Submitted:
10 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Background:Patients with chronic kidney disease (CKD), especially those undergoing dialysis, encounter complex nutritional challenges. Key dietary factors such as protein and fluid intake, potassium and sodium levels, and co-morbidities significantly influence dietary planning for CKD patients. A standardized approach to dietary recommendations for CKD patients is ineffective due to the diverse needs of individual patients. Social media platforms have become a popular source of dietary information, often advocating low-carb, high-protein diets, and other combinations purported to be universally beneficial. However, these generalized online dietary recommendations lack the individualized approach necessary for CKD patients. Unlike these social media-driven suggestions, established medical guidelines offer a more nuanced view of CKD dietary needs. This study investigates the discrepancies between these sources and their potential impact on patient health. Objective:The primary goal of this study is to identify and analyze the flaws in the dietary recommendation system for CKD patients that might adversely affect their health. By critically evaluating the content of YouTube videos, we aim to compare the dietary advice provided by social media influencers and content creators with established medical guidelines. Our approach combines qualitative and quantitative methods to thoroughly assess the accuracy and reliability of online dietary advice available to CKD patients. Method:We conducted four YouTube searches using keywords related to "diet plan" and "chronic kidney disease (CKD)." From each search, the first 30 videos were selected based on relevance, resulting in an initial pool of 120 videos. A stepwise screening process was used to filter out the most relevant and accessible content, ultimately narrowing the sample to 30 videos for in-depth analysis. The videos were evaluated using two scoring systems: the Journal of the American Medical Association (JAMA) score and the Global Quality Scale (GQS) score, which assess video quality. To ensure impartiality, three independent scorers conducted the evaluations. Additionally, two six-point scorecards were used to evaluate the inclusion and accuracy of information on various foods and eating behaviors affecting CKD risk, with higher scores indicating more comprehensive coverage. Data on video characteristics, such as view count, number of likes, and video age, were also collected to provide context and further insight into their reach and influence. Results:The study included 30 videos, with 60% (18 out of 30) posted by or featuring nephrology health professionals. Scorer 1 reported a mean JAMA score of 2.3 (SD 0.61) out of 4 points and a mean GQS score of 2.5 (SD 0.64) out of 5 points. Scorer 2 found a mean JAMA score of 2.5 (SD 0.62) and a mean GQS score of 2.8 (SD 0.73). Scorer 3 reported a mean JAMA score of 2.6 (SD 0.55) and a mean GQS score of 2.8 (SD 0.69). The dietary six-point scorecards revealed a mean score of 3.6 (SD 0.85) for the presence of information and 2.8 (SD 0.88) for the accuracy of the information. Conclusion:The videos analyzed in this study related to diet plans for CKD patients demonstrated generally low scores, indicating a lack of comprehensive and accurate information. Many videos provided incomplete or partial information, which could mislead viewers and potentially cause harm due to incomplete knowledge. This study highlights the need for careful scrutiny of online content, particularly on platforms like YouTube, due to the potential for contradictory information and its harmful consequences. The findings emphasize the necessity for greater accuracy and vigilance in disseminating health-related information to ensure the safety and well-being of CKD patients.
Keywords:
CKD
; Chronic Kidney Dieases
; Dietary Recommendations on Social Media
1. Introduction
Chronic kidney disease (CKD) has become a worldwide epidemic with an occurrence rate in the population of approximately 5%–15% (Nicola., Zoccali, 2016). Prevalence of end-stage renal disease (ESRD) population relying on dialysis is also on the rise (USRDS Annual Data Report, 2015). Suboptimal nutritional intake is common in the population of CKD and ESRD and poses a direct risk for protein malnutrition. (Iguacel, 2013)
A constant debate surrounding the effects of nutritional interventions on kidney function has been ongoing for decades. Social media platforms like Youtube and Instagram are currently playing a vital role in shaping the food choices of every human being.
For example, various influencers and bloggers were seen to suggest a high protein diet to kidney patients to cope up with the Protein Energy Wasting that is common in dialysis patients. However, counteracting the same scientific evidences and studies suggest that excessive protein intake can have detrimental consequences for kidney health.(GJ et.al, 2020). Various studies and experiments conducted have shown that excess protein intake can lead to glomerular hyperfiltration, which in turn is associated with increased intraglomerular pressure and leads to potential kidney damage.(Bilancio et.al, 2019). However, there is no consensus on whether high protein intake has detrimental effects on kidney function in healthy individuals, as some studies suggest that hyperfiltration is a normal adaptive mechanism in response to physiological condition. (Knight, 2003)
This review paper aims to critically evaluate and draw a comparative analysis on the dietary recommendations given on social media with respect to the clinically proven ones.
In the context of CKD, protein restriction, low potassium and low sodium diet, minimal fluid intake is recommended as a treatment modality, and guidelines exist for supporting these nutritional considerations for individuals with chronic renal disease (GJ et.al, 2020)
The National Kidney Foundation (NKF) has extensive recommendations regarding nutritional guidelines for patients with CKD, emphasizing the importance of maintaining a balanced and individualized dietary approach to ensure adequate nutrition and energy intake while avoiding protein-energy wasting (GJ et.al, 2020)
In conclusion, while high protein diets and various other modifications may be beneficial for some individuals, such as those with hypertension, additional research is warranted to better understand the long-term effects of restricted diets on kidney health, particularly in the context of CKD or individuals at risk of CKD.(Friedman et.al, 2012)
The internet, particularly social media platforms like YouTube and Instagram, can be a source of both support and confusion for patients with chronic kidney disease (CKD) undergoing dialysis. One prevalent narrative suggests high-protein diets as the answer to protein-energy wasting (PEW), a common challenge for this population. However, this advice contradicts established medical guidelines, leaving patients, caregivers, and even healthcare professionals grappling with a nutritional dilemma.
However, despite the popularity of web-based information, there are concerns with accessing these sources, including the presence of misinformation and potential harms of making decisions based on unsubstantiated claims. (Tonsaker, et.al 2014)
YouTube is one source of web-based information that deserves attention. It is a video sharing platform founded in 2005 and is the second most highly trafficked website globally, with 34.6 billion visits each month(Neufeld, 2021). In 2020, there were 2.3 billion users of YouTube globally, and this has steadily increased over the last several years. (Iqbal, 2022). The content uploaded to YouTube is extensive. For example, for every minute as of February 2020, a total of 500 hours of video content was uploaded (Ceci, 2020). There are many reasons why people use YouTube, including to learn new things, problem-solving, entertainment, self-care (eg, destress and relaxation), and to improve skills. In a 2019 report, approximately 70% of YouTube users reported that this platform is the first website they go to when trying to learn (Berkowitz et.al, 2019). YouTube can also be easily accessed through different devices, including computers, tablets, and mobile phones. Substantial interest has been generated around the use of YouTube for health-related purposes. To date, a few studies have shown that YouTube videos can be beneficial for improving health-related knowledge, attitudes, and behaviors (Haslam et.al, 2019). However, despite the popularity of this platform and the interest in its use for health-related purposes, the content of YouTube videos is not reviewed to ensure accuracy and comprehensiveness.
To date, several studies have been conducted on the content of health information available on YouTube. These studies have been summarized in different review articles(Haslam et.al, 2019). These articles have reported that, in general, videos do not comprehensively cover various health topics and that the content quality of videos varies widely, with many studies reporting a high prevalence of poor-quality videos or nonuseful videos and a low prevalence of good-quality videos. However, some high-quality videos are available in some topic areas(Warren et.al, 2021). In addition, many studies have found either no relationship between video quality and engagement (eg, views and likes) or a negative relationship (ie, as quality decreases, engagement increases)(Osman et.al, 2022). These articles have also found that videos tend to be of higher quality when they feature health professionals (eg, physicians) or health organizations(Warren et.al, 2021). Owing to the high prevalence of chronic kidney disease worldwide, the strong relationship that diet has with chronic kidney disease, and the popularity of YouTube, information on this topic is needed. Hence, this review dives deep into the complex considerations surrounding nutritional intake for dialysis patients, offering evidence-based insights to navigate this maze.
The purpose of this study was to analyze the content of YouTube videos regarding diet plans suggested for dialysis patients that are easily accessible using default search settings and popularity.
2. Review of Literature
2.1. What Is Chronic Kidney Disease?
Chronic kidney disease (CKD) is the gradual loss of renal function over a period of months or years and is classified into five stages based on the measurement of estimated glomerular filtration rate (eGFR) (Levey, Coresh, 2012)
End stage renal disease (ESRD), or CKD stage 5, represents the most severe form of renal function, is characterized by an eGFR of < 15 mL/min per 1.73 m2 and requires maintenance dialysis or renal transplantation. (National Institute for Health and Care Excellence, 2014)
2.2. What Is Dialysis?
The term dialysis is derived from the Greek words dia, meaning "through," and lysis, meaning "loosening or splitting." It is a form of renal replacement therapy, where the kidney's role of filtration of the blood is supplemented by artificial equipment, which removes excess water, solutes, and toxins. Dialysis ensures the maintenance of homeostasis (a stable internal environment) in people experiencing a rapid loss of kidney function, i.e., acute kidney injury (AKI) or a prolonged, gradual loss that is chronic kidney disease (CKD). It is a measure to tide over acute kidney injury, buy time until a kidney transplant can be carried out, or sustain those ineligible for it. (Murdeshwar, Anjum, 2023)
2.3. What Are the Various Modalities of Dialysis?
There are three broad types of dialysis: Hemodialysis is a therapeutic procedure that uses the extracorporeal circulation of a patient's blood to ameliorate the azotemia, fluid, electrolyte, and acid-base abnormalities characteristic of the uremic syndrome. (Elliott, 2000). Peritoneal dialysis (PD) is a renal replacement therapy based on infusing a sterile solution into the peritoneal cavity through a catheter and provides for the removal of solutes and water using the peritoneal membrane as the exchange surface. (Andreoli, Totoli, 2020)
Continuous renal replacement therapy is a treatment option that is especially suited to the critical care setting. Greater hemodynamic stability, the ongoing ability to optimize fluid balance, and the potential for clearing inflammatory mediators are among the frequently cited advantages continuous veno-venous dialysis modalities offer over traditional intermittent therapies. The concept is simple: blood is pumped from the patient, anticoagulated, and passed through a porous filter where, depending on the desired goal, fluid and/or solutes are removed. The blood is then returned to the patient, without large fluctuations in electrolyte and acid-base balance or renal hypoperfusion. (Hynes, Rankin, 2000)
2.4. What is Protein Energy Wasting (PEW)?
The term PEW was proposed by the “International Society of Renal Nutrition and Metabolism” (ISRNM) (www.RenalNutrition.org) and defined in 2008 as metabolic and nutritional derangements characterised by decreased body stores of protein and energy (body protein and fat masses) (Fouque et.al, 2008). The diagnosis was further characterised in adults to include in addition low serum albumin, low cholesterol and decreased protein intake (Kovesdy, Kalantar, 2009)
Cachexia is a term used as an alternative to PEW. The ISRNM has suggested that cachexia should be reserved for severe PEW. However, definitions are similar, the main difference being that a loss of body weight > 5% is a mandatory criterion for cachexia but supportive for PEW (Rees, Mak,2011)
2.5. Nutritional Considerations of CKD
A CKD diet is tailored to the specific needs of each patient, with protein being a key factor. Those not on dialysis require a low protein intake, while those on dialysis may actually need more protein to compensate for losses. The amount of protein is further determined by creatinine levels, with higher levels indicating a need for stricter protein restriction. Doctors use guidelines like ESPN/ASPEN to determine protein intake, typically starting at 1-1.2 grams per kilogram of body weight. Other important considerations include potassium and sodium restriction, managing diabetes with a low sugar approach, and factoring in any existing health conditions. Interestingly, BMI isn't a direct factor, but ideal body weight (IBW) based on height might be used as a reference for protein intake calculations.
Dietary proteins are digested to amino acids which can be further broken down to generate both acids and bases. Proteins from meat and dairy products (from a typical Western diet) generate predominantly acidic products including hydrogen chloride (HCl), sulfuric acid (H2SO4) and phosphoric acids (H3PO4). These acids are nonvolatile and rely on kidney for their excretion (primarily in the form of ammonium salts and phosphoric salts) (Zha, Qian, 2017). A healthy individual generates net acids, approximately 1 mEq/kg/day (mmol/kg/day), referred to as NEAP (net endogenous acid production). These are rapidly buffered by sodium bicarbonate (NaHCO3) to form sodium salts. During this process, bicarbonate is consumed, which needs to be regenerated, a task accomplished by the kidneys. To achieve a steady acid–base balance, renal tubules must reabsorb ~4500 mEq of filtered HCO3− and generate (through H+ excretion) an additional ~70–80 mEq HCO3− daily, to neutralize the daily net acid generation. (Koeppen, 2009).
2.6. Metabolic and Regulatory Derangements in CKD and ESRD
As shown in Figure 1, kidney dysfunction is associated with defects in acid excretion, systemic inflammation, end-organ hormone resistance and uremic toxin accumulation. These abnormalities can further worsen kidney function, creating a vicious circle, adversely affect patients’ outcome.
2.7. Effect of Social Media on Nutrition
Social media (SM) is defined as forms of electronic communication that allows users to create virtual communities to share information, ideas, messages, and other content such as pictures and videos (“Social Media”, n.d.). Built on collaborative platforms, SM allows and encourages individuals, communities, or organizations to share, co-create, discuss, and participate by posting information online. Some popular SM platforms include Facebook, Twitter, YouTube, Instagram, Snapchat, and TikTok. SM is commonly used to maintain and develop relationships with friends, communicate and interact with others, and seek out information and entertainment (Greenwood et al., 2016).
Over the past decade, the use of SM worldwide has tripled from 0.97 billion people to 2.96 billion people (Brown, 2019), with a significant majority (92.9%) of adolescents using at least one or more SM accounts (Barry et a., 2017). TikTok, a relatively new SM platform, hit worldwide markets in 2016 and recent reports indicate that nearly one-third of users are under the age of 14 (TikTok statistics, 2021 , April 26; Zhong et.al, 2020). Additionally, Instagram which launched back in 2010 is seeing significant growth among age demographics and currently reports 107 million U.S. users, with approximately 4.8 million (4.5%) being adolescents aged 13–17 (Tankovska, 2021). In addition to the growth in users, on average, these adolescents typically check their SM accounts five times a day (Barry et al., 2017) making it a main source for communicating with friends and family as well as a venue for viewing entertainment and information (Keeffe et al., 2011).
People are increasingly using the Internet to access health information (Martin, 2004). And it is quite convenient for people to obtain a wide array of health information. YouTube (http://www.youtube.com) represents one of the most popular social network sites for sharing video content behind Google (Alexa. Top 500 global sites). YouTube was increasingly being used for health information (Madathil et.al, 2005) , and it has a large community user base that allows users to view, upload, and download at free cost, and also communicate and comment easily between the sources of upload and other viewers (Madathil et.al, 2005). However, using the Internet for health and medical information has a variety of disadvantages, including disorganization, complex medical language and lack of peer review (Cline, 2001). Therefore it is essential to assess the quality of the information delivered (Keelan et.al, 2007). To our knowledge, no prior studies have examined the availability of food poisoning education videos on YouTube. Therefore, this study aims to systematically assess the usefulness of YouTube videos regarding food poisoning for improving the professionalism of video websites.
3. Methodology:
3.1. Video Selection:
Our strategy was to search for YouTube videos that would be most accessible to the public searching for educational content regarding diet plan and chronic kidney disease. Google Keyword Planner was used to select 2 chronic kidney disease–related keywords and 3 nutrition and die plan-related keywords. For chronic kidney disease, the top 2 key words associated with this concern were kidney dialysis and ckd. For diet, the top 3 key words associated were dieting, diet plans, food. This resulted in a total of 4 searches dialysis diet plan, diet plan for dialysis, ckd diet plan, diet plan for kidney patients. Video eligbility were determined by screening through various factors.
- At first, the videos were sorted as per the view count to take engagement in count.
- Videos in Hindi and English were considered as both are the majorly spoken ones in India.
- Videos with a duration of less than 20 minutes were chosen, as a 2018 study also found that 90% of respondents preferred instructional and informational videos to be <20 minutes. (TechSmith, 2018)
- Duplicate videos were removed from the list.
- Sponsored content and Advertisement were removed.
- Irrelevant content having no information about the daily diet plan suggestions for Chronic Kidney Disease patients were not included in the analysis.
The YouTube searches were conducted between April 01, 2024 to April 13,2024, using the “Relevance” filters on YouTube to best replicate the search strategy used by the public. This helped us to align the videos as per their view counts which depicts their reach.
The searches were conducted using Google Chrome’s Incognito mode to prevent bias when conducting the searches. A new incognito window was opened to complete each search.
Each of the 4 YouTube searches were completed in a sequence, and the first 30 videos were recorded from each search. The first 30 videos were chosen and an eligibility screening was done. For each eligible video, the keyword used for search, the video url, the information giver, the view count, the like count, the date of posting the topics of discussion were noted down in Microsoft Excel 365.
Initially, 120 videos were screened after searching for specific terms: "Dialysis Diet Plan" (30 videos), "Diet Plan for Dialysis Patient" (30 videos), "CKD Diet Plan" (30 videos), and "diet plan for kidney patients" (30 videos). After eligibility screening, the total number of selected videos was reduced to 30, distributed as follows: 4 for "Dialysis Diet Plan", 7 for "Diet Plan for Dialysis Patient", 8 for "CKD Diet Plan", and 11 for "diet plan for kidney patients". These 30 videos were ultimately included in the analysis. The flowchart also details reasons for exclusion, categorizing them as Sponsored Content (17 videos), Irrelevant content (32 videos), Non-english/Non-hindi content (19 videos), and Duplicate Content (22 videos). This systematic approach ensures a comprehensive and relevant selection of videos for analysis in the study of diet plans for dialysis and kidney patients. The details of the screening is given below in Figure 2.
3.2. Video Scoring System:
3.2.1. Video Quality Evaluation:
The Journal of American Medical Association (JAMA) benchmark criteria (score range, 0-4) (given below as Table 1) was used to assess video accuracy and reliability. The Journal of American Medical Association (JAMA) benchmark criteria was used to evaluate the basic quality and reliability of the videos. The criteria consists of a 4-item (authorship, attribution, disclosure and currency) rating scale. By assigning 1 point for the presence of each criterion, the total JAMA benchmark score was calculated (Zhang et.al, 2020)
The Global Quality Score (GQS; score range, 0-5) (given below as Table 2) was used to assess the quality of the video's content. The Global Quality Scale (GQS) was used to assess the overall quality of all selected videos. As shown below, GQS was a five-point Likert scale based on the quality of information, the flow and ease of use of the information present online.(Li, et.al 2019)
3.2.2. Video Content Scoring
The methodology employed for video content scoring, which involved the utilization of two distinct scorecards.
Scorecard 1: Presence of Crucial Dietary Information (given below as Table 3): The scorecard developed for this study, with a scoring range of 0-6, was meticulously designed to assess the adequacy of essential dietary information related to dialysis presented in YouTube videos. The creation of this scorecard was rooted in the fundamental standards of a dialysis diet, ensuring that all critical areas relevant to this specific topic were comprehensively addressed. The scorecard aimed to measure how well the videos covered vital dietary guidelines necessary for dialysis patients, including but not limited to, protein intake, fluid restrictions, sodium, potassium, and phosphorus management.
Each criterion within the scorecard was chosen based on its significance to the overall health and well-being of dialysis patients, reflecting expert recommendations and clinical guidelines. By systematically evaluating these key areas, the scorecard provides a structured approach to identify whether the videos offer reliable and thorough dietary advice that patients can follow. This structured evaluation ensures that content creators are held to high standards of accuracy and completeness, promoting the dissemination of useful and scientifically-backed information.
The development of this scorecard highlights our commitment to improving the quality of online health information, specifically tailored to the needs of dialysis patients. It serves as a valuable tool for both researchers and viewers, helping to distinguish high-quality educational content from those lacking in essential dietary guidance. This approach not only aids in better health management for patients but also underscores the importance of rigorous standards in the creation of health-related content on public platforms.

Table 3.
Scorecard for checking if related information was passed.
| Scorecard for checking if related information was passed | Questions | Weightage |
| Was potassium intake level informed? | 1 | |
| Was sodium intake level informed? | 1 | |
| Was phosphorous intake level informed? | 1 | |
| Was health condition-wise/co-morbidity customization of diet informed? | 1 | |
| Was protein intake levels informed? | 1 | |
| Was IBW based dietary recommendations informed? | 1 |
Scorecard 2: Correctness and Relevance of Information (given below as Table 4): The second scorecard, encompassing a range from -1 to +1 (Negative-Neutral-Positive), was specifically designed to evaluate the accuracy and relevance of the dietary information presented in YouTube videos concerning dialysis diets. This scorecard, like the first, was formulated based on the fundamental standards of a dialysis diet, ensuring that all crucial aspects of dietary management for dialysis patients were accurately and appropriately conveyed.
This scoring system serves a dual purpose. Firstly, it assesses whether the information presented is factually correct and aligns with established dietary guidelines for dialysis patients. A positive score (+1) indicates that the information is accurate and relevant, a neutral score (0) suggests that the information is neither significantly beneficial nor harmful, and a negative score (-1) highlights the presence of misinformation or irrelevance. This range allows for a nuanced evaluation of each video, distinguishing those that provide valuable, reliable advice from those that could potentially mislead or harm viewers.
The development of this scorecard was guided by the need to ensure that content creators adhere to the highest standards of accuracy in their presentations. It emphasizes the importance of conveying the critical elements of a dialysis diet accurately, such as correct protein intake, fluid restrictions, and the management of electrolytes like sodium, potassium, and phosphorus. By systematically assessing these factors, the scorecard provides a clear and objective measure of the video's informational quality.
4. Data Analysis
4.1. Video Quality Evaluation
Videos were scored using the JAMA and GQS scoring system independently by 3 individuals (Rater 1, Rater 2 and Rater 3) using information presented in either text listed in the video or what was said verbally. Discrepancies were discussed until a consensus was reached.
4.2. Video Content Analysis
The analysis of the content and information passed were done through the content scoring scorecards, using information presented in either text listed in the video or what was said verbally.
Information on video characteristics (ie, view count, number of likes, video age, viewing rate [views/day; calculated by taking the number of views and dividing by number of days since the video was uploaded] (Hassona et.al, 2019), and like rate [likes/view; calculated by taking the number of likes and dividing by the number of views were summarized using descriptive statistics (mean, SD, median, and range) determined using Microsoft Excel 365.
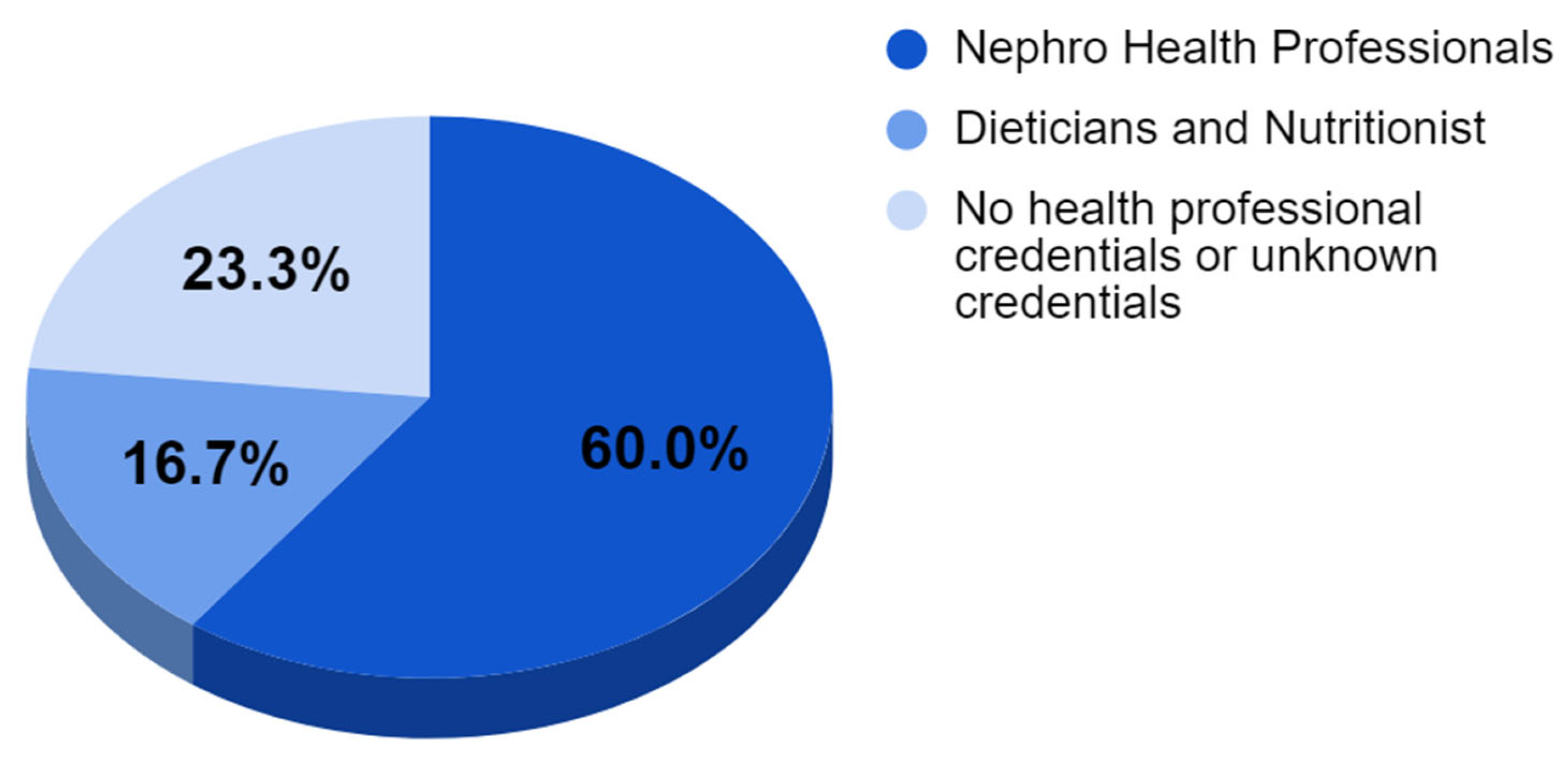
Each video was categorized into 1 of 3 groups based on the author or presenter featured in the video. The four groups were as follows: (1) Nephro Health Professionals; (2) Dieticians and Nutritionist; (3) No health professional credentials or unknown credentials.
Figure 3.
Pie Chart showing distribution of the information giver of the screened video.
Inferential statistics were determined using SPSS Statistics (version 28). Fisher exact test was used to determine whether there were significant differences between categorical scoring, and the Kruskal-Wallis test were used to determine whether there were significant differences between continuous variables. P values of <0.05 were considered significant. The inter-rater reliability was checked through Bland Altman Plots. Spearman correlations were used to examine the relationships between 2 continuous variables.
5. Results
5.1. Search Results:
In total, 30 videos from the 120 searches were considered for inclusion; 90 (75%) videos were removed from the analysis because they (1) were duplicate videos (n=14, 15.5%) or (2) did not meet inclusion criteria (n=32, 35.5%) ie, video did not mention anything related to diet and chronic kidney disease, and also the videos which were not in English or Hindi (n=19, 21.1%) . After these videos were removed, n=30 videos were eligible for analysis. A detailed analysis on the same is given below in Table 5.
5.2. Nutrition Messaging:
The 30 videos observed collectively had 7,211,123 views, with the mean number of views being 240,371. Of all videos observed, in 60% cases the information giver was a doctor/Nephro Health Professionals, for 16.7% of them the information giver was a dietician or nutritionist and 23.3% of them were posted by channels owned by unknown information giver without any proper content source. The mean JAMA score was 2.36 with the highest scores coming from doctors. The mean GQS score was calculated to be 2.56 with the highest scores coming from doctors.
The following tabular data presents the scoring results from multiple raters evaluating a series of videos. For analytical purposes, the videos were categorized based on the credentials of the information provider. Three distinct categories were established: videos presented by medical doctors, those presented by dieticians, and those presented by individuals without formal health professional qualifications. This categorization allows for a comparative analysis of the perceived quality and credibility of information across different levels of professional expertise in the health domain.
In the analysis conducted by Rater 1 (as given above on Table 6), the JAMA and GQS scores were evaluated across different categories of video presenters. For all 30 videos, the mean JAMA score was 2.3 (SD = 0.61, median = 2), while the mean GQS score was 2.5 (SD = 0.62, median = 2.5). When examining the 18 videos presented by Nephro Health Professionals, the mean JAMA score increased to 2.6 (SD = 0.60, median = 3), and the mean GQS score rose to 2.7 (SD = 0.64, median = 3). The 5 videos by Dieticians and Nutritionists showed a mean JAMA score of 2 (SD = 0, median = 2) and a mean GQS score of 2.6 (SD = 0.54, median = 3). Lastly, for the 7 videos with no health professional credentials or unknown credentials, both the mean JAMA and GQS scores were 2, with the JAMA score having a standard deviation of 0.577 and the GQS score showing no variation (SD = 0). Both categories had a median of 2 for both scoring systems. These results suggest variations in perceived quality and credibility across different presenter categories, with Nephro Health Professionals generally receiving higher scores.
The analysis conducted by Rater 2 (as given above on Table 7) revealed varying JAMA and GQS scores across different categories of video presenters. For the entire set of 30 videos, the mean JAMA score was 2.5 (SD = 0.62, median = 3), while the mean GQS score was slightly higher at 2.8 (SD = 0.73, median = 3). The subset of 18 videos presented by Nephro Health Professionals showed notably higher scores, with a mean JAMA score of 2.8 (SD = 0.38, median = 3) and a mean GQS score of 3.2 (SD = 0.64, median = 3). The 5 videos by Dieticians and Nutritionists received somewhat lower scores, with both JAMA and GQS means at 2.4 (SD = 0.54 for both, median = 2). The 7 videos with no health professional credentials or unknown credentials received the lowest scores, with a mean JAMA score of 1.7 (SD = 0.49, median = 2) and a slightly higher mean GQS score of 2.2 (SD = 0.48, median = 2). These results suggest a clear trend in perceived quality and credibility across presenter categories, with Nephro Health Professionals consistently receiving the highest scores, followed by Dieticians and Nutritionists, and then those without professional health credentials.
The analysis conducted by Rater 3 (as given above on Table 8) revealed varying JAMA and GQS scores across different categories of video presenters. For the entire set of 30 videos, the mean JAMA score was 2.6 (SD = 0.55, median = 3), while the mean GQS score was slightly higher at 2.8 (SD = 0.69, median = 3). The subset of 18 videos presented by Nephro Health Professionals showed notably higher scores, with a mean JAMA score of 2.8 (SD = 0.51, median = 3) and a mean GQS score of 3.0 (SD = 0.64, median = 3). The 5 videos by Dieticians and Nutritionists received somewhat lower scores, with a mean JAMA score of 2.4 (SD = 0.54, median = 2) and a higher mean GQS score of 2.8 (SD = 0.83, median = 3). The 7 videos with no health professional credentials or unknown credentials received the lowest scores, with both mean JAMA and GQS scores at 2.2 (SD = 0.48 for both, median = 2 for JAMA and 2 for GQS). These results indicate a clear trend in perceived quality and credibility across presenter categories, with Nephro Health Professionals consistently receiving the highest scores, followed by Dieticians and Nutritionists, and then those without professional health credentials. The data suggests that the professional background of the presenter significantly influences the perceived quality of the video content as assessed by the JAMA and GQS scoring systems.
The dietary scoring analysis across different categories of video presenters (as shown above on Table 9) revealed varying results for two separate scorecards. For Scorecard 1, considering all 30 videos, the mean score was 3.6 (SD = 0.85, median = 3.5). Nephro Health Professionals (n=18) received the highest mean score of 4.0 (SD = 0.72, median = 4), followed by Dieticians and Nutritionists (n=5) with a mean of 3.2 (SD = 0.44, median = 3), and lastly, those with no health professional credentials or unknown credentials (n=7) scoring a mean of 2.7 (SD = 0.48, median = 3). For Scorecard 2, the overall mean score for all videos was 2.8 (SD = 0.88, median = 3). Again, Nephro Health Professionals scored highest with a mean of 3.2 (SD = 0.75, median = 3), while Dieticians and Nutritionists scored a mean of 2.2 (SD = 0.83, median = 2), and those without professional health credentials or with unknown credentials scored a mean of 2 (SD = 0, median = 2). These results suggest a consistent trend across both scorecards, with Nephro Health Professionals consistently receiving the highest scores, followed by Dieticians and Nutritionists, and then those without professional health credentials, indicating that the professional background of the presenter significantly influences the perceived quality of dietary information in the videos.
6. Discussion
6.1. Principal Findings
The JAMA and GQS scoring systems were categorized into distinct classifications of "Good," "Average," and "Poor" to facilitate detailed statistical analysis and enhance the interpretability of the results. For the JAMA score, the ranges were defined as follows: a score of 0-1 was categorized as "Poor," a score of 2 as "Average," and scores ranging from 3-4 as "Good." Similarly, the GQS score ranges were set with scores of 0-1 classified as "Poor," scores of 2-3 as "Average," and scores of 4-5 as "Good."
This categorization allowed for a structured and comparative analysis of the videos based on their quality and reliability. By assigning specific ranges to these categories, we could systematically evaluate and compare the performance of the videos under study. This structured approach enabled us to identify patterns and trends in the data, such as the proportion of videos falling into each category and the factors contributing to these classifications.
The use of these predefined categories also facilitated a clearer understanding of the overall quality of the videos in relation to the standards set by the JAMA and GQS criteria. For instance, videos classified as "Good" according to the JAMA score demonstrated a high level of adherence to the standards of medical accuracy and reliability. In contrast, those rated as "Poor" indicated significant deficiencies in these areas. Similarly, the GQS score classification helped in assessing the overall quality and usefulness of the videos from the viewer's perspective.
This categorization not only streamlined the statistical analysis process but also provided a robust framework for discussing the implications of our findings. It highlighted the areas where the videos excelled or fell short, thereby offering valuable insights for future content creators and researchers aiming to improve the quality of online health information.
Our study provided insightful data regarding the performance scores of Doctors and Non-Doctors in the assessment of their knowledge and understanding of nutrition and diet for CKD patients. Among the Doctors (n=18, representing 60% of the total participants), the distribution of scores revealed that 44.4% (n=8) achieved an "Average" rating, while a notable 55.6% (n=10) attained a "Good" rating. Remarkably, none of the Doctors scored in the "Poor" category, indicating a relatively high baseline of knowledge and competence within this group.
In contrast, the Non-Doctors (n=12, accounting for 40% of the total participants) displayed a different pattern in their performance scores. A significant majority, 83.3% (n=10), scored "Average," suggesting a more moderate level of understanding in this cohort. Only 8.3% (n=1) of Non-Doctors achieved a "Good" rating, markedly lower compared to their Doctor counterparts. Additionally, 8.3% (n=1) of Non-Doctors scored "Poor," highlighting a critical area for improvement within this group.
From these findings, it can be concluded that Doctors are significantly more likely to score "Good" compared to Non-Doctors (55.6% vs. 8.3%, respectively). This disparity underscores the advanced knowledge base and possibly the more rigorous training and exposure that Doctors have concerning CKD nutrition and diet management. Conversely, Non-Doctors are more inclined to score "Average" (83.3% vs. 44.4% for Doctors), indicating a generally acceptable but less proficient level of understanding. The presence of a "Poor" score exclusively among the Non-Doctors (8.3%) further emphasizes the need for enhanced educational interventions targeting this group.
These results (given below in Table 10) suggest a clear division in the levels of expertise between Doctors and Non-Doctors, with Doctors demonstrating superior performance. This underscores the importance of targeted educational programs to elevate the knowledge base of Non-Doctors, ensuring a more uniformly high standard of care and information dissemination across all healthcare providers involved in the management of CKD.
The below Figure 4 gives a graphical representation of the above explained relation of the professional status and the content quality of the videos.
In our study, we sought to uncover the relationships between four key variables: the number of views, JAMA scores, GQS scores, and likes of the videos, employing Spearman's rank correlation coefficient for this analysis. Our findings revealed several noteworthy correlations.
Firstly, when comparing the number of views to JAMA scores, a moderate positive correlation was identified (ρ = 0.422, p = 0.020). This relationship was statistically significant at the 0.05 level, indicating that videos with higher view counts tend to have better JAMA scores. This suggests that videos perceived as more credible or higher in quality are viewed more frequently by the audience.
In contrast, the comparison between views and GQS scores yielded a weak positive correlation (ρ = 0.229, p = 0.223). This relationship was not statistically significant, indicating that the GQS scores do not strongly correlate with the number of views. This lack of significance suggests that GQS, which might measure a different dimension of video quality or user engagement, does not influence view counts in a meaningful way.
Additionally, when examining the relationship between GQS scores and likes, we found a moderate positive correlation (ρ = 0.345, p = 0.062). Although this relationship approached statistical significance, it did not meet the 0.05 threshold. This near-significance suggests a potential trend where higher GQS scores could be associated with more likes, but further investigation is required to confirm this pattern. The comparison between likes and JAMA scores revealed a strong positive correlation (ρ = 0.530, p = 0.003), which was statistically significant at the 0.01 level. This robust relationship indicates that videos with higher JAMA scores, reflecting higher quality and credibility, are also more likely to receive a greater number of likes. This finding suggests that likeability, as an engagement metric, aligns closely with the quality standards measured by JAMA. The strongest and most significant relationship was observed between likes and JAMA scores, suggesting that higher likeability is associated with better JAMA scores. The moderate correlation between views and JAMA scores indicates that higher view counts are associated with better JAMA scores, though to a lesser extent than likes. The weaker and non-significant correlations involving GQS scores suggest that GQS might be measuring a different aspect of performance or quality compared to the other metrics.
Comprehensively, these findings imply that engagement metrics such as views and likes have a positive relationship with JAMA scores, indicating that more engaging content tends to be of higher quality as measured by JAMA. However, it is important to note that causality cannot be inferred from these correlations alone. Further research would be necessary to explore the causal relationships and underlying factors influencing these associations.
The below matrix scatter plot (Figure 5) gives a vivid idea about the above mentioned correlation analysis done.
To mitigate potential individual rater bias, we employed a multi-rater approach wherein three independent evaluators assessed the same video content using identical scorecards. To quantify the overall concordance among these three raters and ensure alignment in their evaluative approaches, we conducted Bland-Altman analyses. This method allowed us to assess the degree of agreement between raters and verify that their interpretations of the scoring criteria were consistently applied across the sample. The Bland-Altman plots suggested that there is generally good agreement between all three raters for both JAMA and GQS scores. However, the agreement appeared to be stronger for JAMA scores compared to GQS scores, as evidenced by the tighter clustering of points around the mean difference line in the JAMA score plots. The wider spread of points in the GQS score plots indicates more variability in ratings between pairs of raters for this scoring system. This could suggest that the GQS scoring criteria may be more subjective or open to interpretation compared to the JAMA scoring criteria. Despite some variability, most data points fall within the limits of agreement for both scoring systems, indicating an acceptable level of agreement between raters overall.
Figure 6.
Bland Altman Plot for JAMA Scoring of Rater 1 vs Rater 2.
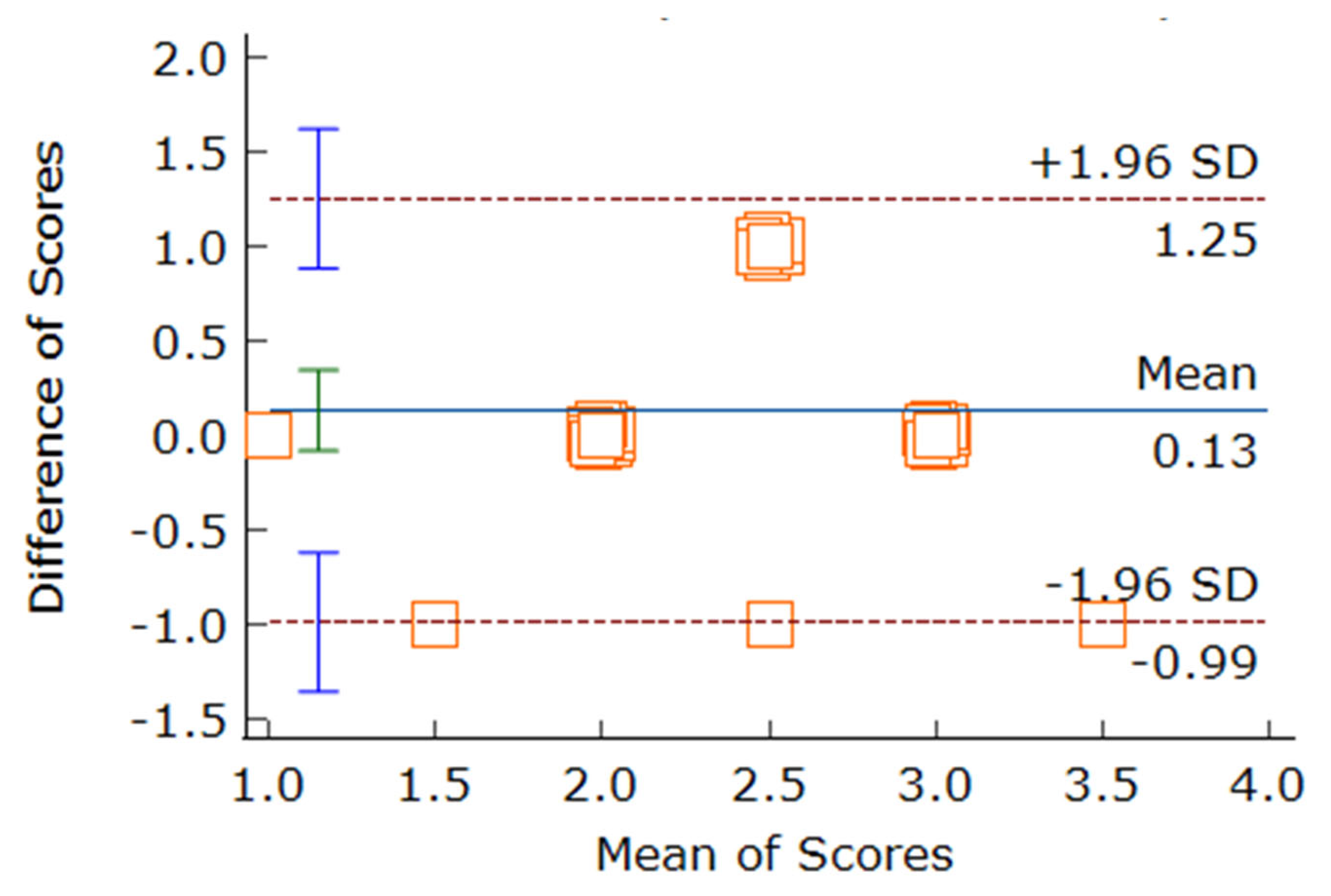
Figure 7.
Bland Altman Plot for GQS Scoring of Rater 1 vs Rater 2.
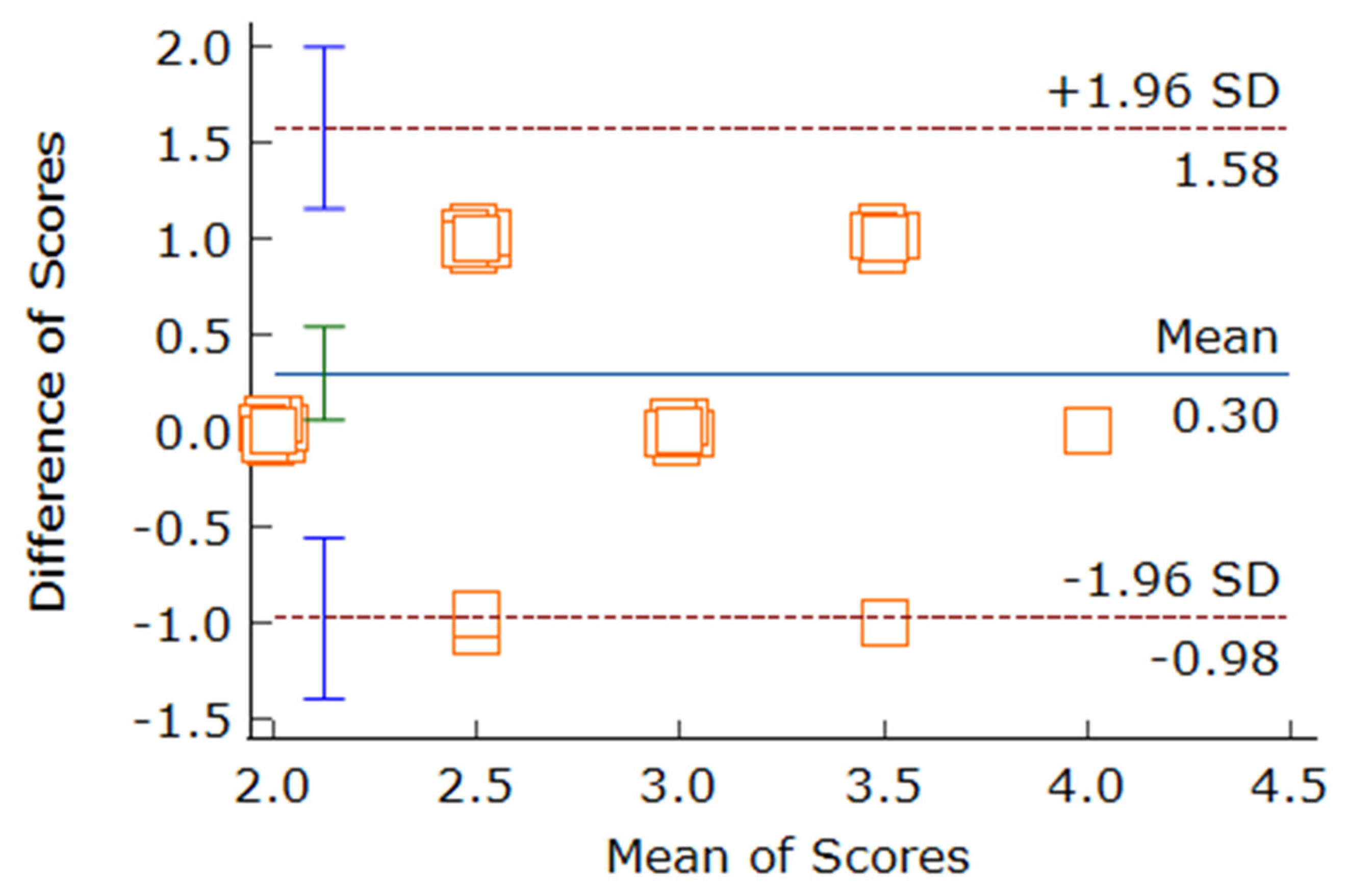
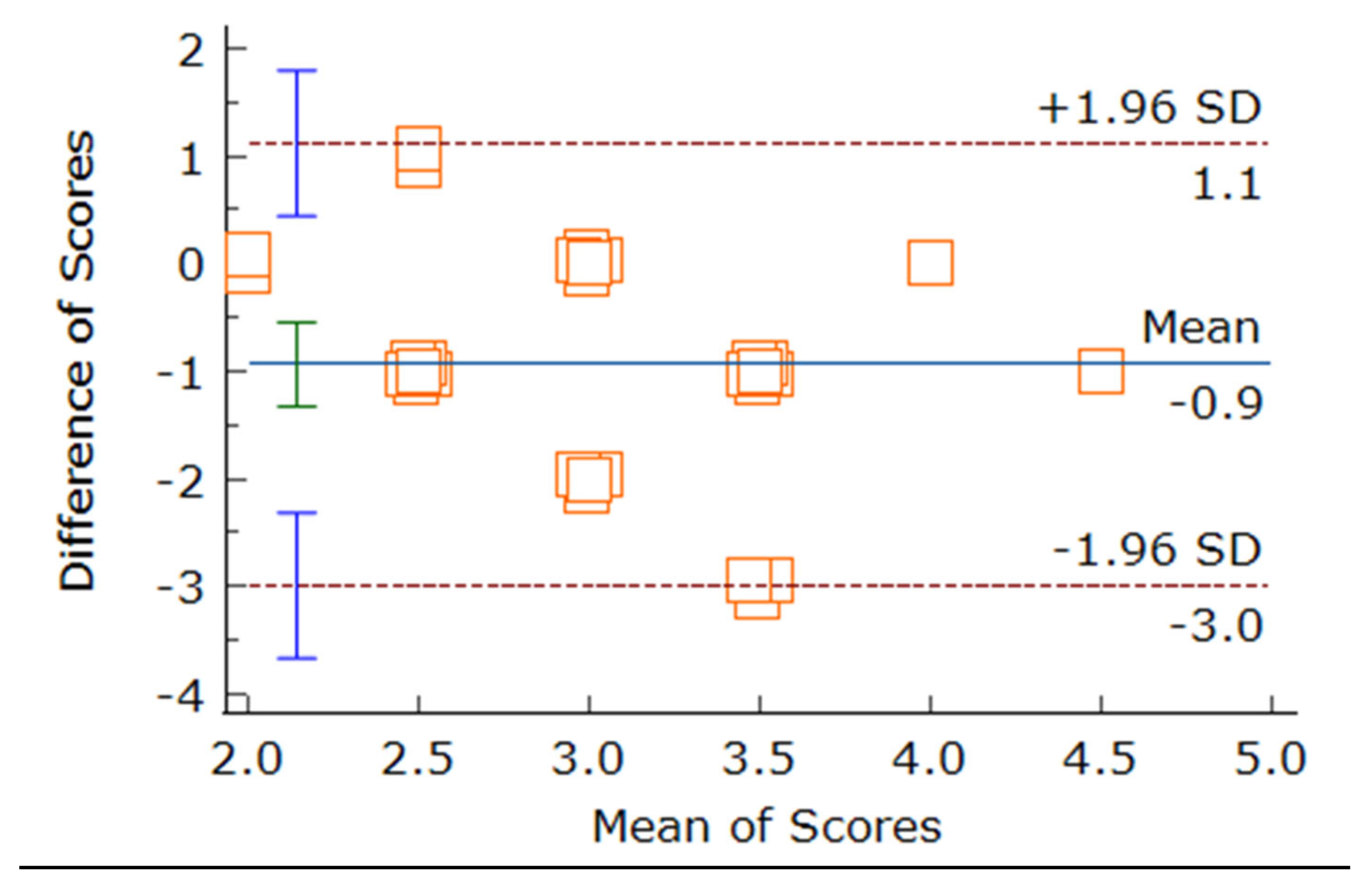
Figure 8.
Bland Altman Plot for JAMA Scoring of Rater 2 vs Rater 3.
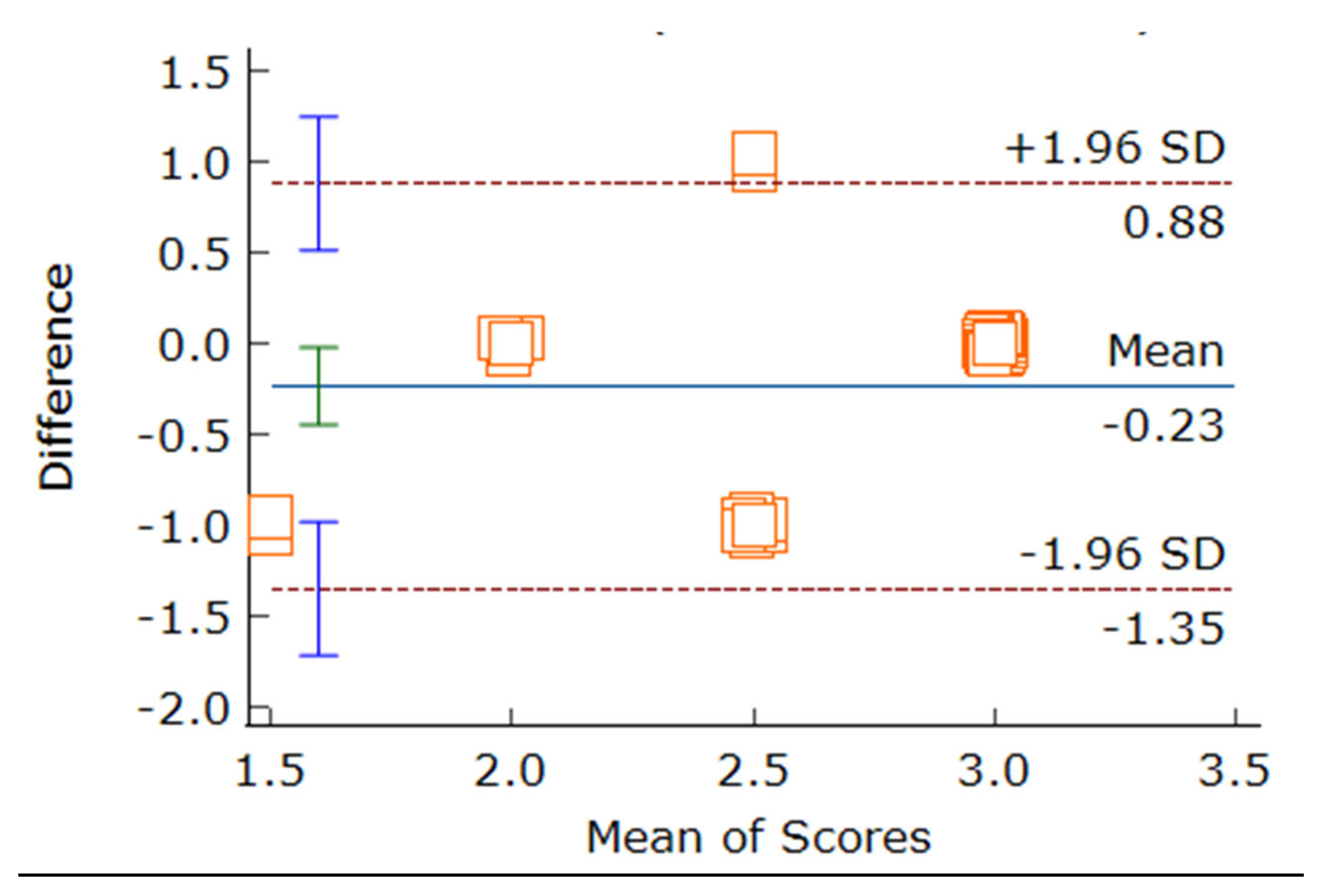
Figure 9.
Bland Altman Plot for GQS Scoring of Rater 2 vs Rater 3.
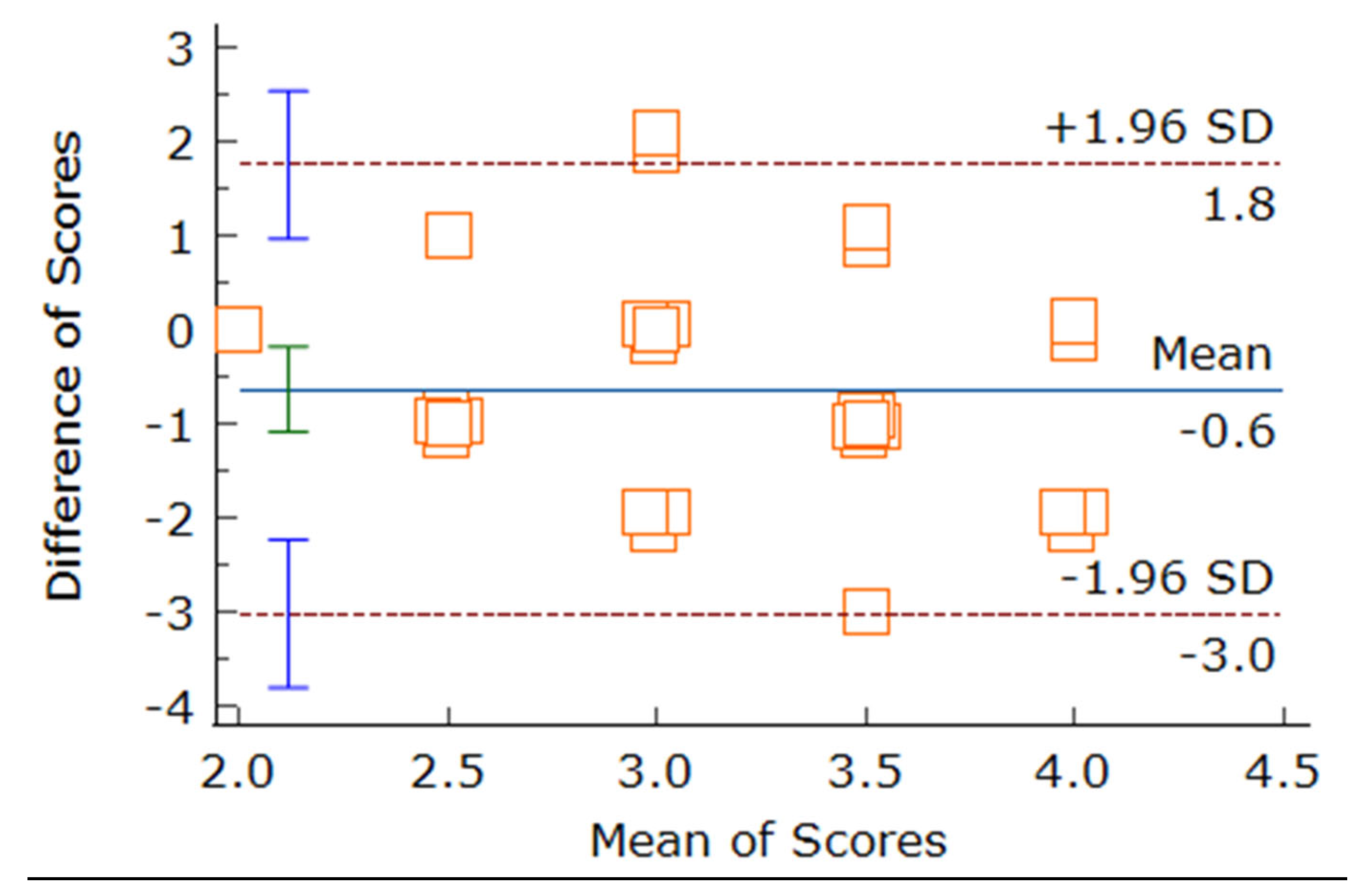
Figure 10.
Bland Altman Plot for JAMA Scoring of Rater 1 vs Rater 3.
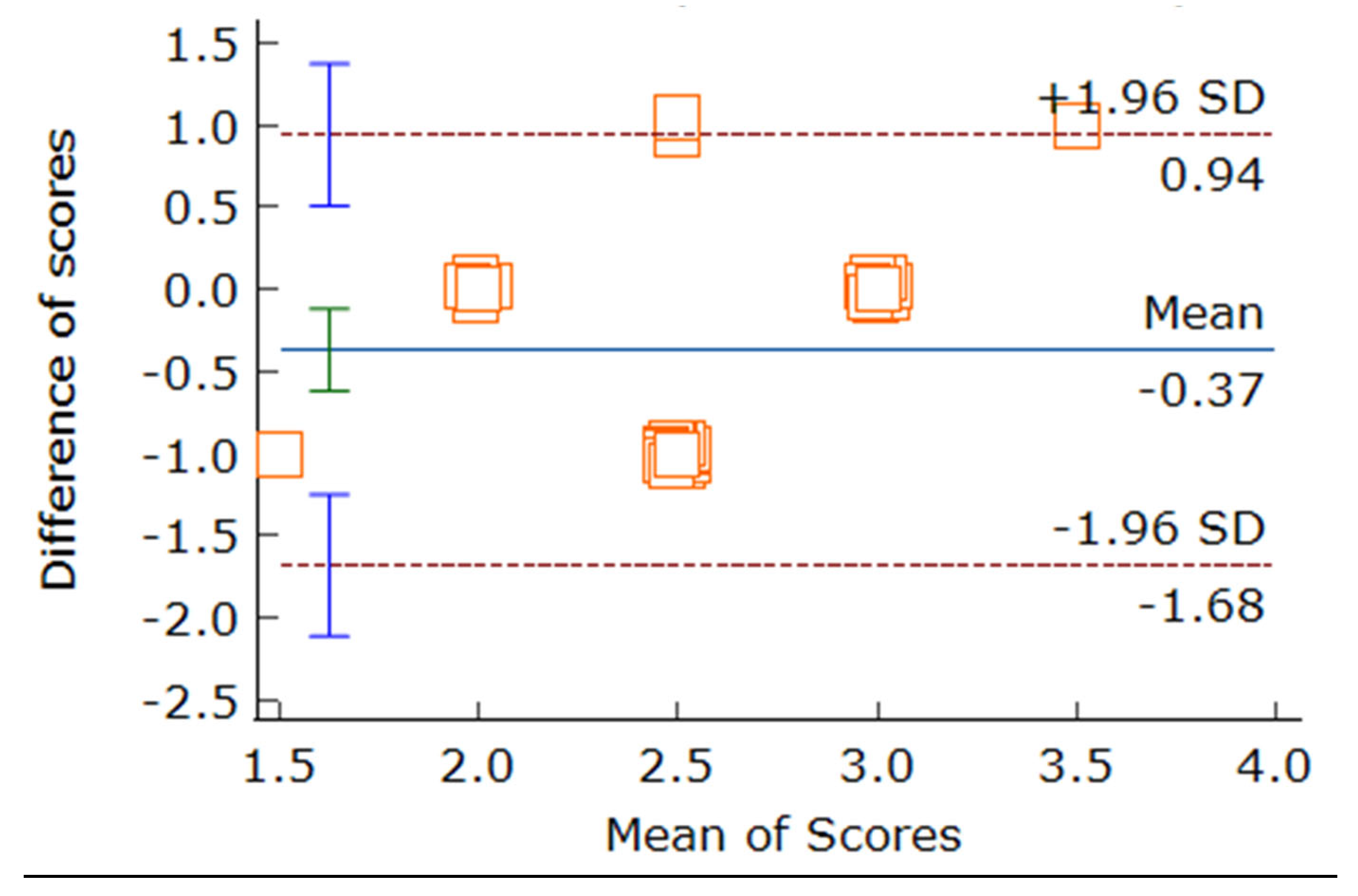
Figure 11.
Bland Altman Plot for GQS Scoring of Rater 1 vs Rater 3.
To analyze it deeper, a Cronbach's Alpha test was conducted for each set of ratings. The reliability of the ratings provided by three raters—Rater 1, Rater 2 and Rater 3—was analyzed using a two-way mixed-effects model with absolute agreement.
For the JAMA Score, the overall internal consistency was found to be good, with a Cronbach's alpha of 0.801 (0.803 based on standardized items). This high level of inter-rater reliability suggests that the raters were consistent in their evaluations. The single measures Intraclass Correlation Coefficient (ICC) was 0.554 (95% Confidence Interval: 0.348 - 0.733), indicating moderate reliability for individual ratings. The average measures ICC was 0.789 (95% Confidence Interval: 0.615 - 0.892), reflecting good reliability when considering the mean of all three raters. Both single and average measures ICCs were statistically significant (p < 0.001), confirming that the observed ICCs are significantly different from zero. The inter-item correlation matrix supported these findings, with moderate to strong positive correlations between raters, ranging from 0.542 - 0.608. This further underscores the consistency among the raters in their scoring of the JAMA criteria.
Regarding the GQS Scores, the overall internal consistency of the ratings was excellent, with a Cronbach's alpha of 0.831 (0.835 based on standardized items). This indicates a high level of inter-rater reliability for the GQS scores. The single measures ICC was 0.594 (95% Confidence Interval: 0.391 - 0.762), suggesting moderate to good reliability for individual ratings. The average measures ICC was 0.814 (95% Confidence Interval: 0.658 - 0.906), indicating excellent reliability for the mean ratings of all three raters. Both single and average measures ICCs were statistically significant (p < 0.001), confirming the significant departure of the observed ICCs from zero. The inter-item correlation matrix revealed moderate to strong positive correlations between raters, ranging from 0.548 - 0.775. Notably, the correlation between Halim and Sayani was particularly strong (0.775), while the correlations involving Arnab were slightly lower but still substantial.
Item statistics for the GQS scores showed mean ratings ranging from 2.57 - 2.87 across raters, with standard deviations between 0.626 and 0.730. This indicates reasonable consistency in scoring patterns among the raters. The high Cronbach's alpha values, significant ICCs, and strong inter-rater correlations collectively highlight the reliability and consistency of the ratings for both JAMA and GQS scores. These findings demonstrate that the scoring methodology used in this study is robust and dependable, ensuring that the evaluations of video content are both accurate and reproducible across different raters.
As a next step, The Kruskal-Wallis H test was utilized to investigate the relationship between designation groups and two scoring systems: JAMA (Journal of the American Medical Association) and GQS (Global Quality Scale). The Kruskal-Wallis test, a non-parametric method, determines whether statistically significant differences exist between two or more groups of an independent variable on a continuous or ordinal dependent variable.
For JAMA scores, the Kruskal-Wallis H statistic was 7.403, with 2 degrees of freedom and an asymptotic significance (p-value) of 0.025. This result indicates a statistically significant difference among the designation groups, suggesting that variations in JAMA scores are associated with different professional categories (H(2) = 7.403, p = 0.025).
Similarly, the analysis for GQS scores revealed a Kruskal-Wallis H statistic of 8.542, with 2 degrees of freedom and an asymptotic significance (p-value) of 0.014. This finding also indicates a statistically significant difference among the designation groups, highlighting that GQS scores vary significantly across different professional categories (H(2) = 8.542, p = 0.014).
Both results are significant at the 0.05 level, with the GQS scores showing a slightly stronger effect (lower p-value) compared to the JAMA scores. These findings suggest that the designation or professional category of individuals significantly influences both JAMA and GQS scores.
The implications of these results are noteworthy. The significant differences in scores indicate that factors related to professional designation, such as background in medicine and professional expertise, may affect performance on these scoring systems. Specifically, it can be inferred that videos produced by doctors tend to be of higher quality and contain better information compared to those created by non-doctors. This disparity underscores the importance of professional expertise in producing content that meets higher quality standards, as reflected in the JAMA and GQS scores.
Lastly, the Kruskal-Wallis H test results highlight the impact of professional designation on the quality of video content related to nutrition and diet for CKD patients. These findings emphasize the need for content creators to have a strong professional background to ensure the delivery of high-quality, reliable information to the audience.
Further to explore the relationship between professional designation (Doctor vs. Non-Doctor) and content presence scorecard performance, Fisher's Exact test was conducted.
The content scorecard utilized in this study was systematically divided into three specific categories: "Good," "Average," and "Poor." These categories were defined by score ranges designed to facilitate a more nuanced and detailed statistical analysis of the evaluated videos. Specifically, a score of 1-2 was categorized as "Poor," indicating significant deficiencies in the quality and comprehensiveness of the content. Scores in the range of 3-4 were classified as "Average," reflecting an acceptable level of content that meets basic standards but lacks excellence in certain critical areas. Finally, scores of 5-6 were categorized as "Good," representing high-quality content that thoroughly addresses essential aspects of the topic with clarity and accuracy.
This structured categorization was crucial for the analysis and interpretation of the data, allowing for a clear differentiation between varying levels of content quality. By assigning specific ranges to each category, the scorecard provided a systematic method to evaluate and compare the performance of the videos under study. This approach enabled the identification of patterns and trends, such as the proportion of videos falling into each category and the factors contributing to these classifications.
Moreover, the predefined categories facilitated a comprehensive understanding of the overall quality of the videos in relation to the established standards. Videos rated as "Good" demonstrated a high level of adherence to quality criteria, ensuring that viewers received reliable and valuable information. In contrast, those rated as "Poor" highlighted areas where significant improvements were needed. This clear delineation helped in pinpointing specific areas of content that require enhancement and provided actionable insights for content creators aiming to elevate the standard of their work.
The results indicate a statistically significant association between these variables (p = 0.001). The crosstabulation of the data reveals notable differences in scorecard performance between Doctors and Non-Doctors.
Doctors demonstrated a higher tendency to score in the "Average Good" (50.0%) and "Good" (27.8%) categories, collectively accounting for 77.8% of their scores. In contrast, Non-Doctors predominantly scored in the "Average" category (75.0%), with a smaller proportion in the "Poor" category (16.7%). It is particularly noteworthy that no Doctors were rated as "Poor," while no Non-Doctors achieved a "Good" rating. These differences underscore a clear disparity in performance between the two groups.
Supporting these findings, the Chi-Square test results (χ² = 14.712, df = 3, p = 0.002) also suggest a significant association between designation and scorecard performance. However, it is important to consider that 62.5% of cells have expected counts less than 5, which may impact the reliability of the Chi-Square test. Given these limitations, Fisher's Exact test provides a more robust indication of the significant relationship, as it does not depend on minimum expected cell frequencies.
Conslusively, these results highlight a strong association between professional designation (Doctor vs. Non-Doctor) and scorecard performance, with Doctors generally achieving higher scores than Non-Doctors. This finding has significant implications for professional development and performance evaluation within the field. It suggests that the expertise and training associated with a medical degree may contribute to a higher quality of content creation, particularly in the context of dietary information for dialysis patients. Therefore, targeted interventions to enhance the skills of Non-Doctors in this area could be beneficial in elevating the overall quality of health information disseminated to the public.
Table 11.
Cross-tabulation for Content Coverage/Authenticity Scoring.
| Designation | Data | Scores | |||
| Average | Good | Poor | Total | ||
| Nephro Health Professionals (NHP) | Count | 13 | 5 | 0 | 18 |
| % within NHP | 72.20% | 27.80% | 0.00% | 100% | |
| Non-NHP | Count | 10 | 0 | 2 | 12 |
| % within NHP | 83.30% | 0.00% | 16.70% | 100% | |
The below Figure 12 gives a graphical representation of the above explained relation of the professional status and the content quality of the videos.
We further examined the relationships between four variables: View, Content, Like, and Correctness, using Spearman's rank correlation coefficient to assess these relationships due to the ordinal nature of the data. The findings revealed significant and nuanced correlations among these variables.
A significant positive correlation was found between View and Content (ρ = 0.422, p = 0.020), indicating a marginally significant relationship where the number of views is associated with higher content quality. This suggests that either higher view counts contribute to better content or that better content attracts more views. The correlation between View and Correctness approached significance but did not reach it (ρ = 0.353, p = 0.056), suggesting a weak to marginally positive relationship. This trend indicates that higher view counts might be associated with increased correctness, but this relationship is not statistically significant at the 0.05 level.
A significant positive correlation was observed between Correctness and Like (ρ = 0.409, p = 0.025), implying that content with higher correctness tends to receive more likes or that more liked content tends to be more correct. The strongest correlation was found between Like and Content (ρ = 0.555, p = 0.001), indicating a moderately strong relationship. This suggests that higher quality content tends to receive more likes or that more liked content is perceived as higher quality.
The scatter plot matrix (as shown below in Figure 13) visually supports these findings, showing positive trends in the relationships between these variables, particularly for Like vs. Content and View vs. Content. These results highlight significant interrelationships among views, likes, content quality, and correctness. The strongest association was found between likes and content quality, suggesting that user engagement, as measured by likes, is closely tied to the perceived quality of the content.
These findings have important implications for content creators and platform managers, emphasizing the need to produce high-quality, accurate content to drive user engagement and visibility. Future research could explore the causal relationships between these variables and investigate other factors that might influence content performance and user engagement. Understanding these dynamics can help optimize content strategies and improve the overall quality of information available to the public.
From the overall study, it was concluded that the content produced by doctors generally had higher content scores compared to that produced by non-doctors. This finding underscores the superior quality and reliability of information provided by professionals with medical training. Despite this, the analysis revealed that there was no strong correlation between view rate and content quality, suggesting that a higher number of views does not necessarily indicate better quality content. However, a strong positive correlation was observed between like rate and content quality. This indicates that while people may watch various videos, they tend to like content based on its reliability and authenticity. Essentially, likes are a more accurate reflection of the perceived quality and trustworthiness of the content rather than just the number of views. This relationship highlights the importance of producing high-quality, accurate content to garner positive user engagement and trust.
7. Limitation
A notable limitation of our study is the potential discrepancy between our search strategies and those actually used by the public to access YouTube videos on nutrition and diet for CKD patients. While we endeavored to replicate typical search behaviors by employing Google Keyword Planner to structure our searches and selecting the top-ranking videos, this approach may not fully capture the diverse and dynamic ways in which users engage with YouTube content. This limitation highlights the inherent variability in public search behaviors and the challenge of accurately mimicking these patterns in a controlled study.
Moreover, the small sample size utilized in our study might be seen as a constraint. However, it aligns with the methodologies of other research assessing health-related content on YouTube (Madathil et al., 2015). Despite this, the limited sample size may affect the generalizability of our findings. Future research should consider using a larger sample size to provide a more comprehensive evaluation of the content quality on this platform. Expanding the sample size would enhance the robustness of the study and allow for more nuanced insights into the breadth and depth of available information.
Another limitation is our exclusion of videos longer than 20 minutes. This criterion, while intended to ensure the analysis of content likely to be fully viewed by users, may have inadvertently omitted videos containing detailed and valuable information. Including longer videos in future studies could provide a more holistic view of the available content and its quality.
Additionally, our study did not account for the presence of misinformation in the evaluated videos, a significant factor given the potential for misleading health information on public platforms. Incorporating an assessment of misinformation into the scoring system in future research would be crucial. This addition would not only enhance the evaluation framework but also address the critical issue of misinformation, ensuring that the quality assessment reflects both the accuracy and reliability of the content.
Comprehensively, while our study provides valuable insights into the quality of YouTube videos on nutrition and diet for CKD patients, addressing these limitations in future research will be essential. A larger sample size, inclusion of longer videos, and consideration of misinformation will contribute to a more thorough and accurate assessment of the health content on this widely used platform.
8. Conclusions
Our study delved into the landscape of YouTube videos addressing nutrition and diet recommendations for patients with Chronic Kidney Disease (CKD). Our findings revealed that while there is a substantial volume of content available on YouTube, the majority of these videos provide a limited scope of information, often lacking in comprehensiveness and depth. Given the alarming rise in CKD prevalence globally and the pivotal role nutrition plays in managing this condition, the necessity for high-quality, evidence-based content on this widely accessed platform cannot be overstated. The investigation highlighted a significant gap in the quality of information being disseminated to the public. Although there are exceptions, the overarching trend points towards a concerning deficiency in reliable, well-researched, and complete content. The implications of such a gap are profound, especially considering that YouTube is often a go-to resource for patients and caregivers seeking health-related information. The potential for misinformation or incomplete guidance to influence health decisions underscores the critical need for improved content curation and creation on this platform.
The study underscores the urgent requirement for collaboration between healthcare professionals, nutrition experts, and content creators to address this issue. It is imperative to develop and promote videos that are not only engaging but also rooted in scientific evidence and best practices in CKD management. Ensuring that the information shared is accurate, comprehensive, and accessible will help empower patients to make informed decisions about their health and dietary practices.
In conclusion, while YouTube remains a popular and potentially powerful tool for health education, the current state of CKD-related nutrition and diet content is far from ideal. Addressing this gap is essential to prevent the spread of misinformation and to support the well-being of CKD patients. By fostering a more informed and health-literate community, we can make strides towards better disease management and improved patient outcomes. The responsibility lies with all stakeholders involved to enhance the quality of information available and to ensure that it truly serves the needs of those seeking guidance on such a critical aspect of their health.
Acknowledgments
First and foremost, I would like to express my deepest gratitude to my supervisor, whose unwavering support, insightful guidance, and invaluable expertise were pivotal in the completion of this thesis. She provided me with the inspiration and motivation to delve deeper into my research, consistently encouraging me to push the boundaries of my understanding. Their patience and willingness to share their vast knowledge have been an immense source of strength throughout this journey. I extend my sincere thanks to my seniors, whose insights and experiences provided me with a clearer perspective on my research. Their readiness to share their knowledge and offer guidance has been invaluable. Their examples of diligence and perseverance have been truly inspiring and have set a high standard for me to aspire to. I am also grateful to my batchmates, whose camaraderie and support have made this journey more enjoyable and fulfilling. The countless discussions, brainstorming sessions, and mutual encouragement we shared were not only academically stimulating but also personally enriching. The bond we formed has been a source of strength, and I cherish the collective learning experience we have had. Lastly, I would like to acknowledge my family and friends for their unwavering support and understanding. Their encouragement and belief in me have been a constant source of motivation. Their patience and love have provided me with the emotional stability needed to complete this project. This would not have been possible without the support and guidance of these remarkable individuals. I am deeply indebted to each one of them for their contributions and encouragement.
References
- Martin WF, Armstrong LE, Rodriguez NR. Dietary protein intake and renal function. Nutr Metab (Lond). 2005 Sep 20;2:25. PMID: 16174292; PMCID: PMC1262767. [CrossRef]
- Bilancio G, Cavallo P, Ciacci C, Cirillo M. Dietary Protein, Kidney Function and Mortality: Review of the Evidence from Epidemiological Studies. Nutrients. 2019 Jan 18;11(1):196. PMID: 30669401; PMCID: PMC6356875. [CrossRef]
- Ko GJ, Rhee CM, Kalantar-Zadeh K, Joshi S. The Effects of High-Protein Diets on Kidney Health and Longevity. J Am Soc Nephrol. 2020 Aug;31(8):1667-1679. Epub 2020 Jul 15. PMID: 32669325; PMCID: PMC7460905. [CrossRef]
- Knight EL, Stampfer MJ, Hankinson SE, Spiegelman D, Curhan GC. The impact of protein intake on renal function decline in women with normal renal function or mild renal insufficiency. Ann Intern Med. 2003 Mar 18;138(6):460-7. PMID: 12639078. [CrossRef]
- Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012 Jan 14;379(9811):165-80. Epub 2011 Aug 15. PMID: 21840587. [CrossRef]
- National Clinical Guideline Centre (UK). Chronic Kidney Disease (Partial Update): Early Identification and Management of Chronic Kidney Disease in Adults in Primary and Secondary Care. London: National Institute for Health and Care Excellence (UK); 2014 Jul. PMID: 25340245.
- Murdeshwar HN, Anjum F. Hemodialysis. 2023 Apr 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 33085443.
- Elliott DA. Hemodialysis. Clin Tech Small Anim Pract. 2000 Aug;15(3):136-48. PMID: 11109715. [CrossRef]
- Hynes-Gay P, Rankin J. Continuous renal replacement therapy: an overview. Dynamics. 2000 Fall;11(3):26-8; quiz 29-30. PMID: 11125463.
- Rees L. Protein energy wasting; what is it and what can we do to prevent it? Pediatr Nephrol. 2021 Feb;36(2):287-294. Epub 2019 Dec 13. PMID: 31834488; PMCID: PMC7815579. [CrossRef]
- Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, Chauveau P, Cuppari L, Franch H, Guarnieri G, Ikizler TA, Kaysen G, Lindholm B, Massy Z, Mitch W, Pineda E, Stenvinkel P, Treviño-Becerra A, Wanner C. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008 Feb;73(4):391-8. Epub 2007 Dec 19. Erratum in: Kidney Int. 2008 Aug;74(3):393. Trevinho-Becerra, A [corrected to Treviño-Becerra, A]. PMID: 18094682. [CrossRef]
- Kovesdy CP, Kalantar-Zadeh K. Why is protein-energy wasting associated with mortality in chronic kidney disease? Semin Nephrol. 2009 Jan;29(1):3-14. PMID: 19121469; PMCID: PMC5500837. [CrossRef]
- Rees L, Mak RH. Nutrition and growth in children with chronic kidney disease. Nat Rev Nephrol. 2011 Sep 27;7(11):615-23. PMID: 21947116. [CrossRef]
- Inoue A, Ishikawa E, Shirai Y, Murata T, Miki C, Hamada Y. Effects of Protein-Energy Wasting (PEW) and hyperphosphatemia on the prognosis in Japanese maintenance hemodialysis patients: A five-year follow-up observational study. Clin Nutr ESPEN. 2020 Apr;36:134-138. Epub 2020 Feb 4. PMID: 32220356. [CrossRef]
- De Nicola L, Zoccali C. Chronic kidney disease prevalence in the general population: heterogeneity and concerns. Nephrol Dial Transplant. 2016 Mar;31(3):331-5. Epub 2015 Dec 29. PMID: 26908831. [CrossRef]
- Ikizler TA, Cano NJ, Franch H, Fouque D, Himmelfarb J, Kalantar-Zadeh K, Kuhlmann MK, Stenvinkel P, TerWee P, Teta D, Wang AY, Wanner C; International Society of Renal Nutrition and Metabolism. Prevention and treatment of protein energy wasting in chronic kidney disease patients: a consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int. 2013 Dec;84(6):1096-107. Epub 2013 May 22. PMID: 23698226. [CrossRef]
- Gracia-Iguacel C, González-Parra E, Pérez-Gómez MV, Mahíllo I, Egido J, Ortiz A, Carrero JJ. Prevalence of protein-energy wasting syndrome and its association with mortality in haemodialysis patients in a centre in Spain. Nefrologia. 2013;33(4):495-505. English, Spanish. PMID: 23897181. [CrossRef]
- Zha Y, Qian Q. Protein Nutrition and Malnutrition in CKD and ESRD. Nutrients. 2017 Feb 27;9(3):208. PMID: 28264439; PMCID: PMC5372871. [CrossRef]
- Koeppen BM. The kidney and acid-base regulation. Adv Physiol Educ. 2009 Dec;33(4):275-81. PMID: 19948674. [CrossRef]
- Fouque D, Aparicio M. Eleven reasons to control the protein intake of patients with chronic kidney disease. Nat Clin Pract Nephrol. 2007 Jul;3(7):383-92. PMID: 17592471. [CrossRef]
- Bellizzi V. Low-protein diet or nutritional therapy in chronic kidney disease? Blood Purif. 2013;36(1):41-6. Epub 2013 May 25. PMID: 23735624. [CrossRef]
- Kovesdy CP, Kalantar-Zadeh K. Back to the future: restricted protein intake for conservative management of CKD, triple goals of renoprotection, uremia mitigation, and nutritional health. Int Urol Nephrol. 2016 May;48(5):725-9. Epub 2016 Feb 17. PMID: 26886110; PMCID: PMC5061032. [CrossRef]
- Dickson LE, Wagner MC, Sandoval RM, Molitoris BA. The proximal tubule and albuminuria: really! J Am Soc Nephrol. 2014 Mar;25(3):443-53. Epub 2014 Jan 9. PMID: 24408874; PMCID: PMC3935594. [CrossRef]
- Peired A, Angelotti ML, Ronconi E, la Marca G, Mazzinghi B, Sisti A, Lombardi D, Giocaliere E, Della Bona M, Villanelli F, Parente E, Ballerini L, Sagrinati C, Wanner N, Huber TB, Liapis H, Lazzeri E, Lasagni L, Romagnani P. Proteinuria impairs podocyte regeneration by sequestering retinoic acid. J Am Soc Nephrol. 2013 Nov;24(11):1756-68. Epub 2013 Aug 15. PMID: 23949798; PMCID: PMC3810076. [CrossRef]
- Ko GJ, Obi Y, Tortorici AR, Kalantar-Zadeh K. Dietary protein intake and chronic kidney disease. Curr Opin Clin Nutr Metab Care. 2017 Jan;20(1):77-85. PMID: 27801685; PMCID: PMC5962279. [CrossRef]
- Riccio E, Di Nuzzi A, Pisani A. Nutritional treatment in chronic kidney disease: the concept of nephroprotection. Clin Exp Nephrol. 2015 Apr;19(2):161-7. Epub 2014 Oct 16. PMID: 25319188. [CrossRef]
- Fouque D, Aparicio M. Eleven reasons to control the protein intake of patients with chronic kidney disease. Nat Clin Pract Nephrol. 2007 Jul;3(7):383-92. PMID: 17592471. [CrossRef]
- Fouque D, Aparicio M. Eleven reasons to control the protein intake of patients with chronic kidney disease. Nat Clin Pract Nephrol. 2007 Jul;3(7):383-92. PMID: 17592471. [CrossRef]
- Bellizzi V. Low-protein diet or nutritional therapy in chronic kidney disease? Blood Purif. 2013;36(1):41-6. Epub 2013 May 25. PMID: 23735624. [CrossRef]
- Rughooputh MS, Zeng R, Yao Y. Protein Diet Restriction Slows Chronic Kidney Disease Progression in Non-Diabetic and in Type 1 Diabetic Patients, but Not in Type 2 Diabetic Patients: A Meta-Analysis of Randomized Controlled Trials Using Glomerular Filtration Rate as a Surrogate. PLoS One. 2015 Dec 28;10(12):e0145505. PMID: 26710078; PMCID: PMC4692386. [CrossRef]
- Goldstein-Fuchs J, Kalantar-Zadeh K. Nutrition Intervention for Advanced Stages of Diabetic Kidney Disease. Diabetes Spectr. 2015 Aug;28(3):181-6. PMID: 26300611; PMCID: PMC4536643. [CrossRef]
- Bellizzi V. Low-protein diet or nutritional therapy in chronic kidney disease? Blood Purif. 2013;36(1):41-6. Epub 2013 May 25. PMID: 23735624. [CrossRef]
- Obi Y, Qader H, Kovesdy CP, Kalantar-Zadeh K. Latest consensus and update on protein-energy wasting in chronic kidney disease. Curr Opin Clin Nutr Metab Care. 2015 May;18(3):254-62. PMID: 25807354; PMCID: PMC4506466. [CrossRef]
- St-Jules DE, Woolf K, Pompeii ML, Kalantar-Zadeh K, Sevick MA. Reexamining the Phosphorus-Protein Dilemma: Does Phosphorus Restriction Compromise Protein Status? J Ren Nutr. 2016 May;26(3):136-40. Epub 2016 Feb 9. PMID: 26873260; PMCID: PMC5986175. [CrossRef]
- Ravel VA, Molnar MZ, Streja E, Kim JC, Victoroff A, Jing J, Benner D, Norris KC, Kovesdy CP, Kopple JD, Kalantar-Zadeh K. Low protein nitrogen appearance as a surrogate of low dietary protein intake is associated with higher all-cause mortality in maintenance hemodialysis patients. J Nutr. 2013 Jul;143(7):1084-92. Epub 2013 May 22. PMID: 23700345; PMCID: PMC3681544. [CrossRef]
- Rhee CM, Ahmadi SF, Kalantar-Zadeh K. The dual roles of obesity in chronic kidney disease: a review of the current literature. Curr Opin Nephrol Hypertens. 2016 May;25(3):208-16. PMID: 26999023; PMCID: PMC5926196. [CrossRef]
- Kalantar-Zadeh K, Tortorici AR, Chen JL, Kamgar M, Lau WL, Moradi H, Rhee CM, Streja E, Kovesdy CP. Dietary restrictions in dialysis patients: is there anything left to eat? Semin Dial. 2015 Mar-Apr;28(2):159-68. Epub 2015 Feb 3. PMID: 25649719; PMCID: PMC4385746. [CrossRef]
- Kucharczuk AJ, Oliver TL, Dowdell EB. Social media's influence on adolescents' food choices: A mixed studies systematic literature review. Appetite. 2022 Jan 1;168:105765. Epub 2021 Oct 20. PMID: 34687823. [CrossRef]
- Madathil KC, Rivera-Rodriguez AJ, Greenstein JS, Gramopadhye AK. Healthcare information on YouTube: a systematic review. Health Informatics J. 2015 Sep;21(3):173–94. [CrossRef]
- Long M, Forbes LE, Papagerakis P, Lieffers JRL. YouTube Videos on Nutrition and Dental Caries: Content Analysis. JMIR Infodemiology. 2023 Aug 10;3:e40003. PMID: 37561564; PMCID: PMC10450531. [CrossRef]
- Bujnowska-Fedak MM, Waligóra J, Mastalerz-Migas A. The Internet as a Source of Health Information and Services. Adv Exp Med Biol. 2019;1211:1-16. PMID: 31273574. [CrossRef]
- Youtube YouTube for Press. 2021. [(accessed on 1 August 2022)]. Available online: https://www.youtube.com/intl/en-GB/about/press/.
- Li HO, Bailey A, Huynh D, Chan J. YouTube as a source of information on COVID-19: a pandemic of misinformation? BMJ Glob Health. 2020 May;5(5):e002604. PMID: 32409327; PMCID: PMC7228483. [CrossRef]
- Pandey A, Patni N, Singh M, Sood A, Singh G. YouTube as a source of information on the H1N1 influenza pandemic. Am J Prev Med. 2010 Mar;38(3):e1-3. PMID: 20171526. [CrossRef]
- Sood A, Sarangi S, Pandey A, Murugiah K. YouTube as a source of information on kidney stone disease. Urology. 2011 Mar;77(3):558-62. Epub 2010 Dec 4. PMID: 21131027. [CrossRef]
- Bora K, Das D, Barman B, Borah P. Are internet videos useful sources of information during global public health emergencies? A case study of YouTube videos during the 2015-16 Zika virus pandemic. Pathog Glob Health. 2018 Sep;112(6):320-328. Epub 2018 Aug 29. PMID: 30156974; PMCID: PMC6381519. [CrossRef]
- Kumar N, Pandey A, Venkatraman A, Garg N. Are video sharing web sites a useful source of information on hypertension? J Am Soc Hypertens. 2014 Jul;8(7):481-90. Epub 2014 May 9. PMID: 25064770. [CrossRef]
- Delli K, Livas C, Vissink A, Spijkervet FK. Is YouTube useful as a source of information for Sjögren's syndrome? Oral Dis. 2016 Apr;22(3):196-201. Epub 2016 Jan 11. PMID: 26602325. [CrossRef]
- Singh AG, Singh S, Singh PP. YouTube for information on rheumatoid arthritis--a wakeup call? J Rheumatol. 2012 May;39(5):899-903. Epub 2012 Apr 1. PMID: 22467934. [CrossRef]
- Radonjic A, Fat Hing NN, Harlock J, Naji F. YouTube as a source of patient information for abdominal aortic aneurysms. J Vasc Surg. 2020 Feb;71(2):637-644. Epub 2019 Oct 11. PMID: 31611104. [CrossRef]
- Gokcen HB, Gumussuyu G. A Quality Analysis of Disc Herniation Videos on YouTube. World Neurosurg. 2019 Apr;124:e799-e804. Epub 2019 Feb 2. PMID: 30721774. [CrossRef]
- World Health Organization (WHO) Food and Nutrition Tips during Self-Quarantine. WHO; Geneva, Switzerland: 2020. [(accessed on 1 August 2022)].
- Fiaccadori E, Sabatino A, Barazzoni R, Carrero JJ, Cupisti A, De Waele E, Jonckheer J, Singer P, Cuerda C. ESPEN guideline on clinical nutrition in hospitalized patients with acute or chronic kidney disease. Clin Nutr. 2021 Apr;40(4):1644-1668. Epub 2021 Feb 9. PMID: 33640205. [CrossRef]
- Brown RO, Compher C; American Society for Parenteral and Enteral Nutrition Board of Directors. A.S.P.E.N. clinical guidelines: nutrition support in adult acute and chronic renal failure. JPEN J Parenter Enteral Nutr. 2010 Jul-Aug;34(4):366-77. PMID: 20631382. [CrossRef]
- Pollard CM, Pulker CE, Meng X, Kerr DA, Scott JA. Who Uses the Internet as a Source of Nutrition and Dietary Information? An Australian Population Perspective. J Med Internet Res. 2015 Aug 26;17(8):e209. PMID: 26310192; PMCID: PMC4642382. [CrossRef]
- Zimmermann M, Jucks R. Investigating the Role of Communication for Information Seekers' Trust-Related Evaluations of Health Videos on the Web: Content Analysis, Survey Data, and Experiment. Interact J Med Res. 2018 Dec 21;7(2):e10282. PMID: 30578181; PMCID: PMC6322917. [CrossRef]
- Zuniga KE, Downey DL, McCluskey R, Rivers C. Need for and Interest in a Sports Nutrition Mobile Device Application Among Division I Collegiate Athletes. Int J Sport Nutr Exerc Metab. 2017 Feb;27(1):43-49. Epub 2016 Aug 24. PMID: 27284955. [CrossRef]
- Trakman GL, Forsyth A, Hoye R, Belski R. Australian team sports athletes prefer dietitians, the internet and nutritionists for sports nutrition information. Nutr Diet. 2019 Sep;76(4):428-437. Epub 2019 Aug 9. PMID: 31397068. [CrossRef]
- Bourke BEP, Baker DF, Braakhuis AJ. Social Media as a Nutrition Resource for Athletes: A Cross-Sectional Survey. Int J Sport Nutr Exerc Metab. 2019 Jul 1;29(4):364–370. PMID: 30160556. [CrossRef]
- Langford A, Loeb S. Perceived Patient-Provider Communication Quality and Sociodemographic Factors Associated With Watching Health-Related Videos on YouTube: A Cross-Sectional Analysis. J Med Internet Res. 2019 May 17;21(5):e13512. PMID: 31102372; PMCID: PMC6543799. [CrossRef]
- Keelan J, Pavri-Garcia V, Tomlinson G, Wilson K. YouTube as a source of information on immunization: a content analysis. JAMA. 2007 Dec 5;298(21):2482-4. PMID: 18056901. [CrossRef]
Figure 1.
Interconnection of CKD progression with metabolic acidosis, inflammation, hormonal resistance and protein catabolism. (A) Kidney dysfunction limits proton (H+) excretion, resulting in a systemic metabolic acidosis. The acidosis causes activation of complement systems, renin angiotensin aldosterone systems and endothelin-1. These acidosis-mediated effects cause CKD progression, forming a viscous cycle. (B) Acidosis promotes inflammation and tissue resistance to multiple anabolic hormones and simultaneously enhances activity of catabolic corticosteroids. Protein catabolism generates acidic products, contributing to acidosis in the setting of CKD and ESRD. Collectively, these abnormalities give rise to a state of protein catabolism, causing sustained negative nitrogen balance, leading to muscle wasting.
Figure 1.
Interconnection of CKD progression with metabolic acidosis, inflammation, hormonal resistance and protein catabolism. (A) Kidney dysfunction limits proton (H+) excretion, resulting in a systemic metabolic acidosis. The acidosis causes activation of complement systems, renin angiotensin aldosterone systems and endothelin-1. These acidosis-mediated effects cause CKD progression, forming a viscous cycle. (B) Acidosis promotes inflammation and tissue resistance to multiple anabolic hormones and simultaneously enhances activity of catabolic corticosteroids. Protein catabolism generates acidic products, contributing to acidosis in the setting of CKD and ESRD. Collectively, these abnormalities give rise to a state of protein catabolism, causing sustained negative nitrogen balance, leading to muscle wasting.
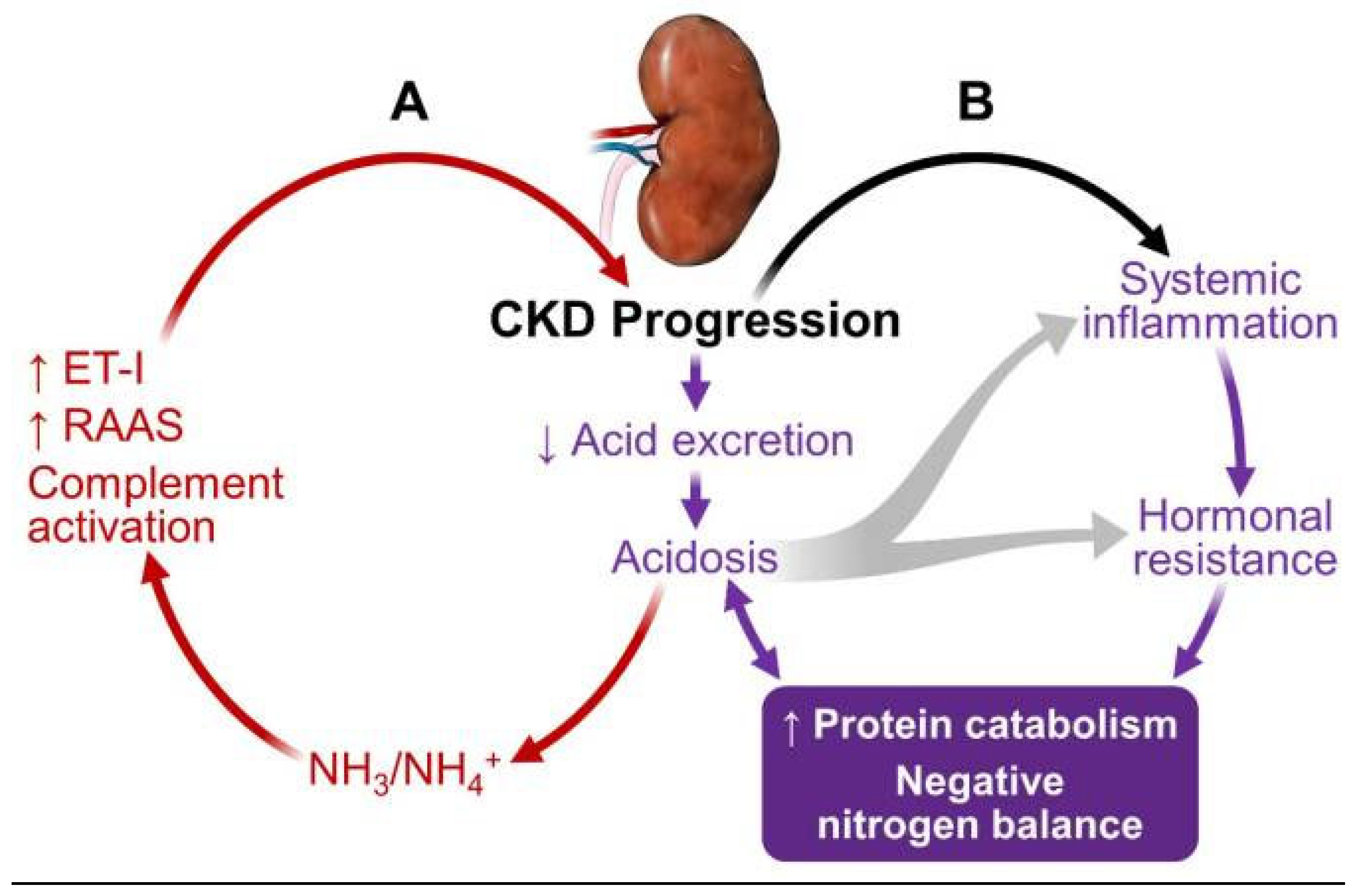
Figure 2.
Flowchart representing the video screening procedure.
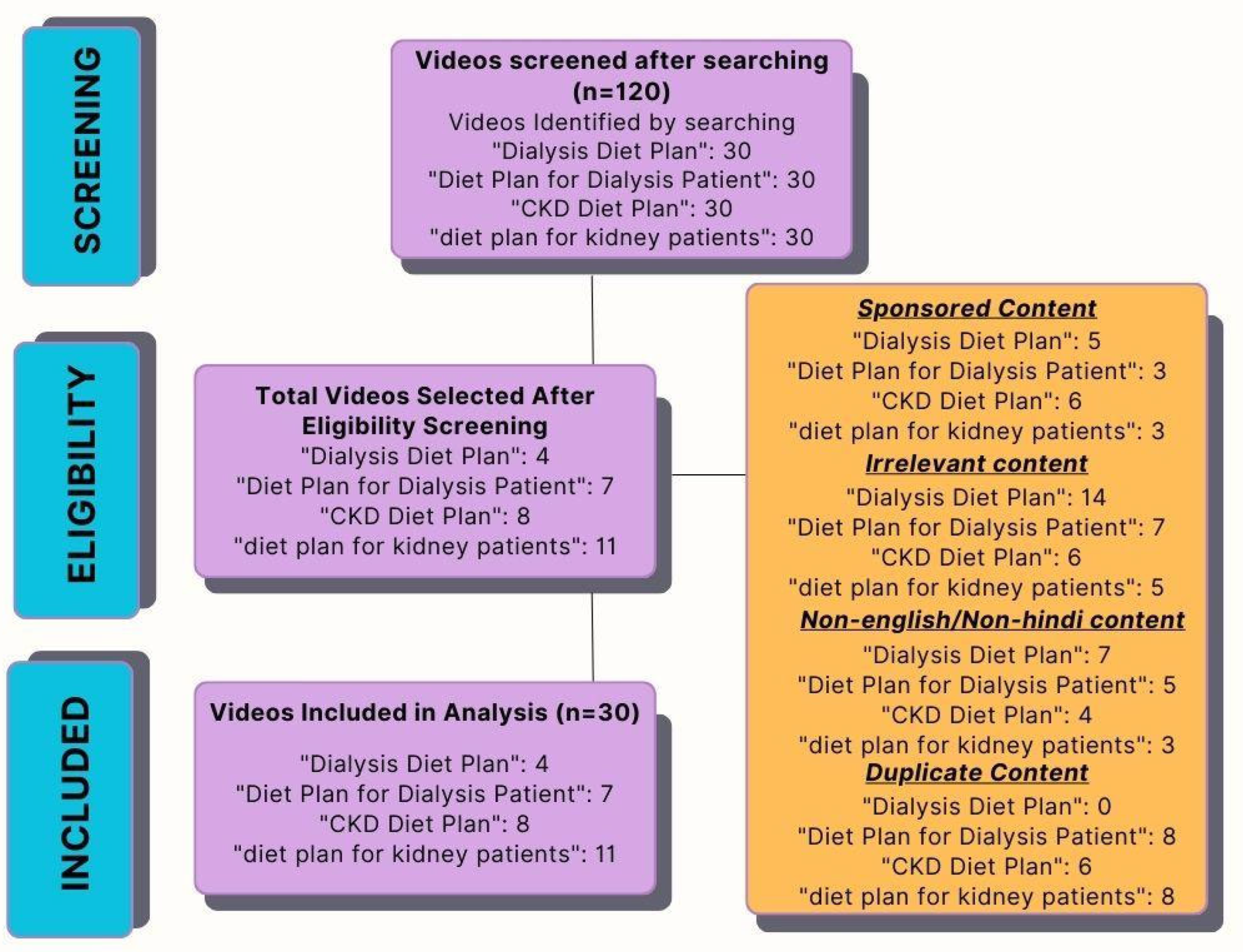
Figure 4.
Graphical Representation of Content Quality as per profession.
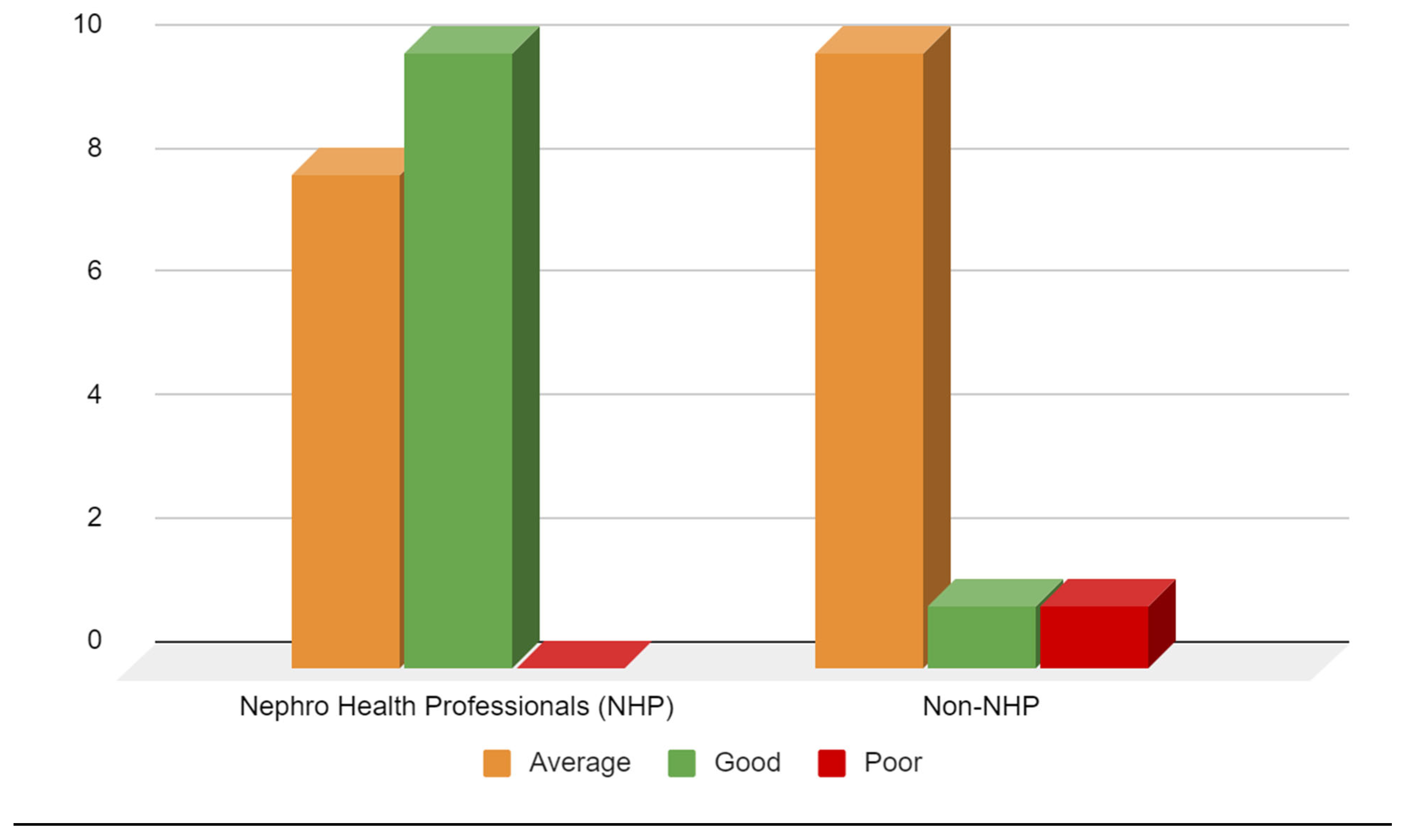
Figure 5.
Scatter matrix plot showcasing the relation between the JAMA Score, GQS Score, Likes and Views on the videos.
Figure 5.
Scatter matrix plot showcasing the relation between the JAMA Score, GQS Score, Likes and Views on the videos.
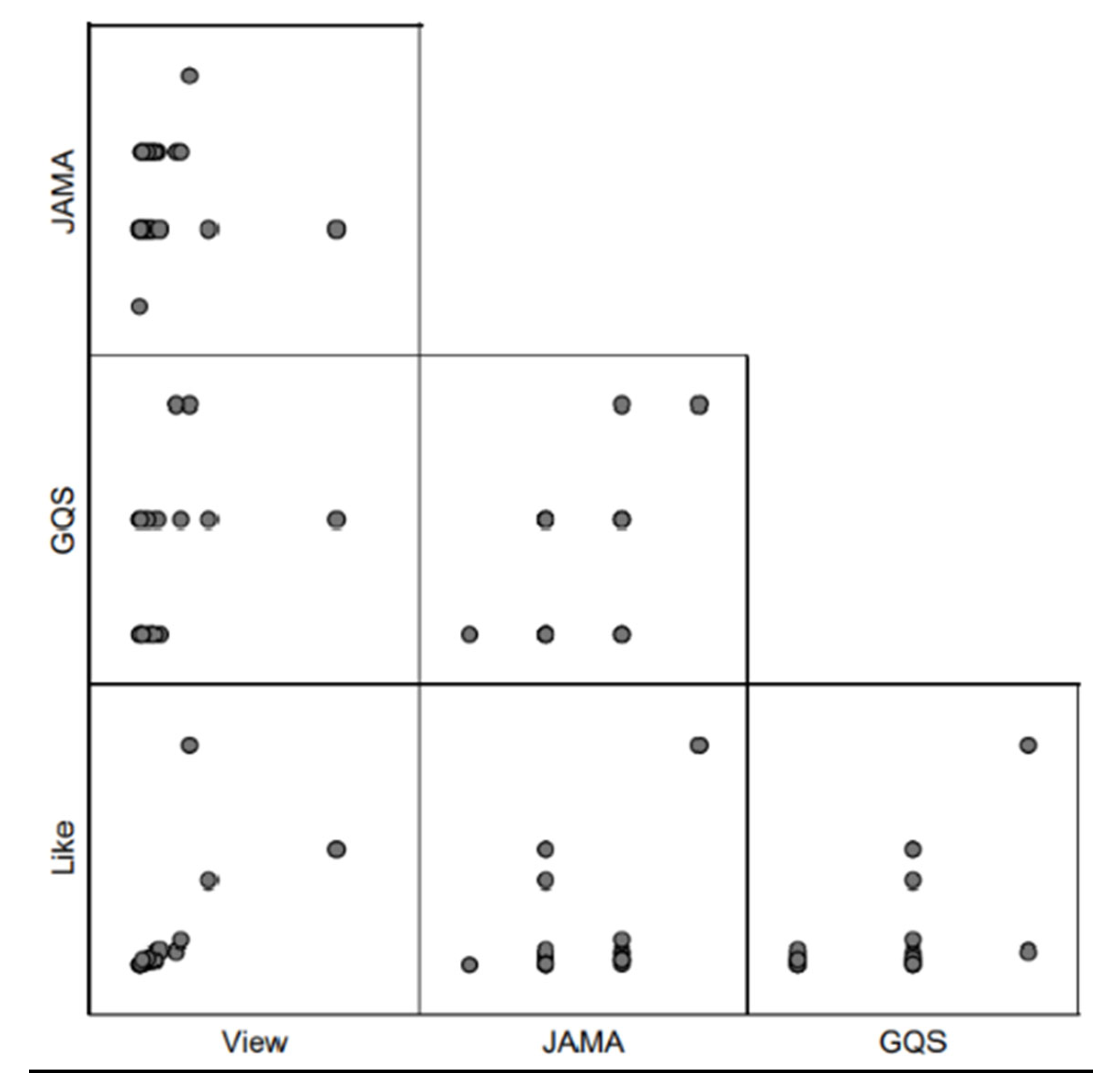
Figure 12.
Graphical Representation of Coverage/Authenticity as per profession.
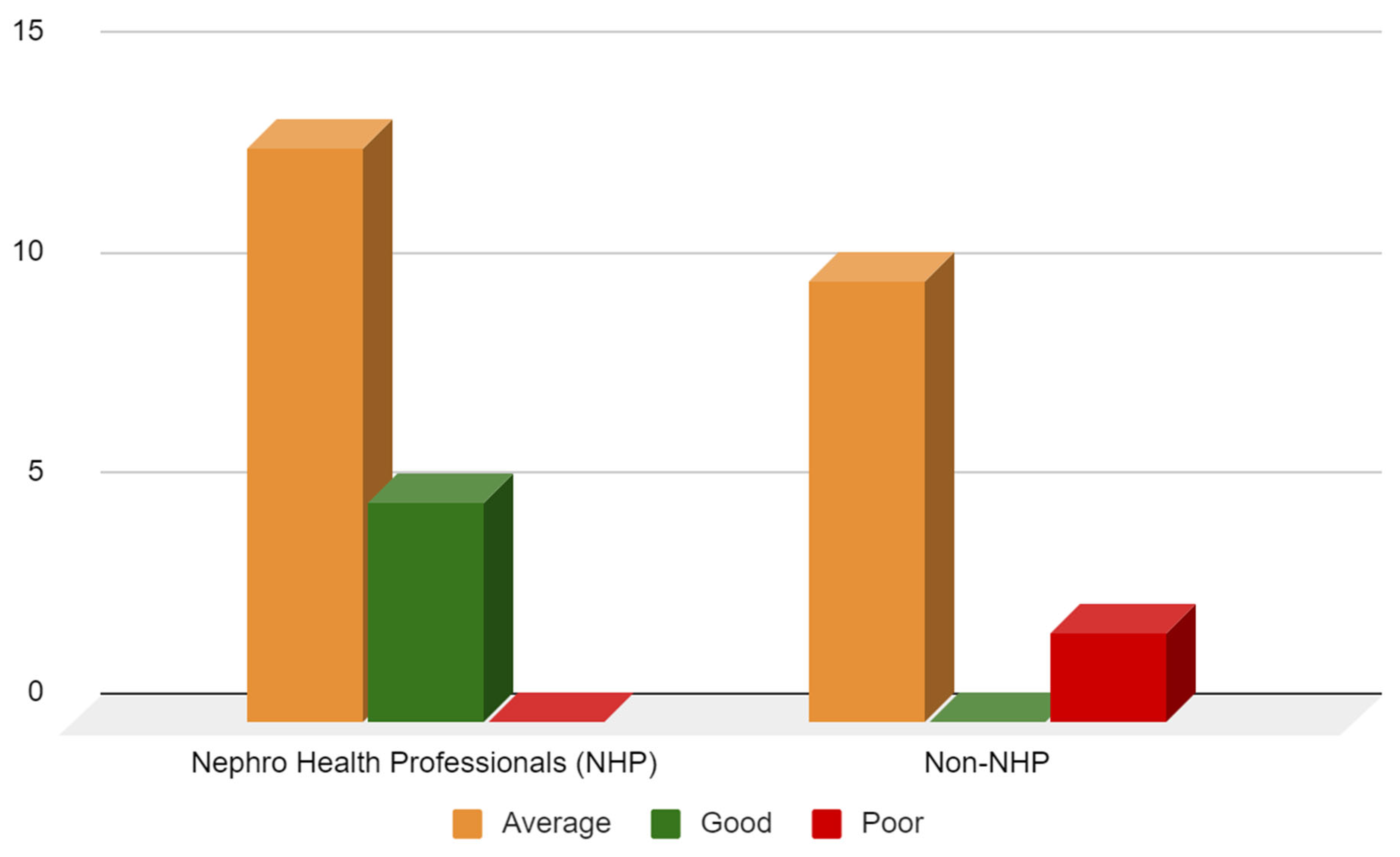
Figure 13.
Scatter matrix plot showcasing the relation between the Presence of Content, Correctness of Content , Likes and Views on the videos.
Figure 13.
Scatter matrix plot showcasing the relation between the Presence of Content, Correctness of Content , Likes and Views on the videos.
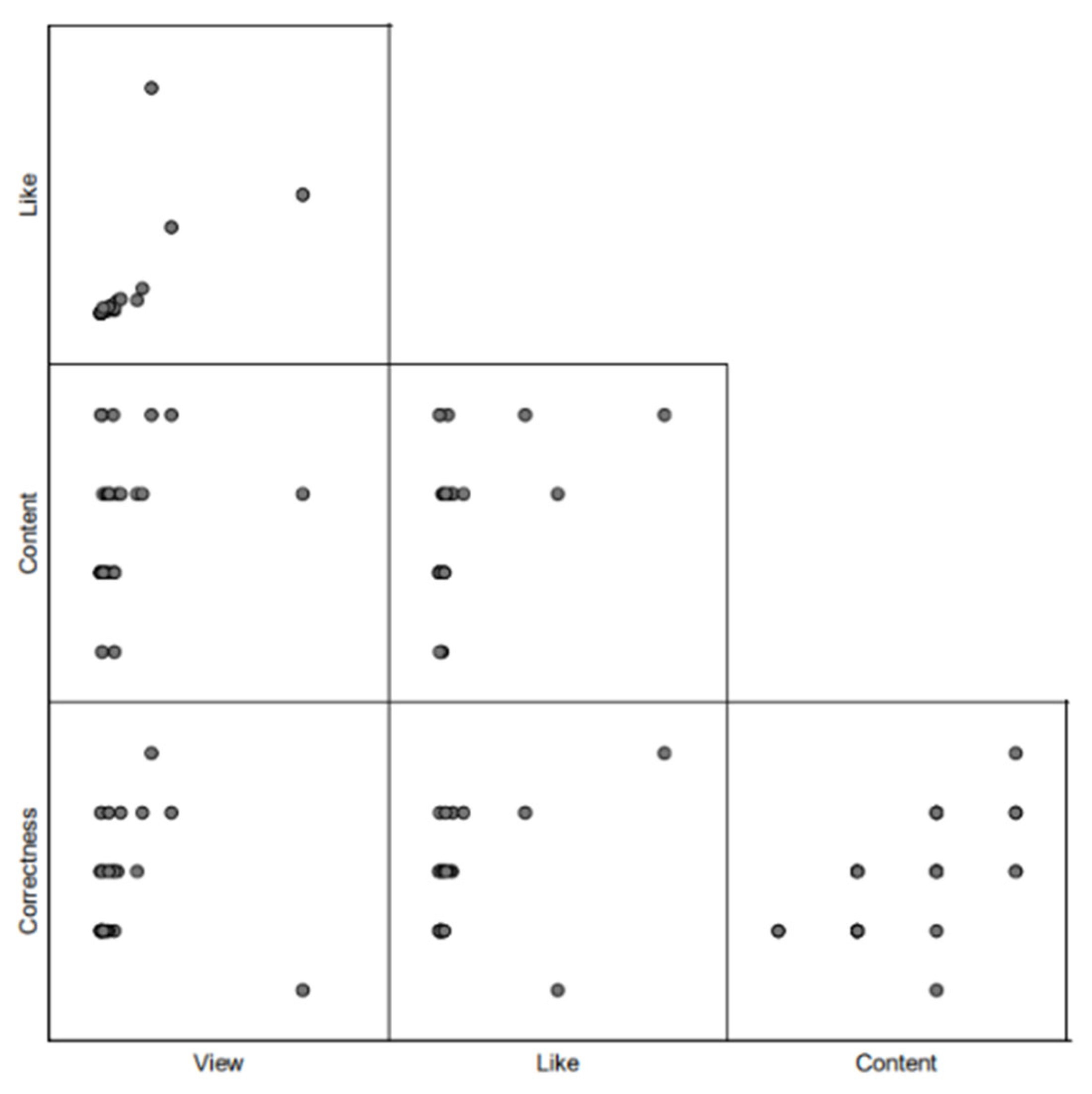
Table 1.
JAMA Scorecard.
| Criteria Description | Description |
| Authorship | Authors and contributors, their affiliations, and relevant credentials should be provided |
| Attribution | References and sources for all content should be listed clearly, and all relevant copyright information noted |
| Disclosure | Web site "owenership" should be prominently and fully disclosed, as should any sponsorship, advertising, underwriting, commercial funding |
| Currency | Dated that content was posted and updated should be indicated |
Table 2.
GQS Scorecard.
| Score | Global Score Description |
| 1 | Poor quality, poor flow of the site, most information missing, not all useful for patients |
| 2 | Generally poor quality and poor flow, some information listed but many important topics missing, of very limited use to patients |
| 3 | Moderate quality, suboptimal flow, some important information is adequately discussed but others poorly discussed, somewhat useful for patients |
| 4 | Good quality and generally good flow, most of the relevant information is listed, but some topics not covered, useful for patients |
| 5 | Excellent quality and excellent flow, very useful for patients. |
Table 4.
Scorecard for checking correctness/quality of information passed.
| Scorecard for checking correctness/quality of information passed | Questions | Weightage | ||
| Positive | Neutral/Not Applicable | Negative | ||
| Was the potassium intake level informed correctly? | 1 | 0 | -1 | |
| Was the sodium intake level informed correctly? | 1 | 0 | -1 | |
| Was phosphorous intake level informed correctly? | 1 | 0 | -1 | |
| Was protein intake levels informed correctly? | 1 | 0 | -1 | |
| Was health condition-wise/co-morbidity customization of diet informed correctly? | 1 | 0 | -1 | |
| Was feasible food suggestions and alternatives given as per indian food recommendation? | 1 | 0 | -1 | |
Table 5.
Characteristics of the YouTube videos on nutrition and CKD included for the analysis.
| Analysis Chart | All Videos (n=30) | Nephro Health Professionals (n=18) | Dieticians and Nutritionist(n=05) | No health professional credentials or unknown credentials (n=7) | |
| Video Age(days) | Mean | 1,507 | 1,477 | 1,620 | 1,502 |
| Standard Deviation | 930.21 | 780.61 | 857.55 | 1397.15 | |
| Median | 1,326 | 1,521 | 1,033 | 1,182 | |
| View count | Mean | 240,371 | 228,619 | 553,418 | 46,984 |
| Standard Deviation | 487390.88 | 250470.43 | 1123003.76 | 62750.60 | |
| Median | 100,191 | 149,390 | 71,193 | 24,212 | |
| Viewing rate (views/number of days since posting) | Mean | 153.8 | 170.1 | 263.8 | 33.3 |
| Standard Deviation | 232.77 | 149.50 | 504.62 | 31.14 | |
| Median | 99.141 | 123.75 | 24.98 | 23.99 | |
| Number of Likes | Mean | 6,281 | 7,909 | 8,378 | 593 |
| Standard Deviation | 15754.72 | 18228.83 | 17680.32 | 665.12 | |
| Median | 1,300 | 1,950 | 587 | 192 | |
| Like rate | Mean | 0.02 | 0.03 | 0.02 | 0.02 |
| Standard Deviation | 0.02 | 0.02 | 0.02 | 0.02 | |
| Median | 0.01 | 0.01 | 0.01 | 0.01 | |
Overall, the 30 included videos had 7,211,123 total views recorded.
Table 6.
JAMA and GQS Scoring done by Rater 1.
| RATER I | |||||
| Analysis Chart | All Videos (n=30) | Nephro Health Professionals (n=18) | Dieticians and Nutritionist(n=05) | No health professional credentials or unknown credentials (n=7) | |
| JAMA Score | Mean | 2.3 | 2.6 | 2 | 2 |
| Standard Deviation | 0.61 | 0.60 | 0 | 0.57 | |
| Median | 2.0 | 3 | 2 | 2 | |
| GQS Score | Mean | 2.5 | 2.7 | 2.6 | 2 |
| Standard Deviation | 0.62 | 0.64 | 0.54 | 0 | |
| Median | 2.5 | 3 | 3 | 2 | |
Table 7.
JAMA and GQS Scoring done by Rater 2.
| RATER 2 | |||||
| Analysis Chart | All Videos (n=30) | Nephro Health Professionals (n=18) | Dieticians and Nutritionist(n=05) | No health professional credentials or unknown credentials (n=7) | |
| JAMA Score | Mean | 2.5 | 2.8 | 2.4 | 1.7 |
| Standard Deviation | 0.62 | 0.38 | 0.54 | 0.48 | |
| Median | 3.000 | 3 | 2 | 2 | |
| GQS Score | Mean | 2.8 | 3.2 | 2.4 | 2.2 |
| Standard Deviation | 0.73 | 0.64 | 0.54 | 0.48 | |
| Median | 3 | 3 | 2 | 2 | |
Table 8.
JAMA and GQS Scoring done by Rater 3.
| RATER 3 | |||||
| Analysis Chart | All Videos (n=30) | Nephro Health Professionals (n=18) | Dieticians and Nutritionist(n=05) | No health professional credentials or unknown credentials (n=7) | |
| JAMA Score | Mean | 2.6 | 2.8 | 2.4 | 2.2 |
| Standard Deviation | 0.56 | 0.51 | 0.54 | 0.49 | |
| Median | 3.000 | 3 | 2 | 2 | |
| GQS Score | Mean | 2.8 | 3.0 | 2.8 | 2.3 |
| Standard Deviation | 0.69 | 0.64 | 0.84 | 0.49 | |
| Median | 3 | 3 | 3 | 2 | |
Table 9.
Dietary Scoring done on the youtube videos for content quality/authenticity analysis.
| Dietary Scoring | |||||
| Analysis Chart | All Videos (n=30) | Nephro Health Professionals (n=18) | Dieticians and Nutritionist(n=05) | No health professional credentials or unknown credentials (n=7) | |
| Scorecard 1 | Mean | 3.6 | 4.0 | 3.2 | 2.7 |
| Standard Deviation | 0.85 | 0.73 | 0.45 | 0.49 | |
| Median | 3.5 | 4 | 3 | 3 | |
| Scorecard 2 | Mean | 2.8 | 3.2 | 2.2 | 2 |
| Standard Deviation | 0.88 | 0.75 | 0.84 | 0 | |
| Median | 3 | 3 | 2 | 2 | |
Table 10.
Cross-tabulation for Content Quality Scoring.
| Designation | Data | Scores | |||
| Average | Good | Poor | Total | ||
| Nephro Health Professionals (NHP) | Count | 8 | 10 | 0 | 18 |
| % within NHP | 44.40% | 55.60% | 0.00% | 100% | |
| Non-NHP | Count | 10 | 1 | 1 | 12 |
| % within NHP | 83.30% | 8.30% | 8.30% | 100% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



