a control group.
Our study also has certain limitations. Firstly, the sample size in each group was limited and only restricted to subjects without diabetes. Another consideration is that the small sample size limited the utility of subgroup analysis (e.g., subjects with and without obesity). Thirdly, monitoring physical activity levels during the study period was not feasible, which prevents a more detailed exploration of the study results.
5. Conclusions
Intermittent fasting regimes, BF and TRE, do not show a negative (or positive) impact on glycemic control and glycemic variability in subjects without diabetes after a 19-day intervention. Results of this preliminary study need to be confirmed in larger carefully controlled cohorts including metabolically healthy subjects as well as individuals with prediabetes and type 2 diabetes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Christina Pappe, Henrik Dommisch and Olga Pivovarova-Ramich; Formal analysis, Beeke Peters and Nico Steckhan; Funding acquisition, Christina Pappe and Olga Pivovarova-Ramich; Investigation, Christina Pappe; Methodology, Beeke Peters, Christina Pappe, Daniela Koppold, Bert Arnrich, Henrik Dommisch, Nico Steckhan and Olga Pivovarova-Ramich; Project administration, Christina Pappe and Olga Pivovarova-Ramich; Resources, Christina Pappe, Bert Arnrich, Andreas Michalsen and Olga Pivovarova-Ramich; Software, Beeke Peters, Bert Arnrich and Nico Steckhan; Supervision, Olga Pivovarova-Ramich; Visualization, Beeke Peters; Writing – original draft, Beeke Peters and Olga Pivovarova-Ramich; Writing – review & editing, Beeke Peters, Christina Pappe, Daniela Koppold, Bert Arnrich, Andreas Michalsen, Henrik Dommisch, Nico Steckhan and Olga Pivovarova-Ramich.
Funding
The study is funded by the German Diabetic Association / Abbott (Adam Heller Prize 2021, OP-R.), by the European Association for the Study of Diabetes (Morgagni Prize 2020, O.P.-R.), by the German Research Foundation (DFG RA 3340/4-1 to O.P.-R., project number 530918029), and by the German Society for Tooth, Mouth and Jaw Diseases (Wissenschaftsförderung, C.L.P.). Funders were not involved in preparation of study design and implementation of the study; data collection, management, data analyzation, and interpretation; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the Charité-Universitätsmedizin Berlin (EA2/091/21, approved on 06.05.2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
We gratefully thank all study participants for their cooperation. We also thank Elisa Parsche and Emily Bader for their excellent technical support in the preparation of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- de Cabo R, Mattson MP. Effects of Intermittent Fasting on Health, Aging, and Disease. The New England journal of medicine. 2019;381(26):2541-51. [CrossRef]
- Rahmatullah, Ahmedani MY, Basit A, Zia S, Hasan I, Masroor Q, et al. Evidence-based risk factors for major complications during Ramadan fasting in people with diabetes grouped under IDF-DAR risk categories. Diabetes research and clinical practice. 2022;185:109234. [CrossRef]
- Ba-Essa EM, Hassanein M, Abdulrhman S, Alkhalifa M, Alsafar Z. Attitude and safety of patients with diabetes observing the Ramadan fast. Diabetes research and clinical practice. 2019;152:177-82. [CrossRef]
- Bahá’u’lláh. The Kitáb-i-Aqdas: The Most Holy Book. 1 ed. ed: London: Baha’i Publishing Trust; 1993. 315 p.
- Mähler A, Jahn C, Klug L, Klatte C, Michalsen A, Koppold-Liebscher D, et al. Metabolic Response to Daytime Dry Fasting in Bahá'í Volunteers-Results of a Preliminary Study. Nutrients. 2021;14(1).
- Hassanein M, Afandi B, Yakoob Ahmedani M, Mohammad Alamoudi R, Alawadi F, Bajaj HS, et al. Diabetes and Ramadan: Practical guidelines 2021. Diabetes Res Clin Pract. 2022;185:109185. [CrossRef]
- Ali T, Lessan N. Chrononutrition in the context of Ramadan: Potential implications. Diabetes/metabolism research and reviews. 2023:e3728. [CrossRef]
- Koppold-Liebscher DA, Klatte C, Demmrich S, Schwarz J, Kandil FI, Steckhan N, et al. Effects of Daytime Dry Fasting on Hydration, Glucose Metabolism and Circadian Phase: A Prospective Exploratory Cohort Study in Baha'i Volunteers. Front Nutr. 2021;8:662310.
- Alawadi F, Rashid F, Bashier A, Abdelgadir E, Al Saeed M, Abuelkheir S, et al. The use of Free Style Libre Continues Glucose Monitoring (FSL-CGM) to monitor the impact of Ramadan fasting on glycemic changes and kidney function in high-risk patients with diabetes and chronic kidney disease stage 3 under optimal diabetes care. Diabetes research and clinical practice. 2019;151:305-12.
- Salti I, Benard E, Detournay B, Bianchi-Biscay M, Le Brigand C, Voinet C, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes care. 2004;27(10):2306-11.
- Zouhal H, Bagheri R, Triki R, Saeidi A, Wong A, Hackney AC, et al. Effects of Ramadan Intermittent Fasting on Gut Hormones and Body Composition in Males with Obesity. Int J Environ Res Public Health. 2020;17(15).
- Lum ZK, Khoo ZR, Toh WYS, Kamaldeen SAK, Shakoor A, Tsou KYK, et al. Efficacy and Safety of Use of the Fasting Algorithm for Singaporeans With Type 2 Diabetes (FAST) During Ramadan: A Prospective, Multicenter, Randomized Controlled Trial. Ann Fam Med. 2020;18(2):139-47.
- Tay J, Thompson CH, Brinkworth GD. Glycemic Variability: Assessing Glycemia Differently and the Implications for Dietary Management of Diabetes. Annu Rev Nutr. 2015;35:389-424. [CrossRef]
- Yu JH, Han K, Park S, Lee DY, Nam GE, Seo JA, et al. Effects of long-term glycemic variability on incident cardiovascular disease and mortality in subjects without diabetes: A nationwide population-based study. Medicine (Baltimore). 2019;98(29):e16317.
- Afandi B, Kaplan W, Al Hassani N, Hadi S, Mohamed A. Correlation between pre-ramadan glycemic control and subsequent glucose fluctuation during fasting in adolescents with Type 1 diabetes. Journal of endocrinological investigation. 2017;40(7):741-4. [CrossRef]
- Saadane I, Ali T, El-Laboudi A, Lessan N. Ramadan fasting in insulin-treated patients is associated with potentially unfavourable changes in glucose metrics: A flash glucose monitoring (FGM) study. Diabetes research and clinical practice. 2021;172:108592. [CrossRef]
- Lessan N, Hannoun Z, Hasan H, Barakat MT. Glucose excursions and glycaemic control during Ramadan fasting in diabetic patients: insights from continuous glucose monitoring (CGM). Diabetes Metab. 2015;41(1):28-36. [CrossRef]
- Elmalti A, Mukhtar M, Kenz S, Skaria S, Elgzyri T. Transient increase in glucose variability during Ramadan fasting in patients with insulin-treated type 2 diabetes: A preliminary study. Diabetes Metab Syndr. 2023;17(4):102745. [CrossRef]
- Aldawi N, Darwiche G, Abusnana S, Elbagir M, Elgzyri T. Initial increase in glucose variability during Ramadan fasting in non-insulin-treated patients with diabetes type 2 using continuous glucose monitoring. Libyan J Med. 2019;14(1):1535747. [CrossRef]
- Peters B, Koppold-Liebscher DA, Schuppelius B, Steckhan N, Pfeiffer AFH, Kramer A, et al. Effects of Early vs. Late Time-Restricted Eating on Cardiometabolic Health, Inflammation, and Sleep in Overweight and Obese Women: A Study Protocol for the ChronoFast Trial. Front Nutr. 2021;8:765543. [CrossRef]
- Schuppelius B, Peters B, Ottawa A, Pivovarova-Ramich O. Time Restricted Eating: A Dietary Strategy to Prevent and Treat Metabolic Disturbances. Frontiers in endocrinology. 2021;12:683140. [CrossRef]
- Tsitsou S, Zacharodimos N, Poulia KA, Karatzi K, Dimitriadis G, Papakonstantinou E. Effects of Time-Restricted Feeding and Ramadan Fasting on Body Weight, Body Composition, Glucose Responses, and Insulin Resistance: A Systematic Review of Randomized Controlled Trials. Nutrients. 2022;14(22). [CrossRef]
- Baum Martinez I, Peters B, Schwarz J, Schuppelius B, Steckhan N, Koppold-Liebscher DA, et al. Validation of a Smartphone Application for the Assessment of Dietary Compliance in an Intermittent Fasting Trial. Nutrients. 2022;14(18). [CrossRef]
- Hill NR, Oliver NS, Choudhary P, Levy JC, Hindmarsh P, Matthews DR. Normal reference range for mean tissue glucose and glycemic variability derived from continuous glucose monitoring for subjects without diabetes in different ethnic groups. Diabetes technology & therapeutics. 2011;13(9):921-8. [CrossRef]
- Pappe CL, Peters B, Dommisch H, Woelber JP, Pivovarova-Ramich O. Effects of reducing free sugars on 24-hour glucose profiles and glycemic variability in subjects without diabetes. Front Nutr. 2023;10:1213661. [CrossRef]
- Hermanides J, Vriesendorp TM, Bosman RJ, Zandstra DF, Hoekstra JB, DeVries JH. Glucose variability is associated with intensive care unit mortality*. Critical Care Medicine. 2010;38(3):838-42. [CrossRef]
- Thomsen MN, Skytte MJ, Astrup A, Deacon CF, Holst JJ, Madsbad S, et al. The clinical effects of a carbohydrate-reduced high-protein diet on glycaemic variability in metformin-treated patients with type 2 diabetes mellitus: A randomised controlled study. Clin Nutr ESPEN. 2020;39:46-52. [CrossRef]
- Hall H, Perelman D, Breschi A, Limcaoco P, Kellogg R, McLaughlin T, et al. Glucotypes reveal new patterns of glucose dysregulation. PLoS Biol. 2018;16(7):e2005143. [CrossRef]
- Broll S, Urbanek J, Buchanan D, Chun E, Muschelli J, Punjabi NM, et al. Interpreting blood GLUcose data with R package iglu. PLoS One. 2021;16(4):e0248560.
- Antoni R, Robertson T, Robertson M, Johnston J. A pilot feasibility study exploring the effects of a moderate time-restricted feeding intervention on energy intake, adiposity and metabolic physiology in free-living human subjects. Journal of Nutritional Science. 2018;7:e22. [CrossRef]
- Chow LS, Manoogian ENC, Alvear A, Fleischer JG, Thor H, Dietsche K, et al. Time-Restricted Eating Effects on Body Composition and Metabolic Measures in Humans who are Overweight: A Feasibility Study. Obesity (Silver Spring). 2020;28(5):860-9. [CrossRef]
- Jamshed H, Beyl RA, Della Manna DL, Yang ES, Ravussin E, Peterson CM. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients. 2019;11(6).
- Moro T, Tinsley G, Bianco A, Marcolin G, Pacelli QF, Battaglia G, et al. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. Journal of translational medicine. 2016;14(1):290.
- Peeke PM, Greenway FL, Billes SK, Zhang D, Fujioka K. Effect of time restricted eating on body weight and fasting glucose in participants with obesity: results of a randomized, controlled, virtual clinical trial. Nutrition & diabetes. 2021;11(1):6. [CrossRef]
- Hutchison AT, Regmi P, Manoogian ENC, Fleischer JG, Wittert GA, Panda S, et al. Time-Restricted Feeding Improves Glucose Tolerance in Men at Risk for Type 2 Diabetes: A Randomized Crossover Trial. Obesity (Silver Spring). 2019;27(5):724-32.
- Martens CR, Rossman MJ, Mazzo MR, Jankowski LR, Nagy EE, Denman BA, et al. Short-term time-restricted feeding is safe and feasible in non-obese healthy midlife and older adults. Geroscience. 2020;42(2):667-86. [CrossRef]
- Parr EB, Devlin BL, Radford BE, Hawley JA. A Delayed Morning and Earlier Evening Time-Restricted Feeding Protocol for Improving Glycemic Control and Dietary Adherence in Men with Overweight/Obesity: A Randomized Controlled Trial. Nutrients. 2020;12(2). [CrossRef]
- Wilkinson MJ, Manoogian ENC, Zadourian A, Lo H, Fakhouri S, Shoghi A, et al. Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome. Cell metabolism. 2020;31(1):92-104 e5.
- Kesztyus D, Cermak P, Gulich M, Kesztyus T. Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre-Post Design. Nutrients. 2019;11(12). [CrossRef]
- Lowe DA, Wu N, Rohdin-Bibby L, Moore AH, Kelly N, Liu YE, et al. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men With Overweight and Obesity: The TREAT Randomized Clinical Trial. JAMA Intern Med. 2020;180(11):1491-9.
- Parr EB, Devlin BL, Lim KHC, Moresi LNZ, Geils C, Brennan L, et al. Time-Restricted Eating as a Nutrition Strategy for Individuals with Type 2 Diabetes: A Feasibility Study. Nutrients. 2020;12(11).
- Phillips NE, Mareschal J, Schwab N, Manoogian ENC, Borloz S, Ostinelli G, et al. The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults. Nutrients. 2021;13(3).
- Yeoh EC, Zainudin SB, Loh WN, Chua CL, Fun S, Subramaniam T, et al. Fasting during Ramadan and Associated Changes in Glycaemia, Caloric Intake and Body Composition with Gender Differences in Singapore. Ann Acad Med Singap. 2015;44(6):202-6.
- Fernando HA, Zibellini J, Harris RA, Seimon RV, Sainsbury A. Effect of Ramadan Fasting on Weight and Body Composition in Healthy Non-Athlete Adults: A Systematic Review and Meta-Analysis. Nutrients. 2019;11(2).
- Sadeghirad B, Motaghipisheh S, Kolahdooz F, Zahedi MJ, Haghdoost AA. Islamic fasting and weight loss: a systematic review and meta-analysis. Public Health Nutr. 2014;17(2):396-406.
- Al-Barha NS, Aljaloud KS. The Effect of Ramadan Fasting on Body Composition and Metabolic Syndrome in Apparently Healthy Men. Am J Mens Health. 2019;13(1):1557988318816925.
- Kessler K, Pivovarova-Ramich O. Meal Timing, Aging, and Metabolic Health. International journal of molecular sciences. 2019;20(8).
- Kohsaka A, Laposky AD, Ramsey KM, Estrada C, Joshu C, Kobayashi Y, et al. High-fat diet disrupts behavioral and molecular circadian rhythms in mice. Cell metabolism. 2007;6(5):414-21.
- Zhao L, Hutchison AT, Liu B, Wittert GA, Thompson CH, Nguyen L, et al. Time restricted eating alters the 24-hour profile of adipose tissue transcriptome in men with obesity. Obesity (Silver Spring). 2022.
Figure 1.
Study design. Intervention start indicates the beginning of intermittent fasting in BF and TRE groups, whereas the control group was instructed not to alter its habitual food and eating timing.
Figure 1.
Study design. Intervention start indicates the beginning of intermittent fasting in BF and TRE groups, whereas the control group was instructed not to alter its habitual food and eating timing.
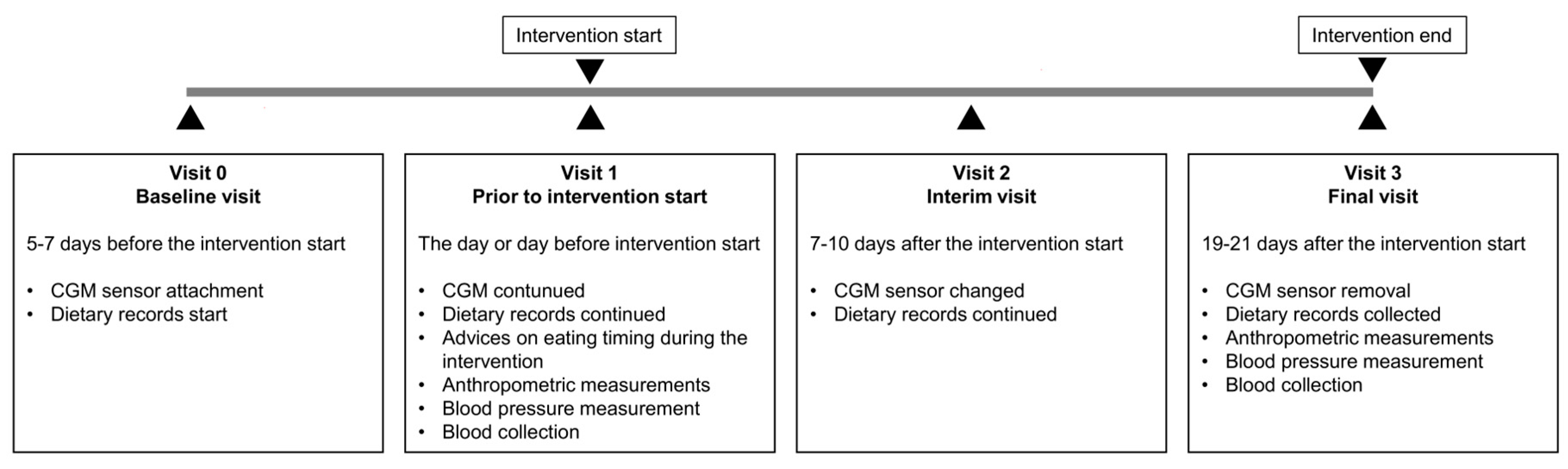
Figure 2.
24-hour glucose profiles and eating windows in the control group (A), BF group (B) and TRE group (C) before and during the intervention. For glucose profiles (above), p-values show the comparison of diurnal glucose profiles between the baseline and intervention phases, calculated by the RM ANOVA. Eating windows (below) are presented for the baseline (bas) and intervention (int) phases. Data is shown as mean ± SD.
Figure 2.
24-hour glucose profiles and eating windows in the control group (A), BF group (B) and TRE group (C) before and during the intervention. For glucose profiles (above), p-values show the comparison of diurnal glucose profiles between the baseline and intervention phases, calculated by the RM ANOVA. Eating windows (below) are presented for the baseline (bas) and intervention (int) phases. Data is shown as mean ± SD.
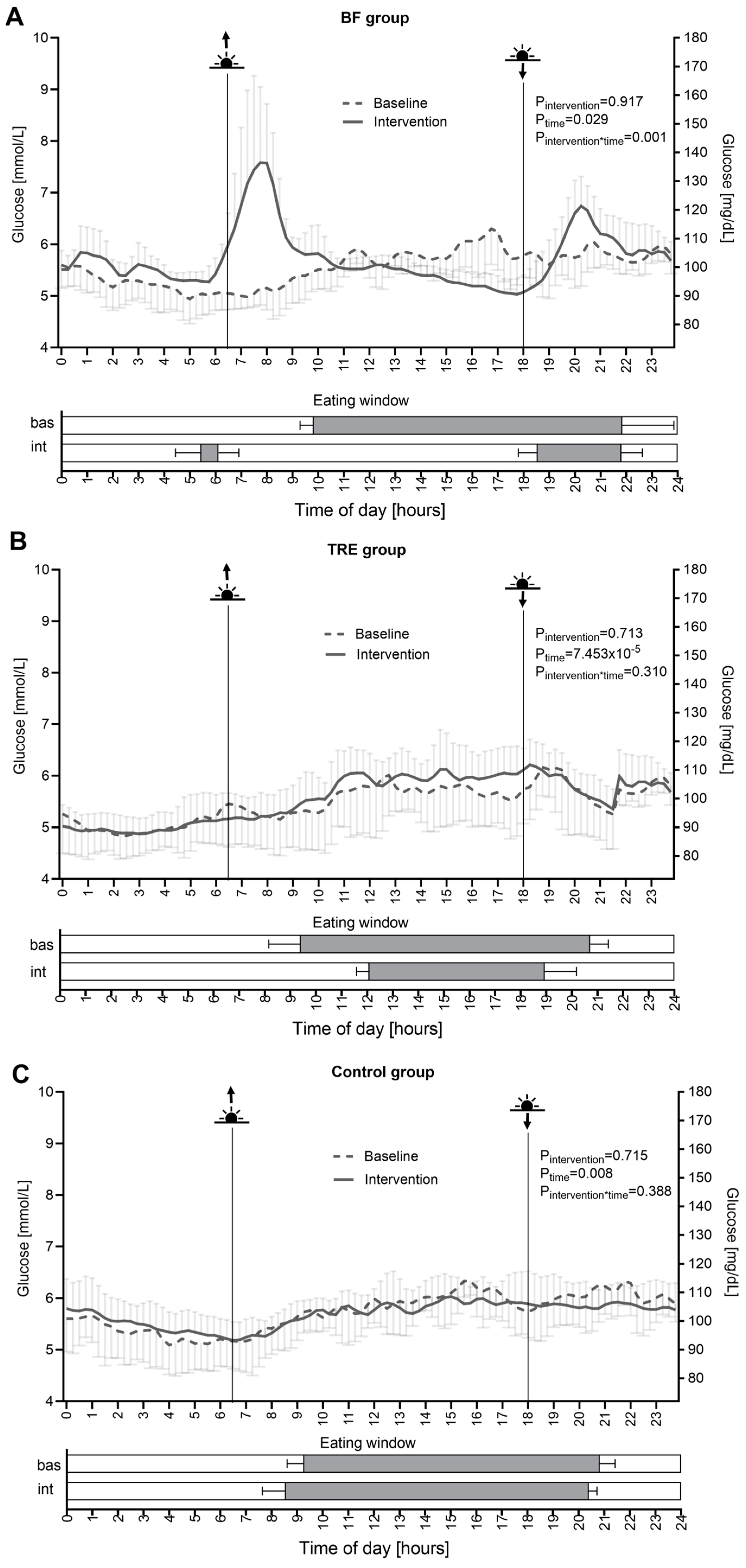
Figure 3.
Timely compliance, energy intake, and macronutrient composition in study groups. (A) Daily eating duration, (B) reduction of the eating window, (C) energy intake, and energy percent of macronutrient composition in control (D), BF (E) and TRE (F) groups. Non-shaded bars depict values at the baseline, shaded bars show values during the intervention. Data is shown as mean ± SD * p < 0.05; **p < 0.01, ***p < 0.001.
Figure 3.
Timely compliance, energy intake, and macronutrient composition in study groups. (A) Daily eating duration, (B) reduction of the eating window, (C) energy intake, and energy percent of macronutrient composition in control (D), BF (E) and TRE (F) groups. Non-shaded bars depict values at the baseline, shaded bars show values during the intervention. Data is shown as mean ± SD * p < 0.05; **p < 0.01, ***p < 0.001.
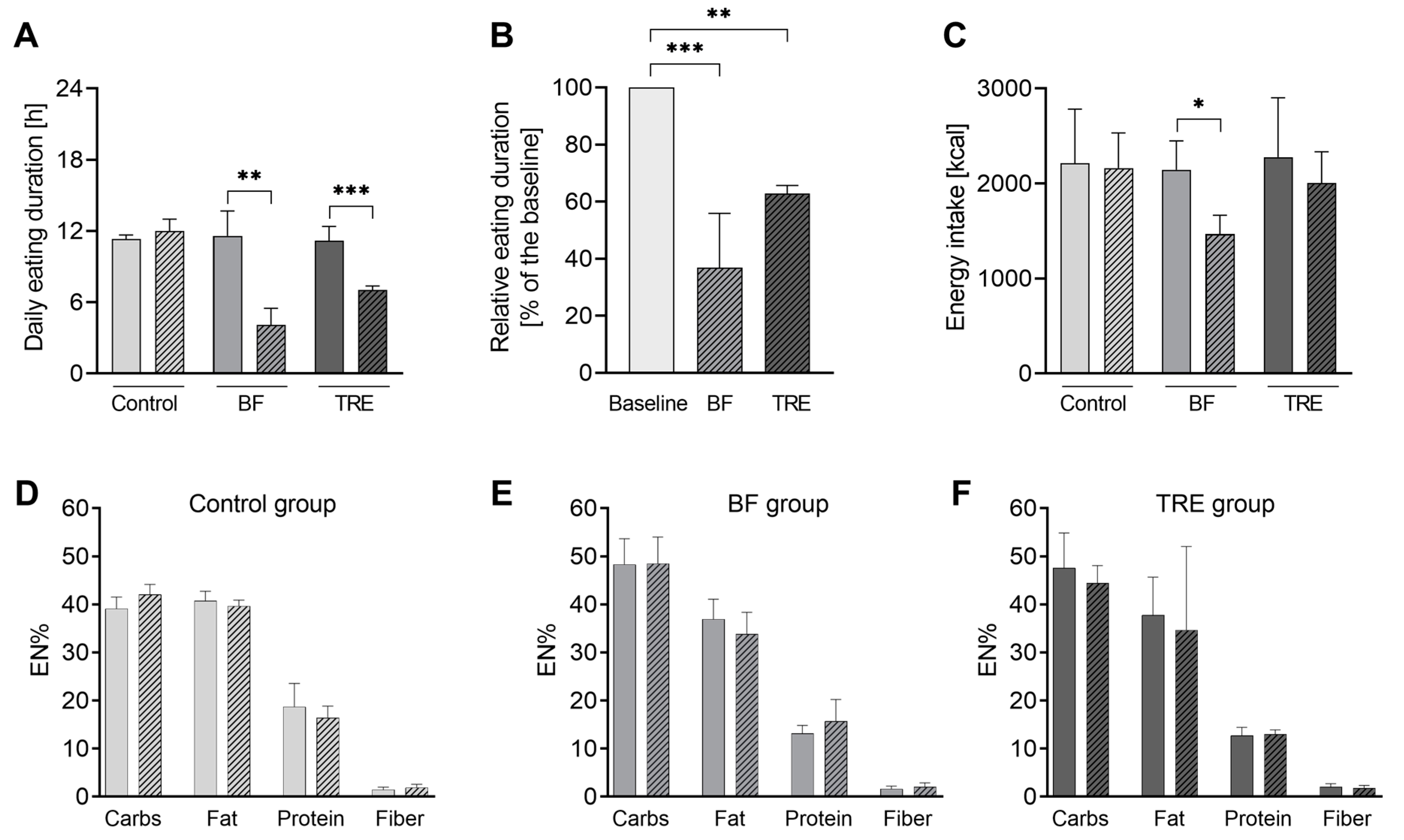
Figure 4.
Changes of anthropometric measures in study groups. (A) Body weight; (B) BMI; and (C) waist circumference. Data is shown as mean ± SD. *p < 0.05, **p < 0.01 in the within-group comparisons of parameters (after the intervention vs. before the intervention) assessed by paired t-test or Wilcoxon test.
Figure 4.
Changes of anthropometric measures in study groups. (A) Body weight; (B) BMI; and (C) waist circumference. Data is shown as mean ± SD. *p < 0.05, **p < 0.01 in the within-group comparisons of parameters (after the intervention vs. before the intervention) assessed by paired t-test or Wilcoxon test.
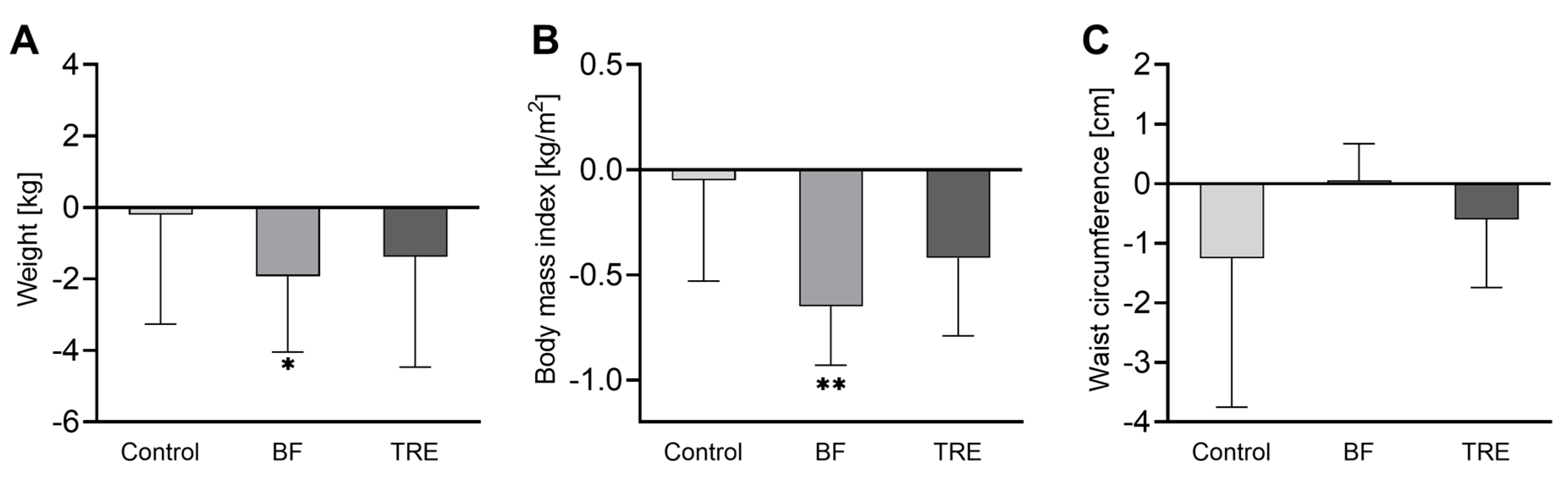
Figure 5.
Percentage of time spent in different glucotype patterns before and during the intervention. Light-grey area reflects proportion in low glucotype range, dark-grey area shows the proportion in the moderate glucotype range, and black area displays the proportion in the severe glucotype range in percentages.
Figure 5.
Percentage of time spent in different glucotype patterns before and during the intervention. Light-grey area reflects proportion in low glucotype range, dark-grey area shows the proportion in the moderate glucotype range, and black area displays the proportion in the severe glucotype range in percentages.
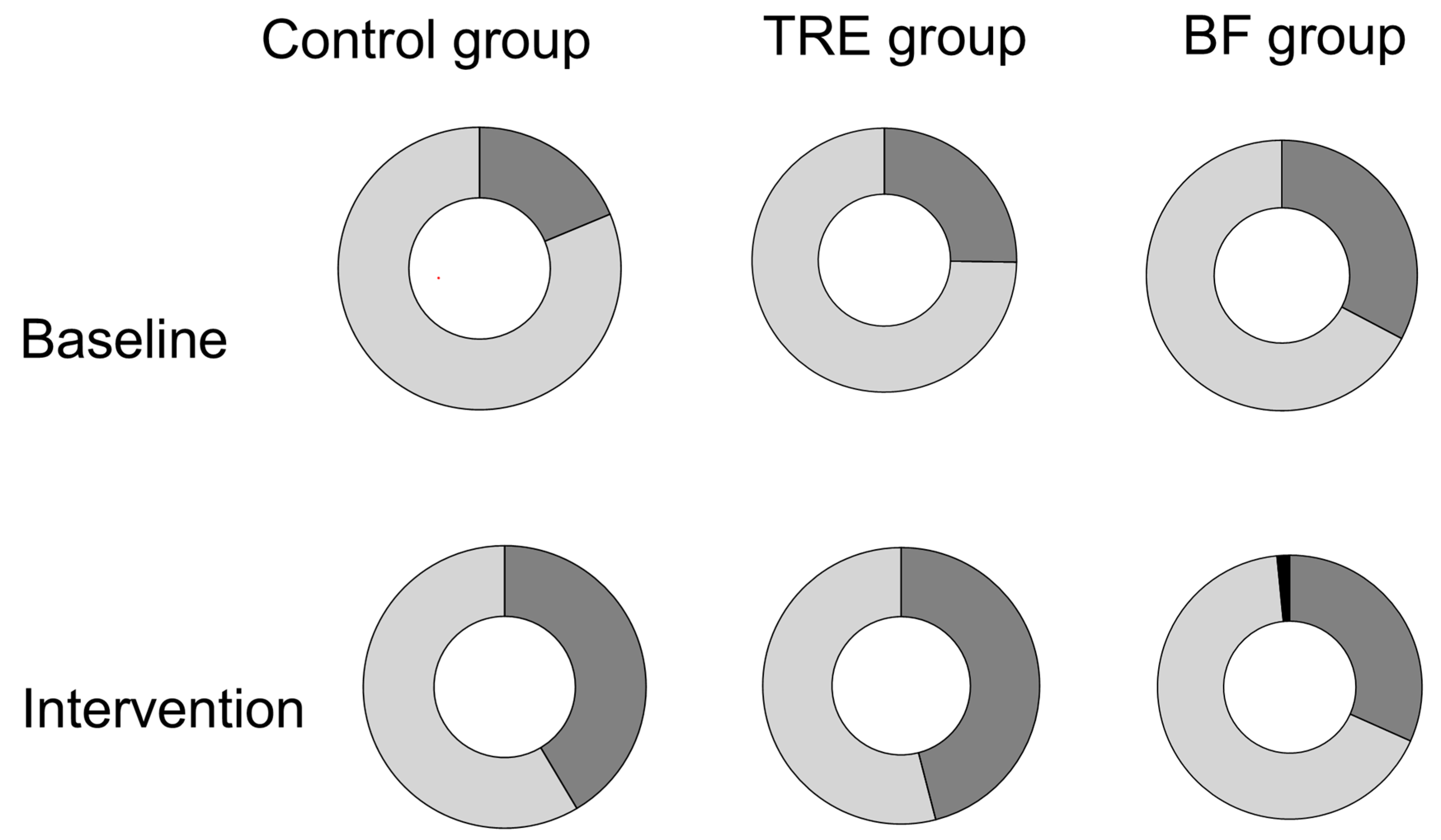

Table 1.
Baseline Characteristics of study population.
| Control group | BF group | TRE group | |
|---|---|---|---|
|
Clinical characteristics N |
4 |
6 |
6 |
| Male | 2 | 3 | 3 |
| Age [years] | 29 (28 – 35) | 31 (22 – 43) | 28 (25 – 32) |
| Weight [kg] | 85.9 ± 24.2 | 80.1 ± 18.1 | 79.5 ± 14.0 |
| BMI [kg/m²] | 27.4 ± 6.2 | 26.8 ± 3.9 | 25.5 ± 3.9 |
| Waist circumference [cm] | 89.5 ± 21.0 | 91.9 ± 17.8 | 85.2 ± 5.8 |
| SBP [mmHg] | 131.0 ± 20.2 | 132.3 ± 10.5 | 126.2 ± 12.6 |
| DBP [mmHg] | 78.0 ± 13.7 | 83.8 ± 6.6 | 85.0 ± 11.1 |
|
Glycemic parameters MSG [mmol/L] |
5.74 ± 0.47 |
5.56 ± 0.30 |
5.44 ± 0.57 |
| Minimum [mmol/L] | 4.96 ± 0.54 | 4.79 ± 0.35 | 4.72 ± 0.51 |
| Maximum [mmol/L] | 6.77 ± 0.44 | 6.68 ± 0.38 | 6.69 ± 0.74 |
| TBR <3.9 mmol/L [%] | 0.20 (0.00 – 4.39) | 0.78 (0.00 – 2.73) | 0.23 (0.00 – 3.83) |
| TAR >10 mmol/L [%] | 0.10 (0.00 – 0.37) | 0.00 (0.00 – 0.81) | 0.00 (0.00 – 0.12) |
| AUCgluc [min x mmol/L] | 8217 ± 673 | 7964 ± 431 | 7789 ± 813 |
| SD [mmol/L] | 0.81 ± 0.29 | 0.83 ± 0.10 | 0.78 ± 0.11 |
| CV [%] | 14.2 ± 5.69 | 14.9 ± 1.55 | 14.4 ± 1.79 |
| MAGE [mmol/L] | 1.03 ± 0.31 | 1.13 ± 0.05 | 1.09 ± 0.12 |
| CONGA [mmol/L] | 5.23 ± 0.44 | 4.96 ± 0.27 | 4.93 ± 0.57 |
| MAG change [mmol/L/h] | 1.12 ± 0.26 | 1.21 ± 0.08 | 1.09 ± 0.09 |
| MODD [mmol/L] | 0.73 ± 0.21 | 0.75 ± 0.08 | 0.66 ± 0.06 |
| LBGI | 1.28 ± 1.09 | 1.44 ± 0.61 | 1.86 ± 1.40 |
| HBGI | 0.78 ± 0.58 | 0.70 ± 0.31 | 0.59 ± 0.21 |
| Glucotype [low:moderate:severe] | 0:4:0 | 0:5:0 | 0:5:0 |
| HbA1c [%] | 5.10 ± 0.29 | 5.13 ± 0.42 | 5.07 ± 0.16 |
Data is shown as mean ± SD when normally distributed and median (IQR) when not normally distributed. BMI, Body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; MSG, mean sensor glucose; TAR, time above range; TBR, time below range; AUCgluc, area under the glucose curve; SD, standard deviation; CV, coefficient of variation; MAGE, mean amplitude of glucose excursions; CONGA, continuous overall net glycemic action; MAG change, mean absolute glucose change; MODD, mean of daily differences; LBGI, low blood glucose index; HBGI, high blood glucose index; HbA1c, glycated hemoglobin; CGM, continuous glucose monitoring.
Table 2.
Changes in glycaemic control and glycaemic variability after the intervention in comparison to the baseline values.
Table 2.
Changes in glycaemic control and glycaemic variability after the intervention in comparison to the baseline values.
| Control group | BF group | TRE group | p-value between groupsc | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Changesa | p-valueb | Changesa | p-valueb | Changesa | p-valueb | BF vs. Control | TRE vs. Control | TRE vs. BF | ||||
| Glycaemic Parameters | ||||||||||||
| MSG [mmol/L] | -0.05 ± 0.24 | 0.710 | 0.17 ± 0.26 | 0.220 | 0.05 ± 0.27 | 0.690 | 0.556 | 0.921 | 0.871 | |||
| Minimum [mmol/L] | 0.20 ± 0.46 | 0.460 | 0.19 ± 0.27 | 0.187 | 0.08 ± 0.25 | 0.520 | 1.000 | 0.941 | 0.939 | |||
| Maximum [mmol/L]f | -0.55 ± 0.19 | 0.011 | 1.41 ± 1.04 | 0.039 | -0.22 ± 0.75 | 0.556 | 0.010 | 0.901 | 0.022 | |||
| TBR <3.9 mmol/L [%] | -0.11 (-2.56 – 0.00) | 0.180 | -0.78 (-2.45 – 0.67) | 0.273 | 0.08 (-2.85 – 0.70) | 0.715 | - | - | - | |||
| TAR >10 mmol/L [%] | -0.07 (-0.31 – 0.00) | 0.180 | 0.38 (0.00 – 2.52) | 0.109 | 0.00 (0.00 – 0.15) | 0.317 | 0.012 | 0.180 | 0.209 | |||
| AUCgluc [min x mmol/L] | -71 ± 343 | 0.705 | 241 ± 367 | 0.216 | 79 ± 388 | 0.673 | 0.548 | 0.912 | 0.876 | |||
| Glycemic Variability | ||||||||||||
| SD [mmol/L] | -0.07 ± 0.14 | 0.423 | 0.13 ± 0.18 | 0.184 | -0.02 ± 0.05 | 0.422 | 0.155 | 0.950 | 0.287 | |||
| CV [%] | -1.19 ± 3.16 | 0.507 | 1.71 ± 2.57 | 0.226 | -0.54 ± 1.34 | 0.422 | 0.270 | 0.971 | 0.422 | |||
| MAGE [mmol/L] | -0.14 ± 0.13 | 0.121 | 0.19 ± 0.34 | 0.251 | -0.12 ± 0.13 | 0.113 | 0.130 | 0.999 | 0.133 | |||
| CONGA [mmol/L] | -0.02 ± 0.22 | 0.893 | 0.18 ± 0.26 | 0.188 | 0.14 ± 0.31 | 0.370 | 0.648 | 0.792 | 0.992 | |||
| MAG change [mmol/L/h] | -0.11 ± 0.06 | 0.036 | -0.10 ± 0.16 | 0.238 | -0.16 ± 0.19 | 0.135 | 1.000 | 0.952 | 0.925 | |||
| MODD [mmol/L] | -0.04 ± 0.09 | 0.473 | -0.12 ± 0.12 | 0.098 | -0.07 ± 0.07 | 0.098 | 0.599 | 0.957 | 0.848 | |||
| LBGI | -0.13 ± 0.72 | 0.738 | -0.28 ± 0.46 | 0.244 | -0.27 ± 0.86 | 0.523 | 0.986 | 0.989 | 1.000 | |||
| HBGI | -0.31 ± 0.40 | 0.220 | 0.60 ± 0.79 | 0.164 | -0.13 ± 0.15 | 0.118 | 0.077 | 0.953 | 0.141 | |||
| HbA1c [%] | -0.08 ± 0.22 | 0.257 | 0.04 ± 0.11 | 0.342 | -0.06 ± 0.11 | 0.547 | 0.628 | 0.998 | 0.683 | |||
ᵃ Data is shown as mean ± SD when normally distributed and median (IQR) when not normally distributed. b Intra-group comparison; p<0.05 by Student’s t-test for normally distributed data or Wilcoxon test for not normally distributed data. c Inter-group comparison by ANOVA test with Sidak post-hoc for normally distributed data and Kruskal-Wallis test with Dunn post-hoc for not normally distributed data. MSG, mean sensor glucose; TAR, time above range; TBR, time below range; AUCgluc, area under the glucose curve; SD, standard deviation; CV, coefficient of variation; MAGE, mean amplitude of glucose excursions; CONGA, continuous overall net glycemic action; MAG change, mean absolute glucose change; MODD, mean of daily differences; LBGI, low blood glucose index; HBGI, high blood glucose index; HbA1c, glycated hemoglobin; CGM, continuous glucose monitoring.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



