Submitted:
05 July 2024
Posted:
09 July 2024
You are already at the latest version
Abstract
Vitiligo is a chronic autoimmune disease characterized by progressive depigmentation of the skin caused by the selective destruction of melanocytes. Although its etiopathogenesis remains unclear, multiple factors are believed to be involved, including genetic and metabolic factors linked to cellular oxidative stress, melanocyte adhesion defects, innate and adaptive immunity. The aim of this review is to provide an overview of the current state of knowledge regarding the role of different cellular mechanisms, including cytokines and chemokines interactions in the pathogenesis of vitiligo. Although there is no definitive cure for vitiligo, excessive progress has been made and several treatments have shown favourable results. A thorough understanding of the basis of the disease, uncover promising drug targets for future research, providing clinical researchers with valuable insights for developing improved treatment options.
Keywords:
treatment
; biologics
; biological drugs
; vitiligo
; Janus kinase inhibitors (JAKs)
; cytokines
1. Introduction
Vitiligo is an autoimmune skin disorder diagnosed in 0.5-2% of the population [1]. The patient typically presents with chalky-white, well-demarked and amelanotic patches on the skin, which may occur in specific areas. In addition, vitiligo patients can also suffer reduced quality of life and serious psychological consequences [2]. Its pathogenesis is believed to be influenced by various genetic and metabolic factors linked to cellular oxidative stress, melanocyte adhesion and innate and adaptive immunity [3].
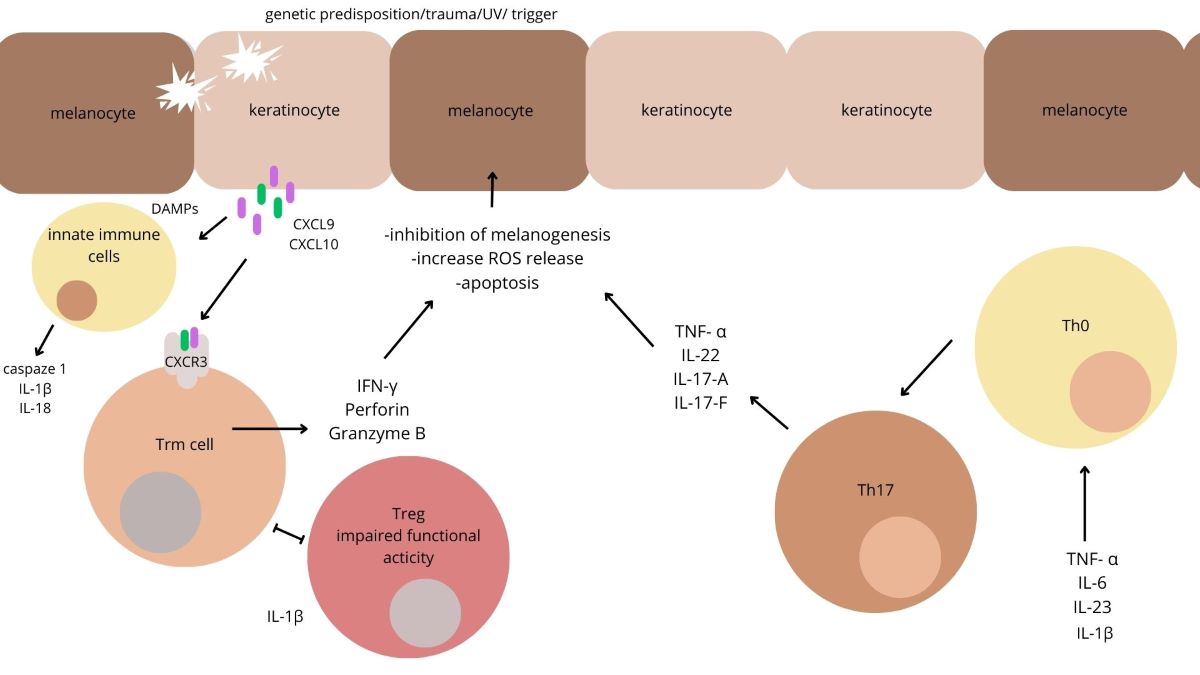
In vitiligo, activation of exogenous and endogenous factors in genetically-predisposed patients stimulates autoimmune processes in which CD8+ T cells exert a cytotoxic effect that causes the direct destruction of melanocytes [4]. While Treg cells suppress autoreactive CD8+ T cells in normal conditions, in vitiligo, this regulatory function is impaired and CD8+ T activation and proliferation remain unopposed [5]. The CD8+ T cells are most commonly directed against melan A, gp100, human tyrosinase-related protein-1 (TRP-1), TRP-2, and tyrosinase [6]. Autoreactive cytotoxic CD8+ cells promote melanocyte destruction and disease progression by local production of IFN-γ. Damaged melanocytes release DAMPs (damage-associated molecular patterns), which are recognized by pattern recognition receptors (PRRs) and NOD-like receptors (NLRs) localized in the cytoplasm of the innate immune system cells. Following activation, the NLRs create inflammasomes; these induce the release of caspase 1, IL-1 β and IL-18, which are involved in the death of melanocytes [7]. IL-1 β activates Th17 cells and promote Treg cell dysfunction. One DAMP, heat shock protein (HSP70), activates dendritic cells to produce IFN-α; these in turn stimulate keratinocytes to generate CXCL9 and CXCL10 which also damage melanocytes [8].
Resident memory (Trm) cells are a subset of T cells whose role is mediate long-term immune response in vitiligo. Trm cells have CD69, CD103 and CD49a on the surface and when activated, they can secrete CXCR3, IFN-α and TNF-α [9]. Trm cells expressing CD69 and CD103 markers are enriched in stable vitiligo skin in contrast to individuals experiencing active disease, this finding is consistent with their function as memory cells that endure even after the resolution of active inflammation [10].
While the pathogenesis of vitiligo is known to a certain extent, there is still no available effective method of treatment. Topical corticosteroids and calcineurin inhibitors are used to obtain repigmentation, and a systemic corticosteroid to stabilize the active vitiligo [11]. PUVA therapy has certain advantages, thanks to its immunosuppressive potential and ability to regenerate melanocytes, but its use is associated with phototoxic effects, nausea and a higher risk of cancer [12]. A safer, and more effective, option than PUVA therapy is narrow-band UVB (nb-UVB) phototherapy [13,14,15], and the combination of nb-UVB with topical treatment is currently the first-line option for clinicians [16,17,18]. However, this treatment does not result in complete repigmentation in all patients and is often a long-term option; furthermore, relapses are common within 12 months following discontinuation of therapy [19].
The aim of this manuscript is to review the role of different cytokines and chemokines in the pathogenesis of vitiligo and examine the potential effectiveness of existing treatment options (Table 1).
1. IL-6
IL-6 is a pro-inflammatory pleiotropic cytokine produced by lymphocytes and macrophages. Together with IL-8, it recruits immune cells to the skin and directs them to target melanocytes [20], and with the inflammatory cytokines TNFα and IL-1β, it has been found to inhibit melanocyte proliferation [21]. IL-6 is believed to act through two molecules: the IL-6 receptor IL-6R and gp130. When IL-6 binds to mIL6R, the membrane-bound form of IL-6R, it forms a complex comprising IL-6, IL-6R and gp130; this complex activates Janus kinases (JAKs), thus triggering two main signaling pathways involved in autoimmune diseases [22]. Indeed, patients with vitiligo have been found to demonstrate higher IL-6 serum concentrations than controls [23,24]. Moreover, as the level of IL-6 in sera positively correlates with disease progression, it can be regarded as a sensitive marker of active vitiligo [25,26].
1.1. IL-6 Inhibitor
IL-6 may inhibit melanogenesis [27], and thus halt disease progression and initiate melanocyte repigmentation. One such treatment involves the use of tocilizumab, a humanized monoclonal antibody directed against the IL-6 receptor. Although only one case report of positive effect of tocilizumab in vitiligo could be found in the literature, the results indicated resolution of facial and periungual vitiligo in a patient treated for seronegative rheumatoid arthritis [28]. Tocilizumab therapy has been found to increase serum IL-6 levels following IL-6R blockage; this increase could potentially have systemic effects, such as exacerbating vitiligo by intensifying the imbalance between Tregs and Th17 cells [29]. Indeed, paradoxical cases of halo naevi developing during tocilizumab therapy have been reported [27]. While there is a low level case- based evidence to suggest some benefit, the drug is not recommended in such indication [30].
2. IL-15
IL-15 belongs to the family of cytokines characterized by a four α-helix bundle structure. It shares the receptor components CD132, i.e., the cytokine receptor γ-chain, and CD122, i.e., the β-chain (IL-2/IL-15Rβ) with IL-2, another key cytokine [31]. In vitiligo, oxidative stress activates NF-κB signaling, thus inducing the expression and trans-presentation of IL-15 in keratinocytes; this enhances the activation and expression of cytotoxic proteins in CD8+ cells through the activation of both STAT3 and STAT5 pathways. IL-15 maintains the signals of Trm cells. These can persist for a long term and be reactivated upon reinfection with the same antigen, promoting disease relapses [32]. IL-15 expression was elevated in both the perilesional skins and blood circulation of individuals with vitiligo, indicating increased levels of locally-expressed and secreted IL-15 in these patients [33]. Il-15 is thought to be an important mediator of T-cell survival in the skin in patients with vitiligo.
2.1. IL-15 Inhibitors
Ex vivo studies indicate that IL-15 supports Trm function and that IL-15-deficient mice exhibit impaired Trm formation. Both human and mouse Trm express the CD122 subunit of the IL-15 receptor, and keratinocytes enhance the expression of CD215, necessary for displaying the cytokine on their surface to activate T cells. The blockage of IL-15 signaling with an anti-CD122 antibody effectively reversed disease progression in mice with established vitiligo. Short-term administration of anti-CD122 inhibited Trm production of IFN-γ, while long-term treatment depleted Trm from skin lesions [34].
Targeting IL-15 or its receptor could serve as a promising approach to developing targeted treatments that inhibit interactions between oxidative stress and release of IL-15 by keratinocytes. AMG 714 binds to IL-15, preventing it from binding with the IL-15 receptor. Use of this drug in vitiligo is being investigated in an ongoing phase IIa clinical trial (NCT04338581) [4].
3. TNF-α
Another important pro-inflammatory cytokine involved in inflammation, cell proliferation, differentiation and apoptosis is TNF-α [35]. TNF-α is directly involved in melanocyte apoptosis, inhibition of melanogenesis and melanocyte stem cell differentiation. It also increases the cytotoxic reaction towards melanocytes [36]. IFN-γ and TNF-α stimulate keratinocytes to produce matrix metallo-proteinase 9 (MMP-9), involved in destabilizing detachment between melanocytes by releasing the soluble form of E-cadherin [37]. In many studies, vitiligo patients demonstrated higher mean serum TNF-α levels than controls, with the level being correlated with disease activity [24,26,38]. These observations were confirmed by De et al., who found patients to have elevated TNF-α levels in serum and in lesional skin compared to controls [23].
3.1. TNF-α Inhibitors
TNF-α blockers such as adalimumab, infliximab and etanercept have been used in various autoimmune and inflammatory conditions [39]. It is possible they may also be of value against vitiligo as TNF-α blockage may modulate the immune response and potentially inhibit the progression of vitiligo spots. While TNF-α inhibitors can stabilize progressive vitiligo in some patients [40], they may also be associated with new-onset vitiligo in others. Most of these cases were observed after the use of adalimumab and infliximab [41,42,43]; however, it remains unclear whether these are co-morbidities or possible side effects. A 2007 pilot study found etanercept to be ineffective at treating vitiligo in all four test cases [44], although researchers reported a mild improvement in vitiligo lesions during treatment [45]. In addition, a 10-year cohort study of 11,442 patients found anti-TNF agents to significantly increase the risk of vitiligo, but not alopecia areata [46].
4. IL-1β
The formation of IL-1β interleukin depends on the activation of two of the NLRs that are part of the inflammasome: NLRP1 and NLRP3 [47]. Being an proinflammatory cytokine, IL-1β can induce rapid release of iNOS and generate a large amount of NO in tissues [48]. Increased IL-1β levels were observed in the sera of active-vitiligo patients, suggesting that IL-1β may play a role in dysregulating melanocytic activity in lesional skin [49]. It has been reported that NLRP1 and IL-1β immunostaining in perilesional skin was significantly associated with progressive disease, and surprisingly, it added significantly more information of the disease progression with regard to the simple lymphocytic infiltrates [50].
5. IL-22
IL-22 belongs to the IL-10 family, which plays a vital role in various inflammatory and infectious diseases. Th22 and Th17 cells are major sources of IL22 [51]. IL-22 influences IL-1β production by activating NLRP3-caspase-1; it also plays a minor role in melanocyte proliferation and melanogenesis, and enhances the synthesis of antimicrobial peptides and chemokines in human keratinocyte cells (HaCaT) [52]. The IL-22–IL-22R system predominantly activates STAT3 via the JAK- STAT pathway. It has been found that serum IL-2 levels were significantly raised in localized vitiligo, whereas IL-17 and IL-22 were significantly raised in generalized vitiligo; however, no correlation was found between IL-22 levels and disease activity or severity [26].
5.1. IL-22 Inhibitor
Antibodies neutralizing IL-22 have yielded promising results against psoriasis and rheumatoid arthritis and they may improve the response to chemotherapy, especially in reducing metastases [53]. No studies have evaluated the effectivity of IL-22 antibodies in vitiligo.
6. IL-17
Studies have suggested that Th17 cells may be involved in the pathogenesis of vitiligo [54]. IL-6, TGF-β and IL-23 drive the differentiation of Th cells into Th17 cells, which then produce various specific cytokines, including IL-17A, IL-17F, IL-22 [55] and TNF-α [56]. Serum IL-17 levels have been found to be elevated in vitiligo patients compared to healthy individuals [57]. Some papers have also demonstrated significant positive correlations between IL-17 levels in serum and lesional skin and the activity, extent and severity of vitiligo [54,58,59]. Furthermore IL-17 is a potent producer of the chemokine CCL20, a molecule that can introduce cytotoxic CD8+ T cells into peripheral tissues from the systemic circulation; these cells are responsible for melanocyte destruction in vitiligo [60]. In addition, in inflammatory vitiligo, IL-17 stimulates keratinocytes to release chemokines that cause an influx of neutrophils, macrophages and dendritic cells, which can also play a role in melanocyte destruction [61].
Th17 cells can be transformed into Th17.1 cells, which demonstrate a shared phenotype of Th17 and Th1 cells, or into Th17ex cells, i.e., transformed Th17 cells that produce IFN-γ instead of IL-17 [62]. These may constitute a novel potential therapeutic target for vitiligo treatment, as recent studies confirm that serum Th17.1 cell levels are elevated in vitiligo patients [63] and that these numbers fall after starting effective treatment [60].
1.1. IL-17A Inhibitors
Secukinumab is a monoclonal antibody that specifically blocks the action of pro-inflammatory interleukin-17A (IL-17A), and thus modulates the immune response. Studies have found it to be effective in the treatment of various immune-mediated inflammatory conditions, including psoriasis, psoriatic arthritis, and ankylosing spondylitis [64]. In one study, a 63-year-old man who developed vitiligo during therapy with adalimumab was reported to experience resolution of both vitiligo and psoriasis after changing treatment to secukinumab [65]. A case report from 2021 also indicated that a patient developed new-onset vitiligo during secukinumab therapy for psoriatic arthritis, but the vitiligo spots slowly began to repigment after one year of therapy [66].
However, some reviews and case series of new-onset vitiligo in individuals undergoing treatment with secukinumab report negative effects [67,68,69]. A single-arm pilot study of secukinumab in treating active non-segmental vitiligo did not find that IL-17 or Th17 cells had a direct pathogenic role in vitiligo; however, it indicated that the balance of Th17/Th17.1/Th1 can change according to disease activity. One promising treatment option for vitiligo may therefore involve modulating the differentiation of Th17 toward Th17/1 and Th1 [63].
Another IL-17A blocker is ixekizumab, which is also widely used in various autoimmune conditions. A case study of a man suffering from psoriasis and psoriatic arthritis found that treatment with adalimumab caused whitening of the hair on the scalp and face, which was reversed after switching to ixekinumab [70]. Interestingly though, most other such studies have reported new cases of vitiligo occurring during ixekizumab therapy [71,72,73].
7. IL-23
IL-23 is a heterodimer composed of the p19 and p40 subunits; it plays a role in the proliferation, maturation and differentiation of Th17 lymphocytes [74]. The IL-23 receptor, consisting of IL-12Rβ1 and IL-23R, is expressed by inflammatory macrophages and DCs. The binding of IL-23 to the receptor leads to antigen presentation by DCs, formation of Th17 cells, and production of IFN-γ. IL-23 is believed to have a central role in autoimmunity, and that its dysregulation or overactivation may contribute to the progression of vitiligo [75]. IL-23 serum levels have demonstrated a positive correlation with the duration, activity and extent of the disease in patients with non-segmental generalized vitiligo [56].
1.1. IL-23 Inhibitor
Tildrakizumab, an IL-23 blocker, is effective in the treatment of psoriasis, rheumatoid arthritis and inflammatory bowel diseases (IBD) [76]. Patients with vitiligo commonly demonstrate increased levels of IL-23 [74,77], and as such it may represent a therapeutic target in vitiligo. Only one study examined the use of tildrakizumab in rapidly-progressive vitiligo: its use resulted in a 55% reduction in Vitiligo Area Scoring Index (VASI) over 12 months [78].
1.2. IL-12 and IL-23 Inhibitor
Ustekinumab is a monoclonal antibody that blocks the p40 subunit common to IL-12 and IL- 23, and thus prevents these cytokines binding to the IL-12Rβ1 chain of their receptors [79]. The drug targets Th1 and Th17 cells, which alter immune cell hypersensitivity, and could hence offer potential benefits in dermatological conditions such as vitiligo, alopecia areata and cutaneous systemic lupus erythematosus [80]. Although IL-23 induces the production of Th17 cells and mediates autoimmunity in vitiligo by influencing the secretion of the IL-17 family [56], little is known of the use of IL-12/23 blockers in practice. Elkady et al. report an impressive improvement in comorbid alopecia areata and vitiligo in a patient with psoriasis [81]. A nationwide retrospective multi-centre study investigated the appearance of new-onset vitiligo during biologic therapy in patients treated for different reasons and evaluated the clinical course of pre-existing vitiligo under biological therapy. Three patients developed new onset vitiligo during ustekinumab treatment, and one patient showed no improvement in their existing vitiligo. Patients with new onset vitiligo were described as showing improvement during ustekinumab treatment. Surprisingly, one repigmentation was reported after switching from adalimumab to ustekinumab [82]. Another study on the drugs and therapeutic subclasses associated with vitiligo reported an association between vitiligo and ustekinumab therapy [83]. However, it is important to note that while some studies have shown ustekinumab to obtain positive responses in terms of repigmentation, the overall data and consensus regarding its effectiveness require further investigations.
8. IFN-γ
IFN-γ is mainly produced by plasmacytoid dendritic cells (pDCs). This cytokine interacts with Janus Kinase 1 (JAK1) and JAK2 on keratinocytes, thus activating the signal transducer and activator of transcription protein (STAT) [5]. After being phosphorylated, STAT moves to the nucleus to induce the transcription of specific genes [84]. The JAK-STAT pathway plays a role in the expression of CXCL9/10/11, i.e., chemokine ligands 9/10/11, that direct T-cells to the epidermis [85,86]. Moreover, these molecules mediate the recruitment of CD8+ T cells via chemokine receptor 3 (CXCR3); these are responsible for the apoptosis of melanocytes [26,37,87]. The results of a comparative study indicate that CXCL10 and IFN mRNA expression was significantly higher in non-lesional and perilesional skin in patients with vitiligo compared to healthy controls. Interestingly, the mRNA expression levels of CXCL10, and particularly IFN-γ, were found to be elevated in the non-lesional skin of active vitiligo patients when compared to those of stable patients, which may suggest that these molecules are related to disease activity [88]. However recent studies have found that in contrast to tissue, patients with vitiligo show decreased IFN-γ serum levels in comparison to controls [23,89].
8.1. JAK Inhibitors
Currently, JAK inhibitors offer great promise for the treatment of vitiligo. The JAKs, viz. JAK1, JAK2, JAK3 and TYK2, are a family of cytoplasmic tyrosine kinases (TYKs). JAK1 and JAK2 modulate the transduction signal after IFN-γ binds to its receptor [90], and as such, the downstream IFN-γ/CXCL10 signaling pathway may be a potential therapeutic target in vitiligo. Recent studies indicate that JAK 1 and JAK3, but not JAK2, demonstrated higher cutaneous expression in vitiligo skin compared to healthy skin [91,92]. Inhibition of the JAK/STAT pathway disrupts the detachment of low E-cadherin melanocytes in the basal layer of the epidermis. Furthermore, it decreases the secretion of MMP-9 by keratinocytes in response to IFN-γ and TNF-α. The levels of MMP-9 are increased in the skin and sera of patients with vitiligo and are responsible for E-cadherin disruption in the basal layer of the epidermis. Inhibition of MMP-9 prevents melanocyte detachment in vitro and in vivo [93].
8.1.1. Ruxolitinib
This molecule is an inhibitor of JAK1 and JAK2. The US Food and Drug Administration (FDA) approved topical ruxolitinib for repigmentation of nonsegmental vitiligo in July 2022 for people aged 12 years and older based on data from the phase III TRuE-V1 and TRuE-V2 clinical trials. The goal of these two phase 3 trials (NCT04052425 and NCT04057573) was to assess the safety and efficiency of the topical ruxolitinib in non-segmental vitiligo. The study involved patients 12 years of age or older with non-segmental vitiligo and depigmentation covering 10% or less of total body surface area. Treatment with 1.5% ruxolitinib cream resulted in greater repigmentation of vitiligo lesions than vehicle control over 52 weeks, but it was associated with acne skin lesions and pruritus at the application area [94].
The drug is believed to act by blocking the JAK1/2 pathway, which interferes with STAT transcription; the pathway itself mediates various inflammatory cytokines, growth factors, interferons and interleukins [95]; however, the exact mechanism of the action remains unclear. One study comparing the effects of ruxolitinib cream and vehicle, and examining the correlation between the level of CXCL10, an immunity biomarker, in skin and VASI scores is currently underway [96]. It has been found that reducing the CXCL10 level may limit melanocyte destruction by reducing the inflow of CD8+ T cells [97]. Oral ruxolitinib has been approved by the FDA and EMA for treating myelofibrosis, polycythaemia vera and acute graft-versus-host disease [98]. Several studies indicate that while these drugs have a good effect of repigmentation in vitiligo patients, the effect disappeared after discontinuation of treatment [99].
8.1.2. Tofacitinib
Tofacitinib an inhibitor of JAK1/3, has been approved by the US FDA for psoriatic arthritis and shows promise for treating plaque psoriasis [100]. It was found to successfully inhibit CXCL10 secretion through the suppression of JAK-STAT signaling in keratinocytes [101]. The first use of oral tofacitinib in vitiligo was reported in 2015, in a case of generalized vitiligo involving approximately 10% of the body surface. Treatment resulted in significant repigmentation: vitiligo patch cover fell to only 5% after five months of treatment [102].
Oral and topical treatments have both yielded positive results, especially in areas of great sun exposure [101,103]. In two patients suffering from vitiligo with facial involvement, a combination of tofacitinib and low-dose, narrowband UVB radiation resulted in significant repigmentation [67]. These findings indicate that tofacitinib may require additional nb-UVB phototherapy to be more effective and to stimulate melanocytes to seed the epidermis, where tofacitinib can suppress the immune response [104]. So far, no clinical trials have investigated the efficiency and safety of tofacitinib in vitiligo patients, and further research is needed in this area.
8.1.3. Baricitinib
Baricitinib is a small molecule that mainly acts on JAK1/2. It is currently approved for rheumatoid arthritis, but can be used in other conditions, such as atopic dermatitis or systemic lupus erythematosus [105]. One preliminary study on four patients with progressing vitiligo found that a combination of baricitinib and high-dose ultraviolet B irradiation caused significant repigmentation without any serious side effects [106]. The effectiveness and tolerance of oral baricitinib with phototherapy is currently being compared to phototherapy in an ongoing randomized clinical trial phase II (NCT04822584), and the results appear promising [37].
8.1.4. Ritlecitinib
Ritlecitinib is an orally-administered biological drug that inhibits JAK3 and the TEC kinase family [107], which may block cytokine activity and decrease the cytotoxic activity of CD8+ T cells. A randomized phase 2b clinical trial found the treatment to be effective against active non-segmental vitiligo over 48 weeks with good tolerance [108]. A phase III clinical trial of ritlecitinib in adults and adolescents with active and stable vitiligo is ongoing (NCT05583526).
8.1.5. Ifidancitinib
Ifidancitinib is a JAK1/3 inhibitor that is currently under investigation in phase II clinical trial for the topical treatment of vitiligo [109]. This drug is able to induce depletion of effector function of T cells and has been used for treating alopecia areata [110]. The effectiveness of 0.46% ifidancitinib solution for treating non-segmental facial vitiligo is under examination (NCT03468855) [111].
8.1.6. Brepocitinib
Brepocitinib is an oral JAK1 and TYK inhibitor that has been used to treat moderate-to-severe plaque psoriasis. A study (NCT03715829) has explored the use of both ritlecitinib and brepocitinib for treating vitiligo, with and without phototherapy [111]. However, there are currently no trials exploring this drug in vitiligo.
8.1.7. Upadacitinib
Upadacitinib is an oral selective JAK1 inhibitor. Recent studies indicates a notable improvement of VASI and DLQI score in recalcitrant vitiligo in patients treated with upadacitinib [112]. Its adverse events and effectiveness are being evaluated in a phase III clinical trial (NCT06118411).
8.1.8. Cerdulatinib
Cerdulatinib demonstrates specificity towards JAK1/3 and spleen tyrosine kinase (SYK) [113]. It has been shown to be effective in B-cell malignancies such as diffuse large B-cell lymphoma, Burkitt lymphoma and chronic lymphocytic leukemia (CLL) [114]. Cerdulatinib (0.37% gel) has been assessed for safety, tolerability, and systemic exposure in adults with vitiligo in II phase clinical trial (NCT04103060); however, the results are not available.
8.1.9. Delgocitinib
Delgocitinib is a JAK1/2/3 and TYK2 inhibitor. It has been found to be effective against vitiligo vulgaris after topical application [115].
Other Perspectives
Vitiligo development is influenced by the IFN-γ-CXCL9/10-CXCR3 pathway and new therapeutic strategies are being designed to take advantage of this. A 2005 study found IFN-γ neutralizing antibodies to induce repigmentation in two of four vitiligo patients who received intradermal perilesional injections [116]. It was also found to reverse vitiligo in mice [117]. CXCL10 is elevated in the skin and serum of vitiligo patients, and CXCR3, its receptor, is expressed on pathogenic T cells. In addition, minimal depigmentation is noted in patients with T cells lacking CXCR3, as well as mice deficient in CXCL10 or treated with a CXCL10-neutralizing antibody. Neutralizing CXCL10 led to repigmentation in mice with established, widespread depigmentation [118]. Vitiligo patients also demonstrate increased CXCR3 levels in antigen-specific T cells in the blood, and present CXCR3+ cells in skin biopsies. It was found that CXCR3 depleting antibody can reverse vitiligo by reducing autoreactive T cell numbers [119].
Latanoprost is a prostaglandin F2alpha analogue primarily used to reduce intraocular pressure in patients with open-angle glaucoma and ocular hypertension. As it induces hypertrichosis and hyperpigmentation due to increased melanogenesis, it may be suitable for treating hypopigmentation disorders such as vitiligo [120]. The combination of latanoprost with nb-UVB therapy is currently under evaluation for treating non-segmental vitiligo in a phase 4 clinical trial (NCT04811326).
Afamelanotide is the first synthesized analogue of α-melanocyte-stimulating hormone (α-MSH). It appears more stable and active than the natural hormone [121]. Its efficacy and safety for inducing repigmentation are under evaluation in patients with vitiligo in two clinical trials: the first as monotherapy (NCT05210582), and the other in combination with nb-UVB light compared to nb-UVB light alone (NCT06109649).
Another promising therapy is the intralesional administration of methotrexate every two weeks. This method appears to be effective among patients with focal vitiligo based on a pilot study; however, further studies on larger groups are necessary [122].
Conclusions
As cytokines and chemokines play such important roles in the pathogenesis of vitiligo, they should also play a role in its treatment. Biologic and small molecules therapies are effective in various immune-mediated inflammatory diseases, including vitiligo; however, they can also provoke vitiligo onset or exacerbate pre-existing disease. Many existing treatments are nonspecific. While our growing understanding of the underlying processes of vitiligo has paved the way for more targeted approaches, the data regarding their mechanisms of action and their efficacy remain broad. JAK inhibitors offer particular promise as treatments, and this is supported in ongoing clinical trials. Nevertheless, there continues to be a need for further research into new and more effective treatments.
Supplementary Materials
None.
Author Contributions
Conceptualization, A.W., M.K.; writing—original draft preparation, M.K., M.K. and P.K.; writing—review and editing, A.W. All authors have read and agreed to the published version of the manuscript.
Funding
Work was completed as part of the statutory work of the Medical University Lodz—503/1-152-01/503-11-002.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bergqvist C, Ezzedine K. Vitiligo: A Review. Dermatology [Internet]. 2020 Nov 1 [cited 2023 Nov 5];236(6):571–92. Available from: https://pubmed.ncbi.nlm.nih.gov/32155629/.
- Ezzedine K, Grimes PE, Meurant JM, Seneschal J, Léauté-Labrèze C, Ballanger F, et al. Living with vitiligo: results from a national survey indicate differences between skin phototypes. Br J Dermatol [Internet]. 2015 Aug 1 [cited 2023 Nov 5];173(2):607–9. Available from: https://pubmed.ncbi.nlm.nih.gov/25892476/.
- Marchioro HZ, Silva de Castro CC, Fava VM, Sakiyama PH, Dellatorre G, Miot HA. Update on the pathogenesis of vitiligo. An Bras Dermatol [Internet]. 2022 Jul 1 [cited 2023 Nov 7];97(4):478. Available from: /pmc/articles/PMC9263675/.
- Iwanowski T, Kołkowski K, Nowicki RJ, Sokołowska-Wojdyło M. Etiopathogenesis and Emerging Methods for Treatment of Vitiligo. Int J Mol Sci [Internet]. 2023 Jun 1 [cited 2024 May 14];24(11). Available from: https://pubmed.ncbi.nlm.nih.gov/37298700/.
- Bergqvist C, Ezzedine K. Vitiligo: A focus on pathogenesis and its therapeutic implications. J Dermatol [Internet]. 2021 Mar 1 [cited 2023 Oct 25];48(3):252–70. Available from: https://pubmed.ncbi.nlm.nih.gov/33404102/.
- Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet [Internet]. 2015 Jul 4 [cited 2023 Feb 8];386(9988):74–84. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25596811.
- Afzali B, Lombardi G, Lechler RI, Lord GM. The role of T helper 17 (Th17) and regulatory T cells (Treg) in human organ transplantation and autoimmune disease. 2007 [cited 2023 Nov 15]; Available from: https://academic.oup.com/cei/article/148/1/32/6457759.
- Mosenson JA, Zloza A, Nieland JD, Garrett-Mayer E, Eby JM, Huelsmann EJ, et al. Mutant HSP70 reverses autoimmune depigmentation in vitiligo. Sci Transl Med [Internet]. 2013 Feb 27 [cited 2024 May 14];5(174). Available from: https://pubmed.ncbi.nlm.nih.gov/23447019/.
- Steinbach K, Vincenti I, Merkler D. Resident-Memory T Cells in Tissue-Restricted Immune Responses: For Better or Worse? Front Immunol [Internet]. 2018 Nov 30 [cited 2024 May 14];9(NOV). Available from: https://pubmed.ncbi.nlm.nih.gov/30555489/.
- Boniface K, Jacquemin C, Darrigade AS, Dessarthe B, Martins C, Boukhedouni N, et al. Vitiligo Skin Is Imprinted with Resident Memory CD8 T Cells Expressing CXCR3. J Invest Dermatol [Internet]. 2018 Feb 1 [cited 2024 May 14];138(2):355–64. Available from: https://pubmed.ncbi.nlm.nih.gov/28927891/.
- Frisoli ML, Essien K, Harris JE. Vitiligo: Mechanisms of Pathogenesis and Treatment. Annu Rev Immunol [Internet]. 2020 Apr 26 [cited 2023 Nov 7];38:621–48. Available from: https://pubmed.ncbi.nlm.nih.gov/32017656/.
- Bae JM, Jung HM, Hong BY, Lee JH, Choi WJ, Lee JH, et al. Phototherapy for Vitiligo: A Systematic Review and Meta-analysis. JAMA Dermatol [Internet]. 2017 Jul 1 [cited 2023 Nov 7];153(7):666. Available from: /pmc/articles/PMC5817459/.
- Yones SS, Palmer RA, Garibaldinos TM, Hawk JLM. Randomized double-blind trial of treatment of vitiligo: efficacy of psoralen-UV-A therapy vs Narrowband-UV-B therapy. Arch Dermatol [Internet]. 2007 May [cited 2023 Nov 7];143(5):578–84. Available from: https://pubmed.ncbi.nlm.nih.gov/17519217/.
- Parsad D, Kanwar AJ, Kumar B. Psoralen-ultraviolet A vs. narrow-band ultraviolet B phototherapy for the treatment of vitiligo. J Eur Acad Dermatol Venereol [Internet]. 2006 Feb [cited 2023 Nov 7];20(2):175–7. Available from: https://pubmed.ncbi.nlm.nih.gov/16441626/.
- Bhatnagar A, Kanwar AJ, Parsad D, De D. Comparison of systemic PUVA and NB-UVB in the treatment of vitiligo: an open prospective study. Journal of the European Academy of Dermatology and Venereology [Internet]. 2007 May 1 [cited 2023 Nov 7];21(5):638–42. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/j.1468-3083.2006.02035.x.
- Nicolaidou E, Antoniou C, Stratigos A, Katsambas AD. Narrowband ultraviolet B phototherapy and 308-nm excimer laser in the treatment of vitiligo: A review. J Am Acad Dermatol. 2009 Mar 1;60(3):470–7. [CrossRef]
- Esmat S, Hegazy RA, Shalaby S, Chu-Sung Hu S, Lan CCE. Phototherapy and Combination Therapies for Vitiligo. Dermatol Clin [Internet]. 2017 Apr 1 [cited 2023 Nov 7];35(2):171–92. Available from: https://pubmed.ncbi.nlm.nih.gov/28317527/.
- Taieb A, Alomar A, Böhm M, Dell’Anna ML, De Pase A, Eleftheriadou V, et al. Guidelines for the management of vitiligo: the European Dermatology Forum consensus. Br J Dermatol [Internet]. 2013 Jan [cited 2023 Nov 7];168(1):5–19. Available from: https://pubmed.ncbi.nlm.nih.gov/22860621/.
- Cavalié M, Ezzedine K, Fontas E, Montaudié H, Castela E, Bahadoran P, et al. Maintenance therapy of adult vitiligo with 0.1% tacrolimus ointment: a randomized, double blind, placebo-controlled study. J Invest Dermatol [Internet]. 2015 Apr 20 [cited 2023 Nov 7];135(4):970–4. Available from: https://pubmed.ncbi.nlm.nih.gov/25521460/.
- Manga P, Elbuluk N, Orlow SJ. Recent advances in understanding vitiligo. F1000Res [Internet]. 2016 [cited 2023 Oct 28];5. Available from: /pmc/articles/PMC5017284/.
- Swope VB, Abdel-Malek Z, Kassem LM, Nordlund JJ. Interleukins 1 alpha and 6 and tumor necrosis factor-alpha are paracrine inhibitors of human melanocyte proliferation and melanogenesis. J Invest Dermatol [Internet]. 1991 [cited 2024 Jan 3];96(2):180–5. Available from: https://pubmed.ncbi.nlm.nih.gov/1899443/.
- Mihara M, Hashizume M, Yoshida H, Suzuki M, Shiina M. IL-6/IL-6 receptor system and its role in physiological and pathological conditions. Clin Sci (Lond) [Internet]. 2012 Feb [cited 2024 Jan 1];122(4):143–59. Available from: https://pubmed.ncbi.nlm.nih.gov/22029668/.
- De A, Choudhary N, Sil A, Sarda A, Raja AHH. A Cross-Sectional Study of the Levels of Cytokines IL-6, TNF-α, and IFN-γ in Blood and Skin (Lesional and Uninvolved) of Vitiligo Patients and their Possible Role as Biomarkers. Indian J Dermatol [Internet]. 2023 [cited 2023 Oct 22];68(1):67. Available from: /pmc/articles/PMC10162755/.
- Karagün E, Baysak S. Levels of TNF-α, IL-6, IL-17, IL-37 cytokines in patients with active vitiligo. Aging Male [Internet]. 2020 [cited 2023 Nov 23];23(5):1487–92. Available from: https://pubmed.ncbi.nlm.nih.gov/33191834/.
- Abdallah M, El-Mofty M, Anbar T, Rasheed H, Esmat S, Al-Tawdy A, et al. CXCL-10 and Interleukin-6 are reliable serum markers for vitiligo activity: A multicenter cross-sectional study. Pigment Cell Melanoma Res [Internet]. 2018 Mar 1 [cited 2023 Oct 22];31(2):330–6. Available from: https://pubmed.ncbi.nlm.nih.gov/29094481/.
- Sushama S, Dixit N, Gautam RK, Arora P, Khurana A, Anubhuti A. Cytokine profile (IL-2, IL-6, IL-17, IL-22, and TNF-α) in vitiligo-New insight into pathogenesis of disease. J Cosmet Dermatol [Internet]. 2019 Feb 1 [cited 2023 Oct 22];18(1):337–41. Available from: https://pubmed.ncbi.nlm.nih.gov/29504235/.
- Kuet K, Goodfield M. Multiple halo naevi associated with tocilizumab. Clin Exp Dermatol [Internet]. 2014 [cited 2023 Oct 23];39(6):717–9. Available from: https://pubmed.ncbi.nlm.nih.gov/24986573/.
- Bunker CB, Manson J. Vitiligo remitting with tocilizumab. J Eur Acad Dermatol Venereol [Internet]. 2019 Jan 1 [cited 2023 Oct 22];33(1):e20. Available from: https://pubmed.ncbi.nlm.nih.gov/29888453/.
- Nishimoto N, Terao K, Mima T, Nakahara H, Takagi N, Kakehi T. Mechanisms and pathologic significances in increase in serum interleukin-6 (IL-6) and soluble IL-6 receptor after administration of an anti-IL-6 receptor antibody, tocilizumab, in patients with rheumatoid arthritis and Castleman disease. Blood [Internet]. 2008 Nov 15 [cited 2023 Oct 23];112(10):3959–64. Available from: https://pubmed.ncbi.nlm.nih.gov/18784373/.
- Choong DJ, Tan E. Does tocilizumab have a role in dermatology? A review of clinical applications, its adverse side effects and practical considerations. Dermatol Ther. 2021 Jul 1;34(4).
- Jabri B, Abadie V. IL-15 functions as a danger signal to regulate tissue-resident T cells and tissue destruction. Nature Reviews Immunology 2015 15:12 [Internet]. 2015 Nov 16 [cited 2024 May 16];15(12):771–83. Available from: https://www.nature.com/articles/nri3919.
- Tokura Y, Phadungsaksawasdi P, Kurihara K, Fujiyama T, Honda T. Pathophysiology of Skin Resident Memory T Cells. Front Immunol [Internet]. 2020 Feb 3 [cited 2024 May 16];11:1. Available from: /pmc/articles/PMC7901930/.
- Chen X, Guo W, Chang Y, Chen J, Kang P, Yi X, et al. Oxidative stress-induced IL-15 trans-presentation in keratinocytes contributes to CD8+ T cells activation via JAK-STAT pathway in vitiligo. Free Radic Biol Med [Internet]. 2019 Aug 1 [cited 2024 May 16];139:80–91. Available from: https://pubmed.ncbi.nlm.nih.gov/31078730/.
- Richmond JM, Strassner JP, Zapata LZ, Garg M, Riding RL, Refat MA, et al. Antibody blockade of IL-15 signaling has the potential to durably reverse vitiligo. Sci Transl Med [Internet]. 2018 Jul 18 [cited 2024 May 16];10(450):7710. Available from: https://www.science.org/doi/10.1126/scitranslmed.aam7710.
- Zelová H, Hošek J. TNF-α signalling and inflammation: interactions between old acquaintances. Inflamm Res [Internet]. 2013 Jul [cited 2024 Jan 1];62(7):641–51. Available from: https://pubmed.ncbi.nlm.nih.gov/23685857/.
- Ahmed R, Sharif D, Jaf M, Amin DM. Effect of TNF-α −308G/A (rs1800629) Promoter Polymorphism on the Serum Level of TNF-α Among Iraqi Patients with Generalized Vitiligo. Clin Cosmet Investig Dermatol [Internet]. 2020 [cited 2024 Jan 3];13:825. Available from: /pmc/articles/PMC7671505/.
- Qi F, Liu F, Gao L. Janus Kinase Inhibitors in the Treatment of Vitiligo: A Review. Front Immunol [Internet]. 2021 Nov 18 [cited 2023 Nov 3];12. Available from: /pmc/articles/PMC8636851/.
- Yang X, Yan L, Ha D, Qu L, Liu L, Tao Y. Changes in sICAM-1 and GM-CSF levels in skin tissue fluid and expression of IL-6, IL-17 and TNF-α in blood of patients with vitiligo. Exp Ther Med [Internet]. 2019 Nov 7 [cited 2023 Oct 21];17(1). Available from: https://pubmed.ncbi.nlm.nih.gov/30651813/.
- Wakabayashi T, Hosohata K, Oyama S, Inada A, Ueno S, Kambara H, et al. Comparison of Adverse Event Profiles of Tumor Necrosis Factor-Alfa Inhibitors: Analysis of a Spontaneous Reporting Database. Ther Clin Risk Manag [Internet]. 2020 [cited 2024 Jan 1];16:741. Available from: /pmc/articles/PMC7439489/.
- Webb KC, Tung R, Winterfield LS, Gottlieb AB, Eby JM, Henning SW, et al. Tumour necrosis factor-a inhibition can stabilize disease in progressive vitiligo. British Journal of Dermatology [Internet]. 2015 [cited 2023 Oct 22]; Available from: https://academic.oup.com/bjd/article/173/3/641/6627485.
- Ramírez-Hernández M, Marras C, Martínez-Escribano JA. Infliximab-induced vitiligo. Dermatology [Internet]. 2005 [cited 2023 Oct 22];210(1):79–80. Available from: https://pubmed.ncbi.nlm.nih.gov/15604556/.
- Posada C, Flórez Á, Batalla A, Alcázar JJ, Carpio D. Vitiligo during Treatment of Crohn’s Disease with Adalimumab: Adverse Effect or Co-Occurrence? Case Rep Dermatol [Internet]. 2011 Jan [cited 2023 Oct 22];3(1):28–31. Available from: https://pubmed.ncbi.nlm.nih.gov/21931575/.
- Phan K, Charlton O, Smith SD. New onset vitiligo in a patient with hidradenitis suppurativa treated with adalimumab. Dermatol Ther [Internet]. 2020 May 1 [cited 2023 Oct 22];33(3). Available from: https://pubmed.ncbi.nlm.nih.gov/32239739/.
- Rigopoulos D, Gregoriou S, Larios G, Moustou E, Belayeva-Karatza E, Kalogeromitros D. Etanercept in the treatment of vitiligo. Dermatology [Internet]. 2007 Jun [cited 2023 Oct 22];215(1):84–5. Available from: https://pubmed.ncbi.nlm.nih.gov/17587849/.
- Campanati A, Giuliodori K, Ganzetti G, Liberati G, Offidani AM. A patient with psoriasis and vitiligo treated with etanercept. Am J Clin Dermatol [Internet]. 2010 [cited 2023 Oct 22];11 Suppl 1(SUPPL. 1):46–8. Available from: https://pubmed.ncbi.nlm.nih.gov/20586509/.
- Bae JM, Kim M, Lee HH, Kim KJ, Shin H, Ju HJ, et al. Increased Risk of Vitiligo Following Anti-Tumor Necrosis Factor Therapy: A 10-Year Population-Based Cohort Study. Journal of Investigative Dermatology. 2018 Apr 1;138(4):768–74. [CrossRef]
- Li S, Kang P, Zhang W, Jian Z, Zhang Q, Yi X, et al. Activated NLR family pyrin domain containing 3 (NLRP3) inflammasome in keratinocytes promotes cutaneous T-cell response in patients with vitiligo. J Allergy Clin Immunol [Internet]. 2020 Feb 1 [cited 2024 May 16];145(2):632–45. Available from: https://pubmed.ncbi.nlm.nih.gov/31756352/.
- Gu R, Shi Y, Huang W, Lao C, Zou Z, Pan S, et al. Theobromine mitigates IL-1β-induced oxidative stress, inflammatory response, and degradation of type II collagen in human chondrocytes. Int Immunopharmacol [Internet]. 2020 May 1 [cited 2024 May 16];82. Available from: https://pubmed.ncbi.nlm.nih.gov/32146317/.
- Bhardwaj S, Rani S, Srivastava N, Kumar R, Parsad D. Increased systemic and epidermal levels of IL-17A and IL-1β promotes progression of non-segmental vitiligo. Cytokine [Internet]. 2017 Mar 1 [cited 2024 May 16];91:153–61. Available from: https://pubmed.ncbi.nlm.nih.gov/28082234/.
- Marie J, Kovacs D, Pain C, Jouary T, Cota C, Vergier B, et al. Inflammasome activation and vitiligo/nonsegmental vitiligo progression. Br J Dermatol [Internet]. 2014 [cited 2024 May 16];170(4):816–23. Available from: https://pubmed.ncbi.nlm.nih.gov/24734946/.
- Cui D, Zhong F, Lin J, Wu Y, Long Q, Yang X, et al. Changes of circulating Th22 cells in children with hand, foot, and mouth disease caused by enterovirus 71 infection. Oncotarget [Internet]. 2016 Dec 21 [cited 2024 May 16];8(17):29370–82. Available from: https://www.oncotarget.com/article/14083/text/.
- Dong J, An X, Zhong H, Wang Y, Shang J, Zhou J. Interleukin-22 participates in the inflammatory process of vitiligo. Oncotarget [Internet]. 2017 Dec 12 [cited 2024 May 16];8(65):109161. Available from: /pmc/articles/PMC5752511/.
- Markota A, Endres S, Kobold S. Targeting interleukin-22 for cancer therapy. Hum Vaccin Immunother [Internet]. 2018 May 9 [cited 2024 Jun 3];14(8):2012. Available from: /pmc/articles/PMC6149728/.
- Singh RK, Lee KM, Vujkovic-Cvijin I, Ucmak D, Farahnik B, Abrouk M, et al. The role of IL-17 in vitiligo: A review. Autoimmun Rev [Internet]. 2016 Apr 1 [cited 2024 Jan 1];15(4):397–404. Available from: https://pubmed.ncbi.nlm.nih.gov/26804758/.
- Belpaire A, van Geel N, Speeckaert R. From IL-17 to IFN-γ in inflammatory skin disorders: Is transdifferentiation a potential treatment target? Front Immunol [Internet]. 2022 Jul 28 [cited 2023 Oct 25];13. Available from: /pmc/articles/PMC9367984/.
- Vaccaro M, Cannavò SP, Imbesi S, Cristani M, Barbuzza O, Tigano V, et al. Increased serum levels of interleukin-23 circulating in patients with non-segmental generalized vitiligo. Int J Dermatol [Internet]. 2015 Jun 1 [cited 2023 Nov 21];54(6):672–4. Available from: https://pubmed.ncbi.nlm.nih.gov/25427848/.
- Bhardwaj S, Rani S, Srivastava N, Kumar R, Parsad D. Increased systemic and epidermal levels of IL-17A and IL-1β promotes progression of non-segmental vitiligo. Cytokine [Internet]. 2017 Mar 1 [cited 2023 Oct 21];91:153–61. Available from: https://pubmed.ncbi.nlm.nih.gov/28082234/.
- Bassiouny DA, Shaker O. Role of interleukin-17 in the pathogenesis of vitiligo. Clin Exp Dermatol [Internet]. 2011 Apr [cited 2023 Nov 15];36(3):292–7. Available from: https://pubmed.ncbi.nlm.nih.gov/21198791/.
- Basak PY, Adiloglu AK, Ceyhan AM, Tas T, Akkaya VB. The role of helper and regulatory T cells in the pathogenesis of vitiligo. J Am Acad Dermatol [Internet]. 2009 Feb [cited 2023 Nov 15];60(2):256–60. Available from: https://pubmed.ncbi.nlm.nih.gov/19022528/.
- Zhang L, Kang Y, Chen S, Wang L, Jiang M, Xiang L. Circulating CCL20: A potential biomarker for active vitiligo together with the number of Th1/17 cells. J Dermatol Sci [Internet]. 2019 Feb 1 [cited 2023 Oct 28];93(2):92–100. Available from: https://pubmed.ncbi.nlm.nih.gov/30655106/.
- Le Poole IC, Van Den Wijngaard RMJGJ, Westerhof W, Das PK. Presence of T cells and macrophages in inflammatory vitiligo skin parallels melanocyte disappearance. Am J Pathol [Internet]. 1996 Apr [cited 2023 Oct 21];148(4):1219. Available from: /pmc/articles/PMC1861531/?report=abstract.
- Basdeo SA, Cluxton D, Sulaimani J, Moran B, Canavan M, Orr C, et al. Ex-Th17 (Nonclassical Th1) Cells Are Functionally Distinct from Classical Th1 and Th17 Cells and Are Not Constrained by Regulatory T Cells. The Journal of Immunology [Internet]. 2017 Mar 15 [cited 2024 Jan 1];198(6):2249–59. Available from: https://dx.doi.org/10.4049/jimmunol.1600737. [CrossRef]
- Speeckaert R, Mylle S, van Geel N. IL-17A is not a treatment target in progressive vitiligo. Pigment Cell Melanoma Res [Internet]. 2019 Nov 1 [cited 2023 Oct 28];32(6):842–7. Available from: https://pubmed.ncbi.nlm.nih.gov/31063266/.
- Aboobacker S, Kurn H, Aboud AM Al. Secukinumab. Turkderm Turkish Archives of Dermatology and Venereology [Internet]. 2023 Jun 20 [cited 2023 Nov 15];56:52–4. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537091/.
- Palazzo G. Resolution of post-adalimumab vitiligo with secukinumab in a patient with psoriasis vulgaris. Oxf Med Case Reports [Internet]. 2020 [cited 2023 Oct 21];2020:13–6. Available from: https://academic.oup.com/omcr/article/2020/1/omz134/5721283.
- Persechino S, Giordano D, Magri F, Persechino F, Lepore A, Verde R, et al. Single Case Vitiligo with Progressive Repigmentation during Secukinumab Treatment in a Patient with Psoriatic Arthritis: A Case Report. Case Rep Dermatol [Internet]. 2021 [cited 2023 Oct 21];13:209–15. Available from: www.karger.com/cde.
- Kim JC, Lee ES. Progression of Pre-Existing Vitiligo during Secukinumab Treatment for Psoriasis. Ann Dermatol [Internet]. 2023 May 1 [cited 2023 Oct 21];35(Suppl 1):S117–21. Available from: https://doi.org/10.5021/ad.21.078. [CrossRef]
- Nieto-Benito LM, Baniandrés-Rodríguez O. New-Onset Vitiligo During Treatment with Secukinumab: Report of Two Cases and Review of the Literature. Clin Drug Investig [Internet]. 2020 Nov 1 [cited 2023 Oct 21];40(11):1089–91. Available from: https://link.springer.com/article/10.1007/s40261-020-00964-w.
- Bouzid S, Hammami-Ghorbel H, Chamli A, Aounti I, Daly W, Kochbati S, et al. Secukinumab-induced vitiligo: A new case report and review of the literature. Therapie [Internet]. 2022 [cited 2023 Oct 21]; Available from: https://pubmed.ncbi.nlm.nih.gov/36566160/.
- Raimondo A, Guglielmi G, Marino C, Ligrone L, Lembo S. Hair whitening in a patient with psoriasis on adalimumab reversed after switching to ixekizumab. JAAD Case Rep [Internet]. 2021 May 1 [cited 2024 Jan 1];11:51–3. Available from: https://pubmed.ncbi.nlm.nih.gov/33912637/.
- Eker H, Kaya İslamoğlu ZG, Demirbaş A. Vitiligo development in a patient with psoriasis vulgaris treated with ixekizumab. Dermatol Ther. 2022 Apr 1;35(4.
- Marasca C, Fornaro L, Martora F, Picone V, Fabbrocini G, Megna M. Onset of vitiligo in a psoriasis patient on ixekizumab. Dermatol Ther [Internet]. 2021 Sep 1 [cited 2024 Jan 1];34(5). Available from: https://pubmed.ncbi.nlm.nih.gov/34436817/.
- Pathmarajah P, Benjamin-Laing Z, Abdurrahman M, Grunova A, Sinclair C. Generalized vitiligo in a psoriatic patient treated with ixekizumab. Dermatol Ther [Internet]. 2022 Dec 1 [cited 2024 Jan 1];35(12). Available from: https://pubmed.ncbi.nlm.nih.gov/36181252/.
- Maddur MS, Miossec P, Kaveri S V., Bayry J. Th17 cells: biology, pathogenesis of autoimmune and inflammatory diseases, and therapeutic strategies. Am J Pathol [Internet]. 2012 Jul [cited 2023 Nov 21];181(1):8–18. Available from: https://pubmed.ncbi.nlm.nih.gov/22640807/.
- Duvallet E, Semerano L, Assier E, Falgarone G, Boissier MC. Interleukin-23: a key cytokine in inflammatory diseases. Ann Med [Internet]. 2011 Nov [cited 2023 Nov 21];43(7):503–11. Available from: https://pubmed.ncbi.nlm.nih.gov/21585245/.
- Verstockt B, Salas A, Sands BE, Abraham C, Leibovitzh H, Neurath MF, et al. IL-12 and IL-23 pathway inhibition in inflammatory bowel disease. Nat Rev Gastroenterol Hepatol [Internet]. 2023 Jul 1 [cited 2023 Oct 22];20(7):433–46. Available from: https://pubmed.ncbi.nlm.nih.gov/37069321/.
- Weaver CT, Elson CO, Fouser LA, Kolls JK. The Th17 Pathway and Inflammatory Diseases of the Intestines, Lungs, and Skin. https://doi.org/101146/annurev-pathol-011110-130318[Internet]. 2013 Jan 24 [cited 2023 Oct 22];8:477–512. Available from: https://www.annualreviews.org/doi/abs/10.1146/annurev-pathol-011110-130318.
- Jerjen R, Moodley A, Sinclair R. Repigmentation of acrofacial vitiligo with subcutaneous tildrakizumab. Australas J Dermatol [Internet]. 2020 Nov 1 [cited 2023 Oct 22];61(4):e446–8. Available from: https://pubmed.ncbi.nlm.nih.gov/32441048/.
- Miyoshi J, Matsuura M, Hisamatsu T. Safety evaluation of ustekinumab for moderate-to-severe ulcerative colitis. Expert Opin Drug Saf [Internet]. 2022 [cited 2024 Jan 1];21(1):1–8. Available from: https://pubmed.ncbi.nlm.nih.gov/34511011/.
- Rawal S, Kianian S, Guo W, Marquez J, Ayasse M, Siamas KA, et al. Alternative uses of ustekinumab for non-indicated dermatological conditions: a systematic review. Arch Dermatol Res [Internet]. 2022 Aug 1 [cited 2023 Oct 21];314(6):503–14. Available from: https://pubmed.ncbi.nlm.nih.gov/34156549/.
- Elkady A, Bonomo L, Amir Y, Vekaria AS, Guttman-Yassky E, York N. Effective use of ustekinumab in a patient with concomitant psoriasis, vitiligo, and alopecia areata. [cited 2023 Oct 21]. [CrossRef]
- L MB, K B, G C, A K, F M, H M, et al. New-onset vitiligo and progression of pre-existing vitiligo during treatment with biological agents in chronic inflammatory diseases. J Eur Acad Dermatol Venereol [Internet]. 2017 [cited 2023 Oct 19];31(1). Available from: https://pubmed.ncbi.nlm.nih.gov/27291924/.
- Anthony N, Bourneau-martin D, Ghamrawi S, Lagarce L, Babin M, Briet M. Drug-induced vitiligo: a case/non-case study in Vigibase® , the WHO pharmacovigilance database. Fundam Clin Pharmacol [Internet]. 2020 Dec 1 [cited 2023 Oct 19];34(6):736–42. Available from: https://pubmed.ncbi.nlm.nih.gov/32246859/.
- Montilla Francisco Gó mez-García Pedro J Gó mez-Arias Jesú Gay-Mimbrera Jorge Hernández-Parada Beatriz Isla-Tejera Juan Ruano AM. Scoping Review on the Use of Drugs Targeting JAK/ STAT Pathway in Atopic Dermatitis, Vitiligo, and Alopecia Areata. Dermatol Ther (Heidelb) [Internet]. 2019 [cited 2023 Nov 5];9. Available from: https://doi.org/10.6084/.
- Tang Q, Sousa J, Echeverria D, Fan X, Hsueh YC, Afshari K, et al. RNAi-based modulation of IFN-γ signaling in skin. Molecular Therapy [Internet]. 2022 Aug 8 [cited 2023 Nov 5];30(8):2709. Available from: /pmc/articles/PMC9372319/.
- Rashighi M, Agarwal P, Richmond JM, Harris TH, Dresser K, Su MW, et al. CXCL10 is critical for the progression and maintenance of depigmentation in a mouse model of vitiligo. Sci Transl Med [Internet]. 2014 Feb 12 [cited 2023 Nov 15];6(223). Available from: https://pubmed.ncbi.nlm.nih.gov/24523323/.
- Liu H, Wang Y, Le Q, Tong J, Wang H. The IFN-γ-CXCL9/CXCL10-CXCR3 axis in vitiligo: pathological mechanism and treatment. Eur J Immunol [Internet]. 2023 Nov 8 [cited 2023 Nov 15]; Available from: https://pubmed.ncbi.nlm.nih.gov/37937817/.
- Maouia A, Sormani L, Youssef M, Helal AN, Kassab A, Passeron T. Differential expression of CXCL9, CXCL10, and IFN-γ in vitiligo and alopecia areata patients. Pigment Cell Melanoma Res [Internet]. 2017 Mar 1 [cited 2024 May 14];30(2):259–61. Available from: https://pubmed.ncbi.nlm.nih.gov/27863059/.
- Yu HS, Chang KL, Yu CL, Li HF, Wu MT, Wu CS, et al. Alterations in IL-6, IL-8, GM-CSF, TNF-alpha, and IFN-gamma release by peripheral mononuclear cells in patients with active vitiligo. J Invest Dermatol [Internet]. 1997 [cited 2024 May 16];108(4):527–9. Available from: https://pubmed.ncbi.nlm.nih.gov/9077486/.
- Rashighi M, Harris JE. Interfering with the IFN-γ/CXCL10 pathway to develop new targeted treatments for vitiligo. Ann Transl Med [Internet]. 2015 Dec 1 [cited 2024 Jan 4];3(21). Available from: https://pubmed.ncbi.nlm.nih.gov/26734651/.
- Nada HR, El Sharkawy DA, Elmasry MF, Rashed LA, Mamdouh S. Expression of Janus Kinase 1 in vitiligo & psoriasis before and after narrow band UVB: a case-control study. Arch Dermatol Res [Internet]. 2018 Jan 1 [cited 2023 Nov 3];310(1):39–46. Available from: https://pubmed.ncbi.nlm.nih.gov/29127481/.
- Abdel Motaleb AA, Tawfik YM, El-Mokhtar MA, Elkady S, El-Gazzar AF, ElSayed SK, et al. Cutaneous JAK Expression in Vitiligo. J Cutan Med Surg [Internet]. 2021 Mar 1 [cited 2023 Nov 3];25(2):157–62. Available from: https://pubmed.ncbi.nlm.nih.gov/33174479/.
- Boukhedouni N, Martins C, Darrigade AS, Drullion C, Rambert J, Barrault C, et al. Type-1 cytokines regulate MMP-9 production and E-cadherin disruption to promote melanocyte loss in vitiligo. JCI Insight [Internet]. 2020 Jun 4 [cited 2024 May 14];5(11). Available from: https://pubmed.ncbi.nlm.nih.gov/32369451/.
- Rosmarin D, Passeron T, Pandya AG, Grimes P, Harris JE, Desai SR, et al. Two Phase 3, Randomized, Controlled Trials of Ruxolitinib Cream for Vitiligo. N Engl J Med [Internet]. 2022 Oct 20 [cited 2023 Nov 5];387(16):1445–55. Available from: https://pubmed.ncbi.nlm.nih.gov/36260792/.
- Howell MD, Kuo FI, Smith PA. Targeting the Janus Kinase Family in Autoimmune Skin Diseases. Front Immunol. 2019 Oct 9;10:490313.
- Study Results | A Study to Evaluate the Mechanism of Action of Ruxolitinib Cream in Subjects With Vitiligo (TRuE-V MOA) | ClinicalTrials.gov [Internet]. [cited 2024 Jan 1]. Available from: https://clinicaltrials.gov/study/NCT04896385?tab=results.
- Tavoletti G, Avallone G, Conforti C, Roccuzzo G, Maronese CA, Mattioli MA, et al. Topical ruxolitinib: A new treatment for vitiligo. Journal of the European Academy of Dermatology and Venereology [Internet]. 2023 Nov 1 [cited 2023 Nov 5];37(11):2222–30. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/jdv.19162.
- Ajayi S, Becker H, Reinhardt H, Engelhardt M, Zeiser R, von Bubnoff N, et al. Ruxolitinib. Recent Results Cancer Res [Internet]. 2018 [cited 2023 Nov 18];212:119–32. Available from: https://pubmed.ncbi.nlm.nih.gov/30069628/.
- Phan K, Phan S, Shumack S, Gupta M. Repigmentation in vitiligo using janus kinase (JAK) inhibitors with phototherapy: systematic review and Meta-analysis. Journal of Dermatological Treatment [Internet]. 2022 [cited 2023 Nov 5];33(1):173–7. Available from: https://www.tandfonline.com/doi/abs/10.1080/09546634.2020.1735615.
- Janus Kinase and Tyrosine Kinase Inhibitors in Dermatology [Internet]. [cited 2023 Nov 5]. Available from: https://www.skintherapyletter.com/dermatology/janus-tyrosine-kinase-inhibitors-review/.
- Liu LY, Strassner JP, Refat MA, Harris JE, King BA. Repigmentation in vitiligo using the Janus kinase inhibitor tofacitinib may require concomitant light exposure. J Am Acad Dermatol [Internet]. 2017 Oct 1 [cited 2023 Nov 5];77(4):675-682.e1. Available from: https://pubmed.ncbi.nlm.nih.gov/28823882/.
- Craiglow BG, King BA. Tofacitinib Citrate for the Treatment of Vitiligo: A Pathogenesis-Directed Therapy. JAMA Dermatol [Internet]. 2015 Oct 1 [cited 2023 Nov 5];151(10):1110–2. Available from: https://pubmed.ncbi.nlm.nih.gov/26107994/.
- Joshipura D, Plotnikova N, Goldminz A, Deverapalli S, Turkowski Y, Gottlieb A, et al. Importance of light in the treatment of vitiligo with JAK-inhibitors. J Dermatolog Treat [Internet]. 2018 Jan 2 [cited 2023 Nov 5];29(1):98–9. Available from: https://pubmed.ncbi.nlm.nih.gov/28581823/.
- Kim SR, Heaton H, Liu LY, King BA. Rapid Repigmentation of Vitiligo Using Tofacitinib Plus Low-Dose, Narrowband UV-B Phototherapy. JAMA Dermatol [Internet]. 2018 Mar 1 [cited 2023 Nov 5];154(3):370–1. Available from: https://pubmed.ncbi.nlm.nih.gov/29387870/.
- Zhang J, Qi F, Dong J, Tan Y, Gao L, Liu F. Application of Baricitinib in Dermatology. J Inflamm Res [Internet]. 2022 [cited 2023 Nov 5];15:1935. Available from: /pmc/articles/PMC8939862/.
- Dong J, Huang X, Ma LP, Qi F, Wang SN, Zhang ZQ, et al. Baricitinib is Effective in Treating Progressing Vitiligo in vivo and in vitro. Dose Response [Internet]. 2022 Apr 1 [cited 2023 Nov 5];20(2). Available from: https://pubmed.ncbi.nlm.nih.gov/35663493/.
- Diotallevi F, Gioacchini H, De Simoni E, Marani A, Candelora M, Paolinelli M, et al. Vitiligo, from Pathogenesis to Therapeutic Advances: State of the Art. Int J Mol Sci [Internet]. 2023 Mar 1 [cited 2024 Jan 18];24(5). Available from: https://pubmed.ncbi.nlm.nih.gov/36902341/.
- Ezzedine K, Peeva E, Yamaguchi Y, Cox LA, Banerjee A, Han G, et al. Efficacy and safety of oral ritlecitinib for the treatment of active nonsegmental vitiligo: A randomized phase 2b clinical trial. J Am Acad Dermatol [Internet]. 2023 Feb 1 [cited 2024 Jan 4];88(2):395–403. Available from: http://www.jaad.org/article/S0190962222029899/fulltext.
- Feng Y, Lu Y. Advances in vitiligo: Update on therapeutic targets. Front Immunol [Internet]. 2022 Aug 31 [cited 2024 Jan 18];13. Available from: /pmc/articles/PMC9471423/.
- Sardana K, Bathula S, Khurana A. Which is the Ideal JAK Inhibitor for Alopecia Areata – Baricitinib, Tofacitinib, Ritlecitinib or Ifidancitinib - Revisiting the Immunomechanisms of the JAK Pathway. Indian Dermatol Online J [Internet]. 2023 Jul 1 [cited 2024 Jan 18];14(4):465. Available from: /pmc/articles/PMC10373824/.
- Liu H, Wang Y, Le Q, Tong J, Wang H. The IFN-γ-CXCL9/CXCL10-CXCR3 axis in vitiligo: Pathological mechanism and treatment. Eur J Immunol [Internet]. 2024 Apr 1 [cited 2024 May 17];54(4):2250281. Available from: https://onlinelibrary.wiley.com/doi/full/10.1002/eji.202250281.
- Su X, Luo R, Ruan S, Zhong Q, Zhuang Z, Xiao Z, et al. Efficacy and tolerability of oral upadacitinib monotherapy in patients with recalcitrant vitiligo. J Am Acad Dermatol [Internet]. 2023 Dec 1 [cited 2024 Mar 11];89(6):1257–9. Available from: https://pubmed.ncbi.nlm.nih.gov/37516357/.
- Coffey G, Betz A, DeGuzman F, Pak Y, Inagaki M, Baker DC, et al. The novel kinase inhibitor PRT062070 (Cerdulatinib) demonstrates efficacy in models of autoimmunity and B-cell cancer. J Pharmacol Exp Ther [Internet]. 2014 Dec 1 [cited 2024 May 17];351(3):538–48. Available from: https://pubmed.ncbi.nlm.nih.gov/25253883/.
- Ma J, Xing W, Coffey G, Dresser K, Lu K, Guo A, et al. Cerdulatinib, a novel dual SYK/JAK kinase inhibitor, has broad anti-tumor activity in both ABC and GCB types of diffuse large B cell lymphoma. Oncotarget [Internet]. 2015 Dec 12 [cited 2024 May 14];6(41):43881. Available from: /pmc/articles/PMC4791274/.
- Yagi K, Ishida Y, Otsuka A, Kabashima K. Two cases of vitiligo vulgaris treated with topical Janus kinase inhibitor delgocitinib. Australas J Dermatol [Internet]. 2021 Aug 1 [cited 2024 May 14];62(3):433–4. Available from: https://pubmed.ncbi.nlm.nih.gov/33667323/.
- Skurkovich S, Skurkovich B, Kelly J. Anticytokine therapy, particularly anti-IFN-gamma, in Th1-mediated autoimmune diseases. Expert Rev Clin Immunol [Internet]. 2005 May [cited 2024 May 17];1(1):11–25. Available from: https://pubmed.ncbi.nlm.nih.gov/20477651/.
- Harris JE, Harris TH, Weninger W, Wherry EJ, Hunter CA, Turka LA. A mouse model of vitiligo with focused epidermal depigmentation requires IFN-γ for autoreactive CD8+ T-cell accumulation in the skin. J Invest Dermatol [Internet]. 2012 [cited 2024 May 16];132(7):1869–76. Available from: https://pubmed.ncbi.nlm.nih.gov/22297636/.
- Rashighi M, Agarwal P, Richmond JM, Harris TH, Dresser K, Su MW, et al. CXCL10 is critical for the progression and maintenance of depigmentation in a mouse model of vitiligo. Sci Transl Med [Internet]. 2014 Feb 12 [cited 2024 May 17];6(223). Available from: https://pubmed.ncbi.nlm.nih.gov/24523323/.
- Richmond JM, Masterjohn E, Chu R, Tedstone J, Youd ME, Harris JE. CXCR3 Depleting Antibodies Prevent and Reverse Vitiligo in Mice. J Invest Dermatol [Internet]. 2017 Apr 1 [cited 2024 May 17];137(4):982–5. Available from: https://pubmed.ncbi.nlm.nih.gov/28126463/.
- Nowroozpoor Dailami K, Hosseini A, Rahmatpour Rokni G, Saeedi M, Morteza-Semnani K, Sadeghi Z, et al. Efficacy of topical latanoprost in the treatment of eyelid vitiligo: A randomized, double-blind clinical trial study. Dermatol Ther [Internet]. 2020 Jan 1 [cited 2024 Jun 24];33(1). Available from: https://pubmed.ncbi.nlm.nih.gov/31758835/.
- Lim HW, Grimes PE, Agbai O, Hamzavi I, Henderson M, Haddican M, et al. Afamelanotide and narrowband UV-B phototherapy for the treatment of vitiligo: a randomized multicenter trial. JAMA Dermatol [Internet]. 2015 Jan 1 [cited 2024 Jun 25];151(1):42–50. Available from: https://pubmed.ncbi.nlm.nih.gov/25230094/.
- Elrewiny EM, Shawky A, Mohamed SFF, Ammar AM, Mansour M, Rageh MA. Intralesional methotrexate in the treatment of localized vitiligo: A pilot study. Australasian Journal of Dermatology [Internet]. 2023 Aug 1 [cited 2024 Jun 25];64(3):e207–11. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/ajd.14071.

Table 1.
Targets and effects of drugs used in the treatment of vitiligo.
| Drug | Target | Effect |
|---|---|---|
| Tocilizumab [27,28,29] | IL-6 receptor | Lack of effectiveness, new vitiligo lesions (case reports) |
| anti-CD122 [33] | IL-15 | Repigmentation of vitiligo lesions (mice model) |
| IL-15 monoclonal antibody (AMG 714) [34] | IL-15 | Ongoing phase IIa clinical trial |
| Adalimumab Infliximab Etanercept [38,39,40,41,42,43,44,45] |
TNF- alpha | Increased risk of new-onset vitiligo, controversial therapeutic results (case reports, cohort study) |
| - | IL-1β | - |
| IL-22 neutralizing antibody [53] | IL-22 | - |
| Ustekinumab [79,80,81] | IL-12 and IL-23 | New vitiligo lesions, controversial therapeutic results (case reports, case/non-case study) |
| Secukinumab [64,65,66,67,68,69] Ixekizumab [71,72,73] |
IL-17A | Appearance of new vitiligo lesions (case reports) |
| Tildrakizumab [78] | IL-23 | Insufficient studies (case report) |
| Ruxolitinib [96,97,98,99] | JAK1/2 | Good clinical response, repigmentation of vitiligo lesions (approved by FDA and EMA in adults and adolescents from 12 years of age with non-segmental vitiligo) |
| Tofacitinib [102,103,104] | JAK1/2/3 | Repigmentation of vitiligo lesions, nbUVB may increase clinical effect (case reports, retrospective case series) |
| Baricitinib [36,105,106] | JAK1/2 | Repigmentation of vitiligo lesions, nbUVB may increase clinical effect (phase II clinical trial) |
| Ritlecitinib [108,110] |
JAK3/TEC | Repigmentation of vitiligo (phase III clinical trial) |
| Ifidancitinib [109,110] | JAK1/3 | Repigmentation of vitiligo lesions (phase II clinical trial) |
| Brepocytinib [111] | JAK1/TYK | No results (phase II clinical trial) |
| Upadacitinib [112] | JAK1 | Repigmentation of vitiligo lesions (phase III clinical trial) |
| Cerdulatynib [113,114] | JAK1/3 | No results (phase II clinical trial) |
| Delgocitinib [115] | JAK1/2/3, TYK2 | Good clinical response (case reports) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



