
Submitted:
04 July 2024
Posted:
05 July 2024
You are already at the latest version
Abstract
(1) Background: In a society with an advancing aging rate, medical systems are coming under pressure due to an increasing flow of elderly patients with multiple somatic diseases, exacerbated by their fragile psychological and sociological backgrounds. We aimed to investigate the relationship be-tween frailty and loneliness in elderly people. Our research question was “Is there a link between the loneliness and frailty in elderly people?” (2) Methods: To assess the link between loneliness and frailty, we conducted a search accessing Index Medicus and PubMed; the timeframe of our research was from 2013 till 2023. Data regarding the study population, as well as loneliness and fragility assessments and approaches, were extracted. (3) Results: A positive relationship between loneliness and the appearance and progression of frailty in elderly people is argued for. (4) Conclusions: Maintaining a balance in the body’s functionality for as long as possible requires the diagnosis and periodic assessment of health status at any age and, due to the various socio-financial and emotional implications, is particularly imperative for elderly patients. Frailty can be prevented, and it appears that it could even be reversed if early diagnosis and appropriate interventions are made. Therefore, knowledge of relevant risk factors—most likely including loneliness—is an absolute necessity to slow down, stop, and even reverse the frailty process.
Keywords:
frailty
; loneliness
; elderly
; quality of life
; aging
; patient-centered care
1. Introduction
1.1. Background
In a society with an advanced aging rate, medical systems are put under pressure due to the increasing flow of elderly patients with multiple somatic diseases, exacerbated by their fragile psychological background. Maintaining a balance in the body’s functionality for as long as possible requires the diagnosis and periodic assessment of health status at any age, which, due to the various socio-financial and emotional implications, is particularly imperative for elderly patients. A positive relationship between loneliness and the appearance and progression of frailty in elderly people has been argued [1,2,3]. Frailty is potentially preventable, and it seems that it could even be reversed if early diagnosis and appropriate interventions are made. Therefore, knowledge of the associated risk factors is an absolute necessity to slow down, stop, or even reverse the frailty process. All these are arguments for carrying out our study.
1.2. Rationale and Knowledge Gap
Frailty is a state of vulnerability, arising as a result of degradation of the physiological reserve and the ability to maintain homeostasis. In this state, some deleterious factors that are generally considered to be minor can trigger a significant decrease in health status.
Frailty can be assessed through the Fried phenotype model or the frailty index (FI) including its electronic version eFI, by utilizing routine medical data. The Fried phenotype model, which focuses on physical frailty as a clinical pre-disability syndrome [4], identifies frailty when three of the following five criteria are met: weak grip strength, slow walking speed, low physical activity or decreased mobility, exhaustion, and unintentional weight loss [5]. The frailty index, also known as the cumulative deficit model, examines the accumulation of various 'deficits' (symptoms, signs, diseases, and disabilities) [6] at the level of different systems [1,7]. It has been estimated that approximately 25–50% of people older than 85 are frail [8]. It is important to specify that up to 75% of these people may not present severe frailty, highlighting the importance of studying the etiology of frailty and methods for its prevention [8], as well as frailty evaluation methods [9]. A study published in 2018 reported that, globally, 3.5–27.3% of non-institutionalized adults were frail [10]. Various risk factors for frailty have been proposed, including advanced age, male sex, low body mass index, lack of physical activity, excess medication, smoking, alcoholic beverages, malnutrition, and lack of vitamin D. Patients with diabetes, hearing problems, or depression seem to be more prone to frailty compared to those with cardiovascular or ophthalmological problems [7,10].
Studies [1,3,11] have reported a positive relationship between loneliness and worsening frailty, as well as a negative impact with recovery from the pre-frail or frail state. Loneliness is correlated with a lack of physical activity, representing a way in which the occurrence of fragility can be favored [12].
Frailty increases the risk of developing disability, the risk of hospitalization or institutionalization, and risk of mortality [3,13]. An increased frailty index is associated with increased reporting of loneliness in older adults, as well as an increased risk of worsening loneliness over time [1,12].
Classification
A commonly used frailty assessment tool based on clinical judgment and physical examination is the Clinical Frailty Scale [14]. Depending on the degree of frailty, patients can be divided into very good condition (robust, active, energetic people), good condition (they have no signs of illness but are less fit than those in the first category), intermediate condition (with well-controlled medical problems), very mild frailty (daily activities limited by disease symptoms but not dependent on others), mild frailty (need help with more complex activities, such as walking to the store or taking care of the house), moderate frailty (requires support for all outdoor activities, as well as some activities inside the house such as climbing stairs, showering, or dressing), severe frailty (completely dependent for all physical and cognitive activities but stable and without risk of imminent death), very severe frailty (completely dependent and nearing end of life, may die from minor ailments), and terminally ill (life expectancy less than 6 months) [15].
Pre-frailty represents an intermediate state between frailty and robustness, with an increased risk for the transition to frailty [16]. Individuals with this frailty prodrome are also exposed to adverse health effects, such as an increased risk of developing cardiovascular disease or depressive syndromes, or the worsening of pre-existing cognitive impairment.
Frailty is a clinical syndrome characterized by an increased vulnerability to seemingly unknown stressors [6] due to low psychological reserves, marked by a decline in the ability to maintain body homeostasis and multiple organ deficiency [1] as a result of the accumulation of age-related deficits. Although distinct from multi-morbidity, frailty overlaps with an advanced degree of disability and dependence on specialized help in the last decade of life [17].
Understanding the fluidity of frailty status between robust, pre-frail, and frail [16], it is important to consider potential interventions to improve the quality of life and maintain the functionality of older adults. Although it is closely related to age, frailty is not an inevitable and irreversible process, and it is imperative to understand the catalyst in the transition from robust to pre-frail or from pre-frail to frail in order to select the optimal population for slowing or preventing deterioration of functional status [18].
Loneliness is a natural phenomenon, being a feeling that appears in certain periods of life and affects people regardless of age, gender, or other socio-demographic characteristics. It should be noted that one may have a low number of social interactions but no negative emotions related to this fact; on the other hand, loneliness can also be felt by people who have social contacts and participate in collective activities [19].
Therefore, some authors delineate a difference between “emotional loneliness” and “social loneliness.” The first is a subjective, qualitative assessment of the discrepancy between the level of desired social contact and the current level of social contact, while the second is called “social isolation” and is an objective, quantitative assessment, which reflects the number of social contacts had by a person [6]. Social isolation is a factor of interest due to the possible two-way relationship it has with frailty, the hypothesis being a ‘withdrawal’ syndrome resulting from a continuous deterioration (decrease) of vital energy or through a lack of interest or capacity in engaging in social contacts [6]. However, it is difficult to understand the causal factors and the effects of this process. Generally, physical degradation precedes mental degradation, and an amelioration of frailty also leads to an amelioration of loneliness. In older adults, however, it has been observed that the reverse relationship is not true: an improvement in loneliness does not always lead to an improvement in frailty [12]. Therefore, promoting social connections, encouraging participation in social activities, and developing adequate social support are key factors in maintaining the health and well-being of older people [19].
Evaluation
To understand the impact of loneliness on frailty among older people, it is important to establish clear definitions and measurement tools for each concept. In this regard, various definitions and measurement tools have been proposed in the literature.
According to Sha et al. [12], there exists a reciprocal relationship between frailty and loneliness, and they share a pro-inflammatory phenotype [20]; however, the initial effect of frailty on subsequent loneliness is greater than if the events occurred in the opposite direction. This suggests that physical health has a greater influence on mental health than vice versa, in agreement with a previous study by Luo et al. [21]. The same study [12] showed that the effects of loneliness on frailty impairment in a six-year cohort were stronger than those in the shorter three-year cohorts.
Taking this information into account, it is clear that, to care for the frail elderly, psychosocial needs must be addressed in addition to physical ones [22]. People with frailty have varied physical and psychosocial needs at their end of life, which may benefit from geriatric and palliative care. Frailty services should be tailored to the needs and preferences of patients at their end of life [22], especially because elderly adults who live in specialized institutions, who are far from their friends and family, are more likely to experience loneliness, compared to individuals living in the community. Furthermore, loneliness influences the involvement in physical and social activities, which functions as a mediator in the loneliness–frailty relationship, with decreasing involvement leading to the progression of frailty [23].
1.3. Objective
The frailty of the elderly is potentially preventable, and, therefore, knowing the associated risk factors is an absolute necessity both for prevention and to slow down, stop, and even reverse the frailty process once it has set in. We present a narrative review based on the available literature focusing on frailty and loneliness or social isolation in elderly people. Our question research was “Is there a link between the loneliness and frailty in elderly people?”
2. Materials and Methods
The search strategy
Although the frequency of frailty and loneliness is high, the mechanism by which loneliness influences the progression of frailty remains incompletely elucidated. To assess the link between frailty and loneliness, we conducted a search accessing Index Medicus and PubMed in September–December 2023 (Table 1).
The following search strategy was used: loneliness AND frailty AND ( fulltext:(“1” OR “1”) AND mj:(“Frail Elderly” OR “Aging” OR “Geriatric Assessment” OR “Health of the Elderly” OR “Quality of Life” OR “Activities of Daily Living” OR “Primary Health Care” OR “Risk Factors” OR “Prevalence”) AND la:(“en”)) AND (year_cluster:[2013 TO 2023]).
The inclusion criterion was any study (either descriptive or analytic) enrolling adult patients over the age of 60 diagnosed with frailty (either using Clinical Diagnostic Criteria for frailty or other validated diagnostic scales or instruments) and/or loneliness.
Studies were excluded if they were in a language other than English or if the full text was not freely available.
Studies not identified using this search strategy that were subsequently identified and met the mentioned inclusion criterion were also included in our study.
Study appraisal
The first evaluation was made by reading the title and abstract. The subsequent evaluation of the remaining articles involved reading the full text to determine eligibility for inclusion in our study. Duplicate articles were excluded.
Data regarding the study populations, as well as the loneliness and fragility assessment and approach, were extracted. We took descriptive or analytic studies enrolling adult patients diagnosed with frailty and/or loneliness into consideration.
During data extraction, we took into account the fact that, in the literature, in order to implement intervention strategies that are as suitable as possible for the target groups, different methods for assessing loneliness and fragility have been proposed. Furthermore, loneliness and frailty have been classified over time according to various criteria. For instance, loneliness can be assessed via self-reported scales that capture feelings of social isolation, emotional distress, and lack of companionship. Regarding the risk factors that can also represent the starting point for intervention plans, loneliness can be addressed through increasing social support, increasing opportunities for social interaction, improving social skills, and socio-cognitive training [19].
Frailty, on the other hand, can be measured using multi-dimensional instruments that assess physical function, cognition, nutrition, and other relevant domains, such as the frailty index or frailty phenotype (Clinical Frailty Scale [15], Edmonton Frail Scale (https://edmontonfrailscale.org/validation-scale-and-spread), FRAIL scale (https://www.bgs.org.uk/sites/default/files/content/attachment/2018-07-05/rockwood_cfs.pdf), INTER-FRAIL (jgs13029-sup-0001-TableS1-S2.docx) Prisma-7, Sherbrooke Postal Questionnaire (https://www2.gov.bc.ca/assets/gov/health/practitioner-pro/bc-guidelines/frailty-prisma7.pdf), Short Physical Performance Battery (https://geriatrictoolkit.missouri.edu/SPPB-Score-Tool.pdf ), and Study of Osteoporotic Fractures Index (https://agingresearchbiobank.nia.nih.gov/studies/sof/ ) or newer scales, for example, Kihon's list(http://jssf.umin.jp/pdf/Kihon%20Checklist.pdf ) [18].
Taking all these aspects into account, we decided to assess any study (either descriptive or analytic) enrolling adult patients diagnosed with frailty—either using Clinical Diagnostic Criteria for frailty, Fried frailty phenotype assessment, the Short Physical Performance Battery (SPPB), the Frailty Deficit Index (FDI), the Tilburg Frailty Indicator (TFI), Clinical-Functional Vulnerability Index-20 (IVCF-20; instrumental daily living activity, cognition, mood, mobility, communication, and multiple comorbidities), the Edmonton Frail Scale, or the Comprehensive Geriatric Assessment (CGA)—and/or loneliness.
3. Results
Starting from the association between frailty and loneliness, 213 articles were selected. After reading the titles and abstracts, 74 studies were excluded. The full texts of all remaining articles were read, and two independent authors (E.B. and A.C.G.) evaluated and included the eligible articles. Different opinions were discussed with all the other authors until a consensus was reached. Finally, only 18 studies were analyzed (Table S1).
Through examining the relationship between loneliness and frailty, our aim was to shed light on possible ways in which social isolation may contribute to physical decline and increased vulnerability among older adults. We set out to explore the epidemiology of loneliness and frailty, risk factors and potential consequences, classification systems, and discussions of the impact of loneliness on frailty [8,24].
Several studies have examined the prevalence and incidence of loneliness and frailty among older adults. For example, a study by Clegg et al. [8] found that approximately 10–40% of older adults experience moderate to severe loneliness. Regarding frailty, another study [25] showed that the prevalence of frailty among community-dwelling older adults ranges from 4% to 59%, depending on the diagnostic criteria used. Another study estimates that approximately 25–50% of people over 85 are frail [26]. It is important to specify that up to 75% of these people may not present pronounced frailty, highlighting the importance of studying the etiology of frailty and methods for its prevention [8]. Sha et al. have reported that greater loneliness was related to an increased risk of worsening frailty and remaining frail [13]. Moreover, it seems that elderly men with a high level of loneliness had a worse degradation of clinical status through frailty compared to elderly women [13].
Although frailty is chronologically and biologically related to age, occurs with a higher prevalence in women than in men, and is usually associated with chronic diseases [27], there is great heterogeneity in terms of the prevalence and degree of impairment associated with frailty in groups of people who fall under the same clinical–biological criteria. The higher prevalence of frailty among women may be explained by having, on average, lower body mass and lower muscle strength. In addition, it should be taken into account that women live longer on average than men, and the association of increased age with frailty has been demonstrated in various studies [27]. The association of frailty with chronic diseases—with up to 66% of older adults suffering from at least two chronic conditions [25]—calls for more effective prevention strategies to reduce potential risks. Due to the increasing incidence of obesity in adults, particularly abdominal obesity, it is necessary to pay more attention, as this condition is associated with an increased risk of frailty through the predisposition to pro-inflammatory status, cardiovascular diseases, and hormonal imbalances. This co-association of several emerging factors with basic diseases of the individual is called multi-morbidity, and there are many studies that attest to the cause–effect relationship between this condition and the association of frailty with mortality [28]. However, a study by Zucchelli et al. [26], based on a population aged over 60 years established in Stockholm, Sweden, showed an increased mortality risk in pre-frail and frail individuals, compared to those in whom these conditions are not present, even in the absence of multiple chronic pathologies.
Damluji et al. [29] found that pre-frailty and physical frailty phenotypes were associated with a high risk of major adverse cardiovascular events and mortality, despite rigorous control of cardiovascular risk factors, during 6 years of follow-up. Their conclusion was that efforts should be made to integrate frailty assessment as part of primary cardiovascular prevention programs for older adults at risk of cardiovascular disease, which are essential in daily cardiovascular clinical practice. As the growth of the adult population has been recorded worldwide, it is imperative to evaluate the efficiency and effectiveness of programs to maintain active status through promoting physical exercise, adequate nutrition, and cognitive training to prevent or even reverse frailty in patients with cardiovascular risk [29].
These factors can be considered intrinsic, but there are also extrinsic variables, mainly included under the name of social vulnerability (relating to socio-economic level, social relations, and family support) which, in the context of their decrease, have been associated with greater fragility and an increased rate of in-hospital death [19].
According to a 2020 report by the National Health and Aging Trends Study, in the United States, a significant number of older adults (approximately 7.7 million people) experienced loneliness and social isolation [30]. Before the Coronavirus Disease 2019 (COVID-19) pandemic, about 24% of adults aged 65 and older living in the community were socially isolated, and 4% of them were severely isolated [30]. Some studies have pointed out that approximately one in four community-dwelling adults are socially isolated. It seems that, among older adults, risk factors for social isolation include male gender, lower income, and lower educational attainment [28,30,31].
During the COVID-19 pandemic, some studies showed that there were no significant changes at the level of the elderly population regarding isolation, with the elderly feeling social isolation less acutely compared to other population groups [31].
According to a study based on data from the U.S. Health and Retirement Study, 43% of Americans aged 60 and older reported feeling lonely [11]. Additionally, a survey conducted by The American Association of Retired Persons (AARP) found that 35% of adults over the age of 45 feel lonely [32].
In Europe, around 20% of older people experience loneliness. This means that 1 in 5 older people feel a sense of isolation and lack of social connection. The percentage varies by country, with higher levels of loneliness in countries such as Sweden and Norway (over 25%) and lower levels in Spain and Greece (under 15%), underscoring the scale of the problem and the significant social impact on older people. It is important to pay attention to this aspect and develop prevention and intervention strategies to combat loneliness and promote well-being among the older population [33].
Older people who feel lonely and socially isolated have certain characteristics in common. These include older age, single status, male gender, low education, and low income [33]. Social isolation increases the risk of loneliness and can be assessed using five indicators:
- Status of being unmarried or non-cohabitant, living without another family member in the same house;
- Less than monthly contact with own children who do not live in the same house as them (physically, in writing, or by phone);
- Less than monthly contact with other family members who do not live in the same house as them (physically, in writing, or by telephone);
- Less than monthly contact with friends (physical, written, or by phone) who do not live in the same house as them;
According to the results obtained from the analyses performed by Maltby et al. [6], social isolation—as assessed in the English Longitudinal Study of Aging and in accordance with the elements suggested by Gale et al. [1]—includes three dimensions:
a) ‘Nuclear family’—through the status of unmarried or non-cohabitant and isolation from children;
b) ‘Immediate family’—through isolation from parents and relatives;
c) ‘Extended social network’—isolation from friends and social organizations.
In addition, another finding described by Maltby et al. [6] is that social isolation, compared to having an extensive social network, predicts the frailty index for a period of more than four years both for basic frailty and other variables (e.g., age, socio-economic status, educational abilities, depressive symptoms, smoking).
RISK FACTORS
The definition of frailty is mainly based on physical markers, such as low grip strength or a decrease in mobility and balance, without taking into account (most of the time) domains related to cognitive, mental, and social health, which can be reflected in loneliness and social isolation [34,35,36].
Although there are factors (Figure 1) that predispose older individuals to the development of frailty, including low socio-economic status, comorbidities, poor diet, and sedentary lifestyles, everyone in their latter part of life is at risk of becoming frail [37]. Nevertheless, to the point where it becomes a pre-death phase, frailty is potentially preventable [37], and there is a belief that it could even be reversed if there is an early screening process followed by appropriate interventions [38].
Aging is a factor of physiological frailty, regardless of the level of physical activity [2]. Elderly individuals become more vulnerable when they have concomitant chronic diseases, are exposed to acute infections, or are prone to falls [2]. Studies have demonstrated that an increase in the C-reactive protein (CRP) level, fibrinogen, and overall inflammatory activity, as well as increased blood cortisol, are also risk factors for frailty [19]. In addition to clinical, biological, and lifestyle factors, social criteria such as social isolation or loneliness [37] should be included in screening programs for frailty [19].
The bidirectional relationship between frailty and loneliness was assessed in a study [13] that followed the transition of frailty in two cohorts after 2008, followed up in 2011 and 2014. Tendencies to remain in a frailty state were associated with increased levels of loneliness observed over a period of three years: compared to patients who never felt lonely, those who often felt lonely were less likely to remain in the robust or pre-frail state. Additionally, in the group following a worsening of health, loneliness was a risk factor, such that increased levels of loneliness were associated with increased frailty over time [13].
According to Hanlon et al., social isolation and/or loneliness are risk factors for increased hospitalization at all levels of frailty [3]; moreover, it seems that risk of loneliness is more pronounced in those with a robust or pre-frail status [3,13].
Having a conjugal life, living with a partner, and being sexually active are factors correlated with robustness. Older people involved in couple activities seem to have a high quality of life based on common concerns for well-being, maintaining their social role, sharing common interests, and spending time practicing physical activity or having a healthy lifestyle. Companionship, trust, affection, and complicity are expressed in a particular way by older adults and seem to play an essential role in maintaining psychosocial identity and preserving interest in everyday life [39].
A possible problem for elderly couples is represented by the fact that, with advancing age comes the difficulty of managing age-specific conditions or comorbidities. Sometimes, it is necessary for one of the members of the couple to take on the role of caregiver of the life partner, which can represent a serious problem for elderly individuals, especially for those who live alone (either because they have no offspring, or because their offspring live at long distances). It seems that female caregivers, caregivers with cognitive deterioration, and individuals who need help in carrying out household activities are the most prone to rapid deterioration and require a lot of attention from relevant healthcare providers [40].
4. Discussion
The aging process and the association of chronic diseases with advanced age are conditions that necessitate careful evaluation and investigation of the health status. The prevalence of many diseases is increased in older populations. Surviving longer with diseases can be a factor in reducing functionality, implicitly leading to limitation of the activities of the elderly who then become dependent on their family and social care.
Aging causes not only numerous changes in the body and the appearance of chronic diseases but also socio-economic changes that represent a challenge both for elderly individuals and for society. Maintaining an adequate physical and mental status allows a better quality of life, which can ensure the involvement of older adults in social, economic, and cultural life. These aspects also contribute not only to increasing the life span of the elderly but also to maintaining the satisfaction of being useful to oneself and to those around.
With the passing of years and the appearance of disability, elderly individuals will come to depend on their family and society. In addition to the socio-economic support, active frailty screening is essential for the early detection of changes specific to the frailty syndrome and to ensure prompt interventions.
In primary healthcare, the proactive identification of loneliness, especially for the elderly population, should be a priority and should be constantly carried out at every medical visit, regardless of the physical health status of the patient, in order to ensure optimal interventions at the right time [3]. After assessing the patient's degree of frailty and loneliness and/or social isolation, the attending physician can offer patient-centered care, which could lead to more optimistic results and avoid worsening of his/her condition [37].
The loss of autonomy in elderly individuals is associated with needs of a medical, social, and psycho-affective nature [41], which must be evaluated according to the criteria for classification in degrees of dependence in different types of assessment grids for the elderly[42,43]. In Romania, the national grid for assessing the needs of the elderly was revised in 2023, ensuring the complete assessment of dependent elderly people (https://www.mmuncii.ro/j33/images/Documente/MMPS/Rapoarte_si_studii_MMPS/DPSS/2022_Substantiation_Study_for_LTC_Strategy_2023-2030_EN.pdf). Thus, seniors can be provided with social and medical services adapted to their individual needs. Society can support seniors who need assistance with personal care not only through ensuring access to professional care services but also by creating help centers where the elderly can benefit from the provision of basic needs ranging from accommodation, care, and feeding to psychological support, social interaction, occupational therapy, religious/spiritual services, or legal counseling [22,33,44].
In addition to the involvement of social services, the roles of primary care providers and geriatric specialists are essential. Furthermore, with growing importance as the degree of disability increases, palliative care services are representative multi-disciplinary stakeholders in the healthcare context [22,41,44] and are the most suitable to develop current and terminal medical care approaches, being one of the few services that can offer a holistic approach to the patient and those close to them [22,44].
Social isolation and loneliness are risk factors for chronic diseases but can also be their consequence [41]. There exists a two-way path between them, and social isolation and loneliness can also dissuade an individual to fight against disease and weakness, reducing the chances of effectiveness of therapeutic interventions and worsening their status. Approaching the palliative rehabilitation care model adapted to elderly people with chronic non-oncological conditions can represent an opportunity to maintain interest in involvement in daily activities, thus maintaining their motivation to live as actively as possible in the last part of their lives [41].
The primary limitation of our study arises from the design of the included studies and their heterogeneity in terms of the evaluation of frailty and/or loneliness or social isolation. In this context, no final resolution can be postulated. Further studies are required to better understand the double pathway between frailty and loneliness in elderly individuals.
5. Conclusions
Considering the increasing prevalence of frailty, its early identification through risk factor assessment (including loneliness and/or social isolation) must become a standard of care for elderly patients. Loneliness can be seen as both a risk factor and a consequence of frailty, and it should be evaluated in the individual context of each elderly person. Taking into account the patient's degree of frailty and his/her peculiarities, the care team can provide patient-centered care, which may lead to more optimistic outcomes, avoid the worsening of medical conditions, and ensure peaceful and active ageing for older adults.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Summary of included studies.
Author Contributions
The idea of this material was developed by E.B. and R.I.N., who, during the Pathophysiology Workshop attended by 3rd year students at the Faculty of Medicine from Carol Davila University of Medicine and Pharmacy, presented the particularities of caring for elderly people who live alone and asked the students enrolled in the working group (M.I.A, A.V.C., C.A.A., M.A., A.C.B., and A.C.A.) to document themselves on this topic. E.B., A.C.G., R.I.N., I.H., G.T., M.-M.M.-M., and D.A.I. verified the information provided by the students. Considering that the topic is of great interest, all the participants decided to become involved in this literature review and continued the documentation. E.B. and A.C.G. performed data acquisition and drafted the manuscript. E.B. contributed to work conception and revised the manuscript. E.B., A.C.G., R.I.N., I.H., G.T., M.-M.M.-M., and D.A.I. performed the final revision of the manuscript. All authors discussed the results and contributed to the final manuscript. E.B., R.I.N., and D.A.I. gave the final approval. All authors read and approved the final version of the manuscript. †These authors equally contributed to this work as co-first authors.
Funding
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila from Bucharest, Romania, through the institutional program “Publish not Perish.”.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
E.B.: A.C.G., G.T., and R.I.N. are extremely grateful to educators and participants in the RESPACC project (“Writing for academic and professional journals—multiplier event” conducted by Sheila Payne and Daniela Moșoiu), including all the country facilitators (HOSPICE Casa Speranței Foundation, Romania: Oana Predoiu; Transilvania University, Romania: Daniela Moșoiu; University of Navarra, Spain; Galilee Palliative Care Unit, Greece). This material has been written in accordance with the recommendations received during that workshop.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gale, C.R.; Westbury, L.; Cooper, C. Social isolation and loneliness as risk factors for the progression of frailty: The english longitudinal study of ageing. Age Ageing 2018, 47, 392–397. [Google Scholar] [CrossRef]
- Ozic, S.; Vasiljev, V.; Ivkovic, V.; Bilajac, L.; Rukavina, T. Interventions aimed at loneliness and fall prevention reduce frailty in elderly urban population. Medicine (Baltimore) 2020, 99, e19145. [Google Scholar] [CrossRef]
- Peter Hanlon, B.N., Lynsay Crawford, Marina Politis, Frances Mair, Bhautesh Jani and Jim Lewsey. Combinations of frailty, social isolation and loneliness and the risk of adverse health outcomes: A uk biobank analysis. The Annals of Family Medicine 2023, 21.
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.L. The frailty syndrome: Definition and natural history. Clin Geriatr Med 2011, 27, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Maltby, J.; Hogervorst, E.; Stephan, B.; Sun, X.; Tang, P.; Law, E.; Mukaetova-Ladinska, E.B. The development of a quality of life scale for informal carers for older adults. Gerontol Geriatr Med 2020, 6, 2333721420920424. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Hu, J.; Wu, D. Risk factors for frailty in older adults. Medicine (Baltimore) 2022, 101, e30169. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Shi, S.M.; McCarthy, E.P.; Mitchell, S.L.; Kim, D.H. Predicting mortality and adverse outcomes: Comparing the frailty index to general prognostic indices. J Gen Intern Med 2020, 35, 1516–1522. [Google Scholar] [CrossRef]
- Walston, J.; Buta, B.; Xue, Q.L. Frailty screening and interventions: Considerations for clinical practice. Clin Geriatr Med 2018, 34, 25–38. [Google Scholar] [CrossRef]
- Perissinotto, C.M.; Stijacic Cenzer, I.; Covinsky, K.E. Loneliness in older persons: A predictor of functional decline and death. Arch Intern Med 2012, 172, 1078–1083. [Google Scholar] [CrossRef]
- Sha, S.; Pan, Y.; Xu, Y.; Chen, L. Associations between loneliness and frailty among older adults: Evidence from the china health and retirement longitudinal study. BMC Geriatr 2022, 22, 537. [Google Scholar] [CrossRef] [PubMed]
- Sha, S.; Xu, Y.; Chen, L. Loneliness as a risk factor for frailty transition among older chinese people. BMC Geriatr 2020, 20, 300. [Google Scholar] [CrossRef]
- Mendiratta, P.; Schoo, C.; Latif, R. Clinical frailty scale. In Statpearls, Treasure Island (FL) ineligible companies. Disclosure: Caroline Schoo declares no relevant financial relationships with ineligible companies. Disclosure: Rafay Latif declares no relevant financial relationships with ineligible companies., 2024.
- Mendiratta, P.; Schoo, C.; Latif, R. Clinical frailty scale. In Statpearls, Treasure Island (FL) ineligible companies. Disclosure: Caroline Schoo declares no relevant financial relationships with ineligible companies. Disclosure: Rafay Latif declares no relevant financial relationships with ineligible companies., 2023.
- Siriwardhana, D.D.; Hardoon, S.; Rait, G.; Weerasinghe, M.C.; Walters, K.R. Prevalence of frailty and prefrailty among community-dwelling older adults in low-income and middle-income countries: A systematic review and meta-analysis. BMJ Open 2018, 8, e018195. [Google Scholar] [CrossRef]
- O'Caoimh, R.; O'Donovan, M.R.; Monahan, M.P.; Dalton O'Connor, C.; Buckley, C.; Kilty, C.; Fitzgerald, S.; Hartigan, I.; Cornally, N. Psychosocial impact of covid-19 nursing home restrictions on visitors of residents with cognitive impairment: A cross-sectional study as part of the engaging remotely in care (eric) project. Front Psychiatry 2020, 11, 585373. [Google Scholar] [CrossRef]
- Kojima, G. Increased healthcare costs associated with frailty among community-dwelling older people: A systematic review and meta-analysis. Arch Gerontol Geriatr 2019, 84, 103898. [Google Scholar] [CrossRef] [PubMed]
- Yanguas, J.; Pinazo-Henandis, S.; Tarazona-Santabalbina, F.J. The complexity of loneliness. Acta Biomed 2018, 89, 302–314. [Google Scholar]
- Zhao, Y.; Lin, T.; Hou, L.; Zhang, M.; Peng, X.; Xie, D.; Gao, L.; Shu, X.; Yue, J.; Wu, C. Association between geriatric nutritional risk index and frailty in older hospitalized patients. Clin Interv Aging 2021, 16, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.S.; Chui, E.W.T.; Li, L.W. The longitudinal associations between physical health and mental health among older adults. Aging Ment Health 2020, 24, 1990–1998. [Google Scholar] [CrossRef]
- Stow, D.; Spiers, G.; Matthews, F.E.; Hanratty, B. What is the evidence that people with frailty have needs for palliative care at the end of life? A systematic review and narrative synthesis. Palliat Med 2019, 33, 399–414. [Google Scholar] [CrossRef]
- Zhang, Y.; Kuang, J.; Xin, Z.; Fang, J.; Song, R.; Yang, Y.; Song, P.; Wang, Y.; Wang, J. Loneliness, social isolation, depression and anxiety among the elderly in shanghai: Findings from a longitudinal study. Arch Gerontol Geriatr 2023, 110, 104980. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.; Hankins, M.; Windle, G.; Bilotta, C.; Grant, R. A short measure of quality of life in older age: The performance of the brief older people's quality of life questionnaire (opqol-brief). Arch Gerontol Geriatr 2013, 56, 181–187. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Chin, K.L.; Mazidi, M.; Zomer, E.; Ilomaki, J.; Zullo, A.R.; Gasevic, D.; Ademi, Z.; Korhonen, M.J.; LoGiudice, D.; et al. Global incidence of frailty and prefrailty among community-dwelling older adults: A systematic review and meta-analysis. JAMA Netw Open 2019, 2, e198398. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, A.; Vetrano, D.L.; Marengoni, A.; Grande, G.; Romanelli, G.; Calderon-Larranaga, A.; Fratiglioni, L.; Rizzuto, D. Frailty predicts short-term survival even in older adults without multimorbidity. Eur J Intern Med 2018, 56, 53–56. [Google Scholar] [CrossRef]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J Am Geriatr Soc 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Chen, Y.; Wang, K.; De Fries, C.M.; Huang, Z.; Xu, H.; Yang, Z.; Hu, Y.; Xu, B. Associations between multimorbidity and frailty transitions among older americans. J Cachexia Sarcopenia Muscle 2023, 14, 1075–1082. [Google Scholar] [CrossRef]
- Damluji, A.A.; Chung, S.E.; Xue, Q.L.; Hasan, R.K.; Moscucci, M.; Forman, D.E.; Bandeen-Roche, K.; Batchelor, W.; Walston, J.D.; Resar, J.R.; et al. Frailty and cardiovascular outcomes in the national health and aging trends study. Eur Heart J 2021, 42, 3856–3865. [Google Scholar] [CrossRef] [PubMed]
- Cudjoe, T.K.M.; Roth, D.L.; Szanton, S.L.; Wolff, J.L.; Boyd, C.M.; Thorpe, R.J. The epidemiology of social isolation: National health and aging trends study. J Gerontol B Psychol Sci Soc Sci 2020, 75, 107–113. [Google Scholar] [CrossRef]
- Luchetti, M.; Lee, J.H.; Aschwanden, D.; Sesker, A.; Strickhouser, J.E.; Terracciano, A.; Sutin, A.R. The trajectory of loneliness in response to covid-19. Am Psychol 2020, 75, 897–908. [Google Scholar] [CrossRef]
- Donovan, N.J.; Blazer, D. Social isolation and loneliness in older adults: Review and commentary of a national academies report. Am J Geriatr Psychiatry 2020, 28, 1233–1244. [Google Scholar] [CrossRef]
- Fakoya, O.A.; McCorry, N.K.; Donnelly, M. Loneliness and social isolation interventions for older adults: A scoping review of reviews. BMC Public Health 2020, 20, 129. [Google Scholar] [CrossRef] [PubMed]
- Apostolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; Holland, C. Predicting risk and outcomes for frail older adults: An umbrella review of frailty screening tools. JBI Database System Rev Implement Rep 2017, 15, 1154–1208. [Google Scholar] [CrossRef] [PubMed]
- Apostolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; D'Avanzo, B.; Gwyther, H.; et al. Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: A systematic review. JBI Database System Rev Implement Rep 2018, 16, 140–232. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Mitnitski, A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin Geriatr Med 2011, 27, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.P.; Morley, J.E.; Ong, P.; et al. Frailty: An emerging public health priority. J Am Med Dir Assoc 2016, 17, 188–192. [Google Scholar] [CrossRef]
- Souza Junior, E.V.; Silva, C.D.S.; Piropo, U.S.; Santos, B.; Guedes, T.P.; Siqueira, L.R.; Sawada, N.O. Effects of sexuality on frailty and quality of life in the elderly: A cross-sectional study. Rev Bras Enferm 2021, 75, e20210049. [Google Scholar] [CrossRef]
- Santos-Orlandi, A.A.D.; Brito, T.R.P.; Ottaviani, A.C.; Rossetti, E.S.; Zazzetta, M.S.; Pavarini, S.C.I. Elderly who take care of elderly: A study on the frailty syndrome. Rev Bras Enferm 2017, 70, 822–829. [Google Scholar] [CrossRef]
- Tziraki, C.; Grimes, C.; Ventura, F.; O'Caoimh, R.; Santana, S.; Zavagli, V.; Varani, S.; Tramontano, D.; Apostolo, J.; Geurden, B.; et al. Rethinking palliative care in a public health context: Addressing the needs of persons with non-communicable chronic diseases. Prim Health Care Res Dev 2020, 21, e32. [Google Scholar] [CrossRef]
- Sepehri, K.; Braley, M.S.; Chinda, B.; Zou, M.; Tang, B.; Park, G.; Garm, A.; McDermid, R.; Rockwood, K.; Song, X. A computerized frailty assessment tool at points-of-care: Development of a standalone electronic comprehensive geriatric assessment/frailty index (efi-cga). Front Public Health 2020, 8, 89. [Google Scholar] [CrossRef]
- Nord, M.; Ostgren, C.J.; Marcusson, J.; Johansson, M. Staff experiences of a new tool for comprehensive geriatric assessment in primary care (pastel): A focus group study. Scand J Prim Health Care 2020, 38, 132–145. [Google Scholar] [CrossRef] [PubMed]
- W.H.O. Improving acess to palliative care. Available online: https://www.who.
Figure 1.
Risk factors for frailty in the elderly.
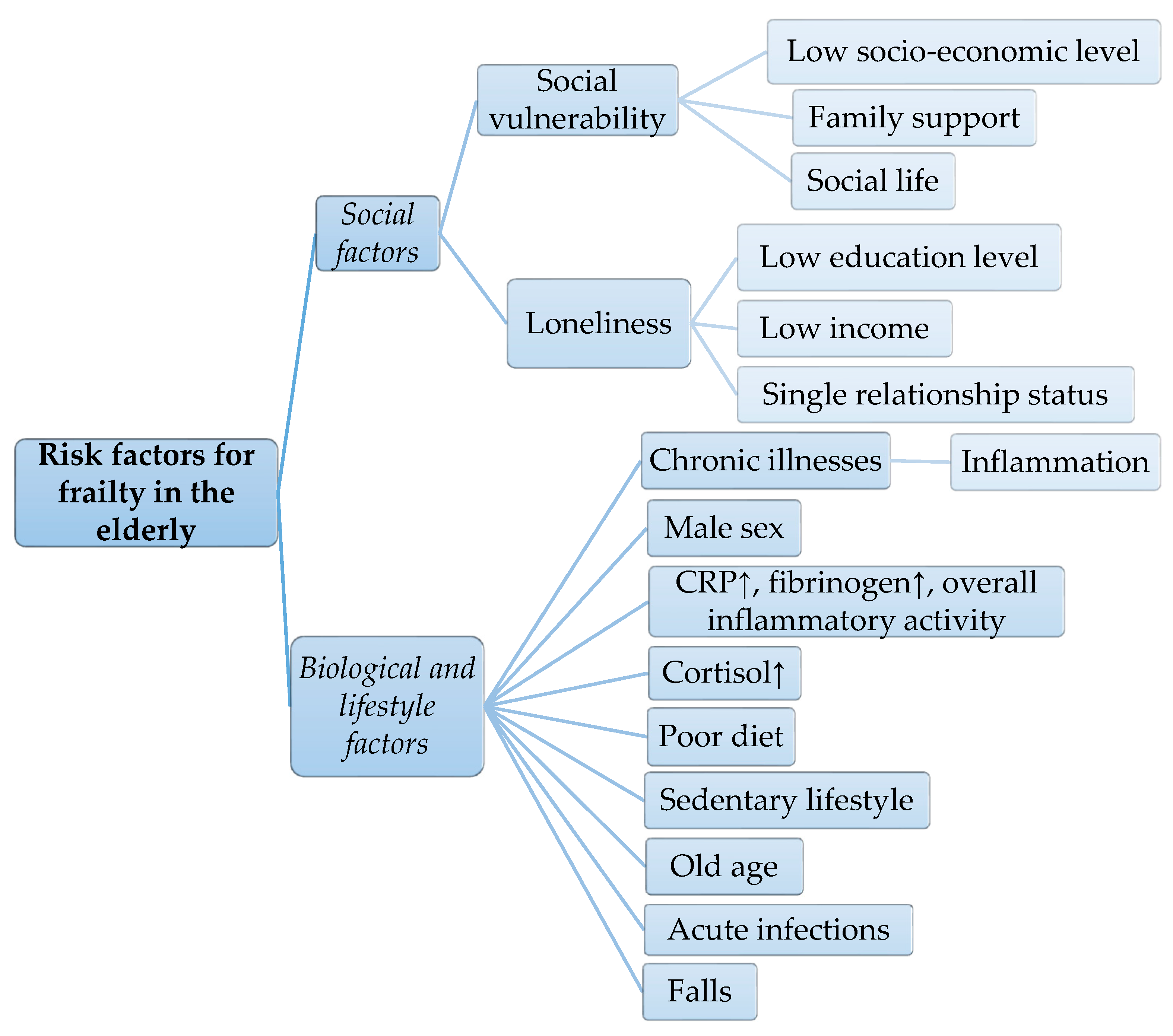

Table 1.
The search strategy summary.
| Criteria | |
|---|---|
| Date of search | |
| September-December 2023 | |
| Databases and other sources searched | Index Medicus |
| PubMed | |
| Search terms used | loneliness AND frailty AND (fulltext:(“1” OR “1”) AND mj:(“Frail Elderly” OR “Aging” OR “Geriatric Assessment” OR “Health of the Elderly” OR “Quality of Life” OR “Activities of Daily Living” OR “Primary Health Care” OR “Risk Factors” OR “Prevalence”) |
| Timeframe | 2013–2023 |
| Inclusion and exclusion criteria | Descriptive or analytic studies enrolling adult patients (over 60 years of age) diagnosed with frailty and/or loneliness; subsequently identified studies that met the mentioned inclusion criteria |
| Selection process | Two independent authors (E.B. and A.C.G.) evaluated and included the eligible articles. Different opinions were discussed with the other authors until a consensus was reached. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



