
Submitted:
15 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Despite ongoing efforts, the relationship between groin strength and injury remains unclear. The challenge of accurately predicting injuries presents an opportunity for researchers to develop pre-vention strategies to reduce the occurrence of such injuries. Consequently, this issue requires further investigation to obtain insights into effective mitigation strategies. In 120 male soccer players the maximum isometric strength of the hip muscle groups was measured, and the strength ratios were calculated. Previous injury and anthropometric data were registered. Injury data were collected following the FIFA/UEFA consensus. The K- Nearest Neighbour (k-NN), was used to predict the incidence of injury, while the significant predictive variables of the k-NN algorithm were fitted into a multivariate logistic regression model (LR) to analyze the likelihood of players sustaining a groin injury. The LR model determined two variables as significant predictors of groin injury. Players were less likely to sustain a groin injury by 76% for each decrease of the Adductors/Abductors isometric strength ratio in the non-dominant limb (OR = 0.238, CI 95%= [(0.098-0.572]). Players with a history of previous injury had a 67% greater risk of sustaining an injury (OR = 0.333, CI 95%= [(0.1068-1.038]). Isometric hip adductor and abductor strength im-balances of the non-dominant lower limb and a history of previous injury were risk factors for groin injury in soccer players.
Keywords:
hip muscle strength ratios
; machine learning
; injury prediction
; soccer
; handheld dynamometer
; groin injury
1. Introduction
Hip and groin problems remain prevalent in team sports that require high-intensity tasks [1,2] including sprinting, sudden changes in direction, and kicking [3]. Groin injury incidence rates (IR) range from 1.5 to 1.9 injuries per 1000 hours of total exposure in elite [4] and amateur [5] levels, with a recurrent rate of 18% within two months [6]. These findings suggest the need to implement effective injury prevention programs to reduce the number and severity of groin injuries. To establish effective injury prevention strategies, it is essential that clinicians identify players at high risk of groin injury.
Deficits in muscle strength are often considered important risk factor for hip and groin injuries [1,7]. Strength-related variables may include maximum absolute strength of the muscles involved [8], the strength difference between the two limbs [9,10], and the ratio of agonist to antagonist muscle strength [11] . Some studies have found that low adductor strength levels increased the risk of sustaining a groin injury by 72% [8] or 80% [10] in soccer players while others have reported no association between hip adductor or abductor strength and hip / groin injuries [12]. The association between hip/groin injury and strength difference in both adductor and antagonist muscles is not well understood.To the best of our knowledge, only one study reported that soccer players with hip abduction imbalances favoring the preferred kicking limb had 42% more chances to sustain a future hip/groin injury [9]. In addition, there is evidence that hockey players with weaker adductors relative to abductors were much more likely to sustain an adductor muscle strain [13]. Hence, the relationship between strength and groin injury in soccer remains unclear, which highlights the necessity for more research in this area.
Multiple factors may be responsible for the inconsistent results regarding the correlation between strength and hip/groin injury. These factors interact with a rather complex pattern that presents difficulties to capture using traditional statistical analysis models, such as logistic regression (LR). Artificial Intelligence (AI) and Machine Learning (ML) have been proposed to analyze problems where multiple risk factors and complexity are involved [14,15]. ML is an advanced tool for data analysis that utilizes algorithms that automatically learn from data to predict events [16]. ML algorithms have been recently applied to predict muscle injuries with high accuracy [17] or to identify players at risk for sustaining a hamstring injury [18]. Moreover, pre-season measurements demonstrated good to excellent accuracy in predicting acute or overuse injury amongst young elite soccer players [19], or whether a previous reported injury is likely to occur in the next season amongst professional NHL players [20]. Contrary to the previous promising studies, researchers reported low predictive accuracy in injury prediction [21], in identifying athletes at high risk for hamstring strain [22] or ACL injury [23]. To the best of our knowledge, application of ML algorithms to describe the complex relationship between strength -related variables and hip and groin injuries have not been previously reported.
Muscle strength improvement is an important element of pre-season and in-season exercise programs for enhancing performance as well as for preventing injuries [24]. From a clinical point of view, screening to identify the risk profile of injury of players would assist practitioners in applying effective preventive interventions. This requires understanding not only of the role of maximum strength capacity of the muscle which sustains injury, but also the strength of the same muscle of one leg relative to the other as well as the strength of the antagonist relative to agonist muscle. The primary objective of this study was to investigate the relationship between various factors and the incidence of groin injury in soccer players using ML algorithms. The use of advanced statistical algorithms, such as ML, may provide new insights into the identification of contributors to groin injuries. We hypothesized that players with deficits in maximum strength and strength imbalances between hip adductors and hip abductors were more likely to sustain a groin injury.
2. Methods
2.1. Study Design and Participants
This prospective study follows the recommendations of the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines [25]. Male amateur soccer players over 14 years of age who participated in the regional soccer league and were injury-free the previous six months before the initial start of the pre-season were eligible to participate. During the off-season period of 2018/19 (June to August), 253 male players from 11 teams participating in a regional amateur league were contacted. Of these, 176 players initially agreed to participate. A total of 120 amateur soccer players gave their informed consent and they were enrolled in this study, all of whom fell under tier 2 according to the Participants Classification Framework [26]. The consort flow diagram (Figure 1) describes in detail the inclusion/excusion procedures. The protocol was approved by the ethics committee of Aristotle University in agreement with the Declaration of Helsinki.
2.2. Data Collection and Injury Data Registation
Anthropometric characteristics (age, stature, and body mass) were collected, and body mass index (BMI) was calculated. Players’ preferred leg(s), years of participation, and previous medical history were recorded. All participants performed four bilateral isometric strength tests at the start of the pre-season: Hip Adduction [27] (ADD) Hip Abduction [28] (ABD), Hip Flexion [29] (HFL), and Knee Flexion [30] (HMS) in a lengthening position. Muscle strength was measured using a KFORCE Muscle Controller (K-force, K-Invent Biomecanique, Montpellier, France). This is a hand-held dynamometer (HDD) which has shown high intra-rated (>. 79), inter-rated (>. 72) reliability [31] and validity (ICC > .79 and 0.89) for force and torque, respectively [32].
2.3. Testing Protocol
The maximum isometric strength tests of the hip muscles were conducted in this predetermined sequence. Isometric hip adduction (ADD) strength was evaluated from the supine position. The hips were slightly abducted to fit the angle of the tester’s elbows as previously described by Nielsen and colleagues [27] (2022). The isometric ABD strength was tested in the side-lying position as previously described by Thorborg and colleagues [28], (2011). The isometric HMS strength was tested in the prone position with the knee flexed 15o (0° = full knee extension) as previously described by Reurink and colleagues [30] (2016). Isometric HFL strength was also evaluated from the supine position with hip and knee in 90 o as described by Thorborg and colleagues [29], (2010). During all tests, the players were told to stabilise themselves by holding on to the sides of the table. In each testing position, the investigator’s hand and another against HHD, to ensure correct action. The tester applied resistance in a fixed position, and the person being tested exerted a 3- second isometric maximum voluntary contraction (MVC) against the dynamometer and the tester. Participants were asked to resist the applied force (break test) [33]. Each test was performed bilaterally starting with the right limb and it was administered 2 times separated by a 30-second resting period. A 2-minute rest period between each of the four tests was applied to avoid a decrease in strength in the testing procedures due to potential fatigue [34]. The highest of the 2 valid MVCs was used for subsequent data analysis and treatment.
2.4. Injury Data Registration
Detailed standardized assessment instructions and specific documentation were provided to the medical teams of the clubs. A hip/groin injury was defined and classified in accordance with the Doha agreement meeting on groin pain in athletes [35]. During the competitive season, all injuries were diagnosed and confirmed by the medical staff of the football club or the medical staff of the local hospital following the recommendations adopted by the Doha agreement [35]. Injury data were collected every week, then verified and subsequently collected by the first author (A.K.) who visited each club weekly. Injury definition and assessment characteristics can be found in Supplementary Material 1a. All injuries were registered following the consensus statement on the definitions of injuries and data collection procedures adopted by the FIFA [36]. The time spent by each player in training and match play were recorded by the clubs’ staff and were then verified by the first author on a weekly basis. The data collection form can be found in Supplementary Material 1b.
2.5. Statistical Analysis
Age, history of previous injury, physical characteristics (BMI), and the isometric absolute strength and strength ratios (Supplementary Material 1c) were the input variables while groin injury status (injured, not injured) was the dependent variable in the model.
2.6. Development of the k-NN Model
The k-Nearest Neighbour (k-NN) algorithm is a fundamental supervised ML algorithm that can handle both regression and classification problems [37]. It is often referred to as ‘lazy learning’ or ‘instance-based learning’ due to its lack of a learning process. Instead, it stores the training dataset and performs computations at runtime [37,38]. The k-NN algorithm has demonstrated its effectiveness in mitigating non-linearity relationships that commonly exist in datasets, making it a valuable tool for various classification problems across different domains [37,38]. In the k-NN algorithm, a sample is assigned to the most common class among its k-nearest neighbors in the data space. To determine these neighbors, a distance matrix is used to calculate and sort the distances of each sample from the others. For the development of the k-NN model, we utilized the Pycaret libraries via the Spyder IDE. Other statistical analyses were conducted using the XL STAT add-in software version 2014 for Windows. We selected k=4 and used the Euclidean distance metric, which was determined to be the best fit for the model. To avoid overfitting, a five-fold cross-validation technique was employed, dividing the dataset into five distinctive folds, and testing each one [39].
The data was divided into a 75:25 ratio for training and testing sets [40]. Specifically, we trained the model with 90 data points and tested it with 30 to predict the occurrence of groin injury. Furthermore, a sensitivity analysis was conducted using feature importance plots to evaluate the significance of isometric strength-related variables in influencing the model’s accuracy. These strength-related variables were then used as inputs to a multivariable binary logistic regression to predict the probability of players sustaining a groin injury.
2.7. Model Evaluation
To validate the k-NN model prediction the following performance measures were calculated: the classification accuracy (ACC), the area under the curve (AUC), the Recall, the Precision (PREC), and the F1 score. ACC is the fraction of correctly classified instances. AUC is a curve that shows the model’s ability to separate classes. A recall is the proportion of true positives among actual positives, while PREC is the proportion of true positives among predicted positives. The F1 score is the harmonic mean of PREC and recall and it measures the average accuracy for both classes.
3. Results
Of the total of 120 participants (mean age: 20.0 ± 6.96 years; BMI: 22.53 ± 2.28 kg/m2, Height: 1.77 ± 0.07 m, body mass: 70.66 ± 10.08 Kg), 22 (18.33%) experienced 25 groin injuries. Two players sustained a reinjury. The mechanisms of injury are presented in Table 1.
The performance of the k-NN model in predicting the players’ chances of sustaining a groin injury is summarised in Table 2. The predictive model achieved a mean accuracy score of 55% and an Area Under the Curve (AUC) of 0.43, indicating a reasonable injury prediction. The Precision and Recall scores indicated that the model predicted more than 60% of positive cases and correctly identified 80% of the actual positive classes.
The confusion matrix of the model that developed after cross-validation is presented in Figure 2. This technique was employed to evaluate the performance of the classifier in predicting the groin injury of the players using the training and test data. The model has correctly predicted 68 out of 74 non-injured players indicating 1 misclassification while 14 injured athletes were correctly classified with no misclassification transpired on the injured players during the training stage of the model. Similarly, the model correctly predicted 4 out of 8 injured athletes whereas 5 non-injured athletes were misclassified out of 29. Overall, the model performed reasonably well in the classification task against the test data, despite a relatively low number of observations as well as the imbalance classes that existed within the data.
Figure 3 demonstrates the graphical visualization of the variable’s contribution toward the performance of the model pipeline via the feature importance plot. It can be observed that 7 out of the 20 variables contributed more to the model performance (>8%) towards the probability of sustaining a groin injury. These (7) variables were further analysed using multivariate logistic regression analysis to determine their contribution to the probability of the players getting injured or not based on odd analysis.
The results of the multivariate regression model are presented in Table 3. The results showed that players with a history of previous injury had a 67% higher risk of sustaining a groin injury (OR = 0.333, CI95% = [(0.1068-1.038]). Additionally, players with a lower adductors/abductors’ isometric strength ratio in the non-dominant limb were less likely to sustain a groin injury by 76% (OR = 0.238, CI95%= [(0.098-0.572]). No other significant contributor variables were found (p> 0.05). Overall, the model presented a well-fitting value (Hosmer-Lemeshow >.05), a good correct global classification (87%), and its discriminant capacity was also notable, with an AUC of 77% at a 95% confidence level. The model accounts for 22% of the players’ likelihood of sustaining groin injury or not i.e., injured, or non-injured (Negelkerke R2 = 22.00).
4. Discussion
The main findings of this study are that (a) the adductor/abductor isometric strength ratio of the non-dominant limb was a significant risk factor for groin injury; (b) soccer players with a history of groin injury were at a higher risk of sustaining a groin injury; (c) the isometric strength of either limb or the adductor/abductor ratio of the dominant limb were not significant injury risk factors. To the best of our knowledge, this study is the first to analyze the interrelationship amongst 20 variables through ML applications to predict groin injury in amateur soccer players.
Hip Adductors isometric strength was not a significant contributor to the injury prediction model, which is in line with previous research [12,41]. In contrast, our results rebut previous findings that reported an increased risk of injury for athletes with a lower hip adductor muscle strength of the dominant limb [2,8,9,10,13]. The discrepancies between studies may be attributed to the corresponding differences in methodology. First, in the present study, an ML algorithm was used to examine potential contributors to groin injury, while previous studies used logistic regression [42,43]. ML algorithms have the advantage of that can model highly non-linear relationships, while logistic regression emphasizes inference [44]. Second, unlike previous studies, we incorporated agonist/antagonist strength ratios (in addition to absolute strength values) as well as hip flexor and knee flexor torque values and ratios into the model (Figure 3). The results of any statistical algorithm depend on the number of input variables, their interactions, and their relationship with the occurrence of the injury. Hence, the results of this study are not directly comparable to those reported by previous studies. Interestingly, however, as in contrast to our expectations, when absolute strength of the adductors or the abductors were inserted into the model together with various relative strength and other potential risk factors, it was not a significant groin injury predictor (Figure 3). Therefore, it is doubtful that players with lower absolute strength values would have a higher risk of groin injury.
The results revealed that players with a lower adductor/abductor isometric strength ratio of the non-dominant limb had a 77% greater chance of sustaining a groin injury (Table 3). This finding is interesting for two reasons. First, it was not the absolute strength of the injured muscle or its antagonist that showed a high predictive capacity, but the relative strength between the two antagonistic muscle groups. A previous study has also reported similar findings in ice hockey players [13]. Second, a cross-sectional study found that professional soccer players with previous groin injuries had a lower adductor/abductor strength ratio compared to asymptomatic players [11]. An imbalance between the adductors and abductors may contribute to an altered motion of lumbo-pelvic system, especially when players perform demanding tasks that include acceleration [45], high-speed running [45], and change of direction (CoD) [45,46] (Table 1). In addition to the hip adductors and abductors, pelvic movement can be affected by different muscles, including the hip and knee flexors, which were also analyzed in this research. Interestingly, while the regression analysis did not demonstrate significant predictive value for the ratios between the hip and knee flexors in terms of injury (Table 3), the machine learning algorithm indicated that the knee flexor/hip flexor strength ratio significantly contributed to the model’s performance (Figure 3). It can be inferred from this that any changes in the coordination or strength of the surrounding muscles around the hip and pelvic region might play a role in the generation of excessive forces in the adductor muscle-tendon units, consequently resulting in the occurrence of injury. However, it is apparent that further investigation is required to validate this suggestion.
Our findings indicated that the balance ratio of the non-injured limb, typically the non-dominant limb, is of primary importance in predicting groin injuries (Figure 3). Previous research reported that athletes with lower abductor strength in their dominant/preferred limb, relative to the other limb, were at a higher risk of sustaining a groin injury [9], but other studies failed to confirm similar association [10]. However, none of these studies has examined strength imbalances in both limbs and their association with injury. A recent study observed a deficit in the hip adductor/abductor strength ratio during the middle and end of the season compared to the preseason, which was more pronounced in the non-dominant limb [47]. This may assist in explaining the present findings, suggesting that strength levels may change during the competitive season, and these changes may differ not only between the hip adductors and abductors but also between the two limbs [47].
Consistent with previous research [3], the leading injury mechanisms were changes in direction (CoD) and acceleration (Table 1). These tasks are characterized by high loads of the adductor longus and gracilis, as well as the encompassing passive structures of the groin area [45]. Furthermore, sprint accelerations show kinematics, kinetics, and adductor muscle forces that are like those observed during changes in direction maneuvers, implying that the phase of acceleration phase at the end of the change of direction movement might be responsible for the development of groin injury [45]. Recent studies have found two main mechanisms responsible for the development of groin pain: (1) high amounts of movement with eccentric contractions [48] and (2) rapid transitions between flexion and extension [49]. Both mechanisms are present during changes in direction and side kicking (passing of the ball), which occur repeatedly during training sessions or games [46,48,49]. Consequently, accumulative high muscle stress during eccentric adductor contractions during these accelerations results in high loads and increases the risk of groin injury [50]. The impact of the non-dominant limb in highly demanding soccer tasks, such as acceleration [45], CoD [46], and kicking [48,51], has been previously documented. During these movements, the nondominant limb should support the body and stabilize the pelvis through closed kinetic chains. For example, during the first ground contact of sprint acceleration, the largest hip adductors’ forces were observed when there was a fast transition from hip abduction to adduction with the hip in extension [46]. Similarly, in cutting maneuvers and inside passing, the largest muscle activity of the adductors was found during rapid muscle lengthening [46]. Speculatively, a lower adductor strength of the non-dominant limb indicates a lower capacity of these muscles to withstand high forces when players change direction, especially when the muscles experience a large stretch while stabilizing the hip of the non-dominant limb during the last phase of the change in direction. Further research is necessary to explain the relationship between non-dominant lower limbs and the development of groin injuries.
The k-NN algorithm which was implemented in this study represents a novel approach to predicting groin injuries in soccer, enforcing previous efforts to predict injuries in professional adult [18], or junior players [19]. However, comparison between various studies is difficult due to differences in algorithm method, injury type or level of play of the study sample. ML analyses the significant variables and identifies those with a high predictive impact on the outcome. The algorithm considers both linear and non-linear relationships between the datasets during these analyses. In contrast, the multivariate logistic regression approach is employed of an odd analysis, predicting the likelihood of injury occurrence. However, it is important to note that the LR algorithm has a limitation: it can only extract data with a linear relationship. Consequently, when the relationship between variables is non-linear, the LR may not be able to identify its importance. Therefore, it is imperative to carefully consider the type of relationship between variables when choosing the appropriate statistical approach for injury prediction. Initially, we attempted to use all variables to fit the LR model, but the performance was subpar. Surprisingly, only one variable, namely “Previous injury,” was found to be significant. This finding emphasizes the limitations of the LR model in accurately capturing non-linear data patterns. However, we have successfully employed the LR model for the likelihood analysis, as demonstrated in the odd analysis.
One notable strength of our study lies in the incorporation of the ratios of the isometric strength variables into the predictive model (Table 3). This approach allows for a comprehensive analysis of all-encompassing variables pertinent to injury prediction. It is important to note that removing these added ratios may yield different results, as our analysis captures the intricate interrelationships among variables. Specifically, when a particular variable is deemed essential, other variables may be considered unimportant and vice versa. Researchers should take heed of these findings and consider the limitations of the LR model when dealing with non-linear data.
Several limitations have been encountered in our research. First, we acknowledge that the sample of players who took part in this study was relatively small, which results in a relatively few numbers of injury incidents. It should be mentioned that this study examined players who took part in an amateur league which consists of 11 teams. Even though we contacted all teams, 6 teams finally participated, a 54.5% recruitment rate which is reasonable. Another limitation is the that by defining injuries as time-loss injuries, we did not consider players’ problems that required medical assistance but did not result in time loss. In addition, it should be noted that the measurements were performed in a field setting, which precluded the application of any belt-fixation. These limitations should be taken into consideration when interpreting our findings. On the other hand, strength of the study was its internal validity, since all measurements were performed by the same investigator.
5. Conclusions
This study utilized a ML algorithm to examine the contribution of 20 variables and indices of hip and knee strength to groin injury in amateur soccer players followed for one season. Low isometric strength ratio of adductors/abductors in the non-dominant limb and history of prior injuries were associated with injury thus emphasizing the importance of addressing strength imbalances in the non-dominant limb. Injury mechanisms involving CoD and acceleration were predominant. Our findings showcase the potential of advanced ML techniques for accurate injury prediction, offering valuable insights for targeted prevention strategies and player well-being.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org
Author Contributions
Conceptualization: A.K.; methodology: A.K. F.C.; software: R.M.; validation: R.M.; statistical analysis: R.M, A.K, E.K.; writing—original draft preparation: A.K.; writing—review and editing: E.K., F.K., P.N.; Supervision: E.K., F.C.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Whittaker, J.L.; Small, C.; Maffey, L.; A Emery, C. Risk factors for groin injury in sport: an updated systematic review. Br. J. Sports Med. 2015, 49, 803–809. [Google Scholar] [CrossRef]
- Engebretsen, A.H.; Myklebust, G.; Holme, I.; Engebretsen, L.; Bahr, R. Intrinsic Risk Factors for Groin Injuries among Male Soccer Players. Am. J. Sports Med. 2010, 38, 2051–2057. [Google Scholar] [CrossRef] [PubMed]
- Serner, A.; Mosler, A.B.; Tol, J.L.; Bahr, R.; Weir, A. Mechanisms of acute adductor longus injuries in male football players: a systematic visual video analysis. Br. J. Sports Med. 2018, 53, 158–164. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gomez, J.A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: a systematic review and meta-analysis. Br. J. Sports Med. 2019, 54, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Kekelekis, A.; Kounali, Z.; Kofotolis, N.; Clemente, F.M.; Kellis, E. Epidemiology of Injuries in Amateur Male Soccer Players: A Prospective One-Year Study. Healthcare 2023, 11, 352. [Google Scholar] [CrossRef] [PubMed]
- Mosler, A.B.; Weir, A.; Eirale, C.; Farooq, A.; Thorborg, K.; Whiteley, R.J.; Hӧlmich, P.; Crossley, K.M. Epidemiology of time loss groin injuries in a men’s professional football league: a 2-year prospective study of 17 clubs and 606 players. Br. J. Sports Med. 2017, 52, 292–297. [Google Scholar] [CrossRef]
- Langhout, R.; Tak, I.; van Beijsterveldt, A.-M.; Ricken, M.; Weir, A.; Barendrecht, M.; Kerkhoffs, G.; Stubbe, J. Risk Factors for Groin Injury and Groin Symptoms in Elite-Level Soccer Players: A Cohort Study in the Dutch Professional Leagues. J. Orthop. Sports Phys. Ther. 2018, 48, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Pérez, V.; Travassos, B.; Calado, A.; Gonzalo-Skok, O.; Del Coso, J.; Mendez-Villanueva, A. Adductor squeeze test and groin injuries in elite football players: A prospective study. Phys. Ther. Sport 2019, 37, 54–59. [Google Scholar] [CrossRef]
- Bourne, M.N.; Williams, M.; Jackson, J.; Williams, K.L.; Timmins, R.G.; Pizzari, T. Preseason Hip/Groin Strength and HAGOS Scores Are Associated With Subsequent Injury in Professional Male Soccer Players. J. Orthop. Sports Phys. Ther. 2020, 50, 234–242. [Google Scholar] [CrossRef]
- Markovic, G.; Šarabon, N.; Pausic, J.; Hadžić, V. Adductor Muscles Strength and Strength Asymmetry as Risk Factors for Groin Injuries among Professional Soccer Players: A Prospective Study. Int. J. Environ. Res. Public Heal. 2020, 17, 4946. [Google Scholar] [CrossRef]
- Belhaj, K.; Meftah, S.; Mahir, L.; Lmidmani, F.; Elfatimi, A. Isokinetic imbalance of adductor–abductor hip muscles in professional soccer players with chronic adductor-related groin pain. Eur. J. Sport Sci. 2016, 16, 1226–1231. [Google Scholar] [CrossRef]
- Schoffl, J.; Dooley, K.; Miller, P.; Miller, J.; Snodgrass, S.J. Factors Associated with Hip and Groin Pain in Elite Youth Football Players: A Cohort Study. Sports Med. - Open 2021, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Tyler, T.F.; Nicholas, S.J.; Campbell, R.J.; McHugh, M.P. The Association of Hip Strength and Flexibility with the Incidence of Adductor Muscle Strains in Professional Ice Hockey Players. Am. J. Sports Med. 2001, 29, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Claudino, J.G.; de Oliveira Capanema, D.; De Souza, T.V.; Serrão, J.C.; Pereira, A.C.M.; Nassis, G.P. Current Approaches to the Use of Artificial Intelligence for Injury Risk Assessment and Performance Prediction in Team Sports: a Systematic Review. Sports Med. - Open 2019, 5, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rico-González, M.; Pino-Ortega, J.; Méndez, A.; Clemente, F.; Baca, A. Machine learning application in soccer: a systematic review. Biol. Sport 2023, 40, 249–263. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Moons, K.G.M. Reporting of artificial intelligence prediction models. Lancet 2019, 393, 1577–1579. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Ayala, F.; Puerta, J.M.; Croix, M.B.A.D.S.; Vera-Garcia, F.J.; Hernández-Sánchez, S.; Ruiz-Pérez, I.; Myer, G.D. A Preventive Model for Muscle Injuries. Med. Sci. Sports Exerc. 2018, 50, 915–927. [Google Scholar] [CrossRef] [PubMed]
- Ayala, F.; López-Valenciano, A.; Martín, J.A.G.; Croix, M.D.S.; Vera-Garcia, F.J.; García-Vaquero, M.D.P.; Ruiz-Pérez, I.; Myer, G.D. A Preventive Model for Hamstring Injuries in Professional Soccer: Learning Algorithms. Int. J. Sports Med. 2019, 40, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Rommers, N.; Rössler, R.; Verhagen, E.; Vandecasteele, F.; Verstockt, S.; Vaeyens, R.; Lenoir, M.; D’hondt, E.; Witvrouw, E. A Machine Learning Approach to Assess Injury Risk in Elite Youth Football Players. Med. Sci. Sports Exerc. 2020, 52, 1745–1751. [Google Scholar] [CrossRef]
- Luu, B.C.; Wright, A.L.; Haeberle, H.S.; Karnuta, J.M.; Schickendantz, M.S.; Makhni, E.C.; Nwachukwu, B.U.; Williams, R.J.; Ramkumar, P.N. Machine Learning Outperforms Logistic Regression Analysis to Predict Next-Season NHL Player Injury: An Analysis of 2322 Players From 2007 to 2017. Orthop. J. Sports Med. 2020, 8. [Google Scholar] [CrossRef]
- Oliver, J.L.; Ayala, F.; Croix, M.B.D.S.; Lloyd, R.S.; Myer, G.D.; Read, P.J. Using machine learning to improve our understanding of injury risk and prediction in elite male youth football players. J. Sci. Med. Sport 2020, 23, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Ruddy, J.D.; Cormack, S.J.; Whiteley, R.; Williams, M.D.; Timmins, R.G.; Opar, D.A. Modeling the Risk of Team Sport Injuries: A Narrative Review of Different Statistical Approaches. Front. Physiol. 2019, 10, 829. [Google Scholar] [CrossRef] [PubMed]
- Jauhiainen, S.; Kauppi, J.-P.; Krosshaug, T.; Bahr, R.; Bartsch, J.; Äyrämö, S. Predicting ACL Injury Using Machine Learning on Data From an Extensive Screening Test Battery of 880 Female Elite Athletes. Am. J. Sports Med. 2022, 50, 2917–2924. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.-L.; Chaouachi, A.; Chamari, K.; Dellal, A.; Wisloff, U. Effect of Preseason Concurrent Muscular Strength and High-Intensity Interval Training in Professional Soccer Players. J. Strength Cond. Res. 2010, 24, 653–660. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. 1), 31–34. [Google Scholar] [CrossRef]
- K. A. Mckay et al., “De fi ning Training and Performance Caliber : A Participant Classi fi cation Framework,” pp. 317–331, 2022.
- Nielsen, M.F.; Thorborg, K.; Krommes, K.; Thornton, K.B.; Hölmich, P.; Peñalver, J.J.; Ishøi, L. Hip adduction strength and provoked groin pain: A comparison of long-lever squeeze testing using the ForceFrame and the Copenhagen 5-Second-Squeeze test. Phys. Ther. Sport 2022, 55, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Thorborg, K.; Couppé, C.; Petersen, J.; Magnusson, S.P.; Hölmich, P. Eccentric hip adduction and abduction strength in elite soccer players and matched controls: a cross-sectional study. Br. J. Sports Med. 2009, 45, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Thorborg, K.; Petersen, J.; Magnusson, S.P.; Hölmich, P. Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand. J. Med. Sci. Sports 2010, 20, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Reurink, G.; Goudswaard, G.J.; Moen, M.H.; Tol, J.L.; Verhaar, J.A.; Weir, A. Strength Measurements in Acute Hamstring Injuries: Intertester Reliability and Prognostic Value of Handheld Dynamometry. J. Orthop. Sports Phys. Ther. 2016, 46, 689–696. [Google Scholar] [CrossRef]
- de Almeida, M.B.; Oliveira, C.; Ornelas, G.; Soares, T.; Souto, J.; Póvoa, A.R.; Ferreira, L.M.A.; Ricci-Vitor, A.L. Intra-Rater and Inter-Rater Reliability of the Kinvent Hand-Held Dynamometer in Young Adults. CiiEM 2023. LOCATION OF CONFERENCE, COUNTRYDATE OF CONFERENCE; p. 12.
- N. Olds, M. N. Olds, M., McLaine, S., & Magni, “Validity and Reliability of the Kinvent Handheld Dynamometer in the Athletic Shoulder Test,” J Sport Rehabil, p. [CrossRef]
- van der Ploeg, H. J. G H Oosterhuis, and van H. der Ploeg J G H Oosterhuis, “The ‘make/break test’ as a diagnostic tool in functional weakness F Break-F Make x 100% F Make Encouragement Index (EI) = F with E-F without E x 100% F without E Fatigue Index (FI),” 1991.
- Sisto, S.A.; Dyson-Hudson, T. Dynamometry testing in spinal cord injury. J. Rehabilitation Res. Dev. 2007, 44, 123–136. [Google Scholar] [CrossRef]
- Weir, A.; Brukner, P.; Delahunt, E.; Ekstrand, J.; Griffin, D.; Khan, K.M.; Lovell, G.; Meyers, W.C.; Muschaweck, U.; Orchard, J.; et al. Doha agreement meeting on terminology and definitions in groin pain in athletes. Br. J. Sports Med. 2015, 49, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand. J. Med. Sci. Sports 2006, 16, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Musa, R.M.; Majeed, A.A.; Taha, Z.; Abdullah, M.; Maliki, A.H.M.; Kosni, N.A. The application of Artificial Neural Network and k-Nearest Neighbour classification models in the scouting of high-performance archers from a selected fitness and motor skill performance parameters. Sci. Sports 2019, 34, e241–e249. [Google Scholar] [CrossRef]
- Musa, R.M.; Majeed, A.P.P.A.; Taha, Z.; Chang, S.W.; Nasir, A.F.A.; Abdullah, M.R. A machine learning approach of predicting high potential archers by means of physical fitness indicators. PLOS ONE 2019, 14, e0209638. [Google Scholar] [CrossRef]
- Trost, S.G.; Zheng, Y.; Wong, W.-K. Machine learning for activity recognition: hip versus wrist data. Physiol. Meas. 2014, 35, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- Taha, Z.; Musa, R.M.; Majeed, A.P.P.A.; Abdullah, M.R.; Abdullah, M.A.; Hassan, M.H.A.; Khalil, Z. The employment of Support Vector Machine to classify high and low performance archers based on bio-physiological variables. IOP Conf. Series: Mater. Sci. Eng. 2018, 342, 012020. [Google Scholar] [CrossRef]
- Bakken, A.; Targett, S.; Bere, T.; Eirale, C.; Farooq, A.; Mosler, A.B.; Tol, J.L.; Whiteley, R.; Khan, K.M.; Bahr, R. Muscle Strength Is a Poor Screening Test for Predicting Lower Extremity Injuries in Professional Male Soccer Players: A 2-Year Prospective Cohort Study. Am. J. Sports Med. 2018, 46, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Esteve, E.; Rathleff, M.S.; Vicens-Bordas, J.; Clausen, M.B.; Hölmich, P.; Sala, L.; Thorborg, K. Preseason Adductor Squeeze Strength in 303 Spanish Male Soccer Athletes: A Cross-sectional Study. Orthop. J. Sports Med. 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- DeLang, M.D.; Garrison, J.C.; Hannon, J.P.; McGovern, R.P.; Christoforetti, J.; Thorborg, K. Short and long lever adductor squeeze strength values in 100 elite youth soccer players: Does age and previous groin pain matter? Phys. Ther. Sport 2020, 46, 243–248. [Google Scholar] [CrossRef]
- Liew, B.X.W.; Kovacs, F.M.; Rügamer, D.; Royuela, A. Machine learning versus logistic regression for prognostic modelling in individuals with non-specific neck pain. Eur. Spine J. 2022, 31, 2082–2091. [Google Scholar] [CrossRef]
- Dupré, T.; Potthast, W. Are sprint accelerations related to groin injuries? A biomechanical analysis of adolescent soccer players. Sports Biomech. 2022, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Dupré, T.; Tryba, J.; Potthast, W. Muscle activity of cutting manoeuvres and soccer inside passing suggests an increased groin injury risk during these movements. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Moreno-Pérez, V.; Peñaranda, M.; Soler, A.; López-Samanes; Aagaard, P.; Del Coso, J. Effects of Whole-Season Training and Match-Play on Hip Adductor and Abductor Muscle Strength in Soccer Players: A Pilot Study. Sports Heal. A Multidiscip. Approach 2021, 14, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Dupré, T.; Funken, J.; Müller, R.; Mortensen, K.R.L.; Lysdal, F.G.; Braun, M.; Krahl, H.; Potthast, W. Does inside passing contribute to the high incidence of groin injuries in soccer? A biomechanical analysis. J. Sports Sci. 2018, 36, 1827–1835. [Google Scholar] [CrossRef] [PubMed]
- Charnock, B.L.; Lewis, C.L.; Garrett, W.E.; Queen, R.M. Adductor longus mechanics during the maximal effort soccer kick. Sports Biomech. 2009, 8, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Emery, C.A.; Meeuwisse, W.H. Risk factors for groin injuries in hockey. Med. Sci. Sports Exerc. 2001, 33, 1423–1433. [Google Scholar] [CrossRef]
- Kellis, E.; Katis, A. Biomechanical characteristics and determinants of instep soccer kick. J. Sports Sci. Med. 2007, 6, 154–165. [Google Scholar]
Figure 1.
The Consort Flow Diagram.
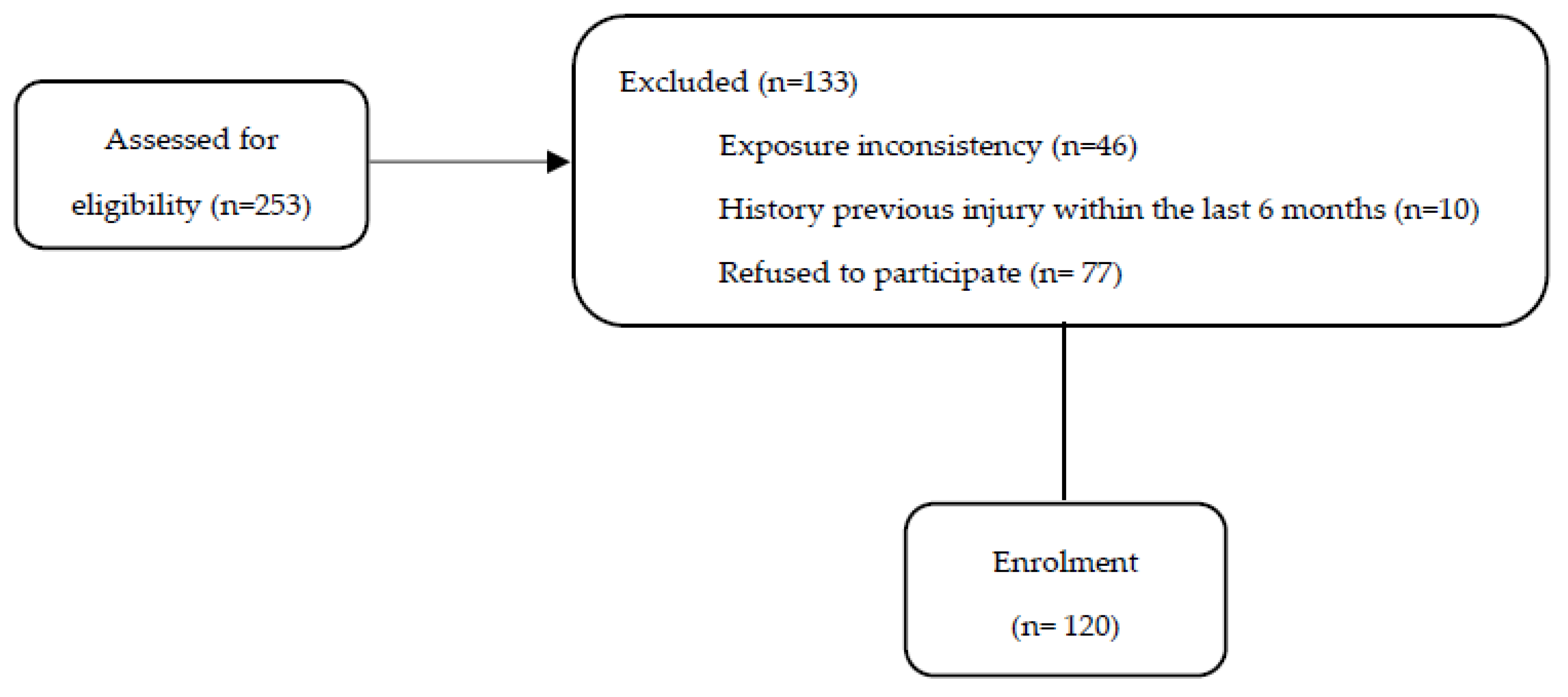
Figure 2.
Confusion matrix of the k-NN : (a) training data set and (b) test data set.
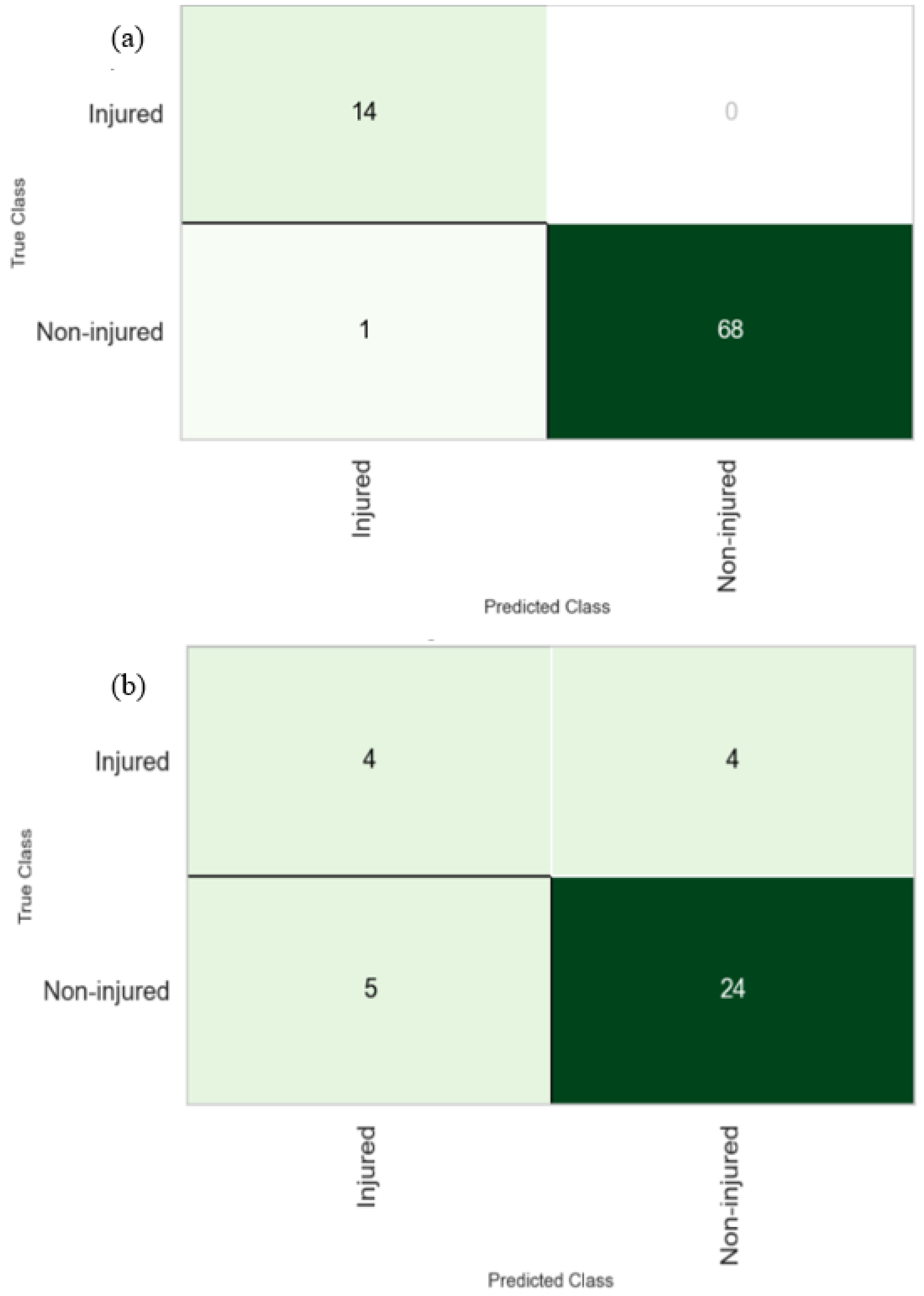
Figure 3.
Variable contribution towards the RL model performance (HFL = Hip flexor; HMS = Knee flexor; ABD = abductor; ADD = Adductors; D = Dominant; ND = Non-dominant).
Figure 3.
Variable contribution towards the RL model performance (HFL = Hip flexor; HMS = Knee flexor; ABD = abductor; ADD = Adductors; D = Dominant; ND = Non-dominant).
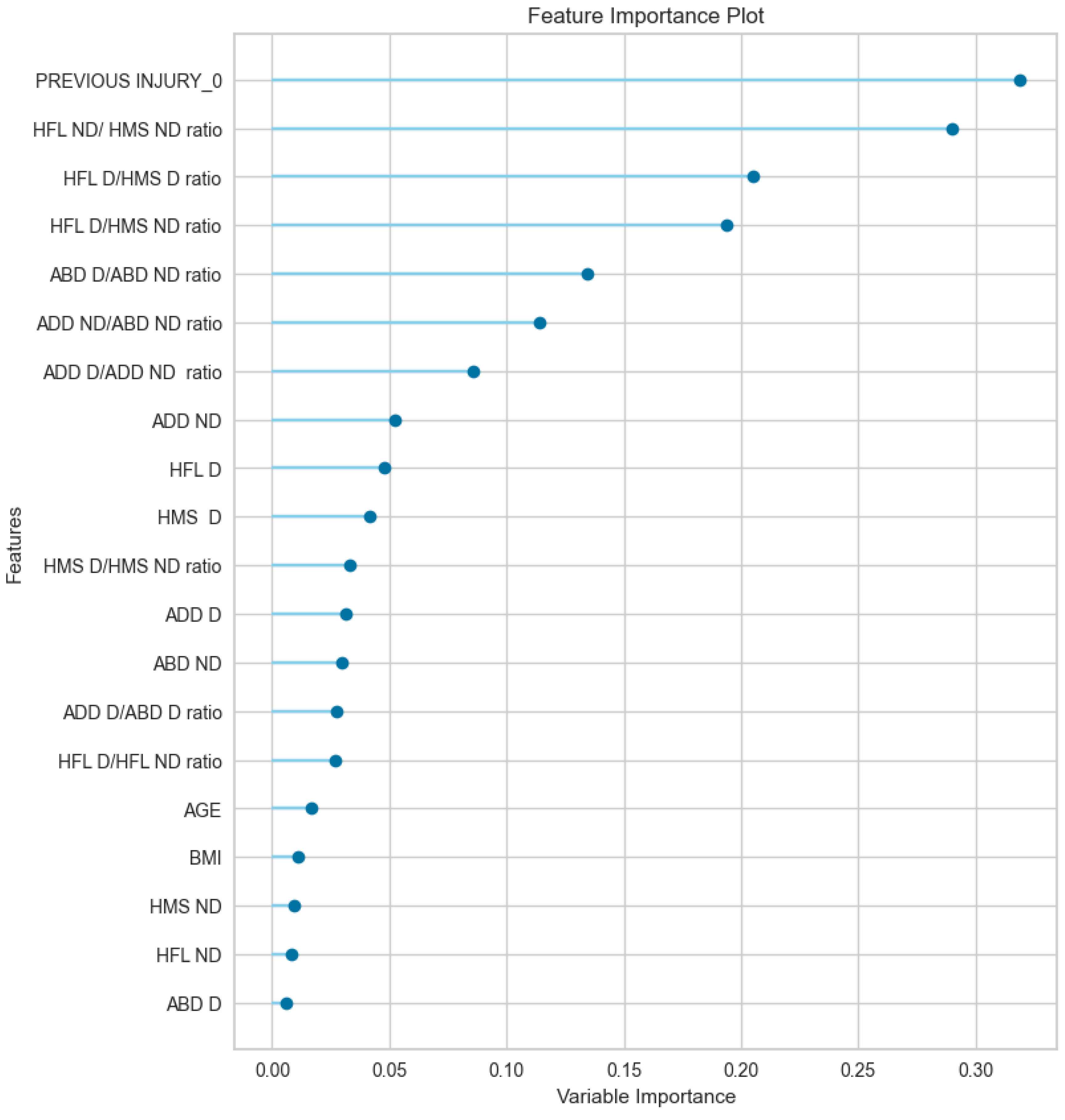

Table 1.
Mechanism of injury.
| Mechanism of groin injury | N |
|---|---|
| Change of direction (CoD) | 12 |
| Acceleration | 4 |
| Stretching | 3 |
| Kicking | 2 |
| inside pass | 2 |
| Decceleration | 2 |
| Total | 25 |
Table 2.
Performance Evaluation of the k-NN model for Predicting adduction injury risk among players.
Table 2.
Performance Evaluation of the k-NN model for Predicting adduction injury risk among players.
| Accuracy | AUC | Recall | Prec. | F1 | |
|---|---|---|---|---|---|
| Mean | 0.556 | 0.425 | 0.609 | 0.806 | 0.688 |
| Std | 0.131 | 0.278 | 0.941 | 0.108 | 0.197 |
Table 3.
The results of the multivariate regression model indicating whether each input variable is a significant contributor. Note. *p<0.05; Nagelkerke R2=22.00; Hosmer Lemeshow (p=0.34); AC= 83%; AUC = 0.774.
Table 3.
The results of the multivariate regression model indicating whether each input variable is a significant contributor. Note. *p<0.05; Nagelkerke R2=22.00; Hosmer Lemeshow (p=0.34); AC= 83%; AUC = 0.774.
| 95% Confidence Interval | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variables | B | SE | Z | p | Odds ratio | Lower | Upper | |
| Intercept | 2.5628 | 1.744 | 1.4697 | 0.142 | 12.972 | 0.4253 | 395.618 | |
| History | -1.0997 | 0.58 | -1.8952 | 0.050* | 0.333 | 0.1068 | 1.038 | |
| HFL ND/ HMS ND ratio | 0.1479 | 1.703 | 0.0869 | 0.931 | 1.159 | 0.0412 | 32.626 | |
| HFL D/HMS D ratio | 0.0499 | 1.354 | 0.0368 | 0.971 | 1.051 | 0.0739 | 14.943 | |
| HFL D/HMS ND ratio | 1.1717 | 1.55 | 0.7558 | 0.45 | 3.228 | 0.1546 | 67.366 | |
| ABD D/ABD ND ratio | 0.4482 | 1.113 | 0.4028 | 0.687 | 1.566 | 0.1768 | 13.862 | |
| ADD ND/ABD ND ratio | -1.4362 | 0.448 | -3.2047 | 0.001* | 0.238 | 0.0988 | 0.572 | |
HFL = Hip flexor; HMS = Knee flexor; ABD = abductor; ADD = Adductors; D = Dominant; ND = Non-dominant; B = beta coefficient; SE = Standard error; Z = Z value; p = level of significance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



