Submitted:
08 July 2024
Posted:
10 July 2024
You are already at the latest version
Abstract
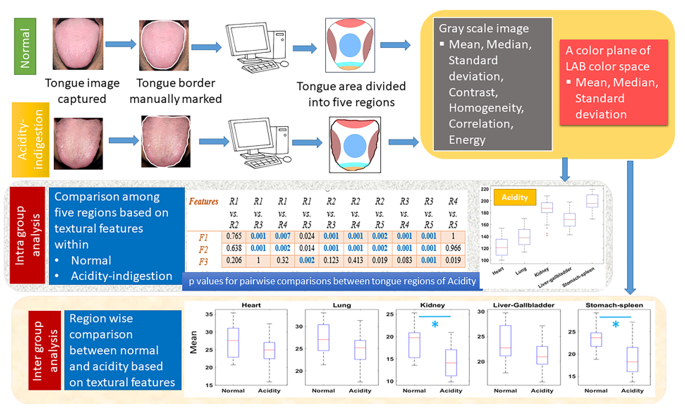
Introduction: In Traditional Chinese Medicine (TCM), tongue diagnosis plays an important role. Besides shape, colour and textural attributes of tongue regions have significance due to their association with different organs (viz. heart, lung, kidney-bladder, liver-gallbladder and stomach-spleen) in health and disease. Although numerous quantitative methods have been proposed to reduce inter and intra observer variability in tongue diagnosis, almost all of them considered only global colour/ textural features i.e. from entire body of tongue. In this work, regional colour and texture information of tongue have been analysed for healthy subjects (NOM) and patients suffering from chronic acidity-indigestion (ACD). Methods: Tongue boundaries are marked manually in each image and then tongue bodies are automatically partitioned into five regions linked with said internal organs. Rough assessments of regions’ boundaries are obtained from literature and then they are fine-tuned according to experts’ advice. As boundaries are not well defined, regions near the common boundary of two or more organs, are not assigned to any organ. Several first and second order statistical features based on grey scale intensities and a* values of LAB colour space (indicative of redness) have been extracted from five different regions of tongue images. Intragroup analysis using Wilcoxon signed rank test compared different regions within individual study group. Additionally, intergroup analysis using Wilcoxon rank sum test compared tongues of NOM with ACD for each region separately. Results: Intragroup analysis reveals a* values are statistically different (p<0.01) between stomach-spleen and liver-gallbladder regions for ACD while no significant change of a* are noted between these regions of normal tongue. It was found from intergroup analysis that correlation (one of the second order texture features extracted from grey scale images) of heart region has significantly decreased while correlation of kidney, liver-gallbladder and stomach-spleen regions significantly increased from NOM to ACD. Conclusion: This study sheds light on importance of inclusion of regional textural analysis of tongue in quantitative studies and can be applied to automated tongue diagnosis for other diseases.
Keywords:
TCM based tongue diagnosis
; tongue colour
; local texture
; chronic acidity
; GLCM
; inter and intragroup analysis.
1. Introduction
The tongue, a complex multifunctional organ, helps humans in chewing, swallowing food and drink along with perceiving taste. As the safety and quality of the oral cavity’s content is transmitted to the central nervous system through the tongue, it is a sensory organ [1]. Tongue is also a motor organ as it aids in speech [1]. Tongue has a potential role in diagnostic practices of both modern and traditional medicines like Ayurveda [2], acupuncture cum Traditional Chinese Medicine (TCM) [3]. As per TCM, tongue is connected to different meridians and the internal organs of the body [4]. Thus, in TCM, tongue’s shape, colour and textural attributes are correlated with overall functional status of the body, vital organs as well as their pathological deviations [4,5,6]. This body of knowledge is known as the basis of tongue diagnosis [7,8,9]. Primarily the tongue body can be divided into five parts viz. tip of the tongue (represents heart and lung), centre (represents stomach and spleen), two sides (represents liver and gallbladder) and the back or the root (represents kidney, bladder, and intestines) [10].
Various tongue features can be treated as the pre-disease indicators even in absence of significant disease symptoms and thus these features can be utilized for preventive medicine and lifestyle adjustment [6]. However, in practice this domain knowledge being qualitative, suffers from subjectivity and inconsistency [11,12].There are several works which quantitatively studied alteration in tongue features from normal to disease conditions [4,7]. Variation of nine tongue features between early stage breast cancer patients and non-breast cancer individuals were studied through an automated tongue diagnosis system [13]. Features extracted from tongue images as well as tongue-coating microbiota was associated with the occurrence and development of gastritis [14]. Hsu et al., 2019 investigated discriminating tongue features to distinguish between type 2 diabetes mellitus from non-diabetes mellitus individuals [15]. In another work, differences of oral microbial profiles among different tongue coatings in chronic insomnia patients were studied [16]. Hence, computer-aided tongue diagnoses have a great potential to provide more reliable and objective health assessments. It can be noted that quantitative comparison of tongue in healthy persons and patients suffering from acidity- indigestion or gastroesophageal reflux disease are scarce [17,18]. In our previous work [17], the analysis done was mostly on categorical data describing different tongue features. Kainuma et al., 2019 analyzedcolour in L*a*b* colour space from four different points of tongue of patients suffering from gastroesophageal reflux disease [18].
Further, interpretable textural features like gray level co-occurrence matrix (GLCM), can provide information on the spatial arrangement of pixel intensities [19]. Thirunavukkarasu et al., 2020 compared GLCM features of diabetes mellitus patients and normal from infrared thermal imaging of tongue [20]. Textural changes especially second order statistics of tongue were not reported much especially in patients suffering from acidity. Additionally, global texture of the whole tongue can lose information about the local texture which is pivotal for quantitative studies. But, very few studies [18,21,22] have quantitatively elucidated the relations/differences between features extracted from different regions of tongue. Detailed analysis of the same may provide valuable clues about tongue of healthy persons and how relationships among different regions change in disease conditions.
In the current study, tongue images of two groups (normal and chronic acidity-indigestion) were captured in standard setting and first order statistics along with GLCM features were extracted from five different tongue regions corresponding to five organs. Then, five different regions of tongue were compared based on extracted textural features within each group as well as between two groups. To the best of our knowledge, this type of region based inter and intragroup analysis of tongue was not reported before.
2. Materials and Methods
2.1. Inclusion of Participants
Selection of normal healthy subjects (NOM) was done after taking full case history following definite history sheet as per TCM [23]. Tongue were also assessed visually by three experts following normal criteria of tongue as per TCM. Selection of patients suffering from acidity-indigestion (ACD) with or without other co morbidity like arthritis, diabetes, hypertension, insomnia etc. was done in same pattern like normal subjects taking full case history. All the patients suffered for at least two years from acidity. Routine examination of blood, stool, and urine was done to assess the general health condition of the subjects. All parameters were within normal range for selected normal subjects. Subjects were taken within the age limit of 18 to 65 years of both sex. Total 16 normal and 18 acidity-indigestion patients were selected for this work.
2.2. Tongue Image Acquisition
All the images were collected from image database of Indian Research Institute for Integrated Medicine (IRIIM), West Bengal, India. Images were captured in a fixed setting using Nikon Coolpix 990. The filming distance between the subject and the camera was kept constant. All volunteers gave informed consent before enrolling in the study.
Precautionary Measures Taken before Image Acquisition
Extension of the tongue: The participants were asked to look at the front horizontally in a sitting position. They were asked to extend their tongues outward and slightly downward, and the surface should be flat and not rolling. Care was taken not to have it extending outward by force lest its colour should be influenced. The image was taken within 10s of the presentation of the tongue.
Coating colour: The tongue coating can be coloured by certain food or drugs e.g., olives, plum or mulberries can make it yellow; smoking can make it grey, etc. Whenever the tongue coating did not accord with the disease condition, ask the patient about diet and medication so as to avoid any misunderstandings. The participants were asked to stop having betel leaf for at least 5-7 days and not to take any coloured food item prior image collection.
All the participants were asked to rinse their mouth with plain water before imaging collection.
Figure 1 shows one sample from each study group.
2.3. Partitioning of Tongue in Different Regions
Tongue boundaries were manually contoured in each image. Then the whole tongue was divided automatically into five regions correspond to five organs (heart, lung, kidney, liver-gallbladder and stomach-spleen) (Figure 2) according the rules described below. The dimensions of each region was initially chosen from literature [10,21,24] and then fine-tuned after discussing with experts. As the boundaries of different regions are not well defined, spaces were kept in between regions of two different organs (except heart and lung which did not have any space between them) according to experts’ advice.
X axis of image increases in right and Y axis increases downwards. If coordinate of A (upper left most corner point of bonding rectangle) is (x, y), then coordinates of other three corner points will be as follows: B (x, y+L), C (x+W, y+L) and D (x+W, y).
Let’s define middle_x=x+W/2
Boundaries of each region were drawn as per below rules:
Heart: Circumference of circle correspond to heart passes through B, C of bounding rectangle and a point having coordinate (middle_x, y+0.92L).
Lung: Circumference of circle correspond to lung passes through (x, y+0.92L), (x+W, y+0.92L) and (middle_x, y+0.84L).
Kidney: Circumference of circle correspond to kidney passes through (x+0.07W, y), (x+0.93W, y), (middle_x, y + 0.18L).
Liver-gallbladder: Y coordinate of three points on circumference of each of the two circles correspond to liver-gallbladders are (y+0.2L), (y+0.6L) and (y+0.84L). X coordinates of first and third points are the leftmost (for left circle) and rightmost (for right circle) x coordinate of the point on tongue body having y coordinates as (y+0.2L) and (y+0.84L) respectively. X coordinates of second point on left and right circle are (middle_x -0.7(middle_x -xg_l)) and (middle_x +0.7(middle_x-xg_l)) respectively where xg_l is the leftmost x coordinate of the point on tongue body having y coordinate as (y+0.6L).
Stomach-spleen: Two endpoints of the major axis of the ellipse correspond to stomach-spleen are (middle_x, y+0.25L) and (middle_x, y+0.75L). Two endpoints of the minor axis are (xs_l, y+0.4L) and (xs_r, y+0.4L) where xs_l=(middle_x -0.7(middle_x -xg_l) + 0.1W) and xs_r = (middle_x +0.7(middle_x-xg_l) − 0.1W).
2.4. Textural Feature Extraction
All the tongue images were converted to gray scale and CIE LAB space. As CIE LAB is more suitable to describe human colour perception [25] and a* (referred to as A colour plane hereafter) value is widely used in automated tongue diagnosis [22], A colour plane of tongue images were considered along with gray scale intensities for feature extraction. Positive a direction indicates shift towards red. Light reflection from saliva caused some pixels having high luminance [22]. These pixels should not be considered for feature extraction. For improving reliability, dynamic thresholds were chosen to remove outlier pixels. For each image, 5 and 95 percentiles of grey scale and a* values of whole tongue body were calculated and values lying within these ranges only were considered for feature extraction. This is especially required for GLCM study as outliers can significantly alter GLCM values by changing lowest and highest bin limits.
The Grey Level Co-occurrence Matrix (GLCM) method is a way of extracting second order statistical texture features by considering the relationship between adjacent pixels in the image. The matrix formulates co-occurrence frequencies of two neighbouring pixels (and ) to present relations at different distances, d, and directions, θ [19].In the present work, a distance d=1 and average of four directions of θ=0°, 45°, 90°, and 135° were used. Mean differences between 5 and 95 percentiles of grey scale values of whole tongue body considering all images was 110. To reduce the computational complexity and considering the grey scale span, four intensity bins had been considered. Bin limits for each image were dynamically defined based on 5 and 95 percentiles of grey scale values of that image. The following four GLCM features were used in this study.
Where and Let
Then
Seven features viz. mean, median, standard deviation, contrast, homogeneity, correlation and energy were extracted from each region of grey scale images.
Three features viz. mean, median and standard deviationof a* values were extracted from each region of tongue images. GLCM features were not considered as a* values of each tongue spanned a very narrow region i.e., average difference between 5 and 95 percentiles of a* values of whole tongue body considering all images was 25.
2.5. Statistical Analysis
Features were compared among different regions within each of the two study groups and between the two groups. Wilcoxon signed rank test and Wilcoxon rank sum test were used for intragroup and intergroup study respectively. p<0.01 was considered to be statistically significant.
3. Results and Discussion
Tongue diagnosis can be included as an auxiliary diagnosis to support the primary healthcare system [26]. But as tongue diagnosis in TCM suffers from subjectivity, several objective approaches have been proposed. Textural features including GLCM were extracted from tongue images to classify diabetes mellitus patients and healthy participants [27]. Further, colour of different regions of tongue provide information about different internal organs [21]. Consequently, computerized tongue diagnosis based on different regions of tongue might improve the diagnostic accuracy [22,28]. In this work, tongue images of normal and patients suffering from chronic acidity-indigestion were divided into five regions based on the method as described in section 2.3 (Figure 3).
In each of the below tables R1: Heart, R2: Lung, R3: Kidney, R4: Liver-Gallbladder R5: Stomach-spleen and F1: Mean, F2: Median, F3: Standard deviation, F4: Contrast, F5: Homogeneity, F6: Correlation, F7: Energy
3.1. Comparison of Textural Features among Different Regions of NOM Tongue
Table 1.1 shows that all the features were significantly different between heart and liver-gallbladder regions while no difference was observed between lung and liver-gallbladder based on grey scale values of normal tongue. Among all features, difference of only mean and median were noted between heart and kidney, heart and liver-gallbladder, lung and kidney. Correlation was significantly different between stomach-spleen (liver-gallbladder) and other organs except heart (lung). Although neither mean nor median was different between kidney and liver-gallbladder, correlation was different. Thus correlation has emerged as an important feature.
No feature was significantly different between heart and lung as well as liver-gallbladder and stomach regions when features were extracted from A colour plane of NOM tongue images (Table 1.2).
3.2. Comparison of Textural Features among Different Tongue Regions of Patients Suffered from Acidity-Indigestion
In contrast to normal, all seven features extracted from grey scale images of ACD tongue were different between heart and other four organs (Table 2.1). Similar to NOM, contrast and homogeneity did not differ between lung as well as kidney and each of liver-gallbladder and stomach-spleen region. Mean, median and correlation were different between all possible pairs. No differences of standard deviation and energy were noted only between lung and kidney.

Table 2.
1. p values @ 1% significance level showing the alterations between regions of ACD tongue images in grey scale.
Table 2.
1. p values @ 1% significance level showing the alterations between regions of ACD tongue images in grey scale.
| Features | R1 vs. R2 | R1 vs. R3 | R1 vs. R4 | R1 vs. R5 | R2 vs. R3 | R2 vs. R4 | R2 vs. R5 | R3 vs. R4 | R3 vs. R5 | R4 vs. R5 |
| F1 | 8.30E-06 | 8.30E-06 | 8.30E-06 | 8.30E-06 | 9.34E-06 | 8.30E-06 | 8.30E-06 | 0.002 | 1.20E-04 | 8.30E-06 |
| F2 | 8.11E-06 | 8.26E-06 | 8.24E-06 | 8.23E-06 | 9.29E-06 | 8.25E-06 | 8.26E-06 | 0.009 | 0.003 | 8.26E-06 |
| F3 | 8.30E-06 | 1.05E-05 | 8.30E-06 | 6.30E-04 | 0.732 | 8.30E-06 | 0.003088 | 9.34E-06 | 0.004 | 8.30E-06 |
| F4 | 9.34E-06 | 0.002 | 2.35E-05 | 7.84E-05 | 0.006 | 0.058 | 0.055 | 0.023 | 0.151 | 0.485 |
| F5 | 9.34E-06 | 4.80E-04 | 1.18E-05 | 2.63E-05 | 0.007 | 0.101 | 0.144 | 0.026 | 0.159 | 0.439 |
| F6 | 8.30E-06 | 8.30E-06 | 8.30E-06 | 1.10E-04 | 0.001 | 8.30E-06 | 0.005 | 2.94E-05 | 2.10E-05 | 8.30E-06 |
| F7 | 8.30E-06 | 9.34E-06 | 8.30E-06 | 2.94E-05 | 0.174 | 8.30E-06 | 0.002 | 1.18E-05 | 0.020 | 8.30E-06 |
Similar to NOM, no feature extracted from A colour plane was significantly different between heart and lung of acidic tongue (Table 2.2). In contrast to NOM, mean and median were different between stomach-spleen and each of heart and liver-gallbladder.
Table 2.
2. p values @ 1% significance level showing the alterations between regions of ACD tongue images in A colour plane.
Table 2.
2. p values @ 1% significance level showing the alterations between regions of ACD tongue images in A colour plane.
| Features | R1 vs. R2 | R1 vs. R3 | R1 vs. R4 | R1 vs. R5 | R2 vs. R3 | R2 vs. R4 | R2 vs. R5 | R3 vs. R4 | R3 vs. R5 | R4 vs. R5 |
| F1 | 0.439 | 8.30E-06 | 4.57E-05 | 2.94E-05 | 8.30E-06 | 2.63E-05 | 9.34E-06 | 8.30E-06 | 1.49E-05 | 0.002 |
| F2 | 0.849 | 8.30E-06 | 3.29E-05 | 2.10E-05 | 8.30E-06 | 3.29E-05 | 1.05E-05 | 8.30E-06 | 2.63E-05 | 0.002 |
| F3 | 0.082 | 0.517 | 0.000296 | 9.34E-06 | 0.713 | 0.001 | 8.30E-06 | 0.010 | 1.67E-05 | 3.67E-05 |
3.3. Region-Wise Comparison of Textural Features between NOM and ACD
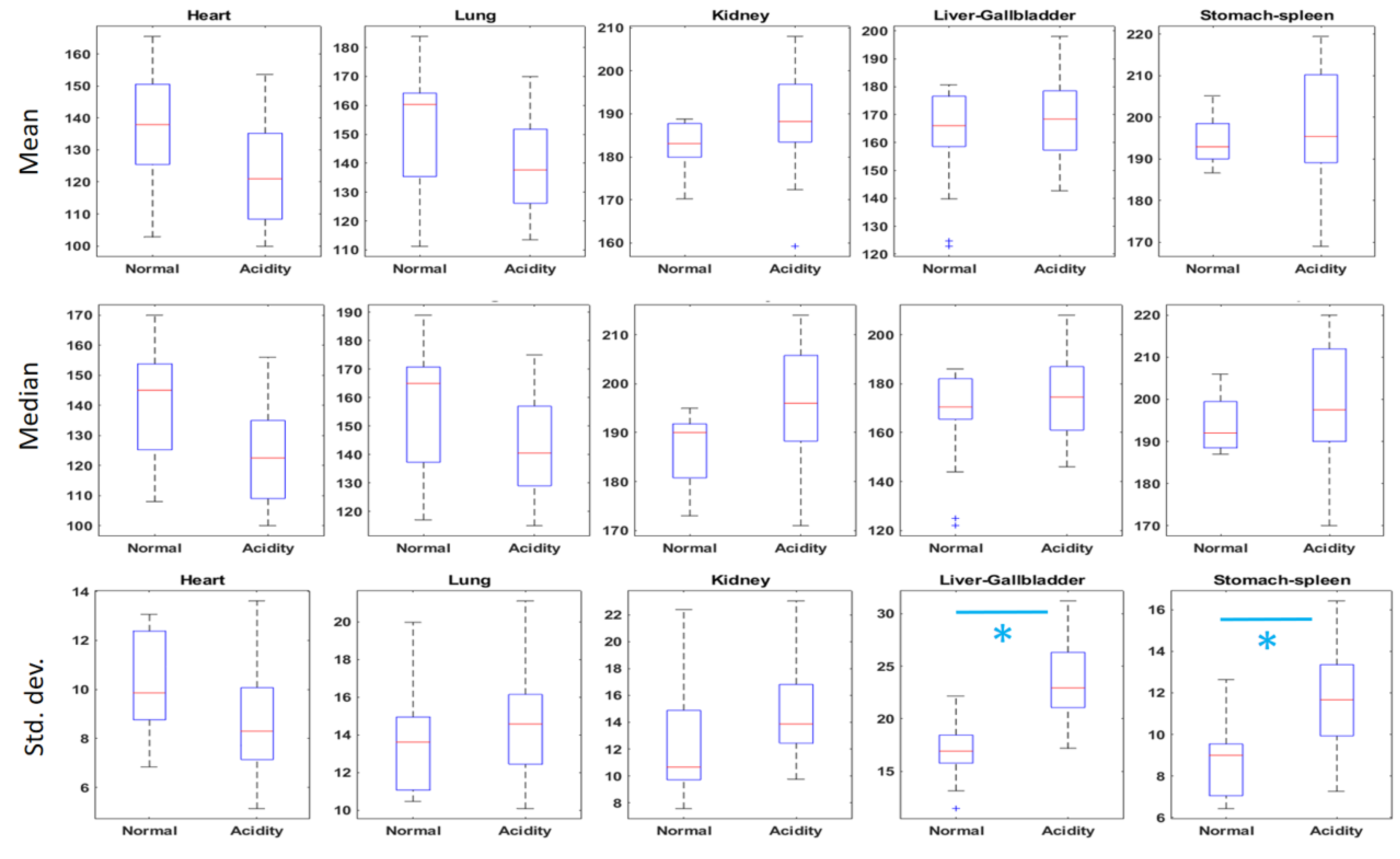
Neither mean nor median was significantly different between NOM and ACD for any region of grey scale images of tongue (Table 3.1). Standard deviations of both liver-gallbladder and stomach-spleen regions have significantly increased from NOM to ACD (Figure 4.1 ). Contrast was significantly decreased from NOM to ACD for all tongue regions and consequently reverse phenomenon was observed for homogeneity (Figure 4.2). Contrast of stomach-spleen region of normal tongue extended up to 0.35 which was highest among all values of contrast. Correlation showed an interesting property. Correlation of heart region has significantly increased while the same of kidney, liver-gallbladder and stomach-spleen regions decreased significantly from NOM to ACD (Figure 4.2). Significant increase of energy from NOM to ACD was observed in both heart and lung regions (Figure 4.2). Table 3.1 shows importance of considering second order features for heart, lung and kidney region where none of mean, median or standard deviation was significantly different between NOM and ACD while three or more GLCM features significantly altered between two study groups
Table 3.1. p values @ 1% significance level showing the alterations between NOM and ACD tongue images in grey scale.
| Organ | F1 | F2 | F3 | F4 | F5 | F6 | F7 |
| Heart | 0.032 | 0.023 | 0.093 | 0.002 | 0.001 | 2.4E-04 | 4.1E-04 |
| Lung | 0.032 | 0.035 | 0.584 | 1.4E-04 | 1.2E-04 | 0.365 | 7.82E-05 |
| Kidney | 0.065 | 0.031 | 0.065 | 0.002 | 0.002 | 0.001 | 0.027 |
| Liver- Gallbladder | 0.814 | 0.545 | 1.02E-08 | 3.27E-06 | 6.67E-06 | 1.01E-05 | 0.920 |
| Stomach-Spleen | 0.462 | 0.234 | 0.004 | 0.003 | 0.003 | 6.23E-05 | 0.044 |
Figure 4.
1. Boxplots showing region wise variation of mean, median and standard deviation between NOM and ACD tongue images in grey scale. * signifies p<0.01.
Figure 4.
1. Boxplots showing region wise variation of mean, median and standard deviation between NOM and ACD tongue images in grey scale. * signifies p<0.01.
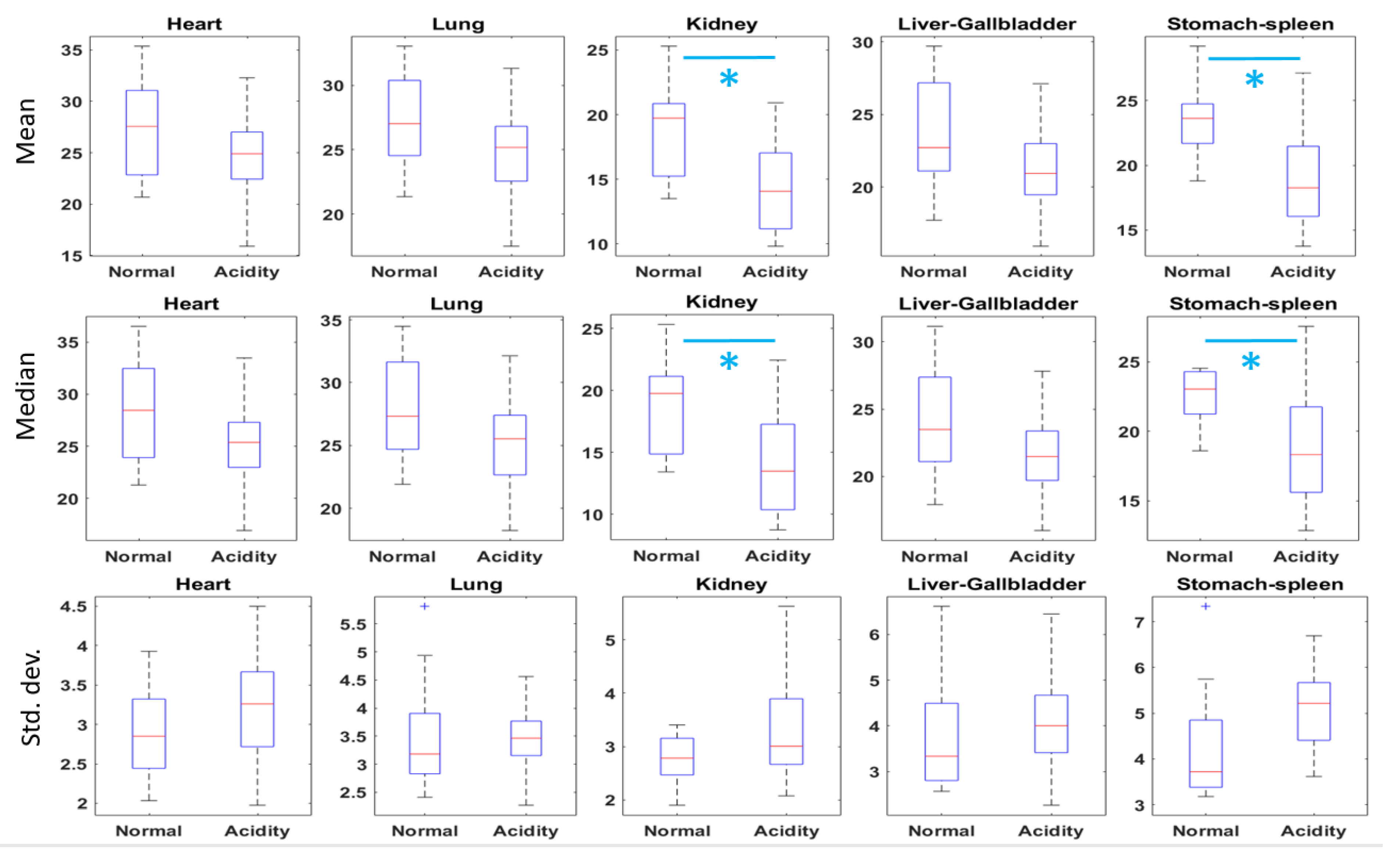
A colour plane of tongue images revealed that mean and median a* values of kidney and stomach-spleen regions have significantly decreased from NOM to ACD (Figure 5.1). No significant difference of standard deviation was found between NOM and ACD in any region of A colour plane of tongue images (Table 3.2).
Figure 4.
2. Boxplots showing organ wise variation of GLCM features between NOM and ACD tongue images in grey scale. * signifies p<0.01.
Figure 4.
2. Boxplots showing organ wise variation of GLCM features between NOM and ACD tongue images in grey scale. * signifies p<0.01.
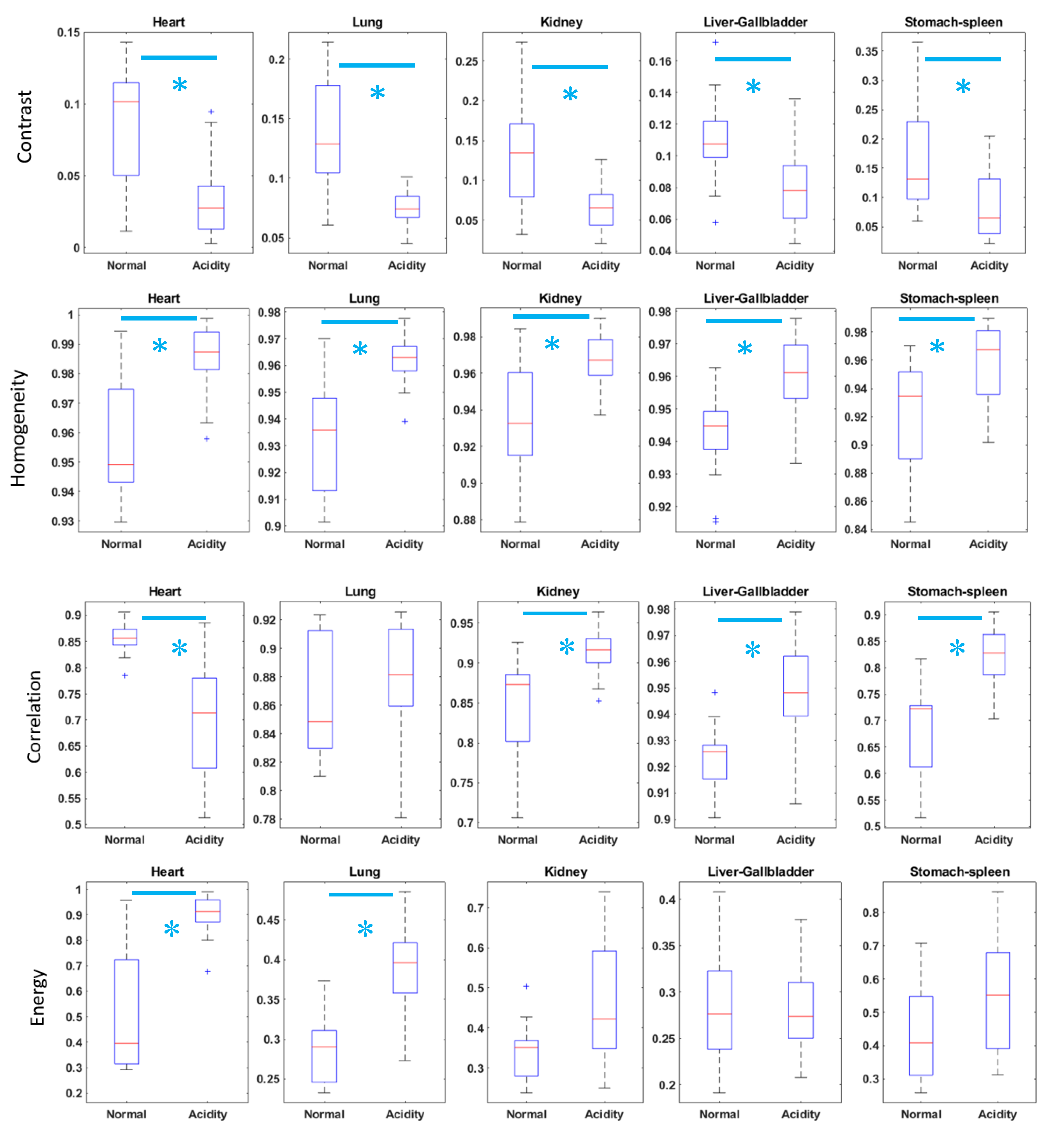
Table 3.2. p values @ 1% significance level showing the alterations between NOM and ACD tongue images in A colour plane.
| Organ | F1 | F2 | F3 |
| Heart | 0.107 | 0.099 | 0.251 |
| Lung | 0.107 | 0.086 | 0.659 |
| Kidney | 0.003 | 0.005 | 0.160 |
| Liver- Gallbladder | 0.015 | 0.015 | 0.052 |
| Stomach-spleen | 0.001 | 0.007 | 0.030 |
Figure 5.
1. Boxplots showing organ wise variation of mean, median and standard deviation of a* values between NOM and ACD tongue images. * Signifies p<0.01.
Figure 5.
1. Boxplots showing organ wise variation of mean, median and standard deviation of a* values between NOM and ACD tongue images. * Signifies p<0.01.
3.3.1. Significance of Findings from Tongue Color and Texture Analysis in the Light of TCM
In English there is no word to encompass the meaning of Qi but it is described through transformation and movement. Taoism provides a conceptual framework for TCM and understanding of Qi. It mentions that Qi is everywhere and profoundly interactive. In traditional and contemporary TCM practice, Qi is understood through its context, type, function and by the assessment of health and illness [29,30]. In certain qualitative terms, Qi is differentiated in human body according to its source, function and distribution. These terms are yuan qi (primary qi), zong qi (pectoral qi), ying qi (nutrient qi) and wei qi (defensive qi) and as per source they may be further classified into congenital qi (like Yuan qi) and acquired qi (like zong qi, ying qi and wei qi). Again congenital qi and acquired qi are dependent on each other for production and nourishment.
In the light of above discussion, tongue color change, i.e., the decreased redness in stomach-spleen region in ACD compared to that of NOM (Figure 5.1) possibly indicated depletion of Qi in the concerned zang-fu organs, in particular the spleen deficiency [30]. Additionally, textural analysis revealed that all the tongue regions of ACD became more homogeneous compared to NOM (Figure 4.2). The loss of heterogeneity/ contrast in each region of tongue in ACD (Figure 4.2) was again very indicative in the light of TCM. It possibly demonstrated the changes of normal structural and functional diversity, including distribution of Qi of varied zang-fu organs as manifested through different regions of tongue in acidity patients [29,30]. This finding further supports the idea that pathology means loss of information and normal heterogeneity [31].
4. Conclusion
Global textural analysis of tongue may obscure local information which is equally essential for tongue diagnosis in TCM. Further, in majority of existing handful of reports on regional analysis of tongue, the regions did not correlate directly to different organs. Current study has compared textural features extracted from five different tongue regions which has direct association with internal organs for healthy subjects and patients suffering from chronic acidity-indigestion. Inter and intra group comparisons demonstrate how the relationships among different regions alter from NOM to ACD and thus establish significance of local textural analysis. In future, finding from non-invasive imaging techniques of different body organs in disease conditions can be correlated with features extracted from corresponding regions of tongue for further validation. Inclusion of more study sample is required in future to apply machine learning based techniques. Extending the present methodology of regional analysis to other diseases may improve accuracy of computerized tongue diagnosis.
Funding
This research work was funded by Indian Research Institute for Integrated Medicine, Mourigram, West Bengal, India.
Acknowledgements
The authors acknowledge all staff and health workers of Indian Research Institute for Integrated Medicine, Mourigram, West Bengal, India.
Conflict of Interest
The authors declare that they have no conflicts of interest in the research.
References
- Doyle, M.E., Premathilake, H.U., Yao, Q., Mazucanti, C.H. and Egan, J.M., 2023. Physiology of the tongue with emphasis on taste transduction. Physiological reviews, 103(2), pp.1193-1246. [CrossRef]
- Kurande, V.H., Waagepetersen, R., Toft, E. and Prasad, R., 2013. Reliability studies of diagnostic methods in Indian traditional Ayurveda medicine: An overview. Journal of Ayurveda and Integrative Medicine, 4(2), p.67. [CrossRef]
- Lo, L.C., Cheng, T.L., Chiang, J.Y. and Damdinsuren, N., 2013. Breast cancer index: a perspective on tongue diagnosis in traditional chinese medicine. Journal of traditional and complementary medicine, 3(3), pp.194-203. [CrossRef]
- Balasubramaniyan, S., Jeyakumar, V. and Nachimuthu, D.S., 2022. Panoramic tongue imaging and deep convolutional machine learning model for diabetes diagnosis in humans. Scientific Reports, 12(1), p.186.
- Kirschbaum, B., 2000. Atlas of Chinese tongue diagnosis (Vol. 1). Eastland Press.
- Xie, J., Jing, C., Zhang, Z., Xu, J., Duan, Y. and Xu, D., 2021. Digital tongue image analyses for health assessment. Medical Review, 1(2), pp.172-198. [CrossRef]
- Zhang, B., Kumar, B.V. and Zhang, D., 2013. Detecting diabetes mellitus and nonproliferative diabetic retinopathy using tongue colour, texture, and geometry features. IEEE transactions on biomedical engineering, 61(2), pp.491-501.
- Kawanabe, T., Kamarudin, N.D., Ooi, C.Y., Kobayashi, F., Mi, X., Sekine, M., Wakasugi, A., Odaguchi, H. and Hanawa, T., 2016. Quantification of tongue colour using machine learning in Kampo medicine. European Journal of Integrative Medicine, 8(6), pp.932-941.
- Chen, H.S., Chen, S.M., Jiang, C.Y., Zhang, Y.C., Lin, C.Y., Lin, C.E. and Lee, J.A., 2022. Computational tongue colour simulation in tongue diagnosis. Colour Research & Application, 47(1), pp.121-134. [CrossRef]
- Wang, Y.G., Yang, J., Zhou, Y. and Wang, Y.Z., 2007. Region partition and feature matching based colour recognition of tongue image. Pattern recognition letters, 28(1), pp.11-19.
- Yoo, W.S., Kang, K., Kim, J.G. and Yoo, Y., 2023. Image-Based Quantification of Colour and Its Machine Vision and Offline Applications. Technologies, 11(2), p.49.
- Li, J., Huang, J., Jiang, T., Tu, L., Cui, L., Cui, J., Ma, X., Yao, X., Shi, Y., Wang, S. and Wang, Y., 2022. A multi-step approach for tongue image classification in patients with diabetes. Computers in Biology and Medicine, 149, p.105935. [CrossRef]
- Lo, L.C., Cheng, T.L., Chen, Y.J., Natsagdorj, S. and Chiang, J.Y., 2015. TCM tongue diagnosis index of early-stage breast cancer. Complementary therapies in medicine, 23(5), pp.705-713.
- Cui, J., Cui, H., Yang, M., Du, S., Li, J., Li, Y., Liu, L., Zhang, X. and Li, S., 2019. Tongue coating microbiome as a potential biomarker for gastritis including precancerous cascade. Protein & cell, 10(7), pp.496-509.
- Hsu, P.C., Wu, H.K., Huang, Y.C., Chang, H.H., Lee, T.C., Chen, Y.P., Chiang, J.Y. and Lo, L.C., 2019. The tongue features associated with type 2 diabetes mellitus. Medicine, 98(19), p.e15567.
- Liu, M., Wang, X., Wu, F., Dai, N., Chen, M., Yu, J., Guan, J. and Li, F., 2020. Variations of oral microbiome in chronic insomnia patients with different tongue features. The American journal of Chinese medicine, 48(04), pp.923-944. [CrossRef]
- Bakshi, D. and Pal, S., 2010, December. Introduction about traditional Tongue Diagnosis with scientific value addition. In 2010 International Conference on Systems in Medicine and Biology (pp. 269-272). IEEE.
- Kainuma, M., Furusyo, N., Urita, Y., Ikezaki, H., Ura, K., Nakaguchi, T. and Namiki, T., 2019. Objective tongue colour and gastroesophageal reflux disease: Cross-sectional study. Traditional &Kampo Medicine, 6(1), pp.19-25.
- Nawn, D., Chatterjee, S., Anura, A., Bag, S., Chakraborty, D., Pal, M., Paul, R.R. and Chatterjee, J., 2019. Elucidation of Differential Nano-Textural Attributes for Normal Oral Mucosa and Pre-Cancer. Microscopy and Microanalysis, 25(5), pp.1224-1233.
- Thirunavukkarasu, U., Umapathy, S., Krishnan, P.T. and Janardanan, K., 2020. Human tongue thermography could be a prognostic tool for prescreening the type II diabetes mellitus. Evidence-Based Complementary and Alternative Medicine, 2020.
- Chiu, C.C., 2000. A novel approach based on computerized image analysis for traditional Chinese medical diagnosis of the tongue. Computer methods and programs in biomedicine, 61(2), pp.77-89.
- Jung, C.J., Kim, K.H., Jeon, Y.J. and Kim, J., 2014. Improving colour and shape repeatability of tongue images for diagnosis by using feedback gridlines. European Journal of Integrative Medicine, 6(3), pp.328-336.
- Liangyue, D., Yijun, G., Shuhui, H., Xiaoping, J., Yang, L. and Rufen, W., 2001. Chinese acupuncture and moxibustion. Traditional medicine in Asia, 75.
- Maciocia, G., 1987. Tongue diagnosis in Chinese medicine. Eastland press.
- Zhuo, L., Zhang, P., Qu, P., Peng, Y., Zhang, J. and Li, X., 2016. A K-PLSR-based colour correction method for TCM tongue images under different illumination conditions. Neurocomputing, 174, pp.815-821.
- Tania, M.H., Lwin, K. and Hossain, M.A., 2019. Advances in automated tongue diagnosis techniques. Integrative Medicine Research, 8(1), pp.42-56.
- Fan, S., Chen, B., Zhang, X., Hu, X., Bao, L., Yang, X., Liu, Z. and Yu, Y., 2021. Machine learning algorithms in classifying TCM tongue features in diabetes mellitus and symptoms of gastric disease. European Journal of Integrative Medicine, 43, p.101288.
- Gholami, E. and Tabbakh, S.R.K., 2021. Increasing the accuracy in the diagnosis of stomach cancer based on colour and lint features of tongue. Biomedical Signal Processing and Control, 69, p.102782. [CrossRef]
- Das, D., 2008. Acupuncture - A Universal Total Outlook in Medical Science, Kolkata.
- Ross, J., 1985. Zang fu. The organ system of Traditional Chinese Medicine,2nd ed, Churchill Livingstone, London, pp 262.
- Goldberger, A.L., Amaral, L.A., Hausdorff, J.M., Ivanov, P.C., Peng, C.K. and Stanley, H.E., 2002. Fractal dynamics in physiology: alterations with disease and aging. Proceedings of the national academy of sciences, 99(suppl_1), pp.2466-2472.
Figure 1.
Tongue images of A) Normal B) Acidity-indigestion.
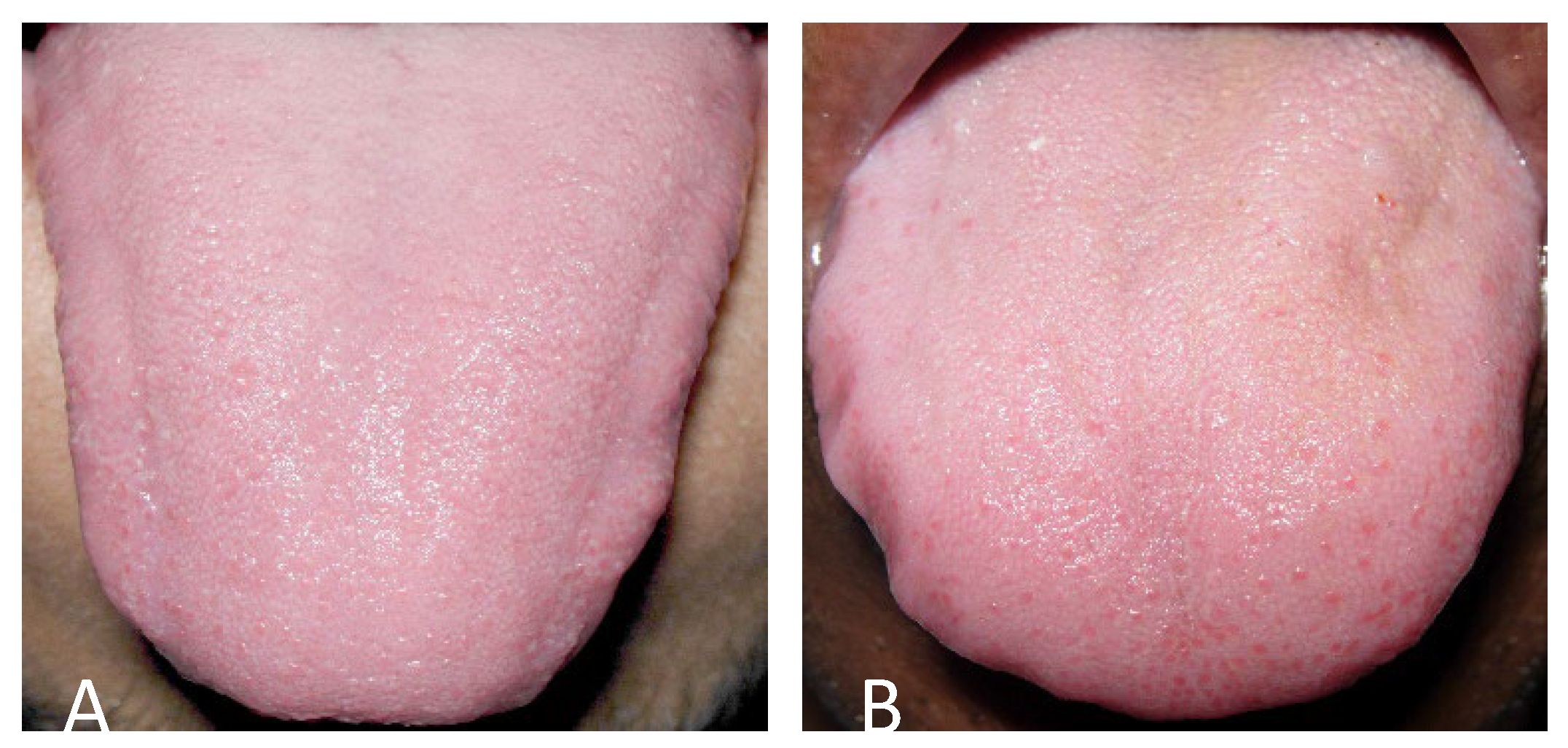
Figure 2.
Partition of tongue in five regions (1: Heart, 2: Lung, 3: Kidney-bladder, 4: liver-gallbladder, 5: stomach-spleen). ABCD is bounding rectangle.
Figure 2.
Partition of tongue in five regions (1: Heart, 2: Lung, 3: Kidney-bladder, 4: liver-gallbladder, 5: stomach-spleen). ABCD is bounding rectangle.
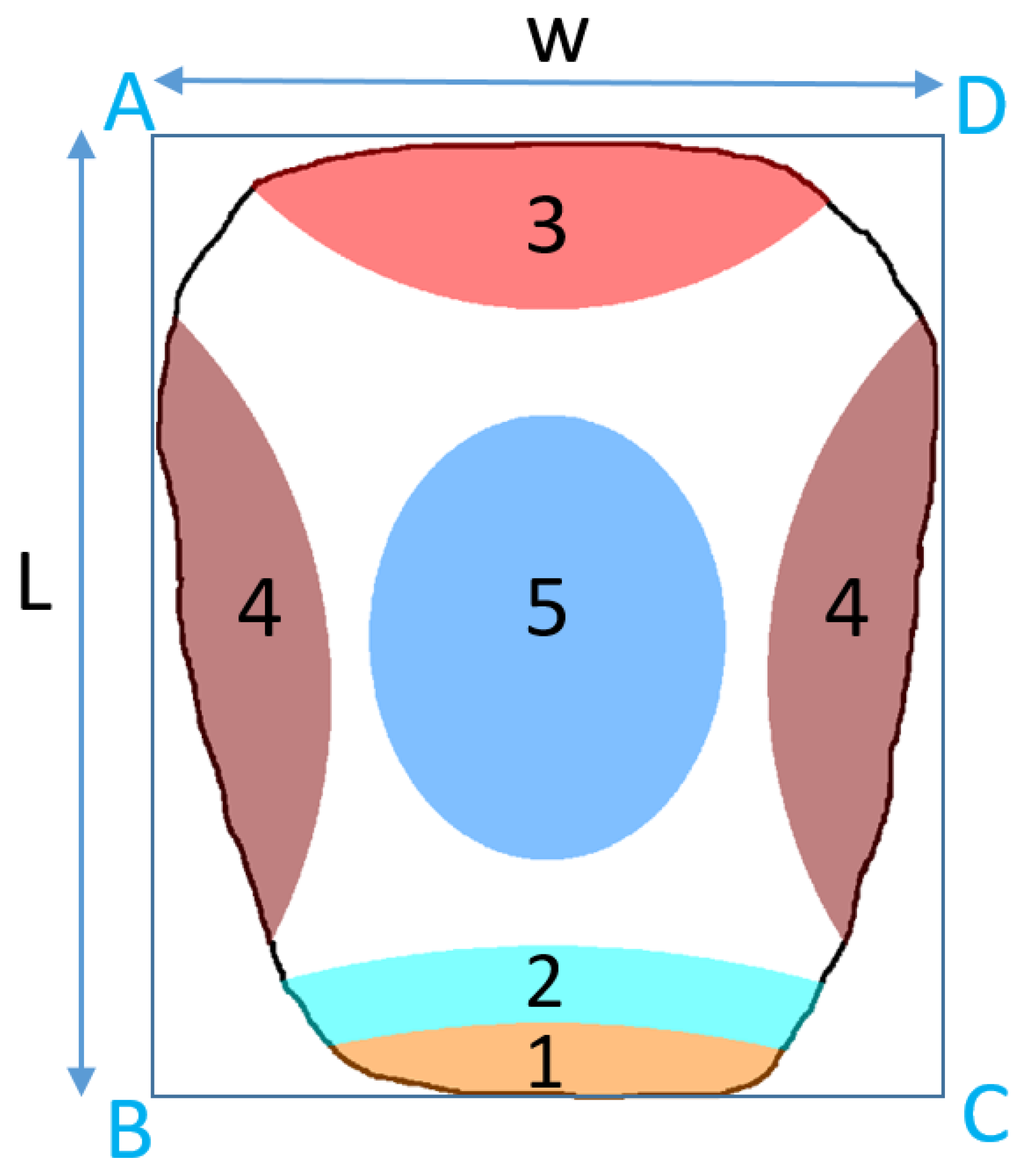
Figure 3.
Examples of automated partitioning of tongues into 5 regions viz. heart, lung, kidney, liver-gallbladder and stomach-spleen. For better visualization of zoning, only tongue boundaries of original tongue images are shown.
Figure 3.
Examples of automated partitioning of tongues into 5 regions viz. heart, lung, kidney, liver-gallbladder and stomach-spleen. For better visualization of zoning, only tongue boundaries of original tongue images are shown.
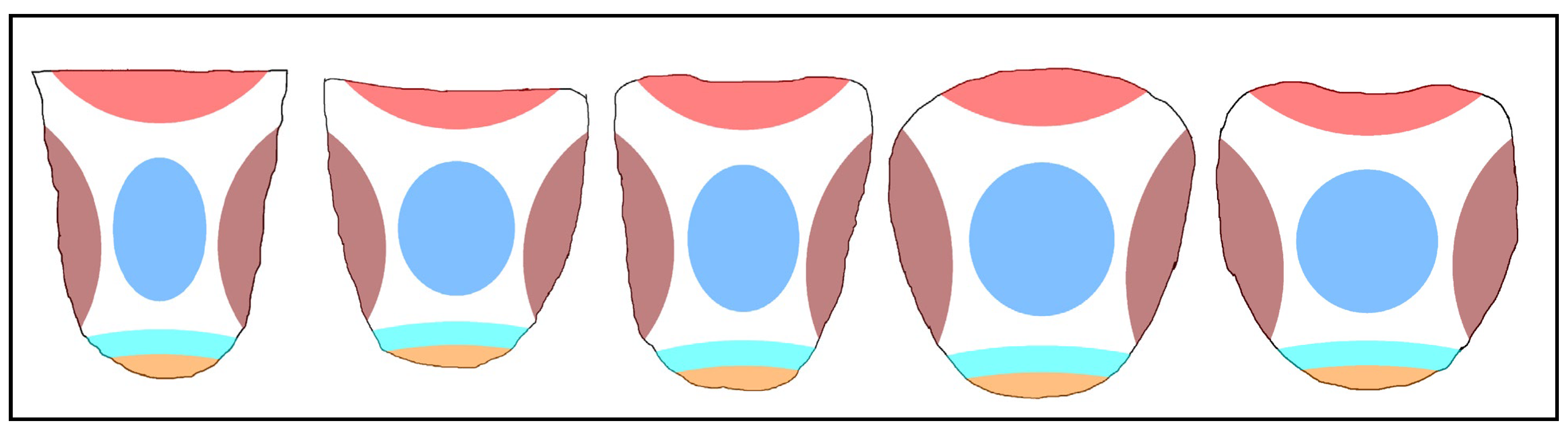
Table 1.
1. p values @ 1% significance level showing the alterations between regions of NOM tongue images in grey scale.
Table 1.
1. p values @ 1% significance level showing the alterations between regions of NOM tongue images in grey scale.
| Features | R1 vs. R2 | R1 vs. R3 | R1 vs. R4 | R1 vs. R5 | R2 vs. R3 | R2 vs. R4 | R2 vs. R5 | R3 vs. R4 | R3 vs. R5 | R4 vs. R5 |
| F1 | 0.001 | 0.001 | 0.002 | 0.001 | 0.007 | 0.067 | 0.001 | 0.019 | 0.002 | 0.001 |
| F2 | 0.001 | 0.001 | 0.002 | 0.004 | 0.01 | 0.132 | 0.001 | 0.041 | 0.117 | 0.001 |
| F3 | 0.001 | 0.52 | 0.002 | 0.175 | 0.054 | 0.278 | 0.002 | 0.002 | 0.024 | 0.001 |
| F4 | 0.005 | 0.042 | 0.01 | 0.014 | 0.638 | 0.067 | 0.206 | 0.365 | 0.083 | 0.054 |
| F5 | 0.005 | 0.042 | 0.007 | 0.014 | 0.7 | 0.032 | 0.147 | 0.365 | 0.083 | 0.054 |
| F6 | 0.175 | 0.638 | 0.01 | 0.019 | 0.24 | 0.067 | 0.002 | 0.003 | 0.002 | 0.001 |
| F7 | 0.002 | 0.102 | 0.003 | 0.365 | 0.206 | 0.52 | 0.024 | 0.067 | 0.365 | 0.014 |
Table 1.
2. p values @ 1% significance level showing the alterations between regions of NOM tongue images in A colour plane.
Table 1.
2. p values @ 1% significance level showing the alterations between regions of NOM tongue images in A colour plane.
| Features | R1 vs. R2 | R1 vs. R3 | R1 vs. R4 | R1 vs. R5 | R2 vs. R3 | R2 vs. R4 | R2 vs. R5 | R3 vs. R4 | R3 vs. R5 | R4 vs. R5 |
| F1 | 0.765 | 0.001 | 0.007 | 0.024 | 0.001 | 0.001 | 0.002 | 0.001 | 0.001 | 1 |
| F2 | 0.638 | 0.001 | 0.002 | 0.014 | 0.001 | 0.001 | 0.002 | 0.001 | 0.001 | 0.966 |
| F3 | 0.206 | 1 | 0.32 | 0.002 | 0.123 | 0.413 | 0.019 | 0.083 | 0.001 | 0.019 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



