
Submitted:
08 July 2024
Posted:
10 July 2024
You are already at the latest version
Abstract
Fungal infections (FIs) are spreading globally causing a significant public health concern. However, its documentation remains sparse in Africa, particularly in Rwanda. This literature review, aims to assess the risk and document current gaps in evidence and policy. It summarizes the published data about FIs in Rwanda, including ten reports published between 1972-and-2022. Blastomyces, Candida, Cryptococcus, Histoplasma, Microsporum, Pneumocystis, Rhinosporidium, and Trichophyton caused human infections. These infections primarily affected the brain, respiratory, urinary and reproductive organs, and they were diagnosed using culturing, histopathology, immunology, and/or microscopic techniques. Our findings provide an overview of the diversity and distribution of FIs, highlighting significant limitations in the country’s diagnostic capacity and surveillance system for FIs. Also, indicating severe gaps in evidence to inform policymaking, guide strategic planning and intervention, underscoring the urgent need to build national capacity in fungal diagnosis, surveillance, and research. Raising awareness among the public, scientific community, healthcare providers, and policymakers remains crucial. Furthermore, this report reveals the threats of FIs on public health and food insecurity in Rwanda. A Multisectoral One Health Strategy is essential in research and intervention to determine and reduce the health and safety impacts of fungal pathogens on human, animal, and the environment.
Keywords:
Fungal infections
; Human
; Soil
; Plants
; Public health
; Healthcare
; One Health
; Global Health
; Food Insecurity
; Africa
1. Introduction
Fungal population is estimated to include over 3.8 million species distributed throughout the world. However, most of them are understudied and poorly characterized [1]. Most of these species infect humans, animals, and/or plants around the world, nevertheless, they are commonly severely neglected mainly because of their historically limited distribution to Low and Middle-income countries in the tropical and sub-tropical regions. Due to the progressive nature of fungal infections (FIs) and the associated delay with their diagnosis, limited development of effective treatment, their burden is relatively high particularly in resources limited settings. They contribute heavily to diseases morbidity, mortality, and disability resulting in severe socioeconomic burden with over 1.5 million deaths annually attributed to FIs [2]. Therefore, the World Health Organization (WHO) has released a list of fungal pathogens of high priority in healthcare, public health, and research (Figure 1) [3,4,5]. Fungal pathogens in this list are ranked into three categories including critical, high and medium priority (Figure 1). This ranking was done based on the public health significant and emergence of antifungal resistance to the currently available antifungal drugs [3,4,5].
Invasive and noninvasive fungal diseases represent a significant challenge for health systems in the Low and Middle-income Countries (LMICs) particularly in tropical and sub-tropical regions of the world. It is of particularly high concern in healthcare settings among the most vulnerable populations groups. These groups include immunocompromised individuals, such as those living with human immunodeficiency virus (HIV), haematological malignancies, organ transplant recipients, and patients undergoing long course immunosuppressive therapy [6,7]. These infections, primarily opportunistic in nature and characterized by the presence of fungal elements in subcutaneous and deep tissues as identified through culture or histopathological investigations [8,9].
In low-resource settings like many African countries, the burden of FIs is exacerbated by poor hygiene situations, the high prevalence of HIV, tuberculosis, and poverty, making timely diagnosis and management critical yet challenging in context of limited budgets allocated to healthcare. The lack of reliable point-of-care tests (POCTs), cost barriers, limited awareness among healthcare providers, delays in diagnosis, and inadequacies in confirmatory blood cultures all contribute to the struggle in addressing invasive fungal diseases (IFDs) effectively [6,7,8,9,10,11,12].
Early diagnosis and prompt initiation of appropriate antifungal therapy are crucial in combating FIs and reducing associated morbidity and mortality rates [13,14,15]. However, the scarcity of data on the burden of invasive fungal diseases in Africa hinders efforts to implement targeted interventions and strategies [8].
Rwanda, a small landlocked country located in East Africa, is known for its stunning landscapes, including lush green hills, serene lakes, and diverse wildlife. With a population size of over 13 million people, Rwanda is one of the most densely populated countries on the African continent, covering an area of about 26,338 square kilometers [16]. Despite its natural beauty and recent economic development, Rwanda faces various health challenges, including Neglected Tropical Diseases (NTDs) and other infectious diseases [17].
This literature review aims to provide an overview of the diversity and distribution of FIs in Rwanda, shedding light on the prevalence, risk factors, and public health implications associated with these infections. By analyzing existing literature and research findings, this review seeks to contribute to the knowledge base surrounding FIs in Rwanda, ultimately guiding policies and practices aimed at preventing, diagnosing, and treating these infections to safeguard public health in Rwanda and the region.
2. Materials and Methods
In this research, we performed a comprehensive literature review utilizing databases such as PubMed, Google Scholar, and African Journal Online to identify published papers concerning FIs in Rwanda. Our search terms included 'histoplasmosis and Rwanda', 'cryptococcosis and Rwanda', 'aspergillosis and Rwanda', 'blastomycosis and Rwanda', 'pneumocystis pneumonia and Rwanda', 'candidiasis and Rwanda', 'mucormycosis and Rwanda', 'emergomycosis and Rwanda', 'talaromycosis and Rwanda', 'blastomycosis and Rwanda', 'sporotrichosis and Rwanda', 'coccidioidomycosis and Rwanda', ‘fungal keratitis and Rwanda’, ‘allergic fungal rhinosinusitis and Rwanda’, ‘allergic bronchopulmonary aspergillosis and Rwanda’, 'dermatophytes and Rwanda’ ‘paracoccidioidomycosis and eumycetoma and Rwanda'. All authors participated in the initial data curation process, following which two authors (EES and AA) screened the publications for relevance. We included retrospective studies, prospective studies, and primarily case series. Case reports were considered for FIs with limited documentation. Furthermore, we conducted 'snowballing' by reviewing references in identified papers for additional publications on FIs that might not have been captured in our initial searches. Papers without clear patient origin information or those focusing on FIs beyond Rwanda were excluded. Each case's data extraction encompassed details such as district, causative agents, infection sites, year, and diagnostic methods.
3. Results
Our systematic search identified ten reports about FIs in Rwanda that were published between 1972 and 2022 [18,19,20,21,22,23,24,25,26,27]. Among the identified FIs, there were two reports on candida infections, two reports on Histoplasma spp., and dermatophytes one report on Blastomyces dermatitidis, Rhinosporidium seeberi, Cryptococcus neoformans, and Pneumocystis carinii each.
In terms of infection sites, while Candida spp. were predominantly affecting the vagina; Histoplasma duboisi was associated with disseminated infections. On the other hand, Blastomyces dermatitidis was linked to cerebellar infections and Rhinosporidium seeberi most commonly affected the nose, conjunctiva. Meanwhile respiratory infections were observed in Cryptococcus neoformans and Pneumocystis carinii and different causative agents were encountered causing dermatophytes affecting the scalp (Table 1).
Candida infections were reported in two districts, specifically Huye and Kicukiro. Histoplasma duboisi cases were identified in the Butaro district. Blastomyces dermatitidis occurrences were documented in Kigali. Rhinosporidium seeberi incidents were recorded in both Gatsibo and Kirehe districts (Table 1).
When diagnosing FIs, it is important to utilize a combination of traditional and advanced techniques. New technologies such as PCR (Polymerase Chain Reaction) and antigen testing are now widely used for accurate and rapid diagnosis of FIs. In this report the diagnosis of these encountered FIs in Rwanda were basically based on the classical and old techniques including culture based and cytology, histopathology and immunological testing. For candida infection encountered in Rwanda the diagnosis was made basically using a culturing technique and germ tube method. Furthermore, histopathological diagnosis was used for the identification of Blastomyces dermatitidis; Rhinosporidium seeberi; Cryptococcus neoformans which considered as nonspecific diagnostic tool and cannot be distinguishing different species within the same genus. Furthermore, Pneumocystis carinii is diagnosed basically using cytological smear collected from Bronchi-alveolar lavage (BAL) based on the presence of foamy alveolar casts (FACs) was the distinctive feature and was noted. For dermatophytes, Trichophyton violaceum; Microsporom langeroni; and Trichophyton verrucosum were identified among children affecting the scalp and the diagnosis was done based on the clinical, direct microscopy and culture (Table 1).
Burden of fungal infection in the plants and soil in Rwanda:
According to our search, only one study was present in regards of the soilborne FIs affecting bean in Rwanda conducted by Rusuku and associates [27]. The comprehensive surveys conducted by the authors were carried out in eight of Rwanda's prefectures including Gikongoro; Butare; Gitarama; Kigali; Byumba; Ruhengeri; Gisenyi and Kibungo between 1989 and 1990 revealed a high prevalence of soilborne fungi pathogenic to common beans, the most consumed agricultural product in Rwanda. Pathogens such as Pythium spp., Macrophomina phaseolina, Rhizoctonia solani, Fusarium oxysporum f. sp. phaseoli, and Sclerotium rolfsii were identified based on various criteria such as symptoms, colony characteristics, reproductive structures, and pathogenicity assessments.
Notably, a significant percentage of sampled plants displayed symptoms associated with soilborne pathogens across different seasons and regions. This widespread distribution and incidence emphasize the potential agricultural impact of these fungi on common bean production in Rwanda. The consistent presence of these pathogens in multiple prefectures over the study period underscores their resilience and threat to crop health. Moreover, it is crucial to recognize that some of these soilborne fungi, including Pythium spp., Macrophomina phaseolina, and Fusarium oxysporum, have the capacity to cause diseases in humans as well. These pathogens can pose health risks to individuals through various means, such as contamination of food crops or soil exposure. Therefore, understanding the prevalence and distribution of these organisms in agricultural settings is not only essential for crop protection but also for safeguarding public health. The findings from these surveys underscore the importance of continued monitoring, research, and preventive measures aimed at mitigating the impact of soilborne fungi not only on agricultural productivity but also on human health [28,29,30].
Figure 2 below highlights the severe limitations on reporting FIs in Rwanda which also suggests limitations in the healthcare services for FIs including the diagnostic capacity, surveillance system, and reporting (Figure 2). This is indicated by the detection of 21 infections in over 50 years throughout the country history, and further highlighted by the lack of reporting any FIs among humans, animals, or in the environment between 1997 and 2013. Particularly that daily practices such as that most of poor communities in Rwanda are using motorbikes for their daily transportation, which require extensive reuse of helmets as it required for riders safety. Such practices are expected to facilitate the sharing of skin related pathogens and intensifies the transmission of dermal infections including fungal, bacterial, parasitic, and viral. Therefore, there is an urgent need for improving the diagnostic services for FIs including the integration of molecular and genomics techniques, implementing a national surveillance to monitor the dynamics of these pathogens and the risk factors associated with their transmission in the country. This will help in developing evidence-based decisions and policies-making as well as strategic planning and resources mobilization to improve the health of affected communities.
4. Discussion
The information provided in this communication highlights the significant burden of FIs in Rwanda, encompassing various types of fungal pathogens affecting both humans and agricultural crops [18,19,20,21,22,23,24,25,26,27]. The reports indicate the presence of FIs caused by Candida spp., Histoplasma duboisi, Blastomyces dermatitidis, Rhinosporidium seeberi, Cryptococcus neoformans, Pneumocystis carinii, and dermatophytes in different regions of Rwanda. It's clear that diagnosing these FIs requires a mix of traditional and advanced techniques, with some reliance on classical methods like culture-based diagnostics, cytology, histopathology, and immunological testing.
In addition to the human health implications, a study on soilborne FIs in Rwanda reported on the prevalence of pathogens such as Pythium spp., Macrophomina phaseolina, Rhizoctonia solani, Fusarium oxysporum f. sp. phaseoli, and Sclerotium rolfsii. These pathogens were reported to mainly affect beans, the main food item on Rwandan diet. This indicates the serious threat of FIs on food security in the country. The widespread distribution of these pathogens across various regions and seasons poses a significant threat to common bean production, emphasizing the need for continuous monitoring, research, and preventive measures [27].
Despite the widespread of chronic invasive Aspergillus rhinosinusitis, subacute invasive aspergillosis, and Candida peritonitis (intraabdominal candidiasis), fungal keratitis, and fungal tracheobronchitis as well as disseminated trichosporonosis and eumycetoma in the region. So far, none of these fungal pathogens or diseases were reported in Rwanda. This suggests severe gaps in knowledge and evidence about the presence, distribution, and health and socioeconomic impacts of FIs in the country, urging for urgent need of building the national capacity in the diagnosis, surveillance, research, and case management as well as public health interventions for the prevention and control of FIs in Rwanda. Considering that FIs can be spread among human and animal populations as well as the environment including plants and soil, cost-effective health policies, strategic planning, and implementation of interventions should be implemented through Multisectoral One Health Strategy [30,31].
Interestingly, the impact of fungal diseases on morbidity and mortality in Africa, exacerbated by weak health systems, adds another layer of complexity to the challenges faced in combating these infections in Rwanda. The World Health Organization's publication of the fungal priority pathogens list underscores the importance of research, development, and public health action in addressing FIs [3,4,5]. The prioritization of common fungal pathogens in Africa as critical and high priority highlights the urgency of the situation, emphasizing the need for enhanced research, diagnostic capabilities, and treatment strategies within Rwanda and other African countries [3]. By aligning with the WHO's guidance and focusing on these priority pathogens, Rwanda can strengthen its efforts in managing and controlling FIs, ultimately improving healthcare outcomes and agricultural sustainability.
Furthermore, Laboratory diagnosis of FIs in Africa presents a significant challenge due to limited resources, access to essential diagnostic tools and lack of necessary expertise. A combination of tests, including microscopy, culture, serology, antigen tests, molecular tests, and histopathology, is typically utilized. Imaging techniques such as x-rays, ultrasound, MRI, and CT scans play a crucial role in diagnosing invasive and chronic fungal diseases, although they may not be reliable for certain conditions like allergic fungal diseases. The diagnostic methods that were used in the detection of FIs in Rwanda were predominantly culture, microscopy, or histopathology. Although, microscopy offers a quick turnaround time but suffers from low sensitivity, requiring a high level of expertise for accurate interpretation. On the other hand, culture is widely regarded as the gold standard for fungal diagnosis, yet it is time-consuming, prone to contamination, and some species may not grow in standard blood culture conditions. Therefore, more investment should be into incorporating the use of molecular tools and genomic analysis for the early detection and monitoring drugs sensitivity among FIs [11,12]. Massive displacements of humans and animals, globalization, unplanned urbanization, and climate change are driving shift in diseases epidemiology [32,33,34,35,36]. This issue is further intensified by changes in the clinical manifestations of diseases and co-infections that alter or mask the original cardinal symptoms that are essential for making accurate differential diagnosis [37,38,39,40,41,42,43,44]. This necessitates improving the diagnostic capacity by integrating diagnostic tools with high sensitivity and specificity to differentiate and characterize infections and co-infections with various pathogens.
Moreover, conducting fungal culture poses challenges in low-income countries due to inadequate maintenance and upkeep of laboratory facilities and equipment, leading to frequent environmental contamination. Limited access to commercial selective media further complicates the process, hindering accurate identification and characterization of fungal species. Fungal culture emerged as the most frequently conducted laboratory diagnostic assay in a majority of African countries. However, the survey conducted by the European Confederation of Medical Mycology (ECMM) and the International Society for Human and Animal Mycology (ISHAM) revealed that only a small percentage of institutions in Africa meet the minimum laboratory standards for clinical mycology [7]. These constraints highlight the urgent need for improved infrastructure, training, and access to essential resources in low-resource settings to enhance the accuracy and efficiency of fungal diagnostics [7].
In resource-limited settings like Africa, the availability of diagnostic services is sparse, with fewer than ten African countries having national surveillance programs for FIs and even fewer possessing reference diagnostic mycology laboratories. The disparity in diagnostic capabilities across the continent is evident, with many diagnostic tests designed for high-income countries and not readily accessible in Africa. While MRI and CT scans are costly, x-rays, a more affordable option, remain unavailable in many primary health centers, placing a financial burden on patients for diagnosis [45]. A recent survey across 50 African countries highlighted variations in diagnostic practices, showing higher rates of chest X-rays and CT scans in the public sector compared to the private sector [46].
Beside building the diagnostic services, considering the wide range of host species for FIs including humans, animals, and plants, there is a crucial need for the implementation of multisectoral transdisciplinary One Health strategy for the prevention and control of fungal pathogens in Rwanda [28,29,30]. Particularly that, the initiative about Assessing the diagnostic capacity for fungal diseases in Africa that was launched in collaboration with the Africa Centres for Disease Control and Prevention (Africa CDC), the Global Action for Fungal Infections (GAFFI), and other stakeholders in the region during the 2nd International Conference on Public Health in Africa (CPHIA), in Kigali, Rwanda in 2022, has urged for strengthening the regional capacity [47]. It highlighted the need for investment in strengthening the diagnostic capacity, surveillance, policymaking, and improve the case management as well as implementation of preventive and control measures to reduce the transmission of FIs. However, to lead cost-effective improvement and capacity building, there is an urgent need for the establishment of regional Centre of Excellence that can lead building the regional capacity and implementation research to generate evidence to inform decision-making, guide interventions, and develop novel prevention, control, and treatment modalities.
5. Conclusions
Moving forward, it is essential to emphasize the importance of further research on fungal infections in Rwanda in humans, animals, and plants as well as on the soil using molecular, genomics, and environmental DNA (e-DNA) tools. Building the capacity of hospitals and laboratories to enhance diagnostic capabilities, treatment strategies, and surveillance of fungal diseases is crucial for better management and control of these infections. By investing in research and improving the healthcare infrastructure, Rwanda can better address the challenges posed by fungal infections and protect both human health and agricultural productivity.
Author Contributions
Conceptualization, C.M.M., A.A., and E.E.S.; methodology, A.A., and E.E.S.; validation, A.A.; investigation, A.A., and E.E.S.; writing—original draft preparation, A.A., and E.E.S.; writing—review and editing, C.M.M., J.C.S.N., M.T., A.A., and E.E.S.; visualization, A.A., and E.E.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hawksworth, D.L.; Lücking, R. Fungal Diversity Revisited: 2.2 to 3.8 Million Species. Microbiology Spectrum 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.D.; Ballou, E.R.; Bates, S.; Bignell, E.M.; Borman, A.M.; Brand, A.C.; Brown, A.J.; Coelho, C.; Cook, P.C.; Farrer, R.A. The Pathobiology of Human Fungal Infections. Nature Reviews Microbiology 2024, 1–18. [Google Scholar] [CrossRef] [PubMed]
- The World Health Organization (WHO). WHO Fungal Priority Pathogens List to Guide Research, Development and Public Health Action; World Health Organization, 2022; ISBN 92-4-006024-3. [Google Scholar]
- Fisher, M.C.; Denning, D.W. The WHO Fungal Priority Pathogens List as a Game-Changer. Nat Rev Microbiol 2023, 21, 211–212. [Google Scholar] [CrossRef] [PubMed]
- Casalini, G.; Giacomelli, A.; Antinori, S. The WHO Fungal Priority Pathogens List: A Crucial Reappraisal to Review the Prioritisation. The Lancet Microbe 2024, 0. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Ekeng, B.E.; Kibone, W.; Nsenga, L.; Olum, R.; Itam-Eyo, A.; Kuate, M.P.N.; Pebolo, F.P.; Davies, A.A.; Manga, M.; et al. Invasive Fungal Diseases in Africa: A Critical Literature Review. Journal of Fungi 2022, 8, 1236. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.; Wu, J.; Cheng, M.; Zhu, X.; Du, M.; Chen, C.; Liao, W.; Zhi, K.; Pan, W. Diagnosis of Invasive Fungal Infections: Challenges and Recent Developments. J Biomed Sci 2023, 30, 42. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W. Global Incidence and Mortality of Severe Fungal Disease. The Lancet Infectious Diseases 2024, 24, e428–e438. [Google Scholar] [CrossRef] [PubMed]
- Pang, K.R.; Wu, J.J.; Huang, D.B.; Tyring, S.K. Subcutaneous Fungal Infections. Dermatologic Therapy 2004, 17, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Lakoh, S.; Orefuwa, E.; Kamara, M.N.; Jiba, D.F.; Kamara, J.B.; Kpaka, S.; Denning, D.W. The Burden of Serious Fungal Infections in Sierra Leone: A National Estimate. Therapeutic Advances in Infection 2021, 8, 20499361211027996. [Google Scholar] [CrossRef]
- Siddig, E. e.; El Had Bakhait, O.; El nour Hussein Bahar, M.; Siddig Ahmed, E.; Bakhiet, S. m.; Motasim Ali, M.; Babekir Abdallah, O.; Ahmed Hassan, R.; Verbon, A.; van de Sande, W. w. j.; et al. Ultrasound-Guided Fine-Needle Aspiration Cytology Significantly Improved Mycetoma Diagnosis. Journal of the European Academy of Dermatology and Venereology 2022, 36, 1845–1850. [Google Scholar] [CrossRef]
- Siddig, E.E.; Ahmed, A.; Hassan, O.B.; Bakhiet, S.M.; Verbon, A.; Fahal, A.H.; van de Sande, W.W. Using a Madurella Mycetomatis-specific PCR on Grains Obtained via Non-invasive Fine-needle Aspirated Material Is More Accurate than Cytology. Mycoses 2023, 66, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Ekeng, B.E.; Kwizera, R.; Salmanton-García, J.; Kibone, W.; van Rhijn, N.; Govender, N.P.; Meya, D.B.; Osaigbovo, I.I.; Hamer, D.H.; et al. Fungal Diseases in Africa: Closing the Gaps in Diagnosis and Treatment through Implementation Research and Advocacy. Journal of Medical Mycology 2023, 33, 101438. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Ahmed, A.; Ali, Y.; Bakhiet, S.M.; Mohamed, N.S.; Ahmed, E.S.; Fahal, A.H. Eumycetoma Medical Treatment: Past, Current Practice, Latest Advances and Perspectives. Microbiology Research 2021, 12, 899–906. [Google Scholar] [CrossRef]
- Kozel, T.R.; Wickes, B. Fungal Diagnostics. Cold Spring Harb Perspect Med 2014, 4, a019299. [Google Scholar] [CrossRef] [PubMed]
- Organic Law Determining the Administrative Entities of the Republic of Rwanda; Official Gazette of the Republic Rwanda: Kigali, 2005.
- Ruxin, J.; Negin, J. Removing the Neglect from Neglected Tropical Diseases: The Rwandan Experience 2008–2010. Global Public Health 2012, 7, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Ndoricyimpaye, E.L.; Obed, T.; Claude, H.J.; d’Amour, M.J.; Denyse, N.; Reverien, R. Candida Albicans Infection among HIV Positive and HIV Negative Women-Case Study at Butare University Teaching Hospital (CHUB), Southern Province of Rwanda. East Africa Science 2020, 2, 76–80. [Google Scholar] [CrossRef]
- Chrysostome, U.J.; Prudence, I.A.; Innocent, N.; Pierre, U.J.; Ezechiel, B.; Fabrice, U.; Julienne, M.; de Dieu, N.J.; Pacifique, M. Comparative Study of Candidiasis among Single and Married Women at Rwanda Military Hospital. Journal of Drug Delivery and Therapeutics 2024, 14, 59–63. [Google Scholar] [CrossRef]
- Jadin, J.B.; Vanderick, F.; Mbonyingabo, M. First Case of Histoplasma Duboisi in Rwanda. 1972. [Google Scholar]
- Dierckxsens, H.; Vanderick, F.; Vandepitte, J.; Ntabomvura, V. Premieres Observations d’histoplasmose à Histoplasma Capsulatum Au Rwanda. Ann Soc Belg Med Trop 1976, 56, 1–10. [Google Scholar] [PubMed]
- Raftopoulos, C.; Flament-Durand, J.; Coremans-Pelseneer, J.; Noterman, J. Intracerebellar Blastomycosis Abscess in an African Man. Clinical neurology and neurosurgery 1986, 88, 209–212. [Google Scholar] [CrossRef]
- Izimukwiye, A.I.; Mbarushimana, D.; Ndayisaba, M.C.; Bigirimana, V.; Rugwizangoga, B.; Laga, A.C. Cluster of Nasal Rhinosporidiosis, Eastern Province, Rwanda. Emerging Infectious Diseases 2019, 25, 1727. [Google Scholar] [CrossRef]
- Batungwanayo, J.; Taelman, H.; Lucas, S.; Bogaerts, J.; Alard, D.; Kagame, A.; Blanche, P.; Clerinx, J.; van de Perre, P.; Allen, S. Pulmonary Disease Associated with the Human Immunodeficiency Virus in Kigali, Rwanda. A Fiberoptic Bronchoscopic Study of 111 Cases of Undetermined Etiology. American journal of respiratory and critical care medicine 1994, 149, 1591–1596. [Google Scholar] [CrossRef] [PubMed]
- Buginco, C. Dermatophytic Infection of the Scalp in the Region of Butare (Rwanda). International Journal of Dermatology 1983, 22, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Bugingo, G. [Causal agents of tinea of the scalp in the region of Butare (Rwanda)]. Ann Soc Belg Med Trop 1993, 73, 67–69. [Google Scholar] [PubMed]
- Rusuku, G.; Buruchara, R.A.; Gatabazi, M.; Pastor-Corrales, M.A. Occurrence and Distribution in Rwanda of Soilborne Fungi Pathogenic to the Common Bean. Plant disease 1997, 81, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Gnat, S.; Łagowski, D.; Nowakiewicz, A.; Dyląg, M. A Global View on Fungal Infections in Humans and Animals: Opportunistic Infections and Microsporidioses. Journal of Applied Microbiology 2021, 131, 2095–2113. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.C.; Gurr, S.J.; Cuomo, C.A.; Blehert, D.S.; Jin, H.; Stukenbrock, E.H.; Stajich, J.E.; Kahmann, R.; Boone, C.; Denning, D.W.; et al. Threats Posed by the Fungal Kingdom to Humans, Wildlife, and Agriculture. mBio 2020, 11, e00449–20. [Google Scholar] [CrossRef] [PubMed]
- One Health: Fungal Pathogens of Humans, Animals, and Plants: Report on an American Academy of Microbiology Colloquium Held in Washington, DC, on October 18, 2017; American Academy of Microbiology Colloquia Reports; American Society for Microbiology: Washington, (DC), 2019.
- Zinsstag, J.; Hediger, K.; Osman, Y.M.; Abukhattab, S.; Crump, L.; Kaiser-Grolimund, A.; Mauti, S.; Ahmed, A.; Hattendorf, J.; Bonfoh, B.; et al. The Promotion and Development of One Health at Swiss TPH and Its Greater Potential. Diseases 2022, 10, 65. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Mahmoud, I.; Eldigail, M.; Elhassan, R.M.; Weaver, S.C. The Emergence of Rift Valley Fever in Gedaref State Urges the Need for a Cross-Border One Health Strategy and Enforcement of the International Health Regulations. Pathogens 2021, 10, 885. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Mohamed, N.S. Arboviral Diseases: The Emergence of a Major yet Ignored Public Health Threat in Africa. The Lancet Planetary Health 2020, 4, e555. [Google Scholar] [CrossRef]
- Ahmed, A.; Mohamed, N.S.; Siddig, E.E.; Algaily, T.; Sulaiman, S.; Ali, Y. The Impacts of Climate Change on Displaced Populations: A Call for Actions. The Journal of Climate Change and Health 2021, 100057. [Google Scholar] [CrossRef]
- Ahmed, A.; Hemaida, M.A.; Hagelnur, A.A.; Eltigani, H.F.; Siddig, E.E. Sudden Emergence and Spread of Cutaneous Larva Migrans in Sudan: A Case Series Calls for Urgent Actions. IDCases 2023, 32, e01789. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Abubakr, M.; Sami, H.; Mahdi, I.; Mohamed, N.S.; Zinsstag, J. The First Molecular Detection of Aedes Albopictus in Sudan Associates with Increased Outbreaks of Chikungunya and Dengue. International Journal of Molecular Sciences 2022, 23, 11802. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Eldigail, M.; Elduma, A.; Breima, T.; Dietrich, I.; Ali, Y.; Weaver, S.C. First Report of Epidemic Dengue Fever and Malaria Co-Infections among Internally Displaced Persons in Humanitarian Camps of North Darfur, Sudan. International Journal of Infectious Diseases 2021, 108, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Ali, Y.; Siddig, E.E.; Mohamed, N.; Ahmed, A. Rift Valley Fever and Malaria Co-infection: A Case Report. Clin Case Rep 2023, 11, e7926. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Mohamed, N.S.; Ahmed, A. Severe Coinfection of Dengue and Malaria: A Case Report. Clinical Case Reports 2024, 12, e9079. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; EL-Sadig, S.M.; Siddig, E.E. Guillain–Barre Syndrome Associated with Hepatitis E Virus Infection: A Case Report. Clinical Case Reports 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Ahmed, A. When Parasites Stray from the Path: A Curious Case of Ectopic Cutaneous Schistosoma Haematobium. QJM: An International Journal of Medicine 2023, 116, 794–795. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, A.T.H.; Abdelkhalig, R.E.; Hamid, E.; Ahmed, A.; Siddig, E.E. Recurrent Abdominal Wall Mass in a Hepatitis B-positive Male: An Unusual Case of Lumbar Mycetoma. Clinical Case Reports 2023, 11, e8275. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, A.T.H.; Abdelkhalig, R.E.; Hamid, E.; Ahmed, A.; Siddig, E.E. Unusual Manifestation of Cystic Mycetoma Lesions: A Case Report. Clinical Case Reports 2023, 11, e8054. [Google Scholar] [CrossRef]
- Ahmed, A.; Hagelnur, A.A.; Eltigani, H.F.; Siddig, E.E. Cutaneous Tuberculosis of the Foot Clinically Mimicking Mycetoma: A Case Report. Clin Case Rep 2023, 11, e7295. [Google Scholar] [CrossRef]
- Driemeyer, C.; Falci, D.R.; Oladele, R.O.; Bongomin, F.; Ocansey, B.K.; Govender, N.P.; Hoenigl, M.; Gangneux, J.P.; Lass-Flörl, C.; Cornely, O.A. The Current State of Clinical Mycology in Africa: A European Confederation of Medical Mycology and International Society for Human and Animal Mycology Survey. The Lancet Microbe 2022, 3, e464–e470. [Google Scholar] [CrossRef] [PubMed]
- Clinton Health Access Initiative (CHAI). The Road to Zero: Report on the Implementation of the Advanced HIV Disease Package of Care in Low- and Middle-Income Countries, 2022.
- Tufa, T.B.; Bongomin, F.; Fathallah, A.; Cândido, A.L.S.; Hashad, R.; Abdallaoui, M.S.; Nail, A.A.; Fayemiwo, S.A.; Penney, R.O.; Orefuwa, E.; Denning, D.W. Access to the World Health Organization-recommended essential diagnostics for invasive fungal infections in critical care and cancer patients in Africa: a diagnostic survey. Journal of infection and public health 2023, 16, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Summarizes the WHO list of fungal priority pathogens (adopted from the WHO open access report [3].
Figure 1.
Summarizes the WHO list of fungal priority pathogens (adopted from the WHO open access report [3].
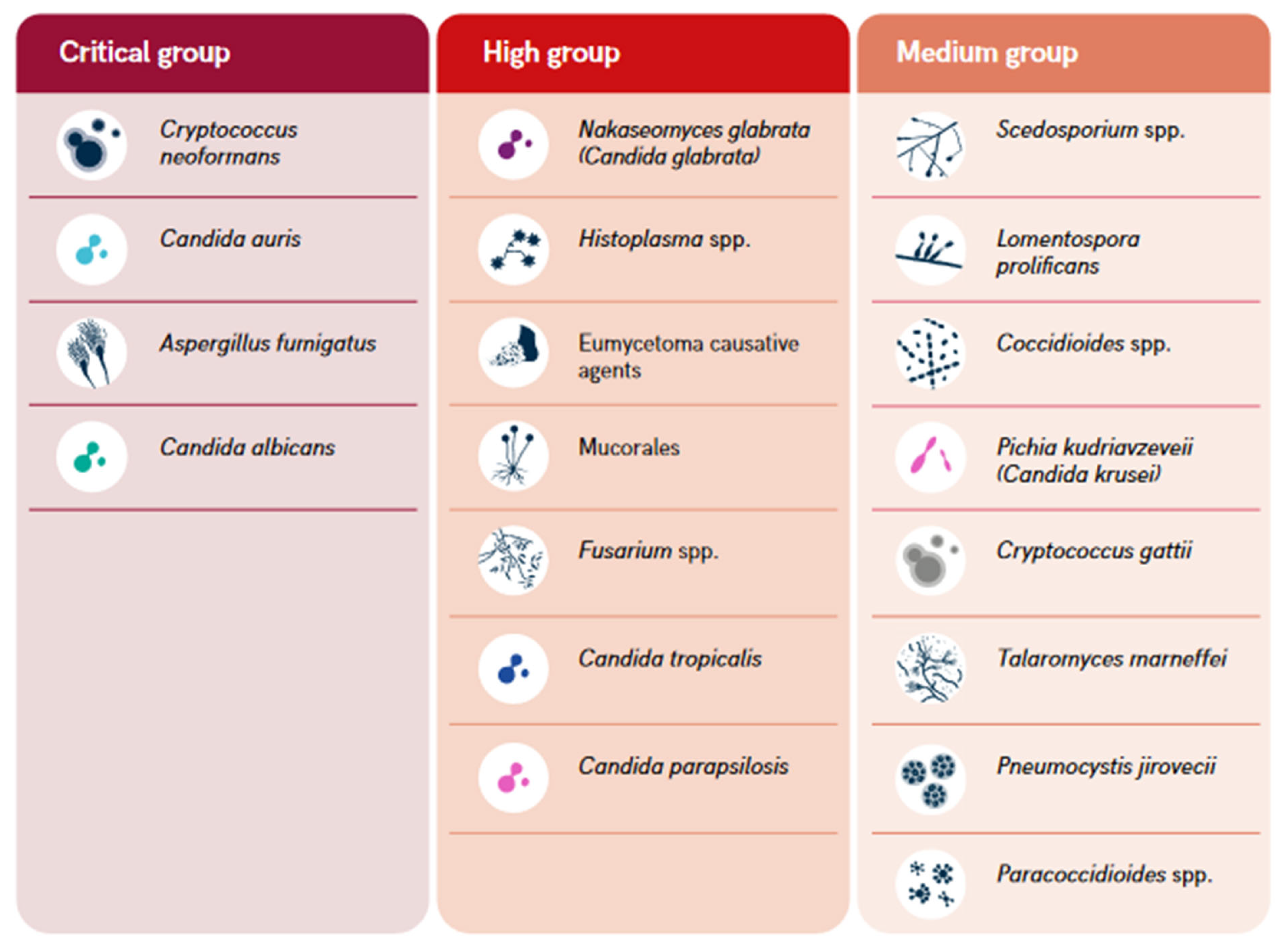
Figure 2.
Diagram shows the limited reporting (possibly the detection) of fungal infections in Rwanda since ever until 2022.
Figure 2.
Diagram shows the limited reporting (possibly the detection) of fungal infections in Rwanda since ever until 2022.
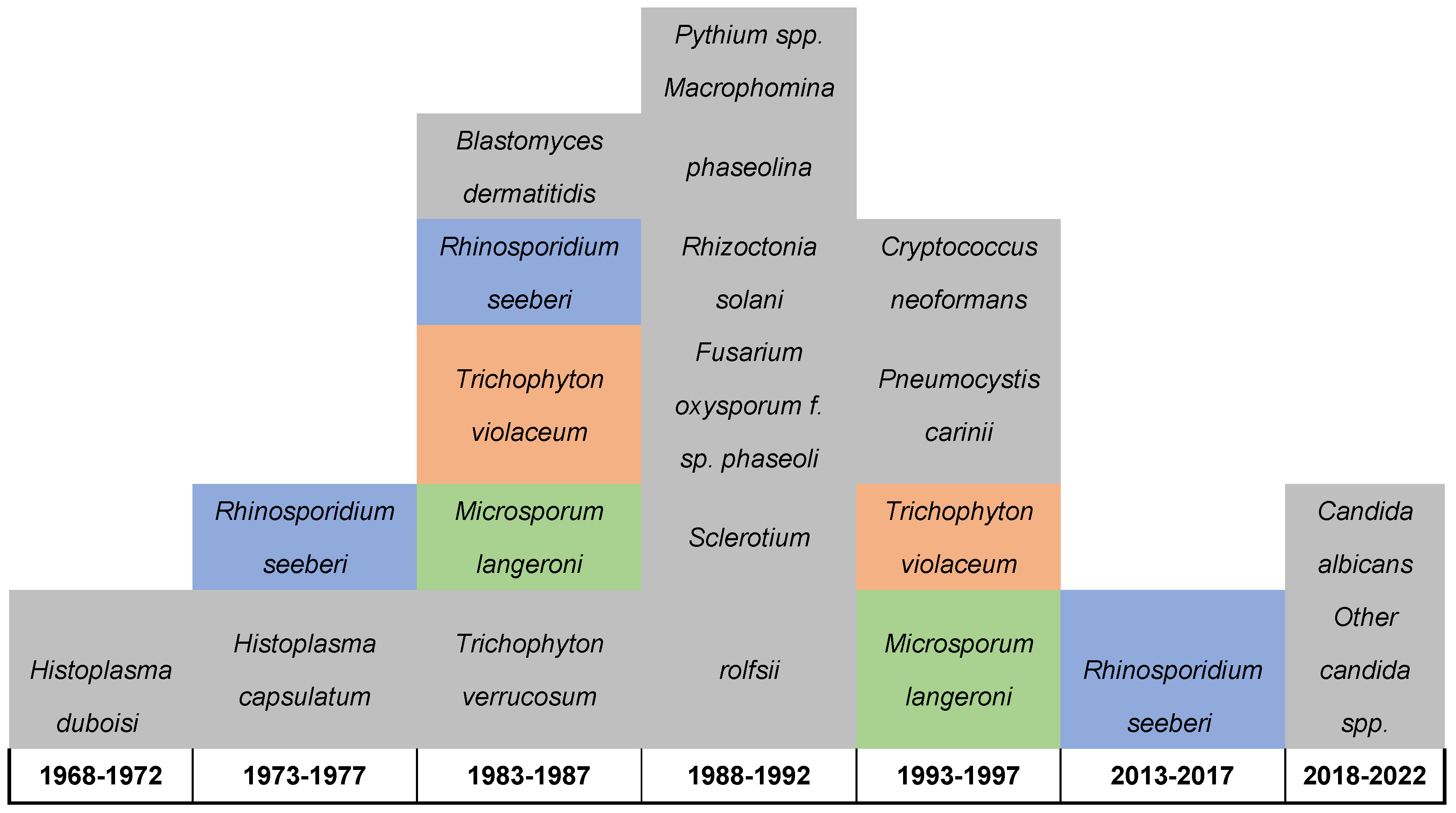

Table 1.
Summarizes the diversity, geographical distribution, year of report, and site of isolation of fungal infections reported in Rwanda between 1972 and 2022.
Table 1.
Summarizes the diversity, geographical distribution, year of report, and site of isolation of fungal infections reported in Rwanda between 1972 and 2022.
| # | Fungal Name | Site of isolations | Year | Diagnostic tool used | District | Reference |
|---|---|---|---|---|---|---|
| 1 |
Candida albicans Other candida spp. |
Vagina | 2021-2022 | Culture technique | Kicukiro District | 19 |
| 2 |
Candida albicans Other candida spp., |
Vagina | 2020 | Culture technique | Huye District | 18 |
| 3 | Rhinosporidium seeberi | Nasal | 2016 | Histopathology | Kirehe District | 23 |
| 4 | Rhinosporidium seeberi | Nasal | 2014-2015 | Histopathology | Gatsibo District | 23 |
| 5 | Cryptococcus neoformans | Respiratory and Brain | 1994 | Culture and histopathology | Kigali District | 24 |
| 6 | Pneumocystis carinii | Respiratory | 1994 | Cytology | Kigali District | 24 |
| 7 | Trichophyton violaceum | Scalp | 1993 | Direct microscope and culture | Butare Distirct | 26 |
| 8 | Microsporum langeroni | Scalp | 1993 | Direct microscope and culture | Butare Distirct | 26 |
| 9 | Pythium spp. | Bean | 1989-1990 | Symptoms, colony characteristics, reproductive structures, and pathogenicity assessments | Gikongoro; Butare; Gitarama; Kigali; Byumba; Ruhengeri; Gisenyi and Kibungo | 27 |
| 10 |
Macrophomina phaseolina |
Bean | 1989-1990 | Symptoms, colony characteristics, reproductive structures, and pathogenicity assessments | Gikongoro; Butare; Gitarama; Kigali; Byumba; Ruhengeri; Gisenyi and Kibungo | 27 |
| 11 | Rhizoctonia solani | Bean | 1989-1990 | Symptoms, colony characteristics, reproductive structures, and pathogenicity assessments | Gikongoro; Butare; Gitarama; Kigali; Byumba; Ruhengeri; Gisenyi and Kibungo | 27 |
| 12 | Fusarium oxysporum f. sp. phaseoli | Bean | 1989-1990 | Symptoms, colony characteristics, reproductive structures, and pathogenicity assessments | Gikongoro; Butare; Gitarama; Kigali; Byumba; Ruhengeri; Gisenyi and Kibungo | 27 |
| 13 |
Sclerotium rolfsii |
Bean | 1989-1990 | Symptoms, colony characteristics, reproductive structures, and pathogenicity assessments | Gikongoro; Butare; Gitarama; Kigali; Byumba; Ruhengeri; Gisenyi and Kibungo | 27 |
| 14 | Blastomyces dermatitidis | Cerebellar | 1986 | Immunology, Histopathology | Kigali district | 22 |
| 15 | Rhinosporidium seeberi | Conjunctiva | 1986 | Histopathology | NA | 23 |
| 16 | Trichophyton violaceum | Scalp | 1983 | Direct microscopic | Butare Distirct | 25 |
| 17 | Microsporum langeroni | Scalp | 1983 | Direct microscopic | Butare Distirct | 25 |
| 18 | Trichophyton verrucosum | Scalp | 1983 | Direct microscopic | Butare Distirct | 25 |
| 19 | Rhinosporidium seeberi | Nasal | 1975-1977 | Histopathology | NA | 23 |
| 20 | Histoplasma capsulatum | NA | 1976 | NA | NA | 21 |
| 21 | Histoplasma duboisi | Disseminated infection | 1972 | Culture technique | Butaro District | 20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



