
Submitted:
09 July 2024
Posted:
10 July 2024
You are already at the latest version
Abstract
Knee osteoarthritis (KO) is an important health condition, affecting one third of the people aged 65 years or more. Pain is the main cause of disability. Pain management in KO includes pharmacological and non-pharmacological modalities. Patient education, lifestyle changes, physical exercise and physical agents are prescribed as a first approach for pain control. Laser therapy is part of many therapeutical protocols, with two forms, low-level laser therapy (LLLT) and high-intensity laser therapy (HILT). The paper aimed at stressing the advantages of HILT, based on a greater wavelength, higher energy delivery and deeper tissue penetration. Research on 23 published trials revealed that analgesic effect is rapid, cumulative and long lasting. Compared to sham, to LLLT or to other associations of therapeutical modalities, HILT provided significantly better results on pain reduction and functional improvement. Ultrasound examination showed reduction of intraarticular inflammation.
Keywords:
knee osteoarthritis
; high-intensity laser therapy
; pain management
1. Introduction
Knee osteoarthritis (KO) represents an important health issue, affecting one third of the people after the age of 65 years [1]. Before age of 50 years, men are more prone to develop KO, and after this age, women are more affected, as more complex hormonal and metabolic changes occur [2]. KO disability arises mainly from pain and, as disease progresses, from movement limitation, misalignment and muscle imbalance.
Laser therapy (LT) is a non-invasive and painless method, which can be applied in a wide variety of conditions [3]. Although low level laser therapy (LLLT) is more commonly used, high intensity laser therapy (HILT) is a new, painless, and strong method with higher density radiation. With a wavelength of 1064, HILT devices can provide deeper penetration. As a difference from LLLT, biological effects of HILT are based less on chromofore absorption and rather on photochemical reactions (as increasing mitochondrial oxidative reaction and adenosine triphosphate, RNA and DNA production) and photobiostimulatory effects. The advantage of HILT over LLLT is that it can reach deeper and larger joints. Through deep thermal action, HILT increases local blood circulation, improves tissue regeneration, and reduces pain and edema. A few studies conducted on osteoarthritis, particularly on knee osteoarthritis (KO) raised attention to this topic and we aimed at summarizing their findings into this paper to raise attention on a new therapeutical method.
Miofascial pain syndrome is a very common cause of disability in the population and an important issue to be addressed in therapy. HILT associated with physical exercise was found more effective that exercise alone in trapezius localization [4,5]. HILT was effective in improving pain in cervical myofascial pain syndrome but not the cervical range of motion (ROM) concluded a meta-analysis, mentioning that, due to the heterogeneity of the trials, the latter allegation could be biased [6]. For chronic neck pain, an association of HILT and physical exercise improved significantly pain and mobility [7]. Subacromial impingement syndrome was successfully managed with a combination of HILT and exercise in terms of pain and function [8]. Patients with low back pain, a frequent health issue, reported improvement of pain and functional status when receiving HILT and physical exercise [9].
Controversial results were reported for HILT in plantar fasciitis management, as different groups of researchers stressed either the effectiveness [10] or the lack of it [11,12] in pain reduction or in functioning [13], inviting further studies. Furthermore, a systematic review from 2020 concludes that HILT may be beneficial in a poly-modal approach of musculoskeletal pain [14].
2. Materials and Methods
Two researchers (D.P., M.I.S.) independently performed a search in the available literature from inception up to May 2024, of databases on PubMed, Google Scholar, Web of Science using a combination of MeSH terms „high intensity laser therapy”, „high-level lase therapy”, „high power laser”, „HILT”, „HLLT” and „knee osteoarthritis”, „gonarthrosis”.
Following the PICO model, we defined inclusion criteria. The inclusion criteria were: 1) papers containing randomized controlled trials, case reports, case series, pilot studies on human adult subjects (above 18 years old) with a 2) diagnosis of KO based on ACR criteria (P), 3) HILT was a therapeutical intervention (I), 4) compared to sham, LLLT and other therapeutical interventions (C), 5) well-defined clinical outcomes: improvement in pain, function, disability, ultrasound examination (O). There were selected articles written in English with full text available. The selection offered 136 papers. Duplicates were excluded and there remained 115 records. During the eligibility process, the authors excluded reviews, systematic, meta-analysis and studies on animal subjects and in vitro studies and there remained 24 papers. One paper lacked full text in English and was excluded. Finally, 23 papers fulfilled the criteria and were included in the actual research. Disagreements were discussed until a consensus was reached. When needed, a third researcher (D.C.) became involved. According to PEDro scale on the quality of RCT, one study had a score under 5; however, the authors decided to retain the paper on the consideration of the number of patients and the accuracy of the protocol. Another trial scored 6 on PEDro scale, the remaining 21 papers scored between 7 and 11. A score of ≥ 7 is considered to be a study of high methodological quality, while a score of ≤ 5 is considered to be of low methodological quality.
See Figure 1. Selection process of relevant trials.
3. Results
The selected 23 papers (with a total number of 1175 patients) were as follows: one prospective, clinical, before and after treatment [15], one prospective, clinical, before and after treatment case series [16], one prospective, open label, before and after clinical trial [17] and 20 prospective randomized trials [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37].
As specified in the inclusion criteria, all papers included patients with KO according to ACR criteria. The severity of KO was assessed with Kelgren and Lawrence criteria and all papers included patients with grades 2 and 3. Pain was the main outcome for all trials and assessed with Visual Analogue Scale. Function was noted mostly with WOMAC index and range of motion ROM, especially on active flexion; one trial used also Lequesne Scale [17]. Disability was assessed in two studies with Knee Injury and Osteoarthritis Outcome Score (KOOS), an auto-administered questionnaire [33,34]. Gait analysis was performed in a small number of studies using different tools (pedobarometry, walking distance without pain, timed up and go test TUG, 6-min walk test 6MWT, 50-feet walk test). Four studies performed knee ultrasound examination following cartilage and synovial thickness and intraarticular fluid. [23,26,31,36] One trial used Berg Balance Scale. [37] See Table 1. The selected trials included in the research
4. Discussion
The management of KO is a complex approach, including medication, physical therapy, behavioral changes, education. Intraarticular hyaluronic acid (HA) is an important step in this process. A prospective randomized study (2009) on 41 patients compared functional status after 4 weekly intraarticular infiltrations with HA versus 10 HILT sessions (2000 – 3000 J / session) on alternate days. Results were compared after therapy and 4 months later. Both groups improved significantly after treatment and maintained progress 4 months later, with no difference between groups. This study introduced HILT as a tool in KO therapy [18].
A prospective, clinical, pre- and post-treatment trial (2011) on 96 patients treated with HILT, ten consecutive daily sessions, showed significant improvement of knee pain after treatment [15]. A case series of 39 former football players with KO received 1 – 3 daily sessions of HILT and reported pain reduction and clinical improvement of swelling and numbness at the end of the treatment and maintenance of the result after one and 3 weeks [16].
We present the papers according to randomization method, comparing HILT to sham, to LLLT and to other physical agents.
4.1. HILT versus Sham/Placebo
Eight trials with a total of 385 patients, compared different regimens of HILT with sham (placebo). Two studies (123 patients) compared HILT alone with sham, on pain, function and gait [17,22]. They concluded that HILT was associated with significant improvements in all items after treatment and the results were maintained at 3 and 4 months. The regimens were either 10 alternate days sessions or 7 daily sessions, with 3000 J/session and biostimulator effect. Six studies compared HILT associated with different conservative therapies (physical exercise, hot packs + interferential therapy + physical exercise, NSAID + topic ointments + physical exercise). Pain (assessed on VAS), function (WOMAC index) and ultrasonographic measurements (femoral condylar cartilage thickness and suprapatellar fluid) were performed at baseline, after treatment and after a timeframe of 4 weeks to 3 months. All trials reported significant improvement of all parameters in intragroup analysis at all moments. As for intergroup analysis, most trials (4 out of 6) reported significant better result in the HILT group for pain and function. Ultrasound measurement of intraarticular fluid found important reduction after HILT therapy [21,26,28,31,32,36] One trial failed to identify a notable difference for HILT versus sham in pain and function [31], whereas one trial reported significant improvement in pain only, not in function [28].
4.2. HILT versus LLLT
LLLT was a longtime part of pain therapy. Five trials compared the two forms of laser therapy (LLLT, HILT), either in monotherapy [27,37] or associated with physical exercise [20,34,35]. A total number of 247 patients reported significant improvement of pain (VAS scores), function (WOMAC index, 50-feet walk test, TUG) and disability (KOOS) in intragroup analysis at the end of therapy and one month later and better results in the HILT group. Compared to sham, both LLLT and HILT were followed by clinical improvement. HILT produced significant improvement in pain scores versus LLLT in all trials. Function was documented in several ways, with an accent on disability evaluation (Berg Balance Scale, TUG, 50-feet walk test) and results were significantly better for HILT patients. Protocols of HILT therapy varied from once a week for 12 weeks, 2 sessions/week for 4 - 6 weeks, 3 sessions/week for 2 weeks to 10 daily sessions. Doses were in the analgesic range (300 J) followed by biostimulatory effect (3000 J) [20,27,34,35,37]
4.3. HILT versus Other Therapeutic Modalities
Six trials included 331 patients receiving therapeutic protocols using different forms of physical agents with analgesic purpose and therapeutical exercise to evaluate the effectiveness of HILT. It is worth noting that all the following schemes included physical exercise as a cornerstone, underlying her importance in the management of KO. The association with different modalities was thought to add value to therapy. Two sessions/week for 3 weeks of either HILT, LLLT or therapeutical ultrasound showed significant better results for HILT on knee pain and function (walking distance and squatting without pain) [19]. Three sessions/week for 4 weeks of either HILT or conventional therapy (TENS + ultrasound) were followed by significant improvements of pain and function (flexion ROM, TUG, 6MWT and WOMAC) in HILT group. The difference was significant at 12 weeks after treatment completion, pleading for a remanent effect of HILT [24]. Ten HILT sessions over 2 weeks proved to be more effective on pain and function (ROM and WOMAC) than low-intensity pulsed ultrasound (LIPUS) [29]. HILT and hot pack for 10 sessions over 2 weeks proved to be more efficient than ultrasound, TENS and hot pack on pain and function (WOMAC), with remanent effect after 6 weeks [25]. HILT (3 sessions/week, 4 weeks) were significantly better than ESWT (4 weekly sessions) on pain and function (WOMAC, 6MWT) after treatment completion [30]. Comparing eight weekly sessions of HILT to high-intensity magnetic stimulation (HIMS) with a standard protocol (shockwave therapy, TENS, massage, physical exercise) showed better scores for pain and function in the HILT patients after therapy [33]. Two of the six above-mentioned trials followed patients after the end of the therapy for 6 and 12 weeks and noted persistence of significant better results for HILT therapeutical schemes [24,25].
A study on different combinations between HILT, glucosamine/chondroitin sulphate (GCS) and physical exercise proved that 2 sessions/week for 6 weeks HILT, together with GCS and physical exercise carried out significantly improvement of pain, function (WOMAC) and ultrasound-measured synovial thickness at the end of treatment; results were maintained 3 months later. Femoral condylar cartilage thickness remained unchanged during the study [23].
5. Conclusions
The analysis performed by the authors lead to the conclusion that HILT is effective in pain reduction, outperforming LLLT and some associations between physical modalities or drug administration. When function and disability were assessed, HILT may produce significant improvement. Remanence of the achievements was documented for an interval between one week and 4 months in 10 out of the 23 trials.
Pain management in musculoskeletal pathologies, including osteoarthritis, is a major cause of disability and a challenge for the clinician. In the pharmacological approach, aside from conventional drugs (NSAIDs, analgesic), new modalities are investigated, such as platelet rich plasma and botulinum toxin [38,39]. In the non-pharmacological approach, new forms of magnetic, ultrasound, shockwave and laser therapy promise additional benefits [40].
The actual use of light therapy in rehabilitation includes laser, with two classes of power, class 3b, low level laser therapy, LLLT, (500 mW or less) and class 4, high intensity lasers, HILT (greater than 500 mW.) LLLT, known under the name of cold lasers, with wavelengths between 632,8 nm and 830 nm, have a small penetration (2 – 3 mm to 2 – 4 cm) and produces biological effects after photons absorption by chromophores. HILT is defined by greater wavelength, 1064 nm, that assures a deeper penetration (up to 10 – 12 cm) and a greater energy delivery. HILT biological effects are based on thermal and chemical effects. The main indication of HILT is pain control through an association of peripheral and central mechanisms. Peripheral mechanisms include spinal gate control modulation, substance P decrease, whereas central mechanisms include endogenous opioid release. In the peripheral tissues, HILT reduces the release of bradykinin and histamine, increasing pain perception threshold.
Researchers aimed to underline the advantages of HILT in musculoskeletal pathology; the present paper focusing on knee osteoarthritis, as a major cause of disability in adult and old population.
Before- and after trials showed the HILT is associated with pain reduction after the first session, with continuing improvement after up to 10 sessions, and remanent result after one to 3 weeks. Compared to placebo/sham, HILT had significant better pain and functional improvement at the end of the therapy that was maintained up to 3 months. However, one trial failed to document any superiority of HILT over placebo regarding the functional status of the patients. HILT and LLLT were able to achieve significant pain control and functional improvement at the completion of the therapy, lasting for at least one month. HILT was found to have better values than LLLT at all moments. Adding HILT to the conservative management of the KO (physical exercise, different combinations of physical agents, oral glucosamine/chondroitin supplements) was documented to improve significantly pain and functional status and reduce disability. Ultrasound examination of the osteoarthritic knee revealed reduction of joint effusion and synovial thickness. It is questionable any evolution of cartilage thickness, as a small number of trials carried out controversial results.
Doses and timing of HILT applications varied through the published papers. Although analgesic action may be visible after a small number of sessions (one to three), most of researchers agree on an amount of 8 to 12 sessions, either daily or with a frequency of 2 – 3/week. Doses per session are mostly 300 J for analgesic effect and 3000 J for biostimulatory action.
Research documented the immediate effect of HILT on pain and function. Some papers followed patients for variable timeframes after therapy and reported maintenance of results after 1 week to 4 months.
This paper underlines the immediate, cumulative and long-lasting analgesic effect of HILT. Function and disability are a direct consequence of pain, but other factors, as inflammation and contractures contribute. Due to deep thermal action, HILT may act on those factors affecting functioning and disability, producing significant improvement comparative to other physical agents.
Pain, functioning and disability approach in KO is based on pharmacological and non-pharmacological modalities; the last ones including patient education and life-style modification, physical exercise and a combination of physical agents, among them HILT with an important analgesic and anti-inflammatory effect.
HILT was used the management of different shoulder pathologies, as subacromial impingement syndrome [41] and frozen shoulder [42], chronic cervical pain [7] or low back pain [43].
High-intensity laser therapy produced significant improvements in pain, and may improve functioning and disability of patients with knee osteoarthritis. HILT must be a part of therapeutic approach of KO, as a non-pharmacologic tool, to increase the effectiveness of associated modalities.
Author Contributions
Conceptualization, D.P. and C.G.P.; methodology, D.P., D.C. and M.I.S; investigation, C.G.P. and M.I.S.; resources, M.I.S.; data curation, C.G.P.; writing—original draft preparation, D.P.; writing—review and editing, D.C.; visualization, D.P.; supervision, D.C. All authors have read and agreed to the published version of the manuscript.
Funding
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila, through the institutional program Publish not Perish.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are available on internet resources.
Acknowledgments
Not applicable
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Turkiewicz. A.; Petersson. I.F.; Bjork. J.; et al. Current and future impact of osteoarthritis on health care: A population-based study with projections to year 2032. Osteoarthritis Cartilage. 2014; 22(11): 1826-32. [CrossRef]
- Nasui. B.A.; Talaba. P.; Nasui. G.A.; et al. The Influence of Diet and Physical Activity on Oxidative Stress in Romanian Females with Osteoarthritis. Nutrients. 2022 Oct 7;14(19):4159. [CrossRef] [PubMed] [PubMed Central]
- Arroyo-Fernández. R.; Aceituno-Gómez. J.; Serrano-Muñoz. D.; et al. High-Intensity Laser Therapy for Musculoskeletal Disorders: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Journal of Clinical Medicine. 2023; 12(4):1479. [CrossRef]
- Dundar. U.; Turkmen. U.; Toktas. H; et al. Effect of high-intensity laser therapy in the management of myofascial pain syndrome of the trapezius: a double-blind, placebo-controlled study. Lasers Med Sci. 2015 Jan;30(1):325-32. Epub 2014 Oct 2. [CrossRef] [PubMed]
- Ahmed. H.; Abu Taleb. E.; Ameen. F. High intensity laser therapy on pain in patients with myofascial trigger points. Egyptian Journal of Physical Therapy.2020;3(1), 1-8. [CrossRef]
- de la Barra Ortiz. H.; Liebano. R.E.; Vera. MA.; et al. Effectiveness of high-intensity laser therapy added to a physical therapy program for the treatment of myofascial pain syndrome - a systematic review and meta-analysis. Advances in Rehabilitation. 2022, 36(3), 35-48. [CrossRef]
- Alayat. M.S.M.; Mohamed. A.A.; Helal. O.F. et al. Efficacy of high-intensity laser therapy in the treatment of chronic neck pain: a randomized double-blind placebo-control trial. Lasers Med Sci. 2016, 31, 687–694 (2016). [CrossRef]
- Yılmaz. M.; Eroglu. S.; Dundar. U.; et al. The effectiveness of high-intensity laser therapy on pain, range of motion, functional capacity, quality of life, and muscle strength in subacromial impingement syndrome: a 3-month follow-up, double-blinded, randomized, placebo-controlled trial. Lasers Med Sci. 2022, 37, 241–250 (2022). [CrossRef]
- Gocevska. M.; Nikolikj-Dimitrova. E.; Gjerakaroska-Savevska. C. Effects of High - Intensity Laser in Treatment of Patients with Chronic Low Back Pain. Open access Macedonian journal of medical sciences, 2019, 7(6), 949–954. [CrossRef]
- Ordahan. B.; Karahan. A.Y.; Kaydok. E. The Effect of High-Intensity versus Low-Level Laser Therapy in the Management of Plantar Fasciitis: A Randomized Clinical Trial. Lasers Med. Sci. 2018, 33, 1363–1369.
- Tkocz. P.; Matusz. T.; Kosowski. Ł. et al. A Randomised-Controlled Clinical Study Examining the Effect of High-Intensity Laser Therapy (HILT) on the Management of Painful Calcaneal Spur with Plantar Fasciitis. J. Clin. Med. 2021, 10, 4891. [CrossRef]
- Naruseviciute. D.; Kubilius. R. The effect of high-intensity versus low-level laser therapy in the management of plantar fasciitis: randomized participant blind controlled trial. Clinical Rehabilitation. 2020;34(8):1072-1082. [CrossRef]
- Yesil. H.; Dundar. U.; Toktas. H. et al. The effect of high intensity laser therapy in the management of painful calcaneal spur: a double blind, placebo-controlled study. Lasers Med Sci. 2020, 35, 841–852 (2020). [CrossRef]
- Ezzati. K.; Laakso. E. L.; Salari. A. et al. The Beneficial Effects of High-Intensity Laser Therapy and Co-Interventions on Musculoskeletal Pain Management: A Systematic Review. Journal of lasers in medical sciences, 2020,11(1), 81–90. [CrossRef]
- Štiglić-Rogoznica. N.; Stamenković. D.; Frlan-Vrgoč. L.; et al. Analgesic effect of high intensity laser therapy in knee osteoarthritis. Collegium antropologicum, 2011, 35 Suppl 2, 183-5. PMID: 22220431.
- White. P.F.; Cao. X.; Elvir-Lazo. L.; et al. Effect of High-Intensity Laser Treatments on chronic pain related to osteoarthritis in former professional athletes: A case series. J Mol Biomark Diagn 2017; 8: 343. [CrossRef]
- Viliani. T.; Carabba. C.; Mangone. G.; Pasquetti. P. High intensity pulsed Nd: YAG laser in painful knee osteoarthritis: the biostimulating protocol. Energy for Health. 2012;9:18–22.
- Viliani. T.; Ricci. E.; Mangone. G.; Graziani. C.; Pasquetti P. Effects of Hilterapia vs.Visco supplementation in knee osteoarthritis patients a randomized controlled clinical trial. Energy for Health. 2009;3:14–17.
- Sabbahi. S. I. Clinical experience using HilterapiaⓇ in ‘knee arthrosis’ Energy for Health. 2009;4, article 24.
- Kheshie. A.R.; Alayat. M.S.; Ali. M.M. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: a randomized controlled trial. Lasers Med Sci. 2014 Jul;29(4):1371-6. Epub 2014 Feb 1. [CrossRef] [PubMed]
- Kim. G.J.; Choi. J.; Lee. S.; Jeon. C.; Lee. K. The effects of high intensity laser therapy on pain and function in patients with knee osteoarthritis. J Phys Ther Sci. 2016 Nov;28(11):3197-3199. Epub 2016 Nov 29. [CrossRef] [PubMed] [PubMed Central]
- Angelova. A.;, Ilieva. E.M. Effectiveness of High Intensity Laser Therapy for Reduction of Pain in Knee Osteoarthritis, Pain Research and Management, 2016, Article ID 9163618, 11 pages, 2016. [CrossRef]
- Alayat. M.S.M.; Aly. T.H.A.; Elsayed. A.E.M. et al. Efficacy of pulsed Nd:YAG laser in the treatment of patients with knee osteoarthritis: a randomized controlled trial. Lasers Med Sci 2017, 32, 503–511. [CrossRef]
- Nazari. A.; Moezy. A.; Nejati. P.; Mazaherinezhad. A. Efficacy of high-intensity laser therapy in comparison with conventional physiotherapy and exercise therapy on pain and function of patients with knee osteoarthritis: a randomized controlled trial with 12-week follow up. Lasers Med Sci. 2019 Apr;34(3):505-516. Epub 2018 Sep 3. [CrossRef] [PubMed]
- Ciplak. E.; Akturk. S.; Buyukavci. R.; Ersoy. Y. Efficiency of high intensity laser therapy in patients with knee osteoarthritis. Medicine Science| International Medical Journal. 2018;7:724–727. [CrossRef]
- Akaltun. M.S.; Altindag. O.; Turan. N.; et al. Efficacy of high intensity laser therapy in knee osteoarthritis: a double-blind controlled randomized study. Clin Rheumatol 2021;40, 1989–1995. [CrossRef]
- Koevska. V.; Nikolic-Dimitrova. E.; Mitrevska. B.; et al. Application of high-intensity laser in pain treatment of patients with knee osteoarthritis. Arch Pub Health. 2021 Nov. 20;13(2):78-90. Available from: https://www.id-press.eu/aph/article/view/6008. [CrossRef]
- Siriratna. P.; Ratanasutiranont. C.; Manissorn. T.; et al. Short-Term Efficacy of High-Intensity Laser Therapy in Alleviating Pain in Patients with Knee Osteoarthritis: A Single-Blind Randomised Controlled Trial. Pain Res Manag. 2022 Oct 21;2022:1319165. [CrossRef] [PubMed] [PubMed Central]
- Samaan. S.S.R.R.; Sedhom. M.G.; Grace. M.O. A randomized comparative study between high-intensity laser vs low-intensity pulsed ultrasound both combined with exercises for the treatment of knee osteoarthritis. Int J Rheum Dis. 2022; 25(8):877–886. [CrossRef]
- Mostafa. M.S.E.M.; Hamada. H.A.; Kadry. A.M.; Zahran. S.S.; Helmy. N.A. Effect of High-Power Laser Therapy Versus Shock Wave Therapy on Pain and Function in Knee Osteoarthritis Patients: A Randomized Controlled Trial. Photobiomodul Photomed Laser Surg. 2022 Mar;40(3):198-204. Epub 2022 Jan 5. [CrossRef] [PubMed]
- Ekici. B.; Ordahan. B. Evaluation of the effect of high-intensity laser therapy (HILT) on function, muscle strength, range of motion, pain level, and femoral cartilage thickness in knee osteoarthritis: randomized controlled study. Lasers Med Sci. 2023 Sep 25;38(1):218. [CrossRef] [PubMed]
- Taheri. P.; Maghroori. R.; Aghaei. M. Effectiveness of High-intensity Laser Therapy for Pain and Function in Knee Osteoarthritis: A Randomized Controlled Trial. Middle East J Rehabil Health Stud. 2024;11(1):e134330. [CrossRef]
- Katana. B.; Macak. A.; Kaljić. E.; Mujezinovic. A.; et al. Comparative analysis of different physical therapy programs in the treatment of people with knee osteoarthritis. Journal of Health Sciences. 2023. [CrossRef]
- Ahmad. M.A.; Moganan. M.A.; Hamid. M.S.; et al. Comparison between Low-Level and High-Intensity Laser Therapy as an Adjunctive Treatment for Knee Osteoarthritis: A Randomized, Double-Blind Clinical Trial. Life. 2023; 13(7):1519. [CrossRef]
- Astri. S.W.; Murdhana. N.; Nusdwinuringtyas. N.; et al. The Comparison Of The Low-Level Laser Therapy And High Intensity Laser Therapy On Pain And Functional Ability In Knee Osteoarthritis. Journal Of The Indonesian Medical Association. 2023; 72(6), 275 - 283. [CrossRef]
- Roheym. M.I.; Morsy. M.E.; Saber. M.; et al. Impact of high-power laser therapy on bilateral knee osteoarthritis: A randomized trial. Fizjoterapia Polska. 2023 23(5); 162-168. [CrossRef]
- Wibisono. K.; Handoyo. R.; Setiawati. E. Comparison Of The Effectiveness Of High Intensity Laser Therapy (HILT) And Low-Level Laser Therapy (LLLT) On Improving Balance In Knee Osteoarthritis. Medica Hospitalia: Journal of Clinical Medicine. 2024; 11. 33-37. [CrossRef]
- Brosseau. L.; Taki. J.; Desjardins. B.; et al. The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Clin Rehabil. (2017) 31:582–624. [CrossRef]
- Poenaru. D.; Sandulescu. M.I.; Cinteza. D. Pain Modulation in Chronic Musculoskeletal Disorders: Botulinum Toxin, a Descriptive Analysis. Biomedicines. 2023 Jul 3;11(7):1888. [CrossRef] [PubMed] [PubMed Central]
- Poenaru. D.; Sandulescu. M.I.; Cinteza. D. Biological effects of extracorporeal shockwave therapy in tendons: A systematic review. Biomed Rep. 2022 Dec 29;18(2):15. [CrossRef] [PubMed] [PubMed Central]
- Karaca. B. Effectiveness of high-intensity laser therapy in subacromial impingement syndrome. Photomed Laser Surg 2016;34:223–228. [CrossRef]
- Kim. S.H.; Kim. Y.H.; Lee. H.R.; Choi. Y.E. Short-term effects of high-intensity laser therapy on frozen shoulder: a prospective randomized control study. Man Ther 2015;20:751–757. [CrossRef]
- Choi. H.W.; Lee. J.; Lee. S.; et al. Effects of high intensity laser therapy on pain and function of patients with chronic back pain. J Phys Ther Sci 2017;29:1079–1081. [CrossRef]
Figure 1.
Selection process of relevant trials.
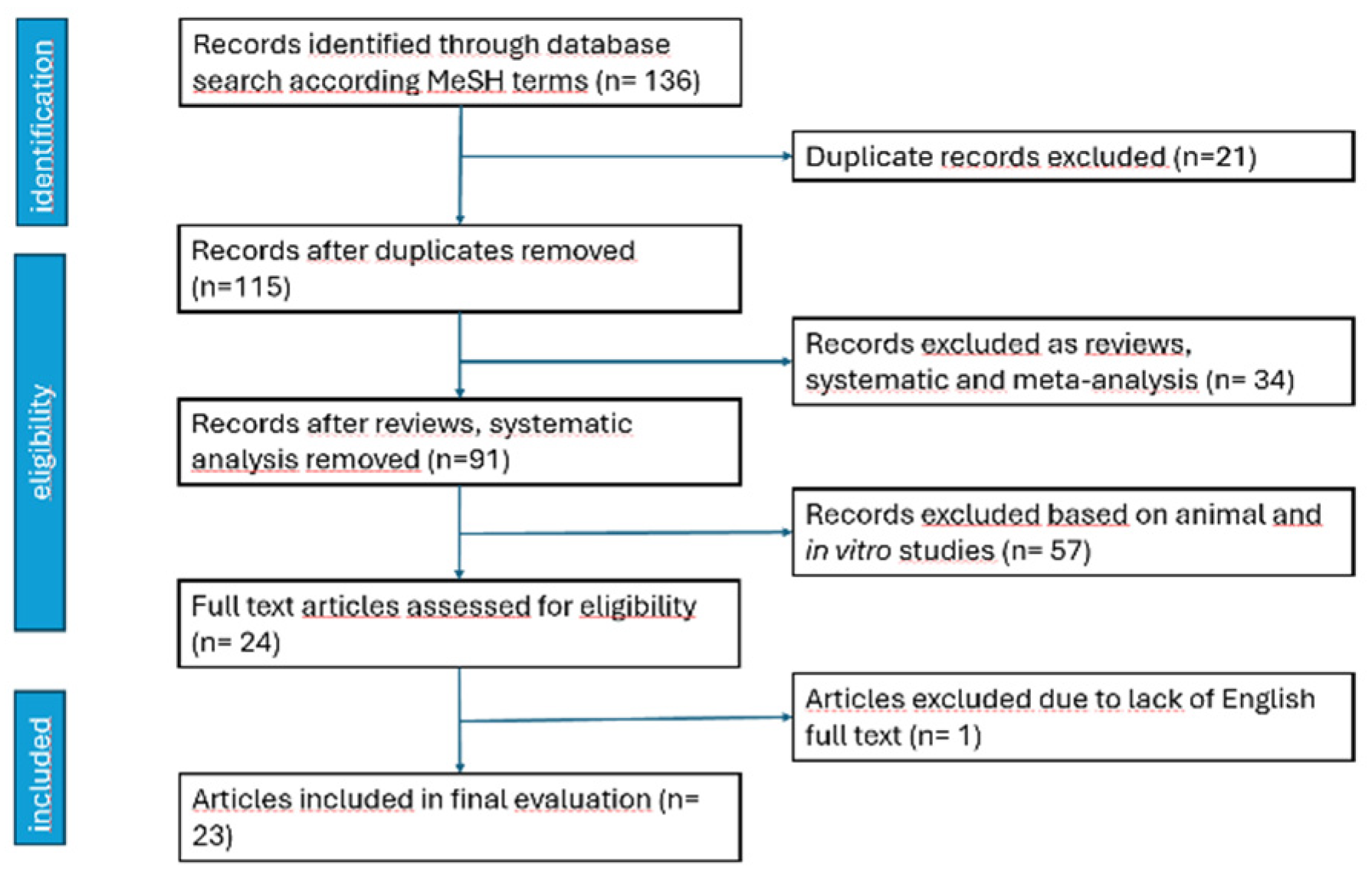

Table 1.
The selected trials included in this research.
| Author, year of the trial | Trial type, no of patients | Intervention | Outcome | Moments of the study | Results |
| Viliani, 2009 [18] | Prospective, randomized, 41 pts | Group A: HA intraarticular (4 weekly infiltrations). Group B: HILT, 10 sessions on alternate day. |
Function (WOMAC, Lequesne scale) | Baseline. End of the treatment. 4 months. |
Intragroup: significant improvement at the end of the treatment, maintaining the values at 4 months |
| Sabbahi, 2009 [19] | Prospective, randomized, 30 pts | HILT + ET. LLLT + ET. US + ET. 2 sessions / week, 3 weeks |
Pain (VAS), Walking distance without pain (in meters), Squatting with/without pain. |
Baseline. End of the treatment. |
Intragroup: improvement for all US and LLLT equally efficient Significant better results for HILT |
| Stiglig-Rogoznica, 2011 [15] | Prospective, clinical, pre- and after treatment, 96 pts | HILT, 10 consecutive days | Pain (VAS) | Baseline. End of the treatment. |
Pain significantly decreased |
| Viliani, 2012 [17] | Prospective, open label, before-after, clinical trial, 34 pts (41 knees) | Group A: HILT (ten sessions, 3000 J/session, on alternate days) Group B: control |
Function (WOMAC) | Baseline. End of the treatment. 4 months. |
Group A improved significantly after treatment and at 4 months (with a slight regression). Group B showed worsening of the parameter. |
| Kheshie, 2014 [20] | Prospective, single-blinded randomized controlled trial, 53 pts | Exercise + HILT Exercise + LLLT Exercise + sham 2 sessions / week, x 6 weeks |
Pain (VAS) Function (WOMAC) |
Baseline. End of the treatment. |
Both LLLT and HILT were better than sham. HILT improved significantly than LLLT. |
| Kim, 2016 [21] | Prospective, randomized, 20 pts | Group CPT (conservative physical therapy), Group HILT (CPT + HILT) 3 times/week, 4 weeks, 1500 J/cm2 |
Pain (VAS) Function (WOMAC) |
Baseline. End of the treatment. |
Intra-group: both groups improved statistically. Inter group: HILT had better scores. |
| Angelova, 2016 [22] | Prospective, pilot trial, randomized, clinical, single-blinded, placebo controlled, 72 patients | HILT (300J/session analgesic, 3000 J/session biostimulatory) versus sham, 7 daily sessions |
Pain Pedobarometric gait analysis (static and dynamic) |
Baseline. End of the treatment. 1 and 3 months. |
HILT group improved significantly after treatment and results were maintained at follow-up |
| Alayat, 2017 [23] | Prospective, single-blinded randomized controlled trial, 67 pts | Group 1: HILT, GCS, ET. Group 2: GCS + ET. Group 3: placebo + ET. 2 sessions/ week, 6 weeks |
Pain (VAS) Function (WOMAC) US (synovial thickness, femoral condylar cartilage) |
Baseline. End of the treatment. 3 months. |
Intragroup: all have significant improvement at 6 weeks, persistent at 3 months, except US cartilage thickness Between groups: HILT improved better, no difference between groups 2 and 3 |
| White, 2017 [16] | Prospective, case series, before- and after treatment, 39 pts | 1 – 3 daily sessions HILT | Pain (VAS) Function (ROM) Clinical issues (swelling, numbness) |
Baseline. End of treatment. 1 – 3 weeks. |
Improvement of all items at all moments |
| Nazari, 2018 [24] | Prospective, assessor-blind, randomized controlled trial, 93 pts | HILT + ET, TENS + US + ET, ET alone, 12 sessions, 3 sessions/week |
Pain (VAS) Function (flexion ROM, timed up and go test TUG, 6-min walk test 6MWT, WOMAC) |
Baseline. End of the treatment. 12 weeks. |
Intragroup: improvements at all moments, all parameters Between groups: HILT had better results on all parameters |
| Ciplak, 2018 [25] | Prospective, randomized, single blinded, 48 pts |
Hotpack + US + TENS + ET Hotpack + HILT + ET 10 sessions /2 weeks |
Pain (VAS) Function (WOMAC) |
Baseline. End of the treatment. 6 weeks. |
HILT was better significantly at all moments |
| Akaltun, 2021 [26] | Prospective, double-blind randomized placebo-controlled, 40 pts | HILT + ET (300J/session analgesia, 3000J/session biostimulation) Placebo + ET 5 sessions /week, 2 weeks |
Pain (VAS) Functional (WOMAC, flexion ROM) US: cartilage thickness |
Baseline. End of the treatment. 6 weeks. |
Both groups: 2 and 6 weeks: VAS, WOMAC-pain, WOMAC-function, WOMAC-stiffness, and WOMAC-total, cartilage thickness and FROM increased, 6 weeks: HILT+ET significant better values for all parameters versus PL+ET |
| Koevska, 2021 [27] | Prospective, one-sided blind randomized comparative study, 72 pts | HILT versus LLLT 10 sessions |
Pain (VAS) |
Baseline. End of the treatment. 30 days. |
Both goups improved significantly. After treatment, pain on VAS had lower scores for HILT groups that LLLT. |
| Siriratna, 2022 [28] | Prospective, randomized, single-blind, parallel group study, 42 pts | Conservative treatment + HILT (562.5 J/session) Conservative treatment + sham 2 – 3 sessions /week, a total of 10 sessions |
Pain (VAS) Function (WOMAC) |
Baseline. End of the treatment. |
Intra-group: both groups improved significantly all items. Inter-group: HILT had lower pain scores, significant. No difference for WOMAC. |
| Samaan, 2022 [29] | Prospective, single blinded, randomized, controlled trial 60 pts |
HILT + ET, LIPUS + ET,ET alone, 5 sessions /week, 2 weeks |
Pain (VAS) Function (ROM, WOMAC) Proprioception accuracy |
Baseline. End of the treatment. |
HILT better results in all parameters |
| Mostafa, 2022 [30] | Prospective, randomized controlled trial, 40 pts | ESWT, one session / week, 4 weeks. HILT, 3 sessions/ week, 4 weeks |
Pain (VAS) Function (6MWT, WOMAC) |
Baseline. End of the treatment. |
Intragroup: both improved Between groups: HILT better results |
| Ekici, 2023 [31] | Prospective, double-blinded, placebo-controlled, randomized, 60 pts | Group 1 (HILT + hotpack + TENS + ET) 300J/session followed by 3000J/session Group 2 (sham laser + hotpack + TENS + ET) 9 sessions / 3 weeks |
Pain (VAS) Functional (flexion ROM, isokinetic muscle strength, WOMAC) US: cartilage thickness |
Baseline. End of the treatment. 3 months |
Both groups improved all items at the end of treatment and at 3 months There was no difference between groups at any moment. |
| Taheri, 2023 [32] | Prospective, randomized, controlled, 56 pts | ET + NSAID + topic ointment. ET + NSAID + topic ointment + HILT (3 session / week, 2 weeks) |
Pain (VAS) Function (WOMAC) |
Baseline. End of treatment. 3 months. |
All parameters were better in HILT group at the end of the treatment and after 3 months |
| Katana, 2023 [33] | Prospective, descriptive, experimental, randomized trial, 60 pts | Group I, standard protocol + HIMS. Group II, standard protocol + HILT One session/week, 8 weeks |
Pain (Likert scale) Functional (ROM) Disability (KOOS) |
Baseline. Middle (4 weeks). End of the treatment (8 weeks). |
Intra-group analysis, both improved all parameters at all moments Intergroup analysis, group II had significant grester improvement at all moments |
| Ahmad, 2023 [34] | Prospective, randomized, double-blinded, parallel-group clinical trial, 34 pts | HILT + ET LLLT + ET Once a week, 12 weeks |
Pain Disability (KOOS) Function (active flexion ROM, Timed Up-and-Go test, TUG) |
Baseline. End of the treatment. |
Intragroup: all parameters improved HILT has significant greater improvement. |
| Astri, 2023 [35] | Prospective, double-blind randomized controlled clinical trial, 61 pts | LLLT + ET HILT + ET 3 sessions / week, 2 weeks |
Pain Function (50-feet walk test) |
Baseline. Pain (after every session). End of the treatment. |
Pain improved in both groups, with better evolution at every moment for HILT Function improved better for HILT |
| Roheym, 2023 [36] | Prospective, randomized, double-blinded, pre-, posttest trial, 30 pts with bilateral KO | ET ET + HILT (300J/session, followed by 3000 J /session) 3 sessions /week, 4 weeks |
US: suprapatellar fluid detection Function (WOMAC) |
Baseline. End of the treatment. |
Intragroup: significant improvements. Better results in HILT. |
| Wibisono, 2024 [37] | Prospective, randomized, pre-test and post-test-controlled, 27 pts | HILT versus LLLT 2 sessions /week, 4 weeks |
Berg Balance Scale | Baseline. End of the treatment. |
Intragroup: both groups improved significantly. HILT improved better. |
LLLT, low-level laser therapy; HILT, high-intensity laser therapy; HA, hyaluronic acid; ROM, range of motion; FROM, flexion ROM; VAS, Visual analogue scale; HP, hot pack; ET, exercise therapy; HIMS, high induction electromagnetic stimulation; LIPUS, Low Intensity Pulsed Ultrasound; KOOS, Knee Injury and Osteoarthritis Outcome Score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



