Submitted:
03 July 2024
Posted:
04 July 2024
You are already at the latest version
Abstract
Introduction: Treating elbow fracture-dislocation is a challenge, especially in the situation of basal-coronoid trans-ulnar fracture. The study ams to explain whether or not the minimal invasive surgery (MIS) would be feasible in elbow dislocation with coronoid fracture. Materials & Methods: At Taipei Veterans General Hospital, patients who had elbow dislocations with coronoid process fractures underwent single one surgeon’s MIS techniques which included the fluoroscopy-guided ulnar anteromedial (FGUAM) approach in the stage of reducing coronoid process. When there is a proximal ulnar fracture, the posterior incision should be necessary, followed by the incision over the lateral or medial elbow in treating radial fractures or ligament injuries. Results: The Flow Diagram about approach recommendation was established in base of defining MIS as not to do cross-plane dissection. Anteriorly rigid fixation for the coronoid process was also emphasized. Conclusions: MIS can be achieved by multiple limited surgical incisions. However, if there is an unstable ulnar metaphysis or ligament avulsion fracture, the posterior approach has to be extended and the so-called MIS fails to be established.
Keywords:
minimal invasive surgery (MIS)
; coronoid process fracture
; elbow terrible-triad
; posteromedial instability
; basal-coronoid trans-ulnar fracture
; trans-olecranon fracture
1. Introduction
1.1. Background
Surgical treatment for fracture-dislocation of the elbow with a concomitant coronoid fracture is a challenge. Clinically at the authors’ institute, the most common types are terrible-triad fractures and Mayo’s basal-coronoid trans-ulnar fracture-dislocations whereas the posteromedial instability is the rarest. In such cases, the injuries include coronoid process fracture, radial head fracture, proximal ulnar fracture, and also ligament injuries. The most critical issue is not the degree of comminution, nor the sequence or technique of how to fix these fragments, but how to restore the stability of the elbow joint with the least damage to the soft tissue, and the patient must be able to engage in passive range of motion (ROM) training immediately post-operatively.
Although conventional extensive approaches can be used to do these fractures well, such as lateral extensile approach [1], fragment-specific approach with reflecting olecranon [2], medial extensile approach [3], or posterior approach with extended to lateral and medial sides [4], there exist soft tissue problems and risk of nerve traction.
In the author's experience, there was a case where the extended posterior approach was used but the coronoid process lost of reduction (Figure 1). At that time, the coronoid process in this case could not be fixed with screw from the rear side, so the Lasso technique was used to fix the fractured coronoid. However, during the immediate ROM training process after surgery, the avulsion force from the brachialis muscle was inevitable. Therefore, this makes the author rethink the necessity of anterior fixation. In addition to the fixed effect, soft tissue dissection is also taken into consideration. The advantage of the front buttress plate is that it can directly provide better resistance to brachialis avulsion force.
In the authors’ institute, a kind of limited anterior approach is conducted by the experienced surgeon. This approach is named as the fluoroscopy-guided ulnar anteromedial (FGUAM) approach and is supposed to be useful to reduce soft tissue damage in the treatment of elbow dislocation with concomitant coronoid fracture.
1.2. Objectives of the Study
Despite the fact that the best surgical method is still controversial, we believe that good results can be obtained with the treatment method that the surgeon is most familiar with. The authors aimed to establish a surgical protocol, the Flow Diagram based on the retrospective cases, explaining whether or not the minimal invasive surgery (MIS) would be feasible in the situation of elbow dislocation with coronoid fracture. The focus of this study is to design a protocol composed of existing surgical techniques and experiences and further to show how to reduce soft tissue dissection. There were two categories in the Flow Diagram, MIS and non-MIS. Every step of the surgical technique was also discussed, including the FGUAM approach.
1.3. Hypothesis
The Flow Diagram can afford the recommendation between MIS and non-MIS approaches whereas the operator can find the clues for treatment strategy in such complicated fracture types.
2. Materials and Methods
Three groups of cases were identified in the study. One had an anteromedial facet fracture of the coronoid process in the situation of posteromedial instability, and another one had transverse coronoid process fractures in terrible-triad fracture-dislocations. The third group had Mayo’s basal-coronoid trans-ulnar fracture dislocation [5]. One single surgeon treated all cases with the same surgical principles. Because the research purpose was to develop a surgical protocol, the number of cases to be accepted was not set initially.
2.1. Pre-Operative Evaluation & Defining MIS
The CT scan with three-dimensional (3D) reconstruction was supposed to be an essential survey for pre-operative planning. Every fractured fragment should be checked by image studies especially the avulsion part of ligament insertion. The surgical approach window was quite different whether the ligament was severed in the middle or inserted. The definition of MIS for elbow was considered by the authors as it did not only depend on the absolute length of the wound, but also on whether the dissection spans different surgical planes. On the other hand, the cross-plane approach was considered as non-MIS. As for the surgical planes, different planes indicated the need for fixing different structures. For example, the buttressing coronoid process needed the anterior plane whereas the avulsed ligament insertion or fractured proximal ulnar bone should be treated through the posterior plane.
In summary, the inclusion criteria for MIS in this study is to confirm whether the surgical wound on each plane during the operation is a limited approach and there is no cross-plane dissection. In addition, the reduction and fixation sequence are set to 4 steps. The surgical techniques for each step are described below.
2.2. Steps of Fixing Coronoid Process Anteriorly
According to the above definition of MIS, if the surgeon expects to avoid cross-plane dissection, anterior fixation for coronoid process is inevitable.
There were 2 steps in the surgical techniques when fixation of the coronoid process anteriorly. In the first step, the fractured coronoid process was exposed with FGUAM approach (Figure 2A,B) which was modified from the original AM approach introduced by Yang et al [6]. When reducing the coronoid fragment, one 1.25mm K-wire was perpendicularly applied. Then the anatomical position of ulnohumeral joint was confirmed under the “splinting force” of the K-wire. A 1.5mm headless compression screw could be chosen and applied just near to the splinting K-wire. In the second step, another buttress plate was used on the coronoid slope (Figure 3). Finally, the provisional K-wire could be exchanged for one another 1.5mm headless compression screw. However, if the base of the coronoid process was broken, the keystone step was not to fix the coronoid process but restore the ulnar metaphysis at first (Figure 4).
2.3. Fixation of Radial Head
According to the authors’ principle, radius fixation was performed only after the fixation of the coronoid process. The fracture site was exposed through Kocher interval [7] and underwent screw and/or plate fixation. In the author's hospital, a hand-system plate is used as the main fixator for radial head fracture (Figure 5). Especially for Asian females with smaller bones, the specific plate for the radial head is often too bulky to pass through the safe zone [8] causing impingement.
2.4. Variant Proximal Ulnar Fractures and Ligaments Injuries
When analyzing comminuted proximal ulnar fractures and surgical approaches, the authors did not rely on the classification of variant trans-olecranon fracture-dislocation [9] nor Monteggia-like fracture-dislocation [10]. We chose the Mayo Classification [5] to mention the fracture as basal-coronoid trans-ulnar fracture and preferred to classify the approach methods into 2 types depending on ligamentous condition, not the fracture type itself. If the preoperative assessment showed avulsion in the ligament insertion (Figure 6) or the ulnar metaphysis was very unstable, then the extensile posterior approach must be used to repair the ligament. If the ligament insertion base was complete and the ulnar metaphysis was relatively stable, then the posterior minimally invasive percutaneous plate osteosynthesis (MIPPO) approach could fix the proximal ulnar fracture (Figure 7). Finally, the elbow stability was checked again under C-arm fluoroscopy to determining whether or not the collateral ligament should be repaired through the lateral or medial surgical window.
2.5. Post-Operative Rehabilitation
The protocol for using a post-operatively functional brace is presented with a Gantt Chart in the study. (Table 1) Under protection with a functional brace, thirty degrees of passive ROM training can be achieved immediately within the first month after surgery. Then it increases by 30 degrees every month.
3. Results
During the case collection process, it was found that patients who did not receive the anterior approach to fix the coronoid process sustained more soft tissue dissection during the operation. Eight cases with limited approaches were included in this protocol development. There were 3 cases of terrible-triad fractures, only one case of posteromedial instability, and 4 cases of basal-coronoid trans-ulnar fracture-dislocations. All patients had a functional arc of the elbow and full forearm rotation not later than 3 months after the operation. There was no malunion nor heterotrophic ossification.
There are 2 main stages and 2 interval stages in this Flow Diagram developed by the authors. The Flow Diagram is shown in Figure 8. The general four steps of fixation sequence is just shown on the top boxes, from the coronoid process to ligament injury. “Stage 1” is the first survey to evaluate whether or not the coronoid process fixation could be the first-step surgery. If coronoid fracture should be fixed, the AM approach with method of FGUAM is recommended by the authors. “Stage 2” is the second survey to check the condition of the proximal ulna. The 2 interval stages are lateral and medial windows for treating radius fracture and ligament injury respectively. The lateral window is for treating radial head as well as for lateral collateral ligament. Lateral collateral ligament can only be treated through the lateral window if it is not an insertion avulsion fracture. In detail, the insertion site anatomically belongs to lateral ulnar collateral ligament, and we surgeons need posterior approach through the Boyd interval to expose it. Finally in the Flow Diagram, the medial window in the last step is for treating medial collateral ligament.
However, in the case of basal-coronoid tran-ulnar fracture-dislocation, it is often impossible to fix the coronoid process independently first, and the ulnar metaphysis and coronoid process must be fixed at the same time. In this kind of situation, the comminuted proximal ulna bone is reduced through 2 surgical windows, the AM and posterior incisions synergistically. Therefore, AM and posterior MIPPO can be done in the same Stage 1. In the group of MIS, all approaches are done with limited incisions.
As shown in the Flow Diagram, if there is an unstable ulnar metaphysis or ligament avulsion fracture, the posterior incision has to be extended to the medial or lateral plane alongside the ulnar bone. In such a case with an extended posterior approach, the so-called MIS fails to be established. Even if the extensile posterior approach is used in the case of unstable metaphysis and avulsion fracture of ligaments, it is still recommended to use the FGUAM approach for coronoid process fracture.
In theory, up to 4 separate approaches can appear according to this flow diagram, but there is no case with more than 3 approaches. In reality, if the fracture-dislocation is complex enough to require four approaches, it will be accompanied by unstable metaphysis or avulsion fracture of ligaments. Therefore, the extensile posterior approach will extend to cover the lateral or medial incision.
4. Discussion
The authors try to explain the proof of concept about MIS approaches, but not the outcome analysis of protocol application. The study Result was the protocol itself, not the clinical outcomes of the included cases.
4.1. Novel Achievements of the Study
The authors provide a specific protocol to illustrate the reduction sequence and the conditions under which MIS for elbow fracture-dislocation can be achieved, and the conditions for non-MIS to be used can be known during preoperative planning. These were not explicitly mentioned in the previous literature. The protocol emphasizes the importance of anterior fixation for the coronoid process. In the Flow Diagram, regardless of whether MIS is available, it is recommended to use the FGUAM approach when the coronoid process fracture should be fixed. Because this approach can avoid cross-plane dissection and increase the feasibility of placing a buttress plate from the anterior side.
4.2. Classification of Comminuted Proximal Ulnar Fractures
In the past, there was a bit of confusion in the classification of proximal ulnar fracture combined with coronoid process fracture, especially when surgeons had to distinguish between Monteggia-like fracture-dislocation and variant types of trans-olecranon fracture-dislocation. Haller et al [11] pointed out that the difference between a monteggia-like fracture and a trans-olecranon fracture lies in whether the proximal radioulnar joint (PRUJ) is dislocated. In fact, it is not easy to confirm whether PRUJ is truly connected with each other when the coronoid base is separated from the ulnar metaphysis. Therefore, we recommend that the Mayo classification about coronoid-centric classification system published by O’Driscoll et al [5] can provide more concise communication and planning before surgery. In the case of trans-ulnar fracture, only when the coronoid process fracture needs to be fixed will the so-called cross-plane dissection be considered. In other words, it is whether or not an extensive approach from the posterior (or lateral or medial) to the anterior plane is necessary to fix coronoid process.
4.3. Approaches for Elbow Dislocation with Coronoid Fracture in the Literature
The authors consider that the approaches to elbow dislocation with coronoid fr should be divided into two categories for discussion. In one group the coronoid process gets fractured but the coronoid base is intact, which is commonly seen in posterior medial instability and terrible-triad fractures. Huh, Jeannie et al compared the exposure through the medial elbow using the flexor carpi ulnaris (FCU)-Splitting and Hotchkiss Over-the-Top approaches [12]. Hou et al reported the single lateral approach for terrible triad injuries [1]. Zeiders et al proposed posterior global incision to restore complicated outcomes of unstable elbow joints [13]. In addition to the single surgical approach of medial, lateral, or posterior incision, some studies also suggest 2-incision technique [14,15].
In another group, there is the unstable coronoid base, whether it is called type IID posterior Monteggia fracture [16], trans-olecranon fracture, or basal-coronoid trans-ulnar fracture. The earlier literature years ago has proposed a fragment-specific approach that they believed could be used for most of these kinds of comminuted fractures [2]. There is also the posterior incision extended to the lateral side with a modified Boyd approach presented by the recent study in which the osteotomy of supinator tuberosity is performed [17]. However, the anterior buttress plate is still difficult to accomplish with this method.
Compared with other structures, the coronoid process is located alone in the anterior plane, which means that if a single surgical approach is to be used, a larger soft tissue dissection will be required to reach the cross-plane especially when rigid anterior fixation is necessary. Therefore, relying on a single surgical approach often damages more soft tissues.
4.4. Challenges in the Flow Diagram
Among this protocol, the most challenging one is the modified AM approach: the fluoroscopy-guided ulnar AM approach. Whether it is treating posteromedial instability, terrible-triad fracture, or basal-coronoid trans-ulnar fracture dislocation, the authors consider that the rigid anterior fixation is essential and recommend using FGUAM approach to decrease soft tissue damage during the fixation of the coronoid process. Compared with the original AM approach, FGUAM requires fluoroscopic assistance to localize the range of the skin incision according to the shape and position of the proximal ulna under a plain radiograph. The curvilinear incision starts from the top of the ulnar border of the olecranon process extending distally to the top of the bicipital tuberosity (Figure 2A). After incision of bicipital aponeurosis and dissection through the interval between the brachial artery and median nerve, it is often easy to find the fractured fragment of coronoid process just in the brachialis muscle. As for the next reduction and fixation, they have a learning curve and also some pitfalls. The critical landmark is the bicipital tuberosity where the brachial artery and median nerve begin to branch. Thus, the dissection and plating are recommended not to exceed that landmark. Because of the limitation of this landmark, the anterior buttress plating can only fix the coronoid process. However, the unstable comminuted coronoid base cannot be well fixed by the anterior plate alone, and additional fixation from the posterior side is necessary.
4.5. Implants Selection
According to the author's experience, the size of the interfragmentary screw used to fix the coronoid process is more suitable to not exceed 2.0mm. However, the screw size of the anatomic locking-compression plate (LCP) exclusive for the coronoid process currently on the market is generally larger than 2.0mm. Thus, the authors recommend using hand-system LCP and the buttress plate directly in front as the main fixation method. The same issue will also occur in radial head fracture. In Asian female with smaller bones, hand-system LCP can better stay in the safe zone of the radial head.
4.6. Limitations of the Study
As a proof of concept, there was no control group in the study. The developed protocol was practical, but there was no comparison to other methods. There was also no consensus about how many cases were needed to develop a surgical protocol. In spite of developing the protocol for surgical techniques exclusively for MIS concept, the good outcome was not the hypothesis of the study and not guaranteed by the protocol neither.
4.7. Future Applications of the Research
In the literatures, the treatment methods for elbow fracture dislocation with coronoid process fracture were mainly based on the experts' specific techniques, and there was no protocol that considered soft tissue dissection or whether MIS could be performed. By promoting the protocol proposed by the authors in the study, we expect that surgeons pay attention to two key points, how to reduce soft tissue dissection through anterior approach, and stability condition around the ligament insertion. If there is no instability near the ligament’s insertion, the extensile approach is probably not necessary. Based on the proof of MIS-concept in the study, the further randomized controlled study in the future probably can be conducted to analyze treatment outcomes.
5. Conclusions
Despite lacking prospectively clinical application and analysis for the protocol, the study is a proof of concept that MIS can be achieved by multiple limited surgical incisions. The key point in the protocol is that reducing and fixing the coronoid process back to the proximal ulna needs FGUAM approach with more reliable anterior fixation, and does not rely on the cross-plane dissection even in the case of unstable metaphysis or ligament avulsion fracture. From another perspective, if the bone structure near the ligament’s insertion is stable, the posterior extensile approach for proximal ulnar fracture can be replaced by posterior MIPPO.
Author Contributions
The research was conducted by CCL at the Division of Orthopaedic Trauma, Department of Orthopaedics and Traumatology, Taipei Veterans General Hospital, Taipei, Taiwan. CCL was responsible for study design and data interpretation. The manuscript was drafted by CCL and proofread by MFC, CSW, CCC, and YPS.
Informed Consent Statement
Patient consent was waived due to retrospective study with no data linked to patient’s privacy.
Conflicts of Interest
The authors declare that they do not have any commercial or associative interest that represents a conflict of interest in connection with the work. All authors read and approved the manuscript.
References
- Hou, F.; Liang, X.; Fan, W.; Zhao, F.; Li, D. Analysis of Twenty-Five Cases of Terrible Triad Injury of the Elbow Surgically Treated with a Single Lateral Approach. Int. Orthop., 2021, 45 (1), 241–246. [CrossRef]
- Beingessner, D. M.; Nork, S. E.; Agel, J.; Viskontas, D. A Fragment-Specific Approach to Type IID Monteggia Elbow Fracture-Dislocations. J. Orthop. Trauma, 2011, 25 (7), 414–419. [CrossRef]
- Lor, K. K. H.; Toon, D. H.; Wee, A. T. H. Buttress Plate Fixation of Coronoid Process Fractures via a Medial Approach. Chin. J. Traumatol., 2019, 22 (5), 255–260. [CrossRef]
- Forthman, C.; Henket, M.; Ring, D. C. Elbow Dislocation with Intra-Articular Fracture: The Results of Operative Treatment without Repair of the Medial Collateral Ligament. J Hand Surg Am, 2007, 32 (8), 1200–1209. [CrossRef]
- Barlow, J. D.; Nieboer, M. J.; Cancio-Bello, A. M.; Morrey, M. E.; Hidden, K. A.; Yuan, B. J.; Sanchez-Sotelo, J.; O’Driscoll, S. W. A Coronoid-Centric Classification System of Proximal Trans-Ulnar Fracture-Dislocations Has Almost Perfect Intraobserver and Interobserver Agreement. J. Shoulder Elbow Surg., 2023, 32 (12), 2561–2566. [CrossRef]
- Yang, X.; Chang, W.; Chen, W.; Liu, S.; Zhu, Y.; Zhang, Y. A Novel Anterior Approach for the Fixation of Ulnar Coronoid Process Fractures. Orthop. Traumatol. Surg. Res., 2017, 103 (6), 899–904. [CrossRef]
- Kocher, T. Operations at the Elbow. Stiles HJ, Paul CB, translators. Textbook of operative surgery. 3rd ed. London: Adam and Charles Black, 1911, 1911, 313–318.
- Hoekzema, N.; Gray, R.; Orbay, J.; Rubio, F.; Vernon, L.; Imada, A.; Mercer, D. Intraoperative Radiographic Method of Locating the Radial Head Safe Zone: The Bicipital Tuberosity View. J. Shoulder Elbow Surg., 2020, 29 (12), 2668–2673. [CrossRef]
- Ring, D.; Jupiter, J. B.; Sanders, R. W.; Mast, J.; Simpson, N. S. Transolecranon Fracture-Dislocation of the Elbow. J. Orthop. Trauma, 1997, 11 (8), 545–550. [CrossRef]
- Ring, D.; Jupiter, J. B.; Simpson, N. S. Monteggia Fractures in Adults. J. Bone Joint Surg. Am., 1998, 80 (12), 1733–1744. [CrossRef]
- Haller, J. M.; Hulet, D. A.; Hannay, W.; Cardon, J.; Tashjian, R.; Beingessner, D. Patient Outcomes After Transolecranon Fracture-Dislocation. J. Am. Acad. Orthop. Surg., 2021, 29 (3), 109–115. [CrossRef]
- Huh, J.; Krueger, C. A.; Medvecky, M. J.; Hsu, J. R.; Skeletal Trauma Research Consortium. Medial Elbow Exposure for Coronoid Fractures: FCU-Split versus over-the-Top. J. Orthop. Trauma, 2013, 27 (12), 730–734. [CrossRef]
- Zeiders, G. J.; Patel, M. K. Management of Unstable Elbows Following Complex Fracture-Dislocations--the “Terrible Triad” Injury. J. Bone Joint Surg. Am., 2008, 90 Suppl 4, 75–84. [CrossRef]
- Chen, H.-W.; Bi, Q. Surgical Outcomes and Complications in Treatment of Terrible Triad of the Elbow: Comparisons of 3 Surgical Approaches. Med. Sci. Monit., 2016, 22, 4354–4362. [CrossRef]
- Liu, G.; Ma, W.; Li, M.; Feng, J.; Xu, R.; Pan, Z. Operative Treatment of Terrible Triad of the Elbow with a Modified Pugh Standard Protocol: Retrospective Analysis of a Prospective Cohort. Medicine (Baltimore), 2018, 97 (16), e0523. [CrossRef]
- Jupiter, J. B.; Leibovic, S. J.; Ribbans, W.; Wilk, R. M. The Posterior Monteggia Lesion. J. Orthop. Trauma, 1991, 5 (4), 395–402. [CrossRef]
- Kokkalis, Z. T.; Bavelou, A.; Kalavrytinos, D.; Sinos, G.; Antzoulas, P.; Panagopoulos, A. Surgical Treatment of Monteggia-Like Lesions With a Modified Boyd Approach. Journal of Shoulder and Elbow Arthroplasty, 2023, 7, 24715492231196624. [CrossRef]
Figure 1.
The coronoid process lost of reduction (yellow circle).
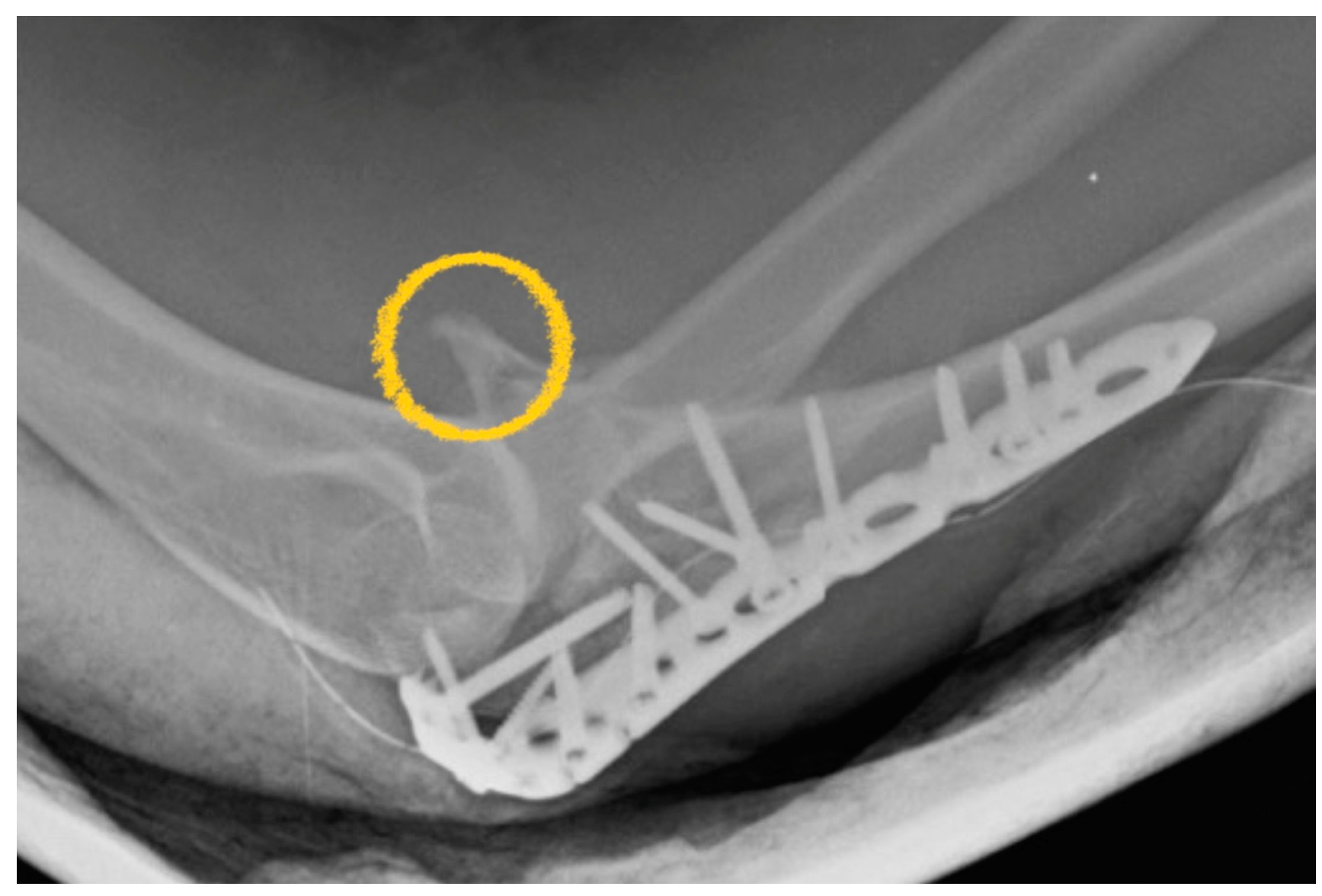
Figure 2.
The fluoroscopy-guided ulnar anteromedial (FGUAM) approach, A) Under a plain radiograph, the curvilinear incision (yellow line) starts from the top of the ulnar border (red line) of the olecranon process extending distally to the top of the bicipital tuberosity, B) Anterior fixation with a plate.
Figure 2.
The fluoroscopy-guided ulnar anteromedial (FGUAM) approach, A) Under a plain radiograph, the curvilinear incision (yellow line) starts from the top of the ulnar border (red line) of the olecranon process extending distally to the top of the bicipital tuberosity, B) Anterior fixation with a plate.
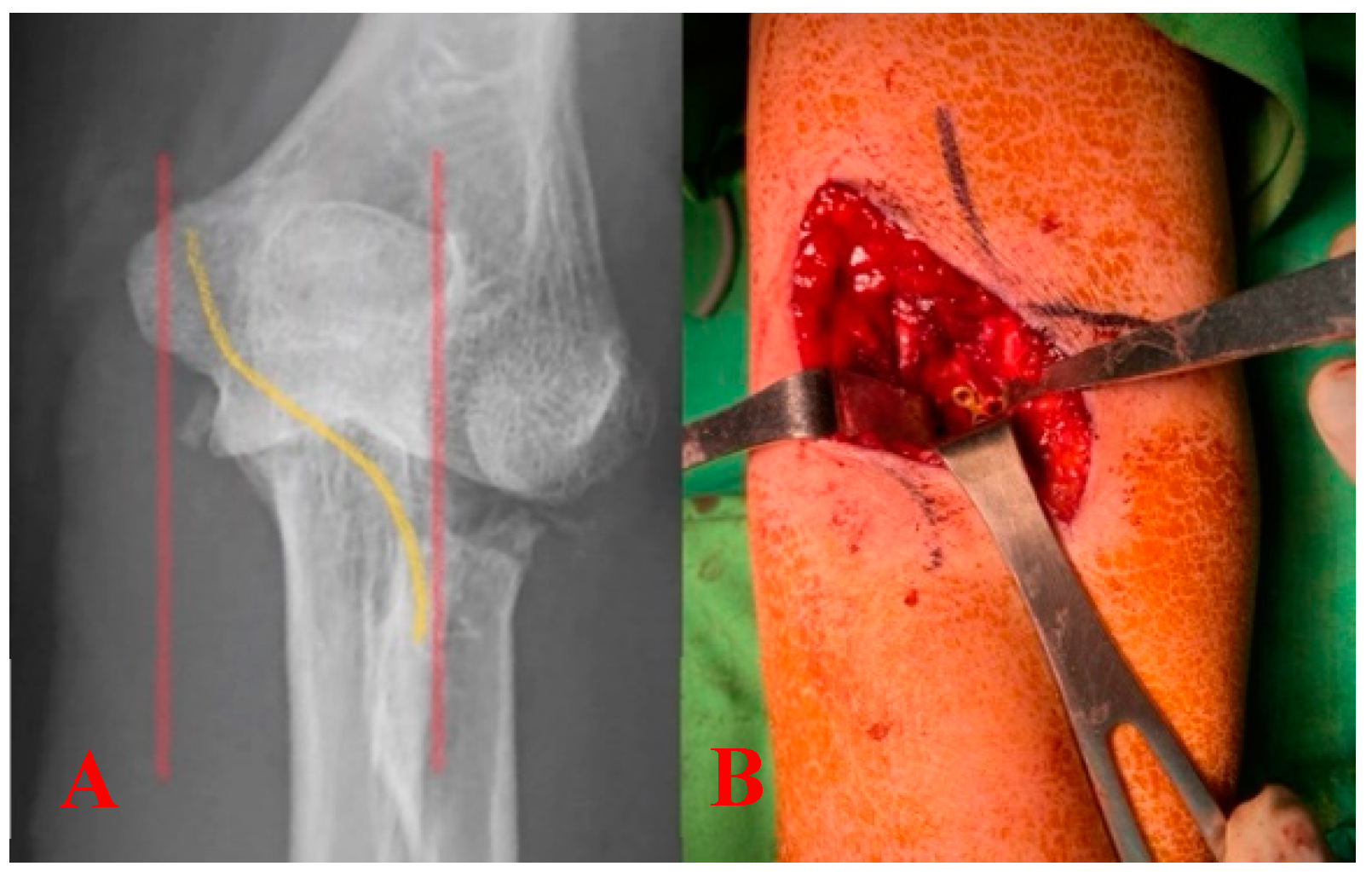
Figure 3.
Fixation of the coronoid process with interfragmentary headless screws and a buttress plate.
Figure 3.
Fixation of the coronoid process with interfragmentary headless screws and a buttress plate.

Figure 4.
The unstable coronoid base should be restored before the fixation of the coronoid process.
Figure 4.
The unstable coronoid base should be restored before the fixation of the coronoid process.
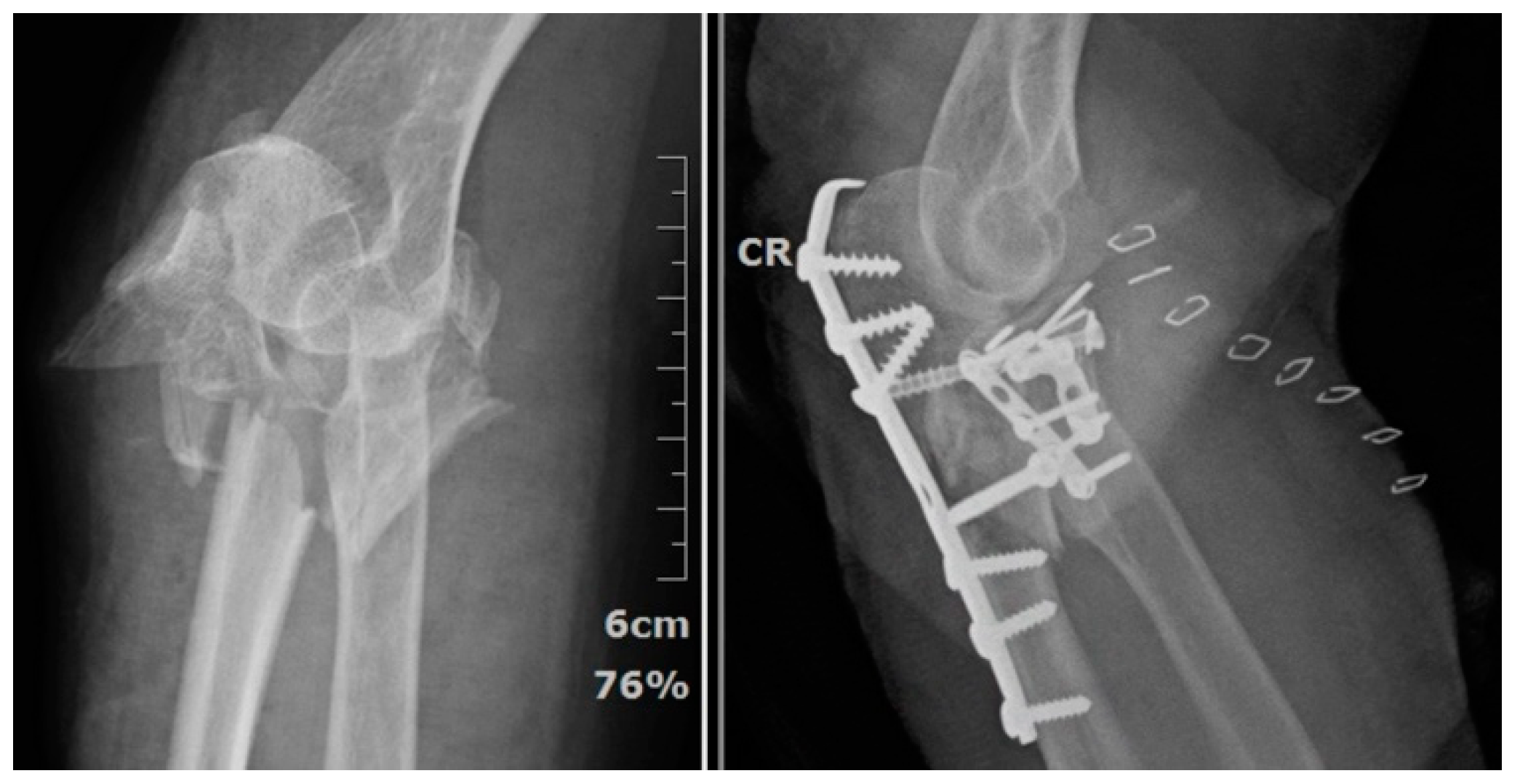
Figure 5.
The hand-system plate being applied to the radial head fracture.
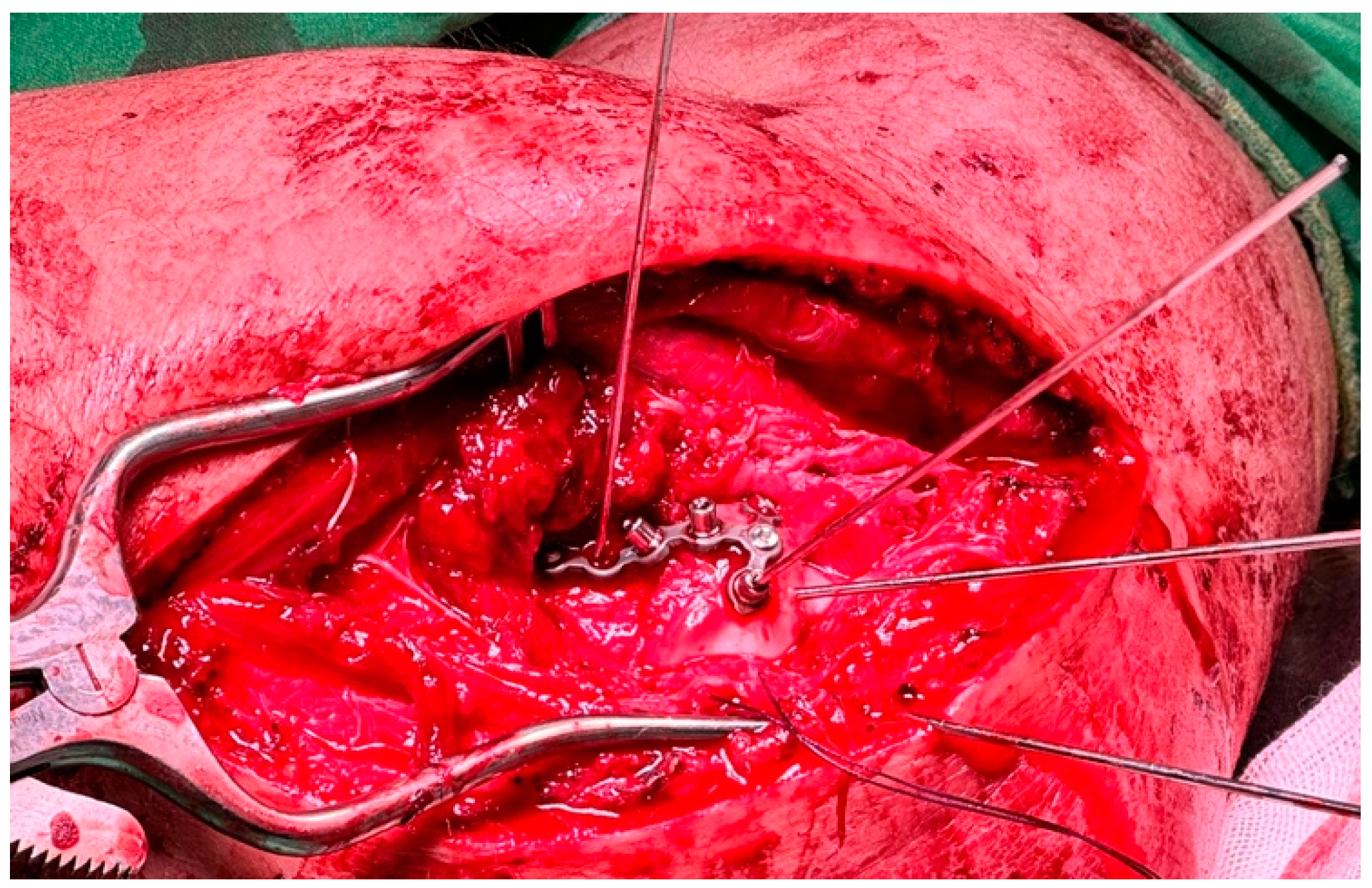
Figure 6.
The base of the lateral ulnar collateral ligament was avulsed (red circle).

Figure 7.
The relatively stable structure of proximal ulna can be fixed with posterior minimally invasive percutaneous plate osteosynthesis (MIPPO) approach.
Figure 7.
The relatively stable structure of proximal ulna can be fixed with posterior minimally invasive percutaneous plate osteosynthesis (MIPPO) approach.
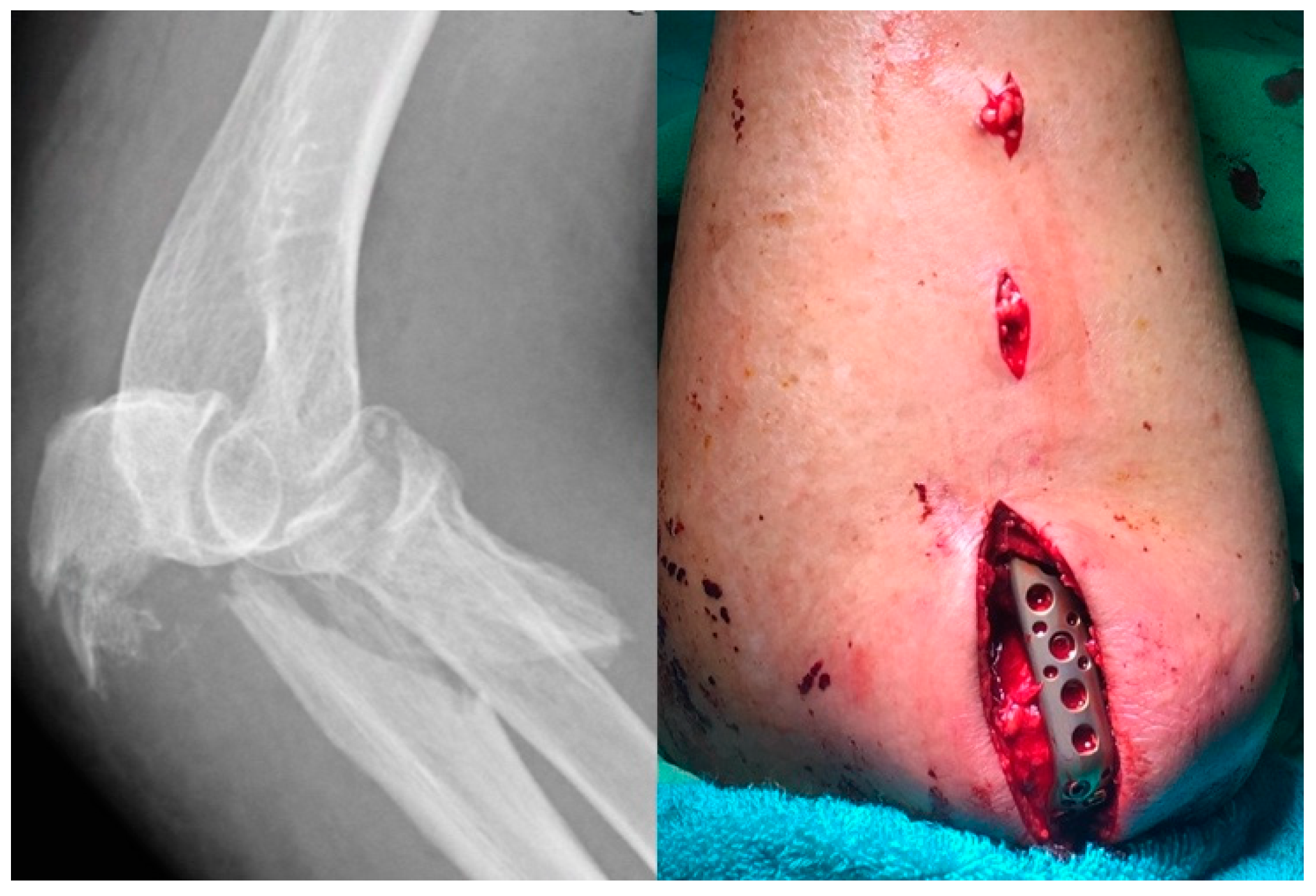
Figure 8.
The Flow Diagram about approach recommendation was established in base of defining minimal invasive surgery (MIS) as not to do cross-plane dissection. The sequence of the upmost boxes from left side to right side represents the recommended the sequence for reduction and fixation. The ulnar metaphysis and coronoid process must be fixed at the same time when the coronoid process base is unstable.
Figure 8.
The Flow Diagram about approach recommendation was established in base of defining minimal invasive surgery (MIS) as not to do cross-plane dissection. The sequence of the upmost boxes from left side to right side represents the recommended the sequence for reduction and fixation. The ulnar metaphysis and coronoid process must be fixed at the same time when the coronoid process base is unstable.
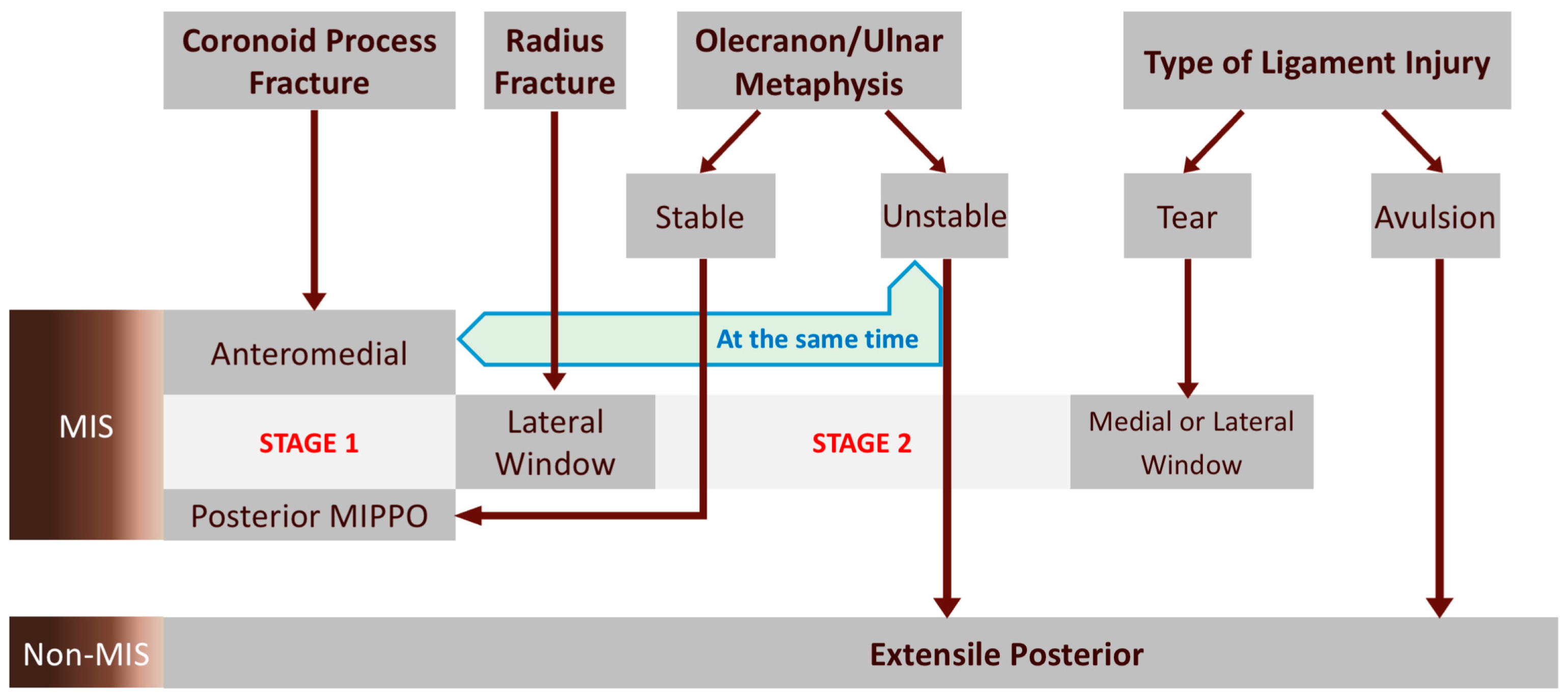

Table 1.
The schedule of post-operatively functional brace.
| Week after OP | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
| 60-90 Degrees | ||||||||||||
| 45-105 Degrees | ||||||||||||
| 30-120 Degrees | ||||||||||||
| Follow-up X-Ray |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



