
Submitted:
06 July 2024
Posted:
09 July 2024
You are already at the latest version
Abstract
: Optical coherence tomography is a non-invasive imaging technique that provides three-dimensional visualization of subsurface tissue structures. OCT has been proposed and explored in literature as a tool to assess oral cancer status, select biopsy sites, or identify surgical margins. Our endoscopic OCT device can generate widefield (centimeters long) imaging of lesions at any location in the oral cavity – but it is challenging for raters to quantitatively assess and score large volumes of data. Leveraging a previously developed epithelial segmentation network, this work develops quantifiable biomarkers that provide direct measurements of tissue properties in three-dimensions. We hypothesize that features related to morphology, tissue attenuation, and contrast between tissue layers will be able to provide a quantitative assessment of disease status (dysplasia through carcinoma). This work retrospectively assesses seven biomarkers on a lesion-contralateral matched OCT dataset of lateral and ventral tongue (40 patients, 70 sites). Epithelial depth and loss of epithelial-stromal boundary visualization provide the strongest discrimination between disease states. The stroma optical attenuation coefficient provides distinction of benign lesions from dysplasia and carcinoma. The stratification biomarkers visualize subsurface changes which provides potential for future utility in biopsy site selection or treatment margin delineation.
Keywords:
optical coherence tomography
; oral cancer
; endoscopic imaging
; cancer morphology
; optical biopsy
1. Introduction
Oral squamous cell carcinoma (OSCC) accounts for almost all malignant tumors of the lip and oral cavity and is often detected in advanced stages associated with high mortality [1,2]. Early diagnosis is associated with better patient outcomes, but this is challenging to achieve.
Oral cancers often progress from normal tissue, through grades of dysplasia, to carcinoma [3,4]. During progression there are cellular changes in size, shape, and nuclear properties, as well as larger changes in tissue architecture [5]. The earliest dysplastic changes (mild dysplasia / grade 1) are characterized by architectural changes and cellular atypia in the bottom third of the epithelium closest to the epithelial-stromal boundary. Moderate (grade 2) dysplasia and severe (grade 3) dysplasia represent changes in the bottom two-thirds of the epithelium and more than two-thirds of the depth of epithelium respectively [4]. While mild and moderate dysplasia are reversible and are generally subject only to monitoring, severe dysplasia through carcinoma requires treatment.
If a biopsy is taken of the lesion, architectural and cytologic changes can be assessed histologically [6]. However, identifying the most pathologic site within a lesion is challenging, and is further complicated by benign lesions which may have a similar appearance to occult lesions [7]. As such, multiple biopsies are often taken to avoid false negatives or underdiagnosis. Tools that allow for noninvasive monitoring of subsurface structures may reduce the need for biopsy in mild and moderate dysplasia, as well as aid in biopsy site selection to improve diagnostic yield. Similarly, surgery is the primary treatment for OSCCs. Capturing all margins reduces recurrence, but excessive margins may have negative cosmetic or functional effects [8]. A tool that could improve margin delineation may improve cancer-free survival and minimize surgery-related morbidities.
Optical coherence tomography (OCT) is a non-invasive, label-free imaging technique that generates high-resolution imaging of subsurface structures at a limited depth [9]. OCT is an interferometric technique: images are produced by scanning a low-coherence beam of light across a sample and interfering the collected backscattered light with a pathlength-matched reference beam. The lateral resolution of OCT is a function of the focusing optics; the axial (depth) resolution is a function of the light source. OCT devices can be tailored to their application: some non-contact scanning devices use supercontinuum light sources and objective lenses to achieve sub-micron resolutions [10], while fiber-optic based endoscopic systems are optimized to access luminal organs at the cost of lower resolutions (~40 µm lateral) [11,12]. This flexibility has allowed OCT to be explored in many cancer imaging applications [13]. The geometry captured in OCT has been shown to correlate precisely with histology [14], and the intensity of OCT can be used to estimate the depth-resolved attenuation coefficient, providing insights into the optical properties of the sample [15].
OCT has been previously explored in oral cancer applications [16]. Studies have assessed ex vivo tumor tissue for diagnostic utility in oral precancerous or potentially malignant lesions [17,18,19,20,21,22,23]. In vivo oral OCT has primarily been conducted with hand-held galvanometer scanning devices [24,25,26,27,28,29]; we have previously shown endoscopic OCT of the oral cavity acquired with rotary-pullback catheters [30]. OCT can visualize keratin, epithelial, and subepithelial layers, the presence or absence of the epithelial-stromal boundary, and microanatomical features such as vasculature, salivary ducts, or rete pegs.
OCT in oral cancer applications is an area of active research, and there is currently no consensus on diagnostic criteria. Approaches from qualitative classification systems [26] to quantitative measurements of epithelial thickness [17,28,31,32], optical attenuation [33], or texture features [22] have been explored. Epithelial thickness has been measured in vivo for different sites across the oral cavity and has been found to vary depending on site [28,29]. And even within the same site, variation between individuals precludes the use of absolute epithelial thickness alone to indicate pathology. In addition, assessment of OCT introduces another challenge: large three-dimensional datasets which require interpretation by an expert rater to identify pathologies of interest. Human assessment of each individual frame is intractable, but AI tools are well-suited to rapid interpretation of images.
We have previously reported a deep learning epithelial segmentation tool [34]. This work leverages that segmentation tool, and previously collected endoscopic oral OCT data [30] to develop quantifiable biomarkers that provide direct measurements of oral tissue properties in three-dimensions. This work explores the ability of these biomarkers to distinguish lesions from their contralaterals as well as between disease states (dysplasia through carcinoma). As mild and moderate dysplasia requires no clinical intervention other than monitoring, we also examine the ability of these biomarkers to distinguish dysplastic lesions that later progress to a lesion requiring intervention. And lastly, as this retrospective dataset is inclusive of imaging at multiple timepoints for a few patients, we explore the reproducibility of measurements and speculate on their potential as a monitoring tool.
2. Materials and Methods
2.1. Study Design
This is a hypothesis-generating study intended to provide future direction for diagnostic criteria in oral OCT measurement. This work represents a retrospective analysis of a larger imaging trial (n=123 patients) from 2014-2017 [30]. Imaging was collected of lesions paired with contralateral site measurements. As patients were recruited from a long-term monitoring clinic, some patients were imaged repeatedly over multiple time points. This work will explore three aims: (1) whether the proposed biomarkers can discriminate between lesion and contralateral and/or between disease states; (2) whether the proposed biomarkers can distinguish future progressors within the mild and moderate dysplasia groups; and (3) whether the proposed biomarkers can be measured repeatably and/or capture longitudinal changes.
Inclusion criteria: For consistency, only images acquired with the same OCT system were selected. While the full dataset includes small numbers of lesions on the lip, soft/hard palate, floor of mouth, gingiva, or vestibule, most cases are lesions on the tongue. This is as anticipated; the oral tongue is the most common subsite for OSCCs and has the worst prognosis [35,36]. We selected lesions only on the lateral and ventral tongue as they are the most histologically comparable; the dorsal tongue contains papillae which changes the appearance of structural features.
Exclusion criteria: Imaging that was of insufficient quality, as characterized by excessive artifacts obscuring the tissue, poor selection of the reference resulting in blurring (assessed by examining the sheath layers), or poor tissue contact (<50% of the volume) with the imaging probe were not included in this study. For all analyses except for aim (3) only one time point per patient was used for this study; the selected time point was chosen using a random number generator.
2.2. OCT System
The OCT system used for this study has been described in detail previously [30]. Briefly, a 50 kHz swept-source laser (SSOCT-1310, Axsun Technologies Inc., Billerica, MA) with 20 mW output power feeds a single-mode fiber 90/10 sample/reference split Mach-Zehnder OCT interferometer. The sample arm consists of a fiber-optic rotary joint that connects to a 0.9 mm diameter side-looking rotary-pullback catheter (Dragonfly OPTIS imaging catheter, Abbott Medical Inc. Westford, MA). A custom-built rotary-pullback drive provides two-dimensional scanning at rotational rates up to 100 Hz and pullback lengths up to 90 mm. To minimize artifacts and improve image quality, fiber-based polarization diversity detection was implemented [37].
As shown in Figure 1, this endoscopic imaging system results in long but narrow images, which includes a region of non-tissue contact for approximately one third of the azimuthal direction (Figure 1a). To allow for good access to all parts of the oral cavity, catheters were inserted into a 1.5mm OD closed-ended plastic sheath that was attached to either a modified saliva ejector with a formable wire or a paddle (Figure 1b) fashioned from a disposable dental mirror with the reflective sticker removed [30]. The sheath was pad printed with black index markers (indicated by ‘m’) spaced every 10 mm to facilitate lesion registration. Whenever possible, index markers were oriented towards the non-tissue side of the catheter holders to not interfere with imaging.
OCT volumes are presented as en face (y-θ) mean intensity projections (Figure 1(i)) and longitudinal (y-z) sections (Figure 1(ii)), where y is the pullback dimension, θ is the circumferential angle around the pullback dimension, and z is the depth into the tissue. The location of longitudinal section locations within the en face projections are indicated with dashed lines. The images are oriented with the distal end of the catheter to the left and the proximal end of the catheter to the right. The color scale ranges from black to gold, which we refer to as ‘dark’ or ‘low intensity’ and ‘bright’ or ‘high intensity’ corresponding the magnitude of light returned from tissue (typically due to backscattering). En face projections are presented with square pixels such that they best represent the geometry of clinical presentation. Longitudinal sections presented in this work are stretched in the A-line direction (z) for better visualization of subtle layering structures. All scale bars are 1 mm.
In longitudinal sections, the epithelium may be visualized as a darkened layer (‘E’) superficial to the brighter stroma (‘S’). This transition much more prominent in the benign lesion (Figure 1d) than the carcinoma (Figure 1c), where there appears to be thicker, brighter epithelium and/or some destruction of the epithelial-stromal boundary such that there is no sharp distinction between epithelium and stroma. Air bubbles (‘b’) in the water between the two catheter sheaths or between the catheter and the tissue appear as oval artifacts in the en face view and vertical shadowed regions in the longitudinal view. There are other artifacts such as non-uniform rotational distortion (not pictured), or occlusive substances such as mucous or markers present in some images; an example is seen in panel Figure 1d(ii) and is labelled ‘a’.
2.3. Image Collection
This study was approved by the Institutional Review Boards of the British Columbia Cancer Agency and the University of British Columbia (Approval number: H11-02516). Volunteers were recruited from the Vancouver General Hospital Innovative Approach to Triage Oral Precancer (VGH iTOP) clinic and provided informed written consent. The iTOP clinic sees and monitors patients that have premalignant oral lesions.
Patients presenting with oral lesions were examined under white light examination by an oral oncologist (CP or SN) followed by autofluorescence evaluation with VELScope. If biopsy of the lesion was deemed necessary as part of normal clinical care the following imaging protocol was performed. Clinical impression based on white light and autofluorescence was used to identify the most abnormal part of the lesion that would be biopsied. One of the black markers on the OCT catheter was placed on this site and a volumetric pullback was collected. Imaging on both sides of the black marker was collected straddling the planned biopsy site. Toluidine Blue solution was then applied to the lesion post-imaging to assist clinical assessment of the lesion. Finally, an incisional or 5 mm punch biopsy was collected and processed following standard practice for histopathological diagnosis.
2.4. Deep Learning Segmentation
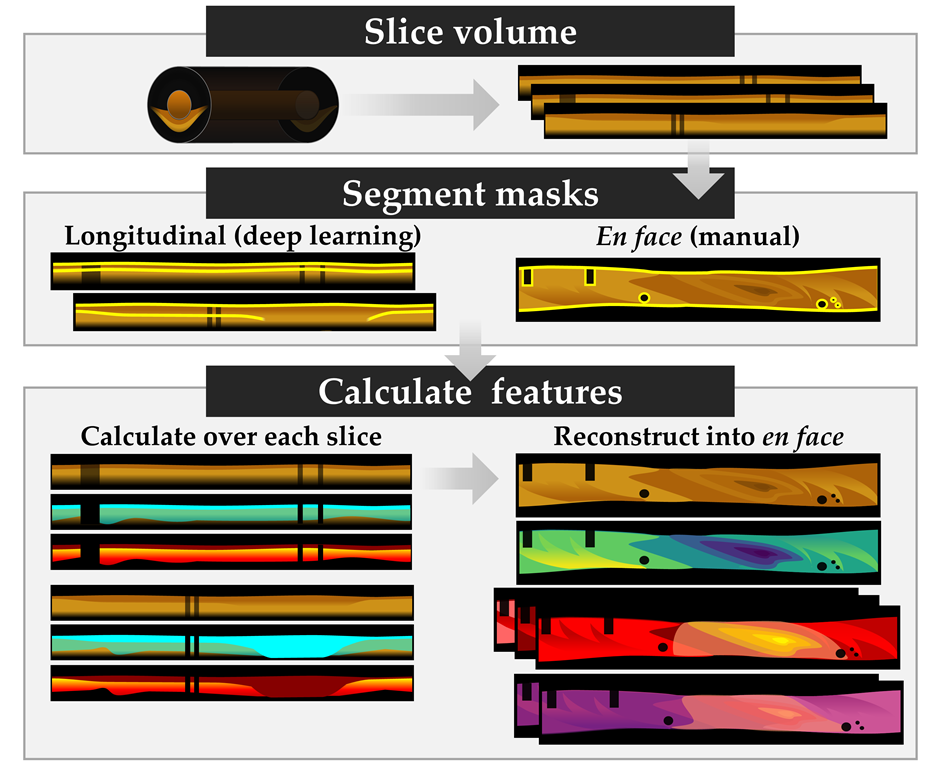
This work explores the potential diagnostic utility of quantitative biomarkers. As it is not possible to manually segment each frame of the volumetric OCT data (the dataset described herein represents >35,000 frames), we use a previously developed deep learning pipeline [34] to segment the surfaces of the epithelium and stroma from longitudinal OCT sections. This allows us to calculate biomarkers on each longitudinal slice and generate en face measurements of each volume.
Briefly, this pipeline consists of a series of two classifiers and two U-Nets were trained on longitudinal sections to (1) identify the field of view (i.e., regions of tissue contact), (2) identify artifacts (bubbles, sheath markers), (3) segment the epithelium surface, and (4) segment the epithelial-stroma interface. Each network was trained and tested independently of each other such that they could be used outside of the pipeline described in [34].
The field-of-view network classifies whole longitudinal slices, rejecting those without sufficient tissue contact. The artifact classifiers used a tile-wise approach to generate a rough estimate of regions where the segmentations may not be trustworthy. While this approach is sufficient for visual assessment, quantitative measurement requires more precision in locating the boundaries of tissue contact and removal of artifacts than the tile-wise training approach of the network provided. As such, this work employed the previously described segmentation networks to identify the epithelium region, but the regions of tissue contact and artifacts were segmented manually on mean en face projections by an experienced OCT rater (JM).
2.5. Image Processing
All image processing is conducted in MATLAB 2023a; deep learning predictions are generated using Python 3.6.9 with a PyTorch framework as previously described. All experiments were performed on a Windows 10 operating system, with Intel Core i7-12700K 3.60 GHz CPU, NVIDIA GeForce GTX 3080Ti GPU, and 32 GB of RAM.
An example of the image processing methods can be seen in Figure 2. First, images are sliced from cylindrical volumes into longitudinal frames (Figure 2(ii)), rescaled such that each pixel is 10 μm square (using the index of refraction of water as an immersion medium) in both the pullback and A-line direction. The example frame (Figure 2(ii-v)) has been rescaled in the A-line direction for presentation purposes. Most volumes are comprised of 504 or 512 longitudinal frames (collected at scan rates of 98 or 100 Hz), 3-9 cm in length, and collected at a pullback speed of 1-10 mm/s. Rescaling allows for each pixel to represent the same geographic area and is done with bicubic interpolation.
Each longitudinal frame was saved as a .tif for interpretation by the deep learning network. After post-processing to remove small gaps as described in [34], the network generates annotation masks containing a single pixel-wide line for the epithelial surface and epithelial-stromal boundary. As shown in Figure 2, the ability of the deep learning network to discriminate epithelium and stroma is subject to its training data. On the left-hand side of this image (Figure 2(ii-v)), hyperparakeratosis (‘HPK’) is present as a bright region above the epithelium; however, keratosis was not labelled by raters as part of the training regime for this network and thus it is misinterpreted as epithelium.
The mean en face projection of the volume was segmented using in-house annotation software developed as part of [34]. This segmentation included (1) the region of tissue contact to retain, (2) artifacts to remove (bubbles, sheath markers, other artifacts), and (3) the area of the volume containing lesion. Lesion annotations were selected using sheath markers for localization against recorded positions and were confirmed against clinical photos. These en face masks are then sliced and scaled in the same fashion as the images to produce a vector containing a flag for each A-line in each longitudinal image.
The epithelial and stromal segmentations are then used to define an epithelial region (‘E’) from the surface of the epithelium to the surface of the stroma, and stromal region (‘S’) from the surface of the stroma to the bottom of the visualized region as shown in (Figure 2(iii)). The bottom of the visualized region is defined as ending when the signal is 6 dB above the intensity of the noisefloor. The noisefloor value is calculated from the bottom 25 pixels (250 μm) of the frame. First, A-lines containing no tissue are excluded (i.e., A-lines that contain no epithelial surface segmentation), then the region is smoothed with a 5-pixel Gaussian kernel, and finally the noisefloor is taken to be the mean value of this region. In regions where there is a loss of epithelial-stromal boundary visualization (‘*’) and the surface of the stroma is not identified by the network as shown in the center of panel (Figure 2(iii)), the assumption is made that the entire depth of the visualized region is epithelium. The epithelium and stroma region masks are saved and are used for calculation of biomarkers.
2.6. Biomarker Measurement
After pre-processing, each longitudinal frame has a mask for the (1) epithelial region, (2) stromal region, (3) regions to exclude due to poor tissue contact or artifacts, and (4) regions to calculate biomarkers over that contain a clinically visible lesion. Seven features are selected for investigation that can be calculated on each longitudinal frame. After calculation, each measurement is reinterpreted as an en face projection as is appropriate for their dimensionality (three-dimensional features are represented as mean en face projections; two- and one-dimensional features do not require additional reinterpretation), allowing the viewer to assess each measurement with the same geometry as their clinical presentation. These measurements are summarized in Table 1: they include morphologic features calculated purely from the epithelial and stromal masks, attenuation features which describe the attenuation coefficient of distinct regions, and stratification features which compare the attenuation coefficient in different regions.
Morphologic features: Epithelial depth is calculated as the height of the epithelial region mask as shown in Figure 2(iii), generating one depth measurement per A-line and reported in μm. The loss of epithelial-stromal boundary is a one-dimensional measurement, reported as a percentage of the total region with no stromal surface segmentation compared to the total region of tissue (i.e., containing an epithelial surface segmentation) excluding artifacts. For visualization purposes, this is also saved as an en face mask of regions with a loss of epithelial-stromal boundary visualization that can be displayed in combination with other en face projections. From previous studies in oral OCT, we anticipate that increases in disease status will correspond to an increase in both epithelial depth and loss of epithelial-stromal boundary visualization [17,28].
Both morphologic features are subject to challenges associated with the geometry of endoscopic scanning. When the A-line is sampling tissue tangential to the tissue surface for example, the probe begins to lose tissue contact at the limits of the azimuthal scan, the epithelial depth may appear artificially deep and/or the epithelial-stromal boundary may no longer be able to be visualized. This also affects the regions over which attenuation coefficient and stratification features are calculated. We refer to this this phenomenon as ‘edge effects’ subsequently.
Attenuation features: The attenuation coefficient () is an optical property of the sample corresponding to the exponential decay of light through the tissue due to scattering and absorption. This provides a quantitative examination of the optical properties of the tissue and is less variable between imaging sessions than intensity which is subject to fluctuations from the power source, catheter quality, reference position, and user handling. The depth resolved (3D) attenuation coefficient is calculated using the method described by Liu et al. [38] over a region from the epithelial surface to the bottom of visualized region (6dB above the noisefloor). This produces a new longitudinal section as demonstrated by Figure 2(v). Mean en face projections are then taken over the entire depth of visualized tissue (‘overall’), epithelial region, and stromal region. From Yang et al., we anticipate that carcinoma will have a lower overall attenuation coefficient than contralateral, though previous work has not examined the epithelium and stroma independently [33].
Stratification features: Lastly, we propose ratiometric features that compare the attenuation coefficient from different regions. For each A-line, we calculate stratification as a ratio of the difference in attenuation coefficient between two regions over their sum which produces a normalized value from -1 to +1.
We anticipate epithelial-stromal stratification will capture changes related to the loss of tissue stratification: as the contrast between the layers is low this value will be near zero and otherwise will characterize the direction of attenuation coefficient difference. Secondly, we explore intraepithelial stratification. Dysplastic grading in oral cancer examines the presence of cellular atypia in each third of the epithelium; however, as healthy epithelium only represents 20-30 pixels (200-300 μm) [29] it was deemed more robust to examine halves rather than thirds. These regions, described as upper epithelium (‘UE’) and lower epithelium (‘LE’), are demonstrated in Figure 2(iv).
2.7. Quantitative and Statistical Analysis
For most biomarkers (except for the one-dimensional loss of epithelial-stromal boundary visualization), each volume includes a measurement for every A-line. This represents thousands of datapoints, some of which may include tissue outside of the area of lesion or regions with edge effects. For statistical analysis, a single median value is used for each biomarker of each volume. Only datapoints within areas of tissue contact are included in the calculation of the median value; all regions labelled as artifacts are excluded. To minimize the impact of edge effects on quantitative analysis, a vertical (azimuthal) erosion operator is applied to the en face tissue contact mask such that only the central 50% of the tissue mask is retained. For lesions, only datapoints within the labelled lesion area are included. Statistical analysis is conducted in TIBCO Statistica 14.
This is a hypothesis-generating study intended to provide future direction for diagnostic criteria in oral OCT measurement. Our sample size is relatively small, and though it is sufficient to allow for examination of subgroups (ex: disease states, sex, age), we cannot control for confounding covariates. As larger scale studies will be required for confirmation of any findings described in this paper, we generally prioritize reduction in type II errors. We have selected a significance level of p<0.05 for all tests, and present p values without correction for multiple comparisons.
The Shapiro-Wilk W test [39] is used to test biomarkers for normality and assess which features required parametric or non-parametric tests. For paired data (lesion/contralateral, male/female), Welch’s paired t-test [40,41] is used for parametric features, and the Wilcoxon rank sum [42] for non-parametric features. Missing data is excluded in a pairwise fashion. To assess associations between the proposed metrics and disease status, the unpaired t-test [43] was used for parametric features and the Mann Whitney U test [44] for non-parametric features. Homogeneity of variances was assessed with Levene’s test [45], and the presence of outliers was assessed with Grubb’s test [46].
To reduce the effect of disease state, statistical analysis of demographic features and other pathologic conditions (acanthosis, keratosis, mucositis) was only performed on contralaterals. For assessment of biomarkers against sex and against other biological conditions, the unpaired t-test was used for parametric features and the Mann Whitney U test for non-parametric features. To assess associations between measurements and age, Spearman’s rank order [47] was used.
For future progression, we are only concerned with changes to the area of lesion. As such, we normalize each lesion to their respective contralateral by subtracting the median contralateral measurement from the median lesion measurement. Cases without a matched lesion and contralateral were excluded. Again, the unpaired t-test was used for parametric features and the Mann Whitney U test for non-parametric features.
Lastly, no statistical analysis was conducted on the longitudinal examinations, as there was no repetition of patients with the same disease state over multiple timepoints that met the inclusion criteria. Only qualitative assessments of trends are discussed for this experiment.
3. Results
3.1. Datasets and Demographics
Table 2 describes the demographic breakdown of the patients in this study to assess whether the proposed biomarkers can discriminate between lesion and contralateral and/or between disease state. We use ‘benign’ to describe lesions that are histopathologically confirmed as non-cancerous and non-dysplastic. To allow for sufficient sample size for each group, dysplasia grade 3 and carcinoma in situ are combined. Similarly, all carcinomas are described as one group; though there is one verrucous carcinoma, all others are squamous cell carcinoma. Contralateral images were taken from the opposite side of the tongue than the lesion whenever possible. However, as the patients in this study were recruited into a long-term monitoring group due to a history of or risk of oral cancers, we cannot assume the contralateral samples represent healthy normal tissue, only that they contained no clinically visible lesions.
The mean age of patients recruited in this study was 58 (29-92) years old. 17 patients were imaged with lesions on the lateral tongue and 23 with lesions on the ventral tongue. The benign lesions exhibited lichenoid mucositis (n=3) and hyperorthokeratosis (n=2). Hyperkeratosis was present in 19% of dysplastic cases, and hyperparakeratosis was present in 35%.
In some cases, contralateral and lesion data is not perfectly paired. 40 patients are included in this study (20 males, 20 females). There is one case included of a contralateral with no corresponding lesion site imaged and 9 lesions with no corresponding contralateral. A plurality of the lesions with no corresponding contralateral are carcinoma cases (n=4/9) as these were patients imaged at time of surgical intervention.
All mild and moderate dysplasias with contralaterals were included for assessment of future progression. Clinical status from time of imaging (2014/07 – 2017/06) to time of writing (2024/04) was reviewed. Patients diagnosed with a dysplasia grade 3, carcinoma in situ, or carcinoma during the follow-up time were considered ‘progressors’; patients without a lesion of a higher disease status were considered ‘non-progressors’ (Table 3). The average time from imaging to diagnosis for progressors was 45 months (22-60 months). At time of imaging, all progressors (n=4) presented with acanthosis, and hyperparakeratosis or hyperkeratosis. This was less consistently present in the non-progressors (n=14): acanthosis (6/14), hyperparakeratosis (4/14), hyperkeratosis (3/14), and hyperorthokeratosis (1/14).
To assess whether the proposed biomarkers can be measured repeatably and/or capture longitudinal changes, five patients (four male, one female) with lesions imaged at multiple timepoints met the inclusion criteria. They are described in Table 4. Dataset demographics for reproducibility / repeatability assessment. Table 4. This represented one patient for each diagnostic state. No patients underwent any surgical or clinical intervention between imaging timepoints. Patient 1 and 3 presented with hyperparakeratosis and acanthosis; patient 4 presented with hyperkeratosis.
3.2. Sample Imaging
We present sample imaging of each disease state reported in this work in Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8 and Figure 9. Each figure contains the measurements of the lesion (a) and contralateral (b). All scale bars are s1 mm, and all figures are presented with the same colourmap scaling for each feature. These are presented as (i) mean en face projection of OCT intensity; (ii) longitudinal section taken from the dashed line in (i); (iii) epithelial depth; (iv) overall attenuation coefficient; (v) epithelium attenuation coefficient; (vi) stroma attenuation coefficient; (vii) epithelial-stromal stratification; and (viii) intraepithelial stratification. Grey regions in panels (vi, vii) represent regions with a loss of epithelial-stromal boundary visualization. The black regions are masked out using the manual en face segmentations to remove areas of poor tissue contact or artifacts such as bubbles; no measurements were taken over these regions. The clinical view of the lesion is present in (c); while this photograph may have been taken after the application of toluidine blue, all OCT was collected prior to application of any contrast dyes. Box and whisker plots (box: upper and lower quartiles; bar: median; whiskers: maximum and minimum) are presented in (d) that summarize the quantitative measurements for all pixels in the area labelled ‘lesion’ in the volume and all pixels in the contralateral volume.
Benign lesion: Figure 3 is imaging of an 81-year-old male patient with a biopsy-confirmed acanthosis with no dysplasia on the left ventral tongue. The area of lesion as determined clinically is the entire length of the scan (purple arrows).
The longitudinal scan (Figure 3a(ii)) demonstrates the hallmarks of acanthosis: thickened and irregular epithelium. This is captured in the en face epithelial depth measurement, which is higher in the lesion (Figure 3a(iii)) than its contralateral (Figure 3b(iii)), with regions of extreme epithelial depth corresponding to a loss of epithelial-stromal boundary visualization which appears as grey regions in panels Figure 3a(vi, vii). The loss of epithelial-stromal boundary in the contralateral is only found at the edges of the volume and thus is likely due to ‘edge effects’. However, the epithelium in the contralateral also appears abnormal with some of the same features as the lesion: ripple-like changes in depth along the length of the scan, and small papillae extending from the epithelial-stromal boundary (white arrows) (Figure 3a,b(ii)).
The attenuation coefficient measurements are lower than their contralateral counterparts, and also lower than the dysplastic lesions presented in Figure 4a and Figure 5a. Regions of higher epithelial depth correspond to regions of decreased overall attenuation coefficient (Figure 3a(iv)) but regions of high epithelial attenuation coefficient (Figure 3a(v)). The stroma attenuation coefficient (Figure 3a(vi)) appears similarly to the overall attenuation coefficient (Figure 3a(iv)).
The epithelium attenuation coefficient Figure 3b(v) captures small pockmarks which are further emphasized in the intraepithelial stratification (Figure 3b(vii)), highlighted by the green arrows. These appear as small bright dots in the epithelium attenuation coefficient (Figure 3b(v)) and dark dots in the intraepithelial contrast (Figure 3b(viii)), indicating that they are changes derived from the lower epithelium. From the longitudinal scan (Figure 3b(ii)), this appears to map to the papillae (white arrows) extending from the epithelial-stromal boundary. These features are more apparent in the contralateral and left side of the lesion where the epithelium is thinner and flatter; they are overshadowed by larger spatial changes which correspond to areas of loss of epithelial-stromal boundary visualization.
Mild dysplasia: Figure 4 is imaging of a 47-year-old male patient with mild dysplasia, hyperparakeratosis, and acanthosis on the left ventral tongue. The boxed region in the center of the scan (purple arrows) shows where the clinically identified margins of the lesion were identified; however, examination of the proposed biomarkers indicates this may not include all the abnormal tissue and may not include the most pathologic regions. Two abnormal regions of epithelial depth (Figure 4a(iii)) are indicated with gold arrows and are outside the clinically selected region.
In the longitudinal OCT sections, the lesion volume (Figure 4a(iii)) has a deeper and more irregular epithelium than its contralateral (Figure 4b(iii)). The contralateral is extremely regular, with very few changes evident in the epithelial depth map. Examining the measurements in Figure 4d(i), the median lesion epithelial depth measurement is nearly double the contralateral and the depth varies more over the volume. There are several regions of extreme epithelial depth visible in the en face epithelial depth map (Figure 4a(iii)) which correspond to a loss of epithelial-stromal boundary visualization. Some of these regions may be artificially high due to edge effects, which appear to be more prominent in the lesion (perhaps due to surface texture impacting catheter contact) but are still present in the contralateral.
Areas with thicker epithelium have a lower overall attenuation coefficient (Figure 4(iv)), higher epithelium attenuation coefficient (Figure 4a(v)), and lower stroma attenuation coefficient (Figure 4a(vi)) where the stroma is still visualized. All attenuation coefficients are higher in this patient than in the patient with the benign lesion (Figure 3a). The overall and stroma attenuation coefficients are lower in the lesion than contralateral, but this relation is reversed in the epithelium.
The epithelial-stromal stratification (Figure 4a(vii)) is increased in the region with greater epithelial depth. There are also textural features in the epithelium attenuation coefficient of the lesion (Figure 4a (v)) which are emphasized in the epithelial-stromal stratification. These textural features are not present in the contralateral, which is regular throughout the volume. The epithelial-stromal stratification
The intraepithelial stratification is consistent across the length of the lesion (Figure 4a(viii)) and contralateral (Figure 4b(viii)). There are a few bright papillae extending from the epithelial-stromal boundary through the epithelium (white arrows, Figure 4a(ii)), but less than in the benign lesion and the pockmark pattern is not as prominent in either stratification metric (Figure 4a(vii, viii)).
Moderate dysplasia: Figure 5 is imaging of a 67-year-old male patient with moderate dysplasia, hyperorthokeratosis, and acanthosis on the left ventral tongue. As in the mild dysplastic case (Figure 4), the clinically selected area of lesion (purple arrows) does not encompass all the abnormal-appearing regions (gold arrows, Figure 5a). The hyperorthokeratosis (‘HOK’, white arrows) is visible in the longitudinal section (Figure 5a(ii)).
The epithelial depth measurements are qualitatively (Figure 5a(iii)) and quantitatively (Figure 5d(i)) similar to the mild dysplasia sample (Figure 4), with increased epithelial depth across the volume compared to their contralaterals and small regions of distinctly increased epithelial depth that correspond to loss of epithelial-stromal boundary visualization. In this patient, the contralateral epithelial depth (Figure 5b(iii)) is higher and contains more ‘edge effects’ than in the mild dysplasia case.
The epithelium attenuation coefficient (Figure 5a(v)) reveals potential margins that are not visible in the en face OCT (gold arrows). These regions have much higher epithelium attenuation coefficient than surrounding tissue or the contralateral. However, they also correspond with the regions of hyperorthokeratosis (‘HOK’) visible in the longitudinal section (Figure 5a(ii)). Hyperorthokeratosis will be included in the epithelial region mask, driving the measured attenuation coefficient up. This effect is especially visible in the region indicated by blue arrows where there is no hyperorthokeratosis, which appears as a dark circle compared to its surroundings in the epithelial attenuation coefficient and both stratification features.
The stratification features provide better visual discrimination of the regions indicated by gold arrows, although the margins differ slightly in Figure 5a(vii) and (viii). From the epithelial-stromal stratification (Figure 5a(vii)), we see that there is an increase in relative epithelial attenuation coefficient. From the intraepithelial stratification (Figure 5a(viii)), it is clear that this change is driven by an increase in the upper epithelium, which corresponds to the region we expect the hyperorthokeratosis to be present in. There are also some textural changes visible at the distal and proximal boundaries of the lesion volume.
There is an increase in epithelial depth (Figure 5a(iii)) at the right-hand side of the image, which does not have corresponding increases in epithelial attenuation coefficient or stratification measurements. This could be either due to an ‘edge effect’ at the end of the OCT acquisition, which could occur due to catheter positioning or movement. However, examining the longitudinal section it appears that this region does not present with the same hyperorthokeratosis, and this region may be an accurate representation of epithelial changes.
Severe dysplasia: Figure 6 is OCT collected of a 56-year-old male patient with severe dysplasia, hyperparakeratosis, and acanthosis on the left ventral tongue. In this case, the clinically selected area of lesion (purple arrows) encompasses the area of abnormality as identified by the proposed biomarkers (gold arrows, Figure 6a) but is less specific to the most abnormal region. Many of the features present similarly to the mild dysfplastic case (Figure 4a): deep epithelium, high attenuation coefficient, loss of epithelial-stromal boundary, and higher stratification in both the epithelial-stromal and intraepithelial biomarkers compared to their respective contralaterals. This case does not present with keratosis visible in the longitudinal scan (Figure 6a(ii)) or throughout the lesion in the same manner as Figure 5a.
An examination of the longitudinal scan (Figure 6a(ii)) shows that the epithelial-stromal boundary is indistinct in the region indicated by gold arrows. This is largely unsegmented by the deep learning network, resulting in most the area being classified as loss of epithelial-stromal boundary. An examination of the margins of the lesion shows epithelial depth increasing as it approaches the area with the loss of epithelial-stromal boundary visualization.
The epithelial-stromal stratification (Figure 6a(vii)) is darker and smoother on the left side of the volume, which is outside of the clinical boundaries for lesion. On the right-hand side of the lesion there are ripples and whorls (green arrows, Figure 6a(vii)), which appear as intensity changes and waves in the epithelial-stromal boundary in the longitudinal section (Figure 6a(ii))). These features are emphasized in the intraepithelial stratification (green arrows, Figure 6a(viii)), where smaller ripples appear more prominently. This is especially visible in the left-hand side of the contralateral (green arrows, Figure 6b(viii)), where there is substantial distortion of the epithelial-stromal boundary, papillae extending into the epithelium (white arrows), and bulb-shaped epithelial protrusions into the stroma. However, some sharp discontinuities in the imaging suggest there may be motion artifacts adding to this effect.
Carcinoma: Figure 7 is imaging from a 76-year-old female patient with a squamous cell carcinoma on the right ventral tongue. The clinically selected area of lesion (purple arrows) encompasses nearly the entire volume, which corresponds well with the areas of abnormality.
As visible in the longitudinal section (Figure 7a(ii)), there is no clear epithelial-stromal boundary throughout most of this volume. Therefore, the epithelial depth (Figure 7a(iii)) appears very deep, and no measurement can be made for most of the stroma attenuation coefficient (Figure 7a(vi)) and epithelial-stromal stratification (Figure 7a(vii)). The epithelial attenuation coefficient is high (Figure 7a(v)), as is the intraepithelial stratification (Figure 7a(viii)), indicating that the attenuation is increased at the surface.
In the contralateral (Figure 7b(ii)), we again see papillae extending from the epithelial-stromal boundary into the epithelium along the length of the volume (white arrows), though they appear more as dark bands rather than the bright (high scattering) features previously demonstrated. This leads to a ripple-like pattern (green arrows) in the intraepithelial stratification (Figure 7b(viii)) with wider peaks and troughs than the ripples in the severe dysplasia case.
3.3. Quantitative Assessment of Disease Status and Contralaterals
We present measurements of each feature for all volumes against disease status in Figure 8. A detailed breakdown is available in Supplementary Table S1. All quantitative measurements are calculated after masking out the edge effects as demonstrated in section 3.2 and assessed for statistical significance via the methods discussed in section 2.7. Using the Shapiro-Wilk W test, epithelium depth, loss of epithelial-stromal boundary, epithelium attenuation coefficient, and intraepithelial stratification were found to not have normal distributions and were treated as non-parametric features for this analysis.
Lesion vs. Contralateral: Using the paired statistical tests described in section 2.7, significant differences (p<0.05) were found between lesion and contralateral in moderate dysplasia, severe dysplasia, and carcinoma for epithelial depth, loss of epithelial-stromal boundary, epithelial attenuation coefficient, and epithelial-stromal stratification. Mild dysplasia and benign lesions appear most similar to their contralaterals and do not have significant differences in their median value, although they may be distinguished visually as demonstrated in section 3.2.
Morphologic features: The contralateral measurements are consistent across all disease states: the median epithelial depth (Figure 8(i)) of contralateral volumes is 160 μm and the mean loss of epithelial-stromal boundary visualization (Figure 8(ii)) is marginal (1%). Both features increase with increasing disease state, and there are statistical differences between carcinoma and all other disease states. Loss of epithelial-stromal boundary visualization appears to provide the best discrimination – in particular, carcinoma (mean 77%) appears entirely distinct from benign lesions (8%), mild (5%) or severe (15%) dysplasia. However, the benign and mild dysplastic lesions are similar. Epithelial depth follows a similar trend, although there is less separation between mean values.
Measurements of moderate dysplasia do not follow the trends of the other disease states. Moderate dysplasia has higher epithelial depth and greater loss of epithelial-stromal boundary visualization than severe dysplasia – although with the caveat of higher standard deviation. This also occurs in the epithelial attenuation coefficient and both stratification measurements. A closer examination of the n=10 moderate dysplasia cases does indicate that there is variability in epithelial appearance: in particular, there are n=2 cases which have a high percentage loss of epithelial-stromal boundary that appear more similar to carcinoma than dysplasia.
Attenuation coefficient features: These features have more overlap when compared to the morphologic features, and less consistency in the contralateral measurements across disease states in the overall and stroma attenuation coefficients. The median attenuation coefficient for all contralaterals is 3.45 mm-1 overall (Figure 8(iii)); 1.20 mm-1 epithelium (Figure 8(iv)); 3.97 mm-1 stroma (Figure 8(v)). While the epithelial attenuation coefficient tends to be lower than the stroma, it increases with disease status whereas the stroma attenuation coefficient decreases. The overall attenuation coefficient appears to be dominated by the stromal contribution.
Benign lesions have a statistically significant lower stroma attenuation coefficient (3.19 mm-1) than mild dysplastic lesions (4.35 mm-1), suggesting that this feature may be useful in discriminating occult from benign lesions. The epithelium attenuation coefficient displays similar discriminatory ability to the morphologic features, with significant differences between carcinoma and all other disease states. The stroma and overall attenuation coefficients have significant differences between mild dysplasia and benign, severe dysplasia, and carcinoma.
Stratification features: The epithelial-stromal stratification (Figure 8(vi)) is consistently negative as the stroma attenuation coefficient is consistently greater than that of the epithelium, but as the differentiation between the epithelium and stroma decreases with disease state this feature approaches zero. Aside from benign lesions, the contralateral is consistently lower than the lesion, representing a stronger contrast between epithelium and stroma as anticipated. There are significant differences between mild dysplasia and benign, severe dysplasia, and carcinoma for the overall and stroma attenuation coefficients.
In the intraepithelial stratification (Figure 8(vii)), there is a subtler trend. The intraepithelial stratification is again consistently negative, indicating that the epithelial attenuation is higher in the region closest to the epithelial-stromal boundary. As disease state increases, the measurement increases (becomes closer to zero), indicating that the epithelium becomes less stratified. There are only two significant differences: between carcinoma and benign, and carcinoma and severe dysplasia.
3.4. Demographic and Other Pathologic Associations
A complete table presenting these biomarkers divided by disease state and per sex is available in the Supplementary Materials in Table S2. There is a significant (p<0.05) difference between male (mean 180 µm) and female (mean 140 µm) epithelial depth.
There is a positive correlation (=0.47, p<0.001) between age and epithelium attenuation coefficient. Breaking this down per sex, there are no significant correlations between age and any biomarker for males, but there are two positive correlations between age and epithelium attenuation coefficient (=0.52, p<0.05) and age and epithelial-stromal stratification (=0.59, p<0.05) for females.
Due to sample size limitations (n=2 lichenoid mucositis, n=2 hyperorthokeratosis), we were limited in our ability to assess the other pathologic conditions described in section 3.1. No statistical difference was found in contralaterals with or without acanthosis, or between contralaterals with or without keratosis (inclusive of hyperkeratosis, hyperorthokeratosis, or hyperparakeratosis). Detailed results are presented in the Supplementary Materials in Table S3.
3.5. Future Progression
To examine whether the proposed biomarkers can distinguish future progressors within the mild and moderate dysplasia groups, we present the measurements of each volume normalized to their respective contralaterals in Figure 9. Further details are presented in the Supplementary Materials in Table S4.
There are more non-progressors than progressors, and the standard deviation in non-progressors is higher in all measurements. The best separation (p<0.05) is in the stroma and overall attenuation coefficients (Figure 9(iii)), where the progressors are higher than their respective contralaterals compared to the non-progressors which are lower than their respective contralaterals. In both lesion and contralateral, these are higher in the non-progressors for overall (3.45/3.32 mm-1 lesion/contralateral progressors to 3.60/3.81 mm-1 non-progressors) and stroma attenuation coefficient (4.04/3.77 mm-1 progressors to 4.35/4.47 mm-1 non-progressors).
In general, progressors present with a lower (though not significant) difference in epithelial depth compared to their contralaterals (Figure 9(i)), more loss of epithelial-stromal boundary (Figure 9(ii)), and less change in epithelial-stromal stratification (Figure 9(iv)). The epithelium attenuation coefficient and intraepithelial stratification are both very similar between progressors and non-progressors (Figure 9(iii)).
3.6. Reproducibility & Repeatability
Next, we explore whether the proposed biomarkers can be measured repeatably and/or capture longitudinal changes in Table 5 with the five patients who were imaged at multiple timepoints. We present contralateral measurements over the two timepoints to assess long-term reproducibility. We present repeated measurements (single timepoint) of lesions to assess short-term repeatability.
All five patients had contralaterals imaged over both timepoints. For almost all cases, the mean contralateral measurements are within the ranges presented in Figure 8 and Tables S1 and S2. The average difference normalized to the mean measurement of each feature for all five patients is: 20% epithelial depth; 30% loss of epithelial-stromal boundary visualization; 15% attenuation coefficient; 10% epithelium attenuation coefficient; 20% stroma attenuation coefficient; 6% epithelial-stromal stratification; 27% intra-epithelial stratification. This indicates that the morphologic masks are the least repeatable between timepoints. This is somewhat expected: as several months passed between imaging timepoints, the contralateral site imaged may not be at the same location.
Two patients had lesions that were imaged repeatedly at a single timepoint: a mild dysplasia (patient 1) and a moderate dysplasia (patient 2). These demonstrate good repeatability of measurement within a single timepoint: they represent taking an image, removing, and readjusting the imaging catheter on the lesion, and taking another image. The average difference normalized to the mean measurement of each feature for these patients is: 16% epithelial depth; 77% loss of epithelial-stromal boundary visualization; 3% attenuation coefficient; 20% epithelium attenuation coefficient; 1% stroma attenuation coefficient; 14% epithelial-stromal stratification; 11% intraepithelial stratification. These results are slightly more consistent than the longitudinal contralateral experiment, but there is still some variation in measurement which may be due to heterogeneity of the lesion and positioning of the imaging catheter.
4. Discussion
4.1. Dataset Limitations
This work is a retrospective analysis, and as such, there are some limitations in the dataset size, composition, and image collection approach. To improve sample size, we have grouped together site and pathologic groups which may merit independent study. This work combines imaging of the lateral (n=16) and ventral (n=23) tongue. We have grouped together benign lesions as any lesion with a biopsy-confirmed non-dysplastic diagnosis. And while 24/39 lesions presented with some combination of candidiasis, lichenoid mucositis, keratosis and/or acanthosis, due to sample size limitations we were only able to analyze the imaging features against presence or absence of acanthosis and keratosis.
Our findings are limited to the co-registered labels of lesion area within each volume. The identified clinical margins are reliant on the 1 cm sheath markers and estimation of lesion size and may not be precisely co-registered. Some of the sample imaging demonstrated such as Figure 4 indicate that the selected margins may be wider than (or may not overlap with) areas of abnormality as visualized by the proposed measurements. As we selected the median value of each measurement over the clinically selected margins as our primary quantitative metric, the inclusion of areas of less- or non-pathologic tissue may have reduced differences between the lesion and contralateral. Additionally, due to the heterogeneous nature of oral cancer, we may have imaged a region that included higher or lower grade lesion than the biopsy results which may have resulted in some drift between disease states.
4.2. Morphologic Measurements
Epithelial depth and changes in the visualization of stratification have previously been described in oral OCT literature [17,28,31]. The increase of epithelial depth and irregular epithelial stratification are a well-documented histopathologic hallmark of dysplastic progression to carcinoma [4]. This work represents the first measurement of these features in an endoscopic OCT system. Previously, the healthy ventral tongue is reported to be measured with OCT as 240 µm (160-320 µm) for 28 healthy volunteers with a mean age of 36 years [29], which is higher but comparable to our findings of 160 µm (120-260 µm) of contralaterals from patients undergoing monitoring for oral lesions with a mean age of 58 years.
Our measurements are limited by the approach taken in the previously developed deep learning segmentation pipeline [34]. A substantial limitation is poor labelling of keratosis: as these regions are labelled as epithelium, this results in increased epithelium depth as well as subsequent changes in the attenuation coefficient and stratification measurements. Additionally, we have rescaled pixels assuming all values are travelling through a medium with the index of refraction of water: this assumption may not hold in all cases. If the index of refraction is over- or under-estimated, the rescaled pixels will no longer be 10 µm which will skew the measurement of epithelial depth.
A major caveat of this work is our methods for regions where the stroma surface is not segmented. In our approach, regions with a loss of epithelial-stromal boundary visualization are labelled such that the epithelial mask contains the entire depth of visualized tissue. The underlying assumption we are making is that the epithelial-stromal boundary is now beyond the viewing range of our system. Previous work has shown that cancer-involved margins have a mean epithelial depth on the order of 580 µm (130-900 µm) [20], which would often be beyond our maximum visualized depth (~750 µm in carcinoma, though varies with attenuation coefficient) – and even if it is within the visualized depth, the contrast lessens deeper into the A-line which may limit the ability to distinguish tissue layers.
The result of this assumption is a higher than usual epithelium depth measurement in regions with a loss of a visualized epithelial-stromal boundary. This also impacts other features as well: the epithelium attenuation coefficient will be taken over a larger region, and the intraepithelial stratification may not represent the ‘upper’ and ‘lower’ regions well. However, using epithelium measurements only over regions of good epithelial-stromal boundary visualization substantially limits the utility of the proposed technique: excluding regions with a loss of epithelial-stromal boundary will exclude the most pathologic regions in cases of disease. In sum, we recommend the reader interpret the measurements presented in this work carefully, particularly those in carcinoma where there is a high loss of epithelial-stromal boundary visualization.
4.3. Attenuation Coefficient Measurements
In this study we are unable to retrospectively characterize and compensate for the confocal effects of each optical catheter, and so we caution that our attenuation coefficient results may not be generalizable to other applications. However, as lesions and contralateral were imaged at the same time we are confident that our findings are not obscured by differences between catheters, and there were only four unique catheters used to collect the data presented in this study. Previous work in our group has found that the effects are minimal in regions with attenuations of 2-3 mm-1 throughout our imaging range; however, findings in this study for stroma attenuation coefficient are beyond that range and may be unreliable. In addition, given that each imaging catheter will have a slightly different working distance they will illuminate a different amount of the stroma which may further impact the stroma measurements.
We are the first group to present depth-resolved and distinct measurements for epithelium and stroma attenuation coefficient. An optical attenuation model has been previously suggested for oral cancer identification in a study of fresh ex vivo surgical samples from 14 oral cancer patients [33], where the average attenuation of squamous cell carcinoma was found to be 3.11 mm-1 and non-cancer margins 5.65 mm-1. This is comparable in trend to our overall attenuation coefficient measurements of 3.05 mm-1 in carcinoma, although our contralateral measurements are lower (3.27 mm-1).
4.4. Stratification Measurements
We anticipated that this feature would capture a decrease in stratification throughout disease progression, as often it becomes more challenging for an expert rater to distinguish epithelium and stroma. Instead, this appears to capture small connective tissue papillae (white arrows, Figure 3a(ii)) in the lower epithelium which may be related to rete ridges or pegs, though co-registered histopathology is required to confirm this. This appears as small frequency ripples or pockmarks in healthy flat tissue but is dominated by larger changes in regions with high variability of epithelium depth. We believe these stratification measurements are promising, but perhaps would be better interpreted with texture analysis features rather than median intensity values.
4.4. Future Progression
Changes in stroma attenuation distinguishing progressors and non-progressors may point to differences in immune infiltration and/or the extracellular matrix across the lesion and contralateral in these two groups. Optical attenuation at 1310 nm has been shown to correlate positively with collagen content in ovarian tissue [48], so an increased stroma attenuation coefficient may point to collagen remodeling in progressors.
While these results are intriguing, this experiment is substantially limited by sample size, with only four patients identified as future progressors with a mean of 45 months from time of imaging to progression. While biopsy results are of the same lesion, we cannot be assured that they were from the same part of the lesion. We may have imaged an area of higher-grade lesion than the biopsy results at time of imaging which could have resulted in cases being falsely labelled as ‘future progressors’. Further study with a larger sample size and correction for the confocal effect are required to understand this phenomenon.
4.5. Future Directions
Larger scale studies are required to confirm the relationship of these measurements to disease status, to develop diagnostic criteria, to understand demographic and other pathologic confounders, and to generalize these findings to other patient cohorts.
While this work focuses on endoscopic OCT, the measurements presented can be translated to galvanometer scanning approaches. The deep learning network is likely not generalizable beyond our endoscopic systems, but similar approaches could be taken to tailor an automated segmentation tool for other OCT devices. With a sufficient segmentation tool (or even with manual segmentation on select OCT frames), the same features could be calculated and examined.
If such a tool is to be used during clinical monitoring, rapid access to these measurements is required. The current analysis of whole-volume OCT through this approach is time intensive; however, this is largely due to visualizing and saving data (longitudinal tiles, masks, etc.) throughout the process. With the device specifications described in the methods (section 2.4), for a 5 cm long pullback (1024x512x5000 pixels before rescaling to 10 µm square pixels), the deep learning network predictions can be generated in 2.5 minutes, and once the masks are generated all measurements can be calculated in 10 minutes. This may be improved via implementation in a language that is faster than MATLAB / Python such as C++.
5. Conclusions
We present quantitative image processing analysis of endoscopic OCT of the oral cavity. This is a hypothesis-generating study intended to provide future direction for diagnostic criteria in oral OCT measurement: it is limited as a single-facility study with a small sample size examining many properties. While we have presented statistically significant findings, we note that we have not corrected for multiple comparisons and thus larger studies are required to confirm these findings.
To briefly summarize, we demonstrate seven quantitative measurements of oral tissue (lateral or ventral tongue) in 40 patients with varying disease state using an endoscopic OCT catheter. These measurements are inclusive of morphology (epithelial depth, loss of epithelial-stromal boundary visualization), mean attenuation coefficients (overall, epithelium, stroma), and stratification of the attenuation coefficients (epithelial-stromal, intraepithelial stratification).
We demonstrate the potential of these measurements to visually distinguish lesion margins, quantitatively differentiate lesion from contralateral, and quantitatively distinguish some disease states. Median epithelial depth and loss of epithelial-stromal boundary visualization increase with disease state. While the epithelium attenuation coefficient increases with disease state, stromal attenuation coefficient decreases and dominates the measured overall attenuation coefficient. Both stratification features become closer to zero (lower contrast) as disease state increases. These changes can be visualized within each volume, although there are confounders such as keratosis which may appear similar to areas of lesion.
In this dataset, median epithelial depth of female contralaterals is lower than that of male patients. There are additionally some suggestive positive correlations between age and epithelial attenuation coefficient. There was no significant difference due to presence of acanthosis or keratosis.
The overall and stroma attenuation coefficient demonstrate potential in distinguishing future progressors within the mild and moderate dysplasia groups. However, the sample size was substantially limited, and additional study is needed to draw conclusions about this effect.
Lastly, we present two cases of repeatable measurements within one timepoint, and five patients capturing some measured change over two timepoints, indicating that these tools may be able to capture longitudinal changes. As OCT is a label-free, non-ionizing imaging technique, this points to the potential for monitoring via imaging.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table S1. Measurements of each feature per disease state. Table S2. Mean measurements of each feature per disease state and sex. Table S3. Measurements of other pathologic results in contralaterals. Table S4. Measurements against future progression status for mild and moderate dysplastic lesions.
Author Contributions
Conceptualization, JM, PML, CFP; methodology, JM; image collection, CP, SN and KL; software, JM, CH, AST, PML; validation, JM; formal analysis, JM; investigation, JM; resources, CP, CM and PL; data curation, JM, KL, CP, SN, PML; writing—original draft preparation, JM.; writing—review and editing, all authors; visualization, JM, CH; supervision, CM and PL; project administration, JM; funding acquisition, CM, CP and PL. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by a Collaborative Health Research Projects grant (462490-2014) from the Canadian Institutes of Health Research (CIHR) and Natural Sciences and Engineering Research Council of Canada (NSERC). The analysis work was supported by Discovery Grant funding from the Natural Sciences and Engineering Research Council of Canada (RGPIN-2023-05592). JM acknowledges fellowship support from the University of British Columbia, the Mitacs Accelerate program, and the British Columbia Cancer Foundation. CH acknowledges scholarship support from NSERC and Simon Fraser University.
Institutional Review Board Statement
This study was approved by the Institutional Review Boards of the British Columbia Cancer Agency and the University of British Columbia (Approval number: H11-002516).
Informed Consent Statement
Volunteers were recruited from the Vancouver General Hospital (VGH) Innovative Approach to Triage of Oral Precancers (iTOP) Clinic and provided informed written consent.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank: Dr. Donald Anderson, Tony Han, Alisa Kami, and Grace Manaog for clinical assistance; Lucas Cahill, Rashika Raizada, Geoffrey Hohert, Sylvia Lam and Dr. Anthony Lee for support in OCT acquisition; Eric Brace, Kimiya Mousavi and Shahed Ejadi for OCT review; Ian Janzen and Allan Zuckermann Cynamon for software support.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians 2021, 0, 1–41. [Google Scholar] [CrossRef]
- Neville, B.W.; Day, T.A. Oral Cancer and Precancerous Lesions. CA: A Cancer Journal for Clinicians 2002, 52, 195–215. [Google Scholar] [CrossRef]
- Almangush, A.; Mäkitie, A.A.; Triantafyllou, A.; De Bree, R.; Strojan, P.; Rinaldo, A.; Hernandez-Prera, J.C.; Suárez, C.; Kowalski, L.P.; Ferlito, A.; et al. Staging and Grading of Oral Squamous Cell Carcinoma: An Update. Oral Oncology 2020, 107, 104799. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, K.; Kavitha, L. Oral Epithelial Dysplasia: Classifications and Clinical Relevance in Risk Assessment of Oral Potentially Malignant Disorders. Journal of Oral and Maxillofacial Pathology: JOMFP 2019, 23, 19. [Google Scholar] [CrossRef] [PubMed]
- Poh, C.F. Biopsy and Histopathologic Diagnosis of Oral Premalignant and Malignant Lesions. 2008, 74.
- Yang, G.; Wei, L.; Thong, B.K.S.; Fu, Y.; Cheong, I.H.; Kozlakidis, Z.; Li, X.; Wang, H.; Li, X. A Systematic Review of Oral Biopsies, Sample Types, and Detection Techniques Applied in Relation to Oral Cancer Detection. BioTech 2022, 11, 5. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.Á.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral Potentially Malignant Disorders: A Consensus Report from an International Seminar on Nomenclature and Classification, Convened by the WHO Collaborating Centre for Oral Cancer. Oral Diseases 2021, 27, 1862–1880. [Google Scholar] [CrossRef] [PubMed]
- Mohamad, I.; Glaun, M.D.E.; Prabhash, K.; Busheri, A.; Lai, S.Y.; Noronha, V.; Hosni, A. Current Treatment Strategies and Risk Stratification for Oral Carcinoma. American Society of Clinical Oncology Educational Book 2023, e389810. [Google Scholar] [CrossRef]
- Fujimoto, J.G.; Drexler, W. Introduction to OCT; 2015; ISBN 978-3-319-06419-2.
- Drexler, W.; Chen, Y.; Aguirre, A.D.; Považay, B.; Unterhuber, A.; Fujimoto, J.G. Ultrahigh Resolution Optical Coherence Tomography. In Optical Coherence Tomography; Drexler, W., Fujimoto, J.G., Eds.; Springer International Publishing: Cham, 2015; pp. 277–318. ISBN 978-3-319-06418-5. [Google Scholar]
- Gora, M.J.; Suter, M.J.; Tearney, G.J.; Li, X. Endoscopic Optical Coherence Tomography: Technologies and Clinical Applications. Biomedical Optics Express 2017, 8, 2405. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Fujimoto, J.G.; Tsai, T.-H.; Mashimo, H. Endoscopic OCT. In Optical Coherence Tomography: Technology and Applications, Second Edition; 2015; pp. 2077–2108 ISBN 978-3-319-06419-2.
- van Manen, L.; Dijkstra, J.; Boccara, C.; Benoit, E.; Vahrmeijer, A.L.; Gora, M.J.; Mieog, J.S.D. The Clinical Usefulness of Optical Coherence Tomography during Cancer Interventions. Journal of Cancer Research and Clinical Oncology 2018, 144, 1967–1990. [Google Scholar] [CrossRef]
- Pahlevaninezhad, H.; Lee, A.M.D.; Rosin, M.; Sun, I.; Zhang, L.; Hakimi, M.; MacAulay, C.; Lane, P.M. Optical Coherence Tomography and Autofluorescence Imaging of Human Tonsil. PLoS ONE 2014, 9, 1–11. [Google Scholar] [CrossRef]
- Vermeer, K.A.; Mo, J.; Weda, J.J.A.; Lemij, H.G.; Boer, J.F. de Depth-Resolved Model-Based Reconstruction of Attenuation Coefficients in Optical Coherence Tomography. Biomedical Optics Express 2013, 5, 322–337. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Kim, S.W.; Hwang, S.H. Efficacy of Optical Coherence Tomography in the Diagnosing of Oral Cancerous Lesion: Systematic Review and Meta-analysis. Head & Neck 2023, 45, 473–481. [Google Scholar] [CrossRef]
- Yang, C.C.; Tsai, M.-T.; Lee, H.-C.; Lee, C.-K.; Yu, C.-H.; Chen, H.-M.; Chiang, C.-P.; Chang, C.-C.; Wang, Y.-M.; Yang, C.C. Effective Indicators for Diagnosis of Oral Cancer Using Optical Coherence Tomography. Opt. Express 2008, 16, 15847. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-K.; Chi, T.-T.; Wu, C.-T.; Tsai, M.-T.; Chiang, C.-P.; Yang, C.-C. (C. C.) Diagnosis of Oral Precancer with Optical Coherence Tomography. Biomed. Opt. Express 2012, 3, 1632. [Google Scholar] [CrossRef] [PubMed]
- Hamdoon, Z.; Jerjes, W.; Upile, T.; McKenzie, G.; Jay, A.; Hopper, C. Optical Coherence Tomography in the Assessment of Suspicious Oral Lesions: An Immediate Ex Vivo Study. Photodiagnosis and Photodynamic Therapy 2013, 10, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Jerjes, W.; Hamdoon, Z.; Yousif, A.A.; Al-Rawi, N.H.; Hopper, C. Epithelial Tissue Thickness Improves Optical Coherence Tomography’s Ability in Detecting Oral Cancer. Photodiagnosis and Photodynamic Therapy 2019, 28, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Obade, A.Y.; Pandarathodiyil, A.K.; Oo, A.L.; Warnakulasuriya, S.; Ramanathan, A. Application of Optical Coherence Tomography to Study the Structural Features of Oral Mucosa in Biopsy Tissues of Oral Dysplasia and Carcinomas. Clin Oral Invest 2021, 25, 5411–5419. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Shang, J.; Liu, C.; Zhang, J.; Liang, Y. Identification of Oral Precancerous and Cancerous Tissue by Swept Source Optical Coherence Tomography. Lasers Surg Med 2022, 54, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Cheng, L.; Yang, J.; Yin, B.; Fan, X.; Yang, J.; Li, S.; Zhong, J.; Huang, X. Noninvasive Oral Cancer Screening Based on Local Residual Adaptation Network Using Optical Coherence Tomography. Med Biol Eng Comput 2022, 60, 1363–1375. [Google Scholar] [CrossRef]
- James, B.L.; Sunny, S.P.; Heidari, A.E.; Ramanjinappa, R.D.; Lam, T.; Tran, A.V.; Kankanala, S.; Sil, S.; Tiwari, V.; Patrick, S.; et al. Validation of a Point-of-Care Optical Coherence Tomography Device with Machine Learning Algorithm for Detection of Oral Potentially Malignant and Malignant Lesions. Cancers 2021, 13, 3583. [Google Scholar] [CrossRef]
- Heidari, A.E.; Suresh, A.; Kuriakose, M.A.; Chen, Z.; Wilder-Smith, P.; Sunny, S.P.; James, B.L.; Lam, T.M.; Tran, A.V.; Yu, J.; et al. Optical Coherence Tomography as an Oral Cancer Screening Adjunct in a Low Resource Settings. IEEE J. Select. Topics Quantum Electron. 2019, 25, 1–8. [Google Scholar] [CrossRef]
- Wilder-Smith, P.; Jung, W.; Brenner, M.; Osann, K.; Beydoun, H.; Messadi, D.; Chen, Z. In Vivo Optical Coherence Tomography for the Diagnosis of Oral Malignancy. Lasers Surg Med 2004, 35, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Sunny, S.P.; Agarwal, S.; James, B.L.; Heidari, E.; Muralidharan, A.; Yadav, V.; Pillai, V.; Shetty, V.; Chen, Z.; Hedne, N.; et al. Intra-Operative Point-of-Procedure Delineation of Oral Cancer Margins Using Optical Coherence Tomography. Oral Oncology 2019, 92, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Panzarella, V.; Buttacavoli, F.; Gambino, A.; Capocasale, G.; Di Fede, O.; Mauceri, R.; Rodolico, V.; Campisi, G. Site-Coded Oral Squamous Cell Carcinoma Evaluation by Optical Coherence Tomography (OCT): A Descriptive Pilot Study. Cancers 2022, 14, 5916. [Google Scholar] [CrossRef] [PubMed]
- Stasio; Lauritano; Iquebal; Romano; Gentile; Lucchese Measurement of Oral Epithelial Thickness by Optical Coherence Tomography. Diagnostics 2019, 9, 90. [CrossRef]
- Lee, A.M.D.; Cahill, L.; Liu, K.; MacAulay, C.; Poh, C.; Lane, P. Wide-Field in Vivo Oral OCT Imaging. Biomedical Optics Express 2015, 6, 2664. [Google Scholar] [CrossRef] [PubMed]
- Gambino, A.; Martina, E.; Panzarella, V.; Ruggiero, T.; Haddad, G.E.; Broccoletti, R.; Arduino, P.G. Potential Use of Optical Coherence Tomography in Oral Potentially Malignant Disorders: In-Vivo Case Series Study. BMC Oral Health 2023, 23, 540. [Google Scholar] [CrossRef]
- Trebing, C.T.; Sen, S.; Rues, S.; Herpel, C.; Schöllhorn, M.; Lux, C.J.; Rammelsberg, P.; Schwindling, F.S. Non-Invasive Three-Dimensional Thickness Analysis of Oral Epithelium Based on Optical Coherence Tomography—Development and Diagnostic Performance. Heliyon 2021, 7, e06645. [Google Scholar] [CrossRef]
- Yang, Z.; Shang, J.; Liu, C.; Zhang, J.; Liang, Y. Identification of Oral Cancer in OCT Images Based on an Optical Attenuation Model. Lasers Med Sci 2020, 35, 1999–2007. [Google Scholar] [CrossRef]
- Hill, C.; Malone, J.; Liu, K.; Ng, S.P.-Y.; MacAulay, C.; Poh, C.; Lane, P. 3-Dimension Epithelial Segmentation in Optical Coherence Tomography of the Oral Cavity Using Deep Learning 2024.
- Chen, S.-W.; Zhang, Q.; Guo, Z.-M.; Chen, W.-K.; Liu, W.-W.; Chen, Y.-F.; Li, Q.-L.; Liu, X.-K.; Li, H.; Ou-Yang, D.; et al. Trends in Clinical Features and Survival of Oral Cavity Cancer: Fifty Years of Experience with 3,362 Consecutive Cases from a Single Institution. CMAR 2018, Volume 10, 4523–4535. [Google Scholar] [CrossRef]
- Lin, N.-C.; Hsien, S.-I.; Hsu, J.-T.; Chen, M.Y.C. Impact on Patients with Oral Squamous Cell Carcinoma in Different Anatomical Subsites: A Single-Center Study in Taiwan. Sci Rep 2021, 11, 15446. [Google Scholar] [CrossRef] [PubMed]
- Pahlevaninezhad, H.; Lee, A.; Cahill, L.; Lam, S.; MacAulay, C.; Lane, P. Fiber-Based Polarization Diversity Detection for Polarization-Sensitive Optical Coherence Tomography. Optics Letters 2014, 1, 283–295. [Google Scholar] [CrossRef]
- Liu, J.; Ding, N.; Yu, Y.; Yuan, X.; Luo, S.; Luan, J.; Zhao, Y.; Wang, Y.; Ma, Z. Optimized Depth-Resolved Estimation to Measure Optical Attenuation Coefficients from Optical Coherence Tomography and Its Application in Cerebral Damage Determination. J. Biomed. Opt. 2019, 24, 1. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591. [Google Scholar] [CrossRef]
- Zimmerman, D.W. A Note on Preliminary Tests of Equality of Variances. Brit J Math & Statis 2004, 57, 173–181. [Google Scholar] [CrossRef]
- Welch, B.L. THE GENERALIZATION OF ‘STUDENT’S’ PROBLEM WHEN SEVERAL DIFFERENT POPULATION VARLANCES ARE INVOLVED. Biometrika 1947, 34, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Wilcoxon, F. Individual Comparisons by Ranking Methods. Biometrics Bulletin 1945, 1, 80–83. [Google Scholar] [CrossRef]
- Student The Probable Error of a Mean. Biometrika 1908, 6, 1. [CrossRef]
- Mann, H.B.; Whitney, D.R. On a Test of Whether One of Two Random Variables Is Stochastically Larger than the Other. Ann. Math. Statist. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Levene, H. Robust Tests for Equality of Variances. In Contributions to Probability and Statistics: Essays in Honor of Harold Hotelling; Stanford University Press: Palo Alto, Calif, 1960; pp. 278–292. [Google Scholar]
- Grubbs, F.E. Procedures for Detecting Outlying Observations in Samples. Technometrics 1969, 11, 1–21. [Google Scholar] [CrossRef]
- Spearman, C. The Proof and Measurement of Association between Two Things. The American Journal of Psychology 1904, 15, 72. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, T.; Biswal, N.C.; Wang, X.; Sanders, M.; Brewer, M.; Zhu, Q. Optical Scattering Coefficient Estimated by Optical Coherence Tomography Correlates with Collagen Content in Ovarian Tissue. Journal of Biomedical Optics 2011, 16, 090504. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
OCT orientation and sample imaging. (a) Endoscopic OCT results in a cylindrical volume as shown on the left. When imaging a non-luminal organ, a portion of the imaging field contains no tissue (right). (b) Image collection is conducted using a dental mirror or saliva ejector to lay the imaging catheter across the surface of the lesion; (c) OCT of a squamous cell carcinoma; panel (i) demonstrates a mean en face projection and panel (ii) demonstrates a longitudinal slice taken from the dashed line shown in (i). There are many bubbles (‘b’) present in this volume and sheath markers (‘m’). (d) OCT of a benign lesion presented in the same orientation as (c). This volume also demonstrates sheath markers (‘m’) as well an artifact where tissue is completely obscured (‘a’). In the longitudinal panels (ii), the epithelium is the first dark line in the tissue ‘E’ and the stroma is the first bright region ‘S’. The basement membrane itself is not resolvable, but the transition between these two regions (‘epithelial-stromal boundary’) is as denoted by the dashed lines. Scale bars 1 mm.
Figure 1.
OCT orientation and sample imaging. (a) Endoscopic OCT results in a cylindrical volume as shown on the left. When imaging a non-luminal organ, a portion of the imaging field contains no tissue (right). (b) Image collection is conducted using a dental mirror or saliva ejector to lay the imaging catheter across the surface of the lesion; (c) OCT of a squamous cell carcinoma; panel (i) demonstrates a mean en face projection and panel (ii) demonstrates a longitudinal slice taken from the dashed line shown in (i). There are many bubbles (‘b’) present in this volume and sheath markers (‘m’). (d) OCT of a benign lesion presented in the same orientation as (c). This volume also demonstrates sheath markers (‘m’) as well an artifact where tissue is completely obscured (‘a’). In the longitudinal panels (ii), the epithelium is the first dark line in the tissue ‘E’ and the stroma is the first bright region ‘S’. The basement membrane itself is not resolvable, but the transition between these two regions (‘epithelial-stromal boundary’) is as denoted by the dashed lines. Scale bars 1 mm.
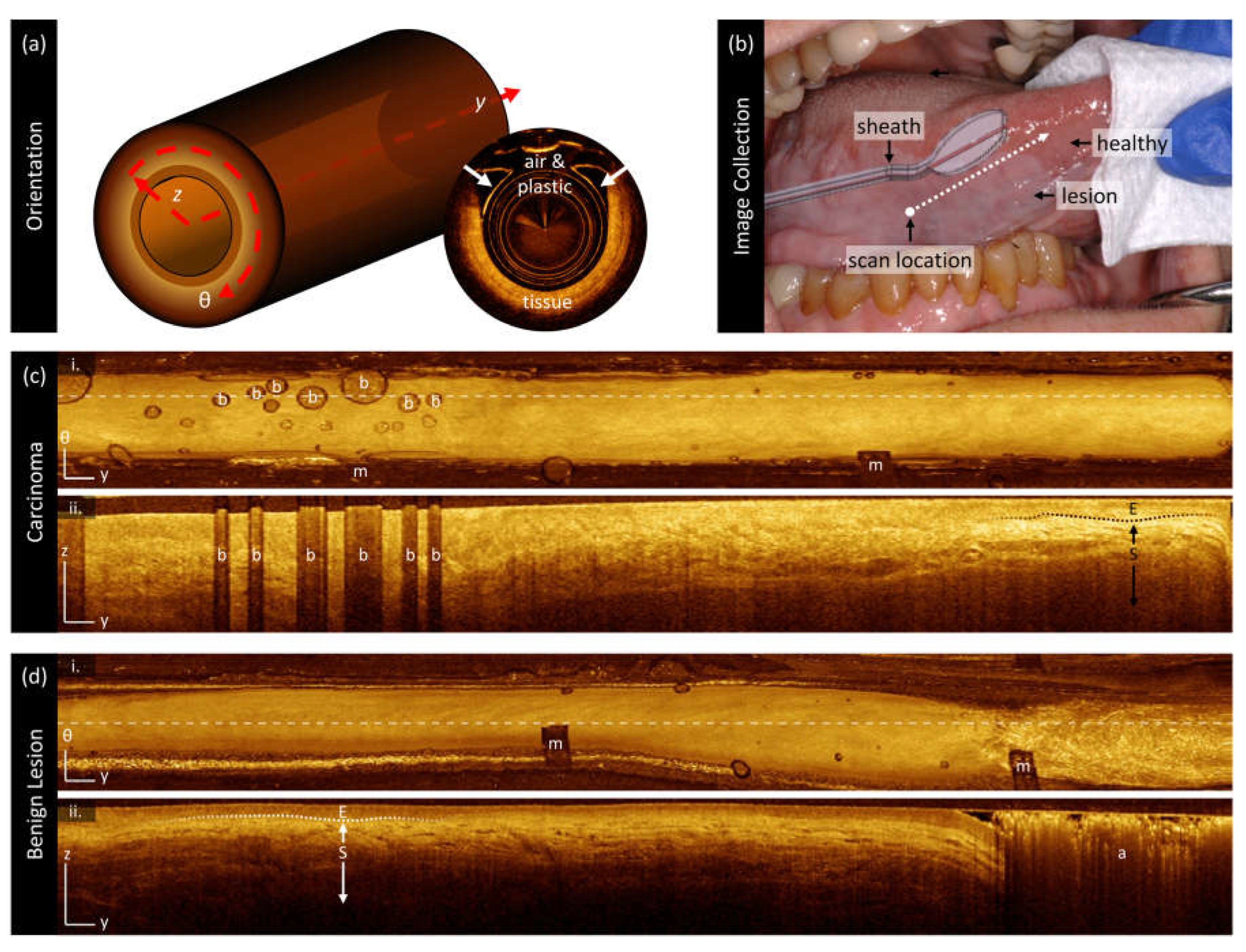
Figure 2.
Biomarker calculation on a longitudinal slice. (i) OCT mean en face projection. (ii) Longitudinal section taken from the dashed line. This sample contains hyperparakeratosis (‘HPK’) which is visualized as a bright layer near the tissue surface on the left-hand side of this scan. The epithelium (‘E’) is darker and present below the hyperparakeratosis on the left. (iii) Longitudinal section overlaid with the segmented regions of epithelium (‘E’) and stroma (‘S’). The epithelial-stromal boundary is illustrated by the blue line. There is a region with loss of epithelial-stromal boundary detection (‘*’) where the entire visualized depth is taken to be epithelium. (iv) Longitudinal section overlaid with the intraepithelial regions: upper epithelium (‘UE’) and lower epithelium (‘LE’). (v) The depth-resolved attenuation coefficient for this frame. The attenuation coefficient of the epithelium is high in the region containing hyperparakeratosis.
Figure 2.
Biomarker calculation on a longitudinal slice. (i) OCT mean en face projection. (ii) Longitudinal section taken from the dashed line. This sample contains hyperparakeratosis (‘HPK’) which is visualized as a bright layer near the tissue surface on the left-hand side of this scan. The epithelium (‘E’) is darker and present below the hyperparakeratosis on the left. (iii) Longitudinal section overlaid with the segmented regions of epithelium (‘E’) and stroma (‘S’). The epithelial-stromal boundary is illustrated by the blue line. There is a region with loss of epithelial-stromal boundary detection (‘*’) where the entire visualized depth is taken to be epithelium. (iv) Longitudinal section overlaid with the intraepithelial regions: upper epithelium (‘UE’) and lower epithelium (‘LE’). (v) The depth-resolved attenuation coefficient for this frame. The attenuation coefficient of the epithelium is high in the region containing hyperparakeratosis.
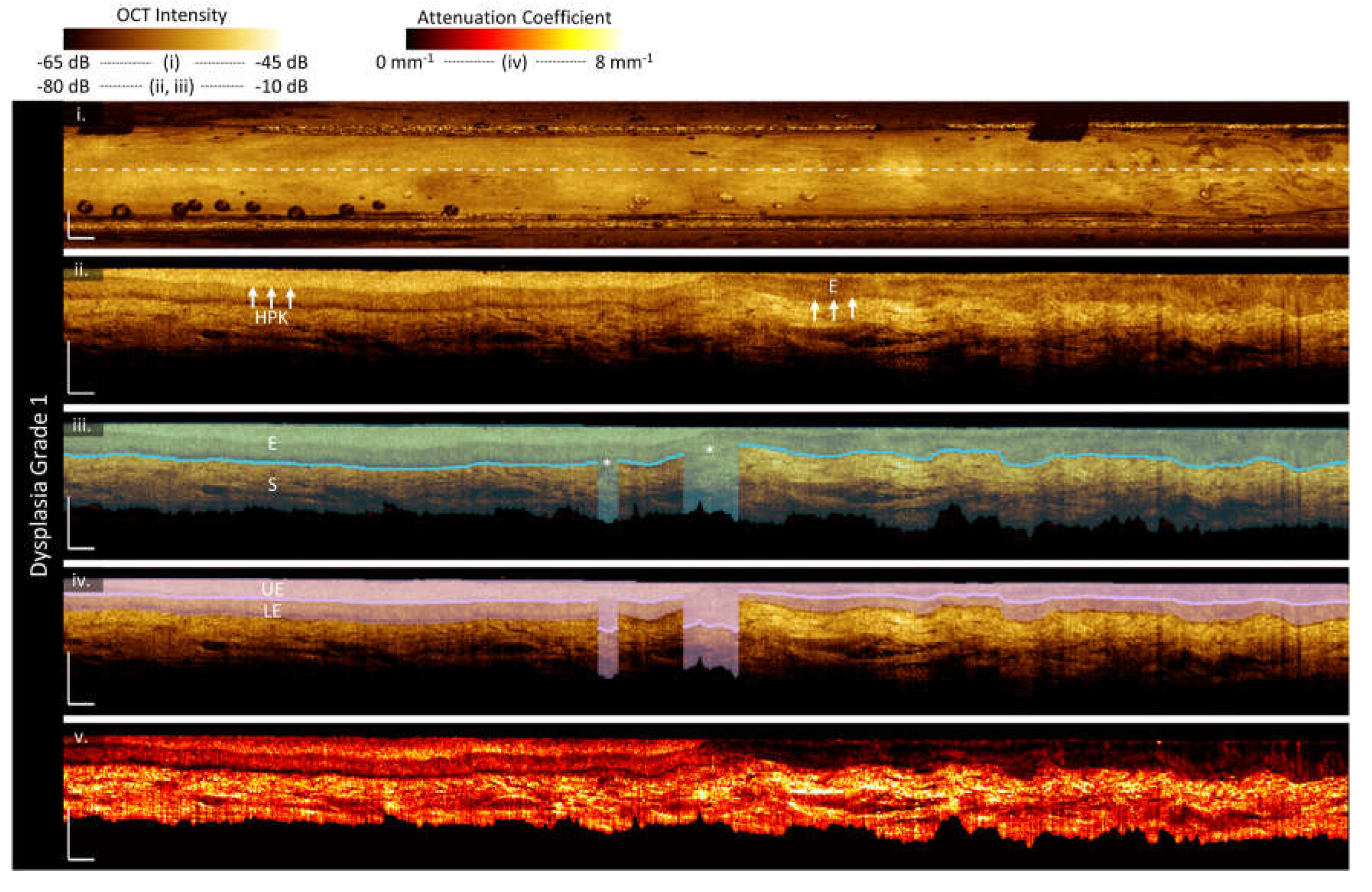
Figure 3.
Sample imaging of a benign acanthotic lesion (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
Figure 3.
Sample imaging of a benign acanthotic lesion (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
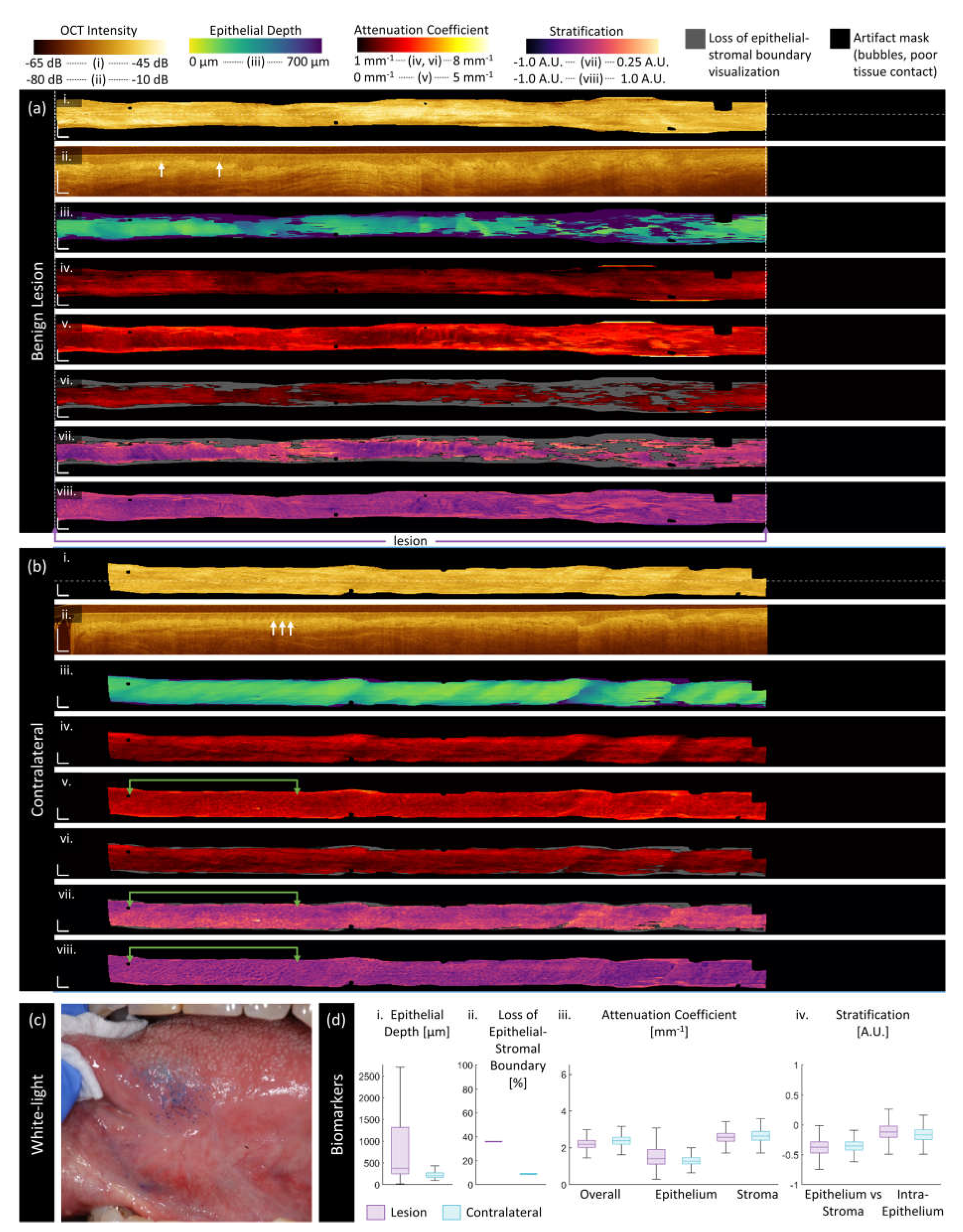
Figure 4.
Sample imaging of a mild dysplasia (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
Figure 4.
Sample imaging of a mild dysplasia (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
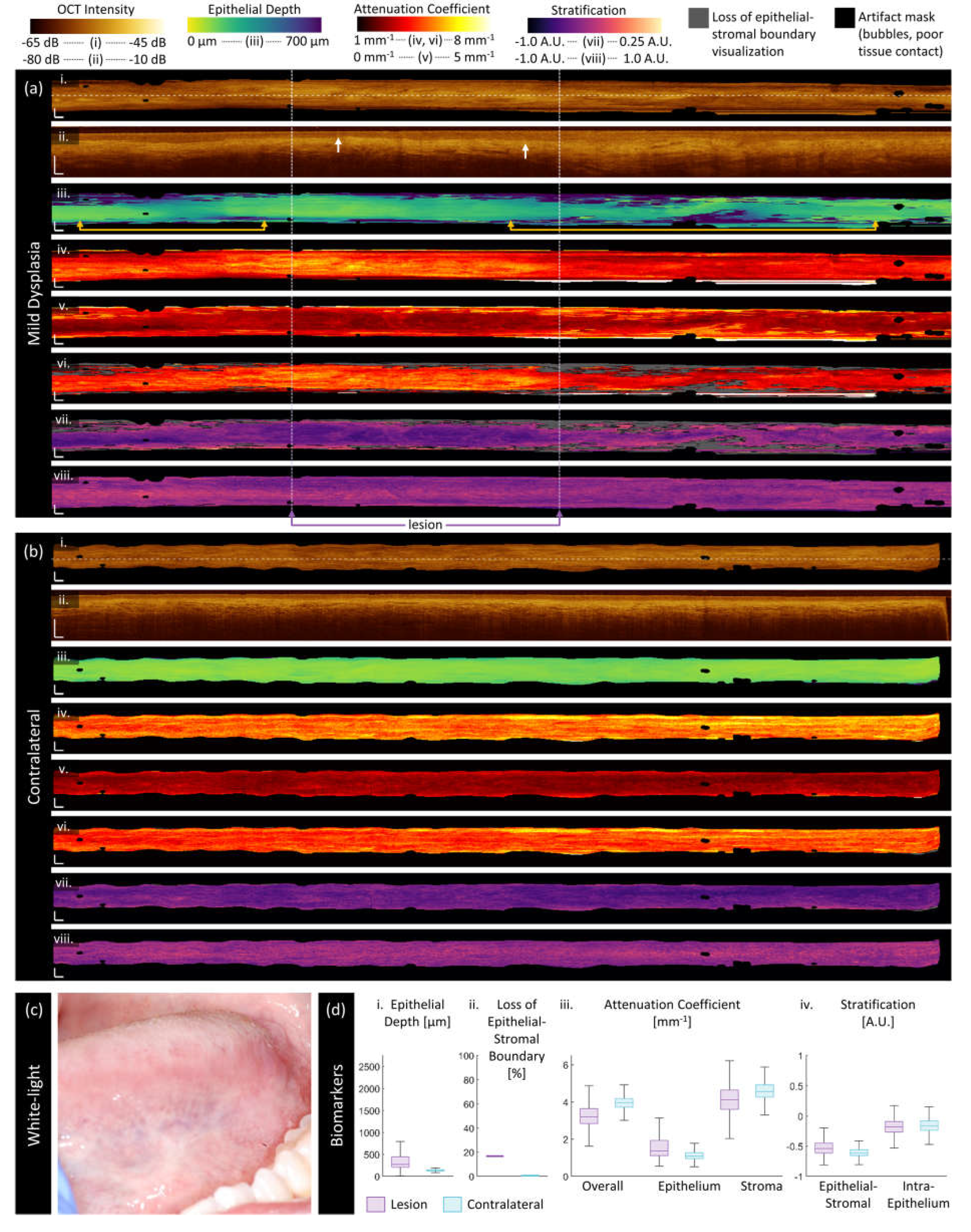
Figure 5.
Sample imaging of a moderate dysplasia (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
Figure 5.
Sample imaging of a moderate dysplasia (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
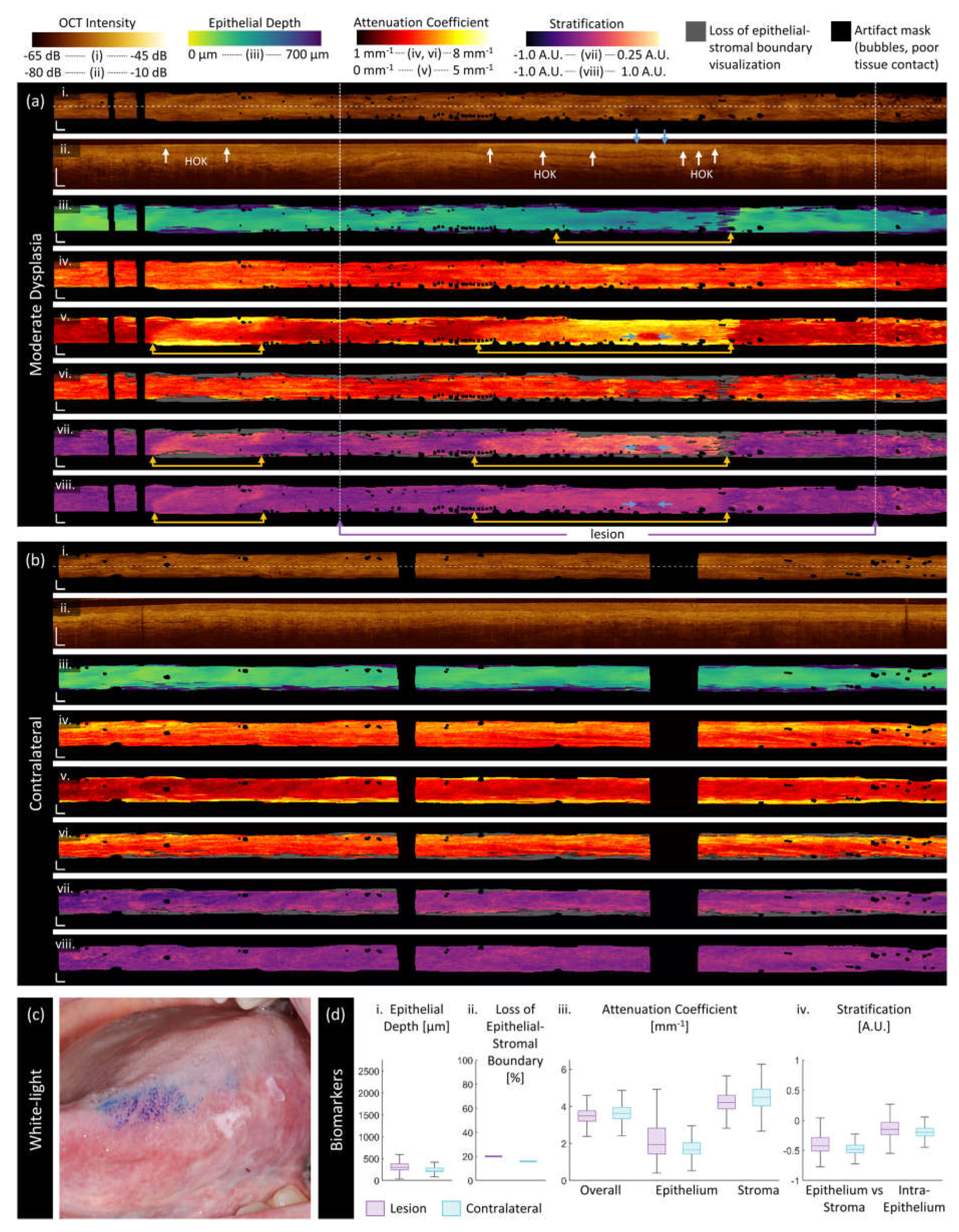
Figure 6.
Sample imaging of a severe dysplasia (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
Figure 6.
Sample imaging of a severe dysplasia (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
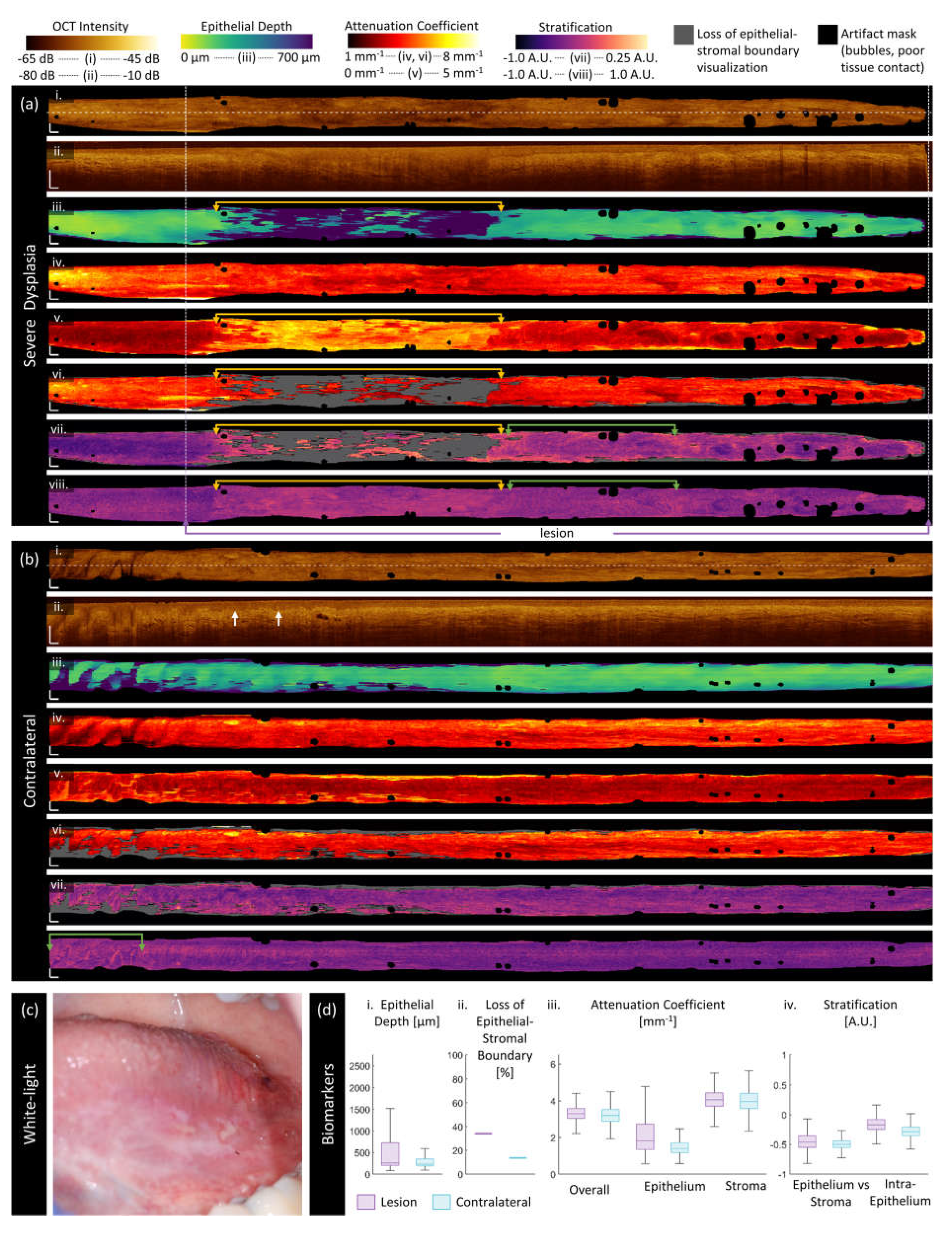
Figure 7.
Sample imaging of a squamous cell carcinoma (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
Figure 7.
Sample imaging of a squamous cell carcinoma (a) and its contralateral (b), with corresponding whitelight photo (c) and box and whisker charts of measurements (d). For panels (a) and (b): (i) OCT mean en face projection; (ii) OCT longitudinal slice from the dashed lines in (i); (iii) epithelial depth; (iv) mean projection of overall attenuation coefficient; (v) mean projection of epithelium attenuation coefficient; (vi) mean projection of stroma attenuation coefficient; (vii) epithelial-stromal stratification (viii) intraepithelial stratification. Grey regions in panels (vi) and (viii) represent loss of epithelial-stromal boundary visualization. All scale bars 1 mm.
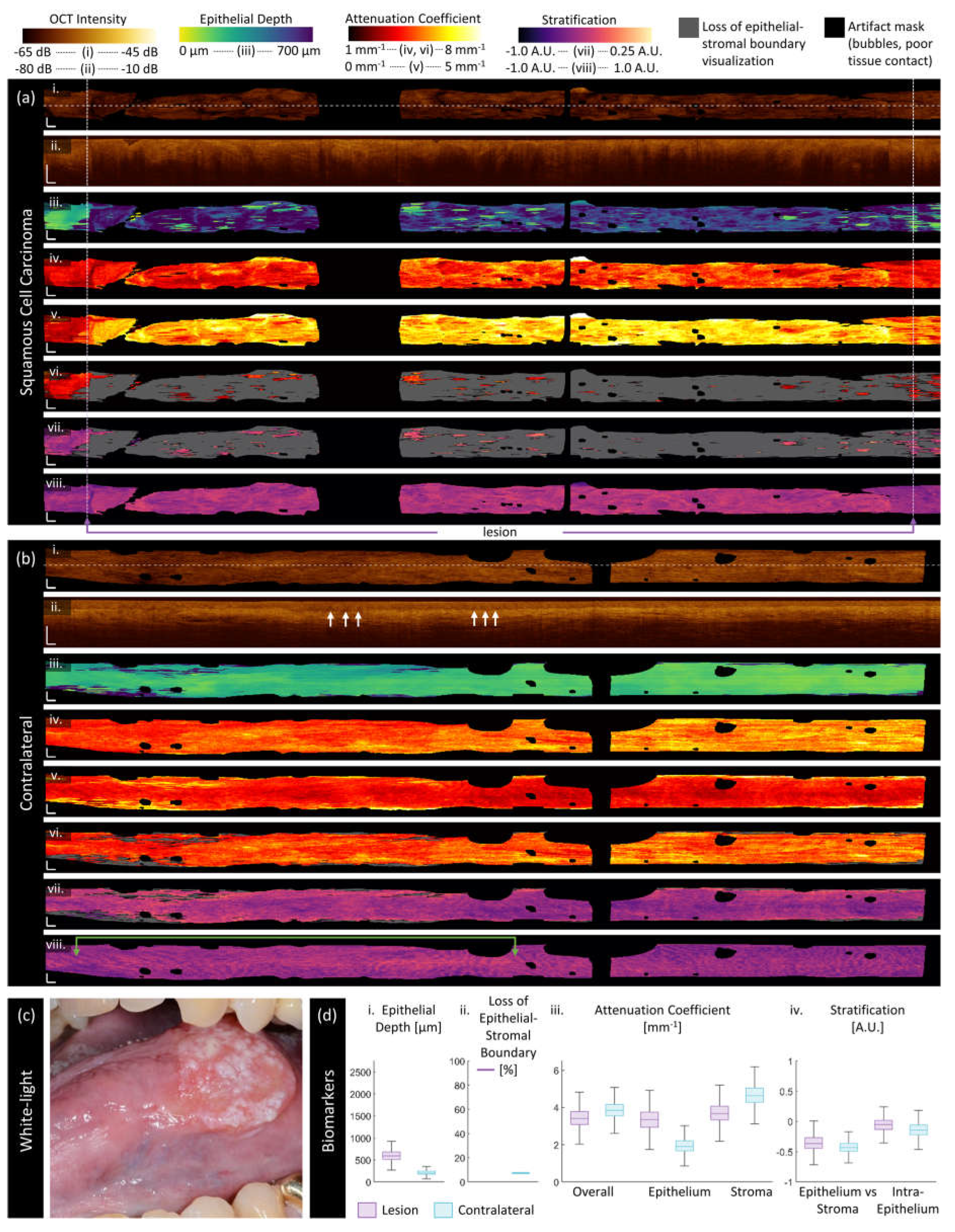
Figure 8.
Measurements against disease status (benign, mild dysplasia ‘D1’, moderate dysplasia, ‘D2’, severe dysplasia and carcinoma in situ, ‘D3/CIS’, squamous cell and verrucous carcinoma ‘Carcinoma’): (i) epithelial depth, (ii) loss of epithelial-stromal boundary visualization, (iii) overall attenuation coefficient, (iv) epithelium attenuation coefficient, (v) stroma attenuation coefficient, (vi) epithelial-stromal stratification, (vii) intraepithelial stratification. Lesions are reported in purple bars and contralaterals in blue. The height of bars is the mean value of medians of all volumes in that category; the error bars are the standard deviation of the medians. The sample size for each group is presented over the bars in (i). Statistically significant differences between disease states are indicated: * = p< 0.05, ** = p<0.01, *** = p<0.001.
Figure 8.
Measurements against disease status (benign, mild dysplasia ‘D1’, moderate dysplasia, ‘D2’, severe dysplasia and carcinoma in situ, ‘D3/CIS’, squamous cell and verrucous carcinoma ‘Carcinoma’): (i) epithelial depth, (ii) loss of epithelial-stromal boundary visualization, (iii) overall attenuation coefficient, (iv) epithelium attenuation coefficient, (v) stroma attenuation coefficient, (vi) epithelial-stromal stratification, (vii) intraepithelial stratification. Lesions are reported in purple bars and contralaterals in blue. The height of bars is the mean value of medians of all volumes in that category; the error bars are the standard deviation of the medians. The sample size for each group is presented over the bars in (i). Statistically significant differences between disease states are indicated: * = p< 0.05, ** = p<0.01, *** = p<0.001.
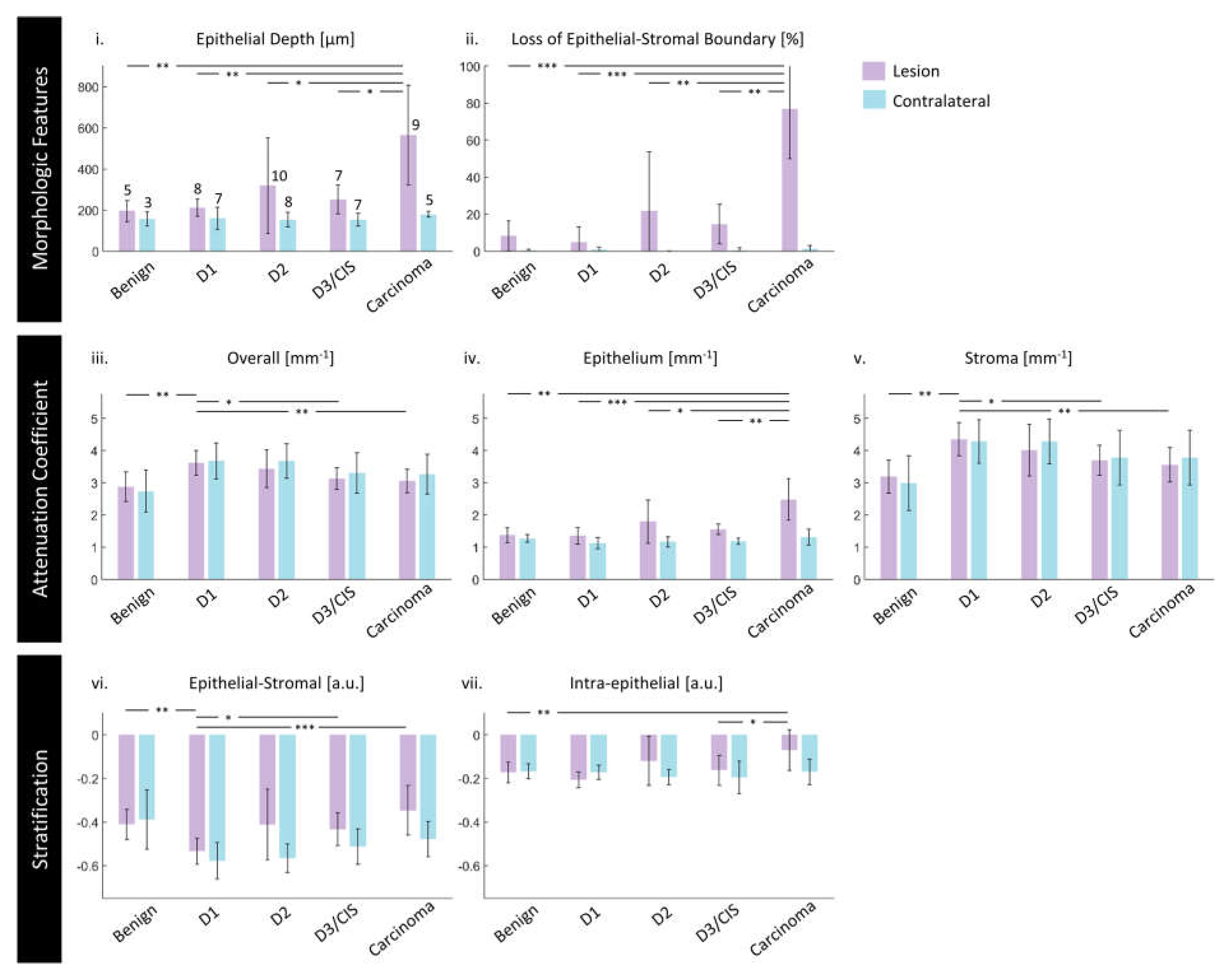
Figure 9.
Measurements against future progression for mild and moderate dysplasias: (i) epithelial depth, (ii) loss of epithelial-stromal boundary visualization, (iii) attenuation coefficients, (iv) stratification. Future progressors are reported in dark purple bars and non-progressors in light purple. The height of bars is the mean value of medians of all volumes after subtraction with the median of their contralateral in that category; the error bars are the standard deviation of the medians after subtraction with their contralateral in that category. The sample size for each group is presented over the bars in (i). Statistically significant differences between disease states are indicated: * = p< 0.05.
Figure 9.
Measurements against future progression for mild and moderate dysplasias: (i) epithelial depth, (ii) loss of epithelial-stromal boundary visualization, (iii) attenuation coefficients, (iv) stratification. Future progressors are reported in dark purple bars and non-progressors in light purple. The height of bars is the mean value of medians of all volumes after subtraction with the median of their contralateral in that category; the error bars are the standard deviation of the medians after subtraction with their contralateral in that category. The sample size for each group is presented over the bars in (i). Statistically significant differences between disease states are indicated: * = p< 0.05.
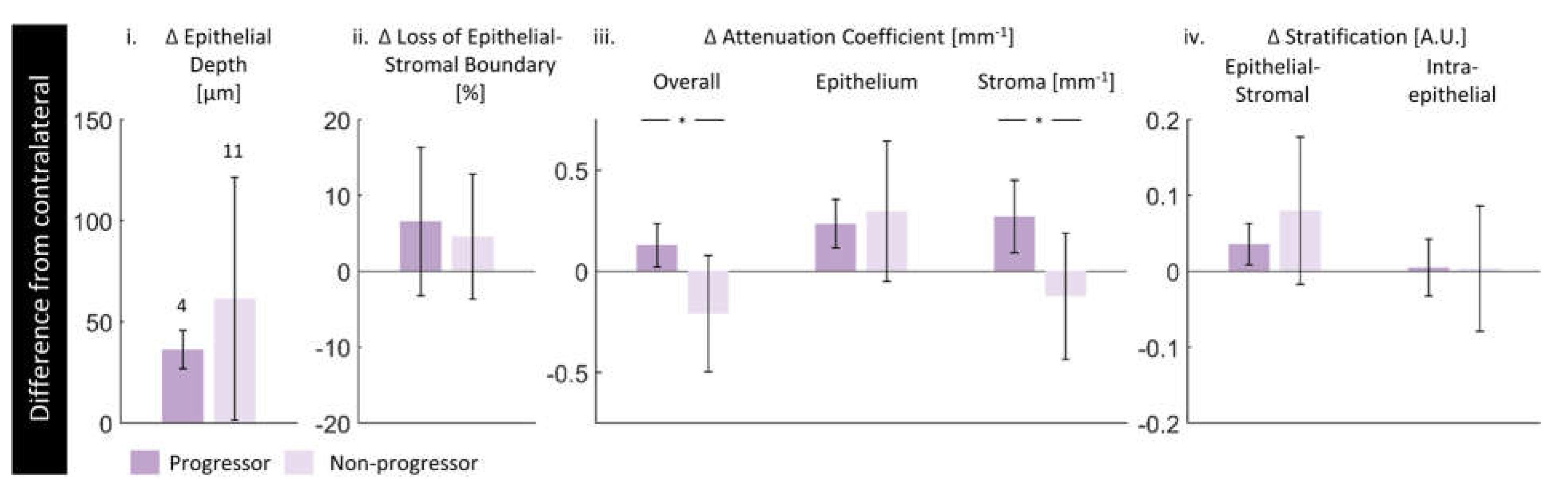

Table 1.
Summary of biomarkers.
| Category | Biomarker | Description | Dimensionality |
|---|---|---|---|
| ‘Morphologic’ | Epithelium depth [μm] |
Height of segmented epithelium region | 2D en face image Range: 0 to ~ 2 mm |
| Loss of epithelial-stromal boundary [%] |
Percentage of loss over volume, excluding artifacts | single value per volume Range: 0 to 100% |
|
| ‘Attenuation’ | Overall attenuation coefficient [mm-1] |
Mean en face projection of attenuation coefficient over the entire depth of visualized tissue | 3D data Range: 0 to ~10 mm-1 |
| Epithelium attenuation coefficient [mm-1] | Mean en face projection of attenuation coefficient over the segmented epithelium region | 3D data Range: 0 to ~10 mm-1 |
|
| Stroma attenuation coefficient [mm-1] |
Mean en face projection of attenuation coefficient over the visualized stroma region | 3D data Range: 0 to ~10 mm-1 |
|
| ‘Stratification’ | Epithelial-Stromal Stratification [a.u.] | 2D en face image Range: -1 to 1 a.u. |
|
| Intraepithelial Stratification [a.u.] |
2D en face image Range: -1 to 1 a.u. |
Table 2.
Dataset demographics for single-timepoint assessment of biomarkers.
| Diagnosis | Lesion | Contralateral | Total | Males | Females |
|---|---|---|---|---|---|
| Only contralateral imaged | 0 | 1 | 1 | 1 | 0 |
| Benign | 5 | 3 | 8 | 3 | 2 |
| Dysplasia grade 1 | 8 | 7 | 15 | 3 | 5 |
| Dysplasia grade 2 | 10 | 8 | 18 | 4 | 6 |
| Dysplasia grade 3 & carcinoma in situ | 7 | 7 | 14 | 3 | 4 |
| Carcinoma (squamous cell, verrucous) | 9 | 5 | 14 | 6 | 3 |
| Total | 39 sites | 31 sites |
40 patients (70 sites) |
20 patients (50%) | 20 patients (50%) |
Table 3.
Dataset demographics for assessment of future progression.
| Diagnosis | Lesion | Contralateral | Total | Males | Females |
|---|---|---|---|---|---|
| Progressors | 4 | 4 | 8 | 1 | 3 |
| Non-progressors | 11 | 11 | 22 | 5 | 6 |
| Total | 15 sites | 15 sites |
15 patients (33 sites) |
6 patients (40%) | 9 patients (60%) |
Table 4.
Dataset demographics for reproducibility / repeatability assessment.
| Patient number | Previous biopsy (time difference) [months] |
Timepoint 1 | Time difference [months] |
Timepoint 2 | ||||
|---|---|---|---|---|---|---|---|---|
| Diagnosis | Lesion | Contra- lateral |
Diagnosis | Lesion | Contralateral | |||
| 1 | D1 (unknown) |
D1 | 1 | 1 | 5 | D1 | 2 | 1 |
| 2 | D2 (10) |
D2 | 2 | 1 | 2 | Hyperplastic candidiasis | 1 | 1 |
| 3 | N/A |
D2 | 1 | 1 | 21 | D2 | 1 | 1 |
| 4 | D2 (16) |
D3 | 1 | 1 | 6 | D3 | 1 | 1 |
| 5 | D2 (13) |
Verrucous carcinoma |
1 | 1 | 6 | Verrucous carcinoma |
1 | 1 |
Table 5.
Measurements of biomarkers across timepoints (contralateral samples) and repeated measurements of lesion within a single timepoint. Data is presented as mean and absolute difference (|timepoint 2 – timepoint 1|) of the two measurements in that category.
Table 5.
Measurements of biomarkers across timepoints (contralateral samples) and repeated measurements of lesion within a single timepoint. Data is presented as mean and absolute difference (|timepoint 2 – timepoint 1|) of the two measurements in that category.
| Morphologic Features | Mean Attenuation Coefficient | Stratification | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patient number | Epithelium depth | Loss of epithelial-stromal boundary visualization |
Overall | Epithelium | Stroma | Epithelial-Stromal | Intra- epithelial |
|||
| [µm] | [%] | [mm-1] | [mm-1] | [mm-1] | [a.u.] | [a.u.] | ||||
| Contralateral (between timepoints) |
1 | 240 50 |
2 3 |
3.05 0.24 |
1.22 0.18 |
3.71 0.55 |
-0.51 0.00 |
-0.21 0.08 |
||
| 2 | 150 20 |
0 0 |
3.59 0.21 |
1.15 0.00 |
4.21 0.25 |
-0.57 0.01 |
-0.12 0.07 |
|||
| 3 | 160 30 |
0 0 |
3.76 1.41 |
1.12 0.11 |
4.47 2.00 |
-0.59 0.11 |
-0.15 0.00 |
|||
| 4 | 120 10 |
0 0 |
4.25 0.90 |
0.95 0.20 |
4.95 1.33 |
-0.68 0.02 |
-0.14 0.06 |
|||
| 5 | 220 80 |
0 0 |
3.60 0.09 |
1.36 0.05 |
4.52 0.41 |
-0.54 0.02 |
-0.23 0.01 |
|||
| Lesion (single timepoint) |
1 | 440 40 |
15 2 |
2.79 0.04 |
1.58 0.21 |
3.62 0.09 |
-0.41 0.05 |
-0.22 0.04 |
||
| 2 | 220 50 |
20 29 |
3.69 0.15 |
1.50 0.39 |
4.59 0.00 |
-0.53 0.08 |
-0.21 0.01 |
|||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



