
Submitted:
16 July 2024
Posted:
17 July 2024
You are already at the latest version
Abstract
The issue of antibiotic resistance represents a significant threat that extends beyond human health, encompassing animal welfare and the sustainability of the natural environment. The inappropriate use of antibiotics, poor sanitation and inadequate control measures, have contributed to the emergence of drug-resistant bacteria, which can spread at the human-animal-environment interface. The documented presence of antimicrobials in agriculture, veterinary medicine and human medicine has convinced all stakeholders of the need to contribute to the development of a "One Health" approach, which recognises the interrelationships between animals, humans and their environment and the need to adopt a common strategy encompassing these sectors to limit the spread of antimicrobial resistance (AMR). Although a number of countries have implemented integrated surveillance systems to monitor antibiotic use and antimicrobial resistance, available data suggest that the use of antibiotics in humans, animals and the environment is increasing worldwide. Consequently, the emergence of antibiotic-resistant pathogens is becoming a recurring concern. This review provides a comprehensive overview of the measures that are necessary to be taken and implemented in order to guarantee global health security.
Keywords:
Antibiotic Resistance
; Infection Control
; One Health Solution
1. Introduction
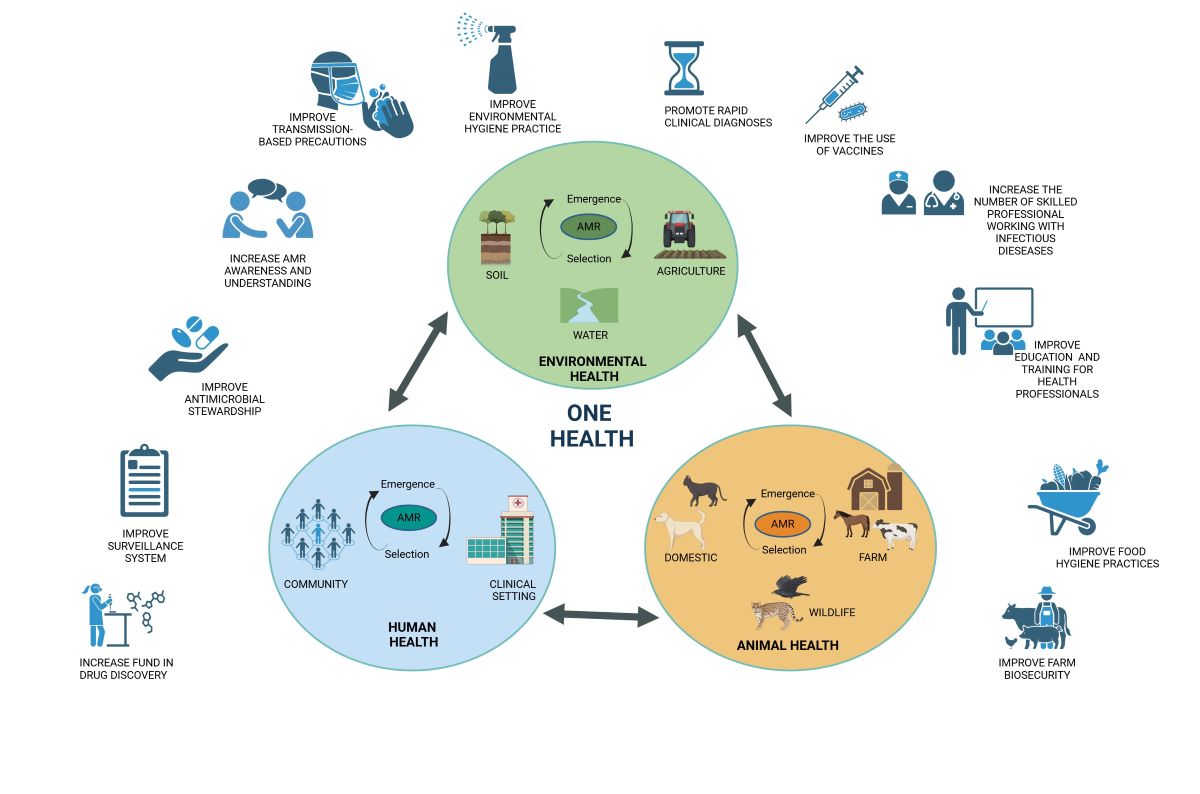
The phenomenon of globalisation, in conjunction with the intensified frequency of global trade and migration, in addition to climate and environmental change, has enabled the emergence, re-emergence, and spread of novel or previously existing infectious diseases caused by microorganisms, often antibiotic-resistant, at a planetary scale [1,2]. The emergence of antibiotic resistance in microbial populations represents a significant threat to both animal and human health and environmental sustainability [3]. The overuse of antibiotics in humans, animals and the environment, in conjunction with the global dissemination of bacterial resistance genes, represents a significant contributing factor in the emergence and dissemination of antibiotic-resistant bacteria [4,5]. In humans, antibiotics are employed for two primary purposes: the treatment of bacterial infections and the prevention of illnesses [6]. The former is referred to as "therapeutic" use, whereas the latter is designated as "prophylactic" use. The latter is particularly prevalent prior to bowel and orthopaedic surgery [7]. The mechanism of action of antibiotics involves either the killing of bacteria or the prevention of their proliferation [8]. Antibiotic resistance occurs when bacteria cease to respond to the antimicrobial agent designed to kill them [4]. It is evident that the inappropriate prescription of antibiotics is a significant contributing factor to the rising incidence of resistance. The prescription of incorrect medication, whether as a result of error or deliberate action, has the potential to facilitate the misuse of antibiotics [9]. Furthermore, the previous Coronavirus Disease 2019 (Covid-19) pandemic has heightened this risk due to the extended periods of hospitalization in the intensive care unit (ICU), high mortality rates, uncertainty surrounding the diagnosis and prognosis, and concerns about potential secondary bacterial infections [10,11]. Consequently, the routine empirical use of antibiotics, frequently in conjunction with other pharmaceutical agents, has become a prevalent approach for the prevention of infection [11]. Furthermore, the administration of antibiotics in an inappropriate dosage can result in ineffective therapeutic outcomes and recurrent infections, which in turn may necessitate a greater reliance on antibiotics [12]. Additionally, poor hygiene and inadequate sanitation in public settings contribute to the global burden of antimicrobial resistance (AMR). The failure to implement effective infection prevention and control practices in healthcare facilities allows the persistence of resistant microbes and their dissemination [13]. The transfer of pathogens between patients and healthcare workers via hand contact or from the hospital environment has been demonstrated to increase the risk of transmission in hospitals [12,14]. The administration of antimicrobial agents to animals destined for human consumption serves several purposes, including the acceleration of growth, the prevention of illness, and the treatment of infected animals [15]. The environment is subject to a considerable influx of antibiotics from a multitude of sources, including human excretion products, veterinary waste and effluents from farming operations [16]. The extensive use of antibiotics in livestock rearing may result in contamination of the agroecosystem via the application of contaminated manure as a fertiliser and irrigation of crops with wastewater [17,18]. Soil and freshwater act as reservoirs for genes encoding the production of antibiotics [19]. Furthermore, the presence of a diverse range of bacteria in these environments, which are naturally capable of producing antibiotics, is a further contributing factor [13]. Additionally, the application of natural fertilisers to agricultural fields contributes to the presence of antibiotics in the environment [20]. It is evident that the contamination of the environment with antibiotics represents a significant public health concern, given their potential for altering the composition and function of the human microbiome, thereby selecting for the proliferation of antibiotic-resistant bacteria [21]. A comprehensive examination of the interconnections between human, animal, and environmental health reveals that antibiotic-resistant bacteria exist in these three domains in ways that are intricately related and mutually influencing [22]. This phenomenon is frequently referred to as the ‘One Health Triangle’ [23]. To effectively address the issue of antibiotic-resistant bacteria, it is essential to adopt a comprehensive approach that integrates rigorous antibacterial resistance (ABR) surveillance across different sectors and levels [23]. It is therefore recommended that such an approach be implemented at both the national and international levels, with individual and combined surveillance measures being considered. The implementation of the One Health approach has the potential to halt the further spread of antibiotic resistance and to facilitate the achievement of enhanced global health outcomes [23,24]. This review emphasises the necessity of maintaining the continued efficacy of existing antimicrobial agents by eradicating inappropriate utilisation. Given the interdependent human, animal, and environmental dimensions of antimicrobial resistance, a One Health perspective is imperative for the regulation of antibiotic resistance, which must encompass improvements in surveillance, stewardship, infection control and sanitation.
2. The Mechanisms of Antibiotic Resistance in Bacteria
The treatment of bacterial infections and the subsequent prevention of further infections became possible with the advent of antibiotics [6]. The development and subsequent therapeutic use of antibiotics represents a major advance in the history of medicine. The mechanisms by which antibiotics exert their antibacterial effects can be broadly divided into five categories: inhibition of cell wall synthesis, inhibition of protein synthesis, disruption of cell membrane integrity, inhibition of nucleic acid synthesis and antimetabolite activity [25] (Table 1).
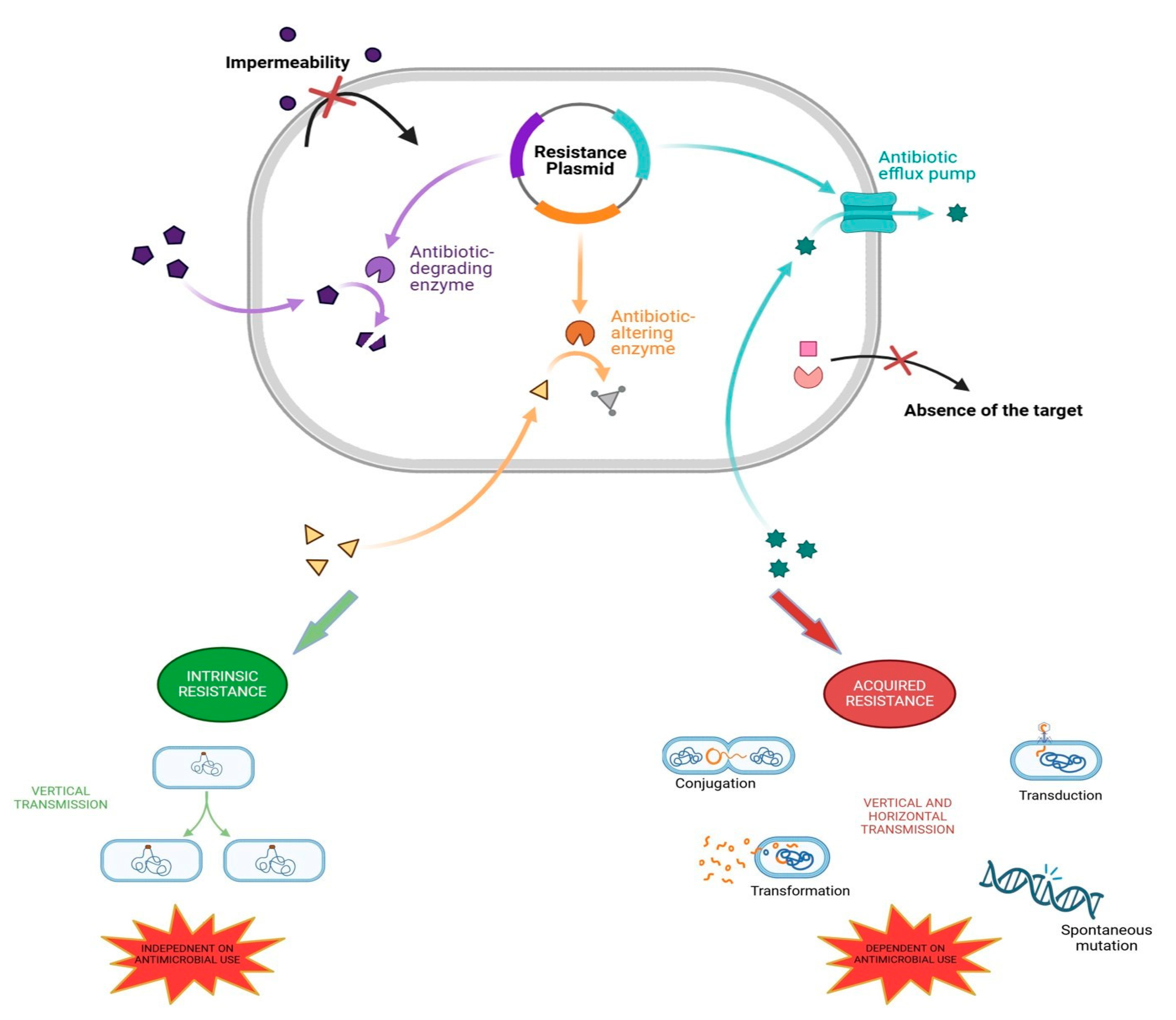
Bacteria are capable of evolving in response to external stimuli in order to ensure their continued existence. This in vivo process is underpinned by a number of key biological processes, including adaptation, reproduction and the spread of bacteria [26]. In the event that a bacterium is unable to proliferate due to the presence of an antibiotic, it may undergo genetic modifications that render it immune to the medication, thus allowing it to survive [27]. This phenomenon, which can be described as antibiotic resistance, represents the natural process whereby bacteria develop drug resistance. Consequently, antibiotic resistance can be defined as the capacity of bacteria to withstand the impact of an antibiotic to which they were previously susceptible, allowing them to survive and thrive [28]. AMR represents a fundamental and inevitable consequence of evolutionary processes whereby microorganisms develop genetic mutations to mitigate the lethal effect of antibiotics [29]. This phenomenon may be attributed to the ancient and continuously evolving mechanisms of resistance that are linked to the continuous competitive interaction between microorganisms for resources [30]. Environmental organisms that produce antibiotics (analogous to those currently employed in pharmaceuticals) as secondary metabolites have evolved a mechanism to protect themselves from the toxic effects of these molecules. Similarly, the microbial organisms that populate specific niches within the ecosystem must also undergo co-evolutionary processes in order to survive and compete for resources [31]. A wide range of studies have tested the existence of resistance genes in isolated caves, permafrost cores and other natural environments that have remained undisturbed by human activity. These studies have demonstrated that the presence of these resistance mechanisms pre-dates the introduction of antibiotics into clinical practice. A significant change since the introduction of antibiotics has been the notable increase in the selection of mobile resistance elements, which has consequently led to the proliferation of drug-resistant pathogenic and non-pathogenic bacteria [31,32]. Two distinct mechanisms of resistance have been observed in bacteria that allow them to withstand the effects of antibiotics, namely intrinsic and acquired resistance. The term "intrinsic resistance" (also known as "innate" or "natural" resistance) is used to describe the inherent or natural resistance of bacteria to antimicrobial agents [33]. The term "intrinsic resistance" is used to describe a characteristic that is inherent to a bacterial species and is not influenced by prior antibiotic exposure or the genetic resistance reservoir in other species [34]. Gram-negative bacteria have an outer membrane that acts as a barrier to antibiotics [35]. Proteus spp., Morganella morganii, Pseudomonas mallei, Chromobacterium spp., Burkholderia cepacia and Serratia marcescens are all naturally resistant to colistin due to the constitutively expression of arnBCADTEF operon and eptB gene, which results in surface modifications of the outer membrane lipopolysaccharide structure and its reduced affinity for the drug [36]. Acquired resistance mechanisms are based on chromosomal mutations or the acquisition of mobile resistance genes, which enable bacteria to obtain the ability to resist the activity of a particular antimicrobial agent to which they were previously susceptible [34]. Acquired resistance is a consequence of the evolutionary process whereby microorganisms adapt to the presence of antibiotics. This adaptation occurs through a number of mechanisms that are associated with the presence of mobile genetic elements such as plasmids, transposons and other mobile elements, capable of transmitting horizontally between bacteria [34]. The phenomenon of horizontal gene transfer (HGT) has emerged as a key driver in the rapid acquisition and dissemination of antibiotic resistance genes among bacteria. This process is mediated by three main mechanisms: transformation, conjugation and transduction. Conjugative plasmids, in particular, have a broad host range and are capable of transferring antibiotic resistance genes (ARGs) between different genera, orders and phyla, thereby contributing to the wider spread of resistance genes [37]. Plasmid-mediated horizontal gene transfer (HGT) is a common occurrence in environments with a high bacterial load, including soil, wastewater treatment plants, and the gut microbiomes of humans and animals [38]. This approach would permit the mobilisation of reservoirs of ARGs from commensal or environmental bacteria to pathogenic ones and vice versa, as well as the acquisition and dissemination of AMR genes within and between bacteria from the human, animal and environmental sectors [39]. The aforementioned mechanisms encompass enzymatic inactivation, a reduction in cellular accumulation of the agent in question, and the modification of cellular targets. The activation of these mechanisms is contingent upon the presence of mobile genetic elements, which include plasmids, transposons and other mobile genetic elements. A variety of cases of acquired antibiotic resistance have been observed, including methicillin-resistant Staphylococcus aureus (MRSA) and trimethoprim-resistant Haemophilus influenzae.
Figure 1.
Mechanism of antibiotic resistance. The initial section of the figure depicts the principal strategies for circumventing the effects of antimicrobial agents, including those that are chromosome- and plasmid-mediated, and belonging to the categories of innate and acquired resistance. The two principal categories of resistance are outlined below. Intrinsic resistance is taxon-specific, independent of previous antibiotic exposure and only vertically transmitted. Acquired resistance, on the other hand, consists of the acquisitions of external ARGs through HGT (conjugation, transformation, transduction) or spontaneous mutations. It can be transmitted either vertically or horizontally and is influenced by antibiotic exposure.
Figure 1.
Mechanism of antibiotic resistance. The initial section of the figure depicts the principal strategies for circumventing the effects of antimicrobial agents, including those that are chromosome- and plasmid-mediated, and belonging to the categories of innate and acquired resistance. The two principal categories of resistance are outlined below. Intrinsic resistance is taxon-specific, independent of previous antibiotic exposure and only vertically transmitted. Acquired resistance, on the other hand, consists of the acquisitions of external ARGs through HGT (conjugation, transformation, transduction) or spontaneous mutations. It can be transmitted either vertically or horizontally and is influenced by antibiotic exposure.
3. Reasons behind Antimicrobial Resistance
The potential dangers associated with the use of antibiotics have been identified since their initial clinical introduction in the 1940s. Since that time, their use and consequently their inappropriate utilisation has increased to a considerable extent [6]. The emergence of penicillin-resistant S. aureus in 1942, following the extensive utilization of penicillin as an antibiotic the previous year, represents a significant example of the impact of the inappropriate use of antibiotics [6]. In the following years, the prevalence of infections caused by penicillin-resistant S. aureus, which had initially been confined to hospitals, began to spread rapidly throughout the community [40]. By the 1960s, more than 80% of both community- and hospital-acquired strains of Staphylococcus aureus exhibited resistance to penicillin [40]. A similar de facto scenario was observed with the introduction of methicillin (a semi-synthetic β-lactam), which was commercialised in 1959 in order to circumvent the growing penicillin resistance observed in S. aureus [41]. These methicillin-resistant strains (MRSA) harbour an altered penicillin-binding protein, designated PBP-2a, which exhibited a reduced affinity for penicillin, thereby conferring resistance to penicillin. The gene mecA, located on the mobile genomic island SCCmec (staphylococcal cassette chromosome mec), is responsible for encoding PBP-2a [41]. Furthermore, Streptococcus pneumoniae and Neisseria gonorrhoeae exhibited a rapid development of resistance to penicillin [42]. In the subsequent decades, a notable advancement was made in the field of antibiotic development with the identification of two antibiotic classes that have become indispensable in combating antibiotic-resistant pathogens. These include the quinolones and vancomycin [43]. The former has a broad spectrum of activity, while the latter is highly active against methicillin-resistant Staphylococcus aureus. Other antibiotics that have addressed bacterial resistance include macrolides, third-generation cephalosporins, daptomycin and linezolid. Nevertheless, despite these advances, the problem of antibiotic resistance remains a significant challenge [6]. An increasing number of bacterial strains are exhibiting resistance to a multitude of antibiotics, thereby reducing their efficacy in combating infection. This has led to an increase in hospitalisations, higher costs for healthcare providers, and an elevated mortality rate [4]. One of the most significant challenges in the global effort to address the growing threat of antibiotic resistance is the slow pace of new antibiotic development. The lengthy and costly process of developing these drugs and the low profitability of these drugs are two of the factors that have led to this situation [13]. Furthermore, significant challenges associated with antibiotic resistance include the unnecessary and inappropriate use of antibiotics. The utilisation of antimicrobial agents in the context of agricultural production and animal husbandry serves to exacerbate the dissemination of antibiotic resistance. Such practices are particularly evident in instances such as the administration of antimicrobial agents as growth promoters in livestock, which has the potential to transfer antibiotic resistance to humans through the food chain [33].
4. Tackling Antibiotic Resistance with a One Health Approach
The 21st century presents novel challenges for the healthcare sector. While medical technology has advanced considerably, it also presents a number of issues that require attention. Among these issues, antibiotic resistance represents a significant concern, as we are now witnessing the emergence of numerous infectious agents that have developed resistance to a multitude of antimicrobial agents [29]. It is becoming increasingly evident that the abuse and overuse of antimicrobial agents in human, veterinary and agricultural medicine have led to the current state of affairs, given that the lack of containment measures for AMR in one area has an indirect impact in others [4]. In light of the aforementioned considerations, it becomes evident that the phenomenon of resistance can only be effectively addressed through a multi-faceted and comprehensive approach, such as One Health, at various levels (local, national, and global), in order to achieve optimal health outcomes for people, animals, and the environment [15]. In contrast to previous research, which focused on human pathogenic bacteria as the primary subject of medical investigation with the objective of controlling infectious diseases, the discovery of environmental ARGs genetically similar to clinical ones has led to a significant shift in the field of medical research. This has provided a more comprehensive understanding of this phenomenon, encouraging the study of genes from both pathogenic and non-pathogenic bacteria, as well as those from commensal and environmental bacteria, and the dynamics involved in the continuous evolution of AMR [18,28]. The introduction of metagenomic analysis and the recognition of the value of descriptive genetic studies have paved the way for the proposal of the concept of resistome. This is defined as the totality of all resistance genes and their precursor elements present in pathogenic and non-pathogenic bacteria. The resistome concept and its investigation in the environment, humans and animals have yielded significant insights into the prevalence, intricacy and heterogeneity of antimicrobial resistance, underscoring the interconnectivity between the One Health sectors [44]. The concept of 'One Health' confers benefits to human and animal health in two distinct ways. Primarily, it ensures that the health of humans and animals is considered holistically. Secondly, it results in significant financial savings in the areas of disease treatment and control. This is achieved through the promotion of interdisciplinary and transdisciplinary collaborations between the disciplines of human and veterinary medicine, in addition to other natural sciences [45]. The One Health approach represents a more expansive conceptualisation of the concept of health, extending the original concept of ‘one medicine’ to encompass ‘one health’ [46]. The term 'One Medicine' was first proposed by Dr Calvin Schwabe in the 1960s. It was based on the close relationship between humans, domestic animals and public health. As evidenced by numerous studies, humans and animals not only share the same environment but also numerous infectious diseases [15]. Furthermore, it has been estimated that up to 75% of human infectious diseases that have arisen or re-emerged in recent decades are zoonotic [47]. A 2020 investigation into the prevalence of schistosomiasis in schoolchildren and cows in Côte d’Ivoire revealed a previously unidentified high proportion of hybrid forms between animal (Schistosoma bovis) and human (Schistosoma haematobium) parasites in humans [48]. This serves to illustrate the manner in which a zoonosis can emerge when there is unrestricted contact between humans and animals. Although the observation of relationships between animal and human disease processes has a history spanning several decades, the One Health approach only achieved political recognition on a global scale in the early 2000s. In 2009, an ad hoc office was established at the Centers for Disease Control and Prevention (CDC). In 2010, the Hanoi Declaration, published subsequent to the International Ministerial Conference on Avian and Pandemic Influenza held in Hanoi, recommended the implementation of the One Health approach on a broad scale. This was subsequently endorsed by 71 countries [49]. In the context of the global pandemic caused by the SARS-CoV-2 virus, the role and activities of the United Nations Environment Programme (UNEP) underwent a significant expansion in close collaboration with the World Health Organization (WHO), the Food and Agriculture Organization of the United Nations (FAO), and the World Organization for Animal Health (WOAH) [50]. In 2021, the aforementioned organisations entered into a memorandum of understanding, thereby establishing themselves as the Quadripartite Alliance. The objective of the Quadripartite Alliance is to collaborate in order to address the impact of current health challenges. In 2022, the Alliance published the Strategic Framework for Collaboration on Antimicrobial Resistance, which sets out the objective of "preserving antimicrobial efficacy and ensuring sustainable and equitable access to antimicrobials for responsible and prudent use in human, animal and plant health, contributing to achieving the Sustainable Development Goals (SDGs)” [51]. The One Health approach offers a promising avenue for the containment of antimicrobial resistance, provided that an interdisciplinary approach is implemented. For example, the source of zoonoses can be more rapidly identified when humans and animals are examined in conjunction with one another. The most effective method of controlling and ultimately eradicating zoonotic diseases such as brucellosis and rabies is to shift the focus from treating affected individuals to containing the diseases in reservoir animals [52]. All joint actions against diseases, in particular those caused by antibiotic-resistant microorganisms, must be founded upon the principle of prevention. In order to prevent the overpopulation of ecosystems and the subsequent outbreak of disease, it is essential to implement effective surveillance systems that facilitate multidisciplinary and intersectoral cooperation [24]. The concept of One Health postulates that a holistic approach to understanding health must be adopted, encompassing both the impact of human actions within human-environmental systems and the interconnectivity of all life on a planetary scale [41]. In addition, the concept of One Health serves to facilitate and encourage collaboration between scientific experts and government authorities, with the objective of achieving a more nuanced understanding of the circumstances under consideration and, consequently, the adoption of more effective actions that are endorsed by all relevant stakeholders [42]. This, in turn, ensures a more enduring and comprehensive impact. The realisation that human, animal and ecosystem health are inextricably linked has prompted a significant shift in thinking regarding the management and achievement of these goals.
5. Antimicrobial Use in Food Animals and Human Health
The animal sector plays a pivotal role in the global effort to combat antimicrobial resistance. The optimal use of veterinary drugs is defined as a strategy that maximises their therapeutic efficacy while simultaneously limiting the emergence of resistance. Since their introduction in the field of veterinary medicine in the 1950s, antimicrobial drugs have consistently constituted a pivotal instrument for the management of infectious diseases among animals [53]. These molecules are of significant value in the treatment of human illness, with a long history of use in the field of medicine. Nevertheless, their prophylactic use is currently restricted to post-surgical applications or the prevention of meningococcal disease. In the field of animal medicine, these drugs have frequently been administered to healthy animals for decades. Nevertheless, the advantages were soon outweighed by the recognition of numerous disadvantages. The continued use of antibiotics can select for bacterial resistance, can mask poor breeding practices, and can facilitate the spread of drug-resistant bacterial infections, which represents a significant global health threat [54]. Antibiotics are commonly used in pigs for the prevention of weaning diarrhoea, in cattle for the prevention of mastitis during the non-lactation period and in the poultry industry for respiratory infections. Practices such as metaphylaxis or prophylaxis are therefore common for the maintenance of health and productivity [55]. In veterinary medicine, metaphylaxis is the administration of antimicrobials to groups of animals at elevated risk of infection, in the absence of clinical signs of disease. Group-level treatments are defined as therapeutic when clinical infections are observed in at least some of the animals in the flock, and as prophylactic when there are no sick animals present, but the animals are at high risk of clinical bacterial infection due to unsanitary or crowded conditions [56]. Today, however, it is unacceptable to allow these treatments as standard practice. They should be reserved for exceptional cases and under close veterinary supervision. The problem of antibiotics in animals is also closely linked to intensive livestock farming. In order to easily meet the ever-increasing demand for animal protein, intensive production systems have been adopted worldwide, in which thousands of animals are kept in a confined space. Overcrowding can lead to the rapid spread of pathogenic (or potentially pathogenic) micro-organisms that can infect farm animals [57]. The practice of using antibiotics for the purpose of promoting growth in food animals has been the subject of considerable controversy. In contrast to the treatment of sick animals, this approach involves the long-term administration of low doses of antimicrobials to food animals with the aim of promoting growth. The administration of antimicrobials to entire groups of animals for prolonged periods at subtherapeutic doses has the potential to select and spread resistant bacteria within animal populations and humans through food or other environmental pathways [58]. The period of exposure is usually longer than two weeks and often extends throughout the life of the animal, as in the case of chickens exposed to antimicrobials for 36 days. It is unwise to use antimicrobials extensively for economic reasons alone when it is clear that such use selects for antimicrobial resistance [59]. It has been argued that the use of antimicrobial growth promoters is a means of compensating for poor hygiene and housing conditions and a substitute for proper animal health management [60]. For these reasons, the WHO advocates the phasing out of the use of antimicrobials for growth promotion. In Europe, the prohibition of the utilisation of antibiotics for the purpose of growth enhancement was implemented in 2006. However, according to the World Organisation for Animal Health, it remains permitted in a minimum of 40 countries globally, the majority of which are situated in the USA [57]. The establishment of the 1969 Swann Committee marked a pivotal point in the efforts to address the One Health dimensions of antimicrobial use in food animals. The Committee introduced a novel regulatory approach for the use of antibiotics in food animals, advocating a cautious limitation of certain commonly used antibiotic feeds. Consequently, a clear distinction was introduced in Europe between antibiotics intended for use in farm animals and those intended for veterinary use [61]. This distinction was not made in the United States or Canada. It should be noted that there are notable differences in the ways that antimicrobials are employed in companion animals (e.g., dogs, cats, pet birds and horses) compared to food-producing animals. The utilisation of antimicrobials in companion animals is comparable to that in humans, as exemplified by the fact that a majority of classes of antimicrobials utilised by humans are employed for animals, including classes of antimicrobials of great importance to human medicine, such as broad-spectrum beta-lactams and quinolones [62]. In veterinary medicine, it is preferable to utilise antibiotics that have not been employed in human medicine, particularly those that possess a narrow spectrum and that are designed to minimise or avoid the use of 'drug cocktails' wherever feasible. It is only through the judicious use of these drugs that their therapeutic efficacy can be maintained and the emergence of resistant microorganisms prevented or reduced. Some antimicrobial compounds have been in use for decades without the emergence of resistance, while other antimicrobials exhibit a slower rate of resistance development. Among the latter, vancomycin is regarded as highly efficacious for the treatment of infection when other commonly used antimicrobial agents are ineffective. Nevertheless, the rising incidence of vancomycin resistance, particularly in healthcare settings, represents a significant concern, given that vancomycin-resistant enterococci (VRE) have been identified as a leading cause of infection-related mortality [63]. Despite collaborative initiatives and supportive regulatory measures introduced in multiple countries, antibiotics in livestock are employed at a significantly elevated rate than is necessary. Of greater concern, a considerable proportion of countries persist in utilizing one or more critically important antimicrobials, such as colistin. The most recent Antimicrobial Use in Animals Report, published in May 2024 by WOAH, indicates an alarming 2% global increase in antibiotic use between 2019 and 2021, following several years of significant downward trends [61]. The European Union permits the therapeutic usage of approved antimicrobials in animals, including fluoroquinolones and other antibiotics essential to human health. However, their usage is subject to limitations, such as the restriction on employing third-generation cephalosporins in poultry. The extensive use of fluoroquinolones in poultry flocks has resulted in the development of resistance to these antibiotics among isolates of Campylobacter jejuni in various countries. Notably, this phenomenon has not been observed in Australia, a country where fluoroquinolones have never been approved for use in livestock [54]. It is well established that the use of different antimicrobial substances belonging to the same class of antibiotics favours the survival of bacteria that possess genes for the same resistance mechanism, a phenomenon known as cross-resistance. In Denmark, the use of avoparcin, a vancomycin analogue, as a growth-promoting agent in poultry farming has been identified as a contributing factor in the observed increase in VRE among chickens. The subsequent ban of vancomycin in 1995 in Denmark was found to be associated with a significant reduction in the prevalence of VRE in chicken faecal samples [64]. A similar phenomenon was observed with regard to the reduction of resistance to erythromycin (a macrolide) among E. faecium and E. faecalis isolates from swine. This occurred following the rapid decrease in the use of tylosin (also a macrolide) as a growth promoter [65]. The use of drugs should be employed only when other measures are either impractical or ineffective. It is the responsibility of farmers to regularly monitor the health of their animals and to contact a veterinary surgeon when there are any changes in the animals’ general health status, in order to ensure that early diagnoses are made and that any infected animals are isolated as soon as possible. It is crucial that veterinarians play an instrumental role in this context, ensuring the appropriate use of drugs. This entails providing instructions to farmers regarding the doses and schedules of treatment, which should be based on clinical evidence and, where possible, laboratory tests. It is also imperative to consider the training of personnel working on farms. The correct mixing of powdered medicines into water or liquid feed, and the appropriate cleaning of feed boxes, can prevent the dangerous accumulation of previous residues and minimise the dispersion of pharmacologically active ingredients into the environment [54]. The following section presents a number of potential preventative and corrective measures to address the issue of antibiotic resistance in livestock.
- The prohibition of the routine administration of antibiotics on farms in order to compensate for inadequate hygiene standards and to stimulate growth.
- It is recommended that there be a reduction in intensive farming and an increase in outdoor rearing in order to reduce overcrowding and stress, which are known to cause routine disease.
- A higher minimum weaning age for piglets is proposed as a means of reducing the incidence of weaning diarrhoea.
- It is recommended that animal health be monitored and that infected animals be isolated in order to prevent the spread of disease through the process of metaphylaxis.
- It is recommended that drugs be administered only after a careful clinical assessment and laboratory analysis have been conducted.
- It is of the utmost importance to maintain the highest standards of hygiene at breeding sites.
6. Antimicrobial Resistance from a One Health Perspective
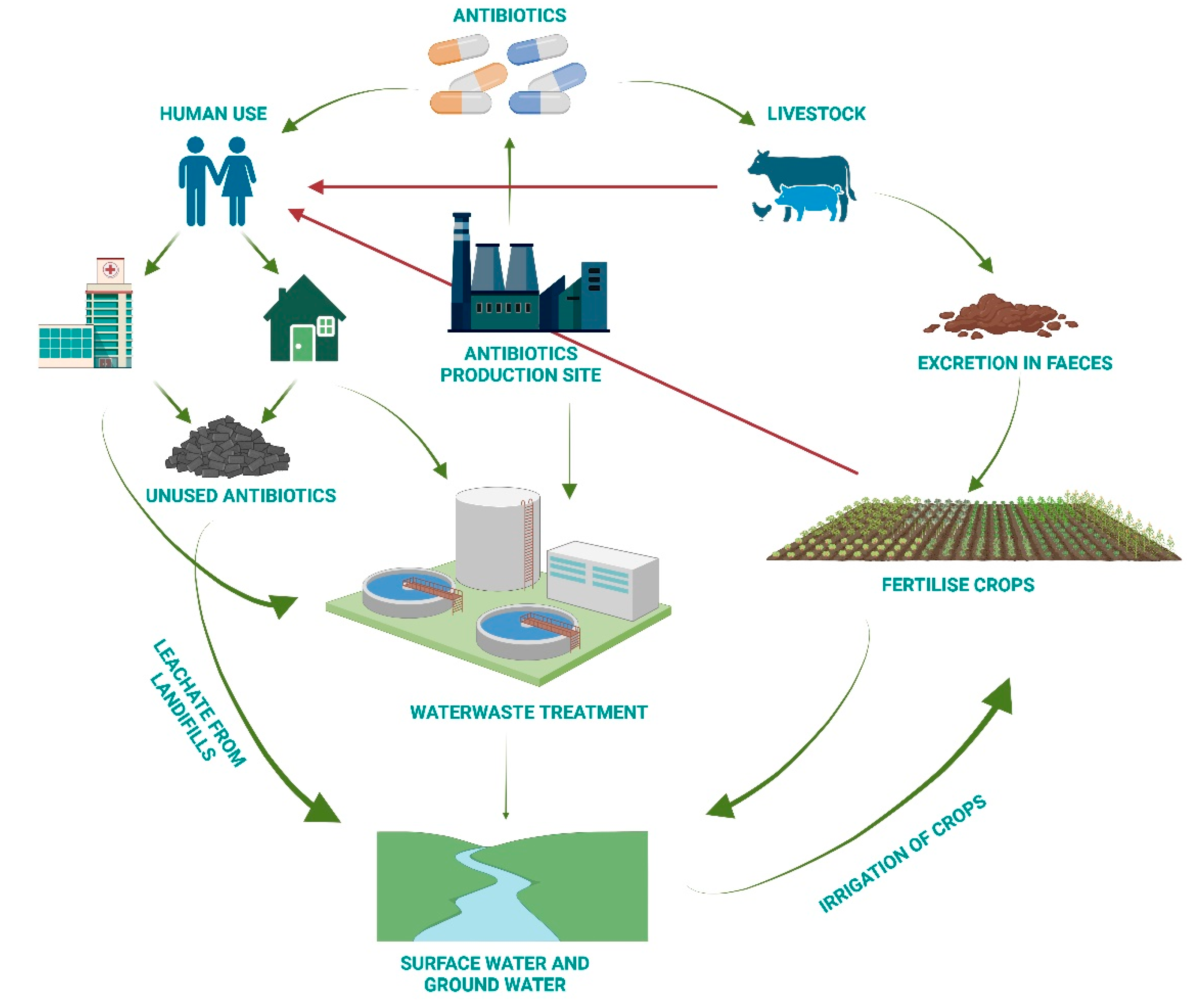
While there are notable discrepancies between countries in the pace of regulatory reform pertaining to the use of antibiotics in animals, a considerable number of amendments have been implemented in this domain over the past 15 years, largely driven by concerns about the impact on human health [13]. A noteworthy example is the diffusion of 16S rRNA methylases (as the armA gene), an enzyme that has the capacity to block aminoglycosides. The enzyme was initially isolated from a Klebsiella pneumoniae strain, which was isolated from a human urinary tract infection. Subsequently, the enzyme was identified in an Escherichia coli strain isolated from a pig [66]. The condition demonstrates the necessity for coordinated surveillance of human and animal isolates in order to prevent cross-species transfer of antimicrobial resistance genes and the subsequent evolution of antibiotic resistance. Given that the majority of these methylases are located on mobile genetic elements such as phages and plasmid-mediated transposons, they are readily transferred between bacterial species via horizontal transfer. Consequently, they play a pivotal role in the development and dissemination of bacterial resistance to antibiotics in a variety of environments, including companion animals, food, wastewater treatment plants and clinical settings [67]. As an additional illustrative example, one might consider colistin. Colistin has been employed in human and veterinary medicine for over half a century. Nevertheless, there are several significant differences between its utilisation in these two contexts. Firstly, colistin is nephrotoxic and neurotoxic, which has led to its discontinuation as a human medicine but not as a veterinary drug. Secondly, colistin is extensively employed in veterinary medicine, either for therapeutic or prophylactic purposes, particularly for the control of diarrhoeal diseases in pigs and poultry. Currently, colistin represents a last line of defence for intravenous use in the management of multidrug-resistant Gram-negative infections, including carbapenem-resistant Acinetobacter baumannii and Enterobacteriaceae, which are predominantly observed in intensive care settings [68]. The dissemination of resistance to this antibiotic amongst microorganisms is of considerable concern, particularly given that this appears to be driven by the extensive use of colistin in animals, rather than in humans. The plasmid-mediated colistin resistance (mcr-1) gene has been identified in a variety of organisms, including wildlife, food animals, humans, and the environment. The gene was first identified in China, which accounts for the majority of global colistin consumption in veterinary medicine. Nevertheless, its utilisation in Europe is also considerable. To date, a greater number of plasmid-mediated colistin resistance genes (mcr-2, mcr-3, mcr-4, mcr-5) have been reported in different bacterial species, often in conjunction with genes that have the ability to hydrolyse penicillins, cephalosporins, monobactams and carbapenems [69]. Although concerns regarding antimicrobial resistance initially focus on antimicrobial use in animal feeds, subsequent research has demonstrated that the environment plays a crucial role in this phenomenon. It has been well-documented that when antimicrobials are administered in a clinical setting, the majority of active molecules are secreted by the host, whether human or animal, through urine or faeces [13]. Although some antibiotics, such as carbapenems and isoniazid, are only intended for human use, the majority of antimicrobial classes are utilised in both humans and animals (e.g. erythromycin and ampicillin), with few other classes limited to veterinary use. Furthermore, some other antimicrobials, such as streptomycin, are used for the bacterial disease control of fruit, such as apples and pears, citrus, and some vegetables. The antimicrobials used in aquaculture are not only persistent in the fish products, but also remain in the aquatic environment for a long time, thus exerting a selective pressure [7]. The active molecules, in conjunction with the bacteria and mobile genetic elements, are transported to wastewater, where they are dispersed and ultimately shared among bacteria, including environmental bacteria. Consequently, antimicrobial-resistant genes can be identified not only in clinically significant bacteria, but also in environmental bacteria when wastewater and environmental reservoirs are examined [70]. From the perspective of One Health, which prioritises antimicrobial resistance, there is a pressing need to focus on preventive and remedial actions that can counteract the spread of dangerous multi-resistant strains in the environment through wastewater. Antimicrobial residues that enter surface waters are often present in concentrations that are insufficient to kill bacteria but high enough to promote the development of resistant bacteria and resistance genes. Wastewater treatment facilities for municipal and hospital effluents represent a significant repository for antibiotics and their metabolites. For example, Rodriguez-Mozaz et al. (2020) reported the detection of 53 antibiotics in the final effluent of wastewater treatments from seven countries in Europe. The study identified a range of antibiotics, including penicillin, cephalosporins, tetracyclines, sulphonamides, and nitroimidazole [71]. The active principle of the drug is not completely metabolised; rather, a significant proportion is excreted through urine and faeces, along with a portion of resistant bacteria in the organism. It is also important to consider that in many cases, the disposal of unused drugs does not occur in an appropriate manner, which contributes to the entry of drug residues into common drains. Moreover, the discharge of pharmaceuticals into waterways from industrial production sites must be considered. It is evident that wastewater treatment does not always result in the complete elimination of residual substances. Moreover, European and American regulations currently lack established limits for antimicrobial concentrations. Furthermore, in low-income countries, the absence of sewage systems, inadequate treatment technologies and the prevalence of practices such as the discharge of wastewater into rivers all contribute to the development of dangerous human health risks through cross-contamination [30,71].
The following section presents a number of potential preventative and corrective actions:
- a.
- Increase awareness of the recycling of expired drugs in appropriate containers.
- b.
- Conduct research into new technologies for wastewater treatment.
- c.
- Take action on treatment facilities to minimise residual traces.
- d.
- Select the process that removes the greatest quantity of antibiotics.
- e.
- Set rigorous limits for antibiotic concentrations in water.
Figure 2.
Sources and potential destinations of antibiotics in the environment. The principal sources of antibiotic residue dispersion in the environment are antibiotic production, human use and livestock farming. The persistence of these substances at major wastewater treatment facilities, the leaching of these substances into the soil from landfills and the use of contaminated water all contribute to the development of potential human health risks.
Figure 2.
Sources and potential destinations of antibiotics in the environment. The principal sources of antibiotic residue dispersion in the environment are antibiotic production, human use and livestock farming. The persistence of these substances at major wastewater treatment facilities, the leaching of these substances into the soil from landfills and the use of contaminated water all contribute to the development of potential human health risks.
7. A Multi-Step Plan to Fight Antimicrobial Resistance
The spectre of a "post-antibiotic" era has prompted the implementation of numerous policy initiatives, the majority of which acknowledge the pivotal role of individual behaviours and choices in promoting the judicious use of antimicrobials and preventing the dissemination of infections. In accordance with the One Health approach, the WHO developed the global action plan (AMR-GAP) in 2015 with the objective of implementing all the necessary actions to impede the emergence and spread of resistant bacteria, reinforce One Health surveillance, enhance diagnostic techniques for the identification and characterisation of resistant bacteria, and accelerate research and development of new antibiotics and therapies. This was followed by the formulation of numerous national action plans (AMR-NAP) in various countries [72]. The set of strategies employed in the fight against AMR encompasses the following: AMR surveillance systems, antimicrobial stewardship programmes, pharmaceutical policies (including limits on antibiotic use without prescription and restrictions on counterfeit, substandard antimicrobials), information-based strategies, as well as mass information campaigns, the implementation of Infection Prevention and Control (IPC) programmes and the encouragement of the use of vaccines, are all examples of strategies that can be employed in the fight against AMR. The WHO defines surveillance as the continuous, systematic collection, analysis and interpretation of health-related data that is necessary for the planning, implementation and evaluation of public health practice. This process enables the identification of the scale of the AMR problem, the emergence of new AMR, the spread of a particular resistance, and the association of a certain outbreak with a particular resistance [73]. Global surveillance of antimicrobial consumption and resistance should address three fronts: 1) monitoring consumption in animals and humans; 2) monitoring resistance proportions of resistant microorganism-drug combinations, along with their health effects on humans; 3) investigating the genetic basis of their resistance. The Global Antimicrobial Resistance and Use Surveillance System (GLASS) is the inaugural global initiative that collects national data on antimicrobial resistance for a select group of bacterial pathogens that are commonly associated with human infections. Despite the close collaboration between GLASS and AMR regional networks and the ongoing efforts to improve laboratory and surveillance capacity, various challenges and gaps still exist in the quality of data provided by the current systems. In the context of animal health, a comprehensive global framework for the collection, analysis and dissemination of AMR data remains lacking [74]. In regard to the consumption of antimicrobials in animals, the World Organization for Animal Health has, in collaboration with Food and Agriculture Organization of the United Nations and the World Health Organization, created a global database on antimicrobial agents intended for use in animals. The database was launched in October 2015. In contrast, there are no formal, standardized global efforts to measure antimicrobial concentrations or antimicrobial-resistant bacteria and genes in the environment, specifically in plants and crops, soil and water systems. This lack of data makes it challenging to accurately quantify the extent of the challenge in these sectors [23,43]. The creation of efficient surveillance networks depends on a number of factors, including the communities involved, the variations in data and sample collection methods, as well as microbial testing procedures and data sharing policies. The difficulties encountered in logistics and a lack of resources, coupled with the issues surrounding data management, act as significant obstacles to the implementation of reliable and collaborative AMR surveillance, thereby resulting in a non-representative nature of the available data. The expansion of laboratory network capacity can facilitate the rapid detection of AMR, the identification of new threats and the development of strategies to prevent the emergence of infections. Furthermore, the AMR-GAP acknowledges the significance of optimising antibiotic utilisation, emphasising the role of antimicrobial stewardship programmes (ASPs) in achieving this objective. Antimicrobial stewardship (AMS) can be defined as the practice of regulating the use of antimicrobials in a way that preserves the effectiveness of the antimicrobials in question while ensuring their continued availability to those who need them [75]. The implementation of AMS programs necessitates the formation of a specialized and dedicated team, in addition to the establishment of a data repository that provides a clear understanding of the prevailing circumstances within the nation and facilitates the development of a tailored program that aligns with the local context. From the perspective of One Health, the implementation of an effective AMS programme must include interventions targeting the prescribing behaviours of both human and animal healthcare professionals. Furthermore, efforts must be made to promote responsible antibiotic manufacturing practices, ensure the safe disposal of unused antibiotics, and implement effective waste management strategies to promote responsible antibiotic use throughout the product's lifespan. Furthermore, the optimal use of antibiotics within veterinary medicine must be optimised [22,76].
|
BOX 1: Focus on measures of infection control in hospitals. A bundle can be defined as a set of a few evidence-based practices that, when applied together and correctly, result in an improvement in the quality and outcome of processes that is greater than that achieved through the implementation of the practices separately. Bundles exist for different types of patients and different contexts (for example, bundles for the prevention of sepsis and for the management of catheters). It is also of paramount importance to implement infection control strategies, related to the local epidemiological context, in addition to adherence to standard hygiene precautions such as the use of personal protective equipment and hand washing. These strategies include specific measures to be used to treat infected patients and contain the spread of infection to other patients admitted to the same operating unit. Furthermore, it is of the utmost importance to implement infection control strategies that are aligned with the local epidemiological context. In addition, it is imperative to adhere to standard hygiene precautions, including the use of personal protective equipment and handwashing. Such strategies encompass the implementation of specific measures to be employed in the treatment of infected patients and the containment of the spread of infection to other patients admitted to the same operating unit. In particular, the following measures may be considered: 1. It is recommended that all individuals who may be at risk of multidrug resistance (MDR) bacteria (i.e. those who have previously been hospitalised, transferred from other departments, or have a history of previous infections) undergo screening upon admission to the hospital. 2. In the event of an infected patient, it is recommended that they be isolated, and any potential contacts should be placed in single rooms or, if necessary, in cohorts. 3. It is of the utmost importance that the environment in which the patient with an infectious disease is situated be thoroughly sanitised. 4. The distribution of healthcare personnel and equipment to the infected patient. The primary obstacle to the effective implementation of these regulations is frequently the dearth of sufficient financial resources to employ a sufficient number of adequately trained personnel and the lack of suitable premises for the isolation of patients. As a potential alternative proposal, one may consider the approach proposed by the French AP-HP outbreak control group in their prospective studies conducted in multi-hospital centres in France. In the work of Fournier et al., it is demonstrated how, in settings where it is not feasible to assign dedicated staff to each individual patient, hospitals have adopted the strategy of reorganising healthcare. This method involves initiating care on the ward from contact patients and concluding with infected patients, with the aim of minimising the potential for contamination. The implementation of this and other control measures has led to a statistically significant reduction in the incidence of outbreaks caused by antibiotic-resistant bacteria. |
The absence of a universal definition of AMS across sectors contributes to a lack of clarity, impeding communication on AMS and AMR between different sectors and making it challenging to identify how stewardship can manifest in concrete actions. Another strategy that has been highlighted is the enhancement of diagnostic use. The advent of new diagnostic technologies, such as rapid diagnostic tests, has the potential to inform medical decisions and curtail the unnecessary use of antibiotics. These tests facilitate the rapid acquisition of information about patients, which can inform the appropriate course of treatment and reduce the likelihood of antibiotic prescriptions being issued unnecessarily. Similarly, the enhancement of biosecurity in farm settings, the promotion of infection prevention and control practices and the improvement of human and veterinary vaccination coverage are widely recognised strategies for the prevention of the spread of infections and the avoidance of the unnecessary demand for antibiotics [77]. The Global Action Plan (GAP) advocates for enhanced national antimicrobial resistance awareness, with particular focus on diverse target groups within human, animal, and agricultural sectors. This includes incorporating AMR as an integral component of various awareness campaigns, educational programs, training initiatives, certification procedures, and development strategies across diverse domains. Moreover, the implementation of food safety policies is a viable approach to preventing foodborne illness in food establishments. A growing body of literature suggests that a range of food safety and hygiene policies, referred to as hazard analysis and critical control points (HACCP)-based interventions, can help to reduce the emergence of foodborne illnesses throughout the food supply chain. The training is designed to provide food service workers with the knowledge and skills necessary to maintain personal hygiene, implement safe food preparation techniques, and store food in an appropriate and safe manner [73]. Finally, AMR-GAP emphasises the significance of adequate funding to guarantee the implementation of the policies outlined in the various action plans. In contrast, a lack of adequate funding allocated to the issue of antimicrobial resistance represents a further impediment, particularly in countries with a medium to low level of socioeconomic development. In such countries, governments may not accord the highest priority to funding for these initiatives, perceiving them as being less urgent than other matters of public concern. The design and implementation of AMR policies necessitates interactions with a multitude of stakeholders from various sectors with disparate interests, influence, and positions regarding the policy options (e.g., healthcare providers, veterinarians, farmers, and pharmaceutical manufacturers, along with local and national regulatory bodies). These interactions have the potential to enhance the probability of attaining the policy objectives. Additionally, it is crucial to recognize that the efficacy of AMR policies can undergo changes over time, necessitating adaptations in the conceptualization and implementation of these policies to accommodate evolving necessities within a given environment. This underscores the necessity for enhanced strategies from a multi-sectoral perspective, including intensified efforts to address persisting deficiencies [72].
Figure 3.
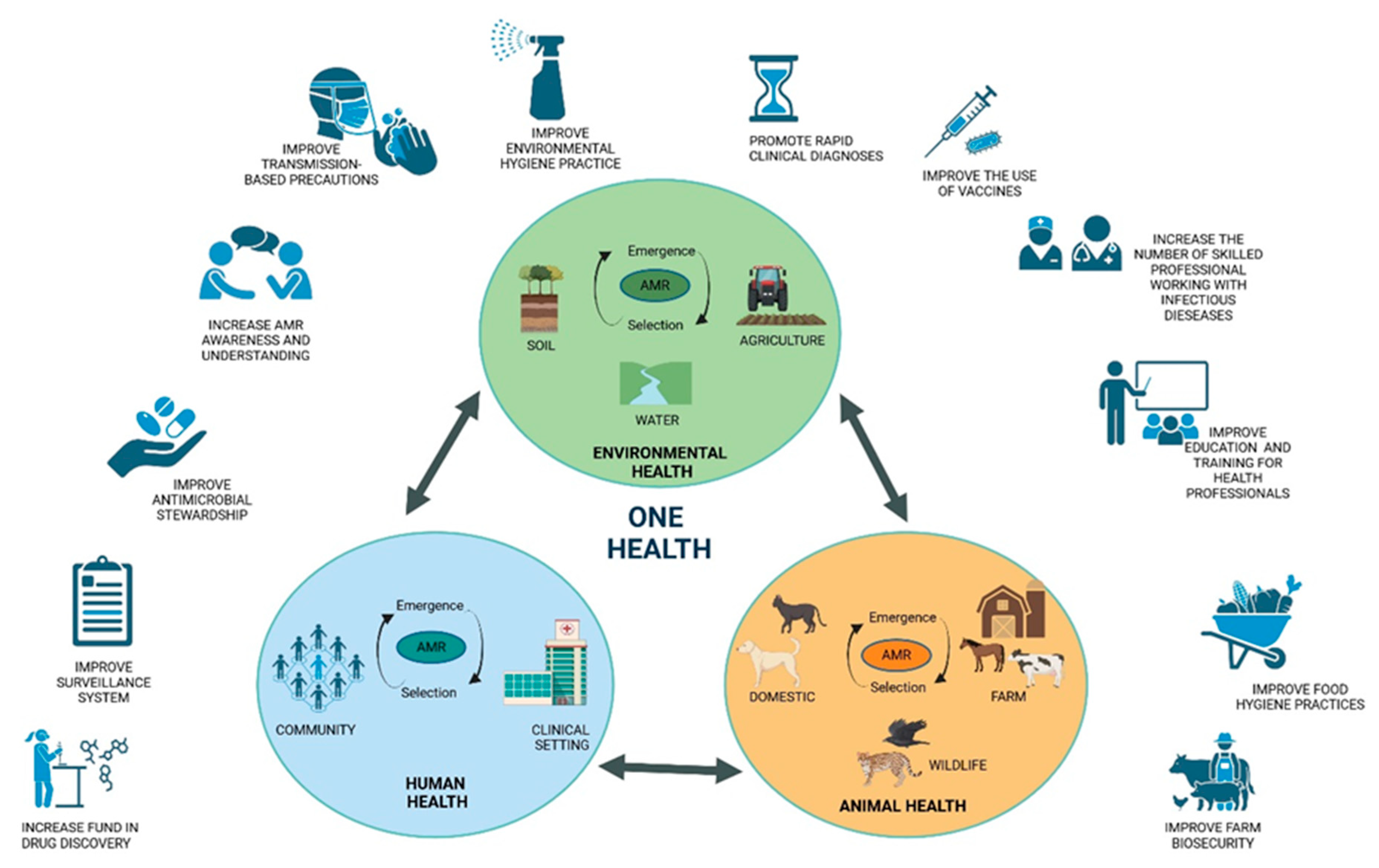
The Challenge of Antimicrobial Resistance in the Concept of One Health. The following schematic representation depicts the emergence, selection and dissemination of AMR within and between each of the "One Health" sectors (human-environment-animal), together with the multisectoral policies that should be implemented to prevent and reduce the health effects of AMR.
Figure 3.
The Challenge of Antimicrobial Resistance in the Concept of One Health. The following schematic representation depicts the emergence, selection and dissemination of AMR within and between each of the "One Health" sectors (human-environment-animal), together with the multisectoral policies that should be implemented to prevent and reduce the health effects of AMR.
8. What Can Each of Us Do to Contribute to the Solution?
It is necessary to consider a hypothetical scenario in which the prevalence of infectious diseases renders them effectively untreatable in humans, animals and plants. Such a scenario could become a reality as bacteria, viruses and parasites become resistant to antimicrobial agents. Antimicrobial resistance represents one of the most pressing health concerns of our time, with economic reports indicating that the potential reduction in life expectancy worldwide by 2035 could be as much as two years. There are solutions to this global threat, and it is of the utmost importance that everyone plays a role in combating it (box 2).
| Box 2. The potential impact of each individual on the global threat of antimicrobial resistance. |
| If you are a citizen: |
| - Do not use antibiotics to treat colds or viral diseases; - Do not take antibiotics without a prescription; - Follow your doctor's instructions; Do not stop or extend treatment without approval; - Do not use antibiotics prescribed for other people or used for previous treatments; - Dispose of expired or unused medications in the appropriate containers; - Never visit at-risk subjects (infants, elderly, immunocompromised, hospitalized) if you are sick; - Learn more about antibiotic resistance and spread the news. |
| If you are a health worker: |
| - Administer antibiotics after careful clinical evaluation; - Choose the right antibiotic based on laboratory results; - Carefully evaluate the case before administering an antibiotic as prophylaxis; - Do effective antimicrobial stewardship; - Strictly observe hand hygiene practices and take all necessary precautions before visiting a patient; - Minimize contact between colonized and noncolonized patients. |
| If you are a member of health management: |
| - Monitor infections in the hospital; - Create guidelines for controlling alert microorganisms; - Ensure hygiene and infection control regulations are followed; - Ensure the environment is properly disinfected; - Correct errors promptly; - Ensure there are enough protective equipment and health staff; - Train health care workers. |
| If you are a breeder: |
| - Don't use antibiotics to make your animals grow; - Don't use antibiotics to prevent infections; - Don't use antibiotics without your vet's advice; - Follow your vet's instructions; - Look after your animals and keep an eye on their health; - Keep your production site clean. |
| If you are a policymaker: |
| - Raise awareness about antibiotic use and AMR; - Train the next generation; - Collect antibiotic use data to encourage research; - Invest in new technologies and drugs. |
9. Conclusion
Antimicrobial resistance represents one of the most significant challenges to public health and modern medicine to date. The global scale of the problem presents a significant risk of irreparably undermining the achievement of the Sustainable Development Goals. The most recent data from the World Health Organization (WHO) indicates that 1.27 million deaths were directly attributable to antibiotic-resistant bacteria in 2019, with an estimated additional 5 million deaths. The pandemic from COVID-19 and the indiscriminate use of antibiotics in the early period, in the absence of effective antivirals or in an attempt to counteract the numerous co-infections, may have further aggravated the burden. A multitude of collaborative initiatives and strategic frameworks have been established by various countries with the objective of combating AMR. However, the actual implementation of these plans is constrained by significant discrepancies between states. The most effective approach to combating AMR is to adopt a "One Health" approach, which considers the health of humans, animals, and the environment. In order to effectively combat AMR through the One Health approach, it is of paramount importance to establish international collaborations among nations. Such global actions play a pivotal role in accelerating global progress, innovating in order to guarantee a safe future for all and providing resources to enable sustainable responses. Furthermore, the establishment of these partnerships represents a pivotal step in the comprehensive monitoring of antimicrobial usage and consumption across animal, human, and environmental domains. This is of paramount significance, as enhancing global surveillance of drug resistance represents a vital step in effectively combating AMR. It can be reasonably assumed that these outcomes will be achieved when antimicrobials are used for therapy purposes only, and only rarely for prophylaxis, and never for growth promotion. Furthermore, it is imperative that rigorous control measures be implemented to guarantee that only a limited quantity of antimicrobials are introduced into the ecosystem, with a particular focus on minimising the prevalence of antibiotic-resistant bacterial strains.
Author Contributions
Conceptualization, C.B., E.P. and S.De.G.; figure and preparation of the original draft S. De.G., E.P. A.M., G.P., D.G. and S.Z.; proofreading and editing, C.B., G.M. E.P. and S.De.G. All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chala, B.; Hamde, F. Emerging and Re-emerging Vector-Borne Infectious Diseases and the Challenges for Control: A Review. Frontiers in public health 2021, 9, 715759. [Google Scholar] [CrossRef] [PubMed]
- Berndtson, A.E. Increasing Globalization and the Movement of Antimicrobial Resistance between Countries. Surgical infections 2020, 21, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Matuszewska, M.; Murray, G.G.R.; Ba, X.; Wood, R.; Holmes, M.A.; Weinert, L.A. Stable antibiotic resistance and rapid human adaptation in livestock-associated MRSA. eLife 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Muteeb, G.; Rehman, M.T.; Shahwan, M.; Aatif, M. Origin of Antibiotics and Antibiotic Resistance, and Their Impacts on Drug Development: A Narrative Review. Pharmaceuticals 2023, 16. [Google Scholar] [CrossRef] [PubMed]
- Vidovic, N.; Vidovic, S. Antimicrobial Resistance and Food Animals: Influence of Livestock Environment on the Emergence and Dissemination of Antimicrobial Resistance. Antibiotics 2020, 9. [Google Scholar] [CrossRef]
- Uddin, T.M.; Chakraborty, A.J.; Khusro, A.; Zidan, B.R.M.; Mitra, S.; Emran, T.B.; Dhama, K.; Ripon, M.K.H.; Gajdacs, M.; Sahibzada, M.U.K.; et al. Antibiotic resistance in microbes: History, mechanisms, therapeutic strategies and future prospects. Journal of infection and public health 2021, 14, 1750–1766. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Alam Tumpa, M.A.; Zehravi, M.; Sarker, M.T.; Yamin, M.; Islam, M.R.; Harun-Or-Rashid, M.; Ahmed, M.; Ramproshad, S.; Mondal, B.; et al. An Overview of Antimicrobial Stewardship Optimization: The Use of Antibiotics in Humans and Animals to Prevent Resistance. Antibiotics 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, G.; De Gaetano, S.; Midiri, A.; Zummo, S.; Biondo, C. The Challenge of Overcoming Antibiotic Resistance in Carbapenem-Resistant Gram-Negative Bacteria: "Attack on Titan". Microorganisms 2023, 11. [Google Scholar] [CrossRef]
- Benmerzouga, I.; Al-Zammay, S.A.; Al-Shammari, M.M.; Alsaif, S.A.; Alhaidan, T.M.; Aljofan, M. Practices of patients consuming antibiotics and knowledge about antibiotic resistance in Hail region - Saudi Arabia. Future science OA 2019, 5, FSO420. [Google Scholar] [CrossRef]
- Wu, G.; Lu, J.; Liu, D.; He, Y. Characteristics and risk factors of secondary bacterial infections in COVID-19 patients. Antimicrobial stewardship & healthcare epidemiology : ASHE 2023, 3, e156. [Google Scholar] [CrossRef]
- Biondo, C.; Ponzo, E.; Midiri, A.; Ostone, G.B.; Mancuso, G. The Dark Side of Nosocomial Infections in Critically Ill COVID-19 Patients. Life 2023, 13. [Google Scholar] [CrossRef]
- Endale, H.; Mathewos, M.; Abdeta, D. Potential Causes of Spread of Antimicrobial Resistance and Preventive Measures in One Health Perspective-A Review. Infection and drug resistance 2023, 16, 7515–7545. [Google Scholar] [CrossRef] [PubMed]
- Salam, M.A.; Al-Amin, M.Y.; Salam, M.T.; Pawar, J.S.; Akhter, N.; Rabaan, A.A.; Alqumber, M.A.A. Antimicrobial Resistance: A Growing Serious Threat for Global Public Health. Healthcare 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Abbas, S. The challenges of implementing infection prevention and antimicrobial stewardship programs in resource-constrained settings. Antimicrobial stewardship & healthcare epidemiology : ASHE 2024, 4, e45. [Google Scholar] [CrossRef]
- Pokharel, S.; Shrestha, P.; Adhikari, B. Antimicrobial use in food animals and human health: time to implement 'One Health' approach. Antimicrobial resistance and infection control 2020, 9, 181. [Google Scholar] [CrossRef] [PubMed]
- Manyi-Loh, C.; Mamphweli, S.; Meyer, E.; Okoh, A. Antibiotic Use in Agriculture and Its Consequential Resistance in Environmental Sources: Potential Public Health Implications. Molecules 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, U.; Moodley, A.; Osbjer, K. Antimicrobial resistance at the livestock-human interface: implications for Veterinary Services. Revue scientifique et technique 2021, 40, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Polianciuc, S.I.; Gurzau, A.E.; Kiss, B.; Stefan, M.G.; Loghin, F. Antibiotics in the environment: causes and consequences. Medicine and pharmacy reports 2020, 93, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Ma, L.; Yu, Q.; Yang, J.; Su, W.; Hilal, M.G.; Li, X.; Zhang, S.; Li, H. The source, fate and prospect of antibiotic resistance genes in soil: A review. Frontiers in microbiology 2022, 13, 976657. [Google Scholar] [CrossRef]
- Visca, A.; Di Gregorio, L.; Clagnan, E.; Bevivino, A. Sustainable strategies: Nature-based solutions to tackle antibiotic resistance gene proliferation and improve agricultural productivity and soil quality. Environmental research 2024, 248, 118395. [Google Scholar] [CrossRef]
- Fu, Y.; Dou, Q.; Smalla, K.; Wang, Y.; Johnson, T.A.; Brandt, K.K.; Mei, Z.; Liao, M.; Hashsham, S.A.; Schaffer, A.; et al. Gut microbiota research nexus: One Health relationship between human, animal, and environmental resistomes. mLife 2023, 2, 350–364. [Google Scholar] [CrossRef] [PubMed]
- Aslam, B.; Khurshid, M.; Arshad, M.I.; Muzammil, S.; Rasool, M.; Yasmeen, N.; Shah, T.; Chaudhry, T.H.; Rasool, M.H.; Shahid, A.; et al. Antibiotic Resistance: One Health One World Outlook. Frontiers in cellular and infection microbiology 2021, 11, 771510. [Google Scholar] [CrossRef] [PubMed]
- Pandey, S.; Doo, H.; Keum, G.B.; Kim, E.S.; Kwak, J.; Ryu, S.; Choi, Y.; Kang, J.; Kim, S.; Lee, N.R.; et al. Antibiotic resistance in livestock, environment and humans: One Health perspective. Journal of animal science and technology 2024, 66, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Joji, R.M.; Shahid, M. Evolution and implementation of One Health to control the dissemination of antibiotic-resistant bacteria and resistance genes: A review. Frontiers in cellular and infection microbiology 2022, 12, 1065796. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, G.; Midiri, A.; Gerace, E.; Biondo, C. Bacterial Antibiotic Resistance: The Most Critical Pathogens. Pathogens 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Armitage, J.P. Behavioral responses in bacteria. Annual review of physiology 1992, 54, 683–714. [Google Scholar] [CrossRef]
- Munita, J.M.; Arias, C.A. Mechanisms of Antibiotic Resistance. Microbiology spectrum 2016, 4. [Google Scholar] [CrossRef]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: a global multifaceted phenomenon. Pathogens and global health 2015, 109, 309–318. [Google Scholar] [CrossRef]
- Michael, C.A.; Dominey-Howes, D.; Labbate, M. The antimicrobial resistance crisis: causes, consequences, and management. Frontiers in public health 2014, 2, 145. [Google Scholar] [CrossRef]
- Larsson, D.G.J.; Flach, C.F. Antibiotic resistance in the environment. Nature reviews. Microbiology 2022, 20, 257–269. [Google Scholar] [CrossRef]
- Mullis, M.M.; Rambo, I.M.; Baker, B.J.; Reese, B.K. Diversity, Ecology, and Prevalence of Antimicrobials in Nature. Frontiers in microbiology 2019, 10, 2518. [Google Scholar] [CrossRef] [PubMed]
- Perron, G.G.; Whyte, L.; Turnbaugh, P.J.; Goordial, J.; Hanage, W.P.; Dantas, G.; Desai, M.M. Functional characterization of bacteria isolated from ancient arctic soil exposes diverse resistance mechanisms to modern antibiotics. PloS one 2015, 10, e0069533. [Google Scholar] [CrossRef] [PubMed]
- Hasan, C.M.; Dutta, D.; Nguyen, A.N.T. Revisiting Antibiotic Resistance: Mechanistic Foundations to Evolutionary Outlook. Antibiotics 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Reygaert, W.C. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS microbiology 2018, 4, 482–501. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Hassan, K.A. The Gram-negative permeability barrier: tipping the balance of the in and the out. mBio 2023, 14, e0120523. [Google Scholar] [CrossRef] [PubMed]
- Aghapour, Z.; Gholizadeh, P.; Ganbarov, K.; Bialvaei, A.Z.; Mahmood, S.S.; Tanomand, A.; Yousefi, M.; Asgharzadeh, M.; Yousefi, B.; Kafil, H.S. Molecular mechanisms related to colistin resistance in Enterobacteriaceae. Infection and drug resistance 2019, 12, 965–975. [Google Scholar] [CrossRef]
- Michaelis, C.; Grohmann, E. Horizontal Gene Transfer of Antibiotic Resistance Genes in Biofilms. Antibiotics 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Aminov, R.I. Horizontal gene exchange in environmental microbiota. Frontiers in microbiology 2011, 2, 158. [Google Scholar] [CrossRef]
- von Wintersdorff, C.J.; Penders, J.; van Niekerk, J.M.; Mills, N.D.; Majumder, S.; van Alphen, L.B.; Savelkoul, P.H.; Wolffs, P.F. Dissemination of Antimicrobial Resistance in Microbial Ecosystems through Horizontal Gene Transfer. Frontiers in microbiology 2016, 7, 173. [Google Scholar] [CrossRef]
- Turner, N.A.; Sharma-Kuinkel, B.K.; Maskarinec, S.A.; Eichenberger, E.M.; Shah, P.P.; Carugati, M.; Holland, T.L.; Fowler, V.G., Jr. Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research. Nature reviews. Microbiology 2019, 17, 203–218. [Google Scholar] [CrossRef]
- Lade, H.; Joo, H.S.; Kim, J.S. Molecular Basis of Non-beta-Lactam Antibiotics Resistance in Staphylococcus aureus. Antibiotics 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Zahari, N.I.N.; Engku Abd Rahman, E.N.S.; Irekeola, A.A.; Ahmed, N.; Rabaan, A.A.; Alotaibi, J.; Alqahtani, S.A.; Halawi, M.Y.; Alamri, I.A.; Almogbel, M.S.; et al. A Review of the Resistance Mechanisms for beta-Lactams, Macrolides and Fluoroquinolones among Streptococcus pneumoniae. Medicina 2023, 59. [Google Scholar] [CrossRef]
- Selvarajan, R.; Obize, C.; Sibanda, T.; Abia, A.L.K.; Long, H. Evolution and Emergence of Antibiotic Resistance in Given Ecosystems: Possible Strategies for Addressing the Challenge of Antibiotic Resistance. Antibiotics 2022, 12. [Google Scholar] [CrossRef]
- Lee, K.; Kim, D.W.; Lee, D.H.; Kim, Y.S.; Bu, J.H.; Cha, J.H.; Thawng, C.N.; Hwang, E.M.; Seong, H.J.; Sul, W.J.; et al. Mobile resistome of human gut and pathogen drives anthropogenic bloom of antibiotic resistance. Microbiome 2020, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Lerner, H.; Berg, C. The concept of health in One Health and some practical implications for research and education: what is One Health? Infection ecology & epidemiology 2015, 5, 25300. [Google Scholar] [CrossRef]
- Destoumieux-Garzon, D.; Mavingui, P.; Boetsch, G.; Boissier, J.; Darriet, F.; Duboz, P.; Fritsch, C.; Giraudoux, P.; Le Roux, F.; Morand, S.; et al. The One Health Concept: 10 Years Old and a Long Road Ahead. Frontiers in veterinary science 2018, 5, 14. [Google Scholar] [CrossRef]
- Ng, V.; Sargeant, J.M. A quantitative approach to the prioritization of zoonotic diseases in North America: a health professionals' perspective. PloS one 2013, 8, e72172. [Google Scholar] [CrossRef] [PubMed]
- Angora, E.K.; Allienne, J.F.; Rey, O.; Menan, H.; Toure, A.O.; Coulibaly, J.T.; Raso, G.; Yavo, W.; N'Goran, E.K.; Utzinger, J.; et al. High prevalence of Schistosoma haematobium x Schistosoma bovis hybrids in schoolchildren in Cote d'Ivoire. Parasitology 2020, 147, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Viet, H.; Lam, S.; Nguyen-Mai, H.; Trang, D.T.; Phuong, V.T.; Tuan, N.D.A.; Tan, D.Q.; Thuy, N.T.; Thuy Linh, D.; Pham-Duc, P. Decades of emerging infectious disease, food safety, and antimicrobial resistance response in Vietnam: The role of One Health. One health 2022, 14, 100361. [Google Scholar] [CrossRef]
- Mazzeo, A.; Tremonte, P.; Lombardi, S.J.; Caturano, C.; Correra, A.; Sorrentino, E. From the Intersection of Food-Borne Zoonoses and EU Green Policies to an In-Embryo One Health Financial Model. Foods 2022, 11. [Google Scholar] [CrossRef]
- Mettenleiter, T.C.; Markotter, W.; Charron, D.F.; Adisasmito, W.B.; Almuhairi, S.; Behravesh, C.B.; Bilivogui, P.; Bukachi, S.A.; Casas, N.; Becerra, N.C.; et al. The One Health High-Level Expert Panel (OHHLEP). One health outlook 2023, 5, 18. [Google Scholar] [CrossRef]
- Alkorta, I.; Garbisu, C. Expanding the focus of the One Health concept: links between the Earth-system processes of the planetary boundaries framework and antibiotic resistance. Reviews on environmental health 2024. [Google Scholar] [CrossRef] [PubMed]
- Palma, E.; Tilocca, B.; Roncada, P. Antimicrobial Resistance in Veterinary Medicine: An Overview. International journal of molecular sciences 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Caneschi, A.; Bardhi, A.; Barbarossa, A.; Zaghini, A. The Use of Antibiotics and Antimicrobial Resistance in Veterinary Medicine, a Complex Phenomenon: A Narrative Review. Antibiotics 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Osei Sekyere, J. Antibiotic Types and Handling Practices in Disease Management among Pig Farms in Ashanti Region, Ghana. Journal of veterinary medicine 2014, 2014, 531952. [Google Scholar] [CrossRef] [PubMed]
- Credille, B.; Berghaus, R.D.; Jane Miller, E.; Credille, A.; Schrag, N.F.D.; Naikare, H. Antimicrobial Metaphylaxis and its Impact on Health, Performance, Antimicrobial Resistance, and Contextual Antimicrobial Use in High-Risk Beef Stocker Calves. Journal of animal science 2024, 102. [Google Scholar] [CrossRef] [PubMed]
- Economou, V.; Gousia, P. Agriculture and food animals as a source of antimicrobial-resistant bacteria. Infection and drug resistance 2015, 8, 49–61. [Google Scholar] [CrossRef]
- McEwen, S.A.; Collignon, P.J. Antimicrobial Resistance: a One Health Perspective. Microbiology spectrum 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Abreu, R.; Semedo-Lemsaddek, T.; Cunha, E.; Tavares, L.; Oliveira, M. Antimicrobial Drug Resistance in Poultry Production: Current Status and Innovative Strategies for Bacterial Control. Microorganisms 2023, 11. [Google Scholar] [CrossRef]
- Collignon, P.J.; McEwen, S.A. One Health-Its Importance in Helping to Better Control Antimicrobial Resistance. Tropical medicine and infectious disease 2019, 4. [Google Scholar] [CrossRef]
- Patel, S.J.; Wellington, M.; Shah, R.M.; Ferreira, M.J. Antibiotic Stewardship in Food-producing Animals: Challenges, Progress, and Opportunities. Clinical therapeutics 2020, 42, 1649–1658. [Google Scholar] [CrossRef]
- Joosten, P.; Ceccarelli, D.; Odent, E.; Sarrazin, S.; Graveland, H.; Van Gompel, L.; Battisti, A.; Caprioli, A.; Franco, A.; Wagenaar, J.A.; et al. Antimicrobial Usage and Resistance in Companion Animals: A Cross-Sectional Study in Three European Countries. Antibiotics 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Ayobami, O.; Willrich, N.; Reuss, A.; Eckmanns, T.; Markwart, R. The ongoing challenge of vancomycin-resistant Enterococcus faecium and Enterococcus faecalis in Europe: an epidemiological analysis of bloodstream infections. Emerging microbes & infections 2020, 9, 1180–1193. [Google Scholar] [CrossRef]
- Lu, K.; Asano, R.; Davies, J. Antimicrobial resistance gene delivery in animal feeds. Emerging infectious diseases 2004, 10, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.R.; Fedorka-Cray, P.J.; Barrett, J.B.; Ladely, S.R. Effects of tylosin use on erythromycin resistance in enterococci isolated from swine. Applied and environmental microbiology 2004, 70, 4205–4210. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Zeng, M.; Zhang, N.; Wang, M.; Gu, B.; Li, J.; Jin, H.; Xiao, W.; Li, Z.; Zhao, H.; et al. Prevalence of 16S rRNA Methylation Enzyme Gene armA in Salmonella From Outpatients and Food. Frontiers in microbiology 2021, 12, 663210. [Google Scholar] [CrossRef] [PubMed]
- Hazards, E.P.o.B.; Koutsoumanis, K.; Allende, A.; Alvarez-Ordonez, A.; Bolton, D.; Bover-Cid, S.; Chemaly, M.; Davies, R.; De Cesare, A.; Herman, L.; et al. Role played by the environment in the emergence and spread of antimicrobial resistance (AMR) through the food chain. EFSA journal. European Food Safety Authority 2021, 19, e06651. [Google Scholar] [CrossRef]
- Tietgen, M.; Sedlaczek, L.; Higgins, P.G.; Kaspar, H.; Ewers, C.; Gottig, S. Colistin Resistance Mechanisms in Human and Veterinary Klebsiella pneumoniae Isolates. Antibiotics 2022, 11. [Google Scholar] [CrossRef]
- Yin, Y.; Qiu, L.; Wang, G.; Guo, Z.; Wang, Z.; Qiu, J.; Li, R. Emergence and Transmission of Plasmid-Mediated Mobile Colistin Resistance Gene mcr-10 in Humans and Companion Animals. Microbiology spectrum 2022, 10, e0209722. [Google Scholar] [CrossRef]
- Mutuku, C.; Gazdag, Z.; Melegh, S. Occurrence of antibiotics and bacterial resistance genes in wastewater: resistance mechanisms and antimicrobial resistance control approaches. World journal of microbiology & biotechnology 2022, 38, 152. [Google Scholar] [CrossRef]
- Rodriguez-Mozaz, S.; Vaz-Moreira, I.; Varela Della Giustina, S.; Llorca, M.; Barcelo, D.; Schubert, S.; Berendonk, T.U.; Michael-Kordatou, I.; Fatta-Kassinos, D.; Martinez, J.L.; et al. Antibiotic residues in final effluents of European wastewater treatment plants and their impact on the aquatic environment. Environment international 2020, 140, 105733. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.W.K.; Millar, B.C.; Moore, J.E. Antimicrobial Resistance (AMR). British journal of biomedical science 2023, 80, 11387. [Google Scholar] [CrossRef] [PubMed]
- Majumder, M.A.A.; Rahman, S.; Cohall, D.; Bharatha, A.; Singh, K.; Haque, M.; Gittens-St Hilaire, M. Antimicrobial Stewardship: Fighting Antimicrobial Resistance and Protecting Global Public Health. Infection and drug resistance 2020, 13, 4713–4738. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Wang, Y.; Mulchandani, R.; Van Boeckel, T.P. Global surveillance of antimicrobial resistance in food animals using priority drugs maps. Nature communications 2024, 15, 763. [Google Scholar] [CrossRef] [PubMed]
- Do, P.C.; Assefa, Y.A.; Batikawai, S.M.; Reid, S.A. Strengthening antimicrobial resistance surveillance systems: a scoping review. BMC infectious diseases 2023, 23, 593. [Google Scholar] [CrossRef]
- Ashiru-Oredope, D.; Garraghan, F.; Olaoye, O.; Krockow, E.M.; Matuluko, A.; Nambatya, W.; Babigumira, P.A.; Tuck, C.; Amofah, G.; Ankrah, D.; et al. Development and Implementation of an Antimicrobial Stewardship Checklist in Sub-Saharan Africa: A Co-Creation Consensus Approach. Healthcare 2022, 10. [Google Scholar] [CrossRef]
- Nashwan, A.J.; Barakat, M.; Niaz, F.; Tariq, S.; Ahmed, S.K. Antimicrobial Resistance: Stewardship and One Health in the Eastern Mediterranean Region. Cureus 2024, 16, e58478. [Google Scholar] [CrossRef]

Table 1.
The mode of action and targets of antibacterial drugs.
| Mode of action | Drug class | Targets | Resistance | Specific drugs |
|---|---|---|---|---|
|
inhibition of cell wall synthesis |
Beta-Lactams |
Penicillin-binding protein |
blaZ mecA ampC bla |
Penicillins, Cephalosporins, Carbapenems Monobactams |
| Glycopeptides |
Peptidoglycan subunits | van | Vancomicin | |
| Polypeptides | Peptidoglycan subunits |
bceAB bceRS bacA |
Bacitracin | |
|
inhibition of protein synthesis |
Aminoglycosides | 30 s subunit |
aadA1 erm |
Gentamicin, Tobramycin Amikacin, Streptomicin |
| Tetracyclines | 30 s subunit |
tetM tetX |
Metacycline, Doxycycline, Minocycline | |
| Amphenicoli | 50 s subunit | cat | Chloramphenicol | |
| Macrolides | 50 s subunit | erm | Azithromycin Clarithromycin Erythromycin Fidaxomicin |
|
| Lincosamides | 50 s subunit | erm | Clindamycin | |
|
disruption of cell membrane integrity |
Polymyxins | Lipopolysaccharides |
mcr1 arnBCADTEF |
Colistin |
| Lipopeptides | Depolarizing the cell membrane | mprF | Daptomycin | |
|
inhibition of nucleic acid synthesis |
Quinolones | DNA |
gyrA grlA |
Ciprofloxacin Levofloxacin |
| Rifamycin | RNA |
drrABC, rpoB |
Rifampicin | |
| Antimetabolite activity | Pyrimidines + Sulfonamides | Folic acid synthesis enzymes | sul dfr | Trimethoprim-Sulfamethoxazole |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



