
Submitted:
13 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Staphylococcus aureus is an opportunistic human pathogen and a leading cause of bloodstream infections. It can acquire different antibiotic resistance genes, leading to treatment failure. Aim: We elaborate on the genomic characteristics; antibiotic resistance, virulence, pathogenicity, phylogenomics and clonal diversity of S. aureus implicated in bloodstream infections. Six multidrug-resistant (MDR) S. aureus, three methicillin-resistant S. aureus (MRSA) and three methicillin-sensitive S. aureus obtained from blood cultures underwent whole genome sequencing and bioinformatics analysis. All isolates carried different permutations and combinations of resistance genes including, blaZ, mecA, aac(6')-aph (2''), ant(9)-Ia, ant(6)-Ia, mepR, fosB, norA, norC, lmrS, arlS, arlR, mgrA, kdpD and sdrM. We found 6 spa types (t9475, t355, t045, t1265, t1257, and t7888) with varying profiles of virulence genes responsible for immune invasion, enterotoxins, adhesion/biofilm, haemolysins, and leukotoxins. Panton-Valentine leukocidin (Luk-PV) was found in one MSSA isolate. Two SCCmec types IVd(2B) and I(1B) were identified. Isolates belonged to four multilocus sequence types (MLSTs), the most common of which was ST5 (n=3). The STs were clustered into two clonal complexes CC5 and CC8. We found two MRSA clones typed as ST5-CC5-t045-SCCmec_I(1B), and the human-associated MRSA endemic clone ST612-CC8-t1257-SCCmec_IVd(2B). The insertion sequences IS30 and IS6 associated with virulence were found in two isolates. The presence of virulent MDR S. aureus in bloodstream infections poses a clinical concern because of limited treatment options and increased risk of mortality.
Keywords:
Staphylococcus aureus
; bloodstream infections
; whole-genome sequencing
; antibiotic resistance
; virulence
1. Introduction
Staphylococcus aureus is a Gram-positive bacterium inhabiting healthy individuals’ nostrils and skin. However, it has become an important opportunistic pathogen in communities and hospitals [1]. It causes severe skin infections, pneumonia, endocarditis, and bloodstream infections (BSIs) [2]. BSIs caused by S. aureus infections have high morbidity and mortality if not treated timeously [3]. The most significant risk factors for S. aureus BSIs are intravascular devices, surgical procedures, and a debilitated immune system [4].
Methicillin-resistant S. aureus (MRSA) has become a significant cause of BSIs. MRSA poses a major public health threat because of multidrug resistance to different antibiotic classes that limit treatment options [5]. Resistance is mediated by the mecA gene, found on a mobile genetic element (MGE) known as the staphylococcal cassette chromosome mec (SCCmec) [6]. Methicillin-susceptible S. aureus (MSSA) is also emerging as a causative agent of BSIs [7] and has been reported to display high virulence and multidrug resistance [8].
The pathogenicity of S. aureus depends on its ability to produce a wide array of virulence factors involved in adhesion, invasion of host tissues, immune system evasion, and biofilm formation [9,10]. Virulence factors and multiple resistance genes can be transmitted by horizontal gene transfer (HGT) [11] on diverse MGEs, amongst which plasmids are reported as the primary sources for dissemination [4].
The epidemiology of S. aureus strains indicates that its molecular characteristics continually change over time, resulting in new clones, which vary by region. In a study in the United States, ST5 and ST8 were the most prevalent sequence types [12]. In South Africa, ST612 is dominant in the hospital environment [13]. The ST612-IV [2B], belonging to spa type t1257, was identified as a typical clone in clinical settings [14] and sporadically in poultry settings [15]. The ST5 and ST8 clones are commonly associated with BSIs and the pandemic lineages of S. aureus, such as the clonal complex CC8 and CC5 [16]. Notably, the sequence types ST612, ST5, ST8, and ST72 have displayed high resistance to most antibiotic drug classes and are challenging to treat [16].
Multidrug-resistant (MDR) S. aureus infections pose a serious clinical concern. A high incidence of pathogenic MDR MRSA has been reported, and the data suggest that its prevalence is increasing in Africa [17]. A recent South African study investigating the genetic relatedness of hospital-acquired-associated MRSA isolates in two hospitals revealed that all isolates were resistant to aminoglycosides and β-lactams. All the isolates carried the aacA-aphD and mecA-resistant genes and clusters of virulence genes [18]. We elaborate on the genomic characteristics, antibiotic resistance, virulence, pathogenicity, phylogenomics, and clonal diversity of six S. aureus clinical strains implicated in bloodstream infections at a regional hospital in the KwaZulu-Natal province in South Africa
2. Results
2.1. Patient Demographics and Characteristics
The 6 isolates investigated in this study were obtained from patients who visited a regional hospital in the uMgungundlovu District in the KwaZulu-Natal Province. Three of the six isolates were recovered from the neonatal ICU (n=3, 50%), two from surgical wards and one isolate from the paediatric ward. Four patients were males, while 2 were females. The age distribution of patients ranged from 0 to 33 years old, and the mean age was 8.83 years (Table 1). The demographic details of the source participants of the isolates that were selected for WGS are shown in Supplementary Table 1.
2.2. Antibiotic Susceptibility Test Results
The isolates displayed varying phenotypic resistance profiles with most being resistant to penicillin G (n=6), tetracycline (n=5), doxycycline (n=5), clindamycin (n=5), moxifloxacin (n=5), rifampicin (n=4), and erythromycin (n=3). The lowest resistance was against nitrofurantoin, tigecycline, and chloramphenicol (n=1) (Table 1).
2.3. Phenotypic and Genotypic Identification of MRSA Isolates
MRSA isolates were confirmed by phenotypic resistance to cefoxitin (Table 1), and the detection of the mecA gene using polymerase chain reaction (PCR).
2.4. Genomic Features
The genome size of our draft genomes ranged from 2.7Mb to 2.9Mb. The genomic characteristics of the sequences, in relation to G+C content (%), number of RNAs, number of coding sequences, size, N50, L50, coverage and are shown in Supplementary Table 2.
Isolates harboured various permutations and combinations of ARGs which included ARGs against β-lactams [blaZ, mecA], aminoglycosides [aac(6’)-aph(2’‘), aad(6’), ant(9)-la, ant(6)-Ia, aph(2’‘)-Ia, aph(3’)-IIa, kdpD sat-4], trimethoprim [dfrG, dfrC], macrolides [erm(C), erm(A)], tetracycline [tet(K), tet(M), mepR, mepA], flouroquinolones [parE, parC, mgrA, arlS, arlR, grlA, gyrA, norA, norC, sdrM (multidrug efflux pumps)], rifampicin [rpoB] and fosfomycin [fosB, murA], (Table 2). There was a good concordance between ARGs and phenotypic profiles for blaZ, mecA, and aminoglycoside resistance genes in MRSA and MSSA isolates.
We identified known mutations in the gyrA, gyrB, parC, and parE genes found in the quinolone resistance-determining region (QRDR) known to confer fluoroquinolone resistance in some isolates (supplementary material). Also, the major facilitator superfamily (MFS) antibiotic efflux pump (norA, norC), which can also confer resistance to fluoroquinolones, was identified in most isolates. We detected two known mutations (H481N, I527M), and a putatively novel mutation in the rpoB gene (F737Y) conferring resistance to rifampicin in one isolate (S31).
2.5.1. MLST, spa typing, and Clonal Complex
MLST typing revealed a total of four sequence types, ST5 (n=3), ST152 (n=1), ST612 (n=1), and ST8 (n=1). Two MRSA isolates belonged to CC8 (n=2), and CC5 (n=1), while one MSSA isolate belonged to CC5. Two MSSA strains belonging to ST152 and ST5 that could not be classified into a CC. The genetic diversity of the isolates was confirmed by spa typing which revealed six different spa types: t9475, t1265, t355, t045, t1257, t7888 (Table 2). CC and spa type combinations were CC8-t9475, CC8-t1257, CC5-t045 among MRSA isolates, and CC5-t1265 belonging to one MSSA isolate. There was no association observed between STs, spa type, and CC. The grouping of the STs, and spa-types yielded six genotypes, i.e., ST8-t9475, ST152-t355, ST5-t045, ST5-t1265, ST612-1257, ST5-t7888 indicating that isolates were not clonally related.
The SCCmecFinder analysis identified two SCCmec types, i.e., IVd (2B), and I (1B) among the MRSA isolates (Table 2). One MRSA isolate was non-typeable (NT) for SCCmec. The combination of MLST, CC, spa, and SCCmec yielded the ST612-CC8-t1257-SCCmec_IVd (2B), and ST5-CC5-t045-SCCmec_I (1B), clones both of which have been reported in South Africa.
2.5.2. Mobilome (Plasmids, Insertion Sequences, Intact Prophages, and SCCmec Elements)
Analysis of the six isolates genomes identified various MGEs, including plasmid replicons, IS’s, prophages, and SCCmec elements. A total of eight different plasmid replicons were detected of which rep20 (n=3), was the most prevalent (Table 2). There were no associations between plasmid replicons and STs. However, the rep7c was found in CC8 isolates in addition to other plasmid replicons, while rep16 and rep5a were found in isolates with the non-typeable CC. The rep20 plasmid replicon was associated with CC5 and CC8 isolates. The rep10 was carried in CC8 and CC5 isolates, while the re7a and rep21 were carried in CC8 and CC5 isolates, respectively. IS6 and IS256 were identified in three isolates, and their occurrence was not associated with any STs or CC (Table 2). A total of six intact prophages were detected, of which the most identified were PHAGE_Staphy_phi2958PVL (n=2), and PHAGE_Staphy_P282 (n=2) (Table S5). PHAGE_Staphy_phiJB was associated with the dfrG gene.
2.5.3. Virulome and Pathogenicity of S. aureus Strains
A total of 82 virulence genes were detected across the isolates (Table S3). The virulence genes belonged to the five main virulence determinant classes of S. aureus: adherence factors, immune evasion, enzymes (exoenzymes), toxins and the secretion system. It is noteworthy that the most prevalent toxins were hemolysins i.e., gamma (hlg), delta (hld), alpha (hly/hla), staphylococcal enterotoxins (se, set, sel) genes, and leucocidin genes (lukD/E), while lukS-PV, lukF-PV genes were detected in two isolates (S24 & S29). The prediction of isolates pathogenicity towards humans yielded a high average probability score (Pscore ≈ 0.980).
2.6. Genetic Environment of the ARGs and Virulence Genes
The co-carriage of ARGs, and virulence genes was evident across the isolates. Using NCBI annotation, we identified blaZ genes on five isolates in parallel with cacD, virulence genes, and type 1 toxin-antitoxin system. Across the isolates, most blaZ genes were associated with regulator genes blaR and blaI and frequently found with either a recombinase, integrase, cadmium resistance (cadD) gene, or type I toxin-antitoxin system (Table 3). A similar genetic context was detected in S13 isolate, where blaZ, blaR, and blaI were flanked by IS6, cadD, a type I toxin-antitoxin system, on a contig with the closest nucleotide homology to a plasmid from S. aureus pER10678.3A.1 (CP051928.1), suggesting that ARGs, heavy metal resistance genes (HMRGs), and virulence genes may be mobilised by plasmids (Table 3). It is noteworthy that the IS1182 was associated with the mecA, mecI and mecR1 genes together with recombinases, while IS6 bracketed the mecA gene and its regulatory genes (mecI and mecR) in one isolate (S11). Most ARGs, including erm(A), ant(9)-Ia, dfrG, tet(M) were associated with a recombinase and integrase. One isolate was found harbouring the dfrG gene bracketed by ISL3, and recombinases.
2.6.1. Regulatory Genes
The accessory gene regulator system (agr) involved in the regulation and expression of toxins, exoenzymes, and biofilm was detected in all isolates. Isolates carried agr type I and II. The distribution of the agr group in MRSA was: agr I (n=1), agr II (n=2), while in MSSA agr I (n=2), and agr II (n=1).
2.7. Phylogenomics
Phylogenetic trees generated from genomes that were obtained from BV-BRC (coloured in purple) (Figure 1), including isolates from the present study (coloured in green).
3. Discussion
We studied the genomic characteristics of six MDR S aureus isolates implicated in BSIs. The study analysed the resistome, virulome, mobilome, phylogeny, and genetic environment of the resistance genes using WGS and bioinformatics. The genomes analysed herein were predominantly recovered from patients ≤1-year-old.
There was a diversity of ARGs encoding resistance to different antibiotics and good concordance between the observed phenotypic and genotypic resistance. The incidence of ARG’s encoding resistance to β-lactams, aminoglycosides, macrolides, fosfomycin, trimethoprim, tetracycline, and genes coding multidrug resistance (MDR) efflux pumps (norA, mepR, arlR, mgrA, and lmrS) was not dependent on the clonal type. Resistance genes found in this study included erm genes which mediate macrolide–lincosamide–streptogramin B (MLSB) resistance, the aminoglycoside-modifying enzymes, MFS antibiotic efflux pump (msrA, norA, norC), which also confers resistance to fluoroquinolones [25]. The erm(C) and erm(A) genes that are commonly found in MLSB-resistant S. aureus were found in erythromycin and clindamycin resistant isolates (Table 2), which was expected since resistance to erythromycin co-selects resistance to other antibiotics, such as streptogramin B (MLSB) and lincosamides [26]. The ermC gene is among the primary erm type which facilitates ribosome methylation of the 23S rRNA, triggering conformational changes, resulting in drug binding inhibition [27], and have been reported in clinical S. aureus isolates from South Africa [28]. In this study, the ermC encoding macrolide resistance was carried on a plasmid, on a contig that had the closest nucleotide homology to plasmids from S. epidermidis strain TMDU-137 plasmid p5, complete sequence (CP093178.1), implying the likelihood of horizontal transfer of ermC genes in clinical S. aureus isolates. The ermC are often plasmid-mediated, resulting in high resistance to macrolides in S. aureus [29].
The blaZ gene which inactivates penicillin through hydrolysis of the beta-lactam ring was observed in all six isolates that were phenotypically resistant to penicillin. The blaZ genes have also been isolated in clinical isolates of Staphylococci in South Africa [30]. In this study, the blaZ genes were found on contigs with closest homology to either chromosomes or plasmids. This agrees with a study done in Spain that analysed ARGs presence in chromosomes and plasmids from the genomes of S. aureus. WGS analysis of S. aureus revealed that blaZ (n=2) were located on chromosomic contigs, while blaZ was found in plasmid contigs in three isolates [31]. It is important to note that most blaZ and associated MGEs from isolates belonging to ST5 (S13, S34) isolated from the intensive care unit (ICU), and paediatric ward (S29) were located on contigs that had the closest homology to plasmids, implying that plasmids play a crucial role in mobilizing the blaZ gene in clinical S. aureus isolates. The S29 isolate belonging to t045-CC5 lineage, carried assortment of ARGs encoding resistance to different antibiotics (Table 4). Similar ARGs in MRSA lineage t045-CC5-MRSA were also reported in a study conducted in South Africa, where t045-CC5 MRSA lineages obtained from different clinical samples from South Africa and Nigeria reported that t045 lineages were MDR, suggesting that this lineage is hospital-associated, and their multidrug resistance nature may compromise treatment [32].
Also, the blaZ genes, heavy metal genes and associated MGEs were carried on either plasmid or chromosome. The blaZ and cadAC genes were found on the genetic element recombinase:blaI:blaR1:blaZ:cadC:cadA for isolates S24 (MSSA) that was from the ICU, and S29 (MRSA) from the paediatric ward, suggesting co-selection of heavy metal resistance dissemination and adaptation in different wards. The cadA gene confers a high resistance to cadmium and other heavy metals like zinc and lead in S. aureus isolates [33]. The cadA was associated with a plasmid, similar to the findings of a study that was done by Al-Trat et al. (2023) in Malaysia who used WGS to analyse the plasmid content of clinical MRSA isolates, and reported that heavy metal resistance plasmids harboured cadmium resistance genes with the majority being cadAC [34]. The HMRGs have been reported to trigger co-selection mechanism with antibiotics, which may complicate treatment [35]. This may pose a challenge especially among patients in the ICU where broad-spectrum antibiotics are often used.
Tetracycline resistance genes (tetK, tetM) were observed in two isolates. Isolate S11 carried tet(K) associated with a genetic context: plasmid recombination:tet(K) that had a high similarity to S. epidermidis BPH0662, plasmid: 1 (LT614820.1), which could be significant in mobilising TET resistant genes. Also, the tet(M) was bracketed by integrase and IS256 in isolate S31. The IS256 is a retrotransposon that can mobilize the resistance genes through a copy-and-paste mechanism and has been shown to confer a robust genomic plasticity in MRSA strains [36]. We found mutations in gyrA, gyrB parC, parE, and rpoB, implicated in fluoroquinolone and rifampicin resistance. However, the detection of double mutations of gyrA/parC could be associated with high levels of resistance to fluoroquinolones [37].
We found that ARGs, and virulence genes were associated with MGEs, which may enable their transfer within and between plasmids and chromosomes [38]. In this study, the mecA gene was located on IS1182 in two isolates, surrounded by recombinase in genetic context mecA:mecR1::IS1182::recombinase. The insertion sequence IS1182 was present in 2/3 MRSA strains that contained mecA. IS1182 has been shown to occur close to the SCCmec element and increase resistance through inactivating lytH gene encoding a putative lytic enzyme in pathogenic MRSA isolates [39].
MLST typing, clonal complex, spa typing, and SCCmec typing were used to analyse the molecular characteristics of the S. aureus isolates. Four ST types and two clonal clusters (CCs) were found among the six clinical isolates in this study, with ST5, the most predominant complex clonal CC5 and CC8. Generally, clonal lineages ST5, ST8, ST152, and ST612 are among the most commonly reported in hospital environments, along with other sequence types of S. aureus [40]. S. aureus ST5, belonging to CC5, was predominant in this study and was previously reported among patients with bloodstream infections at Ruijin Hospital in Shanghai [3]. The detection of clonal complexes CC5 and CC8 agrees with a study by Smith et al. [16], which also found CC8, and CC5 were predominant in a study that analysed the genomic epidemiology of MRSA and MSSA from bloodstream infections in the USA. Their results revealed that the MDR phenotype observed in strains belonging to CC5 and CC8 was responsible for the occurrence of multidrug and methicillin resistance in the S. aureus population. MRSA strains belonging to CC8 and CC5 are frequently associated with global outbreaks and have been identified in Africa [41].
The spa typing revealed six different spa types, suggesting a non-clonal MRSA and MSSA distribution. The detection of spa types t1257, t045 and t355 agrees with a study conducted in South Africa, which analysed the diversity of SCCmec elements and spa types in S. aureus isolates from blood culture in the Gauteng, KwaZulu-Natal, Free State, and Western Cape provinces [14], in which t037 and t1257 were the most common and predominated throughout the seven-year study period. In this study, some antibiotic resistance genes were associated with specific MRSA clones belonging to spa types t1257 and t045, t9475. Shittu et al. (2021) found the spa types t045 and t1257 to be the most prevalent and associated with genes conferring resistance to aminoglycosides, trimethoprim, macrolides and tetracycline in clinical isolates of S. aureus from South Africa and Nigeria.
The analysis of SCCmec types revealed the presence of SCCmec type IVd (2B) and SCCmec type I (B) carrying the mecA gene, which occurred in tandem with mecR1 in both isolates. However, one MRSA (S11) isolate had a non-typeable SCCmec element cassette due to the missing cassette chromosome recombinase (ccr) gene complex [42]. The ccr gene complex is an essential component required to facilitate the integration or excision of the SCCmec element in the staphylococcal chromosome, and their loss has also been reported [43]. The SCCmec IV detected in our study is associated with the spa type t1257, previously reported in South Africa in S. aureus obtained from poultry isolates [15], implying its possible transfer between humans and animals.
We found different MRSA genotypes ST612-t1257-CC8, ST8-t9475-CC8, and ST5-t045-CC5, suggesting that MRSA isolates were not clonally and epidemiologically related. The ST612-t1257-CC8 identified in this study, is an endemic MRSA clone which have been reported in animal and clinical settings [14,15]. The ST5-I-MRSA, known as the pandemic British EMRSA-3 clone, was detected in the paediatric ward. This is similar to a study conducted in South Africa, where the t045-MRSA strain occurred in paediatric patients [18]. The isolation of t045-ST5-MRSA strain could confirm its successful persistence in the hospital and its capacity to cause infections in neonatal and paediatric wards [44].
Several virulence factors, including adherence, immune invasion, toxins, and exoenzymes associated with invasive infections, were detected in our isolates. The virulence genes encoding clumping factor proteins (clfA and clfB) are involved in the pathogenesis of S. aureus, including bacteremia [9]. Consistent with pathogenic S. aureus strains isolated in various environments globally, our isolates were characterized by icaADBC operon and (sdrC, sdrD, sdrE) involved in biofilm-forming genes [45]. Most strains haboured genes, including the alpha and gamma-hemolysin genes (hlgA, hlgB, hlgC, hly/hla, hlb), and the ica operon associated with pathogenicity and adhesion. Additionally, our isolates were characterised by various toxins, including lukE/D genes, and panton-valentine leukocidin (PVL) lukS-PV/lukF-PV genes in one MSSA, and MRSA strains. The expression of these PVL toxin genes in S. aureus isolates, lyses host cells and promotes virulence of the bacteria [46], which might worsen the outcomes S. aureus infection. Consistent with clinical S. aureus strains, our isolates were characterised by a capsular polysaccharide (CP) serotype 8, which shields the bacterial pathogen from host immune defence mechanisms associated with increased virulence in BSIs [47].
Most virulence genes including those encoding SEs, sak, hlg, luk, scn clfA, sbi, and associated MGEs were carried on chromosomes in the majority of isolates. The ica gene operon and vra genes were found to be associated with ISs (IS30, IS6) and recombinase for S11 (ST8) isolate from the surgical ward. The ica genes vraDEH genes have been shown to play an important role in biofilm formation [48], daptomycin resistance in S. aureus [49]. which could enhance antibiotic resistance traits and chronic infection. The occurrence of ST8-t9475 MRSA strains co-harbouring ica genes and genes encoding daptomycin resistance in ST8 MRSA could be advantageous to the ST8-t9475 colonization, invasion, and survival in the surgical ward. The virulence genes encoding SEs, eap, scn, sak, sph, lukH, and cadA, were found on a contig that had high sequence similarity to S. aureus strain ER10678.3 plasmid pER10678.3A.1 (CP051928.1), implying that they are mobilized by plasmids. Virulence genes, including those encoding hla/hld, toxin production, and biofilm formation, are plasmid-mediated [50], thus could easily facilitate their transfer resulting in highly pathogenic strains that may be difficult to treat.
Phylogenomic analyses revealed that the clinical isolates in this study clustered mainly with clinical isolates from hospital patients (Figure 2). ST5 study isolates were closely related to clinical isolates from South Africa suggesting possible dissemination of ST5 strains and adaptation in hospital environments. Furthermore, ST152 isolate was closely related to ST152 strains from Egypt and Ghana, implying a possible spread and epidemiological linkage between these isolates. ST152-PVL-producing S. aureus isolates is particularly frequent and widespread in West and Central Africa [51], and livestock [52]. The ST152- PVL-positive MSSA, has also been reported from cutaneous abscesses among mine workers at a gold mine in Gauteng, South Africa [53]. Identifying ST152 in livestock and humans suggests animal–human transmission, which requires further investigation. ST8 and ST612 isolates were closely related to ST8 isolated from Tanzania, indicating that ST612 is a double-locus variant of ST8. ST8 and ST612 isolates are potentially multidrug-resistant and highly virulent strains associated with hospital outbreaks [54].
4. Materials and Methods
4.1. Ethical Consideration
The study isolates were part of a larger surveillance study using the Global Antimicrobial Resistance and Use Surveillance System (GLASS) guidelines. Ethical approval for the study was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal under the following reference number BCA444/16.
4.2. Sample Collection and Bacterial identification
Forty-five putative Staphylococcus isolates were collected from blood cultures sourced from hospitals within the uMgungundlovu district in the KwaZulu-Natal province from November 2017 to December 2018. Isolates were identified by the National Health Laboratory Services (NHLS) using the automated VITEK 2 system (BioMérieux, MarcyL’Etoile, France). The WGS study sample consisted of a subset of 10 MDR isolates, the selection of isolates was based on their antibiograms. However, 4 isolates were excluded during the quality control process.
4.3. Antimicrobial Susceptibility Testing and MRSA detection
Antibiotic susceptibility of the S. aureus isolates was determined by the Kirby–Bauer disk-diffusion and interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) or Clinical and Laboratory Standards Institute (CLSI) breakpoints. The following antibiotics were tested: penicillin G (10 µg), ampicillin (10 µg), cefoxitin (30 µg) tigecycline (15 µg), nitrofurantoin (300µg), (interpreted using EUCAST breakpoints) (EUCAST, 2017), ciprofloxacin (5 µg), levofloxacin (5 µg), moxifloxacin (5 µg), erythromycin (15 µg), gentamicin (10µg), amikacin (30 µg), chloramphenicol (30µg), tetracycline (30µg), doxycycline (30µg), sulphamethoxazole/trimethoprim (1.25 µg + 23.75 µg), teicoplanin (30 µg), linezolid (30 µg), clindamycin (2 µg), rifampicin (5 µg) (interpreted using CLSI breakpoints) (CLSI, 2017). All antibiotic discs were from Oxoid (Oxoid, Basingstoke, UK). S. aureus ATCC 29213, was used as the control. Multidrug resistance (MDR) was defined as resistance to one or more antibiotics belonging to three or more different antibiotic classes [21].
4.4. Whole-Genome Sequencing (WGS) and bioinformatic analysis
The genomic DNA was extracted from the S. aureus isolates using the GenElute Bacterial Genomic DNA kit (Sigma Aldrich, St. Louis, USA) according to the manufacturer’s instructions. The quantity and quality of the extracted gDNA was analysed using NanoDrop 8000c (Thermo Scientific, Waltham, MA, USA). The Nextera XT DNA Library Preparation Kit (Illumina, San Diego, CA, USA) was used for library preparation. WGS was conducted using an Illumina NextSeq Machine (Illumina, San Diego, CA, USA). Good quality trimming of raw reads was done using Sickle v1.33 (https://github.com/najoshi/sickle). The raw reads were assembled spontaneously using the SPAdes v3.6.2 assembler (https://cab.spbu.ru/software/spades/). Subsequently, all contiguous sequences were submitted to NCBI and assigned accession numbers under BioProject
4.5. Genomic Analysis and Annotation
The draft genomes were submitted to GenBank and assigned accession numbers under the BioProject PRJNA400143. Analysis including antibiotic resistance genes, virulence factors and pathogenicity, mobile genetic elements (MGEs), plasmid replicons, and genotyping including MLST, spa, and SCCmec typing were performed the Centre for Genomic Epidemiology (CGE) (https://www.genomicepidemiology.org/services/), and their respective databases. Antibiotic resistance genes (ARGs) and other ABR determinants were identified using the CGE ResFinder 4.1 (https://cge.cbs.dtu.dk/servic es/ResFinder/), and the comprehensive antibiotic resistance database (https://card.mcmaster.ca/analyze/rgi). Virulence factors were identified using the virulence factor database (VFDB: http://www.mgc.ac.cn/VFs/main.htm. PHASTER was used to identify prophage elements (https://phaster.ca/). The accessory gene regulator (agr) typing was conducted through nucleotide BLAST. GenBank accession numbers AFS50129.1, AFS50128.1, AFS50130.1, and AFS50131.1 were used as reference sequences for agr type I to IV, respectively [22]. The synteny and genetic environment of ARGs and associated MGEs were investigated using GenBank’s general feature format (GFF3) files. The GFF3 files were imported into Geneious Prime 2020. 2 (https://www.geneious.com) for analysis [23]. The arginine catabolic mobile element (ACME) is a genomic island in Staphylococci that contains virulence factors including an arginine deiminase (arc) pathway and an oligopeptide permease (opp-3) system, which contribute to enhanced pathogenicity [24]. The ACME genes within the genomes were detected and aligned. Alignment of the ACME components made up of the arc operon, the opp-3 operon, and the kdp operon, was used to classify the ACME components as follows: arc and opp-3 operons (type I), the arc operon only (type II), the opp-3 operon only (type III), the arc and kdp operons (type IV), and all three arc, opp, and kdp operons (type V), using Pathosystems Resource Integration Center (PATRIC) (https://www.patricbrc.org/) annotations.
4.6. Single Nucleotide Polymorphism (SNP) Analysis in Antibiotic Resistance Strains
Mutations conferring resistance to fluoroquinolones and rifampicin were determined using BLASTN (https://blast.ncbi.nlm.nih.gov/Blast.cgi?PAGE_TYPE=BlastSearch). Briefly, gyrA, gyrB, parC, parE, and rpoB genes in a reference susceptible S. aureus ATCC 29213 were aligned with the corresponding genes from resistant isolates in this study with BLASTn to call for SNPs in those genes using the Clustal Omega tool (European Molecular Biology Laboratory). Mutations in the genomes of the study isolates were manually curated and tabulated.
4.7. Phylogenomic Analysis
Whole-genome sequences of S. aureus isolates from blood culture curated at the bacterial and viral bioinformatics resource center (BV-BRC) online platform (https://www.bv-brc.org/) from Northern Africa (Egypt, Algeria, Sudan), Western Africa (Ghana), and Eastern Africa (Tanzania) were downloaded and used together with our study’s isolates for phylogeny analysis. The selection of isolates was based on the sample source (blood culture). A phylogenomic tree of S. aureus was built using BV-BRC’s Phylogenetic Tree Building tool, using the nucleotide and amino acid sequences from 1,000 shared genes (https://www.bv-brc.org/). The generated phylogenetic trees were visualized, annotated, and edited using iTOL (https://itol.embl.de/) and Figtree (http://tree.bio.ed.ac.uk/software/figtree/).
4.8. Nucleotide Sequence Accession Number
The nucleotide sequences of MRSA (S29, S11, S31) and MSSA (S13, S24, S34) isolates were submitted to the NCBI GenBank database under the following accession numbers; JADQTH000000000, JADIXB000000000, JADIXC000000000, JADIXA000000000, JADIXE000000000, JADIXD000000000.
5. Conclusions
The study presents an insight into ARGs, virulence genes, MGEs, and genetic diversity of S. aureus collected from a public hospital in uMgungundlovu. We observed high diversity of spa types, STs, predominance of CC8, and CC5 indicating the genetic variability of S. aureus in hospital settings. The occurrence of pathogenic and MDR strains in the hospital setting, especially in ICU can pose a serious threat that limits the therapeutic options available. Here, we demonstrate that while MRSA displayed multidrug resistance, MSSA reflect potentially increasing resistance to the antibiotics used for treatment. Continuous surveillance and monitoring of MRSA and MSSA strains circulating in hospital environments is needed.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Patient demographics; Table S2: Genomic characteristics of S. aureus strains; Table S3: Virulence genes identified in MSSA and MRSA isolates in this study; Table S4: Distribution of insertion sequences and plasmid replicon among the Staphylococcus aureus strains; Table S5: Distribution of intact prophage region among the Staphylococcus aureus strains.
Author Contributions
Conceptualization, B.H., DGA and S.Y.E; methodology, B.H. A.I. and A.L.K.A; formal analysis, B.H., D.G.A., J.M., J.A. and A.L.KA; investigation, B.H.; resources, A.I., D.G.A. and S.Y.E ; writing—original draft preparation, B.H.; writing—review and editing, B.H., J.A., J.M., A.I., A.L.K.A., D.G.A., and S.Y.E; supervision, S.Y.E., A.L.K.A and D.G.A. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: This work was supported by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation of South Africa (Grant No. 98342), the SA MRC and UK MRC Newton Fund and the SAMRC Self-Initiated Research Grant and the College of Health Sciences university of KwaZulu-Natal, South Africa.
Institutional Review Board Statement
Ethical approval for the study was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal under the following reference number BCA444/16. The study isolates were part of a larger surveillance study using the Global Antimicrobial Resistance and Use Surveillance System (GLASS) guidelines.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We are grateful to Sumayya Haffejee of the National Health Laboratory Services for her assistance during sample collection and obtaining demographic data.
Conflicts of Interest
S.Y.E. is a chairperson of the Global Respiratory Infection Partnership and member of the Global Hygiene Council, both funded by unrestricted educational grants from Reckitt and Benckiser (Pty.), UK. The remaining authors declare that research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Asadollahi, P.; Farahani, N.N.; Mirzaii, M.; Khoramrooz, S.S.; van Belkum, A.; Asadollahi, K.; Dadashi, M.; Darban-Sarokhalil, D. Distribution of the Most Prevalent Spa Types Among Clinical Isolates of Methicillin-Resistant and-Susceptible Staphylococcus Aureus Around the World: A Review. Front. Microbiol. 2018, 9, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Tu, C.; Tan, C.; El-Sayed Ahmed, M.A.E.G.; Dai, M.; Xia, Y.; Liu, Y.; Zhong, L.L.; Shen, C.; Chen, G.; et al. Antimicrobial Resistance, Virulence Genes Profiling and Molecular Relatedness of Methicillin-Resistant Staphylococcus Aureus Strains Isolated from Hospitalized Patients in Guangdong Province, China. Infect. Drug Resist. 2019, 12, 447–459. [Google Scholar] [CrossRef] [PubMed]
- Gu, F.; He, W.; Xiao, S.; Wang, S.; Li, X.; Zeng, Q.; Ni, Y.; Han, L. Antimicrobial Resistance and Molecular Epidemiology of Staphylococcus Aureus Causing Bloodstream Infections at Ruijin Hospital in Shanghai from 2013 to 2018. Sci. Rep. 2020, 10, 6019. [Google Scholar] [CrossRef] [PubMed]
- Diekema, D.J.; Hsueh, P.R.; Mendes, R.E.; Pfaller, M.A.; Rolston, K. V.; Sader, H.S.; Jones, R.N. The Microbiology of Bloodstream Infection: 20-Year Trends from The SENTRY Antimicrobial Surveillance Program. Antimicrob. Agents Chemother. 2019, 63, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.A.; Sharma-Kuinkel, B.K.; Maskarinec, S.A.; Eichenberger, E.M.; Shah, P.P.; Carugati, M.; Holland, T.L.; Fowler, V.G. Methicillin-Resistant Staphylococcus Aureus: An Overview of Basic and Clinical Research. Nat. Rev. Microbiol. 2019, 17, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Hadyeh, E.; Azmi, K.; Seir, R.A.; Abdellatief, I.; Abdeen, Z. Molecular Characterization of Methicillin Resistant Staphylococcus Aureus in West Bank-Palestine. Front. Public Heal. 2019, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Zhou, W.; Zhan, Q.; Chen, Y.; Luo, Q.; Shen, P.; Xiao, Y. Genomic Epidemiology and Characterisation of Penicillin-Sensitive Staphylococcus Aureus Isolates from Invasive Bloodstream Infections in China: An Increasing Prevalence and Higher Diversity in Genetic Typing Be Revealed. Emerg. Microbes Infect. 2022, 11, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Liu, J.; Zhan, Y.; Wang, L.; Jiang, Y.; Zhang, Y.; Sun, N.; Hou, N. Molecular Typing Revealed the Emergence of PVL-Positive Sequence Type 22 Methicillin-Susceptible Staphylococcus Aureus in Urumqi, North Western China. Infect. Drug Resist. 2019, 12, 1719–1728. [Google Scholar] [CrossRef] [PubMed]
- Foster, T.J. The MSCRAMM Family of Cell-Wall-Anchored Surface Proteins of Gram-Positive Cocci. Trends Microbiol. 2019, 27, 927–941. [Google Scholar] [CrossRef]
- Foster, T.J.; Geoghegan, J.A.; Ganesh, V.K.; Hook, M. Adhesion, Invasion and Evasion: The Many Functions of the Surface Proteins of Staphylococcus Aureus. Nat. Rev. Microbiol. 2014, 12, 46–62. [Google Scholar] [CrossRef]
- Warnes, S.L.; Highmore, C.J.; Keevil, C.W. Horizontal Transfer of Antibiotic Resistance Genes on Abiotic Touch Surfaces: Implications for Public Health. MBio 2012, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Greenwood-Quaintance, K.E.; Uhl, J.R.; Cunningham, S.A.; Chia, N.; Jeraldo, P.R.; Sampathkumar, P.; Nelson, H.; Patel, R. Molecular Epidemiology of Staphylococcus Aureus Bacteremia in a Single Large Minnesota Medical Center in 2015 As Assessed Using MLST, Core Genome MLST and Spa Typing. PLoS One 2017, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Perovic, O.; Iyaloo, S.; Kularatne, R.; Lowman, W.; Bosman, N.; Wadula, J.; Seetharam, S.; Duse, A.; Mbelle, N.; Bamford, C.; et al. Prevalence and Trends of Staphylococcus Aureus Bacteraemia in Hospitalized Patients in South Africa, 2010 to 2012: Laboratory-Based Surveillance Mapping of Antimicrobial Resistance and Molecular Epidemiology. PLoS One 2015, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Singh-Moodley, A.; Lowe, M.; Mogokotleng, R.; Perovic, O. Diversity of SCCmec Elements and Spa Types in South African Staphylococcus Aureus MecA-Positive Blood Culture Isolates. BMC Infect. Dis. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Amoako, D.G.; Somboro, A.M.; Abia, A.L.K.; Allam, M.; Ismail, A.; Bester, L.; Essack, S.Y. Genomic Analysis of Methicillin-Resistant Staphylococcus Aureus Isolated from Poultry and Occupational Farm Workers in Umgungundlovu District, South Africa. Sci. Total Environ. 2019, 670, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.T.; Eckhardt, E.M.; Hansel, N.B.; Eliato, T.R.; Martin, I.W.; Andam, C.P. Genomic Epidemiology of Methicillin-Resistant and-Susceptible Staphylococcus Aureus from Bloodstream Infections. BMC Infect. Dis. 2021, 21, 1–14. [Google Scholar] [CrossRef]
- Schaumburg, F.; Alabi, A.S.; Peters, G.; Becker, K. New Epidemiology of Staphylococcus Aureus Infection in Africa. Clin. Microbiol. Infect. 2014, 20, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Strasheim, W.; Perovic, O.; Singh-Moodley, A.; Kwanda, S.; Ismail, A.; Lowe, M. Ward-Specific Clustering of Methicillin-Resistant Staphylococcus Aureus Spa-Type T037 and T045 in Two Hospitals in South Africa: 2013 to 2017. PLoS One 2021, 16, 1–16. [Google Scholar] [CrossRef] [PubMed]
- EUCAST European Committee on Antimicrobial Susceptibility Testing, Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 8 2017. Accessed on November 2018. www.eucast.org/clinical_breakpoints/, 0–77.
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Seventh Informational Supplement. CLSI Document M100-S27. 2017; ISBN 1562387855.
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Francois, P.; Koessler, T.; Huyghe, A.; Harbarth, S.; Bento, M.; Lew, D.; Pittet, D.; Schrenzel, J. Rapid Staphylococcus Aureus Agr Type Determination by a Novel Multiplex Real-Time Quantitative PCR Assay. J. Clin. Microbiol. 2006, 44, 1892–1895. [Google Scholar] [CrossRef]
- Mbanga, J.; Amoako, D.G.; Abia, A.L.K.; Allam, M.; Ismail, A.; Essack, S.Y. Genomic Insights of Multidrug-Resistant Escherichia Coli From Wastewater Sources and Their Association With Clinical Pathogens in South Africa. Front. Vet. Sci. 2021, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Conly, J.; McClure, J.A.; Kurwa, H.A.; Zhang, K. Arginine Catabolic Mobile Element in Evolution and Pathogenicity of the Community-Associated Methicillin-Resistant Staphylococcus Aureus Strain USA300. Microorganisms 2020, 8, 275. [Google Scholar] [CrossRef] [PubMed]
- Foster, T.J. Antibiotic Resistance in Staphylococcus Aureus. Current Status and Future Prospects. FEMS Microbiol. Rev. 2017, 41, 430–449. [Google Scholar] [CrossRef] [PubMed]
- Silva, V.; Hermenegildo, S.; Ferreira, C.; Manaia, C.M.; Capita, R.; Alonso-Calleja, C.; Carvalho, I.; Pereira, J.E.; Maltez, L.; Capelo, J.L.; et al. Genetic Characterization of Methicillin-Resistant Staphylococcus Aureus Isolates from Human Bloodstream Infections: Detection of MLSB Resistance. Antibiotics 2020, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Asante, J.; Govinden, U.; Owusu-Ofori, A.; Bester, L.A.; Essack, S.Y. Molecular Characterization of Methicillin-Resistant Staphylococcus Aureus Isolates from a Hospital in Ghana. African J. Clin. Exp. Microbiol. 2019, 20, 164. [Google Scholar] [CrossRef]
- Mkhize, S.; Amoako, D.G.; Shobo, C.O.; Zishiri, O.T.; Bester, L.A. Genotypic and Phenotypic Characterizations of Methicillin-Resistant Staphylococcus Aureus (MRSA) on Frequently Touched Sites from Public Hospitals in South Africa. Int. J. Microbiol. 2021; 6011045. [Google Scholar] [CrossRef]
- McCarthy, A.J.; Lindsay, J.A. The Distribution of Plasmids That Carry Virulence and Resistance Genes in Staphylococcus Aureus Is Lineage Associated. BMC Microbiol. 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Ocloo, R.; Newton-Foot, M.; Ziebuhr, W.; Whitelaw, A.C. Molecular Epidemiology and Antibiotic Resistance of Staphylococci Other than Staphylococcus Aureus in Children in Cape Town, South Africa. Front. Microbiol. 2023, 14, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Pennone, V.; Prieto, M.; Avelino, Á.; Cobo-diaz, J.F. Antimicrobial Resistance Genes Analysis of Publicly Available Staphylococcus Aureus Genomes. 2022, 1–19.
- Shittu, A.O.; Adesoji, T.; Udo, E.E. DNA Microarray Analysis of Staphylococcus Aureus from Nigeria and South Africa. PLoS One 2021, 16, 1–11. [Google Scholar] [CrossRef]
- Parsons, C.; Lee, S.; Kathariou, S. Dissemination and Conservation of Cadmium and Arsenic Resistance Determinants in Listeria and Other Gram-Positive Bacteria. Mol. Microbiol. 2020, 113, 560–569. [Google Scholar] [CrossRef]
- Al-Trad, E.I.; Chew, C.H.; Che Hamzah, A.M.; Suhaili, Z.; Rahman, N.I.A.; Ismail, S.; Puah, S.M.; Chua, K.H.; Kwong, S.M.; Yeo, C.C. The Plasmidomic Landscape of Clinical Methicillin-Resistant Staphylococcus Aureus Isolates from Malaysia. Antibiotics 2023, 12, 733. [Google Scholar] [CrossRef]
- Zhong, Q.; Cruz-Paredes, C.; Zhang, S.; Rousk, J. Can Heavy Metal Pollution Induce Bacterial Resistance to Heavy Metals and Antibiotics in Soils from An Ancient Land-Mine? J. Hazard. Mater. 2021, 124962. [Google Scholar] [CrossRef] [PubMed]
- Kleinert, F.; Kallies, R.; Hort, M.; Zweynert, A.; Szekat, C.; Nagel, M.; Bierbaum, G. Influence of IS256 on Genome Variability and Formation of Small-Colony Variants in Staphylococcus Aureus. Antimicrob. Agents Chemother. 2017, 61, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Chen, C.C.; Lu, Y.C.; Chuang, Y.C.; Tang, H.J. The Clinical Significance of Silent Mutations with Respect to Ciprofloxacin Resistance in MRSA. Infect. Drug Resist. 2018, 11, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Mbelle, N.M.; Feldman, C.; Osei Sekyere, J.; Maningi, N.E.; Modipane, L.; Essack, S.Y. Publisher Correction: The Resistome, Mobilome, Virulome and Phylogenomics of Multidrug-Resistant Escherichia Coli Clinical Isolates from Pretoria, South Africa. Sci. Rep. 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Wang, W.; Baker, M.; Hu, Y.; Xu, J.; Yang, D.; Maciel-Guerra, A.; Xue, N.; Li, H.; Yan, S.; Li, M.; et al. Whole-Genome Sequencing and Machine Learning Analysis of Staphylococcus Aureus from Multiple Heterogeneous Sources in China Reveals Common Genetic Traits of Antimicrobial Resistance. mSystems 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Sands, K.; Carvalho, M.J.; Spiller, O.B.; Portal, E.A.R.; Thomson, K.; Watkins, W.J.; Mathias, J.; Dyer, C.; Akpulu, C.; Andrews, R.; et al. Characterisation of Staphylococci Species from Neonatal Blood Cultures in Low- and Middle-Income Countries. BMC Infect. Dis. 2022, 22, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Lawal, O.U.; Ayobami, O.; Abouelfetouh, A.; Mourabit, N.; Kaba, M.; Egyir, B.; Abdulgader, S.M.; Shittu, A.O. A 6-Year Update on the Diversity of Methicillin-Resistant Staphylococcus Aureus Clones in Africa: A Systematic Review. Front. Microbiol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Elshabrawy, W.; Elsayed Zaki, M.; Farag Kamel, M. Genetic and Phenotypic Study of Methicillin-Resistant Staphylococcus Aureus Among Patients and Health Care Workers in Mansoura University Hospital, Egypt. Iran. J. Microbiol. 2017, 9, 82–88. [Google Scholar]
- Soliman, M.S.; Soliman, N.S.; El-Manakhly, A.R.; Elbanna, S.A.; Aziz, R.K.; El-Kholy, A.A. Genomic Characterization of Methicillin-Resistant Staphylococcus Aureus (MRSA) by High-Throughput Sequencing in A Tertiary Care Hospital. Genes (Basel). 2020, 11, 1–17. [Google Scholar] [CrossRef]
- Abdulgader, S.M.; van Rijswijk, A.; Whitelaw, A.; Newton-Foot, M. The Association Between Pathogen Factors and Clinical Outcomes in Patients With Staphylococcus Aureus Bacteraemia in a Tertiary Hospital, Cape Town. Int. J. Infect. Dis. 2020, 91, 111–118. [Google Scholar] [CrossRef]
- Peng, Q.; Tang, X.; Dong, W.; Sun, N.; Yuan, W. A Review of Biofilm Formation of Staphylococcus Aureus and Its Regulation Mechanism. Antibiotics 2023, 12, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, M.T.; Lubkin, A.; Reyes-Robles, T.; Day, C.J.; Lacey, K.A.; Jennings, M.P.; Torres, V.J. Identification of a Domain Critical for Staphylococcus Aureus LuKED Receptor Targeting and Lysis of Erythrocytes. J. Biol. Chem. 2020, 295, 17241–17250. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.; Timofeyeva, Y.; Jamrozy, D.; Rojas, E.; Hao, L.; Silmon de Monerri, N.C.; Hawkins, J.; Singh, G.; Cai, B.; Liberator, P.; et al. Molecular Epidemiology and Expression of Capsular Polysaccharides in Staphylococcus Aureus Clinical Isolates in the United States. PLoS One 2019, 14, 356. [Google Scholar] [CrossRef] [PubMed]
- Singh, S. , Singh, S. K., Chowdhury, I., & Singh, R. Understanding the Mechanism of Bacterial Biofilms Resistance to Antimicrobial Agents. Open Microbiol. J. 2017, 11, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Popella, P.; Krauss, S.; Ebner, P.; Nega, M.; Deibert, J.; Götz, F. VraH Is the Third Component of the Staphylococcus Aureus VraDEH System Involved in Gallidermin and Daptomycin Resistance and Pathogenicity. Antimicrob. Agents Chemother. 2016, 60, 2391–2401. [Google Scholar] [CrossRef] [PubMed]
- Bukowski, M.; Piwowarczyk, R.; Madry, A.; Zagorski-Przybylo, R.; Hydzik, M.; Wladyka, B. Prevalence of Antibiotic and Heavy Metal Resistance Determinants and Virulence-Related Genetic Elements in Plasmids of Staphylococcus Aureus. Front. Microbiol. 2019, 10, 1–14. [Google Scholar] [CrossRef]
- Abdulgader, S.M.; Shittu, A.O.; Nicol, M.P.; Kaba, M. Molecular Epidemiology of Methicillin-Resistant Staphylococcus Aureus in Africa: A Systematic Review. Front. Microbiol. 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Agabou, A.; Ouchenane, Z.; Essebe, C.N.; Khemissi, S.; Chehboub, M.T.E.; Chehboub, I.B.; Sotto, A.; Dunyach-Remy, C.; Lavigne, J.P. Emergence of Nasal Carriage of ST80 and ST152 PVL+ Staphylococcus Aureus Isolates from Livestock in Algeria. Toxins (Basel). 2017, 9, 303. [Google Scholar] [CrossRef] [PubMed]
- Ismail, H.; Govender, N.P.; Singh-Moodley, A.; Van Schalkwyk, E.; Shuping, L.; Moema, I.; Feller, G.; Mogokotleng, R.; Strasheim, W.; Lowe, M.; et al. An Outbreak of Cutaneous Abscesses Caused by Panton-Valentine Leukocidin-Producing Methicillin-Susceptible Staphylococcus Aureus Among Gold Mine Workers, South Africa, November 2017 to March 2018. BMC Infect. Dis. 2020, 20, 1–13. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, H.; Wang, B.; Zhou, Y.; Xu, Y.; Rao, L.; Ai, W.; Guo, Y.; Wu, X.; Yu, J.; et al. Identification of Methicillin-Resistant Staphylococcus Aureus ST8 Isolates in China with Potential High Virulence. Emerg. Microbes Infect. 2022, 11, 507–518. [Google Scholar] [CrossRef]
Figure 1.
Circular phylogenetic tree with colour annotations depicting the relationship between S. aureus isolates from this study coloured in green and African blood culture isolates coloured in purple.
Figure 1.
Circular phylogenetic tree with colour annotations depicting the relationship between S. aureus isolates from this study coloured in green and African blood culture isolates coloured in purple.
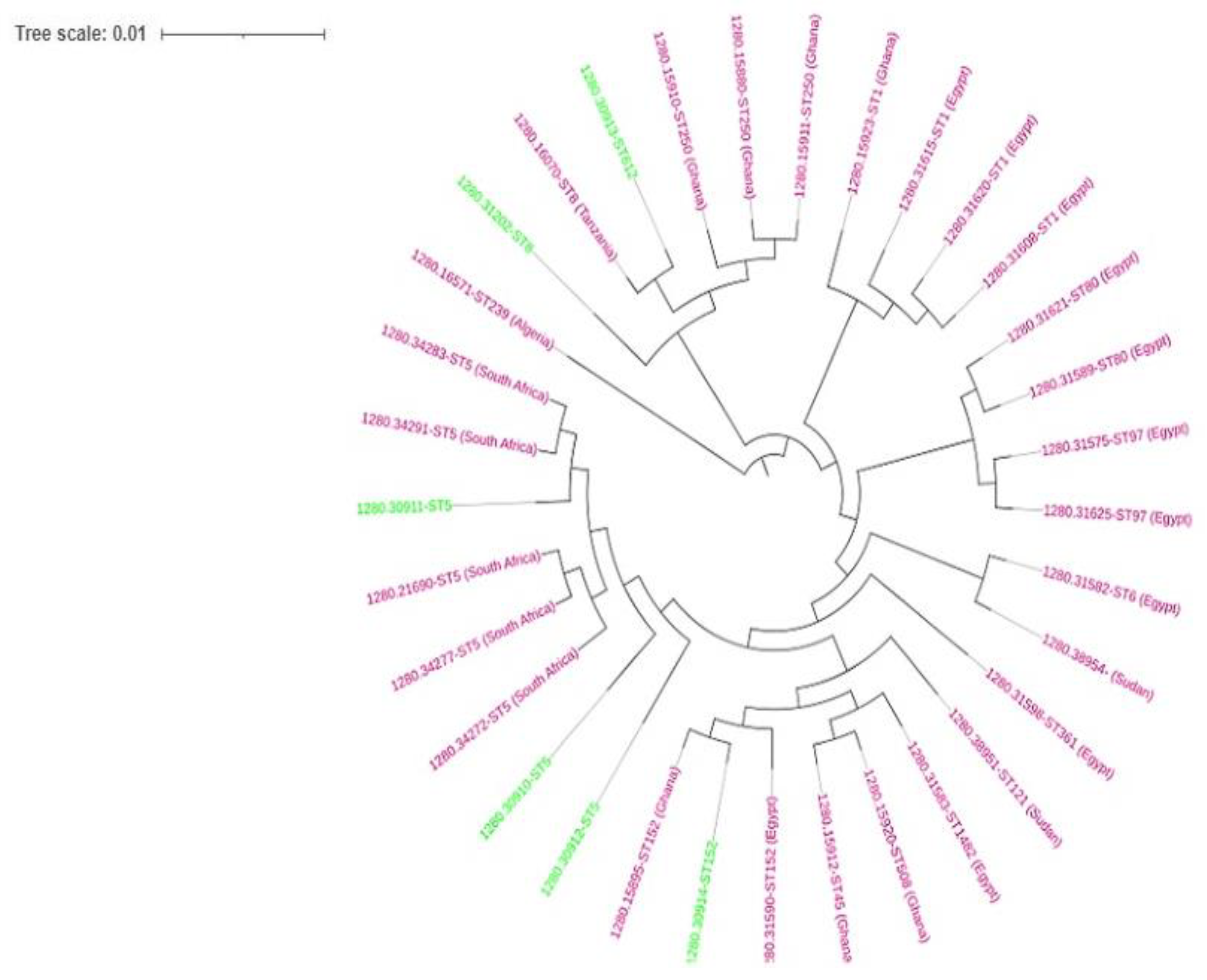
Figure 2.
The phylogenetic branch and metadata [spa type, sequence type (ST), clonal complex, SCCmec types and ARGs coupled using Phandango (https://github.com/jameshadfield/phandango/wiki) in S. aureus isolates.
Figure 2.
The phylogenetic branch and metadata [spa type, sequence type (ST), clonal complex, SCCmec types and ARGs coupled using Phandango (https://github.com/jameshadfield/phandango/wiki) in S. aureus isolates.
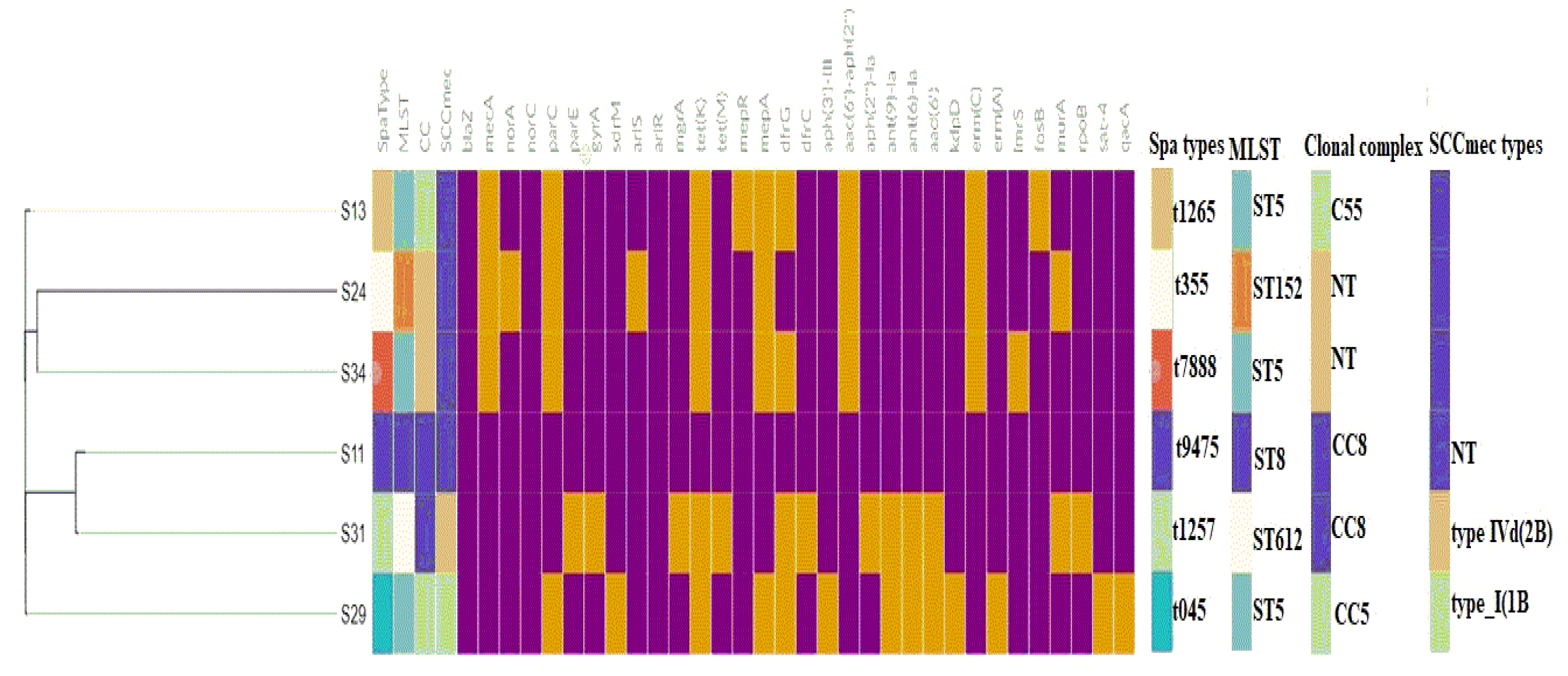

Table 1.
Antibiotic susceptibility profiles, age and demographic characteristics of patients with BSIs attributed to S. aureus.
Table 1.
Antibiotic susceptibility profiles, age and demographic characteristics of patients with BSIs attributed to S. aureus.
| Isolate ID | Species | Sex | Ward | Age | Antibiotics | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PEN | AMP | FOX | CIP | MXF | LEV | GEN | AMK | ERY | CLI | TET | DOX | TGC | CHL | NIT | SXT | VAN | RIF | LZD | TEC | |||||
| S11 | MRSA | F | Surgical ward | 17 years | R | R | R | R | R | R | R | R | R | R | R | R | R | I | S | R | S | R | R | R |
| S29 | MRSA | M | Paediatric ward | <1 year | R | R | R | R | R | R | R | R | I | R | R | R | S | I | S | R | S | I | R | R |
| S31 | MRSA | F | Surgical ward | 3 years | R | R | R | R | R | R | R | R | R | R | R | R | S | R | S | R | S | R | R | R |
| S24 | MSSA | M | ICU | 33 years | R | S | S | R | R | R | S | S | R | R | R | I | S | I | R | R | S | R | I | I |
| S13 | MSSA | M | ICU | <1 year | R | S | S | R | R | R | I | R | I | R | I | R | S | S | S | I | S | S | I | R |
| S34 | MSSA | M | NICU | <1 year | R | S | S | R | R | R | I | R | I | R | R | R | S | I | S | S | S | I | S | S |
Key: PEN, penicillin; AMP, ampicillin; FOX, cefoxitin; CIP, ciprofloxacin; MXF, moxifloxacin; LEV, levofloxacin; GEN, gentamicin, AMK, amikacin; ERY, erythromycin; CLI, clindamycin; TET, tetracycline; DOX, doxycycline; TGC, tigecycline; CHL, chloramphenicol; NIT, nitrofurantoin; SXT, trimethoprim-sulfamethoxazole; VAN, vancomycin; RIF, rifampicin; LZD, linezolid and TEC, teicoplanin. R, resistant; I, intermediate; S, susceptible; M, male; F, female; NICU, neonatal intensive care unit; ICU, intensive care unit.
Table 2.
Genotypic characteristics of the of S. aureus implicated in BSIs.
| Isolate ID | MRSA/MSSA | MLST | spa Type | Resistome | Plasmid replicon type | Insertion sequences | Confirmed CRISPRs (CAS) | Clonal complex | *SCCmec type | agr type b | ACME type | Pathogenicity score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S11 | MRSA | ST8 | t9475 | blaZ, mecA, aac(6’)-aph(2’‘), parC, dfrG, erm(C), grlA, tetK, mepR, mepA, norA, norC, fosB, arlR, arlS, mgrA, sdrM, kdpD | rep10, rep7a, rep7c | - | 6 (0) | CC8 | - | Type I | Type II | 0.982 (882) |
| S29 | MRSA | ST5 | t045 | blaZ, mecA, aph(3’)-III, aac(6’)-aph(2’‘), ant(6)-Ia, ant(9)-Ia, aad(6’), erm(C), erm(A), qacA, mepR, fosB, arlR, arlS, norA, norC, mgrA, sat-4 | rep10, rep21 | IS6, IS256 | 12 (0) | CC5 | SCCmec type I(1B) | Type II | - | 0.98 (914) |
| S31 | MRSA | ST612 | t1257 | blaZ, mecA, aac(6’)-aph(2’‘), aph(2’‘)-Ia, aad(6’), ant(6)-Ia, ant(9)-Ia , tet(M), mepR, mepA, dfrC, parC, erm(C), parE, gyrA, rpoB, fosB, arlR, arlS, norA, norC, murA, sdrM, kdpD | rep7c, rep20 | IS256, IS6 | 7 (0) | CC8 | SCCmec type IVd(2B) | Type I | - | 0.976 (978) |
| S24 | MSSA | ST152 | t355 | blaZ, dfrG, mepR, mgrA, arlR, kdpD, norC, sdrM, murA | rep16, rep5a | - | 8 (0) | - | - | Type IV | - | 0.975(225) |
| S13 | MSSA | ST5 | t1265 | blaZ, norA, norC, arlR, arlS, sdrM, mgrA, fosB, kdpD | rep20 | - | 9 (0) | CC5 | - | Type II | - | 0.985 (844) |
| S34 | MSSA | ST5 | t7888 | blaZ, norA, norC, sdrM, mepR, arlS, alrR, kdpD, mgrA, fosB, lmrS | rep19, rep16, rep20, rep5a | 1S6 | 7 (0) | - | Type II | - | 0.983 (871) |
*SCCmec typing was predicted with the SCCmecFinder, MSSA –Methicillin-susceptible Staphylococcus aureus, MRSA- Methicillin-resistant Staphylococcus aureus2.5. In Silico ARGs Analysis.
Table 3.
Genetic context of virulence genes in S. aureus isolates.
| Strain (MLST) | Strain | Contig | Synteny of virulence genes and MGEs | Plasmid/chromosomal sequence with closest nucleotide homology (accession number) |
|---|---|---|---|---|
| S11 (ST8) | MRSA | 4 | pmtC:pmtB:pmtA:eap::scn::sak:::sph::lukG::lukH::intergrase:::agrB | S. aureus strain Laus385 chromosome (CP071350.1) |
| 6 | icaR::icaD:icaB:icaC:vraD:vraE:vraH::IS30:vraH::recombinase:IS6 | S. aureus strain TF3198 chromosome, complete genome (CP023561.1) | ||
| 10 | lukE:lukD::splA::epiE::splA:splB:splC:splD:splE:splF::pepA1:transposase | S. aureus strain 82 chromosome, complete genome (CP031661.1) | ||
| S29 (ST5) | MRSA | 53 | type I toxin-antitoxin system:IS6:cadD | S. aureus strain MIN-175 chromosome (CP086121.1) |
| 40 | clfA:vwb:emp | S. aureus strain ER02693.3 chromosome, complete genome (CP030605.1) | ||
| S31(ST612) | MRSA | 11 | pmtD:pmtC:pmtB:pmtA::eap:scn::sak | S. aureus strain 2395 USA500, complete genome (CP007499.1) |
| 15 | lukE:lukD::::splA:splB:splC:splF::type I restriction-modification system | S. aureus strain NRL 02/947 chromosome, complete genome (CP103850.1) | ||
| 19 | lukG:lukH:pathogenicity island:intergrase::phenol-soluble modulin:agrB | S. aureus strain 2395 USA500, complete genome (CP007499.1) | ||
| 22 | seq:sek:integrase::::emp:clfA | S. aureus strain 2395 USA500, complete genome (CP007499.1) | ||
| 33 | recombinase::universal stress protein:::cadD::seq:sek:integrase:::emp:clfA | S. aureus plasmid SAP017A, complete sequence (GQ900382.1) | ||
| 64 | sea:putative holin-like toxin | S. aureus strain R50 chromosome, complete genome (CP039167.1) | ||
| S13 (ST5) | MSSA | 4 | sbi:hlgA:hlgC:hlgB | S. aureus strain AR462 chromosome, complete genome (CP029086.1) |
| 5 | scpA:::eap::scn:sak::::::intergrase:sph:lukH:sbi:hlgA:hlgC:hlgB | S. aureus strain pt239 chromosome, complete genome (CP049467.1) | ||
| 15 | IS6::cadD:::sed:sej:ser::recombinases:cpA::eap::scn:sak::integrase:sph:lukH | S. aureus strain ER10678.3 plasmid pER10678.3A.1 (CP051928.1) | ||
| S24 ST152) | MSSA | 8 | arsB::crcB::scn:sak:::recombinase::type II toxin-antitoxin system toxin:intergrase | S. aureus strain UMCG579 chromosome, complete genome (CP091066.1) |
| 21 | cadD:type toxin-antitoxin::integrase | S. aureus strain GHA13 chromosome (CP043911.1) | ||
| 11 | BrxA/BrxB:::msrA:msrB:::norD::cspA:cvfB | S. aureus strain NGA84b chromosome, complete genome (CP051165.2) | ||
| S34 (ST5) | MSSA | 7 | eap/map::scn:sak::::sea:::type II toxin-antitoxin:integrase:sph:lukG:lukH | S. aureus strain HPV107 chromosome, complete genome (CP026074.1) |
| 8 | clfA:vwb:emp::thermonuclease protein:::sek:seq::pathogenicity island | S. aureus strain B4-59C chromosome, complete genome (CP042153.1) | ||
| 12 | sem:sei:seu:sen:seg:::lukE:lukD::splA:splB:splC:splD:splF | S. aureus strain ER03588.3 chromosome, complete genome (CP030595.1) | ||
| 14 | isdB:isdA:isdC:isdD:isdE:isdF::isdG::ecb::efb:scb | S. aureus strain B3-17D chromosome, complete genome (CP042157.1) | ||
| 20 | SSL13:SSL12:hyl | S. aureus strain NAS_AN_239 chromosome, complete genome (CP062409.1) |
*Virulence gene(s) in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



