
Submitted:
04 July 2024
Posted:
05 July 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Patients who survived critical COVID-19 frequently reported post-acute sequelae of COVID-19 (PASC) such as psychosomatic and neurocognitive health problems. The goal of this study was to identify clinical risk factors and other predictors for such long-term consequences in severely ill COVID-19 patients.
Adult COVID-19 intensive care unit (ICU) survivors from August 2020 to May 2021 were enrolled. A broad range of clinical, laboratory and chest computed tomography (CT) data was collected during ICU stay. The association between ICU predictors and psychosomatic, respiratory and neurocognitive assessments 12 months after ICU discharge was analyzed using univariate regression analysis.
In 17 patients (mean age 58.9 ± 11.4 years), laboratory markers (CRP, lymphocytes, hemoglobin), ICU severity (SOFA, SAPS II, need for mechanical ventilation), complications (ARDS), and lung CT data (ground-glass opacity) were promising predictors of depressive and anxiety symptoms, fatigue, and sleep problems.
Recovery of psychosomatic health such as fatigue, depression and anxiety correlated with lower levels of inflammation and high hemoglobin levels. ARDS, mechanical ventilation and worse SOFA and SAPS II scores were further risk factors for depressive and anxiety symptoms. Our study identified novel associations such as pulmonary ground-glass opacity being positively associated with depression, anxiety, fatigue, and insomnia levels.
Keywords:
COVID-19
; Intensive Unit Care
; ICU
; Predictive Model
; Psychosomatic Health
1. Introduction
The pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has pushed worldwide healthcare systems to their limits. Most affected individuals were asymptomatic or suffered from mild flu-like symptoms, while about 15-19% of Swiss patients required intensive care unit (ICU) admission in the first and second wave [1,2]. Most ICU patients had underlying comorbidities like hypertension, chronic kidney disease, congestive heart failure, type 2 diabetes mellitus or were immunocompromised [3,4].
Reports indicate that critically ill coronavirus disease 2019 (COVID-19) patients who survived the ICU stay frequently reported persistent mental health problems at 1 and 6 months after ICU discharge. Up to one-third of patients experienced moderate symptoms of anxiety and depression, alongside medium to high stress levels.4 COVID-19 survivors further showed somatic symptoms like loss of appetite, ageusia, anosmia, nausea and diarrhoea, weight- and muscle loss in post-ICU recovery [5,6]. Post-acute sequelae of COVID-19 (PASC) encompasses persistent, exacerbated, or newly occurring neuropsychological and physical symptoms following acute COVID-19 illness [7,8] These include persistent shortness of breath, reduced mobility, fatigue, and memory impairment [9] The development of PASC during or after a COVID-19 infection that persists for longer than four weeks and cannot be explained by any alternative diagnosis has been defined as long COVID. At present, the exact definition of long COVID is still evolving [10,11]. It poses a substantial challenge to healthcare systems with WHO estimating a prevalence between 10-20% [12] The elusive diagnosis and lack of treatment options for long COVID often result in referrals to multiple specialists, amplifying healthcare costs [13].
In this study, we assessed the frequency and severity of long-term complaints in a cohort of COVID-19 patients in need for ICU treatment. Further, we investigated associations between these complaints and clinical risk factors collected during the acute ICU phase. The clinical outcomes focused on psychosomatic aspects alongside respiratory and neurocognitive aspects 12 months after the initial ICU admission. The goal of this study was to identify ICU factors, in addition to pre-existing factors, that may predict 12-month follow-up outcome in severely ill COVID-19 patients.
2. Materials and Methods
2.1. Screening and Informed Consent
Adult patients (≥ 18 years) with laboratory-confirmed (polymerase chain reaction; PCR) and severe COVID-19 disease in need for ICU treatment between February 24, 2020, and March 1, 2021, were enrolled in a multicentre observational cohort study in three Swiss tertiary care hospitals [14] Exclusion criteria were COVID-19 diagnosis after ICU discharge or a lack of informed consent. All ICU survivors were invited by e-mail and phone to participate in this single-center follow-up study at the Cantonal Hospital St. Gallen.
2.2. Study Procedure and Data Collection
The survivors were investigated for long-term outcome at the Cantonal Hospital St. Gallen, a tertiary hospital in Eastern Switzerland, between August 2020 and May 2021, 12 (±1) months after ICU discharge. Informed consent was obtained from all patients. If a patient was unable to provide informed consent, proxy consent was obtained from relatives. We extracted health-related data including demographics, medical history, chest computed tomography (CT) scans, laboratory data, ICU severity scores (within the first 24h after ICU admission), complications, and treatment forms from the electronic medical records. We quantified lung CT data at ICU admission, focusing on typical COVID-19 radiological patterns such as crazy-paving, ground-glass opacity, as well as light and heavy consolidation as a relative expression of healthy lung tissue [15,16]. Concerning dietary behavior, we retrospectively assessed patients’ consumption of various food products (individual foods and food groups such as fruit, vegetables, meat, and fish) and beverages over a 4-week period at the time of COVID-19 onset with the Food Frequency Questionnaire (FFQ) originated from the University Hospitals of Geneva [17] When evaluating the FFQ, reference was made to the recommended nutritional portion of a specific food group based on Swiss recommendations.17 Patients fulfilled these recommendations with the intake of fruit (≥2/day), vegetables (≥3/day), meat (≤5/week), and fish (≥1/week). According to the overall Swiss recommendations, eating healthy means to meet at least three of the four food group recommendations mentioned above [17]
Patients completed several validated questionnaires to evaluate persistent COVID-19 symptoms, current psychosomatic health, respiratory and neurocognitive function at the Cantonal Hospital St. Gallen 12 (±1) months after ICU discharge (Table S1). Psychosomatic questionnaires were completed at the study site either in tablet or paper-pencil format with assistance of the study team, including an interpreter when necessary due to the questionnaires being in German language. Neurologists assessed neurocognitive function using validated tools, and performed clinical examinations to exclude neurodegenerative or other neurological conditions that could impair cognition. We further measured cognitive performance using both subjective (by patients) and external (by relatives) evaluation. Patients then underwent pulmonary function and exercise tolerance testing at the outpatient clinic of the Department of Pulmonary and Sleep Medicine at the Cantonal Hospital St. Gallen. We further used WatchPATTM (Itamar Medical Inc.), a portable device used for sleep monitoring and diagnosing sleep disorders, to analyze sleep architecture during a typical night’s sleep at the patients’ homes. WatchPATTM measures various parameters during sleep, including breathing rate, blood oxygen saturation, snoring, and movements, enabling comprehensive assessment of sleep patterns and identification of potential sleep-related issues [18]. See Supplemental Table S1 for all collected data 12 (±1) months after ICU discharge.

Table S1.
Assessment of clinical outcome 12 (±1) months after ICU stay.
| Psychosomatic assessment |
Insomnia Severity Index (ISI) for measuring insomnia and sleep difficulties [19] |
| Fatigue Severity Scale (FSS) for measuring fatigue [20] | |
| Patient Health Questionnaire (PHQ-SADS) for measuring depression (PHQ-9), anxiety (GAD-7), and somatic symptoms (PHQ-15) [21] | |
| Hospital Anxiety and Depression Scale (HADS) for measuring depression and anxiety [22] | |
| Impact of Event Scale-Revised (IES-R) for measuring posttraumatic stress [23] | |
| 5-Level EQ-5D version (EQ-5D-5L) for measuring quality of life [24] | |
| Respiratory assessment | Current and persisting COVID-19 symptoms |
| Pulmonary function (spirometry, plethysmography, DLCO) | |
| Exercise tolerance (6-minute walk test; 6MWT) | |
| Sleep architecture (home overnight polygraphy with WatchPATTM) [18] | |
| Neurocognitive assessment | Montreal Cognitive Assessment (MoCA) for measuring cognitive dysfunction [25] |
| Bayer Activities of Daily Living Scale (B-ADL) for measuring deficits in the performance of everyday activitie [26] | |
| Digit Symbol Substitution Test (DSST) for measuring global cognitive function, especially attention, processing speed, and executive function [27] | |
| Clinical neurological examination for detection of a cerebral or neurodegenerative disease (yes/no). Assessment of overall cognitive performance: by neurologists (normal/borderline/impaired), subjective (same/worse), and by relatives (same/worse pre-post COVID-19) |
2.3. Statistical Analyses
Our study design required a total of 55 patients for an expected 80% statistical power based on a priori power analysis with Gpower software for a simple linear regression and an expected medium effect size (Cohen’s F2) of 0.15 [28]. We imputed missing predictor data with the MICE (multiple imputation by chained equation) R package (v3.9.0) [29]. Using a strategy called multiple imputation, then deletion (MID), we used all cases for imputation of the predictor variables (X) and then excluded all cases with imputed endpoint variables (Y) from the analysis [30].
As predictor variables, we used clinical characteristics and risk factors including demographics, personal medical history, nutritional habits at COVID-19 onset, lung CT results, laboratory data, ICU severity scores, complications, and treatment forms during the ICU stay. We first analyzed clinical outcomes at the 12-month follow-up visit with a descriptive approach. Therefore, we analyzed all interval-scaled and continuous endpoints by creating nested violin-boxplots with the use of the ggplot2 R package (v3.5.1) [31]. The distributions of psychosomatic and neurocognitive score results were compared visually with established cut-off values from the literature [19,20,21,22,23,24,25,26,27]. In a second step, we performed univariate linear, logistic, and ordinal regression models to investigate the association between demographic and ICU variables and 12-month clinical outcomes. Cluster analysis was performed to identify relevant groups of associations between possible predictors and endpoints using the gplots R package (v3.1.3.1) [32]. We used R statistical software (v4.1.1) [33] and a significance level of 5% for all statistical analyses with Bonferroni correction for multiple testing [34].
3. Results
Out of 58 severely ill COVID-19 patients treated in the ICU at the Cantonal Hospital St. Gallen, 22 (~38%) died and 19 (~33%) decided not to participate in this follow-up study. A total of 17 patients (mean age 58.9 ± SD 11.4, range 35–77) were included in the cohort. Death (~38%) and lack of willingness to participate in the follow-up study (~33%) were the main reasons for the small sample size. Missing predictor variables at ICU admission consisted of lung CT data (11.8%) and laboratory data, specifically, lymphocytes (23.5%), interleukin-6 (29.4%), troponin (11.8%), NT-proBNP (17.6%), LDH (5.9%), and D-dimers (29.4%). There were no missing values concerning psychosomatic endpoints. Patients showed 17.6% and 4.8% missing values in the respiratory and neurocognitive endpoints, respectively. In detail, missing data consisted of WatchPATTM parameters and items of the MoCA test. Table 1 shows patients’ baseline characteristics symptoms at COVID-19 onset, and the collected data during ICU stay, while Table S2 shows patients’ nutritional habits at COVID-19 onset.
Table 1.
Baseline and clinical variables during ICU stay.
| PATIENT CHARACTERISTICS | CASES (N = 17) |
|---|---|
|
Demographics Male sex, n (%) |
13 (76.5) |
| Age, years, mean (SD) | 60 (11.4) |
| 18-30 years, n (%) 31-45 years, n (%) 46-60 years, n (%) 61-75 years, n (%) >75 years, n (%) |
0 (0) 2 (11.8) 7 (41.2) 8 (47) 0 (0) |
| Weight, kg, mean (SD) Height, cm, mean (SD) Body mass index (BMI), kg/m2, mean (SD) Years of primary and secondary education, mean (SD) |
90.8 (18) 172.2 (7.3) 30.5 (5.2) 11.4 (3.3) |
|
Personal medical history, n (%) Any comorbidity Hypertension Cardiovascular disease Chronic lung disease Asthma Dyslipidemia/statin use |
13 (76.5) 9 (52.9) 1 (5.9) 2 (11.8) 2 (11.8) 3 (17.6) |
|
Symptoms at COVID-19 onset, n (%) Fever Cough Headache Night sweats Chills Shivering Myalgia Joint pain Dyspnea Inspiratory chest pain Retrosternal chest pain Loss of appetite Weight loss |
10 (58.8) 13 (76.5) 11 (64.7) 9 (52.9) 10 (58.8) 10 (58.8) 8 (47.1) 8 (47.1) 9 (52.9) 10 (58.8) 9 (52.9) 10 (58.8) 8 (47.1) |
|
Findings on lung CT scans at ICU admission, mean (SD) Ground-glass opacity in % of normal lung Crazy-paving in % of normal lung Light consolidation in % of normal lung Heavy consolidation in % of normal lung |
39.0 (4.3) 26.9 (5.8) 8.0 (4.1) 0.4 (0.2) |
| Laboratory data at ICU admission, mean (SD) | |
| Hemoglobin in g/l Thrombocytes in G/l1 Troponin in ng/l2 NT-proBNP in ng/l Creatinine in umol/l3 Bilirubin in umol/l CRP in mg/l Leukocytes in G/l Interleukin-6 in pg/ml4 Lymphocytes in G/l D-dimers in ng/ml LDH in IU/l |
128.4 (18.2) 271.1 (117.2) 30.5 (49.7) 758.6 (615.7) 73.2 (24.4) 9.3 (6.1) 208.1 (93.6) 10.2 (3.6) 103.9 (119.3) 0.9 (0.5) 2045 (1384.5) 602.6 (224.8) |
| Clinical scores, syndromes and complications during ICU stay | |
| Admission SOFA5 score (SD) Discharge SOFA score (SD) Admission SAPS6 II (SD) Hospital-acquired pneumonia (HAP) more than 48h after hospital admission, n (%) Community-acquired pneumonia (CAP) at hospital admission or within 48h (other than COVID-19), n (%) Acute confusional syndrome, n (%) Acute respiratory distress syndrome (ARDS), n (%) Other complications (acute kidney/hepatic injury, septic shock), n (%) Partial arterial oxygen pressure (PaO2) in mmHg (mean, SD) Fraction of inspired oxygen (FiO2) in % (mean, SD) Highest body temperature in °C (mean, SD) ICU stay duration in days (mean, SD) Hospital stay duration in days (mean, SD) Intubation duration in mechanically ventilated patients in days (mean, SD) |
5.8 (3.4) 2.5 (0.9) 33.6 (12.7) 3 (17.6) 2 (11.8) 5 (29.4) 10 (58.8) 3 (17.6) 59.3 (8.0) 53.1 (18.4) 38.2 (0.8) 13 (9.5) 23 (12.6) 10 (4.1) |
|
ICU treatment, n (%) Corticosteroid treatment Noradrenalin treatment Prophylactic LMW heparin Low-flow oxygen treatment Non-invasive ventilation (NIV) Mechanical ventilation Extracorporeal membrane oxygenation (ECMO) Intubation Prone position ventilation Tracheostomy Hemofiltration/hemodialysis |
15 (88.2) 5 (29.4) 12 (70.6) 3 (17.6) 5 (29.4) 7 (41.2) 2 (11.8) 9 (52.9) 8 (47.1) 3 (17.6) 0 (0) |
Table S2.
Dietary behavior assessed with the FFQ questionnaire.
|
Nutritional habits at COVID-19 onset Fruit OK (≥2/day) Vegetables OK (≥3/day) Meat OK (≤5/week) Fish OK (≥1/week) Swiss recommendations OK (≥3 of the 4 recommendations above) |
9 (52.9%) 6 (35.3%) 9 (52.9%) 8 (47.1%) 6 (35.3%) |
12 (±1) months after ICU discharge, the most frequently reported symptoms were persisting cough (76.5%), headaches (64.7%) as well as anosmia, dysgeusia and loss of appetite in 58.8% of patients. When considering established cut-off points, very few patients showed score values for psychosomatic and neurocognitive diseases at the 12-month follow-up visit. Figure 1 provides a summary of the descriptive statistical analysis of all endpoints.
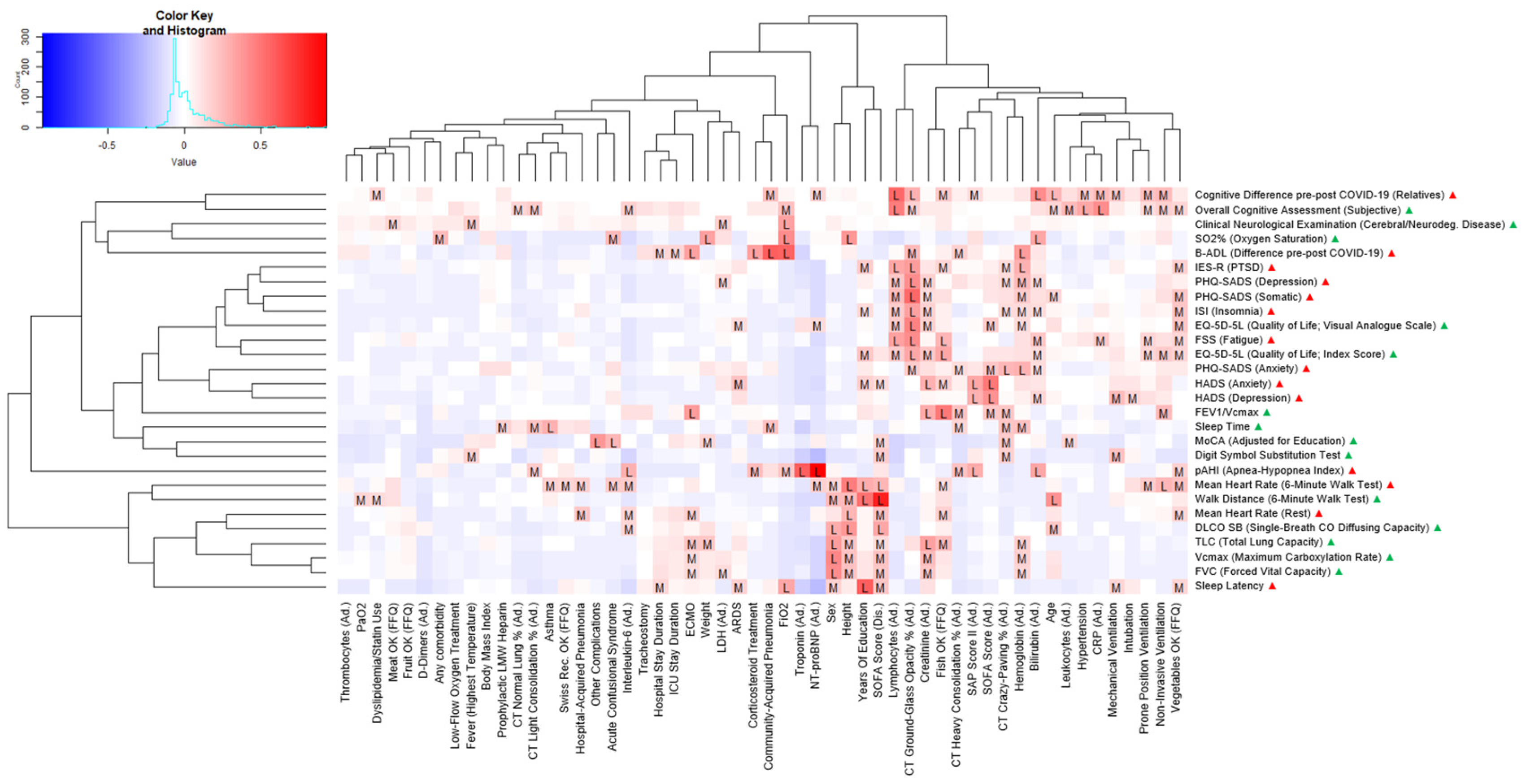
Our sample size of 17 patients provided an actual statistical power of 32% based on a post-hoc power analysis with Gpower software for a simple linear regression and an expected medium effect size (Cohen’s F2) of 0.15 [28]. Based on univariate linear, logistic, and ordinal regression analyses, we identified several variables associated with long-term outcomes. However, these findings did not remain statistically significant after Bonferroni adjustment for multiple testing. Figure 2 and Figure 3 show two heatmaps representing p-values and effect sizes in order to illustrate health clusters between predictors and associated endpoints. The following two examples illustrate how to read the figures: A high CRP was positively correlated with a higher score in the FSS questionnaire indicating worse fatigue in a statistically relevant way with a medium effect size (adjusted R2). Extracorporeal membrane oxygenation (ECMO) was negatively associated with total lung capacity (TLC) in a statistically relevant way and was therefore associated with a smaller lung capacity with a medium effect size (adjusted R2).
Inflammatory or infectious (CRP, lymphocytes), cardiac (troponin, NT-proBNP), renal (creatinine), and hematologic (hemoglobin) markers were among the most promising predictors. Other relevant predictors consisted of ICU clinical severity (SOFA, SAPS II, need for mechanical ventilation), complications (ARDS), and lung CT data (ground-glass opacity). The main endpoints associated with these predictors were psychosomatic outcome measures (fatigue, depressive, and anxiety symptoms) and sleep problems (sleep apnea, insomnia). In particular, higher levels of inflammation (CRP, lymphocytes) predicted worse outcome of fatigue, depression, and anxiety. The presence of ARDS and worse ICU severity scores (SOFA, SAPS II) were further predictors for worse depression and anxiety symptoms. The need for mechanical ventilation was significantly associated with higher depression scores. Concerning these affective symptoms, high hemoglobin and creatinine levels were associated with a better outcome. Cardiac makers (troponin, NT-proBNP) were further positively associated with sleep apnea. Ground-glass opacity in the lung CT scans was positively associated with depression, anxiety, fatigue, and insomnia levels and an overall impairment of quality of life.
4. Discussion
Our study provides several main results. The higher the disease severity in the acute phase of COVID-19, the more likely patients in need for ICU treatment will suffer from long-term sequelae. Higher levels of inflammatory markers, higher ICU severity scores and markers of organ dysfunction – e.g., the need for mechanical ventilation, more ground-glass opacities in the lung CT scan, presence of ARDS and elevated cardiac biomarkers – were associated with worse outcome of fatigue and affective symptoms such as depression and anxiety. While higher hemoglobin and creatinine levels seemed to be protective factors for those.
Multiple neurological, cardiopulmonary, gastrointestinal, and dermatological symptoms, described as the multiorgan phenotype (MOP) of acute COVID-19, were linked to an elevated risk of protracted recovery.9 When hospitalization was required, Evans and colleagues7 identified female sex, obesity, and invasive mechanical ventilation in COVID-19 patients as associated with lower likelihood to recover full quality of life with a substantial deficit in median EQ-5D-5L index score at one year after discharge. They further found a correlation between increased inflammatory mediators (including interleukin-6) and cognitive impairment at 5 months, emphasizing the idea of persistent systemic inflammation and its consequences on cognitive performance.7 In our study, we confirmed the association of inflammatory markers (CRP, lymphocytes) with fatigue and affective symptoms. Irwin, Olmstead and Carroll [35] concluded that there is a growing body of evidence linking sleep disturbances to the risk of inflammatory diseases and all-cause mortality, possibly through effects of sleep disturbances on two systemic inflammatory markers (CRP, interleukin-6). Our results showed the same relation as CRP (but not interleukin-6) positively predicted fatigue, however with a small effect size. Recently a correlation was shown between higher CRP in the general population and reduced sleep quality and increased fatigue, corroborating our findings. [36,37,38,39,40] Al-Hakeim et al. [41] mentioned the significant role of activated immune-inflammatory and oxidative and nitrosative stress (IO&NS) pathways in determining the long-term outcome of a COVID-19 infection. Chronic fatigue syndrome (CFS), major depression (MD), and generalized anxiety disorder (GAD) are all characterized by activated IO&NS pathways and increased levels of inflammatory mediators, including CRP [37]. Six months or more after SARS-CoV-2 infection, elevated CRP levels are significantly associated with concomitant fatigue severity [42]. In contrast to the positive correlation observed between elevated lymphocyte levels and fatigue in our study, Swanink et al. [43] did not find any significant changes in absolute lymphocyte counts among patients with chronic fatigue syndrome (CFS) and the control group. However, aligning with our findings, Zheng et al. [44] described low levels of lymphocytes in acutely infected COVID-19 patients.
Similar to our study, Naudé et al. [45]. described a correlation between elevated CRP levels and depression as well as generalized anxiety disorder. Furthermore, Azevedo et al. [46] demonstrated that patients who suffered from both SARS-CoV-2 infection and major depression showed notably higher CRP levels compared to COVID-19 patients without concurrent depression. It is plausible that inflammatory markers may help predicting the long-term mental health outcome of COVID-19 and identify patients with fatigue and affective disorders.
One severe complication of the SARS-CoV-2 virus is acute respiratory distress syndrome (ARDS), which affected more than half of our patients. In our analysis, presence of ARDS predicted 12-month anxiety. A multi-site, longitudinal cohort study found that ARDS survivors experienced persistent psychiatric issues, anxiety, depression, and posttraumatic stress disorder [47]. Palakshappa et al. [48] reported similar outcomes involving 629 patients from three different trials with a significant proportion of ARDS survivors having substantial mental health symptoms. The prevalence of substantial symptoms of depression, anxiety, and PTSD at 6 months reached 36%, 42%, and 24%, respectively. Our study revealed a significant association between mechanical ventilation, the presence of ARDS, and depressive symptoms. Pre-pandemically, depressive symptoms one year after discharge had been reported in ICU survivors of mechanical ventilation, but to our knowledge not previously described in COVID-19 [49].
It is widely recognized that anemia can lead to symptoms such as fatigue, irritability, and concentration problems, which are often associated with depression components. However, findings from a large cohort study conducted by Lever van Milligen et al. [50] and another study by Chen et al. [51] failed to provide significant evidence of a direct connection between depression, anxiety, and hemoglobin levels. In a study by Jackowsa et al. [52] a positive relationship between hemoglobin levels and sleep duration was observed. Our data showed that higher hemoglobin levels were associated with lower scores in depression and anxiety questionnaires. Concerning protective factors against depression and anxiety, our data further identified higher levels of creatinine being associated with lower depression scores. The scientific evidence on the correlation between creatinine and affective symptoms such as depression or anxiety is sparse and incongruent. One study by Ibrahim et al. [53] reported no association between creatinine and depression, while a study by Ogrizovic et al. [54] found a positive correlation between creatinine and depression. The findings of Bossola et al. [55] showed that patients with lower creatinine were more depressed.
Concerning the Sepsis-Related Organ Failure Assessment (SOFA) score at ICU admission, we observed elevated scores for both HADS scores, assessing anxiety and depression, along with a low self-assessment of current health in our patients. This correlation is plausible, as the prolonged ICU stay, poor and critical condition as well as the uncertainty and anxiety experienced by the patients directly impact mental health. [56] Similar findings emerged in evaluating the Simplified Acute Physiology Score (SAPS) II even outside of COVID-19. [57] The lung diffusion capacity 12-months after ICU stay was reduced in patients with an elevated SOFA score at ICU discharge. This is likely multifactorial including pulmonary edema, which decreases the gas exchange surface area and consequently lowers DLCO, inflammation and subsequent fibrosis. [57]
In our study, both heart failure markers troponin and NT-proBNP positively predicted higher Apnoea-Hypopnoea Index (pAHI) scores with large effect sizes. Sasaki et al. [58] demonstrated a correlation between elevated NT-proBNP levels and sleep difficulties, as well as short sleep duration, which aligns with our findings. Several studies have reported that poor sleep is a risk factor for coronary heart disease and stroke. [59,60,61] However, there are limited data regarding the association between poor sleep and heart failure. Laugsand et al. [62] stated a positive relationship between the number of insomnia symptoms, namely the difficulty initiating or maintaining sleep and having nonrestorative sleep, and heart failure. Concerning sleep apnea, Hübner et al. [63] and Tasci et al. [64] found no correlation between changes in NT-proBNP and the pAHI as measured by the WatchPATTM which contrasts with our findings of a positive prediction. In contrast, Vartany et al. [65] found no correlations between the evening baseline or post-sleep NT-proBNP levels and obstructive sleep apnea syndrome (OSAS). Lazzarino et al. [66] reported that certain individuals, when exposed to intense stress or exhibiting exaggerated stress responses, release both inflammatory factors and cardiac troponin in response. This observation mirrors the elevated troponin levels in stress-induced Takotsubo cardiomyopathy [67,68]. Several studies have further demonstrated an association between sleep apnea and increased troponin levels. However, this association lost statistical significance after adjusting for cardiovascular risk factors [69,70].
In analyzing our lung CT data, ground-glass opacity showed notable associations with some endpoints. Patients with pulmonary ground-glass opacity scored worse in depression, anxiety, fatigue, and insomnia questionnaires. In addition, these patients experienced an overall lower quality of life. Compared with initial lung CT scans, 78% of the COVID-19 hospital survivors still had some pulmonary ground-glass opacity showing up on lung scans at a one-year follow-up [71]. These residual lesions are further associated with lower peripheral oxygen saturation as it was the case in our patients [72]. To our knowledge our study is the first to describe pulmonary ground-glass opacity as predictor of depression, anxiety, fatigue, and insomnia scores.
This study has several limitations. Most importantly, the small sample size of 17 patients resulted in a low statistical power. Therefore, the results have to be interpreted cautiously. Secondly, despite having pre-post COVID-19 difference scores for several neurocognitive endpoints (e.g., B-ADL, external cognitive assessment), other endpoints lacked a pre-COVID-19 reference value. For instance, we had no data on the psychosomatic or respiratory health prior to the COVID-19 and ICU stay, e.g., depressive symptoms or 6-minute walk test performance. Conversely, the strengths of our study consisted of a broad range of interdisciplinary predictors and endpoints using detailed validated questionnaires as well as the identification of novel associations between ICU factors and relevant long-term health outcomes in COVID-19.
5. Conclusions
The cumulative prevalence of critically-ill COVID-19 survivors reporting at least one persisting symptom four months after recovery was as high as 45%, particularly for fatigue and weakness [73]. High levels of inflammatory or cardiac injury parameters, need for mechanical ventilation and presence of ARDS or ground-glass opacity may identify subgroups of COVID-19 patients who deserve close follow-up regarding long-term psychological well-being and quality of life. Our results contribute towards a better understanding of the mechanisms underlying the long-term risk profile of COVID-19 but – given the small sample size – should be interpreted rather as hypothesis generating.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, W.C.A., D.A.S., and C.R.K.; Methodology, W.C.A., N.G., K.G.F., T.Fi., G.R.K, M.Fr., M.H.B., and D.A.S.; Software, N.G.; Validation, G.R.K, U.P., M.Fr., M.H.B., D.A.S., and W.C.A.; Formal Analysis, N.G. and D.A.; Investigation, D.A., K.G.F., T.Fi., and T.Fr.; Resources, W.C.A., G.R.K, U.P., M.Fi., M.H.B., T.Fr., M.B., and D.A.S.; Data Curation, N.G. and D.A.; Writing – Original Draft Preparation, N.G., D.A., and W.C.A.; Writing – Review & Editing, W.C.A., D.A.S., M.Fr., M.B., and T.Fi.; Visualization, N.G.; Supervision, W.C.A. and D.A.S.; Project Administration, W.C.A. and D.A.S.; Funding Acquisition, W.C.A., G.R.K., U.P., M.H.B., and D.A.S. Reading and approval of final manuscript: All authors.
Funding
This research was funded by intramural grants from the Cantonal Hospital St. Gallen (20/13 and 21/18; to W.C.A).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Eastern Switzerland (EKOS) (BASEC Nr. EKOS 20/058).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
First: we thank all patients, relatives, and healthcare workers involved in the treatment of COVID-19 patients during the course of the study and the pandemic as a whole, including Cornelia Knapp, Susanne Nigg, Thomas Egger, Andrea Blöchlinger, Tia Wisser, Melanie Gätzi, Patrick Münger, and Gianina Toller (Cantonal Hospital St. Gallen). We further thank Natacha Noël and Julien Lamour for their support regarding the Food Frequency Questionnaire (FFQ).
Conflicts of Interest
W.C.A. received funding from Swiss National Science Foundation (33IC30_201300), Cantonal Hospital St. Gallen, OM Pharma, FUNGINOS, and Gilead. Payment for lectures and presentations: Pfizer, GSK, MSD, and Gilead; paid to his institution. Payment for travel to meetings: Pfizer, GSK, and Gilead; paid to his institution. Participation at Advisory Boards: MSD, Sanofi, Pfizer, GSK, OM Pharma, and Janssen; paid to his institution.
| 1 | 109/l (giga/l) |
| 2 | 109 gram/l (nanogram/l) |
| 3 | 106 mol/l (micromole/l) |
| 4 | 1012 gram/ml (picogram/ml) |
| 5 | Sequential organ failure assessment score |
| 6 | Simplified acute physiology score |
References
- Eythorsson, E.; Helgason, D.; Ingvarsson, R. F.; Bjornsson, H. K.; Olafsdottir, L. B.; Bjarnadottir, V.; Runolfsdottir, H. L.; Bjarnadottir, S.; Agustsson, A. S.; Oskarsdottir, K.; Thorvaldsson, H. H.; Kristjansdottir, G.; Armannsdottir, B.; Bjarnason, A.; Johannsson, B.; Gudlaugsson, O.; Gottfredsson, M.; Sigurdsson, M. I.; Indridason, O. S.; Palsson, R. Clinical Spectrum of Coronavirus Disease 2019 in Iceland: Population Based Cohort Study. BMJ 2020, 371, m4529. [Google Scholar] [CrossRef]
- Anderegg, N.; Panczak, R.; Egger, M.; Low, N.; Riou, J. Survival among People Hospitalized with COVID-19 in Switzerland: A Nationwide Population-Based Analysis. BMC Med 2022, 20, 164. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; Cheng, Z.; Yu, T.; Xia, J.; Wei, Y.; Wu, W.; Xie, X.; Yin, W.; Li, H.; Liu, M.; Xiao, Y.; Gao, H.; Guo, L.; Xie, J.; Wang, G.; Jiang, R.; Gao, Z.; Jin, Q.; Wang, J.; Cao, B. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Carola, V.; Vincenzo, C.; Morale, C.; Pelli, M.; Rocco, M.; Nicolais, G. Psychological Health in COVID-19 Patients after Discharge from an Intensive Care Unit. Front Public Health 2022, 10, 951136. [Google Scholar] [CrossRef] [PubMed]
- Aguila, E. J. T.; Lontok, M. A. D.; Francisco, C. P. D. Follow Your Gut: Challenges in Nutritional Therapy During the COVID-19 Pandemic. Clin Gastroenterol Hepatol 2020, 18, 2638–2639. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Bischoff, S. C.; Breda, J.; Wickramasinghe, K.; Krznaric, Z.; Nitzan, D.; Pirlich, M.; Singer, P.; endorsed by the ESPEN Council. ESPEN Expert Statements and Practical Guidance for Nutritional Management of Individuals with SARS-CoV-2 Infection. Clin Nutr 2020, 39, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- PHOSP-COVID Collaborative Group. Clinical Characteristics with Inflammation Profiling of Long COVID and Association with 1-Year Recovery Following Hospitalisation in the UK: A Prospective Observational Study. Lancet Respir Med 2022, 10, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zang, C.; Xu, Z.; Zhang, Y.; Xu, J.; Bian, J.; Morozyuk, D.; Khullar, D.; Zhang, Y.; Nordvig, A. S.; Schenck, E. J.; Shenkman, E. A.; Rothman, R. L.; Block, J. P.; Lyman, K.; Weiner, M. G.; Carton, T. W.; Wang, F.; Kaushal, R. Data-Driven Identification of Post-Acute SARS-CoV-2 Infection Subphenotypes. Nat Med 2023, 29, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Sahanic, S.; Tymoszuk, P.; Ausserhofer, D.; Rass, V.; Pizzini, A.; Nordmeyer, G.; Hüfner, K.; Kurz, K.; Weber, P. M.; Sonnweber, T.; Boehm, A.; Aichner, M.; Cima, K.; Boeckle, B.; Holzner, B.; Rumpold, G.; Puelacher, C.; Kiechl, S.; Huber, A.; Wiedermann, C. J.; Sperner-Unterweger, B.; Tancevski, I.; Bellmann-Weiler, R.; Bachler, H.; Piccoliori, G.; Helbok, R.; Weiss, G.; Loeffler-Ragg, J. Phenotyping of Acute and Persistent Coronavirus Disease 2019 Features in the Outpatient Setting: Exploratory Analysis of an International Cross-Sectional Online Survey. Clinical Infectious Diseases 2022, 75, e418–e431. [Google Scholar] [CrossRef] [PubMed]
- CDC. Post-COVID Conditions. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 12 May 2024).
- Soriano, J. B.; Murthy, S.; Marshall, J. C.; Relan, P.; Diaz, J. V.; WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. Lancet Infect Dis 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus disease (COVID-19): Post COVID-19 condition. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-post-covid-19-condition (accessed on 12 May 2024).
- Pfaff, E. R.; Girvin, A. T.; Bennett, T. D.; Bhatia, A.; Brooks, I. M.; Deer, R. R.; Dekermanjian, J. P.; Jolley, S. E.; Kahn, M. G.; Kostka, K.; McMurry, J. A.; Moffitt, R.; Walden, A.; Chute, C. G.; Haendel, M. A.; Consortium, T. N. Who Has Long-COVID? A Big Data Approach [Preprint]. medRxiv 2021. [Google Scholar] [CrossRef]
- Albrich, W. C.; Ghosh, T. S.; Ahearn-Ford, S.; Mikaeloff, F.; Lunjani, N.; Forde, B.; Suh, N.; Kleger, G.-R.; Pietsch, U.; Frischknecht, M.; Garzoni, C.; Forlenza, R.; Horgan, M.; Sadlier, C.; Negro, T. R.; Pugin, J.; Wozniak, H.; Cerny, A.; Neogi, U.; O’Toole, P. W.; O’Mahony, L. A High-Risk Gut Microbiota Configuration Associates with Fatal Hyperinflammatory Immune and Metabolic Responses to SARS-CoV-2. Gut Microbes 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Fischer, T.; Baz, Y. E.; Scanferla, G.; Graf, N.; Waldeck, F.; Kleger, G.-R.; Frauenfelder, T.; Bremerich, J.; Kobbe, S. S.; Pagani, J.-L.; Schindera, S.; Conen, A.; Wildermuth, S.; Leschka, S.; Strahm, C.; Waelti, S.; Dietrich, T. J.; Albrich, W. C. Comparison of Temporal Evolution of Computed Tomography Imaging Features in COVID-19 and Influenza Infections in a Multicenter Cohort Study. European Journal of Radiology Open 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Goyal, N.; Chung, M.; Bernheim, A.; Keir, G.; Mei, X.; Huang, M.; Li, S.; Kanne, J. P. Computed Tomography Features of Coronavirus Disease 2019 (COVID-19): A Review for Radiologists. J Thorac Imaging 2020, 35, 211–218. [Google Scholar] [CrossRef] [PubMed]
- De Abreu, D.; Guessous, I.; Vaucher, J.; Preisig, M.; Waeber, G.; Vollenweider, P.; Marques-Vidal, P. Low Compliance with Dietary Recommendations for Food Intake among Adults. Clin Nutr 2013, 32, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Pang, K. P.; Gourin, C. G.; Terris, D. J. A Comparison of Polysomnography and the WatchPAT in the Diagnosis of Obstructive Sleep Apnea. Otolaryngol Head Neck Surg 2007, 137, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Morin, C. M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Valko, P. O.; Bassetti, C. L.; Bloch, K. E.; Held, U.; Baumann, C. R. Validation of the Fatigue Severity Scale in a Swiss Cohort. Sleep 2008, 31, 1601–1607. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R. L.; Williams, J. B. W.; Löwe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A Systematic Review. Gen Hosp Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A. S., & Snaith. The Hospital Anxiety and Depression Scale, 1983. [CrossRef]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of Event Scale: A Measure of Subjective Stress. Psychosom Med 1979, 41, 209–218. [Google Scholar] [CrossRef] [PubMed]
- EQ-5D-5L – EQ-5D. https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/ (accessed 2023-12-04).
- Nasreddine, Z. S.; Phillips, N. A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J. L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J Am Geriatr Soc 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Hindmarch, I.; Lehfeld, H.; de Jongh, P.; Erzigkeit, H. The Bayer Activities of Daily Living Scale (B-ADL). Dement Geriatr Cogn Disord 1998, 9 Suppl 2, 20–26. [Google Scholar] [CrossRef]
- Jaeger, J. Digit Symbol Substitution Test: The Case for Sensitivity Over Specificity in Neuropsychological Testing. J Clin Psychopharmacol 2018, 38, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Erdfelder, E.; Faul, F.; Buchner, A. GPOWER: A General Power Analysis Program. Behavior Research Methods, Instruments, & Computers 1996, 28, 1–11. [Google Scholar] [CrossRef]
- Buuren, S. V.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Soft. 2011, 45. [Google Scholar] [CrossRef]
- Von Hippel, P. T. 4. Regression with Missing Ys: An Improved Strategy for Analyzing Multiply Imputed Data. Sociological Methodology 2007, 37, 83–117. [Google Scholar] [CrossRef]
- Wickham, H. (2016). Ggplot2: Elegant Graphics for Data Analysis. https:\ggplot2.tidyverse.o.
- Warnes, Maintainer Gregory R., et al. “Package ‘Gplots’.” Various R Programming Tools for Plotting Data.
- Team, R. R: A Language and Environment for Statistical Computing. MSOR connections 2014. [Google Scholar]
- Armstrong, R. A. When to Use the Bonferroni Correction. Ophthalmic and Physiological Optics 2014, 34, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M. R.; Olmstead, R.; Carroll, J. E. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Gaines, J.; Vgontzas, A. N.; Fernandez-Mendoza, J.; He, F.; Calhoun, S. L.; Liao, D.; Bixler, E. O. Increased Inflammation from Childhood to Adolescence Predicts Sleep Apnea in Boys: A Preliminary Study. Brain Behav Immun 2017, 64, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Jokela, M.; Virtanen, M.; Batty, G. D.; Kivimäki, M. Inflammation and Specific Symptoms of Depression. JAMA Psychiatry 2016, 73, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Orre, I. J.; Reinertsen, K. V.; Aukrust, P.; Dahl, A. A.; Fosså, S. D.; Ueland, T.; Murison, R. Higher Levels of Fatigue Are Associated with Higher CRP Levels in Disease-Free Breast Cancer Survivors. J Psychosom Res 2011, 71, 136–141. [Google Scholar] [CrossRef]
- Cho, H. J.; Seeman, T. E.; Bower, J. E.; Kiefe, C. I.; Irwin, M. R. Prospective Association between C-Reactive Protein and Fatigue in the Coronary Artery Risk Development in Young Adults Study. Biol Psychiatry 2009, 66, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Karshikoff, B.; Sundelin, T.; Lasselin, J. Role of Inflammation in Human Fatigue: Relevance of Multidimensional Assessments and Potential Neuronal Mechanisms. Front Immunol 2017, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Al-Hakeim, H. K.; Al-Rubaye, H. T.; Al-Hadrawi, D. S.; Almulla, A. F.; Maes, M. Long-COVID Post-Viral Chronic Fatigue and Affective Symptoms Are Associated with Oxidative Damage, Lowered Antioxidant Defenses and Inflammation: A Proof of Concept and Mechanism Study. Molecular Psychiatry 2023, 28, 564–578. [Google Scholar] [CrossRef] [PubMed]
- Hartung, T. J.; Neumann, C.; Bahmer, T.; Chaplinskaya-Sobol, I.; Endres, M.; Geritz, J.; Haeusler, K. G.; Heuschmann, P. U.; Hildesheim, H.; Hinz, A.; Hopff, S.; Horn, A.; Krawczak, M.; Krist, L.; Kudelka, J.; Lieb, W.; Maetzler, C.; Mehnert-Theuerkauf, A.; Montellano, F. A.; Morbach, C.; Schmidt, S.; Schreiber, S.; Steigerwald, F.; Störk, S.; Maetzler, W.; Finke, C. Fatigue and Cognitive Impairment after COVID-19: A Prospective Multicentre Study. EClinicalMedicine 2022, 53, 101651. [Google Scholar] [CrossRef] [PubMed]
- Swanink, C. M.; Vercoulen, J. H.; Galama, J. M.; Roos, M. T.; Meyaard, L.; van der Ven-Jongekrijg, J.; de Nijs, R.; Bleijenberg, G.; Fennis, J. F.; Miedema, F.; van der Meer, J. W. Lymphocyte Subsets, Apoptosis, and Cytokines in Patients with Chronic Fatigue Syndrome. J Infect Dis 1996, 173, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional Exhaustion of Antiviral Lymphocytes in COVID-19 Patients. Cell Mol Immunol 2020, 17, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Naudé, P. J. W.; Roest, A. M.; Stein, D. J.; de Jonge, P.; Doornbos, B. Anxiety Disorders and CRP in a Population Cohort Study with 54,326 Participants: The LifeLines Study. World J Biol Psychiatry 2018, 19, 461–470. [Google Scholar] [CrossRef] [PubMed]
- De Azevedo Cardoso, T.; Silva, R. H.; Fernandes, J. L.; Arent, C. O.; Amboni, G.; Borba, L. A.; Padilha, A. P. Z.; Botelho, M. E. M.; Maciel, A. L.; Barichello, T.; Morales, R.; Soares, S. J. B.; Bagatini, M. D.; Dallagnol, C.; Brighenti, M. E.; Ignácio, Z. M.; Quevedo, J.; Ceretta, L. B.; Réus, G. Z. Stress Levels, Psychological Symptoms, and C-Reactive Protein Levels in COVID-19: A Cross-Sectional Study. J Affect Disord 2023, 330, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Bienvenu, O. J.; Friedman, L. A.; Colantuoni, E.; Dinglas, V. D.; Sepulveda, K. A.; Mendez-Tellez, P.; Shanholz, C.; Pronovost, P. J.; Needham, D. M. Psychiatric Symptoms after Acute Respiratory Distress Syndrome: A 5-Year Longitudinal Study. Intensive Care Med 2018, 44, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Palakshappa, J. A.; Krall, J. T. W.; Belfield, L. T.; Files, D. C. Long-Term Outcomes in Acute Respiratory Distress Syndrome: Epidemiology, Mechanisms, and Patient Evaluation. Crit Care Clin 2021, 37, 895–911. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.; Tomlinson, G.; Chu, L.; Robles, P.; Matte, A.; Burns, S.; Thomas, C.; Lamontagne, F.; Adhikari, N. K. J.; Ferguson, N.; Friedrich, J. O.; Rudkowski, J. C.; Skrobik, Y.; Meggison, H.; Cameron, J.; Herridge, M.; Herridge, M. S.; Chu, L. M.; Matte, A.; Tomlinson, G.; Chan, L.; Thomas, C.; Friedrich, J. O.; Mehta, S.; Lamontagne, F.; Levasseur, M.; Ferguson, N. D.; Adhikari, N. K. J.; Rudkowski, J. C.; Meggison, H.; Skrobik, Y.; Flannery, J.; Bayley, M.; Batt, J.; Santos, C. dos; Abbey, S. E.; Tan, A.; Lo, V.; Mathur, S.; Parotto, M.; Morris, D.; Flockhart, L.; Fan, E.; Lee, C. M.; Wilcox, M. E.; Ayas, N.; Choong, K.; Fowler, R.; Scales, D. C.; Sinuff, T.; Cuthbertson, B. H.; Rose, L.; Robles, P.; Burns, S.; Cypel, M.; Singer, L.; Chaparro, C.; Chow, C.-W.; Keshavjee, S.; Brochard, L.; Hebert, P.; Slutsky, A. S.; Marshall, J. C.; Cook, D.; Cameron, J. I. Determinants of Depressive Symptoms at 1 Year Following ICU Discharge in Survivors of ≥ 7 Days of Mechanical Ventilation: Results From the RECOVER Program, a Secondary Analysis of a Prospective Multicenter Cohort Study. Chest 2019, 156, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Lever-van Milligen, B. A.; Vogelzangs, N.; Smit, J. H.; Penninx, B. W. J. H. Hemoglobin Levels in Persons with Depressive and/or Anxiety Disorders. J Psychosom Res 2014, 76, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-H.; Yeh, H.-L.; Tsai, S.-J. Association of Lower Hemoglobin Levels with Depression, Though Not with Cognitive Performance, in Healthy Elderly Men. Psychiatry Clin Neurosci 2012, 66, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Jackowska, M.; Kumari, M.; Steptoe, A. Sleep and Biomarkers in the English Longitudinal Study of Ageing: Associations with C-Reactive Protein, Fibrinogen, Dehydroepiandrosterone Sulfate and Hemoglobin. Psychoneuroendocrinology 2013, 38, 1484–1493. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.; El Salamony, O. Depression, Quality of Life and Malnutrition-Inflammation Scores in Hemodialysis Patients. Am J Nephrol 2008, 28, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Simic Ogrizovic, S.; Jovanovic, D.; Dopsaj, V.; Radovic, M.; Sumarac, Z.; Bogavac, S. N.; Stosovic, M.; Stanojevic, M.; Nesic, V. Could Depression Be a New Branch of MIA Syndrome? Clin Nephrol 2009, 71, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Bossola, M.; Ciciarelli, C.; Di Stasio, E.; Conte, G. L.; Vulpio, C.; Luciani, G.; Tazza, L. Correlates of Symptoms of Depression and Anxiety in Chronic Hemodialysis Patients. Gen Hosp Psychiatry 2010, 32, 125–131. [Google Scholar] [CrossRef]
- Ringdal, M.; Plos, K.; Lundberg, D.; Johansson, L.; Bergbom, I. Outcome after Injury: Memories, Health-Related Quality of Life, Anxiety, and Symptoms of Depression after Intensive Care. J Trauma 2009, 66, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Mazeraud, A.; Polito, A.; Sivanandamoorthy, S.; Porcher, R.; Heming, N.; Stoclin, A.; Hissem, T.; Antona, M.; Blot, F.; Gaillard, R.; Chrétien, F.; Annane, D.; Bozza, F. A. B.; Siami, S.; Sharshar, T.; Groupe d’Explorations Neurologiques en Réanimation (GENER). Association Between Anxiety and New Organ Failure, Independently of Critical Illness Severity and Respiratory Status: A Prospective Multicentric Cohort Study. Crit Care Med 2020, 48, 1471–1479. [Google Scholar] [CrossRef]
- Sasaki, N.; Yamamoto, H.; Ozono, R.; Maeda, R.; Kihara, Y. Sleeping Difficulty and Subjective Short Sleep Duration Are Associated with Serum N-Terminal Pro-Brain Natriuretic Peptide Levels in the Elderly Population. Intern Med 2020, 59, 2213–2219. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F. P.; Cooper, D.; D’Elia, L.; Strazzullo, P.; Miller, M. A. Sleep Duration Predicts Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Prospective Studies. Eur Heart J 2011, 32, 1484–1492. [Google Scholar] [CrossRef] [PubMed]
- Laugsand, L. E.; Vatten, L. J.; Platou, C.; Janszky, I. Insomnia and the Risk of Acute Myocardial Infarction.
- Li, Y.; Zhang, X.; Winkelman, J. W.; Redline, S.; Hu, F. B.; Stampfer, M.; Ma, J.; Gao, X. Association Between Insomnia Symptoms and Mortality: A Prospective Study of US Men. Circulation 2014, 129, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Laugsand, L. E.; Strand, L. B.; Platou, C.; Vatten, L. J.; Janszky, I. Insomnia and the Risk of Incident Heart Failure: A Population Study. Eur Heart J 2014, 35, 1382–1393. [Google Scholar] [CrossRef] [PubMed]
- Hübner, R.-H.; El Mokhtari, N. E.; Freitag, S.; Rausche, T.; Göder, R.; Tiroke, A.; Lins, M.; Simon, R.; Bewig, B. NT-proBNP Is Not Elevated in Patients with Obstructive Sleep Apnoea. Respir Med 2008, 102, 134–142. [Google Scholar] [CrossRef]
- Tasci, S.; Manka, R.; Scholtyssek, S.; Lentini, S.; Troatz, C.; Stoffel-Wagner, B.; Lüderitz, B. NT-pro-BNP in Obstructive Sleep Apnea Syndrome Is Decreased by Nasal Continuous Positive Airway Pressure. Clin Res Cardiol 2006, 95, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Vartany, E.; Imevbore, M.; O’Malley, M.; Manfredi, C.; Pasquarella, C.; Scinto, L.; Fine, J. N-terminal Pro-brain Natriuretic Peptide for Detection of Cardiovascular Stress in Patients with Obstructive Sleep Apnea Syndrome. Journal of Sleep Research 2006, 15, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Lazzarino, A. I.; Hamer, M.; Gaze, D.; Collinson, P.; Rumley, A.; Lowe, G.; Steptoe, A. The Interaction between Systemic Inflammation and Psychosocial Stress in the Association with Cardiac Troponin Elevation: A New Approach to Risk Assessment and Disease Prevention. Preventive Medicine 2016, 93, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Lazzarino, A. I.; Hamer, M.; Gaze, D.; Collinson, P.; Steptoe, A. The Association Between Cortisol Response to Mental Stress and High-Sensitivity Cardiac Troponin T Plasma Concentration in Healthy Adults. Journal of the American College of Cardiology 2013, 62, 1694–1701. [Google Scholar] [CrossRef] [PubMed]
- Boyd, B.; Solh, T. Takotsubo Cardiomyopathy: Review of Broken Heart Syndrome. JAAPA 2020, 33, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Raut, S.; Gupta, G.; Narang, R.; Ray, A.; Pandey, R. M.; Malhotra, A.; Sinha, S. The Impact of Obstructive Sleep Apnoea Severity on Cardiac Structure and Injury. Sleep Medicine 2021, 77, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Einvik, G.; Røsjø, H.; Randby, A.; Namtvedt, S. K.; Hrubos-Strøm, H.; Brynildsen, J.; Somers, V. K.; Omland, T. Severity of Obstructive Sleep Apnea Is Associated with Cardiac Troponin I Concentrations in a Community-Based Sample: Data from the Akershus Sleep Apnea Project. Sleep 2014, 37, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; Zhang, X.; Qu, Y.; Fan, Y.; Li, X.; Li, C.; Yu, T.; Xia, J.; Wei, M.; Chen, L.; Li, Y.; Xiao, F.; Liu, D.; Wang, J.; Wang, X.; Cao, B. 1-Year Outcomes in Hospital Survivors with COVID-19: A Longitudinal Cohort Study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Al-Hakeim, H. K.; Al-Jassas, H. K.; Morris, G.; Maes, M. Increased ACE2, sRAGE, and Immune Activation, but Lowered Calcium and Magnesium in COVID-19. Recent Adv Inflamm Allergy Drug Discov 2022, 16, 32–43. [Google Scholar] [CrossRef] [PubMed]
- The prevalence and long-term health effects of Long Covid among hospitalised and non-hospitalised populations: a systematic review and meta-analysis - eClinicalMedicine. Available online: https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(22)00491-6/fulltext (accessed on 17 May 2024).
Figure 1.
Psychosomatic, respiratory, and neurocognitive outcomes 12 months after ICU discharge. Nested violin-boxplots of all interval-scaled and continuous endpoints (orange for psychosomatic endpoints, green for respiratory endpoints, and blue for neurocognitive endpoints). In each plot, red points and dashed gray lines indicate mean values and clinical cut-off points, respectively.
Figure 1.
Psychosomatic, respiratory, and neurocognitive outcomes 12 months after ICU discharge. Nested violin-boxplots of all interval-scaled and continuous endpoints (orange for psychosomatic endpoints, green for respiratory endpoints, and blue for neurocognitive endpoints). In each plot, red points and dashed gray lines indicate mean values and clinical cut-off points, respectively.
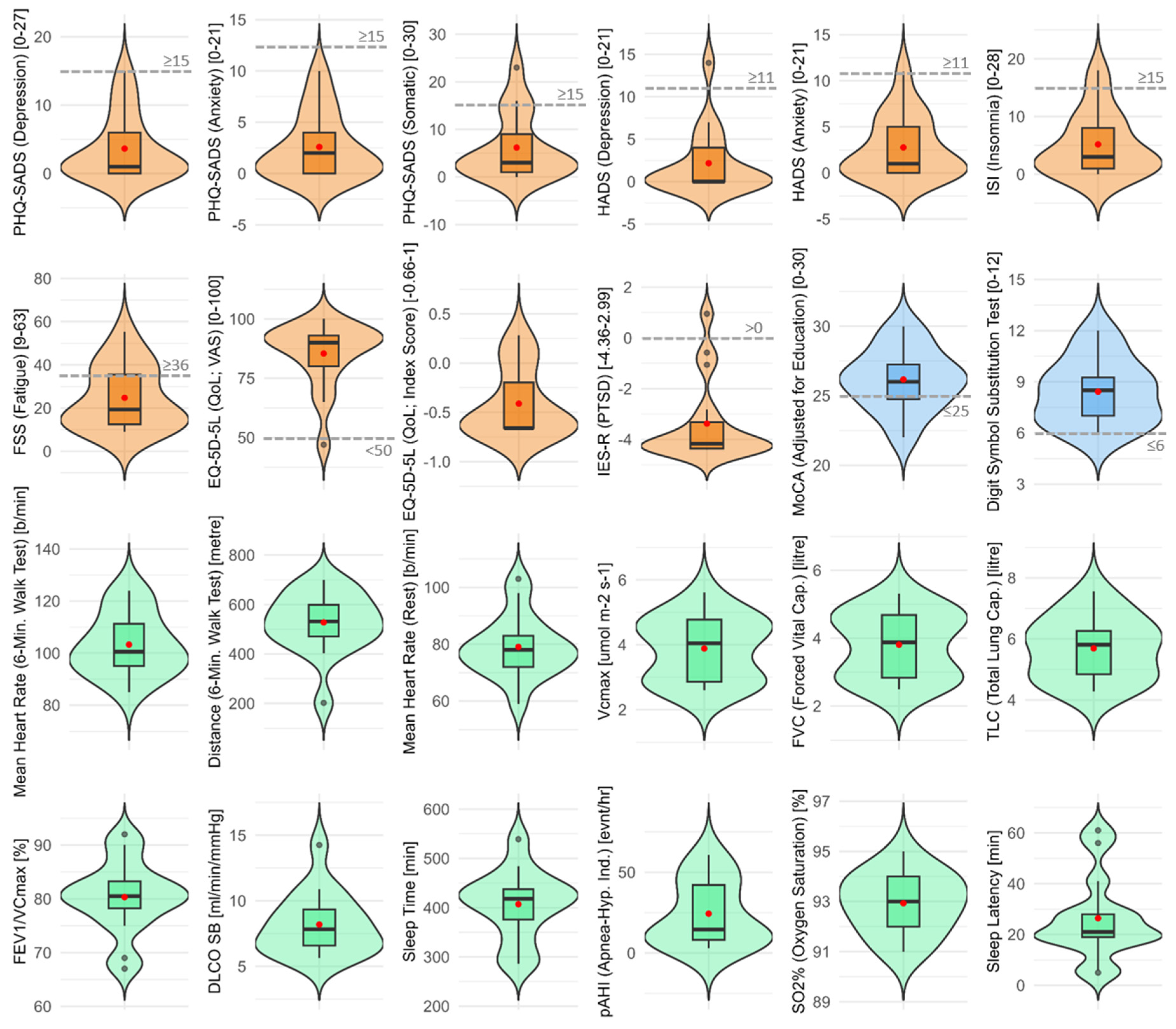
Figure 2.
Variables associated with clinical outcomes at 12 months (p-values, univariate regressions). Heatmap consisting of predictor variables (x-axis), endpoints (y-axis), and p-values (blue for p-values close to zero, red for p-values close to 1) for all calculated predictions whereas a plus (+; positive regression coefficient) and minus (-; negative regression coefficient) both indicate statistical significance. The terms “Ad.” and “Dis.” next to a predictor stand for “ICU admission” and “ICU discharge”, respectively, indicating the timepoint of data collection. The five yes/no FFQ predictors are based on the Food Frequency Questionnaire where a “OK” indicates that they fulfilled nutritional recommendations based on Swiss recommendations.17 Next to the endpoints, green and red triangles show that higher scores indicate better or worse outcomes, respectively.
Figure 2.
Variables associated with clinical outcomes at 12 months (p-values, univariate regressions). Heatmap consisting of predictor variables (x-axis), endpoints (y-axis), and p-values (blue for p-values close to zero, red for p-values close to 1) for all calculated predictions whereas a plus (+; positive regression coefficient) and minus (-; negative regression coefficient) both indicate statistical significance. The terms “Ad.” and “Dis.” next to a predictor stand for “ICU admission” and “ICU discharge”, respectively, indicating the timepoint of data collection. The five yes/no FFQ predictors are based on the Food Frequency Questionnaire where a “OK” indicates that they fulfilled nutritional recommendations based on Swiss recommendations.17 Next to the endpoints, green and red triangles show that higher scores indicate better or worse outcomes, respectively.
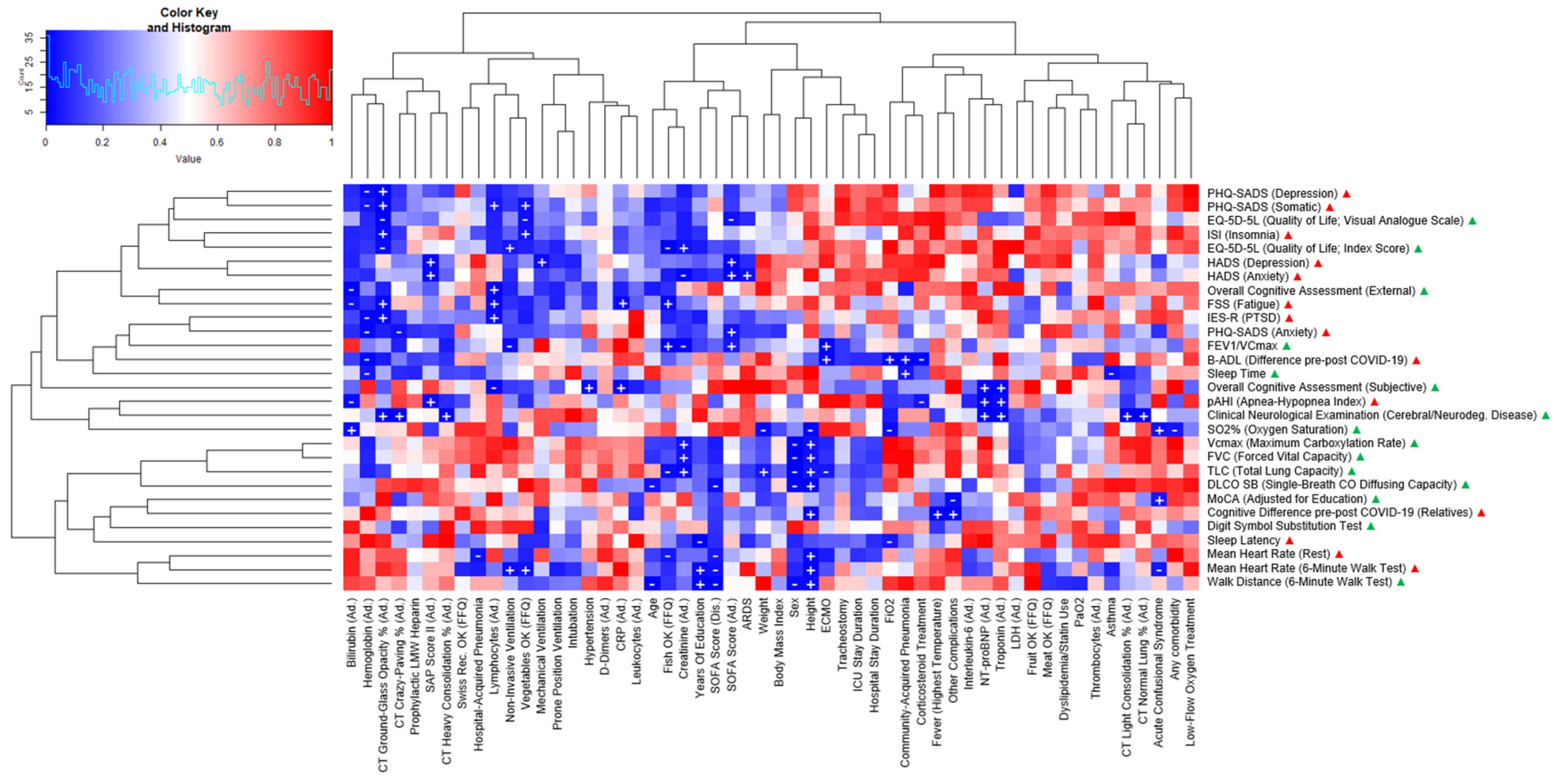
Figure 3.
Variables associated with clinical outcomes at 12 months (effect sizes, univariate regressions). Heatmap consisting of predictor variables (x-axis), endpoints (y-axis), and effect sizes (blue for effect sizes close to -1, red for effect sizes close to +1) for all calculated predictions whereas “L” and “M” indicate large and medium effect sizes of adjusted R2 or pseudo-McFadden R2 ≥ 0.26. The terms “Ad.” and “Dis.” next to a predictor stand for “ICU admission” and “ICU discharge”, respectively, indicating the timepoint of data collection. The five yes/no FFQ predictors are based on the Food Frequency Questionnaire where a “OK” indicates that they fulfilled nutritional recommendations based on Swiss recommendations.17 Next to the endpoints, green and red triangles show that higher scores indicate better or worse outcomes, respectively.
Figure 3.
Variables associated with clinical outcomes at 12 months (effect sizes, univariate regressions). Heatmap consisting of predictor variables (x-axis), endpoints (y-axis), and effect sizes (blue for effect sizes close to -1, red for effect sizes close to +1) for all calculated predictions whereas “L” and “M” indicate large and medium effect sizes of adjusted R2 or pseudo-McFadden R2 ≥ 0.26. The terms “Ad.” and “Dis.” next to a predictor stand for “ICU admission” and “ICU discharge”, respectively, indicating the timepoint of data collection. The five yes/no FFQ predictors are based on the Food Frequency Questionnaire where a “OK” indicates that they fulfilled nutritional recommendations based on Swiss recommendations.17 Next to the endpoints, green and red triangles show that higher scores indicate better or worse outcomes, respectively.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



