
Submitted:
15 July 2024
Posted:
16 July 2024
You are already at the latest version
Abstract
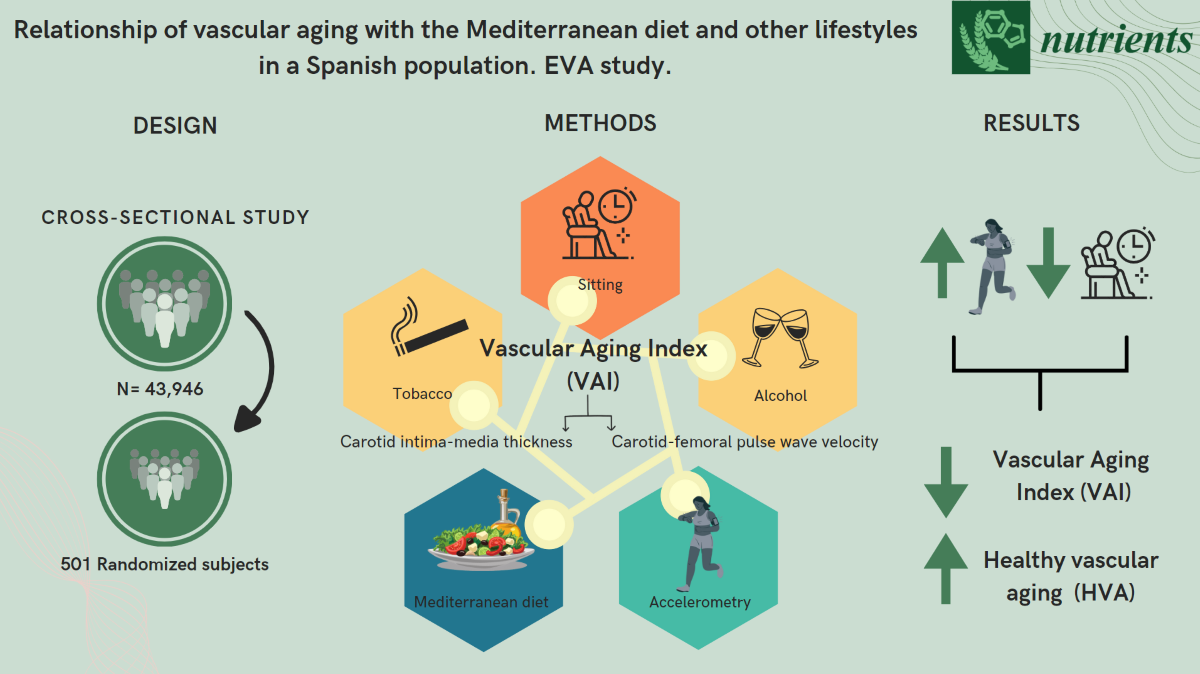
The aim of this study was to analyze the relationship between healthy vascular aging (HVA) and the Mediterranean diet alongside other lifestyles in a Spanish population aged 35 to 75 years without previous cardiovascular diseases. Methods: Cross-sectional descriptive study with 501 individuals aged 35 to 75 years recruited from five health centers by random sampling stratified by age and sex (55.90±14.24 years, 49.70% men). HVA was determined in two steps. Step 1: Subjects with vascular damage to the carotid arteries or peripheral arterial disease were classified as non-HVA. Step 2: The study population was classified by age and sex using the percentiles of the vascular aging index (VAI), with VAI ≤p25 considered HVA and >p25 considered non-HVA. The VAI was estimated using the following formula (VAI = (log (1.09) × 10 cIMT + log (1.14) cfPWV) × 39.1 + 4.76. Carotid-femoral pulse wave velocity (cfPWV) was measured with the SphygmoCor® device and carotid intima-media thickness using Sonosite Micromax® ultrasound. Mediterranean diet (MD) adherence, alcohol and tobacco use were recorded through validated questionnaires. Physical activity was assessed with the ActiGraph-GT3X® accelerometer. Results: The mean VAI value was 61.23±12.86; (Men 63.47±13.75 and women 59.04±11.54; p<0.001). HVA was found in 18.9% (men 19.9% and women 17.8%). In the multiple regression analysis after adjusting for possible confounding factors, the mean VAI value showed a positive association with alcohol use (β=0.020) and sedentary hours per week (β=0.109), and a negative association with hours of activity per week (β=-0.102) and with the number of healthy lifestyles (β=-0.640). In the logistic regression analysis after adjusting for possible confounding factors, and compared to those classified as non-HVA, subjects classified as HVA were more likely to show adherence to MD (OR = 0.571), perform more than 26 hours per week of physical activity (OR = 1.735), spend less than 142 hours per week being sedentary (OR = 1.696), and have more than two healthy lifestyles (OR = 1.877). Conclusion: The results of this study suggest that the more time spent doing physical activity and the less time spent sitting, the lower the vascular aging index and the greater likelihood of being classified in the group of subjects showing HVA.
Keywords:
Mediterranean diet
; tobacco
; alcohol
; physical activity
; sedentary time
; healthy vascular aging
1. Introduction
In Western societies, population aging represents one of the biggest issues for sustainable development. Currently 9% of the European population is aged over 65 years, and this is expected to rise to 25% by 2050 [1]. Vascular aging (VA) is characterized by the appearance of endothelial dysfunction and increased hardening of elastic arteries, an important risk factor for the development of age-related cardiovascular diseases. VA is mediated by excessive production of reactive oxygen molecules (ROS) and increased inflammation, causing reduced vasodilatory bioavailability of nitric oxide and remodeling of the arterial wall [2]. The rate of VA development depends on exposure to different factors damaging the arterial wall and the time of exposure to these factors, among which different lifestyles play an important role [3,4]. Thus, healthy lifestyle habits, such as regular aerobic exercise and certain components in the diet, coupled with dietary caloric restriction, are considered ‘frontline’ strategies for preventing and/or treating endothelial dysfunction linked to age [5].
There is currently no consensus on the best method to define VA. Methods to assess VA based only on arterial stiffness [6,7] are likely incomplete. Some authors consider that using the 10th and 90th or 25th and 75th percentiles of carotid-femoral pulse wave velocity (cfPWV) by age group to define a threshold value is more appropriate than establishing a fixed cut-off point (cfPWV > 10 m/sec), given that percentile-based reference values are more accurate in identifying increased cardiovascular risk since cfPWV is influenced by age and sex. Others authors defend the analysis of arterial wall structure to define VA by measuring the intima-media thickness (IMT) of the carotid arteries, alongside arterial stiffness, as offering a more precise assessment of VA. Thus, the vascular aging index (VAI) published by Nilsson et al. [8] integrates the IMT of the carotid artery and the cfPWV, two of the measures most used individually to estimate VA, reflecting arterial stiffness and subclinical atherosclerosis. This parameter was shown to predict cardiovascular events with good accuracy, providing complementary information in predicting the risk of cardiovascular diseases [8]. Considering all of the above, it is believed that the best definition of VA should be one that takes into account the following variables: age, blood pressure and sex (variables that have the greatest influence on arterial stiffness), as well as the cfPWV percentiles of the reference population studied (given the differences between populations) [9].
It has been shown that regular physical exercise (especially aerobic exercise) reduces arterial stiffness in the general population, thereby improving VA [5,10,11]. This occurs through increased availability of endothelial nitric oxide and a decrease in chronic low-grade vascular inflammation [3]. Moreover, numerous publications have described VA as being negatively associated with physical activity, and sedentary lifestyles have similarly been shown to have a positive link with arterial stiffness in adults [12,13,14]. While the association of VA with exercise was not found in the Framingham study [15], it was reported in a recent review [2] that aerobic exercise improves stiffness in the large arteries in middle-aged men and women. However, similar improvements through aerobic exercise training were not observed in estrogen-deficient postmenopausal women, suggesting that the effect differs with age between sexes [2].
The Mediterranean diet (MD) is the best known and most widely researched dietary pattern worldwide. It is characterized by the consumption of a wide variety of foods, such as extra virgin olive oil, legumes, cereals, nuts, fruits, vegetables, dairy products, fish and wine [16,17]. Many of these foods provide various phytonutrients, among which polyphenols and vitamins play an important role [16,17]. It is currently one of the healthiest dietary patterns, probably due to the combination of many elements with antioxidant and anti-inflammatory properties [17,18,19,20]. These effects may be mediated by its beneficial composition of macronutrients (proteins, fats, carbohydrates) and micronutrients (vitamins, minerals) [21]. Numerous studies, systematic reviews and meta-analyses have established the protective effects of the Mediterranean diet against several chronic diseases, such as diabetes [22], obesity [23], cardiovascular diseases [19,24,25], cancer [20], aging disorders [26,27], cognitive impairment [18] and general mortality [28]. Furthermore, a recent review by the Cochrane Library [24] showed the benefits of the Mediterranean diet in the primary prevention of cardiovascular diseases, reducing mortality from ischemic heart disease, improving the lipid profile, blood pressure, glycemia and adiposity; however, the level of evidence was weak to moderate and benefits in secondary prevention were not found [24]. Thus, MD constitutes a useful tool in preventing cardiovascular diseases, making it one of the dietary patterns with the best relationship with cardiovascular diseases and other health outcomes [20,29,30]. However, studies that have analyzed the effect of diet on VA and endothelial dysfunction have focused more on certain nutrients and micronutrients than on dietary patterns, and the role that the MD pattern plays in endothelial dysfunction as a precursor to increased arterial stiffness and VA is unclear [21].
Smoking favors endothelial dysfunction by decreasing nitric oxide and increasing oxidative stress, and by the production of proinflammatory cytokines that increase inflammation, vascular stiffness and therefore VA. Thus, the MESA study demonstrated that continuous smoking over a period of 10 years was linked to a greater increase in the progression of cfPWV, compared to non-smokers [31], This increase only occurred in men but not in women. Numerous other publications that also have described the positive association between VA and smoking [12,13,14]. In summary, while smoking accelerates VA and is closely related to atherosclerosis, smoking cessation can reduce the risk of vascular diseases. With regard to alcohol, some studies have shown a beneficial effect on VA of low or moderate alcohol consumption, particularly in the form of red wine [32,33]. However, excessive alcohol use is associated with an increase in arterial stiffness and a consequent increase in vascular aging [34,35].
Currently, value is attached not only to the number of years lived but also to their quality, and the WHO thus defines Healthy Aging as “the process of developing and maintaining functional ability that enables well-being in older age” [36]. This ability is understood to include a person’s capacity to satisfy their basic needs, to learn, grow and make decisions, to walk freely, to build or maintain relationships, thus contributing to the society that needs these outcomes. Achieving healthy aging must be focused on promoting healthy lifestyle habits that reduce the development of pathologies associated with aging in order to increase the quality of life of the aging population [36].
Few studies have so far jointly analyzed the effect of different lifestyles on healthy vascular aging (HVA) in the same population sample, and fewer have assessed physical activity and sedentary time as objectively measured with an accelerometer for a week. The main aim of this study is therefore to analyze the relationship of HVA with different lifestyles in Caucasian subjects aged between 35 and 75 without previous cardiovascular disease, with a secondary aim being to analyze sex differences.
2. Materials and Methods
2.1. Study Design
This cross-sectional descriptive study analyzes data from the 501 subjects included in the EVA study Association between different risk factors and the accelerated vascular aging study [37] registered at ClinicalTrials.gov. Identifier NCT02623894.
2.2. Study Population
The subjects were selected following random sampling with replacement stratified by age group (35, 45, 55, 65 and 75 years) and by sex. A total of 501 subjects were selected from 5 urban health centers, 100 subjects from each age group (50 men and 50 women). The reference population was the 43,946 subjects registered in the individual health card system. The inclusion of subjects in the study was carried out between June 2016 and the November 2017. Inclusion criteria were being aged between 35-75 years and having signed the informed consent. Exclusion criteria were having a terminal illness or not being able to travel to the research unit for any other reason, having a history of cardiovascular disease or a glomerular filtration rate < 30ml/min/1.73m2, being diagnosed with chronic inflammatory disease or any acute inflammatory process in the last three months or being treated with estrogen, testosterone or growth hormone.
Figure 1 is a flow diagram of the subjects included, excluded and the causes by age and sex groups, as well as the reference population.
2.3. Variables and Measuring Instruments
A detailed description of the study methodology, together with the inclusion and exclusion criteria, can be found in the study protocols [37].
2.3.1. Healthy Lifestyles
2.3.1.1. Mediterranean Diet
Adherence to the MD was assessed using the PREDIMED study questionnaire [38]. This questionnaire has been validated in the Spanish population and consists of 14 items, 12 of which ask about the frequency of food consumption and two about the typical eating habits of the Spanish population. Each question is scored zero or one, with one point scored for: use of olive oil as the main cooking fat, daily consumption of four or more tablespoons of olive oil (one tablespoon = 13.5 g), two or more servings of vegetables, three or more pieces of fruit, less than one serving of red or processed meat, less than one serving of animal fat, less than a 100 ml cup of sugary drinks, eating white meat in greater proportion to red meat, weekly consumption of seven or more glasses of wine, three or more servings of legumes, three or more servings of fish, three or more servings of nuts or dried fruits, two or more servings of sofrito (home-made sauce of onions and/or garlic and tomato, slow-fried in extra-virgin olive oil) and less than two baked goods. The final score ranges between 0 and 14 points, with MD adherence considered for a score above the median (7 or more points) [38].
2.3.1.2. Alcohol and Smoking
Alcohol consumption was recorded using a standardized questionnaire (recording type and amount of alcohol ingested during a week, in g/week). Adequate alcohol consumption for women was considered to be <140 g/week and for men <210 g/week [39].
Smoking was assessed with the questionnaire used in the Monica study [40], recording whether the participant was a smoker or not, the number of cigarettes per day and the years they had been smoking.
2.3.1.3. Physical Activity and Sedentary Time
Physical activity was objectively assessed using the validated ActiGraph-GT3X® accelerometer (ActiGraph, Shalimar, FL, USA) [41]. The original data from the accelerometers were collected at a frequency of 30 Hz. The specific requirements for their use were as follows: a) the accelerometers were fixed at the waist and placed on the axillary line at the level of the iliac crest of the hip right or left; b) the accelerometer was used for seven consecutive days, except when bathing or swimming. Data were invalid if the number of days was <3 days per week or the wear time was <8 h per day. Data were recorded at 1-minute intervals. The accelerometers recorded the time of physical activity performed measured in hours per week, and sedentary time per week.
2.3.2. Assessment of Vascular Structure, Function and Vascular Aging
2.3.2.1. Assessment of intima-media thickness (IMT) of the carotid arteries was performed by two trained researchers, with intraclass and intraobserver correlation coefficient values of 0.974 and 0.897 for interobserver agreement in the measurements made in 20 subjects before starting the study. The device used was the Sonosite Micromax® ultrasound machine (Sonosite Inc., Bothell, WA, USA), with a 5-10 MHz multifrequency high-resolution linear transducer and Sonocal software (Washington, USA) that automatically measures the IMT of carotid arteries. The IMT measurements were carried out following the protocol published by our research group [42].
2.3.2.2. The ankle-brachial index was measured using the VaSera VS-1500® device (Fukuda Denshi, Tokyo, Japan). The presence of vascular injury was established following the criteria included in the clinical practice guidelines [43].
2.3.2.3. Assessment of Carotid-Femoral Pulse Wave Velocity (cfPWV) was analyzed with the patient in the supine position using the SphygmoCor® device (AtCor Medical Pty Ltd., Head Office, West Ryde, Australia), which calculates cfPWV by estimating the time delay with respect to the R wave of the electrocardiogram. To do this, the distance between the sternal notch and the point where the sensor is placed on the carotid and femoral arteries was determined by means of a measuring tape [44]. The quality of the pulse wave is established by the device-specific software, and the manufacturer’s instructions were followed at all times to estimate the cfPWV.
2.3.2.4 Vascular Aging Index (VAI)
The VAI was estimated with the following formula [30]:
VAI = (log (1.09) x 10 cIMT + log (1.14) × aPWV) × 39.1 + 4.76
where cIMT is the carotid intima-media thickness, aPWV is the aortic pulse wave velocity equivalent to cfPWV, and log is the natural logarithm with base e. VAI is a parameter that combines methods to measure different arterial properties. It takes into account the IMT-assessed vascular structure of the carotid arteries, which reflects already established atherosclerosis, and the equivalent of aPWV to cfPWV, which reflects arterial stiffness [44].
2.3.3. Definition of Healthy Vascular Aging
Healthy vascular aging (HVA) was determined in two steps: Step 1: Subjects with vascular injury in the carotid arteries or peripheral arterial disease were classified as non-HVA. Step 2: The studied population was classified by age and sex using the VAI percentiles [8]. Subjects with values ≤ 25th percentile were classified as HVA and subjects with values > 25th percentile as non-HVA.
2.3.4. Anthropometric Measurements and Cardiovascular Risk Factors
Blood pressure, weight and height were measured at the Primary Care Research Unit of Salamanca (APISAL) following the recommendations published in the study protocol [37]. Subjects were considered to have hypertension if they were taking antihypertensive drugs or with blood pressure values ≥140/90 mmHg; to have type 2 diabetes mellitus if they were taking hypoglycemic agents or had fasting plasma glucose values ≥126 mg/dl or HbA1c ≥ 6.5%; to have dyslipidemia if they were taking lipid-lowering agents or had fasting total cholesterol values ≥ 240 mg/dl, low-density lipoprotein cholesterol (LDL-C) ≥ 160 mg/dL, high-density lipoprotein cholesterol (HDL-C) ≤ 40 mg/dl in men and ≤ 50 mg/dl in women, or triglycerides ≥ 150 mg/dl. Obesity was defined as having a BMI ≥ 30 kg/m2 [43].
2.3.5. Analytical Tests
Venous blood samples were taken between 08:00 and 09:00 hours after subjects had fasted for 12 hours. Fasting plasma glucose, serum total cholesterol, high-density lipoprotein cholesterol, and triglyceride levels were measured using a standard enzyme. Glycosylated hemoglobin was measured with an automated immunoturbidimetric assay method. All analytical tests were processed in the same laboratory [37].
2.4. Statistical Analysis
Data are presented using means ± standard deviations and numbers or percentages depending on whether variables are continuous or categorical. The comparison between men and women was done with chi-square tests for percentages and Student’s t tests for continuous variables. The Pearson correlation coefficient was used to analyze the relationship between continuous variables.
To analyze the association between the average VAI score and the different lifestyles, six multiple linear regression models were used, using the VAI as dependent variable and the number of healthy lifestyles, average MD adherence score, weekly alcohol consumption in g/week, years of smoking, number of active hours per week and number of sedentary hours per week as independent variables.
To analyze the association between HVA individuals and different lifestyles, six logistic regression models were used. Those classified as HVA or not HVA were dependent variables (coded HVA=1, No HVA=0), healthy lifestyles (coded Yes=1, No=0) were independent variables. The median score for the different healthy lifestyles, except in the case of alcohol, which was used if they had adequate alcohol consumption or not (considered to be <140 g/week in women and 210 g/week in men).
In all models, age, sex, mean arterial pressure, atherogenic index, HbA1c and body mass index were included as adjustment variables.
All analyses were performed globally and by sex. The SPSS Statistics program for Windows, version 28.0 (IBM Corp, Armonk, NY, USA) was used. A value of p < 0.05 was considered the statistical significance limit.
2.5. Ethical Principles
This EVA Project was approved by the Drug Research Ethics Committee of the Salamanca health area on 04/05/2015 (CEIm reference code PI 15/01039). Before the start of the study, all participants signed the informed consent. During the course of the study, the standards of the Declaration of Helsinki [45] and the WHO guidelines for observational studies were followed. Subject confidentiality was guaranteed at all times, in accordance with the provisions of Organic Law 3/2018, of December 5 on personal data protection and the guarantee of digital rights, and European Parliament Regulation (EU) 2016/679 and the Data Protection Council of April 27, 2016 (GDPR).
3. Results
3.1. Lifestyles, Risk Factors, and Vascular Structure and Function of the Subjects Included, Overall and by Sex
In the overall analysis, the mean MD score was 7.15±2.07 with adherence to the MD of 42.7%. Average alcohol consumption was 40.47±63.15 grams per week and adequate consumption was 50.1%. The years of smoking average was 12.98±17.41 and the percentage of subjects who had never smoked was 73.3%. Hours of physical activity per week was 27.09±9.52, with 49.7% doing more than 26 hours per week. Mean sedentary time was 140.75±9.56 hours per week, with 51.1% being sedentary for under 142 hours per week. The average number of healthy lifestyles was 2.66±1.29 and 50.5% had more than 2 healthy lifestyles. In the analysis by sex, women showed higher values of MD, total physical activity and the average number of healthy lifestyles, and less alcohol consumption and sedentary time per week than men. In the overall analysis, the mean value for IMT was 0.682±0.109 mm, cfPWV was 6.53±2.03 m/sec and the VAI was 61.23±12.86. These values were higher in men than in women. Table 1 presents the values of the different cardiovascular risk factors as well as the drugs used in hypertension, dyslipidemia and type 2 diabetes mellitus treatment, overall and by sex.
3.2. Lifestyles, Risk Factors, and Vascular Structure and Function According to Vascular Aging
Table 2 shows the mean values for lifestyles, cardiovascular risk factors and IMT, cfPWV and VAI parameters in subjects with HVA and without HVA. Total physical activity was 29.19 vs 26.58 hours per week; sedentary hours per week was 138 vs 141, the percentage of subjects who had never smoked was 69.1% vs 67.0% and the percentage of subjects with more than 2 healthy lifestyles was 60.6% vs 48.3% in subjects classified as HVA compared to those classified as non-HVA (p<0.05). All cardiovascular risk factors, except total cholesterol and LDL cholesterol, showed more favorable values in subjects classified as HVA. The parameters of vascular structure and function and the VAI showed similar results.
Figure 4 represents the differences in the VAI values between subjects with healthy lifestyles and without healthy lifestyles, overall and by sex.
3.3. Correlation of Vascular Aging with Mediterranean Diet and Other Lifestyles
Table 3 shows the correlation of the VAI with lifestyles adjusted by age, overall and by sex. The VAI showed a negative association with the mean value of MD (r=-0.102), hours of total physical activity (r=-0.158) and the number of healthy lifestyles (r=-0.199), and a positive association with consumption of alcohol (r=0.228), years of smoking (r=0.092) and sedentary time (r=0.165).
3.4. Association between Vascular Aging Index and Healthy Lifestyles, Multiple Regression Analysis
In multiple regression analysis after adjustment for potential confounders, the mean VAI value showed a negative association with hours of total physical activity per week (β=-.102, 95% CI: -0.176 to -0.028) and with the number of healthy lifestyles (β=-0.640, 95% CI: -1.195 to -0.086) and positive association with alcohol consumption (β=0.020, 95% CI: 0.008 to 0.032) and with sedentary hours per week (β=0.109; 95% CI: 0.036 to 0.183). The analysis by sex yielded similar results, as shown in Table 4, except for alcohol consumption and number of healthy lifestyles, which were significant in men but not in women.
3.5. Association between Vascular Aging Index and Healthy Lifestyles, Logistic Regression Analysis
In the logistic regression analysis after adjustment for possible confounding factors, compared to non-HVA, subjects classified as HVA were more likely to have Mediterranean diet adherence (OR = 0.571; 95% CI: 0.333 to 0.981), to do more than 26 hours per week of physical activity (OR = 1.735; 95% CI: 1.048 to 2.871), to be sedentary for less than 142 hours per week (OR = 1.696; 95% CI: 1.025 to 2.805) and have more than 2 healthy lifestyles (OR = 1.877; 95% CI: 1.123 to 3.136). In the analysis by sex, the results were similar, although there were no significant differences except for smoking in men, as reflected in Table 5. The text continues here.
4. Discussion
To our knowledge, this is the first study to analyze the relationship of estimated HVA and VAI with different lifestyles in a Spanish adult population without a history of cardiovascular disease. The main findings of this study are: 1) using the VAI as an aging criterion, approximately one in five subjects is classified as HVA and 2) in both multiple and logistic regression analyses, the lifestyles most strongly associated with the VAI and with HVA is the amount of physical activity and sedentary time, measured objectively in hours/week with an accelerometer over seven days.
In line with results published by other authors, this study shows that the more hours of physical activity and the fewer hours of sedentary activity, the lower the VA. Thus, numerous studies have shown a negative association of arterial stiffness with physical activity and a positive association with sedentary lifestyle in adults [12,13,14], with aerobic exercise in particular improving VA [5,10,11], and longitudinal studies have shown that the increase in arterial stiffness over five years, measured with the cfPWV, is linked to time spent doing physical activity and sedentary time [46]. Ahmadi et al. [47], for example, found that limiting sedentary time was associated with slower progression of aortic stiffness. However, this association has not been found in all studies, as with the case of the Framingham study [15], probably because physical activity was not objectively measured with an accelerometer in that study. On the other hand, a recent review [2] shows that aerobic exercise improves the stiffness of large arteries in middle-aged men and women, although the same effects were not observed in postmenopausal women with estrogen deficiency, suggesting that the effect may differ with age between sexes [2]. Supporting the results of this present study, other authors have found that time spent watching television is related to worse cardiovascular health [48,49], and Wennman et al. [50] found that the risk of cardiovascular disease was higher in men who spent four hours or more watching television and in women watching two to three hours. Therefore, taking into account the benefits of physical activity [51] and the dangers of a sedentary lifestyle [52], it seems logical that HVA improves with increased physical activity and decreased sedentary time. Nevertheless, sedentary lifestyles are becoming more prevalent worldwide due to the lack of available spaces for exercise, the increase in sedentary occupational behaviors such as office work, and the greater usage of electronic devices, television or video [53]. Indeed, studies carried out in Europe, the United States and Australia have shown that adults spend half of their working day (4.2 hours/day) and around 2.9 hours/day of their free time sitting [54].
As in previous studies, MD adherence was higher in women [55]. Contrary to what would be expected, the mean MD score did not show an association with the VAI, either overall or by sex. However, the overall analysis showed an OR of 0.571 in logistic regression, after adjusting for possible confounding factors. Similarly, the increase in cfPWV over 5 years has not been associated with the MD [46]. Nevertheless, there are several studies that show subjects with adherence to a MD pattern having improved endothelial function, inflammation, oxidative stress or other conditions that predispose people to cardiovascular events, such as obesity or type 2 diabetes mellitus, suggesting that it may play an important role in HVA by preventing the onset of certain diseases and improving the VA process [21,56]. Thus, some authors consider that dietary patterns such as MD should be considered ‘frontline’ strategies in preventing and/or treating age-related cardiovascular dysfunction [5]. However, it should not be forgotten that, as shown in a recent review [27], the majority of studies carried out have focused on the benefits of certain components of MD in specific processes of general aging without specifically analyzing the effect on VA or HVA, concluding that the benefits of the MD become more important in older people, especially for achieving healthy aging. Different studies have thus shown the benefits of magnesium and potassium in preventing the reduction of muscle mass [57], improved bone and mineral homeostasis with diets rich in calcium, vitamins D, A, B, C, E and minerals such as potassium and magnesium, thereby modulating long-term bone health [58], improved bone density and prevention of osteoporosis in Spanish postmenopausal women [59], and increased immune responses through vitamin D, E and probiotic intake [60,61]. For all of the above, although there is sufficient evidence of the MD pattern having general health benefits, questions remain about whether it is the MD pattern or certain micronutrients and vitamins that are responsible for HVA, and whether the effect is the same in all the age groups and in both sexes. Therefore, more research is needed to provide a better understanding of the mechanism of how the MD acts on aging, although on the basis of the current evidence, the MD could be recommended as an anti-aging therapy to prevent frailty and maintain functionality until the final stages of life [26].
In this study, alcohol consumption measured in grams per week was positively associated with the VAI overall and in men. These results are in line with those shown by Hwang et al. [62], and data published in a review in 2022 [34] analyzing the relationship between arterial stiffness and alcohol consumption concluded that greater alcohol consumption is associated with worse arterial stiffness values, using different measurement methods (oscillometry or tonometry) and obtaining similar results across the different populations studied (European, American and Asian) and for almost all types of alcoholic beverages consumed. Some studies only show an association between alcohol intake and cfPWV in men [34,35]. This association was not found in our logistic regression analysis, and is a result that is not consistent with what has been published by several authors who have suggested a J-shaped relationship between alcohol consumption and arterial stiffness measured with cfPWV [35,63]. The discrepancies between this study and others may be explained by different reasons. The VAI used as a criterion is an aging index that, in addition to arterial stiffness, takes into account the thickness (IMT) of the carotid artery. Furthermore, we cannot forget that the studies analyzed were heterogeneous, using different methods to measure arterial stiffness, with alcohol consumption recorded subjectively, and the majority were cross-sectional studies. All of this, together with the fact that many of the studies have methodological weaknesses and may overestimate the benefits of alcohol on cardiovascular diseases, making the results inconclusive [64,65,66]. Therefore, the debate on the relationship between alcohol consumption and VA remains an open one, given that the relationship is complex and potentially affected by several factors such as the type of alcohol, consumption levels, sex and age differences.
This study did not find an association between years of smoking and VAI, in line with some other studies that did not yield significant changes in the chronic effect of smoking on arterial stiffness [34]. However, most studies, as reflected in the results of the Gutenberg Health Study published in 2023, have concluded that chronic smoking is strongly and dose-dependently associated with an increase in arterial stiffness, regardless of sex, but with an association that is stronger in men [67], but they used the stiffness index and the increase index as measures of stiffness. On the other hand, in the logistic regression analysis we only found an association in men, in line with the results published by other authors [68], suggesting different patterns of vascular system stiffness in men and women due to smoking.
Finally, hormonal and non-hormonal factors influence differences between the sexes. The protection of endogenous estrogen until menopause in women is well known. Furthermore, in males, arterial stiffness increases linearly from puberty, which indicates that females intrinsically have stiffer main arteries than males, effects that are mitigated by sex steroids during reproductive life. Other factors, such as height, body fat distribution, and inflammatory factors may also play a role [69]
Limitations and strengths
This study has a number of limitations and strengths. The main limitation is that the analysis is based on cross-sectional data, which prevents us from establishing causality. Another limitation is that three of the four lifestyles analyzed were recorded subjectively through questionnaires. Among the strengths of the study are sample selection through random sampling stratified by age and sex groups from a reference population of more than 43,000 subjects, while the measurement of IMT of carotid arteries and cfPWV were performed under standardized conditions, by experienced evaluators and with validated devices. Furthermore, all analytical measurements were carried out in laboratories with adequate quality controls.
5. Conclusions
The results of this study suggest that the longer we do physical activity and the less time we spend sitting, the lower the rate of vascular aging and the greater the likelihood of being classified in the group of subjects showing HVA.
Author Contributions
Conceptualization, M.A.G.-M; D.G.-F and L.G.-S.; methodology, M.A.G.-M. G.O.-L and M.G.-S.; formal analysis, M.A.G.-M. and L.G.-O.; investigation, L.G.-S., M.G.-S.; data curation, M.A.G.-M., E.R.-S.; writing—original draft preparation, L.G.-S. and D.G.-F.; writing—review and editing, project administration, M.A.G.-M., L.G.-S.; funding acquisition, M.A.G.-M; L.G.-S. All authors have read and accepted the published version of the manuscript.
Funding
This study was funded by the Regional Health Agency of the Castilla y León government through research projects (GRS 1193/B/15), by the Carlos III Health Institute (ISCIII) of the Ministry of Science and Innovation, by project RD21/0016/0010 of the research network RICAPPS (Red de Investigación en Cronicidad, Atención Primaria y Promoción de la Salud), and by the research project PI21/00454 financed by the Next Generation EU, Recovery and Resilience Mechanism (RRM). Human resources were also obtained through the Castilla y León government research program (INT/M/02/17 and INT/M/04/15), from the biomedical research institute of Salamanca (IBSAL) (IBI21/00001) and the Carlos III Health Institute (INT22/00007). None played any role in the study design, data analysis, reporting of results, or the decision to submit the manuscript for publication.
Institutional Review Board Statement
All staff involved in this study were trained before the study began. This study was approved by the ethics committee of the Drug Research Ethics Committee of the Salamanca health area.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare that no conflict of interest.
References
- Mitchell, E.; Walker, R. Global ageing: successes, challenges and opportunities. Br J Hosp Med (Lond) 2020, 81, 1–9. [Google Scholar] [CrossRef]
- Moreau, K.L.; Clayton, Z.S.; DuBose, L.E.; Rosenberry, R.; Seals, D.R. Effects of regular exercise on vascular function with aging: Does sex matter? Am J Physiol Heart Circ Physiol 2024, 326, H123–h137. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P.; Cunha, P.G.; Lacolley, P.; Nilsson, P.M. Concept of Extremes in Vascular Aging. Hypertension 2019, 74, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Nowak, K.L.; Rossman, M.J.; Chonchol, M.; Seals, D.R. Strategies for Achieving Healthy Vascular Aging. Hypertension 2018, 71, 389–402. [Google Scholar] [CrossRef]
- Clayton, Z.S.; Craighead, D.H.; Darvish, S.; Coppock, M.; Ludwig, K.R.; Brunt, V.E.; Seals, D.R.; Rossman, M.J. Promoting healthy cardiovascular aging: emerging topics. J Cardiovasc Aging 2022, 2. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S. Defining vascular aging and cardiovascular risk. J Hypertens 2012, 30 Suppl, S3–8. [Google Scholar] [CrossRef]
- Bruno, R.M.; Nilsson, P.M.; Engström, G.; Wadström, B.N.; Empana, J.P.; Boutouyrie, P.; Laurent, S. Early and Supernormal Vascular Aging: Clinical Characteristics and Association With Incident Cardiovascular Events. Hypertension 2020, 76, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Nilsson Wadström, B.; Fatehali, A.H.; Engström, G.; Nilsson, P.M. A Vascular Aging Index as Independent Predictor of Cardiovascular Events and Total Mortality in an Elderly Urban Population. Angiology 2019, 70, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Sanchez, M.; Gomez-Sanchez, L.; Patino-Alonso, M.C.; Cunha, P.G.; Recio-Rodriguez, J.I.; Alonso-Dominguez, R.; Sanchez-Aguadero, N.; Rodriguez-Sanchez, E.; Maderuelo-Fernandez, J.A.; Garcia-Ortiz, L.; et al. Vascular aging and its relationship with lifestyles and other risk factors in the general Spanish population: Early Vascular Ageing Study. J Hypertens 2020, 38, 1110–1122. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Qi, L.; Xu, L.; Sun, X.; Liu, W.; Zhou, S.; van de Vosse, F.; Greenwald, S.E. Effects of exercise modalities on central hemodynamics, arterial stiffness and cardiac function in cardiovascular disease: Systematic review and meta-analysis of randomized controlled trials. PLoS One 2018, 13, e0200829. [Google Scholar] [CrossRef] [PubMed]
- Murray, K.O.; Mahoney, S.A.; Venkatasubramanian, R.; Seals, D.R.; Clayton, Z.S. Aging, aerobic exercise, and cardiovascular health: Barriers, alternative strategies and future directions. Exp Gerontol 2023, 173, 112105. [Google Scholar] [CrossRef]
- Kucharska-Newton, A.M.; Stoner, L.; Meyer, M.L. Determinants of Vascular Age: An Epidemiological Perspective. Clin Chem 2019, 65, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Appiah, D.; Capistrant, B.D. Cardiovascular Disease Risk Assessment in the United States and Low- and Middle-Income Countries Using Predicted Heart/Vascular Age. Sci Rep 2017, 7, 16673. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P.; Cunha, P.G.; Lacolley, P.; Nilsson, P.M. Concept of Extremes in Vascular Aging. Hypertension 2019, HYPERTENSIONAHA11912655. [CrossRef]
- Niiranen, T.J.; Lyass, A.; Larson, M.G.; Hamburg, N.M.; Benjamin, E.J.; Mitchell, G.F.; Vasan, R.S. Prevalence, Correlates, and Prognosis of Healthy Vascular Aging in a Western Community-Dwelling Cohort: The Framingham Heart Study. Hypertension 2017, 70, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Román, G.C.; Jackson, R.E.; Reis, J.; Román, A.N.; Toledo, J.B.; Toledo, E. Extra-virgin olive oil for potential prevention of Alzheimer disease. Rev Neurol (Paris) 2019, 175, 705–723. [Google Scholar] [CrossRef] [PubMed]
- Martini, D. Health Benefits of Mediterranean Diet. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Kaddoumi, A.; Denney, T.S., Jr.; Deshpande, G.; Robinson, J.L.; Beyers, R.J.; Redden, D.T.; Praticò, D.; Kyriakides, T.C.; Lu, B.; Kirby, A.N. , et al. Extra-Virgin Olive Oil Enhances the Blood-Brain Barrier Function in Mild Cognitive Impairment: A Randomized Controlled Trial. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-Style Diet for the Primary and Secondary Prevention of Cardiovascular Disease: A Cochrane Review. Glob Heart 2020, 15, 56. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Fekete, M.; Szarvas, Z.; Fazekas-Pongor, V.; Feher, A.; Csipo, T.; Forrai, J.; Dosa, N.; Peterfi, A.; Lehoczki, A.; Tarantini, S. , et al. Nutrition Strategies Promoting Healthy Aging: From Improvement of Cardiovascular and Brain Health to Prevention of Age-Associated Diseases. Nutrients 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean Diet Effects on Type 2 Diabetes Prevention, Disease Progression, and Related Mechanisms. A Review. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Di Bella, G.; Cusumano, C.; Parisi, A.; Tagliaferri, F.; Ciriminna, S.; Barbagallo, M. Mediterranean diet in the management and prevention of obesity. Exp Gerontol 2023, 174, 112121. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst Rev 2019, 3, CD009825. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst Rev 2019, 3, Cd009825. [Google Scholar] [CrossRef] [PubMed]
- Andreo-López, M.C.; Contreras-Bolívar, V.; Muñoz-Torres, M.; García-Fontana, B.; García-Fontana, C. Influence of the Mediterranean Diet on Healthy Aging. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Mazza, E.; Ferro, Y.; Pujia, R.; Mare, R.; Maurotti, S.; Montalcini, T.; Pujia, A. Mediterranean Diet In Healthy Aging. J Nutr Health Aging 2021, 25, 1076–1083. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Di Bella, G.; Veronese, N.; Barbagallo, M. Impact of Mediterranean Diet on Chronic Non-Communicable Diseases and Longevity. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- D’Innocenzo, S.; Biagi, C.; Lanari, M. Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Román-Viñas, B.; Sanchez-Villegas, A.; Guasch-Ferré, M.; Corella, D.; La Vecchia, C. Benefits of the Mediterranean diet: Epidemiological and molecular aspects. Mol Aspects Med 2019, 67, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, Y.; Teixido-Tura, G.; Ambale-Venkatesh, B.; Noda, C.; Chugh, A.R.; Liu, C.Y.; Redheuil, A.; Stacey, R.B.; Dietz, H.; Gomes, A.S. , et al. Ten-year longitudinal change in aortic stiffness assessed by cardiac MRI in the second half of the human lifespan: the multi-ethnic study of atherosclerosis. Eur Heart J Cardiovasc Imaging 2016, 17, 1044–1053. [Google Scholar] [CrossRef] [PubMed]
- Karimi, L.; Mattace-Raso, F.U.; van Rosmalen, J.; van Rooij, F.; Hofman, A.; Franco, O.H. Effects of combined healthy lifestyle factors on functional vascular aging: the Rotterdam Study. J Hypertens 2016, 34, 853–859. [Google Scholar] [CrossRef]
- Weber, T.; Wassertheurer, S.; Hametner, B.; Moebus, S.; Pundt, N.; Mahabadi, A.A.; Roggenbuck, U.; Lehmann, N.; Jockel, K.H.; Erbel, R. Cross-sectional analysis of pulsatile hemodynamics across the adult life span: reference values, healthy and early vascular aging: the Heinz Nixdorf Recall and the MultiGeneration Study. J Hypertens 2019, 37, 2404–2413. [Google Scholar] [CrossRef] [PubMed]
- Del Giorno, R.; Maddalena, A.; Bassetti, S.; Gabutti, L. Association between Alcohol Intake and Arterial Stiffness in Healthy Adults: A Systematic Review. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, D.; Britton, A.; Brunner, E.J.; Bell, S. Twenty-Five-Year Alcohol Consumption Trajectories and Their Association With Arterial Aging: A Prospective Cohort Study. J Am Heart Assoc 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Marcos, M.A.; Martinez-Salgado, C.; Gonzalez-Sarmiento, R.; Hernandez-Rivas, J.M.; Sanchez-Fernandez, P.L.; Recio-Rodriguez, J.I.; Rodriguez-Sanchez, E.; García-Ortiz, L. Association between different risk factors and vascular accelerated ageing (EVA study): study protocol for a cross-sectional, descriptive observational study. BMJ Open 2016, 6, e011031. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M. , et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J Nutr 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Sanidad, M.d. Límites de Consumo de Bajo Riesgo de Alcohol. Actualización del Riesgo Relacionado con los Niveles de Consumo de Alcohol, el Patrón de Consumo y el Tipo de Bebida. Ministerio de Sanidad Madrid, Spain: 2020.
- The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. WHO MONICA Project Principal Investigators. J Clin Epidemiol 1988, 41, 105–114. [Google Scholar] [CrossRef]
- Melanson, E.L., Jr.; Freedson, P.S. Validity of the Computer Science and Applications, Inc. (CSA) activity monitor. Med Sci Sports Exerc 1995, 27, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Marcos, M.A.; Recio-Rodríguez, J.I.; Patino-Alonso, M.C.; Agudo-Conde, C.; Gómez-Sanchez, L.; Gómez-Sanchez, M.; Rodríguez-Sánchez, E.; García-Ortiz, L. Protocol for measuring carotid intima-media thickness that best correlates with cardiovascular risk and target organ damage. Am J Hypertens 2012, 25, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A. , et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens 2018, 36, 2284–2309. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.D. , et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J Hypertens 2012, 30, 445–448. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [CrossRef] [PubMed]
- Navarro Cáceres, A.; Navarro-Matías, E.; Gómez-Sánchez, M.; Tamayo-Morales, O.; Lugones-Sánchez, C.; González-Sánchez, S.; Rodríguez-Sánchez, E.; García-Ortiz, L.; Gómez-Sánchez, L.; Gómez-Marcos, M.A. , et al. Increase in Vascular Function Parameters According to Lifestyles in a Spanish Population without Previous Cardiovascular Disease-EVA Follow-Up Study. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi-Abhari, S.; Sabia, S.; Shipley, M.J.; Kivimäki, M.; Singh-Manoux, A.; Tabak, A.; McEniery, C.; Wilkinson, I.B.; Brunner, E.J. Physical Activity, Sedentary Behavior, and Long-Term Changes in Aortic Stiffness: The Whitehall II Study. J Am Heart Assoc 2017, 6, e005974. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Grunseit, A.; Midthjell, K.; Holmen, J.; Holmen, T.L.; Bauman, A.E.; van der Ploeg, H.P. Cross-sectional associations of total sitting and leisure screen time with cardiometabolic risk in adults. J Sci Med Sport 2014, 17, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Wilkens, L.R.; Park, S.Y.; Goodman, M.T.; Monroe, K.R.; Kolonel, L.N. Association between various sedentary behaviours and all-cause, cardiovascular disease and cancer mortality: the Multiethnic Cohort Study. Int J Epidemiol 2013, 42, 1040–1056. [Google Scholar] [CrossRef] [PubMed]
- Wennman, H.; Vasankari, T.; Borodulin, K. Where to Sit? Type of Sitting Matters for the Framingham Cardiovascular Risk Score. AIMS Public Health 2016, 3, 577–591. [Google Scholar] [CrossRef] [PubMed]
- Park, W.; Park, H.Y.; Lim, K.; Park, J. The role of habitual physical activity on arterial stiffness in elderly Individuals: a systematic review and meta-analysis. J Exerc Nutrition Biochem 2017, 21, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Leiva, A.M.; Martínez, M.A.; Cristi-Montero, C.; Salas, C.; Ramírez-Campillo, R.; Díaz Martínez, X.; Aguilar-Farías, N.; Celis-Morales, C. [Sedentary lifestyle is associated with metabolic and cardiovascular risk factors independent of physical activity]. Rev Med Chil 2017, 145, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Moon, J.H.; Kim, H.J.; Kong, M.H.; Oh, Y.H. Sedentary Lifestyle: Overview of Updated Evidence of Potential Health Risks. Korean J Fam Med 2020, 41, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Tigbe, W.W.; Granat, M.H.; Sattar, N.; Lean, M.E.J. Time spent in sedentary posture is associated with waist circumference and cardiovascular risk. Int J Obes (Lond) 2017, 45, 689–669. [Google Scholar] [CrossRef] [PubMed]
- Caparello, G.; Galluccio, A.; Giordano, C.; Lofaro, D.; Barone, I.; Morelli, C.; Sisci, D.; Catalano, S.; Andò, S.; Bonofiglio, D. Adherence to the Mediterranean diet pattern among university staff: a cross-sectional web-based epidemiological study in Southern Italy. Int J Food Sci Nutr 2020, 71, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Lista, J.; Perez-Martinez, P.; Garcia-Rios, A.; Perez-Caballero, A.I.; Perez-Jimenez, F.; Lopez-Miranda, J. Mediterranean Diet and Cardiovascular Risk: Beyond Traditional Risk Factors. Crit Rev Food Sci Nutr 2016, 56, 788–801. [Google Scholar] [CrossRef] [PubMed]
- Granic, A.; Sayer, A.A.; Robinson, S.M. Dietary Patterns, Skeletal Muscle Health, and Sarcopenia in Older Adults. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Sahni, S.; Mangano, K.M.; McLean, R.R.; Hannan, M.T.; Kiel, D.P. Dietary Approaches for Bone Health: Lessons from the Framingham Osteoporosis Study. Curr Osteoporos Rep 2015, 13, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rey, J.; Roncero-Martín, R.; Rico-Martín, S.; Rey-Sánchez, P.; Pedrera-Zamorano, J.D.; Pedrera-Canal, M.; López-Espuela, F.; Lavado García, J.M. Adherence to a Mediterranean Diet and Bone Mineral Density in Spanish Premenopausal Women. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Jovic, T.H.; Ali, S.R.; Ibrahim, N.; Jessop, Z.M.; Tarassoli, S.P.; Dobbs, T.D.; Holford, P.; Thornton, C.A.; Whitaker, I.S. Could Vitamins Help in the Fight Against COVID-19? Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Daviglus, M.L.; Bell, C.C.; Berrettini, W.; Bowen, P.E.; Connolly, E.S., Jr.; Cox, N.J.; Dunbar-Jacob, J.M.; Granieri, E.C.; Hunt, G.; McGarry, K. , et al. National Institutes of Health State-of-the-Science Conference statement: preventing alzheimer disease and cognitive decline. Ann Intern Med 2010, 153, 176–181. [Google Scholar] [CrossRef]
- Hwang, C.L.; Piano, M.R.; Thur, L.A.; Peters, T.A.; da Silva, A.L.G.; Phillips, S.A. The effects of repeated binge drinking on arterial stiffness and urinary norepinephrine levels in young adults. J Hypertens 2020, 38, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Sanchez, J.; Garcia-Ortiz, L.; Rodriguez-Sanchez, E.; Maderuelo-Fernandez, J.A.; Tamayo-Morales, O.; Lugones-Sanchez, C.; Recio-Rodriguez, J.I.; Gomez-Marcos, M.A. The Relationship Between Alcohol Consumption With Vascular Structure and Arterial Stiffness in the Spanish Population: EVA Study. Alcohol Clin Exp Res 2020, 44, 1816–1824. [Google Scholar] [CrossRef]
- Krittanawong, C.; Isath, A.; Rosenson, R.S.; Khawaja, M.; Wang, Z.; Fogg, S.E.; Virani, S.S.; Qi, L.; Cao, Y.; Long, M.T. , et al. Alcohol Consumption and Cardiovascular Health. Am J Med 2022, 135, 1213–1230. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M. Alcohol’s Impact on the Cardiovascular System. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Claas, S.A.; Arnett, D.K. The Role of Healthy Lifestyle in the Primordial Prevention of Cardiovascular Disease. Curr Cardiol Rep 2016, 18, 56. [Google Scholar] [CrossRef] [PubMed]
- Hahad, O.; Schmitt, V.H.; Arnold, N.; Keller, K.; Prochaska, J.H.; Wild, P.S.; Schulz, A.; Lackner, K.J.; Pfeiffer, N.; Schmidtmann, I. , et al. Chronic cigarette smoking is associated with increased arterial stiffness in men and women: evidence from a large population-based cohort. Clin Res Cardiol 2023, 112, 270–284. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Hahad, O.; Kuntic, M.; Keaney, J.F.; Deanfield, J.E.; Daiber, A. Effects of tobacco cigarettes, e-cigarettes, and waterpipe smoking on endothelial function and clinical outcomes. Eur Heart J 2020, 41, 4057–4070. [Google Scholar] [CrossRef] [PubMed]
- Kane, A.E.; Howlett, S.E. Differences in Cardiovascular Aging in Men and Women. Adv Exp Med Biol 2018, 1065, 389–411. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of the study, indicating reference population by age decade, overall and by gender, subjects included and excluded, and the main causes of exclusion.
Figure 1.
Flow diagram of the study, indicating reference population by age decade, overall and by gender, subjects included and excluded, and the main causes of exclusion.
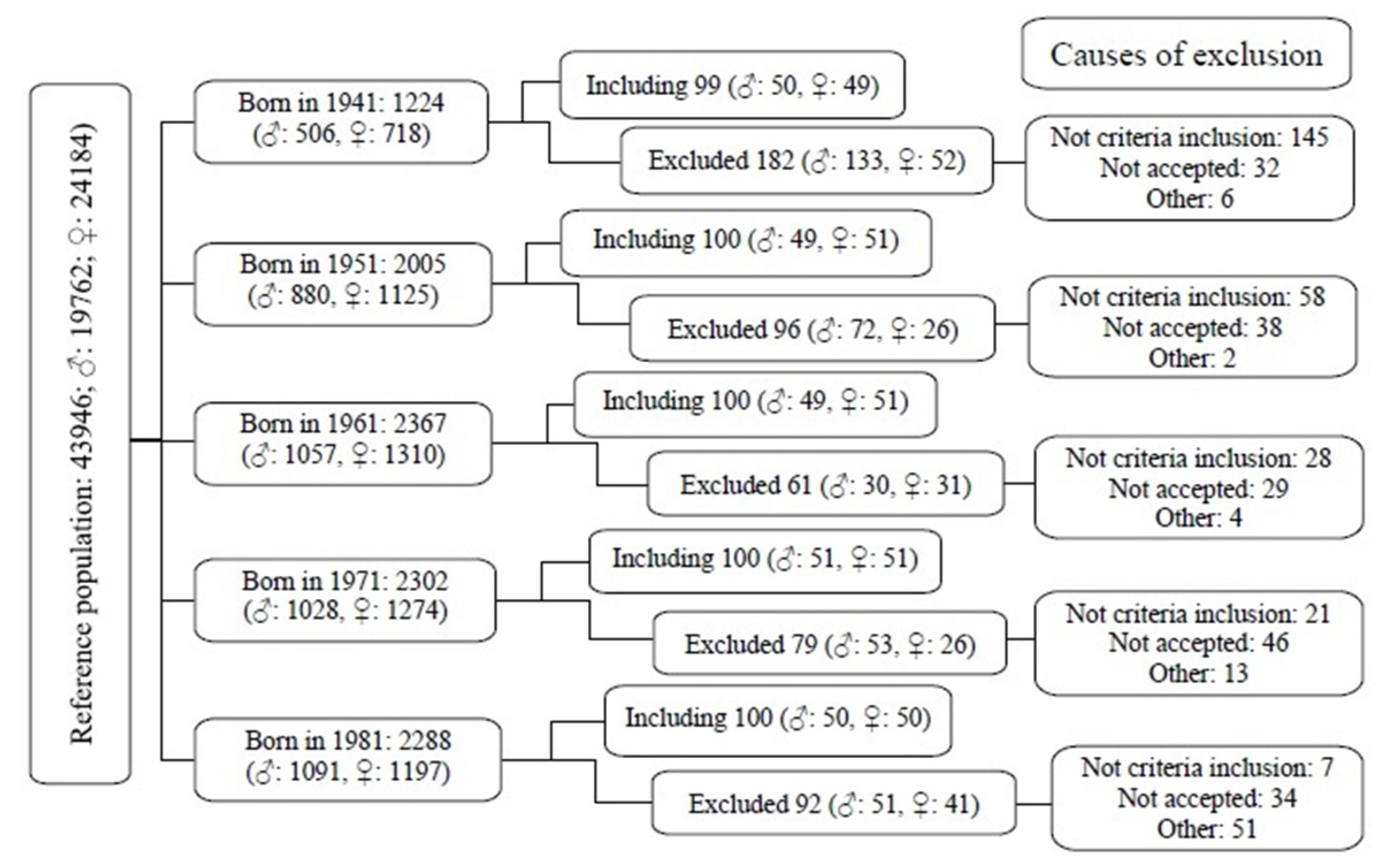
Figure 2.
Percentage of subjects overall according to the number of healthy lifestyles.
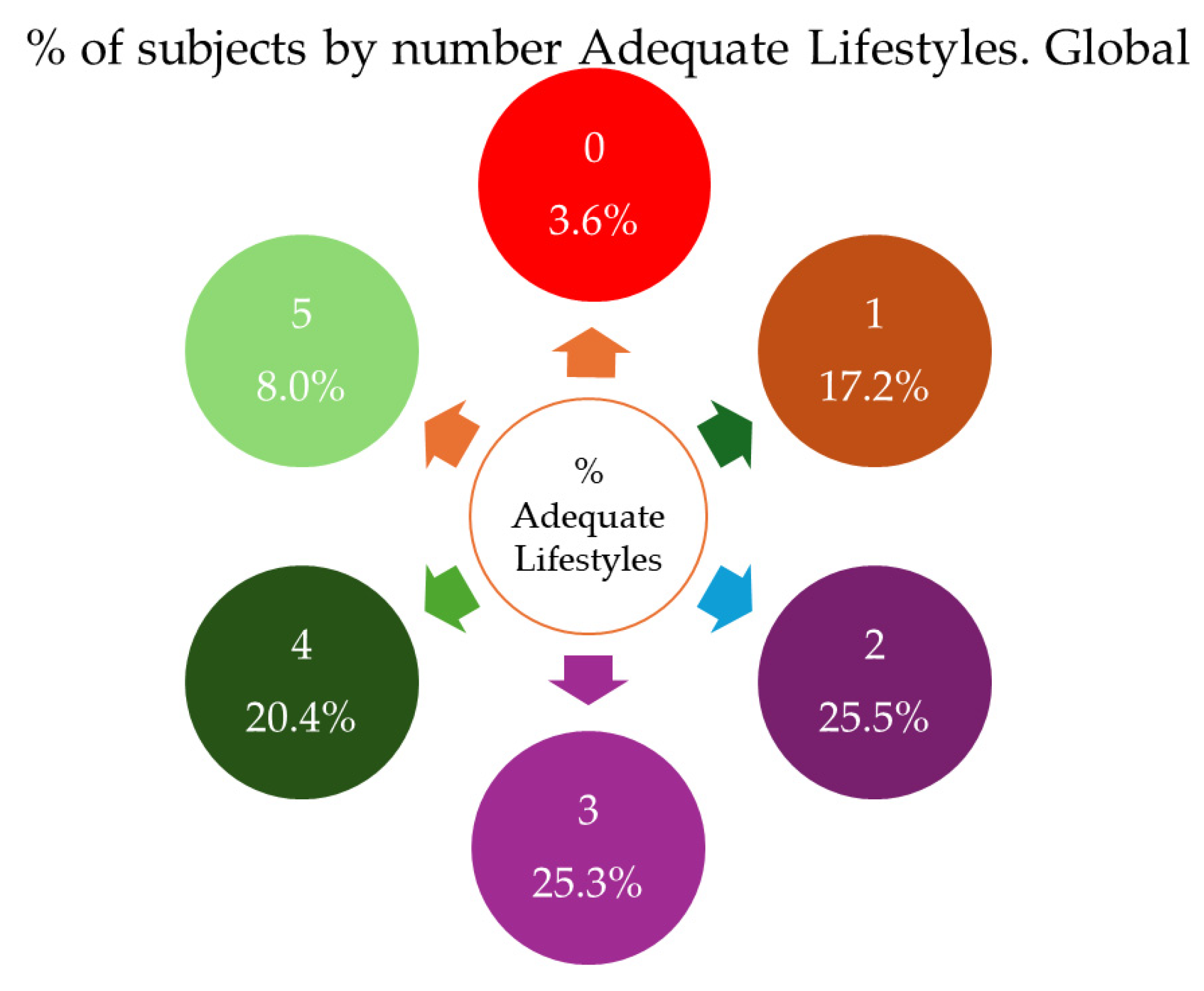
Figure 3.
Percentage of subjects by sex according to the number of healthy lifestyles.
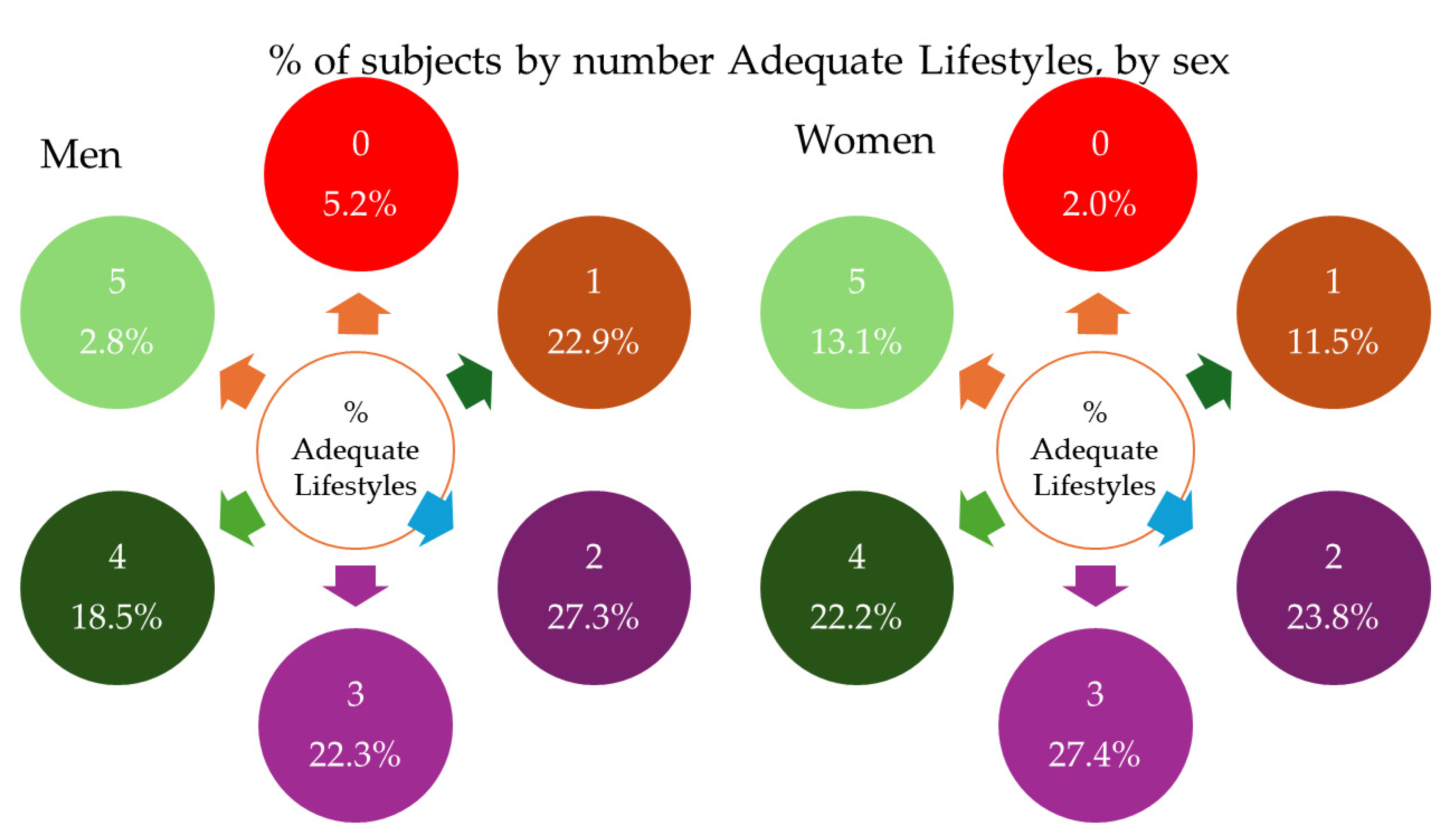
Figure 4.
Differences in VAI scores between subjects with and without healthy lifestyles, overall and by sex. MD, Mediterranean diet; AA, adequate alcohol consumption; PAT h/W, physical activity total hours/week; S h/W, sedentary hours per week; HL, number of healthy lifestyles; VAI, vascular aging index. Brown represents the overall results, blue the results for men and pink the results for women. *p<0.005.
Figure 4.
Differences in VAI scores between subjects with and without healthy lifestyles, overall and by sex. MD, Mediterranean diet; AA, adequate alcohol consumption; PAT h/W, physical activity total hours/week; S h/W, sedentary hours per week; HL, number of healthy lifestyles; VAI, vascular aging index. Brown represents the overall results, blue the results for men and pink the results for women. *p<0.005.
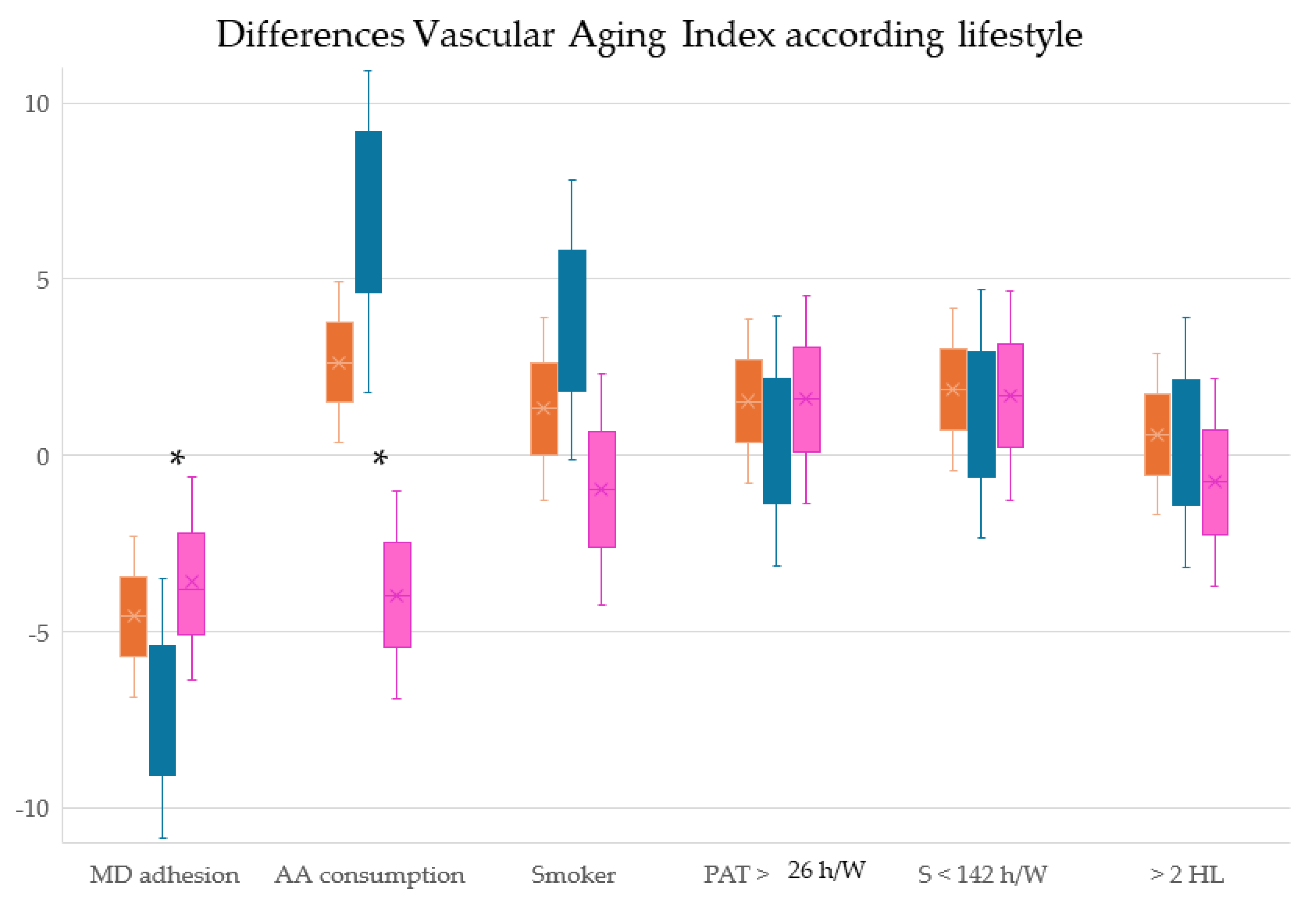

Table 1.
Lifestyles, Risk Factors, and Vascular Structure and Function of the subjects included in overall and by sex.
Table 1.
Lifestyles, Risk Factors, and Vascular Structure and Function of the subjects included in overall and by sex.
| Lifestyles | Global (501) | Men (249) | Women (252) | p value | |||
| Score the MD | 7.15 | ± 2.07 | 6.68 | ± 1.97 | 7.60 | ± 2.08 | <0.001 |
| Adherence to DM, n (%) | 214 | 42.7% | 89 | 35.7% | 125 | 49.6% | 0.001 |
| Alcohol consumption, (g/W) | 40.47 | ± 63.15 | 61.54 | ± 74.65 | 19.64 | ± 39.54 | <0.001 |
| Adequate alcohol consumption, n (%) | 251 | 50.1% | 94 | 37.8% | 157 | 62.3% | <0.001 |
| Years of smoking | 12.98 | ± 17.41 | 14.43 | ± 18.91 | 11.55 | ± 15.69 | 0.064 |
| Never smoked, n (%) | 367 | 73.3% | 183 | 73.5% | 184 | 73.0% | 0.920 |
| Total physical activity, (h/W) | 27.09 | ± 9.52 | 26.01 | ± 9.51 | 28.17 | ± 9.43 | 0.011 |
| More than 26 h/W, n (%) | 246 | 49.7% | 107 | 43.1% | 139 | 56.3% | 0.004 |
| Sitting Time, (h/W) | 140.75 | ± 9.56 | 141.78 | ± 9.57 | 139.72 | ± 9.45 | 0.017 |
| Less than 142 h/W, n (%) | 253 | 51.1% | 113 | 45.6% | 140 | 56.7% | 0.015 |
| Number of healthy lifestyles | 2.66 | ± 1.29 | 2.35 | ± 1.24 | 2.96 | ± 1.28 | <0.001 |
| More than 2 healthy lifestyles, n (%) | 253 | 50.5% | 102 | 41.0% | 151 | 59.9% | <0.001 |
| Conventional risk factors | |||||||
| Age (years) | 55.90 | ± 14.24 | 55.95 | ± 14.31 | 55.85 | ± 14.19 | 0.935 |
| Systolic blood pressure, (mmHg) | 120.69 | ± 23.13 | 126.47 | ± 19.52 | 114.99 | ± 24.96 | <0.001 |
| Diastolic blood pressure, (mmHg) | 75.53 | ± 10.10 | 77.40 | ± 9.38 | 73.67 | ± 10.46 | <0.001 |
| Mean arterial pressure, (mmHg) | 90.58 | ± 12.61 | 93.76 | ± 11.13 | 87.44 | ± 13.21 | <0.001 |
| Pulse pressure, (mmHg) | 45.17 | ± 19.81 | 49.06 | ± 16.68 | 41.31 | ± 21.83 | <0.001 |
| Hypertensive, n (%) | 147 | 29.3% | 82 | 32.9% | 65 | 25.8% | 0.095 |
| Antihypertensive, n (%) | 96 | 19.2% | 50 | 20.1% | 46 | 18.3% | 0.650 |
| Total-Cholesterol, (mg/dl) | 194.76 | ± 32.49 | 192.61 | ± 32.26 | 196.88 | ± 32.65 | 0.142 |
| LDL-Cholesterol, (mg/dl) | 115.51 | ± 29.37 | 117.43 | ± 30.12 | 113.61 | ± 28.54 | 0.148 |
| HDL-Cholesterol, (mg/dl) | 58.75 | ± 16.16 | 53.19 | ± 14.12 | 64.22 | ± 16.20 | <0.001 |
| Triglycerides, (mg/dl) | 103.06 | ± 53.20 | 112.28 | ± 54.40 | 93.95 | ± 50.46 | <0.001 |
| Atherogenic index | 3.53 | ± 1.07 | 3.84 | ± 1.12 | 3.24 | ± 0.93 | <0.001 |
| Dyslipidemic | 191 | 38.1% | 95 | ± 38.2% | 96 | 38.1% | 98.9% |
| Lipid-lowering, n (%) | 102 | 20.4% | 49 | 19.7% | 53 | 21.0% | 0.740 |
| Plasma glucose, (mg/dl) | 88.21 | ± 17.37 | 90.14 | ± 18.71 | 86.30 | ± 15.73 | 0.013 |
| HbA1c, (%) | 5.49 | ± 0.56 | 5.54 | ± 0.63 | 5.44 | ± 0.47 | 0.043 |
| Diabetes mellitus tipe 2, n (%) | 38 | 7.6% | 26 | 10.4% | 12 | 4.8% | 0.018 |
| Hypoglycemic, n (%) | 35 | 7.0% | 23 | 9.2% | 12 | 4.8% | 0.055 |
| Body mass index, (kg/m2) | 26.52 | ± 4.23 | 26.90 | ± 3.54 | 26.14 | ± 4.79 | 0.044 |
| Waist circumference (cm) | 93.33 | ± 12.01 | 98.76 | ± 9.65 | 87.93 | ± 11.70 | <0.001 |
| Obesity, n (%) | 94 | 18.8% | 42 | 16.9% | 52 | 20.6% | 0.304 |
| Abdominal obesity, n (%) | 193 | 38.6% | 78 | 31.3% | 115 | 45.8% | 0.001 |
| Structure. vascular function and aging | |||||||
| Intima Media Thickness. (mm) | 0.682 | ± 0.109 | 0.699 | ± 0.116 | 0.665 | ± 0.100 | 0.001 |
| cfPWV, (m/sec) | 6.53 | ± 2.03 | 6.86 | ± 2.20 | 6.21 | ± 1.79 | <0.001 |
| Vascular Aging Index | 61.23 | ± 12.86 | 63.47 | ± 13.75 | 59.04 | ± 11.54 | <0.001 |
The values are displayed as means ± standard deviations for continuous data and as number and proportions for categorical data. MD, mediterranean diet; g/W, grams/week; h/W, hours/week; LDL, low-density lipoprotein; HDL, high-density lipoprotein; HbA1c, glycosylated hemoglobin; cfPWV, femoral carotid pulse wave velocity. p: Differences between men and women.
Table 2.
Lifestyles, Risk Factors, and Vascular Structure and Function according to vascular aging.
| Lifestyles | HVA (94, 18.9%) | Non HVA (407, 81.1%) | p | ||
| Score the DM | 6.91 | ±2.20 | 7.20 | ±2.05 | 0.226 |
| Adherence to DM, n (%) | 33 | 35.1% | 180 | 44.6% | 0.106 |
| Alcohol consumption, (g/W) | 34.89 | ±57.99 | 41.94 | ±64.46 | 0.331 |
| Adequate alcohol consumption, n (%) | 47 | 50.0% | 202 | 50.0% | 1.000 |
| Years of smoking | 12.45 | ±15.41 | 12.90 | ±17.70 | 0.820 |
| Never smoked, n (%) | 65 | 69.1% | 299 | 67.0% | 0.037 |
| Total physical activity, (h/W) | 29.19 | ±9.79 | 26.58 | ±9.41 | 0.017 |
| More than 26 h/W, n (%) | 56 | 60.2% | 188 | 47.1% | 0.028 |
| Sitting Time, (h/W) | 138.57 | ±9.81 | 141.28 | ±9.44 | 0.014 |
| Less than 142 h/W, n (%) | 57 | 61.3% | 194 | 48.6% | 0.029 |
| Number of healthy lifestyles | 2.74 | ±1.20 | 2.63 | ±1.32 | 0.444 |
| More than 2 healthy lifestyles, n (%) | 57 | 60.6% | 195 | 48.3% | 0.039 |
| Conventional risk factors | |||||
| Age (years) | 52.64 | ±13.29 | 56.66 | ±14.34 | 0.010 |
| Systolic blood pressure, (mmHg) | 109.59 | ±12.61 | 123.32 | ±24.28 | <0.001 |
| Diastolic blood pressure, (mmHg) | 71.10 | ±8.28 | 76.56 | ±10.24 | <0.001 |
| Mean arterial pressure, (mmHg) | 83.93 | ±9.00 | 92.14 | ±12.87 | <0.001 |
| Pulse pressure, (mmHg) | 38.48 | ±8.90 | 46.76 | 21.30 | <0.001 |
| Hypertensive, n (%) | 0 | 0.0% | 147 | 36.4% | <0.001 |
| Antihypertensive, n (%) | 0 | 0.0% | 96 | 19.3% | <0.001 |
| Total-Cholesterol, (mg/dl) | 193.27 | ±32.39 | 194.95 | ±32.50 | 0.651 |
| LDL-Cholesterol, (mg/dl) | 113.42 | ±28.02 | 115.87 | ±29.72 | 0.469 |
| HDL-Cholesterol, (mg/dl) | 62.42 | ±18.00 | 57.85 | ±15.62 | 0.014 |
| Triglycerides, (mg/dl) | 83.33 | ±32.99 | 107.66 | ±55.97 | <0.001 |
| Atherogenic index | 3.32 | ±1.09 | 3.59 | ±1.06 | 0.027 |
| Dyslipidemic | 29 | 30.9% | 160 | 39.6% | 0.126 |
| Lipid-lowering, n (%) | 13 | 13.8% | 88 | 21.8% | 0.086 |
| Plasma glucose, (mg/dl) | 83.41 | ±10.27 | 89.41 | ±18.49 | <0.001 |
| HbA1c, (%) | 5.30 | ±0.29 | 5.53 | ±0.59 | <0.001 |
| Diabetes mellitus tipo 2, n (%) | 0 | 0.0% | 38 | 9.4% | 0.002 |
| Hypoglycemic, n (%) | 0 | 0.0% | 35 | 7.0% | 0.003 |
| Body mass index, (kg/m2) | 24.43 | ±3.26 | 27.00 | ±4.29 | <0.001 |
| Waist circumference (cm) | 88.48 | ±9.41 | 94.45 | ±12.28 | <0.001 |
| Obesity, n (%) | 6 | 6.4% | 88 | 21.8% | 0.001 |
| Abdominal obesidad, n (%) | 21 | 22.3% | 171 | 42.4% | <0.001 |
| Structure. vascular function and aging | |||||
| Intima Media Thickness. (mm) | 0.62 | ±0.08 | 0.70 | ±0.11 | <0.001 |
| cfPWV, (m/sec) | 4.83 | ±0.75 | 6.93 | ±2.02 | <0.001 |
| Vascular Aging Index | 50.51 | ±5.67 | 63.74 | ±12.78 | <0.001 |
The values are displayed as means ± standard deviations for continuous data and as number and proportions for categorical data. MD, mediterranean diet; g/W, grams/week; h/W, hours/week; LDL, low-density lipoprotein; HDL, high-density lipoprotein; HbA1c, glycosylated hemoglobin; HVA, healthy vascular aging; cfPWV, femoral carotid pulse wave velocity. p: Differences between HVA and non HVA.
Table 3.
Correlation between index vascular aging and lifestyles.
| VAI | Global (501) | Men (249) | Women (251) |
|---|---|---|---|
| Score the MD | -0.102* | -0.082* | 0.058 |
| Alcohol consumption,g/W | 0.228** | 0.221** | -0.040 |
| Year smoking | 0.092* | 0.105 | 0.010 |
| Total physical activity, (h/W) | -0.158* | -0.120 | -0.161* |
| Sitting Time, (h/W) | 0.165** | 0.135* | -0.162* |
| Number of healthy lifestyles | -0.199** | -0.197** | -0.063 |
Correlation de Pearson Age-adjusted. MD, Mediterranean diet; g/W, grams/week; VAI, Vascular Aging Index. Pearson Coefficient. * p < 0.05; ** p < 0.01.
Table 4.
Asociation between vascular aging and lifestyles. Multiple Regression Analysis.
| VAI | β | (IC | 95%) | p |
| Global | ||||
| Score the DM | -0.056 | -0.418 | to 0.307 | 0.763 |
| Alcohol consumption,g/W | 0.020 | 0.008 | to 0.032 | 0.001 |
| Year smoking | 0.028 | -0.013 | to 0.069 | 0.185 |
| Total physical activity, (h/W) | -0.102 | -0.176 | to -0.028 | 0.007 |
| Sitting Time, (h/W) | 0.109 | 0.036 | to 0.183 | 0.004 |
| Number of healthy lifestyles | -0.640 | -1.195 | to -0.086 | 0.024 |
| Men | ||||
| Score the MD | -0.044 | -0.598 | to 0.509 | 0.875 |
| Alcohol consumption,g/W | 0.020 | 0.005 | to 0.034 | 0.008 |
| Year smoking | 0.045 | -0.014 | to 0.103 | 0.133 |
| Total physical activity, (h/W) | -0.096 | -0.203 | to 0.011 | 0.080 |
| Sitting Time, (h/W) | 0.108 | 0.001 | to 0.214 | 0.048 |
| Number of healthy lifestyles | -1.054 | -1.741 | to -0.367 | 0.003 |
| Women | ||||
| Score the MD | -0.010 | -0.459 | to 0.439 | 0.965 |
| Alcohol consumption,g/W | -0.005 | -0.027 | to 0.018 | 0.690 |
| Year smoking | -0.023 | -0.080 | to 0.033 | 0.416 |
| Total physical activity, (h/W) | -0.099 | -0.195 | to -0.002 | 0.044 |
| Sitting Time, (h/W) | 0.099 | 0.195 | to 0.003 | 0.043 |
| Number of healthy lifestyles | -0.256 | -0.820 | to 0.309 | 0.373 |
Multiple regression: dependent variables (estimated Vascular Aging with VAI). Lifestyle independent variables. Adjustment variables: age, mean arterial pressure, atherogenic index, body mass index, and glycosolated hemoglobin. MD, Mediterranean diet; g/W, grams/week; VAI, Vascular Aging Index.
Table 5.
Asociation between healthy vascular aging and lifestyles. Logistics Regression Analysis.
| VAI | OR | (IC | 95%) | p |
| Global | ||||
| MD adhesion | 0.571 | 0.333 | to 0.981 | 0.042 |
| AA consumption | 0.993 | 0.606 | to 1.627 | 0.977 |
| Smoker | 0.648 | 0.375 | to 1.119 | 0.119 |
| PAT > 26 h/W | 1.735 | 1.048 | to 2.871 | 0.032 |
| ST - 142 h/W | 1.696 | 1.025 | to 2.805 | 0.040 |
| > 2 HL | 1.877 | 1.123 | to 3.136 | 0.016 |
| Men | ||||
| MD adhesion | 0.413 | 0.170 | to 1.004 | 0.051 |
| AA consumption | 0.852 | 0.425 | to 1.708 | 0.653 |
| Smoker | 0.382 | 0.162 | to 0.902 | 0.028 |
| PAT > 26 h/W | 1.825 | 0.878 | to 3.793 | 0.107 |
| ST - 142 h/W | 1.738 | 0.838 | to 3.604 | 0.136 |
| > 2 HL | 1.998 | 0.956 | to 4.175 | 0.066 |
| Women | ||||
| MD adhesion | 0.766 | 0.377 | to 1.558 | 0.462 |
| AA consumption | 0.968 | 0.465 | to 2.014 | 0.931 |
| Smoker | 0.812 | 0.381 | to 1.731 | 0.589 |
| PAT > 26 h/W | 1.668 | 0.817 | to 3.404 | 0.160 |
| ST - 142 h/W | 1.655 | 0.810 | to 3.379 | 0.167 |
| > 2 HL | 1.769 | 0.848 | to 3.692 | 0.128 |
Multiple regression: dependent variables (estimated Vascular Aging with VAI). Lifestyle independent variables. Adjustment variables: age, mean arterial pressure, atherogenic index, body mass index, and glycosolated hemoglobin. MD, Mediterranean diet; g/W, grams/week; AA consumption, Adequate alcohol consumption; PAT H/W, Physical activity total hours/week; ST H/W, Sitting hours per week; HL, Number of healthy lifestyles; VAI, Vascular Aging Index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



