
Submitted:
15 July 2024
Posted:
16 July 2024
You are already at the latest version
Abstract
Purpose: To evaluate prognostic factors for visual outcome in patients with diabetes who have undergone vitrectomy (PPV) for severe proliferative diabetic vitreo-retinopathy (PDVR) in at least one eye in the past 15 years. Methods: Medical records of 132 eyes of 66 patients were analyzed (median age 52ys 21-80; patients with type 1/2 diabetes 40/26, median follow-up 38 months 9-125). Correlation between final good visual outcome defined as 0.5≤ best corrected visual acuity (BCVA) and prognostic factors (age, sex, type and duration of diabetes, metabolic status, BCVA, diabetic retinopathy status, data of preoperative management, data of vitrectomy, postoperative complications) were analyzed. Results: BCVA improved significantly in the entire study cohort (from median 0.05 min-max 0.001-1 to 0.32 0.001-1, p <0.000). Visual stabilization was achieved in the majority of patients, and relatively good visual acuity (0.5≤BCVA) was maintained in more than one third of eyes. Multivariable GEE statistics showed that in addition to duration of diabetes and stable HbA1c values, only preoperative tractional macular detachment proved to be an independent significant predictor of visual outcome. Conclusions: Pars plana vitrectomy is a useful tool when performed early before tractional macular detachment. However, long-term visual stability can only be achieved with good metabolic control.
Keywords:
proliferative diabetic retinopathy
; pars plana vitrectomy
; HbA1c
; visual acuity
; tractional macular detachment
1. Introduction
Diabetic retinopathy (DR) continues to be a leading cause of blindness among working-age adults in developed countries, despite advances in screening techniques and treatment options. It is estimated to affect around 90 million of the 463 million people living with diabetes mellitus worldwide [1]. The most important sight threatening complication is proliferative retinopathy (PDR), which will develop in approximately 50% of Type 1 and 25% of Type 2 patients after 20 years of duration, according to the Wisconsin Epidemiological Study [2].
Effective treatment options include panretinal laser photocoagulation (PRP), intravitreal anti-vascular endothelial growth factor (anti-VEGF) therapy and pars plana vitrectomy (PPV).
While PRP has been the traditional method for preventing severe vision loss for many years, and anti-VEGF injections have been shown to be an effective option for patients with PDR, it is important to note that both treatments can be associated with significant treatment burden and may require multiple retreatments. The Early Treatment of Diabetic Retinopathy Study (ETDRS) demonstrated that PRP can reduce the incidence of severe visual impairment by 50%. However, in 15% of PDR cases, vitrectomy may be required due to non-resolving vitreous hemorrhage, tractional retinal detachment, or combined tractional and rhegmatogenous retinal detachment [3,4]. Additionally, it is important to note that 33% of eyes treated with anti-VEGF and lost to follow-up may develop tractional retinal detachment. [3,4].
Since Robert Machemer performed the first PPV in a patient with PDR in 1973 to treat non-clearing vitreous hemorrhage, vitrectomy has undergone significant development and modernization, resulting in a broadening of the indications for vitrectomy and improved outcomes. Vitrectomy in patients with diabetes is usually performed in cases of tractional retinal detachment (TRD) involving the posterior pole and non-clearing vitreous hemorrhage. Positive outcomes have also been observed in instances of progressive fibrovascular proliferation, ghost cell glaucoma, and diabetic macular edema (DME) resulting from traction [2,3]. The outcomes of vitreous surgery have been significantly improved due to various advancements in the field. These include the introduction of wide-angle visualization, small-diameter instruments with high cutting speeds and precise pressure control, the use of anti-VEGF drugs, and the ability to perform endolaser coagulation. The benefits of early vitrectomy, especially in younger patients with an attached posterior hyaloid, include preserved vision, reduced treatment burden, and fewer subsequent treatments. [3,4,5]. However, the role of pars plana vitrectomy (PPV) in the treatment algorithm for proliferative diabetic retinopathy (PDR) is still controversial. Clinical management and visual outcomes could be enhanced by a better understanding of the real-world long-term outcomes of vitrectomy for PDR. Enhanced BCVA outcomes can lead to an improved quality of life for patients with advanced diabetic complications who may be at risk of losing their ability to work and live independently.
The aim of the study was to analyze factors that may influence the maintenance of good visual acuity. The patients in this study underwent vitrectomy for severe proliferative diabetic retinopathy in one eye within 2-4 weeks of their first visit to our tertiary care center.
The fellow eye underwent vitrectomy or was spared surgery with a personalized treatment plan including panretinal laser coagulation or intravitreal anti-VEGF injections, depending on its condition.
2. Materials and Methods
2.1. Standard Protocols, Approval, Data Availability
The patients involved in our retrospective study underwent pars plana vitrectomy for complications associated with PDR at least once in one eye while being examined and treated at the Department of Ophthalmology, Semmelweis University, Budapest, Hungary between 2008-2022. The data was extracted from the Medsol system. The study was approved by the Institutional Ethics Review Board at Semmelweis University (SE RKEB 59/2023) and was carried out in accordance with the Principles of the Helsinki Declaration. The datasets are planed to be deposited in the Dryad database.
2.2. Patients’ Clinical Data Analysis
Inclusion criteria were the following: (1) Type 1 or Type 2 diabetic patients who underwent vitrectomy in at least one eye for severe PDR (2) at least 6-months follow-up period after the last surgery, (3) information on metabolic control (at least data at first and last visit), ophthalmological status, details of surgery and other ophthalmological interventions in both eyes throughout follow-up.
The main outcome measure was final best-corrected visual acuity at the end of follow-up.
The following data were collected: Baseline systemic parameters included: age, sex, type and duration of DM, hemoglobin A1c (HbA1c) level, hypertension, renal and cardiovascular complications. Regarding the glycemic control, HbA1c levels were collected from the time at first vitrectomy, and from the time of the last visits. In addition, mean HbA1c was also calculated from the data available during the entire follow-up period. Patients with a GFR less than 30 mL/min/1.73 m2 or who were under nephrological care or receiving hemodialysis were counted as patients with renal insufficiency. We also collected information on other serious systemic diseases such as uncontrolled hypertension, stroke and cardiovascular (CV) complications, the latter including a history of acute ischemic heart disease or heart failure.
Baseline, intra- and postoperative ocular parameters included the first BCVA (when the patient first attended our department), preoperative and final BCVA (measured on the ETDRS chart), status of DR (posterior hyaloid detachment, PVD; vitreous hemorrhage; tractional retinal detachment, TRD; macular tractional detachment, MRD rubeosis), pre-/postoperative panretinal photocoagulation (PRP), pre- and postoperative anti-VEGF injections, epiretinal membranes, surgical techniques, intra- and postoperative complications, need for postoperative antiglaucoma treatment or cataract surgery. Depending on media opacity, ultrasonography and optical coherence tomography were used to assess posterior segment status. Macular morphology was examined using spectral domain optical coherence tomography (OCT). The macular structure was scanned using the radial line software algorithm (RTVue-XR Avanti, Optovue, Fremont, CA, USA). Fluorescein angiography was performed to detect peripheral ischemia and any proliferative foci.
2.3. Management
All first eyes and some fellow eyes underwent vitrectomy. Indications for vitrectomy were: recurrent or non-resolving vitreous hemorrhage and/or tractional retinal detachment, tractional macular edema, detachment. When a patient was first seen with severe bilateral PDR requiring surgery, the eye with the better visual prognosis was selected for vitrectomy. The 23-gauge 3-port pars plana vitrectomy was performed under regional or general anesthesia by two experienced vitreoretinal surgeons (RZ, EM). In cases of progressive lens opacities or anterior proliferative vitreoretinopathy, surgery was combined with phacoemulsification and posterior lens implantation. Triamcinolone acetate (TCA) was used to stain the vitreous and facilitate removal of the posterior hyaloid. Membranectomy or membrane peeling was performed using a bimanual technique under a chandelier light source.
Panretinal laser coagulation was added. Silicon oil (1300cst, SiO) or octafluoropropane (C3F8) was used as endotamponade. In our cohort, preoperative anti-VEGF injections were used to treat central macular edema or as adjuvant therapy 3-5 days before PPV in cases of florid proliferation to prevent intraoperative bleeding. After surgery, uncomplicated cases received a combination of mydriatic, steroid, and non-steroid anti-inflammatory eye drops 3 times daily for 2 weeks.
Treatment of the fellow eye was determined based on the stage of PDR and individualized treatment was applied. Central macular edema was treated with anti-VEGF intravitreal injection five times in monthly period, followed by pro renata protocol. Intravitreal steroid implantation was also considered, especially in cases of persistent intraretinal fluid. In these cases, panretinal laser treatment was also recommended to the patients if extensive peripheral ischaemia was detected on fluorescein angiography. In cases of severe nonproliferative or mild proliferative retinopathy, panretinal laser coagulation according to ETDRS protocol was the first choice of treatment. Anti-VEGF intravitreal injection was also used as adjuvant treatment in florid cases and cases with central macular eodema.
The normalization of the patients’ metabolic parameters and the ophthalmic treatment occurred in parallel. Surgeons have not waited for CH metabolism to normalize because it has been observed that it can take several months while retinopathy progresses rapidly. At the same time, it was considered important to maintain blood pressure at target levels before vitrectomy.
2.4. Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics 25 (SPSS Inc., Chicago, IL, USA). Non-parametric tests were used as the Saphiro-Wilk’s test confirmed non-normal distribution of data. Main outcome measure was final visual acuity, and subanalysis was performed specifically for the group of eyes with good BCVA (0.5≤BCVA) The eyes of the patients were divided into three groups, (a) primary vitrectomized eyes, (b) fellow eyes that also underwent vitrectomy during follow-up, (c) non-vitrectomized fellow eyes.
Fisher’s exact test was used to compare categorical parameters. Comparisons were made using the Mann-Whitney U test for unpaired parameters and the Wilcoxon signed rank test for paired pre- and post-operative parameters.
To detect any correlation between parameters and final BCVA, the non-parametric Spearman’s bivariate test was utilized. The effect of predisposing factors on final BCVA was assessed through multivariable analysis using the general estimating equation (GEE) model. This test takes into account the within-subject correlation of parameters (right vs. left eye) by considering inter-eye correlations and between-visit correlation of parameters as repeated measurements.
In addition, the inclusion of both ocular and non-ocular risk factors as covariates in general estimating equation models allows simultaneous control for their effect on the dependent variables. Covariates assessed as potential confounding factors, based on a priori hypotheses, included age, duration of diabetes, HbA1c level, hypertension, and retinopathy status. (tractional macular detachment, tractional retinal detachment elsewhere, preoperative glaucoma, rubeosis, best corrected visual acuity at first visit)
3. Results
3.1. Patients Characteristics
Medical records of 73 consecutive patients with PDR were analyzed, seven patients were excluded due to lack of regular HgbA1c data.
All of the patients were referred to us due severe proliferative retinopathy requiring vitrectomy in at least one eye. The data analyzed included 66 first vitrectomized eyes, 31 fellow eyes that also underwent vitrectomy during follow-up, and 35 non-vitrectomized fellow eyes.
At the first visit, patients with type 1 diabetes were found to be significantly younger, had a longer duration of diabetes, and higher HgbA1c levels compared to patients with type 2 diabetes. There were no discernible differences in other systemic parameters, such as sex, renal insufficiency, severe cardiovascular complications, or unstable blood pressure, between the two types of diabetes. Furthermore, we did not observe any significant differences in preoperative ophthalmological status between these groups. The baseline characteristics of our patients are summarized in Table 1.
3.2. Surgery
A total of 157 vitrectomies were performed in our study population, in 97 eyes of 66 patients (97/132 eyes, 73%) (median value, min-max 1; 1-4). Of the whole cohort, 54 eyes (55.67%) underwent only one vitrectomy, while 43 eyes (44.33%) required multiple vitrectomies. Silicone oil was applied in 58 eyes, and silicone oil explantation was also counted as an additional surgery. Combined phacoemulsification-vitrectomy was performed in 30 eyes (30/97 vitrectomized eyes, 31%). Posterior hyaloid detachment was confirmed during the surgery in 29 eyes (29/97 vitrectomized eyes, 30%), mainly in Type 1 diabetic patients (20 versus 9 eyes in type 1 or type 2 diabetics, respectively; Fisher’s test, p value= 0.1). The first eye underwent vitrectomy within a month after first attendance. 31 patients (47%, 31/66 patients, type 1 diabetes: 17; type 2 diabetes: 14) required surgery on both eyes. The median interval between the first and second eye surgeries was 2 months (min-max: 1-33). 15 eyes (48%, 15/31 patients) underwent surgery within 3 months.
Severe intraoperative complications occurred in four eyes with tractional retinal detachment. During membrane peeling, retinal tears developed in 3 legally blind eyes, resulting in rhegmato-tractional retinal detachment and blindness. The fourth patient was on monoclonal antibody anticoagulation for atrial fibrillation, which was discontinued 24 hours before surgery. During the otherwise uneventful surgery, an extensive subchorioidal hemorrhage involving the posterior pole developed resulting in legal blidndness.
Postoperative complications: In the early postoperative period, bleeding into the vitreous cavity was the most common complication (38 eyes), which resolved in all cases within 1-3 months. At the end of the follow-up, combined antiglaucoma eye drop therapy was required for 39 eyes (39/132, 29%). Out of these patients, 10 eyes developed refractory glaucoma developed, 2 eyes underwent shunt implantation, and the others underwent cyclophotocoagulation.
At the end of follow-up, active neovascularisation was found on the iris in 10 eyes and on the disc or elsewhere on the retina in 5 eyes (15/132 eyes 11%). Tractional retinal detachment was described in 9 eyes, among them all but one eye became blind or legally blind. Foveal center-involved persistent intraretinal fluid was observed in 12 eyes despite treatment with anti-VEGF intravitreal injection and intravitreal steroid implant.
Changes in ophthalmological parameters in the 3 study groups are summarized in Table 2.
3.3. Functional Results
Best corrected visual acuity improved significantly in the entire study cohort (from median 0.05 min-max 0.001-1 to 0.32 0.001-1, p <0.000). However, when analyzing the three study groups, only the first vitrectomized group showed a significant improvement (from median 0.04 min-max 0.01-1 to 0.2 0.001-1, p <0.000). In the group of vitrectomized fellow eyes and non-vitrectomized fellow eyes the observed changes were not significant (Figure 1) Good final BCVA was maintained in 53 eyes (53/132, 40%). At first attendance, 88 eyes (66%, 88/132) were legally blind, BCVA improved to equal or better than 0.5 in 22 eyes (22/88, 25%). 52 eyes (52/88, 59%) remained legally blind. Changes in BCVA in the three study groups are summarized in Figure 1.
Of the 97 vitrectomized eyes, 83 eyes (85%, 85/97) were legally blind at the first visit. Good final BCVA was achieved in 30 eyes (30%, 30/97; out of them 21 were legally blind). At the final visit, 43% (43/97) of the eyes were legally blind.
In the group of first vitrectomized eyes (66 eyes of 66 patients), the majority were legally blind at baseline (64 eyes, 64/66, 96%). Of those, 18 eyes (28%,18/64) had BCVA≥0.5 and 26 eyes (26/64, 40%) remained legally blind after surgery
In the group of fellow eyes that underwent vitrectomy (31 eyes),. Out of the 19 legally blind eyes (61%, 19/31), only three eyes had a final good BCVA. Good BCVA was maintained in 11 eyes (35%,11/31)
Out of the 35 non-vitrectomized fellow eyes, three were kept for observation as we believed that intervention would not be beneficial. Two of these eyes had extensive tractional retinal detachment and were nearly blind, while the third had a burned-out TRD nasal to the disc and a BCVA of 1.0. The remaining 32 eyes were treated with panretinal laser, anti-VEGF injections, or steroid implants.
3.4. Factors Affecting final BCVA
The results of the univariate statistical analysis indicate that several general and ophthalmological factors may have a significant impact on good visual acuity at the end of follow-up. These factors are summarized in Table 3. However, abnormal preoperative HbA1c levels were associated with a higher incidence of tractional retinal detachment (p=0.059), and a higher mean HbA1c level was linked to an increased risk of developing rubeosis (p=0.014).
Multivariable analysis was performed to determine which factors had the most significant and independent effect on visual outcome, as multiple interactions between these factors were expected.
In eyes with a good final visual acuity (BCVA≥0.5), several factors were found to be significant predictors according to multivariate analysis using the GEE method (quasi goodness of fit, 39,974). These factors are disease duration (p=0.022), mean HbA1c (p=0.002) and preoperative MRD (P=0.001).
4. Discussion
In the current study, which examined the long-term outcomes of patients who underwent vitrectomy for PDR or received personalized management over the past 15 years, our main findings were as follows: (a) PPV was found to be a viable option for improving visual function in patients with advanced PDR; (b) panretinal laser coagulation with the addition of intravitreal anti-VEGF injection is a well-established treatment for severe non-proliferative retinopathy and proliferative retinopathy without tractional detachment; (c) among the ophthalmological data, it was observed that preoperative macular tractional detachment was the main predictor of the final visual outcome; (d) from the general conditions, the duration of the disease and the average Hba1c level had the most important influence on the final visual acuity. The majority of our patients achieved visual stabilization, with over half of them having relatively good visual acuity (0.5≤BCVA) in one eye. However, it is worth noting that two-thirds of the eyes that were legally blind at the beginning remained legally blind.
These findings are consistent with those reported in previous studies based on real-world experience. Early PPV can prevent the development of tractional retinal detachment, stabilize the fundus long-term, and reduce the number of complications and medical costs. Nowadays, early surgery is more and more preferred because better postoperative visual acuity can be achieved if vitrectomy is performed in the pregliotic phase [17]. Berrocal et al. demonstrated the beneficial effects of early PPV both in terms of postoperative BCVA and the rate of subsequent treatments required, when compared to patients who received PRP or PPV, in a follow-up of 8 years. The only disadvantage was the faster progression of cataract in this group [18]. The DRCR.net protocol AB compared aflibercept and early vitrectomy with PRP in the treatment of PDR with VH. While no significant difference was reported in long-term VA outcomes over 24 weeks, early vitrectomy resulted in faster visual recovery and less recurrent vitreous hemorrhage [5,19].
Recently, Berrocal et al. suggested that the posterior hyaloid position may play a crucial role in determining the appropriate approach to vitrectomy. Previous studies have also highlighted the impact of the posterior hyaloid on the progression of PDR earlier. [15,16]. Younger patients, with attached or partially detached posterior hyaloid are more likely to progress to vitreous hemorrhage or TRD. Complete PVD in older patients may be a protective factor against the progression to PDR and TRD, as neovascular vessels can only grow on the surface of the retina in the absence of a vitreoretinal interface. Berrocal found in a retrospective real-world study that eyes with complete PVD can be treated with less aggressive PRP and anti-VEGF, but the more beneficial treatment for eyes with no- or partial PVD should be PPV with hyaloid removal and less confluent PRP [18]. However, the detection of posterior hyaloid attachment can be can be often a challenge in diabetic patients due to the frequent occurrence of vitreous schisis. In such cases, the posterior hyaloid is divided into multiple layers, and in our experience, its exact position can only be determined during surgery by injecting triamcinolone acetate into the vitreous cavity. At the time of surgery, attached hyaloids were found in the majority of our patients, and as one of its beneficial aspects, vitrectomy has been shown to eliminate the traction caused by posterior hyaloids, which may prevent or stop the formation of tractional retinal detachment. Our study cohort showed that tractional retinal detachment reaching the macula was a major negative predictive factor for poor final visual outcome. According to a recent meta-analysis by McCollough et al., patients with PDR and TRD have a high anatomic success rate of up to 90%, but despite this success, final postoperative visual acuity (VA) remains low, and the only significant factor for good visual outcome was good preoperative VA [48].
With adjuvant preoperative anti-VEGF injections, surgical safety can be further improved and the incidence of intra- and postoperative complications can be reduced: intraoperative bleeding occurs less frequently, the need for intraoperative endodiathermy decreases, and shorter surgery times, fewer iatrogenic retinal tears, fewer early postoperative recurrent VHs or its faster absorption can be achieved [20,21]. With the preoperative administration of intravitreal anti-VEGF injections, the surgical technique has also become simpler, e.g., the membranes become easier to peel off. Zhao et al. also reported better postoperative BCVA after PPVs supplemented with adjuvant anti-VEGF treatment [22]. In our patient cohort, this method was frequently used and found effective in preventing severe intraoperative bleeding and facilitating membrane peeling. However, in cases of preoperative adjuvant treatment, it is important to remember to perform panretinal laser treatment during and after surgery, since the anti-VEGF administered during pretreatment only provides adequate VEGF inhibition for four weeks and most of it is removed during vitrectomy. As observed in our current study, the utilization of this technique did not have a significant effect on the final BCVA, nor did reduce the risk of postoperative hemorrhage.
The most common postoperative complications in our study were rubeosis with secondary glaucoma, and vitreous hemorrhages (VH), which are in line with the literature. In the most severe cases, retinopathy progression to anterior segment neovascularization was in the background of glaucoma formation, where the IOP was not manageable with topical therapy and Ahmed shunt implantation was the only effective long-term solution. Some patients experienced a severe increase in IOP during the early postoperative period due to posterior synechiae and pupillary block. In these cases, Nd-YAG iridotomy was not always successful due to bleeding from the rubeotic iris tissue.
The development of VH, observed in 10.2% of our cohort, is not uncommon during the postoperative weeks and months, as other studies have reported an incidence of 4-45% in PDR patients [23,24]. Motoda et al. reported that the most important predictor of bleeding in the late postoperative period is the duration of the surgery [25]. In addition, fibrovascular proliferation in the sclerotomy wound is also mentioned as one of the possible causes of bleeding [26]. The use of gas tamponade, cryotherapy of the sclerotomy sites, preoperative anti-VEGF treatment and aggressive preoperative PRP treatment can significantly reduce the likelihood of postoperative VH [27]. In our experience, postoperative vitreous hemorrhage did not have a significant negative impact on final visual acuity as it usually resolved spontaneously or after anti-VEGF injection within three months after surgery. In cases where the hemorrhage persisted, we decided to perform another surgery to complete the panretinal laser coagulation and to prevent the formation of secondary rubeosis or ghost cell glaucoma.
Silicone oil is used in the most severe cases. In the long term, however, it has been linked to an increased risk of secondary glaucoma and neovascularization [27]. In our study cohort, we used SiO as an endotamponade when traction could not be completely removed, severe diffuse bleeding was observed during the surgery, or multiple retinal brakes were found in several location. The use of SiO was not an independent risk factor for surgical failure in our patient cohort, but if we could not remove it within six months, or even by the end of the follow-up, valuable visual acuity could not be achieved. In these cases or macular degenerative changes, or permanent retinal traction was observed at the end of the follow-up.
In terms of general health, mean Hba1C levels and their values at the end of the follow-up were the only significant predictors of long-term valuable visual acuity preservation.
In our experience, PPV can assist our patients in gaining time to control their diabetes, but their vision can only be preserved if their glycemic metabolism is stabilized in the long term. Although earlier surgery may be advantageous, the focus should be on identifying patients at high risk of developing MRD and preventing it.
Data from the randomized multicenter studies as well as findings of recent publications on real-life experience with PPV in PDR are summarized in Supplementary Table S1.
Strengths of this study include the long duration of follow-up, the relatively large sample size, and the collection of initial vitrectomy data at a single tertiary center, which reduces external sources of variability. In addition, we evaluated several possible confounding factors, such as metabolic status data, in addition to ophthalmological findings, providing a comprehensive assessment of the long-term outcomes of vitrectomy for PDR in real-world practice.
Limitations: A major limitation is the retrospective nature of the study, which did not allow standardization of measurements. Additionally, the heterogeneity of the study cohort and the multiple potential interactions between systemic and ophthalmological factors may complicate the interpretation of the results.
5. Conclusions
In conclusion, this study retrospectively analyzed patients who underwent vitrectomy for advanced PDR. Among the systemic parameters, the duration of diabetes and Hba1c level were significant predictors of visual outcome in our study cohort. In addition, our analysis of ophthalmological parameters revealed that macular tractional detachment had a significant negative effect on long-term visual preservation. Therefore, early vitrectomy can be considered as a useful tool to provide patients with the necessary time to achieve good metabolic control and maintain a high quality of life and working ability during their active years.
6. Patents
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Zs.R, M.E, D.Sz.; methodology, M.E, D.Sz.; software, Zs.Sz;.; investigation, D.Sz, Zs.Sz;.; data curation, Zs.R, D.Sz; writing—original draft preparation, M.E, D.Sz.; writing—review and editing, Zs.R;; supervision, Z.Zs.N; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Informed Consent Statement
The study was approved by the Institutional Ethics Review Board at Semmelweis University (SE RKEB 59/2023) and was carried out in accordance with the Principles of the Helsinki Declaration.
Data Availability Statement
The datasets are planned to be deposited in the Dryad database.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sun, H., et al., IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract, 2022. 183: p. 109119. [CrossRef]
- Klein, R., et al., The Wisconsin Epidemiologic Study of Diabetic Retinopathy: XXII the twenty-five-year progression of retinopathy in persons with type 1 diabetes. Ophthalmology, 2008. 115(11): p. 1859-68.
- Flynn, H.W., Jr., et al., Pars plana vitrectomy in the Early Treatment Diabetic Retinopathy Study. ETDRS report number 17. The Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology, 1992. 99(9): p. 1351-7. [CrossRef]
- Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. The Diabetic Retinopathy Study Research Group. Ophthalmology, 1981. 88(7): p. 583-600.
- Antoszyk, A.N., et al., Effect of Intravitreous Aflibercept vs Vitrectomy With Panretinal Photocoagulation on Visual Acuity in Patients With Vitreous Hemorrhage From Proliferative Diabetic Retinopathy: A Randomized Clinical Trial. Jama, 2020. 324(23): p. 2383-2395.
- Khan, R., et al., Need for Vitreous Surgeries in Proliferative Diabetic Retinopathy in 10-Year Follow-Up: India Retinal Disease Study Group Report No. 2. Ophthalmic Research, 2021. 64(3): p. 432-439. [CrossRef]
- Figueira, J., et al., Ranibizumab Plus Panretinal Photocoagulation versus Panretinal Photocoagulation Alone for High-Risk Proliferative Diabetic Retinopathy (PROTEUS Study). Ophthalmology, 2018. 125(5): p. 691-700. [CrossRef]
- Tonello, M., et al., Panretinal photocoagulation versus PRP plus intravitreal bevacizumab for high-risk proliferative diabetic retinopathy (IBeHi study). Acta Ophthalmol, 2008. 86(4): p. 385-9. [CrossRef]
- Gross, J.G., et al., Panretinal Photocoagulation vs Intravitreous Ranibizumab for Proliferative Diabetic Retinopathy: A Randomized Clinical Trial. Jama, 2015. 314(20): p. 2137-2146.
- Gross, J.G., et al., Five-Year Outcomes of Panretinal Photocoagulation vs Intravitreous Ranibizumab for Proliferative Diabetic Retinopathy: A Randomized Clinical Trial. JAMA Ophthalmol, 2018. 136(10): p. 1138-1148.
- Sivaprasad, S., et al., Clinical efficacy of intravitreal aflibercept versus panretinal photocoagulation for best corrected visual acuity in patients with proliferative diabetic retinopathy at 52 weeks (CLARITY): a multicentre, single-blinded, randomised, controlled, phase 2b, non-inferiority trial. Lancet, 2017. 389(10085): p. 2193-2203. [CrossRef]
- Nicholson, L., et al., Mechanistic Evaluation of Panretinal Photocoagulation Versus Aflibercept in Proliferative Diabetic Retinopathy: CLARITY Substudy. Invest Ophthalmol Vis Sci, 2018. 59(10): p. 4277-4284. [CrossRef]
- Nicholson, L., et al., Retinal Nonperfusion Characteristics on Ultra-Widefield Angiography in Eyes With Severe Nonproliferative Diabetic Retinopathy and Proliferative Diabetic Retinopathy. JAMA Ophthalmol, 2019. 137(6): p. 626-631. [CrossRef]
- Maturi, R.K., et al., Effect of Intravitreous Anti-Vascular Endothelial Growth Factor vs Sham Treatment for Prevention of Vision-Threatening Complications of Diabetic Retinopathy: The Protocol W Randomized Clinical Trial. JAMA Ophthalmol, 2021. 139(7): p. 701-712.
- Gella, L., et al., Prevalence of posterior vitreous detachment in the population with type II diabetes mellitus and its effect on diabetic retinopathy: Sankara Nethralaya Diabetic Retinopathy Epidemiology and Molecular Genetic Study SN-DREAMS report no. 23. Jpn J Ophthalmol, 2012. 56(3): p. 262-7. [CrossRef]
- Ono, R., et al., Prospective assessment of proliferative diabetic retinopathy with observations of posterior vitreous detachment. Int Ophthalmol, 2005. 26(1-2): p. 15-9. [CrossRef]
- Early vitrectomy for severe vitreous hemorrhage in diabetic retinopathy. Two-year results of a randomized trial. Diabetic Retinopathy Vitrectomy Study report 2. The Diabetic Retinopathy Vitrectomy Study Research Group. Arch Ophthalmol, 1985. 103(11): p. 1644-52.
- Berrocal, M.H. and L. Acaba-Berrocal, Early pars plana vitrectomy for proliferative diabetic retinopathy: update and review of current literature. Curr Opin Ophthalmol, 2021. 32(3): p. 203-208. [CrossRef]
- Glassman, A.R., et al., Visual Acuity, Vitreous Hemorrhage, and Other Ocular Outcomes After Vitrectomy vs Aflibercept for Vitreous Hemorrhage Due to Diabetic Retinopathy: A Secondary Analysis of a Randomized Clinical Trial. JAMA Ophthalmol, 2021. 139(7): p. 725-733.
- Simunovic, M.P. and D.A. Maberley, ANTI-VASCULAR ENDOTHELIAL GROWTH FACTOR THERAPY FOR PROLIFERATIVE DIABETIC RETINOPATHY: A Systematic Review and Meta-Analysis. Retina, 2015. 35(10): p. 1931-42.
- Zhang, Z.H., et al., Vitrectomy with or without preoperative intravitreal bevacizumab for proliferative diabetic retinopathy: a meta-analysis of randomized controlled trials. Am J Ophthalmol, 2013. 156(1): p. 106-115.e2. [CrossRef]
- Zhao, X.Y., S. Xia, and Y.X. Chen, Antivascular endothelial growth factor agents pretreatment before vitrectomy for complicated proliferative diabetic retinopathy: a meta-analysis of randomised controlled trials. Br J Ophthalmol, 2018. 102(8): p. 1077-1085. [CrossRef]
- Lee, B.J. and H.G. Yu, Vitreous hemorrhage after the 25-gauge transconjunctival sutureless vitrectomy for proliferative diabetic retinopathy. Retina, 2010. 30(10): p. 1671-7. [CrossRef]
- Oshima, Y., et al., Microincision vitrectomy surgery and intravitreal bevacizumab as a surgical adjunct to treat diabetic traction retinal detachment. Ophthalmology, 2009. 116(5): p. 927-38. [CrossRef]
- Motoda, S., et al., Predictors of postoperative bleeding after vitrectomy for vitreous hemorrhage in patients with diabetic retinopathy. J Diabetes Investig, 2018. 9(4): p. 940-945. [CrossRef]
- Hershberger, V.S., et al., Fibrovascular ingrowth at sclerotomy sites in vitrectomized diabetic eyes with recurrent vitreous hemorrhage: ultrasound biomicroscopy findings. Ophthalmology, 2004. 111(6): p. 1215-21. [CrossRef]
- Yang, C.M., P.T. Yeh, and C.H. Yang, Intravitreal long-acting gas in the prevention of early postoperative vitreous hemorrhage in diabetic vitrectomy. Ophthalmology, 2007. 114(4): p. 710-5.
- Yoshida, S., et al., Increased vitreous concentrations of MCP-1 and IL-6 after vitrectomy in patients with proliferative diabetic retinopathy: possible association with postoperative macular oedema. Br J Ophthalmol, 2015. 99(7): p. 960-6. [CrossRef]
- Naithani, P., et al., Role of topical nepafenac in prevention and treatment of macular edema after vitreoretinal surgery. Retina, 2012. 32(2): p. 250-5. [CrossRef]
- Jung, Y.H. and Y. Lee, Efficacy of vitrectomy combined with an intraoperative dexamethasone implant in refractory diabetic macular edema. Acta Diabetol, 2019. 56(6): p. 691-696. [CrossRef]
- Elman, M.J., et al., Intravitreal Ranibizumab for diabetic macular edema with prompt versus deferred laser treatment: 5-year randomized trial results. Ophthalmology, 2015. 122(2): p. 375-81. [CrossRef]
- Elman, M.J., et al., Expanded 2-year follow-up of ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology, 2011. 118(4): p. 609-14. [CrossRef]
- Diabetic Retinopathy Clinical Research, N., et al., Randomized trial of peribulbar triamcinolone acetonide with and without focal photocoagulation for mild diabetic macular edema: a pilot study. Ophthalmology, 2007. 114(6): p. 1190-1196.
- Jampol, L.M., A.R. Glassman, and N.M. Bressler, Comparative Effectiveness Trial for Diabetic Macular Edema: Three Comparisons for the Price of 1 Study From the Diabetic Retinopathy Clinical Research Network. JAMA Ophthalmol, 2015. 133(9): p. 983-4.
- Ross, E.L., et al., Cost-effectiveness of Aflibercept, Bevacizumab, and Ranibizumab for Diabetic Macular Edema Treatment: Analysis From the Diabetic Retinopathy Clinical Research Network Comparative Effectiveness Trial. JAMA Ophthalmol, 2016. 134(8): p. 888-96.
- Wells, J.A., et al., Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med, 2015. 372(13): p. 1193-203.
- Maturi, R.K., et al., Effect of Adding Dexamethasone to Continued Ranibizumab Treatment in Patients With Persistent Diabetic Macular Edema: A DRCR Network Phase 2 Randomized Clinical Trial. JAMA Ophthalmol, 2018. 136(1): p. 29-38.
- Lauermann, P., et al., Risk Factors for Severe Bleeding Complications in Vitreoretinal Surgery and the Role of Antiplatelet or Anticoagulant Agents. Ophthalmol Retina, 2021. 5(8): p. e23-e29. [CrossRef]
- Randomized clinical trial evaluating intravitreal ranibizumab or saline for vitreous hemorrhage from proliferative diabetic retinopathy. JAMA Ophthalmol, 2013. 131(3): p. 283-93.
- Berrocal, M.H., L. Acaba-Berrocal, and A.M. Acaba, Long-Term Outcomes of Same Patient Eyes Treated with Pars Plana Vitrectomy in One Eye and Conventional Treatment in the Other for Complications of Proliferative Diabetic Retinopathy. J Clin Med, 2022. 11(18). [CrossRef]
- Patel, V., et al., Outcomes of Pars Plana Vitrectomy with Panretinal Photocoagulation for Treatment of Proliferative Diabetic Retinopathy Without Retinal Detachment: A Seven-Year Retrospective Study. Clin Ophthalmol, 2023. 17: p. 471-478. [CrossRef]
- Schreur, V., et al., Long-term outcomes of vitrectomy for proliferative diabetic retinopathy. 2021. 99(1): p. 83-89. [CrossRef]
- Gupta, B., et al., Visual and anatomical outcomes following vitrectomy for complications of diabetic retinopathy: The DRIVE UK Study. Eye, 2012. 26(4): p. 510-516. [CrossRef]
- Liao, M., et al., Characteristics and outcomes of vitrectomy for proliferative diabetic retinopathy in young versus senior patients. BMC Ophthalmol, 2020. 20(1): p. 416. [CrossRef]
- Sato, T., et al., Characteristics of cases with postoperative vitreous hemorrhage after 25-gauge vitrectomy for repair of proliferative diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol, 2017. 255(4): p. 665-671. [CrossRef]
- Yorston, D., et al., Predictive clinical features and outcomes of vitrectomy for proliferative diabetic retinopathy. Br J Ophthalmol, 2008. 92(3): p. 365-8. [CrossRef]
- Tandias, R., et al., Posterior vitreous detachment status as a predictive factor for outcomes of vitrectomy for diabetic vitreous hemorrhage. Retina, 2022. 42(6): p. 1103-1110. [CrossRef]
- McCullough P, Mohite A, Virgili G, Lois N. Outcomes and Complications of Pars Plana Vitrectomy for Tractional Retinal Detachment in People With Diabetes A Systematic Review and Meta-analysis JAMA Ophthalmol, 2023. 141(2):186-195. [CrossRef]
Figure 1.
Changes in the median (min-max) best corrected visual acuity (BCVA) in the three subgroups. The star indicates significant changes between BCVA at first and final visits, respectively. The BCVA at first referral was preserved in fellow eyes.
Figure 1.
Changes in the median (min-max) best corrected visual acuity (BCVA) in the three subgroups. The star indicates significant changes between BCVA at first and final visits, respectively. The BCVA at first referral was preserved in fellow eyes.
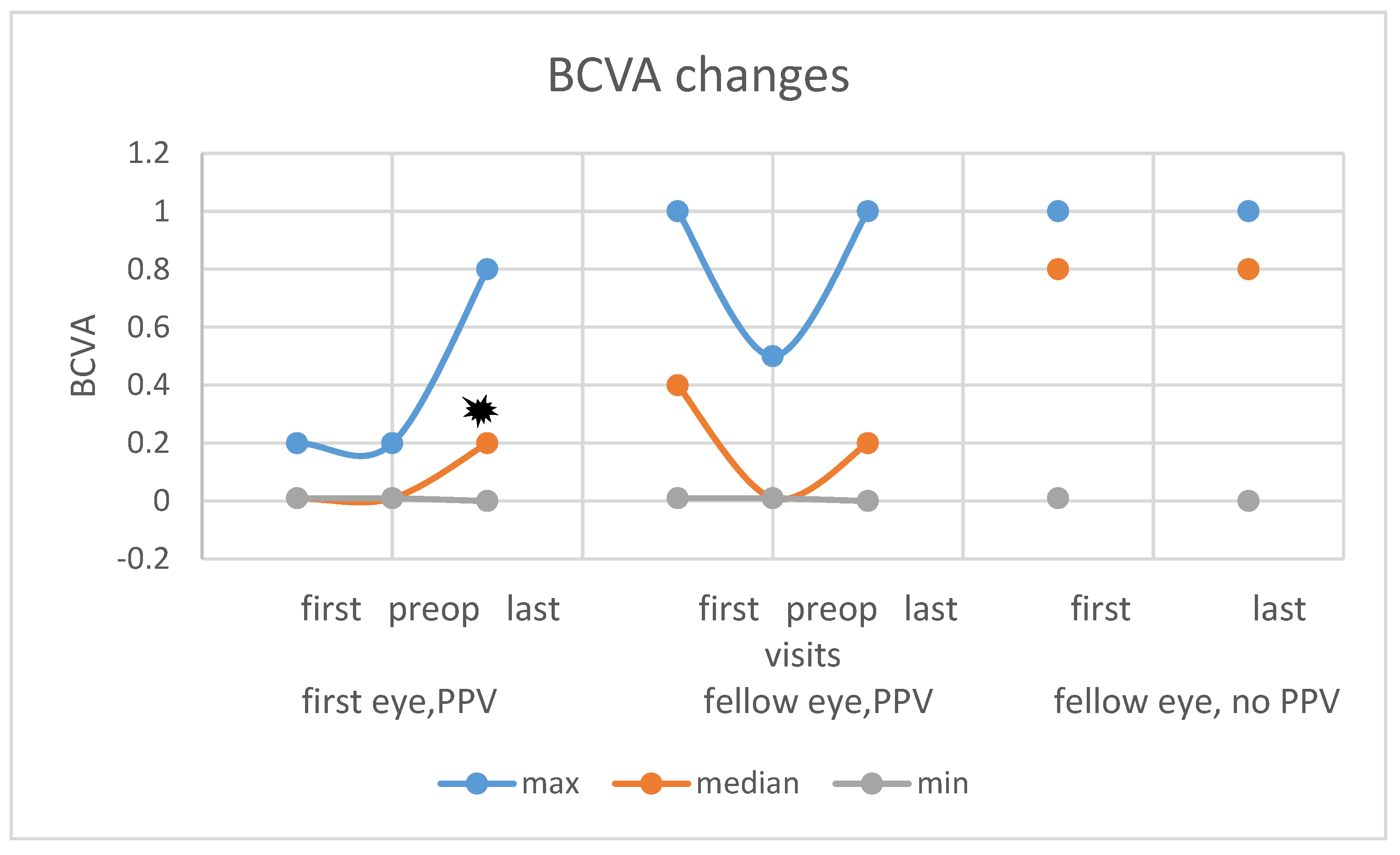

Table 1.
Baseline characteristics of our patients. PPV: pars plana vitrectomy; CV: cardiovascular; DM: diabetes mellitus, MRD: macular tractional detachment, TRD: tractional retinal detachment elsewhere, ns: not significant.
Table 1.
Baseline characteristics of our patients. PPV: pars plana vitrectomy; CV: cardiovascular; DM: diabetes mellitus, MRD: macular tractional detachment, TRD: tractional retinal detachment elsewhere, ns: not significant.
| Overall | Type 1 | Type 2 | p-value | |
| General characteristics | ||||
| Number (female/male) |
66 (22/45) | 40 (15/25) | 26 (19/7) | ns |
| Age, years | 52 (21-80) | 45 (21-78) | 58 (45-80) | 0.000* |
| follow up after PPV on first eye, months (mean min-max) | 38 (9-125) | 32.5 (9-125) | 38.5 (9-102) | ns |
| Duration of DM, years | 20 (0-57) | 24 (0-50) | 15 (2-57) | 0.000* |
| Systemic characteristics | ||||
| HbA1c (%) at the time of first PPV (mean min-max) | 7.3 (5.5-13.5) | 7.8 (5.7-12.4) | 7 (5.5-11.6) | 0.029* |
| HbA1c (%) at the end of follow-up (mean min-max) | 7.3 (5.1-17.0) | 7.6 (5.1-17) | 6.9 (5.4-9.2) | 0.004* |
| Mean HbA1c (%) (mean min-max) |
7.5 (5.4-13.1) | 7.7 (5.4-13.1) | 7.2 (5.6-10.4) | 0.002* |
| Renal insufficiency, (patients) | 9 | 7 | 2 | ns |
| Severe CV complications (patients) | 17 | 10 | 7 | ns |
| Unstable blood pressure (patients) | 18 | 12 | 6 | ns |
| Visual acuity | ||||
| BCVA at first attendance (mean min-max) | 0.05 (0.001-1) | 0.1 (0.005-1.0) | 0.04 (0.01-1.0) | ns |
| Good BCVA at first attendance (eyes) | 38 | 27 | 11 | ns |
| Legally blind at first attendance (eyes) | 86 | 46 | 40 | ns |
| Preoperative ocular factors | ||||
| Iris rubeosis at first attendance (eyes) | 9 | 7 | 2 | ns |
| Glaucoma at first attendance (eyes) | 11 | 5 | 6 | ns |
| MRD before ppv (eyes) | 44 | 29 | 15 | ns |
| TRD before ppv (eyes) | 46 | 28 | 18 | ns |
| Vitreous hemorrhage (eyes) | 85 | 49 | 36 | ns |
| Preoperative anti-VEGF injections (eyes) | 41 | 29 | 12 | ns |
| Preoperative laser (eyes) | 96 | !! | !! | ns |
Table 2.
Changes in anatomical findings in the three study groups. (Good functional outcome: 0.5≤BCVA (eyes), legally blind: BCVA≤0.2).
Table 2.
Changes in anatomical findings in the three study groups. (Good functional outcome: 0.5≤BCVA (eyes), legally blind: BCVA≤0.2).
| parameters at first/at final (No. of eyes); | all eyes (n=132) | First eyes (n=66) | Fellow eyes with PPV (n=31) | Fellow eyes without PPV (n=35) |
| good BCVA | 38/53 | 1/21 | 13/10 | 24/24 |
| legally blind eyes | 80/61 | 58/38 | 13/17 | 13/10 |
| tractional retinal detachment | 47/9 | 27/4 | 18/3 | 3/3 |
| macular tractional detachment | 44/2 | 28/9 | 14/0 | 2/2 |
| posterior hyaloid detachment | 29/- | 24/- | 5/- | - |
| silicone oil usage | -/58 | -/38 | -/20 | - |
| intraoperative complication | -/2 | -/2 | -/0 | - |
| postop. vitreous hemorrhage | -/21 | -/17 | -/4 | - |
| neovascularization on iris | 9/10 | 5/6 | 4/4 | - |
| glaucoma | 11/39 | 7/26 | 4/13 | - |
| refractory stage glaucoma | 0/10 | 0/5 | 0/5 | - |
Table 3.
Results of Spearman rank correlation. Parameters listed below might have impact on the development of BCVA.
Table 3.
Results of Spearman rank correlation. Parameters listed below might have impact on the development of BCVA.
| good BCVA at final | ||
| parameter | correlation coefficient | p value |
| age | ,246** | 0,004 |
| type of DM | -0,028 | 0,752 |
| duration of DM | ,181* | 0,037 |
| HbA1c at baseline | -0,144 | 0,100 |
| HbA1c at final | -0,162 | 0,063 |
| HbA1c, average | -,173* | 0,047 |
| renal failure | 0,035 | 0,692 |
| severe CV complication | -0,129 | 0,140 |
| unstable blood pressure | -,189* | 0,030 |
| follow-up | 0,039 | 0,657 |
| fellow eye in severe condition | ,201* | 0,021 |
| legal blindness at start | -,406** | 0,000 |
| good BCVA at START | ,469** | 0,000 |
| first BCVA | ,404** | 0,000 |
| rubeosis | -,222* | 0,011 |
| preoperative secondary glaucoma. | -,247** | 0,004 |
| vitreous hemorrhage | 0,023 | 0,824 |
| tractional macular detachment | -0,448 | 0,000 |
| posterior hyloid detachment | ,355** | 0,018 |
| vitrectomy must be performed | -,313** | 0,000 |
| phaco-combined vitrectomy | -,236** | 0,006 |
| silocon oil was used | -,417** | 0,000 |
| number of ppv | -,279** | 0,001 |
| preoperative use of anti-VEGF | 0,120 | 0,245 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



