
Submitted:
03 July 2024
Posted:
03 July 2024
You are already at the latest version
Abstract
Multidrug resistant organisms (MDROs) outbreaks have been steadilyincreasing in Intensive care units (ICUs). Still, healthcare institutions and workers (HCW) reached no unanimity on how and when implementing infection prevention and control (IPC) strategies. We aimed to provide a pragmatic, physician practice-oriented, resume of strategies towards different MRDOs outbreaks in ICU. We performed a narrative review on IPC in ICUs, investigating patient-to-staff ratios, education, isolation, decolonization, screening and hygiene practices, outbreak reporting, cost-effectiveness, reproduction-number(R0), and future perspectives. The most effective IPC strategy remains unknown. Most studies focus on a specific pathogen or disease, making the clinician losing the big picture. IPC strategies proved their cost-effectiveness regardless typology, country, or pathogen. A standardized, universal, pragmatic protocol for HCW education should be elaborated. Likewise, a rapid outbreak recognition tool elaboration (i.e., an easy-to-use mathematical model) would improve early diagnosis and spreading prevention. Further studies are needed to express in favor or against MDROs decolonization. New promising strategies are emerging and need to be tested in the field. The lack of IPC strategies application has made, and still makes ICUs a major MDROs reservoir into the community. In a not-too-distant future genetic engineering and phage therapies could represent a plot-twist in MDROs IPC strategies.
Keywords:
Infection prevention and control
; hospital-acquired infections
; outbreak
; multidrug resistant bacteria
; acinetobacter baumanii
; candida auris
; vre
; kpc
; basic reproduction number
; decolonization
Introduction
Hospital acquired infections (HAI) are a major concern for public health and a major issue in ICU [1]. HAI per definition are infections acquired after hospitalization that manifest themselves 48 hours after admission to the hospital. Most common HAI include ventilator-associated pneumonia (VAP), central line-associated bloodstream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI) [1].
According to WHO Global Report on Infection Prevention and Control (IPC) of 2022, 7% in high-income countries and 15% in low- and middle-income countries (LMICs) of patients acquire at least one HAI during hospitalization [2].
These numbers raise dramatically if we take into consideration only adult ICUs: almost one out of three (30%) hospitalized patients develop a HAI: in fact, almost half of all cases (48.7%) of sepsis with organ dysfunction treated in ICUs are hospital-acquired[2,3] , resulting fatal in 52.3% [3].
These global estimates of HAI frequency are probably downgraded by several factors: the lack of HAI surveillance and outbreak reporting systems, poor adherence to standardized protocols and poor studies quality [2].
The reason for ICU higher percentages grounds only partially to its intrinsic risk factors for infection acquisition (i.e., the use of invasive devices, high severity of acute illness, predisposing underlying conditions, being at age extremities [4]): the lack of infection control is the real killer.
According to WHO, Infection prevention and control (IPC) national programs and operational plans are not available in all countries and, when available, they could be not fully implemented. This is the case of Italy and Romania in Europe; Bolivia, Costa Rica and Honduras in south-central America; India, Nepal, Bhutan, Myanmar, Tagikistan, Turkmenistan, Iraq and Afghanistan in Asia [2]. In Africa, 15 out of 54 states find themselves in this condition [2].
These programs are a key element to put IPC into practice and contrast multidrug resistant organism (MDRO) spreading in- and out-side from the hospital setting.
IPC is based on two different, but complementary approaches: the targeted and the universal. The targeted approach consists in screening and isolation, whose details are usually contained in a bundle.
The aim of this narrative review of literature is to summarize and display the most successful and pragmatic strategies to achieve infection control in ICU outbreaks.
Methodology
This review reports the major risk factors for HAI acquisition identified in ICU setting and proposed strategies in guidelines, WHO recommendations, international institutional statements, outbreaks report in the last 25 years, although not being comprehensive of all literature as a systemic review would do. Every statement and statistics reported in the following section of the paper are referred to adult ICU departments, unless otherwise marked.
The search was conducted on PubMed electronic database and included only peer-reviewed articles. No language restriction was applied. Publications were firstly screened by title, abstract and year of publishing by CF. Afterwards, CF evaluated the full articles in order to assess the eligibility for inclusion, and consequently reviewed by DP, LP and PT. The quality of data and accuracy of description of the proposed strategy, together with the novelty, were considered as the most-weighting factors in selection process.
Outbreaks Genesis
A HAI outbreak could be defined as an increased number of cases of a certain HAI among patients or healthcare personnel superior to the expected number, which is clustered by time and place [5,6,7].
Transmission occurs differently depending on the pathogen, involving environmental, health-care organizational, laboratory and host-dependent factors [4].
Routes of transmission for some of the most common pathogens isolated in ICU [8] are displayed in Table 1. Hematogenous route was not listed as the routinary use of gloves for invasive procedures is commonly adopted and effectively prevents from blood-borne diseases.
Although outbreaks involve a large number of individuals, risk factors for HAI acquisition should be taken into consideration for both type of patient and type of infection.
Risk Factors for Outbreak
Outbreaks generally depart from a non-diagnosed infected or a colonized patient for a transmittable disease [26]. Therefore, the first risk factor is represented by the lack of diagnosis.
A rapid outbreak recognition tool (i.e., an easy-to-use mathematical model) should be proposed to improve early diagnosis and spreading prevention. For example, the identification of [3] cases in 5 days could be an outbreak triggered test as experimented by Elliot et al [27].
Several are the factors that interlude the outbreak genesis both generic and pathogen-specific. All generic risk factors are listed as separate paragraphs in this review, including patients’ colonization (Box.1) [19,28,29] management, and pathogen-specific risk factors as sub-paragraphs or focus.
Among the most underrated, artificial fingernails have been associated with HAIs, such as Serratia marcescens bloodstream infections (BSI) in hemodialysis patients [30] and ESBL-producing Klebsiella pneumoniae and Pseudomonas aeruginosa invasive infections in neonatal ICUs [31].
Notably, a body mass index (BMI) ≥30 and elevated number of hospitalization have also been associated with a major risk of acquiring MRSA [32,33], CRE [34], and VRE [34] colonization.
Intravenous and inhalation drugs use are important risk factor to community-acquisition of MRSA colonization, therefore they have to be screened at admission [32].
Strategies
IPC strategies are multiple and synergic. All variables that are worth considering in the purpose of a successful infection control process are reported below. They include patient-to- nurse ratio (PNR), patient-to-intensivist ratio (PIR), healthcare staff education, isolation types, MRDOs decolonization, hand hygiene, shoe hygiene, screening, environmental cleaning, antimicrobial stewardship program, outbreak reporting, special populations, cost-effectiveness and R0, new experimented strategies, and future perspectives. The quality of evidence and strength of these practices according to the pathogen are listed in ESCMID guidelines for Infection Control 2014 [9]. To our knowledge, no further updates have been published of these guidelines.
- NURSE-TO-PATIENT RATIO
There is solid literature and strong guidelines regarding the patient to nurse ratio (PNR) (Table 2). This ratio should be 1 : 1 or 1 : 2, according to the kind of ICU. Several international organizations have stated that in ICU setting every patient must have immediate access to an ICU specialist nurse, suggesting a PNR of 1:1.
- 2.
- PHYSICIAN/PATIENT RATIO
Currently there is no clear recommendation on the patient to intensivist ratio (PIR) by actual guidelines (Table 3). Five studies have been published on this topic before Jeremy M. Kahn et al. tried in 2023 to give an answer to this question with a multicenter cohort study on 29 ICUs in 10 hospitals in the United States of America [39]. They failed to find an association between a higher intensivist-to-patient ratio and higher mortality.
Neuraz et al. in 2015 were the first to find an association with PIR, namely a two-fold increase in shift-specific mortality among French ICU patients cared for by doctors with > 14 vs < 8 patients [40]. Moreover, Gershengorn HB et al. in 2017 conducted a similar study in United Kingdom, finding a positive association between PIR (patient-to-intensivist ratio) and ICU patients mortality also among British ICU patients [41]. Five years later, Georgshengorn et al. repeated the study on Australian and New Zeland ICUs, but no association with PIR was found [42].
Furthermore, studies conducted on this topic in the USA always failed to find an association between PIR and ICU mortality.
However, as Kerlin MP and Caruso P. stated in their paper and also Kahn et al. pointed out, all the five studies that preceded their one suffer from several methodological limitations [39,43]. For instance, they took into consideration intensivist-to-patient ratios averaged over the length of the entire ICU stay, overlooking that ICU census changes day by day and that could obscure daily variations that could influence outcomes. Moreover, they generally extrapolated intensivist-to-patient ratios from ICU census data, neglecting that intensivists may provide care in multiple ICUs within a single day. Additionally, in all these studies intensivists were in the majority Anesthesiologists/Intensivists, but many other specialists, ranging from 10% to 30% approximately, belonged to different medical specialties.
- 3.
- EDUCATION
Beyond nurse- and physician-to patient rations, HCW education on IPC is what affects the most infectious diseases transmission and relative associated mortality.
Therefore, not only nurses, but all healthcare personnel (physicians, healthcare workers, medical and nursing students, cleaning staff) [48] should undergo an “IPC course” as soon as they are hired by the hospital, just before taking an active part in ward activities [49,50]. Furthermore, a “refresh IPC course” periodically, established by hospital protocols, not inferior to once per year (or per month, according to local epidemiology). The frequency of the “refresh IPC course” should be rapidly implemented in case of an outbreak [51].
IPC courses should provide information on pathogens’ transmission, isolation and hand hygiene instructions, and a practical simulation of the procedures. An initial and final practice test should be performed in order to verify the effectiveness of the course and awareness achieved among the healthcare personnel.
The Cochrane Effective Practice and Organisation of Care (EPOC) group elaborated a seven-items educational model to enhance the uptake of educational contents (Box.2).
Nowadays IPC educational and training programs, when present, differ consistently among WHO countries [53], rarely provided by academic institutions, and frequently practicing IPC physicians are not specialized in infectious disease or clinical microbiology [53]. WHO latest guidelines on core components of IPC programmes [48] (Box.3) suggest a different and targeted training for each of the identified three categories of HCW: IPC specialists, HCW involved in patients care (i.e., nurses, health care assistants), and auxiliary personnel (cleaning, administrative and managerial staff). No standardized, universal, pragmatic education protocol has been elaborated so far, so we reported some of valuable examples (Table 4).
- 4.
- ISOLATION
Isolation of the colonized/infected patient is a key moment for infection control [9]. Without isolation, the others IPC approaches may be not sufficient.
According to ESCMID guidelines of 2014, precautionary isolation for recently-admitted patients in ICU should be always performed in order to avoid the uprise of infection clusters among ICU patients and staff, and further hospital clusters [9]. Isolation should be discontinued only after the negative result of screening procedures (see SCREENING section).
Isolation rooms are preferably single rooms whenever possible. It is mandatory to provide a single room in case of neutropenic patients or specific airborne diseases (measles, varicella virus, tuberculosis) [26].
There are three kinds of isolation: contact isolation, respiratory isolation, or both.
The kind of isolation that should be adopted varies depending on where the pathogen was isolated.
Respiratory Isolation
Respiratory isolation is required every time a respiratory airways samples (rhinopharyngeal swabs, sputum, bronchial airways liquid fluid or aspirate) result positive for a potential air-spreading pathogen for human being [9]. Such pathogens are listed in Table 1.
Two kinds of respiratory isolation room should be available in every ICU [60]:
- A negative-pressure room for patients who resulted to be colonized or infected by potential air-spreading pathogens;
- A positive-pressure for patients who are likely more susceptible of acquiring an infection, such as solid-organ transplanted (SOT) recipients, hematopoietic stem cell transplanted (HSCT) patients, presence of hematological disorders, chronic use of corticosteroids, calcineurin inhibitors, anti-metabolites and other immunosuppressants.
The duration of isolation depends on the possibility of pathogen eradication [9].
Whenever the pathogen is eradicated, the patient can quit the isolation room.
A single isolation room is mandatory in case of some airborne pathogens (tuberculosis, measles, varicella virus) and neutropenic patients [26] .
Contact Isolation
Contact isolation is required every time a skin or rectal samples (swabs) result positive for a potential direct or indirect contact transmitted pathogen for human being, especially MDROs (multi-drug resistant organisms) [26]. That include all resistance acquirable through plasmid transmission, among others ESBL (Extended-Spectrum Beta-lactamase) resistance [26]. Such pathogens were listed in Table 1.
Contact isolation is also required in case of diagnosis of particular diseases known for being transmitted also by contact (i.e., Ebola).
Contact isolation is mandatory for both infected and colonized patients by these organisms [9,26]. CRE rectal colonization could last up to one year [61], while VRE’s for approximately 6 months [62]. MRSA skin colonization has been reported to be in average 9 months [63,64,65], older age is associated with a longer duration of colonization for both MRSA [63] and CRE.
- 5.
- MDROs DECOLONIZATION
Although the eradication of the pathogen could possibly serve to prevent both further transmission and infection development [66], is not currently recommended.
Gram Negative Bacteria (GNB)
There is no recommendation in favor or against routine MDR-GNB decolonization in ICU patients by actual guidelines.
In general patients, ESCMID-EUCIC guidelines do not recommend routine decolonization of 3GCephRE and CRE carriers, though they do not extend this statement to immunocompromised (e.g., ICU, neutropenic or transplanted patients) as only few studies have been conducted on this population. Its effectiveness and long-term side effects are encouraged to be assessed through appropriate RCTs (randomized control trials) [67].
However, several recent studies suggest an increased risk of CRE infection development in CRE colonized ICU patients [68,69,70,71] and satisfactory rates of decolonization effectiveness [72,73].
For CRAB (carbapenem-resistant Acinetobacter baumannii), AGRE (aminoglycoside-resistant Enterobacteriaceae), CoRGNB (colistin-resistant Gram-negative organisms), CRSM (cotrimoxazole-resistant Stenotrophomonas maltophilia), FQRE (fluoroquinolone-resistant Enterobacteriaceae), PDRGNB (pan-drug-resistant Gram-negative organisms), and XDRPA (extremely drug-resistant Pseudomonas aeruginosa) carriers the evidence is still limited and no recommendation have been proposed neither for ICU nor for non-ICU carriers [67].
Gram Positive Bacteria (GPB)
To our knowledge, MRSA decolonization with intranasal mupirocin and chlorhexidine bathing is not explicitly recommended by any guidelines [12], except for those on an orthopedic or cardio- surgery waiting list [74]. Still, there are many evidences that systemic screening followed by decolonization of MRSA in all ICU patients (universal approach), decreases the incidence of MRSA colonization or infection up to 52% [75]. In fact, SHEA/IDSA/APIC guidelines highlight that active surveillance with contact precautions is inferior to universal decolonization in reducing MRSA isolation in adult ICUs [12] (REDUCE MRSA Trial) [76] and universal decolonization with daily CHG bathing plus 5 days of nasal decolonization should be performed in this setting to reduce endemic MRSA clinical cultures [12] (quality of evidence: high). Therefore, endemic status should be assessed. Predictors of decolonization failure, could be the respiratory tract colonization [77], younger age (0-17 years) [66], refugee status [66] and having one or more comorbidities [66], who would possibly need different decolonization strategies.
However, physicians should bear in mind that MRSA colonization is associated with a 4-fold increase in the risk of MRSA infection development [78]. More than 50% of MRSA colonized patients develop the infection in ICU setting [79] and MRSA colonization is also associated to an increase in hospital admission, with further consequent possible transmission and outbreak development [80].
As far as we know, no guidelines have been elaborated on VRE decolonization indications or practice. That was probably due to the scarcity of studies conducted on this topic so far. Some studies on MRSA decolonization, showed that chlorhexidine bathing could be effective in reducing VRE acquisition and infection development too [12]. Cheng et al. obtained VRE decolonization applying a combination of polyethylene glycol for bowel preparation, a five-day course of oral absorbable linezolid and non-absorbable daptomycin to suppress any remaining VRE, and subsequent oral Lactobacillus rhamnosus GG, beyond environmental cleaning and isolation [81]. A non-antibiotic decolonization protocol for both VRE and CRE have been recently proposed by Choi et al. consisting in a 4-items bundle: using a glycerin enema for mechanical evacuation, daily lactobacillus ingestion for restoration of normal gut flora, chlorhexidine bath, and bed sheets and clothing changed every day [82]. Both proposed protocols need to be experimented in further studies to assess their efficacy, but firstly, studies on VRE decolonization benefits should be conducted.
Candida Auris (CA)
According to the Centers for Disease Control and Prevention (CDC), the efficacy of Candida auris decolonization is not known [83]. Chlorhexidine or topical antifungals have been proposed empirically, but evidences are still scares.
Candida auris is nowadays the biggest emergent threat in USA and European ICU as, contrarily to other MRDOs, no antifungal, single or in combination, have shown solid efficacy. Thus, IPC measures are the best available weapon. Beyond ECDC in-hospital hygiene recommendations, contact tracking, single-room contact isolation, surveillance though periodic skin-swab testing of the healthcare personnel, co-hospitalised patients, and cohabitants who came in contact with the C. auris carrier, could result to be effective in tackling C. auris spreading.
- 6.
- HAND HYGIENE
Hand hygiene (HH) is crucial for infection control. According to WHO recommendations, hand hygiene should be performed passing from one patient to another in all settings regardless the presence of an ongoing infection or colonization.
WHO recommendations on HH are based on two rules: the six movements and the five moments of hand hygiene [59].
Healthcare staff cannot exempt itself from knowing these rules and put them into practice as per the strong evidence these practices have shown.
It has been proved that appropriate HH is associated with a reduction of HAI incidence up to 50% [84], including a 50% reduction in MRSA infections.
Although the success rate in preventing HAI development and spreading declared by WHO, a systematic review conducted by Kathryn Ann Lambe and colleagues in 2019 enhanced that mean HH compliance was only 59.6% in adult ICU, ranging from 64.4% of high-income countries to 9.1% of low-income countries. This percentage also varies in consideration to the type of ICU (neonatal 67.0%, pediatric 41.2%, adult 58.2%) and the type of healthcare workers (nurses 43.4%, physicians 32.6%, others 53.8%) [85].
A Brazilian study esteemed that with a 20-second manipulation of a without adhering to contact precautions, there was a 45% possibility that HCW (healthcare worker) hands got contaminated with a CRE. After shaking hands with this HCW, the possibility to get contaminated likewise was of 22% [86]. If the first HCW had used gown and gloves or would have washed his hands, that would have been respectively 10% and 0% [86].
In case of outbreak, it would be useful to implement compliance with direct observations of the “five moments” performed by healthcare workers followed by individualized verbal feedback [51].
- 7.
- SHOE HYGIENE (SH)
Shoe soles represent a potential vector for pathogen transmission [87]. As well as hand-hygiene, HCW shoe bottoms can carry pathogens from an environment to another. Therefore, decontamination in needed when passing from a patient to another, especially when MDRO carrier. Rashid et al. conducted a systematic review looking for an effective decontamination strategy for shoe soles in 2016, but did not succeed. This was also due to the scarcity of data present on this topic. Among mechanical strategies, the use of shoe covers or disposable boots seemed to be the most effective in reducing bacterial load in sanitary setting, while adhesive mats proved to be ineffective [87]. Among chemical strategies, tanks or adhesive mats supplemented with 3-1 benzoisothiazolin or 0.2% benzylkonium were able to reduce bacterial load [87]. Also treating boots with peroxygen disinfectant reduces bacterial load up to 1.4 log10.Boot baths with 6% sodium hypochlorite seems to prevent virus transmission [88].
On a par with HCW shoes, all HCW equipment including badges, stethoscopes, oximeters, ultrasonography probe, but also smartphones, should be disinfected with antiseptics such as chlorhexidine and benzalkonium, although MDR-efflux pump QAC carriers or GNB could be resistant [89].
- 8.
- SCREENING
Key points for MDROs screening are summarized in Box.4.
- Risk-assessment scores
Risk-assessment scores (Table 5) could be applied at admission and recalculated daily in order to foresee the risk of colonization acquisition and/or infection. Hereby, HCW can promptly put into practice the consequential IPC measures.
To our knowledge, no definitive colonization score was elaborated so far for CRAB and CRPA, although Dalben et al. identified some colonization risk factors for their acquisition in ICU: male sex, surgery prior to admission, APACHE II score and colonization pressure in the week before an outcome [90]. Tacconelli et al. identified some others risk factors for CRAB colonization and infection development, such as quinolones use [91]. Meschiari et al. identified as independent risk factors the use of permanent devices, mechanical ventilation, urinary catheters, McCabe score, length of stay, and carbapenem use for CRAB colonization acquisition in ICU setting [92].
- b.
- CRAB screening
Actually, there is no consensus on CRAB active screening strategies [9]. Garnacho-Montero J et al recommend weekly rectal, pharyngeal, and tracheal swabs [105]. Valencia-Martìn et al. found a sensitivity of 96% combining rectal and pharyngeal swabs compared to 78% of rectal swab only [106]. Different values, but same conclusion were drawn by Nutman et al.: 94% sensitivity combining buccal mucosa, skin, and rectal swabs compared to 74% rectal swab only [107]. They also found that the most sensible swab was the buccal mucosa for respiratory culture-positive patients and the skin swab for respiratory-negative patients. Meschiari et al. found that skin samples (100%), followed by the rectal samples (86%) showed the best sensitivity, but due to the waiting period to receive screening test they suggested adopting contact precautions measures to all ICU patients until outbreak end [51].
- c.
- Rectal screening for carbapenem resistant Gram negative bacteria (CR- GNB)
This screening should be performed at ICU admission and repeated at least once a week according to local epidemiology [9,108]. In order to promptly identify CR-GNB rectal colonized or CR-GNB infected patient, an active surveillance system involving the microbiology laboratory and infection control staff should be implemented [109].
- Single-use gloves and gowns wearing during assistance (worn at the moment of entering in the room of the CR-GNB colonized patient and removed at the moment of quitting the patient’s room)
- Gloves and gowns should be used individually for every CR-GNB colonized patient, since the CR-GNB could vary for species and resistance profile
- Gloves and gowns should be changed according to the WHO guidelines in the ‘Five moments’ and ‘six movements’ [59].
- d.
- Skin screening for MRSA
As for rectal screening, the skin screening should be performed at admission and repeated at least weekly in ICU [110]. Other situations in which active screening is encouraged are: preoperatively, upon initiating dialysis, at admission to a particular unit, or upon identifying a potential outbreak [110]. Swab samples should be collected in nostrils, throat, and perineum. Other sites could include be wound, sputum or eyes. [66]
- e.
- Environmental samples surveillance
Environmental samples should be collected according to the CDC Environmental Checklist for Monitoring Terminal Cleaning is order to prevent the spreading of CR-GNB and other dangerous microorganisms, paying particular attention to high-touch surfaces [111](see the Cleaning section).
Environmental samples should be collected with sterile BHI moistened gauze, as normal swabs revealed a low sensitivity for Acinetobacter baumanii (0 to 18%) [51,112].
- f.
- Whole genome sequencing (WGS)
Genomic characterization of CR-GNB could be useful to identify putative transmission chains [113] and to stratify patients [51]. For instance, lately, non-functional adeN was found to be associated with an increased virulence and hyper invasiveness [114]. In Meschiari et al. study [51] only two patients who acquired a CRAB clone with inactivation of adeN survived, probably because of a younger age and better immune status. Their hypothesis was that the inactivation of adeN could have contributed to higher mortality rates of their outbreak, similarly to other studies [115,116,117], despite appropriate therapy with cefiderocol.
- 9.
- ENVIRONMENTAL CLEANING
The room and bed cleaning are essential for IPC in ICU. For this reason, the cleaning should be standardized with a hospital protocol and realized on a routine basis or when a patient is moved or discharged from the room (ie, terminal cleaning). In the protocol, environmental service personnel training, use of checklists, and/or monitoring of ‘high-touch’ contact surfaces with healthcare workers’ hands should be provided [111].
The ICU cleaning encloses both surfaces and air cleaning.
Air Cleaning
Ventilation system, together with an appropriate use of heating and air conditioning are fundamental in preventing the acquisition of HAI. High-efficiency particulate air (HEPA) could be useful for the prevention of fungi infections, including Aspergillus spp [118] . Recently, air purifiers seem to be effective in reducing microbial load in the air and on surfaces in ICU [119], and worth to be included in ICU cleaning routine.
Surfaces Cleaning
The cleaning, including the isolation rooms and the open space areas, should be performed with 10% sodium hypochlorite for environmental surfaces and hydrogen peroxide wipes for all medical devices. This has also proved to be effective against C. auris contamination [120,121].
It should be performed on all surfaces, particularly focused on the most ‘High-touch’ surfaces [111], defined by Kisk Huslage et al. in 2015 as sustaining more than 3 contacts per interaction with the patient [111]. Among the 109 ICU surfaces studied, three were identified as ‘high touch surfaces, namely the bed rail, the bed surface, and the supply cart. These 3 surfaces accounted for 40.2% of the contacts recorded in the ICUs. Considering the medical-surgical floor, the ‘high touch’ surfaces, defined as sustaining more than 1 contacts per interaction, were: the bed rail, the over-bed table, the intravenous pump, and the bed surface (48.6% of all contacts with medical-surgical floors). In the same study, appeared that Bed rails had the highest frequency of contact in both types of healthcare settings, accounting for 7.76 contacts per interaction in the ICUs [111].
Anyway, in order to write the hospital protocol, a local assessment of which are the ‘high-touch’ surfaces should be performed and integrated with above-mentioned data.
Of course, the protocol must take into consideration the concentration and type of pathogens found on the specific environmental surfaces, to address the best kind of disinfection.
Several studies demonstrated that standard cleaning with self-monitoring is insufficient to control the CRAB environmental spread [51,122]. This information becomes more relevant considering that environmental contamination seems to be the most frequent source of CRAB cross-transmission in ICU [51,122,123].
Moreover, Carling PC et al. highlighted that less than 50% of standardized environmental surfaces have been cleaned during the terminal room cleaning [124].
The cleaning process should not only follow the CDC Environmental Checklist for Monitoring Terminal Cleaning guidelines [125], but also put into practice the Meschiari ‘cycling radical cleaning and disinfection’ from ‘five-component bundle’ protocol [51]. Environmental contamination appeared to represent the most frequent source
Recently, “No-touch” cleaning methods have been developed, including UV cleaning, and pressurized hydrogen peroxide. Although being effective, they tend to be not well-tolerated, expensive, and limitedly practical, as they require hours before the room being ready for a new patient [126,127]. This makes the cycling radical cleaning and disinfection method [51] preferable as faster, easy to use and cost-effective.
- 10.
- ANTIMICROBIAL STEWARDSHIP PROGRAM
IPC in ICU setting is the result of a teamwork [128,129,130]and effective communication [131]. Beyond ICU personnel (doctors, nurses, HCWs), four key roles are needed to perform the antimicrobial stewardship: the infectious diseases’ specialist (IDS) [132], the clinical microbiologist [132,133], and the clinical pharmacology specialist [134].
In case no protocol has been elaborated at facility level, the IDS should be consulted [135]:
- Whenever an infectious disease is suspected;
- When the patient presents fever;
- Whenever a new cultural or serological positivity is released by the microbiological laboratory;
- For antimicrobic therapies initiation, monitoring, and discontinuation.
Adherence to IDS recommendations by the treating doctor has been proved to be of paramount importance for disease progression and outcome, also in terms of mortality [136,137].
The timing of specialists’ consultation is essential, and a proactive compared to an event-triggered approach would be preferrable [132]. In this regard, Zwerwer et al. recently managed to develop a machine-learning model able to predict infection-related consultations in ICUs up to eight hours in advance based on electronic health records [132].
The IDS should perform at least the first consultation for every patient at bedside, visiting the patient [138]. The IDS should visit the patient every time an important clinical change is present. According to the number and severity of patients suffering from bacterial, virological or fungine infection, a minimum number of weekly visits should be planned [135].
Although many studies witness the commonly inappropriate prescription of those antibiotics identified as ‘Reserve antibiotics’ in WHO AWaRe antibiotic book [139] worldwide, no exclusivity to IDS prescribers have been established [140].
For hospitals without IDS services, Zimmermann et colleagues are currently conducting a trial with the purpose to identify means to comprehensively and sustainably improve the quality of care of patients with infectious diseases in those settings (trial registration: DRKS00023710) [141].
Antimicrobial stewardship (AMS) remains pivotal and complementary to IPC in fighting antimicrobial resistance.
- 11.
- OUTBREAK REPORTING
Manuscripts on IPC are mainly conducted during outbreaks. The main limitation of this kind of literature is that is scares and frequently different risk factors are taken into consideration from a study to another [4].
Another limitation is that a universal outbreak definition is lacking [26,142]. One of the most accurate definition list for different pathogens’ outbreak is the one offered by the Division of Infectious Disease Epidemiology, West Virginia, USA [5].
The ORION statement (Outbreak Reports and Intervention Studies of Nosocomial Infection statement, 2007) by Sheldon Stone and colleagues proposed a standardized way of reporting an outbreak, that could be useful in prevention and/or management of future outbreaks, other than contributing to current literature [143].
The statement consisted in a 22-items checklist including information on: the number of colonized, infected, and deceased patients; the type of medical department; the number of beds on the ward; performance of genotyping; the study design; and data on costs.
A decade ORION statement publication, outbreak reports globally still did not provide the basic information in the event [142]. After 2017, only a review on CRAB and CRPRA outbreaks mentioned the statement, apparently not using it though for the selection of the outbreak reports, but highlighting the importance of an appropriate reporting [144].
- 12.
- CRE PREVENTION AMONG SPECIAL POPULATIONS
Haematological patients
Among CRE rectal colonized haematological patients, in a recent retrospective study by Xia Chen et al., receiving proton pump inhibitors and admission to ICU (P < 0.05) were identified as risk factors for subsequent CRE infection development [145]. Receiving proton pump inhibitors is recognized to be a predisposing factor to infection also by extended spectrum β-lactamase-producing Enterobacteriaceae. Among this kind of haematological patients, gastrointestinal injury, tigecycline exposure and carbapenem resistance score were not associated with subsequent CRE infection, which may be responsible for subsequent CRE infection in other haematological disorders [146], as well as high-risk disease and mucositis [147].
Neutropenic patients
According to ESCMID-EUCIC guidelines, there are no conclusive evidences on 3GCephRE carriers decolonization benefits in this population. In particular, decolonization of 3GCephRE has been associated to temporary effectiveness and an increased risk of developing ESBL-E BSI in neutropenic colonized patients [67].
For future clinical trials on decolonization by this pathogen, they suggest using the combination of oral colistin sulphate (50 mg (salt) four times daily) and neomycin sulphate (250 mg (salt) four times daily) in severe neutropenic patients [67].
Hemodialysis patients
Patients using a temporary line for vascular access have a greater risk of colonization by MRSA [148].
- 13.
- COST-EFFECTIVENESS AND MDROs REPRODUCTIVE NUMBER (R0)
Cost-effectiveness of IPC strategies implementation, such as screening, laboratory tools, HCW personnel and bed rotations (that require one bed off regular admissions) are to be considered.
In 2022 WHO’s global report the impact and cost-effectiveness of IPC measures was addressed to encourage the improvement of IPC programmes [149].
Multidrug resistant organisms’ and difficult-to-treat infections are associated to prolonged hospitalization with higher costs in terms of human resources, assistance, drugs, disposables, additional cleaning, length of stay, and laboratory. MDROs reproductive number (R0) should be kept in mind when estimating an outbreak cost (Table 7).
CRE
Lin et al. developed a computational model in order to predict the cost-effectiveness of CRE surveillance strategies in ICU [150]. The cost of a single CRE patient was esteemed to be $639,48 based on literature review. Other than reducing CRE colonization acquisition, they found out that up to $572.000/year could have been saved whenever IPC strategies were implemented in Maryland, USA. That, considering Maryland 2012 incidence of 4.8 CRE every 100.000 persons.
Nowadays the rate of CRE has risen exponentially.
A single identification of a CRE infection or colonization could be responsible up to 11 transmission, according to a Brazilian study [151].
In this study, authors developed a mathematical model to describe the dynamics of transmission of CRE in ICU, and they found CRE transmission R₀ (basic reproduction number) to be 11 with the routine IPC before the implementation of the experimented IPC strategies they performed. After IPC implementations, R₀ dropped to 0,41 (range 0-2,1). To our knowledge, this is the only study that was capable of estimating the R₀ of CRE colonized patients.
Recently, many and effective new antibiotics have been discovered against CRE [152], but their costs are still very high.
VRE
Mac et al. proved the same cost-effectiveness of VRE screening and isolation in medicine ward in Canada [153]. The cost of a single VRE patient was esteemed to be $17,949 [154] while a VRE outbreak €60.524 [155] based on literature review. Equally to Lin et al. for CRE, they proved both VRE colonization acquisition and relative mortality reduction at a cost-effectiveness threshold of $50,000/QALY (quality-adjusted life years) in Toronto, Canada. According to current literature, VRE transmission R₀ was 1.32 (range 1.03-1.46) [156].
MRSA
Chaix et al. esteemed the cost of a single MRSA infection in a French ICU to be $9.275, while IPC measures for MRSA would range from $340 to $1480 per patient and $30.225 for the entire outbreak [157,158]. They proved that a routinary screening together with other IPC measures managed to reduce both costs and MRSA incidence, the latest by 14%. According to a recent review, universal decolonization would be more effective and less expensive than other IPC strategies, but the most effective would be a combination of screening, isolation, and decolonization in ICU setting, even though the most expensive one [159]. Eike Steinig and colleagues conducted the first study on community-acquired MRSA R0 , resulting in a range between 0.97 and 1.60 depending on the strain [160].
In summary, IPC measures in ICU have been proved to be cost-effective wherever MRSA colonization and infection rates are significant, although no cut-off rate has been assessed.
CRAB
Literature on carbapenem-resistant Acinetobacter baumanii (CRAB) outbreak costs is more scares. Coyle et al. elaborated a model estimating CRAB single patient cost up to $55,122 for a 13-days length of stay [161], confirmed by Young et al., who reported a real-life data cost of $60,000 in a Korean ICU [162]. Considering a R0 of 1,5 approximately in Australian ICUs, total outbreak cost would be around $1 million [27]. Implementing IPC measures, the threshold would be
C. auris
Taori et al. analysed the cost a Candida auris outbreak in London, UK, estimated to be €1.217.817, 84. The additional length of stay accounted for half of this sum (€69.645,50/month) [163]. The screening cost for C. auris was esteemed to be €269.984 during outbreak (€51.040/month) [163].
Considering this study, a C. auris outbreak exceeds in costs an average CRE outbreak (€1.1 millions) [164] and Clostridium difficile outbreak (€1.222.376) [165], taking into consideration the long-lasting contamination or the need for closing the ICU for a certain period.
Cost-effectiveness of IPC measures in C. auris outbreaks is still to be assessed. Recently, Rosa et al. managed to prove the positive economic impact of the implementation of an in-house PCR (polymerase chain reaction) to screen patients presenting risk factors for C. auris acquisition at admission in Miami hospitals, USA [166]. The saving margin in two-years post-intervention period was between $772.513,10 and $3 730.480,26, based on a deduced incidence of positivity of 3% [166].
As far as we know, none of C. auris studies conducted so far identified C. auris transmission R₀.
Therefore, IPC represent a solid cost-effective solution for CRE, VRE, MRSA and CDI outbreaks and a possibly cost-effective strategy for C. auris outbreaks, as they seem to be capable to prevent these hospitalizations with associated costs.
Reproductive numbers of other pathogens possible responsible for outbreaks in ICU have been reported in Table 8.
- 14.
- NEW EXPERIMENTED STRATEGIES
Beyond HH and isolation precautions, new experimental IPC strategies have been proposed in the last 10 years. These strategies are focused on MDROs outbreaks (Table 9).
Most recent applications include the employment of Artificial Intelligence and Machine Learning, but literature is still scarce on this topic.
One of the most relevant, easy-to-implement, and effective, is the five-items IPC bundle proposed by Meschiari et al. for CRAB outbreaks in ICU (Box.4) [51]. Notably, A. baumannii outstands for its endurance and it could survive on dry surfaces up 5 months [187], de facto facilitating its spreading.
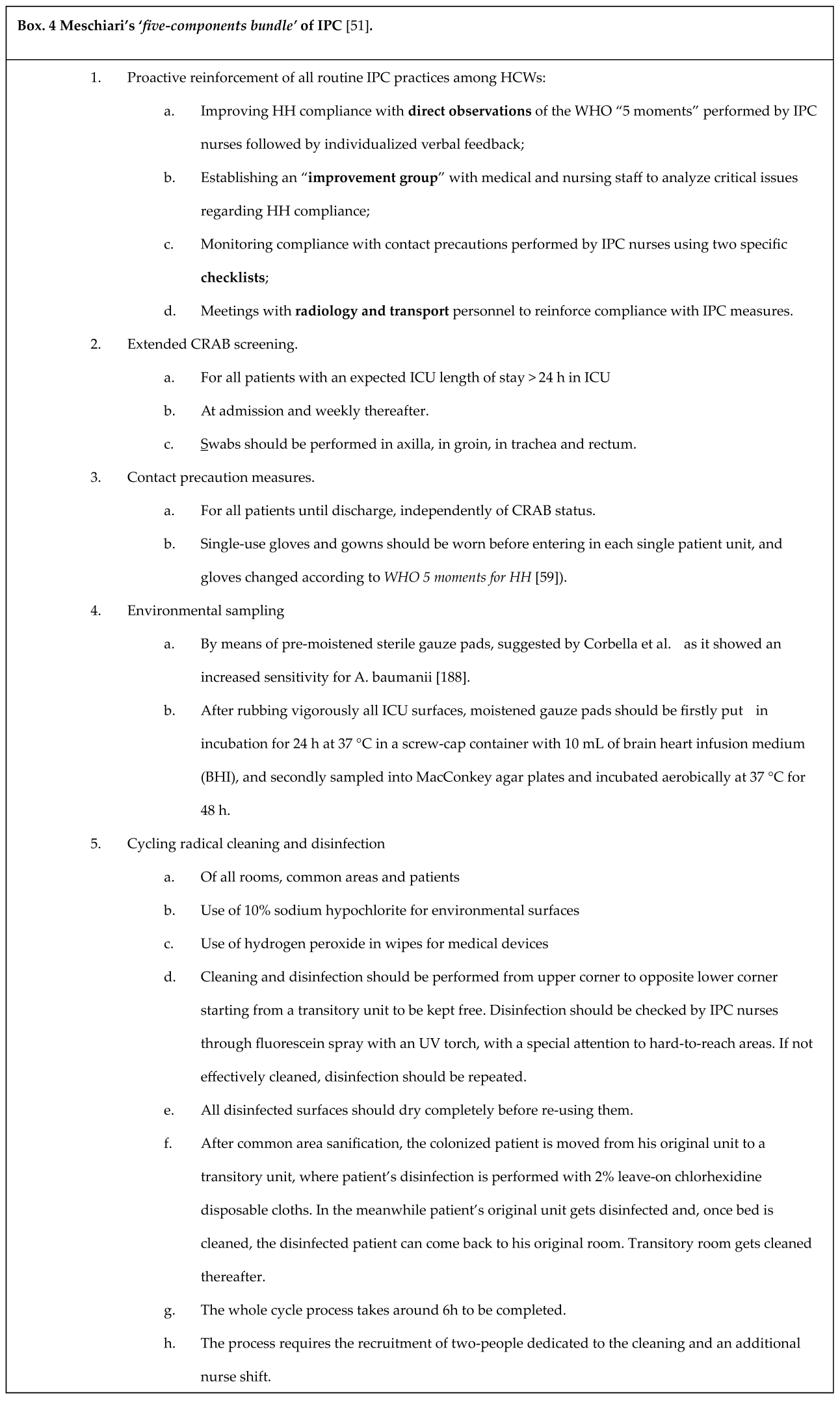
Marianna Meschiari et al. when facing a CRAB outbreak in their ICU, decided to implement and systematize IPC measures, which lead to the elaboration of this successful protocol (Box.4).
While previously existing items n. 2 and n. 3 were intensified and revised (multiple sites vs rectal site for n. 2 and universal vs CRAB-carrier only contact precaution measures for n.3), the items 4 and 5 are novelty in the field. In their study, whole genome sequencing (WGS) analysis was performed for all CRAB isolates, environmental or clinical.
The pitfall of this new method is that it is frequently difficult to create a ‘transitory room’ due to the ICU overcrowding currently affecting many ICU all over the world [189].
Moreover, the whole process takes approximately 6h, that implies the need for supplementary HCWs or, more realistically, healthcare assistant shifts, contributing to work overload [190]. It could be still useful to avoid ICU closure and limiting admissions due to extensive CRAB contamination. It is also applicable to open space ICU, the most affected type of ICU by nosocomial epidemics [191]. After the introduction of the cycling radical cleaning and disinfection in 2018, Modena ICU (Italy) did not experience nosocomial ICU-CRAB outbreaks anymore, but only sporadic cases [51]. Furthermore, ICU alcohol hand rub use increased more than 3 times, and also total antibiotic use dropped in measure of 18,2%, while meropenem and fluoroquinolones of 83,3% and 84% respectively (percentages were calculated based on original article’s data).
- 15.
- FUTURE PERSPECTIVES OF IPC
It has not escaped our notice that IPC strategies could consistently change in the next few years (Table 10). Phage therapy, targeting specific virulence genes and non-antibiotic decolonization strategies seem the most promising ones.
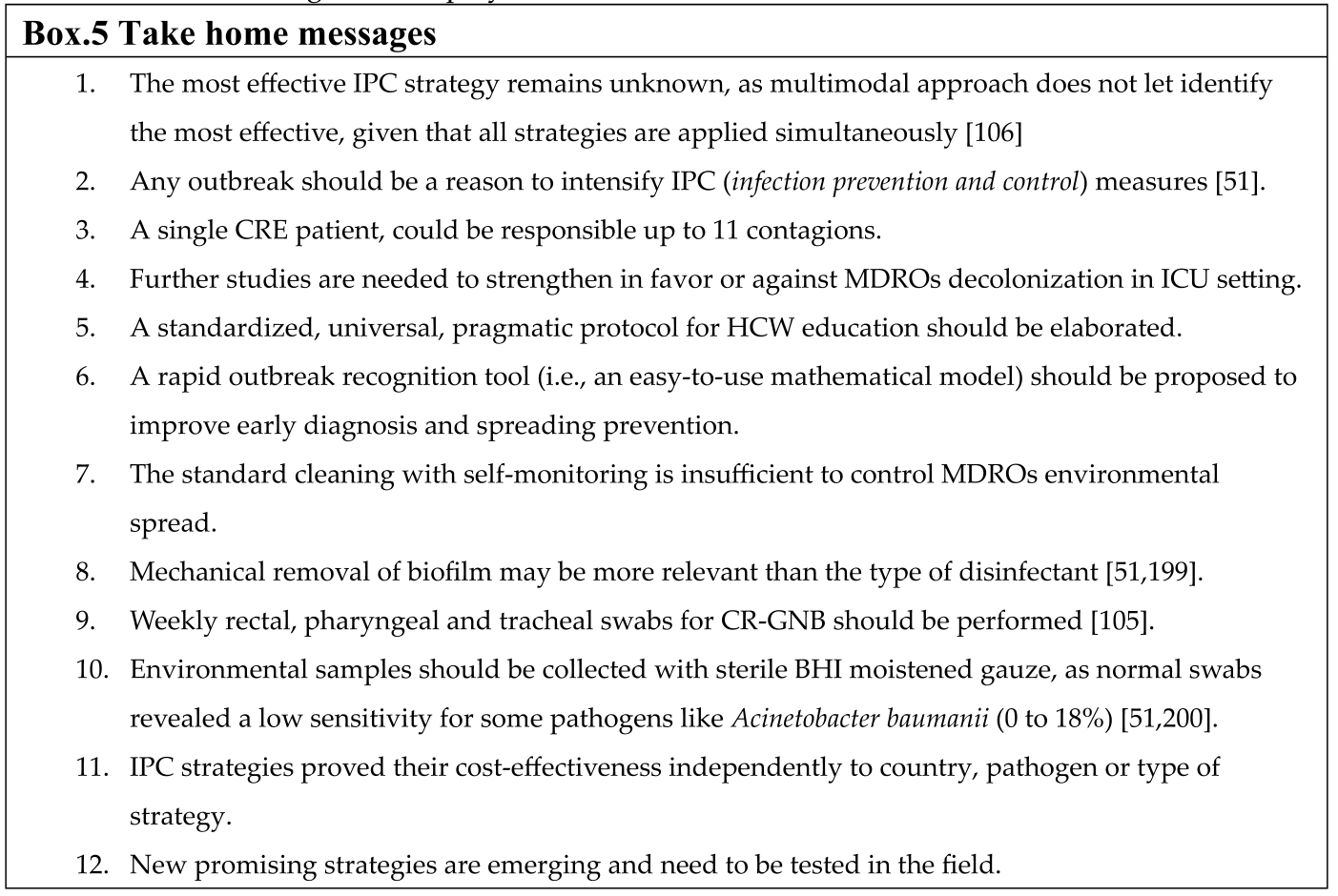
Take-home messages are displayed in Box.5.
Limitations
Limitations of this review include the narrative nature of the study, which lead to the subjectivity in articles and guidelines selection. We decided to mention some of the preventive measure and risk factors among a few special populations to raise physician’s attention towards these categories. A deep focus would require a dedicated, population-based, separate review.
Considering the cost-effective reporting, studies have been conducted in different countries and R0 should have been calculated differently in each setting, therefore these numbers could not be equally applicable to every country or setting.
Conclusions
The lack of IPC strategies or its application, have made and still make hospitals, and ICUs in particular, responsible for an increase of MDROs reservoir into the community [26].
Despite the great number of studies on IPC, it is still difficult to evaluate which is the most effective because of intrinsic study limitations [201].
It would be surely interesting to see if the Meschiari ‘five-bundle protocol’ for CRAB outbreaks, could be applied to other difficult-to-control critical pathogens outbreaks, such as CRE and Candida auris.
A univocal, numeric, and easy to calculate definition of “hospital outbreak” of a certain infective disease is still lacking. This would accelerate the outbreak identification process by healthcare personnel and prompt put in place of IPC strategies. Further studies based on the proposed mathematical model provided by the Brazilian group of Sao Paulo should be encouraged to assess in-hospital-acquired pathogens R₀ [202].
Hopefully, in the future plasmid modifications by genetic engineering would represent a plot-twist in CRE infection control strategies, as well as phage therapies [192].
Author Contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published. Prof. Daniela Pasero suggested the topic of the manuscript and revised the paper. Chiara Fanelli wrote the paper in all its section under the supervision of Prof. Daniela Pasero, Prof. Pierpaolo Terragni, and Laura Pistidda.
Acknowledgements
The authorship credit is based on individual contributions and effort to complete the task.
Conflicts of Interest
All authors have nothing to disclose and declare no conflict of interest. No financial support was received from any organization for the submitted work.
References
- Blot, S.; et al. Healthcare-associated infections in adult intensive care unit patients: Changes in epidemiology, diagnosis, prevention and contributions of new technologies. Intensive Crit Care Nurs 2022, 70, 103227–2022. [Google Scholar] [CrossRef] [PubMed]
- WHO launches first ever global report on infection prevention and control. https://www.who.int/news/item/06-05-2022-who-launches-first-ever-global-report-on-infection-prevention-and-control.
- Markwart, R.; et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med 2020, 46, 1536–1551. [Google Scholar] [CrossRef] [PubMed]
- Zahar - 2018 - Dilemmas in infection control in the intensive car.pdf.
- Bixler, D. Outbreak Investigation. ( 2014.
- World Health Organization. World Health Organization outbreak communication planning guide. Guide de l’OMS sur la planification de la communication lors des flambées de maladies.
- Al-Dorzi, H. M. & Arabi, Y. M. Outbreaks in the adult ICUs. Current Opinion in Infectious Diseases 2017, 30, 432–439. [Google Scholar] [PubMed]
- Jackson, K. C. , Short, C. T., Toman, K. R., Mietchen, M. S. & Lofgren, E. Transient dynamics of infection transmission in a simulated intensive care unit. PLoS One 2022, 17, e0260580. [Google Scholar]
- Tacconelli, E.; et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clinical Microbiology and Infection 2014, 20, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Langford, D. & Williams, V. What does ESBL mean, and why does my patient require contact isolation? Crit Care Nurs Q 2011, 34, 46–51. [Google Scholar]
- Kovacic, A.; et al. Transmission and survival of carbapenem-resistant Acinetobacter baumannii outside hospital setting. International Microbiology. Official journal of the Spanish Society for Microbiology. [CrossRef]
- Popovich, K. J.; et al. SHEA/IDSA/APIC Practice Recommendation: Strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol 2022, 44, 1039–1067. [Google Scholar] [CrossRef] [PubMed]
- Dancer, S. J. Hospital cleaning in the 21st century. Eur J Clin Microbiol Infect Dis 2011, 30, 1473–1481. [Google Scholar] [CrossRef]
- Giovagnorio, F.; et al. Successful control measures to treat the transmission of Candida auris in Northern Italian Hospital. New Microbiol 2024, 46, 395–399. [Google Scholar]
- Luplertlop, N. Pseudallescheria/Scedosporium complex species: From saprobic to pathogenic fungus. Journal de Mycologie Médicale 2018, 28, 249–256. [Google Scholar] [CrossRef]
- Beam, E. L.; et al. Ebola Virus Disease: Clinical Challenges, Recognition, and Management. Nurs Clin North Am 2019, 54, 169–180. [Google Scholar] [CrossRef]
- Kanamori, H. Healthcare-Associated Outbreaks Associated with a Water Reservoir and Infection Prevention Strategies.
- Hoenigl, M.; et al. Global guideline for the diagnosis and management of rare mould infections: an initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology and the American Society for Microbiology. The Lancet Infectious Diseases 2021, 21, e246–e257. [Google Scholar] [PubMed]
- Tacconelli, *!!! REPLACE !!!*; et al. - 2014 - ESCMID guidelines for the management of the infect.pdf.
- Adams, C. E. & Dancer, S. J. Dynamic Transmission of Staphylococcus Aureus in the Intensive Care Unit. Int J Environ Res Public Health 2020, 17, 2109. [Google Scholar] [PubMed]
- Demuyser, T. , De Cock, E. & Sermijn, E. Airborne Aspergillus fumigatus contamination in an intensive care unit: Detection, management and control. J Infect Public Health 2019, 12, 904–906. [Google Scholar] [PubMed]
- Fiore, V.; et al. Mood Reactive Disorders among COVID-19 Inpatients: Experience from a Monocentric Cohort. Med Princ Pract 2021, 30, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Fragkou, P. C. , Moschopoulos, C. D., Karofylakis, E., Kelesidis, T. & Tsiodras, S. Update in Viral Infections in the Intensive Care Unit. Front Med (Lausanne) 2021, 8, 575580–2021. [Google Scholar]
- Shariff, M. , Aditi, A. & Beri, K. Corynebacterium striatum: an emerging respiratory pathogen. J Infect Dev Ctries 2018, 12, 581–586. [Google Scholar]
- Wang, X.; et al. Whole-Genome Sequencing Reveals a Prolonged and Persistent Intrahospital Transmission of Corynebacterium striatum, an Emerging Multidrug-Resistant Pathogen. J Clin Microbiol 2019, 57, e00683–19. [Google Scholar] [CrossRef]
- Zahar, J.-R. Dilemmas in infection control in the intensive care unit. ( 2018. [CrossRef]
- Elliott, T. M.; et al. Cost-effectiveness analysis of whole-genome sequencing during an outbreak of carbapenem-resistant Acinetobacter baumannii. Antimicrob Steward Healthc Epidemiol 2021, 1, e62. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; et al. Predicting the occurrence of multidrug-resistant organism colonization or infection in ICU patients: development and validation of a novel multivariate prediction model. Antimicrob Resist Infect Control 2020, 9, 66. [Google Scholar] [CrossRef] [PubMed]
- Righi, E.; et al. ESCMID/EUCIC clinical practice guidelines on perioperative antibiotic prophylaxis in patients colonized by multidrug-resistant Gram-negative bacteria before surgery. Clinical Microbiology and Infection 2023, 29, 463–479. [Google Scholar] [CrossRef] [PubMed]
- Gordin, F. M.; et al. A cluster of hemodialysis-related bacteremia linked to artificial fingernails. Infect Control Hosp Epidemiol 2007, 28, 743–744. [Google Scholar] [CrossRef]
- Moolenaar, R. L.; et al. A prolonged outbreak of Pseudomonas aeruginosa in a neonatal intensive care unit: did staff fingernails play a role in disease transmission? Infect Control Hosp Epidemiol 2000, 21, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Price, A. M. , Sarween, N., Gupta, I. & Baharani, J. Risk factors and short-term outcomes for methicillin-resistant Staphylococcus aureus and methicillin-sensitive Staphylococcus aureus colonization among hemodialysis patients. Saudi J Kidney Dis Transpl 2019, 30, 1351–1363. [Google Scholar] [PubMed]
- Olsen, K.; et al. Obesity and Staphylococcus aureus nasal colonization among women and men in a general population. PLoS One 2013, 8, e63716. [Google Scholar] [CrossRef]
- Dossett, L. A.; et al. Obesity and site-specific nosocomial infection risk in the intensive care unit. Surg Infect (Larchmt) 2009, 10, 137–142. [Google Scholar] [CrossRef]
- Bray, K.; et al. Standards for nurse staffing in critical care units determined by: The British Association of Critical Care Nurses, The Critical Care Networks National Nurse Leads, Royal College of Nursing Critical Care and In-flight Forum. Nurs Crit Care 2010, 15, 109–111. [Google Scholar] [CrossRef]
- Sharma, S. K. & Rani, R. Nurse-to-patient ratio and nurse staffing norms for hospitals in India: A critical analysis of national benchmarks. J Family Med Prim Care 2020, 9, 2631–2637. [Google Scholar]
- Falk, A.-C. Nurse staffing levels in critical care: The impact of patient characteristics. Nurs Crit Care 2023, 28, 281–287. [Google Scholar] [CrossRef] [PubMed]
- West, E.; et al. Nurse staffing, medical staffing and mortality in Intensive Care: An observational study. Int J Nurs Stud 2014, 51, 781–794. [Google Scholar] [CrossRef] [PubMed]
- Kahn, J. M. , Yabes, J. G., Bukowski, L. A. & Davis, B. S. Intensivist physician-to-patient ratios and mortality in the intensive care unit. Intensive Care Med 2023, 49, 545–553. [Google Scholar] [PubMed]
- Neuraz, A.; et al. Patient Mortality Is Associated With Staff Resources and Workload in the ICU: A Multicenter Observational Study*. Critical Care Medicine 2015, 43, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Gershengorn, H. B.; et al. Association of Intensive Care Unit Patient-to-Intensivist Ratios With Hospital Mortality. JAMA Intern Med 2017, 177, 388. [Google Scholar] [CrossRef] [PubMed]
- Gershengorn, H. B.; et al. Association of patient-to-intensivist ratio with hospital mortality in Australia and New Zealand. Intensive Care Med 2022, 48, 179–189. [Google Scholar] [CrossRef]
- Kerlin, M. P. & Caruso, P. Towards evidence-based staffing: the promise and pitfalls of patient-to-intensivist ratios. Intensive Care Med 2022, 48, 225–226. [Google Scholar] [PubMed]
- Dara, S. I. & Afessa, B. Intensivist-to-Bed Ratio. Chest 2005, 128, 567–572. [Google Scholar] [PubMed]
- Agarwal, A.; et al. SWEAT ICU—An Observational Study of Physician Workload and the Association of Physician Outcomes in Academic ICUs. Crit Care Explor 2022, 4, e0774. [Google Scholar] [CrossRef]
- Kahn, J. M. , Yabes, J. G., Bukowski, L. A. & Davis, B. S. Intensivist physician-to-patient ratios and mortality in the intensive care unit. Intensive Care Med 2023, 49, 545–553. [Google Scholar]
- Estenssoro, E.; et al. Organizational Issues, Structure, and Processes of Care in 257 ICUs in Latin America: A Study From the Latin America Intensive Care Network. Critical Care Medicine 2017, 45, 1325–1336. [Google Scholar] [CrossRef] [PubMed]
- Guidelines on core components of infection prevent.pdf.
- Menegueti, M. G.; et al. Long-term prevention of catheter-associated urinary tract infections among critically ill patients through the implementation of an educational program and a daily checklist for maintenance of indwelling urinary catheters: A quasi-experimental study. Medicine (Baltimore) 2019, 98, e14417. [Google Scholar] [CrossRef] [PubMed]
- Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level. https://www.who.int/publications-detail-redirect/9789241549929.
- Meschiari, M.; et al. A five-component infection control bundle to permanently eliminate a carbapenem-resistant Acinetobacter baumannii spreading in an intensive care unit. Antimicrob Resist Infect Control 2021, 10, 123. [Google Scholar] [CrossRef] [PubMed]
- Flodgren, G.; et al. Tools developed and disseminated by guideline producers to promote the uptake of their guidelines. Cochrane Database Syst Rev 2016, 2016, CD010669. [Google Scholar] [CrossRef] [PubMed]
- Moghnieh, R.; et al. Mapping of infection prevention and control education and training in some countries of the World Health Organization’s Eastern Mediterranean Region: current situation and future needs. Antimicrobial Resistance & Infection Control 2023, 12, 90. [Google Scholar]
- McNett, M.; et al. A Scoping Review of Implementation Science in Adult Critical Care Settings. Crit Care Explor 2020, 2, e0301. [Google Scholar] [CrossRef] [PubMed]
- Barbash, I. J. , Pike, F., Gunn, S. R., Seymour, C. W. & Kahn, J. M. Effects of Physician-targeted Pay for Performance on Use of Spontaneous Breathing Trials in Mechanically Ventilated Patients. Am J Respir Crit Care Med 2017, 196, 56–63. [Google Scholar] [PubMed]
- Mogyoródi, B.; et al. Effect of an educational intervention on compliance with care bundle items to prevent ventilator-associated pneumonia. Intensive and Critical Care Nursing 2023, 75, 103342. [Google Scholar] [CrossRef] [PubMed]
- Phan, H. T.; et al. An educational intervention to improve hand hygiene compliance in Vietnam. BMC Infect Dis 2018, 18, 116. [Google Scholar] [CrossRef]
- your-5-moments-for-hand-hygiene-poster.pdf.
- World Health Organization & WHO Patient Safety. WHO guidelines on hand hygiene in health care. 262 ( 2009.
- Verderber, S. , Gray, S., Suresh-Kumar, S., Kercz, D. & Parshuram, C. Intensive Care Unit Built Environments: A Comprehensive Literature Review (2005–2020). HERD 2021, 14, 368–415. [Google Scholar]
- Mo, Y.; et al. Duration of Carbapenemase-Producing Enterobacteriaceae Carriage in Hospital Patients. Emerg Infect Dis 2020, 26, 2182–2185. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, E. S. , Paras, M. L., Noubary, F., Walensky, R. P. & Hooper, D. C. Natural history of colonization with methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE): a systematic review. BMC Infect Dis 2014, 14, 177. [Google Scholar]
- Scanvic, A.; et al. Duration of colonization by methicillin-resistant Staphylococcus aureus after hospital discharge and risk factors for prolonged carriage. Clin Infect Dis 2001, 32, 1393–1398. [Google Scholar] [CrossRef]
- Sanford, M. D. , Widmer, A. F., Bale, M. J., Jones, R. N. & Wenzel, R. P. Efficient detection and long-term persistence of the carriage of methicillin-resistant Staphylococcus aureus. Clin Infect Dis 1994, 19, 1123–1128. [Google Scholar] [PubMed]
- Larsson, A.-K.; et al. Duration of methicillin-resistant Staphylococcus aureus colonization after diagnosis: a four-year experience from southern Sweden. Scand J Infect Dis 2011, 43, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Yiek, W.-K.; et al. Success rates of MRSA decolonization and factors associated with failure. Antimicrobial Resistance & Infection Control 2022, 11, 143. [Google Scholar]
- Tacconelli, E.; et al. ESCMID-EUCIC clinical guidelines on decolonization of multidrug-resistant Gram-negative bacteria carriers. Clinical Microbiology and Infection 2019, 25, 807–817. [Google Scholar] [CrossRef]
- Debby, B. D.; et al. Epidemiology of carbapenem resistant Klebsiella pneumoniae colonization in an intensive care unit. Eur J Clin Microbiol Infect Dis 2012, 31, 1811–1817. [Google Scholar] [CrossRef]
- Papadimitriou-Olivgeris, M.; et al. KPC-producing Klebsiella pneumoniae enteric colonization acquired during intensive care unit stay: the significance of risk factors for its development and its impact on mortality. Diagn Microbiol Infect Dis 2013, 77, 169–173. [Google Scholar] [CrossRef]
- Pisney, L. M. , Barron, M. A., Kassner, E., Havens, D. & Madinger, N. E. Carbapenem-resistant Enterobacteriaceae rectal screening during an outbreak of New Delhi metallo-β-lactamase-producing Klebsiella pneumoniae at an acute care hospital. Infect Control Hosp Epidemiol 2014, 35, 434–436. [Google Scholar] [PubMed]
- Dickstein, Y.; et al. Carbapenem-resistant Enterobacteriaceae colonization and infection in critically ill patients: a retrospective matched cohort comparison with non-carriers. J Hosp Infect 2016, 94, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Saidel-Odes, L.; et al. A randomized, double-blind, placebo-controlled trial of selective digestive decontamination using oral gentamicin and oral polymyxin E for eradication of carbapenem-resistant Klebsiella pneumoniae carriage. Infect Control Hosp Epidemiol 2012, 33, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Oren, I.; et al. Eradication of carbapenem-resistant Enterobacteriaceae gastrointestinal colonization with nonabsorbable oral antibiotic treatment: A prospective controlled trial. Am J Infect Control 2013, 41, 1167–1172. [Google Scholar] [CrossRef] [PubMed]
- Smith, M. & Herwaldt, L. Nasal decolonization: What antimicrobials and antiseptics are most effective before surgery and in the ICU. Am J Infect Control 2023, 51, A64–A71. [Google Scholar] [PubMed]
- Ridenour, G.; et al. Selective use of intranasal mupirocin and chlorhexidine bathing and the incidence of methicillin-resistant Staphylococcus aureus colonization and infection among intensive care unit patients. Infect Control Hosp Epidemiol 2007, 28, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Huang, S. S.; et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med 2013, 368, 2255–2265. [Google Scholar] [CrossRef]
- Kohler, P. , Bregenzer-Witteck, A., Rettenmund, G., Otterbech, S. & Schlegel, M. MRSA decolonization: success rate, risk factors for failure and optimal duration of follow-up. Infection 2013, 41, 33–40. [Google Scholar]
- Safdar, N. & Bradley, E. A. The Risk of Infection after Nasal Colonization with Staphylococcus Aureus. The American Journal of Medicine 2008, 121, 310–315. [Google Scholar]
- Samuel, P.; et al. Methicillin-Resistant Staphylococcus aureus Colonization in Intensive Care and Burn Units: A Narrative Review. Cureus 2023, 15, e47139. [Google Scholar]
- Olsen, K.; et al. Obesity and Staphylococcus aureus nasal colonization among women and men in a general population. PLoS One 2013, 8, e63716. [Google Scholar]
- Cheng, V. C.; et al. Decolonization of gastrointestinal carriage of vancomycin-resistant Enterococcus faecium: case series and review of literature. BMC Infect Dis 2014, 14, 514. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.; et al. Comprehensive, multisystem, mechanical decolonization of Vancomycin-Resistant Enterococcus and Carbapenem-Resistant Enterobacteriacease without the use of antibiotics. Medicine (Baltimore) 2021, 100, e23686. [Google Scholar] [CrossRef] [PubMed]
- Healthcare Professionals FAQ | Candida auris | Fungal Diseases | CDC. https://www.cdc.gov/fungal/candida-auris/c-auris-health-qa.html (2023).
- Key facts and figures. https://www.who.int/campaigns/world-hand-hygiene-day/2021/key-facts-and-figures.
- Lambe, K. A.; et al. Hand Hygiene Compliance in the ICU: A Systematic Review. Crit Care Med 2019, 47, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- DalBen, M. D. F.; et al. A Model-Based Strategy to Control the Spread of Carbapenem-Resistant Enterobacteriaceae: Simulate and Implement. Infect. Control Hosp. Epidemiol. 2016, 37, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Rashid, T. , VonVille, H. M., Hasan, I. & Garey, K. W. Shoe soles as a potential vector for pathogen transmission: a systematic review. J Appl Microbiol 2016, 121, 1223–1231. [Google Scholar] [PubMed]
- Dee, S. , Deen, J. & Pijoan, C. Evaluation of 4 intervention strategies to prevent the mechanical transmission of porcine reproductive and respiratory syndrome virus. Can J Vet Res 2004, 68, 19–26. [Google Scholar] [PubMed]
- Funk, C. R.; et al. Passenger pathogens on physicians. American Journal of Infection Control 2023, 51, 807–811. [Google Scholar] [CrossRef]
- DalBen, M. F.; et al. Colonization pressure as a risk factor for colonization by multiresistant Acinetobacter spp and carbapenem-resistant Pseudomonas aeruginosa in an intensive care unit. Clinics (Sao Paulo) 2013, 68, 1128–1133. [Google Scholar] [CrossRef]
- Tacconelli, E.; et al. Prediction models to identify hospitalized patients at risk of being colonized or infected with multidrug-resistant Acinetobacter baumannii calcoaceticus complex. Journal of Antimicrobial Chemotherapy 2008, 62, 1130–1137. [Google Scholar] [CrossRef]
- Meschiari, M.; et al. Risk factors for nosocomial rectal colonization with carbapenem-resistant Acinetobacter baumannii in hospital: a matched case–control study. Antimicrob Resist Infect Control 2021, 10, 69. [Google Scholar] [CrossRef]
- Logan, C. , Martin-Loeches, I. & Bicanic, T. Invasive candidiasis in critical care: challenges and future directions. Intensive Care Med 2020, 46, 2001–2014. [Google Scholar]
- Pittet, D. , Monod, M., Suter, P. M., Frenk, E. & Auckenthaler, R. Candida colonization and subsequent infections in critically ill surgical patients. Ann Surg 1994, 220, 751–758. [Google Scholar] [PubMed]
- León, C.; et al. A bedside scoring system (‘Candida score’) for early antifungal treatment in nonneutropenic critically ill patients with Candida colonization. Crit Care Med 2006, 34, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Ostrosky-Zeichner, L.; et al. Improvement of a clinical prediction rule for clinical trials on prophylaxis for invasive candidiasis in the intensive care unit: Prediction rule for Candida in ICU. Mycoses 2011, 54, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; et al. Identifying Patients Harboring Extended-Spectrum-β-Lactamase-Producing Enterobacteriaceae on Hospital Admission: Derivation and Validation of a Scoring System ▿. Antimicrob Agents Chemother 2011, 55, 3485–3490. [Google Scholar] [CrossRef] [PubMed]
- Augustine, M. R.; et al. Clinical Risk Score for Prediction of Extended-Spectrum β-Lactamase–Producing Enterobacteriaceae in Bloodstream Isolates. Infect. Control Hosp. Epidemiol. 2017, 38, 266–272. [Google Scholar] [CrossRef]
- Papafotiou, C.; et al. Predictive score for patients with carbapenemase-producing enterobacterales colonization upon admission in a tertiary care hospital in an endemic area. Journal of Antimicrobial Chemotherapy 2022, 77, 3331–3339. [Google Scholar] [CrossRef]
- Cogliati Dezza, F.; et al. Risk factors for carbapenem-resistant Acinetobacter baumannii (CRAB) bloodstream infections and related mortality in critically ill patients with CRAB colonization. JAC Antimicrob Resist 2023, 5, dlad096. [Google Scholar] [CrossRef]
- Cosentino, F. , Viale, P. & Giannella, M. MDR/XDR/PDR or DTR? Which definition best fits the resistance profile of Pseudomonas aeruginosa? Curr Opin Infect Dis 2023, 36, 564–571. [Google Scholar]
- Torres, K. & Sampathkumar, P. Predictors of methicillin-resistant Staphylococcus aureus colonization at hospital admission. American Journal of Infection Control 2013, 41, 1043–1047. [Google Scholar] [PubMed]
- Boeing, C.; et al. Development and Validation of a Tool for the Prediction of Vancomycin-Resistant Enterococci Colonization Persistence—the PREVENT Score. Microbiol Spectr.
- Hur, E. Y. , Jin, Y. J., Jin, T. X. & Lee, S. M. Development and evaluation of the automated risk assessment system for multidrug-resistant organisms (autoRAS-MDRO). Journal of Hospital Infection 2018, 98, 202–211. [Google Scholar] [PubMed]
- Garnacho-Montero, J.; et al. Task force on management and prevention of Acinetobacter baumannii infections in the ICU. Intensive Care Med 2015, 41, 2057–2075. [Google Scholar] [CrossRef] [PubMed]
- Valencia-Martín, R.; et al. A multimodal intervention program to control a long-term Acinetobacter baumannii endemic in a tertiary care hospital. Antimicrob Resist Infect Control 2019, 8, 199. [Google Scholar] [CrossRef] [PubMed]
- Nutman, A. , Lerner, A., Schwartz, D. & Carmeli, Y. Evaluation of carriage and environmental contamination by carbapenem-resistant Acinetobacter baumannii. Clin Microbiol Infect 2016, 22, 949–e5. [Google Scholar]
- World Health Organization. Guidelines for the Prevention and Control of Carbapenem-Resistant Enterobacteriaceae, Acinetobacter Baumannii and Pseudomonas Aeruginosa in Health Care Facilities. (World Health Organization, Geneva, 2017).
- Magiorakos, A. P.; et al. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: guidance from the European Centre for Disease Prevention and Control. Antimicrobial Resistance & Infection Control 2017, 6, 113. [Google Scholar]
- Popovich, K. J.; et al. SHEA/IDSA/APIC Practice Recommendation: Strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol 2022, 44, 1039–1067. [Google Scholar] [CrossRef] [PubMed]
- Huslage, K. , Rutala, W. A., Sickbert-Bennett, E. & Weber, D. J. A quantitative approach to defining ‘high-touch’ surfaces in hospitals. Infect Control Hosp Epidemiol 2010, 31, 850–853. [Google Scholar] [PubMed]
- Enfield, K. B.; et al. Control of simultaneous outbreaks of carbapenemase-producing enterobacteriaceae and extensively drug-resistant Acinetobacter baumannii infection in an intensive care unit using interventions promoted in the Centers for Disease Control and Prevention 2012 carbapenemase-resistant Enterobacteriaceae Toolkit. Infect Control Hosp Epidemiol 2014, 35, 810–817. [Google Scholar]
- Mangioni, D.; et al. Genomic Characterization of Carbapenem-Resistant Acinetobacter baumannii (CRAB) in Mechanically Ventilated COVID-19 Patients and Impact of Infection Control Measures on Reducing CRAB Circulation during the Second Wave of the SARS-CoV-2 Pandemic in Milan, Italy. Microbiol Spectr 2023, 11, e0020923. [Google Scholar]
- Bogaty, C.; et al. Investigation of a Carbapenemase-producing Acinetobacter baumannii outbreak using whole genome sequencing versus a standard epidemiologic investigation. Antimicrob Resist Infect Control 2018, 7, 140. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S. , Gikas, A., Astrinaki, E. & Kritsotakis, E. I. Excess mortality due to pandrug-resistant Acinetobacter baumannii infections in hospitalized patients. J Hosp Infect 2020, 106, 447–453. [Google Scholar] [PubMed]
- Dickstein, Y.; et al. Treatment Outcomes of Colistin- and Carbapenem-resistant Acinetobacter baumannii Infections: An Exploratory Subgroup Analysis of a Randomized Clinical Trial. Clin Infect Dis 2019, 69, 769–776. [Google Scholar] [CrossRef]
- Jones, C. L.; et al. Fatal outbreak of an emerging clone of extensively drug-resistant Acinetobacter baumannii with enhanced virulence. Clin Infect Dis 2015, 61, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Influence of High-Efficiency Particulate Air Filtr.pdf.
- Arıkan, I.; et al. Effectiveness of air purifiers in intensive care units: an intervention study. J Hosp Infect 2022, 120, 14–22. [Google Scholar] [CrossRef]
- Rapti, V. , Iliopoulou, K. & Poulakou, G. The Gordian Knot of C. auris: If You Cannot Cut It, Prevent It. Pathogens 2023, 12, 1444. [Google Scholar] [PubMed]
- Cadnum, J. L.; et al. Effectiveness of Disinfectants Against Candida auris and Other Candida Species. Infect Control Hosp Epidemiol 2017, 38, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A. O. , Abu-Hanna, J., Carmeli, Y. & Schechner, V. Environmental contamination by carbapenem-resistant Acinetobacter baumannii: The effects of room type and cleaning methods. Infect Control Hosp Epidemiol 2020, 41, 166–171. [Google Scholar] [PubMed]
- Nutman, A. , Lerner, A., Schwartz, D. & Carmeli, Y. Evaluation of carriage and environmental contamination by carbapenem-resistant Acinetobacter baumannii. Clinical Microbiology and Infection 2016, 22, 949–e5. [Google Scholar]
- Carling, P. C.; et al. Improving cleaning of the environment surrounding patients in 36 acute care hospitals. Infect Control Hosp Epidemiol 2008, 29, 1035–1041. [Google Scholar] [CrossRef]
- CDC Environmental Checklist for Monitoring Terminal Cleaning.
- Gray, A. P.; et al. Management of a hospital outbreak of extensively drug-resistant Acinetobacter baumannii using a multimodal intervention including daily chlorhexidine baths. J Hosp Infect 2016, 93, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Molter, G.; et al. Outbreak of carbapenem-resistant Acinetobacter baumannii in the intensive care unit: a multi-level strategic management approach. J Hosp Infect 2016, 92, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Cornistein, W.; et al. Synergy between infection control and antimicrobial stewardship programs to control carbapenem-resistant Enterobacterales. Antimicrob Steward Healthc Epidemiol 2023, 3, e162. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J. P. , Johansson, A. C., Schonberg, M. A. & Howell, M. D. Elements of a High-Quality Inpatient Consultation in the Intensive Care Unit. A Qualitative Study. Annals ATS 2013, 10, 220–227. [Google Scholar]
- Vazquez Guillamet, M. C.; et al. Antimicrobial stewardship for sepsis in the intensive care unit: Survey of critical care and infectious diseases physicians. Infect Control Hosp Epidemiol, 1374. [Google Scholar]
- Bonaconsa, C.; et al. Optimizing infection control and antimicrobial stewardship bedside discussion: a scoping review of existing evidence on effective healthcare communication in hospitals. Clin Microbiol Infect 2024, 30, 336–352. [Google Scholar] [CrossRef] [PubMed]
- Zwerwer, L. R.; et al. Identifying the need for infection-related consultations in intensive care patients using machine learning models. Sci Rep 2024, 14, 2317. [Google Scholar] [CrossRef] [PubMed]
- Kampmeier, S. , Correa-Martinez, C. L., Peters, G., Mellmann, A. & Kahl, B. C. Personal microbiological consultations improve the therapeutic management of Staphylococcus aureus bacteremia. J Infect 2018, 77, 349–356. [Google Scholar]
- Lazure, P.; et al. Gaps and barriers in the implementation and functioning of antimicrobial stewardship programmes: results from an educational and behavioural mixed methods needs assessment in France, the United States, Mexico and India. JAC Antimicrob Resist 2022, 4, dlac094. [Google Scholar] [CrossRef]
- Raineri, E.; et al. Role of the infectious diseases specialist consultant on the appropriateness of antimicrobial therapy prescription in an intensive care unit. Am J Infect Control 2008, 36, 283–290. [Google Scholar] [CrossRef]
- Botelho-Nevers, E.; et al. Dramatic reduction in infective endocarditis-related mortality with a management-based approach. Arch Intern Med 2009, 169, 1290–1298. [Google Scholar] [CrossRef]
- Sellier, E.; et al. Factors and outcomes associated with physicians’ adherence to recommendations of infectious disease consultations for inpatients. J Antimicrob Chemother 2010, 65, 156–162. [Google Scholar] [CrossRef]
- Forsblom, E. , Ruotsalainen, E., Ollgren, J. & Järvinen, A. Telephone consultation cannot replace bedside infectious disease consultation in the management of Staphylococcus aureus Bacteremia. Clin Infect Dis 2013, 56, 527–535. [Google Scholar]
- WHO AWaRe antibiotic book.pdf.
- Seah, V. X. F.; et al. Impact of a Carbapenem Antimicrobial Stewardship Program on Patient Outcomes. Antimicrob Agents Chemother 2017, 61, e00736–17. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, N.; et al. Antimicrobial Stewardship with and without Infectious Diseases Specialist Services to Improve Quality-of-Care in Secondary and Tertiary Care Hospitals in Germany: Study Protocol of the ID ROLL OUT Study. Infect Dis Ther 2022, 11, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Wieland, K. , Chhatwal, P. & Vonberg, R.-P. Outbreak reporting a decade after ORION: where do we stand? The Lancet Infectious Diseases 2017, 17, 476. [Google Scholar] [PubMed]
- Stone, S. P.; et al. The ORION statement: guidelines for transparent reporting of outbreak reports and intervention studies of nosocomial infection. Lancet Infect Dis 2007, 7, 282–288. [Google Scholar] [CrossRef]
- Wieland, K. , Chhatwal, P. & Vonberg, R.-P. Nosocomial outbreaks caused by Acinetobacter baumannii and Pseudomonas aeruginosa: Results of a systematic review. American Journal of Infection Control 2018, 46, 643–648. [Google Scholar] [PubMed]
- Chen, X. , Wen, X., Jiang, Z. & Yan, Q. Prevalence and factors associated with carbapenem-resistant Enterobacterales (CRE) infection among hematological malignancies patients with CRE intestinal colonization. Ann Clin Microbiol Antimicrob 2023, 22, 3. [Google Scholar]
- Ferreira, A. M.; et al. Epidemiology, risk factors and outcomes of multi-drug-resistant bloodstream infections in haematopoietic stem cell transplant recipients: importance of previous gut colonization. J Hosp Infect 2018, 100, 83–91. [Google Scholar] [CrossRef]
- Zhang, L.; et al. Carbapenem-resistant Enterobacteriaceae in hematological patients: Outcome of patients with Carbapenem-resistant Enterobacteriaceae infection and risk factors for progression to infection after rectal colonization. Int J Antimicrob Agents 2019, 54, 527–529. [Google Scholar] [CrossRef]
- Price, A. M. , Sarween, N., Gupta, I. & Baharani, J. Risk factors and short-term outcomes for methicillin-resistant Staphylococcus aureus and methicillin-sensitive Staphylococcus aureus colonization among hemodialysis patients. Saudi J Kidney Dis Transpl 2019, 30, 1351–1363. [Google Scholar] [PubMed]
- WHO launches first ever global report on infection.pdf.
- Lin, G.; et al. Cost-effectiveness of carbapenem-resistant Enterobacteriaceae (CRE) surveillance in Maryland. Infect Control Hosp Epidemiol 2022, 43, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- DalBen, M. de F. et al. A Model-Based Strategy to Control the Spread of Carbapenem-Resistant Enterobacteriaceae: Simulate and Implement. Infect Control Hosp Epidemiol 2016, 37, 1315–1322. [Google Scholar]
- Giacobbe, D. R.; et al. Mortality in KPC-producing Klebsiella pneumoniae bloodstream infections: a changing landscape. J Antimicrob Chemother 2023, 78, 2505–2514. [Google Scholar] [CrossRef] [PubMed]
- Mac, S. , Fitzpatrick, T., Johnstone, J. & Sander, B. Vancomycin-resistant enterococci (VRE) screening and isolation in the general medicine ward: a cost-effectiveness analysis. Antimicrob Resist Infect Control 2019, 8, 168. [Google Scholar]
- Lloyd-Smith, P.; et al. Economic analysis of vancomycin-resistant enterococci at a Canadian hospital: assessing attributable cost and length of stay. J Hosp Infect 2013, 85, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Vancomycin-Resistant Enterococci Isolation and Screening Strategies: Clinical Evidence and Cost-Effectiveness.
- Satilmis, L. , Vanhems, P. & Bénet, T. Outbreaks of Vancomycin-Resistant Enterococci in Hospital Settings: A Systematic Review and Calculation of the Basic Reproductive Number. Infection Control & Hospital Epidemiology 2016, 37, 289–294. [Google Scholar]
- Chaix, C. , Durand-Zaleski, I., Alberti, C. & Brun-Buisson, C. Control of endemic methicillin-resistant Staphylococcus aureus: a cost-benefit analysis in an intensive care unit. JAMA 1999, 282, 1745–1751. [Google Scholar] [PubMed]
- Haddadin, A. S. , Fappiano, S. A. & Lipsett, P. A. Methicillin resistant Staphylococcus aureus (MRSA) in the intensive care unit. Postgraduate Medical Journal 2002, 78, 385–392. [Google Scholar] [PubMed]
- Samuel, P.; et al. Methicillin-Resistant Staphylococcus aureus Colonization in Intensive Care and Burn Units: A Narrative Review. Cureus.
- Steinig, E.; et al. Phylodynamic signatures in the emergence of community-associated MRSA. Proc Natl Acad Sci U S A 2022, 119, e2204993119. [Google Scholar] [CrossRef]
- Coyle, J. R.; et al. Effectiveness and cost of implementing an active surveillance screening policy for Acinetobacter baumannii: A Monte Carlo simulation model. American Journal of Infection Control 2014, 42, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Young, L. S. , Sabel, A. L. & Price, C. S. Epidemiologic, Clinical, and Economic Evaluation of an Outbreak of Clonal Multidrug-Resistant Acinetobacter baumannii Infection in a Surgical Intensive Care Unit. Infect. Control Hosp. Epidemiol. 2007, 28, 1247–1254. [Google Scholar] [PubMed]
- Taori, S. K.; et al. Candida auris outbreak: Mortality, interventions and cost of sustaining control. Journal of Infection 2019, 79, 601–611. [Google Scholar] [CrossRef]
- Otter, J. A.; et al. Counting the cost of an outbreak of carbapenemase-producing Enterobacteriaceae: an economic evaluation from a hospital perspective. Clin Microbiol Infect 2017, 23, 188–196. [Google Scholar] [CrossRef] [PubMed]
- van Beurden, Y. H.; et al. Cost analysis of an outbreak of Clostridium difficile infection ribotype 027 in a Dutch tertiary care centre. J Hosp Infect 2017, 95, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Rosa, R.; et al. Impact of In-house Candida auris Polymerase Chain Reaction Screening on Admission on the Incidence Rates of Surveillance and Blood Cultures With C. auris and Associated Cost Savings. Open Forum Infect Dis 2023, 10, ofad567. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; et al. Cost of hospital management of Clostridium difficile infection in United States-a meta-analysis and modelling study. BMC Infect Dis 2016, 16, 447. [Google Scholar] [CrossRef] [PubMed]
- Otete, E. H.; et al. Parameters for the Mathematical Modelling of Clostridium difficile Acquisition and Transmission: A Systematic Review. PLoS One 2013, 8, e84224. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; et al. Cost-effectiveness of bezlotoxumab and fidaxomicin for initial Clostridioides difficile infection. Clin Microbiol Infect 2021, 27, 1448–1454. [Google Scholar] [CrossRef]
- Elsaid, M. , Nasef, M. A. & Huy, N. T. R0 of COVID-19 and its impact on vaccination coverage: compared with previous outbreaks. Hum Vaccin Immunother 2021, 17, 3850–3854. [Google Scholar]
- Merler, S. & Ajelli, M. Deciphering the relative weights of demographic transition and vaccination in the decrease of measles incidence in Italy. Proc Biol Sci 2014, 281, 20132676. [Google Scholar]
- Majumder, M. S. , Rivers, C., Lofgren, E. & Fisman, D. Estimation of MERS-Coronavirus Reproductive Number and Case Fatality Rate for the Spring 2014 Saudi Arabia Outbreak: Insights from Publicly Available Data. PLoS Curr, 3382. [Google Scholar]
- Liu, W. , Tang, S. & Xiao, Y. Model Selection and Evaluation Based on Emerging Infectious Disease Data Sets including A/H1N1 and Ebola. Comput Math Methods Med 2015, 2015, 207105. [Google Scholar] [PubMed]
- Menardo, F. Understanding drivers of phylogenetic clustering and terminal branch lengths distribution in epidemics of Mycobacterium tuberculosis. eLife.
- Shrestha, S.; et al. Model-based Analysis of Tuberculosis Genotype Clusters in the United States Reveals High Degree of Heterogeneity in Transmission and State-level Differences Across California, Florida, New York, and Texas. Clin Infect Dis 2022, 75, 1433–1441. [Google Scholar] [CrossRef] [PubMed]
- Mathis, A. D.; et al. Maintenance of Measles Elimination Status in the United States for 20 Years Despite Increasing Challenges. Clinical Infectious Diseases 2022, 75, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F. M.; et al. The basic reproduction number (R0) of measles: a systematic review. Lancet Infect Dis 2017, 17, e420–e428. [Google Scholar] [CrossRef] [PubMed]
- Villela, D. a. M.; et al. Zika in Rio de Janeiro: Assessment of basic reproduction number and comparison with dengue outbreaks. Epidemiol Infect 2017, 145, 1649–1657. [Google Scholar] [CrossRef]
- Chowell, G.; et al. The basic reproduction number R0 and effectiveness of reactive interventions during dengue epidemics: the 2002 dengue outbreak in Easter Island, Chile. Math Biosci Eng 2013, 10, 1455–1474. [Google Scholar] [PubMed]
- Khan, M. A. & Fatmawati. Dengue infection modeling and its optimal control analysis in East Java, Indonesia. Heliyon 2021, 7, e06023. [Google Scholar]
- Navarro Valencia, V. A. , Díaz, Y., Pascale, J. M., Boni, M. F. & Sanchez-Galan, J. E. Using compartmental models and Particle Swarm Optimization to assess Dengue basic reproduction number R 0 for the Republic of Panama in the 1999-2022 period. Heliyon 2023, 9, e15424. [Google Scholar]
- Muzembo, B. A.; et al. The basic reproduction number (R0) of ebola virus disease: A systematic review and meta-analysis. Travel Med Infect Dis 2024, 57, 102685. [Google Scholar] [CrossRef]
- Nsubuga, R. N. , White, R. G., Mayanja, B. N. & Shafer, L. A. Estimation of the HIV basic reproduction number in rural south west Uganda: 1991-2008. PLoS One 2014, 9, e83778. [Google Scholar]
- DalBen, M. de F. et al. S: Strategy to Control the Spread of Carbapenem- Resistant Enterobacteriaceae.
- Stachel, A.; et al. Implementation and evaluation of an automated surveillance system to detect hospital outbreak. American Journal of Infection Control 2017, 45, 1372–1377. [Google Scholar] [CrossRef] [PubMed]
- Piaggio, D.; et al. The use of smart environments and robots for infection prevention control: A systematic literature review. Am J Infect Control 2023, 51, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A. , Schwebke, I. & Kampf, G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis 2006, 6, 130. [Google Scholar]
- Corbella, X.; et al. Environmental sampling of Acinetobacter baumannii: moistened swabs versus moistened sterile gauze pads. Infect Control Hosp Epidemiol 1999, 20, 458–460. [Google Scholar] [CrossRef]
- Schwab, F. , Meyer, E., Geffers, C. & Gastmeier, P. Understaffing, overcrowding, inappropriate nurse:ventilated patient ratio and nosocomial infections: which parameter is the best reflection of deficits? J Hosp Infect 2012, 80, 133–139. [Google Scholar] [PubMed]
- Oliveira, A. C. de, Garcia, P. C. & Nogueira, L. de S. Nursing workload and occurrence of adverse events in intensive care: a systematic review. Rev Esc Enferm USP 2016, 50, 683–694. [Google Scholar]
- Bracco, D. , Dubois, M.-J., Bouali, R. & Eggimann, P. Single rooms may help to prevent nosocomial bloodstream infection and cross-transmission of methicillin-resistant Staphylococcus aureus in intensive care units. Intensive Care Med 2007, 33, 836–840. [Google Scholar] [PubMed]
- Hatfull, G. F. , Dedrick, R. M. & Schooley, R. T. Phage Therapy for Antibiotic-Resistant Bacterial Infections. Annu Rev Med 2022, 73, 197–211. [Google Scholar]
- Wang, J.; et al. Isolation and identification of a novel phage targeting clinical multidrug-resistant Corynebacterium striatum isolates. Front Cell Infect Microbiol 2024, 14, 1361045. [Google Scholar] [CrossRef]
- Skurnik, D.; et al. Extended-spectrum antibodies protective against carbapenemase-producing Enterobacteriaceae. J Antimicrob Chemother 2016, 71, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Kalfopoulou, E. & Huebner, J. Advances and Prospects in Vaccine Development against Enterococci. Cells 2020, 9, 2397. [Google Scholar] [PubMed]
- Miller, L. S. , Fowler, V. G., Shukla, S. K., Rose, W. E. & Proctor, R. A. Development of a vaccine against Staphylococcus aureus invasive infections: Evidence based on human immunity, genetics and bacterial evasion mechanisms. FEMS Microbiol Rev 2019, 44, 123–153. [Google Scholar]
- Bae, J. Y.; et al. Association between Pneumonia Development and Virulence Gene Expression in Carbapenem-Resistant Acinetobacter baumannii Isolated from Clinical Specimens. Can J Infect Dis Med Microbiol 2023, 2023, 8265683. [Google Scholar] [CrossRef]
- Wong, F. , de la Fuente-Nunez, C. & Collins, J. J. Leveraging artificial intelligence in the fight against infectious diseases. Science 2023, 381, 164–170. [Google Scholar] [PubMed]
- Ben-Chetrit, E.; et al. An intervention to control an ICU outbreak of carbapenem-resistant Acinetobacter baumannii: long-term impact for the ICU and hospital. Crit Care 2018, 22, 319. [Google Scholar] [CrossRef] [PubMed]
- Enfield, K. B.; et al. Control of simultaneous outbreaks of carbapenemase-producing enterobacteriaceae and extensively drug-resistant Acinetobacter baumannii infection in an intensive care unit using interventions promoted in the Centers for Disease Control and Prevention 2012 carbapenemase-resistant Enterobacteriaceae Toolkit. Infect Control Hosp Epidemiol 2014, 35, 810–817. [Google Scholar]
- Landelle, C. , Pagani, L. & Harbarth, S. Is patient isolation the single most important measure to prevent the spread of multidrug-resistant pathogens? Virulence 2013, 4, 163–171. [Google Scholar]
- DalBen, M. D. F.; et al. A Model-Based Strategy to Control the Spread of Carbapenem-Resistant Enterobacteriaceae: Simulate and Implement. Infect. Control Hosp. Epidemiol. 2016, 37, 1315–1322. [Google Scholar] [CrossRef]

Table 1.
The routes of transmission for some of the most frequent difficult-to-treat pathogens in ICU setting.
Table 1.
The routes of transmission for some of the most frequent difficult-to-treat pathogens in ICU setting.
| Routes of transmission in ICU |
|---|
| Direct or indirect contact Bacteria: MDR-GNB [9] (including CRE, ESBL carriers [10], MDR-Klebsiella spp, MDR-Acinetobacter baumanii [11], and MDR-Pseudomonas aeruginosa), MRSA [12], VRE [13], Clostridium difficile [13] Fungi: Candida auris [14], Scedosporium spp [15] Virus: Ebola virus [16] |
| Water contamination [17] Bacteria: Legionella spp., Pseudomonas spp, Acinetobacter spp, and Serratia Fungi: Aspergillus spp., Mucor spp., Trichosporon spp., Scedosporium spp [18] and Fusarium Virus: Norovirus |
| Air contamination Bacteria [19]: CRE, Acinetobacter baumanii, Pseudomonas aeruginosa, Corynebacterium striatum*, Legionella spp., MRSA [20] Fungi: Aspergillus spp [21], Fusarium spp [18], Scedosporium spp [15,18], Lomentospora spp. [18] Virus: human coronaviruses (including SARS-CoV-2 [22]), Ebola virus [16] |
| Droplet and airborne spread [23] Bacteria: Mycobacterium tuberculosis, Bordetella spp, Pertussis Virus: human coronaviruses (including SARS-CoV-2 [22]), Varicela-Zoster virus, Measles virus, influenza viruses (including H1N1, H2N3, H5N1), Parainfluenza viruses, Respiratory Syncytial Virus, Adenoviruses |
MDR-GNB: Multidrug-resistant gram-negative bacteria; CRE: Carbapenem resistant Enterobacterales; ESBL: Extended-Spectrum Beta-lactamase.*It did not escape our attention that MDR-Corynebacterium striatum is an emerging MDR-GB (Multidrug-resistant gram-positive bacterium) [24] that soon could be included among pathogens the requiring-isolation. Although the route of transmission has not been clearly identified [25], as frequently presented as respiratory infections having similar characteristics compared to MDR-GN ‘s, we decided to list it in ‘Air contamination’ pathogens’ route.
Table 2.
Studies aiming to evaluate patient-to-nurse (PNR) optimal ratio in ICU setting.
| Type of study | Study author and year of publishing | Country | Time period | Sample size | Suggested ICU PNR | Higher ratios are associated with higher mortality |
|---|---|---|---|---|---|---|
| Guidelines | Bray K et al. 2010 (the British Association of Critical Care Nurses, the Critical Care Networks National Nurse Leads) [35] | UK | - | - | 1: 1 | Yes |
| American Nurses Association (ANA) and California Legislation (Assembly Bill No. 394) | California, USA | - | - | 2 : 1 | Yes | |
| Narrative review | Suresh K. Sharma et Ritu Rani 2020 [36] | India | - | - | 1 : 1 | Yes |
| Retrospective observational study | Falk AC 2023 [37] | Sweden | 15 years | 2 ICUs (9,814 patients) | 1 : 1 | Yes |
| Cross-sectional, retrospective, risk adjusted observational study | West E et al. 2014 [38] | UK | 16 years | 65 ICUs (38,168 patients) | 0,5 : 1 | Yes* |
*ICU with 1 : 1 compared to 0,5 : 1 PNR showed a slightly higher estimated mortality in the first group, although not statistically significant. Authors conclude that probably health care managers should consider not only the PNR, but also their educational level, and specific skills. ICU: intensive care unti. PNR: patient-to-nurse ratio.
Table 3.
Studies evaluating the association between intensivist-to-patient ratio and higher mortality rates in ICU setting.
Table 3.
Studies evaluating the association between intensivist-to-patient ratio and higher mortality rates in ICU setting.
| Study author and year of publication | Country | Type of study | Time period | Sample size | Median PIR | Higher ratios resulted to be associated with higher mortality |
|---|---|---|---|---|---|---|
| Neuraz A et al. 2015 [40] | France | Multicenter observational study | 2013 |
5,718 patients (8 ICUs) |
5.6 | Yes |
| Gershengorn HB et al. 2017 [41] | UK | Retrospective cohort study | 2010-2013 |
49,686 patients (94 ICUs) |
8.5 | Yes |
| Dara SI et al. 2005 [44] | USA | Retrospective cohort study | 2001-2003 | 2,492 patients (1 ICU) |
8.4* |
No |
| Gershengorn HB et al. 2022 [42] | Australia and New Zealand | Retrospective cohort study | 2016-2019 | 27,380 patients (67 ICUs) in the “narrow cohort” and 91,206 patients (73 ICUs) in the “broad cohort” | 10.1 | No |
| Agarwal A et al. 2022 [45] | USA | Cross-sectional observational study | 2020-2021 | 1,322 patients (62 ICUs) |
12 | No |
| Kahn JM et al. 2023 [46] | USA | Retrospective cohort study | 2018-2020 | 51,656 patients (29 ICUs) |
11.8 | No |
| Estenssoro E et al. 2017 [47] | Latin America (51% from Brazil, 17% Chile, 13% Argentina, 6% Ecuador, 5% Uruguay, 3% Colombia, and 5% between Mexico, Peru, and Paraguay.) | Cross-sectional observational study | 2015-2016 | 257 ICUs | 1:1-1:3 (11%) 1:4 to 1:7 (46%) > 8 (41%) |
Not evaluated |
*calculated; ICU: Intensive Care Unit; PIR: patient-to-intensivist ratio; UK: United Kingdom; USA: United States of America.
Table 4.
Education models proposed to cope with healthcare-associated infections (HCAI) in Intensive Care Unit (ICU).
Table 4.
Education models proposed to cope with healthcare-associated infections (HCAI) in Intensive Care Unit (ICU).
| Study author and year of publication | Country | Type of infection | Most relevant proposed solution |
|---|---|---|---|
| Menegueti MG et al. 2019 [49] | Brazil | CAUTI |
|
| McNett et al 2020 [54] | USA | VAP |
|
| Mogyodi et al. 2023 [56] | Hungary | VAP |
|
| Phan et al. 2018 [57] | Vietnam | All HCAI |
|
| Moghnieh et al. 2023 [53] | Eastern Mediterranean Region (Afghanistan. Barhain, Iraq, Kuwait, Jordan, Lebanon, Oman, Pakistan, Palestine, Qatar, Sudan, Syria, United Arab Emirates, Yemen) | All HCAI |
|
CAUTI: catheter-associated urinary tract infections. HCAI: healthcare-associated infecitons. HCWs: healthcare workers. VAP: ventilator associated pneumonia. HH: hand hygiene.
Table 5.
Applicable risk-assessment scores for outbreak-related pathogens’ colonization and/or infection development.
Table 5.
Applicable risk-assessment scores for outbreak-related pathogens’ colonization and/or infection development.
| Candida spp. [93] | Colonization | Candida Colonization Index [94] | Ratio of the number of (non-blood) sites colonized with Candida spp /total number of sites cultured Threshold = 0.5 |
PPV = 66% NPV = 100% |
| Infection | Candida score [95] | Candida Score = TPN (1 point), surgery (1 point), severe sepsis (2 points), Multifocal Candida colonization (1 point). Threshold = 2.5 |
Sensitivity = 81% Specificity = 74% PPV = 16% NPV = 98% |
|
| Ostrosky-Zeichner Clinical Prediction Rule [96] |
Mechanical ventilation ≥ 48hours AND Systemic antibiotic AND CVP (on any of day 1–3 of ICU admission) plus ≥1 of: any major surgery (days 7–0), pancreatitis (days 7–0), use of steroids/other immunosuppressive agents (days 7–0), use of TPN (days 1–3), or dialysis (days 1–3) | Sensitivity = 50% Specificity= 83% PPV = 10% NPV = 97% |
||
| ESBL-producing Enterobacteriacae | Colonization | Tumbarello et al. [97] | Recent (≤12 months before admission) hospitalization, transfer from another health care facility, Charlson comorbidity score ≥ 4, recent (≤3 months before admission) β-lactam and/or fluoroquinolone treatment, recent urinary catheterization, and age ≥ 70 years. | With cutoff score ≥3: Sensitivity = 94% Specificity = 41% PPV = 44% NPV = 93% |
| Infection (BSI) | ESBL Prediction Score (ESBL-PS) [98] | Outpatient procedures within 1 month, prior infections or colonization with ESBLE within 12 months, and number of prior courses of β-lactams and/or fluoroquinolones used within 3 months of BSI. | With cutoff score ≥1: Sensitivity = 88% Specificity = 77% PPV = 16% NPV = 99% With cutoff score ≥3: Sensitivity = 43% Specificity = 96% PPV = 33% NPV = 97% |
|
| CPE | Colonization | Papafotiou et al. [99] | Karnofsky score, previous hospitalization, stay in a Long-term care facilty, history of ≥2 different interventional procedures, previous CPE colonization or infection, renal replacement therapy, and diabetes with end-organ damage | With cutoff score ≥27: Sensitivity = 72% Specificity = 81% PPV = 15% NPV = 98% |
| CRAB | Infection | Cogliati Dezza et al. [100] | CRAB colonization, higher CCI, multisite colonization and the need for mechanical ventilation. | Unknown |
| XDR A. baumanii | Colonization | Moghnieh et al. [101] | Urinary catheter placement >6 days, ICU contact pressure for >4 days, presence of gastrostomy tube, and previous use of carbapenems or piperacillinetazobactam | Unknown |
| MRSA | Colonization | Torres et Sampathkumar [102] | Nursing home residence, diabetes, hospitalization in the past year, and chronic skin condition/infection | With cutoff score ≥8: Sensitivity = 54% Specificity = 80% |
| VRE | Colonization | The PREVENT score [103] | Age of ≥60 years, hemato-oncological disease, cumulative antibiotic treatment for >4 weeks, and a VRE infection | Sensitivity = 82% Specificity = 77% PPV = 57% NPV = 92% |
| MDROs | Colonization | AutoRAS- MDRO [104] | Electronic health records (EHRs) | Sensitivity = 81% Specificity= 79% PPV = 49% NPV = 94% |
Table 7.
Table 7. Estimated basic reproduction number (R0), single patient- and associated outbreak- costs of the most common pathogens responsible for outbreaks in ICU based on literature research.
Table 7.
Table 7. Estimated basic reproduction number (R0), single patient- and associated outbreak- costs of the most common pathogens responsible for outbreaks in ICU based on literature research.
| Type of pathogen | Estimated mean single-patient cost per hospital length of stay i | Estimated mean R₀ | Estimated mean outbreak cost | IPC implementation threshold (up to) |
|---|---|---|---|---|
| CRE | $ 639,48 | 11 | €1.1 millions | $572,000 |
| CRAB | $55,122-$ 60,000 | 1.5 | €1.0 millions | $75,000- $93,822/QALY |
| VRE | $17,949 | 1.32 | € 60.524 | $50.000/QALY |
| MRSA | $ 9.275 | 0.97-1.6 [160] | $30.225 | $9.275 |
| C. auris | € 35.818* | Unknown | € 1.2 millions | $3.730.480,26 |
| (HO-CDI) | $30,049 - $34,149 [165,167] | 0.55-7.0 [168] | €1.2 millions | $150 000/QALY [169] |
C.auris: Candida auris; CRAB: carbapenem-resistant Acinetobacter baumanii; CRE: carbapenem-resistant Enterobacteriaceae; HO-CDI: Hospital-acquired Clostridium difficile infection. MRSA: meticillin-resistant Staphylococcus aureus; QALY: quality-adjusted life year. VRE: vancomycin-resistant Enterococci. * Calculated dividing the total cost of the outbreak for the number of patients involved.
Table 8.
Estimated basic reproduction number (R0) of other pathogens possibly responsible for outbreaks in ICU.
Table 8.
Estimated basic reproduction number (R0) of other pathogens possibly responsible for outbreaks in ICU.
| Type of transmission | Type of pathogen | Estimated R₀ (mean) | Country |
|---|---|---|---|
| Airborne | SARS-CoV-2 | 1.4 to 6.7 [170] (4.1) | China, Italy, Korea, Peru |
| SARS virus | 1.7 to 1.9 [171] (1.8) | Hong Kong | |
| MERS virus | 2.0 to 6.7 [172] (4.4) | Saudi Arabia | |
| H1N1 | 1.9 [173] | China | |
| Mycobacterium tuberculosis (MTB) | 0.8 to 1.2 [174] 0.2 to 0.4 [175] (0.29) |
USA |
|
| Measles virus | 0.7 [176] to 25.3 [171] (13)* 12-18 (15) [177] |
USA, Italy, Japan Systemic review |
|
| Vectorborne | Zika virus | 2.3 [178] to 27.2 [179] (14.9) | Brazil, Chile |
| Dengue virus | 1.1 [180]-1.7 [178,181] (1.4) | Indonesia, Brazil | |
| Bloodborne/ Body fluids contact |
Ebola virus | 1.1 to 10 [182] (1.95) [182] | West Africa |
| HIV (viremic) | (36.8) [183] | Uganda |
*The most recent studies suggest a R0<1 thanks to vaccination.
Table 9.
New experimented strategies in the last 10 years to prevent MDROs spreading.
| Study author and year of publication | Country | Study design | Pathogen | Experimental period | Name of the new strategies |
|---|---|---|---|---|---|
| De Freitas DalBen et al. 2016 [184] | Brazil | Prospective study | CRE | Baseline period: 10 monthsIntervention period: 24 weeks | Educational model based on:
|
| Stachel et al. 2017 [185] | USA | Prospective study | MDROs | 8 months | Automated surveillance system to detect hospital outbreak |
| Fitzpatrick et al. 2020 | Ireland | Narrative review | All pathogens | - | Artificial Intelligence in IPC: driven by “big data”, it could find correlations that may indicate medically relevant conditions or identify potential risk factors for outbreaks |
| Meschiari et al. 2021 [51] | Italy | Prospective study | CRAB | 6-years (2013-2019) | Cycling radical cleaning and disinfection |
| Piaggio et al. 2023 [186] | Italy | Systemic review | All pathogens | - |
|
| Zwerwer et al. 2024 [132] | Netherlands | Prospective study | All pathogens | 3-years (2014-2017) | Machine-learning model to predict the need for infection-related consultations in ICU |
ICU: Intensive Care Unit; IPC: Infection prevention and control; USA: United States of America.
Table 10.
Proposed future strategies tackling MDROs spreading in ICU.
| First Author and year of publication | Country | Target pathogen | Aim of the study | Suggested technique |
|---|---|---|---|---|
| Hatfull GF et al. 2022 [192] | USA | MDRB | Fighting antibiotic resistance | Phage therapy |
| Wang J et al. 2024 [193] | China | MDR-Corynebacterium striatum | Fighting antibiotic resistance | Phage therapy |
| Skurnik et al. 2016 [194] | USA | CPE | Vaccine against CPE (including NDM-producers E. coli, E. cloacae, K. pneumoniae, K. pneumoniae carbapenemase (KPC)-producing and PNAG-producing P. aeruginosa) | Vaccine targeting polysaccharide poly-(β-1,6)-N-acetyl glucosamine (PNAG) in CPE |
| Kalfopoulou et Huebner. 2020 [195] | Germany | VRE | Vaccine against Enterococci and VRE | Vaccine targeting capsular polysaccharides and surface-associated proteins in Enterococci |
| Miller et al. 2020 [196] | USA | MRSA | Vaccine against MRSA | Vaccine targeting superantigens and pore-forming toxins in MRSA |
| Meschiari et al. 2021 [51] | Italy | CRAB | IPC measures in CRAB’s outbreaks | Targeting inactivated adeN gene in CRAB |
| Ji Yun Bae et al. 2023 [197] | Korea | CRAB | Identifying virulents CRAB’s genes associated with higher mortality in VAP | Targeting hisF and uspA genes in CRAB |
| Choi et al. 2022 [82] | South Korea | VRE and CRE | New non-antibiotic decolonization strategy | 4-items bundle:
|
| Wong et al. 2023 [198] | USA | All pathogens | Use of artificial intelligence for new antinfective drugs discovery, pathogens’ pathophysiology and transmission understanding, and diagnostics | Artificial intelligence implementation |
| Zwerwer et al. 2024 [132] | Netherlands | All pathogens | Use a machine-learning model to predict the need for infection-related consultations in ICU | Machine-learning model |
CRAB: carbapenem-resistant Acinetobacter baumanii; CRE: carbapenem-resistant Enterobacteriaceae; CPE: carbapenem-producing Enterobacteriaceae. ICU: Intensive Care Unit. MRSA: meticillin-resistant Staphylococcus aureus; PNAG: polysaccharide poly-(β-1,6)-N-acetyl glucosamine. VRE: vancomycin-resistant Enterococci.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



