
Submitted:
02 July 2024
Posted:
03 July 2024
You are already at the latest version
Abstract
Postoperative RT is recommended after breast conserving surgery and mastectomy (with risk factors). Consideration of pros and cons including potential side effects demands for optimization of adjuvant RT and a risk-adapted approach. There is clear de-escalation in fractionation - hypofractionation should be considered standard. For selected low risk situations PBI only or even the omission of RT might be appropriate. In contrast, tendencies in escalating RT are obvious. Preoperative RT seems attractive for patients in whom breast reconstruction is planned or for defining the tumor location more precisely with the potential of giving ablative doses. Dose escalation by a (simultaneous integrated) boost or the combination with new compounds/systemic treatments may increase antitumor efficacy but also toxicity. Despite low evidence, RT for oligometastatic disease is becoming increasingly popular. The omission of axillary dissection in node-positive disease led to an escalation of regional RT. Studies are ongoing to test if any axillary treatment can be omitted and which oligometastatic patients do really benefit from RT. Besides technical improvements the incorporation of molecular risk profiles but also the response to neoadjuvant systemic therapy have the potential to optimize the decision-making if and how local and/or regional RT should be administered.
Keywords:
Adjuvant radiotherapy
; omission of radiotherapy
; partial breast irradiation
; de-escalation
; escalation
; loco-regional irradiation
; optimization
Introduction
Adjuvant treatment in early breast cancer is based on its multi-disciplinarity and is getting more and more complex. RT either after breast conserving surgery (BCS) or mastectomy (PMRT) has a long tradition and is an integral part in the treatment algorithm, but ‘one size fits all’ is past. With the possibility to characterize the tumor situation and the risk of relapse more precisely, optimization either as escalation or de-escalation of the treatment approach is key.
Undoubtedly, local tumor control will be significantly improved by adjuvant RT [1]. This is widely independent from the subgroup of patients with an average 3- to 4-fold relative risk reduction [1]. This improvement in local/-regional control may also convert into better overall survival (OS). However, the absolute risk reduction is mainly defined by the risk at diagnosis, and the gain in local control in low-risk patients might be only a few percent. In addition, impact on OS in low-risk patients has not been proven or is presumably in a range, which is considered clinically negligible.
Furthermore, no positive effect without side effects. We have to be aware of radiotherapeutic acute and potential long-term toxicity. Nearly all patients will get local inflammatory reactions towards the end of irradiation, which are in general well manageable and seldom severe. A lot of different interventions have been tried to reduce acute toxicity for the skin, one of the most promising might be the use of Mepithel film, which could reduce the incidence of radiation dermatitis and improved patient-reported outcomes (PRO) in a recent meta-analysis of three randomized controlled trials [2]. Using modern techniques with intensity-modulated fields led to the reduction of acute toxicity. In daily practice more pronounced (exudative) skin reactions are uncommon and recover normally within a few weeks. Late reactions are more important, as late reactions represent often a scarring of tissue. Regarding local RT, severe induration of the breast is an issue, which can finally lead to the removal of the breast in rare cases. The loss of reconstruction especially after implant-based approaches is a major concern for PMRT, as well as the risk for persistent arm lymph edema after regional irradiation especially in patients who underwent additional axillary lymph node dissection (ALND). Interestingly, limited data couldn’t demonstrate a statistically significant impact on quality of life, neither in the low-risk situation (5-yrs data of the PRIME 1 study) [3], nor in the postmastectomy setting (2-yrs data of the SUPREMO trial) [4]. Increasing implementation of PRO data in clinical studies and in daily routine will give us more insights regarding this important issue. Last but not least, some ev. toxicity for lung, heart and ribs and the possibility of tumor induction by ionizing irradiation demand for optimization of adjuvant RT and a risk-adapted approach.
In the present manuscript, important topics regarding de-escalation but also escalation will be identified and some strategies are discussed to optimize the decision-making if and how local and/or regional RT should be administered.
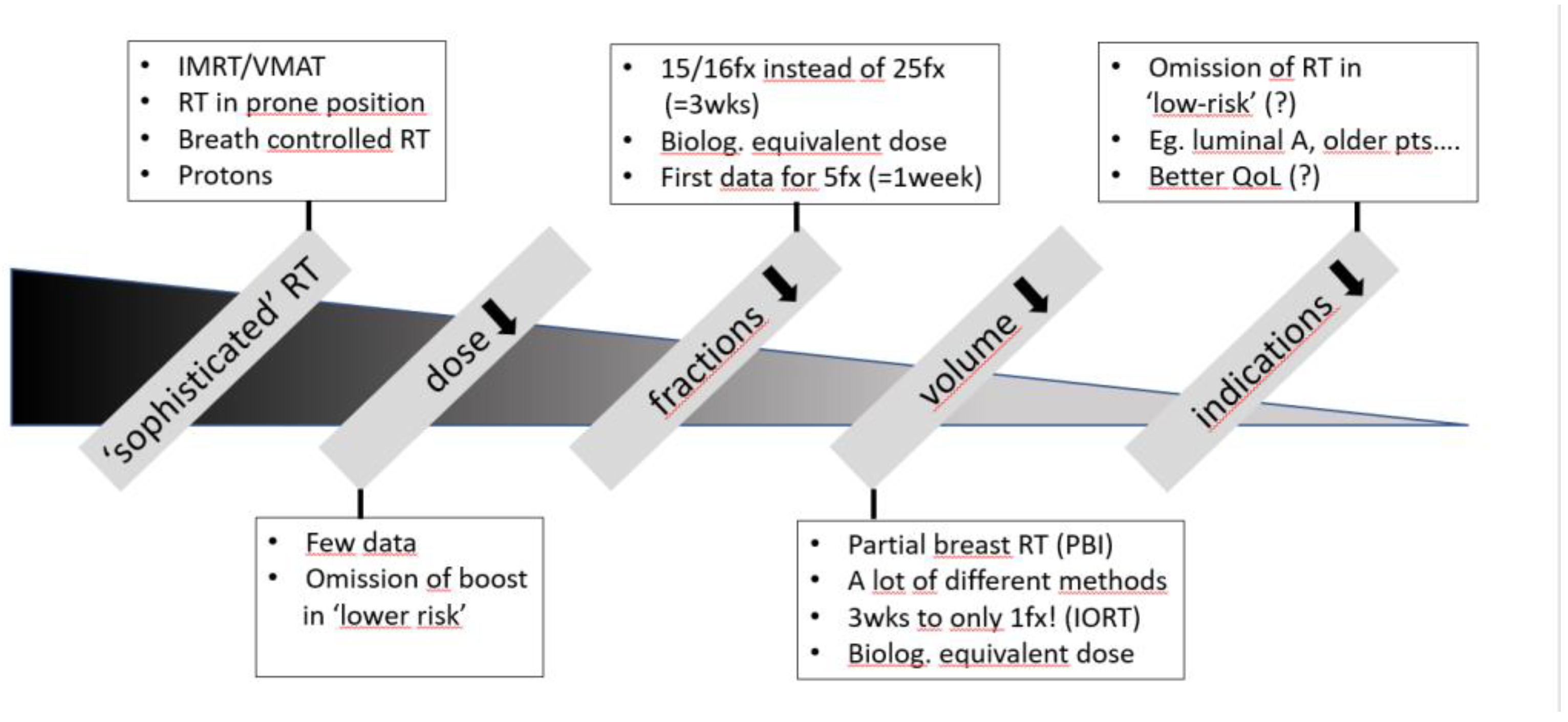
1. Possibilities of De-Escalation (see Figure 1)
1.1‘. Sophisticated’ RT
Technical improvements like intensity-modulated RT (IMRT), volumetric-modulated arc therapy (VMAT) and on-board imaging (OBI) including cone-beam CTs (CBCT) for appropriate positioning of the patient allow an optimized dose-distribution for the target volume and dose application. Acute toxicity like exudative skin alterations will be reduced substantially [5,6]. Irradiation in prone position or breath-controlled in deep inspiration can better spare lung and heart, and especially in patients with large breasts irradiation in prone position can reduce acute reactions [7,8,9]. In general, photons are used. Few centers have the possibility of proton treatment, which is quite complex and expensive due to several reasons. For example, proton treatment in Switzerland is only available at the Paul Scherrer Institute (PSI) in Villigen, Aargau, for certain indications, but breast cancer treatment will not be reimbursed by insurance companies. According to the database of the particle therapy cooperative group (PTCOG; www.ptcog.site) a total of 350336 patients have been treated with protons worldwide from 1954 – 2023, about 7% of them for breast cancer. Protons have a special dose distribution in tissue, and might be beneficial in situations where an organ at risk is just in the nearby of the target volume, which can be an issue for the heart, if loco-regional RT including the parasternal lymph nodes is indicated in left-sided breast cancer. A pragmatic trial in the US (RadComp; RTOG 3510; NCT02603341) [10] is evaluating the comparison of photon and proton RT. The primary endpoint are major cardiovascular events. First results will not be available before 2032. The current evidence as well as ongoing randomized trials are perfectly summarized in a systematic review and meta-analysis by Holt et al., a total of 32 non-randomized studies with 1452 patients and a follow-up of 2 -59 months (mo) were included [11].
Figure 1.
Possibilities for RT de-escalation. Abbreviations: IMRT=intensity-modulated radiotherapy; VMAT=volumetric modulated arc therapy; RT=radiotherapy; fx=fraction; pts=patients; QoL=quality of life; wks=weeks; IORT=intraoperative radiotherapy
Figure 1.
Possibilities for RT de-escalation. Abbreviations: IMRT=intensity-modulated radiotherapy; VMAT=volumetric modulated arc therapy; RT=radiotherapy; fx=fraction; pts=patients; QoL=quality of life; wks=weeks; IORT=intraoperative radiotherapy
The most important point is an intra- and interobserver variability in contouring the planning target volume (PTV) even despite contouring guidelines eg. from ESTRO [12]. Artificial intelligence can help, several systems for automated contouring are on the market. Not only regarding contouring, but also in treatment planning an inter-planner variation is evident [13]. Knowledge-based treatment planning has the potential to produce plans of uniform quality by reducing the inter-planner variability and the duration of the optimization process [14].
1.2. Dose Reduction
After demonstration that boost irradiation can decrease local failure rates [15] the interest to conduct trials for dose reduction was low. To my knowledge the St. Georg and Wollongong Breast -Boost trial (additional boost in combination with reduced whole breast dose) has never been published regarding local control [16]. A small whole breast dose reduction outside of the tumor bed (from 40 Gray - Gy to 36 Gy in 15 fractions) was not inferior in the IMPORT LOW trial [17]. In addition, compared to previous times boost irradiation is generally not any longer given in patients with lower risk considering pros and cons [18].
1.3. Reduction in Fractions
Hypofractionated RT schemes use higher single doses, which is biologically more effective. As a consequence, total dose and overall treatment time have to be reduced to reach comparable biological dose effects. Over decades 25 fractions with a single dose of 2 Gy in total 5 weeks were considered standard, which has been replaced by overwhelming data of a three weeks treatment of 15 or 16 fractions up to a total dose of 40 to 42.5 Gy in breast conservation [19] and after mastectomy [20]. There is a clear trend to further reduce fraction number and overall treatment time, the FAST FORWARD protocol of 5 fractions of 5.2 Gy single dose (ultrahypofractionation) has been already widely adopted especially during the COVID pandemic in several countries, despite the fact that only five years data have been published (but with excellent results) [21]. A German expert panel (DEGRO) is considering the 3 weeks schedule still standard, as moderate or marked late effects increased with longer follow-up in disadvantage of the ultrahypofractionated arm for most items [22]. There is not much data on ultrahypofractionation for regional node irradiation, results for the nodal subgroup in the FAST FORWARD study are pending. Both, simple and complex RT techniques are allowed in the ongoing HYPART trial [23] to create the possibility also for low-income countries to follow this approach. The ESTRO Advisory Committee in Radiation Oncology Practice state, that moderately hypofractionation (the 3-weeks scheme) can be offered to any patient for whole breast, chest wall (with or without reconstruction), and nodal volumes; the 5 fractions schedule can also be offered for non-nodal breast or chest wall (without reconstruction) RT either as standard of care or within a randomized trial or prospective cohort [24].
1.4. Volume Reduction – Partial Breast Irradiation Only (PBI)
Reducing RT volume allows an increase of the single dose, and consequentially also a reduction in fraction number and overall treatment duration. There are several different treatment modalities and schemes available, and PBI can be given pre-, intra- or postoperatively. In general, patients with low-risk for failure have been included in such trials. Both, 5-yrs and 10-yrs outcome data tend to be comparable and low in regard to local failures, in most studies also with reduced toxicity for the PBI arm. For intraoperative treatment (IORT) with a single high dose fraction (about 20 Gy) local failure rates are significantly higher in the ELIOT trial [25]. Another IORT trial (TARGIT-A) yielded similar outcome data, the non-breast-cancer-specific mortality was even better with IORT [26], but was criticized mainly due to statistical issues. Overall, mortality seems to be comparable, the heart-death-rate is 0.3% less for PBI [27]. It’s important to allow the normal tissue enough recovery time. Although less acute toxicity has been observed, there was an increase in moderate late toxicity and worse cosmesis, which might be related to the twice per day treatment scheme (10 fractions of 3.85 Gy over 5-8 days) in the RAPID trial [28]. For low-risk patients PBI is well accepted in several guidelines, eg. the German S3 guideline [18].
1.5. Reduction of Indication (= Omission of RT)
The smaller the initial risk of failure the less is the potential absolute gain due to adjuvant RT. Many trials have evaluated the omission of RT in low-risk situations. Commonly used criteria for low-risk in recent trials after BCS are age (above 65 or 70 years), T-stage (T1 or small T2), hormone-responsiveness, node-negative disease, and no G3 differentiation. All trials have shown a benefit for additional RT regarding local control. However, the absolute difference was rather small, and there was no impact on cause-specific or overall survival (OS). Recently the 10-yrs results of the PRIME 2 study have been published [29]: In selected lower-risk patients, in which adjuvant antihormonal therapy has been prescribed, local failure rates at 10 years were 0.9% with versus 9.5% without RT, with similar OS in both arms. Especially in older women the omission of RT is an option. Discussing pros and cons of additional RT with the patient it is important to mention that these excellent data have been achieved in the backbone of antihormonal therapy. In daily practice it’s not seldom the case that patients at lower risk are reluctant to take five years of tamoxifen or aromatase inhibitors. As consequence they often choose RT as their only treatment. Additional parameters would be helpful to redefine risk and optimize adjuvant treatment for these patients.
There is a long-lasting discussion about PMRT, especially in the intermediate risk group (T1-2 N1). Since the publication of the Danish trials in 1997 and 1999 [30,31], PMRT is recommended for larger T-stage tumors (pT3/pT4) or patients with four or more involved axillary lymph nodes. The 30-year data demonstrate that optimal long-term treatment benefit can only be achieved in both, optimal loco-regional and systemic tumor control, furthermore, PMRT did not result in excess ischemic heart damage, nor in other non-breast cancer related death [32]. Due to some criticism of the DBCG 82b/c trials regarding quality of surgery and systemic therapy, no clear indication for PMRT has been given in the subgroup of patients with pT1/pT2 and 1-3 positive nodes, but the NCCN guidelines state that additional RT ‘should be strongly considered’ [33]. Interestingly, this didn’t change over more than 20 years. Often additional risk factors are used to decide about PMRT ‘yes’ or ‘no’ [18]. The results of the SUPREMO trial, in which patients with 1-3 positive nodes, with stage pT2pN0 and the presence of grade 3 and/ or vascular invasion and with stage pT3pN0 were randomized between loco-regional or no RT following mastectomy, are pending [34]. As ALND is nowadays seldom performed, the exact number of lymph nodes are unknown in most patients. Other factors besides number of nodes are urgently needed to optimize the indication for PMRT.
2. Possibilities of Escalation (see Figure 2)
2.1. Preoperative RT
RT as soon as possible might be beneficial [35]. A large randomized trial has been launched in Germany to test this approach ([36], NEORAD trial), the first patient has been randomized just recently in March 2024. Optimal reconstruction strategies in the setting of PMRT are challenging [37]. Especially for patients, in which mastectomy and breast reconstruction is planned, preoperative RT would avoid irradiation of a reconstructed breast, perhaps with lower side effects and better cosmesis. At ASTRO 2022 retrospective data were presented in patients with mastectomy and DIEP reconstruction, either with pre- or postoperative irradiation [38]. The authors observed a significantly higher incidence of flap contracture (41.9% vs. 1.9%) and fat necrosis (19.4% vs. 12.9%) in patients with PMRT, and a good/excellent cosmetic outcome in 96.1% of women when RT was applied preoperatively vs. 80.6% with PMRT [38]. Preoperative RT might be also beneficial for defining exact tumor location for PBI only or as preceded boost, eg. aiming to achieve higher pCR rates [39,40].
Figure 2.
Possibilities for RT escalation. Abbreviations: RT=radiotherapy; pCR=pathological complete remission; reco=breast reconstruction; chemo=chemotherapy; Re-RT=re-irradiation; BCS=breast conserving surgery; LF=local failure; SIB=simultaneous integrated boost; pts=patients; oligoM1= oligometastatic disease
Figure 2.
Possibilities for RT escalation. Abbreviations: RT=radiotherapy; pCR=pathological complete remission; reco=breast reconstruction; chemo=chemotherapy; Re-RT=re-irradiation; BCS=breast conserving surgery; LF=local failure; SIB=simultaneous integrated boost; pts=patients; oligoM1= oligometastatic disease
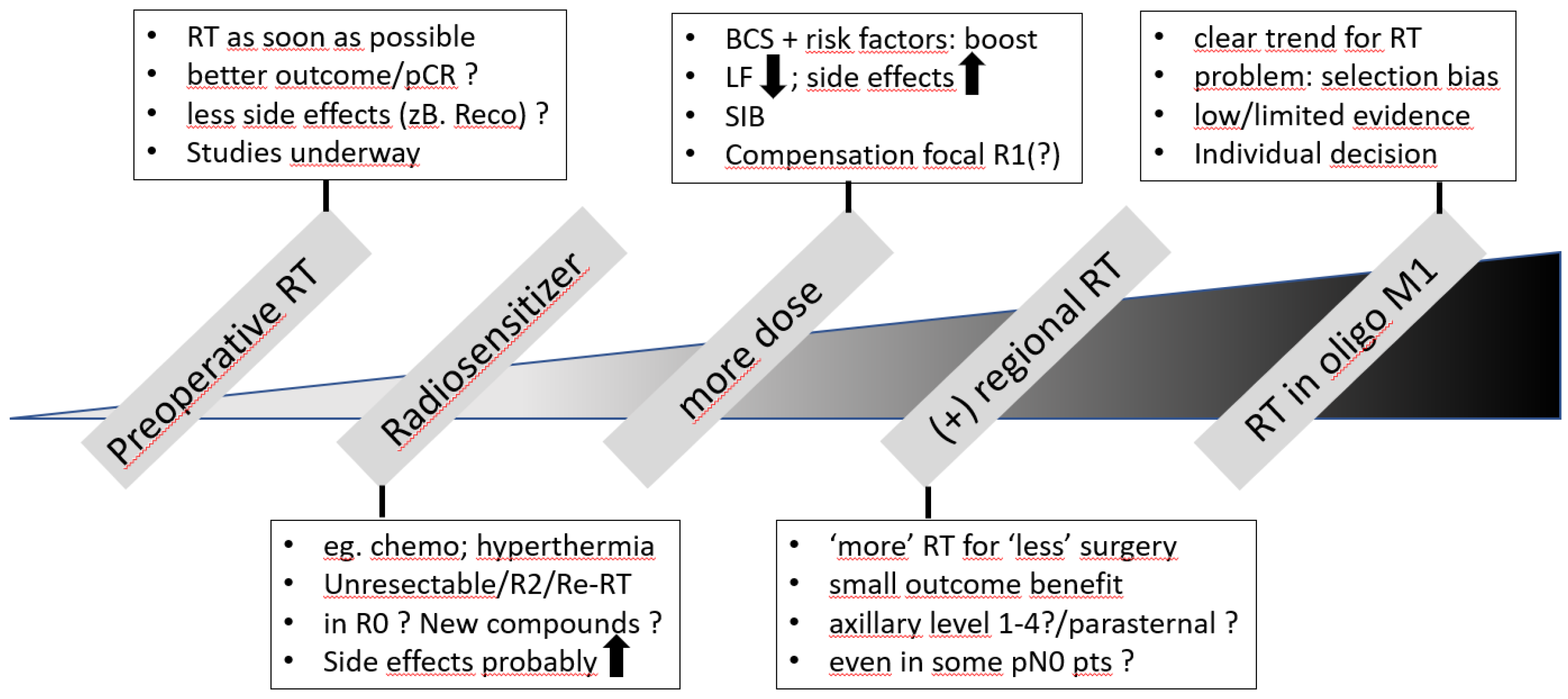
2.2. Radiosensitizer
Simultaneous application of chemotherapy or hyperthermia are well known radiosensitizer. Especially in situations with unresectable tumor or local relapse and previous RT the combination will be used to optimize local control [41]. As concomitant chemotherapy can increase relevant side effects to organs-at-risk like lung and/or heart [42], standard of care is to give both treatments sequentially with chemotherapy first. However, preoperative chemotherapy is becoming more and more popular, and as stated above there is also some rationale for preoperative RT. Therefore, the combination of both especially in the preoperative setting gets more attention. An excellent overview has been recently published [43]. Of particular interest is that three studies [44,45,46] plan to analyze the combination of RT and immunotherapy. Novel drugs, also in combination, are rapidly entering clinical practice. However, data about their optimal use with the focus of combination with RT are seldom provided. An international multidisciplinary consensus summarized this topic and recommendations have been recently published [47]. A very recent multicenter retrospective study suggests that concurrent use of antibody-drug-conjugates and brain irradiation is associated with a higher risk of symptomatic radiation necrosis (27% vs. 7% cumulative incidence at 2 years; p=0.014) in HER2-positive breast cancer patients [48].
2.3. Dose Escalation (Boost)
Additional dose to the tumor bed (= Boost) can improve efficacy after BCS. Besides the possibility of decreasing local failure rates (relative risk reduction of about 50%), no impact on OS could be demonstrated, and giving more dose has also some increase in side effects [15,49]. Therefore, boost irradiation is only recommended in the presence of risk factors. Some of them are young age, node-positivity or close margins. Especially young patients may benefit from a high dose boost. This has been tested in a large phase 3 trial with 2421 patients who were all aged 50 years or younger randomized to standard dose boost (16 Gy in 8 fractions) or high dose boost (26 Gy in 13 fractions). The 10-yrs results have been presented at the 14th European Breast Cancer Conference in March 2024 [50]. The 10-yrs local failure rate was 4.4% with 16 Gy boost vs 2.8% with 26 Gy. This small benefit does not justify the increased impact on cosmetic outcome, as 48% of patients with the high-dose boost experienced severe or moderate fibrosis vs 27% with 16 Gy [50].
Integrating the boost simultaneously (SIB) to whole breast RT provides better dose-homogeneity and reduces overall treatment time. According to a systematic review in 2022 of nine published trials, one of them randomized, a SIB with standard dose seems to be effective and safe [51]. This has been recently confirmed by the IMPORT HIGH trial, whereas a further boost dose escalation from 48 to 53 Gy was not beneficial [52]. The results from the German HYPOSIB trial investigating 48 Gy SIB in 16 fractions are eagerly awaited [53]. Preliminary safety data have been presented at ASTRO, acute skin reactions were less pronounced and occurred two weeks earlier in the HYPOSIB-arm than in the control arm [53]. The RTOG 1005 trial investigated 48 Gy SIB in 15 fractions with noninferiority for local control and similar toxicity for SIB and sequential boost [54]. First data have been presented also for the five-fractions-scheme [55], and other trials are ongoing [56,57]. The HYPORT trial is testing the five-fractions-scheme, both SIB and sequential boost techniques are allowed [56], the RHEAL trial is using sequential boosts [57]. The TARGIT-B trial testing an intraoperative versus a sequential boost is still ongoing, data lock will be end of October 2024 [58]. Interestingly, according to the Dutch database, boost irradiation might counteract the risk of focally involved resection margins (R1) with a small difference in local failure rates at 5 years (1% with vs 3% without re-excision), but without impact on DFS or OS [59].
2.4. Additional Regional RT
Regional lymph nodes irradiation leads to a small but significant improvement of CSS and OS in newer trials, a significant reduction in breast cancer mortality was even seen in pN0 patients, but the difference was very small – 1.6% at 15 years [60,61]. It is unclear, which lymph node area RT (axilla/periclavicular/parasternal) counts most. Newer data indicate that RT of the parasternal lymph nodes might be beneficial, especially in medially located, node-positive tumors and with modern RT technique used [62,63,64]. In a retrospective analysis of the EORTC 22922/10925 randomized trial the 15-yrs OS benefit was 4.9% with ‘modern’ vs 1.1% with ‘old’ technique [64]. Especially trials like ACOSOG Z0011 [65], AMAROS [66] and OTOASOR [67] have led to a dramatic decrease of ALND in patients with positive sentinel lymph node macrometastasis/es in favor of regional RT (identical tumor control, ca. 50% less arm lymph edema). Further optimization is needed to define the subgroup of node-positive patients in which any axillary treatment can be safely omitted.
2.5. RT in Oligometastatic Situations
The concept of an optimized local tumor control in oligometastatic disease is currently evaluated in multiple cancer types including breast. Due to high likelihood of a selection bias it is unclear, which subgroup of patients with oligoM1 might benefit [68]. The randomized NRG-BR002 trial has been presented at ASCO 2022 [69]: The addition of metastasis-directed therapy to standard-of-care systemic treatment did not show a signal for better progression-free survival or OS, therefore the trial was not proceeded to the preplanned phase 3 component. More data are needed to answer this important question. The German S3 Guideline recommends an individual and multidisciplinary decision in selected cases [18].
3. Possibilities for Optimization
3.1. Technical Issues
As mentioned above a lot of technical improvements have led to the possibility of a very sophisticated RT planning and application. IMRT, VMAT, image-guided positioning of the patient/PTV, prone positioning esp. for large breasts and breath-controlled RT (deep inspiration) esp. for left-sided breast cancer are becoming standard of care in RT departments worldwide. Counteracting the inter-observer variability in contouring, which is the basis for the whole treatment chain, is of high priority. We have tested three different AI-solutions in our department, two of them were considered excellent. MRI has a superior soft tissue contrast compared to standard CT-based planning. Especially for contouring and the definition of the CTV (eg. for PBI as boost or as sole irradiation) or the primary tumor itself in case of preoperative RT MRI-based planning might be beneficial. Furthermore, MR-Linacs allow for online adaptive treatment planning before each fraction [70,71], but the impact of this approach regarding clinical benefit is not well known. As the patient’s time on the treatment couch is clearly increased, so far only few institutes (to our knowledge eg. only one in Switzerland) have installed a MR-Linac and even less are using this machine for breast cancer treatment. Proton treatment is of emerging interest, however results from at least six ongoing randomized trials in Denmark, UK, Thailand and the USA have to be awaited [11]. In general, a potential therapeutic gain due to further technical improvements in the future seems to become smaller and smaller.
3.2. Biology-Based Optimization
Several important questions regarding more or less RT are unanswered. While biology- and molecular-driven decisions about adjuvant chemotherapy are current standard, there is lack of data for RT. In low-risk situations it is still unclear in which subgroup RT can be safely omitted. The individual randomized trials showed a significant increase in local failures without RT but no impact on OS. In a meta-analysis omission of RT led to a 6.8-fold increased local failure risk (HR 6.8, 95%-CI 4.23–10.93) [72]. According to results from retrospective analyses molecular signatures have the potential to select patients for RT omission [73]. However, these tests should be evaluated prospectively, before they are used in routine clinical practice. Biology-driven prospective studies including molecular classifiers are ongoing (see Table 1). Nearly all trials have antihormonal treatment as backbone, whereas adjuvant RT is omitted either in single-arm or in a randomized fashion. First results with two to five years follow-up revealed excellent results so far, however long-term data are needed. As co-chair of the ongoing EXPERT trial [79] testing the omission of whole breast irradiation in low-risk patients defined by clinical/histopathological parameters and the PAM50 assay I have to admit that randomizing patients into the trial is not easy. Two main reasons are fear of undertreatment and a must to undergo endocrine therapy (ET). In a patient survey, about half of the patients aged 75 years or older, ET had the biggest negative impact on QoL and patients would rather choose RT instead of ET [82]. Being at low-risk it is questionable if patients really need both, RT and ET. In a retrospective analysis of 496 patients with a median age of 76 years, 62% of them received combined RT+ET and 30% RT monotherapy, long-term recurrence rates were extremely low, even with the omission of endocrine treatment [83]. In the phase 3 EUROPA trial patients aged 70+ years will get randomized to either RT or ET alone, and the primary endpoint will be health-related quality-of-life at 2 years [81]. Another approach to define low risk is the integration of preoperative MRI to assess low local tumor burden. Women aged 50 years or older with cT1N0 non-triple-negative breast cancer were eligible. Those with unifocal cancer had BCS and adequate systemic treatment. If pT1N0/N1mi, RT was omitted (n=201) [84]. The invasive local failure rate at 5 years was 1.0% (upper 95% CI 5·4%) [84]. As local failure rates may increase especially after the end of adjuvant systemic therapy, long-term follow-up has to be awaited to define subgroups of patients which can safely forego RT.
For the distinction of no RT, local or loco-regional RT mainly T- and N-stage are used. Especially the appropriate treatment of the axilla by surgery and or RT has been discussed heavily over the last years. The abovementioned sentinel trials [65,66,67] had as consequence that the exact number of axillary lymph nodes is not any longer known due to the omission of axillary dissection. Whereas AMAROS [65] and OTOASOR [67] used large comprehensive RT fields, ACOSOG Z0011 [65] has furthermore ignited the discussion about the necessity of regional irradiation in these patients, as according to the treatment protocol only breast RT was required. However, the study was lousy in regard to RT documentation. For 605 of 856 patients no RT info was given, and a detailed RT record review was only possible for 228 patients [85]. According to the review, about 81% received tangential RT alone, about half of them with high tangents encompassing parts of the lower axilla, and some patients received directed nodal irradiation via a third field. Overall, there was no significant difference between treatment arms in the use of protocol-prohibited nodal fields [85]. As it is common practice to provide treatment plans (eg. in case of re-irradiation), it is somehow strange that a detailed review was possible for only 228 patients. My personal hypothesis is, that the local radiation oncologist didn’t know about the field restriction within the trial and haven’t sent the documents by realizing this after request. Indeed, radiation oncologists’ use of differing radiation fields in this trial was associated with treating higher risk patients defined by nomograms [86]. The authors observed significant association with higher nomogram estimated risk and supraclavicular irradiation (OR=1.07, 95% CI: 1.04–1.10, p<0.0001) but not high tangents (OR = 0.99, 95% CI:0.96–1.02, p=0.52) [86]. Uncertainties in the ACOSOG Z0011 trial regarding RT led to the discussion of intentional (INT) versus incidental (INC) RT of the axilla and to the implementation of RT QA programs in trials dealing with optimal axillary treatment, eg. the TAXIS trial in clinically node-positive disease [87]. The OPTIMAL phase 3 trial randomized 442 patients to either incidental (by breast only RT) or intentional regional RT [88]. With a median follow-up of 3.7 years, the estimated DFS at 5-years were 93.7% and 93.8% in the INC and INT irradiation groups respectively (one-sided 95% CI: <5.7%; non-inferiority p = 0.075) [88]. Neither in the recently published SINODAR ONE [89] and SENOMAC [90] randomized trials nor in the BOOG 2013-07 nationwide registry trial [91] - all of them supporting the omission of ALND after a positive sentinel lymph node biopsy, exact RT doses to the axillary regions are provided. Thus, the optimal adjuvant regional node irradiation volume for early-stage breast cancer with T1-2N1 remains undetermined. The T-REX phase 3 study randomizes patients with ER+, Her2 negative T1-2 disease with 1-2 sentinel macrometastases (mets) to regional RT or not [92]. The accompanying translational protocol aims to decipher the prognostic and predictive role of tumor biology and gene expression analysis for their potential integration into future adjuvant RT individualization [92]. The probably most important ongoing trial is the Tailor RT (MA39) trial [93], as it uses tumor biology (including Oncotype DX® recurrence score - RS) as eligibility criterion. Initially started for patients with following criteria: low Oncotype Dx RS <18; ER positive/Her2 negative; pT1-2; age 40+ years; and 1-3 macromets after ALND/1-2 SN macromets after BCS/1 macromet after mastectomy, amendments allow also randomisation of patients with micromets, 2 SN macromets after mastectomy, T3N0 disease, age limit 35+ years and an Oncotype DX RS up to 25. A total of 2140 patients will get loco-regional RT as standard vs breast RT only after BCS and no RT at all after mastectomy [93]. A much smaller randomized phase 2 trial, the IMNI PRECISION trial, uses a ‘low-risk’ genomic score (RecurIndex® test) to randomize 214 patients clinically at higher risk to internal mammary node irradiation yes or no [94]. A large SEER database study (n=6509) highlights the possible role of the RS in predicting the outcome of adjuvant RT in T1-2N1 luminal BC patients undergoing BCS. Adjuvant RT was not associated with better 5-year outcomes in the low-risk RS cohort [95]. As of now, the available evidence does not support the inclusion of gene expression assays into the decision-making process for RT. Abovementioned ongoing prospective trials will help to optimize the indication of RT in specific subgroups of patients [96].
3.3. Tumor-Response-Based Considerations
Neoadjuvant systemic treatment (NAST) is becoming more and more popular and for specific subgroups pathological complete remission (pCR) rates are high. In initially node-positive patients undergoing NAST the conversion to ypN0 is an important prognostic factor with better outcome [97]. Treatment response to NAST might offer the possibility to optimize adjuvant RT in regard to indication and volumes. The most important question: When can we avoid PMRT or at least regional irradiation following NAST? Montero et al. reviewed the available literature [98]. The median rates of reported locoregional relapses according to lymph node response following NAST in patients with ypN0 were 3.2% (range 0–7.7%) with and 24.4% (range 7.7-41.7%) without PMRT, in patients with ypN+ 10.8% (range 0–46%) with and 56.3% (range 11.2–100%) without PMRT [98]. However, data are mostly derived from retrospective analyses, and there is an urgent need of prospective and randomized studies. In the RAPCHEM trial [99] patients with cT1-2cN1 were grouped into three risk categories according to the nodal status after NAST, and RT volumes were prespecified for each group. For patients who had ypN0 or pN1mi without risk factors (cT >3 cm, G3, LVI) only whole-breast RT after BCS and no PMRT was foreseen. Despite excellent results (5-yrs locoregional recurrence rates between 2-3%) extrapolation of the trial results to modern practice is difficult. More than 80% of the patients had ALND (even in low risk) and protocol violations were quite common including PMRT in >30% of patients in the low risk group [100]. This serves as good example that randomization is key. The phase 3 ATNEC study is ongoing: cT1-3cN1 patients with ypN0 after NAST will get randomized to additional axillary RT or ALND versus no further axillary treatment [101]. 1900 patients are planned, on January 24th 2024 the 300th patient has been randomized. One of the most awaited studies has been recently presented at the last San Antonio Breast Cancer Symposium: The NSABP B-51/RTOG1304-trial addresses the question of PMRT and RNI in cT1-3 cN1 that convert to ypN0 after NAST. Patients were randomized to WBI with or without regional RT after BCS and loco-regional PMRT versus no PMRT at all [102]. A total of 1556 patients with a median follow-up of 59.5 months could be analyzed. The invasive breast cancer recurrence-free interval at 5 years was similar with 91.8% in the no RNI (59 events) and 92.7% (50 events) in the RNI arm. Of interest was an exploratory subgroup analysis regarding tumor subtype. In fact, there was a statistically significant interaction (p=0.037) favoring RNI in ER/PR+/Her2- patients versus a detrimental effect for ‘more’ RT in triple negative disease (HR 2.3; 1.00-5.25), which contains normally higher loco-regional relapse rates. Events were low and findings might be by chance, which would demand for further follow-up. In a retrospective analysis of 1966 early-stage TNBC a higher abundance of tumor-infiltrating lymphocytes (TIL) was associated with better survival [103]. Regarding the NSABP-B51 findings, one might hypothesize that comprehensive, larger RT-fields might compromise the immune system. A very recent study demonstrated and externally validated the significance of full dosimetric data, particularly the volume of low dose at 1 Gy (V1) of critical structures on lymphopenia after RT in breast cancer patients [104]. This deserves attention as especially modern RT techniques for large fields like VMAT have relatively high values (large volume) of V1 [104]. In this context a re-analysis of the B51 data regarding TILs and lymphopenia - if possible - would be interesting. The current NCCN guideline still strongly consider loco-regional PMRT in patients with cN+ -> ypN0 disease [33], however de-escalation of RT fields is an option after a case-by-case discussion with the patient. For Her2-positive disease, the NRG-BR008 phase 3 trial (HERO) evaluates the omission of RT in early-stage low risk patients after BCS, defined by either pT1N0 or cT-3cm/cN0 with ypT0N0 after neoadjuvant chemotherapy and HER2 targeted therapy. As of 02-05-2024 accrual was 13 of 1300 patients planned [105] - still a long way to go.
Conclusions
Radiotherapy is an important pillar in the adjuvant treatment in breast cancer. Less fractions and less RT-volume like PBI only as well as technical improvements have led to a reduction of side effects and provide better and more convenient treatment. Appropriate patient selection towards low risk of relapse offers the possibility of RT omission. However, so far no subgroup of patients could be identified which did not benefit from adjuvant RT at all. Ongoing studies including biology and molecular assays should answer the question which patients could safely forego irradiation and how RT volumes can be adapted. It is very likely that the response to neoadjuvant systemic treatments could help in optimization.
References
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG), Darby S., McGale P., Correa C., Taylor C., Arriagada R., Clarke M., Cutter D., Davies C., Ewertz M., Godwin J., et al.: Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011 Nov 12;378(9804):1707-16.
- Shariati S., Behroozian T., Kennedy S., Caini S., Herst P.M., Zhang L., Ding K., Karam I., van den Hurk C., Wolf J.R., et al.: Mepithel film for the prevention and treatment of acute radiation dermatitis in breast cancer: a systematic review and meta-analysis of randomized controlled trials. Support Care Cancer. 2023 Aug 16; 31(9): 524.
- Prescott R.J., Kunkler I.H., Williams L.J., King C.C., Jack W., van der Pol M., Goh T.T., Lindley R., Cairns J.: A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial. Health Technol Assess. 2007 Aug;11(31):1-149.
- Velikova G., Williams L.J., Willis S., Dixon J.M., Loncaster J., Hatton M., Clarke J., Kunkler I.H., Russell N.S.: MRC SUPREMO trial UK investigators: Quality of life after postmastectomy radiotherapy in patients with intermediate-risk breast cancer (SUPREMO): 2-year follow-up results of a randomised controlled trial. Lancet Oncol. 2018 Nov;19(11):1516-1529.
- Joseph K., Vos L.J., Gabos Z., Pervez N., Chafe S., Tankel K., Warkentin H., Ghosh S., Amanie J., Powell K., et al.: Skin Toxicity in Early Breast Cancer Patients Treated with Field-In-Field Breast Intensity-Modulated Radiotherapy versus Helical Inverse Breast Intensity-Modulated Radiotherapy: Results of a Phase III Randomised Controlled Trial. Clin Oncol (R Coll Radiol). 2021 Jan;33(1):30-39. [CrossRef]
- Yee C., Wang K., Asthana R., Drost L., Lam H., Lee J., Vesprini D., Leung E., DeAngelis C., Chow E.: Radiation-induced Skin Toxicity in Breast Cancer Patients: A Systematic Review of Randomized Trials. Clin Breast Cancer. 2018 Oct;18(5): e825-e840.
- Jagsi R., Griffith K.A., Moran J.M., Ficaro E., Marsh R., Dess R.T., Chung E., Liss A.L., Hayman J.A., Mayo C.S., et al.: A Randomized Comparison of Radiation Therapy Techniques in the Management of Node-Positive Breast Cancer: Primary Outcomes Analysis. Int J Radiat Oncol Biol Phys. 2018 Aug 1;101(5):1149-1158. [CrossRef]
- Mulliez T., Veldeman L., Speleers B., Mahjoubi K., Remouchamps V., Van Greveling A., Gilsoul M., Berwouts D., Lievens Y., Van den Broecke R., et al.: Heart dose reduction by prone deep inspiration breath hold in left-sided breast irradiation. Radiother Oncol. 2015 Jan;114(1):79-84. [CrossRef]
- Mulliez T., Veldeman L., van Greveling A., Speleers B., Sadeghi S., Berwouts D., Decoster F., Vercauteren T., De Gersem W., Van den Broecke R., et al.: Hypofractionated whole breast irradiation for patients with large breasts: a randomized trial comparing prone and supine positions. Radiother Oncol. 2013 Aug;108(2):203-8. [CrossRef]
- Bekelman J.E., Lu H., Pugh S., Baker K., Berg C.D., de Gonzalez A.B., Braunstein L.Z., Bosch W., Chauhan C., Ellenberg S., et al., RadComp (Radiotherapy Comparative Effectiveness Consortium): Pragmatic randomised clinical trial of proton versus photon therapy for patients with non-metastatic breast cancer: the Radiotherapy Comparative Effectiveness (RadComp) Consortium trial protocol. BMJ Open. 2019 Oct 15;9(10): e025556.
- Holt F., Probert J., Darby S.C., Haviland J.S., Coles C.E., Kirby A.M., Liu Z., Dodwell D., Ntentas G., et al.: Proton Beam Therapy for Early Breast Cancer: A Systematic Review and Meta-analysis of Clinical Outcomes. Int J Radiat Oncol Biol Phys. 2023 Nov 15;117(4):869-882. Epub 2023 Mar 2. [CrossRef] [PubMed] [PubMed Central]
- Offersen B.V., Boersma L.J., Kirkove C., Hol S., Aznar M.C., Biete Sola A., Kirova Y.M., Pignol J-P., Remouchamps V., Verhoeven K., et al.: ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother Oncol 2015; 114: 3 – 10. [CrossRef]
- Nelms BE, Robinson G, Markham J, Velasco K, Boyd S, Narayan S, et al.. Variation in external beam treatment plan quality: An inter-institutional study of planners and planning systems. PractRadiatOncol. 2012; 2(4):296–305. [CrossRef]
- Phurailatpam R., Sah M.K., Wadasadawala T., Khan A., Palottukandy J., Gayake U., Jain J., Sarin R., Pathak R., Krishnamurthy R., et al.: Can knowledge based treatment planning of VMAT for post-mastectomy locoregional radiotherapy involving internal mammary chain and supraclavicular fossa improve performance efficiency? Front Oncol. 2023 Apr 3;13:991952. [CrossRef] [PubMed] [PubMed Central]
- Bartelink, H; Maingon, P; Poortmans, P; Weltens, C; Fourquet, A; Jager, J; Schinagl, D; Oei, B; Rodenhuis, C; Horiot, JC; et al.: Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3 trial. Lancet Oncol. 2015, 16(1), 47–56. [CrossRef]
- Hau E, Browne L, Capp A, Delaney GP, Fox C, Kearsley JH, Millar E, Nasser EH, Papadatos G, Graham PH: The impact of breast cosmetic and functional outcomes on quality of life: long-term results from the St. George and Wollongong randomized breast boost trial. Breast Cancer Res Treat. 2013 May;139(1):115-23.
- Coles CE, Griffin CL, Kirby AM, Titley J, Agrawal RK, Alhasso A, Bhattacharya IS, Brunt AM, Ciurlionis L, Chan C, et al.: IMPORT Trialists. Import low Partial-breast radiotherapy after breast conservation surgery for patients with early breast cancer (UK IMPORT LOW trial): 5-year results from a multicentre, randomised, controlled, phase 3, non-inferiority trial. Lancet. 2017 Sep 9;390(10099):1048-1060. [CrossRef]
- www.leitlinienprogramm-onkologie.de/fileadmin/user_upload/Downloads/Leitlinien/Mammakarzinom_4_0/Version_4.4/LL_Mammakarzinom_Langversion_4.4.pdf (accessed on May 17th, 2024).
- Haviland JS, Owen JR, Dewar JA, Agrawal RK, Barrett J, Barrett-Lee PJ, Dobbs HJ, Hopwood P, Lawton PA, Magee BJ, et al.: START Trialists' Group: The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol. 2013 Oct;14(11):1086-1094.
- Wang SL, Fang H, Song YW, Wang WH, Hu C, Liu YP, Jin J, Liu XF, Yu ZH, Ren H, et al.: Hypofractionated versus conventional fractionated postmastectomy radiotherapy for patients with high-risk breast cancer: a randomised, non-inferiority, open-label, phase 3 trial. Lancet Oncol. 2019 Mar;20(3):352-360.
- Murray Brunt A, Haviland JS, Wheatley DA, Sydenham MA, Alhasso A, Bloomfield DJ, Chan C, Churn M, Cleator S, Coles CE, et al.: FAST-Forward Trial Management Group: Hypofractionated breast radiotherapy for 1 week versus 3 weeks (FAST-Forward): 5-year efficacy and late normal tissue effects results from a multicentre, non-inferiority, randomised, phase 3 trial. Lancet. 2020 May 23;395(10237):1613-1626.
- Krug D, Baumann R, Combs SE, Duma MN, Dunst J, Feyer P, Fietkau R, Haase W, Harms W, Hehr T, et al.: Breast Cancer Expert Panel of the German Society of Radiation Oncology (DEGRO). Moderate hypofractionation remains the standard of care for whole-breast radiotherapy in breast cancer: Considerations regarding FAST and FAST-Forward. Strahlenther Onkol. 2021 Apr;197(4):269-280. Epub 2021 Jan 28. [CrossRef] [PubMed] [PubMed Central]
- Yadav BS, Dahiya D, Kannan P, Goyal S, Laroiya I, Irrinki S, Singh NR, Sharma R: HYPofractionated Adjuvant RadioTherapy in 1 versus 2 weeks in high-risk patients with breast cancer (HYPART): a non-inferiority, open-label, phase III randomized trial. Trials. 2024 Jan 2;25(1):21.
- Meattini I, Becherini C, Boersma L, Kaidar-Person O, Marta GN, Montero A, Offersen BV, Aznar MC, Belka C, Brunt AM, et al.: European Society for Radiotherapy and Oncology Advisory Committee in Radiation Oncology Practice consensus recommendations on patient selection and dose and fractionation for external beam radiotherapy in early breast cancer. Lancet Oncol. 2022 Jan;23(1):e21-e31. [CrossRef]
- Orecchia R, Veronesi U, Maisonneuve P, Galimberti VE, Lazzari R, Veronesi P, Jereczek-Fossa BA, Cattani F, Sangalli C, Luini A, et al.: ELIOT trial Intraoperative irradiation for early breast cancer (ELIOT): long-term recurrence and survival outcomes from a single-centre, randomised, phase 3 equivalence trial. Lancet Oncol. 2021 May;22(5):597-608. [CrossRef]
- JS Vaidya, M Bulsara, Ml Baum, F Wenz, S Massarut, S Pigorsch, M Alvarado, M Douek, C Saunders, HL Flyger, et al.: Long term survival and local control outcomes from single dose targeted intraoperative radiotherapy during lumpectomy (TARGIT-IORT) for early breast cancer: TARGIT-A randomised clinical trial. BMJ. 2020; 370: m2836. [CrossRef]
- Haussmann J, Budach W, Corradini S, Krug D, Tamaskovics B, Bölke E, Djiepmo-Njanang FJ, Simiantonakis I, Kammers K, Matuschek C: No Difference in Overall Survival and Non-Breast Cancer Deaths after Partial Breast Radiotherapy Compared to Whole Breast Radiotherapy-A Meta-Analysis of Randomized Trials. Cancers (Basel). 2020 Aug 17;12(8):2309.
- Whelan TJ, Julian JA, Berrang TS, Kim DH, Germain I, Nichol AM, Akra M, Lavertu S, Germain F, Fyles A, et al.: External beam accelerated partial breast irradiation versus whole breast irradiation after breast conserving surgery in women with ductal carcinoma in situ and node-negative breast cancer (RAPID): a randomised controlled trial. RAPID Trial Investigators. Lancet. 2019 Dec 14;394(10215):2165-2172. [CrossRef]
- Kunkler IH, Williams LJ, Jack WJL, Cameron DA, Dixon JM. Breast-Conserving Surgery with or without Irradiation in Early Breast Cancer. N Engl J Med. 2023 Feb 16;388(7):585-594. [CrossRef]
- Overgaard M, Hansen PS, Overgaard J, Rose C, Andersson M, Bach F, Kjaer M, Gadeberg CC, Mouridsen HT, Jensen MB, Zedeler K. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. Danish Breast Cancer Cooperative Group 82b Trial. N Engl J Med. 1997 Oct 2;337(14):949-55. [CrossRef]
- Overgaard M, Jensen MB, Overgaard J, Hansen PS, Rose C, Andersson M, Kamby C, Kjaer M, Gadeberg CC, Rasmussen BB, et al.: Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet. 1999 May 15;353(9165):1641-8. [CrossRef]
- Overgaard M, Nielsen HM, Tramm T, Højris I, Grantzau TL, Alsner J, Offersen BV, Overgaard J; DBCG Radiotherapy Group. Postmastectomy radiotherapy in high-risk breast cancer patients given adjuvant systemic therapy. A 30-year long-term report from the Danish breast cancer cooperative group DBCG 82bc trial. Radiother Oncol. 2022 May;170:4-13. Epub 2022 Mar 11. [CrossRef] [PubMed]
- www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on June 27th, 2024).
- Kunkler IH, Canney P, van Tienhoven G, Russell NS; MRC/EORTC (BIG 2-04) SUPREMO Trial Management Group. Elucidating the role of chest wall irradiation in 'intermediate-risk' breast cancer: the MRC/EORTC SUPREMO trial. Clin Oncol (R Coll Radiol). 2008 Feb;20(1):31-4. [CrossRef] [PubMed]
- Matuschek C, Nestle-Kraemling C, Haussmann J, et al. Long-term cosmetic outcome after preoperative radio−/chemotherapy in locally advanced breast cancer patients. Strahlenther Onkol. 2019; 195:615–28. [CrossRef]
- www.gbg.de/en/trials/neorad (accessed on May 26th, 2024).
- O'Donnell JPM, Murphy D, Ryan ÉJ, Gasior SA, Sugrue R, O'Neill BL, Boland MR, Lowery AJ, Kerin MJ, McInerney NM. Optimal reconstructive strategies in the setting of post-mastectomy radiotherapy - A systematic review and network meta-analysis. Eur J Surg Oncol. 2021 Nov;47(11):2797-2806. [CrossRef]
- L Admojo, P Chidley, YH Lin, F Foroudi, S Jassal, SW Loh, G Chew, E Bevington, SL Ng, A Hyett, T Leech, WM Ooi, Chionh, M Chao; Comparing Radiotherapy (RT) Late Toxicities to the Reconstructed DIEP Flap in Breast Cancer Patients Treated with Neoadjuvant RT (NART) vs. Post-Mastectomy RT (PMRT); Int J Radiat Oncol Biol Phy, Volume 114, Issue 3, Suppl., S145, November 01, 2022.
- Civil YA, Jonker LW, Groot Koerkamp MPM, Duvivier KM, de Vries R, Oei AL, Slotman BJ, van der Velde S, van den Bongard HJGD. Preoperative Partial Breast Irradiation in Patients with Low-Risk Breast Cancer: A Systematic Review of Literature. Ann Surg Oncol. 2023 Jun;30(6):3263-3279. [CrossRef]
- Meattini I, Francolini G, Di Cataldo V, Visani L, Becherini C, Scoccimarro E, Salvestrini V, Bellini C, Masi L, Doro R, Di Naro F, Loi M, Salvatore G, Simontacchi G, Greto D, Bernini M, Nori J, Orzalesi L, Bianchi S, Mangoni M, Livi L. Preoperative robotic radiosurgery for early breast cancer: Results of the phase II ROCK trial (NCT03520894). Clin Transl Radiat Oncol. 2022 Sep 22;37:94-100. [CrossRef]
- EL Jones, JR Oleson, LR Prosnitz, TV Samulski, Z Vujaskovic, D Yu, LL Sanders, MW Dewhirst: Randomized Trial of Hyperthermia and Radiation for Superficial Tumors. J Clin Oncol. 2005 May 1;23(13):3079-85. [CrossRef] [PubMed]
- Kim DY, Youn JC, Park MS, Lee S, Choi SW, Ryu KH, Kim LS, Shim MS, Lee JJ, Han S. Cardiovascular outcome of breast cancer patients with concomitant radiotherapy and chemotherapy: A 10-year multicenter cohort study. J Cardiol. 2019 Aug;74(2):175-181. [CrossRef]
- Montero A, Ciérvide R. Preoperative Radio(Chemo)Therapy in Breast Cancer: Time to Switch the Perspective? Curr Oncol. 2022 Dec 12;29(12):9767-9787. [CrossRef] [PubMed] [PubMed Central]
- Breast Cancer Study of Preoperative Pembrolizumab + Radiation - Full Text View - ClinicalTrials.gov (accessed on June 2nd, 2024).
- Neo-adjuvant Chemotherapy Combined With Stereotactic Body Radiotherapy to the Primary Tumour +/- Durvalumab, +/- Oleclumab in Luminal B Breast Cancer: - Full Text View - ClinicalTrials.gov (accessed on June 2nd, 2024).
- Converting HR+ Breast Cancer Into an Individualized Vaccine - Full Text View - ClinicalTrials.gov (accessed on June 2nd, 2024).
- Meattini I, Becherini C, Caini S, Coles CE, Cortes J, Curigliano G, de Azambuja E, Isacke CM, Harbeck N, Kaidar-Person O, Marangoni E, Offersen BV, Rugo HS, Salvestrini V, Visani L, Morandi A, Lambertini M, Poortmans P, Livi L; Consensus Panellist Group. International multidisciplinary consensus on the integration of radiotherapy with new systemic treatments for breast cancer: European Society for Radiotherapy and Oncology (ESTRO)-endorsed recommendations. Lancet Oncol. 2024 Feb;25(2):e73-e83. [CrossRef]
- Koide Y, Nagai N, Adachi S, Ito M, Kawamura M, Ito M, Ito F, Shindo Y, Aoyama T, Shimizu H, et al.: Impact of concurrent antibody-drug conjugates and radiotherapy on symptomatic radiation necrosis in breast cancer patients with brain metastases: a multicenter retrospective study. J Neurooncol. 2024 Jul;168(3):415-423. Epub 2024 Apr 22. [CrossRef] [PubMed]
- Chua BH, Link EK, Kunkler IH, Whelan TJ, Westenberg AH, Gruber G, Bryant G, Ahern V, Purohit K, Graham PH, et al.: BIG 3–07/TROG 07.01 trial investigators. Radiation doses and fractionation schedules in non-low-risk ductal carcinoma in situ in the breast (BIG 3-07/TROG 07.01): a randomised, factorial, multicentre, open-label, phase 3 study. Lancet. 2022 Aug 6;400(10350):431-440. [CrossRef]
- S Bosma, E van Werkhoven, H Bartelink, A Fourquet, C Hurkmans, J Maduro, E Rutgers, L Scheijmans, D Schinagl, M Stam, et al.: Young boost randomized phase III trial of high vs low boost radiation in young breast cancer patients: 10-years results. EBCC-14; Milano March 22th-24th, 2024. Abstract no: 4LBA. [CrossRef]
- Schmitt M, Menoux I, Chambrelant I, Hild C, Petit T, Mathelin C, Noël G. Adjuvant hypofractionated radiotherapy with simultaneous integrated boost after breast-conserving surgery: A systematic literature review. Transl Oncol. 2022 Aug;22:101456. [CrossRef]
- Coles CE, Haviland JS, Kirby AM, Griffin CL, Sydenham MA, Titley JC, Bhattacharya I, Brunt AM, Chan HYC, Donovan EM, et al.: IMPORT Trial Management Group. Dose-escalated simultaneous integrated boost radiotherapy in early breast cancer (IMPORT HIGH): a multicentre, phase 3, non-inferiority, open-label, randomised controlled trial. Lancet. 2023 Jun 24;401(10394):2124-2137. [CrossRef]
- J Dunst, D Krug, A Schreiber, AD Boicev, J Zimmer, R Laubach, N Weidner, SE Dinges, M Hipp, R Schneider, et al.: Patient Reported Experience with Treatment Modalities and Safety of Adjuvant Breast Radiotherapy - First Results of the Randomized HYPOSIB - Study. Int J Radiat Oncol Biol Phys, Volume 108, Issue 3 Suppl., S13, November 01, 2020. [CrossRef]
- Vicini FA, Winter K, Freedman GM, et al: NRG RTOG 1005: A phase III trial of hypo fractionated whole breast irradiation with concurrent boost vs. Conventional whole breast irradiation plus sequential boost following lumpectomy for high risk early-stage breast cancer. Int J Radiat Oncol Biol Phys 114:S1, 2022 (3 suppl) 194. [CrossRef]
- Garcia Zanuguera C, Gadea Quintero J, Curbelo Artiles AG, Mateu Castell L, Maturana JEM, Ortiz Gonzalez I, Alastuey I, Pardo J. Safety and feasibility of simultaneous integrated boost in extreme 1-week hypofractionated radiotherapy for early breast cancer. Int J Radiat Oncol Biol Phys, Volume 114, Issue 3, Suppl. E28-E29, 2022.
- Chatterjee S, Chakraborty S: Hypofractionated radiation therapy comparing a standard radiotherapy schedule (over 3 weeks) with a novel 1-week schedule in adjuvant breast cancer: An open-label randomized controlled study (HYPORT-Adjuvant)-study protocol for a multicentre, randomized phase III trial. Trials 21:819, 2020.
- Hypofractionated LocoRegional Radiotherapy in Breast Cancer (RHEAL). https://clinicaltrials.gov/study/NCT04228991 (accessed on May 26th, 2024).
- www.targit.org.uk (accessed on May 26th, 2024).
- Vos EL, Siesling S, Baaijens MHA, Verhoef C, Jager A, Voogd AC, Koppert LB: Omitting re-excision for focally positive margins after breast-conserving surgery does not impair disease-free and overall survival. Breast Cancer Res Treat. 2017 Jul;164(1):157-167.
- Budach W, Bölke E, Kammers K, Gerber PA, Nestle-Krämling C, Matuschek C: Adjuvant radiation therapy of regional lymph nodes in breast cancer - a meta-analysis of randomized trials - an update. Radiat Oncol. 2015 Dec 21; 10:258.
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Radiotherapy to regional nodes in early breast cancer: an individual patient data meta-analysis of 14 324 women in 16 trials. Lancet. 2023 Nov 25;402(10416):1991-2003. [CrossRef]
- Haussmann J, Budach W, Tamaskovics B, Bölke E, Corradini S, Djiepmo-Njanang FJ, Kammers K, Matuschek C: Which target volume should be considered when irradiating the regional nodes in breast cancer? Results of a network-meta-analysis. Radiat Oncol. 2019 Jun 11;14(1):102. [CrossRef]
- Kim YB, Byun HK, Kim DY, Ahn SJ, Lee HS, Park W, Kim SS, Kim JH, Lee KC, Lee IJ, et al.: Effect of Elective Internal Mammary Node Irradiation on Disease-Free Survival in Women With Node-Positive Breast Cancer: A Randomized Phase 3 Clinical Trial. JAMA Oncol. 2022 Jan 1;8(1):96-105.
- Kaidar-Person O, Fortpied C, Hol S, Weltens C, Kirkove C, Budach V, Peignaux-Casasnovas K, van der Leij F, Vonk E, Valli M, eta l.: EORTC Radiation Oncology and Breast Cancer Groups. The association of internal mammary and medial supraclavicular lymph node radiation technique with clinical outcomes: Results from the EORTC 22922/10925 randomised trial. Radiother Oncol. 2022 Jul;172:99-110. [CrossRef]
- Giuliano AE, Ballman KV, McCall L, Beitsch PD, Brennan MB, Kelemen PR, Ollila DW, Hansen NM, Whitworth PW, Blumencranz PW, et al.: Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA. 2017 Sep 12;318(10):918-926. [CrossRef] [PubMed] [PubMed Central]
- Bartels SAL, Donker M, Poncet C, Sauvé N, Straver ME, van de Velde CJH, Mansel RE, Blanken C, Orzalesi L, Klinkenbijl JHG, et al.: Radiotherapy or Surgery of the Axilla After a Positive Sentinel Node in Breast Cancer: 10-Year Results of the Randomized Controlled EORTC 10981-22023 AMAROS Trial. J Clin Oncol. 2023 Apr 20;41(12):2159-2165. Epub 2022 Nov 16. [CrossRef] [PubMed]
- Sávolt Á, Péley G, Polgár C, Udvarhelyi N, Rubovszky G, Kovács E, Győrffy B, Kásler M, Mátrai Z. Eight-year follow up result of the OTOASOR trial: The Optimal Treatment Of the Axilla - Surgery Or Radiotherapy after positive sentinel lymph node biopsy in early-stage breast cancer: A randomized, single centre, phase III, non-inferiority trial. Eur J Surg Oncol. 2017 Apr;43(4):672-679. Epub 2017 Jan 16. [CrossRef] [PubMed]
- Haussmann J, Matuschek C, Bölke E, Orth K, Ghadjar P, Budach W: The Role of Local Treatment in Oligometastatic and Oligoprogressive Cancer. Dtsch Arztebl Int. 2019 Dec 13;116(50):849-856.
- Chmura SJ, Winter KA, Woodward WA, Borges VF, Kamel J, et al. NRG-BR002: a phase IIR/III trial of standard of care systemic therapy with or without stereotactic body radiotherapy (SBRT) and/or surgical resection (SR) for newly oligometastatic breast cancer (NCT02364557). Proc Am Soc Clin Oncol. 2022; 40 (abstr).1007. [CrossRef]
- Ng J, Pennell R, Formenti SC. The initial experience of MRI-guided precision prone breast irradiation with daily adaptive planning in treating early stage breast cancer patients. Front Oncol. 2022;12:1048512. [CrossRef]
- Liu X, Li Z, Yin Y. Clinical application of MR-Linac in tumor radiotherapy: a systematic review. Radiat Oncol. 2023;18:52. [CrossRef]
- Matuschek C., Bolke E., Haussmann J., Mohrmann S., Nestle-Kramling C., Gerber P.A., et al. The benefit of adjuvant radiotherapy after breast conserving surgery in older patients with low risk breast cancer- a meta-analysis of randomized trials. Radiat Oncol. 2017;12(1):60. [CrossRef]
- Sjöström M, Chang SL, Fishbane N, Davicioni E, Zhao SG, Hartman L, Holmberg E, Feng FY, Speers CW, Pierce LJ, et al.: Clinicogenomic Radiotherapy Classifier Predicting the Need for Intensified Locoregional Treatment After Breast-Conserving Surgery for Early-Stage Breast Cancer. .J Clin Oncol. 2019 Dec 10;37(35):3340-3349. [CrossRef]
- Whelan TJ, Smith S, Parpia S, Fyles AW, Bane A, Liu FF, Rakovitch E, Chang L, Stevens C, Bowen J, et al.: LUMINA Study Investigators. Omitting Radiotherapy after Breast-Conserving Surgery in Luminal A Breast Cancer. N Engl J Med. 2023 Aug 17;389(7):612-619. [CrossRef]
- Jagsi R, Griffith KA, Harris EE, Wright JL, Recht A, Taghian AG, Lee L, Moran MS, Small W Jr, Johnstone C, et al.: Omission of Radiotherapy After Breast-Conserving Surgery for Women With Breast Cancer With Low Clinical and Genomic Risk: 5-Year Outcomes of IDEA. J Clin Oncol. 2024 Feb 1;42(4):390-398. [CrossRef]
- LZ Braunstein, J Wong, DA Dillon, YH Chen, P Catalano, O Cahlon, MB El-Tamer, R Jimenez, A Khan, C Perez, et al.: Preliminary report of the PRECISION Trial (Profiling Early Breast Cancer for Radiotherapy Omission): A Phase II Study of Breast-Conserving Surgery Without Adjuvant Radiotherapy for Favorable-Risk Breast Cancer [abstract]. In: Proceedings of the 2022 San Antonio Breast Cancer Symposium; 2022 Dec 6-10; San Antonio, TX. Philadelphia (PA): AACR; Cancer Res 2023;83(5 Suppl):Abstract nr OT1-12-02. [CrossRef]
- Kirwan, C.C.; Coles, C.E.; Bliss, J.; Kirwan, C.; Kilburn, L.; Fox, L.; Cheang, M.; Griffin, C.; Francis, A.; Kirby, A.; et al. It’s PRIMETIME. Postoperative Avoidance of Radiotherapy: Biomarker Selection of Women at Very Low Risk of Local Recurrence. Clin. Oncol. 2016, 28, 594–596. [CrossRef]
- Offersen, B.; Al-Rawi, S.; Bechmann, T.; Kamby, C.; Mathiessen, L.; Nielsen, H.; Nielsen, M.; Stenbygaard, L.; Jensen, M.; Alsner, J. The DBCG RT NATURAL trial: Accelerated partial breast irradiation versus no irradiation for early stage breast cancer, a clinically controlled randomized phase III trial. In Proceedings of the Danske Kræftforskningsdage, Odense, Denmark, 30–31 August 2018.
- EXamining PErsonalised Radiation Therapy for Low-risk Early Breast Cancer (EXPERT), NCT02889874. [Internet] https://clinicaltrials.gov/study/NCT02889874. (accessed on May 26th, 2024).
- White JR, Anderson SJ, Harris EE, et al. NRG-BR007: a phase III trial evaluating de-escalation of breast radiation (DEBRA) following breast-conserving surgery (BCS) of stage 1, hormone receptor1, HER2-, RS 18 breast cancer. J Clin Oncol 2022;40(16_suppl). TPS613-TPS613. [Internet] https://clin.larvol.com/abstract-detail/SABCS%202022/60536546.
- Meattini, I.; Poortmans, P.M.P.; Marrazzo, L.; Desideri, I.; Brain, E.; Hamaker, M.; Lambertini, M.; Miccinesi, G.; Russell, N.; Saieva, C.; et al. Exclusive endocrine therapy or partial breast irradiation for women aged ≥70 years with luminal A-like early stage breast cancer (NCT04134598-EUROPA): Proof of concept of a randomized controlled trial comparing health related quality of life by patient reported outcome measures. J. Geriatr. Oncol. 2021, 12, 182–189. [CrossRef]
- Savard MF, Alzahrani MJ, Saunders D, Chang L, Arnaout A, Ng TL, Brackstone M, Vandermeer L, Hsu T, Awan AA, Cole K, Larocque G, Clemons M. Experiences and Perceptions of Older Adults with Lower-Risk Hormone Receptor-Positive Breast Cancer about Adjuvant Radiotherapy and Endocrine Therapy: A Patient Survey. Curr Oncol. 2021 Dec 8;28(6):5215-5226. [CrossRef]
- A Morris, DA Hanes, H Kaplan; Long Term Outcomes of Radiation (RT)-Monotherapy vs. Combined RT + Endocrine Therapy (RT+ET) in Low-Risk Early-Stage Breast Cancer Patients 70 Years or Older after Breast-Conserving Surgery (BCS). Int J Radiat Oncol Biol Phys Volume 117, Issue 2, Suppl., S5-S6; October 01, 2023. [CrossRef]
- Mann GB, Skandarajah AR, Zdenkowski N, Hughes J, Park A, Petrie D, Saxby K, Grimmond SM, Murugasu A, Spillane AJ, et al.: Postoperative radiotherapy omission in selected patients with early breast cancer following preoperative breast MRI (PROSPECT): primary results of a prospective two-arm study. Lancet. 2024 Jan 20;403(10423):261-270. Epub 2023 Dec 5. [CrossRef] [PubMed]
- Jagsi R, Chadha M, Moni J, Ballman K, Laurie F, Buchholz TA, Giuliano A, Haffty BG. Radiation field design in the ACOSOG Z0011 (Alliance) Trial. J Clin Oncol. 2014 Nov 10;32(32):3600-6. Epub 2014 Aug 18. [CrossRef] [PubMed] [PubMed Central]
- Katz MS, McCall L, Ballman K, Jagsi R, Haffty BG, Giuliano AE. Correction to: Nomogram-based estimate of axillary nodal involvement in ACOSOG Z0011 (Alliance): validation and association with radiation protocol variations. Breast Cancer Res Treat. 2021 Feb;185(3):891. doi: 10.1007/s10549-020-05980-0. Erratum for: Breast Cancer Res Treat. 2020 Apr;180(2):429-436. [CrossRef] [PubMed]
- Henke G, Knauer M, Ribi K, Hayoz S, Gérard MA, Ruhstaller T, Zwahlen DR, Muenst S, Ackerknecht M, Hawle H, et al.: Tailored axillary surgery with or without axillary lymph node dissection followed by radiotherapy in patients with clinically node-positive breast cancer (TAXIS): study protocol for a multicenter, randomized phase-III trial. Trials. 2018 Dec 4;19(1):667. [CrossRef] [PubMed] [PubMed Central]
- Algara López M, Rodríguez García E, Beato Tortajada I, Martínez Arcelus FJ, Salinas Ramos J, Rodríguez Garrido JR, Sanz Latiesas X, Soler Rodríguez A, Juan Rijo G, Flaquer García A. OPTimizing Irradiation through Molecular Assessment of Lymph node (OPTIMAL): a randomized open label trial. Radiat Oncol. 2020 Oct 2;15(1):229. [CrossRef] [PubMed] [PubMed Central]
- Tinterri C, Gentile D, Gatzemeier W, Sagona A, Barbieri E, Testori A, Errico V, Bottini A, Marrazzo E, Dani C, et al.: SINODAR-ONE Collaborative Group. Preservation of Axillary Lymph Nodes Compared with Complete Dissection in T1-2 Breast Cancer Patients Presenting One or Two Metastatic Sentinel Lymph Nodes: The SINODAR-ONE Multicenter Randomized Clinical Trial. Ann Surg Oncol. 2022 Sep;29(9):5732-5744. Epub 2022 May 12. [CrossRef] [PubMed]
- de Boniface J, Filtenborg Tvedskov T, Rydén L, Szulkin R, Reimer T, Kuehn T, Kontos M, Gentilini OD, Olofsson Bagge R, Sund M, et al.: SENOMAC Trialists’ Group; SENOMAC Trialists' Group. Omitting Axillary Dissection in Breast Cancer with Sentinel-Node Metastases. N Engl J Med. 2024 Apr 4;390(13):1163-1175. [CrossRef] [PubMed]
- de Wild SR, van Roozendaal LM, de Wilt JHW, van Dalen T, van der Hage JA, van Duijnhoven FH, Simons JM, Schipper RJ, de Munck L, van Kuijk SMJ, et al.: De-escalation of axillary treatment in the event of a positive sentinel lymph node biopsy in cT1-2 N0 breast cancer treated with mastectomy: nationwide registry study (BOOG 2013-07). Br J Surg. 2024 Apr 3;111(4):znae077. [CrossRef] [PubMed] [PubMed Central]
- Alkner S, de Boniface J, Lundstedt D, Mjaaland I, Ryden L, Vikstrom J, Bendahl PO, Holmberg E, Sackey H, Wieslander E, et al.: Protocol for the T-REX-trial: tailored regional external beam radiotherapy in clinically node-negative breast cancer patients with 1-2 sentinel node macrometastases - an open, multicentre, randomised non-inferiority phase 3 trial. BMJ Open. 2023 Sep 26;13(9):e075543. [CrossRef] [PubMed] [PubMed Central]
- Regional Radiotherapy in Biomarker Low-Risk Node Positive and T3N0 Breast Cancer; https://clinicaltrials.goc/study/NCT03488693 (accessed on May 17th, 2024).
- Qi WX, Cao L, Zheng S, Xu C, Cai R, Xu H, Cai G, Chen J. IMNI PRECISION trial protocol: a phase II, open-label, non-inferior randomized controlled trial of tailoring omission of internal mammary node irradiation for early-stage breast cancer. BMC Cancer. 2022 Dec 27;22(1):1356. [CrossRef] [PubMed] [PubMed Central]
- Xie SJ, Wang RJ, Wu SG, Zhang FX. 21-gene recurrence score in predicting the outcome of postoperative radiotherapy in T1-2N1 luminal breast cancer after breast-conserving surgery. Breast. 2024 Apr;74:103679. Epub 2024 Feb 12. [CrossRef] [PubMed] [PubMed Central]
- Krug D, Baumann R, Budach W, Duma MN, Dunst J, Feyer P, Fietkau R, Haase W, Harms W, Hehr T, et al.: Commercially Available Gene Expression Assays as Predictive Tools for Adjuvant Radiotherapy? A Critical Review. Breast Care (Basel). 2020 Apr;15(2):118-126. Epub 2020 Jan 24. [CrossRef] [PubMed] [PubMed Central]
- Gerber B, Schneeweiss A, Möbus V, Golatta M, Tesch H, Krug D, Hanusch C, Denkert C, Lübbe K, Heil J, et al.: Pathological Response in the Breast and Axillary Lymph Nodes after Neoadjuvant Systemic Treatment in Patients with Initially Node-Positive Breast Cancer Correlates with Disease Free Survival: An Exploratory Analysis of the GeparOcto Trial. Cancers (Basel). 2022 Jan 20;14(3):521. [CrossRef] [PubMed] [PubMed Central]
- Montero Á, Ciérvide R, Poortmans P. When Can We Avoid Postmastectomy Radiation Following Primary Systemic Therapy? Curr Oncol Rep. 2019 Oct 29;21(12):95. [CrossRef] [PubMed]
- de Wild SR, de Munck L, Simons JM, Verloop J, van Dalen T, Elkhuizen PHM, et al. De-escalation of radiotherapy after primary chemotherapy in cT1-2N1 breast cancer (RAPCHEM; BOOG 2010-03): 5-year follow-up results of a Dutch, prospective, registry study. Lancet Oncol. 2022;23(9): 1201–1210.
- Boersma L.J., Verloop J., Voogd A.C., Elkhuizen P.H.M., Houben R., van Leeuwen A.E., et al. Radiotherapy after primary CHEMotherapy (RAPCHEM): practice variation in a Dutch registration study (BOOG 2010-03) Radiother Oncol. 2020;145:201–208.
- Goyal, A.; Cramp, S.; Marshall, A.; Wheatley, D.; Hammonds, N.; Puri, S.; Homer, T.; Vale, L.; Butt, R.; Mir, R.; et al. Abstract OT1-04-01: ATNEC: A Multi-Centre, Randomised Trial Investigating Whether Axillary Treatment Can Be Avoided in T1-3N1M0 Breast Cancer Patients with No Residual Cancer in the Lymph Glands after Neoadjuvant Chemotherapy (Clinicaltrials.Gov: Nct04109079). Cancer Res. 2022, 82, OT1-04-01. [CrossRef]
- Mamounas, E.P. GS02-07 Loco-Regional Irradiation in Patients with Biopsy-Proven Axillary Node Involvement at Presentation Who Become Pathologically Node-Negative after Neoadjuvant Chemotherapy: Primary Outcomes of NRG Oncology/NSABP B-51/RTOG 1304. In Proceedings of the 2023 San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 7 December 2023.
- Leon-Ferre R.A., Jonas S.F., Salgado R., Loi S., de Jong V., Carter J.M., Nielsen T.O., Leung S., Riaz N., Chia S., et al.: International Immuno-Oncology Biomarker Working Group. Tumor-Infiltrating Lymphocytes in Triple-Negative Breast Cancer. JAMA. 2024 Apr 2;331(13):1135-1144. [CrossRef] [PubMed] [PubMed Central]
- Chen F, Zhou P, Ren G, Lee EKW, Liu Q, Shen Y, Wang Y, El Helali A, Jin JY, Fu P, et al.: Interpretable deep learning insights: Unveiling the role of 1 Gy volume on lymphopenia after radiotherapy in breast cancer. Radiother Oncol. 2024 May 19;197:110333. Epub ahead of print. [CrossRef] [PubMed]
- NRG-BR008 (“HERO”): A Phase III Randomized Trial Seeking to Optimize Use of Radiotherapy in Patients with Early-Stage, Low Risk, HER2-Positive Breast Cancer (nrgoncology.org) (accessed on June 27th, 2024).

Table 1.
Important prospective studies in Luminal A (-like), ‘low-risk’ patients.
| Trial | Phase 3 | n | Main selection criteria | Therapy | F-up | Recurrence |
|---|---|---|---|---|---|---|
| LUMINA [74] | no | 500 | 55+ yrs; T1N0; R0(1mm) ; G1-2; Ki-67 -13.25% | ET | 5 yrs | at 5 yrs : 2.3% |
| IDEA [75] | no | 200 | 50-69 yrs; T1N0 R0(2mm); Oncotype RS: -18 | ET | minimum 57mo | overall: 4% |
| PRECISION [76] | no | 690 | 50-75 yrs ; T1N0 ; R0 ; G1-2; PAM50 Luminal A | ET | median 27mo | at 2 yrs: 0.3% |
| PRIMETIME [77] | no | 1623 | 60+ yrs; T1N0; R0(1mm); G1-2; IHC4+C | ET | closed 03/22 | n.a. |
| NATURAL [78] | yes | 926 | 60+ yrs; T1N0; R0(2mm); G1-2 | ET vs ET+PBI | accruing | n.a. |
| EXPERT [79] | yes | 1170 | 50+ yrs; T1N0; R0; G1-2; PAM50 ROR-60 | ET vs ET+WBRT | accruing | n.a. |
| DEBRA [80] | yes | 1670 | 50-70 yrs; T1N0; R0; Oncotype RS -18 | ET vs ET+WBRT | accruing | n.a. |
| EUROPA [81] | yes | 926 | 70+ yrs; T1N0; R0; G1-2 (G3 if T1a/b); Ki67 -20% | ET vs RT(PBI/WBRT) | accruing | n.a. (endpoint : 2 yrs-HRQoL) |
Abbreviations: yrs=years; ET=endocrine treatment; PBI= partial breast irradiation only; WBRT= whole breast radiotherapy; mo=months; F-up= follow-up; n.a.= not available; HRQoL= health related quality of life.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



