
Submitted:
14 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
The recently approved maternal vaccination against respiratory syncytial virus (RSV) can reduce its burden among infants. Vaccine hesitancy/resistance can undermine the beneficial impact of RSV vaccination. The aim of this study was to assess the willingness of pregnant women in Jordan to receive RSV vaccination and its associated determinants. Face-to-face interviews were conducted in obstetrics/gynecology clinics in Jordan during January-February 2024, with convenience sampling. Attitude to RSV vaccination was assessed using the previously validated ABCDEF scale. A total of 404 pregnant women participated in the study with a mean age of 30 years. A majority of the participants showed willingness to receive RSV vaccination (n=313, 77.5%), with hesitancy among 25 participants (6.2%), and resistance among 66 participants (16.3%). Variables that were significantly associated with a higher RSV vaccine acceptance in multivariate analysis were: age <30 years (aOR: 2.45, p=0.010), undergraduates (aOR: 3.27, p=0.026), being a healthcare worker (aOR: 4.50, p=0.036), and the history of previous COVID-19/influenza vaccine uptake (aOR: 2.47, p=0.045). Two out of the six ABCDEF constructs were significantly associated with RSV vaccine acceptance, namely the “Advice” construct (aOR: 10.38, p<0.001) and the “Fear” construct (aOR: 21.49, p<0.001). This study highlighted the multifaceted nature of attitude towards maternal RSV vaccination among pregnant women. The study showed the role of demographic variables, prior vaccination experience, trust in credible health institutions and vaccine safety, and fear of RSV disease consequences in infants in shaping maternal attitude to RSV vaccination. Addressing these factors can help to effectively promote RSV vaccine uptake, subsequently helping to protect infants from the significant RSV disease burden.
Keywords:
maternal immunization
; pregnancy
; vaccine attitude
; vaccine hesitancy
1. Introduction
The respiratory syncytial virus (RSV) is the most common respiratory pathogen among infants contributing to a substantial global health burden [1,2]. This RNA virus is considered a leading cause of lower respiratory tract infections (LRTIs) among infants with substantial morbidity and mortality rates [3,4,5]. Specifically, RSV is responsible for an estimated annual mortality rate exceeding 100,000 among children under the age of 5 years [2]. Therefore, the RSV disease burden motivated the pursuit for effective preventive measures, particularly directed towards the most at-risk populations such as infants [6,7,8].
The recent breakthroughs in RSV preventive approaches were manifested in the development and approval of RSV vaccines for use in pregnant women and among the elderly [9,10,11,12]. Maternal immunization against RSV confers passive immunity to newborns; therefore, this cost-effective approach helps to protect infants against RSV infection when they are most susceptible to severe consequences of RSV disease [13,14,15].
Despite the promising potential of maternal RSV vaccination in protecting infants from RSV disease, the success of this strategy is dependent upon high vaccine uptake among the target population, namely pregnant women [16]. A considerable challenge that needs further investigation is the potential for vaccine hesitancy and resistance among pregnant women considering their heightened perceived risk for themselves and their fetuses [17,18]. A recent narrative review reported that about a third of pregnant women remain unvaccinated despite recommendations from healthcare providers [19].
Vaccine hesitancy is defined as the delay in acceptance or outright refusal of vaccines despite the availability of vaccination services [20]. It is a complex and context-specific phenomenon that varies across time, place, culture, and vaccine type [21,22]. Attitude towards vaccination is influenced by factors such as complacency, convenience, confidence, calculation of benefits and risks, as well as socio-cultural beliefs including misconceptions about vaccine safety and efficacy, which can be of particular importance during pregnancy [19,23,24,25].
Vaccine resistance or hesitancy among pregnant women can be related to several factors. These factors include concerns about the potential adverse effects of vaccines on fetal health and development, perceived risks of vaccination during pregnancy, and the influence of vaccine misinformation [26,27,28,29]. Thus, elucidation of the determinants of vaccine resistance/hesitancy among pregnant women appears essential to develop targeted intervention measures to promote vaccine uptake [30]. In the context of maternal RSV vaccination, this investigation can help to address the challenge of vaccine resistance/hesitancy through the development of targeted communication strategies specifically tailored to engage pregnant women [18,31,32].
Thus, the current study aimed to investigate the attitude of pregnant women towards the recently approved RSV vaccination. This study sought to elucidate the underlying factors which can contribute to RSV vaccine resistance/hesitancy among pregnant women in Jordan utilizing a survey instrument specifically designed for this purpose [16]. In turn, the findings of this study can help to reveal valuable insights into the possible barriers and motivators of RSV vaccine acceptance among pregnant women in Jordan with possible implications in the Arab region where vaccine hesitancy was a notable phenomenon during the coronavirus disease 2019 (COVID-19) pandemic [33].
2. Materials and Methods
2.1. Study Design and Ethics Statement
This cross-sectional study was based on adopting the previously validated “ABCDEF” scale specifically designed for the assessment of the determinants of RSV vaccine attitude in younger women at childbearing age [16]. Data collection was based on conducting structured face-to-face interviews with potential participants recruited from various obstetrics/gynecology clinics across Jordan.
Prior to participation, all participants provided verbal informed consent to ensure voluntary participation in the study. No identifying information or personal identifiers were collected during the interview process to protect the participants’ privacy. The participants were not offered any incentives for participation. The interviews were conducted in Arabic language by five authors (T.K., A.A.-F., L.N., N.A., and R.F.) across multiple public and private clinics located in the Capital Amman, Irbid in the Northern region, and Ma’an in the Southern region of Jordan, to ensure a diverse cross-section of the resident population in Jordan. To ensure the consistency and comparability of collected data across the different interviewers, a structured interview consensus was agreed upon prior to data collection. This consensus was achieved through multiple training sessions for all interviewers to familiarize them with the interview process and how to handle potential queries by the participants. The training included mock interviews with role playing exercises with real-time feedback on performance, how to deal with uncooperative participants, and emphasis on the clarity and consistency in response recording. Emphasis was also placed on the importance of maintaining a neutral tone during the interviews while avoiding leading questions.
Given the constraints of funding and the need to expedite the data collection, a convenience sampling strategy was employed. Inclusion criteria included (1) being pregnant female at any gestational age, (2) current residence in Jordan, and (3) good comprehension in Arabic.
The interviews were conducted between 17 January 2024 and 8 February 2024. The study was approved by the Institutional Review Board (IRB) at Jordan University Hospital (reference number 10/2024/1408), granted on 15 January 2024.
2.2. Sample Size Calculation
To estimate the prevalence of maternal acceptance of the RSV vaccine, the Epitools - Epidemiological Calculators online tool was used [34]. The estimate was based on a presumed proportion of RSV vaccine acceptance at 0.5, with a precision level of ±0.05 within a 95% confidence interval. The basis for estimating the annual number of pregnancies in Jordan was the total number of registered live births which was 197,397, according to the Department of Statistics in Jordan 2021 Statistical Yearbook [35]. Thus, the calculated minimum sample size required for the study was determined to be 385 participants.
2.3. Assessment of the Participants’ Demographic Data
The data collection process started with a short introduction to the study objectives, with a short summary on RSV and its negative impact on infants’ health. Additionally, a short overview was given to the participants regarding the recent U.S. Food and Drug Administration (FDA) approval of the ABRYSIVO vaccine for pregnant women in August 2023 [36]. This overview included a summary of the maternal RSV vaccine evaluation on 7,300 pregnant women, highlighting its FDA-authorized administration between 32 and 36 weeks of gestational age and the reported safety and efficacy results [36].
Upon obtaining the verbal informed consent from the participant, a structured interview was conducted to collect demographic data and vaccination history information. The demographic data included age and gestational age at the time of the interview (categorized as up to 13 weeks and 6 days for the first trimester, 14 weeks to 27 weeks and 6 days for the second trimester, and 28 weeks to over 40 weeks for the third trimester). Additional demographic data included the number of offspring (categorized as none, 1, and 2 or more), the highest level of education attained (high school or less, undergraduate, postgraduate), employment status (unemployed, employed non-healthcare worker (non-HCW), employed as HCW), monthly income of the household (1,000 Jordanian dinar (JOD) or less vs. more than 1,000 JOD), place of residence (the Capital (Amman) vs. outside the Capital), nationality (Jordanian vs. non-Jordanian), and vaccination history. The vaccination history specifically focused on the number of COVID-19 vaccine doses received (0, 1, 2, 3), influenza vaccine uptake during the last 2023 season (yes scored as “1” vs. no scored as “0”), and any prior influenza vaccine uptake before the 2023 season (yes scored as “1” vs. no scored as “0”). A vaccine behavior score (VBS) was calculated by summing the total doses of COVID-19 vaccine received and the scores for influenza vaccine uptake, subsequently categorizing the VBS as < 3 vs. ≥ 3.
2.4. Assessment of Attitude Towards RSV Vaccination
First, the participants were asked about their prior awareness of RSV using the item “Have you heard of RSV before this study?” with “yes” vs. “no” as possible responses.
Second, the willingness to receive RSV vaccination during pregnancy was assessed using the following item “I am willing to receive RSV vaccination in pregnancy if it was safe, effective, and provided for free” with responses based on a 5-point Likert scale (agree, somewhat agree, neutral/no opinion, somewhat disagree, disagree). Subsequently, the responses were grouped into acceptance (agreement), vs. hesitancy/resistance (neutral and disagreement) groups.
Finally, 21 items of the ABCDEF scale were introduced with responses based on a 5-point Likert scale (agree, somewhat agree, neutral/no opinion, somewhat disagree, disagree) [16]. These 21 items formed the six ABCDEF constructs as follows. First, the “Advice” construct comprising three items: (1) My previous experience with vaccinations has been generally positive; (2) I would feel confident if the RSV vaccine was recommended during pregnancy by international organizations; and (3) I would feel confident if the RSV vaccine was recommended during pregnancy by the Ministry of Health.
Second, the “Burden” construct comprising three items: (1) The cost of RSV vaccination is an important factor in my attitude toward its acceptance; (2) I consider my husband’s support essential in shaping my decision to receive RSV vaccination during pregnancy; and (3) I consider the support of my family and social circle to be an important factor in shaping my decision to receive RSV vaccination during pregnancy.
Third, the “Conspiracy” construct comprising three items: (1) Pharmaceutical companies that manufacture vaccines care about their financial gains at the expense of public health; (2) The expansion of vaccine manufacturing could be part of a global conspiracy to increase infertility and reduce human population; and (3) The expansion of vaccine manufacturing could be part of a global conspiracy to increase abortions.
Fourth, the “Danger” construct comprising four items: (1) I am concerned about possible side effects of RSV vaccination; (2) I am afraid that vaccination against RSV during pregnancy may harm the fetus; (3) I am concerned about the safety of vaccination in general for pregnant women; and (4) I have concerns about the long-term side effects of RSV vaccination on the health of pregnant women or the health of the fetus.
Fifth, the “Efficiency” construct comprising four items: (1) The cost of the RSV vaccination must be covered by the pregnant woman’s health insurance; (2) I consider the healthcare providers’ recommendations important in shaping my opinion about RSV vaccination; (3) I would like more information about the benefits of RSV vaccination during pregnancy; and (4) I would like more information about the risks of RSV vaccination during pregnancy.
Sixth, the “Fear” construct comprising four items: (1) RSV infection is considered dangerous among children; (2) I believe that RSV vaccination for pregnant women will protect children from infection with the virus; (3) I think it is important for pregnant women to get RSV vaccination; and (4) I am confident in the safety and effectiveness of RSV vaccination for pregnant women.
Subsequently, a scoring system was employed to evaluate responses to each construct as follows: a response of “agree” was scored as 1, “somewhat agree” as 2, “neutral/no opinion” as 3, “somewhat disagree” as 4, and “disagree” was scored as 5. For each construct, individual scores were summed to derive a total construct score. These cumulative scores were then classified into three categories. For the first three constructs (ABC), scores ranging from 3 to 6 were classified as “agree”, scores between 7 and 11 were classified as “neutral”, and scores from 12 to 15 were classified as “disagree”. For the last three constructs (DEF), the “agree” category comprised scores from 4 to 9, “neutral” comprised scores between 10 and 14, and “disagree” comprised scores from 15 to 20.
2.5. Statistical Analysis
The statistical analysis was performed using IBM SPSS Statistics for Windows, Version 27.0 (Armonk, NY: IBM Corp). To test associations between categorical variables, the chi-squared (χ2) test was employed. Following the preliminary univariate analysis, variables with p values of <0.100 were included in subsequent multivariate analysis using the multinomial logistic regression analysis. The final threshold for statistical significance was established at p<0.050.
The reliability of the six ABCDEF constructs within the survey instrument was evaluated using the Cronbach’s α. This assessment yielded Cronbach’s α values indicating satisfactory to excellent internal consistency across the six constructs as follows. The “Advice” construct demonstrated a Cronbach’s α=0.810, the “Burden” construct Cronbach’s α=0.615, the “Conspiracy” construct Cronbach’s α=0.765, the “Danger” construct Cronbach’s α=0.939, the “Efficiency” construct Cronbach’s α=0.835, and the “Fear” construct Cronbach’s α=0.822.
3. Results
3.1. Description of the Study Sample
The final number of participating pregnant women in this study was 404, with a mean age of 30.1±6.2 years (median=30 years, interquartile range (IQR)=25–35 years). The largest proportion of the study participants was in their first trimester, representing 46.8% (n=189) of the participants, and 47.5% (n=192) had two or more children. A majority of the participants had an undergraduate degree (n=262, 64.9%), were unemployed (n=229, 56.7%), had a monthly household income of ≤1000 JOD (n=263, 65.1%), and were living in the Capital Amman (n=282, 69.8%). Additionally, the vast majority of participants were Jordanians (n=377, 93.3%). Moreover, the majority of participants had a vaccination behavior score of <3 (n=304, 75.2%). Finally, more than half of the study participants heard of RSV before the study (n=219, 54.2%, Table 1).
3.2. Attitude Towards RSV Vaccination in the Study Sample
A majority of the participating pregnant women showed willingness to receive RSV vaccination (n=313, 77.5%), while 25 were hesitant (6.2%), and 66 were resistant (16.3%).
Statistically significant higher proportions of RSV vaccine acceptance was observed among participants < 30 years as opposed to those ≥ 30 years (84.0% vs. 71.1%, p=0.002, χ2=9.662), participants with undergraduate education compared to postgraduates and participants with high school or less education (81.3% vs. 77.0% vs. 65.4%, and p=0.011, χ2=8.932), and HCWs compared to unemployed participants and participants employed as non-HCWs (95.7% vs. 75.1% vs. 70.5%, p<0.001, χ2=17.026). Additionally, higher RSV vaccine acceptance was reported among participants with monthly income of household > 1000 JOD compared to those with income ≤ 1000 JOD (87.9% vs. 71.9%, p<0.001, χ2=13.600), and participants with vaccine behavior scores > 3 as opposed to those with scores ≥ 3 (87.0% vs. 74.3%, p=0.009, χ2=6.909, Table 2).
3.3. Correlation of the ABCDEF Constructs with RSV Vaccine Attitude
The full range of responses to the 21 ABCDEF items stratified based on the attitude to RSV vaccination divided into the acceptance versus hesitancy/resistance groups is shown in (Figure 1). Higher agreement levels were particularly pronounced for all items of the “Advice” and “Fear” constructs.
Analyzing the determinants of RSV vaccine attitude based on the ABCDEF constructs yielded statistically significant results for the six constructs. The agreement with the “Advice” construct was strongly associated with vaccine acceptance, with 82.7% (n=259) of agreeing participants showing vaccine acceptance, compared to only 35.2% (n=32) in the hesitancy/resistance group (p<0.001, χ2=101.666). Similarly, agreement with the “Burden” construct items was significantly associated with a higher vaccine acceptance rate of 72.8% (n=228) compared to 40.7% (n=37) among the participants who were hesitant/resistant (p<0.001, χ2=32.865).
The “Conspiracy” and “Danger” constructs showed less conspicuous patterns despite having statistical significance as follows. Higher agreement with the “Conspiracy” construct items was found in the RSV vaccine acceptance group at 46.0% (n=144) compared to 30.8% (n=28) in the hesitancy/resistance group (p=0.026, χ2=7.282). Higher disagreement with the “Danger” construct items was observed among the RSV vaccine acceptance group (n=51, 16.3%) compared to only four (4.4%) in the hesitancy/resistance group (p=0.009, χ2=9.523).
For the “Efficiency” construct, a vast majority of the vaccine acceptance group (n=298, 95.2%) showed agreement, as opposed to 73.6% (n=67) in the hesitancy/resistance group (p<0.001, χ2=38.749). Finally, 75.7% (n=237) of the participants in the RSV vaccine acceptance group showed agreement with the “Fear” construct items in contrast to 22.0% (n=20) in the hesitancy/resistance group (p<0.001, χ2=107.051, Table 3).
3.4. Multivariate Analysis for the Factors Associated with RSV Vaccine Acceptance
Multinomial logistic regression analysis revealed the statistically significant determinants influencing RSV vaccine acceptance among the participating pregnant women, with a Nagelkerke R2 of 0.529 indicating a moderately high explanatory power of the model.
Age showed a significant association with RSV vaccine acceptance, with women < 30 years being more likely to accept the vaccine (adjusted odds ratio (aOR): 2.45, 95% confidence interval (CI): 1.24–4.85, p=0.010) compared to those ≥ 30 years. Educational level was also a significant determinant of RSV vaccine acceptance with undergraduates being more inclined to accept the RSV vaccine (aOR: 3.27, 95% CI: 1.15–9.27, p=0.026) compared to postgraduates. Occupation was also a significant factor, with higher RSV vaccine acceptance among HCWs compared to employed non-HCWs (aOR: 4.50, 95% CI: 1.10–18.52, p=0.036).
Additionally, the vaccine behavior score (VBS) was a significant determinant of RSV vaccine acceptance in the study sample with a higher vaccine acceptance among the participants with VBS ≥ 3 compared to those with a VBS score of < 3 (aOR: 2.47, 95% CI: 1.02–5.99, p=0.045).
Finally, only two out of the six ABCDEF constructs were significantly associated with RSV vaccine acceptance as follows. The agreement with the “Advice” construct strongly predicted RSV vaccine acceptance as opposed to disagreement (aOR: 10.38, 95% CI: 3.20–33.72, p<0.001). A similar pattern was observed for the agreement with the “Fear” construct as opposed to disagreement (aOR: 21.49, 95% CI: 5.00–92.45, p<0.001, Table 4).
4. Discussion
The current study utilized a previously validated survey instrument designed for the analysis of the potential factors influencing RSV vaccine acceptance among pregnant women [16]. This approach helped to reach detailed insights regarding the attitudes towards the newly approved maternal RSV vaccine in a cohort of pregnant women residing in Jordan. Notably, the results of this study pointed to a pronounced willingness to receive RSV vaccination in the study sample, with 77.5% indicating acceptance to receive the vaccine if provided free-of-charge and if the RSV vaccine was deemed safe and efficacious.
Placing the observed prevalence of RSV acceptance in this study within a broader context was challenging, given the recent introduction and approval of the maternal RSV vaccination and the limited number of recent studies addressing this topic [36,37,38]. However, comparison of this rate with vaccine acceptance rates among pregnant women for other vaccine types such as influenza and COVID-19 could provide helpful clues into the perspectives of pregnant women to vaccination [39,40,41]. Lower acceptance rates were reported in the context of COVID-19, where a systematic review and meta-analysis by Milad Azami et al., covering 19,219 pregnant women across 16 articles, found COVID-19 vaccine acceptance to be 53.5% [42]. In an earlier review, Januszek et al. showed that in various studies, the percentage of pregnant women accepting the COVID-19 vaccine was between 29.7% and 77.4% [43].
In a Turkish study by Daşıkan et al., and using a comparative approach, the COVID-19 vaccine acceptance rates among non-pregnant women of reproductive age were substantially higher at 91.7%, compared to lactating women at 77%, and 59% among pregnant women [44]. In Jordan, COVID-19 vaccine acceptance among pregnant women was much lower at a rate of merely 35.4% [45]. Another Jordanian study by Masa'deh et al. reported that women planning for pregnancy, pregnant women, or breastfeeding women showed significantly higher COVID-19 vaccine hesitancy, compared to other women [46].
Studies on influenza vaccine acceptance among pregnant women further reflected this trend of relatively high levels of vaccination hesitancy [39,47,48,49]. An early comprehensive systematic review from 2014 which involved 45 records, found that influenza vaccination uptake among pregnant women varied significantly, from as low as 1.7% to as high as 88.4% for seasonal influenza, and from 6.2% to 85.7% for A/H1N1 pandemic influenza [47]. Additionally, the aforementioned review showed that many pregnant women were not aware of their increased risk for influenza or its potential complications during pregnancy, often underestimating the personal and fetal risks associated with the disease [47].
The relatively high acceptance rate for the newly approved RSV vaccine observed in our study sample can be attributed to several methodological and contextual factors intrinsic to the current study. These factors may have shaped the participants’ perception of the newly approved RSV vaccine. For example, the use of face-to-face interviews could have led to establishment of rapport and trust between the interviewer and the participant, potentially leading to more favorable views on RSV vaccination [50].
In addition, the decision to participate in the study was informed by an overview detailing the efficacy and safety aspects of maternal RSV vaccination as shown by the results of clinical trials and FDA approval [51,52,53,54]. Moreover, the introductory part of the interview highlighted the significant health risks associated with RSV disease in terms of LRTI with considerable morbidity in infants [3,55]. Importantly, the phrasing of the survey item assessing the major outcome in this study, namely RSV vaccine acceptance might have influenced the results. Specifically, this survey item was conceived to emphasize the key positive features of the recently approved RSV vaccine in terms of its safety and efficacy [51-54]. High confidence in vaccine safety and trust in vaccine effectiveness was recently reported among a sample of 400 pregnant or lactating females in a study that investigated attitude to RSV vaccination in Keyna [56].
Furthermore, the phrasing of this survey item involved the precondition that the RSV vaccine could be free of charge. Consequently, this proposition likely served as an additional motivator towards RSV vaccine acceptance since the financial constraint can be a significant barrier to vaccine acceptance [57].
When vaccines are presented as effective in preventing disease and safe for both mother and child, and further enhanced by being offered free of charge, this approach can motivate positive attitude to vaccination [58,59]. Such an approach can significantly diminish vaccine hesitancy/resistance by reducing the perceived barriers and amplifying the perceived benefits of vaccination [60]. Future campaigns can benefit from these insights to promote RSV vaccine uptake. Thus, it is recommended to develop communication strategies that specifically address maternal concerns regarding vaccine safety, improve the awareness of RSV vaccine benefits, and proactively address potential financial constraints that could hinder maternal RSV vaccination. A previous study by Simas et al., highlighted the importance of effectively tailored messaging that addresses specific concerns and needs among pregnant women, thereby strengthening trust in vaccine programs [61].
Regarding the significant determinants of RSV vaccine in this study, the use of multinomial logistic regression analysis demonstrated a substantial explanatory power. This method yielded significant insights into the determinants of RSV vaccine acceptance among pregnant women in Jordan. Specifically, younger participants showed significantly higher likelihood of RSV vaccine acceptance with aOR of 2.45 as opposed to their older counterparts. This finding might be attributed to fear of poor fetal or maternal outcomes among older pregnant women. Higher level of reluctance to get vaccinated among older women could stem from a heightened sense of caution or previous experiences that make them more cautious about vaccination during pregnancy as well as the documented high risks of pregnancy at an advanced maternal age [62,63,64].
The educational level also emerged as another important determinant of RSV vaccine acceptance among pregnant women in this study with undergraduates being more likely to accept the RSV vaccine compared to postgraduates with an aOR of 3.27. A possible explanation for the lower RSV vaccine acceptance among postgraduates may relate to their more critical approach to health interventions. This reflects calculation of the risks versus benefits of vaccination as demonstrated by the 5C model [24]. Another significant finding in this study was the higher likelihood to accept the RSV vaccine among pregnant HCWs compared to non-HCWs (aOR: 4.50). This result is likely attributed to HCWs’ professional experience of the severe consequences of RSV in infants.
Another interesting finding in this study was the association of RSV vaccine acceptance with a previous history of vaccine uptake. This result suggests that trust and satisfaction from previous vaccination experience might enhance willingness to receive novel vaccines. In line with this finding, a study among HCWs in Jordan reported that prior vaccine uptake was a significant determinant of monkeypox vaccine acceptance [65].
In this study, the analysis of the determinants influencing RSV vaccine acceptance among pregnant women highlighted the profound impact of psychological constructs modeled through the ABCDEF scale, particularly the “Advice” and “Fear” constructs. The “Advice” construct involved items assessing the influence of vaccine endorsement by credible health authorities and organizations and the influence of positive past vaccination experiences. This finding emphasized the importance of credibility and trust in health communication, pointing to the need for clear and consistent messaging about the efficacy and safety of vaccines during pregnancy. A recent qualitative study from Kenya highlighted the importance of this particular concern, since the key questions among pregnant and lactating women regarding maternal RSV vaccination revolved around vaccine safety and potential side effects [66].
Moreover, the “Fear” construct, which included items assessing the perceptions of RSV morbidity in children, the belief in the protective benefits of maternal vaccination, and confidence in vaccine safety and effectiveness, showed an even stronger correlation with vaccine acceptance with aOR of 21.49. This result appeared fathomable considering the pregnant women concerns regarding children’s health. Consequently, this fear appears as a critical factor in maternal decision to receive vaccinations, indicating that emotional engagement and perceived personal relevance of the vaccine benefits are highly effective in influencing positive vaccine behavior [67].
Given the insights provided by the findings of this study, public health strategies to promote RSV vaccine uptake should focus on enhancing both the trust and emotional support provided to pregnant women. Endorsements of the RSV vaccine from respected entities such as the World Health Organization (WHO) and the local health ministries can enhance the perceived credibility of vaccine recommendations based on being reliable sources [68,69,70]. Additionally, the public health messages should clearly address common fears regarding vaccine safety and effectiveness, particularly through sharing compelling evidence and real-world data on the benefits of preventing RSV in newborns with emphasis on the disease burden [71]. A recent study showed the potential role of HCWs in advocating the vaccine through raising community awareness of RSV risk and the benefits of maternal RSV vaccination [72]. This was highlighted in a recent study by Limaye et al. in the context of group B Streptococcus (GBS) vaccines, which showed that a multifactorial approach is needed to appreciate the benefits of a future maternal GBS vaccine by raising awareness of GBS-related harms [73]. Ultimately, using the aforementioned insights can help health campaigns to effectively encourage widespread acceptance of RSV vaccination among pregnant women, thereby enhancing positive infantile health outcomes.
Finally, the findings of this study should be interpreted in light of the following limitations. First, the use of convenience sampling, driven by funding constraints and the need to expedite results could have introduced an element of selection bias in the sample. While the study aimed to ensure geographic diversity by approaching obstetrics and gynecology clinics across the Capital, Northern, and Southern regions of Jordan, this approach might still not fully capture the demographic diversity within the country. Second, the approach of face-to-face interviews to collect data may have led to social desirability bias, where participants might provide responses they perceive as socially acceptable rather than their true attitudes. Third, the involvement of five different authors in conducting interviews could have introduced a slight variability in how questions were presented and interpreted by participants. Fourth, the cross-sectional nature of the study captures attitudes at a single point in time, limiting the ability to assess changes in RSV vaccine attitudes over the course of pregnancy or in response to evolving public health information and vaccine recommendations. Fifth, the reliance on self-reported data regarding previous vaccination behavior was a subject to recall bias and may not accurately reflect actual vaccine uptake among the participants. Finally, while the study provided valuable insights into the attitudes of pregnant women in Jordan, its findings may not be directly generalizable to pregnant women in other countries or cultural contexts.
5. Conclusions
The current study highlighted the multifaceted nature of RSV vaccine acceptance among pregnant women. The attitude towards the newly approved RSV vaccine could be influenced by a complex interplay of demographic and psychological factors. Emphasizing the importance of targeted communication that highlights the safety and efficacy of maternal RSV vaccination with robust support from credible healthcare institutions appeared essential in promoting this new vaccine [74].
Considering the specific demographic, psychological, and emotional factors as well as past vaccine uptake that were significant determinants of attitude to RSV vaccination can help to make public health strategies more effective. These strategies are recommended to rely on targeted interventions. In turn, these measures can significantly contribute to promote maternal RSV vaccination with subsequent beneficial impact in reducing the burden of RSV among infants which are the most vulnerable population.
Author Contributions
Conceptualization: Malik Sallam; Methodology: Malik Sallam, Tleen Kherfan, Amwaj Al-Farajat, Leen Nemrawi, Nada Atawneh, Rand Fram, Ala’a B. Al-Tammemi, Muna Barakat, and Kamil Fram; Software: Malik Sallam; Validation: Malik Sallam, Tleen Kherfan, Amwaj Al-Farajat, Leen Nemrawi, Nada Atawneh, Rand Fram, Ala’a B. Al-Tammemi, Muna Barakat, and Kamil Fram; Formal analysis: Malik Sallam; Investigation: Malik Sallam, Tleen Kherfan, Amwaj Al-Farajat, Leen Nemrawi, Nada Atawneh, Rand Fram, Ala’a B. Al-Tammemi, Muna Barakat, and Kamil Fram; Resources: Malik Sallam and Kamil Fram; Data Curation: Malik Sallam, Tleen Kherfan, Amwaj Al-Farajat, Leen Nemrawi, Nada Atawneh, Rand Fram, Ala’a B. Al-Tammemi, Muna Barakat, and Kamil Fram; Writing - Original Draft: Malik Sallam; Writing - Review & Editing: Malik Sallam, Tleen Kherfan, Amwaj Al-Farajat, Leen Nemrawi, Nada Atawneh, Rand Fram, Ala’a B. Al-Tammemi, Muna Barakat, and Kamil Fram; Visualization: Malik Sallam; Supervision: Malik Sallam and Kamil Fram; Project administration: Malik Sallam All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) at Jordan University Hospital (reference number 10/2024/1408), granted on 15 January 2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author (Malik Sallam).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ABCDEF scale | Advice, Burden, Conspiracy, Dangers, Efficiency, and Fear scale |
| aOR | Adjusted odds ratio |
| CI | Confidence interval |
| COVID-19 | Coronavirus disease 2019 |
| FDA | The United States Food and Drug Administration |
| HCW | Healthcare worker |
| IQR | Interquartile range |
| JOD | Jordanian dinar |
| LRTIs | Lower respiratory tract infections |
| RSV | Respiratory syncytial virus |
| VBS | Vaccine behavior score |
| WHO | World Health Organization |
| GBS | Group B Streptococcus |
References
- Munro, A.P.S.; Martinón-Torres, F.; Drysdale, S.B.; Faust, S.N. The disease burden of respiratory syncytial virus in Infants. Curr Opin Infect Dis 2023, 36, 379–384. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; McAllister, D.A.; O'Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, Y.; Shi, T.; Bont, L.J.; Chu, H.Y.; Zar, H.J.; Wahi-Singh, B.; Ma, Y.; Cong, B.; Sharland, E.; et al. Global disease burden of and risk factors for acute lower respiratory infections caused by respiratory syncytial virus in preterm infants and young children in 2019: a systematic review and meta-analysis of aggregated and individual participant data. Lancet 2024, 403, 1241–1253. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Johnson, E.K.; Shi, T.; Campbell, H.; Chaves, S.S.; Commaille-Chapus, C.; Dighero, I.; James, S.L.; Mahé, C.; Ooi, Y.; et al. National burden estimates of hospitalisations for acute lower respiratory infections due to respiratory syncytial virus in young children in 2019 among 58 countries: a modelling study. Lancet Respir Med 2021, 9, 175–185. [Google Scholar] [CrossRef]
- Baraldi, E.; Checcucci Lisi, G.; Costantino, C.; Heinrichs, J.H.; Manzoni, P.; Riccò, M.; Roberts, M.; Vassilouthis, N. RSV disease in infants and young children: Can we see a brighter future? Hum Vaccin Immunother 2022, 18, 2079322. [Google Scholar] [CrossRef] [PubMed]
- Simões, E.A.F.; Bont, L.; Manzoni, P.; Fauroux, B.; Paes, B.; Figueras-Aloy, J.; Checchia, P.A.; Carbonell-Estrany, X. Past, Present and Future Approaches to the Prevention and Treatment of Respiratory Syncytial Virus Infection in Children. Infectious Diseases and Therapy 2018, 7, 87–120. [Google Scholar] [CrossRef] [PubMed]
- Cromer, D.; van Hoek, A.J.; Newall, A.T.; Pollard, A.J.; Jit, M. Burden of paediatric respiratory syncytial virus disease and potential effect of different immunisation strategies: a modelling and cost-effectiveness analysis for England. Lancet Public Health 2017, 2, e367–e374. [Google Scholar] [CrossRef] [PubMed]
- Gong, X.; Luo, E.; Fan, L.; Zhang, W.; Yang, Y.; Du, Y.; Yang, X.; Xing, S. Clinical research on RSV prevention in children and pregnant women: progress and perspectives. Front Immunol 2023, 14, 1329426. [Google Scholar] [CrossRef] [PubMed]
- Kampmann, B.; Madhi, S.A.; Munjal, I.; Simões, E.A.F.; Pahud, B.A.; Llapur, C.; Baker, J.; Pérez Marc, G.; Radley, D.; Shittu, E.; et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med 2023, 388, 1451–1464. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Pérez Marc, G.; Zareba, A.M.; Falsey, A.R.; Jiang, Q.; Patton, M.; Polack, F.P.; Llapur, C.; Doreski, P.A.; Ilangovan, K.; et al. Efficacy and Safety of a Bivalent RSV Prefusion F Vaccine in Older Adults. N Engl J Med 2023, 388, 1465–1477. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Respiratory Syncytial Virus Prefusion F Subunit Vaccine: First Approval of a Maternal Vaccine to Protect Infants. Paediatr Drugs 2023, 25, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, D.; Wilkins, N.; van Leeuwen, E.; Watson, C.H.; Crofts, J.; Flasche, S.; Jit, M.; Atkins, K.E. Protecting infants against RSV disease: an impact and cost-effectiveness comparison of long-acting monoclonal antibodies and maternal vaccination. Lancet Reg Health Eur 2024, 38, 100829. [Google Scholar] [CrossRef] [PubMed]
- Koltai, M.; Moyes, J.; Nyawanda, B.; Nyiro, J.; Munywoki, P.K.; Tempia, S.; Li, X.; Antillon, M.; Bilcke, J.; Flasche, S.; et al. Estimating the cost-effectiveness of maternal vaccination and monoclonal antibodies for respiratory syncytial virus in Kenya and South Africa. BMC Med 2023, 21, 120. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Abu Raya, B.; Baraldi, E.; Flanagan, K.; Martinon Torres, F.; Tsolia, M.; Zielen, S. RSV Prevention in All Infants: Which Is the Most Preferable Strategy? Front Immunol 2022, 13, 880368. [Google Scholar] [CrossRef] [PubMed]
- Kherfan, T.; Sallam, M. Prospective Attitudes towards Respiratory Syncytial Virus (RSV) Vaccination: Validation of a Survey Instrument among Young Females in Jordan Pending Vaccine Authorization. Vaccines (Basel) 2023, 11, 1386. [Google Scholar] [CrossRef] [PubMed]
- Chawanpaiboon, S.; Anuwutnavin, S.; Kanjanapongporn, A.; Pooliam, J.; Titapant, V. A qualitative study of pregnant women’s perceptions and decision-making regarding COVID-19 vaccination in Thailand. Scientific Reports 2024, 14, 5128. [Google Scholar] [CrossRef] [PubMed]
- Kola-Palmer, S.; Keely, A.; Walsh, J. 'It has been the hardest decision of my life': a mixed-methods study of pregnant women's COVID-19 vaccination hesitancy. Psychol Health 2023, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.L.; Schulkin, J.; Power, M.L. Vaccine hesitancy in pregnant Women: A narrative review. Vaccine 2023, 41, 4220–4227. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Peretti-Watel, P.; Larson, H.J.; Ward, J.K.; Schulz, W.S.; Verger, P. Vaccine hesitancy: clarifying a theoretical framework for an ambiguous notion. PLoS Curr 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: an overview. Hum Vaccin Immunother 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007-2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS One 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed]
- Thomson, A.; Robinson, K.; Vallée-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- Adeyanju, G.C.; Engel, E.; Koch, L.; Ranzinger, T.; Shahid, I.B.M.; Head, M.G.; Eitze, S.; Betsch, C. Determinants of influenza vaccine hesitancy among pregnant women in Europe: a systematic review. Eur J Med Res 2021, 26, 116. [Google Scholar] [CrossRef] [PubMed]
- Simsekoglu, N.; Akyuz, E.; Guven, R.; Pasin, O. Attitudes toward COVID-19 vaccines during pregnancy and breastfeeding. Front Public Health 2024, 12, 1286891. [Google Scholar] [CrossRef] [PubMed]
- Rand, C.M.; Olson-Chen, C. Maternal Vaccination and Vaccine Hesitancy. Pediatr Clin North Am 2023, 70, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Bauer-Maison, N.; Guarna, G.; RD, D.S. Social media misinformation about pregnancy and COVID-19 vaccines: A systematic review. Med Princ Pract 2024. [Google Scholar] [CrossRef]
- Rosso, A.; Massimi, A.; Pitini, E.; Nardi, A.; Baccolini, V.; Marzuillo, C.; De Vito, C.; Villari, P. Factors affecting the vaccination choices of pregnant women for their children: a systematic review of the literature. Hum Vaccin Immunother 2020, 16, 1969–1980. [Google Scholar] [CrossRef]
- Patterson, L.; Berry, E.; Parsons, C.; Clarke, B.; Little, A.; Beggs, J.; Chuter, A.; Jackson, T.; Hsia, Y.; McGrath, H.; et al. Using the COM-B framework to elucidate facilitators and barriers to COVID-19 vaccine uptake in pregnant women: a qualitative study. BMC Pregnancy Childbirth 2023, 23, 640. [Google Scholar] [CrossRef]
- Spina, C.I.; Brewer, S.E.; Ellingson, M.K.; Chamberlain, A.T.; Limaye, R.J.; Orenstein, W.A.; Salmon, D.A.; Omer, S.B.; O'Leary, S.T. Adapting Center for Disease Control and Prevention's immunization quality improvement program to improve maternal vaccination uptake in obstetrics. Vaccine 2020, 38, 7963–7969. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J Multidiscip Healthc 2022, 15, 21–45. [Google Scholar] [CrossRef] [PubMed]
- Epitools - Epidemiological Calculators. Sample size to estimate a proportion or apparent prevalence with specified precision. Available online: https://epitools.ausvet.com.au/oneproportion (accessed on 15 January 2024).
- The Jordan Department of Statistics. Jordan 2021 Statistical Yearbook. Available online: http://dosweb.dos.gov.jo/databank/yearbook/YearBook2021.pdf (accessed on 15 January 2024).
- The U.S. Food and Drug Administration (FDA). FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants (accessed on 12 April 2024).
- McCormack, S.; Thompson, C.; Nolan, M.; Imcha, M.; Dee, A.; Saunders, J.; Philip, R.K. Maternal awareness, acceptability and willingness towards respiratory syncytial virus (RSV) vaccination during pregnancy in Ireland. Immunity, Inflammation and Disease 2024, 12, e1257. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Xiu, S.; Yang, L.; Li, L.; Yang, M.; Wang, X.; Shen, Y.; Wang, W.; Lin, L. Perceptions about respiratory syncytial virus (RSV) and attitudes toward the RSV vaccine among the general public in China: A cross-sectional survey. Hum Vaccin Immunother 2024, 20, 2310916. [Google Scholar] [CrossRef]
- Wilson, R.J.; Paterson, P.; Jarrett, C.; Larson, H.J. Understanding factors influencing vaccination acceptance during pregnancy globally: A literature review. Vaccine 2015, 33, 6420–6429. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, A.; Takaku, M.; Saitoh, A. High rates of vaccine hesitancy among pregnant women during the coronavirus disease 2019 (COVID-19) pandemic in Japan. Human Vaccines & Immunotherapeutics 2022, 18, 2064686. [Google Scholar] [CrossRef]
- Kilada, S.; French, N.; Perkins, E.; Hungerford, D. Pregnant women's attitudes and behaviours towards antenatal vaccination against Influenza and COVID-19 in the Liverpool City Region, United Kingdom: Cross-sectional survey. Vaccine X 2023, 15, 100387. [Google Scholar] [CrossRef] [PubMed]
- Azami, M.; Nasirkandy, M.P.; Esmaeili Gouvarchin Ghaleh, H.; Ranjbar, R. COVID-19 vaccine acceptance among pregnant women worldwide: A systematic review and meta-analysis. PLoS One 2022, 17, e0272273. [Google Scholar] [CrossRef] [PubMed]
- Januszek, S.M.; Faryniak-Zuzak, A.; Barnaś, E.; Łoziński, T.; Góra, T.; Siwiec, N.; Szczerba, P.; Januszek, R.; Kluz, T. The Approach of Pregnant Women to Vaccination Based on a COVID-19 Systematic Review. Medicina (Kaunas) 2021, 57, 977. [Google Scholar] [CrossRef]
- Daşıkan, Z.; Ekrem, E.C.; Kıratlı, D. COVID-19 Vaccine Acceptance Among Pregnant, Lactating, and Nonpregnant Women of Reproductive Age in Turkey: A Cross-Sectional Analytical Study. Disaster Med Public Health Prep 2023, 17, e505. [Google Scholar] [CrossRef] [PubMed]
- AbuAlrub, S.; AlShekh, H.B.; Hani, S.B.; Abu Baker, M. The COVID-19 Vaccination Acceptance among Jordanian Pregnant Women: A Cross-sectional Descriptive Study. The Open Nursing Journal 2023, 17. [Google Scholar]
- Masa'deh, R.; Momani, A.; Rayan, A.; Hamaideh, S.H.; Masadeh, O.M.; Al-Yateem, N. COVID-19 vaccine hesitancy among women planning for pregnancy, pregnant or breastfeeding mothers in Jordan: A cross-sectional study. PLoS One 2023, 18, e0286289. [Google Scholar] [CrossRef] [PubMed]
- Yuen, C.Y.; Tarrant, M. Determinants of uptake of influenza vaccination among pregnant women - a systematic review. Vaccine 2014, 32, 4602–4613. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Wang, Y.; Liang, H.; Chen, Y. Seasonal Influenza Vaccine Acceptance among Pregnant Women in Zhejiang Province, China: Evidence Based on Health Belief Model. Int J Environ Res Public Health 2017, 14, 1551. [Google Scholar] [CrossRef] [PubMed]
- Yuet Sheung Yuen, C.; Yee Tak Fong, D.; Lai Yin Lee, I.; Chu, S.; Sau-mei Siu, E.; Tarrant, M. Prevalence and predictors of maternal seasonal influenza vaccination in Hong Kong. Vaccine 2013, 31, 5281–5288. [Google Scholar] [CrossRef] [PubMed]
- Horsfall, M.; Eikelenboom, M.; Draisma, S.; Smit, J.H. The Effect of Rapport on Data Quality in Face-to-Face Interviews: Beneficial or Detrimental? Int J Environ Res Public Health 2021, 18, 10858. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, P. First RSV vaccine approvals. The Lancet Microbe 2023, 4, e577. [Google Scholar] [CrossRef] [PubMed]
- Topalidou, X.; Kalergis, A.M.; Papazisis, G. Respiratory Syncytial Virus Vaccines: A Review of the Candidates and the Approved Vaccines. Pathogens 2023, 12, 1259. [Google Scholar] [CrossRef] [PubMed]
- Fleming-Dutra, K.E.; Jones, J.M.; Roper, L.E.; Prill, M.M.; Ortega-Sanchez, I.R.; Moulia, D.L.; Wallace, M.; Godfrey, M.; Broder, K.R.; Tepper, N.K.; et al. Use of the Pfizer Respiratory Syncytial Virus Vaccine During Pregnancy for the Prevention of Respiratory Syncytial Virus-Associated Lower Respiratory Tract Disease in Infants: Recommendations of the Advisory Committee on Immunization Practices - United States, 2023. MMWR Morb Mortal Wkly Rep 2023, 72, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Verwey, C.; Dangor, Z.; Madhi, S.A. Approaches to the Prevention and Treatment of Respiratory Syncytial Virus Infection in Children: Rationale and Progress to Date. Paediatr Drugs 2024, 26, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Balsells, E.; Wastnedge, E.; Singleton, R.; Rasmussen, Z.A.; Zar, H.J.; Rath, B.A.; Madhi, S.A.; Campbell, S.; Vaccari, L.C.; et al. Risk factors for respiratory syncytial virus associated with acute lower respiratory infection in children under five years: Systematic review and meta-analysis. J Glob Health 2015, 5, 020416. [Google Scholar] [CrossRef] [PubMed]
- Limaye, R.J.; Sauer, M.; Njogu, R.; Singh, P.; Fesshaye, B.; Karron, R.A. Characterizing Attitudes Toward Maternal RSV Vaccines Among Pregnant and Lactating Persons in Kenya: Key Considerations for Demand Generation Efforts for Vaccine Acceptance. J Pediatric Infect Dis Soc 2023, 12, 638–641. [Google Scholar] [CrossRef] [PubMed]
- Simas, C.; Larson, H.J.; Paterson, P. ''Those who do not vaccinate don't love themselves, or anyone else'': a qualitative study of views and attitudes of urban pregnant women towards maternal immunisation in Panama. BMJ Open 2021, 11, e044903. [Google Scholar] [CrossRef] [PubMed]
- Patterson, L.; Berry, E.; Parsons, C.; Clarke, B.; Little, A.; Beggs, J.; Chuter, A.; Jackson, T.; Hsia, Y.; McGrath, H.; et al. Using the COM-B framework to elucidate facilitators and barriers to COVID-19 vaccine uptake in pregnant women: a qualitative study. BMC Pregnancy and Childbirth 2023, 23, 640. [Google Scholar] [CrossRef] [PubMed]
- Badur, S.; Ota, M.; Öztürk, S.; Adegbola, R.; Dutta, A. Vaccine confidence: the keys to restoring trust. Hum Vaccin Immunother 2020, 16, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.; Kilich, E.; Dada, S.; Kummervold, P.E.; Denny, C.; Paterson, P.; Larson, H.J. “Vaccines for pregnant women…?! Absurd” – Mapping maternal vaccination discourse and stance on social media over six months. Vaccine 2020, 38, 6627–6637. [Google Scholar] [CrossRef] [PubMed]
- Simas, C.; Larson, H.J.; Paterson, P. "Saint Google, now we have information!": a qualitative study on narratives of trust and attitudes towards maternal vaccination in Mexico City and Toluca. BMC Public Health 2021, 21, 1170. [Google Scholar] [CrossRef]
- Correa-de-Araujo, R.; Yoon, S.S.S. Clinical Outcomes in High-Risk Pregnancies Due to Advanced Maternal Age. J Womens Health (Larchmt) 2021, 30, 160–167. [Google Scholar] [CrossRef]
- Li, J.; Yan, J.; Jiang, W. The role of maternal age on adverse pregnancy outcomes among primiparous women with singleton birth: a retrospective cohort study in urban areas of China. J Matern Fetal Neonatal Med 2023, 36, 2250894. [Google Scholar] [CrossRef] [PubMed]
- Bayrampour, H.; Heaman, M.; Duncan, K.A.; Tough, S. Advanced maternal age and risk perception: A qualitative study. BMC Pregnancy and Childbirth 2012, 12, 100. [Google Scholar] [CrossRef]
- Mahameed, H.; Al-Mahzoum, K.; AlRaie, L.A.; Aburumman, R.; Al-Naimat, H.; Alhiary, S.; Barakat, M.; Al-Tammemi, A.B.; Salim, N.A.; Sallam, M. Previous Vaccination History and Psychological Factors as Significant Predictors of Willingness to Receive Mpox Vaccination and a Favorable Attitude towards Compulsory Vaccination. Vaccines (Basel) 2023, 11, 897. [Google Scholar] [CrossRef] [PubMed]
- Limaye, R.J.; Fesshaye, B.; Singh, P.; Karron, R.A. RSV awareness, risk perception, causes, and terms: Perspectives of pregnant and lactating women in Kenya to inform demand generation efforts for maternal RSV vaccines. Hum Vaccin Immunother 2023, 19, 2258580. [Google Scholar] [CrossRef] [PubMed]
- Limaye, R.J.; Malik, F.; Frew, P.M.; Randall, L.A.; Ellingson, M.K.; O’Leary, S.T.; Bednarczyk, R.A.; Oloko, O.; Salmon, D.A.; Omer, S.B. Patient Decision Making Related to Maternal and Childhood Vaccines: Exploring the Role of Trust in Providers Through a Relational Theory of Power Approach. Health Education & Behavior 2020, 47, 449–456. [Google Scholar] [CrossRef]
- Berendes, S.; Mounier-Jack, S.; Ojo-Aromokudu, O.; Ivory, A.; Tucker, J.D.; Larson, H.J.; Free, C. "Figuring stuff out myself" - a qualitative study on maternal vaccination in socially and ethnically diverse areas in England. BMC Public Health 2023, 23, 1408. [Google Scholar] [CrossRef] [PubMed]
- Fesshaye, B.; Wade, S.A.; Lee, C.; Singh, P.; Zavala, E.; Ali, H.; Rahman, H.; Siddiqua, T.J.; Atker, S.; Karron, R.A.; et al. Sources of COVID-19 Vaccine Promotion for Pregnant and Lactating Women in Bangladesh. Vaccines (Basel) 2023, 11, 1387. [Google Scholar] [CrossRef] [PubMed]
- Limaye, R.J.; Singh, P.; Paul, A.; Fesshaye, B.; Lee, C.; Zavala, E.; Wade, S.; Ali, H.; Rahman, H.; Akter, S.; et al. COVID-19 vaccine decision-making among pregnant and lactating women in Bangladesh. Vaccine 2023, 41, 3885–3890. [Google Scholar] [CrossRef] [PubMed]
- Zavala, E.; Fesshaye, B.; Lee, C.; Mutwiwa, S.; Njagi, W.; Munyao, P.; Njogu, R.; Gur-Arie, R.; Paul, A.M.; Holroyd, T.A.; et al. Lack of clear national policy guidance on COVID-19 vaccines influences behaviors in pregnant and lactating women in Kenya. Hum Vaccin Immunother 2022, 18, 2127561. [Google Scholar] [CrossRef] [PubMed]
- Limaye, R.J.; Singh, P.; Fesshaye, B.; Karron, R.A. Lessons learned from COVID-19 vaccine acceptance among pregnant and lactating women from two districts in Kenya to inform demand generation efforts for future maternal RSV vaccines. BMC Pregnancy and Childbirth 2024, 24, 221. [Google Scholar] [CrossRef] [PubMed]
- Limaye, R.J.; Singh, P.; Fesshaye, B.; Lee, C.; Schue, J.; Karron, R.A. "Why has this new vaccine come and for what reasons?" key antecedents and questions for acceptance of a future maternal GBS vaccine: Perspectives of pregnant women, lactating women, and community members in Kenya. Hum Vaccin Immunother 2024, 20, 2314826. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; O'Leary, S.T.; Bednarczyk, R.A.; Ellingson, M.K.; Spina, C.I.; Dudley, M.Z.; Chamberlain, A.T.; Limaye, R.J.; Brewer, S.E.; Frew, P.M.; et al. Multi-tiered intervention to increase maternal immunization coverage: A randomized, controlled trial. Vaccine 2022, 40, 4955–4963. [Google Scholar] [CrossRef]
Figure 1.
Error bars representing the means and 95% confidence interval (CI) of the mean for the full ABCDEF items stratified based on attitude to RSV vaccination. The Advice construct (A), the Burden construct (B), the Conspiracy construct (C), the Danger construct (D), the Efficiency construct (E), and the Fear construct (F).
Figure 1.
Error bars representing the means and 95% confidence interval (CI) of the mean for the full ABCDEF items stratified based on attitude to RSV vaccination. The Advice construct (A), the Burden construct (B), the Conspiracy construct (C), the Danger construct (D), the Efficiency construct (E), and the Fear construct (F).
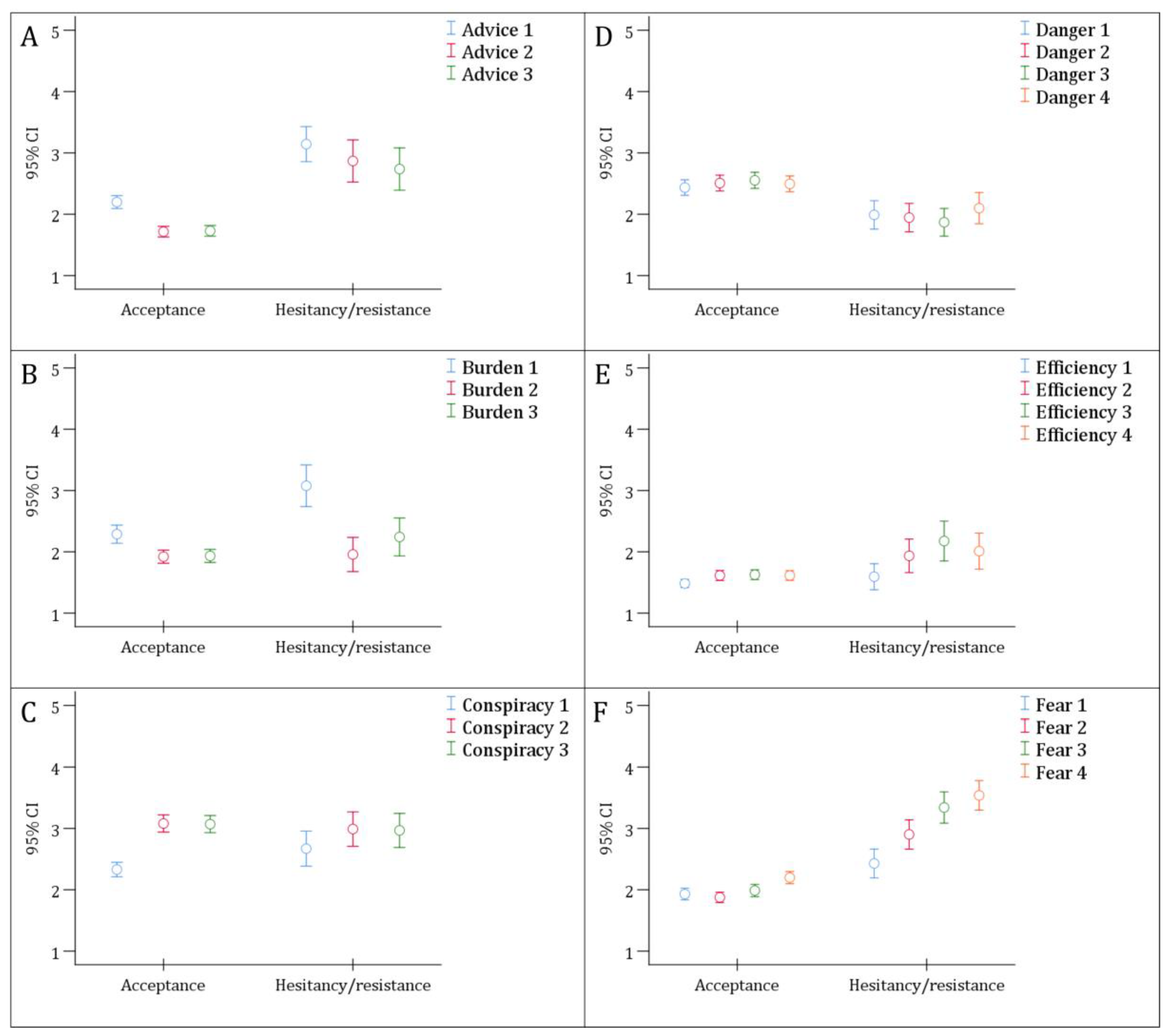

Table 1.
General features of the participating pregnant women (N=404).
| Variable | Category | Count (%) |
|---|---|---|
| Age | < 30 years | 200 (49.5) |
| ≥ 30 years | 204 (50.5) | |
| Pregnancy stage | First trimester | 189 (46.8) |
| Second trimester | 107 (26.5) | |
| Third trimester | 108 (26.7) | |
| Number of children | None | 103 (25.5) |
| One | 109 (27.0) | |
| Two or more | 192 (47.5) | |
| Educational level | High school or less | 81 (20.0) |
| Undergraduate | 262 (64.9) | |
| Postgraduate | 61 (15.1) | |
| Occupation | Unemployed | 229 (56.7) |
| Employed (non-HCW3) | 105 (26.0) | |
| HCW | 70 (17.3) | |
| Monthly income of household | ≤ 1000 JOD4 | 263 (65.1) |
| > 1000 JOD | 141 (34.9) | |
| Residence | Amman | 282 (69.8) |
| Outside the Capital | 122 (30.2) | |
| Nationality | Jordanian | 377 (93.3) |
| Non-Jordanian | 27 (6.7) | |
| Vaccine behavior score1 | < 3 | 304 (75.2) |
| ≥ 3 | 100 (24.8) | |
| Have you heard of RSV2 before this study? | Yes | 219 (54.2) |
| No | 185 (45.8) |
1Vaccine behavior score: Calculated based on the number of COVID-19 vaccine doses received and previous uptake of influenza vaccination; 2RSV: Respiratory syncytial virus; 3HCW: Healthcare worker; 4JOD: Jordanian dinar.
Table 2.
Variables associated with RSV vaccine acceptance in the study sample.
| Variable | Category | RSV4 vaccine attitude | p value, χ2 | |
|---|---|---|---|---|
| Acceptance | Hesitancy/resistance | |||
| Count (%) | Count (%) | |||
| Age | < 30 years | 168 (84.0) | 32 (16.0) | 0.002, 9.662 |
| ≥ 30 years | 145 (71.1) | 59 (28.9) | ||
| Pregnancy stage | First trimester | 142 (75.1) | 47 (24.9) | 0.255, 2.737 |
| Second trimester | 89 (83.2) | 18 (16.8) | ||
| Third trimester | 82 (75.9) | 26 (24.1) | ||
| Number of children | None | 82 (79.6) | 21 (20.4) | 0.159, 3.684 |
| One | 90 (82.6) | 19 (17.4) | ||
| Two or more | 141 (73.4) | 51 (26.6) | ||
| Educational level | High school or less | 53 (65.4) | 28 (34.6) | 0.011, 8.932 |
| Undergraduate | 213 (81.3) | 49 (18.7) | ||
| Postgraduate | 47 (77.0) | 14 (23.0) | ||
| Occupation | Unemployed | 172 (75.1) | 57 (24.9) | <0.001, 17.026 |
| Employed (non-HCW2) | 74 (70.5) | 31 (29.5) | ||
| HCW | 67 (95.7) | 3 (4.3) | ||
| Monthly income of household | ≤ 1000 JOD3 | 189 (71.9) | 74 (28.1) | <0.001, 13.600 |
| > 1000 JOD | 124 (87.9) | 17 (12.1) | ||
| Residence | Amman | 226 (80.1) | 56 (19.9) | 0.051, 3.805 |
| Outside the Capital | 87 (71.3) | 35 (28.7) | ||
| Nationality | Jordanian | 294 (78.0) | 83 (22.0) | 0.360, 0.837 |
| Non-Jordanian | 19 (70.4) | 8 (29.6) | ||
| Vaccine behavior score1 | < 3 | 226 (74.3) | 78 (25.7) | 0.009, 6.909 |
| ≥ 3 | 87 (87.0) | 13 (13.0) | ||
1Vaccine behavior score: Calculated based on the number of COVID-19 vaccine doses received and previous uptake of influenza vaccination; 2HCW: Healthcare worker; 3JOD: Jordanian dinar; 4RSV: Respiratory syncytial virus. Statistically significant p values are highlighted in bold style.
Table 3.
Association of the ABCDEF constructs with RSV vaccine attitude.
| Construct | Category | RSV1 vaccine attitude | p value χ2 | |
|---|---|---|---|---|
| Acceptance | Hesitancy/resistance | |||
| Count (%) | Count (%) | |||
| Advice | Agree | 259 (82.7) | 32 (35.2) | <0.001, 101.666 |
| Neutral | 47 (15.0) | 31 (34.1) | ||
| Disagree | 7 (2.2) | 28 (30.8) | ||
| Burden | Agree | 228 (72.8) | 37 (40.7) | <0.001, 32.865 |
| Neutral | 74 (23.6) | 45 (49.5) | ||
| Disagree | 11 (3.5) | 9 (9.9) | ||
| Conspiracy | Agree | 144 (46.0) | 28 (30.8) | 0.026, 7.282 |
| Neutral | 104 (33.2) | 42 (46.2) | ||
| Disagree | 65 (20.8) | 21 (23.1) | ||
| Danger | Agree | 192 (61.3) | 59 (64.8) | 0.009, 9.523 |
| Neutral | 70 (22.4) | 28 (30.8) | ||
| Disagree | 51 (16.3) | 4 (4.4) | ||
| Efficiency | Agree | 298 (95.2) | 67 (73.6) | <0.001, 38.749 |
| Neutral | 12 (3.8) | 16 (17.6) | ||
| Disagree | 3 (1.0) | 8 (8.8) | ||
| Fear | Agree | 237 (75.7) | 20 (22.0) | <0.001, 107.051 |
| Neutral | 71 (22.7) | 50 (54.9) | ||
| Disagree | 5 (1.6) | 21 (23.1) | ||
1RSV: Respiratory syncytial virus. Statistically significant p values are highlighted in bold style.
Table 4.
Factors associated with RSV vaccine acceptance using multinomial logistic regression.
| RSV1 vaccine acceptance vs. hesitancy/resistance; Nagelkerke R2=0.529 | aOR5 (95% CI6) | p value |
|---|---|---|
| Age | ||
| < 30 years | 2.454 (1.242–4.851) | 0.010 |
| ≥ 30 years | Ref. | |
| Educational level | ||
| High school or less | 0.978 (0.284–3.361) | 0.971 |
| Undergraduate | 3.266 (1.150–9.270) | 0.026 |
| Postgraduate | Ref. | |
| Occupation | ||
| Unemployed | 0.307 (0.074–1.281) | 0.105 |
| Employed (non-HCW2) | 0.222 (0.054–0.906) | 0.036 |
| HCW | Ref. | |
| Monthly income of household | ||
| ≤ 1000 JOD3 | 1.425 (0.582–3.488) | 0.438 |
| > 1000 JOD | Ref. | |
| Residence | ||
| Amman | 1.675 (0.84–3.339) | 0.143 |
| Outside the Capital | Ref. | |
| Vaccine behavior score4 | ||
| < 3 | 0.405 (0.167–0.978) | 0.045 |
| ≥ 3 | Ref. | |
| Advice construct | ||
| Agree | 10.379 (3.195–33.719) | <0.001 |
| Neutral | 3.172 (0.933–10.784) | 0.065 |
| Disagree | Ref. | |
| Burden construct | ||
| Agree | 0.852 (0.150–4.840) | 0.857 |
| Neutral | 0.877 (0.155–4.946) | 0.882 |
| Disagree | Ref. | |
| Conspiracy construct | ||
| Agree | 2.408 (0.867–6.687) | 0.092 |
| Neutral | 1.431 (0.592–3.464) | 0.426 |
| Disagree | Ref. | |
| Danger construct | ||
| Agree | 0.258 (0.043–1.553) | 0.139 |
| Neutral | 0.224 (0.036–1.388) | 0.108 |
| Disagree | Ref. | |
| Efficiency construct | ||
| Agree | 0.866 (0.098–7.622) | 0.897 |
| Neutral | 0.563 (0.052–6.049) | 0.636 |
| Disagree | Ref. | |
| Fear construct | ||
| Agree | 21.489 (4.995–92.446) | <0.001 |
| Neutral | 3.696 (0.953–14.331) | 0.059 |
| Disagree | Ref. |
1RSV: Respiratory syncytial virus; 2HCW: Healthcare worker; 3JOD: Jordanian dinar; 4Vaccine behavior score: Calculated based on the number of COVID-19 vaccine doses received and previous uptake of influenza vaccination; 5aOR: Adjusted odds ratio; 6CI: Confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



