Submitted:
12 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Atypical Polypoid Adenomyoma (APA) is a benign uterine lesion that occurs in women of reproductive age. The histological pattern is characterized by irregular epithelial proliferation and muscular stroma. Our work consists of a systematic review of the literature, including the description and analysis of a case study, and assesses the main immunohistochemical and molecular markers that contribute to making a differential diagnosis against endometrial adenocarcinoma. This allows offering patients conservative treatment compared to the radical management required for endometrial cancer, due to the significant physical and psychological consequences that one procedure or another can have on women's health. The goal of this research is to carry out an adequate diagnosis of APA by providing the necessary information to guide clinical management, establish patient prognosis, and minimize the emotional impact associated with the disease, all in combination with clinical and histopathological findings and complementary imaging tests. In conclusion, an appropriate immunohistochemical and molecular approach, along with the presumptive histological diagnosis, determine the correct classification of the lesion as APA and not as other malignant pathologies, which allows establishing a treatment protocol adjusted to the biological reality of this pathology.
Keywords:
Atypical polypoid adenomyoma
; endometrial cancer
; immunohistochemistry
; molecular biology
1. INTRODUCTION
This article presents a detailed description and thorough analysis of a case involving a 40-year-old female patient with abnormal uterine bleeding. Following a myomectomy and total polypectomy, histopathological diagnosis revealed the presence of an atypical polypoid adenomyoma (APA).
Atypical polypoid adenomyoma (APA) was included in the classification of mixed epithelial and mesenchymal tumours of the uterus along with choriocarcinoma, adenosarcoma, adenofibroma, and adenomyoma by the World Health Organization (WHO) in 2014 [1]. First described by Mazur in 1981 and considered benign at that time, subsequent studies have observed some potential for malignancy, although more extensive research is required to substantiate this hypothesis [2]. According to other authors, there is a medium risk of endometrial carcinoma in women with atypical polypoid adenomyoma, estimated at 8.8% [3]. Literature reveals that APA lesions share immunohistochemical and molecular characteristics with endometrial adenocarcinoma, such as loss of PTEN expression and K-RAS mutations. It has been proposed that APA could be considered analogous to a localized form of atypical endometrial hyperplasia [4].
APA is a rare lesion primarily located in the uterine body, mostly occurring in premenopausal women with a mean age of 39.30 ± 11.01 years, ranging from 17 to 64 years, and an average body mass index of 27.63. It manifests with abnormal vaginal bleeding, dysmenorrhea, polyps, and even infertility or asymptomatic clinical courses, being an incidental finding in infertility studies or abnormal cytology [5,6]. Histologically, it is characterized by irregular proliferation of endometrial glands, which can be tubular or have complex branching, sometimes containing squamous morules with a central focus of necrosis. This epithelial tissue can be arranged in clustered or more spaced configurations, surrounded by smooth fibromuscular stroma organized in short interlaced bundles with minimal cellular atypia and sporadic mitotic cells [7]. Other studies have detected mild cytological atypia in most APA (97%) and endometrioid carcinomas (93%), with a higher mitotic rate in the latter [8].
For diagnosing this non-specific presentation of abnormal uterine bleeding, the initial diagnosis is made through anamnesis and physical and gynecological examination. The first-line imaging test for structural lesions is transvaginal ultrasound, complemented by hysteroscopy with endometrial biopsy for structural causes. Due to the architectural complexity of the lesion, histopathological study using immunohistochemistry (IHC) and molecular pathology techniques is necessary for a proper differential diagnosis with the most common histological type, endometrioid carcinoma, which is mostly low-grade and glandular. Endometrial cancer (EC) is the most common malignant gynecological tumor in Spain and the second in mortality after ovarian cancer. Therefore, it is essential to individualize treatment based on age, clinical presentation, and malignancy potential. In women of childbearing age with reproductive desire, conservative treatment through hysteroscopic resection or even medical treatment with progestogens is advisable due to the estrogen-dependent nature of the pathology, compared to total hysterectomy with bilateral adnexectomy performed as the surgical treatment of choice for endometrial cancer. Chemotherapy, external radiotherapy, and brachytherapy are reserved for inoperable patients or as adjuvant therapy if there is intermediate, high, or advanced risk [9,10]. Rizzuto et al. [11] describe the case of a pregnant woman incidentally diagnosed with endometrial adenocarcinoma within an APA and treated conservatively, leading to a successful term pregnancy.
Advanced immunohistochemistry and molecular pathology techniques were used for lesion diagnosis, crucial for the precise detection of specific biomarkers. Samples were processed using standardized protocols for fixation, paraffin embedding, and sectioning. Immunohistochemical techniques were applied using specific primary antibodies for markers such as b-catenin, h-caldesmon, desmin, vimentin, smooth muscle alpha-actin (SMA), CD10, ki67, ER, PR, pancytokeratin, PTEN, PMS2, MSH6, P53, MLH1, and P16, chosen for their relevance in identifying pathological features of the analyzed lesion. The interpretation of these findings highlights the importance of using specific markers in the precise diagnosis of lesions, providing a solid basis for appropriate therapeutic decisions.
Regarding the results from previous literature studied along with our case, glandular IHC consistently showed positive expression of b-catenin, Ki67, ER, and PR in four studies. Desmin demonstrated strong positivity in five studies. The molecular marker p16 was strongly positive in four studies, while MLH1 and PMS2 were positive in two. Differences in CTNNB1 gene mutations were observed between APA and EC lesions. Comparison between APA and EC highlighted differences in the expression of CD10, h-caldesmon, and p16.
2. MATERIALS AND METHODS
2.1. Literature Search and Selection
For this study, a comprehensive bibliographic review was conducted using PubMed and Google Scholar databases, selecting articles published up to the study's start date. Specific keywords related to immunohistochemistry applied in atypical polypoid adenomyoma were used. Search terms included “atypical polypoid adenomyoma” AND diagnosis, AND immunohistochemistry AND genetics, OR endometrial adenocarcinoma.” A total of thirty-four relevant scientific articles meeting the inclusion criteria were reviewed: thematic relevance, studies focused on immunohistochemistry, and those providing comparable data for histological differentiation between atypical polypoid adenomyoma and endometrial cancer. Additionally, the ONCOSEGO 2023 guide on endometrial cancer was consulted. Online resources from various websites were used for molecular biology studies, such as IMEGEN, Human Genome Variation Society, and PharmGKB.
2.2. Brief description of our patient
A 40-year-old woman presented to the gynecology service with menstrual disturbances and occasional pain, without significant family or personal history. She underwent surgical excision of the endometrium and myometrium. The study was completed with the application of immunohistochemistry techniques in samples previously studied in the literature and our clinical case. For comparison and contrast of results, specific immunohistochemical markers frequently mentioned in the reviewed studies were selected. Procedures followed a standardized protocol, including sample fixation in formalin, paraffin embedding, sectioning into 4 μm thick sections, and subsequent application of specific primary and secondary antibodies. Antibody visualization was performed using a detection kit following the manufacturer’s instructions.
2.3. Data Analysis
Data analysis focused on comparing the expression patterns observed in previous study samples and our case. Qualitative analysis was used to describe the localization and intensity of staining. Results were photographically documented with a microscope, ensuring consistency in lighting and magnification settings. Observed patterns were discussed in the context of findings reported in the literature, using an integrative approach to understand the possible clinical and pathological implications of variations in marker expression.
2.4. Immunohistochemistry
In our case, initial examination was performed with routine hematoxylin-eosin staining, followed by the application of IHC techniques described below. IHC was carried out using diluted antibodies as follows: B-catenin (B-CAT-L-CE 1ml NCL-L-B-CAT), ki67 (KI67-MM1-L-CE 1ml NCL-L-Ki67-MM1), estrogen receptor (ER-6F11-L-CE 1ml NCL-L-ER-6F11), progesterone receptor (PGR-312-L-CE 1ml NCL-L-PGR-312), desmin (DES-DERII-L-CE 1ml NCL-L-DES-DERII), vimentin (VIM-572-L-CE 1ml NCL-L-VIM-572), smooth muscle alpha-actin (SMA-L-CE 1ml NCL-L-SMA), PMS2 (PMS2-L-CE 1ml NCL-L-PMS2), MSH6 (MSH6-L-CE 1ml NCL-L-MSH6), MLH1 (MLH1-L-CE 1ml NCL-L-MLH1), P16 (PA0016 7mL P16), P53 (P53-DO7-L-CE 1ml NCL-L-p53-DO7).
Catenins are cytoplasmic proteins that bind to the highly conserved final portion of the E-cadherin molecule. Beta-catenin is a multiprotein complex of the adherent junction that allows calcium-dependent cell contact, essential for adhesion, signaling, and actin cytoskeleton anchoring. B-catenin acts as an effector of transcription in the Wnt signaling pathway. Positive expression of this molecule, as seen in endometrial cancer, has consequences such as activation of the Wnt signaling pathway, leading to growth, differentiation, and cell proliferation, and is also associated with invasive and metastatic potential of tumor cells, potentially related to higher local invasion and distant spread risk [12].
p16 (INK4a) (Cyclin-dependent kinase inhibitor 2A (CDKN2A)) is a tumor suppressor protein associated with cell cycle progression, specifically regulating the transition from the G1 phase to the S phase. Oncogenic mutations in the CDKN2A gene encoding p16 (resulting in over or underexpression of the protein) are associated with various premalignant and malignant lesions [13].
CD10 or neprilysin is a cell surface metalloendopeptidase that inactivates a variety of biologically active peptides, influencing the regulation of the renin-angiotensin system, the central nervous system, cell differentiation, and plays a role in the pathogenesis of certain cancers and other pathological processes [14].
Caldesmon is a protein found in smooth muscle cells that regulates muscle contraction and organization of the muscle cytoskeleton. It is mainly expressed in tumors of mesenchymal origin [15]. Its role in cancer, including endometrioid cancer, has been studied in relation to its ability to influence cell motility and invasion.
2.5. Molecular Biology
The Action OncoKitDx panel (Grupo Health in Code, Spain) is designed for the analysis of genetic alterations in 59 genes relevant to the development of solid tumors. Covered alterations include point mutations (substitutions, deletions, or insertions), copy number alterations, and rearrangements, with diagnostic and prognostic relevance, as well as therapeutic actionability for representing therapeutic targets and/or predictive markers for approved or clinically developing targeted drugs. Additionally, it integrates microsatellite instability analysis, with potential predictive value in the context of immunotherapy, and pharmacogenetic studies by analyzing variants related to the toxicity or efficacy of major chemotherapy treatments. Study results can help establish personalized therapeutic decisions based on the tumor's genetic alterations.
The Action OncoKitDx panel integrates: Sequencing of complete exonic regions of 55 genes: ALK, ARID1A, ATM, ATRX, BAP1, BRAF, BRCA1, BRCA2, CHEK2, CDH1, CTNNB1, EGFR, ERBB2, ESR1, FGFR1, FGFR2, FGFR3, FGFR4, GNA11, GNAQ, H3F3A, HIST1H3B, HIST1H3H, HRAS, IDH1, IDH2, KIT, KRAS, MAP2K1, MET, MLH1, MSH2, MSH6, MTOR, MYC, NRAS, NTRK1, NTRK2, NTRK3, PALB2, PBRM1, PDGFRA, PIK3CA, PMS2 + 5’UTR, PTEN, POLD1, POLE, RET, ROS1, SDHA, SDHB, SDHD, TERT + 5’UTR, TP53, and VHL.
Sequencing of hotspot regions of the TSC1, TSC2, and AKT1 genes.
Analysis of rearrangements of the ALK, BRAF, EGFR, FGFR2, FGFR3, NRG1, NTRK1, NTRK2, NTRK3, RET, and ROS1 genes. Rearrangement analysis is performed using probes covering the intronic regions where breakpoints have been identified in the indicated genes.
Microsatellite instability (MSI) analysis using a panel of 110 microsatellite regions.
Detection of copy number variations (CNVs) - amplifications and deletions - in the genes covered by the panel and analysis of large chromosomal alterations across the genome, including deletions or gains of entire chromosomes or chromosomal regions.
Detection of pharmacogenetic variants to evaluate the response or toxicity to chemotherapy treatments. Various alterations in seven genes affecting the response to tumors of different origins are analyzed: DPYD (rs3918290, rs67376798, rs55886062, rs115232898, and rs75017182), XRCC1 (rs25487), UGT1A1 (rs4148323), CYP2D6 (rs3892097 and rs5030655), MTHFR (rs1801133), TPMT (rs1142345, rs1800460, rs1800584, and rs1800462), CYP2C9 (rs1799853 and rs1057910).
The preparation of the Action OncoKitDx panel is automated with the Magnis Dx NGS Prep System robot (Agilent, Santa Clara, CA, US). After extracting DNA from the formalin-fixed paraffin-embedded (FFPE) sample, it is enzymatically fragmented and enriched for regions of interest by hybridization with capture probes using SureSelectXT HS technology, following the manufacturer's recommendations. The protocol includes molecular tagging by adding unique molecular identifiers (UMIs), allowing PCR duplicates to be eliminated during library generation, improving the sensitivity and specificity of bioinformatic analysis. High-throughput sequencing is performed on the NextSeq 550 platform using reversible terminator synthesis (paired-end, 2x75bp). Bioinformatic analysis of the results is carried out using a specifically designed analysis pipeline through the Data Genomics platform [16].
The bioinformatic analysis includes the alignment of the obtained sequences with the reference sequence (GRCh37/hg19) for target genes and regions after quality filtering, the identification of variants, and the annotation of variants.
Analytical validation and clinical utility of the Action OncoKitDx panel have been established for both the panel and the Data Genomics analysis program, with in vitro diagnostic marking (CE-IVD) [17].
Technical parameters of the Action OncoKitDx panel obtained in its analytical validation:
Average read depth: 2500x.
Average read depth after UMI analysis: 1600x.
Coverage: 99.3% of bases covered at a minimum read depth of 100x.
•Uniformity: 98.9% of bases covered >20% of the average coverage.
Specificity: > 99%.
Sensitivity: > 99%.
Repeatability: > 99.9%
Reproducibility: > 99.9%.
Requirements, specifications regarding detection limits, and limitations of the Action OncoKitDx panel*:
Required DNA amount: 50-200ng.
Recommended DNA quality: DIN > 3 based on analysis with Genomic DNA ScreenTape Assay and TapeStation 4150 (Agilent).
Recommended tumor cellularity percentage: > 50%.
Minimum tumor cellularity percentage: 30%
Detection limit for point mutations (substitutions, deletions, or insertions): 5%.
Detection limit for copy number variations (CNVs): Estimation of the copy number of covered regions and genes is the result of applying a bioinformatic algorithm that analyzes differences in read depth of obtained sequences.
According to the manufacturer's specifications, a detection limit of 3 copies for gains and 1 copy for losses is established. Based on our experience, an increase in the number of copies above 8 copies could indicate an underlying focal amplification, provided that the analyzed sample's tumor cellularity percentage is >50%. Generally, the lower this percentage, the greater the copy number variation required to indicate underlying gene amplification. Nevertheless, confirmation through a specific quantitative method for CNVs (e.g., fluorescent in situ hybridization, FISH) is recommended if any identified alterations are considered in clinical decision-making.
For rearrangement analysis, mapping of reads on the reference genome differentiates split-reads (reads whose sequence maps to two different genome regions, allowing identification of the fusion point) and discordant read pairs/mate reads (reads that do not include the fusion point but surround it, enabling rearrangement identification).
For microsatellite analysis, at least 99 of the 110 analyzed markers must be evaluable, and classification is based on the percentage of markers showing instability:
High microsatellite instability (MSI-H): 31-100%
Low microsatellite instability (MSI-L): 21-30%
Microsatellite stable (MSS): 0-17%
Inconclusive results: 18-20%
*Detection limits and technical parameters obtained in the analytical validation of the Action OncoKitDx panel are based on samples with the following quality parameters: 200ng DNA and DIN > 3, tumor cellularity percentage > 50%.
There are regions in the genome whose characteristics make it impossible to accurately determine changes in their sequence (homopolymeric, repetitive, or highly homologous regions). Due to the intrinsic limitations of high-throughput sequencing technology for analyzing these regions, clinically relevant variants in the sample may not have been detected. Additionally, for minor alterations in the tumor, a representative number of fragments may not have been obtained during library generation, preventing sufficient sequence numbers for detecting these alterations. According to the manufacturer's specifications, detecting alterations covered by the Action OncoKitDx panel may be compromised when sequencing read depth is less than 200 reads (200x).
Nomenclature of identified mutations and variants follows Human Genome Variation Society (HGVS) recommendations [18].
In the case of online database consultations, the current version at the time of the report was used. The information contained and the interpretation of results based on them are subject to change in future updates. Overall, data analysis and handling of results obtained are based on an interpretive approach reflecting current knowledge at the time of report issuance [19]. Using high-throughput sequencing technology for comprehensive molecular annotation of tumors adheres to recommendations from the European Society of Medical Oncology (ESMO) [20].
The results in this report aim to contribute to better molecular characterization of the patient's tumor, providing information on clinically useful genetic alterations and identifying potential therapeutic targets. However, these results should be considered in the patient's clinical context, and their use in management or therapeutic decision-making will be determined by the oncologist requesting the study.
2.6. Meta-analysis
This study synthesizes findings from previous research by compiling literature with a total of nine articles and 242 cases meeting inclusion criteria, such as immunohistochemical expression in the stroma and glandular epithelium of specific antibodies like CD10, h-caldesmon, desmin, vimentin, smooth muscle alpha-actin (SMA), b-catenin, Ki67, ER, PR, pancytokeratin, PTEN, and molecular study of PMS2, MSH6, P53, MLH1, P16. A simplification strategy was employed to optimize the comprehension of results obtained from different articles as follows: from 1% to 33% positive (+/+++), from 34% to 66% positive (++/+++), 67% to 100% positive (+++/+++) and negative (-) results.
3. RESULTS
In this results section, it is essential to highlight a significant limitation in the comparative analysis of the obtained data. Considerable variability in reporting methodologies was observed among the analyzed studies. While some authors [5,8,17] provided results expressed as a total number of evaluated patients, others limited themselves to reporting the frequency of positive or negative results [21,26,27]. This discrepancy in data presentation prevents the application of conventional statistical techniques for unified analysis.

Table 1.
Study of glandular IHC in APA.
| GLANDULAR IHQ | ||||||
|---|---|---|---|---|---|---|
| No. of Cases | B-Catenin | Ki67 | ER/PR | Pancytokeratin | PTEN+ | |
| OWN CASE | 1 | + | + | + | ||
| YUE | 99 | 2+ | + | + | ||
| TAKASHI | 7 | + | + | |||
| NEMEJCOVA | 21 | 2+ | 3+ | |||
| OTA | 6 | 3+ | ||||
| LU | 36 | + | + | |||
| TERADA | 5 | + | + | 2+ | ||
| SOSLOW | 23 | + | 3+ | |||
Table 2.
Study of stromal IHC in APA.
| ESTROMAL IHQ | ||||||
|---|---|---|---|---|---|---|
| No. | CD10- | H-caldesmon- | Desmin | Vimentin | SMA | |
| OWN CASE | 1 | + | + | |||
| YUE | 99 | - | - | 3+ | 3+ | |
| TAKASHI | 7 | - | + | |||
| LU | 36 | + | - | + | ||
| TERADA | 5 | 2+ | 2+ | 3+ | + | |
| SOSLOW | 23 | 2+ | 3+ | |||
| KIHARA | 12 | 2+ | + | 2+ | 3+ | |
Using glandular IHC, the presence of b-catenin was evaluated. Our findings align with those of three other previous studies, which also reported positive b-catenin expression in the analyzed samples. Including our own case, this positive expression pattern has been observed in a total of four studies, reinforcing the consistency and potential importance as a biomarker in glandular tissue. Ki67 as a cell proliferation marker has been found positive in four studies, although with a low positivity index, as is common in benign tissues. ER and PR show positive results in four studies, along with our own positive findings. Pancytokeratin has shown strong positivity in two studies, similar to our own case. PTEN, a tumor suppressor protein, and its loss may indicate malignant potential, has been analyzed in two studies, resulting in positive outcomes in both. Loss of PTEN expression is commonly observed in endometrial carcinomas, especially in endometrioid types.
In the context of stromal IHC, vimentin shows positive expression in all cases in two studies, noting that beyond these mentioned studies, the presence of this biomarker has not been investigated in the rest of the reviewed literature. Desmin has demonstrated strong positivity in four previously published studies, including our own research, confirming its robust expression pattern in a total of five studies, highlighting desmin's reliability as a biomarker in specific glandular tissues. H-caldesmon has been studied in a limited number of investigations, with two out of three articles reporting predominantly negative results, while the third identifies positive expression. Regarding CD10, it was observed negative in two studies and positive in three, with one study [5] showing negative results, including a sample size of 99 patients, reinforcing its relevance. Lastly, the presence of the SMA antibody shows notable coherence in the reported findings. Specifically, five previous investigations have consistently documented positive results in the expression of this antibody. Adding our own case, our current study reinforces and extends these findings, corroborating the positive association of the SMA antibody.
In the molecular study analysis reflected in Table 3, the p16 marker showed strong positivity in four studies, including our case. MLH1 and PMS2, studied exclusively in two investigations, resulted strongly positive in both cases. Takashi et al. [21] investigated seven APA lesions and found that the CTNNB1 gene was positive for mutations in all cases, suggesting a relationship with β-catenin activity. This finding contrasts with the study by Ota et al. [22], where CTNNB1 mutations were negative in six cases. However, the previous literature shows concordance with the data provided by Takashi.
Table 4 compares the expression of various immunohistochemical markers between atypical polypoid adenomyoma and endometrial adenocarcinoma. CD10 and h-caldesmon were negative in APA, while these markers were positive in EC cases. In contrast, p16 showed positive results in APA and negative in EC. The other markers used (ER, PR, and pancytokeratin) were positive in both cases.
1. Genetic Alterations Mutation study: CTNNB1 (NM_001904.3), mutation: c.94G>T p.(Asp32Tyr), with an allelic frequency of 11%. Rearrangement study: No rearrangements covered by the Action OncoKitDx panel were detected. Copy number variation study: No amplifications or focal deletions of genes covered by the Action OncoKitDx panel, nor alterations in the number of copies affecting large chromosomal regions or complete arms were detected (Figure 1).
2. Microsatellite Instability Study
| Effect | Proportion Instable | Instable Markers | Evaluable Markers/Total Analyzed Markers |
| MSS | 15% | 16 | 105/110 |
3. Pharmacogenetic Study
| Gene | Variant | Genotype | Drug |
| MTHFR (NM_005957) | c.665C>T rs1801133 | G/A | Metotrexato |
4. Histological Study
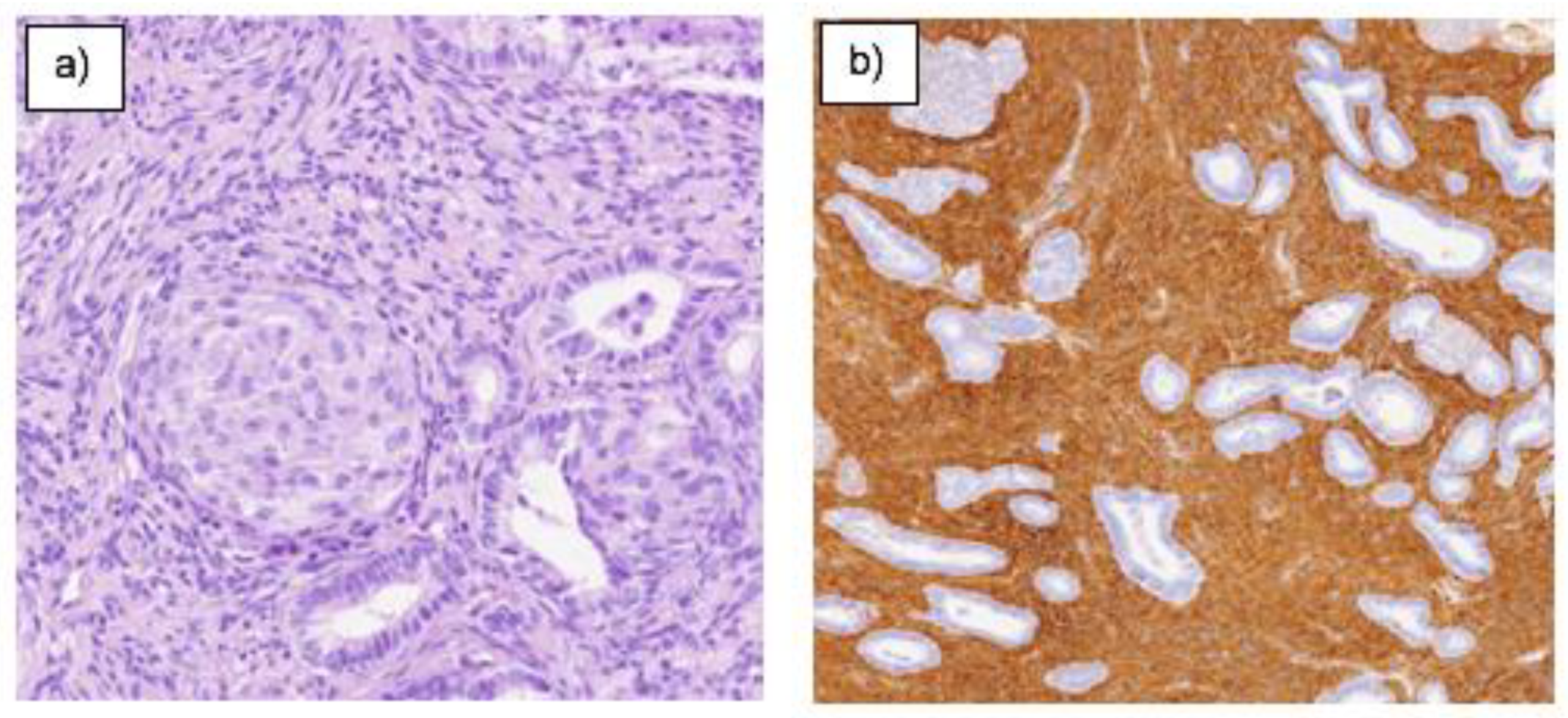
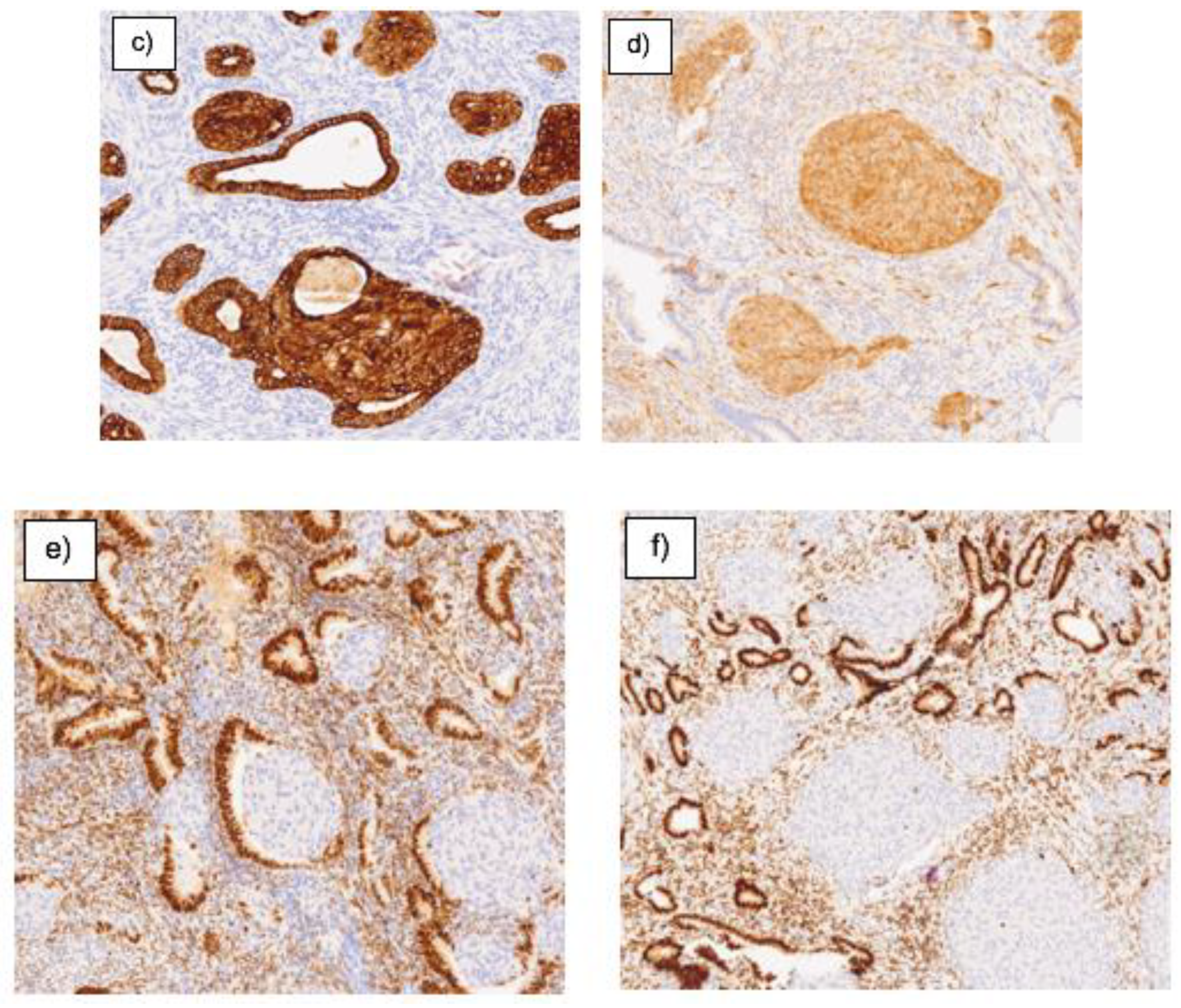
Several fragments were received, measuring 2.1x1.3cm and two fragments measuring 0.6x03cm, with total inclusion of both, corresponding to a myoma and a polyp, respectively. Histologically, a biphasic tumor composed of endometrioid glands, generally with complex architecture and sometimes cytological atypia, is observed. The glandular component often shows a lobulated architecture, benign fibromyomatous stroma, with myxoid change and morular squamous metaplasia. Margin not evaluable due to the type of resection performed. The sample shows a proliferative endometrial appearance, and IHC study reveals the following results: nuclear positivity for b-catenin, pancytokeratin, positive ER and PR in glands, positive SMA and desmin in stromal muscle, and positive P16 in squamous morules.
Figure 2.
a) Morular, stromal, and glandular area observed. H-E 22.50x b) Positive immunostaining of the stroma highlighted. Actin 7.90x. c) Positivity for glandular lining cells and complete staining of the morula. Keratin AE1-AE3 11.85x d) Positive immunoexpression exclusively in morules. P16 11.85x. e) Positive in glandular epithelium and intense, weak, or absent stroma in morules. ER 11.85x f) Positive immunostaining in glandular epithelium, sparse in stroma and absent in morules. PR 7.90x.
Figure 2.
a) Morular, stromal, and glandular area observed. H-E 22.50x b) Positive immunostaining of the stroma highlighted. Actin 7.90x. c) Positivity for glandular lining cells and complete staining of the morula. Keratin AE1-AE3 11.85x d) Positive immunoexpression exclusively in morules. P16 11.85x. e) Positive in glandular epithelium and intense, weak, or absent stroma in morules. ER 11.85x f) Positive immunostaining in glandular epithelium, sparse in stroma and absent in morules. PR 7.90x.
4. DISCUSSION
Key aspects of the expression of various immunohistochemical and molecular markers are addressed based on the area of the tissue studied, highlighting their diagnostic importance and therapeutic potential.
We observed consistent positive expression of β-catenin. This pattern reaffirms its utility as a biomarker in glandular tissue, supporting its role in tumour progression. Similarly, markers such as Ki 67, estrogen and progesterone receptors, and pancytokeratin have also shown uniformity in their positive results across multiple studies, reinforcing their reliability and relevance in specific clinical contexts.
Stromal IHC reveals that markers such as vimentin and desmin exhibit strong and consistent positivity, suggesting their value in identifying specific characteristics of stromal tissue. However, the limited research on other biomarkers such as H-caldesmon and vimentin in the literature points to an opportunity for additional studies that could explore their role in other pathological conditions.
Regarding the differential diagnosis between APA and CE (Table 4), both lesions exhibit positive expression for β-catenin, ER, PR, and pancytokeratin, suggesting similarities in underlying cellular pathways. In both endometrioid carcinoma and atypical polypoid adenomyoma, altered expression of β-catenin plays a role in pathogenesis and may serve as a marker for diagnosis and evaluation of malignant potential. However, mutation patterns and expression dynamics may vary, reflecting differences in the underlying biology of these lesions. It is suggested that abnormalities in the β-catenin gene (CTNNB1) activate certain signalling pathways within the cells. This activation is likely a consequence of genetic mutations and plays a crucial role in how epithelial cells are organised and behave. As for the difference in the p16 marker, in APA this positive expression could be related to atypical cellular changes, with partially active cell cycle regulation, in contrast to CE, where negative expression reflects a more advanced state of cell cycle deregulation and malignancy. Research has shown greater stromal p16 reactivity in APAM compared to myoinvasive endometrioid carcinoma. Pancytokeratin in both cases indicates the epithelial nature of the lesions. H-caldesmon in CE could be involved in tumour progression through its impact on cell mobility, and changes in expression may affect the cells' ability to invade adjacent tissues and spread to distant areas. It is not expressed in normal endometrial stroma or endometrial stromal neoplasms, making it useful as a specific and sensitive marker in the context of uterine mesenchymal tumours. CD10 is a stromal marker and is naturally expressed in normal endometrial stroma, as observed in CE, while in APA the expression is absent or weakly positive.
Other studies have analysed the utility of this marker's IHC for the diagnosis of APA versus CE. In their cohort of seven APA lesions, only one showed weak focal stromal staining among the glands, unlike the 19 myoinvasive carcinomas with clear positivity. Although the study identifies potential markers for differentiating adenomyoma and adenocarcinoma, additional studies with larger samples are necessary to validate these findings.
5. CONCLUSION
Research on atypical polypoid adenomyoma addresses an important diagnostic distinction from endometrioid carcinoma, based on differentiation through immunohistochemical and molecular markers. This differentiation is crucial as APA, being mostly a benign lesion, allows for conservative clinical management in selected cases, unlike CE which requires more radical treatments.
In the differential diagnosis between atypical polypoid adenomyoma and endometrioid carcinoma, the presence of common expression patterns of various biomarkers suggests similarities in their underlying cellular pathways. However, differences in expression dynamics and genetic mutations, especially in genes such as CTNNB1, underscore the distinctions in the biology of these lesions. Additionally, variability in the expression of markers such as p16 and h-caldesmon between APA and CE reflects their differentiated roles in cell cycle regulation and tumour progression.
In the analysis of the obtained data, our results show significant concordance with previously reported findings in the literature. We identified the mutation in the CTNNB1 gene [c.94G>A, p.(Asp32Tyr)], which presented an allele frequency of 11%. This finding reinforces the trends observed in similar studies. Additionally, no rearrangements were observed in the analysed regions, which is in line with expectations based on the pathology under study.
The molecular characterisation of the submitted sample with the Action OncoKitDx panel detected the presence of a point mutation in the CTNNB1 gene [c.94G>A, p.(Asp32Tyr)].
The CTNNB1 gene encodes the transcription factor β-catenin, which is involved in the Wnt signalling pathway and plays an important role in cell adhesion and migration processes. Mutations in the CTNNB1 gene have an oncogenic effect and have been described in various solid tumours, including gynaecological neoplasms. Therapeutic blocking of the Wnt pathway has been considered for the treatment of various tumours, and evidence suggests that tumours with CTNNB1 gene mutations would require direct pharmacological inhibition of β-catenin as they would show resistance to treatments targeting components acting at higher levels of the signalling pathway.
Regarding the microsatellite analysis, the analysed sample shows an absence of microsatellite instability. This result should be considered in the patient's clinical context. Considering immunotherapy-based treatment, evidence points to a relationship between the presence of high microsatellite instability and the response to immune system PD-1/PD-L1 checkpoint inhibitors.
Regarding pharmacogenetic analysis, the c.665C>T variant in the MTHFR gene (rs1801133) was detected, a polymorphism associated with the response to methotrexate treatment. Cancer patients with the heterozygous GA genotype treated with methotrexate may have a higher risk of toxicity than patients with the GG genotype and a lower risk of toxicity than patients with the AA genotype. In interpreting pharmacogenetic study findings, it cannot be ruled out that other genetic and clinical factors may also influence the response to indicated drugs.
The study provides a solid foundation for the use of these biomarkers in clinical diagnosis and suggests areas for future research that could improve our understanding and treatment of these pathological conditions. Additional studies with larger samples are recommended to validate these preliminary findings and potentially discover new diagnostic and therapeutic markers.
Funding
This research received no external funding.
Institutional Review Board Statement
this study did not require ethical approval.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Conflicts of Interest
The authors of this article declare no conflicts of interest. This research was conducted without support from any entity that could benefit directly from the results obtained.
References
- Kurman RJ, World Health Organization. WHO classification of tumours of female reproductive organs: [this book reflects the views of a working group that convened for a consensus and editorial meeting at the International Agency for Research on Cancer, Lyon, 13-15 June 2013]. Lyon: Internat. Agency For Research On Cancer; 2014.
- Mazur MT. Atypical polypoid adenomyomas of the endometrium. The American Journal of Surgical Pathology. 1981 Jul;5(5):473–82. [CrossRef]
- Heatley MK. Atypical polypoid adenomyoma: a systematic review of the English literature. Histopathology. 2006 Apr;48(5):609–10. [CrossRef]
- Němejcová K, Kenny SL, Laco J, Škapa P, Staněk L, Zikán M, et al. Atypical Polypoid Adenomyoma of the Uterus. American Journal of Surgical Pathology. 2015 Aug;39(8):1148–55. [CrossRef]
- Sun Y, Tian L, Liu G. A clinicopathological review of 203 cases of atypical polypoid adenomyoma of the uterus. J Clin Med. 2023;12(4):1511. [CrossRef]
- Kihara A, Amano Y, Yoshimoto T, Matsubara D, Fukushima N, Fujiwara H, et al. Stromal p16 Expression Helps Distinguish Atypical Polypoid Adenomyoma From Myoinvasive Endometrioid Carcinoma of the Uterus. The American Journal of Surgical Pathology. 2019 Nov 1;43(11):1526–35. [CrossRef]
- McCluggage WG. A practical approach to the diagnosis of mixed epithelial and mesenchymal tumours of the uterus. Modern Pathology. 2015 Dec 30;29(S1)–91. [CrossRef]
- Worrell HI, Sciallis AP, Skala SL. Patterns of SATB2 and p16 reactivity aid in the distinction of atypical polypoid adenomyoma from myoinvasive endometrioid carcinoma and benign adenomyomatous polyp on endometrial sampling. Histopathology [Internet]. 2021 Jul 1 [cited 2023 Dec 14];79(1):96–105. Available from: https://pubmed.ncbi.nlm.nih.gov/33459390/. [CrossRef]
- Solima E, Liprandi V, Belloni GM, Vignali M, Busacca M. Recurrent atypical polypoid adenomyoma and pregnancy: A new conservative approach with levonorgestrel-releasing intrauterine system. Gynecologic Oncology Reports [Internet]. 2017 Aug 1 [cited 2024 Apr 4];21:84–5. Available from: https://pubmed.ncbi.nlm.nih.gov/28761925/. [CrossRef]
- ONCOSEGO. Oncoguía cáncer de endometrio (2023) [Internet]. ONCOSEGO. [cited 2024 Apr 4]. Available from: https://oncosego.sego.es/oncoguia-cancer-de-endometrio-2023.
- Rizzuto I, Nicholson R, Dickinson K, Juang HJ, MacNab W, B. Rufford. A case of incidental endometrial adenocarcinoma diagnosed in early pregnancy and managed conservatively. Gynecologic Oncology Reports [Internet]. 2019 May 1 [cited 2023 Dec 15];28:101–3. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6449706/. [CrossRef]
- Masciullo V, Susini T, Corrado G, Stepanova M, Baroni A, Renda I, et al. Nuclear Expression of β-Catenin Is Associated with Improved Outcomes in Endometrial Cancer. Diagnostics (Basel, Switzerland) [Internet]. 2022 Oct 3 [cited 2024 Jan 10];12(10):2401. Available from: https://pubmed.ncbi.nlm.nih.gov/36292090/. [CrossRef]
- Zhao R, Choi BY, Lee M-H, Bode AM, Dong Z. Implications of genetic and epigenetic alterations of CDKN2A (p16 INK4a ) in cancer. EBioMedicine [Internet]. 2016 [cited 2024 Jan 10];8:30–9. Available from: https://pubmed.ncbi.nlm.nih.gov/27428416/. [CrossRef]
- McIntosh GG, Lodge AJ, Watson P, Hall AG, Wood K, Anderson JJ, et al. NCL-CD10–270: A new monoclonal antibody recognizing CD10 in paraffin-embedded tissue. Am J Pathol [Internet]. 1999;154(1):77–82. Available from: http://dx.doi.org/10.1016/s0002-9440(10)65253-4. [CrossRef]
- Zhao W, Cui M, Zhang R, Shen X, Xiong X, Ji X, et al. IFITM1, CD10, SMA, and h-caldesmon as a helpful combination in differential diagnosis between endometrial stromal tumor and cellular leiomyoma. BMC Cancer [Internet]. 2021 Sep 23 [cited 2024 Jan 10];21(1):1047. Available from: https://pubmed.ncbi.nlm.nih.gov/34556086/. [CrossRef]
- IMEGEN [Internet]. Imegen. 2022 Available from: http://www.imegen.es/datagenomics.
- Martínez-Fernández P, Pose P, Dolz-Gaitón R, García A, Trigo-Sánchez I, Rodríguez-Zarco E, et al. Comprehensive NGS Panel Validation for the Identification of Actionable Alterations in Adult Solid Tumors. Journal of Personalized Medicine. 2021 Apr 29;11(5):360. [CrossRef]
- Human Genome Variation Society. [Internet]. [cited 2024 May 10]. Available from: https://www.hgvs.org.
- Garraway LA. Genomics-Driven Oncology: Framework for an Emerging Paradigm. Journal of Clinical Oncology. 2013 May 20;31(15):1806–14. [CrossRef]
- Mosele F, Remon J, Mateo J, Westphalen CB, Barlesi F, Lolkema MP, et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann Oncol [Internet]. 2020 [cited 2024 May 15];31(11):1491–505. Available from: https://pubmed.ncbi.nlm.nih.gov/32853681/. [CrossRef]
- Takahashi H, Yoshida T, Matsumoto T, Kameda Y, Takano Y, Tazo Y, et al. Frequent β-catenin gene mutations in atypical polypoid adenomyoma of the uterus. Human Pathology [Internet]. 2014 Jan 1 [cited 2024 Jan 10];45(1):33–40. Available from: https://pubmed.ncbi.nlm.nih.gov/24182564/. [CrossRef]
- Ota S, Catasus L, Matias-Guiu X, Bussaglia E, Lagarda H, Pons C, et al. Molecular pathology of atypical polypoid adenomyoma of the uterus. Human Pathology. 2003 Aug;34(8):784–8. [CrossRef]
- Yao YB, Xiao CF, Lu JG, Wang C. Caldesmon: Biochemical and Clinical Implications in Cancer. Frontiers in Cell and Developmental Biology. 2021 Feb 18;9. [CrossRef]
- Buza N, Hui P. Immunohistochemistry in Gynecologic Pathology: An Example-Based Practical Update. Archives of Pathology & Laboratory Medicine. 2017 Aug 1;141(8):1052–71. [CrossRef]
- Ohishi Y, Kaku T, Kobayashi H, Aishima S, Umekita Y, Wake N, et al. CD10 immunostaining distinguishes atypical polypoid adenomyofibroma (atypical polypoid adenomyoma) from endometrial carcinoma invading the myometrium. Human Pathology [Internet]. 2008 Oct 1 [cited 2024 Apr 5];39(10):1446–53. Available from: https://pubmed.ncbi.nlm.nih.gov/18619643/. [CrossRef]
- Lu B, Yu M, Shi H, Chen Q. Atypical polypoid adenomyoma of the uterus: A reappraisal of the clinicopathological and immunohistochemical features. Pathology - Research and Practice. 2019 Apr;215(4):766–71. [CrossRef]
- Terada T. Atypical polypoid adenomyoma of the uterus: an immunohistochemical study on 5 cases. Annals of Diagnostic Pathology. 2011 Oct;15(5):338–41. [CrossRef]
- Gao C, Wang Y, Broaddus R, Sun L, Xue F, Zhang W. Exon 3 mutations of CTNNB1 drive tumorigenesis: a review. Oncotarget [Internet]. 2017 Dec 27 [cited 2024 Apr 23];9(4). Available from: https://doi.org/10.18632/oncotarget.23695. [CrossRef]
- Nguyen VHL, Hough R, Bernaudo S, Peng C. Wnt/β-catenin signalling in ovarian cancer: Insights into its hyperactivation and function in tumorigenesis. Journal of Ovarian Research. 2019 Dec;12(1). [CrossRef]
- Katoh M, Katoh M. Molecular genetics and targeted therapy of WNT-related human diseases (Review). International Journal of Molecular Medicine. 2017 Jul 19;
- Yu F, Yu C, Li F, Zuo Y, Wang Y, Yao L, et al. Wnt/β-catenin signaling in cancers and targeted therapies. Signal Transduction and Targeted Therapy. 2021 Aug 30;6(1). [CrossRef]
- Moroney MR, Woodruff E, Qamar L, Bradford AP, Wolsky R, Bitler BG, et al. Inhibiting Wnt/beta-catenin in CTNNB1 -mutated endometrial cancer. Molecular Carcinogenesis. 2021 May 26;60(8):511–23.
- Chakraborty E, Sarkar D. Emerging Therapies for Hepatocellular Carcinoma (HCC). Cancers [Internet]. 2022 Jun 4;14(11):2798. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9179883/. [CrossRef]
- Le DT, Durham JN, Smith KN, Wang H, Bartlett BR, Aulakh LK, et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science. 2017 Jun 8;357(6349):409–13. [CrossRef]
- Bonneville R, Krook MA, Kautto EA, Miya J, Wing MR, Chen HZ, et al. Landscape of Microsatellite Instability Across 39 Cancer Types. JCO precision oncology [Internet]. 2017;2017. Available from: https://pubmed.ncbi.nlm.nih.gov/29850653/. [CrossRef]
- Yan L, Zhang W. Precision medicine becomes reality—tumor type-agnostic therapy. Cancer Communications. 2018 Mar 31;38(1).
- Luchini C, Bibeau F, Ligtenberg MJL, Singh N, Nottegar A, Bosse T, et al. ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: a systematic review-based approach. Annals of Oncology. 2019 Aug;30(8):1232–43.
- PharmGKB [Internet]. PharmGKB. 2019. Available from: https://www.pharmgkb.org/.
Figure 1.
Analysis of copy number variations across the genome, reflecting gains and losses, in red and blue, respectively, of large chromosomal regions.
Figure 1.
Analysis of copy number variations across the genome, reflecting gains and losses, in red and blue, respectively, of large chromosomal regions.
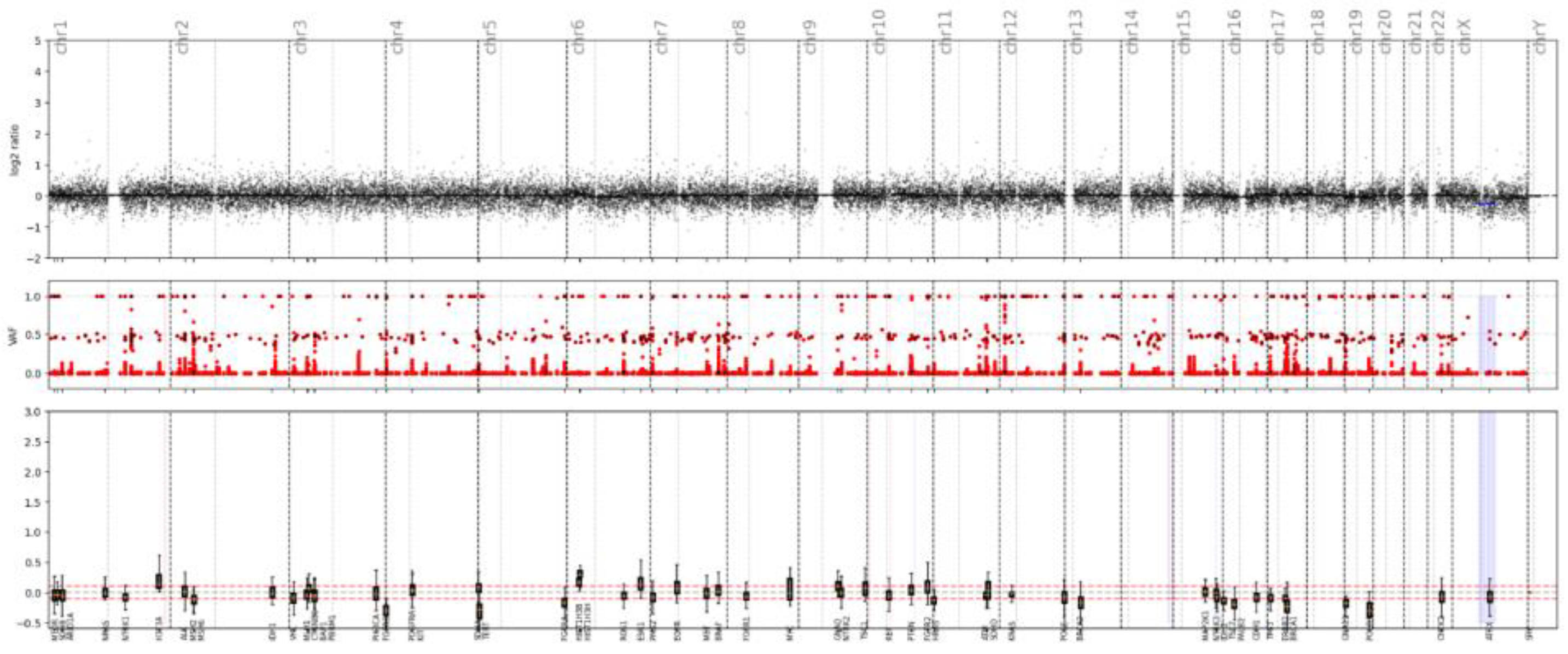
Table 3.
Molecular study of APA.
| MOLECULAR STUDY | |||||||
|---|---|---|---|---|---|---|---|
| No. | PMS2 | MSH6 | P53 | MLH1 | CTNNB1 | P16 | |
| OWN CASE | 1 | + | + | ||||
| NEMEJCOVA | 21 | 2+ | 2+ | N | 3+ | ||
| YUE | 99 | 3+ | 3+ | 2+ | + | 3+ | |
| TAKASHI | 7 | ||||||
| OTA | 6 | N | 3+ | - | |||
| LU | 36 | N | |||||
| WORREL | 32 | 3+ | |||||
| KIHARA | 12 | 2+ | 3+ | ||||
Table 4.
Differential diagnosis between APA and EC.
| MARKERS | Atypical Polypoid Adenomyoma | Endometrial Adenocarcinoma |
|---|---|---|
| B-catenina | + | + |
| P16 | + | - |
| RE | + | + |
| PR | + | + |
| Pancitoqueratina | + | + |
| CD10 | - | + |
| Caldesmon | - | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



