
Submitted:
06 July 2024
Posted:
08 July 2024
You are already at the latest version
Abstract
Oral candidiasis is a common problem among immunocompetent patients. The frequent resistance of Candida strains to popular antimycotics makes it necessary to look for alternative methods of treatment. The authors conducted a systematic review following the PRISMA 2020 guidelines. The objective of this review was to determine whether curcumin-mediated aPDT and blue light could be considered as an alternative treatment for oral candidiasis. PubMed, Google Scholar and Cochrane Library databases were searched using a combination of the following keywords: (Candida OR candidiasis oral OR candidosis oral OR denture stomatitis) AND (curcumin OR photodynamic therapy OR aPDT OR photodynamic antimicrobial chemotherapy OR PACT OR photodynamic inactivation OR PDI). The review included in vitro laboratory studies with Candida spp., in vivo animal studies, and randomized control trials (RCTs) involving patients with oral candidiasis or prosthetic stomatitis, published only in English. The method of elimination of Candida species in the studies was curcumin-mediated aPDT. 757 studies were identified. Following the analysis of the titles and abstracts of the studies, only 42 studies were selected for in-depth screening, after which 26 were included in this study. All studies evaluated the antifungal efficacy of curcumin-mediated aPDT against C. albicans and non-albicans Candida. In studies conducted with planktonic cells solutions, seven studies demonstrated complete elimination of Candida spp. cells. The remaining studies demonstrated only partial elimination. In all cases, experiments on single-species yeast biofilms demonstrated partial, statistically significant inhibition of cell growth and reduction of biofilm mass. In vivo, curcumin-mediated aPDT has shown good antifungal activity against oral candidiasis also in an animal model. However, its clinical efficacy as a potent therapeutic strategy for oral candidiasis requires further RCTs.
Keywords:
aPDT
; Candida
; diode laser
; oral candidiasis
; planktonic cells
; biofilm
Keywords: aPDT; Candida; diode laser; oral candidiasis; planktonic cells; biofilm
1. Introduction
Candida species (C. spp.) are commensal yeasts found on various mucosal surfaces and human skin. A properly functioning immune system limits excessive growth [1,2]. However, in immunocompromised individuals, Candida spp. can become opportunistic pathogens that cause candidiasis. The development of this disease is influenced by both local and systemic factors. Local factors include the use of dentures, poor oral hygiene, dry mouth, smoking, and long-term use of inhaled corticosteroids. Systemic factors include immunodeficiency (such as HIV infection), diabetes mellitus, hematologic diseases (such as leukemia), dysbiosis caused by long-term antibiotic therapy, chemotherapy, use of immunosuppressive drugs after transplantation, and advanced age [3]. Candidiasis is the most prevalent infectious condition of the oral mucosa, and Candida albicans is the most frequently isolated species for oral infections [4]. Candida spp. possess a range of virulence factors, such as strong adhesion and biofilm formation, which impede drug action and increase resistance to antimicrobial agents. Additionally, they exhibit resistance to host defense mechanisms and oxidative stress, produce tissue-destructive hemolytic enzymes, and develop resistance to previously used antifungal drugs [5]. Candida species release proteinases, phospholipases, and acidic metabolites, which damage the structure and function of human cells [6]. The filamentous form (hyphae) of Candida albicans invades the oral mucosa epithelium through endocytosis mediated by epithelial cells or active penetration, where a live hypha penetrates through or between cells. This invasion results in necrosis or apoptosis of cells, causing damage to the colonized epithelium [7]. Systemic candidemia can lead to a high mortality rate, especially in severe cases [8]. Additionally, Candida auris is a rare and highly resistant strain that poses a significant threat, with resistance rates higher than other Candida species. It is known to cause invasive infections in immunocompromised patients, particularly in hospital wards [9]. Candida spp. increase the risk of developing oral squamous cell carcinoma by producing carcinogenic substances such as endogenous nitrosamines and acetaldehyde. The infection causes hydrolases and esterases to promote metaplasia and cause changes in the morphology and genotype of cells. These substances are formed from nitrites and nitrates and are direct carcinogens. This predisposes to the development of precancerous conditions and tumors [10].
To effectively treat oral candidiasis, it is crucial to focus on excluding predisposing factors, improving oral and denture hygiene, discontinuing wearing dentures at night, and cushioning or replacing dentures. Local or systemic antifungal therapy is the traditional pharmacological treatment, which includes four main types of antifungal drugs: polyenes, azoles, allylamines, and echinocandins [11]. By following these methods, successful treatment of oral candidiasis can be achieved with confidence. This treatment may cause adverse effects, such as hepatotoxicity in older individuals. However, it is important to note that the response to treatment can be slow and its effectiveness may be low, with a high risk of disease recurrence [12]. Prolonged exposure to medication or repeated cycles of pharmacological treatment can lead to treatment failures due to the development of microorganism resistance. Although nystatin suspension is currently the first-line drug for the treatment of oral candidiasis, it must be used several times a day for an extended period, which often results in drug resistance and various side effects such as abdominal pain, diarrhea, nausea, vomiting, taste disorders, loss of appetite, and irritation of the mucous membrane [13]. Systemic use of fluconazole or amphotericin B is suggested for patients with lowered immunity. It is important to note that azole group drugs have fungistatic rather than fungicidal effects, which may result in insufficiently effective treatment of immunocompetent patients [14,15].
Alternative methods such as the use of plant derivatives in phytotherapy, probiotics that restore the balance of oral microbiota in the presence of dysbiosis, and antimicrobial photodynamic therapy (aPDT), confidently support or replace traditional pharmacotherapy due to the decreasing efficacy of candidiasis treatment and the development of resistant strains. aPDT is a highly selective operation that destroys microorganisms in a nonspecific manner, without any side effects [16]. The treatment has a high antimicrobial potential and is minimally invasive. Unlike conventional treatments, aPDT does not require a high drug dose to be maintained during therapy. Additionally, the development of microbial resistance is unlikely due to the lack of a specific target in the body [17]. APDT is an effective method for promoting cell damage and death in Candida support species. This therapy involves combining a photosensitizing agent (PS) and a light source that corresponds to the PS absorption band, which in the presence of oxygen causes the formation of reactive species such as singlet oxygen, superoxide radical, hydroxyl radical, and hydrogen peroxide. These products, as a result of the generated oxidative stress, promote cell damage and death [18]. Yeast cells can protect themselves against oxidative stress due to their adaptive abilities. Their larger size, complex structure, thick cell wall, and nuclear membrane make it difficult for aPDT and PS to penetrate the cell. This reduces the number of singlet oxygen targets per unit volume of the cell, requiring higher concentrations of photosensitizer and light doses to effectively inactivate the yeasts. Candida spp. increase the regulation of antioxidants by producing enzymes such as superoxide dismutase and catalase [11].
Curcumin, a natural compound found in turmeric, has been shown to have antioxidant properties. This substance has a wide range of beneficial effects, including anti-inflammatory, antioxidant, anticancer, and antimicrobial properties. It has been shown to alter the integrity of cell membranes and affect membrane-associated proteins [19]. Additionally, it promotes wound healing and epithelial regeneration by stimulating growth factors, activating fibroblasts, promoting granulation tissue formation and collagen synthesis, and neovascularization [20]. Furthermore, it has been demonstrated to effectively absorb blue light. The antifungal effect of curcumin as a PS in photodynamic therapy has been demonstrated to be achieved at 20 µM with light and at 173.73 µM without light [7]. Curcuminoids, including curcumin, demethoxycurcumin, and bisdemethoxycurcumin, have slightly different properties [21]. Bisdemetoxycurcumin binds effectively to bacterial cell walls through hydrogen bonds. However, its disinfectant properties are reduced due to the presence of methoxy groups. It is important to note that curcumin is the strongest antioxidant, followed by demethoxycurcumin and bisdemethoxycurcumin [13]. The clinical application of curcumin is hindered due to its insolubility in water, rapid degradation by hydrolysis, proteolysis, and photodegradation, as well as low bioavailability [22]. However, curcumin can be effectively dissolved in solvents such as 10% dimethyl sulfoxide (DMSO) and ethanol or propylene glycol [23].
This study aimed to evaluate, by a systematic review of in vitro studies, animal studies, and randomized clinical trials, the possibility of eliminating Candida spp. causing oral candidiasis using curcumin-mediated aPDT.
2. Material and Methods
2.1. Focused Question
A systematic review was conducted following the PICO framework, as follows: do C. albicans and non-albicans Candida strains, that often cause oral candidiasis (Population), subjected to curcumin-mediated aPDT (Intervention) compared to the irradiation of blue light alone, curcumin as PS alone or other pharmacological treatment methods (Comparison), result in their eradication or more effective elimination (Outcome)?
2.2. Information Sources and Search Strategy
The review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines [24]. An electronic search through PubMed/Medline, Google Scholar, and Cochrane Library databases was conducted. The following Medical Subject Headings (MeSH) terms, keywords, and their combinations were used: (Candida OR candidiasis oral OR denture stomatitis) AND (photodynamic therapy OR aPDT OR photodynamic antimicrobial chemotherapy OR PACT OR photodynamic inactivation OR PDI OR curcumin). The databases were searched by three authors, each of whom searched separately using the same search terms. The authors then applied additional electronic filters (articles published between January 1, 2007, and January 16, 2024, and only reports published in English). After screening and selecting potential studies for inclusion in the review, all authors jointly assessed the titles and abstracts of the above articles to see whether the study met all inclusion criteria. Subsequently, to collate data from the included studies, the authors performed a collaborative search of the full texts to identify the desired data. Additionally, the authors conducted a snowball search to identify further studies. This involved searching the reference lists of publications that were deemed eligible for full-text review.
2.3. Study Selection
This study hypothesized that curcumin-mediated aPDT may effectively reduce Candida strains and be a supportive or alternative method of treating oral candidiasis to traditional pharmacological methods of treatment. The criteria for the inclusion and exclusion of articles from this review were as follows.
Inclusion criteria:
- in vitro studies involving C. albicans or other non-albicans Candida stains,
- animal studies involving C. albicans or other non-albicans Candida stains,
- RCTs involving patients with oral candidiasis or denture stomatitis,
- Candida elimination method used in vitro studies, in animal studies, and RCT was curcumin-mediated aPDT.
Exclusion criteria:
- case reports or case series,
- letters to the editor,
- historic reviews,
- reviews or systematic reviews,
- books and documents,
- duplicated publications or studies with the same ethical approval number,
- studies published in a non–English language,
- general medical applications,
- aPDT form not used as therapy,
- curcumin used not as a photosensitizer,
- other PS than curcumin was used,
- blue light used without PS,
- no Candida strains evaluated,
- endodontic, carious, or bone models, not related to oral candidiasis.
2.4. Risk of Bias in Individual Studies
In the initial phase of the study selection process, each reviewer individually assessed titles and abstracts to mitigate potential biases in the evaluation process. Cohen’s к test was employed as a tool to quantify the level of inter-reviewer agreement [25]. Any discrepancies regarding the inclusion or exclusion of a study in the review were discussed by the authors until a consensus was reached.
2.5. Quality Assessment and Risk of Bias across Studies
Two reviewers (M.K. and R.W.) conducted independent screenings of the included studies to assess their quality. The criteria used to determine the design, implementation, and analysis of the study were based on the presence of key information for the course of aPDT and the objectivity and verification of study results. The risk of bias was determined by the number of “yes” or “no” responses to the questions below that were assigned to each study.
- Was there a specific concentration of photosensitizer?
- Was the origin of the photosensitizer provided?
- Was an incubation time indicated?
- Were the light source parameters provided, such as type, wavelength, output power, fluence, and power density?
- Were clinical strains of Candida spp. used in the study?
- Was a negative control group included?
- Are numerical results (statistics)?
- No missing outcome data?
Additionally, in the case of RCT:
- Did the study include at least 10 patients per group?
- Was there a minimum 6-month follow-up period?
The information collected about the research was assessed. The classification was based on the total number of “yes” answers to the above questions. In the current study, the degree of bias was calculated according to the point limits given below:
1) High risk: 0-3
2) Moderate risk: 4-6
3) Low risk: 7-8
The scores for each study were calculated, and an overall estimated risk of bias (low, moderate, high) was determined for each included study, following the recommendations outlined in the Cochrane Handbook for Systematic Reviews of Interventions [26].
2.7. Data Extraction
Having reached a consensus regarding the selection of included articles, the two reviewers (M.K. and G.D.) involved subsequently extracted data regarding:
- citation (first author and publication year),
- type of study,
- type of Candida strains used in the study,
- test/control groups,
- follow-up,
- outcomes,
- type and parameters of the light source,
- curcumin concentration,
- use of nanocarriers and additional substances, incubation, and irradiation time.
3. Results
3.1. Primary Outcome
The primary objective of this systematic review was to assess the efficacy of curcumin-mediated aPDT in the eradication of Candida strains responsible for oral candidiasis and to examine the methodologies employed in the studies.
3.2. Study Selection during Full-Text Analysis
A flowchart representing the research approach following the PRISMA 2020 statement [24] is displayed in Figure 1.
A primary search of the databases yielded 757 articles. After applying the additional electronic filters (published in the period from 01/01/2007 to 16/01/2024, and only English language reports), the preliminary number of 757 articles was reduced to 700, and were selected for the title and abstract screening, and after the screening, 658 studies were excluded as they did not fulfill the inclusion criteria. After the removal of 4 duplicated articles, a total of 38 studies underwent a comprehensive analysis of their full texts. Nine of these studies were excluded due to failing to meet the predefined exclusion criteria [27,28,29,30,31,32,33,34,35]. Table 1 presents the excluded studies and the reason for their exclusion.
3.3. Quality Assessment Presentation
Table 2 presents the risk of bias in 29 studies included after full-text analysis. Only studies that scored at least 6 points were included in the review. Of the included studies, 22 studies received a low risk of bias (2 studies received a maximum score of 8/8 [14,36]; the remaining 20 studies received a maximum score of 7/8 [5,11,13,15,23,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]. Seven studies received a moderate risk of bias, with four rated 6/8 [7,52,53,54], and three rated 5/8 [6,55,56]. None of the studies were rated at high risk of bias. Two studies that scored less than 6 points were excluded from further analysis due to the previously adopted criterion.
3.4. Data Presentation
Table 3, Table 4 and Table 5 present the extrapolated data regarding the general characteristics of all 26 studies finally included in the review that fulfilled the eligibility criteria, had characteristics of light sources, and the characteristics of curcumin used as photosensitizers in aPDT protocols.
3.5. General Characteristics of the Included Studies
A total of 26 studies were included in the review. Table 3 lists the articles that met the inclusion criteria. Of these, 19 were in vitro laboratory studies [5,11,13,15,23,36,39,41,43,45,46,47,48,49,50,51,52,53,54], 1 was an in vitro study with additional in situ examination in the oral cavity [42], 3 were in vivo animal studies (a mouse model of oral candidiasis) [7,38,40], and the remaining 3 were randomized controlled trial [14,37,44].
The materials tested in vitro included planktonic cell solutions (three studies) [11,23,43], single-species biofilms (six studies) [5,13,39,42,50,51], and planktonic cultures and biofilms (eleven studies) [15,36,41,45,46,47,48,49,52,53,54]. Animal models were employed, including a mouse model of oral candidiasis after prior pharmacological immunosuppression (prednisolone + tetracycline) [7,38,40].
In vitro studies with planktonic cell solutions were conducted in 96- [5,11,15,36,41,42,45,46,47,48,49,53], 24- [39,42,43,50], and 6-well [13,51] titration plates, Eppendorf tubes [23,54], or Petri dishes [52]. Biofilm studies were conducted on silicone [39], acrylic [50], or Sabouraud dextrose agar [52].
The Candida strains that were tested included Candida albicans (twenty-four tests) [5,7,11,13,14,15,23,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54], Candida krusei (two tests) [37,44], Candida glabrata (five tests) [14,15,37,47,50], Candida tropicalis (four tests) [14,37,43,47], Candida duliniensis (two tests) [15,36], and Candida parapsilosis (one test) [37]. The majority of the studies employed reference strains from the American Type Culture Collection, with five studies utilizing clinical strains (obtained from patients with oral candidiasis) [14,36,37,44,47]. Nineteen studies were conducted exclusively on Candida spp. strains, while eight studies additionally tested: Escherichia coli [39], Staphylococcus aureus MRSA [39,41,49], Streptococcus mutans [41,42,46,50], Aspergillus niger [23,52], Aspergillus flavus [52], Lactobacillus casei [42], Penicillinum griseofulvum [52], Penicillinum chrysogenum [52], Fusarium oxysporum [52], Zygosaccharomyces bailii [52], and Pseudomonas aeruginosa [49].
The experimental groups in the studies analyzed typically included the following treatments: (PS+L+) light irradiation in the presence of a photosensitizer; (PS-L+) light-only treatment without a photosensitizer; (PS+L-) application of only a photosensitizer without the presence of light. The negative control group (PS-L-) consisted of leaving the planktonic cell solution or biofilm in the dark without exposure to light or photosensitizer (curcumin).
3.6. Characteristics of Light Sources Used in aPDT
The characteristics of the physical parameters of the light sources that met the inclusion criteria are presented in Table 4.
In the 22 papers analyzed, a light-emitting diode (LED) was used as the light source, with thirteen studies having a maximum emission peak of 455 nm [7,11,14,15,36,38,40,41,44,45,47,49,50]; five studies 450 nm [5,42,43,48,51]; two studies 430 nm [39,53]; and single studies 435 nm [23], 460 nm [46], 480 nm [37]. The output power of the light sources ranged from 18-480 mW, and the fluences used were in the range of 1.32-200 J/cm2.
In one study, a 405 nm diode laser was used to perform aPDT [54].
3.7. Characterization of Curcumin Used as a Photosensitizer in aPDT.
Characteristics of curcumin used as a photosensitizer in aPDT in studies that met the inclusion criteria are shown in Table 5.
In 21 studies, curcumin was the sole photosensitizer utilized [7,11,13,15,23,36,38,39,40,41,42,43,44,45,46,47,49,50,51,52,53]. In five studies, the efficacy of aPDT with curcumin was compared with other photosensitizers, including methylene blue (one study) [37], Photodithazine (two studies) [5,48], Rose Bengal (one study) [14], toluidine blue (one study) [54], and erythrosine (one study) [54]. In two studies, the efficacy of curcumin-mediated aPDT was further enhanced by the addition of titanium nanodioxide or erythrosine (one study) [13] or potassium iodide (one study) [51]. A total of eighteen studies employed free curcumin [5,48], while in seven studies curcumin was incorporated into previously synthesized formulations, including nanocarriers, nanoparticles, micelles (five studies) [7,23,41,46,49], a microemulsion (one study) [39], or a bioadhesive formula (one study) [42]. Two studies have used curcumin derivatives: bisdemethoxycurcumin and demethoxycurcumin [13,51]. Two studies combined antimicrobial photodynamic therapy with pharmacotherapy: fluconazole (one study) [53] and a commercial antifungal gel- miconazole (one study) [44].
The incubation times employed in the studies were either empirically derived, derived by the authors based on previous studies by other authors, or were previously employed by the authors as a preliminary test. The incubation time used in the studies ranged from 1 min to 40 min. The most frequently used incubation times were 20 min (sixteen studies) [5,7,11,15,36,38,40,43,45,47,48,49,50,51,52,53] and 5 min (six studies) [15,23,39,42,45,46]. In two studies, the incubation time used was not reported [54,56].
The photosensitizer added to the planktonic cells solution or biofilm was kept in the dark, in a darkened room, or under an adhesive dressing until irradiation in all evaluated studies. During the incubation time, in all studies using planktonic solutions, care was taken to thoroughly mix curcumin with the solution.
4. Discussion
All studies that met the inclusion criteria for the review showed significant efficacy of curcumin-mediated aPDT against Candida spp. (efficacy is understood as a reduction in cell number or a reduction in % CFU/ml). In studies conducted with planktonic yeast cell solutions, seven studies showed complete elimination of Candida spp. cells. [15,45,47,48,52,53,54], and the others showed a partial, statistically significant reduction compared to the control group. Similarly, in all cases of experiments performed on monocellular yeast biofilms, only partial growth inhibition and mass reduction were observed after curcumin-mediated aPDT.
In in vivo studies on a mouse model of candidiasis, a statistically significant elimination of yeast from the mucosa, compared to the control group, was observed [7,38]. In a study by Dovigo et al., the results even showed complete elimination of C. albicans from the lingual mucosa in test mice after a single therapeutic intervention (LED 455 nm, fluence 37.5 J/cm2, power density 89.2 mW, curcumin concentration 80 µM) [40]. The therapy was independent of the stage of biofilm development. There was a reduction in the number of yeasts and hyphae in the biofilm [7]. Curcumin-mediated aPDT also promoted a reduction in the expression of C. albicans genes related to adhesion and biofilm formation and genes responsible for the oxidative stress response [5].
In clinical trials with patients, curcumin-mediated aPDT was effective in reducing the number of Candida spp. cells. [14,37,44]. A clinical study by Labban et al. found aPDT to be as effective as topical nystatin therapy - oral rinsing with a nystatin suspension at a concentration of 100,000 UI/mL for 60 seconds, four times a day, for 15 days (no statistical significance between study groups) [14]. Another study by Al-Ghamdi et al. confirmed a reduction in the mycological burden on the mucosa of the prosthetic field compared with conventional therapy with an antifungal gel containing miconazole (2% Daktarin Gel Oral, Janssen-Cilag Pharmaceutica, Belgium) and a reduction in the levels of the pro-inflammatory cytokines IL-6 and MMP-8 in the saliva of patients with prosthetic stomatitis [44].
In studies comparing the efficacy of curcumin-mediated aPDT on different yeast strains, a better effect was observed for C. albicans compared to other non-albicans Candida strains [14,15,43,47,50]. Elimination of the clinical strain C. glabrata required higher concentrations of curcumin than C. albicans and C. tropicalis, yet no eradication of C. glabrata was observed, in contrast to C. albicans and C. tropicalis [47]. In addition, reference strains showing resistance to fluconazole and clinical strains obtained from patients with oral candidiasis showed sensitivity to curcumin-mediated aPDT [14,36,37,44,47]. However, this was lower than the reference strains, which did not show antifungal drug resistance. In a study by Sanita et al., no differences in the efficacy of photodynamic therapy between clinical and reference strains were found for C. dubliniensis [36]. Combined pharmacological treatment with fluconazole at a concentration of 208 µM for 24 hours together with photodynamic therapy using 20 µM curcumin and 430 nm light at a fluence of 9 J/cm2 was able to significantly reduce up to 5% of C. albicans biofilm cell viability when pharmacological monotherapy or photodynamic therapy alone was not sufficiently effective [53]. Experiments on animal models [7,38,40] also confirmed the reduced adhesion of C. albicans to epithelial cells and their ability to penetrate deep into the epithelium (reduced thigmotropism). Yeast cells, on microscopic examination, were only detected in the stratum corneum of the epithelium on the dorsal surface of the tongue [38,40]. In addition, histopathological examination of the epithelium and its lining after aPDT treatment showed only a small number of inflammatory cells in the tissue, which suggested, according to the authors, that the treatment did not exacerbate the inflammatory response of the host tissues [7,38]. Curcumin-mediated aPDT also showed no cytotoxicity to human gingival fibroblasts [13] and to the invertebrate model G. mellonella [43,54].
The efficacy of antimicrobial photodynamic therapy is strongly dependent on many variable parameters of the algorithm, hence the large discrepancy in results obtained by authors using different therapeutic protocols. One of the key elements is the correct selection of the appropriate wavelength of the light source. In photodynamic therapy, it is extremely important that the electromagnetic wavelength of the light used is matched as closely as possible to the maximum absorption of the PS used. Curcumin shows maximum absorption at 430 nm. In Table 3, in the column describing the wavelength of the light source used in the experiment, it is clear that there are large differences in this parameter. A diode laser, with a wavelength of 405 nm [54], LEDs, with a maximum light emission of 430-480 nm were used in 22 studies [5,7,11,14,15,23,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,53]. However, the most commonly used wavelength was 455 nm [7,11,14,15,36,38,40,41,44,45,47,49,50].
Also, blue light alone, without curcumin, shows fungicidal activity against Candida spp. (CUR-L+). It stimulates naturally occurring endogenous photosensitizers in pathogen cells and subsequently leads to the production of cytotoxic oxidative forms. [57,58]. Using the same fluence of blue light as aPDT, however, the efficacy is much lower than when combined with a photosensitizer. In the Jordao et al. study, treatment with blue LED alone (35.7 J/cm2 and 50 J/cm2) promoted a reduction in the expression of C. albicans genes responsible for biofilm formation [5]. Also, a study by Carmello et al. showed that blue LED promoted DNA damage to C. albicans [11]. In contrast, in a study by Dias et al. there was a reduction in both planktonic cell solution and biofilm cells in groups treated with light alone [48].
The second important variable element of the aPDT algorithm is the incubation time used (the time between the addition of PS to, for example, the planktonic solution and the start of irradiation - an extremely important time, as it is needed for the right amount of PS to reach the cell membrane and cytoplasm of the yeast cells). In a study by Schamberger et al. comparing the efficacy of photodynamic therapy applied with different incubation times, it was shown that shorter incubation times resulted in a more pronounced increase in aPDT efficacy against yeast in planktonic solution, indicating the limited stability of curcumin in aqueous solution [23]. Curcumin at a concentration of 50 µM irradiated immediately after being injected into solution (incubation time - 30 seconds) showed strong antimicrobial activity. The use of a five-minute incubation time resulted in a decrease in the efficacy of curcumin-mediated aPDT. Increasing the incubation time to 25 min further enhanced this effect [23]. A completely different result was shown in a study by Andrade et al. In a planktonic solution, the use of different incubation times (1, 5, 10, and 20 min), while keeping the light source settings constant, showed no statistical differences in the elimination efficacy of C. albicans, C. glabrata and C. dubliniensis [15].
The combination of 20 µM curcumin and LED light (fluence 5.28 J/cm2, power density 22 mW/cm2) after 5-, 10-, and 20-minute incubation time, promoted the complete elimination of yeast cells. Therefore, the conclusion was drawn that long incubation times are not required for yeast elimination using curcumin-mediated aPDT. In addition, in the same study, the penetration of curcumin deep into biofilms was also checked at different incubation times. Biofilms after 5- and 20- minute of incubation with 40 µM curcumin were observed with a Leica TCS SPE confocal microscope (Leica Microsystems GmbH, Wetzlar, Germany) in fluorescence mode, using an excitation wavelength of 405 nm and green fluorescence (emission from 450 to 600 nm). Despite the bright green fluorescence observed after a 5-min incubation, brighter fluorescence was observed after a 20-min incubation. Significantly deeper penetration of curcumin after 20 min into monoculture biofilms was observed than after 5 min. Therefore, longer incubation times have been recommended for biofilm elimination [15]. A study by Al-Asmari et al. confirmed that incubating yeast cells with photosensitizer for 10, 20, and 30 min before irradiation showed no significant difference in their reduction [52].
The concentration of the PS used in antibacterial photodynamic therapy against Candida spp. is of paramount importance. Due to the large size of yeast cells (approximately 25-50 times larger than bacteria) and the more complex cell structure (thick cell wall and the presence of a cell nucleus separated from the cytoplasm by a nuclear membrane), a higher concentration of curcumin is required than for the elimination of bacteria [59]. Also, curcumin concentrations used for biofilm destruction must be higher than for planktonic solutions, mainly due to the thickness and complex structure of the biofilm [60]. Several studies have comparatively used different concentrations of photosensitizer [5,15,23,36,38,40,45,47,50,53]. The concentrations of curcumin that obtained the best fungicidal effect in these studies were determined to be: 80 µM [5,38,40,50,53], 40 µM [15,36,47], 20 µM [36,45], 60 µM [39] and 50 µM [23]. The proposed differences can be explained by the different effects of PS concentration on Candida spp. planktonic solutions and monocellular biofilm structures.
In none of the analyzed biofilm studies, complete elimination of Candida spp. cells in this structure were achieved at any of the curcumin concentrations tested.
In a study by Dovigo et al., on a mouse model of oral candidiasis, the application of 20, 40, or 80 µM curcumin with 455 nm light (fluence 37.5 J/cm2; power density 89.2 mW, incubation time 7 min) was able to cause a statistically significant reduction in the number of viable Candida cells compared to untreated mice. However, only a concentration of 80 µM curcumin led to the complete elimination of C. albicans from the mucosa of mouse tongues [40].
The use of a photosensitizer on nanocarriers or as a micellar solution [7,41,46,49] required higher concentrations of curcumin. In two studies, the highest concentration of curcumin evaluated was 260 µM (higher concentrations caused curcumin aggregation) [7,41].
Also, curcumin itself has been shown to exhibit anticancer, antioxidant, anti-inflammatory, and antimicrobial activities and to promote wound healing [61]. As one of the natural products, curcumin has been extensively studied as a drug candidate and has been reported to exhibit antifungal activity against Candida spp. [62]. In a study by Sanita et al., exposure to curcumin alone at the highest concentrations used (30 µM, 40 µM) significantly reduced the viability of the C. dubliensis biofilm compared to the control group. In contrast, in the study by Dias et al. in the C+L- (40 µM) groups, there was a reduction in both planktonic forms and C. albicans biofilm cells [48]. Curcumin at lower concentrations showed no inhibitory effect on Candida spp. Sublethal doses of curcumin showed antifungal effects only when activated with light.
Another very important element influencing the efficiency of the photodynamic response is the physical parameters of the light source, expressed in particular as energy density (fluence). Six studies have compared the effects of different fluences on the efficiency of curcumin-mediated aPDT [5,39,45,47,52,54]. In several of these, complete elimination of planktonic forms of C. albicans was achieved. In the study by Dovigo et al. the most effective and complete elimination of planktonic forms of C. albicans occurred at a fluence of 37.5 J/cm2 (455 nm), combined with a curcumin concentration of 20 µM. Furthermore, the minimum fluence causing complete yeast inactivation in this study was 5.28 J/cm2 [45]. In contrast, a study by Merigo et al. reported 100% inhibition of yeast growth in a planktonic solution using 405 nm diode laser light, with fluences of both 10, 20, and 30 J/cm2) [54]. Comparing the results of all the studies in which complete eradication of C. albicans in planktonic solution was achieved [15,45,47,48,53,54], the fluences used ranged from 5.28 to 18 J/cm2, and these were lower values than when acting with photodynamic therapy on biofilm structures.
In studies in which curcumin-mediated aPDT was directed against Candida spp. biofilms, the applied fluences were higher than in studies conducted on planktonic forms. Applied fluences ranged from 10.8 to 96 J/cm2 [5,13,39,41,42,46,49,50,51,52]. However, no study achieved complete elimination of yeast in the biofilm. In a study by Jordao et al., a C. albicans strain was subjected to LED irradiation (450 nm). At a fluence of 50 J/cm2, the greatest reduction in the expression of C. albicans genes responsible for biofilm formation and adhesion and for the oxidative stress response was observed [5]. The most promising results of photodynamic therapy in in vivo studies were observed in another study by Dovigo et al. in an animal model using 80 µM curcumin and 37.5 J/cm2 fluence irradiation [40]. In a clinical study by Fonseca et al., it was observed that curcumin with a concentration of 80 µM, irradiated with 480 nm light at a fluence of 200 J/cm2, generated a higher amount of free radicals, which is associated with better biofilm elimination [37].
In some of the studies reviewed, additional chemicals were used as additives to increase the efficacy of curcumin-mediated aPDT. In two studies in which curcumin derivatives were used, erythrosine, titanium nano-oxide, or potassium iodide were added to increase the effectiveness of the therapy [13,51]. In the study by Kanpittaya et al., the greatest reductions in biofilm composed of C. albicans cells were achieved using 20 µM bisdemethoxycurcumin in combination with 110 µM erythrosine and when 20 µM bisdemethoxycurcumin was used with 110 µM erythrosine and 10% titanium nano-oxide. These PS with additives achieved statistically significantly higher fungicidal efficacy than pure forms of curcumin derivatives [13]. In a study by Damrongrungruang et al., a therapy combining 40 µM bisdemethoxycurcumin and 110 mM potassium iodide applied for 1 hour showed the greatest reduction in C. albicans biofilm comparable to 1:100 000 IU/mL nystatin therapy [51].
Two clinical trials reported the use of curcumin-mediated aPDT as an adjunctive treatment to pharmacotherapy [44,53]. The clinical study by Al-Ghambi et al. evaluated the treatment of oral candidiasis with an antifungal gel containing miconazole supported by antimicrobial photodynamic therapy. During the 2-month intervention and follow-up of individual patients, all participants were instructed on denture and oral hygiene. In the control group, patients were instructed to apply a topical antifungal gel, hold it in the mouth for 60 seconds, then spit it out. The procedure was repeated four times a day for 15 days. However, in the study group, curcumin-mediated aPDT was added to the antifungal gel treatment protocol. The denture surface and palate were sprayed with 5 ml of PS and then irradiated for 26 min after a 30 min incubation before irradiation. Curcumin-mediated aPDTwas carried out for 4 weeks and 8 weeks, twice a week with a 48-hour break between each session.
Participants in the study undergoing combination therapy showed a significant reduction in C. albicans and C. krusei abundance compared to the group treated with antifungal gel alone [44]. A study by Hsieh et al. on the effect of the combined drug and photodynamic therapy on C. albicans biofilm showed that neither aPDT treatment (reduction to 15%) nor fluconazole monotherapy (reduction to 55% after 24 h and to 20% after 48 h) was sufficiently effective to completely eradicate the infection. In contrast, two treatment protocols: treatment with 208 µM fluconazole for 24 h followed by single aPDT with 20 µM curcumin (fluence 9 J/cm2) or treatment with 208 µM fluconazole for 48 h followed by aPDT with 10 µM curcumin (fluence 9 J/cm2) reduced yeast cells to 5% [53].
Five studies compared curcumin with other photosensitizers used in aPDT to eliminate Candida spp. [5,14,37,48,54]. Studies by Jordao et al. and Dias et al. showed that Phenothiazine was as effective as curcumin in inactivating yeast [5,48]. Bengal Rose [14], erythrosine, and toluidine blue [54] are less effective against Candida spp. while methylene blue [37] showed a stronger effect. The above studies suggest that curcumin is one of the more effective photosensitizers currently used in aPDT for the treatment of oral candidiasis.
5. Conclusions
Curcumin-mediated aPDT against Candida spp. may be an effective alternative form of therapy for oral candidiasis associated with restorations. It appears to be particularly useful when dealing with strains resistant to conventional antifungal agents, which is proving increasingly common in clinical practice. APDT can also be used in combination therapy with conventional drug treatment, resulting in much more effective destruction of yeast than monotherapies used. A limitation of aPDT is that it can only treat superficial, localized areas that are accessible for irradiation. The aPDT protocol often requires several minutes of PS incubation before irradiation, which is difficult to achieve in the oral cavity due to saliva flow, among other reasons. Therefore, attempts are being made to place curcumin in nanocarriers to increase curcumin stability or in adhesive formulations to facilitate application. Despite many laboratory studies, optimal PS concentrations and physical parameters of light sources have not been established, which translates into a lack of a recommended clinical protocol.
In available studies in vivo and mouse models of oral candidiasis, curcumin-mediated aPDT shows effective antifungal activity, against Candida spp. species causing oral candidiasis. However, the clinical efficacy of aPDT as an effective therapeutic method for the treatment of fungal oral infections requires further study.
Author Contributions
Conceptualization, M.K., R.W.; methodology, M.K., R.W.; formal analysis, M.K., G.D.; investigation, M.K. G.D.; data curation, M.K., G.D.; writing—original draft preparation, M.K. R.W.; writing—review and editing, M.K., R.W.; supervision, R.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lopes, J.P.; Lionakis, M.S. Pathogenesis and virulence of Candida albicans. Virulence. 2022 Dec;13(1):89-121. [CrossRef] [PubMed] [PubMed Central]
- Mukaremera, L.; Lee, K.K.; Mora-Montes, H.M.; Gow, N.A.R. Candida albicans Yeast, Pseudohyphal, and Hyphal Morphogenesis Differentially Affects Immune Recognition. Front Immunol. 2017 Jun 7;8:629. [CrossRef] [PubMed] [PubMed Central]
- Akpan, A.; Morgan, R. Oral candidiasis, Postgraduate Medical Journal, Volume 78, Issue 922, August 2002, Pages 455–459. [CrossRef]
- Millsop, J.W.; Fazel, N. Oral candidiasis. Clin Dermatol. 2016 Jul-Aug;34(4):487-94. Epub 2016 Mar 2. [CrossRef] [PubMed]
- Jordão, C.C.; Viana de Sousa, T.; Inêz Klein, M.; Mendonça Dias, L.; Pavarina, A.C.; Carmello, J.C. Antimicrobial photodynamic therapy reduces gene expression of Candida albicans in biofilms. Photodiagnosis Photodyn Ther. 2020 Sep;31:101825. Epub 2020 May 21. [CrossRef] [PubMed]
- Daliri, F.; Azizi, A.; Goudarzi, M.; Lawaf, S.; Rahimi, A. In vitro comparison of the effect of photodynamic therapy with curcumin and methylene blue on Candida albicans colonies. Photodiagnosis Photodyn Ther. 2019 Jun;26:193-198. Epub 2019 Mar 23. [CrossRef] [PubMed]
- Sakima, V.T.; Barbugli, P.A.; Cerri, P.S.; Chorilli, M.; Carmello, J.C.; Pavarina, A.C.; Mima, E.G.O. Antimicrobial Photodynamic Therapy Mediated by Curcumin-Loaded Polymeric Nanoparticles in a Murine Model of Oral Candidiasis. Molecules. 2018 Aug 19;23(8):2075. [CrossRef] [PubMed] [PubMed Central]
- McCarty, T.P.; White, C.M.; Pappas, P.G. Candidemia and Invasive Candidiasis. Infect Dis Clin North Am. 2021 Jun;35(2):389-413. [CrossRef] [PubMed]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; Berkow, E.L.; Castanheira, M.; Magobo, R.E.; Jabeen, K.; Asghar, R.J.; Meis, J.F.; Jackson, B.; Chiller, T.; Litvintseva, A.P. Simultaneous Emergence of Multidrug-Resistant Candida auris on 3 Continents Confirmed by Whole-Genome Sequencing and Epidemiological Analyses. Clin Infect Dis. 2017 Jan 15;64(2):134-140. Epub 2016 Oct 20. Erratum in: Clin Infect Dis. 2018 Aug 31;67(6):987. 10.1093/cid/ciy333. [CrossRef] [PubMed] [PubMed Central]
- Arzmi, M.H.; Dashper, S.; McCullough, M. Polymicrobial interactions of Candida albicans and its role in oral carcinogenesis. J Oral Pathol Med. 2019 Aug;48(7):546-551. Epub 2019 Jun 25. [CrossRef] [PubMed]
- Carmello, J.C.; Pavarina, A.C.; Oliveira, R.; Johansson, B. Genotoxic effect of photodynamic therapy mediated by curcumin on Candida albicans. FEMS Yeast Res. 2015 Jun;15(4):fov018. Epub 2015 Apr 20. [CrossRef] [PubMed]
- Finlay, P.M.; Richardson, M.D.; Robertson, A.G. A comparative study of the efficacy of fluconazole and amphotericin B in the treatment of oropharyngeal candidosis in patients undergoing radiotherapy for head and neck tumours. Br J Oral Maxillofac Surg. 1996 Feb;34(1):23-5. [CrossRef] [PubMed]
- Kanpittaya, K.; Teerakapong, A.; Morales, N.P.; Hormdee, D.; Priprem, A.; Weera-Archakul, W.; Damrongrungruang, T. Inhibitory Effects of Erythrosine/Curcumin Derivatives/Nano-Titanium Dioxide-Mediated Photodynamic Therapy on Candida albicans. Molecules. 2021 Apr 21;26(9):2405. [CrossRef] [PubMed] [PubMed Central]
- Labban, N.; Taweel, S.M.A.; ALRabiah, M.A.; Alfouzan, A.F.; Alshiddi, I.F.; Assery, M.K. Efficacy of Rose Bengal and Curcumin mediated photodynamic therapy for the treatment of denture stomatitis in patients with habitual cigarette smoking: A randomized controlled clinical trial. Photodiagnosis Photodyn Ther. 2021 Sep;35:102380. Epub 2021 Jun 1. [CrossRef] [PubMed]
- Andrade, M.C.; Ribeiro, A.P.; Dovigo, L.N.; Brunetti, I.L.; Giampaolo, E.T.; Bagnato, V.S.; Pavarina, A.C. Effect of different pre-irradiation times on curcumin-mediated photodynamic therapy against planktonic cultures and biofilms of Candida spp. Arch Oral Biol. 2013 Feb;58(2):200-10. Epub 2012 Nov 13. [CrossRef] [PubMed]
- Contaldo, M.; Di Stasio, D.; Romano, A.; Fiori, F.; Della Vella, F.; Rupe, C.; Lajolo, C.; Petruzzi, M.; Serpico, R.; Lucchese, A. Oral Candidiasis and Novel Therapeutic Strategies: Antifungals, Phytotherapy, Probiotics, and Photodynamic Therapy. Curr Drug Deliv. 2023;20(5):441-456. [CrossRef] [PubMed]
- Donnelly, R.F.; McCarron, P.A.; Tunney, M.M. Antifungal photodynamic therapy. Microbiol Res. 2008;163(1):1-12. Epub 2007 Nov 26. [CrossRef] [PubMed]
- Soukos, N.S.; Goodson, J.M. Photodynamic therapy in the control of oral biofilms. Periodontol 2000. 2011 Feb;55(1):143-66. [CrossRef] [PubMed]
- Amalraj, A.; Pius, A.; Gopi, S.; Gopi, S. Biological activities of curcuminoids, other biomolecules from turmeric and their derivatives - A review. J Tradit Complement Med. 2016 Jun 15;7(2):205-233. [CrossRef] [PubMed] [PubMed Central]
- Akbik, D.; Ghadiri, M.; Chrzanowski, W.; Rohanizadeh, R. Curcumin as a wound healing agent. Life Sci. 2014 Oct 22;116(1):1-7. Epub 2014 Sep 6. [CrossRef] [PubMed]
- Tonnesen, H.H.; Arrieta, A.F.; Lerner, D. STUDIES ON CURCUMIN AND CURCUMINOIDS. 24. CHARACTERIZATION OF THE SPECTROSCOPIC PROPERTIES OF THE NATURALLY-OCCURRING CURCUMINOIDS AND SELECTED DERIVATIVES. Pharmazie 1995, 50, 689–693. [Google Scholar]
- Hussain, Z.; Thu, H.E.; Ng, S.F.; Khan, S.; Katas, H. Nanoencapsulation, an efficient and promising approach to maximize wound healing efficacy of curcumin: A review of new trends and state-of-the-art. Colloids Surf B Biointerfaces. 2017 Feb 1;150:223-241. Epub 2016 Nov 30. [CrossRef] [PubMed]
- Schamberger, B.; Plaetzer, K. Photofungizides Based on Curcumin and Derivates Thereof against Candida albicans and Aspergillus niger. Antibiotics (Basel). 2021 Oct 28;10(11):1315. [CrossRef] [PubMed] [PubMed Central]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; Chou, R.; Glanville, J.; Grimshaw, J.M.; Hróbjartsson, A.; Lalu, M.M.; Li, T.; Loder, E.W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L.A.; Stewart, L.A.; Thomas, J.; Tricco, A.C.; Welch, V.A.; Whiting, P.; Moher, D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. [CrossRef] [PubMed] [PubMed Central]
- Watson, P.F.; Petrie, A. Method agreement analysis: a review of correct methodology. Theriogenology. 2010 Jun;73(9):1167-79. [CrossRef] [PubMed]
- Higgins, J.; Savović, J.; Page, M.; Elbers, R.; Sterne, J. Assessing risk of bias in a randomized trial. In: Higgins J., Thomas J., Chandler J., Cumpston M., Li T., Page M., Welch V., editors. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. John Wiley & Sons; Chichester, UK: 2019. pp. 205–228.
- Santezi, C.; Reina, B.D.; Dovigo, L.N. Curcumin-mediated Photodynamic Therapy for the treatment of oral infections-A review. Photodiagnosis Photodyn Ther. 2018 Mar;21:409-415. Epub 2018 Feb 22. [CrossRef] [PubMed]
- Ravazzi, T.P.Q.; de Jesus, I.M.; de Oliveira Santos, G.P.; Reis, T.A.; Rosa, L.P.; Rosa, F.C.S. The effects of antimicrobial photodynamic therapy (aPDT) with nanotechnology-applied curcumin and 450nm blue led irradiation on multi-species biofilms in root canals. Lasers Med Sci. 2023 Nov 6;38(1):254. [CrossRef] [PubMed]
- Pellissari, C.V.; Pavarina, A.C.; Bagnato, V.S.; Mima, E.G.; Vergani, C.E.; Jorge, J.H. Cytotoxicity of antimicrobial photodynamic inactivation on epithelial cells when co-cultured with Candida albicans. Photochem Photobiol Sci. 2016 May 11;15(5):682-90. Epub 2016 Apr 25. [CrossRef] [PubMed]
- Yasini, Z.; Roghanizad, N.; Fazlyab, M.; Pourhajibagher, M. Ex vivo efficacy of sonodynamic antimicrobial chemotherapy for inhibition of Enterococcus faecalis and Candida albicans biofilm. Photodiagnosis Photodyn Ther. 2022 Dec;40:103113. Epub 2022 Sep 10. [CrossRef] [PubMed]
- Dantas Lopes Dos Santos, D.; Besegato, J.F.; de Melo, P.B.G.; Oshiro Junior, J.A.; Chorilli, M.; Deng, D.; Bagnato, V.S.; Rastelli, A.N.S. Curcumin-loaded Pluronic® F-127 Micelles as a Drug Delivery System for Curcumin-mediated Photodynamic Therapy for Oral Application. Photochem Photobiol. 2021 Sep;97(5):1072-1088. Epub 2021 May 17. [CrossRef] [PubMed]
- da Silva, F.C.; Fernandes Rodrigues, P.L.; Santos Dantas Araújo, T.; Sousa Santos, M.; de Oliveira, J.M.; Pereira Rosa, L.; de Oliveira Santos, G.P.; de Araújo, B.P.; Bagnato, V.S. Fluorescence spectroscopy of Candida albicans biofilms in bone cavities treated with photodynamic therapy using blue LED (450 nm) and curcumin. Photodiagnosis Photodyn Ther. 2019 Jun;26:366-370. Epub 2019 May 4. [CrossRef] [PubMed]
- Reina, B.D.; Santezi, C.; Malheiros, S.S.; Calixto, G.; Rodero, C.; Victorelli, F.D.; Chorilli, M.; Dovigo, L.N. Liquid crystal precursor system as a vehicle for curcumin-mediated photodynamic inactivation of oral biofilms. J Biophotonics. 2023 Feb;16(2):e202200040. Epub 2022 Oct 13. [CrossRef] [PubMed]
- Soria-Lozano, P.; Gilaberte, Y.; Paz-Cristobal, M.P.; Pérez-Artiaga, L.; Lampaya-Pérez, V.; Aporta, J.; Pérez-Laguna, V.; García-Luque, I.; Revillo, M.J.; Rezusta, A. In vitro effect photodynamic therapy with differents photosensitizers on cariogenic microorganisms. BMC Microbiol. 2015 Sep 26;15:187. [CrossRef] [PubMed] [PubMed Central]
- Comeau, P.; Manso, A. A Systematic Evaluation of Curcumin Concentrations and Blue Light Parameters towards Antimicrobial Photodynamic Therapy against Cariogenic Microorganisms. Pharmaceutics. 2023 Nov 30;15(12):2707. [CrossRef] [PubMed] [PubMed Central]
- Sanitá, P.V.; Pavarina, A.C.; Dovigo, L.N.; Ribeiro, A.P.D.; Andrade, M.C.; Mima, E.G.O. Curcumin-mediated anti-microbial photodynamic therapy against Candida dubliniensis biofilms. Lasers Med Sci. 2018 May;33(4):709-717. Epub 2017 Nov 13. [CrossRef] [PubMed]
- Fonseca, L.L.; Durães, C.P.; Menezes, A.S.D.S.; Tabosa, A.T.L.; Barbosa, C.U.; Filho, A.P.S.; Souza, D.P.S.P.; Guimarães, V.H.D.; Santos, S.H.S.; de Paula, A.M.B.; Farias, L.C.; Guimarães, A.L.S. Comparison between two antimicrobial photodynamic therapy protocols for oral candidiasis in patients undergoing treatment for head and neck cancer: A two-arm, single-blind clinical trial. Photodiagnosis Photodyn Ther. 2022 Sep;39:102983. Epub 2022 Jun 27. [CrossRef] [PubMed]
- Mima, E.G.O.; Pavarina, A.C.; Jordão, C.C.; Vieira, S.M.; Dovigo, L.N. Curcuminoid-Mediated Antimicrobial Photodynamic Therapy on a Murine Model of Oral Candidiasis. J Vis Exp. 2023 Oct 27;(200). [CrossRef] [PubMed]
- Rocha, M.P.; Ruela, A.L.M.; Rosa, L.P.; Santos, G.P.O.; Rosa, F.C.S. Antimicrobial photodynamic therapy in dentistry using an oil-in-water microemulsion with curcumin as a mouthwash. Photodiagnosis Photodyn Ther. 2020 Dec;32:101962. Epub 2020 Aug 17. [CrossRef] [PubMed]
- Dovigo, L.N.; Carmello, J.C.; de Souza Costa, C.A.; Vergani, C.E.; Brunetti, I.L.; Bagnato, V.S.; Pavarina, A.C. Curcumin-mediated photodynamic inactivation of Candida albicans in a murine model of oral candidiasis. Med Mycol. 2013 Apr;51(3):243-51. Epub 2012 Aug 31. [CrossRef] [PubMed]
- Trigo Gutierrez, J.K.; Zanatta, G.C.; Ortega, A.L.M.; Balastegui, M.I.C.; Sanitá, P.V.; Pavarina, A.C.; Barbugli, P.A.; Mima, E.G.O. Encapsulation of curcumin in polymeric nanoparticles for antimicrobial Photodynamic Therapy. PLoS One. 2017 Nov 6;12(11):e0187418. [CrossRef] [PubMed] [PubMed Central]
- Santezi, C.; Reina, B.D.; de Annunzio, S.R.; Calixto, G.; Chorilli, M.; Dovigo, L.N. Photodynamic potential of curcumin in bioadhesive formulations: Optical characteristics and antimicrobial effect against biofilms. Photodiagnosis Photodyn Ther. 2021 Sep;35:102416. Epub 2021 Jun 29. [CrossRef] [PubMed]
- Marques Meccatti, V.; de Souza Moura, L.; Guerra Pinto, J.; Ferreira-Strixino, J.; Abu Hasna, A.; Alves Figueiredo-Godoi, L.M.; Campos Junqueira, J.; Marcucci, M.C.; de Paula Ramos, L.; Carvalho, C.A.T.; Pucci, C.R.; de Oliveira, L.D. Curcuma longa L. Extract and Photodynamic Therapy are Effective against Candida spp. and Do Not Show Toxicity In Vivo. Int J Dent. 2022 Jul 1;2022:5837864. [CrossRef] [PubMed] [PubMed Central]
- Al-Ghamdi, A.R.S.; Khanam, H.K.; Qamar, Z.; Abdul, N.S.; Reddy, N.; Vempalli, S.; Noushad, M.; Alqahtani, W.M.S. Therapeutic efficacy of adjunctive photodynamic therapy in the treatment of denture stomatitis. Photodiagnosis Photodyn Ther. 2023 Jun;42:103326. Epub 2023 Feb 10. [CrossRef] [PubMed]
- Dovigo, L.N.; Pavarina, A.C.; Ribeiro, A.P.; Brunetti, I.L.; Costa, C.A.; Jacomassi, D.P.; Bagnato, V.S.; Kurachi, C. Investigation of the photodynamic effects of curcumin against Candida albicans. Photochem Photobiol. 2011 Jul-Aug;87(4):895-903. Epub 2011 Jun 13. [CrossRef] [PubMed]
- Dos Santos, D.D.L.; Besegato, J.F.; de Melo, P.B.G.; Junior, J.A.O.; Chorilli, M.; Deng, D.; Bagnato, V.S.; de Souza Rastelli, A.N. Effect of curcumin-encapsulated Pluronic® F-127 over duo-species biofilm of Streptococcus mutans and Candida albicans. Lasers Med Sci. 2022 Apr;37(3):1775-1786. Epub 2021 Oct 19. [CrossRef] [PubMed]
- Dovigo, L.N.; Pavarina, A.C.; Carmello, J.C.; Machado, A.L.; Brunetti, I.L.; Bagnato, V.S. Susceptibility of clinical isolates of Candida to photodynamic effects of curcumin. Lasers Surg Med. 2011 Nov;43(9):927-34. [CrossRef] [PubMed]
- Dias, L.M.; Klein, M.I.; Ferrisse, T.M.; Medeiros, K.S.; Jordão, C.C.; Bellini, A.; Pavarina, A.C. The Effect of Sub-Lethal Successive Applications of Photodynamic Therapy on Candida albicans Biofilm Depends on the Photosensitizer. J Fungi (Basel). 2023 Jan 13;9(1):111. [CrossRef] [PubMed] [PubMed Central]
- Trigo-Gutierrez, J.K.; Calori, I.R.; de Oliveira Bárbara, G.; Pavarina, A.C.; Gonçalves, R.S.; Caetano, W.; Tedesco, A.C.; Mima, E.G.O. Photo-responsive polymeric micelles for the light-triggered release of curcumin targeting antimicrobial activity. Front Microbiol. 2023 Apr 20;14:1132781. [CrossRef] [PubMed] [PubMed Central]
- Quishida, C.C.; De Oliveira Mima, E.G.; Jorge, J.H.; Vergani, C.E.; Bagnato, V.S.; Pavarina, A.C. Photodynamic inactivation of a multispecies biofilm using curcumin and LED light. Lasers Med Sci. 2016 Jul;31(5):997-1009. Epub 2016 Apr 28. [CrossRef] [PubMed]
- Damrongrungruang, T.; Panutyothin, N.; Kongjun, S.; Thanabat, K.; Ratha, J. Combined bisdemethoxycurcumin and potassium iodide-mediated antimicrobial photodynamic therapy. Heliyon. 2023 Jun 27;9(7):e17490. [CrossRef] [PubMed] [PubMed Central]
- Al-Asmari, F.; Mereddy, R.; Sultanbawa, Y. A novel photosensitization treatment for the inactivation of fungal spores and cells mediated by curcumin. J Photochem Photobiol B. 2017 Aug;173:301-306. Epub 2017 Jun 8. [CrossRef] [PubMed]
- Hsieh, Y.H.; Zhang, J.H.; Chuang, W.C.; Yu, K.H.; Huang, X.B.; Lee, Y.C.; Lee, C.I. An in Vitro Study on the Effect of Combined Treatment with Photodynamic and Chemical Therapies on Candida albicans. Int J Mol Sci. 2018 Jan 24;19(2):337. [CrossRef] [PubMed] [PubMed Central]
- Merigo, E.; Conti, S.; Ciociola, T.; Fornaini, C.; Polonelli, L.; Lagori, G.; Manfredi, M.; Vescovi, P. Effect of different wavelengths and dyes on Candida albicans: In vivo study using Galleria mellonella as an experimental model. Photodiagnosis Photodyn Ther. 2017 Jun;18:34-38. Epub 2017 Jan 24. [CrossRef] [PubMed]
- Casu, C.; Orrù, G.; Scano, A. Curcumin/H2O2 photodynamically activated: an antimicrobial time-response assessment against an MDR strain of Candida albicans. Eur Rev Med Pharmacol Sci. 2022 Dec;26(23):8841-8851. [CrossRef] [PubMed]
- Leferman, C.E.; Stoica, L.; Tiglis, M.; Stoica, B.A.; Hancianu, M.; Ciubotaru, A.D.; Salaru, D.L.; Badescu, A.C.; Bogdanici, C.M.; Ciureanu, I.A.; Ghiciuc, C.M. Overcoming Drug Resistance in a Clinical C. albicans Strain Using Photoactivated Curcumin as an Adjuvant. Antibiotics (Basel). 2023 Jul 25;12(8):1230. [CrossRef] [PubMed] [PubMed Central]
- Tsutsumi-Arai, C.; Arai, Y.; Terada-Ito, C.; Imamura, T.; Tatehara, S.; Ide, S.; Shirakawa, J.; Wakabayashi, N.; Satomura, K. Inhibitory effect of 405-nm blue LED light on the growth of Candida albicans and Streptococcus mutans dual-species biofilms on denture base resin. Lasers Med Sci. 2022 Jun;37(4):2311-2319. Epub 2022 Jan 16. [CrossRef] [PubMed]
- Zhang, Y.; Zhu, Y.; Chen, J.; Wang, Y.; Sherwood, M.E.; Murray, C.K.; Vrahas, M.S.; Hooper, D.C.; Hamblin, M.R.; Dai, T. Antimicrobial blue light inactivation of Candida albicans: In vitro and in vivo studies. Virulence. 2016 Jul 3;7(5):536-45. Epub 2016 Feb 24. [CrossRef] [PubMed] [PubMed Central]
- Lin, C.H.; Chien, H.F.; Lin, M.H.; Chen, C.P.; Shen, M.; Chen, C.T. Chitosan Inhibits the Rehabilitation of Damaged Microbes Induced by Photodynamic Inactivation. Int J Mol Sci. 2018 Sep 1;19(9):2598. [CrossRef] [PubMed] [PubMed Central]
- Pinto, A.P.; Rosseti, I.B.; Carvalho, M.L.; da Silva, B.G.M.; Alberto-Silva, C.; Costa, M.S. Photodynamic Antimicrobial Chemotherapy (PACT), using Toluidine blue O inhibits the viability of biofilm produced by Candida albicans at different stages of development. Photodiagnosis Photodyn Ther. 2018 Mar;21:182-189. Epub 2017 Dec 6. [CrossRef] [PubMed]
- Idrees, M.; Kujan, O. Curcumin is effective in managing oral inflammation: An in vitro study. J Oral Pathol Med. 2024 May 21. Epub ahead of print. [CrossRef] [PubMed]
- Lee, Y.S.; Chen, X.; Widiyanto, T.W.; Orihara, K.; Shibata, H.; Kajiwara, S. Curcumin affects function of Hsp90 and drug efflux pump of Candida albicans. Front Cell Infect Microbiol. 2022 Sep 27;12:944611. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
PRISMA 2020 flowchart of selected criteria for the included article reports.
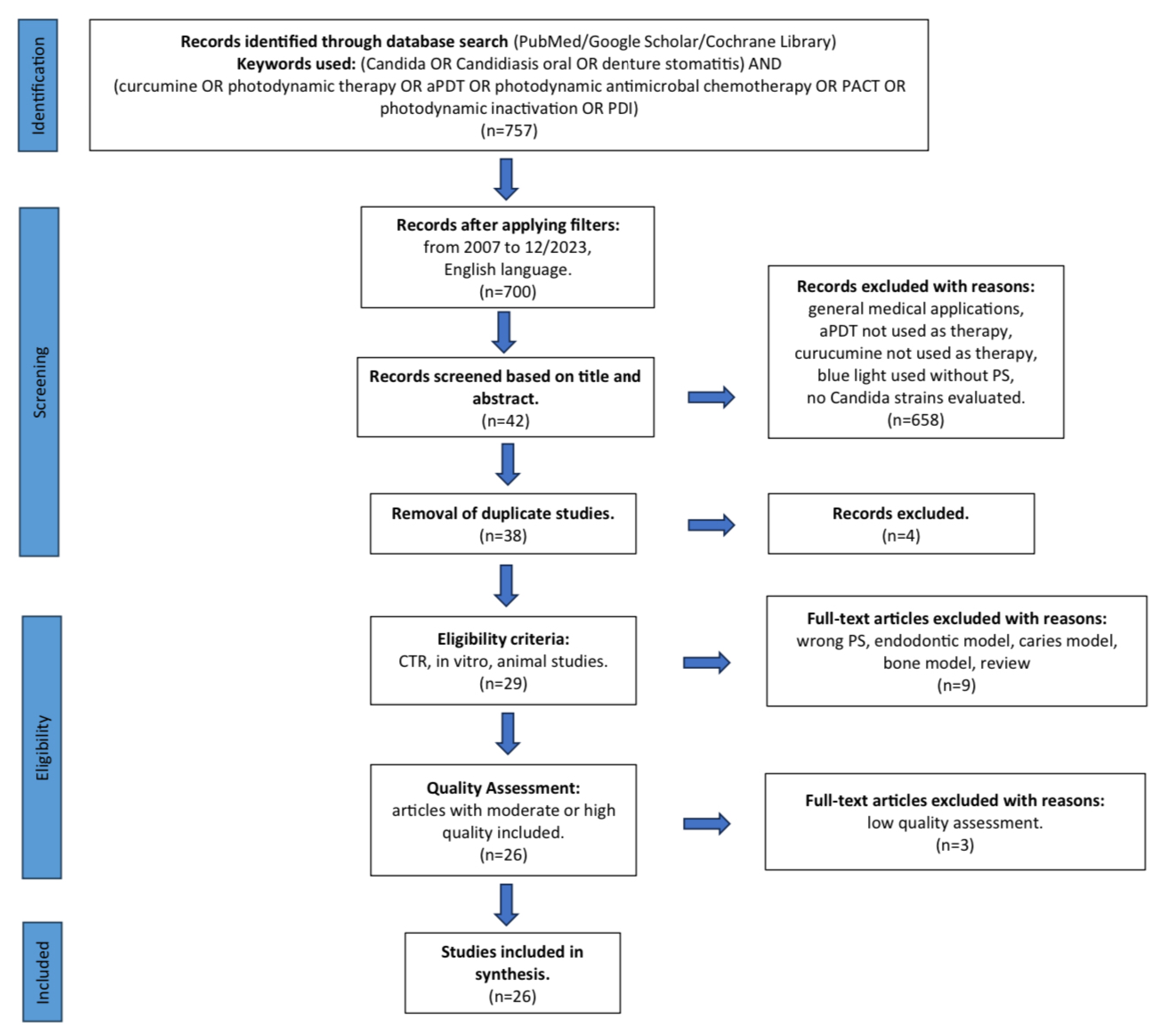

Table 1.
presents a list of excluded studies and the rationale for their exclusion.
| Ordinal Number | Reason for Exclusion | Reference Number |
|---|---|---|
| 1 | Review | [27] |
| 2 | Endodontic model | [28] |
| 3 | Cytotoxicity testing PDT | [29] |
| 4 | Endodontic model | [30] |
| 5 | Caries model | [31] |
| 6 | Bone defect model | [32] |
| 7 | Caries model | [33] |
| 8 | Caries model | [34] |
| 9 | Caries model | [35] |
Table 2.
Risk of bias of 29 studies included for full-text analysis.
| Reference number | PS concentration | Origin of PS | Incubation time | Light source parameters | Clinical strains of Candida spp. | Negative control group | Numerical results available (statistics) | No missing outcome data | 10 patients per group | 6-month follow-up period | Total score 8/2 (RCT) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [5] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [6] | yes | yes | no | yes | no | yes | yes | no | - | - | 5/- |
| [7] | yes | no | yes | yes | no | yes | yes | yes | - | - | 6/- |
| [11] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [13] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [14] | yes | yes | yes | yes | yes | yes | yes | yes | yes | no | 8/1 |
| [15] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [23] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [36] | yes | yes | yes | yes | yes | yes | yes | yes | - | - | 8/- |
| [37] | yes | yes | yes | yes | yes | no | yes | yes | yes | no | 7/1 |
| [38] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [39] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [40] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [41] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [42] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [43] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [44] | yes | no | yes | yes | yes | yes | yes | yes | yes | no | 7/1 |
| [45] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [46] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [47] | yes | yes | yes | yes | yes | yes | yes | no | - | - | 7/- |
| [48] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [49] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [50] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [51] | yes | yes | yes | yes | no | yes | yes | yes | - | - | 7/- |
| [52] | yes | yes | yes | yes | no | no | yes | yes | - | - | 6/- |
| [53] | yes | no | yes | yes | no | yes | yes | yes | - | - | 6/- |
| [54] | yes | yes | no | yes | no | yes | yes | yes | - | - | 6/- |
| [55] | no | yes | no | yes | yes | yes | yes | no | - | - | 5/- |
| [56] | yes | yes | no | yes | yes | yes | yes | no | - | - | 5/- |
Abbreviations: PS – photosensitizer, RCT - Randomized Controlled Trial .
Table 3.
General characteristics of studies that fulfilled the eligibility criteria.
| Reference number | Study design | Candida species | Study group | Outcomes |
|---|---|---|---|---|
| [5] | In vitro study on a 96-well plate | Reference strain C. albicans ATCC 90028 Biofilm |
PS-L-, PS-L+37.5 J, PS-L+50 J, PS+L-40J, PS+L-80 J, PS+L+40/37.5 J, PS+L+40/50 J, PS+L+80/37.5 J, PS+L+80/50 J | aPDT 80/50 J promotes a greater reduction in the expression of C. albicans genes are associated with adhesion and biofilm formation and genes responsible for oxidative stress. |
| [7] | In vivo animal study, the tongues of mice infected with C. albicans | Reference strain C. albicans ATCC 90028 |
CUR+L+, CUR-L-, CUR+L-, AC+L-, AC+L+, CC+L-, CC+L-, NYS1, NYS4; C free CUR, AC anionic CUR, CC cationic CUR, NYS 100 000 IU 1 and 4 x daily | Free CUR shows a better photodynamic effect than NP-CUR in nanocarriers. APDT with free CUR results in tongue epithelial CK13 and CK14 expression like that observed in healthy mice, which was not observed with NYS. |
| [11] | In vitro study on a 96-well plate | Reference strain C. albicans ATCC 18804 Planktonic cultures |
PS+L+, PS+L-, PS-L+, PS-L-, H2O2 10 mM | aPDT caused extensive DNA damage to C. albicans, which was not effectively repaired due to the inhibition caused by CUR. |
| [13] | In vitro study on a 6-well plate | Reference strain C. albicans ATCC 10231 Biofilm |
CUR+L+ (D10, D20, B10, B20, E110, E220, D10+E110, D10+E220, D10+Ti, D20+E110, D20+E220, D20+Ti, B10+E110, B10+E22, B10+Ti, B20+E110, B20+E220, B20+Ti, E110+Ti, E220+Ti, D10+E110+Ti, D10+E220+Ti, D20+E110+Ti, D20+E220+Ti, B10+E110+Ti, B10+E220+Ti, B20+E110+TI, B20+E220+Ti), NYS CUR-L- |
20 µM bisdemethoxycurcumin + erythrosine 110-220 µM + 10% titanium nanoxide tends to generate relatively large amounts of ROS and effectively inhibits Candida albicans without inducing cytotoxicity against normal human gingival fibroblasts. |
| [14] | A randomized controlled clinical trial with a 12-week follow-up | Oral candidiasis, prosthetic stomatitis; C. albicans, C. tropicalis, C. glabrata |
CUR+L+, NYS | CUR-mediated aPDT is as effective as topical NYS therapy in treating denture-induced stomatitis in cigarette smokers. |
| [15] | In vitro study on a 96-well plate | Reference strain C. albicans ATCC 90028, C. glabrata ATCC 2001, C. dubliniensis CBS 7987 Planktonic cell solutions and biofilms |
PS+L+, PS-L+, PS+L-, PS-L- |
C. albicans - cell viability decreases proportionally regardless of concentration, best effect 20 min PIT and 40 µM CUR. C. glabrata - best effect 40 µM CUR, dependence on PIT unclear. C. dubliniensis - Groups irradiated for 4 min were concentration-dependent for extreme values (40 and 20 µM). In contrast, groups irradiated for 8 minutes were concentration and incubation time dependent. |
| [23] | In vitro study in Eppendorf tubes | Reference strain of C. albicans ATCC Mya 273 Planktonic form | CUR-L-, CUR-L+, CUR+L-, CUR+L+; 5µM 0/5/25min, 10µM 0/5/25µM, 20µM 0/5/25min, 50µM 0/5/25min (DMSO 5/10%) | CUR shows the best antimicrobial activity at a concentration of 50 µM without an incubation period regardless of the DMSO concentration. |
| [36] | In vitro study on a 96-well plate | Clinical strain C. dubliniensis CD6, CD7, CD8, reference strain CBS 7987 (control) Plankton cultures and biofilms | PS-L+, PS+L-5, PS+L-10, PS+L-20, PS-L-, PS+L+5, PS+L+10, PS+L+20 (for planctonic forms); PS-L+, PS+L-20, PS+L-30, PS+L-40, PS-L-, PS+L+20, PS+L+30, PS+L+40 (for biofilms) | The best therapeutic effect against plankton forms CUR 20 µM, and against biofilms CUR 40 µM. |
| [37] | Controlled, two-arm, parallel-group, single-blind clinical trial | Clinical strain, oral candidiasis, C. tropicalis, C. parapsilosis, C. krusei, C. glabrata |
MB, CUR | Curcumin at 80 µmol/L irradiated with an energy of 200 J/cm2 is associated with increased free radical generation. CUR was less effective than TBO. |
| [38] | In vivo study in a mice model of oral candidiasis | Reference strain C. albicans ATCC 90028 | CUR+L+20, CUR+L+40, CUR+L+80, CUR+L-20, CUR+L-40, CUR+L-80, CUR-L+, CUR-L- | Histological analysis of the tongues of mice treated with aPDT 80 µM CUR showed a reduced number of Candida cells that were confined to the stratum corneum and low inflammatory response. |
| [39] | In vitro test on silicone samples in a 24-well plates | Reference strain C. albicans ATCC 90028 Biofilm |
L-CUR-, L-CUR+, L+CUR-, L+CUR+ | The antimicrobial effect on C. albicans depends on the concentration of curcumin and the exposure time. The best results are obtained with 60 µg/mL curcumin and 30 min of irradiation. |
| [40] | In vivo study in a mice model of oral candidiasis | Reference strain C. albicans ATCC 90028 |
PS+L+20µM, PS+L+40µM, PS+L+80µM PS+L-20µM, PS+L-40µM, PS+L-80µM, PS-L+, PS-L- |
A curcumin concentration of 80 uM combined with LED light causes the greatest change in the number of C. albicans colonies. |
| [41] | In vitro study on a 96-well plate | Reference strain C. albicans ATCC 90028 Biofilm, planktonic cultures |
CUR+L+ (free CUR, anionic CUR, cationic CUR), CUR+L-, CUR-L+, CUR-L- NL- (anionic and cationic nanoparticles without CUR) | Anionic CUR shows the lowest antibacterial photodynamic effect, cationic CUR was cytotoxic. |
| [42] | In vitro study on a 96-well plate. In situ biofilm study in the oral cavity (volunteers wore palatal appliances containing enamel samples to establish dental biofilms in situ; study on a 24-well plate) | Reference strain C. albicans ATCC 90028 Biofilm |
CUR+L+ (CUR-LCP, CUR-CHIH, CUR-ME, CUR-S), CUR+L-, CUR-L+, CUR-L- | CUR-S is the only formulation that can significantly reduce the viability of the biofilm after photodynamic treatment. |
| [43] | In vitro study on a 24-well plate | Reference strain C. albicans ATCC 18804, C. tropicalis ATCC 13803 Planktonic cultures |
CUR-L- (saline), N (nystatin), C. longa+L-, CUR+L-, CUR-L+, CUR+L+ |
The isolated curcumin longa extract and photodynamic therapy with CUR have antifungal activity against C. albicans and C. tropicalis and no toxicity to the invertebrate model G. mellonella. |
| [44] | Randomized controlled clinical trial with 2-month follow-up | Prosthetic stomatitis; C. albicans, C. krusei |
Group I (antifungal gel therapy), Group II (aPDT CUR + antifungal gel) | CUR-mediated aPDT is an effective treatment method for reducing the mycological burden on the palate mucosa and denture surfaces, as well as improving salivary pro-inflammatory cytokine levels in patients with denture-related stomatitis. |
| [45] | In vitro study on a 96-well plate | Reference strain C. albicans ATCC 90028 Planktonic cultures, biofilm |
PS+L+, PS+L-, PS-L-, PS-L+ | Highest therapeutic efficacy 20 µM CUR, 5.28 J/cm2, 20 min incubated time. |
| [46] | In vitro study on a 96-well plate | Reference strain of C. albicans ATCC 18804 Planktonic forms and biofilm |
PS-L-, PS-L+, CHX, NYS, PS-D+L-, PS-D+L+, PS+D+L-, PS+D+L+, PS-M+L-, PS-M+L+, PS+M+L-, PS+M+L+ | CUR-Plu shows a lower reduction than CUR-DMSO. Multispecies biofilm shows greater resistance than monospecies. CUR-Plu can be considered a stable and effective method for controlling biofilm within a short time after synthesis. |
| [47] | In vitro study on a 96-well plate | Clinical isolates C. albicans Ca1, Ca2, Ca3, Ca4, Ca5; C. glabrata Cg1, Cg2, Cg3, Cg4, Cg5; C. tropicails Ct1, Ct2, Ct3, Ct4, Ct5 Planktonic cell solution and biofilm |
PS+L+, PS+L-, PS-L+, PS-L- | The greatest reduction in the activity of C. albicans, C. tropicalis, and C. glabrata using 40 µM CUR and 18 J/cm2. |
| [48] | In vitro study on a 96-well plate | Reference strain C. albicans ATCC 90028 Planktonic cultures and biofilms |
CUR+L+, CUR+L-, CUR-L+, CUR-L- | C. albicans planktonic cultures are susceptible to subsequent applications of sublethal aPDT doses via CUR. Sublethal aPDT CUR may have made C. albicans cells more resistant to therapy. |
| [49] | In vitro study on a 96-well plate | Reference strain C. albicans SC 5314 Planktonic cultures and biofilms |
CUR-L-, F+CUR-L-, P+CUR-L-, M+CUR-L-, F+CUR+L-, P+CUR+L-, M+CUR+L-, CUR+L-, CUR-UL+, CUR-BL+, M+CUR-UL+, M+CUR+UL+, M+CUR+BL+, F+CUR+BL+, P+CUR+BL+, CUR+BL+, M+CUR+UL+BL+ | CUR-loaded F127 micelles bound to blue light caused biofilm photoinactivation. |
| [50] | In vitro test on acrylic samples in a 24-well plate | Reference strain C. albicans ATCC 90028, C. glabrata ATCC 2001 Biofilm |
PS+L+(24h), PS+L-(24h), PS+L+(48h), PS+L-(48h), PS-L+(24h), PS-L+(48h), PS-L-(24h), PS-L-(48h) | 24- and 48-hour biofilms are susceptible to CUR-mediated aPDT at concentrations assessed at 37.5 J/cm2. |
| [51] | In vitro study on a 6-well plate | Reference strain C. albicans ATCC 10231 Biofilm |
CUR20+L+, CUR40+L+, CUR80+L+, KI+L+, CUR20+KI+L+, CUR40+KI+L+, CUR80+KI+L+, Nystatin, Phosphate-buffered saline | 40 uM bisdemethoxycurcumin + 100 mM KI combined with blue light can effectively reduce C. albicans biofilm after 6 hours with efficacy comparable to NYS. |
| [52] | In vitro test on Petri dishes | Reference strain C. albicans ATCC 10231 Cells in water mixture, cells on agar surface |
PS+L+, PS+L- | C. albicans in an aqueous mixture are inhibited at any light dose, on the agar surface at 96 J/cm2, spore soaking had no significant effect on cell number reduction. |
| [53] | In vitro study on a 96-well plate | Reference strain C. albicans ATCC 90029 Planktonic cell solutions, adherent cultures |
PS+L+, PS+L+ 208 µM fluconazole |
Fluconazole eliminates the yeast form, CUR-aPDT the biofilm. Fluconazole + CUR-aPDT eliminates the growth and virulence of C. albicans. |
| [54] | In vitro test on solid medium plates and in Eppendorf tubes | Reference strain C. albicans SC 5314 Planktonic cell solution, adherent cultures |
PS+L+, PS+L-, PS-L+, PS-L- | 100% inhibition of C. albicans growth at any fluence. |
Abbreviations: L – light, PS – photosensitizer, CUR – curcumin, C. – Candida, ACTT- American Type Culture Collection, h – hours, AC – anionic curcumin, CC – cationic curcumin, NYS – nystatin, MB – methylene blue, CUR – curcumin, N – anionic and cationic nanoparticles without curcumin, DMSO – dimethylsulfoxide, CUR-LCP - liquid crystalline precursor system with curcumin, CUR-CHIH - chitosan hydrogel with curcumin, CUR-ME - microemulsion with curcumin, CUR-S - free curcumin dissolved in 10% DMSO, D – demetoxycurcumin, B – bisdemetoxycurcumin, E – erythrosine, Ti – titanium nanoxide, CHX – chlorhexidine, M – micelles, F – F127, P – P123, UL – ultraviolet, BL – blue light, KI - potassium iodide.
Table 4.
presents the physical parameters of light sources from studies that met the eligibility criteria.
Table 4.
presents the physical parameters of light sources from studies that met the eligibility criteria.
| Reference number | Light source | Wavelength (nm) | Energy density (Fluence) (J/cm2) | Power output (mW) | Irradiation Time | Spot size / Fiber surface area (cm2) |
|---|---|---|---|---|---|---|
| [5] | LED | 450 | 37.5, 50 | 30 | 21, 27 min | - |
| [7] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 37.5 | 75 | 7 min | 0,196 |
| [11] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 37.5 | 89.2 | 7 min | 0.196 |
| [13] | Dental lamp (VALO Ortho Cordless, South Jordan, UT, USA) | 395-480 | 72 | 3200 | 27 sek | 0.747 |
| [14] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 37.5 (denture) 122 (palate) | 260 | 26 min (denture), 20 min (palate) | 0.196 |
| [15] | LED (Institute of Physics Sao Carlos, São Paulo, Brasil) | 455 | 5.28 | 22 | 4 min | - |
| [23] | LED self-made | 435 | 15.8 | - | 60 min | - |
| [36] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 5.28 | 22 | 4 min | 0.196 |
| [37] | Blue LED (New Dent s/n) | 480 | 200 | 480 | 90 sek | 0.216 |
| [38] | LED (University Sao Paulo, Sao Carlos, SP, Brasil) | 455 | 37.5 | 89,2 | 7 min | - |
| [39] | LED (Biotable RGB, MMOptics, Sao Carlos, SP, Brasil) | 430 | 10.8, 32.4 | 18 | 10, 30 min | - |
| [40] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 37.5 | 89.2 | 7 min | 0.196 |
| [41] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 43.2 | 33.58 | 20 min | 0.196 |
| [42] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 450 (440-460) | 18 | 22 | 14 min | 0.196 |
| [43] | Prototype device based on LEDs (Biotable Irrad/LED) | 450 ± 5 | 10, 25 | 110 | 91, 228 sek | - |
| [44] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 37,5 (denture) 122 (palate) | 260 | 26 min (denture), 20 min (palate) | 0.196 |
| [45] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 37.5, 1.32, 2.64, 3.96, 5.28, 6.60, 13.20, 26.40 | 22 | 29 min, 1, 2, 3, 4, 5, 10, 20 min | 0.196 |
| [46] | LED (Biotable RGB, MMOptics, Sao Carlos, SP, Brasil) | 460 | 15 | - | 11 min 36 sek | - |
| [47] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 5.28, 18, 25.5, 37.5 | 22 | n.a | 0.196 |
| [48] | LED (Biotable 3.4, Sao Carlos, Brasil) | 450 | 18 | 47 | 6.38 min | - |
| [49] | LED (Biotable RGB, MMOptics, Sao Carlos, SP, Brasil) | 455 | 33.84 | 47 | 12 min | - |
| [50] | LED (LXHL-PR09, Luxeon III Emitter, Lumileds Lighting, San Jose, California, USA) | 455 (440-460) | 37.5 | 22 | 29 min | 0.196 |
| [51] | Dental lamp (Elipar DeepCure-L Curing Light, 3M, Singapore) | 450 ± 30 | 90 | 950 | 95 sek | 0.785 |
| [52] | Xenon arc lamp (Polilight, PL 500, Rofin Australia Pty Ltd., Victoria, Australia) | 370-680; 420 | 24, 48, 72, 96, 240, 360 | 500 000 | 2, 4, 6, 8, 20, 30 min | - |
| [53] | LED self-made | 430 | 9 | - | 30 min | - |
| [54] | Diode laser blue-violet | 405 | 10, 20, 30 | - | 50, 100, 150 sek | 0.2 |
Abbreviations: LED – light-emitting diode.
Table 5.
Characteristics of curcumin used as a PS in studies meeting eligibility criteria.
| Reference number | Incubation time (in minutes) | Concentration/s of PS used |
|---|---|---|
| [5] | 20 | 40, 80 µM |
| [7] | 20 | 260 µM |
| [11] | 20 | 2,5 µM |
| [13] | 15 | 10, 20 µM |
| [14] | 30 | 5 µg/mL |
| [15] | 1, 5, 10, 20 | 5, 10, 20, 30, 40 µM |
| [23] | 0, 5, 25 | 5, 10, 20, 50 µM CUR + 5% DMSO / 10% DMSO; 10, 50, 100 µM SA-CUR12a |
| [36] | 20 | 5, 10, 20 µM (for planktonic form), 20, 30, 40 µM (for biofilms) |
| [37] | 1 | 80 µM |
| [38] | 20 | 20, 40, 80 µM |
| [39] | 5 | 30, 60 µg/mL |
| [40] | 20 | 20, 40, 80 µM |
| [41] | 40 | 130 µM |
| [42] | 5 | 20, 40, 60, 80 µM |
| [43] | 20 | 100 mg/mL CUR longa / 200 µg/mL CUR |
| [44] | 30 | 5 µg |
| [45] | 5, 20 | 0.005; 0.01; 0.05; 0.1; 0.5; 1; 5; 10; 20 µM |
| [46] | 5 | 270 µM |
| [47] | 20 | 5, 10, 20 µM |
| [48] | 20 | 40 µM |
| [49] | 20 | 63 µM |
| [50] | 20 | 80, 100, 120 µM |
| [51] | 20 | 20, 40, 80 µM bisdemethoxycurcumin + 100 µM KI |
| [52] | 10, 20, 30 | 100-1000 µM, 800 µM |
| [53] | 20 | 1, 5, 10, 20, 40, 80 µM |
| [54] | n.a. | 100 µM |
Abbreviations: CUR – curcumin, DMSO – dimethyl sulfoxide, KI – potassium iodide.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



