
Submitted:
04 July 2024
Posted:
12 July 2024
You are already at the latest version
Abstract
Purpose: We aimed to develop a nomogram able to predict treatment failure, skeletal events and overall survival (OS) in patients with castration-resistant prostate cancer with bone metastases (CRPC-BM) treated with Radium-223 dichloride (223Ra).
Patients and Methods: Patients from Castilla-La Mancha Spanish region was prospectively included in ChoPET-Rad multicenter study, from January 2015 to December 2022. Patients underwent baseline, interim, and end-of-treatment bone scintigraphy (BS) and 18F-Fluorocholine PET/CT (FCH PET/CT) scans, obtaining multiple imaging radiomics as well as clinical and biochemical variables during follow-up and studying their association with the previously defined end-points. Survival analysis was performed using Kaplan-Meier method and Cox regression. Multivariate logistic and Cox regression models were calculated, and these models were depicted by means of nomograms.
Results: Median progression-free survival (PFS) and OS for our population were 4 and 14 months (mo), respectively. The variables that showed the most robust independent significant association with therapeutic failure were baseline alkaline phosphatase (AP) levels (p=0.022) and the characteristics of BM on CT portion of PET/CT (p=0.017). In the case of OS, the significant variables were therapeutic failure (p=0.038), the number of lines received after 223Ra (p
Keywords:
18F-Fluorocholine PET/CT
; radiomics
; Radium-223 dichloride
; castration-resistant prostate cancer with bone metastases (CRPC-BM)
; therapeutic failure
; overall survival
; nomogram.
Introduction
Radioisotope bone-targeted therapy can be divided into calcium analogs such as 223Ra and strontium-89, and bisphosphonate derivatives such as rhenium-186 etidronate. 223Ra, a calcium mimetic drug, is incorporated into bone by osteoblasts, introducing a targeted alpha therapy for the treatment of CRPC-BM in clinical practice [1,2,3,4].
In 2013, the ALSYMPCA study defined a significant improvement in OS of 3.6 months in CRPC-BM, with respect to placebo, which was unique for a radiopharmaceutical therapy [5]. Following this publication, the Food and Drugs Administration and European Medicament Agency (EMA) approved 223Ra as a treatment option for symptomatic CRPC-BM patients with limited extraosseous disease. However, in 2018, ERA-223, a phase 3 randomized study promoted by EMA, investigating the effectiveness of 223Ra in combination with Abiraterone in CRPC compared to a control group with placebo, reported a 29% increase in the number of fractures compared to the placebo group [6].
223Ra, as a calcium analogue, is incorporated into bone by osteoblasts through the same pathway as calcium [7]. In a same manner, BS with diphosphonates spots the bone disease locations where 223Ra will act. However, it is well known, that metastatic CRPC, as an already advanced tumor disease, promotes tumor heterogeneity, with two implications: increasing chance of resistance to different therapies and limiting the disease detection in one step molecular imaging, supporting the use of additional diagnostic procedures.
The higher diagnostic accuracy of choline analogues-PET/CT compared to standard BS in detecting BM, as well as the ability to diagnose extraosseous disease in the same scan moved us to develop a prospective and multicenter study (ChoPET-Rad) [8,9]. We used the unique PET radiotracer available and authorized for prostate cancer use in Spain, the FCH PET, for patient selection before 223Ra and treatment response based on in clinical practice, monitoring 223Ra treatment rely on clinical and biochemical markers, while assessment of response with imaging techniques remains a controversial topic [10,11].
In addition, based on not all patients obtain benefit from 223Ra, patient selection is the cornerstone of the therapy’s effectiveness; however, it is a continuous challenge. In the last decade, despite efforts, no predictive factors have been established in clinical practice [12,13,14,15]. For this purpose, the development of a novel nomogram that includes both clinical and imaging variables, considering findings in BS and FCH PET/CT, for the prediction of therapeutic failure, could be useful for the optimal selection of those CRPC-BM patients eligible for this treatment.
Therefore, we aimed to study the value of FCH PET/CT and BS in patient selection and response assessment. Additionally, based on the scarcely evidence regarding the prognostic factors potentially able to select patients most likely to benefit from 223Ra [16,17], we aimed to obtain a nomogram system including clinical and radiomic variables able to predict therapeutic failure, bone events and OS in patients, with CRPC-BM, underwent 223Ra therapy.
Material and Methods
The present study (ChoPET-Rad) was designed as a prospective, multicentre (six centers) and non-randomized, and approved by an Ethical Committee (internal code:C-52/2016). Informed consent was obtained from all patients.
Patients
Patients with CRPC-BM who met all the inclusion criteria and none of the exclusion criteria for 223Ra treatment were included between January 2015 and December 2022. The inclusion criteria for initiating 223Ra treatment were: (a) patients with CRPC with symptomatic bone metastases and a negative or inconclusive CT for adenopathic involvement larger than 3 cm or visceral metastatic disease performed in the previous 6 weeks to request 223Ra treatment; (b) patients with a good bone marrow reserve that fulfilled the hematologic criteria necessary to administer 223Ra and (c) Eastern Cooperative Oncology Group (ECOG) performance status of 0–2 and life expectancy greater than 6 months.
The exclusion criteria were: (a) patients who denied participating in the study or (b) who did not fulfill any of the inclusion criteria or (c) were diagnosed of visceral or diffuse bone marrow involvement on baseline FCH PET/CT and/or BS.
Patients were scheduled for treating with 223Ra (55 KBq/kg, intravenously) in a 4-week cycle. Patients who had completed a total of six cycles of 223Ra were defined as treatment completion and those who did not finish the complete treatment protocol because of clinical progression or any other cause were considered as treatment failure. Patients maintained androgen deprivation therapy.
Clinical Assessment
Each patient was clinical, hematological and biochemically evaluated before each 223Ra administration and bimonthly or monthly, after the last 223Ra administration, depending on the patient clinical status and the subsequent therapeutic lines.
Clinical variables studied were: age, Gleason score, prostate-specific antigen (PSA), AP and lactate dehydrogenase (LDH) levels, time of evolution of prostate cancer, time of evolution of BM, therapeutic line that 223Ra represented, number and type of treatments received before 223Ra, castration-resistance date, bone events before, while or after 223Ra treatment, have received a bone protective medication like zoledronic acid and ECOG) performance status before 223Ra. LDH and AP were considered as pathological when their values were higher than 333 and 147 U/L, respectively. Treatments received after 223Ra were collected.
Bone or skeletal events (SE) were considered when BM required analgesic treatment with radiotherapy (RT) or orthopedic surgery, as well as the detection of pathological fractures or spinal cord compression syndrome, with or without the need for palliative RT treatment.
Clinical progression was assessed following the Radiographic Assessments for Detection of Advanced Recurrence (RADAR) II group recommendation [18]. when at least two of the following indicators were reached: (1) convincing and consistent rise in PSA, defined as three consecutive rises, resulting in two 50% increases over the basal PSA value, (2) diagnostic imaging progression evidence, or (3) status performance worsening or appearance of clinical symptoms while the patient was on therapy. Diagnostic imaging progression was stablished when any of imaging techniques (BS or FCH PET/CT) defined progression.
223Ra treatment stopping underwent when clinical progression was addressed. However, the decision to stopping treatment, based on early progression (after the third or fourth 223Ra doses), was made by a multidisciplinary team (oncologist and nuclear medicine physician).
Biochemical PSA response was considered when a decrease in absolute PSA value of ≥ 30% between baseline PSA and interim (1 month later the third dose) or end-treatment (1 month later the sixth dose) was observed, and was defined as early or delayed response, respectively. Stability was considered for the rest of biochemical changes. AP and LDH progression were defined as an increase of ≥ 25% from last available determination during treatment with respect to baseline and response as a reduction of ≥ 30%. The rest of the conditions were considered as stability.
Clinical endpoints were: (a) treatment failure, defined as an incomplete 223Ra administration (less than six cycles) because of clinical progression of the disease or hematological toxicity and/or other clinical impairment, (b) PFS, attending to PSA evolution, defined as three consecutive rises in PSA, resulting in two ≥ 50% increases over the basal PSA value and (c) OS, defined as the elapsed time between the date of the start of 223Ra and the date of either death or the last follow-up. Last follow-up was performed in February 2024.
Patients that received less than three doses due to bone marrow failure or constitutional syndrome, among other causes, earlier to assess disease progression attending to PSA values, were excluded from the response assessment group. Each cause of failure was studied and noted individually, although, some of them were due to causes unrelated to the treatment.
Image Acquisition
FCH PET/CT and BS were performed, within a time interval of 4 weeks, before the first administration (baseline), before the fourth (interim) and after the sixth (end-treatment) 223Ra dose. BS was acquired 3 hours after injection of 740 MBq of 99mTc-methylene diphosphonate (MDP) in three reference centers. FCH PET/CT was performed in a unique reference hospital, 5–15 min after intravenous administration of 2–4 MBq/kg, in three-dimensional acquisition mode for 3 min per bed position, from skull to proximal legs. Low dose CT (120 kV, 80 mA) without contrast was performed for attenuation correction and as an anatomical map. The emission data was corrected for scatter, random coincidence events, and system dead time using the provided software.
Imaging Evaluation
Two independent observers visually evaluated FCH PET/CT and BS. In case of discordances, a third observer reviewed the studies to reach a consensus. BM extension was assessed on baseline FCH PET/CT and BS, considering maximum intensity projection in the former and planar images in the latter. Depending on the number of lesions in BS and FCH PET/CT, BM disease was classified as oligometastatic (≤ 5 lesions) or polimetastatic (> 5 lesions). Also, referring to the extension of the bone disease 4 grades were established, understanding grade I as single or oligometastatic disease, grade II between 6 and 20 metastases, grade III more than 20 metastases and grade IV superscan pattern. When more than 4 bone lesions were observed in BS or FCH PET/CT, with at least one extra-axial location, it was considered a high tumor burden. Furthermore, it was compared whether the predominant activity was osteogenic (BS dominant) or metabolic (PET dominant). Finally, morphological translation in the CT portion of FCH PET/CT was assessed, exclusively in pathological locations, and was classified as: predominantly osteoblastic (>50% of blastic lesions), osteolytic (>50% lytic lesions) or mixed (both blastic and lytic combined in a similar proportion).
Definition criteria for bone positivity was the presence of focal tracer uptake higher than background, regardless of its intensity, with or without any underlying lesion in CT and that could not be explained by a benign lesion like osteophytes or radiotracer excretion locations.
Special care was taken analyzing baseline FCH PET/CT where regions of interest were placed obtaining the maximum standardized uptake value (SUVmax) of the most hypermetabolic location and the average SUVmax of the five lesions with the highest FCH activity. Relation between SUVmax of pathological locations and the hepatic one was also compared.
For lymph node evaluation, any node with visually detectable uptake (higher than background) on FCH PET/CT, despite its size, was considered suspicious of malignancy. Rest of pelvic organs as prostate, bladder and seminal vesicles or visceral locations (lung and liver) were evaluated in the same way. Any of these was considered as soft tissue involvement (STI), except to visceral metastases that caused the exclusion of the patient for receiving 223Ra.
For response assessment, interim and end-treatment BS and FCH PET/CT were compared with respect to the previous one, evaluating all the included anatomical areas (preferable axial skeleton and proximal third of extremities), in order to establish response (baseline and interim, respectively), following the criteria for response formulated by the National Prostatic Cancer Treatment Group, formerly called the National Prostatic Cancer Project (NPCP) [19]. and according to criteria of the European Organization for Research and Treatment of Cancer (EORTC), respectively [20]. For progression assessment, the same criteria were used for BS and FCH PET/CT, consisted of the appearance of at least 2 new lesions.
Concordance between FCH PET/CT and BS baseline, interim and end-treatment, understanding this as a similar BM distribution between both techniques, was evaluated by visual inspection and classified as good (≥75% of the lesions), moderate (approximately between 75 and 25% of lesions) and bad (≤25% of lesions).
Statistical Analysis
Statistical analysis was performed using SPSS software (v. 29). Quantitative variables were represented by mean and standard deviation and qualitative variables by frequency and percentage. Relation between qualitative variables was studied using Chi-squared Pearson test.
Kaplan-Meier method and Cox regression were considered to study the prognostic factors of the OS and the PFS. Log-rank test was used to compare the survival curves among categories of each factor. The median follow-up was estimated using the reverse Kaplan-Meier method.
Cohen’s kappa coefficient was used to report the concordance regarding the extension of bone disease between BS and FCH PET/CT, classifying the results as poor (<0.20), weak (0.21-0.49), moderate (0.41-0.60), good (0.61-0.80) and very good (0.81-1.00). Multivariate analysis was carried out using logistic and Cox regression. The final models were obtained with a stepwise method. Finally, these models were depicted by means of nomograms using the package rms in R software (version 4.4.0). Statistical significance was established by p-value < 0.05.
Results
Treatment with 223Ra was requested for 117 patients; however after clinical and imaging data derived from BS, CT and FCH PET/CT, 17 were dismissed for different reasons: 3 due to visceral metastatic disease (pulmonary, hepatic, and cerebral, respectively), 3 with locoregional infiltration (seminal vesicles, bladder, and pelvic lymph nodes, respectively), 4 due to extensive bone marrow infiltration observed by BS and/or FCH PET/CT, 2 with hematological toxicity (anemia and pancytopenia, respectively), 1 with a possible second primary tumor (hypernephroma), 2 for a deteriorated clinical condition with ECOG > 2, 1 for medullary canal infiltration visualized by FCH PET/CT, and 1 due to having a single bone metastatic lesion.
Finally, 100 patients were enrolled in the current study. Clinical and disease characteristics of patients are summarized in Table 1 and 2. Most of them (n=97) had a good clinical status (ECOG 0-1) before the initiation of 223Ra treatment with a Gleason score ≥ 8 in 45 patients. Only 53 patients underwent previous prostate cancer radical treatment: 26 patients underwent prostatectomy (4 of them received adjuvant RT due to affected surgical margins on surgical specimen) and 27 patients were treated with radical RT. The remaining treatments received prior to 223Ra are described in Table 2. Regarding the line of treatment, 223Ra was administered within the first three therapeutic lines in 80 patients, so in the global list of treatments, 223Ra represented the third line (median).
44 patients completed 6 doses of 223Ra therapy. PSA progression was detected in 70 patients during treatment with 223Ra, 54 experiencing it within the first 3 months from the start of treatment (early progression). In 3 other patients was not possible to assess if there was PSA progression as they died before this parameter could be elevated.
Skeletal events before 223Ra initiation occurred in 23 patients and included: 5 pathological fractures, 7 spinal cord compression syndromes, 3 of which were treated with RT, and 11 lesions treated with RT for pain. SE during and after 223Ra were documented in 3 and 26 patients, respectively; and included: 15 lesions treated with RT, 4 pathological fractures, one of which was treated with orthopedic surgery, and 7 cord compressive syndromes, 3 of which were treated with RT. 2 cases of spinal cord compression during 223Ra treatment lead treatment discontinuation.
Regarding bone protective treatments, 90 patients received Denosumab, Zoledronic acid, or both during their disease management (22, 58, and 10, respectively). 44 patients maintained them before, during, and after 223Ra treatment, while the rest only in some of them.
Median follow-up was 73 months with a median PFS and OS of 4 and 14 months, respectively. 97 patients experienced PSA progression during their follow-up, occurring in 70 during treatment with 223Ra, and more specifically in 54 within the first 3 months since the start of treatment. 83 received at least one treatment after 223Ra, with a mean of 2 subsequent lines received. Received treatments included abiraterone, enzalutamide, and one or more lines of chemotherapy in 26, 28, 41, and 28 of them, respectively. For those patients who completed 223Ra treatment, the median OS was 20 months compared to 9 months for those who did not complete it. During the follow-up 92 patients died.
According to the analysis of baseline parameters of imaging techniques, only a single patient did not undergo a baseline BS prior to treatment, while 87 underwent baseline FCH PET/CT. The detailed analysis of baseline parameters derived from the results of these techniques was described in Table 1 and Table 3. They all showed avidity in their lesions for the injected radiopharmaceuticals. Additionally, high tumor burden was observed in 61% of BS and 48% of FCH PET/CT. Furthermore, FCH PET/CT detected STI in sixteen patients, 14 with nodal involvement, 3 with local prostatic disease, and prostatic and nodal disease in 2 patients.
If we focus on the assessment of treatment response, 13 patients were excluded for receiving less than 3 doses of 223Ra: 5 due to hematological intolerance, 2 for symptomatic bone progression, 2 for visceral progression, 2 for primarily digestive intolerance, and the last 2 due to other causes unrelated to 223Ra (traumatic fracture and pulmonary embolism).
Only 7 patients experienced PSA response during 223Ra treatment, 4 of them early responses during the first 3 doses that kept during the rest of treatment and the rest delayed ones, during the second 3 doses.
AP progression was observed in 15 cases, and LDH progression in 17. AP and LDH responses were detected in 22 and 10 cases, respectively.
Regarding binary imaging response (progression vs. no progression), progression was more frequently observed in FCH PET/CT scans both at interim and end-treatment compared to BS. According to the progression pattern in interim FCH PET/CT, in most cases, progression was osseous, but in 15 of them soft tissue involvement was observed: 3 exclusively nodal, 7 nodal and osseous, and 5 visceral and osseous. The proportion of patients who progressed at the end of treatment FCH PET/CT was lower (51.3% vs 64.4% in the interim): 13 exclusively osseous, 3 nodal, 1 visceral, 2 osseous and nodal, and 1 osseous and visceral. The degree of agreement between interim BS and FCH PET/CT was weak (k: 0.349; p<0.001), being higher in the case of binary response assessment (progression vs. no progression) (k=0.447; p<0.001). No agreement was observed between end-of-treatment studies (k=0.157; p=0.120 and k=0.211; p=0.075 in binary response). The distribution of results is shown in Table 4.
The results of the Chi-square analysis between the different variables and therapeutic failure rate and SE during or posterior 223Ra are summarized in Table 5 and Table 6. The number of patients who did not receive complete treatment with 223Ra was associated with those with poorer performance status (ECOG > 0) (p= 0.038), those who did not receive prior bone protective treatment (p= 0.040), or with pathological baseline AP levels (p= 0.030) or LDH and p= 0.039), among others.
In the case of SE, only the variables of additional treatments after 223Ra, OS (≤12 months vs >12 months), and a high tumor burden on FCH PET/CT showed significant associations (Table 6). Paradoxically, patients with a higher number of lines of treatment following 223Ra showed a statistically significant occurrence of new SE during or after 223Ra treatment (p< 0.001). In fact, any additional therapeutic line increased the risk in 42.7%. However, in multivariate analysis, only OS showed significant association with SE as patients with OS longer than 12 months had 10.795 times an increased risk of SE (p= 0.003). This result was inconsistent for a nomogram design based on the higher the OS; the higher is the probability of receiving subsequent therapeutic lines and suffering SE.
Performance status before to 223Ra (p< 0.001) and AP baseline levels (p< 0.001) and LDH (p= 0.033) were found to have a significant impact on OS (Figure 1), as well as other factors such as completion of treatment with 223Ra (p< 0.001). Regarding imaging variables, both the Chi-square test and the Log-Rank test showed that derived FCH PET/CT variables had statistical significance. Thus, high tumor burden (p= 0.003), uptake of the most hipermetabolic lesion above the liver (p< 0.001), or STI in FCH PET/CT study (p= 0.048) were associated with a lower median OS (Figure 2). Focusing on treatment response assessment, only interim studies (BS and FCH PET/CT) showed a significant association with OS, with data extracted from FCH PET/CT being slightly more robust compared to BS (p< 0.001 vs p= 0.004, respectively) (Figure 3). The significant variables in the univariate analysis were included in multivariate analysis for the OS and therapeutic failure variable. In the former, the association of uptake of lesions above the liver (p = 0.011), therapeutic failure (p = 0.001), or pathological baseline AP (p = 0.011) was highlighted as leading to lower OS. Table 7 details the results of the univariate Cox regression and Table 8, Table 9 and Table 10 the results of the Log-Rank test regarding OS.
Based on the independent risk factors obtained from multivariate logistic regression analyses, two nomograms were constructed: one to predict the percentage of therapeutic failure and the other to predict the 1- and 2-year survival rates in patients treated with 223Ra. A point scale from 0 to 100 was used to score each variable, and then the sum of all scores was calculated. The risk of therapeutic failure and death can be predicted by observing the total points. In the first nomogram (therapeutic failure), the variable characteristics of bone metastases on the CT were divided into osteoblastic or rest of lesions (lytic or mixed), and the units of measurement for baseline AP were IU/L. In the second nomogram (OS), the variable lines of treatment after 223Ra were divided into 6 to 1 lines and for the mean SUVmax from 0 to 18. In the case of the response variable on the FCH PET/CT, it was divided into progression and non-progression, and for the rest of the variables, no and yes (Figure 4).
Discussion
Impact on Treatment Response and OS of 223Ra Therapeutic Line
After ERA-223 trial, EMA went further, not only limiting itself to the combination of 223Ra with androgen receptor-targeted agents but also to its prescription as monotherapy, restricting its use, inexplicably, to those patients with CRPC with ≥ six BM who had received at least two systemic therapies administered before223Ra [21]. Following this new indication, the reported OS defined by 223Ra use has decreased with respect to the defined OS in ALSYMPCA or previous works, with median OS ranging from 6 to 12.8 months [22,23,24,25,26,27]. The delay of patient’s inclusion for 223Ra treatment, can be the explanation, allowing cancer cells to adapt to the selective pressures imposed by previous therapies and facilitating the development of a new resistant phenotype making it less sensitive of obtaining benefit of subsequent treatments in terms of response and, most important, survival [26,28,29].
In the present work, despite the delayed use of 223Ra, our median OS (14 months) was in line with ALSYMPCA (14.9 months). However, previous works defined higher median OS (around 17 months) probably explained by patient’s characteristics, as a less castration resistance evolution time, lower values of AP and a reduced number of previous systemic therapy treatments [30,31].
Diagnostic Imaging in Patient Selection
Patients’ benefit and outcome after 223Ra treatment are strongly influenced by patient selection [5,32]. Some biomarkers have been suggested who may benefit from treatment with 223Ra and for monitoring, such as patient characteristics, findings in various imaging techniques, serum levels of collagen metabolism products, soluble factors secreted by osteoblasts, and even molecular aberrations, although with limited evidence [33,34].
Based on patients with shorter OS mostly are in later stages of the disease, novel-imaging techniques as PET/CT could solve partially the suboptimal selection of patients attending to clinical criteria after EMA restrictions [26)]. However, current guidelines, such as those from the European Association of Urology and the American Urological Association, do not include recommendations about diagnostic imaging assessment in patient selection and treatment monitoring of 223Ra in clinical practice [1,2,3,4]. In fact, BM are not typically considered in response evaluation criteria in solid tumors (RECIST) on CT in clinical trials and BS has a limited accuracy [35,36]. Consequently, baseline-imaging parameters in CRPC-BM, which may predict response to 223Ra therapy, are desirable.
Choline analogues-PET/CT and other PET radiopharmaceuticals, such as 68Ga or 18F- prostate specific membrane antigen (PSMA) and 18F-NaF, have shown promising results in the assessment of CRPC, so they could also be a good option for patient selection and response evaluation [37,38,39]. However, imaging restrictions and under-recognition have promoted that the role of these novel-imaging techniques, based on PET/CT, has not been well documented. A recent work revealed that baseline PSMA PET/CT versus CT did not seem to impact biochemical response during 223Ra therapy in mCRPC patients. Nevertheless, patients in the baseline CT group had a significantly shorter OS compared to the PSMA PET/CT group (12.4 vs 19.9 months, respectively), most likely due to under- detection of STI in the former. Therefore, replacing CT with PSMA PET/CT appears to be a valuable screening method for identifying patients who will benefit most from 223Ra therapy [40].
PET/CT-derived functional parameters, such as maximum and mean SUV and lean body mass corrected SUV peak (SUL peak), have been investigated as potential biomarkers for patients’ prognostication before therapy. Previous works using baseline FCH PET/CT have showed controversial results, with no associations of SUVmax with response to treatment [38,41] and negative correlation of SUVmax with PFS and OS in patients receiving enzalutamide [42,43]. Furthermore, volumetric SUV-based parameters, namely metabolically active tumor volume (MATV) and total lesion activity (TLA), both reflecting the burden of metabolically active disease, were found to have significant prognostic impact [41,43,44,45]. In addition, FCH PET may be useful for patients’ stratification before 223Ra therapy, being high MATV the only reported significant predictor of OS (p = 0.003; HR = 7.6) in multivariate Cox analysis [41]. In the current study, both the SUVmax value of the lesion with the highest uptake and the average SUVmax of the 5 lesions with the highest uptake, were evaluated in the FCH PET/CT studies, showing both a significant association with OS. Additionally, perhaps a more robust, or comparable among works, variable such as the existence of at least a lesion with uptake higher than the liver proved to be other independent variable associated with OS (Figure 5 and Figure 6).
Given the similar uptake properties of 223Ra and BS tracer in osteoblastic bone, a reasonable hypothesis is that metastatic disease with higher uptake on BS or 18F-NaF PET/CT compared to FCH PET/CT is more likely to respond to 223Ra therapy, based on increased choline levels can reflect on more aggressive tumor [38,41,43,46,47,48]. Ahmadzadehfar et al., [49] reported that when PSMA PET/CT is used as the gatekeeper in addition to BS, radionuclide therapy with 223Ra may be more effective and have more success regarding changes in the PSA, mainly because of better patient selection with the exclusion of patients with bone marrow involvement or STI [49]. In our case, similar results were found with the combined use of FCH PET/CT and BS, as some of the FCH PET/CT variables had significant associations with OS. These included bone marrow infiltration (median 6 vs 14 months; p < 0.001), uptake of the most hypermetabolic BM above the liver (median 10.5 vs 16 months; p < 0.001) and STI (median 7 vs 14 months; p = 0.048).
Response Assessment
Disease progression on imaging techniques is the most critical parameter for therapeutic change in mCRPC. Besides the limited value of CT and BS for early response evaluation of BM, blood-based biomarkers, including PSA and AP, have showed controversial results. Serum AP has been defined as a very useful marker to assess 223Ra treatment response by some authors [16]. However, in clinical practice, an AP decrease after 223Ra treatment has not been necessarily associated with tumor response on 68Ga-PSMA PET/CT and could coexist with radiologic disease [37]. In fact, AP reflects osteoblasts activity, which is targeted by 223Ra, but does not directly reflect the tumor load. In several studies a decline in AP levels during 223Ra therapy has been associated with improved OS [5,12,50]. Van der Doelen et al. [51], observed that those patients with elevated baseline AP who did not show a ≥10% reduction after the first dose of 223Ra had worse OS compared to those who did reduce their baseline AP values, which could be an early indicator of treatment resistance. In our work, we did not study this association mainly because few patients experienced a reduction of these biochemical markers during 223Ra treatment.
Regarding BS, BSI has been defined as a very useful for both evaluating treatment response and predicting the prognosis of treated patients [16]. In the present work, BM progression was established on BS using NPCP criteria; although without the needed confirmation on a second scan according to the 2x2 rule. In addition, to a more reproducible comparison, we used the same criteria for FCH PET/CT. Only interim BS and FCH PET/CT showed significant association with OS with strongest relation of binary response (progression vs no progression) for interim FCH PET/CT (Table 9).
The Prostate Cancer Working Group pays little attention to PSA changes during and after therapy cycles. However, using PSMA PET/CT, as supportive imaging diagnostic technique for response evaluation, there was a significant correlation between PSA changes and the treatment response according to images, which increases the value of PSA as a reliable tumor marker for the follow-up of these patients [49]. According to our data, we completely agree with the previous assessment, observing that a significant increase in the PSA level during therapy cycles likely occurred because of disease progression on FCH PET/CT. In fact, PSA change has been defined as a very useful marker for prognosis prediction [16]. In the present work, PSA progression was associated with a lower OS (median 12 vs 19 months; p= 0.004). Significant results were also observed when evaluating by periods, comparing progression during the first three doses of 223Ra vs. any other time (median 12 vs 16 months; p= 0.017).
De Jong et al. [37] compared 68Ga-PSMA PET/CT with conventional modalities for response evaluation after 223Ra treatment in patients with mCRPC. After 3 cycles of 223Ra treatment, BS could not distinguish good responders from poor responders. At the end of treatment and at treatment failure, all patients had progressive disease on 68Ga-PSMA PET/CT due to the development of at least 1 new BM, whereas 15% and 43% of patients, respectively, also had progressive disease on conventional imaging. In addition, the interpatient heterogeneity in response was not reflected by PET Response Criteria in Solid Tumors (PERCIST) criteria. Therefore, PERCIST was not considered sufficient to distinguish good responders from poor responders to 223Ra treatment and the authors decided to assess novel parameters of 68Ga-PSMA PET/CT as total tumor volume and voxel-wise heterogeneity.
Standardization and actualization of PET/CT response criteria is necessary and whereas no diagnostic response criteria for FCH PET/CT exist, several criteria have been described for PSMA ligands PET/CT [52,53,54]. We used, the same progression criteria for BS and FCH PET/CT, in accordance with PSMA PET progression criteria defined by Fanti et al. [53]. However, perhaps, a combined assessment of tumor volume variations, should define a more comprehensive response definition.
Skeletal Events
Although the most reported symptomatic skeletal event (SE) in CRPC-BM are the use of external-beam radiotherapy and symptomatic pathologic fractures, the latter, causing in some patients cord compression, are major contributors to morbidity and mortality [40,55].
PARABO study revealed that the number of SE decreased in patients who completed the 6 doses of 223Ra [31]. In addition, in ALSYMPCA study [5] 223Ra prolonged the time to the first SE versus placebo (median of 15.6 vs 9.8 months, respectively), when each was used in combination with the standard of care. In our population, there was no significant decrease in the number of SE in those patients who completed 223Ra treatment with respect to those who had a therapeutic failure (25% vs 27.3%, respectively). However, we observed a delay in the occurrence of these SE, with a median of 19 months compared to 9 months, respectively. In our sample of patients, no significant association was found between SE during or after 223Ra treatment and therapeutic failure (Table 5) and although SE was a reason for 223Ra discontinuation in 3 cases, most of the SE occurred after 223Ra treatment. However, our rate of SE during 223Ra treatment was lower than the previously reported 15% by Palmedo et al. [31], that additionally defined no clear impact of bone health agents on SE in similarity with our results. However, we found a significant association between SE during and after treatment with 223Ra and the number of subsequent lines of treatment received, as well as the OS of these patients. These findings suggest that the presence of subsequent SE increases in parallel with the survival of these patients, as an inherent secondary effect of BM and bone metabolism disturbances due to age and androgen deprivation (Figure 7), in fact, any additional therapeutic line increased the risk in 42.7%. However, in multivariate analysis, only OS showed significant association with SE as patients with OS longer than 12 months had 10.795 times an increased risk of SE. Additionally, a relationship was found between SE, high tumor burden, and BM involvement in the FCH PET/CT but not in the BS, being potentially an important factor for selecting which patients could benefit from closer monitoring. The incidence of SE in the present work (26%) was in accordance with respect to the 33% reported by ALSYMPCA trial [56,57] and also by Bosch et al. [40] during and after 223Ra therapy (36.4% and 28.8% of patients selected with baseline-PSMA vs baseline-CT, respectively), the latter possibly in the context of the presence of a higher volume of bone disease in PSMA group (66.7% vs 48.1%) or a shorter OS of CT group.
Therapeutic Failure
Therapeutic failure understood as not completing treatment with 223Ra, is variable among studies ranging from 20 to 45% [40,41,58]. Previous reports indicate that patients with good prognostic factors are more likely to complete six cycles of 223Ra therapy [58,59,60,61]. Of those, Alva et al. [61] demonstrated that treatment with the full six cycles of 223Ra therapy was associated with ECOG performance status of 0–1, no or mild pain, lower PSA, normal AP, no prior Abiraterone/Enzalutamide therapy, and low BSI, a parameter of bone tumor burden.
In our population, it was similarly observed that a better ECOG performance status, normal baseline AP levels, and a lower number of lesions on BS were associated with completing treatment with 223Ra. Additionally, other variables such as having received a prostatectomy as the initial radical treatment, normal baseline LDH levels, no PSA progression during treatment, and receiving bone protective treatment were significantly associated. In multivariate analysis, the association with the absence of PSA progression during treatment was likely related to the fact that PSA progression was one of the criteria for discontinuing the 223Ra treatment.
Multiple baseline radiomic variables derived from FCH PET/CT, contrary to BS, showed significant associations with therapeutic failure as location, number, extent of BM, activity higher than liver uptake and BM characteristics on CT portion of PET/CT (Table 5).
There was not only a significant association, as with BS, between a higher number of lesions and therapeutic failure, but also significant associations with others as axial and extra-axial BM locations, having more than 20 lesions or a superscan pattern, the presence of lytic or mixed BM, STI and lesion uptake higher than liver uptake. These findings suggest that FCH PET/CT could aid in selecting the best candidates for receiving 223Ra treatment (Table 5).
Prognostic Factors
Various reports have indicated several prognostic indicators, associated with good OS for CRPC-BM patients treated with 223Ra, though the details presented differ and no single method has yet been established. Among factors associated with a better OS highlights: ECOG performance status of 0 [25,51,62,63], a normal value of AP [62,64,65], a lower BSI [15,64,66,67], a lower number of BM (< 20) in BS [30], a normal LDH [15,27], lower PSA values [68] or higher PSA duplication times before 223Ra treatment [30,63].
Although a substantial survival benefit has been described in patients reaching the completion of 223Ra cycles [69,70,71,72,73], a controversial theory is that the 223Ra effective dose is only achieved by giving all the six cycles and that anything less is under-treatment [74]. In the present work, therapeutic failure was a subrogated of disease progression that supports the assessment that the most likely cause of the shorter OS in patients receiving incomplete 223Ra treatment is the early progression caused by advanced stage of their disease.
Extraosseous involvement or STI on PSMA PET, defined as visceral or lymph node metastases after therapy, has been previously associated with significantly shorter OS compared with those without newly detected STI (median OS, 10.6 vs. 14.9 months, respectively; p<0.01) [40]. In our study, however, no differences in OS were detected between both groups (median of 19 months vs 17 months, respectively). Significant differences were only found in baseline studies comparing patients with STI to those with preserved soft tissues, with median OS of 7 months vs 14 months, respectively.
Regarding the response to 223Ra treatment our results showed significant association between non-progression in both BS and FCH PET/CT in interim studies and greater OS, being more notable with FCH PET/CT (Table 10 and Figure 3).
With respect to the impact derived from the association of different prognostic factors, Bauckneht et al. [26] referred a reliable prognostic scoring system not only before the EMA but also after the EMA restriction. They obtained the referred score using four parameters as: neutrophil-to-lymphocyte ratio (< vs. ≥ 3.1), ECOG performance status (0–1 vs. 2–3), number of BM (< vs. ≥ 6) and AP (< vs. ≥ 220) and identifying three distinctive prognostic groups (low-risk, intermediate-risk and high-risk). In the Kitahima et al. [58] nomogram, unfavorable prognosis in patients treated with 223Ra after the EMA amendment was based on some characteristics such as pre-treatment with chemotherapy, lymphadenopathies, high BM tumor burden (depicted by the number of BM at the BS and PSA levels), and low hemoglobin levels. Notably, a more advanced disease was associated with lower OS. We consider that the novel nomograms developed in the present study, using FCH PET/CT, to predict therapeutic failure and prognosis following 223Ra treatment is important for the selection of eligible patients who would receive the greatest benefit. In the therapeutic failure nomogram, baseline AP and character of BM on CT (osteoblastic vs the rest) were robust predictive variables. So non-predominant osteogenic BM and high values of AP were associated to poorer response and treatment discontinuation due to progressive disease. This result is well supported by the biological mechanism of 223Ra and the direct association of osteoblastic disease and AP levels. Thus, these results highlight the importance of an integral evaluation of PET positive BM and their correspondence on CT [75,76].
On the other hand, in the OS nomogram, several variables after multiple readjustments could be incorporated, such as therapeutic failure, number of therapeutic lines after 223Ra treatment, average SUVmax, bone marrow involvement on baseline FCH PET/CT (C pattern) and categorical interim response on FCH PET/CT (progression vs no progression). SE during and after 223Ra treatment, contrary to ERA derived publication [6], was associated with an increase in OS in our population, possibly because longer patient survival conditions their appearance in patients with a damaged bone health based on bone destruction by BM and secondary osteoporosis. However, we extracted this variable from the nomogram considering that SE is a consequence of the survival but not the contrary. Similarly, the higher the patient survival higher is the probability to receive additional therapeutic lines. Lastly, the inclusion of FCH PET/CT as the only significant imaging variable in the nomogram highlights the potential importance of this technique in patients with 223Ra treatment indication.
This study has some limitations, such as the fact that not all patients were evaluated with both imaging techniques and the limited sample of response scans, specially end-treatments studies, mainly explained by the high rate of progression and therapeutic failure. Additionally, although the same experts assessed the studies, some scans were acquired using different equipments, which could limit more reliable comparisons. In BS only planar images were obtained in most of the patients that restrict an effective comparison with a pure tomographic technique as PET/CT. However, to partially palliate this limitation, only maximum intensity projection images were considered for BM classification on FCH PET/CT. Moreover, no standardization exists regarding the therapeutic management after 223Ra treatment. This heterogeneity could affect the OS results. Lastly, no external validation of this nomogram has been performed.
Under the current EMA guidance, patients are offered 223Ra at a later stage in their treatment pathway. The current personalizing medicine demands the creation of validated and simple models for clinicians to assess, which patients will most likely benefit from 223Ra treatment. This justifies the need to find advanced and novel tools that allow for patient selection and earlier evaluation of response or progression to treatment. The hypothesis that the higher diagnostic accuracy of PET/CT radiotracers, as FCH, will lead to better patient selection and, therefore, impact patient’s outcome of the proposed treatment is the cornerstone of the present investigation. In addition, this study reveals that SE seem not to have a detrimental influence on patient survival.
Conclusions
The present work aimed to establish a nomogram, adding FCH PET/CT to different clinical variables, for determining which patients would obtain the maximum benefit from 223Ra treatment, reducing as much as possible therapeutic failure and early death. Baseline FCH PET/CT seems a more robust predictive and prognostic imaging variable compared to BS whereas baseline AP and a non-dominant osteoblastic pattern in CT of PET/ CT seem to have relevance in the prediction of 223Ra treatment discontinuation. Interesting, therapy related variables and baseline and interim FCH PET/CT played role in defining OS in our sample of patients. Thus, FCH PET/CT, irrespective current conventional imaging techniques, could guide clinical decision-making on continuation of 223Ra treatment in patients with CRPC with BM although the results need to be discussed and validated in future works based on new imaging tools
References
- Parker, C.; Castro, E.; Fizazi, K.; Heidenreich, A.; Ost, P.; Procopio, G.; Tombal, B.; Gillessen, S. ESMO Guidelines Committee. Prostate Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2020, 31, 1119–1134. [Google Scholar] [CrossRef]
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Eberli, D.; De Meerleer, G.; De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer-2023.
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D'Amico, A.V.; et al. Prostate Cancer, Version 4.2023, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2023, 21, 1067–1096. [Google Scholar] [CrossRef] [PubMed]
- Lowrance, W.; Dreicer, R.; Jarrard, D.F.; Scarpato, K.R.; Kim, S.K.; Kirkby, E.; Buckley, D.I.; Griffin, J.C.; Cookson, M.S. Updates to Advanced Prostate Cancer: AUA/SUO Guideline. J. Urol. 2023, 209, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fossa, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef]
- Smith, M.; Parker, C.; Saad, F.; Miller, K.; Tombal, B.; Ng, Q.S.; Boegemann, M.; Matveev, V.; Piulats, J.M.; Zucca, L.E.; et al. Addition of radium-223 to abiraterone acetate and prednisone or prednisolone in patients with castration-resistant prostate cancer and bone metastases (ERA 223): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 408–419. [Google Scholar] [CrossRef]
- Brady, D.; Parker, C.C.; O’Sullivan, J.M. Bone-targeting radiopharmaceuticals including radium-223. Cancer J. 2013, 19, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Fuccio, C.; Castellucci, P.; Schiavina, R.; Guidalotti, P.L.; Gavaruzzi, G.; Montini, G.C.; Nanni, C.; Marzola, M.C.; Rubello, D.; Fanti, S. Role of 11C-choline PET/CT in the restaging of prostate cancer patients with biochemical relapse and negative results at bone scintigraphy. Eur. J. Radiol. 2012, 81, e893–e896. [Google Scholar] [CrossRef]
- Beheshti, M.; Vali, R.; Waldenberger, P.; Fitz, F.; Nader, M.; Loidl, W.; Broinger, G.; Stoiber, F.; Foglman, I.; Langsteger, W. Detection of bone metastases in patients with prostate cancer by 18F fluorocholine and 18F fluoride PET-CT: A comparative study. Eur J Nucl Med Mol Imaging 2008, 35, 1766–1774. [Google Scholar] [CrossRef]
- García Vicente, A.M.; Amo-Salas, M.; Cassinello Espinosa, J.; Gómez Díaz, R.; Soriano Castrejón, Á. Interim and end-treatment 18F-Fluorocholine PET/CT and bone scan in prostate cancer patients treated with Radium 223 dichloride. Sci. Rep. 2021, 11, 7389. [Google Scholar] [CrossRef]
- García Vicente, A.M.; González García, B.; Amo-Salas, M.; García Carbonero, I.; Cassinello Espinosa, J.; Gómez-Aldaraví Gutierrez, J.L.; Suarez Hinojosa, L.; Soriano Castrejón, Á. Baseline 18F-Fluorocholine PET/CT and bone scan in the outcome prediction of patients treated with radium 223 dichloride. Clin. Transl. Oncol. 2019, 21, 289–297. [Google Scholar] [CrossRef]
- Sartor, O.; Coleman, R.E.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Vogelzang, N.J.; Bruland, O.; Kobina, S.; Wilhelm, S.; et al. An exploratory analysis of alkaline phosphatase, lactate dehydrogenase, and prostate-specific antigen dynamics in the phase 3 ALSYMPCA trial with radium-223. Ann. Oncol. 2017, 28, 1090–1097. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, D.; Bruland, O.; Guise, T.A.; Suzuki, H.; Sartor, O. Alkaline phosphatase in metastatic castration-resistant prostate cancer: Reassessment of an older biomarker. Future Oncol. 2018, 14, 2543–2556. [Google Scholar] [CrossRef] [PubMed]
- Alva, A.; Nordquist, L.; Daignault, S.; George, S.; Ramos, J.; Albany, C.; Isharwal, S.; McDonald, M.; Campbell, G.; Danchaivijitr, P.; et al. Clinical Correlates of Benefit from Radium-223 Therapy in Metastatic Castration Resistant Prostate Cancer. Prostate 2017, 77, 479–488. [Google Scholar] [CrossRef]
- Fosbøl, M.Ø.; Petersen, P.M.; Kjaer, A.; Mortensen, J. 223Ra Therapy of Advanced Metastatic Castration-Resistant Prostate Cancer: Quantitative Assessment of Skeletal Tumor Burden for Prognostication of Clinical Outcome and Hematologic Toxicity. J. Nucl. Med. 2018, 59, 596–602. [Google Scholar] [CrossRef]
- Kitajima, K.; Igeta, M.; Kuyama, J.; Kawahara, T.; Suga, T.; Otani, T.; Sugawara, S.; Kono, Y.; Tamaki, Y.; Seko-Nitta, A.; et al. Novel nomogram developed for determining suitability of metastatic castration-resistant prostate cancer patients to receive maximum benefit from radium-223 dichloride treatment-Japanese Ra-223 Therapy in Prostate Cancer using Bone Scan Index (J-RAP-BSI) Trial. Eur. J. Nucl. Med. Mol. Imaging. 2023, 50, 1487–1498. [Google Scholar]
- Shariftabrizi A, Kothari S, George S, Attwood K, Levine E, Lamonica D. Optimization of Radium-223 Treatment for Castration-resistant Prostate Cancer: Insights from Skeletal Metastasis Burden and Clinical Parameters. Cancers 2023, 28, 246–251. [Google Scholar]
- Crawford, E.D.; Petrylak, D.P.; Shore, N.; Saad, F.; Slovin, S.F.; Vogelzang, N.J.; Keane, T.E.; Koo, P.J.; Gomella, L.G.; O'Sullivan, J.M.; et al. Prostate Cancer Radiographic Assessments for Detection of Advanced Recurrence (RADAR II) Group. The Role of Therapeutic Layering in Optimizing Treatment for Patients With Castration-resistant Prostate Cancer (Prostate Cancer Radiographic Assessments for Detection of Advanced Recurrence II). Urology 2017, 104, 150–159.
- Slack, N.H.; Karr, J.P.; Chu, T.M.; Murphy, G.P. An assessment of bone scans for monitoring osseous metastases in patients being treated for prostate carcinoma. Prostate. 1980, 1, 259–270. [Google Scholar] [CrossRef]
- Young, H.; Baum, R.; Cremerius, U.; Herholz, K.; Hoekstra, O.; Lammertsma, A.A.; Pruim, J.; Price, P. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: Review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur J Cancer. 1999, 35, 1773–1782.
- European Medicines Agency (EMA). (2020). Provisional assessment report: Provisional measures under Article 20 - XOFIGO (H-20-1459-C-002653-0028). Retrieved from https://www.ema.europa.eu/en/documents/variation-report/xofigo-h-20-1459-c-002653-0028-epar-assessment-report-provisional-measures-article-20_en.pdf.
- Parikh, S.; Murray, L.; Kenning, L.; Bottomley, D.; Din, O.; Dixit, S.; Ferguson, C.; Handforth, C.; Joseph, L.; Mokhtar, D.; et al. Real-world Outcomes and Factors Predicting Survival and Completion of Radium 223 in Metastatic Castrate-resistant Prostate Cancer. Clin. Oncol. 2018, 30, 548–555. [Google Scholar] [CrossRef]
- Wong, W.W.; Anderson, E.M.; Mohammadi, H.; Daniels, T.B.; Schild, S.E.; Keole, S.R.; Choo, C.R.; Tzou, K.S.; Bryce, A.H.; Ho, T.H.; et al. Factors Associated with Survival Following Radium-223 Treatment for Metastatic Castration-resistant Prostate Cancer. Clin. Genitourin. Cancer 2017, 15, e969–e975. [Google Scholar] [CrossRef]
- Kuppen, M.C.; Westgeest, H.M.; van der Doelen, M.J.; van den Eertwegh, A.J.; Coenen, J.L.; Aben, K.K.; van den Bergh, A.C.; Bergman, A.M.; den Bosch, J.V.; Celik, F.; et al. Real-world outcomes of radium-223 dichloride for metastatic castration resistant prostate cancer. Future Oncol. 2020, 16, 1371–1384. [Google Scholar] [CrossRef]
- Frantellizzi, V.; Farcomeni, A.; Follacchio, G.A.; Pacilio, M.; Pellegrini, R.; Pani, R.; De Vincentis, G. A 3-variable prognostic score (3-PS) for overall survival prediction in metastatic castration-resistant prostate cancer treated with 223Radium-dichloride. Ann. Nucl. Med. 2018, 32, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Bauckneht, M.; Rebuzzi, S.E.; Ponzano, M.; Borea, R.; Signori, A.; Frantellizzi, V.; Lodi Rizzini, E.; Mascia, M.; Lavelli, V.; Miceli, A.; et al. Prognostic Value of the BIO-Ra Score in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223 after the European Medicines Agency Restricted Use: Secondary Investigations of the Multicentric BIO-Ra Study. Cancers 2022, 14, 1744. [Google Scholar] [CrossRef] [PubMed]
- van der Doelen, M.J.; Oving, I.M.; Wyndaele, D.N.J.; van Basten, J.P.; Terheggen, F.; van de Luijtgaarden, A.C.M.; Oyen, W.J.G.; van Schelven, W.D.; van den Berkmortel, F.; Mehra, N.; et al. Health-Related Quality of Life, Psychological Distress, and Fatigue in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223 Therapy. Prostate Cancer Prostatic Dis. 2023, 26, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Ge, R.; Wang, Z.; Cheng, L. Tumor microenvironment heterogeneity an important mediator of prostate cancer progression and therapeutic resistance. NPJ Precis. Oncol. 2022, 6, 31. [Google Scholar] [CrossRef] [PubMed]
- Tolkach, Y.; Kristiansen, G. The Heterogeneity of Prostate Cancer: A Practical Approach. Pathobiology 2018, 85, 108–116. [Google Scholar]
- Yamamoto, Y.; Okuda, Y.; Kanaki, T.; Tanaka, R.; Nagahara, A.; Nakai, Y.; Nakayama, M.; Kakimoto, K.I.; Nishimura, K. Clinical indicators for predicting prognosis after radium-223 administration in castration-resistant prostate cancer with bone metastases. Int J Clin Oncol. 2021, 26, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Palmedo, H.; Ahmadzadehfar, H.; Eschmann, S.; Niesen, A.; Schönberger, J.; Barsegian, V.; Liepe, K.; Mottaghy, F.M.; Guan, R.; Pinkert, J.; et al. Pain Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with 223Ra: PARABO, a Prospective, Noninterventional Study. J. Nucl. Med. 2023, 64, 1392–1398. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Carles, J.; Gillessen, S.; Heidenreich, A.; Heinrich, D.; Gratt, J.; Lévy, J.; Miller, K.; Nilsson, S.; Petrenciuc, O.; et al. Radium-223 International Early Access Program Investigators. Radium-223 and concomitant therapies in patients with metastatic castration-resistant prostate cancer: An international, early access, open-label, single-arm phase 3b trial. Lancet Oncol, 2016; 17, 1306–1316. [Google Scholar]
- Ramos, J.D.; Mostaghel, E.A.; Pritchard, C.C.; Yu, E.Y. DNA Repair Pathway Alterations in Metastatic Castration-resistant Prostate Cancer Responders to Radium-223. Clin. Genitourin. Cancer 2018, 16, 106–110. [Google Scholar] [CrossRef]
- Steinberger, A.E.; Cotogno, P.; Ledet, E.M.; Lewis, B.; Sartor, O. Exceptional Duration of Radium-223 in Prostate Cancer with a BRCA2 Mutation. Clin. Genitourin. Cancer. 2017, 15, e69–e71. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Anand, A.; Edenbrandt, L.; Bondesson, E.; Bjartell, A.; Widmark, A.; Sternberg, C.N.; Pili, R.; Tuvesson, H.; Nordle, Ö.; et al. Phase 3 Assessment of the Automated Bone Scan Index as a Prognostic Imaging Biomarker of Overall Survival in Men with Metastatic Castration-Resistant Prostate Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2018, 4, 944–951. [Google Scholar] [CrossRef]
- van der Zande, K.; Oyen, W.J.G.; Zwart, W.; Bergman, A.M. Radium-223 Treatment of Patients with Metastatic Castration Resistant Prostate Cancer: Biomarkers for Stratification and Response Evaluation. Cancers 2021, 13, 4346. [Google Scholar] [CrossRef]
- de Jong, A.C.; Segbers, M.; Ling, S.W.; Graven, L.H.; Mehra, N.; Hamberg, P.; Brabander, T.; de Wit, R.; van der Veldt, A.A.M. 68Ga-PSMA PET/CT for Response Evaluation of 223Ra Treatment in Metastatic Prostate Cancer. J. Nucl. Med. 2023, 64, 1556–1562. [Google Scholar] [CrossRef]
- Donners, R.; Tunariu, N.; Tovey, H.; Hall, E.; Chua, S.; Cook, G.; Du, Y.; Blackledge, M.D.; Parker, C.C.; Koh, D.M. The value of baseline 18F-sodium fluoride and 18F-choline PET activity for identifying responders to radium-223 treatment in castration-resistant prostate cancer bone metastases. Eur. Radiol. 2024, 34, 1146–1154. [Google Scholar] [CrossRef]
- Fuccio, C.; Castellucci, P.; Schiavina, R.; Santi, I.; Allegri, V.; Pettinato, V.; Boschi, S.; Martorana, G.; Al-Nahhas, A.; Rubello, D.; et al. Role of 11C-choline PET/CT in the restaging of prostate cancer patients showing a single lesion on bone scintigraphy. Ann. Nucl. Med. 2010, 24, 485–492. [Google Scholar] [CrossRef]
- Bosch, D.; van der Velden, K.J.M.; Oving, I.M.; Wyndaele, D.N.J.; Weijs, L.E.; van Schelven, W.D.; Oyen, W.J.G.; Te Beek, E.T.; van de Luijtgaarden, A.C.M.; Somford, D.M.; et al. The Impact of Baseline PSMA PET/CT Versus CT on Outcomes of 223Ra Therapy in Metastatic Castration-Resistant Prostate Cancer Patients. J. Nucl. Med. 2024, 65, 541–547. [Google Scholar] [CrossRef]
- Filippi, L.; Spinelli, G.P.; Chiaravalloti, A.; Schillaci, O.; Equitani, F.; Bagni, O. Prognostic Value of 18F-Choline PET/CT in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Radium-223. Biomedicines 2020, 8, 555. [Google Scholar] [CrossRef]
- Maines, F.; Caffo, O.; Donner, D.; Sperduti, I.; Bria, E.; Veccia, A.; Chierichetti, F.; Tortora, G.; Galligioni, E. Serial 18F-choline-PET Imaging in Patients Receiving Enzalutamide for Metastatic Castration-Resistant Prostate Cancer: Response Assessment and Imaging Biomarkers. Future Oncol. 2016, 12, 333–342. [Google Scholar] [CrossRef]
- Caroli, P.; De Giorgi, U.; Scarpi, E.; Fantini, L.; Moretti, A.; Galassi, R.; Celli, M.; Conteduca, V.; Rossi, L.; Bianchi, E.; et al. Prognostic value of 18F-choline PET/CT metabolic parameters in patients with metastatic castration-resistant prostate cancer treated with abiraterone or enzalutamide. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 348–354. [Google Scholar] [CrossRef]
- Vija Racaru, L.; Sinigaglia, M.; Kanoun, S.; Ben Bouallègue, F.; Tal, I.; Brillouet, S.; Bauriaud-Mallet, M.; Zerdoud, S.; Dierickx, L.; Vallot, D.; et al. Fluorine-18-fluorocholine PET/CT parameters predictive for hematological toxicity to radium-223 therapy in castrate-resistant prostate cancer patients with bone metastases: A pilot study. Nucl. Med. Commun. 2018, 39, 672–679. [Google Scholar] [CrossRef]
- Quaquarini, E.; D’Ambrosio, D.; Sottotetti, F.; Gallivanone, F.; Hodolic, M.; Baiardi, P.; Palumbo, R.; Vellani, C.; Canevari, C.; Bernardo, A.; et al. Prognostic Value of 18 F-Fluorocholine PET Parameters in Metastatic Castrate-Resistant Prostate Cancer Patients Treated with Docetaxel. Contrast Media Mol. Imaging 2019, 1–7. [Google Scholar] [CrossRef]
- Letellier, A.; Johnson, A.C.; Kit, N.H.; Savigny, J.F.; Batalla, A.; Parienti, J.J.; Aide, N. Uptake of Radium-223 Dichloride and Early [18F]NaF PET Response Are Driven by Baseline [18F]NaF Parameters: A Pilot Study in Castration-Resistant Prostate Cancer Patients. Mol Imaging Biol. 2018, 20, 482–491. [Google Scholar] [CrossRef]
- Maines, F.; Caffo, O.; Donner, D.; Sperduti, I.; Bria, E.; Veccia, A.; Chierichetti, F.; Tortora, G.; Galligioni, E. Serial 18F-choline-PET imaging in patients receiving enzalutamide for metastatic castration-resistant prostate cancer: Response assessment and imaging biomarkers. Future Oncol. 2016, 12, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Etchebehere, E.C.; Araujo, J.C.; Fox, P.S.; Swanston, N.M.; Macapinlac, H.A.; Rohren, E.M. Prognostic factors in patients treated with 223Ra: The role of skeletal tumor burden on baseline 18F-fluoride PET/CT in predicting overall survival. J. Nucl. Med. 2015, 56, 1177–1184. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Azgomi, K.; Hauser, S.; Wei, X.; Yordanova, A.; Gaertner, F.C.; Kürpig, S.; Strunk, H.; Essler, M. 68Ga-PSMA-11 PET as a Gatekeeper for the Treatment of Metastatic Prostate Cancer with 223Ra: Proof of Concept. J. Nucl. Med. 2017, 58, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Anand, A.; Trägårdh, E.; Edenbrandt, L.; Beckman, L.; Svensson, J.H.; Thellenberg, C.; Widmark, A.; Kindblom, J.; Ullén, A.; Bjartell, A. Assessing Radiographic Response to 223Ra with an Automated Bone Scan Index in Metastatic Castration-Resistant Prostate Cancer Patients. J. Nucl. Med. 2020, 61, 671–675. [Google Scholar] [CrossRef] [PubMed]
- van der Doelen, M.J.; Stockhaus, A.; Ma, Y.; Mehra, N.; Yachnin, J.; Gerritsen, W.R.; Nilsson, S.; van Oort, I.M.; Ullén, A. Early alkaline phosphatase dynamics as biomarker of survival in metastatic castration-resistant prostate cancer patients treated with radium-223. Eur J Nucl Med Mol Imaging. 2021, 48, 3325–3334. [Google Scholar] [CrossRef] [PubMed]
- Gafita, A.; Rauscher, I.; Weber, M.; Hadaschik, B.; Wang, H.; Armstrong, W.R.; Tauber, R.; Grogan, T.R.; Czernin, J.; Rettig, M.B.; et al. Novel Framework for Treatment Response Evaluation Using PSMA PET/CT in Patients with Metastatic Castration-Resistant Prostate Cancer (RECIP 1.0): An International Multicenter Study. J. Nucl. Med. 2022, 63, 1651–1658. [Google Scholar] [PubMed]
- Fanti, S.; Hadaschik, B.; Herrmann, K. Proposal for Systemic-Therapy Response-Assessment Criteria at the Time of PSMA PET/CT Imaging: The PSMA PET Progression Criteria. J. Nucl. Med. 2020, 61, 678–682. [Google Scholar] [CrossRef] [PubMed]
- Fanti, S.; Goffin, K.; Hadaschik, B.A.; Herrmann, K.; Maurer, T.; MacLennan, S.; Oprea-Lager, D.E.; Oyen, W.J.; Rouvière, O.; Mottet, N.; et al. Consensus Statements on PSMA PET/CT Response Assessment Criteria in Prostate Cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Lange, P.H.; Vessella, R.L. Mechanisms, hypotheses and questions regarding prostate cancer micrometastases to bone. Cancer Metastasis Rev. 1998, 17, 331–336. [Google Scholar] [CrossRef]
- Parker, C.C.; Coleman, R.E.; Sartor, O.; Vogelzang, N.J.; Bottomley, D.; Heinrich, D.; Helle, S.I.; O'Sullivan, J.M.; Fossà, S.D.; Chodacki, A.; et al. Three-year Safety of Radium-223 Dichloride in Patients with Castration-resistant Prostate Cancer and Symptomatic Bone Metastases from Phase 3 Randomized Alpharadin in Symptomatic Prostate Cancer Trial. Eur. Urol. 2018, 73, 427–435. [Google Scholar] [CrossRef]
- Sartor, O.; Coleman, R.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O'Sullivan, J.M.; Fosså, S.D.; Chodacki, A.; Wiechno, P.; Logue, J. Effect of radium-223 dichloride on symptomatic skeletal events in patients with castration-resistant prostate cancer and bone metastases: Results from a phase 3, double-blind, randomised trial. Lancet Oncol. 2014, 15, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, K.; Kuyama, J.; Kawahara, T.; Suga, T.; Otani, T.; Sugawara, S.; Kono, Y.; Tamaki, Y.; Seko-Nitta, A.; Ishiwata, Y.; et al. Assessing Therapeutic Response to Radium-223 with an Automated Bone Scan Index among Metastatic Castration-Resistant Prostate Cancer Patients: Data from Patients in the J-RAP-BSI Trial. Cancers 2023, 15, 2784. [Google Scholar] [CrossRef] [PubMed]
- van der Doelen, M.J.; Kuppen, M.C.P.; Jonker, M.A.; Mehra, N.; Janssen, M.J.R.; van Oort, I.M.; Gerritsen, W.R. 223Ra Therapy in Patients With Advanced Castration-Resistant Prostate Cancer With Bone Metastases: Lessons from Daily Practice. Clin. Nucl. Med. 2018, 43, 9–16. [Google Scholar] [CrossRef] [PubMed]
- McKay, R.R.; Jacobus, S.; Fiorillo, M.; Ledet, E.M.; Cotogna, P.M.; Steinberger, A.E.; Jacene, H.A.; Sartor, O.; Taplin, M.E. Radium-223 Use in Clinical Practice and Variables Associated With Completion of Therapy. Clin. Genitourin. Cancer 2017, 15, e289–e298. [Google Scholar] [CrossRef] [PubMed]
- Alva, A.; Nordquist, L.; Daignault, S.; George, S.; Ramos, J.; Albany, C.; Isharwal, S.; McDonald, M.; Campbell, G.; Danchaivijitr, P.; et al. Clinical Correlates of Benefit From Radium-223 Therapy in Metastatic Castration Resistant Prostate Cancer. Prostate 2017, 77, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Carles, J.; Gillessen, S.; Heidenreich, A.; Heinrich, D.; Gratt, J.; Lévy, J.; Miller, K.; Nilsson, S.; Petrenciuc, O.; et al. Radium-223 International Early Access Program Investigators. Radium-223 and Concomitant Therapies in Patients with Metastatic Castration-Resistant Prostate Cancer: An International, Early Access, Open-Label, Single-Arm Phase 3b Trial. Lancet Oncol. 1306. [Google Scholar]
- Hashimoto, K.; Miyoshi, Y.; Shindo, T.; Hori, M.; Tsuboi, Y.; Kobayashi, K.; Fukuta, F.; Tanaka, T.; Miyamoto, S.; Maehana, T.; et al. Dynamic Changes of Bone Metastasis Predict Bone-Predominant Status to Benefit from Radium-223 Dichloride for Patients with Castration-Resistant Prostate Cancer. Cancer Med. 2020, 9, 8579–8588. [Google Scholar] [CrossRef] [PubMed]
- Anand, A.; Trägårdh, E.; Edenbrandt, L.; Beckman, L.; Svensson, J.-H.; Thellenberg, C.; Widmark, A.; Kindblom, J.; Ullén, A.; Bjartell, A. Assessing Radiographic Response to 223Ra with an Automated Bone Scan Index in Metastatic Castration-Resistant Prostate Cancer Patients. J. Nucl. Med. 2020, 61, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, Y.; Tsutsumi, S.; Yasui, M.; Kawahara, T.; Uemura, K.I.; Hayashi, N.; Nozawa, M.; Yoshimura, K.; Uemura, H.; Uemura, H. A Novel Prediction Model for the Completion of Six Cycles of Radium-223 Treatment and Survival in Patients with Metastatic Castration-Resistant Prostate Cancer. World J. Urol. 2021, 39, 3323–3328. [Google Scholar] [CrossRef] [PubMed]
- Frantellizzi, V.; Pani, A.; Ippoliti, M.D.; Farcomeni, A.; Aloise, I.; Colosi, M.; Polito, C.; Pani, R.; Vincentis, G. Scintigraphic Load of Bone Disease Evaluated by DASciS Software as a Survival Predictor in Metastatic Castration-Resistant Prostate Cancer Patients Candidates to 223RaCl Treatment. Radiol. Oncol. 2019, 54, 40–47. [Google Scholar] [CrossRef]
- Nakashima, K.; Makino, T.; Kadomoto, S.; Iwamoto, H.; Yaegashi, H.; Iijima, M.; Kawaguchi, S.; Nohara, T.; Shigehara, K.; Izumi, K.; et al. Initial Experience with Radium-223 Chloride Treatment at the Kanazawa University Hospital. Anticancer. Res. 2019, 39, 2607–2614. [Google Scholar] [CrossRef]
- Frantellizzi, V.; Monari, F.; Mascia, M.; Costa, R.; Rubini, G.; Spanu, A.; Di Rocco, A.; Lodi Rizzini, E.; Cindolo, L.; Licari, M.; et al. Validation of the 3-Variable Prognostic Score (3-PS) in mCRPC Patients Treated with 223Radium-Dichloride: A National Multicenter Study. Ann. Nucl. Med. 2020, 34, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Buscombe, J.; Gillett, D.; Bird, N.; Powell, A.; Heard, S.; Aloj, L. Quantifying the Survival Benefit of Completing All Six Cycles of Radium-223 Therapy in Patients With Castrate-Resistant Prostate Cancer With Predominant Bone Metastases. World J. Nucl. Med. 2020, 20, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Dadhania, S.; Alonzi, R.; Douglas, S.; Gogbashian, A.; Hughes, R.; Dalili, D.; Vasdev, N.; Adshead, J.; Lane, T.; Westbury, C.; et al. Single-centre experience of use of radium 223 with clinical outcomes based on number of cycles and bone marrow toxicity. Anticancer. Res. 2018, 38, 5423–5427. [Google Scholar] [CrossRef] [PubMed]
- Uemura, H.; Uemura, H.; Nagamori, S.; Wakumoto, Y.; Kimura, G.; Kikukawa, H.; Yokomizo, A.; Mizokami, A.; Kosaka, T.; Masumori, N.; et al. Three-year follow-up of a phase II study of radium-223 dichloride in Japanese patients with symptomatic castration-resistant prostate cancer and bone metastases. Int. J. Clin. Oncol. 2019, 24, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, D.; Hatakeyama, S.; Kawaguchi, H.; Hatayama, Y.; Ishibashi, Y.; Kusaka, A.; Noro, D.; Tanaka, T.; Ito, H.; Okuyama, Y.; et al. Effects of six-cycle completion and earlier use of radium-223 therapy on prognosis for metastatic castration-resistant prostate cancer: A real-world multicenter retrospective study. Urol. Oncol. Semin. Orig. Investig. 2022, 40, 64.e1–64.e8. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Arciero, V.; Goldberg, H.; Tajzler, C.; Manganaro, A.; Kozlowski, N.; Rowbottom, L.; McDonald, R.; Chow, R.; Vasisht, G.; et al. Population-based analysis of the use of radium-223 for bone-metastatic castration-resistant prostate cancer in Ontario, and of factors associated with treatment completion and outcome. Cancer Manag. Res. 2019, 11, 9307–9319. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, M.; Buscombe, J.R.; Jacene, H.A.; Klitzke, A.K.; Lamonica, D.; Lu, Y.; Pryma, D.A.; Rohren, E.M.; Speer, T.W.; Subramaniam, R.M.; et al. ACR-ACNM-ASTRO-SNMMI practice parameter for the performance of therapy with radium-223. Am. J. Clin. Oncol. 2020, 43, 539–544. [Google Scholar] [CrossRef]
- Wymenga, L.F.; Boomsma, J.H.; Groenier, K.; Piers, D.A.; Mensink, H.J. Routine bone scans in patients with prostate cancer related to serum prostate-specific antigen and alkaline phosphatase. BJU Int. 2001, 88, 226–230. [Google Scholar] [CrossRef]
- Ebrahim, T.; Hadebe, B.; Aldous, C.; Tinarwo, P.; Nyakale, N. Segmented linear correlations between bone scan index and prostate cancer biomarkers, alkaline phosphatase, and prostate specific antigen in patients with a Gleason score ≥7. Medicine 2022, 101, e29515. [Google Scholar] [CrossRef]
Figure 1.
Kaplan-Meier OS curves of baseline AP levels (upper left panel), LDH levels (upper right panel), and ECOG performance status (lower panel).
Figure 1.
Kaplan-Meier OS curves of baseline AP levels (upper left panel), LDH levels (upper right panel), and ECOG performance status (lower panel).
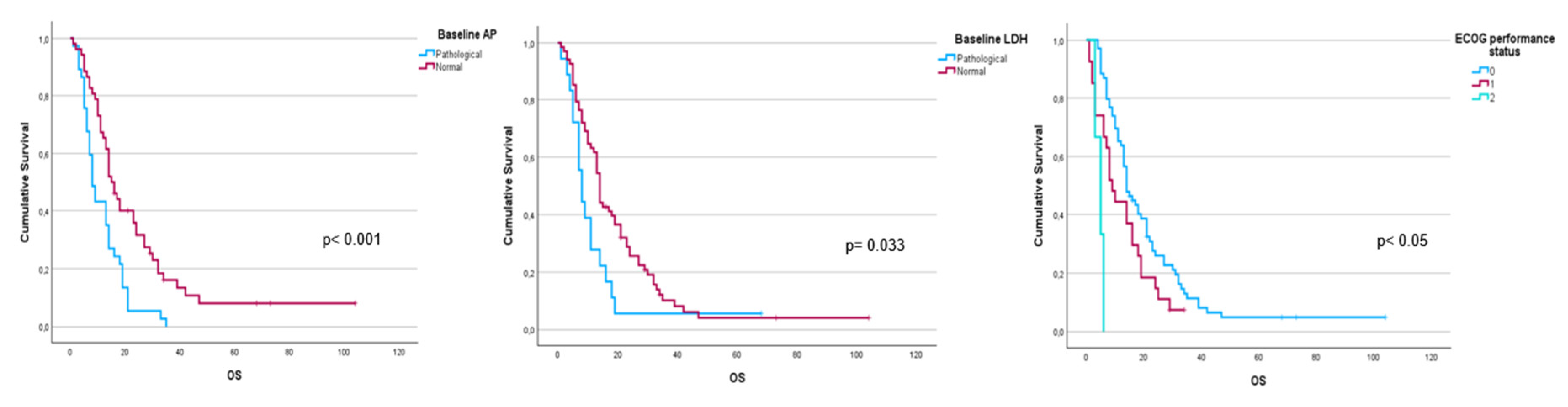
Figure 2.
Kaplan-Meier OS curves of baseline FCH PET/CT radiomics: high tumor burden (upper left panel), uptake higher than liver for the most hypermetabolic bone metastases (upper right panel), bone marrow involvement (lower left panel) and soft tissue involvement (lower right panel).
Figure 2.
Kaplan-Meier OS curves of baseline FCH PET/CT radiomics: high tumor burden (upper left panel), uptake higher than liver for the most hypermetabolic bone metastases (upper right panel), bone marrow involvement (lower left panel) and soft tissue involvement (lower right panel).
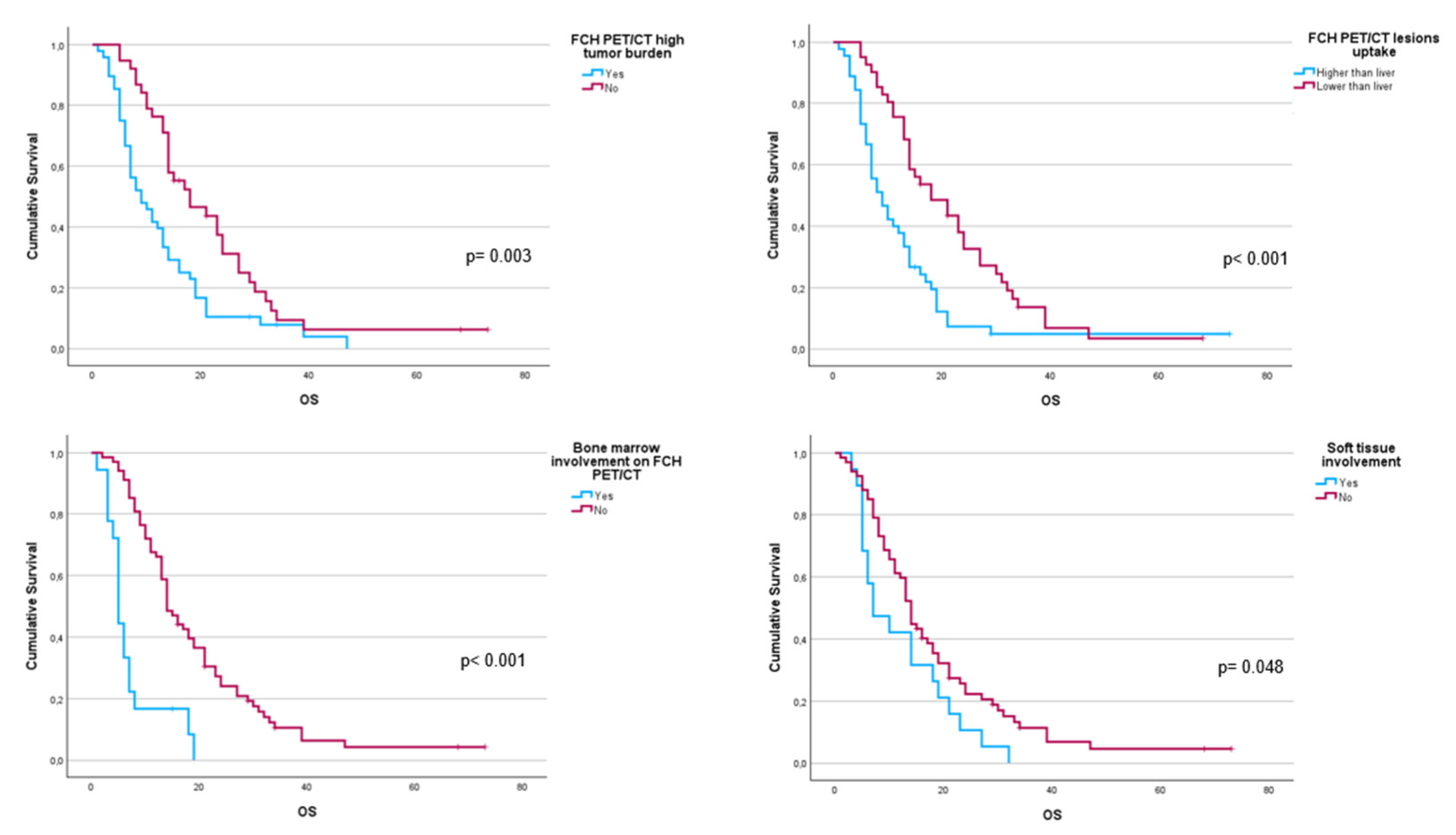
Figure 3.
Kaplan-Meier OS curves of binary response in interim FCH PET/CT scans (left panel) and BS (right panel).
Figure 3.
Kaplan-Meier OS curves of binary response in interim FCH PET/CT scans (left panel) and BS (right panel).
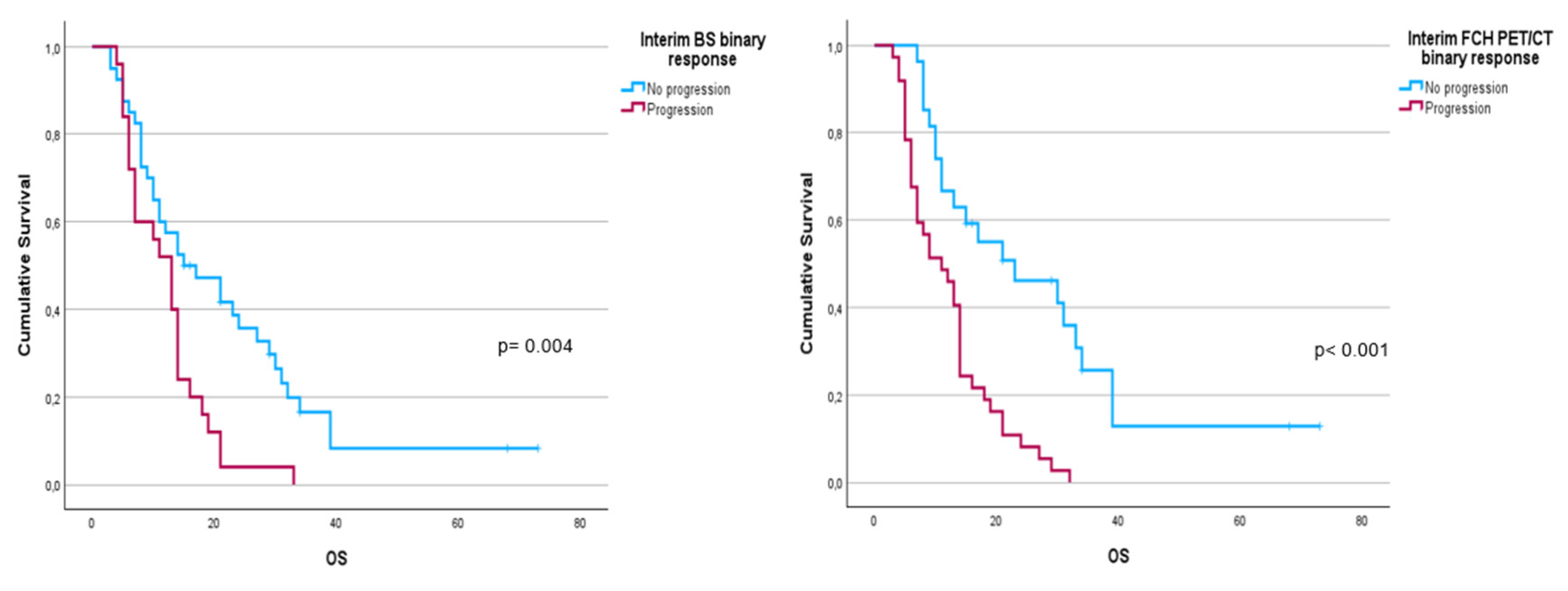
Figure 4.
Designed nomograms to predict therapeutic failure (left panel) and the probability of survival at 12 and 24 months (right panel). The nomograms were developed based on the 100 patients in our population with CRPC-BM who received 223Ra therapy. To obtain the probability of therapeutic failure and survival, the values for each variable of the patients included in each nomogram are marked. Then, a straight vertical line is drawn up to the “Points” line at the top of the nomogram. This determines how many points are attributed to each variable. Once this is done for each variable, the sum of all the points obtained is calculated and added to the “Total Points” line at the bottom of the nomogram. This value is then used to assess the individual probability of predicting the risk of therapeutic failure (left panel) and survival at 12 and 24 months (right panel).
Figure 4.
Designed nomograms to predict therapeutic failure (left panel) and the probability of survival at 12 and 24 months (right panel). The nomograms were developed based on the 100 patients in our population with CRPC-BM who received 223Ra therapy. To obtain the probability of therapeutic failure and survival, the values for each variable of the patients included in each nomogram are marked. Then, a straight vertical line is drawn up to the “Points” line at the top of the nomogram. This determines how many points are attributed to each variable. Once this is done for each variable, the sum of all the points obtained is calculated and added to the “Total Points” line at the bottom of the nomogram. This value is then used to assess the individual probability of predicting the risk of therapeutic failure (left panel) and survival at 12 and 24 months (right panel).
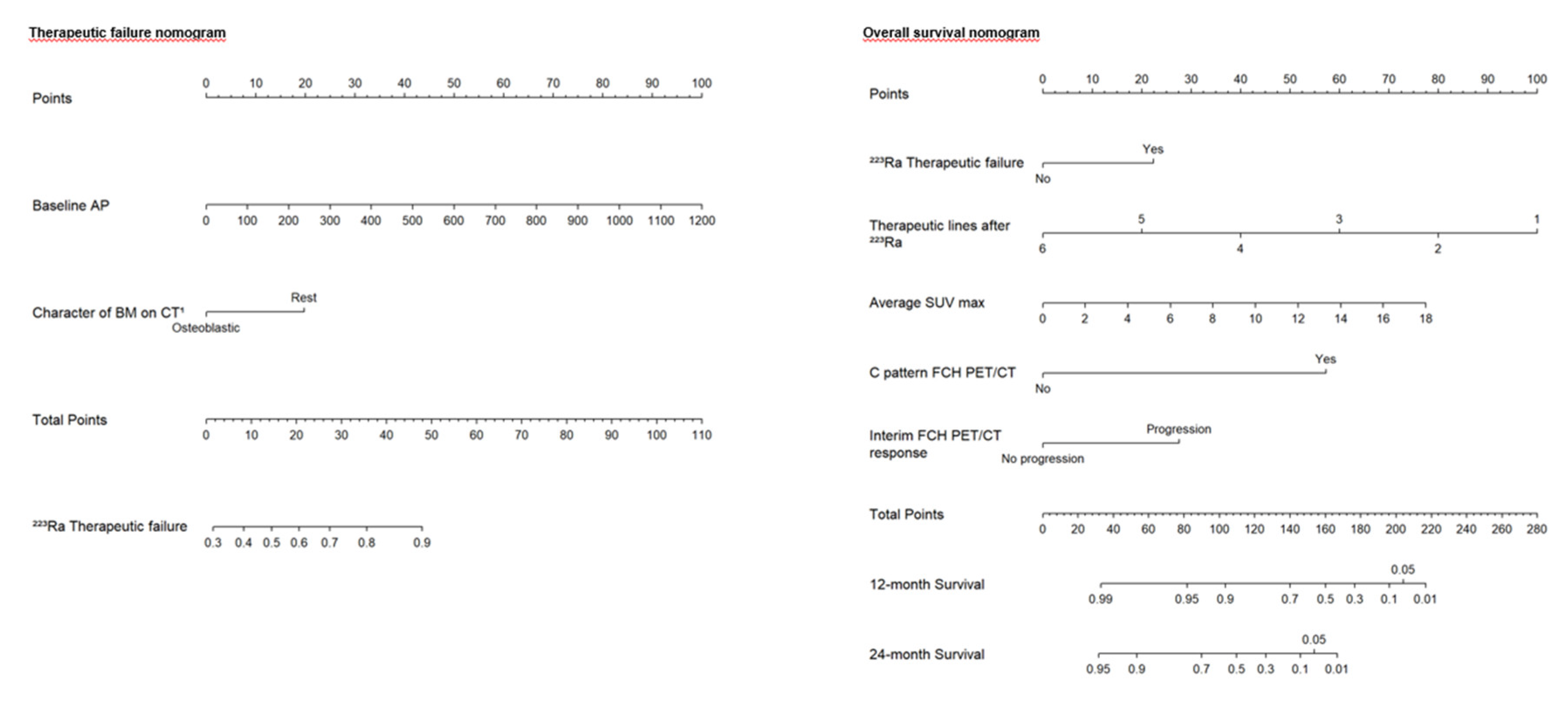
Figure 5.
Patient ≠ 1. 71-year-old man, diagnosed with prostate adenocarcinoma Gleason Score 9 (4+5), underwent prostatectomy followed by adjuvant radiotherapy to the surgical bed due to early PSA progression. Three years after diagnosis, bone metastases were detected, prompting the start of systemic treatment lines (Enzalutamide and Docetaxel). 223Ra was administered as third line. At the start of treatment, the patient was in good general condition (ECOG 0), experienced pain, and had baseline PSA levels of 50.7 ng/dL, AP of 377 IU/L, and LDH of 377 IU/L. Baseline BS (A) shows a polymetastatic disease (> 20 lesions) affecting both the axial and extra-axial skeleton. Baseline FCH PET/CT (B) shows the presence of mixed characteristic BM, bone marrow infiltration, uptake of the most hypermetabolic BM higher than liver and soft tissue involvement at the pelvic lymph nodes. The concordance between both studies was moderate, defining FCH PET/CT more BM with respect to BS.
Figure 5.
Patient ≠ 1. 71-year-old man, diagnosed with prostate adenocarcinoma Gleason Score 9 (4+5), underwent prostatectomy followed by adjuvant radiotherapy to the surgical bed due to early PSA progression. Three years after diagnosis, bone metastases were detected, prompting the start of systemic treatment lines (Enzalutamide and Docetaxel). 223Ra was administered as third line. At the start of treatment, the patient was in good general condition (ECOG 0), experienced pain, and had baseline PSA levels of 50.7 ng/dL, AP of 377 IU/L, and LDH of 377 IU/L. Baseline BS (A) shows a polymetastatic disease (> 20 lesions) affecting both the axial and extra-axial skeleton. Baseline FCH PET/CT (B) shows the presence of mixed characteristic BM, bone marrow infiltration, uptake of the most hypermetabolic BM higher than liver and soft tissue involvement at the pelvic lymph nodes. The concordance between both studies was moderate, defining FCH PET/CT more BM with respect to BS.
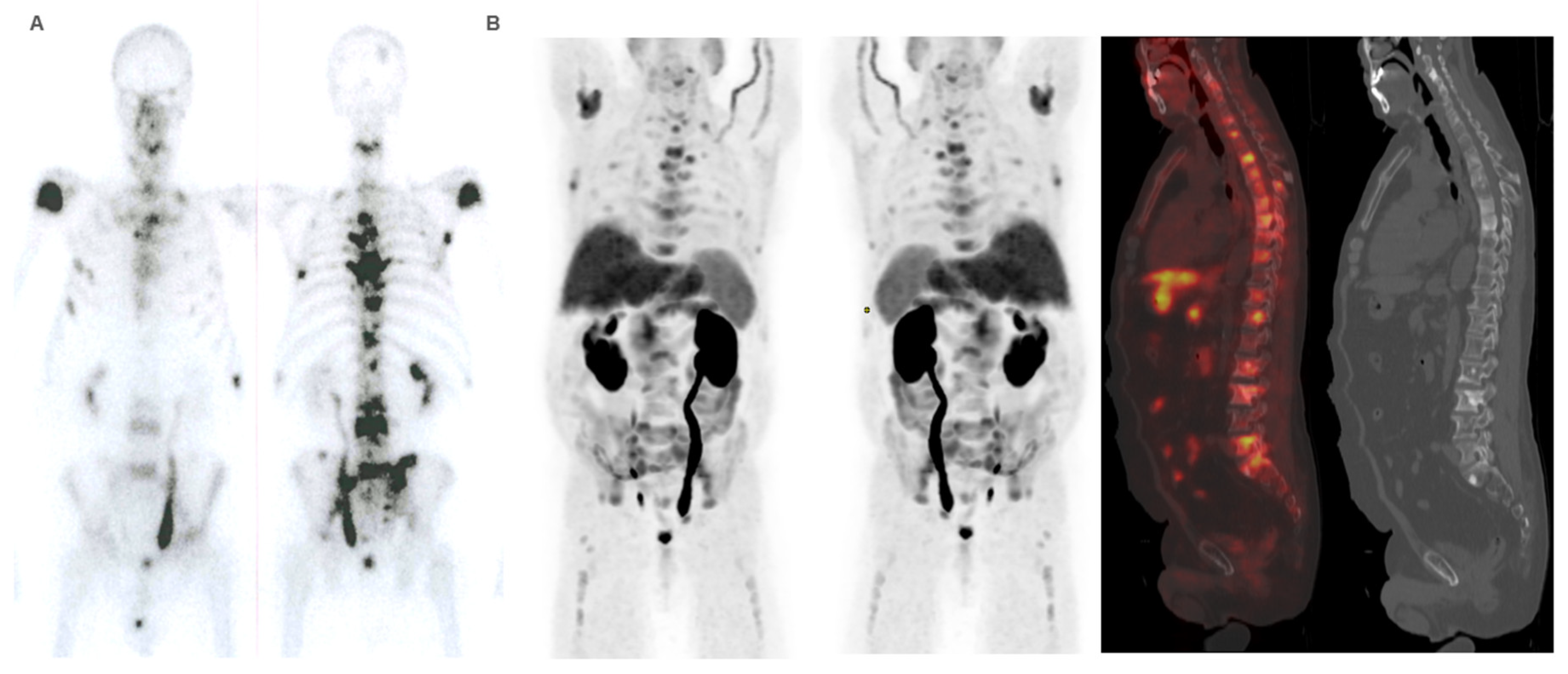
Figure 6.
Patient ≠ 1. PSA and AP showed a steadily increase after 223Ra initiation. Clinical deterioration was observed after third 223Ra administration. Interim BS (A) and FCH PET/CT (B) show disease progression. Patient died 6 months after starting treatment with 223Ra.
Figure 6.
Patient ≠ 1. PSA and AP showed a steadily increase after 223Ra initiation. Clinical deterioration was observed after third 223Ra administration. Interim BS (A) and FCH PET/CT (B) show disease progression. Patient died 6 months after starting treatment with 223Ra.

Figure 7.
Patient ≠ 2. 88-year-old men diagnosed with metastatic prostate cancer, Gleason Score 7 (4+3), from the onset. He received first-line treatment with Enzalutamide until biochemical and bone progression after 5 years. Treatment with 223Ra was proposed as a second-line. Baseline BS and FCH PET/CT (A) shows oligometastatic disease with only axial involvement and predominantly osteoblastic. At the start of 223Ra treatment, patient was in very good general condition (ECOG 0) with baseline PSA levels of 14.9 ng/mL, AP of 73 IU/L, and LDH of 450 IU/L. The patient completed 6 doses of 223Ra, remaining stable in the interim BS and FCH PET/CT studies (B) but showed bone progression at the end of treatment in both the BS and FCH PET/CT (C). His PSA levels increased during the treatment, while AP levels remained stable. After 223Ra treatment, patient received Docetaxel and experienced a bone event that consisted of a painful metastatic bone at 17 months, treated with palliative vertebral radiotherapy. He ultimately died with an OS of 30 months.
Figure 7.
Patient ≠ 2. 88-year-old men diagnosed with metastatic prostate cancer, Gleason Score 7 (4+3), from the onset. He received first-line treatment with Enzalutamide until biochemical and bone progression after 5 years. Treatment with 223Ra was proposed as a second-line. Baseline BS and FCH PET/CT (A) shows oligometastatic disease with only axial involvement and predominantly osteoblastic. At the start of 223Ra treatment, patient was in very good general condition (ECOG 0) with baseline PSA levels of 14.9 ng/mL, AP of 73 IU/L, and LDH of 450 IU/L. The patient completed 6 doses of 223Ra, remaining stable in the interim BS and FCH PET/CT studies (B) but showed bone progression at the end of treatment in both the BS and FCH PET/CT (C). His PSA levels increased during the treatment, while AP levels remained stable. After 223Ra treatment, patient received Docetaxel and experienced a bone event that consisted of a painful metastatic bone at 17 months, treated with palliative vertebral radiotherapy. He ultimately died with an OS of 30 months.
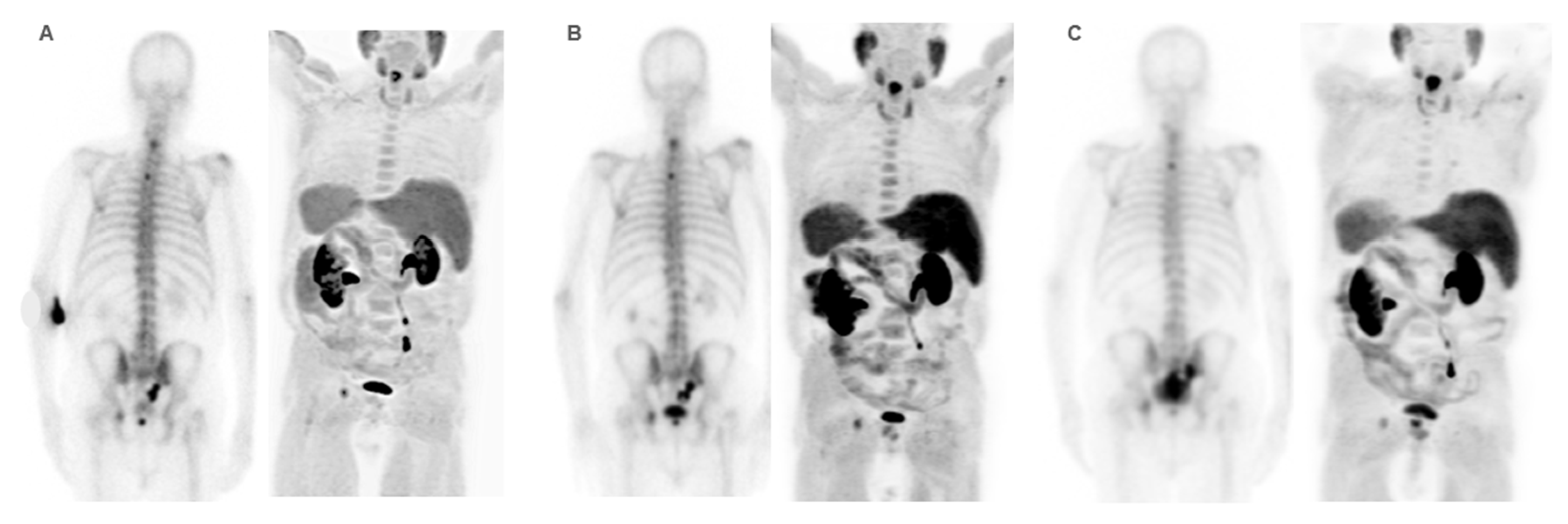
Figure 8.
Patient ≠ 3. 69-year-old man diagnosed with prostate cancer Gleason score 8 (4+4) stage IV T3N1M1 (hepatic, pulmonary, nodal, and bone infiltration). Patient achieved a complete radiologic response after received first-line Docetaxel with and anti-androgen blockade. After progression, Abiraterone-Prednisone was administered with partial biochemical response. 223Ra was administered as third line. Baseline BS and FCH PET/CT (A) shows oligometastatic axial and extra-axial BM on the BS and polymetastatic (6-20 lesions) axial and extra-axial involvement on the FCH PET/CT without soft tissue involvement, with some BM showing lytic characteristics and higher uptake than the liver. Despite this, the concordance between both techniques was good, with metabolic activity predominating over osteogenic. At the start of treatment, the patient was in very good general condition (ECOG 0) with pain and baseline PSA values of 5 ng/dL, AP of 87 IU/L, and LDH of 363 IU/L. He received 6 doses of 223Ra, with PSA values progressing from the start of treatment, although AP and LDH values did not. The interim BS study shows rib deposits interpreted as bone progression while the FCH PET/CT showed stability, explained by the interpretation of rib deposits as probable fractures. However, the end-treatment scans (C) show bone and nodal progression of FCH PET/CT with stability in the BS. Subsequently, treatment with Abiraterone-Prednisone was resumed, followed, shortly after, of Cabazitaxel. Patient died 10 months after 223Ra initiation.
Figure 8.
Patient ≠ 3. 69-year-old man diagnosed with prostate cancer Gleason score 8 (4+4) stage IV T3N1M1 (hepatic, pulmonary, nodal, and bone infiltration). Patient achieved a complete radiologic response after received first-line Docetaxel with and anti-androgen blockade. After progression, Abiraterone-Prednisone was administered with partial biochemical response. 223Ra was administered as third line. Baseline BS and FCH PET/CT (A) shows oligometastatic axial and extra-axial BM on the BS and polymetastatic (6-20 lesions) axial and extra-axial involvement on the FCH PET/CT without soft tissue involvement, with some BM showing lytic characteristics and higher uptake than the liver. Despite this, the concordance between both techniques was good, with metabolic activity predominating over osteogenic. At the start of treatment, the patient was in very good general condition (ECOG 0) with pain and baseline PSA values of 5 ng/dL, AP of 87 IU/L, and LDH of 363 IU/L. He received 6 doses of 223Ra, with PSA values progressing from the start of treatment, although AP and LDH values did not. The interim BS study shows rib deposits interpreted as bone progression while the FCH PET/CT showed stability, explained by the interpretation of rib deposits as probable fractures. However, the end-treatment scans (C) show bone and nodal progression of FCH PET/CT with stability in the BS. Subsequently, treatment with Abiraterone-Prednisone was resumed, followed, shortly after, of Cabazitaxel. Patient died 10 months after 223Ra initiation.
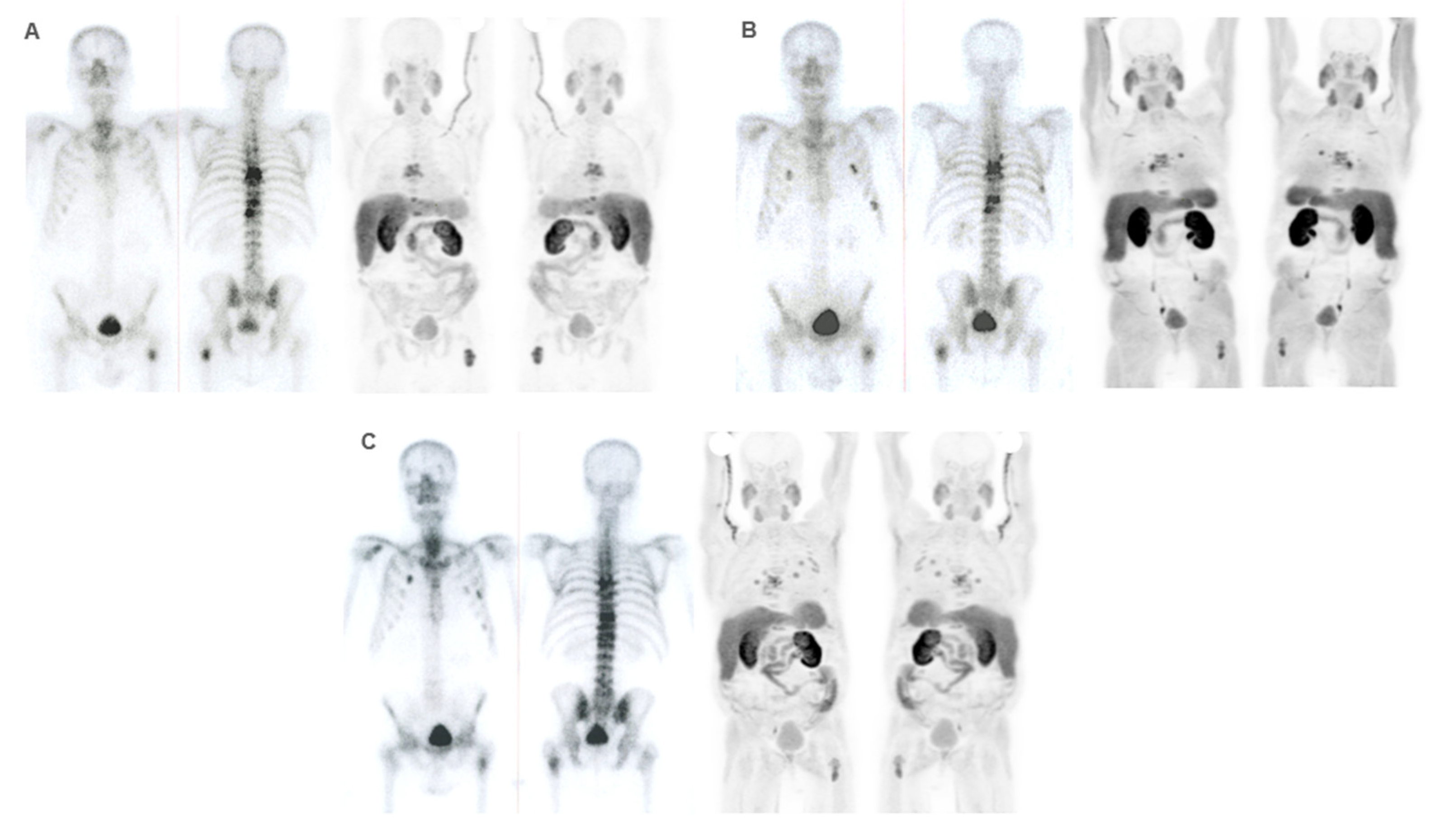

Table 1.
Patient and tumor characteristics.
| Baseline quantitative variables | Mean ± IQR |
|---|---|
| Age (years) | 72.72 ± 8.50 |
| Baseline PSA (ng/ml) | 188.53 ± 913.94 |
| Baseline AP (U/l) | 176.78 ± 187.26 |
| Baseline LDH (U/l) | 400.46 ± 192.37 |
| SUVmax | 8.62 ± 5.37 |
| Average SUVmax | 6.82 ± 4.01 |
| Time variables | Median (Q1 – Q3) |
| Time of evolution of prostate cancer (months) | 62.50 (75.75 – 108.00) |
| Time of evolution of bone metastases (months) | 28.00 (20.00 – 48.00) |
| Time of castration resistance (months) | 21 (12.25–43.00) |
SD: standard deviation, AP: alkaline phosphatase, LDH: lactate dehydrogenase, PSA: prostate specific antigen, IQR: interquartile range.
Table 2.
Patients and tumour qualitative and categorical characteristics (n=100).
| Clinical characteristics | n and % |
|---|---|
| Gleason | |
| ≤ 7 | 46 |
| ≥ 8 | 45 |
| n.a. | 9 |
| Baseline AP | |
| Pathological | 37 |
| Normal | 53 |
| n.a. | 10 |
| Baseline LDH | |
| Pathological | 18 |
| Normal | 69 |
| n.a. | 13 |
| Bone events before to 223Ra | |
| Yes | 23 |
| No | 77 |
| Bone events during or after to 223Ra | |
| Yes | 26 |
| No | 74 |
| Bone protective treatment | |
| Yes | 90 |
| No | 10 |
| Death (*) | |
| Yes | 92 |
| No | 8 |
| Progression (*) | |
| Yes | 97 |
| No | 3 |
| Therapeutic failure | |
| Yes | 56 |
| No | 44 |
| ECOG performance status | |
| 0 | 70 |
| 1 | 27 |
| 2 | 3 |
| Enzalutamide before to 223Ra | |
| Yes | 42 |
| No | 58 |
| Abiraterone before to 223Ra | |
| Yes | 66 |
| No | 34 |
| ChT (**) | |
| First line Docetaxel | 71 |
| 2nd line ChT | 21 |
| Xofigo line | |
| 1 | 3 |
| 2 | 20 |
| 3 | 57 |
| 4 | 13 |
| 5 | 6 |
| 7 | 1 |
| PSA progression during 223Ra | |
| Yes | 70 |
| No | 27 |
| n.a. | 3 |
| PSA progression during 223Ra (detailed 1) | |
| First 3 months | 54 |
| 4-6 dose | 16 |
| n.a. | 30 |
| PSA progression during 223Ra (detailed 2) | |
| First 3 months | 54 |
| Rest | 43 |
| n.a. | 3 |
n: number, %: percentage, AP: alkaline phosphatase, LDH: lactate dehydrogenase, n= number of patients, BM: bone metastases, BS: bone scan, (*) during follow-up, ChT: Chemotherapy, n.a.: not available, ECOG: Eastern Cooperative Oncology Group.
Table 3.
Results of baseline imaging techniques (n=100).
| Baseline imaging characteristics | n and % |
|---|---|
| Lesion localization on BS | |
| Axial | 39 |
| Axial and other | 60 |
| n.a. | 1 |
| Number of BM on BS | |
| Oligomts ≤5 | 27 |
| Polimts >5 | 72 |
| n.a. | 1 |
| Extent of BM on BS | |
| 1-5 lesions | 27 |
| 6-20 lesions | 35 |
| >20 lesions | 30 |
| Superscan | 7 |
| n.a. | 1 |
| High tumour burden on BS | |
| Yes | 61 |
| No | 38 |
| n.a. | 1 |
| Lesion localisation on FCH PET/CT | |
| Axial | 39 |
| Axial and other | 48 |
| n.a. | 13 |
| Number of BM on FCH PET/CT | |
| Oligomts ≤5 | 27 |
| Polimts >5 | 60 |
| n.a. | 13 |
| Extent of BM on FCH PET/CT | |
| 1-5 lesions | 27 |
| 6-20 lesions | 33 |
| >20 lesions | 21 |
| Superscan | 6 |
| n.a. | 13 |
| High tumour burden on FCH PET/CT | |
| Yes | 48 |
| No | 39 |
| n.a. | 13 |
| BM characteristics on CT (*) | |
| Osteoblastic | 56 |
| Osteolitic | 12 |
| Mixed | 19 |
| n.a. | 13 |
| Soft tissue involvement on FCH PET/CT | |
| Yes | 19 |
| No | 68 |
| n.a. | 13 |
| Concordance BS/ FCH PET/CT | |
| Good | 58 |
| Moderate | 12 |
| Bad | 16 |
| n.a. | 14 |
| A pattern on BS/ FCH PET/CT | |
| 1 (predominant metabolic activity) | 22 |
| 2 (predominant osteogenic activity) | 54 |
| 3 (similar uptake in both) | 10 |
| n.a. | 14 |
| B pattern (bone marrow involvement on BS) | |
| Yes | 23 |
| No | 76 |
| n.a. | 1 |
| C pattern (bone marrow involvement on FCH PET/CT) | |
| Yes | 18 |
| No | 69 |
| n.a. | 13 |
| D pattern (FCH PET/CT uptake) | |
| 1 (higher than liver) | 45 |
| 2 (lower than liver) | 42 |
| n.a. | 13 |
n: number, %: percentage, BS: bone scan, BM: bone metastases, FCH PET/CT: 18F-fluorocholine positron emission tomography/computed tomography, (*) CT portion of FCH PET/CT, n.a.: not available.
Table 4.
Response results of interim and end-treatment bone scan and FCH PET/CT.
| Interim FCH PET/CT | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| PR | S | P | |||||||
|
Interim BS (n=63) |
PR | 1 | 0 | 1 | |||||
| S | 7 | 16 | 14 | ||||||
| P | 1 | 2 | 21 | ||||||
| End-treatment FCH PET/CT | |||||||||
| CR | PR | E | P | ||||||
| End-treatment BS (n=38) | PR | 1 | 0 | 2 | 1 | ||||
| E | 1 | 1 | 14 | 12 | |||||
| P | 0 | 0 | 1 | 5 | |||||
CR: complete response, PR: partial response, S: stability, P: progression, BS: bone scan, FCH PET/CT: 18F-fluorocholine positron emission tomography/computed tomography.
Table 5.
Association of clinical and imaging variables with therapeutic failure.
| Variables | χ² | p value |
|---|---|---|
| Clinical and disease characteristics before 223Ra | ||
| Bone events before to 223Ra (categorical) | 1.030 | 0.310 |
| Gleason | 3.438 | 0.931 |
| Gleason (categorical) | 0.566 | 0.452 |
| ECOG | 6.188 | 0.038 |
| Prostatectomy (radical prostate cancer treatment) | 4.386 | 0.036 |
| RT (radical prostate cancer treatment) | 0.230 | 0.632 |
| Enzalutamide (before to 223Ra) | 0.038 | 0.845 |
| Abiraterone (before to 223Ra) | 0.167 | 0.683 |
| Docetaxel (before to 223Ra) | 0.114 | 0.736 |
| 2nd line ChT (before to 223Ra) | 0.376 | 0.540 |
| Xofigo line | 3.797 | 0.620 |
| PSA progression during 223Ra | 19.378 | < 0.001 |
| PSA progression during 223Ra detailed 1 (i) | 5.145 | 0.023 |
| PSA progression during 223Ra detailed 2 (ii) | 18.564 | < 0.001 |
| Baseline AP | 4.735 | 0.030 |
| Baseline LDH | 4.247 | 0.039 |
| Clinical and disease characteristics after 223Ra | ||
| Bone events during or after to 223Ra (categorical) | 0.410 | 0.840 |
| Bone protective treatment (categorical) | 5.213 | 0.040 |
| Death (during follow up) | 11.335 | < 0.001 |
| Progression (during follow up) | 2.43 | 0.253 |
| PFS (≤6 months vs >6 months) | 23.522 | < 0.001 |
| OS (≤12 months vs >12 months) | 18.446 | < 0.001 |
| Baseline imaging techniques results | ||
| BM location on BS | 2.304 | 0.129 |
| Number of BM on BS | 3.300 | 0.069 |
| Extent of BM on baseline BS | 4.637 | 0.205 |
| High tumor burden of BM on BS | 1.674 | 0.196 |
| BM location on FCH PET/CT | 6.584 | 0.010 |
| Number of BM on FCH PET/CT | 10.321 | 0.001 |
| Extent of BM on baseline FCH PET/CT | 14.998 | 0.001 |
| BM characteristics on CT portion of FCH PET/CT | 7.299 | 0.025 |
| BM characteristics on CT portion FCH PET/CT (categorical) (iii) | 7.016 | 0.008 |
| Soft tissue involvement | 4.141 | 0.042 |
| Concordance BS/ FCH PET/CT (iv) | 1.729 | 0.421 |
| A pattern (BS vs FCH PET/CT) | 3.972 | 0.146 |
| B pattern (BS) | 0.343 | 0.558 |
| C pattern (FCH PET/CT) | 3.434 | 0.064 |
| D pattern (FCH PET/CT) | 8.318 | 0.004 |
ChT: chemotherapy, RT: radiotherapy, BM: bone metastases, AP: alkaline phosphatase, LDH: lactate dehydrogenase, ECOG: Eastern Cooperative Oncology Group, PFS: progression-free survival, OS: overall survival, BS: bone scintigraphy, FCH PET/CT: 18F-fluorocholine positron emission tomography/computed tomography, CT: computed tomography, A pattern: osteogenic or metabolic activity predominance, B pattern: bone marrow involvement in bone scintigraphy, C pattern: bone marrow involvement on FCH PET, D pattern: PET uptake on BM higher than liver uptake, (i) first part vs second part of 223Ra treatment, (ii) first part of 223Ra treatment vs ulterior, (iii) osteoblastic vs rest (mixed and osteolytic), (iv) concordance BS/PET: good, moderate or bad.
Table 6.
Association of clinical and imaging variables with skeletal events during or after 223Ra treatment.
Table 6.
Association of clinical and imaging variables with skeletal events during or after 223Ra treatment.
| Variables | χ² | p value | |||
|---|---|---|---|---|---|
| Patient and clinical characteristics before 223Ra | |||||
| Bone events before to 223Ra (yes/no) | 1.198 | 0.274 | |||
| Bone events before to 223Ra (type) | 8.473 | 0.029 | |||
| Gleason | 7.450 | 0.395 | |||
| ECOG | 2.422 | 0.375 | |||
| 223Ra line | 3.624 | 0.651 | |||
| PSA progression during 223Ra | 0.498 | 0.480 | |||
| PSA progression during 223Ra detailed 1 | 0.048 | 1.000 | |||
| PSA progression during 223Ra detailed 2 | 0.256 | 0.613 | |||
| Baseline AP | 1.455 | 0.228 | |||
| Baseline LDH | 0.164 | 0.759 | |||
| Clinical and disease characteristics after 223Ra | |||||
| Aditional treatments (categorical) | 2.157 | 0.225 | |||
| Additional treatments (lines number) | 18.544 | 0.001 | |||
| Additional treatment (Abiraterone) | 3.835 | 0.050 | |||
| Additional treatment (Enzalutamide) | 1.127 | 0.288 | |||
| Additional treatment (ChT) | 5.963 | 0.058 | |||
| Bone protective treatment (categorical) | 0.092 | 1.000 | |||
| Bone protective treatment (descriptive) | 2.816 | 0.250 | |||
| Bone protective treatment (moment) | 1.117 | 0.771 | |||
| Death during follow-up | 0.851 | 0.449 | |||
| Progression during follow-up | 0.086 | 1.000 | |||
| PFS (≤6 months vs >6 months) | 0.837 | 0.360 | |||
| OS (≤12 months vs >12 months) | 7.787 | 0.005 | |||
| Baseline imaging techniques | |||||
| BM location on BS | 0.013 | 0.910 | |||
| Number of BM on BS | 0.217 | 0.641 | |||
| Extent of BM on baseline BS | 0.316 | 0.972 | |||
| BM high tumour burden on BS | 0.000 | 0.992 | |||
| BM on FCH PET/CT | 3.253 | 0.071 | |||
| Number of BM on FCH PET/CT | 0.205 | 0.651 | |||
| Extent of BM on FCH PET/CT | 1.270 | 0.752 | |||
| BM high tumour burden on FCH PET/CT | 5.256 | 0.022 | |||
| BM characteristics on CT portion of FCH PET/CT (descriptive) | 4.036 | 0.134 | |||
| BM characteristics on CT portion of FCH PET/CT (categorical) | 0.368 | 0.618 | |||
| Soft tissue involvement on FCH PET/CT (categorical) | 1.417 | 0.234 | |||
| Soft tissue involvement of FCH PET/CT (descriptive) | 1.273 | 0.718 | |||
| Concordance BS/ FCH PET/CT 1 | 0.842 | 0.622 | |||
| Concordance BS/ FCH PET/CT 2 | 0.031 | 1.000 | |||
| A pattern (BS vs FCH PET/CT) | 1.674 | 0.457 | |||
| B pattern (BS) | 1.218 | 0.270 | |||
| C pattern (FCH PET/CT) | 5.088 | 0.033 | |||
| D pattern (FCH PET/CT) | 3.594 | 0.058 | |||
| Interim imaging techniques | |||||
| Interim BS response | 0.105 | 0.904 | |||
| Interim BS response (categorical) | 0.101 | 0.751 | |||
| Interim FCH PET/CT response | 0.115 | 1.000 | |||
| Interim FCH PET/CT response (categorical) | 0.028 | 0.867 | |||
| Progression localisation | 2.856 | 0.463 | |||
| Concordance BS/ FCH PET/CT 1 | 0.523 | 0.768 | |||
| Concordance BS/ FCH PET/CT 2 | 0.651 | 0.522 | |||
| End-treatment imaging techniques | |||||
| End-treatment BS response | 3.288 | 0.213 | |||
| End-treatment BS response | 1.081 | 0.427 | |||
| End-treatment FCH PET/CT response | 3.934 | 0.287 | |||
| End-treatment FCH PET/CT response | 2.438 | 0.155 | |||
| Progression location | 2.526 | 0.906 | |||
| Concordance BS/ FCH PET/CT 1 | 0.891 | 0.646 | |||
| Concordance BS/ FCH PET/CT 2 | 0.107 | 1.000 | |||
ECOG: Eastern Cooperative Oncology Group, ChT: chemotherapy, RT: radiotherapy, BS: bone scan, FCH PET/CT: 18F-fluorocholine positron emission tomography/computed tomography, CT: portion of FCH PET/CT, BM: Bone metastases, BS: Bone scintigraphy, PSA progression during 223Ra detailed 1: progression at first or second 3 doses, PSA progression during 223Ra detailed 2: progression at 3 first doses o second 3 and beyond, PFS categorical: progression-free survival > 6 months or not, OS categorical: overall survival > 12 months or not, concordance BS/PET 1: good, moderate or bad, concordance BS/ FCH PET/CT 2: good/moderate or bad, A pattern: osteogenic or metabolic activity predominance, B pattern: bone marrow involvement in BS, C Pattern: bone marrow involvement on FCH PET, D pattern: FCH PET uptake higher than liver uptake.
Table 7.
Results of the Cox regression index of clinical and imaging quantitative variables with OS.
Table 7.
Results of the Cox regression index of clinical and imaging quantitative variables with OS.
| Variables | HR | 95% CI of HR | p value |
|---|---|---|---|
| Doses of 223Ra (number) | 0.699 | 0.606-0.807 | < 0.001 |
| Patient age | 1.005 | 0.981-1.030 | 0.666 |
| Time from diagnosis of pCa to 223Ra | 0.122 | 0.995-1.003 | 0.727 |
| Time of evolution of BM to 223Ra | 0.999 | 0.993-1.007 | 0.925 |
| Time of CRPC to 223Ra | 1.003 | 0.994-1.012 | 0.479 |
| Baseline PSA | 1.000 | 1.0001-1.0004 | 0.028 |
| Baseline AP | 1.002 | 1.001-1.004 | < 0.001 |
| Baseline LDH | 1.000 | 0.999-1.001 | 0.511 |
| SUVmax | 1.049 | 1.006-1.092 | 0.023 |
| Average SUVmax | 1.070 | 1.012-1.132 | 0.017 |
HR: hazard ratio, CI: confidence interval, pCa: prostate cancer, CRPC: castration resistance prostate cancer, BM: bone metastases, PSA: prostate specific antigen, AP: alkaline phosphatase, LDH: lactate dehydrogenase, SUV: standardized uptake value.
Table 8.
Long rank (Mantel-Cox) results of association of clinical and tumor characteristics with overall survival.
Table 8.
Long rank (Mantel-Cox) results of association of clinical and tumor characteristics with overall survival.
| Variables | Median (mo) | χ² | p value | |
|---|---|---|---|---|
| Bone events before to 223Ra | Yes | 16 | 0.022 | 0.883 |
| No | 13 | |||
| Bone events during or after to 223Ra | Yes | 19 | 4.998 | 0.025 |
| No | 12 | |||
| Any treatments after 223Ra | Yes | 14 | 25.699 | < 0.001 |
| No | 5 | |||
| Abiraterone after 223Ra | Yes | 23 | 6.614 | 0.010 |
| No | 13 | |||
| Enzalutamide after 223Ra | Yes | 23 | 11.312 | <0.001 |
| No | 13 | |||
| Bone protective treatment | Yes | 14 | 0.113 | 0.737 |
| No | 14 | |||
| Bone protective treatment (Denosumab) | Zolendronic | 16 | 4.228 | 0.040 |
| Both | 8 | 0.329 | 0.566 | |
| Bone protective treatment (Zolendronic) | Denosumab | 13 | 4.228 | 0.040 |
| Both | 8 | 1.506 | 0.220 | |
| Therapeutic failure | Yes | 8 | 29.1 | < 0.001 |
| No | 21 | |||
| Gleason (categorical) | ≥ 8 | 14 | 0.036 | 0.850 |
| Rest | 14 | |||
| ECOG 0 | 1 | 9 | 4.253 | 0.039 |
| 2 | 5 | 23.337 | <0.001 | |
| ECOG 1 | 2 | 5 | 3.874 | 0.049 |
| Enzalutamide before to 223Ra | Yes | 10 | 1.081 | 0.299 |
| No | 16 | |||
| Abiraterone before to 223Ra | Yes | 13 | 2.663 | 0.103 |
| No | 18 | |||
| 2nd line ChT before to 223Ra | Yes | 9 | 0.119 | 0.730 |
| No | 14 | |||
| 1st Docetaxel before to 223Ra | Yes | 14 | 0.958 | 0.328 |
| No | 14 | |||
| 223Ra line 1 | 2 | 15 | 4.168 | 0.041 |
| 3 | 11 | 0.851 | 0.356 | |
| 4 | 14 | 0.243 | 0.622 | |
| 5 | 7 | 5.279 | 0.022 | |
| 7 | 8 | 3.000 | 0.083 | |
| 223Ra line 2 | 3 | 11 | 0.051 | 0.821 |
| 4 | 14 | 0.563 | 0.453 | |
| 5 | 7 | 5.171 | 0.023 | |
| 7 | 8 | 3.725 | 0.054 | |
| 223Ra line 3 | 4 | 14 | 0.766 | 0.381 |
| 5 | 7 | 1.715 | 0.190 | |
| 7 | 8 | 0.551 | 0.458 | |
| 223Ra line 4 | 5 | 7 | 3.208 | 0.073 |
| 7 | 8 | 1.548 | 0.213 | |
| 223Ra line 5 | 7 | 8 | 0.141 | 0.707 |
| 223Ra line (categorical 1) | First 3 | 14 | 0.015 | 0.902 |
| 4rd and beyond | 11 | |||
| 223Ra line (categorical 2) | First 2 | 19 | 0.360 | 0.549 |
| 3rd and beyond | 11 | |||
| PSA progression during 223Ra | Yes | 12 | 8.508 | 0.004 |
| No | 19 | |||
| PSA progression detailed 1 | A | 12 | 0.122 | 0.726 |
| B | 11 | |||
| PSA progression detailed 2 | A | 12 | 5.693 | 0.017 |
| C | 16 | |||
| Baseline AP | Pathological | 8 | 12.581 | < 0.001 |
| Normal | 15 | |||
| Baseline LDH | Pathological | 8 | 4.526 | 0.033* |
| Normal | 14 | |||
PFS: progression free survival, mo: months, χ²: Chi-squared, ECOG: Eastern Cooperative Oncology Group, BS: bone scan, FCH PET/CT: 18F-fluorocholine positron emission tomography/computed tomography, PSA progression A: progression at first 3 doses, PSA progression B: progression at 3 second doses, PSA progression C: progression at 3 second doses and beyond.
Table 9.
Long rank (Mantel-Cox) results of association of baseline imaging variables with overall survival.
Table 9.
Long rank (Mantel-Cox) results of association of baseline imaging variables with overall survival.
| Baseline imaging variables | Median (mo) | χ² | p value | |
|---|---|---|---|---|
| BM location on BS | Axial | 15 | 1.414 | 0.234 |
| Axial and other | 11 | |||
| BM number on BS | Oligometastatic | 17 | 2.534 | 0.111 |
| Polimetastasic | 11 | |||
| Number of BM on BS (1-5 lesions) | 6-20 lesions | 13 | 0.715 | 0.398 |
| > 20 lesions | 8 | 3.454 | 0.063 | |
| Superscan | 5 | 2.531 | 0.112 | |
| Number of BM on BS (6-20 lesions) | > 20 lesions | 8 | 1.289 | 0.256 |
| Superscan | 5 | 0.703 | 0.402 | |
| Number of BM on BS (> 20 lesions) | Superscan | 5 | 0.117 | 0.732 |
| High burden of BM on BS | Yes | 11 | 1.691 | 0.193 |
| No | 16 | |||
| BM location on FCH PET/CT | Axial | 21 | 14.769 | < 0.001 |
| Axial and other | 8 | |||
| Number of BM on FCH PET/CT | Oligometastatic | 18 | 4.814 | 0.028 |
| Polimetastasic | 10 | |||
| Number of BM on FCH PET/CT (1-5) | 6-20 | 13 | 1.215 | 0.270 |
| > 20 | 8 | 7.259 | 0.007 | |
| Superscan | 5 | 16.751 | <0.001 | |
| Number of BM on FCH PET/CT (6 -20) | > 20 | 8 | 3.577 | 0.059 |
| Superscan | 5 | 9.494 | 0.002 | |
| Number of BM on FCH PET/CT (> 20) | Superscan | 5 | 2.081 | 0.149 |
| FCH PET/CT high tumour burden of BM | Yes | 9 | 9.016 | 0.003 |
| No | 18 | |||
| BM characteristics (i) on CT (osteoblastic) | Osteolytic | 13 | 0.196 | 0.658 |
| Mixed | 9 | 3.944 | 0.047 | |
| BM characteristics on CT (osteolytic) | Mixed | 9 | 0.953 | 0.329 |
| BM characteristics on CT (categorical) | Osteoblastic | 14 | 2.620 | 0.106 |
| Rest | 12 | |||
| Soft tissue involvement on FCH PET/CT | Yes | 7 | 3.911 | 0.048 |
| No | 14 | |||
| BS/PET concordance (good) | Moderate | 8 | 4.988 | 0.026 |
| Bad | 13 | 0.896 | 0.344 | |
| BS/PET concordance (moderate) | Bad | 13 | 5.211 | 0.022 |
| A pattern | Osteogenic activity predominance | 15 | 3.718 | 0.054 |
| Similar uptake | 7 | 0.193 | 0.660 | |
| A pattern | Similar uptake | 7 | 0.879 | 0.348 |
| B pattern | Yes | 7 | 2.626 | 0.105 |
| No | 14 | |||
| C pattern | Yes | 5 | 27.266 | < 0.001 |
| No | 14 | |||
| D pattern | Higher than liver | 9 | 13.170 | < 0.001 |
| Lower than liver | 18 | |||
χ²: Chi-squared, mo: months, BM: bone metastases, BS: bone scan, FCH PET/CT: 18F-fluorocholine positron emission tomography/computed tomography, CT: portion of FCH PET/CT, A pattern: osteogenic or metabolic activity predominance, B pattern: bone marrow involvement in bone scintigraphy, C Pattern: bone marrow involvement on FCH PET, D pattern: PET uptake higher than liver uptake, (i) on CT portion of FCH PET/CT.
Table 10.
Long rank (Mantel-Cox) results of association of treatment response imaging variables with overall survival.
Table 10.
Long rank (Mantel-Cox) results of association of treatment response imaging variables with overall survival.
| Variables | Median (mo) | χ² | p value | |
|---|---|---|---|---|
| Interim imaging techniques | ||||
| BS interim response (partial response, 12 mo) | Stability | 17 | 0.018 | 0.892 |
| Progression | 13 | 0.836 | 0.361 | |
| BS interim response (stability) | Progression | 13 | 8.723 | 0.003 |
| BS interim response categorical | No progression | 15 | 8.371 | 0.004 |
| Progression | 13 | |||
| Interim PET response (partial response, 21 mo) | Stability | 23 | 0.011 | 0.917 |
| Progression | 11 | 7.044 | 0.008 | |
| Interim PET response (stability) | Progression | 11 | 13.759 | <0.001 |
| Interim PET response categorical | No progression | 23 | 17.026 | < 0.001 |
| Progression | 11 | |||
| Interim PET progression (bone, 8 mo) | Adenopathic | 14 | 1.543 | 0.214 |
| Bone and adenopathic | 14 | 0.420 | 0.517 | |
| Bone and visceral | 9 | 0.066 | 0.797 | |
| Interim PET progression (adenopathic) | Bone and adenopathic | 14 | 0.347 | 0.556 |
| Bone and visceral | 9 | 0.656 | 0.418 | |
| Interim PET progression (bone and adenopathic) | Bone and visceral | 9 | 1.101 | 0.294 |
| End-treatment images techniques | ||||
| End-treatment BS response (partial response 23 mo) | Stability | 21 | 0.005 | 0.946 |
| Progression | 16 | 2.598 | 0.107 | |
| End-treatment BS response (stability) | Progression | 16 | 2.944 | 0.086 |
| End-treatment BS response categorical | No progression | 23 | 3.470 | 0.063 |
| Progression | 16 | |||
| End-treatment PET response (complete response, 24 mo) | Partial response | 34 | 0.059 | 0.808 |
| Stability | 17 | 0.128 | 0.720 | |
| Progression | 19 | 0.553 | 0.457 | |
| End-treatment PET response (partial response) | Stability | 17 | 0.089 | 0.765 |
| Progression | 19 | 0.373 | 0.542 | |
| End-treatment PET response (stability) | Progression | 19 | 0.264 | 0.607 |
| End-treatment PET response categorical | No progression | 23 | 1.327 | 0.249 |
| Progression | 18 | |||
| End-treatment PET progression (bone, 15 mo) | Adenopathic | 18 | 0.022 | 0.883 |
| Visceral | 10 | 2.762 | 0.097 | |
| Bone and adenopathic | 19 | 1.185 | 0.276 | |
| Bone and visceral | 47 | 2.166 | 0.141 | |
| End-treatment PET progression (adenopathic) | Visceral | 10 | 3.000 | 0.083 |
| Bone and adenopathic | 19 | 1.182 | 0.277 | |
| Bone and visceral | 47 | 1.779 | 0.182 | |
| End-treatment PET progression (visceral) | Bone and adenopathic | 19 | 2.000 | 0.157 |
| Bone and visceral | 47 | 1.000 | 0.317 | |
| End-treatment PET progression (bone and adenopathic) | Bone and visceral | 47 | 1.471 | 0.225 |
χ²: Chi-squared, mo: months, BM: bone metastases, BS: bone scan, FCH PET/CT: 18F-fluorocholine positron emission tomography/computed tomography, CT: portion of FCH PET/CT.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



