
Submitted:
06 July 2024
Posted:
08 July 2024
You are already at the latest version
Abstract
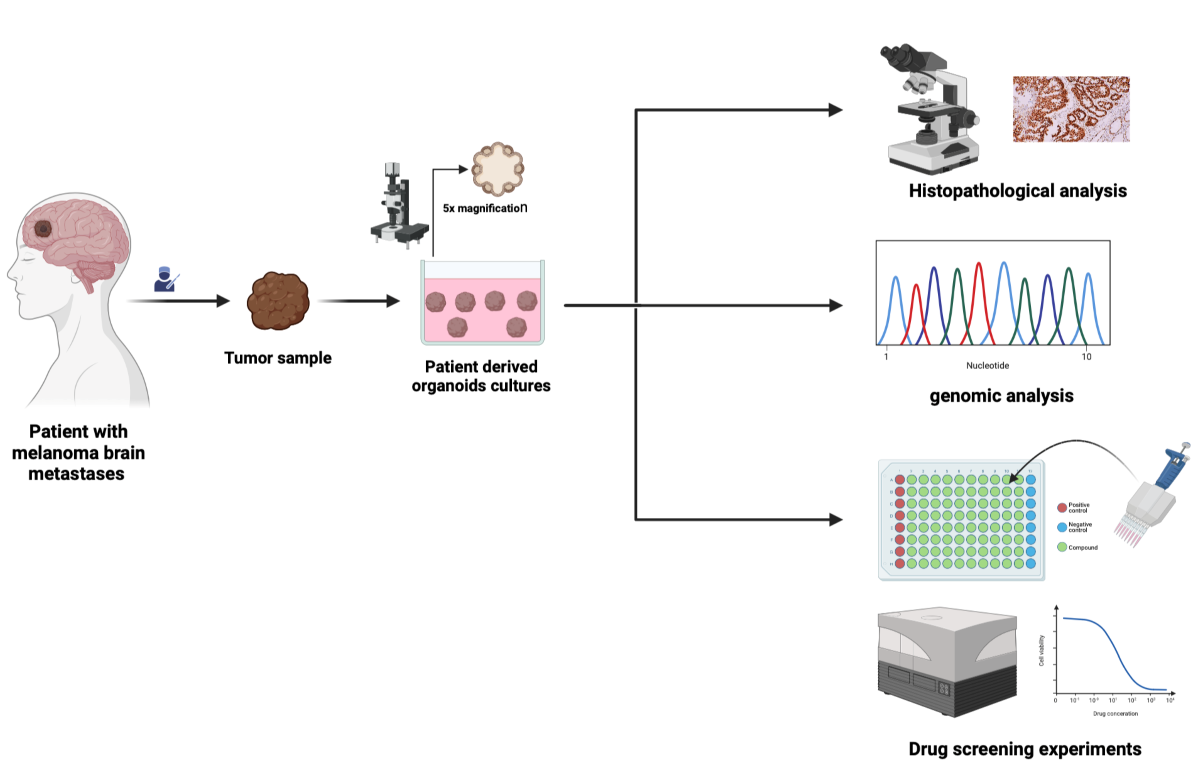
Background and aims: Brain metastases are prevalent in the late stages of malignant melanoma. Multimodal therapy remains challenging. Patient-derived organoids (PDOs) represent a valuable pre-clinical model, faithfully recapitulating key aspects of the original tumor, including the heterogeneity and the mutational status. This study aimed to establish PDOs from melanoma brain metastases (MBM-PDOs) and to test the feasibility of using them as a model for in vitro targeted-therapy drug testing.Methods: Surgical resection samples from eight patients with melanoma brain metastases were used to establish MBM-PDOs. Samples were enzymatically dissociated followed by seeding into low-attachment plates to generate floating organoids. The MBM-PDOs were characterized genetically, histologically, immunohistologically and compared with the parental tissue. The MBM-PDO cultures were exposed to dabrafenib (BRAF inhibitor) and trametinib (MEK inhibitor) followed by cell viability assessment.Results: Seven out of eight cases were successfully cultivated, maintaining the histological, immunhistological phenotype, and the mutational status of the parental tumors. Five out of seven cases harbored BRAF V600E mutations and were responsive to BRAF and MEK inhibitors in vitro. Two out of seven cases were BRAF wild type, one case harboring an NRAS mutation and the other harboring a KIT mutation, and both were resistant to BRAF and MEK inhibitor therapy. Conclusion:We successfully established PDOs from melanoma brain metastases surgical specimens, which exhibited a consistent histological and mutational profile with the parental tissue. Using FDA-approved BRAF and MEK inhibitors, our data demonstrates the feasibility of employing MBM-PDOs for targeted-therapy in vitro testing.
Keywords:
Melanoma
; brain metastases
; BRAF
; Organoids
Importance of the Study
The incidence of malignant melanoma is rising worldwide. Although the five-year survival rate for early-stage melanoma is over 90%, in advanced metastatic stages decreases to 10%. About 60% of melanoma patients develop brain metastases; however, those patients are excluded from clinical trials which hinders the development of new therapeutic approaches for this group of patients. Additionally, the biology of melanoma brain metastases is poorly understood due to the lack of representative research models; hence, there is a critical need to develop novel faithful models. In this study, melanoma brain metastases’ patient-derived organoid culture lines were established from surgical specimens. The organoid cultures faithfully recapitulated the histological and mutational profile of the parental tissue. Drug-sensitivity experiments using the FDA-approved BRAF and MEK inhibitors, dabrafenib and trametinib, demonstrated the feasibility of employing melanoma brain metastases patient-derived organoids as models for targeted-therapy in vitro testing and for the discovery of novel therapeutic targets.
Introduction
Brain metastases are one of the most common and challenging neurologic complications of cancer. It is estimated that approximately 20% of individuals diagnosed with cancer will develop brain metastases [1]. Among these metastatic brain lesions, melanoma stands as the third most frequent cause, accounting for 6%–11% of all cases after lung cancer (41%) and breast cancer (19%) [2,3]. Up to 60% of melanoma patients will develop brain metastasis during disease progression. The management of advanced-stage cancer, especially after the development of brain metastases, necessitates a comprehensive and multimodal treatment approach, including surgery, radiotherapy, chemotherapy, immunotherapy, and targeted therapy; based on the mutational status [1]. BRAF is the gene most commonly affected by point mutations in cutaneous melanoma, which in turn leads to constitutive activation of the MAPK pathway [4]. This promotes tumor progression, but on the other hand represents a molecular target for therapy using MAPK inhibitors, such as BRAF and MEK inhibitors, which have shown response rates of up to 76% in patients with melanomas harboring BRAF mutations [5,6]. The development and the integration of immune checkpoint inhibitors, specifically PD-1 inhibitors (nivolumab and pembrolizumab) and the CTLA-4 blocking antibody (ipilimumab) as combination therapy have significantly improved clinical outcomes for advanced and metastatic melanoma [7,8].
Although checkpoint inhibitors result in long time survival in some patients with metastatic malignant melanoma, regardless of the BRAF mutational status [9], only a group of patients show this favorable response to therapy and these cannot be identified beforehand so far. To understand and decipher the complex nature of melanoma-derived brain metastases, it is essential to establish robust and representative models of melanoma brain metastases, that can be generated efficiently. Patient-derived organoid (PDO) models recapitulate the original tumor in terms of tissue architecture, and maintain the genetic and histological characteristics of the primary tumor and the intratumoral heterogeneity [10,11]. Therefore, PDO models have emerged as a promising in vitro platform serving diverse research purposes, such as biomarker discovery, personalized medicine, and drug screening, providing enhanced insights into tumor biology and the evaluation of responses to novel therapeutic agents [12].In this study, we have successfully established PDO cultures derived from seven surgical samples of melanoma brain metastases (MBM), which faithfully retained the genetic and histological characteristics of the primary tumor. Furthermore, the established MBM-PDO cultures were treated in vitro with targeted therapies, BRAF and MEK inhibitors, to ascertain whether they can accurately predict targeted therapy responses based on their mutational profile. .
Material and Methods
Human Specimens
Informed consent was obtained from patients undergoing craniotomies for brain metastases between 2022 and 2023 in the Department of Neurosurgery, University Hospital Bonn. The experiments were approved by the Ethics Committee of the Medical Faculty, University Bonn (#417/17 with amendment from 2020; #169/23). The clinical-pathological characteristics are given in Table 1. The primary diagnostic was conducted at the Institute for Neuropathology, University Hospital Bonn. Two patients had brain metastases as the first tumor manifestation, while the other six patients experienced brain metastases at an advanced stage (Table 1).
Human Tumor Collection
Tumor tissues were collected in basis medium (Advanced DMEM/F12 supplemented with 1x GlutaMax, 10mM HEPES solution (Carl Roth, Karlsruhe, Germany), 100 μg/mL Normocin (InvivoGen, San Diego CA, USA), and 2.5 µg/mL Amphotericin B (Biowest, Nuaillé, France). The tumor samples were manually cut with scissors followed by further mechanical dissociation using gentleMACS™ C Tubes and the gentleMACS™ Octo Dissociator (Miltenyi Biotec, Bergisch Gladbach, Germany). After filtering the tumor samples using a 1000 µm filter, red blood cell lysis was performed using RBC Lysing Buffer Hybri-Max (Sigma-Aldrich, St. Louis MI, USA). The resultant cell suspensions were then cryopreserved at -80°C using CryoStor CS10 media (Stemcell Technologies, Vancouver, Canada) until the completion of pathological evaluation and tumor mutational analysis of the primary brain metastasis at the Institute for Neuropathology, University Hospital Bonn.
MBM-PDOs Floating Culture
Cryopreserved dissociated tumor samples were thawed and digested in an enzyme mix (1 mg/mL collagenase IV (Rockland Immunochemicals, Limerick, PA, USA), 15 µg/mL DNase (ThermoFisherScientific, Waltham MA, USA), and 10 µM Y-27632-HCL Rock inhibitor (Biogems, Westlake Village, CA, USA) in basis medium, at 37°C for 1 hour followed by incubation with 3-5 ml TrypLE Express (Gibco, ThermoFisherScientific, Waltham MA, USA), and filtered through a 70 µm cell strainer (Avantor, Pennsylvania, USA). Cells were seeded in ultra-low attachment (ULA) plates (Stemcell Technologies, Vancouver, Canada) in melanoma brain metastases patient-derived organoids (MBM-PDO) culture media (Suppl. Table 1), and cultured in a humidified cell culture incubator (37 °C, 5% CO2). The MBM-PDOs culture media was refreshed every three days. MBM-PDO cultures were observed daily, photographed every four days and passaged every 3-4 weeks.
Splitting of PDO-Cultures
The MBM-PDO-cultures were gently transferred from the ULA plates using a pipette, washed several times in basis medium, centrifuged and resuspended in 3-5 mL of TrypLE Express (Gibco, ThermoFisher Scientific, Waltham, MA, USA) and incubated at 37°C for 10 minutes. After washing the organoids with basis medium supplemented with 10% FCS, the cell pellet was resuspended in MBM-PDOs culture medium, seeded in ultra-low attachment (ULA) plates (Stemcell Technologies, Vancouver, Canada) and incubated at 37°C.
Embedding of PDO-Cultures
MBM-PDO cultures were fixed in 4% paraformaldehyde (PFA) overnight at 4°C, pelleted and embedded using HistoGel (Richard-Allan Scientific). The samples were allowed to cool and solidify at 4°C for one day and were then embedded in paraffin following standard protocols.
Immunohistochemistry
For immunohistochemistry (IHC) staining, 2µm thick sections were cut, deparaffinized, and pre-treated according to the standard protocols in the immunohistochemistry laboratory of the Institute of Pathology. Immunohistochemistry was performed on the Medac platform (Melan A: Agilent, clone A103, dilution 1:100; S100:Medac/Cell Marque, clone 4C4.9, dilution 1:2000; HMB45: Agilent, clone HMB45, dilution 1:400; Ki67: Zytomed, mouse anti-human, dilution 1:250, clone K-2;, CD8: Agilent; clone C8/144B, dilution 1:50) or on Ventana platform (CD4: Roche, clone SP35, ready-to-use-antibody). Slides were counterstained with hematoxylin and examined under the microscope (Olympus BX 50) for evaluation of reactivity.
Mutational Analysis
The mutational analysis for brain metastases was conducted either by next-generation sequencing (NGS) (Institute of Pathology) or pyrosequencing (Institute of Neuropathology). For primary tumors, DNA from paraffin-embedded material was extracted using the Maxwell RSC DNA FFPE Kit (Promega). DNA isolation from the organoids was carried out using the DNeasy Blood and Tissue kit (QIAGEN,Hilden, Germany).
Next Generation Sequencing (NGS)
DNA was eluted in 120 µl nuclease-free water and the concentration was determined on a Quantus™ fluorometer using the QuantiFluor® ONE ds DNA System (Promega). Generation of the sequencing library was performed using a QIAseqTM targeted DNA custom panel (Qiagen) with an input of 40 ng DNA. Amplification products were subjected to next generation sequencing on an Illumina MiSeq sequencer (Illumina). Sequencing data were analyzed for genomic variants using the CLC Genomics Workbench/Server 23 (Qiagen Bioinformatics).
Pyrosequencing of BRAF codon 600
Pyrosequencing was used to determine the sequence at hotspot codon 600 of the BRAF gene. A 122-bp fragment of BRAF- exon 15 was amplified using following primers BRAF-forward 5’-GAAGACCTCACAGTAAAAATAG-3’ and BRAF-reverse 5’-Biotin-ATAGCCTCAATTCTTACCATCC-3’. PCR was performed with the Pyromark PCR Kit (Qiagen) with 15 min 95°C, followed by 40 cycles of 94°C, 60°C and 72°C, 30 sec each and finally 72°C for 10 min. Single-stranded DNA templates were purified on streptavidin-sepharose high-performance beads (GE Healthcare) using the PSQ Vacuum Prep Tool and Worktable (Biotage). Pyrosequencing was performed using PyroMark® Gold Reagents (Qiagen) on the Pyromark Q24 instrument (Biotage) with the pyrosequencing primer 5’-AGGTGATTTTGGTCTAGCTA-3’. Positive and negative controls were used to compare results. Pyrograms were analyzed by PyroMark Q24 software (Biotage) using the allele quantification (AQ) module to determine the percentage of mutant versus wild type alleles according to percentage relative peak height.
Treatment with BRAF and MEK Inhibitors
To evaluate drug sensitivity, MBM-PDO cultures were seeded into a low attachment 96-well cell culture plate (SARSTEDT AG & CO. KG, Germany) with 50 µL of MBM-PDOs-culture medium in each well. After 24 hours of culture, 50 µL of the treatment medium was added to the organoid cultures. These cultures were subjected to a combination therapy of BRAF and MEK inhibitors (Dabrafenib (Cayman Chemical, Michigan, USA) and Trametinib (MCE MedChemExpress, Monmouth Junction, USA)), at various concentrations (1 μM, 0.5 μM, 0.25 μM, and 0.125 μM).
Measurement of Intracellular ATP
After 72 hours of drug treatment, the intracellular level of ATP was measured by Cell Titer-Glo 3D assay (Promega, G9682). Briefly, 100 µL of the Cell Titer-Glo reagent was added to each well followed by incubation at room temperature on an orbital shaker for one hour to ensure adequate cell lysis. After incubation, 100 µL samples were transferred to a white Nunc MicroWell 96-Well, Nunclon Delta-Treated, Flat-Bottom Microplate (Thermo Scientific,Massachusetts, USA). Luminescence measurements were conducted using a SPARK microplate reader (TECAN, Männedorf, Switzerland) with an integration time of 500 ms at the Institute of Experimental Oncology, University Hospital Bonn. Relative viability was calculated as a percentage, normalized to the vehicle control.
Results
Establishment and Cultivation of MBM-PDOs
To establish PDOs from melanoma brain metastases, we developed a 3D culture protocol that did not rely on tissue extracellular matrices such as Matrigel or collagen (Figure 1A). The PDO-cultures were successfully established from MBM samples in 7 out of 8 cases (Figure 1B), resulting in an overall success rate of 87.5%. We could cultivate metastases from previously untreated as well as from previously treated brain melanoma metastases (Table 1).
The PDO cultures from different patients exhibited a range of distinct morphologies, which were discernible by light microscopy examination of histological hematoxylin and eosin (H&E) stained sections (Figure 1C). Some of these cultures displayed a spherical structure with elongated, well-defined borders, while others exhibited a rounded structure or less structured organoids positioned adjacent to each other (Figure 1C). The intra-culture morphological variance of the PDOs was very low.
The growth rate of MBM-PDOs exhibited variation between different patients. The MBM-PDOs with a high rate of proliferation required passaging every 10-14 days, whereas the slower-proliferating organoids were re-passaged every 20-25 days. We evaluated the organoids' rate of growth by employing Ki-67 staining and distinguished them as having either a low or a high proliferation rate (≤ or > 40% of Ki-67 positive nuclei) (Suppl. Table 2). Five of the organoid cultures exhibited a high proliferation rate, while the remaining two organoid cultures displayed a low proliferation rate, and these distinctions were observed across different days.
MBM-PDOs Preserve Key Histological Features of Their Original Tumors
We could cultivate the organoids over a median of six passages (range four to twelve passages) and the histological and immunohistological features of the MBM-PDOs remained stable during passages.
To confirm that the PDOs faithfully recapitulated the histomorphology and histological features observed in the original tumors, we conducted a comparative immunohistochemical (IHC) staining. The cultivated MBM-PDOs exhibited positivity for melanoma markers, including S100, Melan A, and HMB45, consistent with their expression in the parental tumor samples (Figure 2).
However, it is noteworthy that the PDO cultures did not preserve the tumor immune microenvironment, resulting in negative stainings for CD4 and CD8 (Figure 2).
Importantly, the PDO cultures displayed stability in their melanoma immunohistochemistry markers, maintaining positive staining for S100 and Melan A even after multiple passages (Figure 3 A, B).
MBM-PDOs Recapitulate the Mutational Profiles of Their Original Tumors
Five out of the seven melanoma brain metastases harbored BRAF V600E mutations and two out of the seven cases had other less frequent mutations (one NRAS mutation, one KIT mutation). Those two cases were exposed to a panel next generation sequencing to test for further mutations. Five out of the seven MBM-PDO cultures fully maintained the mutational profile of the parental brain metastasis tissue. One case with BRAF wild type lost in vitro the POLE mutation demonstrated in the parental tumor (Table 2). In addition, one MBM-PDO culture acquired a TERT mutation that was not found in the parental tumor.
MBM-PDOs with BRAF V600E Mutations Show Therapy Response to BRAF and MEK Inhibitors
MBM-PDO cultures were treated with a combination of dabrafenib (BRAF-inhibitor) and trametinib (MEK-inhibitor) at four different concentrations (1µM+1µM, 0.5µM+0.5µM, 0.25µM+0.25µM, 0.125µM+0.125µM) for three days, followed by cell viability assessment (Figure 4A). The efficacy of the BRAF and MEK inhibitors on the responding PDO cultures was visually apparent through morphological changes in the organoids (Figure 4C). MBM-PDO cultures with the BRAF V600E mutation exhibited good therapy responses to the targeted therapy, involving the BRAF and MEK inhibitors, resulting in significant reductions in cell viability (<50%); whereas BRAF wild type cultures showed no changes in cell viability (Figure 4B). All four cases treated with BRAF and MEK inhibitors had a high proliferation rate (Ki-67 > 40%) (Suppl. Table 2).
Discussion
Patient-derived models, such as organoids and tumoroids, are important tools for studying tumor biology and for testing newly developed treatment modalities [13,14,15,16]. Recently, Sun et al. (2023) described organoids derived from primary mucosal melanomas. These organoids retained the histological and molecular features of the primary tumors and could be utilized for assessing drug therapy responses. Currently, limited data about organoid generation from primary skin melanoma are available [17,18].
To our knowledge, this is the first study establishing organoids from melanoma brain metastases. We were able to successfully cultivate seven out of eight cases for up to 10 passages. The one case which failed to grow was a brain metastasis relapse, which recurred following surgical resection of a melanoma brain metastasis, followed by stereotactic radiotherapy and immune checkpoint inhibitor therapy. This may be due to the prior therapy and the fact that we tried to cultivate tissue of a relapsed metastasis.
The MBM-PDO-cultures were stable in culture for several passages, preserving the immunohistological phenotype of the parental tumors throughout the passages, which is in line with the observations of Sun et al. in mucosal melanoma organoids (Sun et al. 2023). The MBM-PDO cultures exhibited varying proliferative activities, as revealed by Ki-67 staining. Some MBM-PDO cultures were highly proliferative (>40% positive nuclei), while others were lowly proliferative (<40%). The proliferation rate was concordant between the MBM-PDOs and their parental tumors We assessed the mutational status of the parental brain metastasis tissue and the MBM-PDO cultures and observed that BRAF mutations were conserved in culture. Five out of seven MBM-PDO cultures (71%) fully recapitulated the mutational profile of their parental tumors. Notably, both MBM-PDO cultures from BRAF wild type melanomas also had TERT promotor mutations. TERT mutations are common in melanoma (69%) and are associated with poor prognosis [19]. The most frequent mutation in primary brain tumors as well as in metastasis is the C250T mutation, corresponding to the mutation observed in our two cases. Interestingly, Blanco-Garcia et al. also noticed that the C250T TERT mutation was often associated with NRAS mutations, which was detected in one of our two cases with a TERT mutation. Melanoma brain metastases are the primary cause of death in 60-70% of melanoma cases [20]. Since the introduction of tyrosine kinase inhibitors and the MAPK inhibitors for the treatment of metastatic melanomas, the overall survival of patients increased dramatically. Two clinical studies, COMBI-d and COMBI-v, conducted on patients with metastasized melanoma and BRAF V600E and V600K mutations, showed a 5-year overall survival rate of 34% and a median overall survival time of 25.9 months with Dabrafenib plus Trametinib treatment [21]. For melanoma brain metastases with BRAF V600 mutations, a combination therapy with dabrafenib and trametinib is effective; however, responses are less durable than those of extracranial metastases with the same mutations [22]. The COMBI-r study reported a 10.8 months overall survival for patients with melanoma brain metastases with BRAF V600E or V600K mutations treated with dabrafenib/trametinib as the first-line therapy [23].We aimed to test the feasibility of utilizing MBM-PDO cultures as an in vitro platform to identify the efficacy of targeted therapy. To that end, we treated four cultures with a combination of dabrafenib/trametinib. As expected and described by Sun et al, the treatment response correlated with the mutational status of the tumors [24]. Two MBM-PDO cultures harboring BRAF V600E mutations had a very good response to the combination therapy, as assessed by cell viability, while BRAF wild type cultures were insensitive. Interestingly, also the MBM-PDOs harboring an NRAS mutation was insensitive to therapy. Since we treated the PDOs with MEK inhibitors, besides BRAF inhibitors, we expected a therapy response, even if was not as pronounced as for PDOs with BRAF mutations. This underlines the individualized patients’ response to targeted therapy.
In conclusion, we successfully established patient-derived organoids from melanoma brain metastases, which faithfully recapitulated the histological and mutational characteristics in culture, over passages. In vitro drug testing demonstrated the capacity of the MBM-PDOs to reveal targeted-therapy susceptibilities, which highlights their great potential in preclinical research, drug discovery, and personalized medicine.
Additional information
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
SAE and the study were partially supported by the Bonfor internal funding program of the Medical Faculty Bonn. AF is funded by the Deutsche Krebshilfe through a Mildred Scheel Nachwuchszentrum Grant (Grant number 70113307).
Contributors
Study concept and design: MIT, SEA, MH, EG. Acquisition of data: SEA, RH, AW, GG. Analysis and interpretation of data: all coauthors. Drafting of the manuscript: SEA, MIT, RH, JS, AF, GG, AW, MS. Critical revision of the manuscript for important intellectual content: all coauthors.
Acknowledgments
The authors thank Ms. Susanne Steiner, Ms. Agnes Leier and Mr. Carsten Golletz for their excellent technical assistance. We are grateful to Ms. Frigga Hönig (Administrative Assistant) who help us with the sample logistics We thank the staff of the Institute of Pathology, the Institute of Neuropathology and the medical staff of the Clinic for Neurosurgery for their support.
Ethics approval
The study was performed according to the Declaration of Helsinki. Informed consent was obtained from all patients included. The study was approved by the Ethics Committee of the Medical Faculty, University Bonn (#417/17 with amendment from 2020; #169/23).
Competing Interests
The authors have no competing interest regarding this study.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
| PDO: patient-derived-organoids |
| MBM: melanoma brain metastases |
| MBM-PDO: patient-derived-organoids from melanoma brain metastases |
| NGS: next-generation sequencing |
References
- Achrol AS, Rennert RC, Anders C, et al. Brain metastases. Nat Rev Dis Primers. 2019;5(1):5. [CrossRef]
- Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr Oncol Rep. 2012;14(1):48-54. [CrossRef]
- Stelzer KJ. Epidemiology and prognosis of brain metastases. Surg Neurol Int. 2013;4(Suppl 4):S192-202. [CrossRef]
- Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417(6892):949-954. [CrossRef]
- Robert C, Karaszewska B, Schachter J, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. 2015;372(1):30-39. [CrossRef]
- Ascierto PA, McArthur GA, Dréno B, et al. Cobimetinib combined with vemurafenib in advanced BRAF(V600)-mutant melanoma (coBRIM): updated efficacy results from a randomised, double-blind, phase 3 trial. Lancet Oncol. 2016;17(9):1248-1260. [CrossRef]
- Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N Engl J Med. 2019;381(16):1535-1546. [CrossRef]
- Robert C, Ribas A, Schachter J, et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019;20(9):1239-1251. [CrossRef]
- Robert C, Carlino MS, McNeil C, et al. Seven-Year Follow-Up of the Phase III KEYNOTE-006 Study: Pembrolizumab Versus Ipilimumab in Advanced Melanoma. J Clin Oncol. 2023;41(24):3998-4003. [CrossRef]
- Kim M, Mun H, Sung CO, et al. Patient-derived lung cancer organoids as in vitro cancer models for therapeutic screening. Nat Commun. 2019;10(1):3991. [CrossRef]
- Karkampouna S, La Manna F, Benjak A, et al. Patient-derived xenografts and organoids model therapy response in prostate cancer. Nat Commun. 2021;12(1):1117. [CrossRef]
- Wensink GE, Elias SG, Mullenders J, et al. Patient-derived organoids as a predictive biomarker for treatment response in cancer patients. NPJ Precis Oncol. 2021;5(1):30. [CrossRef]
- Freitas de Morais E, Da Siquara Rocha LdO, Souza Santos JL de, et al. Use of Three-Dimensional Cell Culture Models in Drug Assays for Anti-Cancer Agents in Oral Cancer: Protocol for a Scoping Review. J Pers Med. 2023;13(11). [CrossRef]
- Sahgal P, Patil DT, Bala P, et al. Replicative stress in gastroesophageal cancer is associated with chromosomal instability and sensitivity to DNA damage response inhibitors. iScience. 2023;26(11):108169. [CrossRef]
- Vazquez-Armendariz AI, Tata PR. Recent advances in lung organoid development and applications in disease modeling. J Clin Invest. 2023;133(22). [CrossRef]
- Ren X, Huang M, Weng W, et al. Personalized drug screening in patient-derived organoids of biliary tract cancer and its clinical application. Cell Rep Med. 2023;4(11):101277. [CrossRef]
- Ou L, Liu S, Wang H, et al. Patient-derived melanoma organoid models facilitate the assessment of immunotherapies. EBioMedicine. 2023;92:104614. [CrossRef]
- Zhou S, Lu J, Liu S, et al. Role of the tumor microenvironment in malignant melanoma organoids during the development and metastasis of tumors. Front Cell Dev Biol. 2023;11:1166916. [CrossRef]
- Blanco-García L, Ruano Y, Blanco Martínez-Illescas R, et al. pTERT C250T mutation: A potential biomarker of poor prognosis in metastatic melanoma. Heliyon. 2023;9(8):e18953. [CrossRef]
- Gutzmer R, Vordermark D, Hassel JC, et al. Melanoma brain metastases - Interdisciplinary management recommendations 2020. Cancer Treat Rev. 2020;89:102083. [CrossRef]
- Robert C, Grob JJ, Stroyakovskiy D, et al. Five-Year Outcomes with Dabrafenib plus Trametinib in Metastatic Melanoma. N Engl J Med. 2019;381(7):626-636. [CrossRef]
- Davies MA, Saiag P, Robert C, et al. Dabrafenib plus trametinib in patients with BRAFV600-mutant melanoma brain metastases (COMBI-MB): a multicentre, multicohort, open-label, phase 2 trial. Lancet Oncol. 2017;18(7):863-873. [CrossRef]
- Berking C, Livingstone E, Debus D, et al. COMBI-r: A Prospective, Non-Interventional Study of Dabrafenib Plus Trametinib in Unselected Patients with Unresectable or Metastatic BRAF V600-Mutant Melanoma. Cancers (Basel). 2023;15(18). [CrossRef]
- Sun L, Kang X, Ju H, et al. A human mucosal melanoma organoid platform for modeling tumor heterogeneity and exploring immunotherapy combination options. Sci Adv. 2023;9(43):eadg6686. [CrossRef]
Figure 1.
(A) Graphical abstract for the MBM-PDOs generation. Tumor samples are dissociated into single cell suspensions and grown in low-attachment plates (created with BioRender.com). (B) Bright-field images of PDOs after 1 day and 10 days of culture establishment (scale bar 100 µm). (C) Bright-field images (5x magnification) and hematoxylin and eosin staining (10x magnification) showing different phenotypes of MBM-PDOs.
Figure 1.
(A) Graphical abstract for the MBM-PDOs generation. Tumor samples are dissociated into single cell suspensions and grown in low-attachment plates (created with BioRender.com). (B) Bright-field images of PDOs after 1 day and 10 days of culture establishment (scale bar 100 µm). (C) Bright-field images (5x magnification) and hematoxylin and eosin staining (10x magnification) showing different phenotypes of MBM-PDOs.
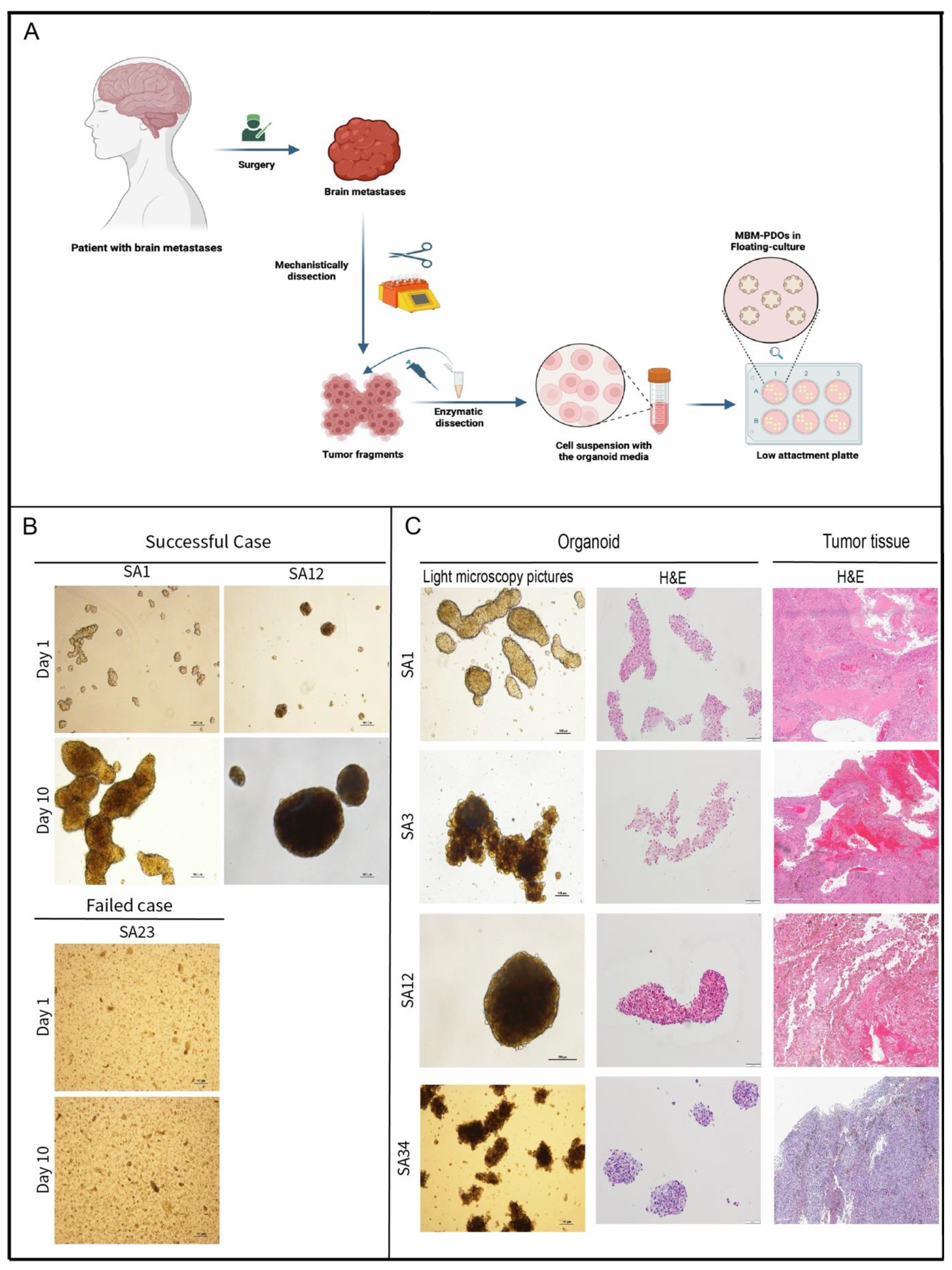
Figure 2.
Representative images of hematoxylin & eosin staining and immunohistochemical staining (for Melan A, S100, HMB45, CD4, CD8, and Ki67) of the parental tumors and their MBM-PDO cultures (10x and 20x magnification).
Figure 2.
Representative images of hematoxylin & eosin staining and immunohistochemical staining (for Melan A, S100, HMB45, CD4, CD8, and Ki67) of the parental tumors and their MBM-PDO cultures (10x and 20x magnification).
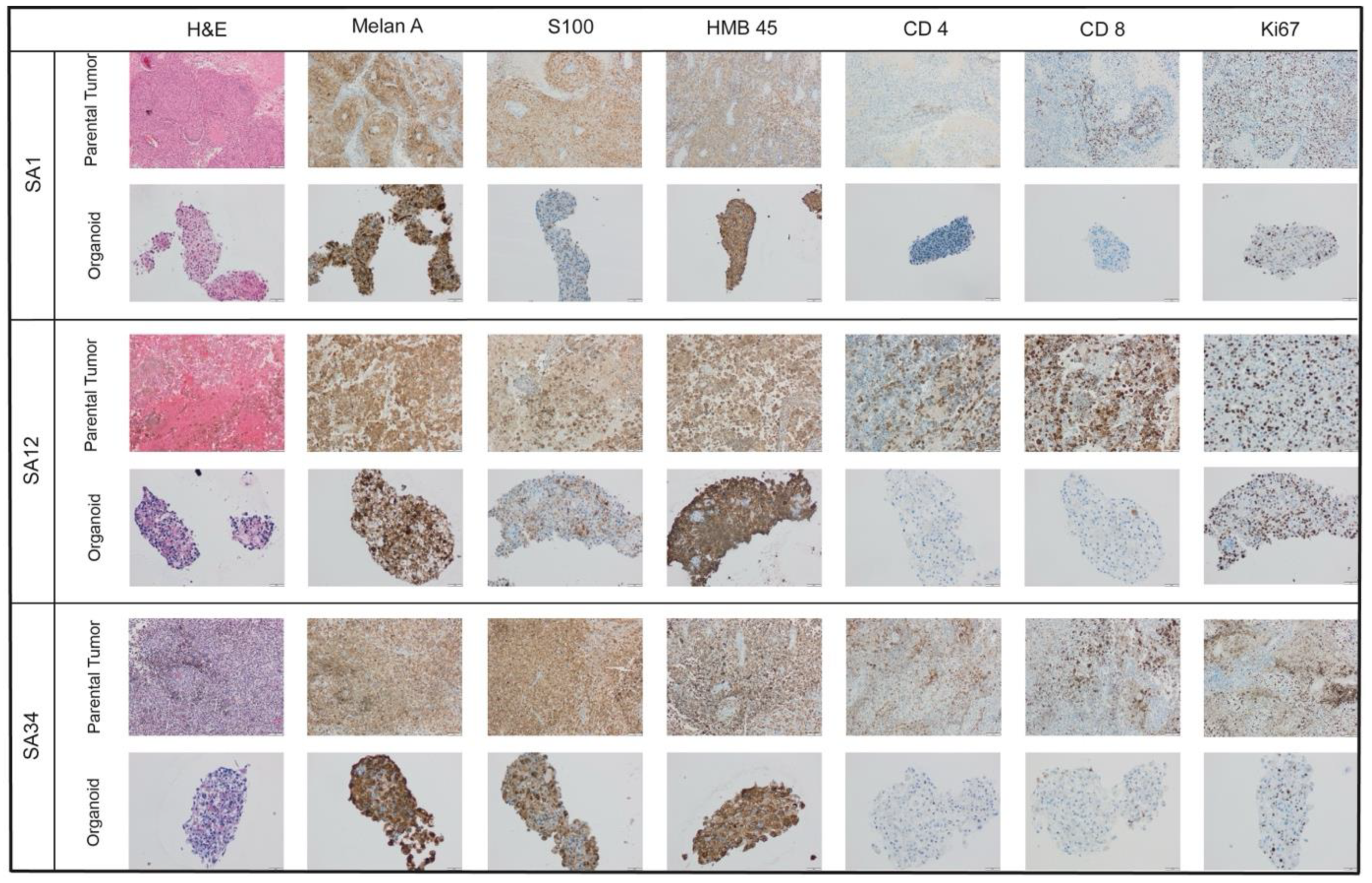
Figure 3.
Bright-field images (5x magnification) and representative images of immunohistochemical stainings for Melan A and S100- Staining (10x magnification) of different passages showing the stability of organoid-morphology and immunohistochemical profile. (A) SA34 MBM PDO-culture. (B) SA1 MBM PDO-culture. P; Passage.
Figure 3.
Bright-field images (5x magnification) and representative images of immunohistochemical stainings for Melan A and S100- Staining (10x magnification) of different passages showing the stability of organoid-morphology and immunohistochemical profile. (A) SA34 MBM PDO-culture. (B) SA1 MBM PDO-culture. P; Passage.
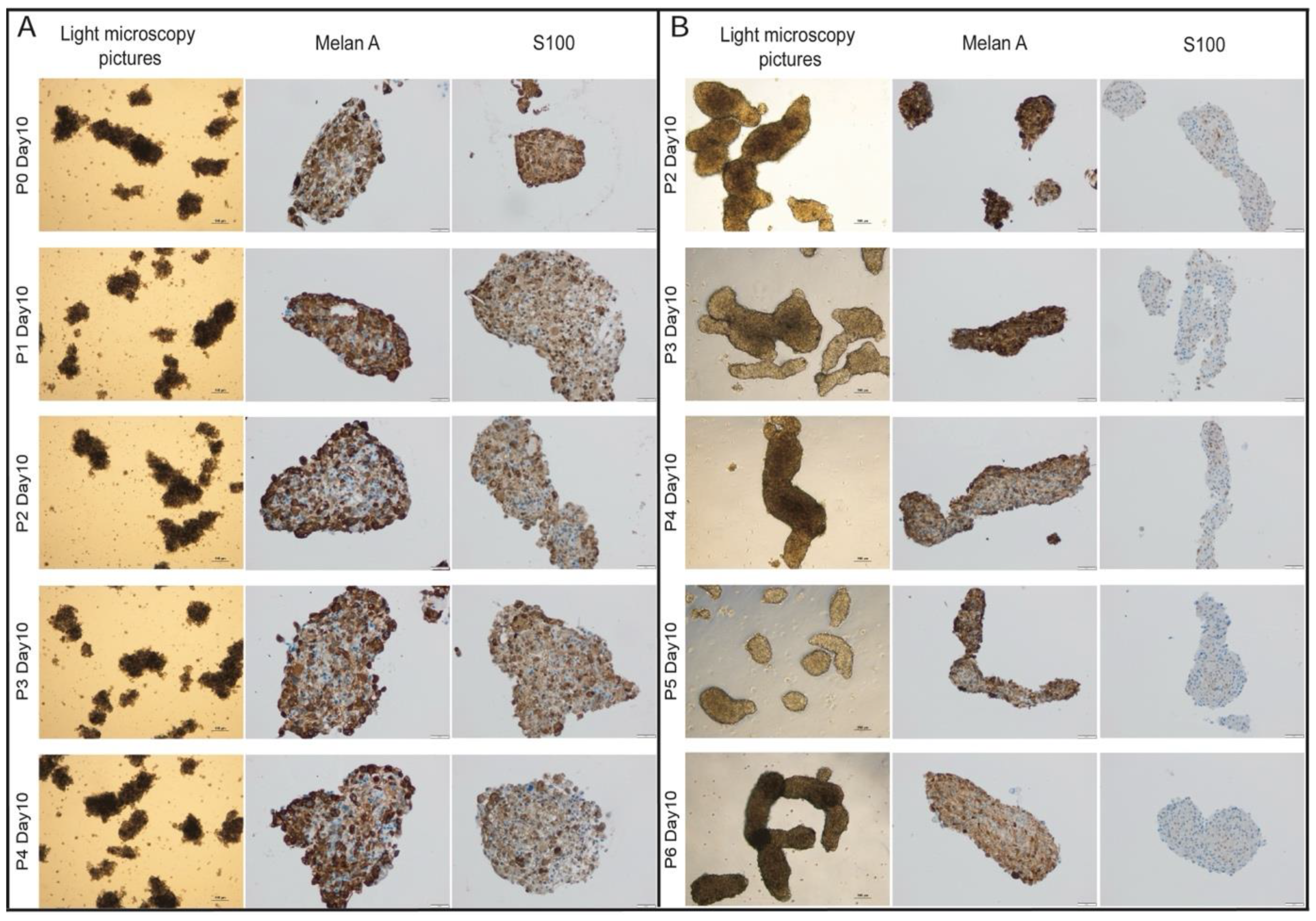
Figure 4.
(A) Graphical abstract for the in vitro drug sensitivity assay (Created with Biorender.com). (B) A dose-response graph depicting the cell viability of MBM-PDO cultures treated with different concentrations of dabrafenib and trametinib for 72 hours. Cell viability, assessed using the CellTiter-Glo assay (Promega), was normalized to the vehicle control. Each condition was tested in technical and biological triplicates. Data are presented as mean ± SEM. (C) Representative brightfield microscopy images of MBM-PDO cultures taken after 72 hours of treatment with 1µM and 0.125µM dabrafenib and trametinib, as well as vehicle control (top row) (scale bar 100 µm).
Figure 4.
(A) Graphical abstract for the in vitro drug sensitivity assay (Created with Biorender.com). (B) A dose-response graph depicting the cell viability of MBM-PDO cultures treated with different concentrations of dabrafenib and trametinib for 72 hours. Cell viability, assessed using the CellTiter-Glo assay (Promega), was normalized to the vehicle control. Each condition was tested in technical and biological triplicates. Data are presented as mean ± SEM. (C) Representative brightfield microscopy images of MBM-PDO cultures taken after 72 hours of treatment with 1µM and 0.125µM dabrafenib and trametinib, as well as vehicle control (top row) (scale bar 100 µm).
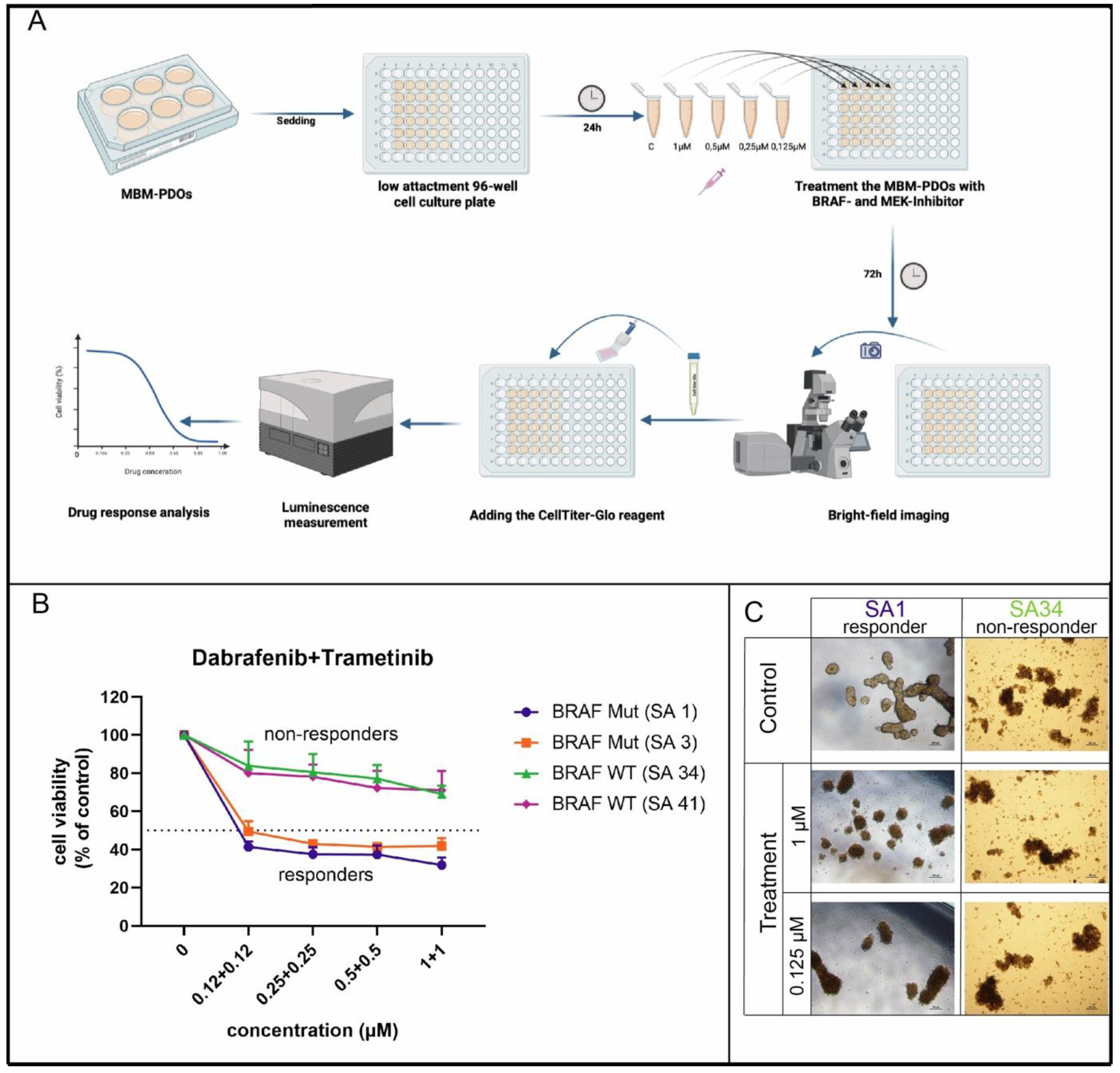

Table 1.
Clinico-pathological characteristics.
| Age | Median | 55 | |
| Sex | Male | 5 (62.5%) | |
| Female | 3 (37.5%) | ||
| Localization | Frontal | 4 (50%) | |
| Parietal | 3 (37.5%) | ||
| Occipital | 1 (12.5%) | ||
| Number of brain metastases | singular | 6 (75%) | |
| multiple | 2 (25%) | ||
| Extracranial metastases | 0 | 5 (62.5%) | |
| Pulmonary | 1 (12.5%) | ||
| Osseous | 2 (25%) | ||
| TNM | T | pTx (First diagnosis) | 2 (25%) |
| pT1 | 0 (0%) | ||
| pT2 | 1 (12.5%) | ||
| pT3 | 4 (50%) | ||
| pT4 | 1 (12.5%) | ||
| N | pN0 | 5 (62.5%) | |
| pN1 | 2 (25%) | ||
| pN2 | 1 (12.5%) | ||
| M | pM1 | 8 (100%) | |
| Mutation | BRAF V600E | 5 (62.5%) | |
| BRAf wildtype | 3 (37.5%) | ||
| Therapy | pre neurosurgical resection | Stereotactic Radiotherapie | 3 (37.5%) |
| Interferon therapy | 2 (25%) | ||
| Combination immunotherapy | 3 (37.5%) | ||
| post neurosurgical resection | BRAF and MEK inhibitor (tafinlar mekinist) | 2 (25%) | |
| Combination immunotherapy (Nivolumab,Ipilimumab) | 3 (37.5%) | ||
Table 2.
Mutational analysis of the primary tumors and paired PDO.
| Case | Primary tumor | Organoid |
| SA1 | BRAF V600 E | BRAF V600 E |
| SA3 | BRAF V600 E | BRAF V600 E |
| SA12 | BRAF V600 E | BRAF V600 E |
| SA17 | BRAF V600 E | BRAF V600 E |
| SA20 | BRAF V600 E | BRAF V600 E |
| SA34 | BRAF V600 WT NRAS p.Q61K |
BRAF V600 WT NRAS p.Q61K TERT c.146C>T |
| SA41 | BRAF WT KIT p.L576P TERT c.146C>T TERT c.125_124delinsTT POLE c.1360-1>A |
BRAF V600 WT KIT p.L576P. TERT c.146C>T TERT c.125_124delinsTT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



