
Submitted:
13 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Polycystic ovary syndrome (PCOS) is a common condition in reproductive-age women. Women with PCOS are at higher risk of pregnancy complications including gestational diabetes (GDM). The prevalence of PCOS and GDM varies according to the diagnostic criteria used. The mechanism for the occurrence of GDM in women with PCOS is still unclear. Materials & Methods- A systematic search of the electronic database was done using keywords like PCOS, and GDM to include studies between April 2008 and March 2023 where uniform diagnostic criteria were used. Studies were excluded with high-risk of bias after the assessment of bias, and meta-analysis was done with relative risks and confidence intervals. Results & Discussion-Out of 1896 search results, 95 were selected for full-text. The quality of the studies was scrutinized and a total of 28 studies were included as they fulfilled the inclusion criteria. The incidence of GDM in women with PCOS was found to be 10.55 % (2.9- 54.9%) from pooled data involving 1,280,245. The prevalence of PCOS in women diagnosed with GDM was found from pooled data of 36,351 women in retrospective studies to be 2.47% (1.5- 50.1%). Selection predominantly included cohort studies, most commonly from China. The meta-analysis reported the risk of GDM is higher in women with PCOS than in those without PCOS (HR: 1.59, 95% CI: 1.27–1.91, p < 0.001). Family history of diabetes, ethnicity, pre-pregnancy BMI, insulin resistance, gestational weight gain, use of assisted reproductive techniques, and multifetal gestation were the risk factors for GDM in women with PCOS. Conclusion- The prevalence of GDM in patients with PCOS is high, but the causality is complex. The newer predictive models are promising in clarifying the causative relationships, yet use various parameters at different cut-offs. There is a need for the development of universally acceptable parameters for the early prediction of GDM in women with PCOS.
Keywords:
polycystic ovary syndrome
; gestational diabetes mellitus
; systematic review
; meta-analysis
; risk factors for gestational diabetes
1. Introduction
Polycystic ovary syndrome (PCOS) is one of the most prevalent endocrine conditions affecting women of reproductive age. Approximately, 5 to 10% of women have the condition [1]. According to the population investigated and the diagnostic criteria employed, the prevalence can be between 8 to 30% in reproductive-aged women, making it the most prevalent endocrinopathy in society [2,3,4]. In 2019, the prevalence of PCOS in the Middle East and Africa was 6,647,566 cases, with an age-standardized point prevalence of 2079.7 per 100,000 women representing a 37.9% increase in 29 years [5]. It is one of the main growing concerns among adolescents all over the world [6]. Amenorrhea, oligomenorrhea, obesity, infertility, and anovulation are among the common symptoms of PCOS [7]. Although alternative prediction models including anti-mullerian hormone (AMH), Body mass index (BMI), and serum hormone binding globulin (SHBG) are suggested, the most accepted diagnostic criteria is the Rotterdam criteria [8]. Diagnosis by Rotterdam criteria includes (2 out of 3) of the following-
- Oligo- or anovulation
- Clinical and/or biochemical signs of hyperandrogenism,
- Polycystic ovaries
and exclusion of other etiologies (congenital adrenal hyperplasia, androgen-secreting tumors, Cushing’s syndrome) [9]. Most patients of PCOS can conceive after receiving treatment with menstrual cycle adjustment, ovulation induction, and assisted reproductive technology, but because of the influence of underlying diseases, although the pregnancy can be successful, the likelihood of complications during pregnancy is relatively high [8,10]. PCOS can cause various pregnancy complications, affecting the mother, fetus, and neonate. Complications include pregnancy-induced hypertension, preeclampsia, GDM, spontaneous preterm birth, and an increased necessity for a cesarean section in the mother. Regarding fetal outcomes, PCOS has also been correlated with elevated neonatal morbidity, prematurity, fetal growth restriction, birth weight variations (both large and small for gestational age), and transfer to the Neonatal Intensive Care Unit [11].
Gestational Diabetes Mellitus (GDM) is defined as impaired glucose tolerance that is induced by pregnancy, perhaps from exaggerated physiologic changes in glucose metabolism [12,13]. It is a common complication in pregnancy having a significant negative impact on pregnancy and there is an increasing trend in the prevalence of GDM [14,15,16]. The prevalence of GDM can vary significantly depending on the diagnostic criteria used [17]. Different studies report a prevalence between 5.4%- 37.7% depending on the criteria used [18,19,20,21,22]. There is considerable controversy in the criteria for the diagnosis of GDM. This is mainly because of the lack of set standard reference intervals. As GDM is influenced by genetics, ethnicity, lifestyle, and socioeconomic and societal factors, having a standard global criterion is a challenge. The available diagnostic criteria proposed by different associations include the American Diabetes Association, World Health Organization, International Association of Diabetes and Pregnancy Study Group (IADPSG), the Australasian Diabetes in Pregnancy Society (ADIPS), Diabetes Canada, German Association for Gynecology and Obstetrics (DGGG), Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) Study Cooperative Research Group, and few others [23,24,25,26]. Commonly used diagnostic criteria for GDM are ADA, IADPSG, and WHO all using Oral glucose tolerance tests (OGTT) [20,27,28] [Table 1].
There are various risk factors for GDM identified through previous research. Studies including 18589 and 16 286 pregnant women in China reported risk factors for GDM as advanced maternal age, higher pre-pregnancy body mass index (BMI), a family history of diabetes, weight gain during pregnancy, and habitual smoking [18,29]. Another study reported higher parity, previous history of GDM, and previous history of macrocosmic babies as additional risk factors [30]. PCOS has been linked to an increased risk of GDM [31]. The proposed mechanism includes a rise of hormones such as estrogen, progesterone, and prolactin, which exacerbates the underlying insulin resistance (IR) present in women with PCOS leading to GDM [2]. It has been reported through meta-analyses that women with PCOS are at significantly higher risk for GDM (ranging from 2.8-3.7) compared to those without PCOS [32,33,34,35]. However, there are significant inconsistencies among studies regarding diagnostic criteria. Moreover, in countries where risk-based screening is practiced, PCOS is considered a condition for GDM screening, but in countries with universal screening, the same protocol is used for women with and without PCOS [36].
The exact prevalence of GDM in PCOS women is still unknown due to differences in diagnostic criteria for both PCOS and GDM and the inability to rule out effects of confounders like ethnicity, and obesity. In a few studies, having a first-degree relative with type 2 diabetes mellitus, serum levels of fasting glucose, fasting insulin, androstenedione, and SHBG levels before conception were identified as predictors of GDM [37]. Furthermore, a significant proportion of women with PCOS may have pre-gestational DM [38] and unless screened for earlier in the pregnancy, the prevalence of GDM will be inaccurate. Hence through this scoping review, we aim to find out the gross prevalence of GDM in women with PCOS and explore the effect of confounders.
2. Materials and Methods
Selection criteria
A systematic search of PubMed, Embase, MedRxiv, BioRxiv, Google Scholar, EBSCO MEDLINE, Web of Science, and Scopus electronic databases was done. Medical subject handling terms (MeSH) and free-text term keywords like Polycystic ovary syndrome, and PCOS were used in combination with gestational diabetes, GDM, and diabetes to include studies between April 2008 and March 2023. A random effect model was very helpful in pooling incidence in females associating PCOS to GDM using statistical analyses. The search consisted of only English-language articles including Cohorts, case-control studies, case reports, and case series. After a thorough screening, no randomized control trials were found.
Inclusion criteria
The studies fulfilling both 1 and 2 were included for review.
- Studies reporting pregnant women with pre-pregnancy confirmed PCOS by Rotterdam criteria.
- Studies using either 100 grams or 75 grams Oral Glucose Tolerance Test (OGTT) for screening GDM.
- Studies including both PCOS and GDM.
Exclusion criteria
Exclusions consisted of duplicated studies, review articles, articles in languages other than English, articles where full-text can only be purchased, studies where PCOS and GDM were diagnosed with other criteria, or self-reported. Conference abstracts, expert opinions, and critical appraisals were also excluded.
Quality assessment and Bias
The quality of the studies was critically evaluated using Joanna Briggs Institute Critical Appraisal Checklist for Systematic Reviews [39]. The bias was independently assessed by three reviewers. The study was considered to be having low risk of bias with affirmative responses of more than 70%, moderate with 50%-69%, and high with 49% or fewer affirmative responses. Studies demonstrating a high risk of bias were excluded from the study.
Statistical analysis
Statistical Package for Social Sciences (SPSS) version 29 was used for the analysis of data. The incidence and prevalence of GDM were reported as simple percentages in the pooled sample. The pooled relative risk was calculated from the pooled sample from studies with control groups and meta-analysis was done with relative risk (RRs), confidence intervals (CIs), and heterogeneity (I2) being calculated.
3. Results
3.1. Study Characteristics
After a thorough search, a total of 1896 results were retrieved. All the abstracts and study titles were screened and duplicates were removed. There were 1868 studies excluded as they either did not fit the inclusion criteria (1, 2, 3), results were duplicates, animal studies, other language studies, only abstracts were available, PCOS and/or GDM were diagnosed with other criteria, or were self-reported. Finally, after the quality assessment, 22 articles were included in the analysis for the prevalence of GDM in PCOS (prospective) and 6 articles for coexisting PCOS in GDM (retrospective).
The 28 eligible studies consisted of six prospective cohort studies, 15 retrospective cohort studies, five case-control studies, and two cross-sectional studies. It included studies from the Netherlands (3), China (8), Canada (2), Iran (3), one each from India (1), Italy, Korea, Sweden, Saudi Arabia, Mexico, Japan, Taiwan, Finland, United Kingdom, and United States of America [Supplementary Table S1]. One of the studies involved women from three countries Norway, Sweden, and Iceland. This screening process for inclusion and eligibility was carried out by three independent reviewers, any disagreements were discussed, and the final study inclusions were agreed upon. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) show the final study inclusions (Figure 1).
The characteristics of the included studies are described in Supplementary material-1. 22 studies were meeting the inclusion criteria for the incidence of GDM in women with PCOS. One study was conducted in two phases and on separate samples. In a total population of 1,280, 245 women, the crude incidence was found to be 10.55% (2.9- 54.9%) [Table 2].
After the calculation of the incidence of GDM by percentages from pooled data, the studies were further excluded if they did not have a control arm or showed a moderate risk of bias. Fifteen studies with a low risk of bias were assessed by meta-analysis to explore the risk of GDM among pregnant women with PCOS, incorporating a population of 1,257,526. These studies predominantly included cohort studies. The majority of the studies reported that the risk of GDM is higher in women with PCOS than in those without PCOS (HR: 1.59, 95% CI: 1.27–1.91, p < 0.001). A forest plot of a random-effects model was created to calculate the overall HR (I² = 84%, p < 0.001) [Figure 2].
A funnel plot was generated to assess potential publication bias in the studies examining the risk of GDM among pregnant women with PCOS. The plot included 15 studies, incorporating a total population of 1,257,526. In this analysis, the funnel plot revealed slight asymmetry, suggesting a possible presence of publication bias [Figure 3].
3.2. Prevalence of PCOS in GDM (Retrospective Studies)
There were six retrospective studies in this review that explored the prevalence of pre-pregnancy PCOS in women diagnosed with GDM. The pooled data shows a prevalence of 2.47% (1.5- 50.1%) of PCOS in women diagnosed with GDM through this review [Table 3].
3.3. Other Risk Factors in PCOS Contributing to the Development of GDM
There were a few studies that reported a combination of risk factors that are present in patients with PCOS and can lead to GDM in pregnancy with or without the presence of PCOS. These factors can be considered as confounders when we assess the risk of GDM in PCOS [Figure 4].
Most of these studies either did not provide direct evidence through analysis, used different diagnostic criteria for diagnosis, or the conditions were self-reported. Through this review, among the risk factors identified were high BMI, preexisting Insulin resistance (IR), advanced maternal age, use of assisted reproductive techniques (ART), multifetal gestation, South Asian and Chinese ethnicity, and a family history of diabetes in first-degree relatives [Table 4]. However, an independent analysis of individual risk factors through multivariate analysis could not be done due to inadequate information on actual sample sizes and the nature of this review.
4. Discussion
Among the risk factors identified were high BMI, preexisting IR, advanced maternal age, use of ART, multifetal gestation, South Asian and Chinese ethnicity, and a family history of diabetes in first-degree relatives. In a previous meta-analysis, of 33 studies with a total sample of 2697, 954 were diagnosed as GDM. The estimated odds ratio of being diagnosed with GDM was 3.46 (95% CI: 2.80–427). However, here the effect of the presence of PCOS in either group was not explicitly analyzed [95]. In a recent meta-analysis of 33 studies exploring pregnancy and neonatal complications in women with PCOS conceived through ART, the OR of GDM was 1.51 (95% CI:1.17-1.94). The study however did not include women with PCOS conceived naturally or other confounders [96]. Another meta-analysis including the population-based registry from Massachusetts, reported a 51% greater risk of GDM (CI: 1.38–1.65) in patients with PCOS. However, PCOS was identified by ICD codes and included subjects from a single site [97].
4.1. Risk of GDM in PCOS
Pregnancy is a diabetogenic state. The physiological changes in pregnancy to ensure an adequate supply of glucose for the fetus predispose women to develop GDM [94]. IR is a part of normal physiological change in pregnancy. Having a condition with preexisting IR increases the risk of GDM further [72,73]. Conversely, another study in Saudi Arabia showed no significant differences in IR between PCOS and GDM [60]. Several features present in PCOS patients confer a higher risk of GDM in affected women, namely co-existent obesity, IR, hyperandrogenism, and excessive gestational weight gain [61,99,100,101]. As women with PCOS suffer from subfertility and are more likely to need assisted reproduction to conceive, they have a higher prevalence of multifetal gestation, which can also lead to GDM [102].
There were a few studies where either or both PCOS and GDM were self-reported. The findings pointed to pre-pregnancy BMI and hyperandrogenism as predictors of GDM with or without PCOS [63,65]. A larger case-control study (both self-reported), involving 8612 women in Australia revealed a significantly higher risk of GDM in PCOS (11.2% vs 3.8%; p < .001), with similar mean BMI between PCOS and non-PCOS women [84]. Similar results were seen in other self-reported studies where GDM was more prevalent in women with a family history of diabetes [90,103].
4.1.1. Family History of Diabetes, Ethnicity, and Occurrence of GDM
A family history of type-2 diabetes in first-degree relatives is considered a strong risk factor for GDM in pregnancy. In a study among pregnant women in Yemen, the univariate analysis showed family history to be an independent significant predictor of GDM (p<0.001) [90]. However, the PCOS diagnosis was self-reported and GDM was diagnosed by FBG and RBG. Studies also show a significantly higher prevalence of GDM in women with a family history of diabetes and among certain ethnic groups [55,104,105]. A cross-sectional study involving 231,618 women in Canada reported a higher prevalence of GDM in South Asian and Chinese women across all levels of BMI when compared with the general population [91]. The larger proportion of patients were Indian, Pakistani, or Other Asian origin in the PCOS group compared to the non-PCOS group was shown by another study in the United Kingdom [89]. Also, Asian women had the highest pregnancy weight gain with or without PCOS in another study, further increasing the influence of ethnicity on GDM occurrence [72].
4.1.2. PCOS and Insulin Resistance
It has been hypothesized that women with PCOS have basal IR and hence are more susceptible to developing GDM [74]. The fasting insulin levels as well as IR are high in patients with PCOS even in the presence of normal glucose levels [75,76]. In another study involving 83 women with PCOS [53 lean with BMI= 21.5 ± 1.8 kg/m2; 30 obese BMI= 29.6 ± 3.7 kg/m2] and in 15 healthy women (BMI 21.6 ± 1.8 kg/m2), it has been shown that basal blood glucose and fasting insulin levels were significantly higher in PCOS (both lean and obese) as compared to the control group (p <.02; 0.000001). However, IR was only higher in obese PCOS (not in lean) compared to controls [77]. It has also been reported that IR is present in PCOS even with normal BMI [78]. When compared to diet alone, women with GDM treated with additional insulin sensitizers could achieve better glycemic control, and metformin has been used in PCOS patients to prevent GDM. This also points out the possible role of IR [79,80,83]. Despite these findings, IR in PCOS women cannot be completely explained by abdominal adiposity and is influenced by other factors associated with PCOS like abnormal insulin signaling, adipokine secretion, endothelial dysfunction, as well as defective lipid and steroid metabolism [81,82].
4.1.3. GDM and Obesity
There has been considerable debate about whether GDM risk is related to associated factors like obesity in patients with PCOS. Women diagnosed with PCOS are likely to be overweight or obese in 60% of cases [9]. It is also suggested that for every one-unit increment in BMI, the risk of PCOS increases by nearly 10% and that increased BMI is significantly associated with GDM but not PCOS [60]. A multicenter case–control study involving 1,146 women with singleton pregnancies reported increased odds of GDM by 7% with each unit increase in pre-pregnancy BMI and PCOS not being a significant contributor to the diagnosis of GDM [61].
In a study involving 336 IVF cycles in women with PCOS, the participants were divided into obese PCOS, non-obese PCOS, obese non-PCOS, and non-obese non-PCOS. It has been shown that GDM was significantly higher in the obese group (with or without PCOS) compared to women with or without PCOS having normal BMI [41]. Similar findings were reported in a previous study where GDM was significantly higher in women with higher pre-pregnancy BMI, but not increased in PCOS [46,67]. Furthermore, a secondary analysis of longitudinal studies looking at risk factors for GDM like maternal age, ethnicity, BMI, smoking, and education reported that BMI trajectory was independently associated with GDM (OR 2.5) and stronger than PCOS (OR 1.89). However, the limitations included self-reported PCOS and BMI [66]. Previous meta-analyses report that women with PCOS are at significantly higher risk for GDM compared to those without PCOS. When patients are age- and BMI-matched, the risk is significantly higher in normal and overweight women with PCOS [68,69]. In contrast, the risk of GDM in obese women (BMI > 30 kg/m2) with and without PCOS was similar in another study [70]. In countries with universal screening, the same protocol is used for women with and without PCOS. However, where risk-based screening is practiced, such as the National Institute for Health and Clinical Excellence guidelines in the UK, PCOS status is important to recognize alongside ethnicity, positive family history, and BMI [72,73]. A larger meta-analysis and meta-regression involving 63 studies also pointed out that increased maternal pregnancy complications including GDM in PCOS are independent of obesity. The odds of having GDM in PCOS patients was 2.89. The odds for GDM were greater for ovulatory, anovulatory, and hyperandrogenic phenotypes for PCOS. However, the included studies did not follow consistent parameters for GDM diagnosis [72,73]. When patients were matched for age and BMI with controls, there were no differences in the incidence of GDM in patients with or without PCOS [71].
Conversely, a 2-phage cohort study involving more than 18000 pregnant women showed an overall higher prevalence of GDM in women with PCOS. The risk was significantly higher in normal-weight subjects with PCOS than non-PCOS women (26.5% vs. 16.2%, p=0.02). However, in the overweight/ obese group, no difference in risk of GDM was observed between PCOS and non-PCOS subjects (p=0.7). The second phase independent cohort confirmed the risk for GDM associated with PCOS in normal-weight women (p<0.0001) [51]. 21% of women were found to have PCOS in another study of 1545 women with GDM. The researchers reported that these women were younger, had higher BMIs, and had an increased risk of additional pregnancy complications like preeclampsia [106]. It has been seen in other studies that IR was increased in women with PCOS and previous GDM compared with controls, but low-grade inflammation assessed by serum tumor necrosis factor-alpha, highly sensitive C-reactive protein concentrations, white blood cell, and neutrophil count were increased only in women with PCOS compared with BMI-matched controls. Thus, indicating that chronic low-grade inflammation is unlikely to be responsible for the occurrence of GDM in patients with PCOS [107].
4.1.4. GDM and Gestational Weight Gain
Weight gain in pregnancy, especially in the first 20 weeks is a significant contributor to abnormal OGTT in the next 10 weeks and the need for insulin therapy [108]. The lean or overweight PCOS women gain more weight during pregnancy compared with women without PCOS, having the same BMI [84,85,86]. This weight gain mainly occurs in the second and third trimesters in over-weight women with PCOS, compared with women without PCOS [83] and this gain in the later half is significantly associated with pregnancy complications including GDM [87,88]. However, this trend is not observed in obese women with PCOS [85]. Women after childbirth are more likely to retain the GWG and be overweight or obese in subsequent pregnancies and develop GDM [109,110]. Hence, isolated pregnancy weight gain is not conclusive of GDM occurrence in the context of PCOS, and should be analyzed in view of pre-pregnancy BMI [51,111].
4.1.5. GDM and ART
It has been reported that ART can increase the risk of developing GDM. As women with PCOS are more likely to need ART for conception, this can be an important factor. In a previous study exploring GDM in 60 women with PCOS conceived after ovulation induction, it was concluded that the risk of GDM is not higher in PCOS women compared to the age and BMI-matched non-PCOS controls [90]. However, there were variable diagnoses of PCOS in this study. When the risk of GDM is compared between different ART procedures, it was reported that GDM is significantly more common in in-vitro fertilization/intracytoplasmic sperm injection and intrauterine insemination groups compared to spontaneous conception group despite all the three groups being similar in age, pre-pregnancy BMI and weight gain in pregnancy. However, this study excluded women with PCOS [93].
Women with PCOS are more likely to receive ART, conceive at higher maternal age and the chances of multifetal gestation is higher in PCOS and ART. In a recent study involving large samples of 13,732 ART mothers and 386, 660 non-ART mothers, it has been reported that at advanced maternal age (≥ 40 years) the prevalence of GDM was higher in the ART group compared to non-ART [94]. Having a twin pregnancy also increased the risk of GDM significantly compared to singleton pregnancies. However, there was no significant difference in the likelihood of GDM among mothers who had twins between ART and non-ART groups. In the younger age group (age< 40 years), there were higher odds of GDM for ART singleton mothers, compared with non-ART singleton mothers. The BMI, smoking status, PCOS, and type of ART procedure were not reported for most of the subjects in this study [94].
4.2. Prevalence of PCOS in GDM
A few of the retrospective studies reported the prevalence of PCOS among women diagnosed with GDM [60,62,63]. A retrospective cohort study included 34 686 women with GDM and identified that 1.5% of women with GDM had PCOS compared to 1.2% of women who did not have GDM [62]. It points out to the possibility of additional risk of developing diabetes in women who developed GDM in pregnancy. Factors in women with PCOS likely contribute to the development of metabolic diseases like diabetes and hypertension outside pregnancy, do increase the risk of GDM during pregnancy.
4.3. Predictors of GDM in PCOS Patients
In a recent study, the authors used a nomogram model to predict the occurrence of GDM in 434 pregnant women with PCOS. 23.9 % of women developed GDM (n=104) and the significant predictors of GDM were first-trimester Hemoglobin A1c, advanced maternal age (≥35 years), total cholesterol levels, low-density lipoprotein cholesterol levels, systolic blood pressure, family history, BMI, and testosterone were predictive factors of GDM (P<0.05) [55]. Earlier studies reported the level of serum SHBG concentrations before conception as the most significant predictor for GDM in women with PCOS [40,50]. Factors in PCOS that were significantly independent predictive of GDM were age ≥30 years, BMI≥24 kg/m2, increased IR (≥22.69), increased fasting insulin (≥22.71mIU/L), testosterone (≥2.85 nmol/L), androstenedione (≥6.63 nmol/L) and SHBG (<64.22 nmol/L) but positive family history of DM was not a significant predictor of GDM in women with PCOS by another recent systematic review [53]. While some factors are pre-pregnancy BMI, and smoking are modifiable, other risk factors like ethnicity and family history of DM are non-modifiable [112].
Strengths and limitations- The scope of this study is limited by the absence of any randomized control trials due to the nature of the condition. Also, this lack of consistency and comprehensiveness of risk factors in the studies posed a challenge when attempting to perform a meta-analysis within the scope of this review. This review was not registered with the PROSPERO trial registry. However, the inclusion of studies with set criteria for diagnosis of PCOS and GDM addresses the lacunae of inconsistent diagnosis in other reviews. Including studies with low risk of bias, and risk factor analysis were the strengths of this review. In addition, the proposal with methodology, and search strategy was reviewed by the institutional research board and was approved before the commencement of the research.
5. Conclusions
The prevalence of GDM in patients with PCOS is high, but the causality is complex. Although distinct entities in themselves, both GDM and PCOS are interrelated. The association between them is likely due to similar etiopathogenetic pathways through metabolic syndrome, ethnicity, IR, hormonal changes, subfertility, advanced age at conception, fertility treatments, and resultant multifetal gestation. The newer predictive models are promising in clarifying the causative relationships, yet use various parameters at different cut-offs. Conditions like advanced maternal age at pregnancy, use of assisted reproduction, obesity, and PCOS are on the rise worldwide. Hence, there is a need for the development of universally acceptable parameters for the early prediction of GDM in women with PCOS and prospective, blinded cohort studies for the exclusion of confounding variables.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. S1- Details of included studies.
Author Contributions
Rajani Dube (RD), Taniqsha Bambani (TB), Sahina Saif (SS), Noha Hashmi (NH), Mohammed Anas Mohammed Faruk Patni (MA) and Noopur R. Kedia (NK) contributed to the research in the following roles-Conception and design of the study: TB, SS, NH, NK, RD. Proposal writing: TB, NK. Acquisition of data: TB, SS, NH, RD. Analysis and/or interpretation of data: RD, MA, NK. Drafting the manuscript: RD, TB, SS, NH, MA. Revising the manuscript critically for important intellectual content: RD, MA. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ehrmann, D.A. Polycystic ovary syndrome. N Engl J Med. 2005, 352, 1223–1236. [Google Scholar] [CrossRef] [PubMed]
- Sirmans, S.M.; Pate, K.A. Epidemiology, diagnosis, and management of polycystic ovary syndrome. Clin Epidemiol 2013, 6, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.; Deeks, A.; Moran, L. Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010, 8, 41–41. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R.; Carmina, E.; Chen, Z.; Dunaif, A.; Laven, J.S.; Legro, R.S.; Lizneva, D.; Natterson-Horowtiz, B.; Teede, H.J.; Yildiz, B.O. Polycystic ovary syndrome. Nat Rev Dis Primers 2016, 2, 16057. [Google Scholar] [CrossRef] [PubMed]
- Asghari, K.M.; Nejadghaderi, S.A.; Alizadeh, M.; Sanaie, S.; Sullman, M.J.M.; Kolahi, A.-A.; Avery, J.; Safiri, S. Burden of polycystic ovary syndrome in the Middle East and North Africa region, 1990–2019. Sci. Rep. 2022, 12, 1–11. [Google Scholar] [CrossRef]
- United Nations Children’s Fund (UNICEF). Progress for children: a report card on adolescents; UNICEF: NewYork, 2012. [Google Scholar]
- Hahn, S.; E Janssen, O.; Tan, S.; Pleger, K.; Mann, K.; Schedlowski, M.; Kimmig, R.; Benson, S.; Balamitsa, E.; Elsenbruch, S. Clinical and psychological correlates of quality-of-life in polycystic ovary syndrome. Eur. J. Endocrinol. 2005, 153, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Strowitzki, T. Advanced diagnosis of polycystic ovary syndrome—new prediction models with standard parameters. Fertil. Steril. 2021, 115, 92–93. [Google Scholar] [CrossRef]
- The Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop group Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [CrossRef] [PubMed]
- Koric, A.; Singh, B.; VanDerslice, J.A.; Stanford, J.B.; Rogers, C.R.; Egan, D.T.; Agyemang, D.O.; Schliep, K. Polycystic ovary syndrome and postpartum depression symptoms: a population-based cohort study. Am. J. Obstet. Gynecol. 2021, 224, 591–e1. [Google Scholar] [CrossRef]
- D’alterio, M.N.; Sigilli, M.; Succu, A.G.; Ghisu, V.; Laganà, A.S.; Sorrentino, F.; Nappi, L.; Tinelli, R.; Angioni, S. Pregnancy outcomes in women with polycystic ovarian syndrome. Minerva Obstet. Gynecol. 2022, 74, 45–59. [Google Scholar] [CrossRef]
- Eroglu, D.; Zeyneloglu, H.B. Metabolic disorders in patients with recent gestational diabetes mellitus. J. Obstet. Gynaecol. Res. 2006, 32, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Hauth, J.C.; Gilstrap, L.C.I.I.I.; Wenstrom, K.D. Diabetes. In: Cunningham FG, editors. Williams Obstetrics. New York: McGraw-Hill; 2005;1172–1173.
- Zhu, Y.; Zhang, C. Prevalence of Gestational Diabetes and Risk of Progression to Type 2 Diabetes: a Global Perspective. Curr. Diabetes Rep. 2016, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Saravanan, P.; A Magee, L.; Banerjee, A.; Coleman, M.A.; Von Dadelszen, P.; Denison, F.; Farmer, A.; Finer, S.; Fox-Rushby, J.; Holt, R.; et al. Gestational diabetes: opportunities for improving maternal and child health. Lancet Diabetes Endocrinol. 2020, 8, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Rajab, K.E.; Issa, A.A.; Hasan, Z.A.; Rajab, E.; Jaradat, A.A. Incidence of gestational diabetes mellitus in Bahrain from 2002 to 2010. Int. J. Gynecol. Obstet. 2012, 117, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, M.M.; Dhatt, G.S.; Punnose, J.; Koster, G. Gestational diabetes: dilemma caused by multiple international diagnostic criteria. Diabet. Med. 2005, 22, 1731–1736. [Google Scholar] [CrossRef] [PubMed]
- Leng, J.; Shao, P.; Zhang, C.; Tian, H.; Zhang, F.; Zhang, S.; Dong, L.; Li, L.; Yu, Z.; Chan, J.C.N.; et al. Prevalence of Gestational Diabetes Mellitus and Its Risk Factors in Chinese Pregnant Women: A Prospective Population-Based Study in Tianjin, China. PLOS ONE 2015, 10, e0121029–e0121029. [Google Scholar] [PubMed]
- Eades, C.E.; Cameron, D.M.; Evans, J.M. Prevalence of gestational diabetes mellitus in Europe: A meta-analysis. Diabetes Res. Clin. Pr. 2017, 129, 173–181. [Google Scholar] [CrossRef]
- Bashir, M.M.; Ahmed, L.A.; Elbarazi, I.; Loney, T.; Al-Rifai, R.H.; Alkaabi, J.M.; Al-Maskari, F. Incidence of gestational diabetes mellitus in the United Arab Emirates; comparison of six diagnostic criteria: The Mutaba’ah Study. Front. Endocrinol. 2022, 13, 1069477. [Google Scholar] [CrossRef]
- Agarwal, M.M.; Dhatt, G.S.; Othman, Y. Gestational diabetes in a tertiary care hospital: implications of applying the IADPSG criteria. Arch. Gynecol. Obstet. 2012, 286, 373–378. [Google Scholar] [CrossRef]
- Hashim, M.; Radwan, H.; Hasan, H.; Obaid, R.S.; Al Ghazal, H.; Al Hilali, M.; Rayess, R.; Chehayber, N.; Mohamed, H.J.J.; Naja, F. Gestational weight gain and gestational diabetes among Emirati and Arab women in the United Arab Emirates: results from the MISC cohort. BMC Pregnancy Childbirth 2019, 19, 1–11. [Google Scholar] [CrossRef]
- Feig, D.S.; Berger, H.; Donovan, L.; Godbout, A.; Kader, T.; et al. Diabetes Canada Clinical Practice Guidelines Expert Committee Diabetes Pregnancy Can, J. Diabetes. 2018;42(Suppl. S1):S255–82.
- Vitacolonna, E.; Succurro, E.; Lapolla, A.; Scavini, M.; Bonomo, M.; Di Cianni, G.; Di Benedetto, A.; Napoli, A.; Tumminia, A.; Festa, C.; et al. Guidelines for the screening and diagnosis of gestational diabetes in Italy from 2010 to 2019: critical issues and the potential for improvement. Acta Diabetol. 2019, 56, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- HAPO Study Cooperative Research Group; Metzger, B. E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCance, D.R.; Hod, M.; et al. Hyperglycemia and Adverse Pregnancy Outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef]
- Behboudi-Gandevani, S.; Amiri, M.; Bidhendi Yarandi, R.; Ramezani Tehrani, F. The impact of diagnostic criteria for gestational diabetes on its prevalence: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Rani, P.R. Screening and Diagnosis of Gestational Diabetes Mellitus, Where Do We Stand. J. Clin. Diagn. Res. 2016, 10, QE01–4. [Google Scholar] [CrossRef] [PubMed]
- Cortel, M.R.B.P.; Manalo, M.E.M.; Canivel, R.R.C.; Matias, R.S.; Dizon, A.J.B.; Bacani, M.N.S.; Dalmacio, J.S.B. Screening and Diagnosis of Gestational Diabetes Mellitus Using 75-g Oral Glucose Tolerance Test Following the WHO, ADA, and IADPSG Criteria. J. Diabetes Metab. 2018, 09, 1–4. [Google Scholar] [CrossRef]
- Yang, H.; Wei, Y.; Gao, X.; Xu, X.; Fan, L.; He, J.; Hu, Y.; Liu, X.; Chen, X.; Yang, Z.; et al. Risk factors for gestational diabetes mellitus in Chinese women—a prospective study of 16 286 pregnant women in China. Diabet. Med. 2009, 26, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, U.J.; Latif, L. RISK FACTORS ASSOCIATED WITH GESTATIONAL DIABETES MELLITUS IN FEMALES PRESENTED AT A TERTIARY CARE HOSPITAL OF LAHORE. Biomedica 2015, 31, 315–317. [Google Scholar]
- Brennan, L.; Teede, H.; Skouteris, H.; Linardon, J.; Hill, B.; Moran, L. Lifestyle and Behavioral Management of Polycystic Ovary Syndrome. J. Women's Heal. 2017, 26, 836–848. [Google Scholar] [CrossRef]
- Boomsma, C.; Eijkemans, M.; Hughes, E.; Visser, G.; Fauser, B.; Macklon, N. A meta-analysis of pregnancy outcomes in women with polycystic ovary syndrome. Hum. Reprod. Updat. 2006, 12, 673–683. [Google Scholar] [CrossRef]
- Kjerulff, L.E.; Sanchez-Ramos, L.; Duffy, D. Pregnancy outcomes in women with polycystic ovary syndrome: a meta-analysis. Am J Obstet Gynecol. 2011;204:558.e551-556.
- Qin, J.Z.; Pang, L.H.; Li, M.J.; Fan, X.J.; Huang, R.D.; Chen, H.Y. Obstetric complications in women with polycystic ovary syndrome: a systematic review and meta-analysis. Reprod. Biol. Endocrinol. 2013, 11, 1–56. [Google Scholar] [CrossRef]
- Yu, H.F.; Chen, H.S.; Rao, D.P.; Gong, J. Association between polycystic ovary syndrome and the risk of pregnancy complications: a PRISMA-compliant systematic review and meta-analysis. Medicine. 2016;95:e4863.
- NICE guideline [NG3]. Diabetes in pregnancy: management from preconception to the postnatal period. Available online: https://www.nice.org.uk (accessed on 11 January 2024).
- de Wilde, M.A.; Veltman-Verhulst, S.M.; Goverde, A.J.; Lambalk, C.B.; Laven, J.S.E.; Franx, A.; Koster, M.P.H.; Eijkemans, M.J.C.; Fauser, B.C.J.M. Preconception predictors of gestational diabetes: a multicentre prospective cohort study on the predominant complication of pregnancy in polycystic ovary syndrome. Hum. Reprod. 2014, 29, 1327–1336. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, R.; Rasul, R.A. The Prevalence of Prenatal Diabetes Mellitus in Rania City: Women with Polycystic Ovaries. kufa J. Nurs. Sci. 2023, 13. [Google Scholar] [CrossRef]
- The Joanna Briggs Institute Checklist for Randomized Controlled Trials. Available online: http://joannabriggs.org/research/critical-appraisal-tools.html (accessed on 3 January 2022).
- Altieri, P.; Gambineri, A.; Prontera, O.; Cionci, G.; Franchina, M.; Pasquali, R. Maternal polycystic ovary syndrome may be associated with adverse pregnancy outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 149, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Veltman-Verhulst, S.M.; Van Haeften, T.W.; Eijkemans, M.J.C.; De Valk, H.W.; Fauser, B.C.J.M.; Goverde, A.J. Sex hormone-binding globulin concentrations before conception as a predictor for gestational diabetes in women with polycystic ovary syndrome. Hum. Reprod. 2010, 25, 3123–3128. [Google Scholar] [CrossRef] [PubMed]
- Han, A.R.; Kim, H.O.; Cha, S.W.; Park, C.W.; Kim, J.Y.; Yang, K.M.; Song, I.O.; Koong, M.K.; Kang, I.S. Adverse pregnancy outcomes with assisted reproductive technology in non-obese women with polycystic ovary syndrome: a case-control study. Clin. Exp. Reprod. Med. 2011, 38, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Roos, N.; Kieler, H.; Sahlin, L.; Ekman-Ordeberg, G.; Falconer, H.; Stephansson, O. Risk of adverse pregnancy outcomes in women with polycystic ovary syndrome: population based cohort study. BMJ 2011, 343, d6309–d6309. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Muñoz, E.; Castellanos-Barroso, G.; Ramírez-Eugenio, B.Y.; Ortega-González, C.; Parra, A.; Castillo-Mora, A.; De la Jara-Díaz, J.F. The risk of gestational diabetes mellitus among Mexican women with a history of infertility and polycystic ovary syndrome. Fertil. Steril. 2012, 97, 1467–1471. [Google Scholar] [CrossRef] [PubMed]
- Ashrafi, M.; Sheikhan, F.; Arabipoor, A.; Hosseini, R.; Nourbakhsh, F.; Zolfaghari, Z. Gestational diabetes mellitus risk factors in women with polycystic ovary syndrome (PCOS). Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 181, 195–199. [Google Scholar] [CrossRef] [PubMed]
- de Wilde, M.A.; Goverde, A.J.; Veltman-Verhulst, S.M.; Eijkemans, M.J.C.; Franx, A.; Fauser, B.C.J.M.; Koster, M.P.H. Insulin action in women with polycystic ovary syndrome and its relation to gestational diabetes. Hum. Reprod. 2015, 30, 1447–1453. [Google Scholar] [CrossRef]
- Sawada, M.; Masuyama, H.; Hayata, K.; Kamada, Y.; Nakamura, K.; Hiramatsu, Y. Pregnancy complications and glucose intolerance in women with polycystic ovary syndrome. Endocr. J. 2015, 62, 1017–1023. [Google Scholar] [CrossRef]
- Jin, J.; Lu, Z.; Li, Y.; Cowart, L.A.; Lopes-Virella, M.F.; Huang, Y. Docosahexaenoic acid antagonizes the boosting effect of palmitic acid on LPS inflammatory signaling by inhibiting gene transcription and ceramide synthesis. PLoS One. 2018, 13: e0193343.
- Xiao, Q.; Cui, Y.-Y.; Lu, J.; Zhang, G.-Z.; Zeng, F.-L. Risk for Gestational Diabetes Mellitus and Adverse Birth Outcomes in Chinese Women with Polycystic Ovary Syndrome. Int. J. Endocrinol. 2016, 2016, 1–6. [Google Scholar] [CrossRef]
- Xia, H.; Zhang, R.; Sun, X.; Wang, L.; Zhang, W. Valuable predictors of gestational diabetes mellitus in infertile Chinese women with polycystic ovary syndrome: a prospective cohort study. Gynecol. Endocrinol. 2017, 33, 448–451. [Google Scholar] [CrossRef]
- Zheng, W.; Huang, W.; Zhang, L.; Tian, Z.; Yan, Q.; Wang, T.; Zhang, L.; Li, G. Early pregnancy metabolic factors associated with gestational diabetes mellitus in normal-weight women with polycystic ovary syndrome: a two-phase cohort study. Diabetol. Metab. Syndr. 2019, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fougner, S.L.; Vanky, E.; Løvvik, T.S.; Carlsen, S.M. No impact of gestational diabetes mellitus on pregnancy complications in women with PCOS, regardless of GDM criteria used. PLOS ONE 2021, 16, e0254895. [Google Scholar] [PubMed]
- Li, X.; Liu, X.; Zuo, Y.; Gao, J.; Liu, Y.; Zheng, W. The risk factors of gestational diabetes mellitus in patients with polycystic ovary syndrome. Medicine 2021, 100, e26521. [Google Scholar] [CrossRef] [PubMed]
- Pattnaik, L.; A Naaz, S.; Das, B.; Dash, P.; Pattanaik, M. Adverse Pregnancy Outcome in Polycystic Ovarian Syndrome: A Comparative Study. Cureus 2022, 14, e25790. [Google Scholar] [CrossRef]
- Ouyang, P.; Duan, S.; You, Y.; Jia, X.; Yang, L. Risk prediction of gestational diabetes mellitus in women with polycystic ovary syndrome based on a nomogram model. BMC Pregnancy Childbirth 2023, 23, 1–8. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, X.; Zhao, H.; Ding, H.; Tan, J.; Chen, J.; Zhang, R.; Azziz, R.; Yang, D. Risks for Gestational Diabetes Mellitus and Pregnancy-Induced Hypertension Are Increased in Polycystic Ovary Syndrome. BioMed Res. Int. 2013, 2013, 1–6. [Google Scholar] [CrossRef]
- Sterling, L.; Liu, J.; Okun, N.; Sakhuja, A.; Sierra, S.; Greenblatt, E. Pregnancy outcomes in women with polycystic ovary syndrome undergoing in vitro fertilization. Fertil. Steril. 2016, 105, 791–797. [Google Scholar] [CrossRef]
- Liu, S.; Mo, M.; Xiao, S.; Li, L.; Hu, X.; Hong, L.; Wang, L.; Lian, R.; Huang, C.; Zeng, Y.; et al. Pregnancy Outcomes of Women With Polycystic Ovary Syndrome for the FirstIn VitroFertilization Treatment: A Retrospective Cohort Study With 7678 Patients. Front. Endocrinol. 2020, 11. [Google Scholar] [CrossRef]
- Qiu, M.; Qu, J.; Tian, Y.; Wang, Y. The influence of polycystic ovarian syndrome on obstetric and neonatal outcomes after frozen-thawed embryo transfer. Reprod. Biomed. Online 2022, 45, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, T.; Albogami, A.; Allhuaidan, A.; Alfawaz, S.; Murad, S.; Kofi, M. Prevalence of Gestational Diabetes Mellitus and Associated Risk Factors Among Pregnant Women Attending Antenatal Care in Primary Health Care Centers in Riyadh, Saudi Arabia. Fam. Med. Prim. Care: Open Access 2021, 5. [Google Scholar] [CrossRef]
- Mustaniemi, S.; Vääräsmäki, M.; Eriksson, J.G.; Gissler, M.; Laivuori, H.; Ijäs, H.; Bloigu, A.; Kajantie, E.; Morin-Papunen, L. Polycystic ovary syndrome and risk factors for gestational diabetes. Endocr. Connect. 2018, 7, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Bond, R.; Pace, R.; Rahme, E.; Dasgupta, K. Diabetes risk in women with gestational diabetes mellitus and a history of polycystic ovary syndrome: a retrospective cohort study. Diabet. Med. 2017, 34, 1684–1695. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, A.; Hanley, A.; Ni, A.; Tomlinson, G.; Feig, D.S. Does the presence of polycystic ovary syndrome increase the risk of obstetrical complications in women with gestational diabetes? J. Matern. Neonatal Med. 2010, 23, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Foroozanfard, F.; Moosavi, S.G.A.; Mansouri, F.; Bazarganipour, F. Obstetric and Neonatal Outcome in PCOS with Gestational Diabetes Mellitus. 2014, 8, 7–12.
- Kashanian, M.; Fazy, Z.; Pirak, A. Evaluation of the relationship between gestational diabetes and a history of polycystic ovarian syndrome. Diabetes Res. Clin. Pr. 2008, 80, 289–292. [Google Scholar] [CrossRef]
- Kakoly, N.S.; Earnest, A.; Moran, L.J.; Teede, H.J.; Joham, A.E. Group-based developmental BMI trajectories, polycystic ovary syndrome, and gestational diabetes: a community-based longitudinal study. BMC Med. 2017, 15, 1–9. [Google Scholar] [CrossRef]
- Turhan, N.; Seçkin, N.; Aybar, F.; Inegöl, I. Assessment of glucose tolerance and pregnancy outcome of polycystic ovary patients. Int. J. Gynecol. Obstet. 2003, 81, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, A. Increasing prevalence of gestational diabetes mellitus: a public health perspective. Diabetes Care. 2007;30 Suppl 2:S141–S6.
- Callesen, N.F.; Ringholm, L.; Stage, E.; Damm, P.; Mathiesen, E.R. Insulin requirements in type 1 diabetic pregnancy: do twin pregnant women require twice as much insulin as singleton pregnant women? Diabetes Care. 2012;35:1246–8.
- Elkholi, D.G.E.Y.; Nagy, H.M. The effects of adipocytokines on the endocrino-metabolic features and obstetric outcome in pregnant obese women with polycystic ovary syndrome. Middle East Fertil. Soc. J. 2014, 19, 293–302. [Google Scholar] [CrossRef]
- Haakova, L.; Cibula, D.; Rezabek, K.; Hill, M.; Fanta, M.; Zivny, J. Pregnancy outcome in women with PCOS and in controls matched by age and weight. Hum. Reprod. 2003, 18, 1438–1441. [Google Scholar] [CrossRef]
- Bahri Khomami M, JohamAE, Boyle JA, et al. The role of maternal obesity in infant outcomes in polycystic ovary syndrome—a systematic review, meta-analysis, and meta-regression. Obes Rev 2019, 20, 842–858. [CrossRef] [PubMed]
- Khomami, M.B.; Boyle, J.A.; Tay, C.T.; Vanky, E.; Teede, H.J.; Joham, A.E.; Moran, L.J. Polycystic ovary syndrome and adverse pregnancy outcomes: Current state of knowledge, challenges and potential implications for practice. Clin. Endocrinol. 2018, 88, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Yao, K.; Bian, C.; Zhao, X. Association of polycystic ovary syndrome with metabolic syndrome and gestational diabetes: Aggravated complication of pregnancy. Exp. Ther. Med. 2017, 14, 1271–1276. [Google Scholar] [CrossRef]
- Esmaeilzadeh, S.; Tahmasbpour, E.; Gholinezhad-Chari, M. Hyperhomocysteinemia, insulin resistance and body mass index in Iranian young women with polycystic ovary syndrome. Middle East Fertil. Soc. J. 2017, 22, 149–155. [Google Scholar] [CrossRef]
- Stepto, N.K.; Cassar, S.; Joham, A.E.; Hutchison, S.K.; Harrison, C.L.; Goldstein, R.F.; Teede, H.J. Women with polycystic ovary syndrome have intrinsic insulin resistance on euglycaemic-hyperinsulaemic clamp. Hum. Reprod. 2013, 28, 777–784. [Google Scholar] [CrossRef]
- VrbÍková, J.; Cibula, D.; Dvor̆áková, K.; Stanická, S.; Šindelka, G.; Hill, M.; Fanta, M.; Vondra, K.; Škrha, J. Insulin Sensitivity in Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2004, 89, 2942–2945. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin Resistance and the Polycystic Ovary Syndrome Revisited: An Update on Mechanisms and Implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef]
- Afandi, B.; Hassanein, M.M.; Majd, L.M.; Nagelkerke, N.J.D. Impact of Ramadan fasting on glucose levels in women with gestational diabetes mellitus treated with diet alone or diet plus metformin: a continuous glucose monitoring study. BMJ Open Diabetes Res. Care 2017, 5, e000470. [Google Scholar] [CrossRef]
- Dube, R. Using Metformin in Pregnancy for Different Indications: Are We Any Wiser now? Applied Clinical Research, Clinical Trials & Regulatory Affairs.2016;3:3-19.
- Dumesic, D.A.; Oberfield, S.E.; Stener-Victorin, E.; Marshall, J.C.; Laven, J.S.; Legro, R.S. Scientific Statement on the Diagnostic Criteria, Epidemiology, Pathophysiology, and Molecular Genetics of Polycystic Ovary Syndrome. Endocr. Rev. 2015, 36, 487–525. [Google Scholar] [CrossRef]
- Dube, R. Does endothelial dysfunction correlate with endocrinal abnormalities in patients with polycystic ovary syndrome? Avicenna J. Med. 2016, 06, 91–102. [Google Scholar] [CrossRef]
- Chowdhury, F.; Dube, R.; Riyaz, R.; Khan, K.; Al-Zuheiri, S.T.S.; Rangraze, I.R. Title-Efficacy of metformin as monotherapy in gestational and pre-gestational diabetic pregnant women. J. Adv. Pharm. Educ. Res. 2024, 14, 84–90. [Google Scholar] [CrossRef]
- Joham, A.E.; Ranasinha, S.; Zoungas, S.; Moran, L.; Teede, H.J. Gestational Diabetes and Type 2 Diabetes in Reproductive-Aged Women With Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2014, 99, E447–E452. [Google Scholar] [CrossRef] [PubMed]
- Kent, J.; Dodson, W.C.; Kunselman, A.; Pauli, J.; Stone, A.; Diamond, M.P.; Coutifaris, C.; Schlaff, W.D.; Alvero, R.; Casson, P.; et al. Gestational Weight Gain in Women With Polycystic Ovary Syndrome: A Controlled Study. J. Clin. Endocrinol. Metab. 2018, 103, 4315–4323. [Google Scholar] [CrossRef] [PubMed]
- Palomba, S.; de Wilde, M.A.; Falbo, A.; Koster, M.P.; La Sala, G.B.; Fauser, B.C. Pregnancy complications in women with polycystic ovary syndrome. Hum. Reprod. Updat. 2015, 21, 575–592. [Google Scholar] [CrossRef]
- Durie, D.E.; Thornburg, L.L.; Glantz, J.C. Effect of Second-Trimester and Third-Trimester Rate of Gestational Weight Gain on Maternal and Neonatal Outcomes. Obstet. Gynecol. 2011, 118, 569–575. [Google Scholar] [CrossRef]
- Siega-Riz, A.M.; Viswanathan, M.; Moos, M.-K.; Deierlein, A.; Mumford, S.; Knaack, J.; Thieda, P.; Lux, L.J.; Lohr, K.N. A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: birthweight, fetal growth, and postpartum weight retention. Am. J. Obstet. Gynecol. 2009, 201, 339–e1. [Google Scholar] [CrossRef]
- Rees, D.A.; Jenkins-Jones, S.; Morgan, C.L. Contemporary Reproductive Outcomes for Patients With Polycystic Ovary Syndrome: A Retrospective Observational Study. J. Clin. Endocrinol. Metab. 2016, 101, 1664–1672. [Google Scholar] [CrossRef]
- Ali, A.D.; Mehrass, A.A.-K.; Al-Adhroey, A.H.; Al-Shammakh, A.; Amran, A. Prevalence and risk factors of gestational diabetes mellitus in Yemen. Int. J. Women's Heal. 2016, 8, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Read, S.; Berger, H.; Feig, D.; Fleming, K.; Ray, J.G.; Shah, B.R.; Lipscombe, L. Influence of Ethnicity on the Association between Body Mass Index and Prevalence of Gestational Diabetes. Diabetes 2020, 69. [Google Scholar] [CrossRef]
- Vollenhoven, B.; Kovacs, S.G.; Burge, H.; Healy, D. Prevalence of gestational diabetes rnellitus in polycystic ovarian syndrome (PCOS) patients pregnant after ovulation induction with gonadotrophins. Aust N Z J Obstet Gynaecol 2000; 40:1:54-8.
- Ashrafi, M.; Gosili, R.; Hosseini, R.; Arabipoor, A.; Ahmadi, J.; Chehrazi, M. Risk of gestational diabetes mellitus in patients undergoing assisted reproductive techniques. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 176, 149–152. [Google Scholar] [CrossRef]
- Wang, Y.A.; Nikravan, R.; Smith, H.C.; Sullivan, E.A. Higher prevalence of gestational diabetes mellitus following assisted reproduction technology treatment. Hum. Reprod. 2013, 28, 2554–2561. [Google Scholar] [CrossRef] [PubMed]
- Moosazadeh, M.; Asemi, Z.; Lankarani, K.B.; Tabrizi, R.; Maharlouei, N.; Naghibzadeh-Tahami, A.; Yousefzadeh, G.; Sadeghi, R.; Khatibi, S.R.; Afshari, M.; et al. Family history of diabetes and the risk of gestational diabetes mellitus in Iran: A systematic review and meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, S99–S104. [Google Scholar] [CrossRef] [PubMed]
- Ban, M.; Sun, Y.; Chen, X.; Zhou, X.; Zhang, Y.; Cui, L. Association between maternal polycystic ovarian syndrome undergoing assisted reproductive technology and pregnancy complications and neonatal outcomes: a systematic review and meta-analysis. J. Ovarian Res. 2024, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Farland, L.V.; E Stern, J.; Liu, C.-L.; Cabral, H.J.; Coddington, C.C.; Diop, H.; Dukhovny, D.; Hwang, S.; A Missmer, S. Polycystic ovary syndrome and risk of adverse pregnancy outcomes: a registry linkage study from Massachusetts. Hum. Reprod. 2022, 37, 2690–2699. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [PubMed]
- Popova, P.V.; Klyushina, A.A.; Vasilyeva, L.B.; Tkachuk, A.S.; Bolotko, Y.A.; Gerasimov, A.S.; Pustozerov, E.A.; Kravchuk, E.N.; Predeus, A.; Kostareva, A.A.; et al. Effect of gene-lifestyle interaction on gestational diabetes risk. Oncotarget 2017, 8, 112024–112035. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Hu, Y.; Zeng, J.; Zheng, L.; Ye, P.; Wei, D.; Chen, D. Analysis of risk factors related to gestational diabetes mellitus. Taiwan. J. Obstet. Gynecol. 2020, 59, 718–722. [Google Scholar] [CrossRef] [PubMed]
- West, S.; Ollila, M.; Franks, S.; Piltonen, T.; Jokelainen, J.; Nevalainen, J.; Puukka, K.; Ruokonen, A.; Järvelin, M.; Auvinen, J.; et al. Overweight, obesity and hyperandrogenemia are associated with gestational diabetes mellitus: A follow-up cohort study. Acta Obstet. et Gynecol. Scand. 2020, 99, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Alkaabi, J.; Almazrouei, R.; Zoubeidi, T.; Alkaabi, F.M.; Alkendi, F.R.; Almiri, A.E.; Sharma, C.; Souid, A.-K.; Ali, N.; Ahmed, L.A. Burden, associated risk factors and adverse outcomes of gestational diabetes mellitus in twin pregnancies in Al Ain, UAE. BMC Pregnancy Childbirth 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Juber, N.F.; Abdulle, A.; AlJunaibi, A.; AlNaeemi, A.; Ahmad, A.; Leinberger-Jabari, A.; Al Dhaheri, A.S.; AlZaabi, E.; Mezhal, F.; Al-Maskari, F.; et al. Maternal Early-Life Risk Factors and Later Gestational Diabetes Mellitus: A Cross-Sectional Analysis of the UAE Healthy Future Study (UAEHFS). Int. J. Environ. Res. Public Heal. 2022, 19, 10339. [Google Scholar] [CrossRef]
- Hedderson, M.M.; Darbinian, J.A.; Ferrara, A. Disparities in the risk of gestational diabetes by race-ethnicity and country of birth. Paediatr. Périnat. Epidemiology 2010, 24, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, A.; Giveon, S.; Rubin, C.; Novikov, I.; Ziv, A.; Kalter-Leibovici, O. Gestational diabetes risk in a multi-ethnic population. Acta Diabetol. 2019, 57, 263–269. [Google Scholar] [CrossRef]
- Manoharan, V.; Wong, V.W. Impact of comorbid polycystic ovarian syndrome and gestational diabetes mellitus on pregnancy outcomes: a retrospective cohort study. BMC Pregnancy Childbirth 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Thomann, R.; Rossinelli, N.; Keller, U.; Tirri, B.F.; De Geyter, C.; Ruiz, J.; Kränzlin, M.; Puder, J.J. Differences in low-grade chronic inflammation and insulin resistance in women with previous gestational diabetes mellitus and women with polycystic ovary syndrome. Gynecol. Endocrinol. 2008, 24, 199–206. [Google Scholar] [CrossRef]
- Barnes RA, Wong T, Ross GP, et al. Excessive weight gain before and during gestational diabetes mellitus management: What is the impact? Diabetes Care 2020, 43, 74–81. [CrossRef]
- Gilmore, L.A.; Klempel-Donchenko, M.; Redman, L.M. Pregnancy as a window to future health: Excessive gestational weight gain and obesity. Semin. Perinatol. 2015, 39, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Oken, E.; Kleinman, K.P.; Belfort, M.B.; Hammitt, J.K.; Gillman, M.W. Associations of Gestational Weight Gain with Short- and Longer-term Maternal and Child Health Outcomes. Am. J. Epidemiology 2009, 170, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Rf, G.; Sk, A.; S, R.; M, M.; Ja, B.; Mh, B.; N, L.; G, H.; F, C.; L, R.; et al. Association of Gestational Weight Gain with Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. Yearb. Paediatr. Endocrinol. 2018. [Google Scholar] [CrossRef]
- Alejandro, E.U.; Mamerto, T.P.; Chung, G.; Villavieja, A.; Gaus, N.L.; Morgan, E.; Pineda-Cortel, M.R.B. Gestational Diabetes Mellitus: A Harbinger of the Vicious Cycle of Diabetes. Int. J. Mol. Sci. 2020, 21, 5003. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow chart for study inclusions.
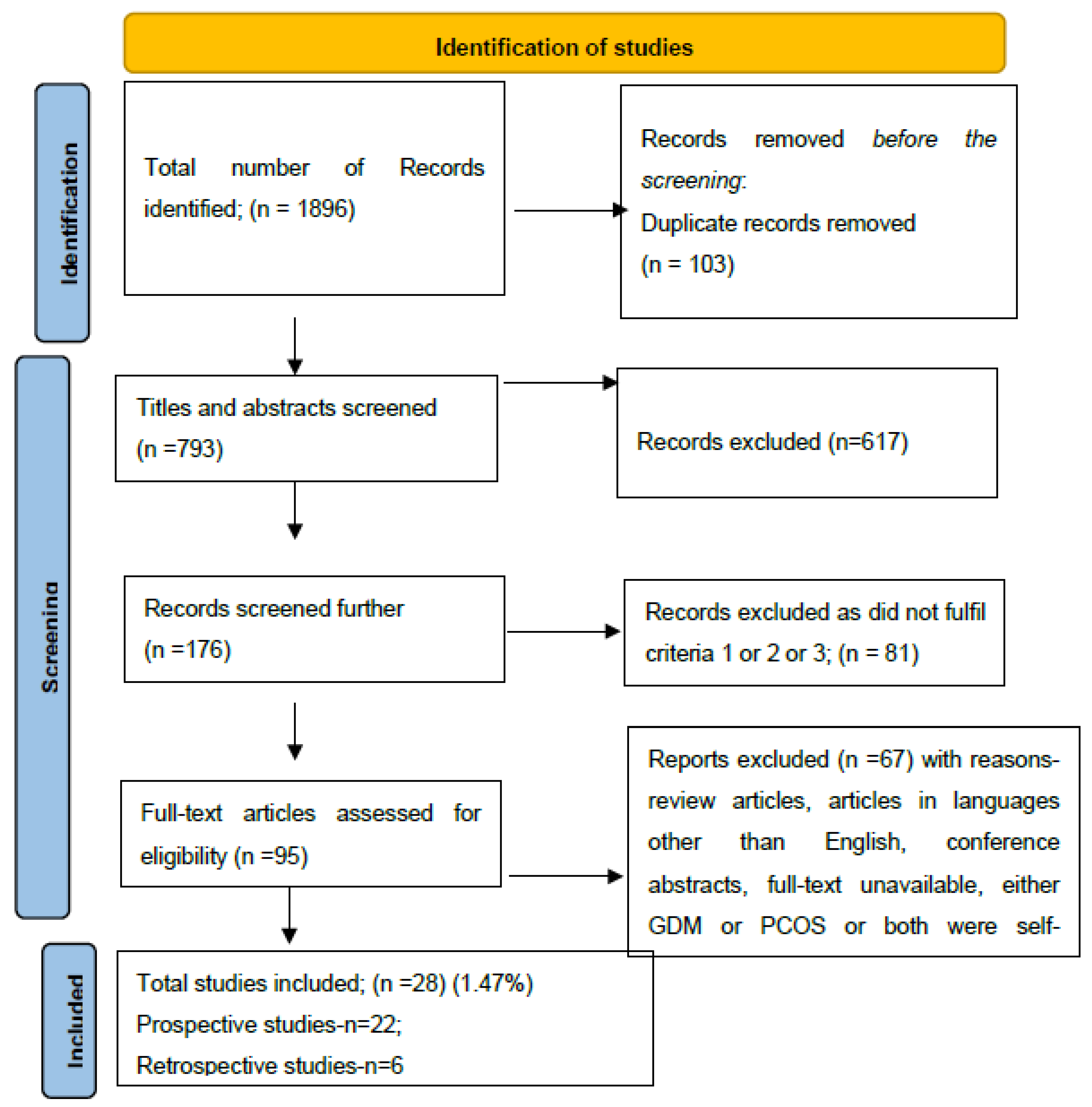
Figure 2.
Forest Plot.

Figure 3.
Funnel Plot.

Figure 4.
Risk factors of GDM in women with PCOS.
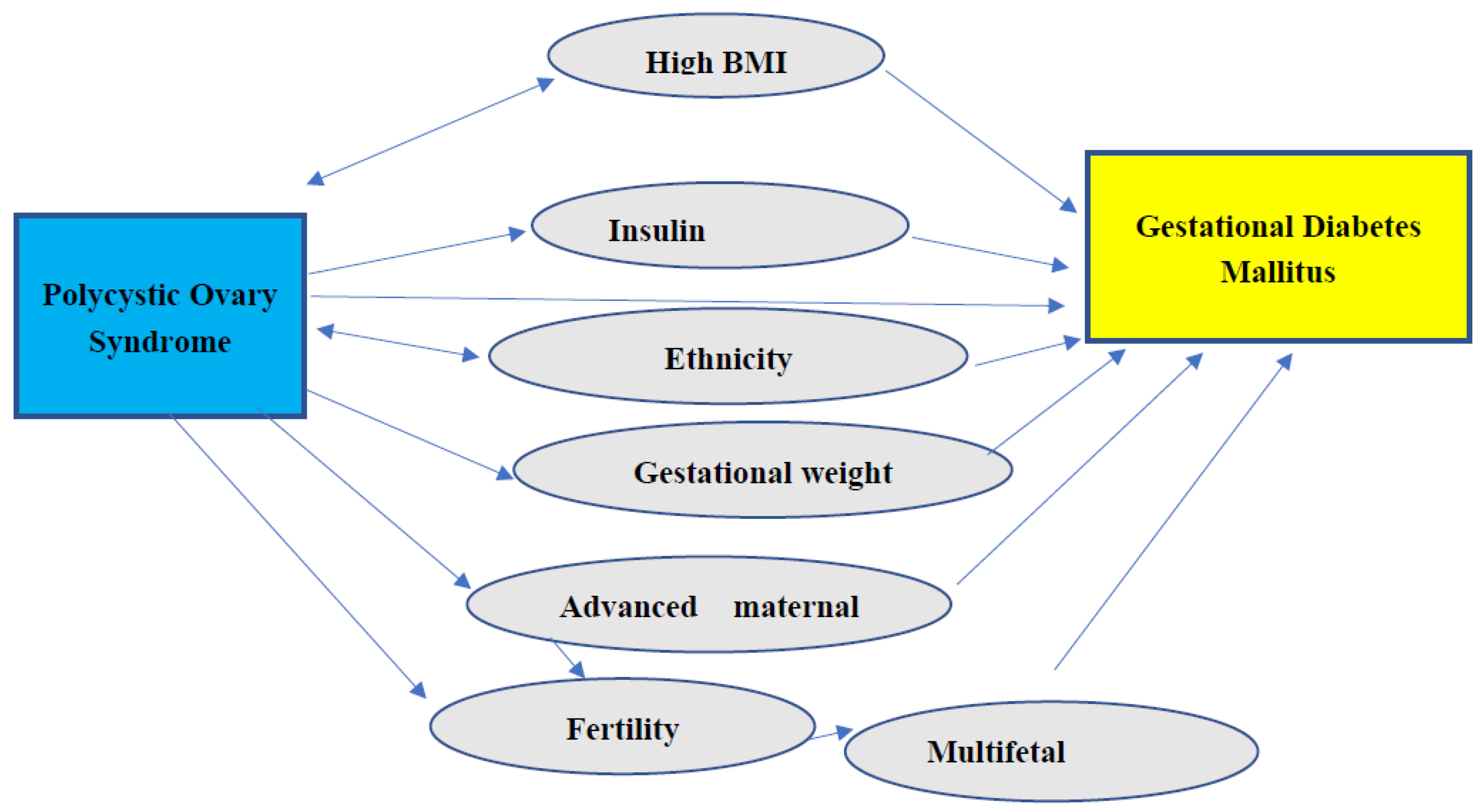

Table 1.
Diagnosis of GDM.
| Threshold for GDM diagnosis | Fasting [mmol/L (mg/dL)] |
1HPG [mmol/L (mg/dL)] |
2HPG [mmol/L (mg/dL)] |
|---|---|---|---|
| 75-g OGTT | |||
| ADA | 5.1 (92.0) | 10.0 (180.0) | 8.5 (152.0) |
| IADPSG | 5.1 (≥92.5) | 10.0 (≥180.0) | 8.5 (≥153.0) |
| WHO | 5.1–6.9 (92.0–125.0) | ≥10.0 (180.0) | 8.5–11.0 (153.0–199.0) |
Table 2.
Incidence of GDM in women with PCOS.
| Author [Reference] |
Sample size | Prevalence of GDM n (%) |
Prevalence of PCOS | Serial number |
|---|---|---|---|---|
| Altieri et al. [40] | 516 | 3 (20%) | 15 | |
| Veltman-Verhulst et al. [41] | 50 | 21 (42%) | 50 | |
| Han A R et al. [42] | 336 | 10 (2.9%) | 336 | |
| Roos N et al. [43] | 1,195,123 | 125 (3.3%) | 3787 | |
| Reyes-Munoz et al. [44] | 104 | 14 (26.9%) | 52 | |
| de Wilde et al. [37] | 326 | 41 (21.6%) | 189 | |
| Ashrafi et al. [45] | 702 | 104 (44.4%) | 234 | |
| de Wilde et al. [46] | 72 | 22 (30.5%) | 72 | |
| Sawada et al. [47] | 113 | 12 (24.5%) | 64 | |
| Pan et al. [48] | 7,629 | 636 (20.46%) | 3,109 | |
| Xiao et al. [49] | 2389 | 64 (18.1%) | 352 | |
| Rees et al. [87] | 27,204 | 253 (4.4%) | 9068 | |
| Xia et al. [50] | 94 | 31 (32.9%) | 94 | |
| Zheng et al. -1[51] | 566 | 39 (26.5%) | 242 | 14 A. |
| Zheng et al. -2[51] | 18,106 | 135 (22.09%) | 877 | 14 B. |
| Fougner et al. [52] | 791 | 297 (41.1%) | 722 | |
| Li et al. [53] | 196 | 47 (23.98%) | 196 | |
| Patnaik et al. [54] | 102 | 9 (17.6%) | 51 | |
| Ouyang et al. [55] | 434 | 104 (24%) | 434 | |
| Wang et al. [56] | 814 | 79 (54.9 %) | 144 | |
| Sterling et al. [57] | 394 | 11 (15.5%) | 71 | |
| Liu et al. [58] | 7678 | 37 (9.7%) | 381 | |
| Qiu et al. [59] | 16,506 | 272 (14.49%) | 1876 | |
| Total | 1,280,245 | 2, 366 (10.55%) | 22,416 |
Table 3.
Prevalence of PCOS in women with GDM.
| Serial no. | Reference | GDM (n) | PCOS (n) |
|---|---|---|---|
| 1. | 60 | 125 | 15 |
| 2. | 61 | 1014 | 174 |
| 3. | 62 | 34,686 | 520 |
| 4. | 63 | 171 | 44 |
| 5. | 64 | 261 | 131 |
| 6. | 65 | 94 | 15 |
| Total | 36,351 | 899 |
Table 4.
Factors in PCOS women associated with GDM.
| Serial no. | Factor [ reference] | Evidence [reference] |
|---|---|---|
| 1. | High BMI [41,46,51,61,66,67,68,69,70,71] |
High BMI increases PCOS [41] High BMI causes GDM but not PCOS [46,60,61,66,67,68,69,70,71] Normal BMI with PCOS had a higher risk of GDM than obese [51] |
| 2. | IR [72,73,74,75,76,77,78,79,80,81,82,83] |
IR was higher in Obese PCOS only [77] IR was higher even with a normal BMI [78] Use of Insulin sensitizers in patients with PCOS [79,80,81,82,83] |
| 3. | Gestational weight gain (GWG) [72,84,85,86,87,88] | GWG is higher in certain ethnicities [72] Overweight women have higher GWG [84,85,86] |
| 4. | Ethnicity and family history [55,72,89,90,91] | GWG is higher in certain ethnicities [72] GDM and PCOS both have a higher prevalence in certain ethnicities [81,82,83,84,85,86,87,88,89] |
| 5. | Multifetal gestation, ART [92,93,94] |
GDM is not higher in PCOS conceived with ART if age and BMI matched [90] GDM is higher with ART compared to spontaneous conception and in Multifetal gestation following ART [93,94] |
[ART= Assisted Reproductive Techniques].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



