
Submitted:
10 July 2024
Posted:
10 July 2024
You are already at the latest version
Abstract
Polymeric composites are prone to undergo damage, such as microcracks, during their operation, that can ultimately lead to catastrophic failure. To contradict such problem, effort has been put, by the scientific community, towards developing self-healing composites that, by mimicking biological systems, can autonomously and prematurely repair flaws, extending durability and improving security of materials. The present review explores the progress being made in such area, focusing on extrinsic self-healing methods, considering that they can be employed to a variety of materials. Reservoir-based techniques, that resort to capsules, hollow fibers or microvascular networks, and thermoplastic-based ones are overviewed, prioritizing innovative approaches made in recent years. At last, promising practical applications for self-healing composites are highlighted and future challenges and opportunities are pointed out.
Keywords:
Polymer-matrix composites
; Smart materials
; Material Resilience
; Self-healing
1. Introduction
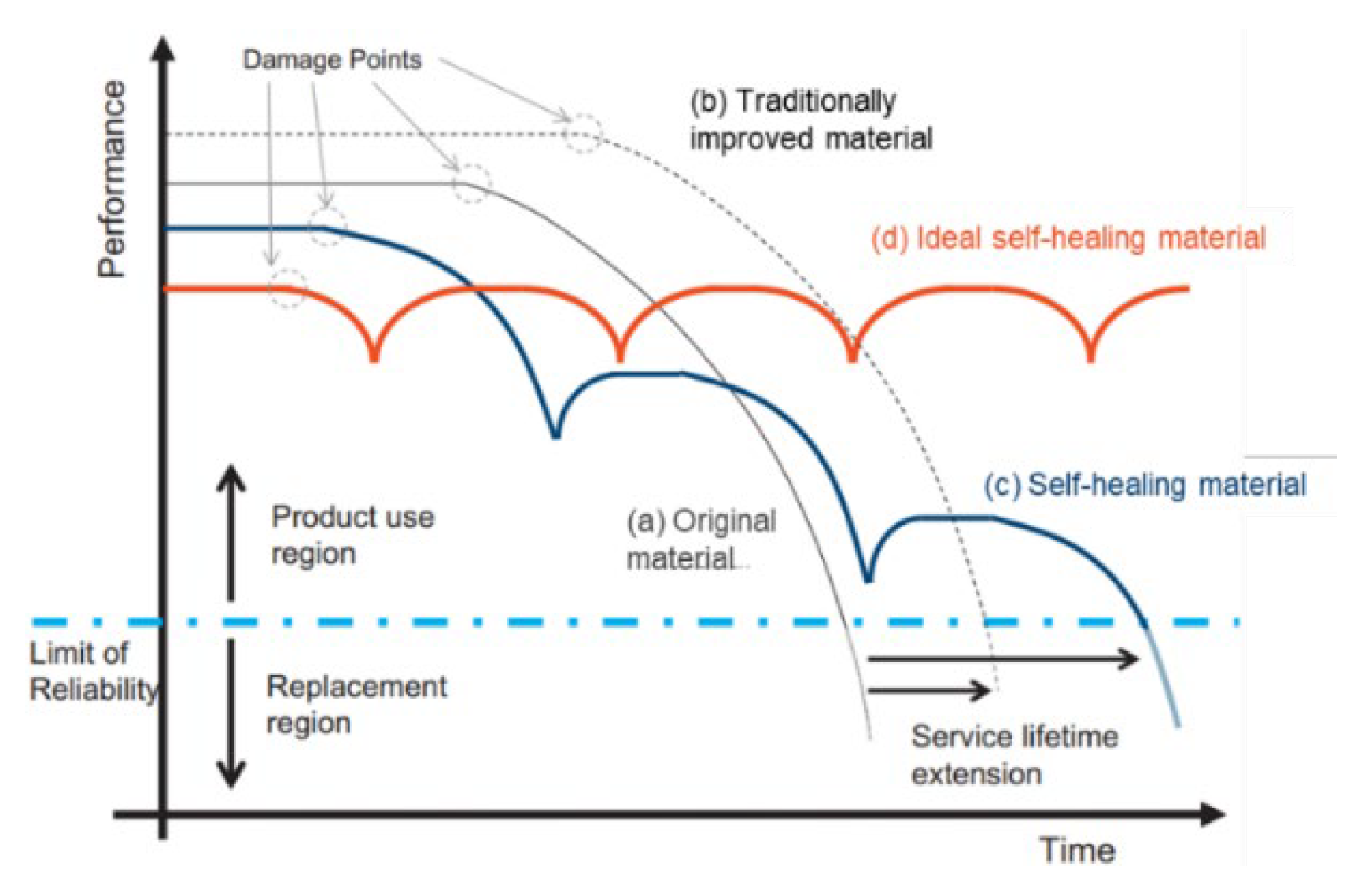
Self-healing polymeric-matrix composites, as the name suggests, are materials able to, when subjected to external damage, autonomously repair the affected area, without manual intervention, and recover their integrity and functional properties (for example strength, conductivity or biomedical characteristics) thus mimicking biological regeneration systems. In addition to the self-healing characteristics, these materials can still contain fillers responsible for providing other properties, like reinforcing fibers. The aforementioned damages include not only small imperfections caused, for example, by micro delamination of the incorporated fibers or by microcracking, but also fracture or other damage resulting of wear and environmental factors, such as pressure, impact or mechanical and thermal loads, and other defects derived from photodegradation, corrosion or chemical abrasion. These defects either formed during fabrication or during service life, if not detected and repaired in time, can compromise the integrity of the material, potentially causing more serious damage and, ultimately, leading to its catastrophic failure. Most structural and high-performance composites are constituted by a thermosetting matrix that entails challenges when it comes to repair, for that reason, self-healing becomes relevant, particularly in the case of microfractures that occur within the structure of materials and are therefore difficult to detect and repair. Hence, with this type of approach, it is possible to assess damage at an early stage and therefore increase the service life of composites, as the graph in Figure 1 [11] schematizes, reduce the need for maintenance, as well as the associated costs, improve the safety of structures and increase the possibilities of less conservative designs. In light of this, an ideal self-healing composite (Figure 1 [11]) should be able to naturally, repeatedly and consistently fix itself to the extent of a considerable, but not too large damage, regardless of its size [1,2,3,4,5,6,7,8,9].
The relevance of self-healing capacity is, therefore, clear, considering the demand for functional materials for modern applications. Thus, the market of self-healing materials in general (not specifically self-healing polymer-matrix composites) is expected to grow in a compound annual growth rate of 56,5 % from 2021 to 2029. Within this context, the construction segment will be the largest consumer of these materials, holding approximately 55,5 % of the market and it is expected to undergo the fastest growth during the analyzed period. Despite that, automotive and electronic devices manufacturing industries are expected to endorse growth altogether with paints and coatings [10].
Figure 1.
Comparison between the lifetime expansion of self-healing materials and traditional ones. Adapted from " Effect of polymer architecture on the intrinsic self-healing character of polymers" by Santiago J. Garcia, used under CC BY 4.0 [https://doi.org/10.1016/j.eurpolymj.2014.01.026] [11].
Figure 1.
Comparison between the lifetime expansion of self-healing materials and traditional ones. Adapted from " Effect of polymer architecture on the intrinsic self-healing character of polymers" by Santiago J. Garcia, used under CC BY 4.0 [https://doi.org/10.1016/j.eurpolymj.2014.01.026] [11].
It is against this background that this paper was written, aiming to explore and summarize the recent and most innovative developments on the topic of self-healing polymer composites and how they can redefine the future path of material resilience. A review of the different approaches to self-healing is provided, focusing on the working principles and their main strengths and weaknesses, and backed on relevant experimental works elaborated in recent years. The applications that the studied materials might find are also highlighted, together with the challenges and opportunities of this field.
2. Approaches to Self-Healing
The mechanism of self-healing can be divided into two major types: intrinsic repair, which occurs through reversible intra and/or inter molecular interactions between the polymeric chains of the material itself (such as dynamic non-covalent bonds or hydrogen bonding), and extrinsic repair, which occurs through the action of extraneous healing agents that are, in turn, incorporated into the composite’s matrix, which does not have the repairing capacity itself. For this last case, the response is either based on polymerization reactions, catalyzed or not, such as ring-opening or cationic polymerization; intertwining or cross-linking of the polymer chains by the action of curing agents [1,12]. Other extrinsic repair response includes the incorporation of thermoplastic polymers [1,4]. Extrinsic self-healing stands out for its high healing efficiency, low cost and possibility to be implemented to a more diverse range of materials, whilst intrinsic self-healing is limited to materials with inherent reversible molecular interactions that need rigorous reaction conditions and are therefore tendentially dependent of external stimulus (such as temperature or UV light) to act. Besides that, it is also limited to smaller volumes of damage, considering that the repair occurs on a molecular scale. Nevertheless, intrinsic self-healing also possesses advantages, such as repeatability of self-repair, easiness of application and less limitations concerning integration and compatibilization of the healing agents [6,13,14,15,16]. This review is primarily concerned with extrinsic self-healing, due to the possibility to extrapolate its principles to a wider range of materials and to make the system act independently.
Although the response of the repair process itself is, in part, similar for the different approaches to extrinsic self-healing, the mechanism will rely on the chemical groups present around the fracture, which, in turn, differs whether it involves only the matrix material or both the matrix and other fillers. Thus, the effectiveness of the process depends on the reactivity of the healing agent with the surfaces it comes into contact with [4]. The material’s relaxation time is also considered crucial to the repair mechanism, assuming that slow relaxation is favorable to the self-repair mechanism, as it contributes to the rearrangement of polymer chains [4].
2.1. Healing Efficiency
When developing a self-healing composite, its performance should be evaluated and quantified. Therefore, repair efficiency is preferably calculated which often consists of the ratio between the mechanical properties of the material, before and after repair or of the self-healed material compared to the virgin one (Equation 1). Still, some authors may also consider other alternative formulas. Ergo, a perfectly healed material would have an efficiency of 1 (η=1). This variable can be defined based on several mechanical properties, some examples being fracture resistance, fracture stress, material strength or moduli related to mechanical properties (e.g. Young's modulus) [4,17]. An adequate property ought to be chosen according to the final purpose of the composite, for example, impact strength is particularly important when it comes to fiber composites for aerospace and military sectors [14]. Nevertheless, the fact that the self-healing composites’ efficiency is not determined in the same way in all studies, especially regarding the mechanical property under analysis, makes the comparison between the different methods under development not linear.
2.2. Self-Healing trough Reservoirs
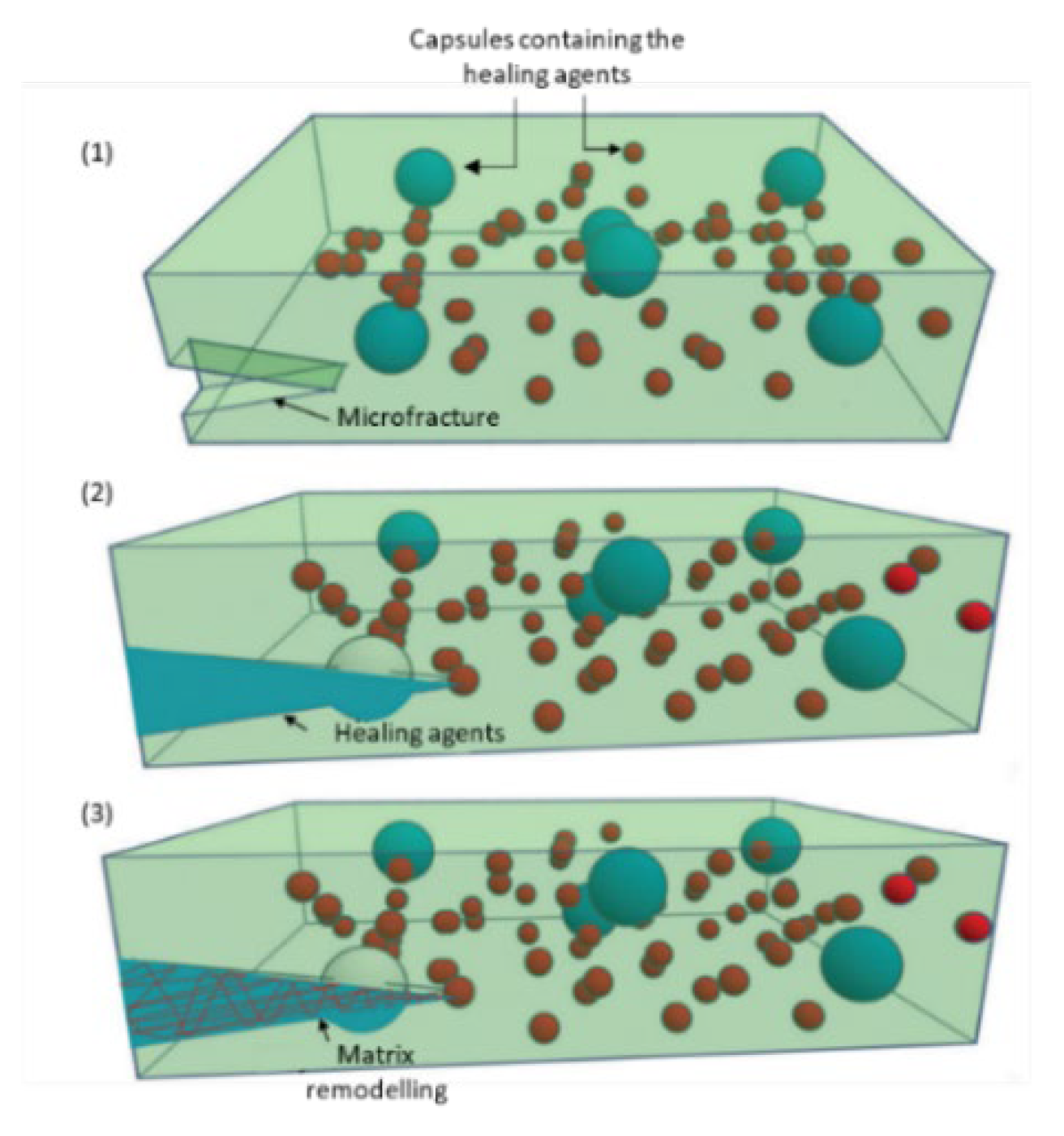
The reparative response trough reservoirs incorporated into the matrix occurs in 3 main steps, as shown in Figure 2 [1]: first the driving action, that is, the damage that will lead to the breakdown of the reservoirs and consequent release of the repair compounds contained therein, then their transport to the site of damage, for example the crack, and finally the chemical reparation of the matrix with the aim to restore the structural integrity of the material [1,12].
There are diverse types of structures for these reservoirs, particularly capsules, hollow fibers and capillary networks, typically consisting of an inert material compatible with the matrix and intended to protect the repairing agents from unwanted reactions or changes on their chemical properties. Generally, to achieve an efficient self-healing composite, it is necessary to consider some important factors concerning the reservoirs, namely strength, which should ensure safe handling and processing and good storage stability, so that no deformation takes place and breakage only happens when the material’s damage occurs, and excellent interface adhesion, which guarantees that, when the fracture is formed, the container ruptures and the healing agent is released. In some cases, compatibilizers might be necessary for that purpose. Likewise, the incorporation of the reservoirs in the matrix is relevant, considering that they must be rightly embedded and uniformly distributed [1,2,13,18,19]. Ultimately, the quantity, shape and size of these reservoirs can be adjusted to the material’s final application [17].
When it comes to the healing agents, they should ensure not only high reactivity, but also good flowability and adhesion/compatibility with the polymeric matrix, despite the possibility of either being different of the matrix or not [18]. Additionally, such reactivity must allow them to also react quickly and effectively regenerate the composite material in question. Other relevant properties of these reactants include good storage stability within the structures that contain them, so that they do not react undesirably, degrade at common composites’ manufacturing temperatures or entail safety risks. Furthermore, surface tension, contact angle and permeability must be adequate, so that the diffusion process is efficient and gaps are quickly filled. [1,4,20].
On the early development stages of extrinsic self-healing composites, one pioneer approach was the employment of dicyclopentadiene which undergoes ring-opening metathesis polymerization catalyzed by the Grubb’s catalyst. However, in late years research has been dedicated to developing more efficient healing agents, not only based on catalyzed ring-opening polymerization, such as 5-ethylene-2-norbornene, that exhibits a superior healing efficiency, but also resorting to polymers similar to the matrix, as is the case of epoxy resins combined with curing agents [8,18]. These stand out for having a better affinity with the mentioned matrix and lower curing temperature, resulting in superior self-healing potential, however they are also more viscous and less reactive than catalyst-based systems and can, therefore, create limitations concerning processability [18].
To promote a better performance of the reservoir-based self-healing systems, the possibility of using solvents has also been addressed either to facilitate the transport of the catalyst [21] or to penetrate the polymeric matrix, weaken the intermolecular forces, intensify the movement of the polymeric chains and lead to swelling of the material, which will improve the contact between the fracture components and facilitate repair [22]. Furthermore, for systems where encapsulated resins are used, it should be considered that, even if the curing agent can react at room temperature, the viscosity of the resin, at such conditions, can be a limitation when it comes to its ability to infiltrate fractures.
Other nanomaterials of which carbon nanotubes are example can also be stored inside the reservoirs as an additional component that can not only promote the reinforcement of the newly solidified polymer (either on a resin/hardener system or on a monomer/initiator one), improving the mechanical properties’ recovery, but also potentially contribute to the restoration of other functional properties, such as electrical conductivity [23,24].
2.2.1. Capsules
Capsule-based self-healing composites (Figure 2 [1]) are the most extensively studied ones, particularly the ones that resort to microcapsules, due to the variety and the easiness of implementation in different polymeric systems, resulting in a thorough description of the fabrication methods. Capsules can either be single, with, for example, the catalyst embedded in the matrix, or double, containing more than one regenerating reactant in the same capsule or in different capsules [1].
Within this context, H.Hu et al. [25] explored the development of an epoxy resin based composite, where two different types of microcapsules were used: one containing the same polymer as the matrix (12 wt%) and the other containing an amine curing agent (8 wt%) that would react with the first one. The healing conditions consisted of 24 h at room temperature, followed by 6 h, at 50 ºC. It was concluded that the healing efficiency, evaluated through the fracture toughness, was about 80,4 %. Alternatively, C. Y. Zhang et al. [26] proposed the encapsulation of styrene and benzoyl peroxide separately, so that the first was polymerized through initiation with the second, upon microcapsule breakage. Such reservoirs were incorporated into an epoxy-based matrix and a maximum healing efficiency of 65 % was attained, through impact tests, when 15 wt% of styrene loaded capsules and 3 wt% of benzoyl peroxide loaded capsules were employed and after 24 h, at 25 ºC. The materials’ multi-repairability was also analyzed and a reduction of about 20 % to 30 % was detected for the second and third repairs. On a different approach, H. H. Zamal et al. [27] encapsulated a mixture of monomers of 5-ethylidene-2-norbornene with multi-walled carbon nanotubes, which were then dispersed (10 wt%) in an epoxy polymeric matrix, together with a ruthenium Grubbs catalyst, responsible for initiating ring opening metathesis polymerization reaction. It was highlighted that an ambient temperature curing resin was chosen for the matrix to prevent catalyst degradation. The main conclusions were firstly that the presence of the microcapsules contributed to the reinforcement of the material and secondly that the carbon nanotubes increased the strength of the polymer synthesized upon capsule rupture, which was reflected on an improved healing efficiency of 97 %, calculated by fracture toughness, after healing at room temperature, for 48 h. Another distinct concept worth analyzing is the one brought by R. Rodriguez et al. [28] where microcapsules (20 wt%) containing an epoxy resin (equal to the matrix one) on the inside and a curing initiator catalyst (Scandium triflate (III)) on the outer surface were prepared. This type of structure amplified the probability of the encapsulated resin reacting with the catalyst and, consequently, an efficiency of 79,1 % was attained after healing at 120 ºC, for 24 h, analyzed in terms of fracture toughness recovery. Furthermore, Shunze Cao et al. [15] explored the utilization of multicore-like bilayer calcium-alginate capsules, containing epoxy resin on the inside core, whereas a curing agent was on the outer one. Such structures were synthesized through multi-stage encapsulation and incorporated (15 % volume fraction) into epoxy-based foams whose purpose was to integrate foam core sandwich structures. The advantage of this type of microcapsules was their capability to promote a more adequate mixture of the two healing agents. It was suggested that, when compared to conventional dual capsule systems, the multicore capsules exhibited better multiple self-healing performance, with a maximum efficiency greater than 80 % for the first cycle, determined through the elastic modulus. Nevertheless, this efficiency decreased throughout the cycles. Moreover, the compressive strength and stiffness of the foams were improved.
On their work, Amanda R. Jones et al. [29] explored the self-healing of carbon fiber/epoxy interfaces, aiming to prevent fiber/matrix debonding, which has consequences on the mechanical properties of the material. For that purpose, micro-capsules containing a resin solvent solution responsible for interface regeneration were incorporated into the reinforcing carbon fibers’ surface. Upon debonding, the microcapsules underwent rupture, releasing the healing agents that repaired the interface. The usage of a binder to stabilize the capsules on the fibers’ surface was assessed, as well has the impact of the coverage of microcapsules at the interface. It was concluded that a maximum of 91 % recovery of the interfacial shear strength could be achieved. Finally, an innovative concept was introduced by Wrihao Yuan et al. [30], that, aside from incorporating microcapsules containing epoxy resin and mercaptan into the polymeric matrix, modified silver nanoparticles on the surface of the reinforcing carbon fibers. The purpose of such approach was that the reaction between the epoxy resin and mercaptan repaired the polymeric matrix, while a coordination connection was stablished between the sulfhydryl group of the mercaptan and the silver nanoparticles, contributing to the regeneration of the fiber/matrix interface. Besides that, the healing reaction between the epoxy resin and the mercaptan is strongly exothermic, therefore thermal signals were released from the crack healing, which were then captured by an infrared thermal imager, thus the damage and the healing reaction could be monitored. A healing efficiency of 80 % was attained after 24 h, at room temperature, for a microcapsules’ content of 15 wt%, evaluated by fracture toughness. Besides that, the healing effectiveness at the interface, analyzed resorting to the interface shear strength, reached 74 %, for the same microcapsule content.
Nevertheless, these structures have some limitations, particularly with regard to the amount of repairing agent they contain, making it impossible to know when it has been completely consumed or to feed it back into the system, as the number of capsules is finite [3,12]. Other effects that must be considered include the probability of microfractures meeting the capsules randomly dispersed in the matrix, so that the repair agent is released; the material, size distribution and thickness of these capsules, the aforementioned compatibility with the matrix, the hypothesis of particle coalescence and the influence that these characteristics have on the properties of the matrix itself. Furthermore, after the capsules break and the regenerating compound is released, the empty capsule remains in the matrix, allowing the accumulation of tension at the site, which could have negative consequences, especially in the case of structural composites, ultimately leading to the re-occurrence of a damage in the same location. However, this behavior is still little studied. Besides that, after the second impact, the failures must follow a path that assures that the crack meets the unbroken microcapsules, otherwise the damage might not be healed, routing the possibility of microcrack expansion into a more complicated macro-damage. Additionally, microcapsules may not be suitable for composites which are manufactured under high pressures, considering that their shape can be deformed [14,18,26]. Urea-formaldehyde, melamine-urea-formaldehyde and polyurethane capsules are preferably used, considering that they exhibit mechanical resistance so as not to be degraded during processing, but are still soft enough to rupture relatively quickly when necessary [4,18]. Commonly in situ or interfacial polymerization or generally methods that resort to emulsion or melt dispersion are used, where the core content of the microcapsules is dispersed in a solution of the shell polymer’s components or vice-versa. Initially droplets are formed and then the polymeric layer is synthetized and solidified around them. There are some parameters that are determinant for the morphology and size of the microcapsules, that, in turn, influence the composite’s characteristics and these include: stirring rate, temperature, reaction time, weight ratio of core/shell material and emulsifier content, if applicable. For instance, smaller microcapsules with a smoother surface and no evidence of collapse stand out for promoting less negative impacts on the composite’s mechanical properties, since they possess smaller tendency to agglomerate, reduce the stress concentration and cause less filling fiber misorientation. [14,18,25,31].
2.2.2. Hollow Fibers
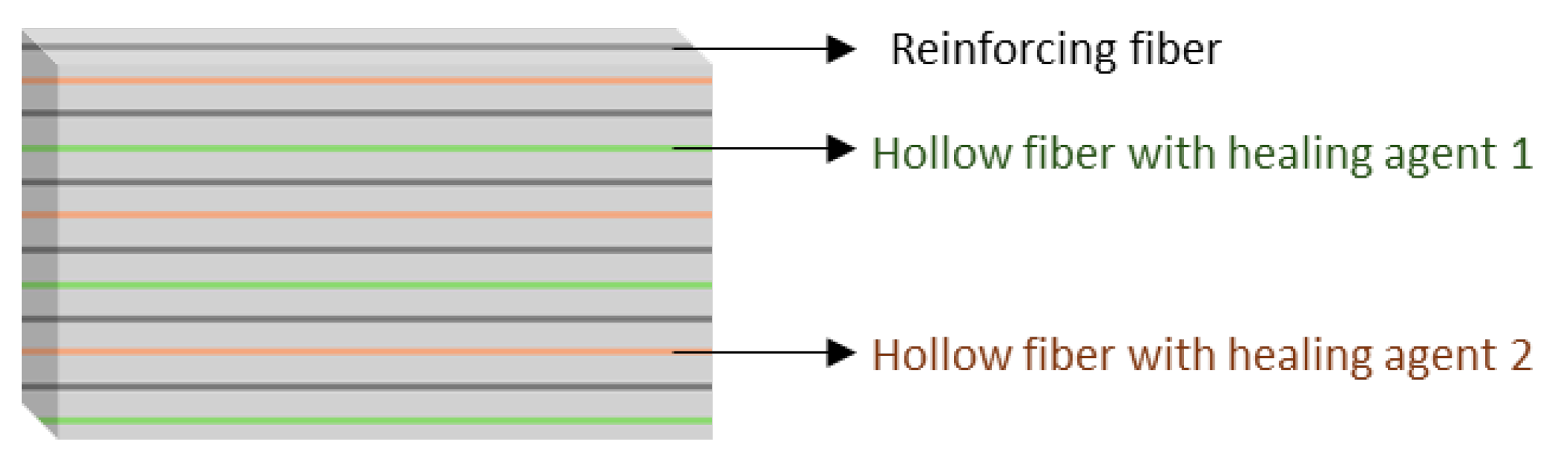
In what concerns hollow fibers (Figure 3 [4]), their operating principle is similar to that of capsules, however, they allow to overcome some of the lasts’ limitations, particularly with regard to storing larger volumes of healing agent and transporting them to greater distances. It is also worth noting that the fibers may cover a greater volume of the material, increasing the probability of the reservoir breaking when the fracture occurs, and can be arranged on demand, contributing to a more uniform distribution of the healing agents through the final material, even benefiting the stoichiometric mixture of the referred reactants. These fibers can be incorporated directly between the reinforcing fibers. Similarly to the microcapsules, two healing agents can circulate on different fibers, as shown in Figure 3 [1,4,18].
In this setting, A. Adili et al. [32] developed a healing system combining an epoxy resin and an amine curing agent, both equal do the matrix’s materials and each one deposited inside a different glass fiber. It was observed that, when empty, the glass fibers negatively affected the material’s strength, due to stress concentration and crack initiation. Despite that, it was concluded that smaller distances between the fibers were synonymous of a higher amount of healing agent and, therefore, resulted in an improved healing performance. Additionally, when positioned in angles of 45 º, the fibers underwent higher shear stress and consequently were more prone to fracture, ensuing a wider diffusion of the healing agents and contributing to a better healing efficiency, which was 42 %, determined by tensile strength, after 48 h, at 70 ºC. By contrast, S. Kling [33] proposed a healing response based on a polyester resin system stored inside tin hollow glass fibers, with an outer diameter of 13 µm, and integrated into an epoxy matrix composite. One type of fiber was filled with the catalyzed unsaturated polyester resin and the other one contained the initiator (methyl ethyl ketone peroxide) dissolved in dimethyl phthalate. This option was justified by the fact that this reacting system is not as sensitive to the mixing ratio and method as others. It was demonstrated that the composite was self-healable at 23 ºC, during 120 h. A method based on the combined answer of a monomer and catalyst can also be applied to these structures, as I. Radovic et al. [21] proposed. Herein, the monomer dicyclopentadiene was mixed with a solvent (N, N′-dimethylformamide) and fed to one type of fiber, whereas the first generation Grubbs catalyst, also dissolved in a solvent (preferably toluene, since other solvents such as dichloromethane can deactivate the catalyst during processing) was fed to another type. In this case it was found that, when filled with the healing components, the fibers actually operated as reinforcing agents, and the healing efficiency, determined through impact tests, achieved a value of 53 %, after 24 h, at 25 ºC.
On a different approach, S. A. M. Sadeghi et al. [34] developed a core-shell nanofibers mat resorting to single nozzle electrospinning, where epoxy resin and a mercaptan-based epoxy hardener were enclosed. This mat was then incorporated into an epoxy resin-based composite and it was noted that the presence of healing agent on the surface of the nanofibers promoted a good adhesion between the matrix and the mat. The conclusion was that the material was able to self-heal and restore flexural modulus and strength, after being kept at 10 ºC, for 200 min.
A groundbreaking strategy was developed by Y. Zhu et al. [35] where the mixing of the healing agents with a foaming agent was evaluated, together with the utilization of polypropylene tubes. These tubes were chosen, considering that they allow for the healing agents to be easily filled into larger tubes whose diameter can then be reduced, overcoming not only the difficulty of filling narrow tubes, but also preventing the weakening of the mechanical properties caused by larger tubes. Besides that, the tubes’ flexibility admits their knitting together with the traditional reinforcing fibers, in this case glass fibers, which is beneficial for materials with complicated shapes. Although polypropylene’s natural non-polarity can compromise interfacial adhesion, there is the possibility of modifying its physicochemical properties in order to improve such interaction. Finally, this polymer does not tend to react with the healing compounds that it contains. Nevertheless, the polypropylene tubes had to be irradiated by UV light with the aim of embrittling and polarizing the surface, so that they would break upon damage of the composite. The healing response relied on an epoxy resin cured by a thiol and amine mixture, and 2,2’-Azobis-(2,4-dimethylvaleronitrile) was added as the foaming agent, that does not affect the healing agents’ cure. The material was previously pressurized so that when damage occurred the high internal pressure of the foaming agent favored the spreading of the healing reactants over the damages. The healing efficiency, determined through flexural strength of the healed specimen in comparison to the virgin one, was about 93 %, but a decrease on such parameter was identified when the storage time increased, due to leakage of the pressurized foaming agent, and therefore it was suggested that polypropylene impermeability could be improved.
At this point, it can be highlighted that the main challenge of this approach is the filling of the hollow fibers, due to their reduced diameter. Some techniques include filling from top or drawing from bottom, and typically they are achieved by capillary action assisted by vacuum to aid the infiltration [14]. Besides that, if the diameter of the fibers is too small, the viscosity of the regenerating agent can limit its transport to the damaged area. As shown, the utilization of glass fibers is typically reported, considering that they break at lower energy levels, and it is conjectured that they can act not only as a transport route for the repairing agents in question, but also as a structural reinforcement of the composite material [1,4,16]. The application of carbon nanotubes is also suggested, however it is assumed that their high resistance may not allow breakage during fracture formation [17]. Besides that, the amount and spatial distribution of the fibers should also be object of scrutiny due to their effects on the mechanical behavior and healing response of the composite, as some of the previously mentioned articles highlight [16].
Figure 3.
Scheme of a composite consisting of hollow fibers containing the healing agents and reinforcing fibers.
Figure 3.
Scheme of a composite consisting of hollow fibers containing the healing agents and reinforcing fibers.
2.2.3. Microvascular Networks
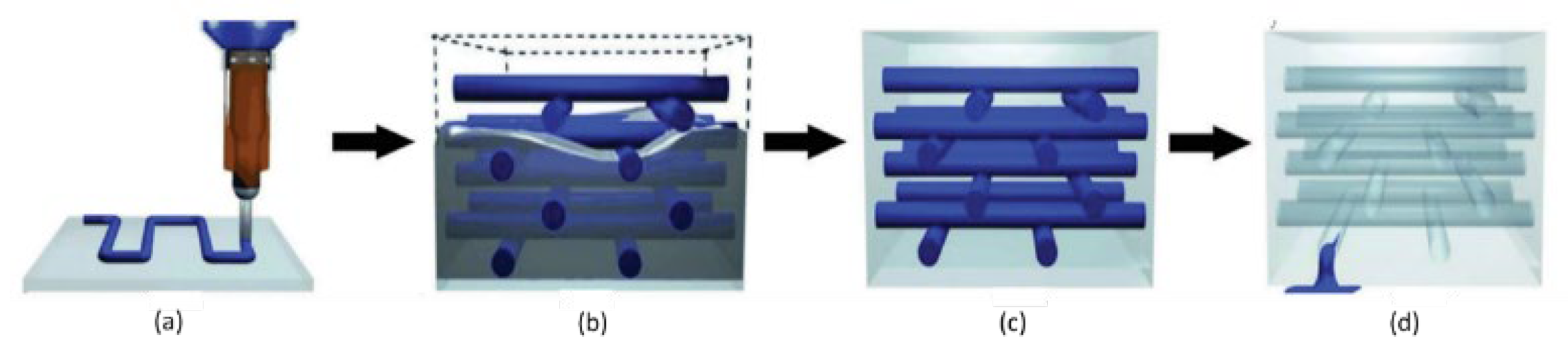
To overcome the limitations associated to capsules and hollow fibers, interest has grown in studying the distribution of the healing agents through capillary networks which, as the name suggests, consist of 2D or 3D networks of interconnected microchannels that transport the compounds in question to the damaged areas. This method is, in part, similar to the previous one, however, the connected network of channels makes it possible to continuously feed the damage site, allowing more than one repair event to be carried out in the same location, which is complemented by the fact that the system can be refed. Hence, fresh healing agent can be supplied, preventing it from being stored for too long and eventually lose its activity. In this context, the hypothesis of integrating reservoirs capable of automatically detecting the need for repair and consequently feeding the healing agent to the system has already been considered [1,17,18]. With this model, it is also possible to add the repairing compounds in distinct types of capillaries. This perspective is, therefore, considered one of the most promising ones in the field of auto repair materials [1,3]. Still, the development and practical application of this concept is difficult, especially in large-scale materials. Capillary networks can be developed based on non-removable or removable preforms. In the first case, like the other types of reservoirs, the capillaries must be broken so that the repairing reactants are released in the fracture, arising concerns already mentioned. In the second case, the structure of the material intrinsically integrates the hollow capillary network where the repaired agents circulate, meaning that they can flow immediately to the damage, when it is formed, without the need for reservoir breakage. However, this last option poses some limitations, on the one hand the compounds circulating in the network are not protected, being in direct contact with the matrix, and on the other hand there is possibility of channels’ deformation during the manufacturing process [18,36]. The proposals for the development of removable preforms involve wires coated with a release agent that allows manual extraction of such wires, or 3D printing using a non-permanent material/fugitive organic ink made up of a mixture of high and low molecular weight hydrocarbons, for example a mixture of 60 % petroleum jelly and 40 % microcrystalline wax. The vascular network is developed at an initial stage and only then the material itself is formed, as shown in Figure 4 [1]. The mentioned fugitive ink is removed after the matrix resin has cured, by heating at a moderate temperature, under light vacuum, so that it is liquified. In such way, the final material is left with space in channels than can be filled with the healing agents [1,14,19,37].
On that matter, R. Eslami-Farsani et al. [38] designed a microvascular network resorting to digital light processing method, based on the Vat polymerization technique and using a 3D printer. Such network was made of two different sub-networks: one where the epoxy resin flowed (the same as the matrix) and another with the curing agent. Besides the microvascular system, the composite was also reinforced with glass fiber. It was concluded that the network presence led to a reduction on composite’s tensile strength, however, it was also suggested that such problem could be overcame by selecting a more rigid material for the network. A healing efficiency of 89 % was calculated resorting to tensile strength, after 7 days at ambient conditions. Moreover, R. S. Amano et al. [39] imprinted a vascular network on one layer of glass fiber reinforced composite. The vascular network was filled with dicyclopentadiene, while Grubbs catalyst was infused in this same layer, such system was responsible for the self-healing response. Two types of patterns for the vascular networks were analyzed: square and hexagonal. It was concluded that the average strength of the composite, attained via three-point bending test, nearly doubled after recovery, which is attributed to the reaction of the healing agents and the formation of polydicyclopentadiene which is about 50 % as strong as the matrix’s epoxy resin. Additionally, it was observed that a hexagonal grid favors the access to the contained healing agent, during the damage formation. The final purpose of these developed materials was to produce self-healing wind turbine blades.
O. Fifo et al. [19] proposed an alternative approach where an in vivo vascular channel was employed for self-healing of a glass fiber polyester composite. It preferably resorted to an automated process of injection of a single-part adhesive (cyanoacrylate adhesive) into a 2D network of hollow channels directly integrated within de composite. Such network was built resorting to a nylon cord coated with wax that was removed at the end of the preparation. This network was located at the material’s mid-plane, so that damages originating from either surface could contact the hollow channels. An average recovery of 84 % of the flexural stiffness and 46 % of the loading strength was determined, based on bending tests, after self-healing at ambient conditions, for 24 h. Furthermore, J. F. Patrick et al. [37] resorted to sacrificial poly(lactic acid) monofilaments arranged in two different patterns through the woven fabric of an epoxy resin based fiber reinforced composite that were removed after the composite’s cure. The healing answer was based on the action of an epoxy resin and an amine-based curing agent, both of low viscosity. The first configuration was parallel, with the mixing of the two components being limited to adjacent layers, while the second one was a herringbone design, where the blending of the healing components was favored by the overlapping of the networks. For that reason, it was concluded that the herringbone design provided higher healing efficiencies for specimens healed at 30 ºC, for 48 h. Additionally, over 100 % healing efficiency as observed due to the higher fracture toughness of the healed polymer, when compared to the structural matrix. Tree successive healing cycles were performed and after each one, higher loads were necessary for the crack to propagate.
Relevant parameters for the microvascular networks include the microchannels’ dimensions, as well as the network feeding mode, the pressure of the vascular system and the viscosity of the repairing agent, to ensure that it is properly distributed. Therefore, if necessary, pumps can be incorporated outside to direct the flow of the repair agent to the damaged areas [1,14,17].
Figure 4.
Manufacturing process of a self-healing composite material consisting of a capillary network: (a) Deposition of the non-permanent material to develop the network of capillaries, (b) Deposition of the matrix material, (c) Solidification of the material, (d) Removal of the non-permanent material and final shape of the composite with the network of capillaries. Adapted from " Progress and challenges in self-healing composite materials" by Shafiqul Islam and Gajanan Bhat, used under CC BY 3.0. [https://doi.org/10.1039/D0MA00873G] [1].
Figure 4.
Manufacturing process of a self-healing composite material consisting of a capillary network: (a) Deposition of the non-permanent material to develop the network of capillaries, (b) Deposition of the matrix material, (c) Solidification of the material, (d) Removal of the non-permanent material and final shape of the composite with the network of capillaries. Adapted from " Progress and challenges in self-healing composite materials" by Shafiqul Islam and Gajanan Bhat, used under CC BY 3.0. [https://doi.org/10.1039/D0MA00873G] [1].
There is also the possibility of combining the aforementioned approaches based on reservoirs, in order to take advantage of the benefits that each one provides. For example, the resin can be in hollow fibers, while the corresponding curing agent is microencapsulated [40].
2.3. Self-Healing trough Thermoplastic Polymers
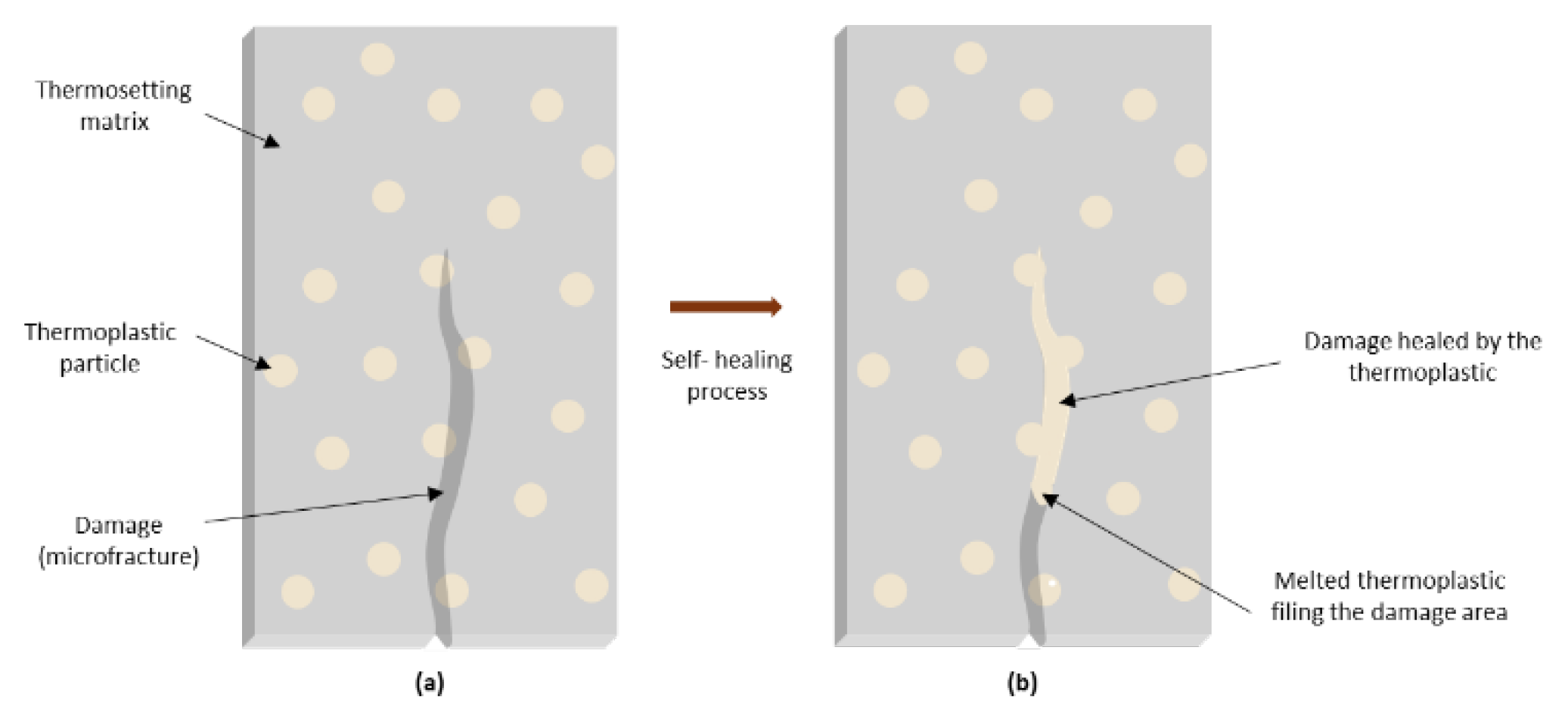
In the case of self-healing using thermoplastic polymers, these are incorporated into the matrix, for example in the shape of particles, films or fibers, either mixed with the thermosetting resin or incorporated between the carbon fiber plies, prior to resin impregnation. Upon heating and consequent melting, the thermoplastic migrate by diffusion to the flaws, when they arise, and establish chemical bonds with their surfaces, as schematized on Figure 5 [41]. Accordingly, a good affinity between the thermoplastic and the commonly thermosetting matrix is required, so that an efficient healing occurs and there is stress transfer between the thermoplastic and the epoxy matrix. Some of the thermoplastic polymers already investigated for this purpose include poly(ethylene co methacrylic acid) (EMAA), poly(methyl methacrylate) (PMMA), ethylene vinyl acetate (EVA), poly(ethylene co glycidyl)-methacrylate (PEGMA), poly(vinyl butyral) (PVB), styrene ethylene butadiene copolymer (SEBS) and acrylonitrile-butadiene-styrene (ABS). In addition to these factors, some authors [41,42] also highlight the roll of small bubbles present inside the thermoplastic, particularly EMAA, that expand upon heating, generating a high internal pressure difference that will force the thermoplastic into the crack, imposing the polymer flow. Such bubbles are theorized to be formed as a result of chemical reactions taking place between the thermosetting matrix and the thermoplastic polymer containing carboxylic acid groups on their structure, that produce water as a volatile product whose solubility in the polymer is very limited. Such reactions might include condensation between the hydroxyl groups of the epoxy matrix and the carboxylic acid groups of the filling polymer or amidation of these carboxylic groups. One of the main disadvantages of the present alternative is that it requires temperature for the melting and diffusion of the repairing polymer to occur, meaning it is not a completely autonomous system. However, it theoretically allows for unlimited cycles of self-healing, since it can be repetitively melted and solidified [4,18,43,44].
Within this framework, A. Azevedo et al. [44] incorporated poly(ethylene-co-methacrylic acid) microparticles (5 wt%) between prepreg layers at the mid-plane of carbon-epoxy laminates. The incorporated thermoplastic established chemical interactions with the epoxy matrix, promoting a strong interfacial adhesion what, in turn, contributed to a complete recovery of the interlaminar shear strength, after healing at 150 ºC, during 30 min. Nevertheless the addition of poly(ethylene co methacrylic acid) promoted a slight increase in the glass transition temperature and a decrease on the composite’s interlaminar shear strength and storage modulus, when compared to the virgin material. Differently, M. Peñas-Caballero et al. [43] developed an innovative approach where poly(methyl methacrylate) was applied, as a healing agent, to reinforcing carbon fibers, by spray coating, and directly mixed with the epoxy-based matrix, amounting for 20 wt% PMMA. It was concluded that the thermoplastic polymer interacted with the epoxy thermosetting polymer through a transesterification reaction. However, trials with a zinc acetate catalyst led to the observation that such interaction was not the driving mechanism for the healing process, which was rather led by the softening and flow of the polymer. Nevertheless, the reaction still improved the interface adhesion and was therefore favored by the catalyst action. Furthermore, the fibers were uniformly coated, but some reduction of the mechanical properties was observed. Despite that, the composites exhibited up to 53 % healing efficiency, determined by the fracture toughness, after heating at 150 ºC, for 120 min.
Another breakthrough method was proposed by B. Chen et al. [45], where polyamine nanofibers where electrospinned and deposited on the surface of an unidirectional carbon fiber fabric. This thermoplastic polymer was uniformly distributed between the interlayers of a carbon reinforced epoxy composite. The main objective was that the polyamine entangled fibers worked both as a toughening material for the interlayer of the composite and as a self-healing agent. The addition of 1,2 wt% of the thermoplastic polymer increased the interlaminar shear strength by 17,6 % and the bending properties by 14,7 %, due to the large specific surface area and the good interaction between the polyamide and the epoxy matrix, that improves the interface adhesion. The healing process took place at 130 ºC, during 20 min, and the efficiency was analyzed throughout 3 cycles, resorting to the interlaminar shear strength. A maximum value of 110,44 % was determined for the first one, for an electrospinning time of 3 h. It was also highlighted that the incorporated fibers did not affect the storage modulus, nor the glass transition temperature of the composites. Innovatively, R. B. Ladani et al. [42,46] developed a carbon fiber reinforced epoxy composite aimed to resist the growth of delamination cracks and self-heal such flaws. For that purpose, they resorted to through- the-thickness z-binders, namely one type made of carbon fiber, to achieve the first goal, and the second one made of thermoplastic filaments, particularly poly(ethylene-co-methacrylic acid), to achieve the second one. The hybrid composite underwent an increase both on the mode I fracture toughness (1200 %) and on the mode II fracture toughness (75 %). Self-healing was then stimulated at 150 ºC, for 30 min. A recovery of 35-40 % of the original value of the mode I fracture toughness was observed, whilst a restore of 25 % of the original mode II fracture toughness was measured. The significant difference between the two cases is justified by the fact that the molten thermoplastic polymer could more easily flow into the mode I wider delamination crack.
Anyhow, the temperature dependence could be overcome through the utilization of an encapsulated solvent that, during the formation of the fracture, would be released, dissolving the thermoplastic, transporting it to the necessary area and evaporating at the end, in a somewhat similar approach to the previously described capsules [20,47]. Another alternative would be to induce localized fusion, using superparamagnetic nanoparticles, that is, nanoparticles that only exhibit magnetization when subjected to an external magnetic field, embedded in thermoplastic. Thus, upon the application of such field, the temperature of the nanoparticle/polymer interface would increase, triggering the melting of the thermoplastic that would flow towards the failure. Graphene can also lead to localized heating when exposed to electricity, infrared radiation or electromagnetic waves, so the application of a principle similar to the previous one is also a hypothesis [17].
In light of this, K. M. Chang [47] developed a composite where a thermoplastic resin, poly(bisphenol A-co-epichlorohydrin), was dispersed on an carbon fiber reinforced epoxy matrix, together with an encapsulated solvent (ethyl phenyl acetate). The healing efficiency of such system was compared with a traditional one, where temperature was used to melt the thermoplastic resin instead, and the conclusion was that no statistically significant differences existed between the two approaches. That meant that the usage of solvents was as feasible as the conventional method and the healing efficiency determined through tensile tests was 57 %.
As explained in the reservoir-based approach, here it is also important to address the consequences of thermoplastic incorporation on the composites’ mechanical properties, considering that strength reduction might occur. For that reason, there are limitations regarding the dimensions of the incorporated particles, nevertheless it is suggested that thermoplastic repairing agents are efficient and easier to prepare and incorporate into the matrix, when compared to the capsule and fiber systems discussed in the previous paragraphs. [4,18].
Figure 5.
Healing process using thermoplastic particles: (a) Fracture formation; (b) Melting of the thermoplastic polymer, followed by cooling and consequent matrix reparation.
Figure 5.
Healing process using thermoplastic particles: (a) Fracture formation; (b) Melting of the thermoplastic polymer, followed by cooling and consequent matrix reparation.
Throughout this review it becomes clear that providing a composite with self-healing capacity comes at the expense of some of the materials’ properties, mostly mechanical ones. For that reason, the choice of an adequate approach to self-healing will depend on the nature of the materials involved, its applications, the adequacy of a certain stimulus and the compromise between the properties’ loss and the necessary healing efficiency.
3. Applications
Self-healing composites can be implemented in varied areas, especially standing out in applications with difficult access and high inspection and maintenance costs, such as wind turbine blades. Some examples include aerospace and aeronautic industry, particularly structural parts, for example wings, which must withstand high temperatures and pressures and resist impact, fatigue, corrosion and environmental factors. In fact, the European Space Agency has considered self healing materials as “one of the most futuristic concepts” for space crafts, due to the extreme fluctuations of the environmental conditions and the high velocity impacts that these can undergo. As a matter of fact, it is estimated by his agency that the materialization of this principle could double the lifetime of an erth-orbiting spacecraft, therefore halving the overall cost of the mission [5,27,48]. Also, in the automotive industry, these composites might find application in vehicle body parts, bumpers, tires and even batteries that can recover from damage, such as dents, puncture damage and wear, thus maintaining appearance, functionality and performance. In such way, the materials in question contribute to improve the safety, efficiency, lifespan and even the environmental impact of vehicles, minimizing the need for replacements of repairs. Another example involves civil engineering structures, such as buildings or even pipes, being that self-healing capacity would allow them to resist not only damage and deterioration, but also natural disasters, such as earthquakes, floods or fires. In this way, the safety, integrity, durability and resilience of infrastructures would also be improved here, reducing repair costs. In the same line of thought, their employment in defense should also be considered, as they can contribute to a wider lifespan of military equipment and also improve their security. On a different approach, these materials can be used in biomedicine, to produce implants, prostheses and sutures, which can resist the biological environment, recovering from damage caused, for example, by infection or inflammation. This would improve the functionality, effectiveness and durability of biomedical devices, reducing possible complications associated with side effects. Additionally, self-healing composites have also been considered for coatings, as they can repair damages and prevent failure as consequence of corrosion [14].
4. Challenges, Opportunities and Future Prospects
In light of this review, interest in self-healing composites with polymeric matrixes has indeed been growing in recent years, however, such technology is yet to be scaled up for practical applications, as the repair efficiency can vary significantly depending on damage size and the environmental conditions, such as pressure or temperature, at which the material is used, affecting, for example, the viscosity of the repair agent. Additionally, the repair times obtained so far are too long to be able to avoid the catastrophic failure of a composite that is being applied in practice. It is also important to consider that, over time, regenerating agents can lose their reactivity, causing the material to lose its self-repairing capacity. Besides that, the efficiency of this capacity tends to reduce as multiple failure and repair cycles occur. Moreover, although through numerical simulations a prediction can be made of where the material is going to fail, it is not completely accurate and therefore it is not possible to forecast where the self-healing system should be specifically introduced. Furthermore, and as previously discussed, it is very important to take into account that functionalization with self-repairing agents can trigger significant changes in the morphology and performance of the material and, consequently, in its physical and mechanical properties. It is also essential to consider that a sufficient amount of energy is necessary for these structures to break, being that if this energy is dissipated before reaching the reservoirs, the damage will not be repaired [1,4,8,17,18,19]. Aside from that, the studied systems that make use of catalysts are unaffordable in realistic practical applications, considering the high price, sensibility and toxicity of catalysts [15,49]. For these materials to be applied in practice, such limitations must be thoroughly studied and overcame.
In addition, the self-healing activity can still be innovated, for example through combination with other functionalities, including shape memory or stimulus responsiveness, like pH, temperature or electric field. Another interesting concept is the combination of repair activity with the signalization of this same action, for example through the presence of a fluorescent compound or through the thermal monitoring of the healing reaction [30,50]. This principle would be particularly interesting for applications of difficult to access, since, on the one hand, the self-repairing action allows the damage caused to be reversed, to a certain extent and, on the other hand, the signalization of the repair action allows the identification of the area where the damage and reparation occurred.
With this in mind, it is understandable that there still are opportunities for new research to be developed in this field, both to refine the current knowledge on self—healing materials and transfer it into real life applications and to improve and develop even smarter and more functional materials, adapted to the necessities of the future.
5. Conclusions
This review has provided an insight into extrinsic self-healing mechanisms for polymer composites, highlighting their autonomy and applicability to different types of materials. Two global approaches exist to prepare such composites, namely through the incorporation of either reservoirs containing the healing agents or thermoplastics. Among the first category, capsules are the most investigated ones, standing out for their easiness of application and being target of groundbreaking approaches, aimed to increase their efficiency. However, hollow fibers and microvascular networks have been emerging, due to their wider coverage of the materials’ volume and the capability of being refed. Such reservoirs are also under deep study, as alternatives are emerging to facilitate their integration on the composites’ structure. On their turn, thermoplastics have also been greatly explored considering their theoretical illimitation of healing cycles. Yet investigation is committed with developing alternative polymer melting mechanisms, that allow the total independency of the healing process. However, globally all the methods are tendentially synonym of jeopardized mechanical properties.
All in all, research shows that work still needs to be developed in order to transfer such knowledge to practical applications and to further innovate the field of self-healing composites.
Author Contributions
Conceptualization, M.L.D. and L.N.; investigation, M.L.D; writing—original draft preparation, M.L.D.; supervision, L.N., C.M., J.B., F.C and R.F.; project administration, , L.N., C.M., J.B., F.C and R.F.; funding acquisition, F.C and R.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the interface program (“Projeto Fibrenamics/CTI”) – “Programa base no âmbito do Plano de Recuperação e Resiliência aprovado nos termos do Aviso de Abertura de Concurso (AAC) nº 03/C05-i02/2022”.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Islam, S.; Bhat, G. Progress and Challenges in Self-Healing Composite Materials. Mater. Adv. 2021, 2, 1896–1926. [CrossRef]
- Priyadarsini, M.; Rekha Sahoo, D.; Biswal, T. A New Generation Self-Healing Composite Materials. Materials Today: Proceedings 2021, 47, 1229–1233. [CrossRef]
- Mercy, J.L.; Prakash, S. Self Healing Composite Materials: A Review. International Journal of ChemTech Research 2016.
- Cioffi, M.O.H.; Bomfim, A.S.C.; Ambrogi, V.; Advani, S.G. A Review on Self-healing Polymers and Polymer Composites for Structural Applications. Polymer Composites 2022, 43, 7643–7668. [CrossRef]
- Zhang, Z.P.; Rong, M.Z.; Zhang, M.Q. Self-Healable Functional Polymers and Polymer-Based Composites. Progress in Polymer Science 2023, 144, 101724. [CrossRef]
- Nik Md Noordin Kahar, N.N.F.; Osman, A.F.; Alosime, E.; Arsat, N.; Mohammad Azman, N.A.; Syamsir, A.; Itam, Z.; Abdul Hamid, Z.A. The Versatility of Polymeric Materials as Self-Healing Agents for Various Types of Applications: A Review. Polymers 2021, 13, 1194. [CrossRef]
- Kausar, A. Self-Healing Polymer/Carbon Nanotube Nanocomposite: A Review. Journal of Plastic Film & Sheeting 2021, 37, 160–181. [CrossRef]
- Vintila, I.S.; Badea, T.; Draghici, S.; Petrescu, H.A.; Cucuruz, A.; Iovu, H.; Hadar, A. Mechanical Characterization of DCPD and ENB Healing Systems in Glass Fibre Composites. Mater. Plast. 2020, 57, 278–289. [CrossRef]
- Srinivas, M.; Yelamasetti, B.; Vishnu Vardhan, T.; Mohammed, R. A Critical Review on Self-Healing Composites. Materials Today: Proceedings 2021, 46, 890–895. [CrossRef]
- Self-Healing Materials Market- Global Industry Analysis and Forecast (2022-2029)- By Product Type, Technology, Application, and Region. MAXIMIZE MARKET RESEARCH. Available online: www.maximizemarketresearch.com/market-report/global-self-healing-materials-market/65964/ (accessed on 20 December 2023).
- Garcia, S.J. Effect of Polymer Architecture on the Intrinsic Self-Healing Character of Polymers. European Polymer Journal 2014, 53, 118–125. [CrossRef]
- Kanu, N.J.; Gupta, E.; Vates, U.K.; Singh, G.K. Self-Healing Composites: A State-of-the-Art Review. Composites Part A: Applied Science and Manufacturing 2019, 121, 474–486. [CrossRef]
- Song, M.-M.; Wang, Y.-M.; Liang, X.-Y.; Zhang, X.-Q.; Zhang, S.; Li, B.-J. Functional Materials with Self-Healing Properties: A Review. Soft Matter 2019, 15, 6615–6625. [CrossRef]
- Je, P.C.; Sultan, M.T.; Selvan, C.P.; Irulappasamy, S.; Mustapha, F.; Basri, A.A.; Safri, S.N.A. Manufacturing Challenges in Self-Healing Technology for Polymer Composites — a Review. Journal of Materials Research and Technology 2020, 9, 7370–7379. [CrossRef]
- Cao, S.; Zhu, W.; Liu, T. Bio-Inspired Self-Healing Polymer Foams with Bilayered Capsule Systems. Composites Science and Technology 2020, 195, 108189. [CrossRef]
- Ghorbanpour Arani, A.; Miralaei, N.; Farazin, A.; Mohammadimehr, M. An Extensive Review of the Repair Behavior of Smart Self-Healing Polymer Matrix Composites. Journal of Materials Research 2023, 38, 617–632. [CrossRef]
- Scheiner, M.; Dickens, T.J.; Okoli, O. Progress towards Self-Healing Polymers for Composite Structural Applications. Polymer 2016, 83, 260–282. [CrossRef]
- Wang, J.; Tang, J.; Chen, D.; Xing, S.; Liu, X.; Hao, J. Intrinsic and Extrinsic Self-healing Fiber-reinforced Polymer Composites: A Review. Polymer Composites 2023, 44, 6304–6323. [CrossRef]
- Fifo, O.; Ryan, K.; Basu, B. Glass Fibre Polyester Composite with in Vivo Vascular Channel for Use in Self-Healing. Smart Mater. Struct. 2014, 23, 095017. [CrossRef]
- Jones, A.R.; Watkins, C.A.; White, S.R.; Sottos, N.R. Self-Healing Thermoplastic-Toughened Epoxy. Polymer 2015, 74, 254–261. [CrossRef]
- Radovic, I.; Stajcic, A.; Radisavljevic, A.; Veljkovic, F.; Cebela, M.; Mitic, V.V.; Radojevic, V. Solvent Effects on Structural Changes in Self-Healing Epoxy Composites. Materials Chemistry and Physics 2020, 256, 123761. [CrossRef]
- Wu, X.; Zhang, Y.; Chen, H.; Zhang, L.; Xie, G. Solvent Effect of Microcapsules Endows Self-Lubricating Polymer Composites with Wear in-Situ Self-Healing Function. Colloids and Surfaces A: Physicochemical and Engineering Aspects 2023, 676, 132158. [CrossRef]
- Icduygu, M.G.; Asilturk, M.; Altan, M.C. Microcapsules of Poly(Methyl Metharcylate) Containing Epoxy Resin and Multi-Walled Carbon Nanotubes.; Lyon, France, 2017; p. 030017.
- Caruso, M.M.; Schelkopf, S.R.; Jackson, A.C.; Landry, A.M.; Braun, P.V.; Moore, J.S. Microcapsules Containing Suspensions of Carbon Nanotubes. J. Mater. Chem. 2009, 19, 6093. [CrossRef]
- Hu, H.; Zhang, L.; Yu, R.; Yuan, L.; Yang, Y.; He, X.; Wang, J.; Li, Z. Microencapsulation of Ethylenediamine and Its Application in Binary Self-Healing System Using Dual-Microcapsule. Materials & Design 2020, 189, 108535. [CrossRef]
- Zhang, C.Y.; Jiang, X.B.; Rong, M.Z.; Zhang, M.Q. Free Radical Polymerization Aided Self-Healing. Journal of Intelligent Material Systems and Structures 2014, 25, 31–39. [CrossRef]
- Zamal, H.H.; Barba, D.; Aïssa, B.; Haddad, E.; Rosei, F. Failure Analysis of Self-Healing Epoxy Resins Using Microencapsulated 5E2N and Carbon Nanotubes. Smart Mater. Struct. 2021, 30, 025011. [CrossRef]
- Rodriguez, R.; Bekas, D.G.; Flórez, S.; Kosarli, M.; Paipetis, A.S. Development of Self-Contained Microcapsules for Optimised Catalyst Position in Self-Healing Materials. Polymer 2020, 187, 122084. [CrossRef]
- Jones, A.R.; Cintora, A.; White, S.R.; Sottos, N.R. Autonomic Healing of Carbon Fiber/Epoxy Interfaces. ACS Appl. Mater. Interfaces 2014, 6, 6033–6039. [CrossRef]
- Yuan, W.; Zhang, Z.; Li, Y.; Huang, Y.; Zhong, Z.; Hu, Z. Self-Healing and in-Situ Real-Time Damage-Reporting Fiber-Reinforced Composite. Composites Science and Technology 2024, 245, 110344. [CrossRef]
- Wang, R.; Hu, H.; Liu, W.; He, X.; Guo, Q. The Effect of Synthesis Condition on Physical Properties of Epoxy-containing Microcapsules. J of Applied Polymer Sci 2012, 124, 1866–1879. [CrossRef]
- Adli, A.; Shelesh-Nezhad, K.; Khoshravan Azar, M.; Mohammadi-Aghdam, M. The Effect of Vascular Self-Healing Pattern on Mechanical Behaviour and Healing Performance of Epoxy/Glass Composite. Plastics, Rubber and Composites 2020, 49, 79–90. [CrossRef]
- Kling, S.; Czigány, T. Damage Detection and Self-Repair in Hollow Glass Fiber Fabric-Reinforced Epoxy Composites via Fiber Filling. Composites Science and Technology 2014, 99, 82–88. [CrossRef]
- Sadeghi, S.A.M.; Borhani, S.; Zadhoush, A.; Dinari, M. Self-healing Performance of Hybrid Core-shell Nanofibers Mat Containing Epoxy-mercaptan at Subroom Temperature. Polymer Composites 2021, 42, 2422–2431. [CrossRef]
- Zhu, Y.; Ye, X.J.; Rong, M.Z.; Zhang, M.Q. Self-Healing Glass Fiber/Epoxy Composites with Polypropylene Tubes Containing Self-Pressurized Epoxy and Mercaptan Healing Agents. Composites Science and Technology 2016, 135, 146–152. [CrossRef]
- Mohammadi, M.A.; Eslami-Farsani, R.; Ebrahimnezhad-Khaljiri, H. Experimental Investigation of the Healing Properties of the Microvascular Channels-Based Self-Healing Glass Fibers/Epoxy Composites Containing the Three-Part Healant. Polymer Testing 2020, 91, 106862. [CrossRef]
- Patrick, J.F.; Hart, K.R.; Krull, B.P.; Diesendruck, C.E.; Moore, J.S.; White, S.R.; Sottos, N.R. Continuous Self-Healing Life Cycle in Vascularized Structural Composites. Advanced Materials 2014, 26, 4302–4308. [CrossRef]
- Eslami-Farsani, R.; Khalili, S.M.R.; Khademoltoliati, A.; Saeedi, A. Tensile and Creep Behavior of Microvascular Based Self-Healing Composites: Experimental Study. Mechanics of Advanced Materials and Structures 2021, 28, 384–390. [CrossRef]
- Amano, R.S.; Lewinski, G.; Shen, R. Imprinted Glass Fiber-Reinforced Polymer Vascular Networks for Creating Self-Healing Wind Turbine Blades. Journal of Energy Resources Technology 2022, 144, 062107. [CrossRef]
- Lee, M.W. Prospects and Future Directions of Self-Healing Fiber-Reinforced Composite Materials. Polymers 2020, 12, 379. [CrossRef]
- Meure, S.; Wu, D.Y.; Furman, S. Polyethylene-Co-Methacrylic Acid Healing Agents for Mendable Epoxy Resins. Acta Materialia 2009, 57, 4312–4320. [CrossRef]
- Ladani, R.B.; Pingkarawat, K.; Nguyen, A.T.T.; Wang, C.H.; Mouritz, A.P. Delamination Toughening and Healing Performance of Woven Composites with Hybrid Z-Fibre Reinforcement. Composites Part A: Applied Science and Manufacturing 2018, 110, 258–267. [CrossRef]
- Peñas-Caballero, M.; Chemello, E.; Grande, A.M.; Hernández Santana, M.; Verdejo, R.; Lopez-Manchado, M.A. Poly(Methyl Methacrylate) as Healing Agent for Carbon Fibre Reinforced Epoxy Composites. Polymers 2023, 15, 1114. [CrossRef]
- Azevedo Do Nascimento, A.; Fernandez, F.; S. Da Silva, F.; P.C. Ferreira, E.; D. Melo, J.D.; Cysne Barbosa, A.P. Addition of Poly (Ethylene-Co-Methacrylic Acid) (EMAA) as Self-Healing Agent to Carbon-Epoxy Composites. Composites Part A: Applied Science and Manufacturing 2020, 137, 106016. [CrossRef]
- Chen, B.; Cai, H.; Mao, C.; Gan, Y.; Wei, Y. Toughening and Rapid Self-healing for Carbon Fiber/Epoxy Composites Based on Electrospinning Thermoplastic Polyamide Nanofiber. Polymer Composites 2022, 43, 3124–3135. [CrossRef]
- Ladani, R.B.; Nguyen, A.T.T.; Wang, C.H.; Mouritz, A.P. Mode II Interlaminar Delamination Resistance and Healing Performance of 3D Composites with Hybrid Z-Fibre Reinforcement. Composites Part A: Applied Science and Manufacturing 2019, 120, 21–32. [CrossRef]
- Chang, K.M.; Sottos, N.R. Self-Healing of Transverse Crack Damage in Carbon Fiber Composites. Composites Science and Technology 2023, 242, 110158. [CrossRef]
- European Space Agency Develops Self-Healing Materials. Assembly Automation 2006, 26. [CrossRef]
- Everitt, D.T.; Luterbacher, R.; Coope, T.S.; Trask, R.S.; Wass, D.F.; Bond, I.P. Optimisation of Epoxy Blends for Use in Extrinsic Self-Healing Fibre-Reinforced Composites. Polymer 2015, 69, 283–292. [CrossRef]
- Feng, H.; Yu, F.; Zhou, Y.; Li, M.; Xiao, L.; Ao, Y. Fabrication of Microcapsule-Type Composites with the Capability of Underwater Self-Healing and Damage Visualization. RSC Adv. 2020, 10, 33675–33682. [CrossRef]
Figure 2.
Healing process using repair agents stored in reservoirs, in this example capsules: (a) Fracture formation; (b) Release of repair agents contained in the reservoirs; (c) Reparation of the matrix. Adapted from " Progress and challenges in self-healing composite materials" by Shafiqul Islam and Gajanan Bhat, used under CC BY 3.0. [https://doi.org/10.1039/D0MA00873G] [1].
Figure 2.
Healing process using repair agents stored in reservoirs, in this example capsules: (a) Fracture formation; (b) Release of repair agents contained in the reservoirs; (c) Reparation of the matrix. Adapted from " Progress and challenges in self-healing composite materials" by Shafiqul Islam and Gajanan Bhat, used under CC BY 3.0. [https://doi.org/10.1039/D0MA00873G] [1].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



