
Submitted:
10 July 2024
Posted:
11 July 2024
You are already at the latest version
Abstract
The main objective of this study was the adaptation of the scale named AUTODDIS in the cultural and social dimensions and analyze its reliability and validity. The reliability and validity were assessed through a pilot study conducted with a population of students with intellectual disabilities. The linguistic adaptation was done through expert judgment, including each indicator: the adequacy, the coherence, the relevance, and the clarity. After the scale adaptation, the scale pilot was conducted to explore its technical properties. It was performed in a public school for students with intellectual disabilities. For the content, the validity coefficient result was 0,998 while the complete reliability result was α, 978. For the reliability subscales, the results were the following: Autonomy α, 941; self-initiation α, 925; self-direction α, 970; self-regulation α, 804, and self-concept α, 935. The results confirm the AUTODDIS scale as a valid and reliable instrument to evaluate the self-determination. However, it is necessary to apply to a larger number of people with intellectual disability to generalize these results.
Keywords:
Self-determination
; Disability
; Quality of life
; Intellectual disability
1. Introduction
Different countries and nations have ratified the Universal Declaration of the Human rights and the International Covenants that promote the freedom and rights of all people. Furthermore, the countries and nations are committed with the International Convention on the Rights of Persons with Disabilities [1], considering the base rights of this group and the core principles, for instance, “the individual autonomy, including the freedom to take own decisions, and the self-independence of the people” [1] (p.5). Likewise, this convention in the article N° 12 establishes the right to legal capacity of the person, as well as the capacity to have rights and exercise those rights [2]. In the same way, the International Convention indicates that the countries may pro-vide the necessary support to people with disabilities to exercise their legal capacity. Consequently, the different nations commit, recognize, and proclaim the rights, will, and individual preferences of each person. Meanwhile, it is a government’s duty to promote the necessary actions to guarantee this commitment.
The advance in the field of Intellectual Disability (ID) allows us to understand that support systems are essential, and they are building around values that increase the self-determination, the inclusion, the people rights, the individual development, the relationships, and the physical, emotional and material well-being. These support systems include elements such as the choice and the personal autonomy promoting the development and the individual well-being; in addition, they reduce the disability impact [3]. Therefore, international organizations and the theory advances in disability field show us that the government shall guarantee strategies and measures to ensure equal opportunities for people with ID in each dimension of their lives. In the educational field, the equal opportunity is the timely access to inclusive, comprehensive, and quality education. An education with all the essential supports to become in agents responsible for their lives exercising their self-determination.
Self-determination development is essential for individual well-being. Van Loon indicates [4] self-determination as an essential feature which provide a fundamental principle for people with and without disability to improve their live quality. This feature makes it possible to become the causal agent of their actions, using the autonomy, making choices, resolving problems and taking their own decisions.
Several authors have directed their research to build a concept for self-determination [5,6,7,8] one referent in this field is Wehmeyer [9]. This author proposes a theoretical framework that supports self-determination [10], explaining it in a functional model. He explains how the self-determination allows the “act as the main agent in a person’s life and makes decisions regarding the life quality of a free person without influences or undue external interferences” [11] (p.20). Consequently, each person is the central agent of their life, responsible for maintaining or improving their life quality; there-fore, acting or deciding will depend on them. Wehmeyer presents the self-determination as a mix of four principal features: autonomy, self-regulation, empowerment, and self-realization, which allow the construct comprehension. This model has made possible the creation of a theoretical foundation and provides assessment tools for people with disabilities [12,13].
Recently, some authors [14,15] have reconceptualized this functional model with the principles of human agents [9]. They propose the Causal Agency Theory: this theory, shows a deep understanding about the self-determination [15], arguing that all people can be causal agent in their own lives regardless of disabilities or associated conditions. The theory has three fundamental principles: the volitional action (deciding), agency action (acting), and control-action beliefs (believing) [13]. These principles are based on five essential features: the autonomy, self-initiation, self-direction, self-regulation, and self-concept. Acting in a volitional way implies doing it with autonomy, choosing main objectives based on preferences [16]. The choices are conscious and involve initiation and the ability to carry out the objectives [9]. Agency action self-regulates a per-son’s own actions and let progress towards proposed objective with perseverance [17]. Finally, the control-action beliefs determine beliefs and actions. They are the foundations for beliefs of expectations of control, beliefs in capabilities, and beliefs in causality [9]. The Causal Agency Theory emphasizes the active role that the person plays in his or her own life [13]. Likewise, it is an opportunity: to create assessments aligned with emerging studies, to include best practices to design and validate tolls, and assess people’s self-determination [18].
Wehmeyer [9], points out it is indisputable that anyone can develop self-determined actions if they have support and opportunities to do it. When people are growing up, they can acquire self-determined skills, such as setting goals, making decisions, and solving problems, among others. This implies the need for an internal sense of control, being persistent, and able to adapt to challenges in different situations [19]. Personal, contextual factors such as the family structure and the socio-economic level have a powerful influence [20], similarly [21] they show the influence of contextual factor in people with ID.
There are several factors influencing the promotion of self-determination. Its development will depend on the context. Different investigations have shown the lack of opportunities for people with ID in their contexts to make decisions in all life’s areas [22]. In the rare opportunities that people with ID have been assessments, they have given a high importance of the self-determination dimension [23] because of the influence that have in their lives. Lachapelle [24] set on that self-determination predicted belonging to a group with a high or low quality of life, these results are related to choosing opportunities. Other studies that have evaluated life quality in people with ID presented the lowest score in self-determination with respects to the other dimensions [25,26,27]. In Chile, the studies conducted have shown that among self-determination dimension, there are abilities less developed for the right promotion of it [20,28]. These worrying findings are an invitation to reflect about legal and regulatory provisions available in each country to support the development of self-determination –especially for people with ID. Resources and strategies are needed to identify the individual support necessities for each person. Both will let to evaluate the progress –or not—of self-determination. Then, undoubtedly, self-determination is a central factor for people with ID for detect the needs and to offer supports. It is necessary to have a reliable and validated assessment focusing on life activities where the person participates. This assessment tool with indicators was created from evidence and updated theories; and it considers observable milestones vis-a-vis self-determination theory.
At this point, although there are instruments that evaluate self-determination in people with intellectual disabilities and trough them it has reached important conclusions to promote self-determination [12,29,30]. In Chile, these tools are still scarce, and they are not adapted to the local reality, so it is necessary to expand this area of re-search.
A recent tool for self-determination assessment, supported by the theory of Causal Agency, with the aggregate to report adequate psychometric properties is the AU-TODDIS scale: Assessment of Self-Determination in Youth and Adults with Intellectual Disabilities [31]. This scale evaluates people with intellectual disabilities from an objective perspective (i.e., a professional perspective). Furthermore, this scale includes indicators connected with three dimensions from the Causal Agency; they are: volitional action, agential action, and beliefs of control and action. They are divided into five subscales: autonomy, self-initiation, self-direction, self-regulation, and self-concept. Therefore, the instrument has theoretical and scientific demonstration about its effectiveness [15,31,32,33,34].
Based on the arguments presented about the relevance of self-determination in persons with intellectual disabilities. Ensuring the existence of valid and reliable evaluations, thus, of instruments supported by scientific evidence is unavoidable. For this reason, the main objective of this pilot study was to adapt linguistically and culturally the AUTODDIS self-determination scale, to subsequently analyze its reliability and validity, in one: applying it to a group of Chilean students with intellectual disabilities.
2. Materials and Methods
2.1. Study Design
A cross-sectional descriptive study was used to explore a self-determination test for people with ID via the AUTODDIS Scale. This instrument was created in Spain, so the authorization was obtained from one of the authors to conduct the cultural and linguistic adaptation and to analyze its reliability and validity. Five experts in the field of linguistics and self-determination were consulted. The expert participation was conditional on the informed consent of them. A protocol was delivered to them, which contained the following: an identification section, the presentation to the instrument to be evaluate, the scale with its respective evaluation guideline to evaluate each section with its respective dimensions. Finally, the judges scored each of the items on the scale. Finally, a few modifications, suggested by the experts were made to some of the words on the scale adapted to the Chilean reality.
Once the scale adaptation was completed, the researchers contacted the educational leaders of a public school who serve students with ID. This is a unique school because it is the only special school for this population in all the district. The team authorized and signed the informed consent for the school’s participation in the research. The school’s population consisted in a total of 50 students, ranging in age from 5 to 26 years. The students’ sample was conditioned to a. the informed consent signed by each teacher, b. informed consent signed for parents and/or caregivers, and c. the assent of the students. The final sample consisted of 28 students (N=28) with intellectual disabilities whose ages ranged from 11 to 25 years. Those students who did not participate were due two causes: 1. They were younger and/or 2. Their parents did not sign the consent for the study.
2.2. Procedure
It was a collaborative work between the educational institution and the research team. Previously, the approval of the University’s Ethics, Bioethics and Biosafe Committee was obtained.
The school principal selected teachers who knew their students very well and who had knowledge of the construct of self-determination. The research team trained these teachers in the steps for the application of the AUTODDIS scales. The scale was ap-plied individually in a physical format (i.e., paper). Each teacher evaluated his or her student in each of the subdimension of the scale. To ensure students’ anonymity, identification codes were used to replace their names and surnames for all student participants.
The parents and/or caregivers, principals, and teachers at the school were in-formed about the nature of the study through a document that was read and signed by all those collaborating with this research. All instruments were applied under confidentiality protocols and duly endorsed by the Ethics, Bioethics, and Biosafety Committee of the University of Concepción, Chile (CEBB 1282-2022, October 2022). All procedures complied with the Declaration of Helsinki and Singapore for research involving human subjects.
2.3. Assessment Instrument
2.3.1. For linguistic and Cultural Adaptation, the Validity Coefficient was Used
The content validity coefficient (CVC) was taken by expert judgment to confirm the degree which the instrument measures the variable to be studied. To obtain the CVC of the AUTODDIS scale, first, an evaluation guideline with scores from 1 to 4 was applied [35]. The judges scored with a Likert format each of the items on the scale considering these criteria: Not compliant (1 point); low level (2 points); moderate level (3 points), and for the highest level (4 points). These scores were established to rate the following: a. sufficiency (i.e., the item belonged to the dimension in which it is sufficient to obtain the measurement of it), b. coherence (i.e., the logical relationship between the item and the dimension and/or indicator measured), c. relevance (i.e., it is an essential item which must be included), and d. clarity (i.e., the item was easily understood meaning its syntactics and semantics were adequate).
The AUTODDIS scale [30] was used to pilot and assess self-determination: This scale allows the assessment of people with intellectual disabilities between 11 and 40 years of age. It is composed of six dimensions, these are:
- Autonomy, composed of 7 items
- Self-initiation, composed of 6 items
- Self-direction, composed of 12 items
- Self-regulation, composed of 3 items
- Self-realization composed of 6 items, and
- Empowerment composed of 12 items.
The scale has a total of 46 items. The scale is presented in a Likert format, ranging from strongly agree (4 points), agree (3 points), disagree (2 points), and strongly disagree (1 point).
The instrument was designed to be answered in 25 minutes by an evaluator who knows the person with ID very well and for a minimum of four months.
2.4. Sociodemographic Data
Through the application of the AUTODDIS scale, teachers also provided sociodemographic information such as sex, age, diagnosis, level of intellectual disability and place of residence. They used the psychological reports provided by the educational unit as a reference to complete the information required.
2.5. Statistical Analysis
The analysis conducted by expert judges examined the con-tent validity coefficient to stablish agreement among the experts for each section of the scale and its 46 items. Sufficiency, clarity, coherence and relevance were confirmed [36].
In the same way, the reliability of the instrument was analyzed considering the dependent variable of Self-determination, defined as “a dispositional characteristic that becomes manifest when the person act as a causal agent of his or her own life” [13] (p. 258). It is composed of the following dimensions: Autonomy, understood as the ability to act without undue influence of others; self-initiation, the ability to act when the person decides to do it; self-direction, ability to act by addressing own’s actions to-wards the achievement of personal goals; self-regulation/adjustment: ability to make alternatives and adjust the action to overcome any obstacles; self-concept, the knowledge that each person has of their abilities and limitation, as well as the personal value that it has of itself; and empowerment: ability to express self-defense and self-representation behaviors.
For the reliability process, an internal consistency analysis of the total scale and its subscales was conducted using Cronbach’s alpha coefficient through SPSS statistical program. Data distribution was established using Shapiro-Wilk normality test. Since the sample did not present a normal distribution among the responses of its sub-scales, non-parametric test was applied, and descriptive and inferential analysis were performed.
3. Results
3.1. Results of Linguistic and Cultural Adaptation of the Scale AUTODDIS
The summary of the evaluation done by the expert judges in each section, according to the categories requested, is presented, including their observations and changes suggested, which were limited to specific modification in indicator for the scale: in the identification section, vocabulary adjustments are evident which translated into a low percentage of reading and comprehension error for the items. The suggested changes were:
- In the informant’s data section, changing the word Speech Therapist for Speech Pathologist and Health Services for Healthcare Services.
- In the data of the person assessment, the recommended changes were the following: autonomous community by region, primary education for elementary education, secondary education for high school education, funded for subsidized, ordinary classroom for regular classroom, vocational center for employment center, and assisted living facility for apartment.
- In the section of autonomy subscale in the section items, they recommended replacing the word snack for light meal. There are few changes as specified the Table 1.

Table 1.
Categories for expert evaluation of content validity.
| Category | Qualification | Indicator | Observations |
|---|---|---|---|
| Sufficiency Items that belong to one dimension are sufficient to have the measurement of it. |
1. It does not meet the criterion | Items are not enough to measure the dimension | |
| 2. Low level | Items measure few aspects of the dimension, but they do not correspond to the total dimension | ||
| 3. Moderate level | Some items must be aggregate to measure the dimension completely | ||
| 4. High level | Items are enough | ||
| Coherence The item has a logic relationship with the dimension or indicator which is measuring |
1. It does not meet the criterion | The item has not not logical relationship with the dimension | |
| 2. Low level | The item has a tangential relationship with the dimension | ||
| 3. Moderate level | The item has a moderate relationship with the dimension that is measuring | ||
| 4. High Level | The item is completely related to the dimension to measure. | ||
| Relevance The item is essential or fundamental, that is, it must be included |
1. It does not meet the criterion | The item, it can be eliminated without affecting the dimension measurement | |
| 2. Low level | The item it has some relevance, but another item is including what is measure | ||
| 3. Moderate level | The item is important | ||
| 4. High Level | It is a relevant item, and it should be included | ||
| Clarity The item can be easily understood. Its syntactic and semantic are adequate |
1. It does not meet the criterion | The item is not clear at all | |
| 2. Low level | The item requires quite a few modifications or a large modification in the use of the words according to their meaning or by the order of the same | ||
| 3. Moderate level | It is necessary a specific item modification or some of the item’s terms modification | ||
| 4. High Level | The item is clear in semantic and syntax |
Note: taken from the author [35].
3.1.2. Content Validity Coefficient
the assessment of the content validity coefficients considered categories to examine criteria fulfillment and item precision. Table 1 provides evidence of the assessment conducted for each of the 46 items on the scale.
An Excel database was created to place each of the expert scores and observations. This data calculated the content validity coefficient based on Hernández-Nieto [36] who indicates that in order to obtain the validation of the instrument, it is correct using respective calculations through Excel and the following formula:
Figure 1.
calculations formula. Note: taken from [36].
Figure 1.
calculations formula. Note: taken from [36].
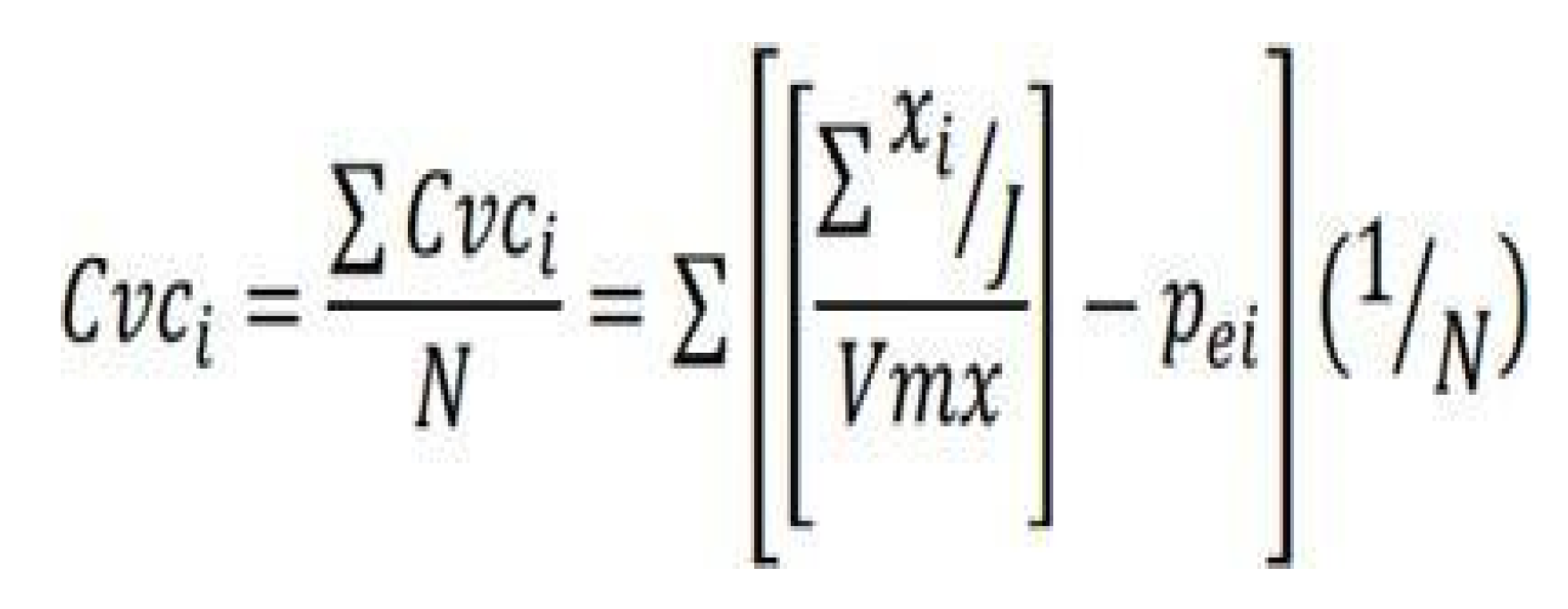
According to Hernández- Nieto, each of the components of the formula are interpreted as follows: N= Total number of items in the data collection instrument. Sxi= Sum of the scores assigned by each judge J to each item. i.Vmx= Maximum value of the scale used by the judges. Pei=Probability of error for each item (probability of random agreement among the judges). J=Number of judges assigning scores to each item [36] (p. 72).
The formula presented allowed the measurement of the content validity coefficient granted by expert judges (CVC) in Excel with a result of 0.998. These results according to [36] are excellent. Further, it presents a high validity and agreement among expert judges regarding each of the items. Each of the items present a score higher than 0.80, so according to the author, any of items of the scale it was eliminate.
Table 2.
Assessment scale CVC.
| CVC | Assessment |
| <.60 | Unacceptable |
| ≥.60 | Deficient |
| >.71 y < .80 | Acceptable |
| > .80 y < .90 | Good |
| > .90 | Excellent |
Note: [36] (p.72).
3.2. Reliability, Internal Consistency Analysis
Teachers assessed the students with intellectual disabilities with Self-determination scale using scores on each of the scale items. The Figure 2 shows us the evidence of each teacher assessing the different dimensions of self-determination marking their perception with options ranging from strongly agree to strongly disagree.
Table 3 presents the analysis of internal consistency and the reliability results obtained from the general analysis of the total scale, and its subscales show a α= .978; it indicates that the scale is reliable to measure self-determination in each of the dimensions and in the general level. Consequently, the scale demonstrates adequate internal consistency.
Table 4 shows the reliability results for the full sample (N=28) using the assessment provided by the teachers. The reliability results are excellent as a whole [30]. They meet satisfactorily the requirements set to ensure the accuracy of the information obtained with the scale [32]. All subscales show reliability indices higher than .800 with the self-direction subscales presenting a greater internal consistency (value α =.970) and the self-regulation/adjustment subscale show less internal consistency (value α=.804). These results are similar with those of the research of [30] (N=541), which indicate the coincidence in the evaluation between families and professionals with an N=106.
Similarly, the subscales of autonomy, self-initiation, and self-concept show reliability indices superior to α =. 900; therefore, they present an excellent reliability. One of the subscales (i.e., self-regulation) shows a lower result. This result can be attributed according to Frias-Navarro [37] to the lower number of items presented by the subscales. Because when calculating Alpha a greater number of items increases reliability. In this case, the subscale of self-regulation has a reduced number of items (3).
3.3. Descriptive Statistical Results of the General Scale
The results from the evaluation conducted by the teachers to the students with intellectual disabilities show that the teachers ‘perceptions regarding the self-determination of their students are low. This is evident with a mean of 49.07 and a standard deviation of 17.8 points. Observing the mean in percentile ranges, it is observed it has a value of 24, which indicates that students with ID are below the mean in self-determination, comparing with their pairs in age. Furthermore, all the student participants have a low level of self-determination. Table 5 illustrates this.
3.4. Descriptive Statistical Results for Each Subscale
According to the results on Table 6, the assessment conducted by the teacher on their students with ID demonstrated that autonomy, self-initiation, and self-concept dimensions have similar mean scores (17.18, 14.75 and 13.54). It places them as report the statistical data of the scale, in the value of the 40th percentile. This result is below the mean, although the sample shows a higher level of achievement in the items on this subscale.
In the results for empowerment dimension, the mean is 24.36 with a standard deviation of 10.2. observing the percentile ranges, they show a value of 28. This value confirm that the sample (N=28) presents a low level of empowerment. It is followed by self-direction dimension that obtained a mean of 17.82 and a standard deviation of 7.4, and finally, self-regulation dimension with a mean of 5 and a standard deviation of 4.2. The last two subscales yield a percentile of 18, placing the sample (N=28) bellow the mean in self-direction and self-regulation skills. Then, it is possible to indicate that results for self-direction and self-regulation dimensions are place in an insufficient level.
3.5. Results Coefficient of Each Subscale
Table 7 presents the general statistical result for the subscales on the coefficient obtained connected with the direct score and the items in each of them. In the table below, the subscale that obtain the most favorable results was autonomy, which has a mean of 0.61; self-initiation has 0.61. Some assessments present ideal scores for students with intellectual disabilities in these two dimensions of self-determination. While the mean results for dimensions of empowerment and self-concept are 0.51 and 0.56 respectively, which are read as a result neither low nor high, but a moderate or acceptable level.
The lowest results in level of achievement are in self-direction with a mean of 0.37 and self-regulation with a mean of 0.42. In addition, based in the analysis, it was found that the lowest achievement levels per item are within these subscales. Moreover, no participant obtained an ideal score in any of these two dimensions of self-determination.
4. Discussion
The goal of this study was to linguistically and culturally adapt the AUTODDIS self-determination scale. Also, the goal was to analyze its reliability and validity through a pilot study with ID students.
The findings of the study show that AUTODDIS self-determination scale fully meets the criteria of sufficiency, coherence, and clarity. Obtaining a validity of .998, which from the lent to Hernández- Nieto [36], is in the excellent category. This implies that the Scale does measure the variable of interest [37,38]. The items are developed in a way that it is possible to obtain precise information from the six subscales of self-determination, and these dimensions and their items are sufficient to measure the dimensions that compose it; are easy to understand for the participants; the indicators are coherent; and there are relevant to the results [15,31,32,33,34,39,40].
From a practical perspective, if this instrument is applied again in a sample of people with intellectual disabilities, it would deliver reliable data on the levels of self-determination. However, to validate this instrument at a national level, it is necessary to use a larger sample of people with ID to cover the different contexts of the country.
Regarding the instrument, is it possible to indicate that AUTODDIS scale is an instrument with a high level of reliability, whose result was α =.978, which mean excellence for its consistent and coherent results. Also, this implies that the scale is an instrument to be applied for other studies exploring self-determination in people with ID in Chilean context since it will provide reliable results for data analysis. This pilot shows in the general results from teachers’ evaluation a low level of self-determination. This result is consistent with the study conduct in Chile during 2020 using the INICO ARC Scale. Its results concluded that Chilean students with intellectual disabilities have a low level of self-determination [41] also, its results are similar the results of previous studies investigating quality of life [26].
In the subscales results, few of them present high levels of achievement: they are autonomy, self-initiation, and self-concept. Although, it is necessary to clarify that they are above the other subscales, but these are below the arithmetic mean. In the first place, autonomy is present as the best developed component. So, it is inferred that supporting self-determination in activities of personal care helps satisfy basic needs such as clothing, food, and hygiene. Secondly, it can be concluded that self-initiation is at the second level of achievement and is linked to voluntary performing actions based on personal interests and preferences [30]. Thirdly, self-concept, which Verdugo de-fined [30] as beliefs about the individual abilities to achieve an objective. From the data obtained, it can be reasonable conclude that there is a low level of development in this area, which include a lack of knowledge about own strengths and difficulties. This confirms international studies that agree that people with ID have few opportunities to generate positive and realistic self-awareness [42].
The subscales with lowest level of achievement are as follows: empowerment, self-regulation, and self-directions. These dimensions depend on the characteristics of agency, which are related to the capacity to be restrained in their decisions. So, acting in a personal determined way is limited. Something similar happens with the development of attitudes and skills connected to empowerment. There are scarce possibilities for the population with ID; these findings are consistent with the literature in the field where Tamarit [43] points that these barriers are linked to the fact that people with disabilities have been historically oppressed. They have a right to be protagonists of their lives, make decision freely, express their opinions, and defend their proposals. They have had violated rights in different levels such as political, cultural, and practical throughout history. In addition, there are studies that show how the family members of people with ID tend to limit the opportunity to carry out action to reinforce their beliefs of control-action [21,44], families have a tendency to stop their desires to fulfill themselves in everyday tasks as a manifestation of overprotection [26], such as making decision related to the home, and addressing challenging goals that support self-knowledge about their abilities and limitations [45].
For self-regulation scale, it can be noted that the pilot study coincides with some studies that place self-regulation within the dimensions with less development [46]. Likeise Mithaug [47] indicates that many people with intellectual disabilities have limitations to define personal goals, supervising their behavior, choosing and an evaluating and actions plan, which are central elements of self-regulated people. In addition, Zimmerman [48] describes how the lack of social learning experiences is one of the factors that affect negatively self-regulation, so the active participation in different social context is key to improving these skills. Active participation become in inclusive context and a way to promote the full inclusion of this group.
Finally, the pilot study showed that the subscale with the lowest score was self-direction. This subscale is related to actions that involve setting goals or future; identifying the changes to achieve the goals; and planning and focusing actions on an objective [30]. The scores could be explained from the connection between this subscale and executive functions and the construct of intellectual functioning, which include characteristics such as, reasoning, planning, and problem solving [3]. Thus, since significant limitations in intellectual functioning are a part of the diagnosis of ID. These results could be explained from the diagnosis of each participant. However, there are consensus about the influence in the intellectual functioning of other dimension as human performing and support systems, which have a key role in it.
Limitations, Strengths, and Future Research
The main future research that emerges from this study it the application of AU-TODDIS instrument to a larger sample to ensure that the evaluation is adapted for all country. Also, this would allow more significant results to be obtained with respect to the level of self-determination of population with intellectual disability in Chile. It is possible to develop a complete profile of the most developed indicators and those that should be enhanced. Likewise, through application to significant population, it will be possible to standardize the instrument in Chile because the country does not have adapted instruments to assess self-determination.
5. Conclusions
Self-determination is key in every person and a matter of social justice for people with intellectual disabilities who often have had a limited participation in the society. They have been segregated and left aside in Chile. The country’s society has an erroneous perception that tends to see this group as a charity object, infantilizing them during their lives which leads the overprotection, limiting their actions and without respecting their right. Their preferences and desires are not important because they are under the protection of others.
One etiological perspective of ID from the integrated approach [3]; it remarks the perspective of justice with emphasis on human and legal rights. In this field, a funda-mental risk factor is the denial of rights from the society and “the way in which societies are structured: that is the way that resources are focused and distributed” [49].
A changed in support systems is needed which effectively begin by identifying needs for people with ID. Self-determination is a key element in the inclusion process, to promote it, the support systems need to become effective, person-centered, and holistic strengthening choices for people with ID. For a recognition of rights, the com-bination of moral and political criteria is required [5] to identify strategies that will help to develop the abilities that this group needs to be treated as real citizens [50].
Education shall promote and enhance the skills that promotes self-determination in people with intellectual disabilities, decision making, their autonomy, self-regulation, and empowerment. Then, they can create, decide, and act to achieve their objectives. Achieving full self-determination requires adapted assessment tools to identify support needs, from which individual improvement plans and programs can be created to improve quality of live.
Author Contributions
Conceptualization, LC-D., VV-G. and GS-V.; methodology, LC-D., VV-G. and RZ-L.; validation, LC-D., VV-G., GS-V. and RZ-L.; formal analysis , LC-D., GS-V.,VV-G. and RZ-L; research, LC-D., VV-G., RZ-L., LD-O., JD-C. and IH-O.; resources, LC-D., GS-V. and RZ-L.; data curation, LC-D., LD-O., JD-C., IH-O. and MS-C.; writing, preparation of the original draft, LC-D., GS-V.,VV-G., RZ-L., MS-C., LD-O., JD-C., IH-O, I.C., E.E.-S. and A.M.-M.; writing, revision, and editing, LC-D., VV-G., GS-V.,MS-C., RZ-L., LD-O., JD-C.,IH-O, I.C., E.E.-S. and A.M.-M.; supervision, LC-D., VV-G. y RZ-L. All authors have read and accepted the published version of the manuscript.
Funding
Please add: This research was funded by the project “Increasing the research capacity and connection with the environment of the Doctorate in Education program of the University of Concepción with a focus on gender parity.” Baseline project FB0003. Center for Advanced Research in Education, University of Chile.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and ap-proved by Ethics Committee of Universidad de Concepción, Chile (protocol code CEBB 1282-2022 and date of approval October 22, 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written in-formed consent has been obtained from the patient(s) to publish this paper.
Conflicts of Interest
Declare conflicts of interest or state “The authors declare no conflicts of interest.
References
- Nations U. Convention on the Rights of Persons with Disabilities and Optional Protocol. 2006. Disponible en línea: file:///C:/Users/Lenovo/Downloads/tccconvs.pdf (consultado el 28 de Mayo de 2024).
- Dinerstein RD. Implementing Legal Capacity Under Article 12 of the UN Convention on the Rights of Persons with Disabilities: The Difficult Road From Guardianship to Supported Decision-Making. Human Rights Brief. 2012,19 (2), 8-12.
- Schalock RL, Luckasson RA, Tassé MJ. Defining, diagnosing, classifying, and planning supports for people with intellectual disability: an emerging consensus. Siglo Cero Revista Española sobre Discapacidad Intelectual. 2021, 52(3),29-36. [CrossRef]
- Van Loon J. Autodeterminación para todos. La autodeterminación en Arduin. Revista española sobre discapacidad intelectual. 2012,37,35 – 46.
- Wehmeyer ML. The Arc's Self-Determination Scale. Procedural Guidelines. United States, 1995, 1-129.
- Walker HM, Calkins C, Wehmeyer ML, Walker L, Bacon A, Palmer SB, et al. A Social-Ecological Approach to Promote Self-Determination. Exceptionality. 2011,19(1), 6-18. [CrossRef]
- Arellano AA; Peralta F. Autodeterminación de las personas con discapacidad intelectual como objetivo educativo y derecho básico: estado de la cuestión. Revista Española de Discapacidad. 2013,1 (1), 97-117. [CrossRef]
- Wehmeyer ML. Self-Determination and Individuals with Severe Disabilities: Re-examining Meanings and Misinterpretations. Research & Practice for Persons with Severe Disabilities. 2005, 30, 113-20. [CrossRef]
- Wehmeyer ML. The Importance of Self-Determination to the Quality of Life of People with Intellectual Disability: A Perspective. Int J Environ Res Public Health. 2020, 17(19). [CrossRef]
- Wehmeyer ML. Self-Determination and Mental Retardation. Revista internacional de investigaciones sobre retraso mental. 2001,24, 1-48.
- Wehmeyer L; Kelchner K; Richards S. Essential Characteristics of Self Determined Behavior of Individuals With Mental Retardation. American Journal on Mental Retardation. 1996, 100, 6, 632-642.
- Verdugo MA; Sánchez, E; Gómez, M; Fernández, R; Wehmeyer, ML; Badia Corbella, M; González GF; Calvo Álvarez, MI. Escala ARC-INICO de Evaluación de la Autodeterminación. Manual de aplicación y corrección. Instituto Universitario e Integración a la comunidad: Salamanca, España,2014.
- Shogren KA; Wehmeyer, ML; Palmer, SB; Forber-Pratt, AJ; Little, TJ; Lopez, S. Causal Agency Theory: Reconceptualizing a Functional Model of Self-Determination. Education and Training in Autism and Developmental Disabilities. 2015, 50, 3, 251-63.
- Shogren KR; Raley SK. Self-Determination and Causal Agency Theory. Integrating Research into Practice. Positive Psychology and Disability Series. Springer Nature Switzerland: Laurence Kansas, 2022 pág. 1-149.
- Vicente E; Mumbardó-Adam C; Guillén VM; Coma-Rosello T; Bravo-Alvarez MA; Sánchez S. Self-Determination in People with Intellectual Disability: The Mediating Role of Opportunities. Int J Environ Res Public Health. 2020, 17(17).
- Mumbardó AC; Sánchez E; Giné C; Guardia J; Raley SK; Verdugo MA. Promoviendo la autodeterminación en el aula: el modelo de enseñanza y aprendizaje de la autodeterminación. Siglo Cero Revista Española sobre Discapacidad Intelectual. 2018, 48(2).
- Palmer SB; Wehmeyer ML; Shogren KA. The Development of Self-Determination During Childhood. In: Wehmeyer ML, Shogren KA, Little TD, Lopez SJ, editors. Development of Self-Determination Through the Life-Course. Springer: Dordrecht, The Netherlands, 2017. págs. 71-88.
- Raley SK; Shogren KA; Rifenbark GG; Anderson MH; Shaw LA. Comparing the Impact of Online and Paper-and-Pencil Administration of the Self-Determination Inventory: Student Report. Journal of Special Education Technology. 2019, 35(3), 133-44.
- Pérez MP. Aportes de la educación musical a las personas con discapacidad visual en la promoción de la autodeterminación. Ricercare. 2020, 13, 3-25.
- Álvarez-Aguado I; Vega V; González SH; González-Carrasco F; Jarpa M; Campaña K. Autodeterminación en personas con discapacidad intelectual que envejecen y algunas variables que inciden en su desarrollo. Interdisciplinaria Revista de Psicología y Ciencias Afines. 2021, 38(3),139-54.
- Vicente E; Pérez-Curiel P; Mumbardó AC; Guillén VM; Bravo-Alvarez MA. Personal Factors, Living Environments, and Specialized Supports: Their Role in the Self-Determination of People with Intellectual Disability. Behav Sci (Basel). 2023, 13(7).
- Wehmeyer ML; Metzler, CA. How Self -Determined Are People With Mental Retardation? The National Consumer Survey. Mental Retardation. 1995, 33, 111-9.
- Schalock R; Verdugo, MA; Jenaro, C; Wang, M; Wehmeyer, M; Jiancheng, X; Lachapelle, Y. Cross-Cultural Study of Quality of Life Indicators. American Journal On Mental Retardation. 2005,110, 4, 298–311.
- Lachapelle Y; Wehmeyer ML; Haelewyck MC; Courbois Y; Keith KD; Schalock R; et al. The relationship between quality of life and self-determination: an international study. J Intellect Disabil Res. 2005, 49(Pt 10):740-4.
- Santamaría M; Verdugo MA; Orgaz, B; Gómez, LE; De Urríes, FDB. Calidad de vida percibida por trabajadores con discapacidad intelectual en empleo ordinario. Siglo Cero: Revista Española sobre Discapacidad Intelectual.2012, 43(242),46-61.
- Castro L; Cerda G; Vallejos V; Zúñiga D; Cano R. Calidad de vida de personas con discapacidad intelectual en centros de formación laboral. Avances en Psicología Latinoamericana. 2016, 34(1), 175-86.
- Gómez M; Verdugo MA. El cuestionario de evaluación de la calidad de vida de alumnos de educación secundaria obligatoria: descripción, validación inicial y resultados obtenidos tras su aplicación en una muestra de adolescentes con discapacidad y sin ella. Siglo Cero: Revista Española sobre Discapacidad Intelectual.2004,35(212), 5-17.
- Vega V; ÁLvarez-Aguado I; González H; González F. Avanzando en autodeterminación: estudio sobre las autopercepciones de personas adultas con discapacidad intelectual desde una perspectiva de investigación inclusiva. Siglo Cero Revista Española sobre Discapacidad Intelectual. 2020, 51(1).
- Muñoz-Cantero JM & Losada-Puente L. Validación del constructo de autodeterminación a través de la escala ARC-INICO para adolescentes. Revista Española de Pedagogía. 2019, 77(272), 43-62.
- Verdugo MA; Sánchez, E; Guillén, VM; Sánchez, S; Ibáñez, A; Fernández, R; Vived, E. Escala AUTODDIS: Evaluación de la autodeterminación de jóvenes y adultos con discapacidad intelectual. Manual de aplicación y corrección. Instituto Universitario e Integración a la comunidad: Salamanca, España, 2021; pág 1-86.
- Vicente E; Verdugo MA; Guillén VM; Martinez-Molina A; Gómez LE; Ibañez A. Advances in the assessment of self-determination: internal structure of a scale for people with intellectual disabilities aged 11 to 40. J Intellect Disabil Res. 2020,64(9),700-12.
- Verdugo MA; Vicente E; Guillen VM; Sanchez S; Ibanez A; Gomez LE. A measurement of self-determination for people with intellectual disability: description of the AUTODDIS scale and evidences of reliability and external validity. Int J Dev Disabil. 2023,69(2),317-26.
- Vicente E.; Guillén VM; Fernández-Pulido R; Bravo MA; Vived E. Avanzando en la evaluación de la Autodeterminación: diseño de la Escala AUTODDIS. Aula Abierta. 2019,48(3),301-10.
- Vicente E; Guillén VM; Gomez LE; Ibañez A; Sánchez S. What do stakeholders understand by self-determination? Consensus for its evaluation. J Appl Res Intellect Disabil. 2019,32(1),206-18.
- Galicia LA; Balderrama JA; Edel R. Content validity by experts judgment: Proposal for a virtual tool. Apertura 2017,9(2),42-53.
- Hernández-Nieto RA. Contributions to Statistical Analysis: The Coefficients of Proportional Variance, Content Validity and Kappa; CreateSpace Independent Publishing Platform, 2002; págs 100-228.
- Frías-Navarro, D. Apuntes de estimación de la fiabilidad de consistencia interna de los ítems de un instrumento de medida. Universidad de Valencia. Valencia, España, 2022. https://www.uv.es/friasnav/AlfaCronbach.pdf (revisado 6 de junio 2024).
- Hernández R; Fernández, C; Baptista, P. Metodología de la investigación, cuarta ed.; McGraw-Hill: México, México, 2014; pág.102-256.
- Chiner E. Universidad de Alicante, Alicante, España. Materiales docentes de la asignatura Métodos, Diseños y Técnicas de Investigación Psicológica, 2011.
- Escobar J; Cuervo Á. Validez de contenido y juicio de expertos: una aproximación a su utilización. Avances en medición. 2008,6,27-36.
- Álvarez-Aguado I; Vega-Córdova V; Campaña-Vilo K; González-Carrasco F; Spencer-González H; Arriagada-Chinchón R. Habilidades de autodeterminación en estudiantes chilenos con discapacidad intelectual: avanzando hacia una inclusión exitosa. Revista Colombiana de Educación. 2020,79,369-94.
- Peralta F; Alquegui, B; Arteta, R; Landa, M; Santesteban, I. Intervención para el desarrollo de la autoconsciencia en alumnos con retraso mental: propuesta de actividades. Revista Española sobre Discapacidad Intelectual. 2004,35(3),18-30.
- Tamarit J; Espejo, L. Experiencias de empoderamiento de personas con discapacidad intelectual o del desarrollo. Siglo Cero: Revista Española sobre Discapacidad Intelectual. 2013,44(246):26-39.
- Vicente E; Mumbardó-Adam, C; Coma, T; Gine, C; Alonso, V. Autodeterminación en personas con discapacidad intelectual y del desarrollo: revisión del concepto, su importancia y retos emergentes. Revista Española de Discapacidad. 2018, 6(2),7-25.
- Arellano A; Peralta F. Self-determination of young children with intellectual disability: understanding parents' perspectives. British Journal of Special Education.2013, 40(4),175-81.
- Losada-Puente L.; Muñoz JM. Validación del constructo de autodeterminación a través de la escala ARC-INICO para adolescentes. Revista Española de Pedagogía. 2019, 272, 143-162.
- Mithaug DE. Equal Opportunity Theory; SAGE PublicationsThousand Oaks. EEUU, 1996; pág.
- Murte PA. Diseño de un programa de formación para la transición a la vida adulta en personas con discapacidad intelectual: uso del dinero a través de la autorregulación. Nivel Master, Universidad de Almaría, España, 5 de marzo,2012.
- Cruz-Velandia I. ; Hernandez J. Exclusión social y discapacidad; Editorial Universidad del Rosario: Bogota, Colombia, 2006; págs. 210.
- Rozo Reyes CM; Monsalve AM. Discapacidad y justicia distributiva: una mirada desde la bioética. Revista Colombiana de Psiquiatría. 2011, 40(2):336-51.
Figure 2.
Example of Autonomy subscale.
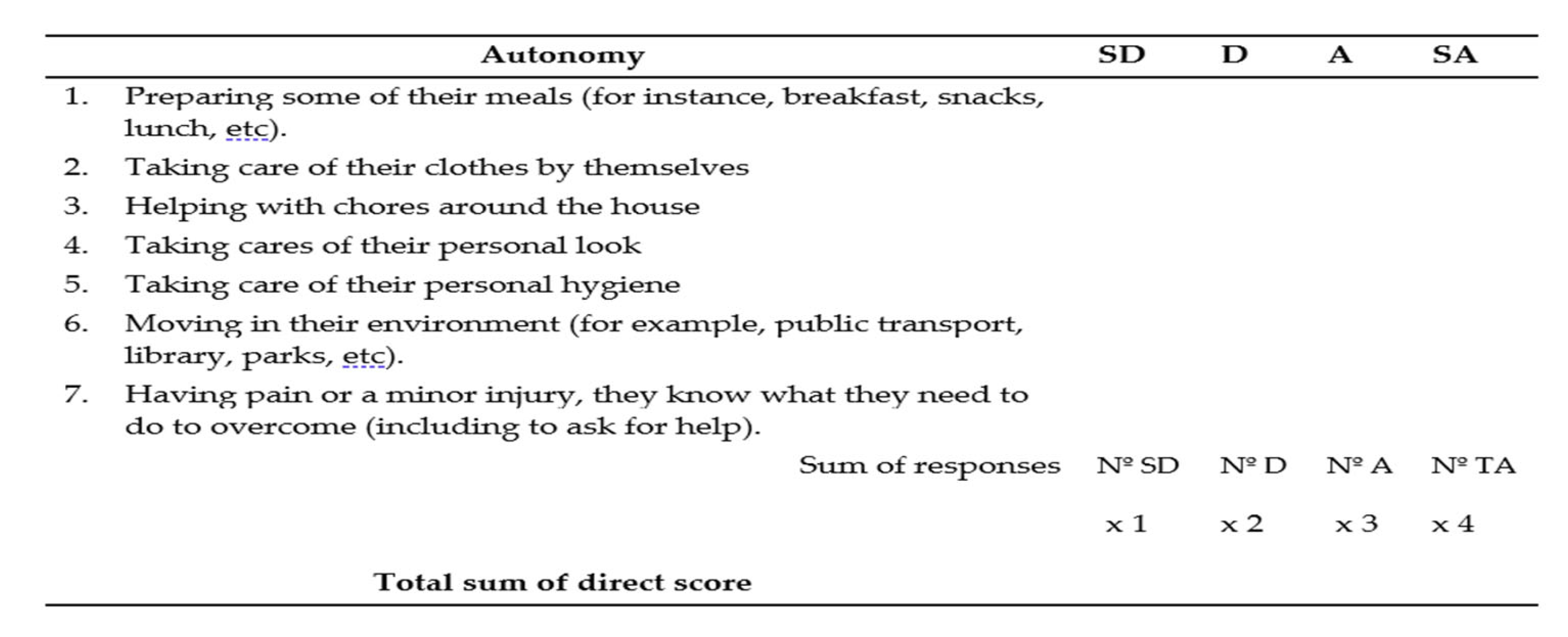
Table 3.
Cronbach’s Alpha results.
| Cronbach’s Alpha | N° elements |
| .978 | 46 |
Table 4.
Reliability results of subscales in AUTODDIS.
| Subscale | Cronbach’s Alpha | Nº of elements |
|---|---|---|
| Autonomy | .941 | 7 |
| Self-initiation | .925 | 6 |
| Self-direction | .970 | 12 |
| Auto-regulation/Adjustment | .804 | 3 |
| Self-concept | .935 | 6 |
| Empowerment | .958 | 12 |
Table 5.
Descriptive analysis of the general scale.
| Descriptive | ||||
|---|---|---|---|---|
| Statistical | Standard error | |||
|
Standard score total scale |
Mean | 49.07 | 3.367 | |
| 95% confidence interval for the mean |
Lower limit | 42.16 | ||
| Upper limit | 55.98 | |||
| Mean cut to 5% | 48.77 | |||
| Median | 49.50 | |||
| Variance | 317.402 | |||
| Standard deviation | 17.816 | |||
| Minimum | 23 | |||
| Maximum | 82 | |||
| Range | 59 | |||
Table 6.
Descriptive statistics for each subscale.
| Direct score autonomy subscale |
Direct score Self-initiation subscale |
Direct score self-direction subscale |
Direct score self-regulation subscale |
Direct score self-concept subscale |
Direct score empowerment subscale |
|
|---|---|---|---|---|---|---|
| N Valid | 28 | 28 | 28 | 28 | 28 | 28 |
| Lost | 0 | 0 | 0 | 0 | 0 | 0 |
| Mean | 17.18 | 14.75 | 17.82 | 5.00 | 13.54 | 24.36 |
| Median | 18.50 | 15.00 | 12.00 | 5.00 | 13.50 | 23.50 |
| Modal | 20* | 15 | 12 | 3 | 6 | 12* |
| Standard dev. | 6.360 | 5.434 | 7.444 | 2.055 | 5.594 | 10.275 |
| Variance | 40.448 | 29.528 | 55.411 | 4.222 | 31.295 | 105.571 |
| Minimum | 7 | 6 | 12 | 3 | 6 | 12 |
| Maximum | 28 | 24 | 35 | 10 | 24 | 46 |
Table 7.
Coefficient of each subscale.
| Autonomy subscale coefficient | Self-initiation subscale coefficient | Self-direction subscale coefficient | Self-regulation subscale coefficient |
Self-concept subscale coefficient |
Empowerment subscale coefficient |
|
| N Valid | 28 | 28 | 28 | 28 | 28 | 28 |
| Lost | 0 | 0 | 0 | 0 | 0 | 0 |
| Mean | .61 | .61 | .37 | .42 | .56 | .51 |
| Median | .66 | .63 | .25 | .42 | .56 | .51 |
| Modal | .71 | .63 | .25 | .25 | .25 | .25 |
| Standard dev. | .23 | .23 | .16 | .17 | .23 | .21 |
| Minimum | .25 | .25 | .25 | .25 | .25 | .25 |
| Maximum | 1.00 | 1.00 | .73 | .83 | 1.00 | .96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



